RFK Jr. Dismantles Doctor’s Pro-Vaccine Stance in Town Hall Meeting
By Madhava Setty, M.D. | The Defender | June 29, 2023
Epistemology is the theory of knowledge. Epistemologists ask the foundational question, “How do we know what we know?”
Robert F. Kennedy Jr. on Wednesday appeared in a town hall meeting hosted by NewsNation and moderated by journalist Elizabeth Vargas.
The exchanges between Kennedy — chairman on leave from Children’s Health Defense — Vargas and Dr. Tariq Butt, a family medicine doctor in the audience, demonstrated the real quagmire the scientific community finds itself in.
Doctors and journalists cannot see the difference between believing and knowing. If we were in a rational world, there wouldn’t be the need for censorship and shadowbanning.
Nor would many of the vaccines on the childhood immunization schedule, as presently formulated and tested, have found their way into the arms of young human beings.
In 13 short minutes, Kennedy deftly demonstrated to the audience that our problem isn’t just a failure of epidemiology — it’s one of epistemology:
Vargas first framed the topic this way:
“The biggest controversy surrounding your candidacy is your stance on childhood vaccines. Nearly every scientific and medical organization including the CDC [Centers for Disease Control and Prevention], the FDA [U.S. Food and Drug Administration], the AMA [American Medical Association], the American Academy of Pediatrics, all say you’re wrong on this issue.”
Vargas opened the door for Kennedy to not only clarify his position — which he said has been distorted and misrepresented no matter how many times he has tried to set the record straight — but she also revealed how little thought and research she has done into the controversy.
Kennedy pointed out the reality of the situation. These are not organizations that have independently arrived at their conclusions. The AMA, the American Academy of Pediatrics and “nearly all scientific and medical organizations” take information coming from the CDC and FDA as gospel.
In other words, if the CDC and the FDA are wrong, the entire medical establishment is wrong.
There’s a difference between consensus and herd mentality — a fact that never seemed to register with Vargas.
Kennedy is immensely knowledgeable about vaccine science and the regulatory process, as well as its corruption by Pharma interests. Moreover, he is a seasoned litigator and is not careless in his delivery. He correctly asks Vargas for clarification: “On what issue?”
Vargas first alludes to the possibility that vaccines could be the cause of autism and harm.
Kennedy immediately asks the obvious, “So you are saying that these organizations claim that vaccines NEVER damage kids?”
Vargas is forced to backpedal:
“I don’t think anyone is saying they never have. There may be a child here [or there], but overall vaccines have saved millions and millions of lives.”
Vargas is demonstrating the lack of understanding the public has about the issue. How can anyone claim that vaccines have saved millions and millions of lives if proper prospective studies with matched unvaccinated controls have never been conducted?
Kennedy makes this abundantly clear in his response to Dr. Butt, who asks Kennedy this question:
“Eradication of chicken pox and polio in the U.S. and in many parts of the world is a result of regular vaccination. MMR [measles, mumps, rubella] and many diseases are preventable. There is little evidence of these diseases in the vaccinated population. Your vaccine stance is dangerous to the health and well-being of millions. Medical experts are deeply concerned about your message. How can we help you come to the side of science?”
Kennedy admits there is evidence that vaccines have reduced the risk of mortality and morbidity from the diseases they target. However, he argued, without long-term prospective studies around all-cause mortality/morbidity in vaccinated populations nobody — no matter how educated or how big an organization you represent, he said — can claim there is an overall benefit.
Kennedy’s answer to the question dismantles the issue to the very core, catching Dr. Butt off guard. His methodical response should have proven to the audience that the family medicine doctor has very little grasp of all the available evidence.
Dr. Butt clearly wasn’t aware of analyses like this one that concluded that a “Mass varicella vaccination is expected to cause a major epidemic of herpes zoster, affecting more than 50% of those aged 10-44 years at the introduction of vaccination.”
Should studies like this guide public policy in the U.S.? They certainly do in the U.K., where health officials do not recommend universal vaccinations against chickenpox for precisely the reason Kennedy states.
Of all the preventable diseases out there, why would Dr. Butt use chickenpox as an example of how Kennedy’s vaccine stance is dangerous to the health and well-being of millions? Could it be that a doctor with a microphone was unaware of the science?
Was Dr. Butt aware of the enormous tragedy caused by the DTP (diptheria, tetanus, pertussis) vaccine in Africa? After 30 years of observation, it was shown that children vaccinated with the DTP shot were dying of other causes at 10 times the rate of the unvaccinated. We would have never known about this if no one actually looked.
The devastation caused by the DTP vaccine is not limited to the continent of Africa. Kennedy informed the audience that the flurry of lawsuits against manufacturers of this vaccine led to the passing of the National Childhood Vaccine Injury Act of 1986, which has protected vaccine manufacturers from any liability.
As a concession to the public, this law also created the Vaccine Adverse Event Reporting System, or VAERS, to “protect” and warn the public of potential vaccine danger; a system that has been shown to underreport injuries as commonly as it gets ignored.
Though Kennedy did not discuss the MMR and polio vaccines, his point was clear: Unless proper, long-term, prelicensure placebo-controlled safety studies are done we cannot determine if more harm than good is being done.
Dr. Butt’s response to the likely damage caused by the varicella and DTP vaccines was all too predictable: “A person can take a medicine and then get involved in a motor vehicle accident.” In other words, correlation does not prove causation!
Dr. Butt has good intentions. He is also particularly skilled at picking the weakest examples to prove his point.
The issue with the varicella vaccine was the resulting increased risk of herpes zoster infection (shingles). The issue with the DTP vaccine was the increased risk of death from other prevalent diseases that proved to be more deadly for the kids who received the vaccine.
We are not talking about random traumatic injuries that have nothing to do with immune modulation.
Furthermore, was Dr. Butt aware that the “correlation does not equal causation” argument can be used to dismiss vaccine benefits as well?
This double standard is mindlessly applied by vaccine proponents. Trials don’t prove causation, only correlation. That goes for efficacy too. On what grounds can one say that a vaccine caused a decrease in the disease it targets while assuring us that it was only correlated with an increase in side effects?
Trials just measure the incidence of things in two (or more) groups of participants. It’s a mathematical comparison. No causation is ever proven.
Vargas took issue with Kennedy’s claim that not one vaccine on the childhood immunization schedule has been subjected to a prelicensured placebo-controlled trial.
Vargas: “Yes they have.”
Kennedy: “No.”
Vargas: “Yeah, they have!”
And later …
Vargas: “The FDA says, and in fact, on its website, you can clearly see vaccines go through three stages of testing against double-blind placebo. They already DO that testing.”
Kennedy: “Elizabeth, you can say that.”
Vargas: “I’m not saying that. The FDA is saying that.”
Kennedy: “The FDA is not saying that.”
Vargas: “Yes they do! They say that on their website!”
Kennedy: “They will not tell you that there’s a vaccine that has ever undergone a long-term placebo-controlled trial prior to licensing because it’s not true.”
The reason why this embarrassing (and mildly entertaining) spectacle is important to dissect is because of what it reveals about the stubbornness we have about being right. Did Vargas actually scour the FDA website prior to this public exchange?
She couldn’t have for the obvious reason that no such statement from them exists on their website as she maintained.
Why is she so sure that she is right? I would venture to say it is because someone whom she trusts more than Kennedy told her that.
But was she really listening to what Kennedy was saying? Kennedy demanded a citation from Dr. Anthony Fauci in a face-to-face meeting with him in 2016. Fauci couldn’t produce one but promised he would.
He never did — so Kennedy (and attorney Aaron Siri) sued him and the U.S. Department of Health and Human Services (HHS). After a year of litigation, they finally obtained a written statement from the HHS which still does not cite a single study but assures us that inert placebos are not required to demonstrate safety in childhood vaccines.
Of course, there is no reason Vargas should trust Kennedy if she has not visited the Children’s Health Defense website where the letter from the HHS is made available.
But at what point should she have paused and honestly asked herself about what she really knew and not just what she thought she did?
In this case, the spectacle arose not because Vargas was wrong, but because she was so sure she was right.
It’s also worthwhile to consider what was on the line for her, personally. Was she able to face the possibility that the vaccines we have been injecting into our own bodies and our children have never been tested against a placebo?
Her argumentative responses to Kennedy’s views, which he defended with several key citations off the top of his head, reflected the real impediments the public has toward seeing reality for what it is. What would it mean if Kennedy has been right all along?
As a veteran journalist for NewsNation and previously for Fox and A&E Networks, Vargas should have come prepared. Kennedy has previously made himself very clear that he is willing to change his mind. “Show me where I got it wrong.”
Kennedy asks Vargas to cite a single prelicensure, placebo-controlled vaccine study. She couldn’t because no one can. There aren’t any.
Kennedy pointed out the real issue: “We have a corrupt federal agency [FDA] that is lying to the AMA and all those agencies and all those doctors. But those agencies are controlled by Pharma. That is the problem.”
Without any studies to cite or any way to refute Kennedy’s damning allegations, Vargas chose to confront Kennedy with the fact that some of his family members disagree with his stance on vaccines.
Kennedy: “Does your family agree with everything that you say?”
Vargas: “Definitely not. You got me on that one.”
Madhava Setty, M.D. is senior science editor for The Defender.
This article was originally published by The Defender — Children’s Health Defense’s News & Views Website under Creative Commons license CC BY-NC-ND 4.0. Please consider subscribing to The Defender or donating to Children’s Health Defense.
Rogan’s RFK interview is full of vitally-important taboo info
BY BILL RICE, JR. | JUNE 26, 2023
Yesterday, I spent several hours reading the transcript of the 3-hour interview RFK, Jr. recently did with Joe Rogan. The conversation was fascinating. Any U.S. citizen interested in more detailed information on Kennedy’s thoughts can simply watch this interview (a link to the Rogan episode and a transcript are included in this article which summarizes the interview).
I particularly recommend the final paragraphs of the CHD article, where Kennedy talks about the mothers of autistic children who finally convinced him to look into a possible connection between vaccines and autism.
Here are highlights that jumped out to me after reading transcripts of the entire interview:
- Kennedy said (again) that he’s NOT running on the “vaccine issue” and only talks about vaccines when specifically asked a question about them by an interviewer.
- However, he did say he’s not going to dodge a legitimate question when asked. He also said that he didn’t plan on doing any more in-depth interviews like this in the future, suggesting this conversation with Rogan should provide sufficient answers on why and how he got so interested in the vaccine issue … an intellectual quest which later informed his conviction that the entire public health establishment has become brazenly and shockingly corrupt and captured.
- Kennedy said alarms went off when he had a phone conversation with Dr. Paul Offit about mercury in vaccines and caught this extremely-influential vaccine booster in an obvious lie. Kennedy also noted that this man said he would get back to him with specific scientific studies that backed up his vaccine autism point (that there was bad “mercury” and “safe” mercury). Kennedy said this revered scientist never did provide the promised study(ies).
- Kennedy also recounts a similar conversation with Dr. Fauci, who told Kennedy that he would provide germane studies on some topic Kennedy had challenged Fauci on …. and Fauci never followed through.
One of Kennedy’s main points is that whenever he wanted to see the published peer-reviewed scientific studies backing different conclusions of the Science Establishment … the members of the Scientific Establishment couldn’t and didn’t do this.
Kennedy also notes he personally knows and had spoken to many leading authorities in the public health bureaucracies and he always got the impression these leaders had not read any of the scientific studies that Kennedy had read. They weren’t even familiar with these studies.
- Rogan talked a good bit about censorship and how he (Rogan) had been maligned and intentionally discredited for comments he’d made. Almost as an aside, Kennedy noted that he had been censored for “18 years” (!)
