A former police detective involved in the investigations of roughly 250 sudden infant death syndrome (SIDS) cases claimed that roughly 50% occurred within 48 hours of a vaccination.
In a video interview today with The Defender, the detective, who gave only her first name, “Jennifer,” said she and her husband were detectives in the police department of a major U.S. city with a population of over 300,000 for a combined seven years, from roughly 2003 to 2010.
Jennifer said she is keeping her last name and city name undisclosed to protect her family. She said:
“The pharmaceutical industry does not want to be threatened by those sorts of secrets coming out. So, I’m a mother of many children, and their safety is my number one priority, my family’s safety. I’m a mama bear before I’m anything else.”
Jennifer said she hadn’t initially questioned the safety of vaccines. But that changed when she noticed a recurrent pattern among the police reports for SIDS cases in her unit.
“I’m like, what is the main thing that is true with all of these, the recurring theme with all of these babies? And that’s that they were recently vaccinated,” she said.
She estimated that around half of the SIDS cases involved babies who had received a vaccination in the 48 hours before their death and a “pretty decent number” of additional cases had received a vaccination in the week before their death.
The pattern was strongest among 6-month-olds, she said.
What particularly concerned Jennifer was that although the police reports noted these babies’ recent vaccinations, that information went unmentioned on the county coroner’s autopsy reports and death certificates.
“It didn’t make sense to me,” she said.
She discovered it wasn’t just her county coroner. Coroners across the U.S. are trained not to record vaccination information on autopsy reports, she said.
Some states are working to change that.
In May, Oklahoma and Louisiana passed legislation that amends existing public health law by directing coroners to document any vaccines administered within 90 days of death on autopsy reports for children under age 15 who died unexpectedly and without explanation.
Pediatrician: ‘The threat of death in SIDS is real’
Jennifer’s realization that many SIDS deaths happened soon after vaccination prompted her to start researching vaccines.
Around that time, she and her husband were looking for a pediatrician for their children. Jennifer told the pediatrician about the SIDS pattern she saw and that she and her husband did not want to vaccinate their kids.
The pediatrician acknowledged that there are risks with vaccination and said he would respect their choice, Jennifer said.
He shared that he once vaccinated a baby for hepatitis B, and it died the next day. “He’s like, I 100% believe that it was that vaccine,” she said.
The pediatrician told Jennifer he had many parents of unvaccinated kids whose medical files are super thin. The medical files of the vaccinated kids he served are really thick, he said.
Jennifer, who also shared about her conversation with the pediatrician in a 2023 interview with Steve Kirsch, told The Defender :
“He goes, there is a downside to vaccines. First of all, the threat of death in SIDS is real, and he’s like, it messes with the immune system, so it opens the door to asthma, allergies.”
The pediatrician told Jennifer that he was not supposed to tell parents any of this.
“He’s like, in fact, the American Academy of Pediatrics (AAP) actually trains us on how to deflect when parents think that their child’s having a vaccine reaction or that they’re hesitant. We’re supposed to deflect and tell them those are unrealistic fears and that it’s just coincidence that this happened after the vaccine,” Jennifer said.
But his conscience wouldn’t let him do that, he told her.
Journal removes peer-reviewed analysis showing potential SIDS-vaccines link
The public debate about a possible link between vaccines and SIDS has recently heated up.
Last week, Idaho mother Andrea Shaw — whose twin babies died eight days after receiving their 18-month vaccines — was arrested for allegedly murdering her twins. Shaw said doctors ignored her when she warned that the twins’ father had previously experienced a bad reaction to a flu vaccine.
Last month, U.S. Health Secretary Robert F. Kennedy Jr. and Sen. Ron Johnson (R-Wis.) wrote to the journal Toxicology Reports, demanding to know why a 2021 peer-reviewed paper that presented data suggesting a possible link between vaccination and SIDS was recently removed from the Toxicology Reports website.
In a June 29 letter, Johnson called on the editor-in-chief of Toxicology Reports and the CEO of Elsevier, which owns the journal, to release all records related to the decision to remove vaccine researcher Neil Z. Miller’s analysis: “Vaccines and sudden infant death: An analysis of the VAERS database 1990-2019 and review of the medical literature.”
The analysis lined up with what Jennifer witnessed in police reports following SIDS deaths.
Miller found that from 1990 to 2019, many more SIDS reports were filed in the Vaccine Adverse Event Reporting System (VAERS) in the first few days after vaccination compared to later on after vaccination.
The paper also included a comprehensive review of the scientific literature on vaccines and SIDS, including documentation of large increases in SIDS rates following the rollout of national immunization campaigns and case reports of SIDS in babies who were recently vaccinated.
Although Toxicology Reports published Miller’s analysis in June 2021 after it passed the peer-review process, the journal on April 9 posted a removal notice for Miller’s article, citing “serious methodological flaws.”
Miller told The Defenderin an earlier interview why he believes the removal was unjustified. He said:
“The core findings of my paper — the temporal clustering of infant deaths in the immediate post-vaccination window, the historical SIDS rate spike following the national immunization campaign, the full literature review — remain unrefuted.
“No one has engaged with the data. They simply made the paper disappear. That should concern every parent, every researcher, and anyone who believes science advances through open inquiry rather than institutional gatekeeping.”
ICD revision eliminated vaccination as official cause of death
Research published since Miller’s analysis has also suggested a link between SIDS and vaccines. For instance, a 2025 study suggested that infants with underdeveloped liver pathways may be more susceptible to SIDS after vaccination, because their bodies cannot process toxic chemicals present in small quantities in vaccines.
The SIDS diagnosis didn’t exist until the late 1960s, when the category was created in response to a rise in sudden unexplained infant deaths.
In the early 1960s, the number of vaccines administered to most U.S. infants increased, according to Miller’s analysis.
As SIDS rates rose, so did parental concern that SIDS was connected to vaccination. However, health officials assured parents that unexplained death following vaccination was “merely coincidental,” Miller wrote.
He also said that before 1979, the International Statistical Classification of Diseases and Related Health Problems (ICD) included cause-of-death classifications associated with “prophylactic vaccination” as an official cause of death.
However, in 1979, the ICD was revised, and that category was eliminated. As a result, “medical examiners are compelled to misclassify and conceal vaccine-related fatalities under alternate cause-of-death classifications,” Miller wrote.
In 2025, Donald Trump’s administration once again imposed travel restrictions on citizens of various countries, particularly in Africa, the Middle East, and the Caribbean. The measures have already produced concrete effects on international events hosted in the United States. One of the best-known cases was that of Somali referee Omar Abdulkadir Artan, who was prevented from entering the country and, consequently, from officiating at the 2026 World Cup despite having been selected by FIFA.
Beyond their impact on sports, the restrictions raised even greater concerns at the United Nations, whose headquarters are located in New York, as they may hinder the participation of diplomats and representatives of member states in the organization’s work. Indeed, the Trump administration revoked or denied visas to Mahmoud Abbas and around 80 members of the Palestinian Authority and the PLO before the opening of the 2025 annual session of the General Assembly. Several members of the Somali delegation were also denied visas, preventing their participation in the meeting.
Shortly after the White House announced the travel restrictions, UN Secretary-General spokesperson Stéphane Dujarric washed his hands of the matter and, in practice, sided with Trump by stating that it is up to each country to decide how it controls its borders and who may enter its territory. No one is naïve enough to believe that if Somalia or Palestine had adopted such measures, and the affected representatives were Americans, Dujarric’s position would have been the same.
According to him, the executive order indicated that diplomats, holders of G4 visas, and United Nations personnel were exempt from the new restrictions. He added that the United States, as the host country of the UN headquarters, has obligations arising from international treaties to facilitate the movement of the organization’s personnel and delegates, noting that these responsibilities were contemplated in the presidential decree.
But this is not new. The United States has long denied entry to representatives of undesirable countries. Although Trump’s travel restrictions are particularly outrageous, previous administrations also denied or limited access for representatives of member states.
Over the decades, diplomats from countries subject to sanctions or restrictions, such as Sudan, Iran, and Venezuela, have faced delays or denials in obtaining visas to attend UN meetings. These practices have effectively thrown the 1947 Headquarters Agreement into the trash, despite its requirement that the United States, as host country, allow accredited representatives of member states to enter.
In the late 1940s, the United States barred members of nongovernmental organizations linked to the Italian Communist Party, which was part of Italy’s government. In 1988, during Ronald Reagan’s administration, Yasser Arafat was prevented from entering the country to address the UN General Assembly on the grounds of national security concerns. In response, the Assembly held its session devoted to the Palestinian question in Geneva, with Arafat present—the leader of the PLO, an organization already recognized at that time as the representative of Palestine at the UN.
The United States also denied entry to Iranian diplomat Hamid Aboutalebi, who in his youth had participated in the hostage crisis at the American embassy in Tehran. Years later, when he was appointed Iran’s ambassador to the UN, he was denied entry.
Over the last few decades, cases involving the issuance of visas to citizens of Cuba, Russia, and Venezuela have become frequent. Washington has been accused of using visa applications as a tool to restrict diplomatic access to UN headquarters in New York, thereby violating its legal obligations as host country.
Cubans are among the diplomats who have most frequently denounced violations of the UN Headquarters Agreement.
An emblematic case occurred in 2006. Diplomat Rodolfo Benítez, then a counselor at Cuba’s mission to the UN, received authorization to participate in a seminar for diplomats from permanent missions to the UN held at West Point. Although approximately 40 diplomats from various countries were authorized to attend, the United States denied travel authorization to the Cuban representative. Cuba denounced the measure before the UN Committee on Relations with the Host Country, arguing that the decision was discriminatory and harmed the normal functioning of the mission.
In 2007, Washington again denied authorization for two Cuban diplomats to leave the restricted 25-mile area around Columbus Circle in Manhattan in order to participate in an informal meeting of the Working Group on the Crime of Aggression held at Princeton University. Havana formally protested before the UN.
Furthermore, for decades Cuban diplomats—as well as North Korean and Syrian diplomats—accredited to the UN were subject to severe travel restrictions within the United States, being allowed to circulate only within a limited area around New York City. The General Assembly repeatedly adopted resolutions calling for the removal of these restrictions.
During Barack Obama’s administration, the Sudanese delegation accused Washington of violating the Headquarters Agreement by denying a visa to then-Sudanese President Omar al-Bashir. He was supposed to lead Sudan’s delegation during the annual General Assembly debates. The United States argued that the arrest warrant issued by the International Criminal Court would oblige American authorities to arrest him if he were allowed to enter the country. However, the United States is not a signatory to the Rome Statute and has received various officials subject to ICC arrest warrants, including, more recently, Israeli Prime Minister Benjamin Netanyahu.
In 2024, under Joe Biden’s administration, China’s representation to the UN informed the Committee on Relations with the Host Country, a body linked to the General Assembly, that Washington had repeatedly denied visas to personnel responsible for maintaining the facilities of China’s mission.
The Chinese representative drew attention to General Assembly Resolution 78/116, emphasizing that the privileges and immunities of delegations and diplomatic missions cannot be restricted because of the bilateral relations of the host country. The diplomat urged the United States to fulfill its obligations and issue the visas without delay.
Complaints from diplomats and the public increased significantly during the first Trump administration. In 2019, Russia and Iran went so far as to disrupt the work of certain General Assembly committees in protest against the denial of visas to diplomats from both countries. Iran stated that 58 representatives faced restrictions on participating in the Assembly’s annual opening session, while Russia reported that 18 diplomats still lacked visas.
Preventing delegates from participating in UN activities seriously undermines the foreign policy of the affected countries. According to experts, countries currently included on Trump’s restriction lists may obtain visas for only a limited number of representatives, making it more difficult for them to participate simultaneously in different meetings. The diplomatic missions of these countries also face difficulties in bringing technical experts, reducing the quality of participation in specialized debates. Furthermore, the senior leaders of the affected nations become unable to conduct bilateral and multilateral meetings and negotiations, and it is well known that behind-the-scenes conversations are among the most valuable activities at meetings held under the auspices of the United Nations.
Somalia illustrates this problem. Currently an elected member of the United Nations Security Council, the country appears on Trump’s restriction list. In February 2025, it even voted in favor of a United States-sponsored resolution on a “path to peace” regarding the war in Ukraine—that is, not even bowing to American dictates enabled the African country to escape the sanction. A Somali diplomat told the PassBlue website that the country already faced strict controls on the issuance of visas to diplomats and that the new measures could also harm Somali students and business people.
