Prion Disease and the mRNA Shots: Some Light in the Dark
By John-Michael Dumais | The Defender | July 6, 2023
In a 2022 paper, Stephanie Seneff, Ph.D., Peter McCullough, M.D., MPH, and others discussed how the COVID-19 mRNA vaccines produce G-quadruplexes and microRNAs that can lead to prion disease.
The effect becomes significantly worse after the second dose of the Pfizer shot.
Prions are pathogenic agents that can induce the abnormal folding of cellular proteins, leading to diseases such as bovine spongiform encephalopathy (mad cow disease), Creutzfeldt-Jakob disease (CJD) and Alzheimer’s.
In his June 20 Substack post, researcher Adam Gaertner provides an accessible mini-tutorial on the complex and inspirational nature of cellular proteins. He addresses the structure and function of prions, the mechanisms by which they form, and how they can wreak havoc on any organ, especially the brain.
Prion disease can lead to a number of rare, progressive neurodegenerative disorders such as dementia, ataxia and spasticity before it becomes fatal, typically within just a few years of diagnosis.
Gaertner challenges the orthodoxy that there is no cure for prion disease by discussing several recent discoveries that offer “some unexpectedly good news.”
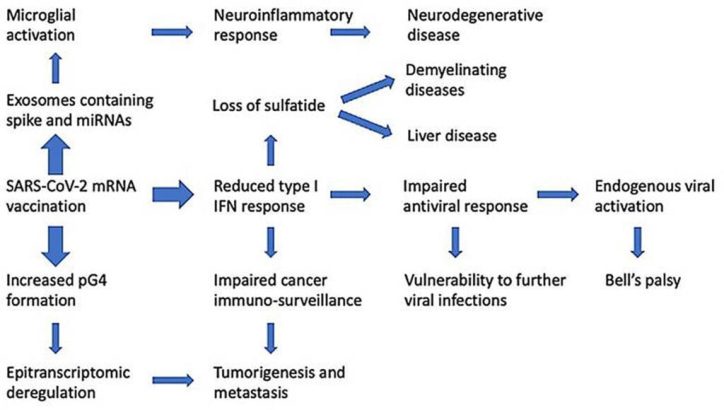
Innate immune suppression by SARS-COV-2 mRNA vaccinations: The role of G-quadruplexes, exosomes and micrornas. Credit: Seneff, Nigh, Kyriakopoulos and McCullough.
Further investigation into mRNA and CJD
Gaertner began his research work into potentially useful therapeutics for prion disease and has also funded the development of a non-invasive prion blood test.
He even undertook his own study of people who were diagnosed with or died of CJD-like symptoms (n=60) after receiving the (mostly Pfizer) mRNA jab.
Nevertheless, he readily admits that he has yet to establish absolute proof of causation.
In a European Union document related to the approval of the vaccine, Gaertner discovered what could be the smoking gun: The liquid nanoparticles used to encase the mRNA came primarily from cow fat. According to Gaertner, the document in question even admitted mRNA’s potential to cause prion protein contamination.
Nearly a year after Gaertner publicized his discovery — which convinced some but not all researchers — a paper by Jean-Claude Perez documented 26 cases of “a new form of CJD” observed within a few days of the Pfizer, Moderna or AstraZeneca vaccinations.
Of these, 20 people died within less than five months of the injection. (At the time of the paper’s publication, only one of the 26 had survived.)
The ‘good news’
While admitting that “there is not, ordinarily, a whole lot of good news to be had concerning prion diseases,” Gaertner outlined a mechanism by which “residues on the spike [protein] bind to the many and varied amyloidogenic proteins,” thus resulting in the blood clots observed by more than a few embalmers since the introduction of the mRNA shots.
He explained how this process can “bind up” the prionic proteins:
“So, what we essentially have here is, instead of a silently cascading apocalypse, buried deep inside parts of the brain that we will never reach, we likely, instead, have these long, stringy, vein-shaped agglomerations of the various amyloid proteins, binding together wherever they meet, and apparently at least somewhat resistant to being broken down by the body’s natural processes for dealing with such eventualities.”
The “really good news” comes from the way ivermectin binds directly to the spike protein — which has itself been described as a “prion-like” protein — thus blocking the spike from connecting to the ACE-2 receptor and “preventing the key from ever entering the keyhole.”
According to Gaertner, ivermectin also prevents the “amyloidogenic aggregations to the spike protein,” thereby arresting the production and proliferation of the prionic proteins. He adds:
“Ivermectin is, without a shadow of a doubt at this point, a true miracle drug: With so many applications, from antiviral, to cancer treatment, to anti-inflammatory, and of course in its originally recognized anti-parasitic application, there should be little wonder why the powers that be have done their best to diminish it as ‘horse paste.’”
Gaertner also notes that in a “very unscientific poll” he conducted on Twitter, 80% of respondents reported that a single, low dose of ivermectin significantly improved “brain fog,” a common post-COVID-19 symptom.
He described a number of “relevant investigational therapeutics” for use against the spike protein and its effects, including serrapeptase, quercetin, methylene blue and resveratrol, some of which demonstrate a “very broad range of useful actions.”
Expressing his belief that the lack of progress on therapeutics for neurodegenerative diseases is likely due to “your run-of-the-mill Pharma and charity corruption,” Gaertner nonetheless found cause for optimism.
“There’s been a lot of progress, on a lot of fronts, and more comes regularly as the world continues waking up,” he said.
John-Michael Dumais is a news editor for The Defender. He has been a writer and community organizer on a variety of issues, including the death penalty, war, health freedom and all things related to the COVID-19 pandemic.