- … Kennedy also said that nobody has ever debated him on these topics, and cited examples of “debates” or events that were supposed to happen and never did.
- One such “debate” was supposed to be Kennedy vs. one of these alleged science authorities at a hearing in the Connecticut Senate (if memory serves, on the autism question).
- According to Kennedy, a Connecticut elected official asked Kennedy to participate in a hearing with this other authority. Later, Kennedy was told it would be him vs. two executives, then three, then four.
- Kennedy, as it turns out, would only get six minutes to make his points. Still, Kennedy said (paraphrasing): “This is not fair, but okay. I’ll be there.” The debate/testimony was later cancelled – after Kennedy had flown “on the red-eye” to Connecticut on his own dime to participate. Nobody told him why this hearing with him was cancelled. Kennedy just assumes someone told these people to NOT debate RFK, Jr. This scenario should sound very familiar today. (Think the “Hotez debate.”)
- I found Kennedy’s points about the explosion of autism to be very convincing. His main point is that nobody his age (or my age) grew up with anyone who had the severe autism that is common with many children today.Kennedy does note that observations such as this do NOT equal scientific “causation” or “correlation” … but when so many mothers of autistic children keep reaching the same conclusion, this should be enough anecdotal evidence to launch serious and real scientific studies and genuine scientific investigations, Kennedy argues.
- Kennedy’s points about VAERS picking up only a tiny fraction of vaccine injuries and deaths are very persuasive and important. (This is the topic of one of my next articles, which will highlight the fact Ed Dowd’s work on “all-cause excess” deaths is STILL being ignored by the mainstream media – 18 months after Dowd, among others, began to highlight this.)
- Regarding his book The Real Anthony Fauci, Kennedy notes that the book sold more than one million copies in its “first three months.” Oddly (to me), Kennedy said he doesn’t know how many copies this book sold after this because he hasn’t looked at the numbers.
- I’ve been curious about the book’s cumulative sales figure as every story I can find on the book says only that it “sold more than one million copies.”
- This is certainly a true statement, but I wonder if the book might have sold at least two million copies by now. Kennedy also points out that nobody at mainstream “news” organizations reviewed the book and very few “independent” book-sellers ever stocked the book in their stores (a point I made in a recent column.) Also, for some reason, lists of “best-selling” books often omitted The Real Anthony Fauci from these sales rankings.
- The above anecdotes should tell the public that most owners of book stores (and the “free press”) believe in banning certain books (more specifically, they don’t stock or mention books that question the prevailing orthodoxy).
- Question: How many copies of The Real Anthony Fauci would have been sold if this book had been available in bookstores all over the world (like other big best-sellers)? Would this have made a difference and perhaps saved lives?
Note: Joe Rogan said his entire thinking about vaccines, public health and Kennedy changed dramatically after he did read this book. Question: Think if Rogan had not read this book. He probably would have never had Kennedy on his show and Rogan probably would never have become one of the leading contrarian voices on the “authorized narrative.” This shows the power of the written word or of one book … and why such a book had to be censored.
- According to Kennedy, the vast majority of the book’s sales came from just one source – Amazon. (Authors like Naomi Wolf and many other skeptics of the official narratives have also published “taboo” Covid books. This question also occurs to me: How many additional copies of these books would have been sold if readers interested in these topics had seen them and been able to buy them if they had been available in local bookstore? (I guess this is another “unknown unknowable.”)
* Rogan made interesting points about how other podcasters are seemingly being bullied with the threat of “de-platforming” or “de-monetization” if the hosts of these shows invite contrarian Covid speakers onto their shows as guests (including Rogan himself).
* Rogan mentioned that he knows several comedian friends who think like he does, which he suggests helped him maintain his sanity in these New Normal Covid times. Kennedy later asked Rogan (paraphrasing), “Who are these people? I haven’t heard any stand-up comedians doing gigs where they poke fun of this Covid madness.” The Kimmels and Colberts of the world were (and still are) all singing from the same “authorized narrative” hymnal.
- Kennedy provides a good bit of detail about his life as an environmental lawyer and how he and his allies in his cause helped clean up the Hudson River waterways. It was his belief that mercury was getting into fish that later led him to believe that the same toxic mercury (far more dangerous than lead, according to Kennedy) was being injected into children with their mandatory vaccines.
- According to Kennedy, this was a point that mothers kept making to him at Kennedy’s speaking engagements. Finally, one of these mothers showed up at his house, dropped an 18-inch pile of documents on his door step and told Kennedy she wasn’t leaving until he read these documents.
- Kennedy read them … and the rest is … history … History that also explains why Robert Kennedy, Jr. is now the No. 1 threat to the Big Pharma/Medicine/Science establishment. It also explains how a once popular liberal environmental lawyer almost instantly became a pariah to the Establishment and a conspiracy-spreading, wacko kook.
- Kennedy notes that he has filed “hundreds” of lawsuits and every one of them deal with “science.” Regarding the narrative that everyone should “trust the science and the experts,” Kennedy makes a great point in his conversation with Rogan:
- Every lawsuit he has ever been a part of includes “experts” … from both sides. Kennedy gives an example of one big environmental lawsuit where the defendants called experts from prestigious academic institutions like Harvard, Stanford and Yale as witnesses. But the plaintiffs also called “expert” witnesses who were professors at the same colleges. So the obvious question is: What “experts” are more credible? This, Kennedy says, is for a jury to decide (and plenty of juries sided with Kennedy’s experts).
Kennedy also pointed out that almost all of the “new” vaccines since the late ’80s allegedly “protect” children from diseases that do not pose a real health risk to them. He gave the example of the Hepatitis B vaccine newborns get at the hospital. Kennedy pointed out this is a “vaccine” to allegedly provide “protection” against a disease that might affect only a few of these children 16 to 30 years later – if they became a prostitute or a needle drug user.
I thought Kennedy was also very persuasive, making his point that advancements in nutrition, sanitation and “engineering” almost completely explain the disappearance of most childhood or adult diseases in the last century or so (for example, refrigeration.)
This leads people like me to conclude that the Mother of All medical scams might be the one that tells us that “vaccines” are the wonder-drug of our times and have saved millions of lives. This is almost certainly a “false” or at least “dubious” narrative. (But a profitable one for Big Pharma).
Yet another fascinating segment was when Kennedy explains the “95 percent effective” canard. He points out that the best metric flowing from Pfizer’s limited safety trials should have been the conclusion that it takes 22,000 doses of Covid vaccine to (maybe) prevent one “Covid” death.
If this is the case (and it apparently is), “You better be sure that vaccine isn’t causing any deaths,” Kennedy states. As Kennedy points out, in the Pfizer trials only three people died from Covid in the ensuing six months – one person in the “vaccinated” group, and two in the “unvaccinated” group.
However, four or five more people in the “vaccinated” group later died from “all causes.” But identifying deaths from “any cause” was not a goal of the study. (It took a Freedom of Information request and a judge’s ruling to release this key information to the public … something Pfizer didn’t want to do for 75 years).
So trial participants had a much greater chance of dying (from any cause) if they’d received the Covid vaccine than if they had not been vaccinated. Question asked by Kennedy: Shouldn’t this data point/finding have been the big headline and enough to stop the vaccines?
Regarding the “vaccines-cause autism” theory, Kennedy does not definitively or categorically blame just vaccines. He seems to be saying many factors probably explain this – including vaccines.
Kennedy notes that when he was a child he received three childhood vaccines. Today, children MUST get 72 shots (from 16 vaccines). Kennedy also noted that five of his children suffer from food allergies, something that also was almost unheard of when Kennedy was growing up.
Kennedy also did a great job explaining how Big Pharma got immunity from vaccine lawsuits, per hugely-significant legislation passed in the Reagan administration in 1986. This gave Big Pharma a license to make “billions of dollars,” Kennedy argues.
All Pharma companies had to do was come up with a new “vaccine” and make sure this vaccine got placed on the childhood immunization schedule (which apparently was a sure-thing).
I also found it interesting that RFK, Jr. acknowledges that his own uncle, Sen. Ted Kennedy – who was chairman of an important Senate Health Committee at the time – helped pass this world-changing legislation. That is, it wasn’t just President Reagan who made this possible; it was the Democrats in Congress too – including his own uncle.
Kennedy also debunks the accepted wisdom that vaccines are “safe” by pointing out the whole reason this legislation was passed into law was because vaccines are obviously not (always) safe. Vaccines are inherently unsafe – this is why the industry needed legal immunity from lawsuits to keep producing them, says Kennedy.
My main-take away from this in-depth interview is how well Kennedy knows this material. During this 3-hour interview, Kennedy didn’t refer to any notes. He cited study after study from memory. He had read these studies – critically – and quickly identified the holes and likely cover-ups in them.
I’m convinced this is the real reason no expert or authority will debate someone like Kennedy (or, for example, Steve Kirsch). They all know Kennedy knows this material better than they do. And they all know that they can’t answer Kennedy’s key questions.
Hopefully, more people will take the time to watch this 3-hour interview or read the transcripts. If they do, they’ll see that Kennedy is not some crazy “kook.” I also commend Joe Rogan for giving RFK, Jr. this 3-hour platform to express his views and more fully discuss these life-and-death public health issues.
The disgrace of Australia’s pandemic betrayal
By Paul Collits | TCW Defending Freedom | June 27, 2023
What exactly do you do when your country betrays you and disgraces itself before the world? When you find out that it is run by thugs and goons? When just about no one in the political class has the moral compass and the spine to stand up for you? When your fellow citizens turn on you if you dared to question things?
 If you are John Stapleton, a retired Aussie journalist, you write a 450-page book about it. You call it Australia Breaks Apart. You write uncomprehendingly, elegantly, passionately, even elegiacally, ashamed, still shaking your head in disbelief, three years after a ho-hum virus called by the powers-that-be ‘Covid’ reached our shores.
If you are John Stapleton, a retired Aussie journalist, you write a 450-page book about it. You call it Australia Breaks Apart. You write uncomprehendingly, elegantly, passionately, even elegiacally, ashamed, still shaking your head in disbelief, three years after a ho-hum virus called by the powers-that-be ‘Covid’ reached our shores.
Surely these words could be written about just about every country in the world, you might think. Two quick responses – we were the worst, and surely we, of all places, should have been above all this.
Whether the book explains to international readers how this all happened, I’m not sure. I am far from certain that anyone could explain it. But let us explore what the book does do.
The title suggests one of the main themes, that of division and enmity. There were members of the dobber class, the Covid winners (largely in the employ of government or corporates), the lap-top class, the blatherers. People on ‘the other side’ were routinely demonised. Granny killers, conspiracy theorists, neo-Nazis and so on. Many of these folks were morally upright, seasoned professionals, not rent-a-crowd ideologues. Australia did indeed break apart, literally as well as socially. State and territory borders were closed by spooked politicians on a whim and for very few Covid cases. Fear and derangement were everywhere. Subjugation.
There are things in the book that even those who lived through the nightmare will not have known. These matters should have been known, and most likely would have been, if not for the cover-ups and the wilful non-reportage of stories in the interest of defending ‘the narrative’.
The book tells not only the story of Covid policy excesses, but also of a resistance movement that grew into something astonishing. This underground, though in plain sight, movement of angry men and women became hundreds of thousands, if not millions. It has remained invisible only because the quisling Covid class and their corrupt media puppets refused to acknowledge that it even existed, other than being a ‘tiny’ bunch of anti-vaxxer conspiracy theorists to be ignored.
John Stapleton doesn’t ignore them. He tells their story. This makes his book unique. The expected villains are all there, in graphic detail – Victoria premier Daniel Andrews, a truly appalling political figure, the thug police, the slippery bob-each-way villain-prime minister Scott Morrison, the other premiers and chief ministers, the unaccountable bureaucrats, the public health gauleiters, the Pharma-funded academics, the media shills. But what emerges in the book is an account of how resistance to tyranny can form and grow. This will be an invaluable resource when the medical totalitarians come for us next time, as surely they will.
