$12 Billion Over 10 Years: Pharma, Medical Devices Industries Shell Out Direct Payments to US Physicians
By Brenda Baletti, Ph.D. | The Defender | April 11, 2024
The pharmaceutical and medical devices industries paid physicians more than $12 billion over 10 years, according to a study published last month in JAMA.
The analysis found the industries made 85,087,744 payments totaling $12.13 billion to 826,313 physicians — 57.1% of practicing physicians across 39 specialties.
Orthopedic surgeons, neurologists and psychiatrists, and cardiologists received the most money. Trauma surgeons and pediatric surgeons received the least.
The drugs with the highest payouts were blood thinners Xarelto and Eliquis, along with Humira, an immunosuppressant.
The three medical devices with the highest payouts were robotic surgery systems, da Vinci Surgical System and Mako SmartRobotics, and CoreValve Evolut, a heart valve.
“Money given to doctors has a purpose: it is for marketing,” cardiologist Dr. John Mandrola and co-author of the study wrote on his Substack. “If these direct payments to doctors did not work, industry would not spend billions.”
Dr. Andrew Foy, lead author of the paper, told The Defender in an email he thought some people might find the numbers “shocking” and he hoped it would renew interest in having conversations about physician-industry payments and facilitate more research.
The researchers tracked and compared payments made to physicians across and within specialties. They also identified the top 25 drugs and medical devices associated with the largest total payments.
The analysis included only money received for consulting, travel, food, entertainment, education, gifts, grants and honoraria. The researchers excluded other major external funding sources for physicians such as research funding and royalties.
They analyzed data from 2013-2022 in the Open Payments database, established in 2013 by the Physician Payments Sunshine Act as part of the Affordable Care Act.
Legislators designed the Sunshine Act to address growing public concerns about Big Pharma’s influence over doctors. At the time, several studies had shown that increased interaction with pharmaceutical representatives influenced physician prescribing behavior.
The act requires medical product manufacturers to disclose to the Centers for Medicare and Medicaid Services any payments or other transfers of value made to physicians or teaching hospitals. Open Payments publishes the payments on its website.
The analysis found that payments varied significantly across specialties. The highest-paid specialties like orthopedic surgery received $1.36 billion, and neurology and psychology specialties received $1.32 billion. The lowest-paid specialties received substantially less.
Pediatric surgeons and trauma surgeons received only $2.89 million and $6.96 million respectively.
Payments also varied significantly among physicians within the same specialty, with a small number of physicians in each specialty receiving the largest amounts of money — often exceeding $1 million — while the median physician received significantly less, typically less than $100, ranging from zero to $2,339.
“Our paper is a modest analysis. It does not explain the problem of financial conflicts of interest. But it is a lot of money. And it’s highly targeted to lucrative procedures,” Mandrola wrote.
“Industry influence is way too strong,” he added, and commonly results in medical devices being approved “despite dodgy evidence.”
He said many doctors believe collaboration between industry and physicians is a good thing that drives innovation. However, he said, these payments weren’t simply supporting collaboration.
“Most of it, I would argue, is for marketing and goodwill. Goodwill goes a long way to help establish practice patterns.”
Top drugs and devices on list net billions for pharma
The blood thinner Xarelto, used to prevent blood clots from forming due to an irregular heartbeat or after hip or knee replacement surgery, topped the payment list, accounting for $176.3 million.
The drug, made by Bayer and marketed by Janssen Pharmaceuticals, was Bayer’s top drug in 2023, generating about 4.1 billion euros in revenue.
Payments for Eliquis, another blood thinner used to treat the same conditions, amounted to $102.62 million. Pfizer and Bristol-Myers Squibb manufacture Eliquis.
Pfizer in 2023 brought in over $6.7 billion from the drug, its second-most profitable product behind the Comirnaty COVID-19 vaccine. Bristol-Myers Squibb’s sales topped $12 billion.
Eliquis costs U.S. customers 3 to 7 times more than customers in other high-income countries.
Humira, an immunosuppressant used to treat rheumatoid arthritis, psoriasis and other autoimmune conditions paid out $100.17 million to physicians. Over the last two decades, the drug netted over $200 billion for drugmaker AbbieVie, which listed the medication at $50,000 per year.
Bayer, Pfizer, Bristol-Myers Squibb and AbbieVie did not immediately respond to requests for comment.
Other top drugs included diabetes treatments Invokana, Jardiance, and Farxiga, Dupixent, a drug for allergic diseases, and Botox.
The two medical devices topping the list — da Vinci Surgical System, which paid $307.5 million, and Mako SmartRobotics, which paid $50 million — are machines for robotic-assisted surgeries.
Mako focuses on hip and knee replacements. Da Vinci netted approximately $7.12 billion in 2023 and investors were “blown away” by the “robot-fueled growth” of Mako SmartRobotics device installation for hip and knee replacements. Mako’s parent company Stryker made over $20 billion last year.
Several cardiology devices also made the list, including the third-highest payer CoreValve Evolut, another heart valve, Sapien 3 and LifeVest, a wearable defibrillator. They are all part of their parent companies’ multi-billion dollar product portfolios.
Conflicts of interest
The problem of physicians’ financial ties to pharmaceutical companies has plagued the industry for decades and garnered significant media attention.
Perhaps most famously, Purdue Pharma used misleading marketing to make massive profits from sales of opioids, sparking an epidemic. Nearly 645,000 Americans died from opioid overdose between 1999 and 2021.
However, Purdue Pharma’s policy of paying physicians has long been common practice. Research studies during the last two decades have found the vast majority of physicians accept payments and gifts from pharmaceutical companies. Influential studies include those by the Institute of Medicine and the Medicare Payments Advisory Commission that led to the passage of the Sunshine Act.
This latest study and other recent studies show that despite new mechanisms for transparency in payments, the payments continue.