This article was originally published by The Defender — Children’s Health Defense’s News & Views Website under Creative Commons license CC BY-NC-ND 4.0. Please consider subscribing to The Defender or donating to Children’s Health Defense.
YouTube Censors Australian Politician’s Maiden Speech to Parliament
By Rebekah Barnett | Brownstone Institute | July 8, 2023
‘30 minutes of truth bombs’ is how one Twitter user described Liberal Democrat John Ruddick’s maiden speech to the New South Wales (NSW) Parliament, last Wednesday 28 June.
Indeed, Ruddick, who left the Liberal Party in 2021 after public disagreements over the Party’s handling of the pandemic response, said out loud in parliament what many Australians have been saying for some time now – at first privately, around dinner tables, but increasingly more publicly, over workplace water coolers or at the pub, as saying the obvious becomes more socially acceptable.
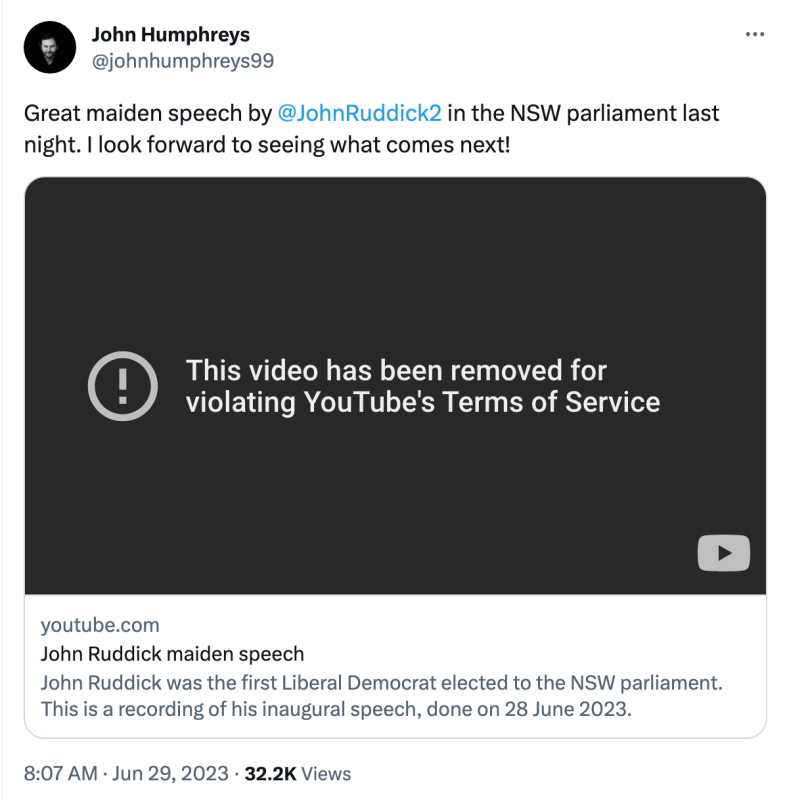
Nevertheless, what is socially acceptable offline is not necessarily acceptable on social media. YouTube swiftly removed Ruddick’s speech from its platform, just seven hours after it was uploaded. The NSW Liberal Democrats say this is the first time in Australian history that a politician’s maiden speech has been censored by the platform.

The interference of the social media giant in Australia’s political discourse is ironic given this line from Ruddick’s speech: “We libertarians are plotting to take over the world … so we can leave you all alone.”
A spokesperson for the Lib Dems says, “We initially posted the video on party founder Dr John Humphreys’ YouTube account. We then circulated that link on other social media – for example, this tweet from Dr John, which you can see now links to a takedown notice.”
YouTube claims that the video violated its ‘medical misinformation policy’, and implied that removing the video was necessary to ensure that YouTube remains a ‘safe place for all.’
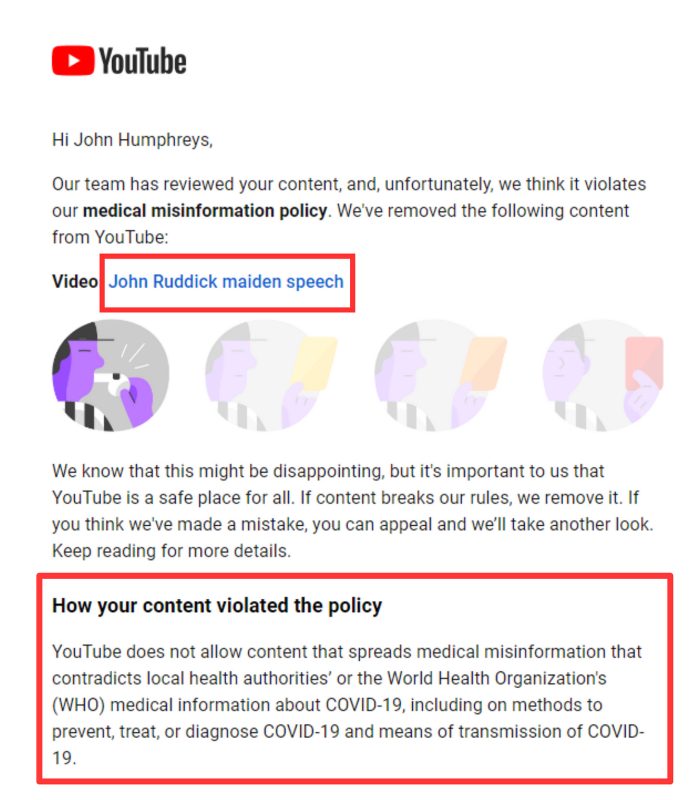
Note the definition of ‘medical misinformation’ as information that, “contradicts local health authorities’ or the World Health Organization’s (WHO) medical information about COVID-19.”