The story is told through the eyes of Old Alex (the author), an old-time ‘pressman’ with a nose for a story and an unquenchable desire to unearth the truth. And, importantly, an open mind and no corporate constraints. Like many Covid dissidents, Stapleton made new friends during the Covid years, just about all of them independent truth-tellers. Citizen journalists. And he lost all sense of mainstream journalism having a soul and a purpose. Silent journalists were high up on Stapleton’s list of Covid criminals to be despised. But the stories of new voices and new connections among the refuseniks show the book to be about heroes as well as villains.
Journalism had very few dissidents who spoke out. Nor did the public servants or politicians or the police, but there were a few brave souls among the latter (for example) who broke ranks and saw Covid police brutality as a hill on which (professionally) to die. There was Andrew Cooney in New South Wales and Krystle Mitchell in Victoria.
These brave hearts were not willing to go along to get along, as rubber bullets penetrated backs, grandmothers were shoved to the pavement then pepper-sprayed, and the heads of mentally challenged innocents were smashed against concrete floors in downtown Melbourne. These stories of fascist policing were systematically smothered by the legacy media and the protesters pilloried and defamed.
The book details so much more. The scandal of the quarantine camps, for example. Those gazillion-dollar, Orwellian white elephants. The bullshit Covid-speak pronouncements from on high. The thousands upon thousands of (often massive) fines for Covid misdemeanours. The National Cabinet mutual protection narratives. All based on lies. Deadly lies. Some of the Covid class still promote the shots. Amid the ever-rising, murky waters of excess deaths. Including, perhaps, that of the Australian legend Shane Warne. Deaths still unexamined by the Covid class.
We need this book, and those like it. More straight history than exposé, but no less significant for this. True crime reporting, if you will. And if you didn’t hate the Covid class before you open the book, I guarantee you will by the end, if not sooner.
There are those who might say, why dredge it all up again since we have ‘moved on’? Well, among those that Covid refuseniks detest the most, the ‘let’s just move on’ types rank pretty high. This book should be for them to read and to reflect upon. To contemplate the massive pain caused, and to ponder the fact that it is all likely to happen again, what with the great reset people and the pandemic planning industry already on high alert for the first opportunity to crank up the machine again. Moving on, not holding ‘them’, the Covid class, to account, will only make the next instalment all the more likely.
Oh yes, for those who lived through the nightmare, John Stapleton’s gripping book, while reviving painful memories in great detail, is a must-read account of the evil that men (and women) do. It is a thundering reminder, too, of the need for Covid accountability, and a spur to further action among a new Coalition of the Willing minded to pursue it, and who simply must not give up the fight in the face of performative Covid class insouciance. It is ironic, too, that Australia Breaks Apart has been published just as the stampede for the exit door by Covid’s decision-makers has reached a crescendo.
In the dying days of the narrative, there was a national election, with one party of despised Covideers replaced by another, and around a third of now largely unrepresented voters, many of them the deplorables featured in Stapleton’s book, refusing to support either major party. The great political escape raises the question, was all the protesting worth it? I recently put a similar question to Ian Plimer, the doyen of Australian climate sceptics – why does he keep writing books when the climate writing seems to be on the wall? He replied that it was critical that when the history of all this comes to be written one day, there will be a record of the madness.
Buy this book, this chronicle of the new totalitarianism, the definitive account of Covid Australia, then circulate it widely among those might think it didn’t really matter what they did to us. A short review cannot do justice to this deeply authentic, often transcendent and, indeed, magisterial work. An astonishing achievement. An Australian story.
See also:
Essential Reading for the Dissident, the Disenfranchised, the Disillusioned
Serious adverse events from Pfizer’s mRNA vaccine are not “rare”
Maryanne Demasi, reports | June 27, 2023
Drug regulators and public health agencies have saturated the airways with claims that serious harms following covid vaccination are “rare.”

But there has been very little scrutiny of that claim by the media, and I could not find an instance where international agencies actually quantified what they meant by the term “rare” or provided a scientific source.
The best evidence so far, has been a study published in one of vaccinology’s most prestigious journals, where independent researchers reanalysed the original trial data for the mRNA vaccines.
The authors, Fraiman et al, found that serious adverse events (SAEs) – i.e. adverse events that require hospitalisation – were elevated in the vaccine arm by an alarming rate – 1 additional SAE for every 556 people vaccinated with Pfizer’s mRNA vaccine.
According to a scale used by drug regulators, SAEs occurring at a rate of 1 in 556 is categorised as “uncommon,” but far more common than what the public has been told.

Therefore, I asked eight drug regulators and public health agencies to answer a simple question: what is the official calculated rate of SAEs believed to be caused by Pfizer’s mRNA vaccine, and what is the evidence?
The agencies were FDA, TGA, MHRA, HC, PEI, CDC, ECDC and EMA.
The outcome was startling.
Not a single agency could cite the SAE rate of Pfizer’s vaccine. Most directed me to pharmacovigilance data, which they all emphasised does not establish causation.
The Australian TGA, for example, referred me to the spontaneous reporting system but warned, “it is not possible to meaningfully use these data to calculate the true incidence of adverse events due to the limitations of spontaneous reporting systems.”
Both the German regulator (PEI) and European CDC referred me to the European Medicines Agency which, according to its own report, saw no increase at all in SAEs. “SAEs occurred at a low frequency in both vaccinated and the placebo group at 0.6%.”
The UK regulator MHRA went so far as to state it “does not make estimations of a serious adverse event (SAE) rate, or a rate for adverse reactions considered to be causally related for any medicinal product.”
The US FDA, on the other hand, did conceded that SAEs after mRNA vaccination have “indeed been higher than that of influenza vaccines,” but suggested it was justified because “the severity and impact of covid-19 on public health have been significantly higher than those of seasonal influenza.”
Despite analysing at the same dataset as Fraiman, the FDA said it “disagrees with the conclusions” of the Fraiman analysis. The agency did not give specifics on the areas of disagreement, nor did it provide its own rate of SAEs.
In response to the criticism, Joe Fraiman, emergency doctor and lead author on the reanalysis said, “To be honest, I’m not that surprised that agencies have not determined the rate of SAEs. Once these agencies approve a drug there’s no incentive for them to monitor harms.”
Fraiman said it’s hypocritical for health agencies to tell people that serious harms of the covid vaccines are rare, when they have not even determined the SAE rate themselves.
“It’s very dangerous not to be honest with the public,” said Fraiman, who recently called for the mRNA vaccines to be suspended.
“These noble lies may get people vaccinated in the short term but you’re creating decades or generations of distrust when it’s revealed that they have been misleading the public,” added Fraiman.
Dick Bijl, a physician and epidemiologist based in the Netherlands, agreed. “It goes to show how corrupted these agencies are. There is no transparency, especially since regulators are largely funded by the drug industry.”
Bijl said it’s vital to know the rate of SAEs for the vaccines. “You must be able to do a harm:benefit analysis, to allow people to give fully informed consent, especially in young people at low risk of serious covid or those who have natural immunity.”
Bijl said the mainstream media has allowed these agencies to make false claims about the safety of vaccines without interrogating the facts.
“The rise of alternative media is strongly related to the lies being told by the legacy media, which just repeats government narratives and industry marketing. In the Netherlands, there is a lot of discussion about the distrust in public messaging,” said Bijl.
CDC Panel Recommends Pfizer Pneumococcal Vaccines for Infants, RSV Vaccines for Adults
By Michael Nevradakis, Ph.D. | The Defender | June 26, 2023
Advisers to the Centers for Disease Control and Prevention (CDC) last week recommended newly approved vaccines for respiratory syncytial virus (RSV) — despite concerns about the efficacy and safety of the new vaccines, potentially harmful interactions with the flu and COVID-19 vaccines and the unspecified cost for the vaccines.
In a three-day meeting that ended Friday, the CDC’s Advisory Committee on Immunization Practices (ACIP) also:
- Recommended a new pneumococcal conjugate vaccine as an “option” for children.
- Discussed COVID-19 bivalent vaccines and vaccines for meningitis, polio, dengue, monkeypox and chikungunya vaccines.
- Discussed proposals regarding the vaccine schedule.
- Suggested the removal of egg allergies as a contraindication to vaccines made in eggs.
For Dr. Meryl Nass, an internist, biological warfare epidemiologist and member of the Children’s Health Defense (CHD) scientific advisory committee, last week’s proceedings lacked the due diligence needed to fully ascertain the safety of the vaccines and treatments being reviewed.
Writing on her blog, Nass stated:
“The mission of CDC and the ACIP members is to sign off on all possible vaccines as safe and effective, and to never turn over any stones that could reveal anything different. Then to roll all vaccines out to as broad a group of humans as humanly possible.”
ACIP says seniors ‘may’ get RSV vaccine, but overlooks other safety concerns
According to MedPage Today, ACIP recommended the new RSV vaccines for older adults on Wednesday “but opted not to give their strongest endorsement,” instead recommending “a talk with [a] medical provider first.”
STAT reported that ACIP recommended “anyone 60 and over should be able to get one of the new [RSV] vaccines … if they and their physicians think it would be worthwhile.”
According to STAT, ACIP was initially slated to vote on a broader recommendation that would have “urged all people 65 and older to get vaccinated” for RSV.
However, “that recommendation was watered down” after “several members of the committee expressed serious concerns about the decisions they were being asked to make based on the data the companies had provided.”
Reuters reported that while some committee members wanted to stick with the broader recommendation, “others had concerns that there was not enough data about how effective the vaccines are in people over the age of 75 and other high-risk groups.”
Two votes followed. In one, ACIP was asked whether “adults 65 years of age and older are recommended to receive a single dose of RSV vaccine.” The committee voted 9-5 to recommend that those age 65 and over “may” get an RSV vaccine after consultation with a doctor or pharmacist.
The other vote asked ACIP’s members whether “individual adults ages 60-64 may receive a single dose of RSV vaccine, using shared clinical decision-making” — that is, consultation with a doctor or pharmacist. Here, the result was 13-0 in favor, with one abstention.
ACIP’s recommendations are headed to the desk of outgoing CDC Director Rochelle Walensky, who is expected to sign off on them early this week. Her last day as head of the CDC is June 30. However, ACIP recommendations are not considered final until they are published in the Morbidity and Mortality Weekly Report.
The FDA recently approved the two vaccines — Pfizer’s Abrysvo and GSK’s Arexvy.
According to STAT, “It is expected both companies will provide vaccines to the market in time for the next RSV season.” However, the mild recommendations from ACIP “will likely lead to a lower uptake of the new vaccines than the manufacturers might have expected.”
Nass noted that data presented to ACIP indicated that out of 40,000 participants in the RSV vaccine clinical trials, six developed Guillain-Barré syndrome (GBS), a rare disorder in which the immune system attacks the nerves or a GBS-type illness. This was compared to no GBS cases in the control group.
According to CNN, some ACIP members expressed concern that few adults over 75 and older were enrolled in the Pfizer and GSK clinical trials, even though they represent the group most at risk from RSV.
The immunocompromised and those living in “settings such as nursing homes are also at elevated risk but were not enrolled in the studies,” STAT reported.
In addition, according to MedPage Today, approvals of the two RSV vaccines “were based on efficacy data spanning a single RSV season.” At the ACIP meeting, Pfizer and GSK representatives “presented data showing that vaccine efficacy largely held up through the first part of the second RSV season, but did drop slightly.”
Some concerns were also raised regarding the concurrent administration of RSV vaccines alongside flu and COVID-19 shots.