In 1947, the United States signed the Headquarters Agreement, committing itself to allow the entry of persons essential to the functioning of the UN. Subsequently, however, the U.S. Congress added a clause preserving the country’s right to deny entry on national security grounds. The UN challenged this addition, arguing that it was not part of the original agreement.
The controversy persisted until an understanding was reached with then Secretary-General Dag Hammarskjöld. It was agreed that the United States would notify the Secretary-General in advance if it intended to deny entry to representatives of any member state. This arrangement worked until 1988, when Yasser Arafat was denied a visa on national security grounds.
Larry Johnson, former adjunct professor at Columbia Law School and former UN Assistant Secretary-General for Legal Affairs, told PassBlue that the United States argued in 1988 that, by failing formally to object to the confidential invocation of national security clauses since the early 1950s, the UN had effectively accepted the practice.
UN member states and the UN Secretariat have responded in different ways to visa denials over the years. The most forceful response occurred precisely in the Arafat case in 1988, when the General Assembly transferred its entire session on Palestine to Geneva as a form of public protest.
The episode involving Arafat also led to the creation of the General Assembly’s Committee on Relations with the Host Country, tasked with dealing with visa-related problems and other issues between the United States and the other UN member states.
However, after the collapse of the USSR and the imposition of U.S. domination over the globe, the countries of the UN bowed to Washington’s will. Instead of immediately resorting to direct confrontational measures such as boycotts or relocating meetings, the Secretariat began encouraging countries to submit their complaints to the Host Country Committee. This body can recommend resolutions, request advisory opinions, or even initiate arbitration proceedings to address disputes, which in practice produces no results.
Deciding who can and cannot participate in UN activities in New York is not the only diplomatic and geopolitical advantage of hosting the world’s principal international organization. The main advantage is that virtually all heads of state, foreign ministers, ambassadors, and negotiators regularly pass through New York.
This allows the United States to maintain direct and constant contact with almost every government on the planet, hold bilateral meetings alongside UN activities, monitor diplomatic trends in real time, and exert informal influence over international negotiations. Even countries that do not maintain close diplomatic relations with Washington end up maintaining some level of contact on American territory—their representatives are more easily spied upon and co-opted.
Although this is an aspect rarely emphasized publicly, the concentration of foreign diplomatic missions in New York is a valuable source of information for American intelligence services. Historically, agencies such as the CIA and the FBI have devoted significant resources to monitoring diplomatic activities linked to the UN. Physical proximity facilitates the observation of negotiations, informal contacts, recruitment of sources, and collection of information about foreign governments.
Even without officially controlling the UN, hosting the organization also gives the United States important logistical advantages. Washington can organize side events, receive delegations at American institutions, involve universities, research centers, and foundations, and promote political propaganda through its media outlets.
Of course, all this is considered perfectly normal by the propagandists of American imperialism. But what would they say if the UN headquarters were moved to Moscow or Beijing?
Marie Stopes lobbied Parliament to compulsorily sterilise people she called “parasites.” She branded her contraceptives “Prorace” and “Racial.” She bequeathed her clinics not to the Family Planning Association but to the Eugenics Society. She also sits in the BBC viewers’ top 100 Great Britons, appears on Royal Mail postage stamps, and is remembered as the woman who gave British women reproductive choice. Mark Halliday Sutherland’s grandfather was the doctor Stopes sued for libel in 1923 after he accused her of “exposing the poor to experiment.” The trial ran two-and-a-half years across three courts. Dr Halliday Sutherland won.
Behind Stopes stood a longer tradition. Thomas Malthus wrote in 1798 that population would outrun food supply and that poverty was therefore a natural law rather than a consequence of governance. Mark traces the pattern forward from there: through Galton’s eugenics, Stopes’s sterilisation campaigns, H.G. Wells’s “faith to kill,” Margaret Sanger’s plan to corral millions of Americans onto government farms, Paul Ehrlich’s proposal to add sterilants to water supplies, and John Holdren’s “planetary regime.” The same three solutions keep reappearing across a century: more top-down control, restricted births, increased deaths. What changes is the marketing.
Mark grew up believing a simpler version — the one still repeated by the BBC — in which his grandfather was a backward Catholic obstructing a feminist pioneer. In 2013 he found Halliday’s papers in the cellar of his mother’s house. Seven years of research later he published Exterminating Poverty: The true story of the eugenic plan to get rid of the poor, and the Scottish doctor who fought against it, drawing on primary sources with nearly 700 citations across 320 pages. He is Sydney-based, currently working from London as a coach and facilitator, and writes on Substack about how the ideas that drove Stopes’s clinic never really went away — they just changed clothes.
The interview traces how organisations rename themselves to soften their image (the Eugenics Society is now the Adelphi Genetics Forum; the Voluntary Euthanasia Society is now Dignity in Dying), why the Society’s 1960 decision to pursue “crypto-eugenics” still shapes what gets said and what doesn’t, and what Mark reads in a Canadian paper modelling CAD $1.273 trillion in savings from expanded MAiD. Halliday Sutherland predicted in 1929 that the end of European civilisation might come from “a lack of European children.” A century on, fertility rates across the developed world are collapsing.
With thanks to Mark Halliday Sutherland.
1. You’re an author, researcher, facilitator and coach based in Sydney — but a lot of your work centres on a libel trial in 1920s London involving your own grandfather. How did you end up here, and what was the journey that led you into this material?
The first two parts were intentional: I met an Australian girl in London. I emigrated to Australia and we got married. I work as a freelance facilitator and coach in the field of leadership and management.
The author/researcher parts arose from circumstances.
My grandfather, Dr Halliday Sutherland, died in 1960. I was born six months later and was named in his memory. During his life, Halliday was a well-known doctor, author and public speaker but after his death, his fame faded fast.
If he was remembered at all, it was as the man who had attacked Marie Stopes, the woman who founded Britain’s first birth control clinic. In 1922, Halliday accused her of “exposing the poor to experiment” and (she said) called for her to be jailed. She sued him for libel and they fought a bitter legal battle for two-and-a-half years.
Marie Stopes died in 1958. She was famous in her lifetime and, in some ways, her fame increased after her death. She was the subject of five major biographies and things were named after her: buildings, multi-national organisations and memorial lectures. Blue plaques appeared on the buildings in which she had lived and worked.
In short, Stopes was the secular saint of Britain’s birth control movement and was said to have given British women reproductive choice.
To learn about my grandfather’s legal battle, I went to the biographies of Stopes. These cast him as a backward-looking Roman Catholic who wanted to tie women to the kitchen sink. This was the fellow after whom I had been named, and in the context of growing up in the 1970s and 1980s it was, to be honest, a bit of an embarrassment.
In 2013 I rediscovered Halliday’s papers in the cellar of my mother’s house, and I began researching his life more closely. I found that while the biographies of Stopes had included many true facts about him, they had omitted many other true facts that told a very different story. I learned that in 1920s Britain, Halliday had been at the forefront of the opposition to eugenics.
Back then, eugenics was at its height and had many supporters in the establishment and the intelligentsia. Stopes’ clinic was a eugenic project that sought to transform Britain (and Britons). Her aim was to eliminate the reproduction of people she considered “undesirable” while increasing the numbers of those who were “fit”. Zoe Williams of The Guardian wrote that Stopes’ “… eugenics programme was actually slightly to the right of Hitler’s, just because her definition of defective is so broad.”
Stopes’ biographies and the articles written about her often repeated Sutherland’s libel that she was “Exposing the poor to experiment”, but they always left out the crux of Halliday’s argument: “if children are to be denied to the poor as a privilege of the rich, then it would be very easy to exploit the women of the poorer classes” especially in the lower grades of work. He warned that Britain would become a “servile state” – essentially, a slave state in which poor and working class people had no societal role other than as workers.
As you might imagine, my views changed. For all the talk about the “Roman Catholic doctor” I learned that Halliday’s opposition to eugenics began long before his conversion to Roman Catholicism. It arose from his work as a specialist in Consumption – TB of the lungs – a disease of poverty that killed 50,000 Britons and disabled a further 150,000 each year at that time.
Mainstream eugenicists believed that Consumption was a “racial disease” primarily caused by a person’s heredity. Yes, they knew that germs were involved, but they said that the crucial factor was the narrow lungs inherited from their parentage. Halliday disagreed. Based on his work and research, he said that Consumption was caused primarily by infection and bad living conditions. He said that Consumption could be prevented and, if caught early enough, cured.
It wasn’t merely an academic difference. Karl Pearson, professor of eugenics at London University said the way to eliminate Consumption was to “let nature take its course” and prevent the reproduction of the tuberculous. Sir James Barr was the 1912 president of the British Medical Association who said:
“Until we have some restriction in the marriage of undesirables the elimination of the tubercle bacillus is not worth aiming at. It forms a rough, but on the whole very serviceable check, on the survival and propagation of the unfit … if to-morrow the tubercle bacillus were non-existent, it would be nothing short of a national calamity. We are not yet ready for its disappearance.”
The link between tuberculosis and Stopes was that, when she opened the Mothers’ Clinic in 1921, it was the restriction that Barr had been hoping for. He wrote a letter of congratulation:
“You and your husband have inaugurated a great movement which I hope will eventually get rid of our C3 population and exterminate poverty. The only way to raise an A1 population is to breed them.”
He became a vice-president of her Society for Constructive Birth Control and Racial Progress (CBC) and testified on her behalf in court.
Having learned these aspects of the story, what was I to do?
To begin with, I contacted historians, biographers and others who wrote articles about Stopes and, when relevant, I told them about my research. Sometimes, I would provide digital copies of unique documents from Halliday’s personal papers. I was always polite – friendly even – hoping that the evidence would start a dialogue and even, down the track, lead to them incorporating my research.
High hopes indeed! I never heard back and only rarely received reply.
I realised that if I didn’t make a permanent record of the true story, such as writing a book, the truth would die with me. That’s when “Exterminating Poverty. The true story of the eugenic plan to get rid of the poor, and the Scottish doctor who fought against it” was born. I published it in paperback in August 2020.
Obviously, being a grandson means that people will accuse me of bias. For this reason, I have focused on the words, actions and artefacts of both Stopes and Sutherland from primary sources. “Exterminating Poverty” has almost 700 citations in its 320 pages.
2. You’ve said you grew up believing a false story about your own grandfather — the “Catholics against contraceptives” version. When did you first realise the accepted history was wrong, and what was that moment like?
It wasn’t a single moment rather than many. Initially I felt indignant anger that the story had been falsified and simplified to a “good-guy-versus-bad-guy” trope to favour Stopes.
When I appreciated the size of the project, there were moments of bewilderment and the realisation that if I didn’t finish the book, I would have wasted an enormous amount of time.
There were moments of intense elation when I found key pieces of evidence.
One highlight was spending two days with my brother and co-author in the Wellcome Institute Library in London. Stacks of boxes containing Stopes’ papers, reading what she had written and taking photographs. Frisson and disbelief when I saw evidence that she had interfered with the sworn statements of her witnesses and induced even induced one of them to lie to the court! Followed by a curry and a few beers in the evening. What’s not to like?
Sometimes the construction or the wording of the biographies was odd, or there were significant documents that should have been easy to find but were not. This made me suspicious and I sensed that I should follow that path. It was very rewarding because I found huge gaps in the accounts that had been published.
These days, I feel frustrated at the inertia of the “accepted” history remaining in place despite evidence to the contrary, especially by the BBC which bangs on and on about misinformation and disinformation but which will not amend its accounts of the trial.
3. For readers who’ve never heard of the Stopes v. Sutherland libel trial, what was actually at stake in that courtroom — beyond the surface dispute about contraceptives?
It was about the future of Britain: would contraceptives become commonplace and, if they did, would it be subordinated to eugenic ideology?
The ‘Tenets of the CBC’ and Stopes’ testimony in court clearly expressed the eugenic direction of her work. It was just as much her aim:
“… to secure conception to those married people who are healthy, childless, and desire children, as it is to furnish security from conception to those who are racially diseased, already overburdened with children, or in any specific way unfitted for parenthood.”