Hear that? Galileo just rolled in his grave.
So what did Ruddick actually say about Covid that might have disturbed the information gatekeepers?
- He said that the NSW government had enacted an “authoritarian Covid police state.”
- He said that the NSW government had given in to “vaccine extremism,” telling the public, ‘we won’t let you out until you take multiple injections of not only a rushed vaccine but of an entirely new class of vaccine’.
- He said that, “NSW Health published weekly data showing, the fewer vaccines you had, the less likely you went to hospital or ICU. The fatality rate was similar for the vaxxed and the unvaxxed.”
- He said that, “since the vaccine rollout there has been a 15-20 per cent increase in excess deaths in nations like Australia that had mass mRNA injections,” and questioned whether this might have anything to do with the vaccines, or from locking people up for so long.
- He said that take-up of the fifth shot is low – “too many know of others with bad reactions.”
- He said that ivermectin, an anti-viral drug that won the 2015 Nobel Prize for Medicine, was disingenuously smeared as a horse dewormer. He noted the financial incentives for suppressing ivermectin as a potential treatment for Covid, despite researchers around the world testifying to its efficacy.
- He said that there have been over 137,000 adverse events reported to the Therapeutic Goods Administration following Covid vaccination, and that many drugs have been pulled from the market for far less than this.
Agree or disagree as you please, but all these claims are evidence-based. As a friend of mine said when disagreeing with my insistence, in late 2021, that the vaccines would not be effective in preventing/reducing transmission, “We believe different scientists.”
The video of Ruddick’s maiden speech has been reposted on YouTube via the Lib Dems main account, and has not yet been taken down. You can watch the speech in full via the Lib Dems twitter account.
Spectator has also published the transcript of Ruddick’s speech in full.
A spokesperson for the Lib Dems said on Friday,
“We’re obviously very disappointed that YouTube feels the need to censor something not only from NSW Parliament but as time-honoured as a maiden speech, but we also oddly must thank them as we’ve benefited from the Streisand effect.
“The video already has over 225,000 views on one tweet, and is also being viewed in Facebook groups, on Telegram and (for now anyway) a little bit on the federal LibDems YouTube page. The interest in the speech certainly seems to have increased exponentially after the YouTube removal, and we’re getting inundated with positive comments and questions.”
Other notable ‘truth bombs’ from Ruddick’s speech include his criticism of blown-out government debt, and his concern that pursuing a net zero carbon economy is a “reckless folly.”
While the Lib Dems are benefiting from the Streisand effect for the time being, Member of the European Parliament, Christine Anderson, is dealing with YouTube censorship by suing the social media platform. Anderson reports that YouTube blocked two videos from parliamentary sessions in which she acted on the official Special Committee on the COVID-19 Pandemic.
Anderson has described YouTube’s censorship as “anti-democratic,” saying, “I will not put up with uncontrolled influence on this scale, which is why I have now taken the necessary legal steps to… ensure that all citizens have unfiltered access to relevant information at all times.”
Rebekah Barnett reports from Western Australia. She is a volunteer interviewer for Jab Injuries Australia and holds a BA in Communications from the University of Western Australia. Find her work on her Substack page, Dystopian Down Under.
Leaked Memo Shows Mayo Clinic Doubles Down On Censorship
By Didi Rankovic | Reclaim The Net | July 7, 2023
Reports this week expose Mayo Clinic as “doubling down” on speech restrictions it previously chose to impose affecting Dr. Michael Joyner.
The information comes from an internal memo sent to Mayo Clinic College of Medical Science, which is interpreted as sticking to a policy of preventing this medical organization’s members from speaking freely.
Previously, Joyner, a professor, was punished for his public statements related to his research, concerning public health, including topics such as Covid, and transgenderism and, in general, making comments that were construed as being against some government policies, that is, something that was well within his right to do.
But Mayo Clinic took the stance that what was more important, and takes precedence was for Joyner to toe the line – i.e., stick to “prescribed messaging” and rather than focus on his medical expertise, worry more ardently about the clinic’s chosen “brand” and (ideological?) standing it derives from that.
The Joyner incident came to light in early June, and after Foundation For Individual Rights and Expression (FIRE) urged the health facility to withdraw the decision. Mayo Clinic’s Chief Communication Officer Halena Gazelka a while later the same month penned the memo, recommending to those in charge to effectively ignore the criticism.
One of the key points of the controversy is that the college has made a “promise” to its teachers and students of the right to free speech – which clearly wasn’t exercised when Joyner got suspended, and had a gag-order placed on him.
In the memo, Gazelka fairly brazenly advises college leadership to keep saying that Mayo Clinic continues to be “fully committed to academic freedom and expression.”
Joyner, who is still banned from talking to reporters without the college’s permission, might be surprised to learn this.
Furthermore, in the same vein of “tweaking reality,” the memo wants the college to push the narrative that Joyner’s punishment did not come as a result of his statements about transgender athletes, but because of his criticism (“unprofessional comments”) regarding the National Institute of Health’s (NIH) regulation of convalescent plasma.
There’s also a whiff of character assassination here, as the memo recommends framing the whole thing as sour grapes on Joyner’s part:
“Dr. Joyner’s comments about the NIH did not reflect the expression of a scientific or academic opinion but instead were an expression of his personal frustration with the NIH’s regulation of a therapy he had championed,” wrote Gazelka.
Now that government COVID malfeasance is exposed, what will the GOP do about it?
By Daniel Horowitz – conservative review – July 6, 2023
We are now 2+ years into consuming reams of information showing the vaccines were devastating to humanity. What will Republicans do about it other than whine about censorship? Refusing to focus on vaccine injury and the perfidy of the government-vaccine complex is an act of self-censorship.