According to STAT, “these vaccines will likely be given at the same time of the year … and it’s not yet clear if giving the vaccines at the same time undermines the immune responses they generate” because studies of concomitant administration of COVID and RSV vaccines are still underway.
GSK claimed that when its RSV vaccine was administered along with a flu vaccine, “It was safe and well-tolerated,” CNN reported.
The cost of the vaccine also drew criticism. According to MedPage Today, Pfizer and GSK proposed a range of prices spanning between $180 and $295, but according to STAT, “Both companies resisted strong pressure from the committee to commit to a firm price.”
According to Reuters, “Pfizer and GSK have said they expect RSV vaccines to eventually become multibillion-dollar sellers.” However, Fierce Pharma reported that ACIP’s “tepid endorsement for the vaccines could hinder sales.”
For 2023, GSK “expects the U.S. market to be in the range of 10 million to 15 million people, a fraction of the size of the expected flu or COVID-19 market,” Reuters stated.
Pneumococcal vaccine approved as ‘option’ for infants as young as 2 months old
ACIP voted unanimously in favor of adding Pfizer’s new 20-valent pneumococcal conjugate vaccine (Prevnar, or PCV20) — currently administered only to adults — as an “option” for children, MedPage Today reported.
According to the AAP, “Pfizer’s PCV20 adds serotypes 8, 10A, 11A, 12F, 15B, which are not covered in PCV15,” a previously existing vaccine.
ACIP voted in favor of:
- Routine use of either PCV20 or PCV15 in children aged 2-23 months.
- Administration of either PCV15 or PCV20 in children aged 24-59 months with incomplete PCV vaccination status, and in children aged 24-71 months with certain underlying conditions and incomplete PCV vaccination status.
- Vaccination of children between 2 and 18 years of age with PCV20, or with pneumococcal polysaccharide vaccine (PPSV23) if they previously had only received PCV13 or PCV15.
- A single dose of PCV15 or PCV20 to children between 6 and 18 years of age with any risk condition who have not received any dose of PCV13, PCV15 or PCV20. If PCV15 is administered, the committee said it should be followed by a dose of PPSV23 at least eight weeks after the initial vaccination.
According to Nass, PPSV23 is “very inflammatory” and it is “unclear how well/if it works.”
Moreover, according to MedPage Today, ACIP expanded its definition of high-risk children to include conditions such as moderate persistent and severe persistent asthma, chronic kidney disease (excluding dialysis patients), chronic liver disease and those with renal failure on maintenance dialysis.
Some committee members “expressed concern over the lack of clinical data for the new vaccines,” MedPage Today reported, including “no effectiveness and no efficacy data on either PCV15 or PCV20.”
Nass noted that “the CDC presented no good data on these new vaccines,” instead presenting “economic models” in lieu of this data, adding, though, that “reliable data to plug into the models” is lacking.
Despite this missing data, an ACIP member quoted by Nass said, “Our CDC colleagues are masters at epidemiology surveillance that will give us the answer in [the] future” — “In other words,” Nass said, “‘we won’t know if it works unless we give it to millions of children, so what are we waiting for?’”
Third monkeypox vaccine dose not recommended — for now
ACIP considered, but rejected, recommending a third dose of the Jynneos vaccine for monkeypox.
However, the committee did encourage “2-dose vaccinations among persons who do not have immunity and optimizing immune function … ideally before mpox exposure.”
ACIP also recommended “persons eligible for vaccination, particularly those with advanced HIV and other immunocompromising conditions, should receive two doses of Jynneos vaccine,” adding that “Additional research on the durability of Jynneos vaccine-induced immunity is needed.”
In response, Nass remarked, “Let me remind you that monkeypox is essentially like shingles … It is a mild disease and there is no need for a vaccine for 99.9% of people; and if you get it, you will probably have real immunity afterwards.”
“CDC is willing to give it along with COVID vaccines, even though that probably magnifies the risk of myocarditis,” Nass added.
The committee also discussed, but did not act on, proposals to expand the use of Jynneos to children and pregnant and breastfeeding women.
Other vaccines also on ACIP’s agenda, but no decisions made
According to APP, “ACIP members reviewed data on Friday regarding the safety of aluminum in vaccines,” reviewing the results of a study finding a possible link between aluminum and childhood asthma.
However, it was determined that the study had “important limitations” and that its findings “do not prove causation,” although “a follow-up study with a larger group of children and longer follow-up time” will subsequently be performed. Ultimately, ACIP “did not recommend changing the vaccine schedule.”
Nass noted that links between aluminum, and diabetes and eczema, were also discussed, with a “small positive association” found in the case of eczema and asthma.
ACIP members also examined the possibility of “simplifying COVID vaccine recommendations for children ages 2-4 years,” according to the APP, looking “at the possibility of requiring only one dose for this group instead of two to three.”
ACIP’s COVID-19 vaccine work group said “it would support a single, potentially annual, dose for children ages 2 years and older, while maintaining multiple doses for those under 2.” However, no vote was taken.
Some committee members argued that “Simplifying the recommendations also may lead to more children getting vaccinated,” citing low uptake in children under age 2.
A new pentavalent meningococcal vaccine, combining two existing vaccines into one, was also discussed — a vaccine which, according to Nass, “is not needed.” No discussion of the safety of the existing meningitis vaccines took place at the meeting, Nass said.
Also on ACIP’s agenda was a recommendation under consideration for a single polio shot for all individuals who are unsure whether they were fully vaccinated as children or who expect to visit high-risk environments. Again, no decisions were made.
Vaccines for dengue and chikungunya — two mosquito-borne diseases which are rare in the U.S. — were also discussed by ACIP, with no outcome arising from the meeting.
Reactogenicity got magically turned into safety, and safety got thrown away’
ACIP also voted 14-0 that it is no longer necessary for individuals with egg allergies to receive their flu vaccine in a medical setting, noting that “immunization best practice guidelines already call for all vaccine providers to be equipped to handle anaphylaxis,” as reported by the American Academy of Pediatrics (AAP).
“Any flu vaccine appropriate for the person’s age and health status can be used regardless of whether it is egg-based,” AAP stated. This decision awaits CDC approval.
“CDC has been trying to get rid of vaccine contraindications for the past five years, despite lack of supportive evidence,” Nass said. Following ACIP’s vote, “egg allergies as a contraindication or precaution for flu shots is about to disappear.”
Nass told The Defender that while “there used to be three things a vaccine had to be tested for — purity, potency and safety,” safety has now “morphed into sterility” — meaning it doesn’t contain “outside germs,” according to a new definition from the U.S. Department of Health and Human Services.
“There used to be a word — reactogenicity — for acute reactions to a vaccine,” Nass said, referring to the physical manifestation of the body’s inflammatory response to vaccination. She also noted that “safety” was “primarily concerned with longer-term or non-resolving side effects,” including “serious side effects.”
“But reactogenicity got magically turned into safety, and safety got thrown away.”
Michael Nevradakis, Ph.D., based in Athens, Greece, is a senior reporter for The Defender and part of the rotation of hosts for CHD.TV’s “Good Morning CHD.”
This article was originally published by The Defender — Children’s Health Defense’s News & Views Website under Creative Commons license CC BY-NC-ND 4.0. Please consider subscribing to The Defender or donating to Children’s Health Defense.
mRNA: Vaccine or Gene Therapy? The Safety Regulatory Issues
Dr. Helene Banoun Elucidates the History of Misguided Use of Genetic Code for Vaccination
By Peter A. McCullough, MD, MPH | Courageous Discourse | June 26, 2023
I have been impressed with the quality of scholarship from independent academic researchers during the pandemic. During this time there has been a silence from academia in terms of any viewpoints that deviate from the mainstream scientific narrative. Dr. Helene Banoun is an independent researcher, former research fellow at INSERM (French Institute for Health and Medical Research), Marseille, France. She has published several very important review papers during the crisis.
Dr. Banoun has recently published an analysis on the mRNA vaccines in consideration of definitions and regulations that apply to gene therapy. For most people vaccinated, it was the first time they had been injected synthetic genetic code for a potentially lethal foreign protein (Wuhan Spike protein). A perfectly compliant American who started the COVID-19 vaccination program on time is on their seventh mRNA injection—an astonishing observation given the lack of any safety information concerning the cumulative effect of frequent, serial administrations. Banoun makes the case that they should be classified as gene therapy products. I have heard no counter arguments to the contrary.

Banoun, H. mRNA: Vaccine or Gene Therapy? The Safety Regulatory Issues. Int. J. Mol. Sci. 2023, 24, 10514. https://doi.org/10.3390/ijms241310514
Banoun goes on to state: “The wide and persistent biodistribution of mRNAs and their protein products, incompletely studied due to their classification as vaccines, raises safety issues. Post-marketing studies have shown that mRNA passes into breast milk and could have adverse effects on breast-fed babies. Long-term expression, integration into the genome, transmission to the germline, passage into sperm, embryo/fetal and perinatal toxicity, genotoxicity and tumorigenicity should be studied in light of the adverse events reported in pharmacovigilance databases.”
This is important for discussants and litigators to have this predicate. Genetic vaccines are gene therapy products, all the regulations, laws, and safety protections should be called for and pointed out when missing in the discussion on the next steps to be taken on mRNA genetic vaccines.
Aluminium and Breast Cancer
Building the scientific case
BY DR CHRISTOPHER EXLEY | JUNE 20, 2023
In my recent book I write about building a case for an aetiological role for aluminium in breast cancer. Herein I will revisit the chapter in my book and examine the case for aluminium anew.
My interest in breast cancer was sparked by the research of oncologist Philippa Darbre linking breast cancer incidence and occurrence with the regular use of antiperspirants. My interest in these ‘cosmetics’ went back much further and I was concerned that antiperspirants were significant contributors to the body burden of aluminium. Please read my book for an account of the history, but to cut a long story short, I collaborated with Darbre and we showed that breast tissue biopsies obtained from women with breast cancer contained aluminium. Of particular interest was that breast tissues closest to the underarm consistently contained a higher content of aluminium. Of course, our research was ignored by the breast cancer community and campaigned against by breast cancer charities, including the charity that provided the breast tissue biopsies used in our study! However, it was followed up by a number of research groups in Europe and the US and evidence began to be put forward to support aluminium as a carcinogen in breast cancer. Perhaps foremost amongst these groups is research led by Stefano Mandriota in Switzerland. Mandriota, an oncologist of some repute, showed that mouse mammary epithelial cells underwent malignant transformations upon exposure to aluminium. Aluminium-induced tumours were the result of genomic instability. The most recent publication from this group highlights the importance of chromosome instability in aluminium’s carcinogenicity. Mandriota’s meticulous cell and animal studies are building the case for a role for aluminium in breast cancer. These studies continue today and deserve our full support.
A role for aluminium in breast cancer is not dependent upon a link to the regular use of antiperspirants. However, the most definitive clinical trial yet to fully investigate such a link makes a very compelling case. The study found both significantly increased concentrations of aluminium in breast tissue in breast cancer and a significant increased risk of breast cancer in women who used an antiperspirant several times a day. Confirmation of increased content of aluminium in breast tissue in breast cancer asks the question at least as to the role played by aluminium-based antiperspirants in the accumulation of aluminium in breast tissue. Note that contrary to the information repeatedly reported by the antiperspirant industry these ‘cosmetics’ do not prevent sweating by simply acting as plugs in the sweat gland. These ‘cosmetics’ prevent sweating by inhibition of the activity of the sweat gland by aluminium. The industry is well aware of this but cannot admit to such since this would change the categorisation of antiperspirants from simple cosmetics to a medicine. The latter requiring authorisation through clinical trials demonstrating both safety and efficacy. (Well, this used to be the case prior to covid vaccines.) Since sweating is a significant route of excretion of aluminium from the body, inhibiting sweating in the underarm region is likely to promote accumulation of aluminium in the surrounding tissue.