In the early 1920s, Stopes was the preeminent name in birth control and, backed by some of the leading lights of that era, she planned to create a network of clinics across Britain. She had rivals though and was intensely sensitive to criticism. She was itching to sue some of them and Dr Sutherland was chosen because he represented two groups that criticised her: Roman Catholics and the medical doctors.
Had she won the case, she would have silenced her critics and her project would have gained momentum. Because she lost and had costs awarded against her, it slowed her down. It delayed the eugenic aspects of birth control and the agitation for the compulsory sterilisation of defectives. This latter part did not regain momentum until the late 1920s/early 1930s and when a private member’s bill was introduced to Parliament in July 1931, it was defeated.
I think that her desire for publicity was the Achilles heel of her strategy. Too much time was spent in the trial of her eminent witnesses testifying what an upright person she was. In addition, Stopes decided to testify in the trial, something that she was not required to do.
That was all very well, but a better approach would have been to put the full weight of the burden of proof on Sutherland: he had to justify that what he had written was true. The approach that Stopes took gave the defence ample opportunity to undermine the veracity of her witnesses.
4. Marie Stopes appears on postage stamps and was voted one of the “Greatest Britons.” You argue this celebration rests on a serious omission. What’s the part of her story that consistently gets left out?
In around 2000, the BBC announced a list of its viewers’ “Greatest Britons” and Stopes was listed in the top 100. The Guardian newspaper urged its readers to “find out why Dr Marie Stopes deserves to be called a Great Briton,” followed by this:
“Women, can you imagine your body being the property of your husband? Being permanently pregnant through ignorance? Then thank Dr Marie Stopes. The lifestyle and personal fulfilment enjoyed by British women today owes more than many realise to this remarkable character.”
In other words, Stopes gave women reproductive freedom. The bit they always leave out is that Stopes campaigned and lobbied for laws to compulsorily sterilise people she considered “undesirable”. Had the laws that Stopes campaigned for been enacted, “reproductive choice” would have been made by a state official.
Another thing is that, while there is greater openness about Stopes’ eugenic beliefs today, academics and biographers present her eugenics as being adjacent to her birth control work rather than central to it. The “Tenets of the CBC” and her brand names for her contraceptives – Prorace and Racial – show that eugenics was central to her work. Indeed, when she died, she bequeathed her clinics not to the Family Planning Association but to the Eugenics Society.
5. Why do you think authors and researchers leave it out?
While one thinks of academics and biographers as being free to write what they like, I have formed the opinion that in relation to Stopes they are not. I get the impression that there is a relatively small network and, if you want to be included in it, you must toe the party line. To publicly dissent from what your well-established predecessors have written is a no-no and it will lead to your exclusion.
I formed this opinion when I read an interview with June Rose (author of “Marie Stopes and the Sexual Revolution”) in The Independent newspaper.
What the author reveals about her subject will cause a great deal of controversy, possibly exposing the biographer to ridicule, perhaps even cries of betrayal. ‘I am very apprehensive about the book’s reception,’ she said.
She does not talk easily about herself and is somewhat fearful of being known as the woman who brought Marie Stopes crashing from her pedestal … But Miss Rose has left us with a creature who could never find a place in the saintly calendar.
She said: ‘I hope this book celebrates Marie Stopes’s achievement as a sexual revolutionary. I would be upset if it didn’t. But I recognise there are sections which will alienate people, including feminist friends of mine.’
This surprised me because Rose’s book is well-researched and based on primary sources. Given this firm footing, why was she worried? And as for betrayal, who or what were being betrayed?
One of the things that Rose did was to destroy a foundation myth of Stopes’ story – that she was entirely ignorant about sex prior to and during her first marriage to Reginald Ruggles-Gates in 1911. According to the myth, it was only after the failure of her first marriage that she found out about sex by studying in the British Library.
Fortunately, I am outside that field, so am free of those constraints.
6. Thomas Malthus has been dead for nearly two centuries, yet you call him the prototype for a way of thinking that’s still with us. What did he actually argue, and why did your grandfather call it “a quack remedy for poverty”?
The entirety of Dr Sutherland’s 1922 book “Birth Control: A Statement of Christian Doctrine Against the Neo-Malthusians” is a root and branch demolition of Malthusianism, too lengthy to go into here.
More was G.K. Chesterton’s withering attack which Sutherland quoted to great effect:
Artificial birth control is one of the many quack remedies advertised for the cure of poverty, and G. K. Chesterton has given the final answer to the Malthusian assertion that some form of birth control is essential because houses are scarce:
“Consider that simple sentence, and you will see what is the matter with the modern mind. I do not mean the growth of immorality; I mean the genesis of gibbering idiocy. There are ten little boys whom you wish to provide with ten top-hats; and you find there are only eight top-hats. To a simple mind it would seem not impossible to make two more hats; to find out whose business it is to make hats, and induce him to make hats; to agitate against an absurd delay in delivering hats; to punish anybody who has promised hats and failed to provide hats. The modern mind is that which says that if we only cut off the heads of two of the little boys, they will not want hats; and then the hats will exactly go round. The suggestion that heads are rather more important than hats is dismissed as a piece of mystical metaphysics. The assertion that hats were made for heads, and not heads for hats savours of antiquated dogma. The musty text which says that the body is more than raiment; the popular prejudice which would prefer the lives of boys to the mathematical arrangement of hats, — all these things are alike to be ignored. The logic of enlightenment is merciless; and we duly summon the headsman to disguise the deficiencies of the hatter. For it makes very little difference to the logic of the thing, that we are talking of houses and not of hats …. The fundamental fallacy remains the same; that we are beginning at the wrong end, because we have never troubled to consider at what end to begin.”
What Dr Sutherland really hated about Malthusianism was that Malthus:
“… forged a law of nature, namely, that there is always a limited and insufficient supply of the necessities of life in the world. From this false law he argued that, as population increases too rapidly, the newcomers cannot hope to find a sufficiency of good things; that the poverty of the masses is not due to conditions created by man, but to a natural law; and that consequently this law cannot be altered by any change in political institutions.”
7. H.G. Wells wrote in 1901 about “the faith to kill” and a future state that would euthanise the “feeble, ugly, inefficient.” How did a celebrated novelist — and someone widely seen as a progressive thinker — arrive at that?
H.G. Wells was not alone in advocating the killing of the unfit to achieve the perfection of mankind.
In 1900, Dr W. Duncan McKim had advocated “a gentle, painless death; and this should be administered not as a punishment, but as an expression of enlightened pity for the victims—too defective by nature to find true happiness in life—and as a duty toward the community and toward our own offspring.”
Wells’ fellow Fabian, G.B. Shaw said that people should go before a committee once every few years to justify their lives: “If you can’t justify your existence, if you’re not pulling your weight in the social boat; if you are not producing as much as you consume or perhaps a little more, then clearly we cannot use the big organization of society for the purpose of keeping you alive, because your life does not benefit us, and it can’t be of very much use to yourself.”
Novelists Virginia Woolf and D.H. Lawrence also advocated the killing of the feeble.
These prejudices were given academic backing. Karl Binding and Alfred Hoche’s “Permitting the Destruction of Life Unworthy of Living” (“Die Freigabe der Vernichtung Lebensunwerten Lebens“) was published in 1920 and was later used as the basis for the Nazi party’s T4 Aktion. Apparently, when Binding and Hoche learned this, they expressed surprise saying that it was an academic thought experiment rather than an instruction as to what should be done.
In fact, there was so much talk of killing the feeble that it would have been surprising had it not happened.
Dr Sutherland for one was not surprised. In 1921, his article in the Westminster Gazette referred to “a Super-Eugenist, greatly daring” who would “slay every consumptive in the land tonight”.
In his 1925 book, Birth Control Exposed, he wrote:
“If a wave of madness passed over our country, and this eugenic nightmare came true, we might very well ask what tribunal is to decide as to which of us is unfit. About you who are reading this book, I know nothing whatever, but I have a shrewd suspicion that the neo-malthusians have already decided about me. The point is that when these people discuss sterilization, they picture themselves sitting round a table and ordering other people to be sterilized. In the same way Communists, when they talk about the bloody revolution, always picture themselves knocking other people on the head, and indeed they become very angry when I tell them that the other people will retaliate. And thus do all enemies of freedom.”
In 1933 his short story called “The Perfect Eugenic State” incorporated a poison gas lethal chamber which was used to rid society of its defective elements.
To someone who had his eyes open, it was clear where it was all going. And yet sadly this line of thinking continues today.
Giubilini and Minerva’s “After birth abortion: why should the baby live?” was published by the British Medical Journal on 23 February 2012.
In it, the authors asserted that “‘after-birth abortion’ (killing a newborn) should be permissible in all the cases where abortion is, including cases where the newborn is not disabled.” When the article caused controversy, the authors expressed surprise on the grounds that it was an academic paper, not a manifesto.
More recently, Renate Lindeman of Substack’s “Liberty Letter” posted an article about a Canadian study that:
“… explores the potential economic savings from expanding medical assistance in dying, where it is currently a leading cause of death, to include vulnerable groups that cost the government more than they contribute in taxes. These groups include individuals with severe mental health issues, the homeless, drug users, retired elderly, and indigenous communities. Both voluntary and non-voluntary scenarios were analyzed, projecting total savings of up to CAD $1.273 trillion by 2047. With an estimated 2.6 million deaths in the voluntary scenario, mostly among mentally ill and elderly populations, this cost-saving measure raises significant ethical concerns. Financially incentivizing MAiD could shift healthcare priorities away from providing necessary support, potentially devaluing vulnerable lives and fostering a troubling reliance on assisted death as an economic solution. The findings highlight a need for ethical scrutiny of MAiD policy expansion.” [Emphasis added]
No doubt the authors of this papers will express surprise if and when it is used as the basis to “off” Canadian citizens to save money. Plus ca change …
8. You’ve traced how organisations repeatedly rename themselves to soften their image — the Eugenics Society becoming the Galton Institute and then the Adelphi Genetics Forum, the Voluntary Euthanasia Society becoming Dignity in Dying. What does that pattern tell us, and why does it work?
It is all about marketing and making your ideas acceptable. Part of this is to make it appear as if what you are saying is new and important. This is because people are obsessed with novelty, so presenting old ideas won’t work. Further, your ideas have to be repackaged to conform to the mores of contemporary society.
It is a good idea to choose a name that does not clearly state your agenda. Better still, choose one that will make your opponents prima facie look bad. For instance, calling your society “Dying with Dignity” is good because if your opponent says: “I disagree with dying with dignity”, they appear to be callous. “Killing Old People,” not so much.
The stated motivation also plays a role: to advocate eugenics for the purposes of national efficiency and racial purity is now not permitted. Using it in the cause of “science” is, such as the promise to prevent genetic diseases. And there are a number of organisations that will facilitate your zygotes (through IVF) and then test them for personality traits, height, IQ and so on to give you the ideal designer baby. So what is now forbidden to nation states is permitted to families – if they have the money.
9. You’ve highlighted a 1960 decision by the Eugenics Society to pursue its aims through what it called “crypto-eugenics.” That’s a striking phrase. What did they mean by it, and where do you see that approach still operating?
In the aftermath of the Second World War, membership of Britain’s Eugenics Society fell by almost one-half. To address this, it resolved: “the Society should pursue eugenic ends by less obvious means, that is by a policy of crypto-eugenics, which was apparently proving successful with the US Eugenics Society.”
Of course, “crypto” means secret, not less obvious, but maybe I am nit-picking.
What it meant is that they were going to continue what they were doing and were going to do it covertly. For instance, it meant that the name of their journal changed from The Eugenics Review to The Journal of Biosocial Science. It took longer for the Society to change its name to the “less-evocative” Galton Institute in 1989, and in 2021 it changed its name to the even less evocative Adelphi Genetics Forum.
Eugenics and population control are controversial. While I don’t think that today’s eugenicists, whether in the Adelphi Genetics Forum or elsewhere, would feel bound by a 1960 resolution, I do think that they are aware that secrecy facilitates a quiet life.
Owing to the essential nature of secrecy, it’s hard to see if it is being applied or not. Occasionally though one gets whiffs of smoke. For instance, on page 296 of “Life Without Birth” (1970) Stanley Johnson wrote about:
“An inter-departmental committee of senior civil servants was set up to advise the government of population matters. It has now operated for over a year, reporting direct to the powerful home affairs committee of the Cabinet, and advises how legislative and administrative acts can be made to further a policy of population stabilization. Its existence has been deliberately kept secret for fear of political repercussions, and not many people either in Whitehall or Westminster are aware it is there at all.”