There is a bizarre dynamic unfolding as it relates to GOP sentiment toward the vaccine. All Republicans recognize and decry the growing evidence of the government’s collaboration with big tech to censor all information about vaccine injury. Yet they seem to be more upset about the censorship of the information than about the information itself. Why is there no push from Republicans to defund the vaccines and fix the regulatory and legal structures that allowed Operation Warp Speed to occur and that continue to gaslight the next iteration of rushed, dangerous vaccines?
In an extraordinary ruling on Independence Day itself, Louisiana federal Judge Terry Doughty issued a broad injunction against all government agencies on working with social media companies to censor politically unfavored speech. Citing “substantial evidence” of government’s “dystopian” violations of the First Amendment, Judge Doughty prohibited the federal government from “encouraging, pressuring, or inducing in any manner the removal, deletion, suppression, or reduction of content containing protected free speech.” The injunction not only includes the HHS agencies censoring COVID information, but also the FBI, the Cybersecurity and Infrastructure Security Agency, the State Department, the DOJ, and the White House censoring all forms of protected speech.
This ruling comes a week after the House Judiciary committee produced a preliminary report showing DHS’ CISA was behind the censorship enterprise. It turns out that CISA funded a nonprofit group to work with social media on a process, known as “switchboarding,” which would “trigger content moderation” to “ensure priority treatment of misinformation reports.”
Republicans seem united in combating this censorship and plan to include provisions in the relevant appropriations bills for fiscal year 2024 to block funding for these surveillance and censorship programs. However, where is the same degree of outrage about the dangers of the vaccines themselves?
We now have over two years of information showing ubiquitous injury stemming from damage to all parts of the body, particularly cardiac and neurological. Whether it’s VAERS, European data, countless independent studies, epidemiological data, excess deaths and “died suddenly” mysteries correlating with the take-up of the vaccines, health insurance data, life insurance data, or disability data – we have enough evidence to convict this shot for murder if it were a human standing for trial. Yet not only have these vaccines not been defunded, the same framework that rushed their approval has already been used for countless other new vaccines.
The government’s new shell game is to concede the existence of these problems, but play semantics with the term “rare” when describing their risk. Science Insider published a piece acknowledging the “rare link between coronavirus vaccines and Long Covid–like illness,” including blood clotting, heart inflammation, and neurological disorders. Even Peter Marks, the man at the center of Operation Warp Speed, admitted, “We can’t rule out rare cases.”
“If a provider has somebody in front of them, they may want to take seriously the concept [of] a vaccine side effect,” admits the director of the FDA’s Center for Biologics Evaluation and Research, two years after emails show he ignored concerns of rushing the vaccine amidst a pileup of adverse event reporting.
However, what is rare? The CDC’s own pharmacovigilance program showed a 7.7% rate of clinical-level injury. Coupled with the underreporting rate in VAERS, there were likely millions of severe and long-term injuries, including several hundred thousand deaths in the U.S. So yes, we can suggest that 92% of people didn’t experience clinical levels of injury and 98%-99% didn’t experience long-term and deadly injuries. In that sense, I guess you can say it’s rare. But how many people are we talking about when 5.5 billion people were given at least one dose? Potentially, millions of deaths and hundreds of millions of injuries! Just consider the fact that 25% of injuries reported to VAERS and about a third reported by the European Medicines Agency are considered serious, well beyond the standard of 15%.
House Republicans can no longer ignore the problem with the vaccines. They must also stop ignoring the endless approvals of monkeypox and RSV shots based on dubious data and the same rushed framework. To that end, Speaker McCarthy should take the following actions.
- Defund all COVID shots in the HHS, DOD, and FDA funding bills.
- Create a commission of members of Congress to examine the rationale, safety, and efficacy data of all vaccines, beginning with the new ones recently approved and in the pipeline.
- Refuse to sign off on the Senate version of the Pandemic and All-Hazards Preparedness Act unless major reforms are enacted curtailing pandemic authorities.
- Bar any involvement in a WHO pandemic treaty or expansion of the International Health Regulations.
- Repeal immunity for vaccine manufacturers, including the provision in the 21st Century Cures Act of 2016 that extends the immunity to vaccines offered to pregnant women.
To this day, we still can’t get Republicans to shake their support for the V-word even in red states. Last week, Ohio Gov. Mike DeWine, the consummate COVID fascist governor, used his line-item veto to strike a provision from the budget ending vaccine mandates in colleges. “University and college dormitories and student housing are congregate settings where such policy may be of great importance to ensure resident safety,” said DeWine of vaccine mandates in his veto message. It takes a new level of cognitive dissonance to support mandates on those who don’t want the shot out of fear of harming those who did supposedly get the protection that evidently fails to protect unless the other person gets it!
Republicans all agree that our government engaged in an unprecedented operation to cover up the truth about vaccines. How come their curiosity stops at the degree of exposing the cover-up with no interest in delving into what exactly they are trying to cover up? After all, this is the only product that automatically goes into every arm of every baby multiple times after birth with a set schedule mandated by schools. Certainly the COVID shots are proven to be poison, but is there no interest in uncovering the broader truth?
© 2023 Blaze Media LLC. All rights reserved.
Lancet Study on Covid Vaccine Autopsies Finds 74% Were Caused by Vaccine – Journal Removes Study Within 24 Hours
BY WILL JONES | THE DAILY SCEPTIC | JULY 6, 2023
A Lancet review of 325 autopsies after Covid vaccination found that 74% of the deaths were caused by the vaccine – but the journal removed the study within 24 hours.
The study, a pre-print that was awaiting peer-review, is written by leading cardiologist Dr. Peter McCullough, Yale epidemiologist Dr. Harvey Risch and their colleagues at the Wellness Company and was published online on Wednesday on the pre-print site of the prestigious medical journal.