And those payments are particularly high among physicians with prominent roles directing public policy.
For example, last year The New York Times revealed that while advisers at the National Academies of Sciences, Engineering, and Medicine were shaping public policy on opioids, they were also accepting payments from the Sackler family who owned Purdue Pharma.
Last month, The Defender reported that most of the nine new members appointed to the vaccine advisory committee for the Centers for Disease Control and Prevention have received substantial direct payments or research funding from Big Pharma — largely from the companies whose products they will be reviewing.
Foy said he thought a major part of the problem is that physicians and researchers believe that if they make their conflicts of interest transparent, the problem is resolved.
“As if someone cannot be transparent about their conflicts and highly biased at the same time,” he said.
He said that payments don’t necessarily lead directly to prescribing one specific drug for which a payment is received.
Instead, he said, he worries that the payments lead to, “overly enthusiastic recommendations or guidelines from medical organizations to use new products when they have not been sufficiently tested, or where the evidence is not strong enough, to recommend them over old standards or nothing at all (in some cases).”
Industry payments to physicians, Foy said, have a way of “tilting physicians’ sympathy toward industry and the ‘medical advancements’ that come from industry so that they (the physicians) more willingly adopt new products just for the sake of ‘industry advancement’ even if they don’t have a direct COI [conflict of interest] with that particular product.”
Physicians, he said, “become cheerleaders for industry and more open to adopting new products simply due to this attachment.”
For example, he said it is not uncommon at medical conferences for attendees to stand up and cheer results from “late-breaking” research studies whose “benefits are very rarely ever more than marginal, tiny, or ‘teensy-weensy’ at best.”
“I never understood it,” Foy wrote.
Direct payments aren’t the only way industry collaborates with physicians, Foy said.
Industry ads are featured on the homepage of medical journals and ads bombard physicians at major medical conferences.
He said this gives the impression that “the event is built around industry and its involvement.”
He said he doesn’t think that anyone tries to hide the relationships. “The main reason being, at least in my opinion, is that many physicians, perhaps even the majority, believe that physician-industry collaboration is a net benefit to patients and society,” he said.
“I don’t necessarily share that view; however, I don’t believe there is strong, objective evidence to support one side or the other.”
Brenda Baletti Ph.D. is a reporter for The Defender. She wrote and taught about capitalism and politics for 10 years in the writing program at Duke University. She holds a Ph.D. in human geography from the University of North Carolina at Chapel Hill and a master’s from the University of Texas at Austin.
This article was originally published by The Defender — Children’s Health Defense’s News & Views Website under Creative Commons license CC BY-NC-ND 4.0. Please consider subscribing to The Defender or donating to Children’s Health Defense.
WHO Official Admits Vaccine Passports May Have Been a Scam
By Paul D. Thacker | The DisInformation Chronicle | April 12, 2024
The World Health Organization’s Dr. Hanna Nohynek testified in court that she advised her government that vaccine passports were not needed but was ignored, despite explaining that the COVID vaccines did not stop virus transmission and the passports gave a false sense of security. The stunning revelations came to light in a Helsinki courtroom where Finnish citizen Mika Vauhkala is suing after he was denied entry to a café for not having a vaccine passport.
Dr. Nohynek is chief physician at the Finnish Institute for Health and Welfare and serves as the WHO’s chair of Strategic Group of Experts on immunization. Testifying yesterday, she stated that the Finnish Institute for Health knew by the summer of 2021 that the COVID-19 vaccines did not stop virus transmission
During that same 2021 time period, the WHO said it was working to “create an international trusted framework” for safe travel while EU members states began rolling out COVID passports. The EU Digital COVID Certificate Regulation passed in July 2021 and more than 2.3 billion certificates were later issued. Visitors to France were banned if they did not have a valid vaccine passport which citizens had to carry to buy food at stores or to use public transport.
But Dr. Nohynek testified yesterday that her institute advised the Finnish government in late 2021 that COVID passports no longer made sense, yet certificates continued to be required. Finnish journalist Ike Novikoff reported the news yesterday after leaving the Helsinki courtroom where Dr. Nohynek spoke.

Dr. Nohynek’s admission that the government ignored scientific advice to terminate vaccine passports proved shocking as she is widely embraced in global medical circles. Besides chairing the WHO’s strategic advisory group on immunizations, Dr. Nohynek is one of Finland’s top vaccine advisors and serves on the boards of Vaccines Together and the International Vaccine Institute.
The EU’s digital COVID-19 certification helped establish the WHO Global Digital Health Certification Network in July 2023. “By using European best practices we contribute to digital health standards and interoperability globally—to the benefit of those most in need,” stated one EU official.
Finnish citizen Mika Vauhkala created a website discussing his case against Finland’s government where he writes that he launched his lawsuit “to defend basic rights” after he was denied breakfast in December 2021 at a Helsinki café because he did not have a COVID passport even though he was healthy. “The constitution of Finland guarantees that any citizen should not be discriminated against based on health conditions among other things,” Vauhkala states on his website.
Vauhkala’s lawsuit continued today in Helsinki district court where British cardiologist Dr. Aseem Malhotra will testify that, during the COVID pandemic, some authorities and medical professionals supported unethical, coercive, and misinformed policies such as vaccine mandates and vaccine passports, which undermined informed patient consent and evidence-based medical practice.
You can read Dr. Malhotra’s testimony here.
CDC Demonstrates Failure of Public Health Management of the COVID-19 Pandemic
BY DR. HARVEY RISCH | APRIL 1, 2024
In so many words—and data—CDC has quietly admitted that all of the indignities of the Covid-19 pandemic management have failed: the masks, the distancing, the lockdowns, the closures, especially the vaccines, all of it failed to control the pandemic. It’s not like we didn’t know that all this was going to fail, because we said so as events unfolded early on in 2020, that the public health management of this respiratory virus was almost completely opposite to principles that had been well established through the influenza period, in 2006. The spread of a new virus with replication factor R0 of about 3, with more than one million cases across the country by April 2020, with no potentially virus-sterilizing vaccine in sight for at least several months, almost certainly made this infection eventually endemic and universal.