The industry actively ignores the science and attempts to defend itself by funding studies that desperately look to minimise the role of antiperspirants in the accumulation of aluminium in breast tissue. Let me be frank about such published work. I do not believe them. They set out to prove a point and, hey presto, the results prove their point. The recent study I have highlighted is wholly funded by the antiperspirant industry, its interpretation is wholly dependent upon the premise that antiperspirants are simply acting as plugs in sweat glands and as a clue to its bias one can notice that it only cites industry publications and completely ignores all previous independent research in this field. One can only surmise that the journal editor and manuscript referees are either stupid or, perhaps more likely, industry affiliates.
I have built a case for a role for aluminium in breast cancer and I will continue to watch with interest the new and independent research that tests this role. In the meantime those who are interested might like to visit the website of my good friend Eileen whose untiring work endeavours to bring this story to a wider audience.
Clinical Trial to License RotaTeq, Like Almost All Childhood Vaccines, Did Not Use a Placebo Control
Those attacking RFK are wrong
BY AARON SIRI | INJECTING FREEDOM | JUNE 25, 2023
Robert F. Kennedy, Jr. is on record stating that almost all childhood vaccines were licensed based on clinical trials that did not include a placebo control. He is correct.
Nonetheless, numerous news outlets, such as Stat News in its article titled “Correcting Robert F. Kennedy Jr.’s vaccine ‘facts’”, are stating Mr. Kennedy is wrong because they claim the clinical trial relied upon to license the rotavirus vaccine, RotaTeq, did include a placebo control. They are wrong.
A placebo is defined by the CDC as a “substance or treatment that has no effect on living beings.” This means a saline injection or water drops in mouth.

RotaTeq is administered via oral drops. A “placebo” would have been water drops in the mouth. The control used in the trial, however, included bioactive ingredients including almost all the ingredients in the RotaTeq vaccine itself.
How do I know this? Because in 2018, on behalf of ICAN, we were investigating the control used in each clinical trial relied upon by the FDA to license each childhood vaccine.
In that review, we found that while the package insert for the RotaTeq vaccine says the control in its clinical trial was a “placebo,” when we read the FDA’s clinical trial review for RotaTeq, the ingredients of this so-called “placebo” were redacted:
So, on behalf of ICAN we submitted a Freedom of Information Act Request to the FDA for “Documents sufficient to identify the ingredients of the ‘placebo’ in the prelicensure clinical trials identified in Section 6.1 of the package insert for RotaTeq.”
In a response dated June 14, 2018, the FDA provided the requested documents which clearly show that the control was not a placebo. Rather, it included polysorbate-80, sodium citrate, sodium phosphate, and sucrose.
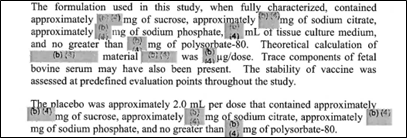
These same four ingredients are also contained in RotaTeq. The only difference between the vaccine and the control is that RotaTeq also included tissue culture medium and rotavirus reassortments. So, bottom line: the control used in the RotaTeq clinical trial was not a placebo since it included bioactive ingredients.
For example, here is what the NIH explains about sodium phosphate, one of the ingredients in the control:
Sodium Phosphate can cause serious kidney damage and possibly death. In some cases, this damage was permanent, and some people whose kidneys were damaged had to be treated with dialysis (treatment to remove waste from the blood when the kidneys are not working well). Some people developed kidney damage within a few days after their treatment, and others developed kidney damage up to several months after their treatment.
And as these studies and data sheet make clear, polysorbate-80 is far from an inert substance, is bioactive, and can have safety concerns, especially when given to infants.
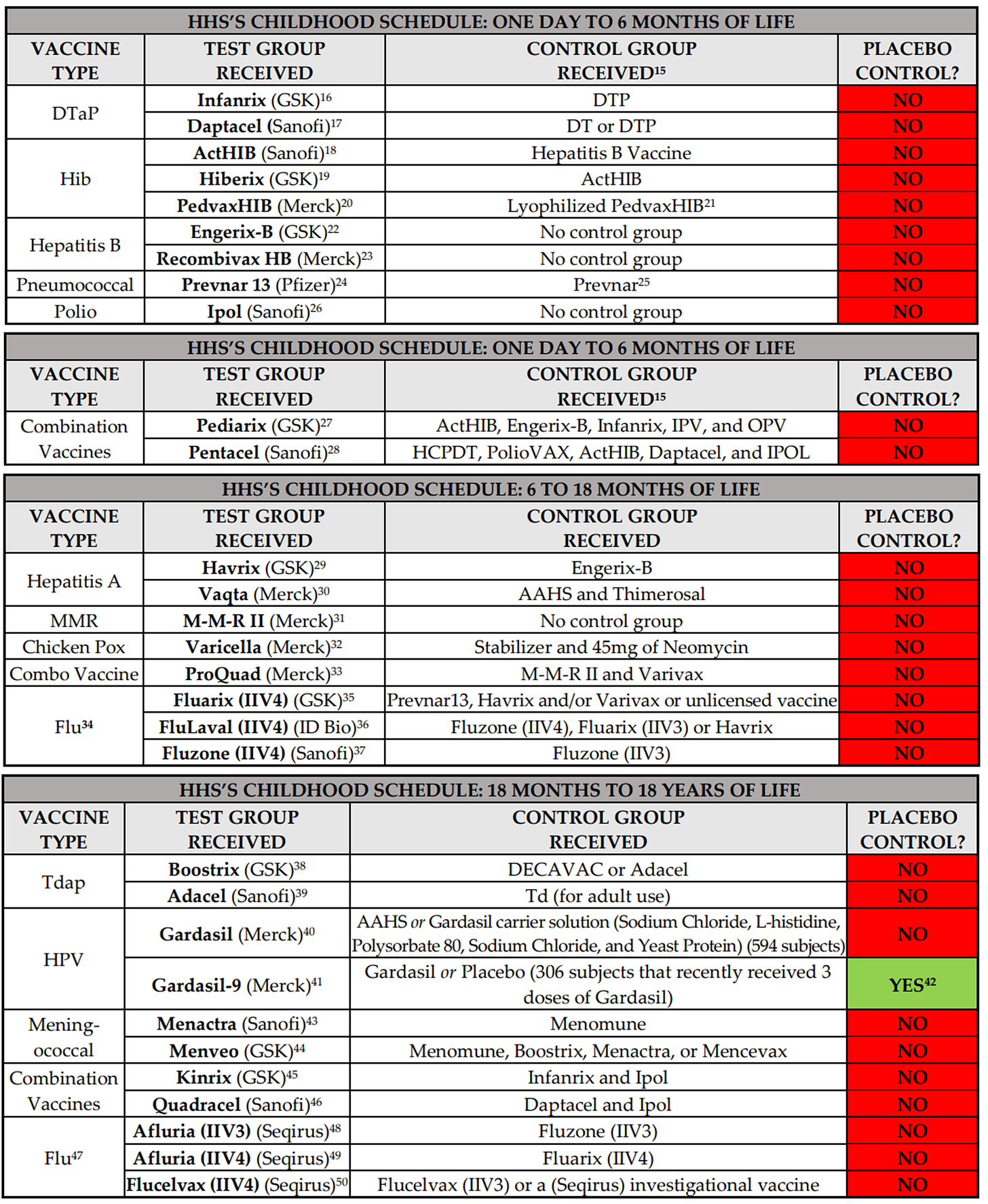
Bottom line, Robert F. Kennedy, Jr.’s claim that virtually all childhood vaccines were licensed based on clinical trials that did not include a control group that received a placebo is correct. The undisputable evidence for this claim, all from FDA or pharma sources, is detailed on pages 3 to 7 of a response we sent to HHS on December 31, 2018. (In sharp contrast to virtually all other childhood vaccines, the clinical trial relied on to license Pfizer’s Covid-19 vaccine for teenagers 12 to 17 years of age appears to have had a placebo control group, though we are still reviewing that claim.)
Here are copies of the charts from that 2018 response to HHS which show what the control group received in each clinical trial for each childhood vaccine:
It is also why the following claim by Dr. Paul Offit in his article “Should Scientists Debate the Undebatable” is categorically false: “All vaccines are tested in placebo-controlled trials before licensure.”
I would more than welcome a public debate with Dr. Offit on this point and would welcome being proven wrong – would gladly prefer that products injected into babies not have this safety gap. Oh, but wait, Dr. Offit says it is undebatable, which again shows precisely why there must always be complete, uncoerced choice when it comes to any medical product.
What is really incredible about the attacks on Mr. Kennedy is that he has made clear he has no intention of changing anyone’s right to obtain vaccines. Everyone who wants to keep vaccinating will be free to do so. He just wants to assure freedom of choice and help those who are injured by these products.
The media and medical profession’s attack on this position is callous. Just as they care about those injured by infectious disease, as Mr. Kennedy certainly does, they should also care about those injured by vaccines. Mr. Kennedy is clear that we can and should do both. And to his amazing credit, no amount of insult or attack has moved him from his position that we must protect every American, including those injured by these pharma products.
Was SARS-CoV-2 entirely novel or particularly deadly?
BY THOMAS VERDUYN, DR TODD KENYON, DR JONATHAN ENGLER | PANDA | JUNE 22, 2023
As part of our inquiry into the drivers of excess deaths, we take a step back and address the central theme of the Covid-era narrative: that SARS-CoV-2 is a novel virus that is so deadly that drastic measures were needed to contain it.
In the previous articles of this mini series about excess deaths we looked at how effective the Covid shots were at arresting Covid [1, 2] and also how bad the “first wave” in New York city was.[3] There are good reasons behind why we chose to address these two topics first. One reason is that an honest look at these issues helps establish a balanced understanding of what might be driving excess deaths since 2020. Another reason is that both topics were central to the official narrative emanating from government sources and the mainstream media. We were told that the whole point of the lockdowns was to delay the spread of SARS-CoV-2 until a vaccine could be developed that would spare us from overwhelmed hospitals like what happened in places like New York and Italy.
As has been shown, and to put it mildly, the Covid shots did not perform nearly as well as promised. Sadly, the burden of the adverse events caused by the experimental shots turned out to be worse than the disease.[4] Furthermore, by a close examination of excess deaths in New York city in early 2020, and in particular by a comparison to what happened on the Diamond Princess, it was concluded that the tragedy in New York was not compatible with the spread of a virus such as SARS-CoV-2, let alone any other generally mild respiratory virus.
All of this presses us to take a step back and address the central theme of the Covid-era narrative, namely the idea that SARS-CoV-2 is a novel virus that is particularly deadly; so deadly that drastic measures were needed to contain it. We begin with a look at the idea that the virus is novel.
1. How novel is SARS-CoV-2?
In the field of virology, the term “novel virus” typically means that the virus was recently discovered. This definition, of course, tells us nothing at all about when the virus first existed. Thus, for instance, the first human-coronavirus was found in 1961.[5] It was labeled B814 and identified as a cause of the common cold. This does not mean that this particular cold-causing coronavirus suddenly appeared in that year. No, and much to the rather, it only means someone finally found it. The ability to isolate, identify and sequence RNA viruses is a relatively new science. The patent on the process used in PCR machines was first granted in 1987.[6] It was in 2003, only 20 years ago, that the first human reference genome was sequenced. Despite all the efforts by many scientists, mankind has not yet sequenced every virus on planet earth. It is quite possible we never will. As a result, we are hardly in a position to assert when a particular virus (or strain of a virus) first appeared. Even if sequencing of a virus could prove beyond reasonable doubt that it was made in a laboratory, unless we had lab records to prove when it was made, it would still be nearly impossible to determine when it first infected someone. At best we might be able to estimate a timeframe by using antibody tests applied to stored specimens. The fact that SARS-CoV-2 is a relatively mild virus with symptoms similar to that caused by the flu only compounds the challenge. All we know for certain about this virus is that labs first began testing for it in early 2020.