I don’t know if the committee is still going.
10. Across roughly a century of figures — Galton, Stopes, Wells, Shaw, Sanger, Ehrlich, Holdren — you argue the same three solutions keep reappearing: more top-down control, restricting births, and increasing deaths. Why do you think that particular combination is so persistent?
I think that the solutions are consistent because whether they realise it or not, they draw on the same traditions. At the heart of this is a deep-seated anger at God (the ultimate expression of which is to profess that God does not exist), a deep-seated hatred of humanity, and the hubristic belief that they alone can fix the problems.
While the names you mention are presented as great intellects, their solutions they present don’t arise from some great intellectual feat. In fact, their “solutions” are rather obvious.
As Dr Sutherland put it in 1936:
“When responsible and thoughtful members of society begin to advocate the prevention and destruction of human life by means of contraceptives, abortion, infanticide, sterilisation, and euthanasia, it is an evil omen, and the sign of a civilization whose creative power is spent.”
In his Letter to the 21st Century, I think Isiaih Berlin was on the money:
“If you are truly convinced that there is some solution to all human problems, that one can conceive an ideal society which men can reach if only they do what is necessary to attain it, then you and your followers must believe that no price can be too high to pay in order to open the gates of such a paradise. Only the stupid and malevolent will resist once certain simple truths are put to them. Those who resist must be persuaded; if they cannot be persuaded, laws must be passed to restrain them; if that does not work, then coercion, if need be violence, will inevitably have to be used—if necessary, terror, slaughter … then the end justified any methods that needed to be used, literally any.”
“But you must believe me, one cannot have everything one wants—not only in practice, but even in theory. The denial of this, the search for a single, overarching ideal because it is the one and only true one for humanity, invariably leads to coercion. And then to destruction, blood—eggs are broken, but the omelet is not in sight, there is only an infinite number of eggs, human lives, ready for the breaking. And, in the end, the passionate idealists forget the omelet and just go on breaking eggs.”
11. You’ve drawn a direct line between earlier euthanasia advocacy and Canada’s MAID programme today. What specifically are you seeing in MAID that connects it to that older tradition?
Both concern killing of humans and changing the law so that it isn’t categorised as murder. The only difference is the way it is marketed.
If you think that Canada’s MAiD program is all about compassion, I suggest you read “Government Economics of Expanding Canada’s Medical Assistance in Dying to Vulnerable Populations and the Ethical Implications of Allowing the State to Control Death” by Uzair Jamil and Joshua M Pearce which indicates the direction in which MAiD is going. Hat tip to Renate Lindeman of Substack’s “Liberty Letter” for drawing this to my attention.
12. Paul Ehrlich wrote about adding sterilants to the water supply. Margaret Sanger proposed corralling millions of people onto government farms. These sound almost cartoonishly extreme today — yet they came from mainstream, celebrated figures. How should a reader make sense of that?
I think that Ehrlich’s and Sanger’s solutions were aligned to the mores of their times so were less conspicuous then than they are now. The solutions being advocated today would appear to be cartoonish to people who don’t live within the context of our times.
Things change so fast these days that it doesn’t take long for the context to change and for things that look sensible to become ridiculous and cartoonish.
The reaction to Covid provided a lot of these: hospital staff dancing in TikTok videos, the normalisation of collapsing sportsmen and women, Perspex partitions on school desks and so on.
For me, the idea that cows and, in particular, their farts are a huge problem to the extent that the herds need to be culled. And the W.E.F.’s “You’ll own nothing. And you’ll be happy.” And to ignore the impact that solar weather has on the earth’s climate and to focus on carbon dioxide. All of these ridiculous and clownish things will be seen for what they are in due course (if they are not perceived that way already).
13. You’ve placed climate change advocacy in the same lineage as Malthusianism and Ehrlich’s Population Bomb. What are the tells that make you see it as a continuation of an older pattern rather than something genuinely new?
It has the same “scarcity” mentality. Our existence on the earth, wonderful to behold and evidence of an Almighty and loving God for some, is in fact a cosmic prank! There are lots of people, but there isn’t enough stuff!
The tradition of Malthusianism and Ehrlich’s Population Bomb and Al Gore’s Inconvenient Truth is to predict disasters to frighten people to act. It is also traditional that, when the predicted disasters don’t occur, they don’t apologise or admit that they were wrong.
Human nature hasn’t changed all that much. Many people feel the need to tell other people how to live their lives and even whether to live their lives. When you look at problems at the highest levels, they do appear to be insoluble, but that is sometimes because of the level at which you are looking at the problem makes it insoluble.
To the Malthusians, the problem is always the population. Poverty, war, shortages and famine are always caused by over-population, rather than by defective governance, injustice, incompetence, greed, selfishness and corruption.
14. You write that “many current events are noise that distract us from reading the signal,” and that history helps separate the two. For a reader who wants to start spotting the pattern themselves, what are the practical tells — the things to watch for when someone says “we have to act now”?
The way history is taught is “this is what happened in the past,” in other words, something removed and distant from your life. The reality is that history is the continuation and encapsulation of ideas (in the broadest sense of that word) in the present. Study history in that context.
Get to grips with the fact that no one can know everything about any particular event, so be sceptical of the explanations you are given. It doesn’t mean you reject good explanations, so much as realise that at best, they are only approximations, albeit good ones.
And be sceptical that revolutions happen spontaneously, without leadership, planning, organisation and money. “People were hungry, they needed bread, so they overthrew the king and set up a republic,” – what nonsense!
The “Occupy Wall Street” movement was a real organic movement. It didn’t translate into political change because it lacked leadership, planning, organisation and money. So be skeptical when movements (and leaders) arise from nowhere and are presented as organic and grass-roots.
I think Hudson’s Law is sound. It states that anything that is (1) presented as a global crisis (2) admits only global solutions (3) and suppresses dissent, is definitively a scam.
I think you should be acquainted with the “MINDSPACE” paper produced by the Behavioural Insights unit. You can download a copy at: https://www.bi.team/publications/mindspace/ The Behavioural Insights unit – colloquially known as the “Nudge Unit” – advises governments on the deployment of psychological techniques in implementing their policies. If you are aware of their techniques, you will be better able to see when they are being used against you.
Finally, try to develop discernment. Be patient with yourself when you get it wrong, but do keep going!
15. Your grandfather predicted in 1929 that “the cataclysm which may end the eighth known epoch in civilisation may be a lack of European children.” Nearly a century later, fertility rates are collapsing across the developed world. What do you think he’d want people to take from that?
One sentence: “If our civilisation is to survive we must abandon those ideals that lead to decline.”
This comes from the final paragraphs of Birth Control (1922):
“Our declining birth-rate is a fact of the utmost gravity, and a more serious position has never confronted the British people. Here in the midst of a great nation, at the end of a victorious war, the law of decline is working, and by that law the greatest empires in the world have perished. In comparison with that single fact all other dangers, be they war, of politics, or of disease, are of little moment. Attempts have already been made to avert the consequences by partial endowment of motherhood and by saving infant life. Physiologists are now seeking the endocrinous glands and the vitamins for a substance to assist procreation. ‘Where are my children?’ was the question shouted yesterday from the cinemas. ‘Let us have children, children at any price,’ will be the cry of tomorrow.
“And all these thoughts were once in the mind of Augustus, Emperor of the world from the Atlantic to the Euphrates, from Mount Atlas to the Danube and the Rhine. The Catholic Church has never taught that ‘an avalanche of children’ should be brought into the world regardless of consequences. God is not mocked; as men sow, so shall they reap, and against a law of nature both the transient amelioration wrought by philanthropists and the subtle expediences of scientific politicians are alike futile. If our civilisation is to survive we must abandon those ideals that lead to decline. There is only one civilisation immune from decay, and that civilisation endures on the practical eugenics once taught by a united Christendom and now expounded almost solely by the Catholic Church.”
16. What are you working on now, and where can readers follow your work and stay in touch with what comes next?
I have a Substack which is free, and I curate hallidaysutherland.com (I am contactable through these sites).
I have been living in London for the last 18 months, so I am focusing on rebuilding my coaching practice and facilitation work.
I continue to promote “Exterminating Poverty: The true story of the eugenic plan to get rid of the poor, and the Scottish doctor who fought against it” through speaking engagements and interviews like this one. I hope that one day it will be made into a feature film.
Thank you for the opportunity to tell your readers and subscribers this important story.
Israel’s supporters have gone apoplectic over a short post on X from the journalist Mehdi Hasan, highlighting Israel’s peculiar marriage laws.
Hasan asks: “Did you know that you can’t have a civil or secular marriage in Israel?”
He’s not wrong. Israel has banned civil marriage. You can wed only in a ceremony strictly controlled by religious authorities. If you want a civil marriage, you have to travel to another country.
Why, you might reasonably wonder. Isn’t Israel a modern, secular, western-style liberal democracy? After all, that’s what our politicians and media keep telling us.
The most popular rejoinder to Hasan from Israel’s apologists – that the situation is no better in Saudi Arabia – is not quite the flex they seem to imagine. So Israel offers the same human rights protections as Saudi Arabia? Impressive.
Others have pointed out that Israel inherited the so-called “millet” system from the Ottoman empire, which gave the leaders of each confessional group across the Middle East autonomous control over their community’s religious affairs.
Doubtless, 150 years ago the system worked relatively well in reducing communal tensions in religiously diverse parts of a large empire. It prevented officials in Constantinople – modern-day Istanbul – from getting dragged deeply into the day-to-day affairs of its often distant subjects.
But 150 years ago, Britain sent children up chimneys to sweep them. The law was changed around that time to stop this abusive and dangerous practice.
Israel was established nearly eight decades ago, supposedly as a secular, western-style liberal democracy. It has had 78 years to change those archaic Ottoman marriage laws.
Why hasn’t it done so?
All the bluster decrying Hasan’s post is a desperate attempt to deflect attention away from the fact that Israel’s antiquated marriage laws survive because they are useful to Israel.
In fact, they are more than that. They are a core component of Israel’s version of apartheid – a racist system of segregation Israel has successfully shielded from the view of western publics with the help of western politicians and media.
‘Demographic threat’
Israel’s ban on civil marriage is central to its efforts to prevent what past racist societies, such as apartheid South Africa and the American Deep South, termed “miscegenation” – that is, sexual relations between different ethnic groups. You might remember that the Nazis had unpleasant views on this subject too.
Preventing assimilation in the Jewish state is completely legitimate and not at all racist. You are assuming as a basis for the discussion that preventing intermarriage is wrong, while ignoring the fact that most [Jewish] girls who go with Arabs are poor girls who are being used.
Former education minister Rafi Peretz called mixed marriages involving Jews a “second Holocaust”.
In Israel, such views are entirely mainstream. In 2018, Yitzhak Herzog, Israel’s current president and the former leader of an ostensible leftwing Israeli party, described mixed marriages among American Jews as a “plague” for which a “solution” had to be found – presumably by copying Israel’s approach.
In Israel, the chief concern is not about marriages between Jews and the Palestinians under occupation – which Israel and its supporters like to present, bogusly, as a straightforward “security” matter.
In the occupied territories, Israel uses far blunter methods than laws to prevent any kind of intimate relations developing between Jews and a captive Palestinian population. It prefers physical containment and violence.
Palestinians under occupation are forcibly separated from Israeli Jews. They are hemmed into their own tightly confined ghettoes by Israel’s network of steel and concrete barriers; by the Israeli army; by checkpoints; by separate, apartheid roads in the West Bank; and by Jewish militias living on stolen lands in so-called “settlements”.
There is little chance of interaction, let alone intermarriage, in such circumstances – except when Israeli soldiers or armed Jewish settlers come rampaging into Palestinian communities to destroy crops, kill livestock, poison wells, torch homes and cars, and beat up – and sometimes kill – the inhabitants.
Nonetheless, there is still a potential vulnerability in Israel’s system of segregation.
In 1948, Israel expelled 80 per cent of the Palestinian population from their homes and lands in an area that was henceforth to be called, not Palestine, but the “Jewish” state of Israel.