Covid-19 starts as an annoying, intense, uncomfortable flu-like illness, and for most people, ends uneventfully two-three weeks later. Thus, management of the Covid-19 pandemic should not have relied upon counts of cases or infections, but on numbers of deaths, numbers of people hospitalized or with serious long-term outcomes of the infection, and of serious health, economic and psychological damages caused by the actions and policies made in response to the pandemic, in that order of decreasing priorities. Even though numbers of Covid cases correlate with these severe manifestations, that is not a justification for case numbers to be used as the actionable measure, because Covid-19 infection mortality is estimated to range below 0.1% in the mean across all ages, and post-infection immunity provides a public good in protecting people from severe reinfection outcomes for the great majority who do not get serious “long-Covid” on first infection.
Nevertheless, once the Covid-19 vaccines were rolled out, with a new large wave of the delta strain spreading across the US in July-August 2021 even after eight months of the vaccines taken by half of Americans, instead of admitting policy error that the Covid vaccines do not much control virus spread, our public health administration doubled down, attempting then to compel vaccination on as many more people as could be threatened by mandates. That didn’t work out too well as seen when the large Omicron wave hit the country during December 2021-January 2022 in spite of some 10% more of the population getting vaccinated from September through December of 2021.
A typical mandate example: in September 2021, Washington Governor Jay Inslee issued Emergency Proclamation 21-14.2, requiring Covid-19 vaccination for various groups of state workers. In the proclamation, the stated goal was, “WHEREAS, COVID-19 vaccines are effective in reducing infection and serious disease, and widespread vaccination is the primary means we have as a state to protect everyone … from COVID-19 infections.” That is, the stated goal was to reduce the number of infections.
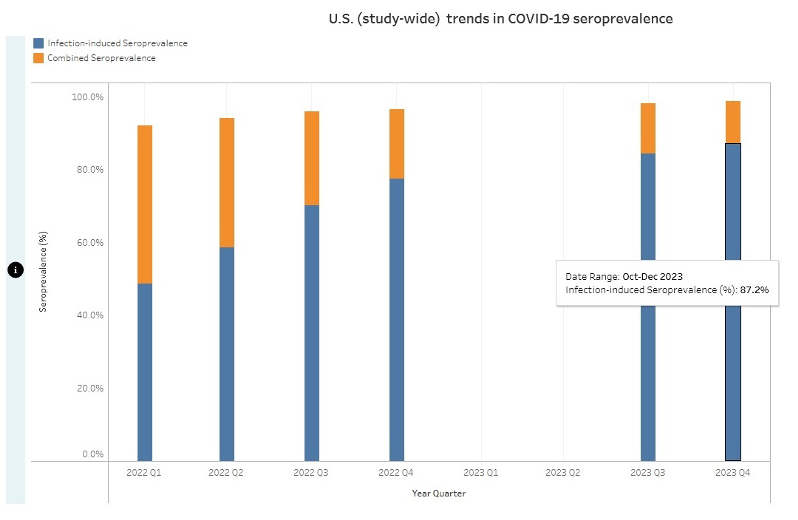
What the CDC recently reported (see chart below), however, is that by the end of 2023, cumulatively, at least 87% of Americans had anti-nucleocapsid antibodies to and thus had been infected with SARS-CoV-2, this in spite of the mammoth, protracted and booster-repeated vaccination campaign that led to about 90% of Americans taking the shots. My argument is that by making policies based on number of infections a higher priority than ones based on the more serious but less common consequences of both infections and policy damages, the proclaimed goal of the vaccine mandate to reduce spread failed in that 87% of Americans eventually became infected anyway.
In reality, neither vaccine immunity nor post-infection immunity were ever able fully to control the spread of the infection. On August 11, 2022, CDC stated, “Receipt of a primary series alone, in the absence of being up to date with vaccination through receipt of all recommended booster doses, provides minimal protection against infection and transmission (3,6). Being up to date with vaccination provides a transient period of increased protection against infection and transmission after the most recent dose, although protection can wane over time.” Public health pandemic measures that “wane over time” are very unlikely to be useful for control of infection spread, at least without very frequent and impractical revaccinations every few months.
Nevertheless, infection spread per se is not of consequence, because count of infections is not and should not have been the main priority of public health pandemic management. Rather, the consequences of the spread and the negative consequences of the policies invoked should have been the priorities. Our public health agencies chose to prioritize a failed policy of reducing the spread rather than reducing the mortality or the lockdown and school and business closure harms, which led to unnecessary and avoidable damage to millions of lives. We deserved better from our public health institutions.