The real problem with all of this is that during the Covid era the term “novel virus” was used by many outlets (including universities, journals, the media, and government officials) to mean something quite different from “recently discovered.”[7] For example, the GoodRx website has an article in which the authors say that “SARS-CoV-2, the virus that causes COVID-19, is a “novel coronavirus.” This means it’s different from all viruses like it.” They go on to say that “In medicine, novel refers to a virus or bacteria that wasn’t known to affect humans. This means that the bug is either brand new or was only found in animals or other life forms.” [8] Likewise, Dr. Tam, the chief medical officer of Canada, recently wrote, “In March 2020, Canada was faced with a… virulent pathogen… for which there was no natural immunity… and no effective antivirals.” So we see that the official narrative was not only that SARS-CoV-2 was recently discovered, but that it did not exist before late December 2019, was different from other viruses, was newly capable of infecting humans, was entirely new to our immune system, and was outside the scope of what doctors knew how to treat.
Are any of these claims true? Other than the fact that it was recently identified, the other claims are either false or dubious at best. It is useful to examine each claim on its own. We begin with a brief investigation into the possibility that SARS-CoV-2 existed before December 2019. Actually, there is growing evidence that SARS-CoV-2 was around long before it suddenly acquired international attention. For instance, by searching through the public sequencing data archives, a group of researchers found that soil samples collected in Antarctica between Dec 2018 and Jan 2019 contained “sequence fragments matching the SARS-CoV-2 reference genome…” [9] This was so contrary to the official narrative that the authors later suggested that it had to be on account of laboratory contamination issues. But their findings were not unique. For example, by examining human blood samples taken in Italy before the Covid era, researchers found that already by September of 2019 some individuals (none of whom were sick at the time) had SARS-CoV-2 specific antibodies in their blood.[10 11] Other studies have found similarly.[12] Therefore, there is good evidence that the virus existed long before it garnered any attention.
Second, was SARS-CoV-2 that different from other viruses? The very fact that the virus was named “SARS-CoV-2” informs us that virologists think it is similar enough to SARS that it didn’t even warrant an entirely new name. Indeed, the two viruses are said to share “79.5% sequence identity.” [13] Despite the 20.5% difference, and notwithstanding the 17 year time lapse, studies have shown that people that were infected with SARS “possess long-lasting memory T cells… that displayed robust cross-reactivity to the N-protein of SARS-CoV-2.”[14] Therefore, although possessing differences, it cannot be said that this virus is that different from other coronaviruses.
Third, was this virus newly capable of infecting humans? To answer this question, it may help to consider RaTG13, a bat coronavirus that is said to be the closest to our virus. The two viruses are reported to be 96% similar.[15] Although it is commonly assumed that bat coronaviruses cannot infect humans without either a modification to its RNA or via an intermediate host, it is possible that bat coronaviruses jump to humans all the time, only without making us sick. For instance, a study done in 2018 found good evidence to conclude that bat coronaviruses are capable of infecting humans regularly, noting also that the “infections were subclinical or caused only mild symptoms.” [16] Conversely, experiments with blood samples of health care workers known to have had Covid demonstrated efficient neutralization of RaTG13.[15] Of particular significance in this regard is the little known fact that the PCR test for Covid, as designed by Drosten, was initially verified by making sure it detected coronaviruses from “bats in Europe and Asia.”[17] In other words, a positive PCR test may have indicated nothing more or less than the presence of a harmless bat coronavirus already endemic among humans. Although the Drosten test was later superseded by other tests, the official narrative emerged rapidly out of case detection using the Drosten test. Unfortunately, it is not clear to what extent this influenced early test results. In any case, it is certainly not novel that a virus of this sort could infect humans.
Fourth, is this virus entirely new to our immune system? Certainly not, for it was known from early on in the Covid-era that a significant percentage of people were immune to this supposedly novel virus. We previously observed that only 19% (712 of 3711) of the people on board the Diamond Princess cruise ship tested positive for the virus, and of these only a smaller fraction yet actually became ill.[4] Similarly, a group of researchers from Singapore “detected SARS-CoV-2 specific T cells in individuals with no history of SARS [or] Covid-19.” Remarkably, they also detected T cells in people that had no known contact with anyone that had had either SARS or Covid.[14] Likewise, a study in the UK found that many health care workers repeatedly tested negative despite repeated exposure to Covid.[18] The authors of that study concluded that “some individuals may clear subclinical infection before seroconversion.” Why did so many people never get Covid? Multiple researchers have concluded that it was likely a result of memory T-cells from a previous infection with a common cold or flu.[19, 20, 21, 22]
What percentage of people had sufficient prior immunity to prevent illness? Those same researchers found it was about 50%. For instance, a study by Grifoni et al “detected SARS-CoV-2-reactive CD4+ T cells in ~ 40% – 60% of unexposed individuals, suggesting cross-reactive T cell recognition between circulating ‘common cold’ coronaviruses and SARS-CoV-2.” [23] In other words, about half the population was destined to never become noticeably ill from Covid for the simple reason that they recently had a cold. Nor is this particularly surprising since it was known that the original SARS virus had also cross-reacted with other coronaviruses.[24] Thus, the virus was not entirely novel to our immune system.
Fifth, was this virus new to doctors? As may be gathered from the fact that Covid was around long before March 2020, it is almost certain that before doctors were told that they were dealing with a novel virus that they supposedly did not know how to treat, they must have unknowingly treated Covid as if it was any normal respiratory or influenza-like-illness. To the best of our knowledge, there is no record of doctors reporting an unusual increase in untreatable respiratory disease, at least not until the WHO officially declared Covid a pandemic. Even after doctors were advised it was an entirely new disease, treatment protocols were rapidly developed in multiple places.[25, 26, 27]
In summary, SARS-CoV-2 was “novel” only in the sense that it was first discovered in early 2020. It is certain that it existed globally for at least six months before this. Already by January 2020 about half the world’s population was immune to this virus. Nor was Covid outside the parameters of known treatments available for respiratory diseases. These facts should have been front and center in the media, and should have had a strong influence on government policies. Sadly, all this information was buried.
Of course, if Covid was not novel, it is impossible that it should have caused any excess deaths in 2020. It follows from this sobering conclusion that any and all excess deaths had to have been caused by other factors.
2. How deadly was Covid?
As was just pointed out, at least half of the population was essentially immune to Covid. For these people Covid was a non-issue. What about the other half? How lethal was it for them? Central to a proper answer of this question is the fact that our immune system is confronted with novel proteins all the time. Our survival does not depend on us having seen them or anything similar before. Rather, the immune system learns from all foreign material, remembers the experience, and serves to make future encounters less noteworthy. If at some point in the future a virus should arise that was both novel to our immune system and untreatable, even this would not necessarily mean that the virus was something to fear; certainly not to the extent of causing a cataclysm like we have recently witnessed.
In a previous article of this series [1] we made mention of a World Health Organization bulletin that estimated the Infection Fatality Rate (IFR) of Covid to be 0.23%.[28] That same bulletin also advised it might be substantially less than this. As data accumulated, the IFR was indeed found to be lower, eventually converging on a global average of about 0.15%.[29] For people under 70 years old, the average IFR of Covid drops down to 0.07%.[30] Of course these estimates were determined using information from death certificates and PCR test results, which (as shall be explained below) may have introduced significant inflationary errors into the results. The IFR of Covid may therefore be much less than 0.15%.
Moreover, it is well established that severe Covid illness is generally linked to those with underlying medical conditions, meaning it is rare in healthy individuals. For instance, a study looking at more than half a million people hospitalized in the USA with Covid found that 94.9% “had at least 1 underlying medical condition.” [31]
Nevertheless, for the sake of argument let us accept these estimates at face value and proceed to ask how Covid compares with the flu? The IFR of influenza is generally considered to be about 0.1%, and in a typical season about 8% of Americans get sick from the flu.[32] As for Covid, despite the unprecedented numbers of people that were tested for this virus, the total number of Covid cases in the USA during 2020 totaled 19.2 million,[33] or about 5.7% of the population. Thus, by all metrics it would appear that Covid in 2020 was on par with or less than a normal flu season.
The fact that Covid is not a particularly lethal disease was known since early 2020. For instance, the UK government officially declared that “as of 19 March 2020, Covid-19 is no longer considered to be an HCID in the UK.” [34] The acronym HCID stands for “high consequence infectious diseases.” Therefore, for the vast majority of people, the wonderful and immensely complicated human immune system was more than adequate to fight off a Covid infection.
If in fact Covid was only as bad as a normal flu season, why did it garner so much attention? And why have government dashboards suggested that Covid is causing millions of excess deaths in the world? The answer to the first of these two questions will have to be postponed for a future article. As for the second question, it is helpful to look a little closer at excess deaths in 2020. A recent study by Levitt et al analyzed all-cause mortality rates in 33 countries from 2009 to 2021. They found that during this 13 year window, the year 2020 was the worst year with the highest mortality for only four countries: “UK, Italy, Spain and Belgium.” [35] Another 10 countries had “the highest mortality in 2021.” (USA and Poland were the worst). As for the remaining 19 countries, either 2009 or 2010 had the highest mortality.
Was there anything particularly special about 2009 that made it the worst year for more than half these countries? Actually, it was found to be the worst for two simple reasons: mortality rates have in general been decreasing over time, and 2009 is as far back as the study went. Of interest is that in 2009 the WHO declared a pandemic on account of the H1N1 virus. Nothing special came of it, however, for “the total number of influenza-related deaths worldwide… proved similar to the number in a relatively mild year of seasonal influenza.” [36]
The fact that 2020 was the worst year for only 4 of these 33 countries lends support to our conclusion that Covid was about as bad as a normal flu season. The fact that 2021 was the worst year for 10 countries helps reinforce our previous findings that the Covid shots did very little to prevent Covid deaths and instead caused a great deal of deaths from adverse events.
3. Covid Data Issues
How is it possible that a mortality analysis seems to contradict reports about millions of Covid cases and deaths? There are several good reasons for this apparent discrepancy. For starters, and as was mentioned in a previous article,[1] on April 20, 2020 the WHO mandated changes to the way death certificates were to be filled out. The document stated that “a death due to Covid-19 is defined for surveillance purposes as a death resulting from a clinically compatible illness.” [37] In other words, since influenza typically has identical symptoms to Covid, flu deaths were to be labeled as Covid deaths. While this may be useful for “surveillance purposes,” it does not help us determine if Covid caused any excess deaths. Nor is it useful for making accurate comparisons between Covid and the flu. And it most definitely makes it difficult to calculate the IFR of Covid.
The WHO document went on to say: “A death due to Covid-19 may not be attributed to another disease (e.g. cancer)… Always apply these instructions whether they can be considered medically correct or not.” Therefore, even if cancer was the actual cause of death, if the person so much as tested positive for Covid, the death certificate was to say that Covid was the cause of death. The end result of this change in policy is that the number of deaths caused by Covid has been significantly over-counted in most countries.[38, 39, 40, 41] What was not affected by the protocol change was how many people died from all causes. This is why all-cause mortality studies are so relevant during the Covid-era.
Another issue muddying the waters is the PCR test used to identify a Covid case. Despite the fact that the PCR test is based on remarkable technology, it has various shortcomings when used as it was to establish a Covid case. Very briefly, a few such issues are:
- If the cycle threshold is too high, it will return a high number of false positives.[42]
- As disease prevalence decreases, the risk of false positives increases.[43, 44]
- The number and type of primers used for identifying the presence of SARS-CoV-2 has the potential to pick up fragments originating from some other source.[45, 46] (As we saw above, harmless bat coronaviruses may give a false positive.)