A few Palestinians remained, however, inside those borders – mostly from oversight or error. Despite covert efforts by Israel for several years after the 1948 war to force them out of the state, its officials soon came under international pressure to give these stranded Palestinians citizenship – even if in practice, as we shall see, this conferred on them very inferior rights.
Even today, Israel is extremely worried about a supposed threat from its third-class Palestinian “citizens” – officially termed “Israel’s Arabs”. Given a higher birth rate, their numbers have grown exponentially over eight decades. They now comprise a fifth of Israel’s population.
Israeli journalists, academics and politicians, including prime minister Benjamin Netanyahu, regularly call the country’s Palestinian citizens a “demographic threat”, and endlessly worry about the “Palestinian womb”.
No state of all its citizens
But Israel faces a countervailing pressure. If it makes its treatment of Palestinian citizens too obviously racist and oppressive, some outsiders might start to realise it is not the secular western-style liberal democracy it claims to be.
You will hear the pro-Israel lobby in the West tell you that so-called “Israeli Arabs” have exactly the same rights as Israel’s Jewish population, guaranteed by Israel’s Declaration of Independence. That is not even remotely true.
Adalah, a leading legal rights group in Israel, has a database showing more than 70 laws that explicitly discriminate between Jewish citizens and Palestinian citizens. These laws form the core of Israel’s apartheid system.
Israel’s Basic Laws, a sort of constitution, explicitly exclude any principle of civic equality. Every attempt by a Palestinian party in Israel to get a debate in the parliament on Israel becoming a “state of all its citizens” – that is, a liberal democracy – is barred from discussion. And in 2018 the Israeli government passed a Nation-State Law declaring that Israel belongs exclusively to the Jewish people, not to all citizens who live there.
As with Palestinians under occupation, Israel has almost entirely confined its Palestinian citizens to their own segregated, underfunded, under-resourced communities (townships) on less then 3 per cent of the country’s territory.
A small minority of Palestinian citizens inside Israel live in segregated, deprived neighbourhoods of what are misleadingly termed “mixed” cities. Other Palestinian citizens, the most oppressed of all, live in communities inhabited by their families for centuries but which have been criminalised by an Israeli state that refuses to recognise them.
Many hundreds of Jewish rural communities, by contrast, operate effectively as exclusive membership clubs. They have the power to exclude Palestinian citizens – a right they take full advantage of.
Separate planning structures ensure massively overcrowded Palestinian communities inside Israel are unable to build new homes and expand. Palestinian children are schooled in a separate and much inferior education system.
For the who wish to dig deeper, I have written a lengthy essay setting out the details of Israel’s apartheid system here.
The ban on civil marriage inside Israel’s borders is not usually cited, even by critics, as an example of its apartheid system of rule. But the ban persists because it is the ideal way to conceal segregation under the veneer of equal treatment.
Israel’s Palestinian citizens must marry in ceremonies conducted by their religious community’s leaders: by Muslim clerics, or by various Christian churches, or by the Druze clergy.
It is the same for Jews in israel. They must be married by an Orthodox rabbi.
So everyone faces the same restrictions. But the point is this: the equality of treatment ensures very unequal outcomes. It is designed that way.
Fascist thugs
Inside Israel, intermarriage is only possible if one party can convert to their partner’s religion.
Israel’s Orthodox rabbinate makes it impossible for Palestinians under occupation to convert to Judaism in Israel, with the head of its conversion authority stating in 2016 that any such applicants are rejected “without review because of their ethnic origin”.
Meanwhile, Israel makes it almost as difficult for anyone else considered a non-Jew to convert to Judaism, most especially Palestinian citizens. Over decades, there have been only a handful of such cases.
In practice, this means that in any relationship between a Palestinian citizen of Israel and an Israeli Jew, it almost always falls to the Israeli Jew to convert to the religion of the Palestinian citizen, whether a Muslim, Christian or Druze. That entails the Jewish partner losing their Jewish status and the many consequential privileges inside Israel that derive from that status.
Israel has found this is a much better solution than apartheid South Africa’s, where blacks and whites were explicitly barred by law from marrying. Israel can achieve the same result more quietly.
Given the entirely segregated structure of Israeli society, and the strong social taboos among Israeli Jews on “miscegenation”, the number of intermarriages in Israel between Jews and Palestinian citizens barely reaches double digits each year.
There are even groups like Lehava – Israel’s version of the Ku Klux Klan – that go around beating up Palestinians caught anywhere near the Jewish neighbourhoods of Jerusalem and terrorising any young Jewish women suspected of being romantically involved with a Palestinian. Lehava hold noisy and disruptive protests to shame the odd Jewish woman who converts and marries a Palestinian citizen.
All of this happens with a quiet wink from the authorities. The current police minister, Itamar Ben Gvir, has long been a patron of the fascist, Jewish supremacist thugs of Lehava.
In the rare cases of a Jew converting and marrying a Palestinian citizen, the Palestinian partner faces innumerable legal and social obstacles to integrating into a Jewish community to which they do not belong.
Instead, the Jewish partner moves to a Palestinian community – an Israeli version of a township like Soweto – and educates their children inside the vastly inferior “Arab” school system. The former Jew loses most of the ethnic privileges they previously enjoyed inside the world’s only “Jewish” state.
Faced with this as their future, such couples often seize the opportunity for neither to convert and instead marry and live abroad.
Unwelcome guests
None of these difficulties are accidental. It is exactly how you would expect an apartheid system that prefers to obscure its apartheid character to structure its laws – and thereby help its lobby in the West, including the western political and media class, to claim that Israel is “the only democracy in the Middle East”.
Israel learnt from the mistakes of the old South Africa. It mastered the modern arts of public relations – or at least it did until Benjamin Netanyahu tore up the script by erasing Gaza.
Inside Israel, the apartheid system extends far beyond marriage laws to touch all areas of life.
Here is another way Israel has obscured its apartheid system – again not in the occupied territories, but inside Israel itself.
The same system that denies Israelis the possibility of a civil or secular marriage also refuses to recognise that they have any kind of civil or secular identity, simply as Israelis. By law, everyone in Israel must belong to a confessional group, identified as a Jew, Muslim, Christian or Druze.
Which makes sense of another little-known fact about Israel: Israel is the only country in the world that does not recognise its own – in this case, Israeli – nationality. Why? For the simple reason that, were Israelis to share a common national identity, it would be much harder for the Israeli state to operate its apartheid system.
Israeli nationality exists only as a fiction on Israeli passports to allow the population to travel internationally. Inside Israel, everyone is identified by their confessional group.
In Israel, “Jewish” is treated as a nationality. Remember the 2018 Nation State Law. What it declared is that the state of Israel belongs exclusively to the “nation” of Jews – that is, to every Jew around the globe, not just those living in Israel.
Muslims and Christians are lumped together into a similarly artificial “Arab” nationality, while the Druze have their own, different nationality. The same Nation State Law makes clear that the state of Israel does not belong to these other, non-Jewish “nations”, despite their families having lived on the same lands for centuries. Palestinian citizens are nothing more than guests – and unwelcome ones at that.
This segregation carries through to Israel’s ID cards. These cards, which must be carried at all times, used to include a section that expressly showed the “nationality” of each Israeli. But this section attracted uncomfortable scrutiny during a lengthy and ultimately unsuccessful legal battle by a group of dissident Israelis seeking recognition of an Israeli nationality. Officials removed the category from the card. However, Israel’s population register still includes a nationality classification.
In addition to Jew, Arab and Druze, there are more than 120 other categories to deal with all the anomalies. I was just one such anomaly after I married a Palestinian Christian and entered a lengthy and difficult naturalisation process. My nationality was classed as “British”.
Why all this complexity? Why all this unique weirdness?
Because Israel needs to conceal its system of apartheid. The old South Africa simply said: one law for whites and another for blacks.
Israel knows this no longer plays well. So it has devised a convoluted, baffling system that few understand as a way to avoid attracting attention and criticism.
Special Jewish rights
So let’s end with just one example of how Israel’s apartheid system works in practice.
Notionally, Israel confers on all its citizens – Jews, Muslims, Christians, Druze – equal rights as citizens. But with a sleight of hand, it then undermines those equal rights by conferring superior “national” rights on one group only, Jews. If there is a conflict between a citizenship right and a Jewish “national” right, you’ve probably already guessed that the Jewish national right takes precedence.
Education is a good illustration. All Israeli citizens enjoy a right to have their children educated, because education is a citizenship right. But lots of veiled manoeuvres – like extra budgets for National Priority Areas, special subsidies for Jewish religious schools, funding from the diaspora, and bigger tax disbursements from central government for Jewish local authorities – mean Jewish schools are far better funded than “Arab” schools.
Education for Israel’s Palestinian citizens has been underfunded for eight decades. So even though Israel’s apologists will claim the funding gaps are slowly narrowing, the continuing shortfall simply compounds a decades-long historical injustice. Arab schools are so far behind they can never catch up without aggressive additional funding Israel clearly has no intention of ever providing them with.
There are massive shortages of classrooms and staff in dilapidated school buildings. Old books are often grossly outdated and poorly translated into Arabic by the state. Palestinian educational leaders have no input into the curriculum the community’s children are taught. There are strict controls by Jewish (usually racist) officials over what can be taught and who can teach. And on top of all this, huge cultural biases in qualifying tests make it far harder for Palestinian citizens to gain entry to universities in Israel.
There are many other problems in education. For example, nearly one in 10 Palestinian children in Israel live in historic communities built on lands that the Israeli state now wishes to “Judaise” – reserve for the Jewish population – and are therefore denied all recognition.
Treated like criminals, these children rarely have schools in their communities because no permanent buildings are allowed. What buildings there are cannot be connected to the electricity or water grids. Even children of kindergarten age must typically travel long distances – sometimes close to 60 km a day – to get to a licensed school.
The forms of discrimination in education alone are endless. But they do not stop there. The discrimination is replicated in all major facets of life for Israel’s more than 2 million Palestinian citizens through these conceptual and legal contortions over religion, citizenship and nationality.
None of this should be a surprise. It is exactly what you would expect in an apartheid state like Israel.
In 1959, Ingeborg Bachmann concluded that the truth is something people can be expected to handle, since they are quite capable of enduring it, no matter how uncomfortable it may be. Literature, she argued, should neither conceal nor gloss over the truth.
This is all the more true of the media, which for years have failed to fulfill their duty as the fourth estate. The world is heading toward a new world war, and the majority of humanity is unable to assess the risks and opportunities when the media distort the facts through their propaganda in such a way that the truth vanishes into an ever-thickening fog. The dumbing down has reached such a level that even politicians in the West believe the propaganda of their own media and act accordingly. The falsehoods that politicians spread are no longer perceived by them as lies; for the most part, their intellect is simply not sufficient for that. It must be stated that politicians have first and foremost become “ambassadors” of an ever-declining level of education—and continue to do so—and, as a result, have become victims of their own propaganda.
This article attempts to show that it is still possible to separate the wheat from the chaff, because the truth is hidden amid all the garbage in the news coverage.
Don’t Forget About Evil
In the article “Will Evil Prevail?,” I pondered who actually determines geopolitical events around the world. I discussed the “City of London” and the “Rothschilds” as examples of forces that steer the world from behind the scenes. They are thus also responsible for wars, coups, and other upheavals in our world. Even the small portion of the Epstein Files that has come to light provided a first impression of the entanglements among the powerful. See “Epstein – ‘Concierge of Evil’ – Dangerous Questions.” For example, the Rothschild family was dragged back into the public eye; the very family that has gone to great lengths to convince the world that it has exerted no influence since World War II and merely operates a few private banks, museums, and vineyards. It should come as no surprise that discussion of the contents of the Epstein Files—or their further releases—has completely vanished from the media; one might well wonder who controls the media.
Incidentally, the ‘deep state’ is not a concept peddled by a few crackpots. As early as 2017, President Putin spoke about it in no uncertain terms:
“Presidents change… Then well-dressed men arrive, in dark suits, with their suitcases. They start explaining how things really work… and everything changes instantly.”
Control is exercised either directly by shareholders or indirectly through political or economic influence—for example, by controlling advertising revenue, blacklisting, or manipulating view counts on YouTube channels. Control over the media in the Collective West is, de facto, complete—not a bad achievement.