Harvey A. Risch, MD, PhD
References Cited
1. Inglesby TV, Nuzzo JB, O’Toole T, Henderson DA. Disease mitigation measures in the control of pandemic influenza. Biosecur Bioterror. 2006;4(4):366-75. https://www.liebertpub.com/doi/10.1089/bsp.2006.4.366
2. Ramirez VB. What Is “R-naught”? Gauging Contagious Infections. Healthline, June 14, 2023. https://www.healthline.com/health/r-naught-reproduction-number
3. Worldometer. United States Coronavirus Cases. March 28, 2024. https://www.worldometers.info/coronavirus/country/us/
4. Gupta S. Was I wrong about the Covid infection fatality rate?. UnHerd, April 5, 2023. https://unherd.com/newsroom/how-wrong-was-i-on-covid-ifr/
5. Inslee J. PROCLAMATION BY THE GOVERNOR AMENDING PROCLAMATIONS 20-05 and 20-14: 21-14.2. COVID-19 VACCINATION REQUIREMENT. Issued September 27, 2021. https://governor.wa.gov/sites/default/files/proclamations/21-14.2%20-%20COVID-19%20Vax%20Washington%20Amendment%20(tmp).pdf
6. CDC. 2022-2023 Nationwide COVID-19 Infection- and Vaccination-Induced Antibody Seroprevalence (Blood donations). March 22, 2024. https://covid.cdc.gov/covid-data-tracker/#nationwide-blood-donor-seroprevalence-2022
7. Our World in Data. Total number of people who received at least one dose of COVID-19 vaccine. Downloaded March 27, 2024. https://ourworldindata.org/grapher/people-vaccinated-covid
8. Massetti GM, Jackson BR, Brooks JT, Perrine CG, Reott E, Hall AJ, Lubar D, Williams IT, Ritchey MD, Patel P, Liburd LC, Mahon BE. Summary of Guidance for Minimizing the Impact of COVID-19 on Individual Persons, Communities, and Health Care Systems – United States, August 2022. MMWR Morb Mortal Wkly Rep. 2022;71(33):1057-1064. https://www.cdc.gov/mmwr/volumes/71/wr/mm7133e1.htm
Dr. Harvey A. Risch MD, PhD is a Professor Emeritus of Epidemiology at the Yale School of Public Health and a guest contributor for Peter Navarro’s Taking Back Trump’s America
Austrian officials must have known all along that “covid” was a nothing-burger
Startling disclosures from official documents
BY JONATHAN ENGLER | APRIL 08, 2024
A colleague in HART has drawn my attention to this article on “TKP”, an Austrian sceptical website. As usual, machine translation does a good enough job to discern the gist for us non-German speakers.
It is reported that in an official government report entitled Virus Epidemiological Information No. 18/20 published in April 2020:
Prof. Judith Aberle reported on evidence of immunity against SARS-CoV-2 through T cells in blood samples from Austria going back to 2018 and in some other countries even as far back as 2015. It would probably have been the duty of the MedUni Vienna to make the public aware of the findings about widespread immunity.
The article goes on to state that Prof. Aberle disclosed that:
… in studies from the USA, Singapore, Germany, the Netherlands and Great Britain, SARS -CoV- 2 specific T -Cells were detected:
“Depending on the study, T cells against SARS-CoV-2 could be detected in 20 to 50 percent of blood donors. In Austria, too, in our previous studies we found T cells against various SARS-CoV-2 proteins in 30 percent of the blood samples from 2018-2019, i.e. before the pandemic.”
The actual reports in question are available here, and the specific one cited above (report 18-20) here.
Sure enough, Google translate confirms the Professor states the following:
Interestingly, T cells against SARS-CoV-2 can also be found in some pPeople who have not yet had contact with the new coronavirus. Show that several international studies from the USA, Singapore, Germany, the Netherlands and Great Britain. Those used for these investigations Blood samples come from healthy people from 2015-2018, i.e. a long time before SARS-CoV-2 first appeared in China. Depending on the study, 20 to 50 percent of blood donors have T cells detected against SARS-CoV-2 become. In our previous studies in Austria we have also found 30 Percent of blood samples from 2018-2019, i.e. before the pandemic, T cells found against various SARS-CoV-2 proteins. We now know about it Studies from the USA and Germany show that it is primarily about memory T cells are involved in infections with those four known Coronaviruses have been formed that cause relatively mild respiratory infections cause. They are called HCoV-OC43, -229E, -HKU1 and -NL63, occur worldwide and cause around 30% of colds However, you can get it back every year.
So, she is basically suggesting that the T cell reactivity comes from previous exposure to other coronaviruses.
However, as the article states:
The other explanation, which is at least as plausible, would be that SARS-CoV-2 spread significantly before 2020.
Whether “the virus” was “novel” or not seems to be an academic question, unless the new virus was causing lots of extra illness or death. But – as would be expected for something for which so many people seemed able to mount an adequate immune defence – it wasn’t.
The article then links to a piece from a few days ago about a recent episode of a TV show held in “Hangar 7” in which various state officials either maintained that covid was a terrible disease or that it couldn’t have been known back in spring 2020 that it wasn’t.
But, as the article points out:
- In an 9 April 2020 edition of the same program John Ioniodis’s data suggesting very low mortality was discussed.
- On April 10th , a TKP article was published in which not only Ionnidis’ findings were presented, but also the French study by Didier Raoult with the telling title ” SARS-CoV-2: fear versus data “, as well as a study from Wuhan with similar infection mortality.
- Even the decidedly mainstream vienna.at on April 7, 2020 reported that: “Analysis shows: Covid-19 victim curve corresponds to “normal” mortality”, concluding: “The Covid-19 victim curve in Austria roughly corresponds to the “normal” mortality for men and women in the individual age groups”.

Translated: Analysis shows: Covid-19 victim curve corresponds to “normal” mortalitySo the article states plainly that:
So the facts were well known, people knew about it.
It goes on to quote Dr Christian Fiala of the Karolinska Institut:
Ultimately, the alleged danger of the virus was only “scaled up” in order to get the mRNA into people. The virus was pretty insignificant and I think the many discussions about its laboratory origin were smoke grenades or media hype to attribute a meaning to the virus that it didn’t even have. It was never about the virus, it was about the mRNA.
This business concept is now obvious.
It will be interesting to see if these revelations result in any more indignation in the Austrian population than we are seeing in other countries – where, considering the scale of the lies and harms caused, voices are extraordinarily muted.
Disasters Cost More Than Ever — But Not Because of Climate Change
From the archives, a look back and an update

Fundraiser from 2014. We learned from Wikileaks that Tom Steyer, the Center for American Progress, and Michael Mann were behind the curtain. Just $10? Deplatforming me should get at least $15!