However, less than 24 hours later, the study was removed and a note appeared stating: “This preprint has been removed by Preprints with the Lancet because the study’s conclusions are not supported by the study methodology.” While the study had not undergone any part of the peer-review process, the note implies it fell foul of “screening criteria”.
The original study abstract can be found in the Internet Archive. It reads (with my emphasis added):
Background: The rapid development and widespread deployment of COVID-19 vaccines, combined with a high number of adverse event reports, have led to concerns over possible mechanisms of injury including systemic lipid nanoparticle (LNP) and mRNA distribution, spike protein-associated tissue damage, thrombogenicity, immune system dysfunction and carcinogenicity. The aim of this systematic review is to investigate possible causal links between COVID-19 vaccine administration and death using autopsies and post-mortem analysis.
Methods: We searched for all published autopsy and necropsy reports relating to COVID-19 vaccination up until May 18th, 2023. We initially identified 678 studies and, after screening for our inclusion criteria, included 44 papers that contained 325 autopsy cases and one necropsy case. Three physicians independently reviewed all deaths and determined whether COVID-19 vaccination was the direct cause or contributed significantly to death.
Findings: The most implicated organ system in COVID-19 vaccine-associated death was the cardiovascular system (53%), followed by the hematological system (17%), the respiratory system (8%) and multiple organ systems (7%). Three or more organ systems were affected in 21 cases. The mean time from vaccination to death was 14.3 days. Most deaths occurred within a week from last vaccine administration. A total of 240 deaths (73.9%) were independently adjudicated as directly due to or significantly contributed to by COVID-19 vaccination.
Interpretation: The consistency seen among cases in this review with known COVID-19 vaccine adverse events, their mechanisms and related excess death, coupled with autopsy confirmation and physician-led death adjudication, suggests there is a high likelihood of a causal link between COVID-19 vaccines and death in most cases. Further urgent investigation is required for the purpose of clarifying our findings.
The full study does not appear to have been saved in the Internet Archive, but can be read here.
Without further detail from the Lancet staff who removed the paper it is hard to know what substance the claim that the conclusions are not supported by the methodology really has. A number of the authors of the paper are at the top of their fields so it is hard to imagine that the methodology of their review was really so poor that it warranted removal at initial screening rather than being subject to full critical appraisal. It smacks instead of raw censorship of a paper that failed to toe the official line. Keep in mind that the CDC has not yet acknowledged a single death being caused by the Covid vaccines. Autopsy evidence demonstrating otherwise is clearly not what the U.S. public health establishment wants to hear.
Dr. Clare Craig, a pathologist and co-Chair of the HART pandemic advisory group, says that in her view the approach taken in the study is sound. She told the Daily Sceptic:
The VAERS system [of vaccine adverse event reporting] is designed to alert to potential harms without necessarily being the best way of measuring the extent of those harms.
Quantifying the impact of deaths can be done by looking at overall mortality rates in a country.
However, this is imperfect as a deficit of deaths would be expected after a period of excess deaths, making the accuracy of any baseline dubious.
An alternative approach of auditing such deaths through autopsy is sound.
There may be a bias [in the study] towards reporting the autopsies of deaths where there was evidence of causation and the likelihood of causation might be exaggerated by that bias. For example, 19 of the 325 deaths were due to vaccine-induced immune thrombocytopenia and thrombosis (VITT) but these reports may be overrepresented because of the regulators’ willingness to acknowledge such deaths.
Nevertheless, it is important that attempts are made to quantify the risk of harm and censorship of these attempts, rather than open scientific critique, does nothing to help reassure people.
Biden Administration Files Notice of Appeal Against Social Media Censorship Collusion Ban
By Christina Maas | Reclaim The Net | July 5, 2023
The US Justice Department has formally filed a notice of appeal against a court ruling that prohibits federal agencies and officials from engaging in discussions with social media companies to censor speech on their platforms.
The ruling in favor of free speech, justified by First Amendment rights, has been met with consternation by the Biden Administration, which says it poses a restriction on their efforts to counter the dissemination of what it says is “misinformation.”
The appeal was submitted to the 5th US Circuit Court of Appeals in New Orleans this past Wednesday, in response to an injunction imposed by US District Judge Terry Doughty, alongside a lengthy opinion on the case.
Judge Doughty asserted in his detailed ruling that the manner in which federal officials communicated with technology giants such as Twitter and Facebook about the removal or restriction of content – specifically pertaining to Covid the 2020 election likely constituted a violation of First Amendment protections for US citizens.
Information, whether truthful or not, is not supposed to be in the purview of the government to police. Though, the Biden administration has attempted to defend its engagement with social media companies as a necessary approach to protecting public health and safety.
Conversely, the plaintiffs, who include the Republican attorneys general of Missouri and Louisiana, contend that the federal government’s communication with these companies amounted to a state-sanctioned censorship campaign.
In the initial ruling, Judge Doughty issued an injunction preventing a wide range of federal entities from engaging in communication with any social media company to urge, encourage, pressure, or induce the removal or suppression of speech.
However, the ruling does provide for certain exceptions. Notably, it permits government engagement with social media companies in instances involving criminal activity (including that which is election-related), national security concerns, or other threats to public security.
The appeal by the Justice Department marks a significant development in an ongoing legal matter that has far-reaching implications for the relationship between the government and social media platforms and the ability of the government to suppress speech.
Walensky Warns Public to Beware of ‘Misinformation’ and ‘Politicized Science’
By Brenda Baletti, Ph.D. | The Defender | July 5, 2023
As she ended her tenure last week as director of the Centers for Disease Control and Prevention (CDC), Dr. Rochelle Walensky warned the American public to be on guard against “misinformation” and the “politicization of science.”