Consider this: freedom of speech is championed very vocally by politicians and the media at every opportunity, whether appropriate or not. Practically “in tandem,” it is restricted in the very same breath by first denouncing the spread of “fake news” and “hate speech”—that is, the expression of genuine freedom of speech—just as loudly, and then defining and enforcing it as a criminal offense for one’s own political gain.
Ultimately, then, it is the state that defines what “fake news” and “hatespeech” mean. As a result, a right that is no longer absolute but has been relativized collapses under this restriction. In Germany, the desired political direction of judicial decisions is ensured through the political appointment of judges to the Federal Constitutional Court. The process for selecting judges to the European Court of Justice follows a similar procedure.
The consequences of this restriction are deliberate and obvious. Analysts who express even the most well-founded opinions that do not suit the tastes of those in power are stripped of their rights, dispossessed, and portrayed as criminals without due process. The method of choice is, for example, EU sanctions, which were originally enacted to target terrorists but are now—with the support of the general public—imposed on the most objective experts, such as the Swiss citizen (and thus non-EU citizen) Jacques Baud; see our coverage on this. The result of this targeted political influence is reporting in the traditional media that no longer has anything to do with the truth, but often turns it on its head.
All Geopolitical Crises Stem from a Single Source
All military conflicts around the world must be understood as a single package, a comprehensive strategy. The same people who are fueling the war against Iran and the violent creation of “Greater Israel” are also responsible for the conflict in Ukraine and the war between Europe and Russia that will likely unfold soon—and many other conflicts, such as those in Africa, which we have neglected in our blog, are likewise part of this strategy. Everything is interconnected, and it shows a lack of geopolitical understanding when journalists defend the war—waged with genocidal methods—against Iran, Lebanon, and Gaza, while simultaneously supporting Russia’s actions in Ukraine. The forces triggering and fueling these conflicts are identical. Understanding this is very helpful in grasping the overall geopolitical situation.
The overall picture is not hard to understand: After hundreds of years of colonial rule over the rest of the world, the Collective West has already lost the economic race against the Global South; more on this below. While wars over the past 500 years have been about who in the West would wield the scepter of hegemony over the colonial empire, today’s conflicts are about whether the Collective West can maintain its colonial empire. The odds are against it, as we have already outlined in our series “The War Between Two Worlds Has Begun.” At that time, we anticipated many individual conflicts spanning decades, but without a world war. This relatively optimistic thesis now seems to be faltering, as aggression between the world powers is escalating daily, the Collective West refuses to abandon the arrogance of the colonial master, and completely overestimates itself with spurious arguments.
The Defence Budget as a Measure of Military Strength Is a Fallacious Argument
For decades, the Americans have led the world to believe that they have the strongest armed forces in the world. This claim is backed up by an astronomical figure: the U.S. military budget of no less than 1.5 trillion U.S. dollars. That is 10 times more than the Russian military budget, or even 190 times more than Iran’s military budget, which amounted to 7.89 billion U.S. dollars in 2024. NATO, excluding the US, spent 608 million U.S. dollars.
Nevertheless, the US—along with Israel—suffered defeats in both the 12-Day War and the ongoing war, which has spiraled out of control. NATO, alongside the US, is suffering defeat in Ukraine. The massive budgets in the West are a clear indication that the military there is not designed to defend freedom, but rather to rake in as much money as possible. As a result, a weapons system in the West is considered successful if it can be sold—for as much money as possible—to its own armed forces or those of third countries. In 2024, we compared two combat helicopters that experts deemed equivalent: the Russian Kamov KA-52 and the American AH-64 Apache. The Apache costs 155 million U.S. dollars; the Kamov costs 16 million. On top of that, Western weapons systems are produced in virtually homeopathic doses, and it is impossible to increase production to a level capable of sustainably supporting a protracted conflict—it is too expensive, too complex, and combined with an industrial capacity that simply no longer exists.
In the medium term, the US will not be able to produce high-quality military equipment in sufficient quantities at reasonable costs, as it currently faces a multi-faceted problem: First, there is a lack of will, since profit is the primary goal of the military-industrial complex. Second, due to 30 years of deindustrialization, the US no longer has the industrial base necessary to produce weapons in quantities sufficient for wartime.
Rather, the focus is on making a profit. Objective observers should realize that such a strategy is bound to lead to disaster in a crisis—as has been demonstrated in the Middle East and Ukraine. According to various experts, the West has fallen at least a decade behind its competitors in both missile technology and drones in those regions.
Iran, for example, whose defense spending is about 200 times less than that of the US, possesses hypersonic missiles that are extremely difficult to intercept. In contrast, the Collective West still has no operational hypersonic weapons. Critics attribute this to a combination of profit-seeking, arrogance, and corruption within the military-industrial complex.
If the West wants to operate on an equal footing militarily in the future, it would have to fundamentally reform the military-industrial complex—a task that seems nearly impossible given the existing economic and political balance of power; this industry is controlled by the groups discussed above.
A Lack of Will to Fight in the West
How does the Collective West react to the wars it has lost? — It increases its military budgets without addressing the necessary structural issues. In the West, there is a mistaken belief that everything can be solved with money. In Russia, the defense industry is essentially state-owned, and therefore there is a strong interest in producing high-quality but affordable weapons.
Thus, there will only be a change in the US if the American pursuit of profit in weapons production were seriously called into question—and if society were able to attract the best minds to the defense industry in the interest of American society as a whole, which is not the case today. American missile physicists earn more as analysts at investment banks, and they have no motivation to serve their country, given the poor state of the will to defend the West. In Germany, for example, one figure dashes any hope for greater willingness to serve: out of 300,000 young Germans, 530 are willing to perform military service—that’s 0.17%! (Source: Süddeutsche Zeitung ). This figure stands in stark contrast to statements made by Boris Pistorius, the German Minister of Defense, who announced as early as 2024:
“We must be combat-ready by 2029,” the minister said. “We must provide a deterrent to prevent things from escalating to the extreme.”
The outlook for the Collective West to prepare its armed forces for war is thus bleak. Nevertheless, the Europeans and Americans seem to be charging headlong into a world war with outdated yet overpriced weapons systems and without the necessary will to defend themselves among the population. This not only seems insane—it is insane. The facts speak for themselves. Who would do such a thing? Corrupt politicians, like the ones we described at the beginning.
The Economy as an Indicator of Losing
If we look at the economic data, it is easy to see that the Collective West has already lost the economic race. History teaches us that, in such a situation, war is the only option left.
For years, I have been drawing attention to the devastating national debt and the grotesque valuations in the financial markets. On top of that, the Collective West also cheats when calculating economic power. All of this is done to maintain a narrative that allows the US to continue to be portrayed as number one. If you calculate GDP on a purchasing power parity basis—that is, taking into account the local purchasing power of individual countries—the US has already lost.
According to this calculation, China ranks ahead of the US, Russia ahead of Japan, and Germany.
Furthermore, the Collective West, as the aggressor, finds itself in a domestic political and economic situation that does not allow for a military showdown with Russia, Iran, and China: US debt stands at over 121%—the last time this was the case was at the end of World War II, following an industrial war that brought the US global dominance. After 35 years, and under economic and political conditions that remained favorable to the US, this debt was reduced to below 40%.
In 1945, the Americans reached the height of their power. Together with the Soviet Union, they dominated the course of the war, held 22,000 metric tons of gold, and American industry produced 70% of the world’s manufactured goods. This is what true “full spectrum dominance” looks like: military dominance, industrial dominance, gold—because whoever has the gold sets the rules. Now the US is once again facing a world war, and the situation looks much like it did after the last war, with one major difference: China is at least the US’s economic equal, with far more favorable economic conditions.
These are not the conditions necessary for a military conflict on a global scale—neither financially, nor economically, nor, consequently, politically.
Middle East
It is clear from the text of the MOU that Iran has defeated both Israel and the US militarily; otherwise, the Americans would never have signed such a document. Israel cannot, without risking the collapse of its own delusions of great-power status, comply with the spirit of the document and end the war in Lebanon and Gaza. Therefore, there will be no peace.
Our comments on this topic: “Iran Defeats the US – Thoughts.” In Iran, voices are growing louder claiming that the president and foreign minister are not negotiating hard enough—public pressure in Iran is calling for a tougher stance toward the US and Israel. Iran’s Supreme Leader, Mojtaba Khamenei, has approved the memorandum of understanding (MoU) with the US to end the regional war under certain conditions. However, in a public statement, he said that he fundamentally held a “different view,” but had agreed to the agreement after receiving guarantees from President Masoud Pezeshkian that Iran’s national rights and the “Resistance Front” would be safeguarded. This is a clear indication that the Iranians are ultimately unwilling to make compromises at the expense of Lebanon and Gaza.
It is to be expected that the conflict in the Middle East will continue: Neither the US nor Israel is willing to accept defeat in the war and deal with its consequences. This stance maintains a state of limbo that could tip in one direction or the other at any moment. However, this strategy is countered by the fact that time is running out for the West because of Hormuz. The dwindling oil reserves were the main reason the US signed this MOU in its current form in the first place. The Americans are thus seeking a state of limbo that allows them to prepare their next military steps in peace; however, this state can only be maintained if the Strait of Hormuz remains open in the meantime. While approximately 130 ships passed through the Strait of Hormuz daily until February 28, 2026, these numbers dropped to practically zero, then stabilized at 5%–10% of pre-war levels, before surging to 70 ships on June 25, 2026. These figures should be treated with caution: It is said that the majority of these 70 ships were exporting oil from Iran after the US lifted the oil sanctions upon signing the agreement. If the Israelis do not withdraw from Lebanon and the Iranians remain steadfast—which is to be expected—then the Strait of Hormuz will remain a congested bottleneck: the time bomb for the West’s supply of raw materials continues to tick.
The Iranians can wait—the Americans cannot. When assessing the situation, one should simply disregard Donald Trump’s statements, because Trump speaks of peace one moment and war the next, changing his mind sometimes several times a day. He seems to believe that he can achieve something with the Iranians through this “New York-style deal-making” terror, but that is not the case, since he achieves only one thing: Americans are increasingly proving themselves to be agreement incapable, thereby threatening world peace.
War in Europe
The armed conflict in Ukraine, instigated by the West, began in 2014. Only those who do not classify Ukraine’s years-long artillery shelling of the Donbass as an act of war claim that the Russians started the war in February 2022. This is just one fact that is so obvious that one can only wonder at the West’s arguments that Russia is the aggressor.
Another fact is that this war has completely transformed the technology and tactics of warfare—the parties had to adapt to a new kind of war dominated by drones and missiles. Tank columns and troop concentrations are attacked by inexpensive drones as soon as they are detected—and they are detected very quickly. The warring parties had to undergo migration and learn this new art of warfare. The Russians, in particular, have done this successfully and now dominate the battlefield in a new way: through slow, efficient advances, because massed attacks produce only one thing—heavy casualties. Similar waves of technological advancement have occurred time and again. The machine gun, which was already in use before World War I but whose significance was underestimated at the time, brought an end to maneuver warfare as early as the first year of the war, when large columns of soldiers advanced toward the enemy and were wiped out. Toward the end of World War I, the tank brought some movement back to the front lines. However, comparing the frontline situation in Ukraine to that of World War I is a flawed analogy: Slow movements in small groups seem, so far, to be the only way to survive the drone barrage and maintain mobility.
Recently, Western media have been reporting that the Ukrainians have the upper hand in the war. However, this is fake news that has nothing to do with the reality on the ground. One must distinguish between the fighting on the front lines and NATO’s drone attacks in Russia. On the Donbass front, only a few fortified cities still stand in the Russians’ way; once those are taken, the Donbass will be liberated. Beyond that, there are no longer any fortifications worth taking seriously. Rather than going into details, I refer you to one of the best channels, Military Summary, which has been providing a twice-daily update on the situation at the front since the war began.
The West has not yet recognized the signs of the times. Its experts believe they will be successful in a war against Russia. However, they have not even defined their war aims in any way. Thus, they have no strategic plan against Russia other than to weaken it.
First and foremost, the Germans set the start of the war against Russia for 2030. However, it is now 2026, and the Germans apparently assume that, with Ukraine acting as their proxy, they can send drones and cruise missiles into Russia with impunity until 2030. Europe’s approach is, of course, coordinated with the US. The use of these weapons systems is not possible without American input. President Putin made this very clear a few days ago.