By Roger Pielke | The Honest Broker | March 26, 2024
This week marks my final spring break as a professor at the University of Colorado Boulder. Ten years ago this week, during spring break while on vacation with my family, I was dealing with the consequences of what appeared to be an online mob seeking to get me fired from Nate Silver’s 538 where I had just been hired as a writer.
My first piece for 538 was a summary of recent IPCC report consensus conclusions on disasters and extreme events. The apparent mobbing worked.1 I soon lost my position as a writer at 538.
Not long after, I was under investigation by a member of Congress.2 I lost the support of my university and my role in the center I had founded, so I moved across campus to work on sports governance.3 I have little doubt that I remained employed only thanks to academic tenure. It was quite an experience.
Two years later, in 2016, courtesy of the Wikileaks publication of John Podesta’s emails, it was revealed that the Center for American Progress, funded by billionaire Tom Steyer and in collaboration with the ever-present Michael Mann, had been engaged in a well-funded campaign to delegitimize my research, hurt my career, and to have me removed as a writer at 538.4
I can draw a straight line from those events a decade ago to where I am today. And given where I am today, I wouldn’t change a thing. I have no hard feelings towards Nate — He got played and did what he felt he had to at the time.
Below, I have reproduced my first column at 538 in 2014 that was apparently so threatening to some in the climate advocacy community.5 I also add a post-script below. How does it hold up?

In the 1980s, the average annual cost of natural disasters worldwide was $50 billion. In 2012, Superstorm Sandy met that mark in two days. As it tore through New York and New Jersey on its journey up the east coast, Sandy became the second-most expensive hurricane in American history, causing in a few hours what just a generation ago would have been a year’s worth of disaster damage.
Sandy’s huge price tag fit a trend: Natural disasters are costing more and more money. See the graph below, which shows the global tally of disaster expenses for the past 24 years. It’s courtesy of Munich Re, one of the world’s largest reinsurance companies, which maintains a widely used global loss data set. (All costs are adjusted for inflation.)

In the last two decades, natural disaster costs worldwide went from about $100 billion per year to almost twice that amount. That’s a huge problem, right? Indicative of more frequent disasters punishing communities worldwide? Perhaps the effects of climate change? Those are the questions that Congress, the World Bank and, of course, the media are asking. But all those questions have the same answer: no.
When you read that the cost of disasters is increasing, it’s tempting to think that it must be because more storms are happening. They’re not. All the apocalyptic “climate porn” in your Facebook feed is solely a function of perception. In reality, the numbers reflect more damage from catastrophes because the world is getting wealthier. We’re seeing ever-larger losses simply because we have more to lose — when an earthquake or flood occurs, more stuff gets damaged. And no matter what President Obama and British Prime Minister David Cameron say, recent costly disasters are not part of a trend driven by climate change. The data available so far strongly shows they’re just evidence of human vulnerability in the face of periodic extremes.
To identify changes in extreme weather, it’s best to look at the statistics of extreme weather. Fortunately, scientists have invested a lot of effort into looking at data on extreme weather events, and recently summarized their findings in a major United Nations climate report, the fifth in a series dating back to 1990. That report concluded that there’s little evidence of a spike in the frequency or intensity of floods, droughts, hurricanes and tornadoes. There have been more heat waves and intense precipitation, but these phenomena are not significant drivers of disaster costs. In fact, today’s climate models suggest that future changes in extremes that cause the most damage won’t be detectable in the statistics of weather (or damage) for many decades.
On Earth, extreme events don’t happen in a vacuum. Their costs are rising, sure, but so is overall wealth. When we take that graph above and measure disaster cost relative to global GDP, it changes quite a bit.6

Occasionally, big disasters bring outsize costs — especially the Kobe earthquake in 1995, Hurricane Katrina in 2005 and the Honshu earthquake in 2011 — but the overall trend in disaster costs proportional to GDP since 1990 has stayed fairly level. Of course, wealthy countries hold all of the sway in worldwide cost estimates, which tips the scales when we’re looking for a “global” perspective on extreme events. U.S. hurricanes, for example, are responsible for 58 percent of the increase in the property losses in the Munich Re global dataset.
That’s just the property bill. There’s a human toll, too, and the data show an inverse relationship between lives lost and property damage: Modern disasters bring the greatest loss of life in places with the lowest property damage, and the most property damage where there’s the lowest loss of life. Consider that since 1940 in the United States 3,322 people have died in 118 hurricanes that made landfall. Last year in a poor region of the Philippines, a single storm, Typhoon Hayain, killed twice as many people.
We can start to estimate how countries may weather crises differently thanks to a 2005 analysis of historical data on global disasters. That study estimated that a nation with a $2,000 per capita average GDP — about that of Honduras — should expect more than five times the number of disaster deaths as a country like Russia, with a $14,000 per capita average GDP.2 (For comparison, the U.S. has a per capita GDP of about $52,000.)
In the 20th century, the human toll of disasters decreased dramatically, with a 92 percent reduction in deaths from the 1930s to the 2000s worldwide. Yet when the Boxing Day Tsunami struck Southeast Asia in 2004, more than 225,000 people died.
So the frequency of disasters still matters, and especially in countries that are ill-prepared for them. After 41 people died in two volcanic eruptions in Indonesia last month, a government official explained the high stakes: “We have 100 million people living in places that are prone to disasters, including volcanoes, earthquakes and floods. It’s a big challenge for the local and central governments.”
When you next hear someone tell you that worthy and useful efforts to mitigate climate change will lead to fewer natural disasters, remember these numbers and instead focus on what we can control. There is some good news to be found in the ever-mounting toll of disaster losses. As countries become richer, they are better able to deal with disasters — meaning more people are protected and fewer lose their lives. Increased property losses, it turns out, are a price worth paying.