- The PCR test is capable of finding virus fragments,or intact virus in the airway, but is not capable of determining if a person is actually infected with Covid. Since clinical symptoms were not required to be present, many uninfected individuals falsely tested positive. [47, 48]
Every issue listed above has the tendency to inflate Covid deaths.
4. Covid in Canada
To put things into perspective, and to tie all these ideas together, it is appropriate to consider one particular country in more detail as an example. Let us consider Canada. Statistics Canada records that 16,151 deaths in 2020 were attributed to Covid.[49] This is slightly more than twice the number of deaths attributed to “Influenza and Pneumonia” in an average year in Canada (7304 deaths/yr). How is it possible that Covid was more than twice as deadly as the flu if the two illnesses are about the same?
The answer is either that the number of Covid deaths was overcounted due to all the issues just mentioned or that influenza deaths were underdiagnosed in the past. Unfortunately, it is now nearly impossible to determine the exact error rate. Nevertheless, by considering only the last of the issues in the above list, it is possible to demonstrate how significant the inflation factor really is.
Dr. Bullard, head of the provincial laboratory in Winnipeg Manitoba, testified that PCR tests do not verify infection and were never intended to be used to diagnose respiratory illness.[50] He went on to say that about 56% of positives in Canada belonged to people that were not infected with Covid. If we accept this percentage, in all likelihood at least 56% of the deaths attributed to Covid in Canada were a result of a false positive. Applying this error rate to Covid deaths in Canada in 2020 brings the number of deaths down to 7,106. It is duly noted that this number is slightly lower than the yearly average for influenza deaths in the preceding four years. If we use this adjusted amount, and plot mortality in Canada in 2020 by the top 15 leading causes of death, we can see the relative significance of Covid in Canada.

Figure 1. Source: Statistics Canada. Table 13-10-0392-01
Covid mortality was adjusted down by 56% to account for false positives.
In Figure 1 above, cancer and heart issues dwarf all other causes of death. The number of deaths attributed to flu and pneumonia is several thousand below average. This resulted from the fact that, according to the WHO mandate, many deaths that would normally have been classified as influenza were labeled as Covid because the two are clinically compatible illnesses. Also, Canadian labs changed the way they tested for the flu: “changes in laboratory testing practices as a result of the public health response to… Covid-19… may affect the comparability of data to previous… seasons.” [51] What is clear from this chart is that Covid was not particularly lethal, was no worse than a normal flu season, and certainly unworthy of the unprecedented attention it received.
Conclusion
In conclusion, it is safe to say that SARS-CoV-2 was “novel” in early 2020 solely because of the simple fact that that is when it was first detected. Not only was Covid treatable, but at least 50% of people had sufficient immunity from a previous common cold to prevent noticeable illness. It can also be said that Covid was not unusually lethal, since the mortality burden was only as bad as a normal flu season. Covid mortality (when adjusted for only one of several factors) ranked ninth among the leading causes of death in Canada, the same rank normally held by influenza and pneumonia.
Of course, it could be argued that the reason Covid deaths were this low is because government mandated lockdowns and other non-pharmaceutical interventions prevented a Covid catastrophe. It is this important topic that we plan to cover in our next article of this series.
References
- Kenyon, Todd et al, “It is impossible that the vaccines saved 14 million lives in 2021,” Panda, 2023, https://pandata.org/drivers-of-excess-deaths-part1/
- Verduyn et al, “How many lives were actually saved by the Covid-19 vaccines?” Panda, 2023, https://pandata.org/how-many-lives-were-actually-saved-by-the-covid-19-vaccines/
- Kenyon, Todd et al, “What the Diamond Princess tells us about NYC in spring 2020,” Panda, 2023, https://pandata.org/what-the-diamond-princess-tells-us-about-nyc-in-spring-2020/
- Verduyn, Thomas et al, “Did side effects from the Covid shots cause an excess mortality?” Panda, 2023, https://pandata.org/did-side-effects-from-the-covid-shots-cause-any-excess-mortality/
- Akronson, Jeffrey, “Covid-19: First coronavirus was described in The BMJ in 1965,” BMJ 2020;369:m1547
- Mulley, Kary, US Patent, 1987, http://patentimages.storage.googleapis.com/cc/f0/3e/dc51b1fb4af2e6/US4683202.pdf
- Morris, Dylan, “Novelty Means Severity: The Key To the Pandemic,” Insight, 2021, https://www.theinsight.org/p/novelty-means-severity-the-key-to
- Billingsley, Alyssa, Pinto-Garcia, Patricia, “The Novel Coronavirus: What Are Novel Viruses, and How Do They Impact Public Health?” GoodRx Health, 2023, https://www.goodrx.com/conditions/covid-19/what-does-novel-coronavirus-mean-science-medical-definition
- István Csabai, Krisztián Papp, Dávid Visontai et al. “Unique SARS-CoV-2 variant found in public sequence data of Antarctic soil samples collected in 2018-2019,” 23 December 2021, PREPRINT (Version 1) available at Research Square https://doi.org/10.21203/rs.3.rs-1177047/v1
- Apolone G, Montomoli E, Manenti A, et al. “Unexpected detection of SARS-CoV-2 antibodies in the prepandemic period in Italy.” Tumori Journal. 2021;107(5):446-451. doi:10.1177/0300891620974755
- Antonella Amendola, et al, “Molecular evidence for SARS-CoV-2 in samples collected from patients with morbilliform eruptions since late 2019 in Lombardy, northern Italy,” Environmental Research, Volume 215, Part 1, 2022, 113979,ISSN 0013-9351, https://www.sciencedirect.com/science/article/pii/S0013935122013068
- Jones, Will, “The Evidence COVID-19 Was Spreading Silently Around the World in Late 2019,” 2022, The Daily Sceptic, The Evidence COVID-19 Was Spreading Silently Around the World in Late 2019 – The Daily Sceptic
- Rossi GA, Sacco O, Mancino E, Cristiani L, Midulla F. “Differences and similarities between SARS-CoV and SARS-CoV-2: spike receptor-binding domain recognition and host cell infection with support of cellular serine proteases.” Infection. 2020 Oct;48(5):665-669. doi: 10.1007/s15010-020-01486-5. Epub 2020 Jul 31. PMID: 32737833; PMCID: PMC7393809
- Le Bert, N., Tan, A.T., Kunasegaran, K. et al. “SARS-CoV-2-specific T cell immunity in cases of COVID-19 and SARS, and uninfected controls.” Nature 584, 457–462 (2020). https://doi.org/10.1038/s41586-020-2550-z
- Cantoni, D., Mayora-Neto, M., Thakur, N. et al. “Pseudotyped Bat Coronavirus RaTG13 is efficiently neutralised by convalescent sera from SARS-CoV-2 infected patients.” Commun Biol 5, 409 (2022). https://doi.org/10.1038/s42003-022-03325-9
- Wang, N., Li, SY., Yang, XL. et al. “Serological Evidence of Bat SARS-Related Coronavirus Infection in Humans, China.” Virol. Sin. 33, 104–107 (2018). https://doi.org/10.1007/s12250-018-0012-7
- Corman, Victor M et al, “Detection of 2019 novel coronavirus (2019-nCoV) by real-time RT-PCR,” Eurosurveillance, 25, 2000045 (2020), https://doi.org/10.2807/1560-7917.ES.2020.25.3.2000045
- Swadling, L., Diniz, M.O., Schmidt, N.M. et al. “Pre-existing polymerase-specific T cells expand in abortive seronegative SARS-CoV-2.” Nature 601, 110–117 (2022). https://doi.org/10.1038/s41586-021-04186-8
- Jose Mateus et al., “Selective and cross-reactive SARS-CoV-2 T cell epitopes in unexposed humans.” Science, 370,89-94(2020). DOI:10.1126/science.abd3871
- Lipsitch, M., Grad, Y.H., Sette, A. et al. “Cross-reactive memory T cells and herd immunity to SARS-CoV-2.” Nat Rev Immunol 20, 709–713 (2020). https://doi.org/10.1038/s41577-020-00460-4
- Humbert, Marion et al, “Functional SARS-CoV-2 cross-reactive CD4+ T cells established in early childhood decline with age,” PNAS, 2023, https://doi.org/10.1073/pnas.2220320120
- Mahajan, S., Kode, V., Bhojak, K. et al. “Immunodominant T-cell epitopes from the SARS-CoV-2 spike antigen reveal robust pre-existing T-cell immunity in unexposed individuals.” Sci Rep 11, 13164 (2021). https://doi.org/10.1038/s41598-021-92521-4
- Grifoni, Alba et al, “Targets of T Cell Responses to SARS-CoV-2 Coronavirus in Humans with COVID-19 Disease and Unexposed Individuals,” Cell, 2020, DOI:https://doi.org/10.1016/j.cell.2020.05.015
- Patrick, David et al, “An Outbreak of Human Coronavirus OC43 Infection and Serological Cross-Reactivity with SARS Coronavirus,” Canadian Journal of Infectious Diseases and Medical Microbiology, 2006, https://doi.org/10.1155/2006/152612
- Front Line Covid Critical Care Alliance, Treatment Protocol, https://covid19criticalcare.com/treatment-protocols/
- Heart Advisory & Recovery Team, Ivermectin, https://www.hartgroup.org/category/ivermectin/
- McCullough PA, et al, “Multifaceted highly targeted sequential multidrug treatment of early ambulatory high-risk SARS-CoV-2 infection (COVID-19).” Rev Cardiovasc Med. 2020 Dec 30;21(4):517-530. doi: 10.31083/j.rcm.2020.04.264. PMID: 33387997.
- Ioannidis, John P A. (2021). “Infection fatality rate of COVID-19 inferred from seroprevalence data.” Bulletin of the World Health Organization, 99 (1), 19 – 33F. World Health Organization. http://dx.doi.org/10.2471/BLT.20.265892
- Ioannidis, John P A. “Reconciling estimates of global spread and infection fatality rates of COVID-19: An overview of systematic evaluations,” European Journal of Clinical Investigation, 2021, https://doi.org/10.1111/eci.13554
- Pezzullo AM, Axfors C, Contopoulos-Ioannidis DG, Apostolatos A, Ioannidis JPA. “Age-stratified infection fatality rate of COVID-19 in the non-elderly population.” Environ Res. 2023 Jan 1;216(Pt 3):114655. doi: 10.1016/j.envres.2022.114655. Epub 2022 Oct 28. PMID: 36341800; PMCID: PMC9613797.
- Kompaniyets, Lyudmyla et al, “Underlying Medical Conditions and Severe Illness Among 540,667 Adults Hospitalized With COVID-19, March 2020–March 2021,” CDC 2021, DOI: http://dx.doi.org/10.5888/pcd18.210123external icon
- Anonymous, “Key Facts About Influenza (Flu),” CDC 2022, https://www.cdc.gov/flu/about/keyfacts.htm
- Anonymous, Our World In Data, Coronavirus (COVID-19) Cases – Our World in Data
- Anonymous, “Guidance High consequence infectious diseases (HCID),” UK government, 2020, https://www.gov.uk/guidance/high-consequence-infectious-diseases-hcid
- Levitt, M., Zonta, F. & Ioannidis, J.P.A. “Excess death estimates from multiverse analysis in 2009–2021.” Eur J Epidemiol (2023). https://doi.org/10.1007/s10654-023-00998-2
- Fineberg, Harvey, “Pandemic Preparedness and Response — Lessons from the H1N1 Influenza of 2009,” N Engl J Med 2014; 370:1335-1342 DOI: 10.1056/NEJMra1208802
- Anonymous, “International Guidelines for Certification and Classification (coding) of Covid-19 as Cause of Death,” World Health Organization, 2020, https://cdn.who.int/media/docs/default-source/classification/icd/covid-19/guidelines-cause-of-death-covid-19-20200420-en.pdf (pg 3)
- Audie, Joseph, “Using CDC data and death certificate standards to propose a preliminary estimate for the number of US COVID-19 associated deaths that were caused by or contributed to by SARS-CoV-2 infection,” Research Gate, 2020, https://www.researchgate.net/publication/344228032_Using_CDC_data_and_death_certificate_standards_to_propose_a_preliminary_estimate_for_the_number_of_US_COVID-19_associated_deaths_that_were_caused_by_or_contributed_to_by_SARS-CoV-2_infection
- Fenton, Norman & Neil, Martin & McLachlan, Scott. (2021). What proportion of people with COVID-19 do not get symptoms?. 10.13140/RG.2.2.33939.60968.