Walensky told The Wall Street Journal she hopes Americans will make health decisions based on “their own risk assessment and their own personal risks, but not through politics,” emphasizing that public health recommendations also shouldn’t be politicized.
“Ironically, this comes after two-and-a-half years of Walensky misinforming the public and politicising the science,” investigative journalist Maryanne Demasi, Ph.D., wrote on her Substack.
Demasi and many others took to Twitter to remind people of Walensky’s false statements and politicized decision-making.
Walensky last week published a farewell op-ed in The New York Times, in which she wrote that public health is critically important in the U.S., and yet she “fear[s] the despair from the pandemic is fading too quickly from our memories.”
She complained that “the agency [CDC] has been sidelined, chastened by early missteps with Covid and battered by persistent scrutiny.”
She also told the WSJ that public health shouldn’t fall along partisan lines.
Yet stark political partisanship defined her time at the CDC. The WSJ reported that a recent KFF poll showed political affiliation was the strongest demographic predictor of COVID-19 vaccination. And about one-quarter of Americans don’t trust the CDC’s health recommendations, according to a 2022 survey published in the journal Health Affairs.
Walensky acknowledged “missteps in communicating” by the CDC, which, she said, “could have done a better job” making it clear to the public that the agency’s message could change during the pandemic.
But, she told the WSJ, the CDC has a plan to regain public trust in the future — by working directly with media organizations to discuss how to best shape public opinion prior to releasing scientific information to the public.
She said the CDC plans to use a method called “prebunking,” where they will communicate directly with media organizations before they release information to let the media know which details about public health might be “misconstrued.”
According to The Associated Press (AP) “prebunking” by public health agencies allows the agencies to define something as “misinformation” before readers have an opportunity to encounter it elsewhere as possibly true.
Then search engines such as Google prioritize “credible websites” like the U.S. Food and Drug Administration’s (FDA) or the CDC’s in its searches.
FDA Commissioner Robert Califf, the Virality Project and Google are among those who have promoted prebunking as a way to combat misinformation.
Journalist Kim Iversen proposed a different approach Walensky might take to restoring public trust in the CDC.
She said:
“Well, the way to do it is to apologize, to own up to your lies, to own up to the mistakes that you made and to discuss why you did that, why the agency followed such political partisanship when they should have been following science, why they ignored the science that was right in front of them.”
CDC broadcast a long list of ‘misinformation’ during Walensky’s tenure
Throughout her tenure at the CDC, which began when Biden took office in January 2021, Walensky made a series of public statements that have proven to be false.
Evidence has since emerged that Walensky knew many of these statements were false when she made them.
In March 2021, Walensky famously told Rachel Maddow, that “vaccinated people do not carry the virus, don’t get sick.”
The CDC was forced to walk back her statements a few days later. But that message was the basis for vaccine mandates imposed later that year by the Biden administration, businesses, universities and public venues throughout the country.
In a mid-June congressional hearing, Walensky defended her March statements, claiming they were true at the time.
But the Washington Examiner reported on June 20 that emails obtained through a Freedom of Information Act request showed Walensky and Dr. Francis Collins were aware of and discussed “breakthrough cases” of COVID-19 in January 2021 — just before the vaccines became widely available — and yet continued to tell the public the vaccines would prevent transmission.
In that same congressional testimony, Walensky also defended the mask mandates, saying that the summary of Cochrane’s review — which found wearing masks in the community “probably makes little to no difference” in preventing viral transmission — had been “retracted.”
But it was neither retracted nor had the authors of the review changed the language in the summary, Demasi reported.
In June 2021, Walensky told “Good Morning America” that the risk of myocarditis was extremely rare, and there was overwhelming data the vaccines were safe for children — even after hundreds of cases of myocarditis had been reported and the CDC had been aware of a safety signal since February.
Under Walensky, the CDC also gave false information on vaccine safety monitoring, added the COVID-19 vaccines to the childhood vaccine schedule despite known harms, withheld data on boosters from the agency’s own advisers and told pregnant women the vaccine was safe — just days after Pfizer reportedly finalized a report demonstrating it wasn’t.
In a March study by Krohnert and others, researchers compiled instances of errors in data presented by the CDC during the COVID-19 pandemic in publications, press releases, interviews and Twitter. The authors reported 25 instances where the agency under Walensky promoted demonstrably false numbers.
In most (80%) cases, the CDC exaggerated the severity of the pandemic. For example, Walensky gave a briefing on June 23, 2022, during which she claimed COVID-19 was a “top 5 cause of death” in children, which was untrue.
Most recently, the House Select Subcommittee on the Coronavirus Pandemic gave Walensky until July 12 to turn over phone records involving American Federation of Teachers (AFT) President Randi Weingarten. The House is investigating potential political interference on the part of AFT with the CDC’s school reopening recommendations during the COVID-19 pandemic, The Defender reported.
Walensky warns of ‘future threats’
Walensky warned at the end of her Times op-ed:
“I want to remind America: The question is not if there will be another public health threat, but when. The C.D.C. needs public and congressional support if it is going to be prepared to protect you from future threats.”
To take on these “future threats” the Biden administration nominated Dr. Mandy Cohen, an internal medicine physician and former state health secretary of North Carolina, to replace Walensky.
But critics warn Cohen is “a public health COVID authoritarian” who is “fully entrenched in the ‘bio-pharmaceutical complex.’”
Dr. Peter McCullough told The Defender that during the COVID-19 pandemic, Cohen failed to recognize therapeutics and natural immunity, and supported lockdowns, vaccine mandates and masking.