Postscript March 2024
As THB readers well know, I have continued the research that was the subject of the column above. Below is an update to the figures in the column above, adjusted just for inflation and with 11 more years of data.
![]()
Inflation adjusted losses, 1990 to 2023.
Below is the second figure showing weather and climate disaster losses as a proportion of global GDP.

Global weather and climate losses as a percent of global GDP, 1990 to 2023.
I’ve published this analysis in the peer-reviewed literature as well:
Pielke, R. (2019). Tracking progress on the economic costs of disasters under the indicators of the sustainable development goals. Environmental Hazards, 18(1), 1-6.
Editors of Top Science Journals to Testify Before House Pandemic Committee, as Critics Call for End of Taxpayer Funding for ‘Corrupt’ Research
By Michael Nevradakis, Ph.D. | The Defender | April 8, 2024
Amid controversy over censorship in peer-reviewed journals, the editors of three major science journals last week received invitations to testify before the U.S. House of Representatives Select Subcommittee on the Coronavirus Pandemic on the relationship between their publications and the federal government.
Rep. Brad Wenstrup (R-Ohio), chair of the subcommittee, sent the letters to the editors-in-chief of The Lancet, Nature and Science, requesting their testimony for an April 16 hearing titled “Academic Malpractice: Examining the Relationship Between Scientific Journals, the Government, and Peer Review.”
According to Wenstrup’s office, the hearing seeks to examine “whether these journals granted the federal government inappropriate access into the scientific review or publishing process,” noting that the journals had previously communicated with Drs. Anthony Fauci, Francis Collins and other health officials.
Nature Medicine published the now infamous “Proximal Origin” paper in March 2020. The paper, which claimed COVID-19 had zoonotic, or natural, origins was subsequently used in attempts to censor proponents of the “lab-leak theory” of the virus’s origin.
In a press release, Wenstrup said:
“Millions of people worldwide relied on Science, Nature, and The Lancet to provide scientifically accurate and impartial research during the COVID-19 pandemic.
“However, documents show that the federal government may have censored and manipulated the sacred scientific review processes at these journals to progress their preferred narrative about the origins of COVID-19.”
Cardiologist Dr. Peter McCullough welcomed the announcement of the hearing. He told The Defender :
“I used the term ‘academic fraud’ in my Nov. 19, 2020, Senate testimony. During the pandemic, for the first time in my career, I saw fraudulent papers published and valid ones retracted after full peer review.
“Publication actions always went in a consistent theme of duality: suppression of early therapeutics for acute COVID-19 and promotion of mRNA COVID-19 vaccines as safe and effective … Manuscripts demonstrating successful home treatment strategies were impeded, and above all, manuscripts disclosing COVID-19 vaccine injuries, disabilities and deaths were swept under the rug.”
Several experts said scientific journals censored non-establishment views but regularly published “fraudulent” papers.
Epidemiologist and public health research scientist M. Nathaniel Mead told The Defender :
“We have faced an unprecedented level of scientific censorship in the past four years, and this has created a climate of fear for the medical-scientific community, compelling many researchers and scholars to practice self-censorship.
“This has fostered a pervasive hesitancy to broach certain topics, even in venues or contexts that are theoretically supportive of free expression. As a result, dissenting viewpoints that could enhance scientific dialogue are stifled.”
According to molecular biologist Richard Ebright, Ph.D., “Science has published two patently unsound and presumably fraudulent papers on the subject of COVID-19 origins, has not retracted these papers, has refused to open inquiries into those papers, and has used its news division to promote the false narrative that science favors a natural origin of COVID-19 and to dismiss contrary evidence and contrary views.”
Mark Blaxill, chief financial officer of the Holland Center, a private autism treatment center, told The Defender, “Policymakers and legislators often defer to scientists, ‘experts’ and the published record. To the extent that the record is corrupted by political forces that lean to one side of legitimate public policy disputes, the journals are tilting the playing field in favor of powerful interests.”
This has resulted in “the increasing politicization of science,” as a result of which “the body of published science is becoming increasingly weaponized,” Blaxill said.
Similarly, journalist Paul D. Thacker, publisher of The Disinformation Chronicle, told The Defender he hopes “Congress has something better planned than just parading the scientists running these journals before the public and berating them for being corrupt, because documents I’ve reported on show these journal editors have no shame.”
Wenstrup: Journal editors ‘seem to want to ignore’ COVID lab-leak theory
Much of the subcommittee’s focus has centered on “The proximal origin of SARS-CoV-2.” Published on March 17, 2020, in Nature Medicine, the paper concluded that a lab leak was not “plausible.” It soon became “one of the single most impactful and influential scientific papers in history.”
A House investigation and Freedom of Information Act requests later revealed that a month before publication, Fauci and Collins reviewed drafts of the paper. A July 2023 report by the subcommittee found that Fauci, key virologists and government officials used the paper to suppress the COVID-19 lab-leak theory.
Speaking on Fox Business’ “Varney & Co.” last week, Wenstrup said the editors-in-chief to whom he sent letters “should want to weigh in on this because they published articles that seem to want to ignore [the lab-leak theory].”
“When anybody had the hypothesis of it being a lab leak theory … they were scrutinized, they were canceled, they were put down,” Wenstrup added. “A published article doesn’t mean that it’s been peer-reviewed and that it’s been going through the scrutiny that it should take from scientists … Just look at ‘Proximal Origin.’”
During an April 17, 2020, White House Coronavirus Task Force press briefing, Fauci told reporters, in the presence of then-President Donald Trump, “There was a study recently that we can make available to you” which showed that COVID-19 “is totally consistent with a jump of a species from an animal to a human.”
“Fauci helped place the ‘Proximal Origin’ paper and then lied about it right under the nose of the president,” Thacker said. “He was thanked by [virologist] Kristian Andersen for his advice in an email, and then he wants to say he had no role in it.”