- Jensen, Scott, 2023, https://www.youtube.com/watch?app=desktop&v=PHxj_Luclxs&feature=youtu.be
- Beaudoin, John, “500,000 Death Certificates Tell of Signals, Fraud, and Unlawful Deaths,” 2023, https://rumble.com/v2a7wtk-john-beaudoin-500000-death-certificates-tell-of-signals-fraud-and-unlawful-.html
- La Scola B, Le Bideau M, Andreani J, Hoang VT, Grimaldier C, Colson P, Gautret P, Raoult D. “Viral RNA load as determined by cell culture as a management tool for discharge of SARS-CoV-2 patients from infectious disease wards.” Eur J Clin Microbiol Infect Dis. 2020 Jun;39(6):1059-1061. doi: 10.1007/s10096-020-03913-9. Epub 2020 Apr 27. PMID: 32342252; PMCID: PMC7185831.
- Anonymous, “WHO Information Notice for Users 2020/05: Nucleic acid testing (NAT) technologies that use polymerase chain reaction (PCR) for detection of SARS-CoV-2,” World Health Organization, 2021, https://www.who.int/news/item/20-01-2021-who-information-notice-for-ivd-users-2020-05
- Deeks, John, “Why the school testing regime needs to change,” The Post, 2021, https://unherd.com/thepost/why-the-school-testing-regime-needs-to-change/
- Neil, Martin, “Put to the test: use of rapid testing technologies for covid-19,” BMJ 2021; 372 doi: https://doi.org/10.1136/bmj.n208
- Neil, Martin, “UK lighthouse laboratories testing for SARS-COV-2 may have breached WHO Emergency Use Assessment and potentially violated Manufacturer Instructions for Use.” Probability and Risk, 2021, https://probabilityandlaw.blogspot.com/2021/02/uk-lighthouse-laboratories-testing-for.html?m=1
- Deeks, Jonathan, “Operation Moonshot proposals are scientifically unsound,” BMJ 2020; 370 doi: https://doi.org/10.1136/bmj.m3699
- Pollock A M, Lancaster J. “Asymptomatic transmission of covid-19” BMJ 2020; 371 :m4851 doi:10.1136/bmj.m4851
- Anonymous, Statistics Canada. Table 13-10-0392-01 “Deaths and age-specific mortality rates, by selected grouped causes” DOI: https://doi.org/10.25318/1310039201-eng
- Anonymous, “Manitoba Chief Microbiologist and Laboratory Specialist: 56% of positive “cases” are not infectious,” JCCF, 2021, https://www.jccf.ca/manitoba-chief-microbiologist-and-laboratory-specialist-56-of-positive-cases-are-not-infectious/
- Government of Canada, “FluWatch annual report: 2019-2020 influenza season,” 2021, https://www.canada.ca/en/public-health/services/publications/diseases-conditions/fluwatch/2019-2020/annual-report.html
FDA responds to negative efficacy of variant boosters with another variant booster
By Daniel Horowitz – conservative review – June 21, 2023
The human experimentation of Operation Warp Speed was not an anomaly; it is the new normal, and the FDA is just getting started. The agency is now allowing the COVID vaccine manufacturers to change the formulation of their shots to continue to chase variants, themselves created by antigenic drift of the shots. And they continue to do so based on nothing more than measuring antibody titer levels. No human clinical trials necessary! Except, studies now show, and reality confirms, the more they chase variants, the more they create negative efficacy against the existing variant, thereby engendering a “need” for another formulation.
What was the response of the FDA to the increasing news of cataclysmic injuries and negative efficacy of the COVID shots for variants that are no longer dangerous? Last Thursday, the FDA’s VRBPAC unanimously approved a fall booster, advising Pfizer, Moderna, and Novavax to update their formulations for the so-called XBB.1.5 Omicron variant. So, officials pre-emptively approved a shot that doesn’t exist based on antibody level testing without human trials – all for a variant that not only is not dangerous but will actually be extinct by the time this poison reaches the market, just as they did with the bivalent formulation for the BA.4 and BA.4 variants.
To this day, the bivalent shot is the only one available, and according to the CDC, that variant doesn’t even exist! It is true that very few people are dumb enough to get this shot, but what they are trying to do is create an endemic schedule of COVID shots to time perfectly with the flu shots in the fall. They have already groomed people over the generation to “get their flu shot” every fall. So now the pharmacies will be waiting with the COVID needle to complete their seasonal updates.
So, what happens when you keep tricking the body to respond to a virus for strains that no longer exist? As the FDA approved these shots, the agency already had the peer-reviewed Cleveland Clinic study showing negative efficacy of the original COVID shots. Just days before this meeting, the Cleveland Clinic came out with a preprint showing negative efficacy for the bivalent booster shots too.
The study contrasted 11,990 employees of this venerable institution who chose to be “up to date” with the bivalent boosters compared to 36,344 employees who were “not up to date” and tracked their outcomes. It turns out that after about three and a half months, you were about 25% more likely to get COVID after having gotten the boosters as compared to the control group.

After adjusting for confounding factors between the groups, the study authors actually found a 33% rate of negative efficacy!
“This study’s findings question the wisdom of promoting the idea that every person needs to be ‘up-to-date’ on COVID-19 vaccination, as currently defined, at this time,” conclude the Cleveland Clinic researchers. They also observe, “It should be pointed out that there is not a single study that has shown that the COVID-19 bivalent vaccine protects against severe disease or death caused by the XBB lineages of the Omicron variant.”
The push for boosters comes at a time when more evidence proves a strong correlation between excess deaths and the vaccine take-up. A letter published in a peer-reviewed journal of Medicine and Clinical Science shows that Japan and Germany, two highly vaccinated countries, experienced sharp excess deaths coinciding with the vaccine take-up. They found very little excess death during the pandemic months before the vaccine was rolled out.
“It should be investigated to what extent the about 5%-10% highly significantly increased mortalities in Germany and Japan in 2021 and 2022 might be due to the pandemic countermeasures, including the vaccinations with their possibly underestimated immediate or protracted side effects,” concluded the researchers from Japan and Germany.
“From this point of view, it seems possible that a high vaccination rate has contributed to an increased all-cause mortality in some countries.”
The twisted irony is that, according to the CDC’s variant tracker, XBB.1.5 has gone from 80% of cases to less than 40% of cases in just a few months. It will clearly be obsolete by the fall. None of this was discussed at the FDA hearing. Of course, nothing about Pfizer’s own document showing five million cumulative reports of adverse events affecting every organ system was ever discussed. Hence, we have record injuries, negative efficacy, long-term immune imprinting causing the body to constantly respond inappropriately to wrong strains of the virus – all for a virus that is no longer deadly and for a population that has already gotten the virus!
That’s not just a lousy cost-benefit analysis; that is premeditated murder against the American people. What is the GOP plan to stop this? Or do Republicans even care? How can they continue to fund more COVID shots in the HHS appropriations bill, much less the broader FDA/CDC scheme to create new dangerous shots at warp speed?
Just how callously does the FDA regard human life? After its own VAERS system exploded with every adverse event imaginable, an outcome we now know officials anticipated, to this day they have not followed up on those safety signals. For example, according to the Informed Consent Action Network, the Standard Operating Procedures and Policies document for the FDA’s Vaccine Safety Team requires that its staff members identify VAERS adverse event reports that “need a rapid response and complex coordination,” after which they are supposed to “immediately” inform certain FDA management, who then alert other sub-agencies. Did that occur?
Well, more than a year after the ICAN’s record request, the agency responded, “A search of our records did not locate any documents responsive to your request.”
Where is the action from the House GOP? Why are they still only investigating the shutdown of schools in the past, but not the ongoing, premediated unleashing of deadly products on the American people?
Featured Video

US Marines Seized Panama in 1903
or go to
Aletho News Archives – Video-Images
From the Archives
Precedents for Pizzagate
Marc Dutroux, Belgian pedophile, sadist, and serial killer with friends in high places
By Aedon Cassiel | Counter – Currents | December 23, 2016
To reiterate a point that should be clear to the more astute reader, my goal in this series (part 1, part 2) has not been to defend “Pizzagate” as such. My goal has been to defend the people who want to investigate it against specific accusations levied against them by people who think Pizzagate has revealed no intriguing information at all—for a specific reason, which I will be honing in and focusing on much more directly in this closing entry.
Whereas the mainstream critics of Pizzagate would have you believe that the dividing line is between paranoid conspiracy theorist followers of “fake news” and level-headed people who follow trustworthy news sources and rely on cold, hard reason to determine the truth, my goal has been to show that—whatever is or is not happening with Pizzagate itself—this framing of the issue is arrogant, insulting, and the product of extremely narrow tunnel vision. … continue
Blog Roll
 Aletho News
Aletho News- West’s Claims of Non-Involvement in Ukraine Conflict ‘Epitome of Hypocrisy’ – Expert
- Putin aide urges retaliation to ‘Western piracy’
- The Depth Charge in the Womb
- ‘Fox guarding the henhouse’: AMA, Vaccine Integrity Project to conduct their own vaccine safety and efficacy reviews
- Macron, Merz, and von der Leyen Defend Expanded Speech Controls
- Keir Starmer-tied think tank paid PR firm to target The Grayzone
- ‘Israel’ threatens to genocide Gaza if Hamas refuses disarmament
- Apple Just Bought A Sinister ‘Pre-Speech’ Tech Company Implicated In Genocide
- Israel’s new West Bank registration process declares Palestinian land ‘state property’
- Two children killed in Palestinian Authority ambush in West Bank; Hamas slams attack as ‘black mark’
- If Americans Knew
- An error has occurred; the feed is probably down. Try again later.
- No Tricks Zone
- New Study: A 4°C Warmer Beaufort Sea Had ‘No Sea Ice’ 11,700 – 8200 Years Ago
- Unfudging The Data: Dutch Meteorological Institute Reinstates Early 20th Centruy Heat Waves It Had Erased Earlier
- German Gas Crisis…Chancellor Merz Allegedly Bans Gas Debate Ahead of Elections!
- Pollen Reconstructions Show The Last Glacial’s Warming Events Were Global, 10x Greater Than Modern
- Germany’s Natural Gas Storage Level Dwindles To Just 28%… Increasingly Critical
- New Study Rebuts The Assumption That Anthropogenic CO2 Molecules Have ‘Special’ Properties
- Climate Scientist Who Predicted End Of “Heavy Frost And Snow” Now Refuses Media Inquiries
- Polar Bear Numbers Rising And Health Improving In Areas With The Most Rapid Sea Ice Decline
- One Reason Only For Germany’s Heating Gas Crisis: Its Hardcore-Dumbass Energy Policy
- 130 Years Later: The CO2 Greenhouse Effect Is Still Only An Imaginary-World Thought Experiment