Many observers and experts both inside and outside Russia believe that President Putin will soon decide to launch a strike against targets in Europe—including those outside Ukraine.
There is a wide range of opinions on this topic. We have already published several articles on this subject: In “Will 1914 Repeat Itself? Will War Between Europe and Russia Finally Break Out?,” we also examined the Karaganov Doctrine, which advocates the use of nuclear weapons, and concluded that an attack is necessary, but not with nuclear weapons. Scott Ritter subsequently addressed the “Karaganov fallacy” and also spoke out clearly against the use of nuclear weapons.
Conclusion
In the Middle East, I see no realistic chance of ending the war, because that would mean, on the one hand, the withdrawal of American forces, and Israel would then be left alone as a small, genocidal aggressor. The Israelis are under pressure and are continuing their genocide in Gaza and Lebanon, paying no heed whatsoever to agreements between the US and Iran, because for Netanyahu personally, maintaining the war is the only way to survive politically.
In Russia, pressure is mounting on President Putin to adopt a more aggressive stance toward Europe, which is no longer even attempting to conceal its direct involvement in the war against Russia. Russia is intensifying its attacks on Ukraine, in part by destroying every gas station in eastern Ukraine to paralyze transportation logistics. Ground forces are making visible progress, and once the last fortified cities in the Donbas are liberated—which is likely to happen within the next few weeks—the path to the Dnieper will be clear.
President Putin is thus banking on a military solution in Ukraine and waiting for an energy crisis to unfold in Europe, where many flights are already being canceled under flimsy pretexts.
The concerted media coverage in the West claiming that the tide has turned in Ukraine finds not the slightest confirmation in the reality on the ground in Ukraine. The fuel shortage in Russia is also being exaggerated. In some regions, fuel is being rationed at gas stations. However, this is in no way sufficient to change Russia’s course of action.
Very occasionally, I have the opportunity to speak with someone who lives in Kyiv. According to this person, the situation is catastrophic, and over 90% of the population is against Zelensky. When I asked why the people weren’t rising up, the source replied that people were so intimidated by the terror of the security and intelligence services that the communication necessary for an uprising was impossible. Ukraine, which is portrayed by the West as a shining example of democracy, seems to be a time bomb whose ticking goes unheard out of fear.
My concerns that a war between Europe and Russia might break out—even though Europe has virtually no military power—have never been greater. President Putin will not be the one to take the first step toward a Third World War. Only he knows how much longer he will tolerate the West’s systematic provocations and how he will respond to them.
In 1943, the U.S. military was about to armor its bombers in exactly the wrong places. The analysts had examined every bomber that came back from combat, mapped the bullet holes across the airframe, and proposed reinforcing the spots where the holes clustered. The data was right there. You could see it on the planes.
They referred the question to the Statistical Research Group at Columbia University, a small team of mathematicians assembled for the war effort. The Hungarian-born statistician Abraham Wald examined the bullet-hole maps and gave the opposite recommendation. Armor the engines and the cockpit. The places where the returning planes had no bullet holes.
The military analysts had committed a logical error so simple they could not see it. They were studying the planes that came back. The planes shot through the engines and the cockpit did not come back. They had gone down across two oceans and the territory between them. The returning planes did not reveal where bombers were vulnerable. They revealed where bombers could be hit and still fly home.
The bullet holes on the survivors mapped survivable damage, not dangerous damage. Armoring where the holes were meant armoring the places that did not need armoring. The damage that mattered was on the planes you could not examine because they were destroyed.
Wald’s memorandum was classified. Decades later, when his work was declassified and republished, the principle he had identified came to be called survivorship bias.¹ ² It is the most pervasive and least understood logical error in any field that draws conclusions from a visible population of survivors.
The same error sits at the center of the modern screening-and-treatment industry.
The Error Generalized
Survivorship bias operates wherever a process selects what gets seen. The destroyed do not file reports, and the audience reads only what made it through.
Mutual fund performance averages exclude funds that closed. Hedge fund return statistics quietly drop the funds that liquidated. The historical returns of “the market” routinely omit bankruptcies, delistings, and total losses. Funds that lived publish their numbers; funds that died publish nothing. The retail investor reads the winners.
The literature on entrepreneurship was built the same way. CEOs who succeeded wrote memoirs about their habits and their early-morning routines. The thousands of equally disciplined founders who failed wrote nothing because their companies went under. The “success habits” identified by reading the survivors are, in many cases, just habits, shared by the dead and the living alike, with no causal relationship to outcomes.
In architecture, the buildings that survive are studied for their construction methods. The buildings that collapsed in storms, earthquakes, or fires are no longer there to be examined. Old buildings appear well-built because the badly-built ones are gone.
In each case, the visible sample is selected by the very property you are trying to measure. You cannot learn about plane vulnerability from intact planes. You cannot learn about cancer survival from cancer survivors.
Survivorship Bias in Medicine
A woman undergoes mammography in her early fifties. The scan finds a small lesion. She receives a biopsy, a lumpectomy, six weeks of radiation, and five years of tamoxifen. She is alive ten years later. She becomes an advocate, walking in Race for the Cure and telling her sister, her daughter, and the women in her neighborhood that screening saved her life. Get the test.
Her experience is real, her gratitude genuine. The conclusion she draws does not follow from either.
What she does not know, what she cannot know, is what would have happened to her without the screening, the biopsy, the surgery, the radiation, and the years of medication. She cannot run the counterfactual on herself. The version of her that did not get the treatment does not exist, and she has no way to consult it.
The institutions that promoted her screening have access to data she does not. Population-level data, accumulated across decades of randomized and observational studies, is consistent with four overlapping forms of survivorship bias, each of which inflates the apparent success of the system. Together they are sufficient to explain most of what the industry presents as the triumph of “early detection.”
Survivorship Bias Proper
The most direct form: only the living testify.
Eight months after her mastectomy, a woman dies of chemotherapy-induced sepsis. She does not appear at the October fundraiser. Six weeks after his prostatectomy, a man dies of cardiac complications. He writes no op-eds about prostate health. The radiation that “cured” the first cancer induces a second one five years later, and the patient’s family attends a funeral, not a marathon. The chemotherapy regimen that ostensibly drove the tumor into remission also drove the patient’s bone marrow into failure, and she dies of sepsis a year later, recorded by quiet bureaucratic convention as a “cancer death.”
When the public hears about cancer treatment, it hears from the patients who survived. Those who did not survive are statistically invisible. They are counted in mortality columns nobody reads, while their grateful surviving counterparts address the television cameras. The audience for screening campaigns sees a heavily filtered population, filtered by the treatments themselves.
The filtering goes further than visibility. It reaches into the mortality data itself. When a patient on chemotherapy dies of cardiotoxic heart failure, the death is typically coded as a cancer death. When a patient with treatment-induced bone marrow failure dies of sepsis, it is coded as a cancer death. When the surgical complication kills the patient on the operating table, it is generally coded as a cancer death. When the second cancer induced by radiation given for the first cancer kills the patient ten years later, the second cancer is frequently recorded as primary, the radiation that caused it noted in passing if at all. The coding conventions tilt systematically in one direction: failures of treatment are folded back into the column labeled “disease.” The treatment is shielded from blame. The cancer absorbs it. The mortality statistics that institutions cite to justify aggressive treatment are themselves an artifact of how treatment failures are recorded.
Lead-Time Bias
Finding a cancer earlier does not mean treating it earlier extends life. It means knowing about it longer.
Two women with identical lesions, identical biology, and identical eventual outcomes. Both die at age seventy. Woman A is screened at fifty, her cancer is detected, and she is “treated” for the next twenty years. Woman B is unscreened. She develops symptoms at sixty-five, is diagnosed, and dies at seventy.
The standard reporting metric is five-year survival from diagnosis. By that measure, Woman A counts at 100% survival. Woman B counts at 0%. The treatment looks miraculous. Nothing has actually changed. Both women died at seventy. Woman A simply spent twenty years as a patient.
The five-year survival statistic is the standard currency of cancer reporting. In the presence of widespread screening, it is also a metric that can rise to 100% without saving a single life. Between 1950 and 1995, the five-year survival rate for prostate cancer in the United States rose from 43% to 93%. The age-adjusted mortality rate from prostate cancer over the same period barely moved.³ The screened population learned about their cancer earlier. They did not die later.
When you read that “early detection” has improved five-year survival rates for breast, prostate, or thyroid cancer, you are reading a statistic structurally biased toward the appearance of benefit even when no benefit exists.³ ⁴
Length-Time Bias
Screening preferentially detects slow-growing lesions. Aggressive cancers grow rapidly between screening intervals and present symptomatically, not through the scan. Indolent lesions sit for years, available to be detected at the next mammogram or PSA test.
The population of cancers caught by screening is therefore enriched for slow biology, for lesions that were less likely to kill in the first place. Patients with these lesions tend to do well, not because the screening saved them but because their cancers were not going to kill them on any rapid timescale. The aggressive cancers, the ones that genuinely threaten life, frequently arise and progress in the gaps between scans.
Screening catches the cancers least in need of catching. The system then takes credit for the favorable outcomes of patients who would have done well regardless.
Overdiagnosis
The fourth and most powerful form. Many of the lesions detected by screening are not, in any meaningful sense, going to harm the patient. They are stable, non-progressive anatomical findings that medicine has chosen to label as cancer.
Bleyer and Welch, examining three decades of U.S. mammography data, estimated that 31% of breast cancers detected by screening represented overdiagnosis: disease that would never have produced symptoms or shortened life.⁵ The Cochrane systematic review of mammography trials concluded that for every life potentially saved by screening, ten women receive treatment for a cancer that would not have harmed them. The same review found no reduction in all-cause mortality from screening.⁶
In South Korea, the introduction of widespread thyroid ultrasound produced a fifteen-fold increase in thyroid cancer diagnoses over two decades. Mortality from thyroid cancer did not change. The country had not experienced a thyroid cancer epidemic. It had begun finding microscopic lesions that had always existed in the population, at autopsy in people who died of other causes, and that had never killed anyone before they were found and treated.⁷
Autopsy studies of men who died of unrelated causes have found prostate cancer cells in roughly a third of those in their forties, rising to two-thirds by their late sixties.¹⁵ The lifetime mortality from prostate cancer is approximately 3%. Most older men carry the disease into a natural death from something else; they die with prostate cancer, not from it. The PSA test cannot distinguish between the cancer that would have killed and the cancer that would have been silently carried into the grave. It detects both. It produces a diagnosis in both. The men with non-threatening lesions, who vastly outnumber the rest, are subjected to surgery, radiation, and hormonal therapy for a condition that was never going to harm them. They survive what was never threatening. They credit the system. They tell other men to get tested.
The ERSPC trial, the largest prostate cancer screening trial ever conducted, found that PSA screening reduced prostate cancer mortality by a small absolute amount over thirteen years. To prevent one death, approximately twenty-seven men had to be diagnosed and treated, most of whom would not have died from their disease and many of whom were rendered incontinent, impotent, or both by the intervention.⁸
Every overdiagnosed patient is, by definition, a successful “treatment outcome.” She survived a treatment for a condition that was never going to harm her. The system takes credit. She testifies on its behalf.
Why the System Selects for Evangelism
The four biases would matter less if the visible patients were a representative sample. They are not. The system that produces them also amplifies them.
Hospitals run survivor outreach programs. Pharmaceutical companies fund patient advocacy organizations. The pink ribbon ecology, Susan G. Komen, the National Breast Cancer Foundation, the dozens of subsidiary charities, operates almost entirely on survivor testimony. October fills American mailboxes with pink-ribboned testimonials. The American Cancer Society’s national publicity is built on survivor stories. The patient who survived is the asset.
The corporate machinery built around the survivor is substantial. Estée Lauder co-founded the pink ribbon symbol with Self magazine in 1992 and now sells pink-ribbon cosmetics each October. The National Football League runs an annual “Crucial Catch” campaign with players wearing pink cleats and accessories. Major League Baseball stages pink-bat games on Mother’s Day. Yoplait produced pink-lidded yogurt for two decades under the “Save Lids to Save Lives” campaign. Ford sold pink-ribbon merchandise through “Warriors in Pink.” General Mills, KitchenAid, the National Hockey League, the airlines, the cosmetics counters at every major department store all participate. The advertising spend on these campaigns runs into hundreds of millions of dollars annually, dwarfing the portion of the proceeds that ever reaches research and dwarfing many times over the portion of research funding that addresses environmental causes of breast cancer rather than treatment. The campaigns sell screening. The screening produces patients. Most patients survive, because most of what is found in screening was not going to kill them, and they testify. The testimony funds the next round of campaigns.