Wenstrup made a similar observation on “Varney & Co.”:
“‘Proximal Origin’ basically was written by people that were prompted to write it by Dr. Fauci. And all they really talked about was the possibility [that COVID-19] came from nature. If you read this article, it’s full of assumptions and what-ifs, and it completely ignores the lab leak theory.
“And internally, in their discussions, the same authors are saying, ‘Well, we can’t rule out that this came from a lab. It certainly looks engineered.’ So, there’s a problem with using these scientific journals as a be-all end-all.”
Earlier this year, Fauci sat for two days of closed-door interviews with members of the House, during which he reportedly responded with “I don’t recall” over 100 times.
For Thacker, the focus on the “Proximal Origin” paper ignores two other influential scientific papers that also were used try to discredit the “lab-leak theory.”
“This committee has been overly obsessed with ‘Proximal Origin’ … These virologists conspired to launch three different papers into the academic literature. It wasn’t just one paper. You don’t run a propaganda campaign off of just one paper,” Thacker said.
According to Thacker, on Feb. 19, 2020, EcoHealth Alliance’s Peter Daszak and Wellcome Trust’s Jeremy Farrar published a statement in The Lancet that claimed a possible Wuhan lab accident was a “conspiracy theory.”
The statement did not disclose that Daszak was funding research led by Shi Zhengli at the Wuhan Institute of Virology.
On Feb. 26, 2020, scientists working behind the scenes with Zhengli and virologist Ralph Baric, Ph.D., published a commentary in Emerging Microbes & Infections that claimed it was a conspiracy theory to speculate that the pandemic started in a Wuhan lab.
Mead said the pandemic facilitated government intervention in scientific publishing:
“Most of this government influence is happening behind the scenes to avoid the appearance of impropriety. And when a scientific journal such as Nature or Science adopts a rapid publication process for COVID-19-related research … it tends to compromise the quality and reliability of the findings. It also makes it easier for outside influences to dictate the angle or perspective, or overall thrust, of the article in question.
“Beginning in 2020, this collaboration was tightly synchronized so as to allow for rushed authorization of the mRNA vaccines without sufficient risk evaluation and management protocols.”
Mead said this interference limited scientific discourse, adversely impacting the public.
“[During the pandemic] we could not mention the term natural immunity without being castigated or reflexively labeled an ‘anti-vaxxer,’” Mead said. “Early treatment and vaccine safety issues were, of course, also censored.”
Yet, in remarks to The Hill, a spokesperson for subcommittee Democrats accused Republicans of building “an extreme, partisan and conspiratorial narrative against our nation’s public health officials” and have not “revealed a cover-up of the pandemic’s origins nor a suppression of the lab leak theory [by] Dr. Fauci and Dr. Collins.”
Journal editors ‘promote favored narratives and suppress dissent’
Blaxill highlighted the increased use of retractions by scientific and medical journals to silence non-establishment narratives on COVID-19 and other topics. He said:
“One worrisome trend I have seen is the use of retractions rather than public debate to manage scientific disagreements. My experience with the retraction of ‘Autism Tsunami’ was instructive. Our 2021 paper sailed through peer review and was among the most heavily downloaded publications of the year.”
But after criticism of the paper reached the editors of the journal that published the paper, the editors informed Blaxill and his co-authors they intended to “re-review” the paper. A few months later, the paper was retracted.
According to Blaxill, “The retraction process itself is what is broken. Instead of allowing debate to play out in public, through letters and responses in the journal, dissenting opinions and unpopular narratives are canceled.”
Brian Hooker, Ph.D., chief scientific officer for Children’s Health Defense, told The Defender, “In the case of having my own scientific paper retracted in 2014, I know the federal government played a strong role in getting the publication removed from print.”
“When the CDC whistleblower story broke … I was immediately put on notice by the journal (Translational Neurodegeneration ) that the paper would be taken down from their website with a notice of concern. At one point, the journal put a notice on my paper that it was a threat to public health,” Hooker said.
McCullough criticized the use of retractions to silence critical papers. “As an editor-in-chief for over 20 years, I never retracted a paper, nor did I receive pressure from the publisher to pull a valid paper. That is because the peer review process and letter-to-the-editor processes work as data are vetted and interpreted,” he said.
“Scientific journals often manage the peer review and publication process to promote favored narratives and suppress dissent,” Blaxill said. “Scientific merit is rarely the priority in their management. Instead, supporting the favored (or ‘consensus’) narrative is the guiding principle more often than not.”
Experts call for investigation into journals’ relationships with Big Pharma
The experts who spoke with The Defender said that Congress needs to examine more than just the three journals whose editors-in-chief have been invited to testify on April 16.
“They should also be questioning these journal editors about their connections with Big Pharma,” Hooker said. “Journals such as JAMA, Pediatrics, etc., have corporate sponsors through their industry organizations which create myriad conflicts of interest.”
According to Thacker, “If you’re going to be a corrupt journal the way Science Magazine has turned itself into a completely corrupt institution, then we need to begin to think about whether or not publicly funded research can be published in these journals.”
“Taxpayers are funding this research, which ends up in these corrupt journals and lines the pockets of people running these corrupt journals. That needs to end. Something needs to be done to ensure that if you’re not going to abide by the basics of ethics and science publishing, then you can’t publish federally funded research,” he added.
Similarly, Francis Boyle, J.D., Ph.D., professor of international law at the University of Illinois and a bioweapons expert who drafted the Biological Weapons Anti-Terrorism Act of 1989, told The Defender :
“The real issue here that must be inquired into by Congress is the fact that Big Pharma has bought and paid for almost all science journals of relevance, to promote their pro-drug, pro-vaccine propaganda and disinformation, to the grave detriment of the public health of the American people.”