Cohen comes to the CDC from the private sector, where she is executive vice president of Aledade and CEO of Aledade Care Solutions, whose executive leadership and board of directors includes people with connections to the World Economic Forum and the Bill & Melinda Gates Foundation.
Walensky congratulated Cohen on her nomination, describing her as “a respected public health leader who helped North Carolina successfully navigate” COVID-19, and whose “unique experience and accomplished tenure in North Carolina … make her perfectly suited to lead CDC as it moves forward by building on the lessons learned from COVID-19 to create an organization poised to meet public health challenges of the future.”
Brenda Baletti Ph.D. is a reporter for The Defender. She wrote and taught about capitalism and politics for 10 years in the writing program at Duke University. She holds a Ph.D. in human geography from the University of North Carolina at Chapel Hill and a master’s from the University of Texas at Austin.
This article was originally published by The Defender — Children’s Health Defense’s News & Views Website under Creative Commons license CC BY-NC-ND 4.0. Please consider subscribing to The Defender or donating to Children’s Health Defense.
Dr. Paul Offit Lets Us Know ‘the Experts’ Have Officially Lost Their Minds
By Madhava Setty, M.D. | The Defender | July 5, 2023
I don’t have a big presence on Twitter. I don’t find the platform suitable for exploring and critiquing interesting ideas. You can say only so much in 280 characters. It’s great for inciting someone or dropping a witty comeback or link without much context.
At least that’s what I thought. Then I stumbled upon a tweet from Dr. Paul Offit. He’s taught me that you can convey a lot in a few short sentences.
Who is Dr. Paul Offit?
Offit is a big name in vaccines. Beyond what is listed below, he also sat on the Advisory Committee on Immunization Practices for the Centers for Disease Control and Prevention (CDC) and is presently a member of the Vaccines and Related Biological Products Advisory Committee for the U.S. Food and Drug Administration (FDA).
He’s had a say in the approval and/or authorization of many biologics, including the COVID-19 mRNA products.
Briefly, Offit is:
- Director of the Vaccine Education Center and professor of pediatrics in the Division of Infectious Diseases at Children’s Hospital of Philadelphia.
- Maurice R. Hilleman Professor of Vaccinology at the Perelman School of Medicine at the University of Pennsylvania.
- An internationally recognized expert in the fields of virology and immunology.
- A founding advisory board member of the Autism Science Foundation and the Foundation for Vaccine Research.
- A member of the Institute of Medicine and co-editor of the foremost vaccine text, “Vaccines.”
- The author or co-author of more than 150 papers in medical and scientific journals in the areas of rotavirus-specific immune responses and vaccine safety.
- The co-inventor of the rotavirus vaccine, RotaTeq®, recommended for universal use in infants by the CDC.
- A recipient of the Charles Mérieux Award from the National Foundation for Infectious Diseases.
His list of accomplishments goes on.
I don’t pretend to know more about vaccines than he does. I’m just an anesthesiologist and engineer. He must be a very smart person. Which is why this tweet is so baffling:
Why is Offit tweeting about placebos and saltwater right now?
It has to do with a truth bomb Robert F. Kennedy Jr. dropped at a town hall event last week.
According to Kennedy, chairman on leave from Children’s Health Defense, he and attorney Aaron Siri sued the U.S. Department of Health and Human Services (HHS) after HHS refused to meet their demand to produce at least one study comparing the safety of a vaccine on the childhood immunization schedule with a true placebo.
In a written response received more than a year later, the HHS did not cite a single such study, instead claiming:
“Inert placebo controls are not required to understand the safety profile of a new vaccine, and are thus not required.”
This stupefying claim made by Melinda Wharton, M.D., MPH, acting director of the National Vaccine Program Office, should be attacked on podcasts and publications everywhere.
How do you know that a new vaccine is safe if it isn’t tested against an inert placebo, Dr. Wharton?
If you are someone who is willing to abandon basic logic and trust every single word spewed by our public health agencies, ask yourself, why then does the FDA demand that medicines be tested against a placebo to ensure safety prior to licensure?
Twitter lit up around this pivotal topic. The tweet from one of the foremost vaccine experts in the world (Offit) was in response to Siri, who, according to Offit, asserted that virtually all vaccines on the childhood vaccination schedule, including RotaTeq (Offit’s brainchild), were not licensed by the FDA based on a placebo-controlled clinical trial.
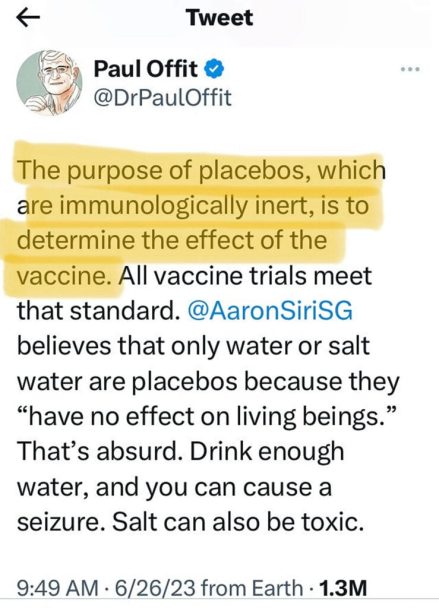
Let’s break down Offit’s attack on Siri. Offit states: “The purpose of placebos, which are immunologically inert, is to determine the effect of the vaccine.”
Yes, Dr. Offit, one purpose of a placebo is to determine the effect of the vaccine. In order to prove that it works, it must do better than an immunologically inert substance. In other words, it must exceed the so-called placebo effect.
But that’s not the only purpose placebos serve. With regard to safety, a new vaccine has to be compared to something that has the least possible chance of causing deleterious effects.