Thacker, who previously worked as an investigator for the U.S. Senate, said, “What we’ve learned from this process is that these scientists cannot be trusted. They lie all the time. I am not sure that this hearing is going to do anything unless they bring the documents out and they start doing referrals over to the Department of Justice.”
Michael Nevradakis, Ph.D., based in Athens, Greece, is a senior reporter for The Defender and part of the rotation of hosts for CHD.TV’s “Good Morning CHD.”
This article was originally published by The Defender — Children’s Health Defense’s News & Views Website under Creative Commons license CC BY-NC-ND 4.0. Please consider subscribing to The Defender or donating to Children’s Health Defense.
Featured Video

More Iran War fallout: Maritime insurance industry shifts from London to China
or go to
Aletho News Archives – Video-Images
From the Archives
Allies Don’t Need Lobbies
By Jay Knott | Dissident Voice | September 24, 2013
In a recent article on Counterpunch, Rob Urie defended the traditional Marxist analysis of US policy in the Middle East. He argues that support for Israel is driven primarily by economic interest, not the Jewish lobby.
He starts by paying tribute to the idea that Western societies are uniquely racist. He says that the “Western narrative” claims there is an “Arab character”, and that this is “antique racist blather”. He gives no definition of these terms. Further, he establishes his credentials as part of the dominant current in the American left by claiming that “over a million people in Iraq died so ‘we’ in the West can drive SUVs.”1
When he tries to criticize bourgeois economics, he makes it clear he doesn’t understand the developments it has made since Marx’s day, using the mathematical discipline known as “game theory”. He dismisses the basic abstraction of economic theory, the idea of the rational individual, on the grounds that it is “devoid of history, culture and political context”. But abstractions are always devoid of something.
He defends a more concrete economic theory, mostly Marxist, with some input from another theorist of capitalist crisis, Hyman Minsky. This concrete theory leads him to the view that US activity in the Middle East is primarily driven by rational capitalist motives, the need to secure a supply of oil.
“Taking the totality of circumstance — former oil company executives launching war on an oil rich nation on a pretext they publicly proclaimed they didn’t believe shortly before taking office — and that upon launching their war proved to be non-existent, requires a willingness to overlook the obvious — that the war on Iraq was for oil, that is difficult to support.”1
Perhaps I’ve misunderstood him, but based on what he says in the rest of the article, this convoluted sentence seems to argue that, because president Bush and vice-president Cheney attacked Iraq on false premises, and they also said it was all about oil, and they are former oil executives, and Iraq has a lot of oil, it’s difficult to deny US attacks on Iraq are all about oil.
In fact, it’s not hard at all. As Urie points out, at times Bush and co. said that attacking Iraq was “protecting the world’s supply of oil.”1 But, as he also points out, they are congenital liars. Why should we believe them when they say they are trying to “protect” the oil supply? Protect it against what? When politicians “admit” attacks on Middle Eastern countries are wars for oil, they are parroting the neo-con party line, feeding the public, both left and right, with a plausible-sounding pretext. For right-wingers, “it’s a war for oil” is a reason to support war, and for leftists, it’s a way to feel better by complaining impotently about corporate greed. Both approaches help the war drive. … continue
Blog Roll
 Aletho News
Aletho News- More Iran War fallout: Maritime insurance industry shifts from London to China
- US-Israeli aggression on Iran triggers review of GCC countries’ investment pledges to Washington
- Russia slams UK plan to seize tankers suspected of carrying its oil
- Pakistan ramps up food exports to Persian Gulf nations as war deepens food insecurity
- Iran submits response to US plan, sets terms for war’s end: Tasnim
- US vs Iran: Kharg Island Talk — Bluff or Escalation? Ex-Military Officer Weighs In
- Zelensky unnecessarily involves Ukraine in the Middle East crisis
- Turkish tanker blacklisted by Ukraine hit in drone attack – media
- Canada, the U.S., and NATO: the inescapable trap
- Villains of Judea: Leonid Radvinsky
- If Americans Knew
- ‘No Innocent Children’: Far-right Israeli Lawmaker Defends Killing of Palestinian Family
- Mossad’s promises helped Netanyahu convince Trump that Iran could be toppled
- US Arms Control Official Refuses To Comment When Asked If Israel Has Nuclear Weapons
- Veterans warn US landing could be ‘more Gallipoli than Vietnam’
- Israel may be committing war crimes in Lebanon – Not a ceasefire Day 167
- In the West Bank, life is a constant battle – 3 articles
- Jacob Reses, one of the most powerful pro-Israel operatives in Trump’s Washington
- Israeli-US assaults kill or injure 87 children a day – Not a ceasefire Day 166
- ‘Forever live by the sword’: Understanding Israelis’ massive support for Iran war
- UN’s special rapporteur on human rights says Israel is systematically torturing Palestinians
- No Tricks Zone
- Devastating Assessment Of Comirnaty Vaccine By Former Senior Pfizer Europe Toxicologist
- New Study: CO2 Is ‘Effectively Negligible’ As An Explanatory Climate Change Factor Since 2000
- Former Pfizer Toxicologist Dr. Helmut Sterz Tells Bundestag Hearing Pfizer Vaccine Should Have Never Been Approved
- Energy Expert: Germany’s Nuclear Phaseout Was A “500 Billion Euro Mistake”
- New Research: South Australia’s Mid-Holocene Sea Surface Temperatures Were 4°C Warmer Than Today
- Storing Green Energy To Last Germany 10 Days Would Require A 60-Million Tonne Battery
- New Studies: UK Sea Levels Were 4 Meters Higher Than Today During The Mid-Holocene
- Destructive Green New Deal: German Energy And Metal Group Warns Of Drastic Crisis
- New Study Documents A 20-Year Pause In Arctic Sea Ice Decline – Driven By Internal Variability
- Wake-up Call: Survey Shows Majority Of Germans Now Favor Postponing Climate Targets!