To be clear, those who eschew a vaccine do not get in line for a shot of an “immunologically inert substance.” They stay away from the vaccine clinic altogether and take their chances.
This is why the placebo must be a true placebo. The best we can possibly do is use saline, a saltwater solution that reasonably matches the sodium concentration in our plasma. It is what is used to dilute medications and replenish blood volume. It’s what you use to store your contact lenses.
Offit then adds this:
“[Aaron Siri] believes that only water or salt water are placebos because they ‘have no effect on living beings.’ That’s absurd. Drink enough water, and you can cause a seizure. Salt can also be toxic.”
Offit is saying that by drinking a large amount of water the plasma sodium concentration in a person can abruptly decrease which, in fact, can lower the seizure threshold. He’s not wrong, it does happen in pathological conditions, especially in the critically ill.
Can salt be toxic? Yes. Ingestion of a large amount of salt will stimulate properly functioning kidneys to increase the absorption of free water, thus mitigating the effect of the salt load. This can cause volume overload and put a person at risk for heart failure and pulmonary edema.
So what — if not 0.2 ml of saline — should we use for a placebo, Dr. Offit? A tiny aliquot of adjuvants (that can include elements like aluminum)? Pro-inflammatory lipid nanoparticles? Viral or toxin deactivators like formaldehyde? Preservatives like thimerosal that contain mercury, one of the most potent neurotoxins known (yes, mercury in this form is still in some flu vaccines according to the CDC)?
All of these substances are “immunologically inert.”
But why would you consider using them as a placebo control if not to mask the potential harm of the vaccine in question?
Is that how inventors of vaccines for our children view placebos? Is that how advisory committee members on the FDA view them? What about the other advisory board members of the Autism Science Foundation? Why would anyone trust any vaccine on the childhood immunization schedule after such comments?
You don’t have to be Maurice R. Hilleman Chair of Vaccinology at the Perelman School of Medicine to see that your comments here are misleading, disingenuous and purposefully inciting.
Moreover, they don’t make any sense.
What would other recipients of your long list of awards have to say about your comments on placebos? I don’t think they would approve, sir.
Your public statements also sully the excellent reputation of the Children’s Hospital of Philadelphia and those who were lucky to train there, like me.
Dr. Setty has been a board certified anesthesiologist since 2002 and has held various leadership positions in his clinical practice.
This article was originally published by The Defender — Children’s Health Defense’s News & Views Website under Creative Commons license CC BY-NC-ND 4.0. Please consider subscribing to The Defender or donating to Children’s Health Defense.
Featured Video

Ian Proud: Economic Reset with Russia to Save Europe
or go to
Aletho News Archives – Video-Images
From the Archives
Magic Hour for Gates
By Gary Jordan | Wake The F*** UP | March 15, 2021
Bill Gates wants to know everything about you.
He wants to control every aspect of your life.
His insatiable thirst for the supervision and scrutiny of every human being alive has sparked a US$1 billion investment that will blanket the earth in video surveillance satellites, providing real-time feedback with a mere one-second delay. He advocates for Orwellian digital tools to track your every move and has bankrolled US$1.7 billion to provide artificial intelligence that will be used to scan each and every visitor to major event venues worldwide. He wants to do away with end-to-end encryption, so he can snoop on your private conversations. He wants to know when and where you travel and who you travel with. He wants you to eat whatever he says you should eat, drink whatever he says you should drink, think how he wants you to think and know only what he wants you to know. Plus he wants to dictate what goes inside your body.
But he doesn’t want you to know a lot about him.
For instance… continue
Blog Roll
 Aletho News
Aletho News- ‘Fox guarding the henhouse’: AMA, Vaccine Integrity Project to conduct their own vaccine safety and efficacy reviews
- Macron, Merz, and von der Leyen Defend Expanded Speech Controls
- Keir Starmer-tied think tank paid PR firm to target The Grayzone
- ‘Israel’ threatens to genocide Gaza if Hamas refuses disarmament
- Apple Just Bought A Sinister ‘Pre-Speech’ Tech Company Implicated In Genocide
- Israel’s new West Bank registration process declares Palestinian land ‘state property’
- Two children killed in Palestinian Authority ambush in West Bank; Hamas slams attack as ‘black mark’
- Israel Needs Time Before Another Iran War—Here’s Why
- US seizes oil tanker for ‘defying Trump’s quarantine’
- Ian Proud: Economic Reset with Russia to Save Europe
- If Americans Knew
- An error has occurred; the feed is probably down. Try again later.
- No Tricks Zone
- New Study: A 4°C Warmer Beaufort Sea Had ‘No Sea Ice’ 11,700 – 8200 Years Ago
- Unfudging The Data: Dutch Meteorological Institute Reinstates Early 20th Centruy Heat Waves It Had Erased Earlier
- German Gas Crisis…Chancellor Merz Allegedly Bans Gas Debate Ahead of Elections!
- Pollen Reconstructions Show The Last Glacial’s Warming Events Were Global, 10x Greater Than Modern
- Germany’s Natural Gas Storage Level Dwindles To Just 28%… Increasingly Critical
- New Study Rebuts The Assumption That Anthropogenic CO2 Molecules Have ‘Special’ Properties
- Climate Scientist Who Predicted End Of “Heavy Frost And Snow” Now Refuses Media Inquiries
- Polar Bear Numbers Rising And Health Improving In Areas With The Most Rapid Sea Ice Decline
- One Reason Only For Germany’s Heating Gas Crisis: Its Hardcore-Dumbass Energy Policy
- 130 Years Later: The CO2 Greenhouse Effect Is Still Only An Imaginary-World Thought Experiment