The patient who died is, from a marketing perspective, a problem. Her death cannot be celebrated. Her family is often grieving and angry. Her doctors generally do not call the local newspaper. She becomes a statistic in a column nobody reads, while the surviving patient in the next room becomes the face of the cause.
This selection is not a conspiracy. It is a structural feature of how the industry communicates. Living patients can be photographed; dead patients cannot. The living speak at events; the dead are credited, by quiet convention, to “the disease.”
The grateful survivor is also psychologically necessary for the treatment to continue being offered in its current form. The patient who has undergone radical mastectomy, six rounds of chemotherapy, weeks of radiation, and years of endocrine therapy must believe, on pain of intolerable cognitive dissonance, that this was necessary and life-saving. To accept that she may have been treated for a lesion that would not have harmed her, that she lost her breast, her hair, her fertility, her cardiac reserve, perhaps her marriage, to a system that misjudged the threat, is psychologically devastating. The mind protects itself. She becomes an advocate.
The advocate then promotes the system to other women, who undergo screening, get diagnosed, get treated, and become advocates in turn. Each cycle generates more survivors, each of whom credits the system that produced them. The dead and the harmed are silent by definition.
The financial scale of this ecosystem is not small. The United States spends roughly two hundred billion dollars annually on cancer-related medical care. Mammography alone is a multi-billion-dollar industry. The PSA test, despite repeated expert task force recommendations against routine screening, generates billions in downstream procedures. The pink ribbon charities raise hundreds of millions per year, much of which goes to “awareness,” that is, to producing more screening, more diagnoses, more treatment, and more survivors. The asset class, the patient, is manufactured by the process that then takes credit for her survival.
In 2018, a Goldman Sachs equity research report posed the question explicitly to its biotechnology clients: “Is curing patients a sustainable business model?”⁹ The analysts noted that one-time cures undermine recurring revenue streams. The pharmaceutical industry’s most profitable customers are chronic patients, not cured ones. The screening-and-treatment cancer model is, from a financial perspective, an excellent business. It produces patients. It treats them for years. Many of them survive, which is what the model needs them to do, because survivors testify and dead patients do not.
Inside the Testimonial
The cancer survivor has four pieces of information. She was screened. Something was found. She received treatment. She is alive years later. From these facts, she draws a single conclusion: the screening and treatment saved her life.
The inference is intuitive but unsupported. The same four facts admit at least three other explanations.
The screening detected a lesion that would never have harmed her. She survived not because of the treatment but in spite of it. The treatment did damage that she absorbed because the rest of her body was healthy enough to recover.
The lesion was real but slow-growing. She would have lived equally long, with less suffering, by doing nothing.
The lesion was real and biologically active, but her body’s repair mechanisms, what the establishment calls her constitution and what terrain medicine recognizes as her terrain, would have managed it. The treatment was incidental to her survival.
She cannot distinguish between these explanations from her own experience. None of them is available to her introspectively. The only way to determine which is correct, at the level of a population, is the randomized controlled trial, the kind of trial that, in most screening contexts, has either not been done with adequate follow-up or has produced equivocal results that the institutions promoting screening do not publicize.
Her testimonial is sincere. It is also, with respect to the question of whether the treatment worked, evidence of nothing in particular. The dead woman two beds down the hall, who received identical screening and identical treatment and died of cardiotoxic chemotherapy, would have a different testimonial if she could give one. The system that asks the survivor to speak does not ask the dead woman’s family to speak. The asymmetry produces the appearance of a treatment success rate the underlying data does not support.
What Survives the Error
Once you see survivorship bias, you cannot unsee it. What remains is not paranoia but a discipline: asking, in every medical context, which population you are looking at and which population is missing.
When a screening campaign reports that “five-year survival rates have improved,” ask whether overall mortality has changed. Five-year survival can rise to 100% without saving a single life if all the increase comes from earlier detection of lesions that were going to be survived anyway. Overall mortality, deaths per hundred thousand population per year, is much harder to manipulate. It is also the only figure that answers the question the survival rate appears to answer.
A cancer survivor telling you her treatment saved her life can be sincere and still wrong about causation. The conviction is real. The causal claim it carries is not derived from anything she has direct access to. You can be glad she is alive without accepting her account of why.
An oncology center’s published survivor outcomes report a filtered population. Ask about the patients who did not complete treatment. Ask about the patients who died of treatment-related complications and were classified as cancer deaths. Ask about the patients whose follow-up was lost because they moved into hospice care or stopped responding to calls. The shape of the population that gets reported is the shape of the population that survived long enough to be counted.
Facing a screening recommendation yourself, the question to ask is the one the military analysts in 1943 did not ask: what does this examination fail to show me? The bullet holes on the surviving bombers concealed the bullet holes on the destroyed ones. The success stories of the screening industry conceal the women treated for lesions they did not have, the men rendered impotent by surgery for cancers that would never have grown, the second cancers induced by the radiation, and the patients whose treatments killed them and who are now counted, by quiet bureaucratic convention, as having died from their disease.
The full investigative case on these screenings, what they detect, what they miss, what they manufacture, and what they cost, has been documented at length in earlier work.¹⁰ ¹¹ ¹² ¹³ ¹⁴
What the Trials Actually Show
Defenders of mammography routinely cite two trials. The Health Insurance Plan of New York trial, begun in 1963, and the Swedish Two-County Trial, conducted between 1977 and 1985, both reported reductions in breast cancer mortality among screened women. Both have been criticized on methodological grounds. The HIP trial’s randomization was uneven, with baseline differences between arms and exclusion rules applied asymmetrically. The Two-County Trial used cluster randomization that did not consistently balance comparison groups and lacked blinded cause-of-death assessment. Its mortality estimates shifted across successive reanalyses. The Cochrane systematic review of mammography trials classified both as carrying significant risk of bias.⁶
The most rigorously conducted breast cancer screening trial, the Canadian National Breast Screening Study, followed nearly ninety thousand women for twenty-five years. It found no reduction in breast cancer mortality from mammography screening, and no reduction in all-cause mortality.¹⁶
All-cause mortality is the figure that resists the gaming. When a study reports that breast cancer deaths fell among screened women but all-cause deaths did not, the women who avoided a death coded as breast cancer died of something else within the same window: heart failure from chemotherapy-induced cardiotoxicity, second cancers induced by the radiation given for the first, complications from the surgery, strokes after years of endocrine therapy. The Cochrane review and meta-analyses across multiple cancers have repeatedly found that all-cause mortality is essentially identical in screened and unscreened populations. The treatment that prevents one death produces another. The cancer-specific column improves; the death column does not. Survivorship bias gives the illusion of a saved life. All-cause mortality data shows that the life, where treatment did anything at all, was traded rather than added.
The Bombers and the Patients
Abraham Wald died in 1950 in a plane crash in the Nilgiri mountains of southern India. The principle he identified outlived him by three-quarters of a century and now sits, unrecognized by the institutions that depend on it, at the center of the modern medical industry.
The bombers that came back showed where a bomber could be shot and still come back. They did not show where a bomber was vulnerable. The cancer survivors who give interviews, walk in fundraisers, and tell their friends to get screened show where the modern oncology machine is not lethal. They do not show where it works.
The patients who died of their treatments are not at the marathon. The patients treated for lesions that would never have killed them have no way to know they were never in danger. The patients whose cancers were going to be survived regardless have no way to credit their own bodies rather than the chemicals introduced into them. They are the bullet holes on the wings: survivable damage, mapped and celebrated, while the damage that mattered remains invisible because the people who suffered it are no longer in the room.
Wald told the military to armor the engines and the cockpit, the places the surviving planes were not hit. The same instruction applies to medicine: look at what the survivors do not show you. The damage that matters is on the planes that did not come back, and on the patients who can no longer testify.
How to Explain This to a Six-Year-Old
Imagine all your friends drink a magic potion that’s supposed to keep them safe. Half of them disappear. The other half come back and tell you the potion worked great.
If you only listen to the friends who came back, you’ll be sure the potion is wonderful. You’ll tell other kids to drink it too.
But the other half are gone. They can’t tell you whether the potion hurt them. You don’t know whether the potion saved the friends who came back, or whether those friends would have been fine without ever drinking it.
When a cancer survivor tells you the treatment saved her life, listen to her kindly. But remember the friends who disappeared. They are part of the story too.
Quick Reference: The Four Biases
Survivorship bias. Only the living testify. Cancer patients who died of their treatments do not give interviews. The visible patient population is filtered by the treatments themselves.
Lead-time bias. Finding a cancer earlier does not extend life. It extends the time you know about it. Five-year survival rates can rise to 100% without saving a single life.
Length-time bias. Screening preferentially catches slow-growing lesions that were less likely to kill in the first place. Aggressive cancers arise and progress between scans, often undetected until they present symptomatically.
Overdiagnosis. Many screen-detected lesions would never have caused harm. The patient is treated for something that was not a threat, survives easily, and credits the treatment.
References
Mangel, M., & Samaniego, F. J. (1984). Abraham Wald’s work on aircraft survivability. Journal of the American Statistical Association, 79(386), 259–267.
Wald, A. (1943). A Method of Estimating Plane Vulnerability Based on Damage of Survivors. Statistical Research Group, Columbia University. (Declassified and republished by the Center for Naval Analyses, 1980.)
Welch, H. G., Schwartz, L. M., & Woloshin, S. (2000). Are increasing 5-year survival rates evidence of success against cancer? JAMA, 283(22), 2975–2978.
Welch, H. G., & Black, W. C. (2010). Overdiagnosis in cancer. Journal of the National Cancer Institute, 102(9), 605–613.
Bleyer, A., & Welch, H. G. (2012). Effect of three decades of screening mammography on breast-cancer incidence. New England Journal of Medicine, 367(21), 1998–2005.
Gøtzsche, P. C., & Jørgensen, K. J. (2013). Screening for breast cancer with mammography. Cochrane Database of Systematic Reviews, Issue 6, CD001877.
Vaccarella, S., Franceschi, S., Bray, F., Wild, C. P., Plummer, M., & Dal Maso, L. (2016). Worldwide thyroid-cancer epidemic? The increasing impact of overdiagnosis. New England Journal of Medicine, 375(7), 614–617.
Schröder, F. H., et al. (2014). Screening and prostate-cancer mortality in a randomized European study: results of the ERSPC at 13 years of follow-up. The Lancet, 384(9959), 2027–2035.
Richter, S., et al. (2018). The Genome Revolution (biotechnology equity research report). Goldman Sachs Global Investment Research, April 10, 2018.
Unbekoming. The 12 Screenings That Manufacture the Patients They Claim to Find.
Unbekoming. The Screening Trap.
Unbekoming. Breast Cancer: What They Didn’t Tell You.
Unbekoming. The PSA Trap: How a Flawed Test Built a Billion-Dollar Industry and Destroyed Millions of Men.
Unbekoming. The Unbekoming Cancer Compendium.
Sakr, W. A., Grignon, D. J., Crissman, J. D., Heilbrun, L. K., Cassin, B. J., Pontes, J. J., & Haas, G. P. (1994). High grade prostatic intraepithelial neoplasia (HGPIN) and prostatic adenocarcinoma between the ages of 20-69: an autopsy study of 249 cases. In Vivo, 8(3), 439–443.
Miller, A. B., Wall, C., Baines, C. J., Sun, P., To, T., & Narod, S. A. (2014). Twenty five year follow-up for breast cancer incidence and mortality of the Canadian National Breast Screening Study: randomised screening trial. BMJ, 348, g366.
The book, also available on Amazon documents “systemized medical abuse” that accelerated during the COVID-19 pandemic.
Chapter 1. From Quackery To Criminality
The medicinal use of mercury offers a long-running example of medically induced harm. Although centuries of whistleblowers have warned that dosing patients with it constitutes reckless quackery—and the U.S. government presently places mercury at number three on its “Substance Priority List,” right under arsenic and lead—the heavy metal has figured prominently in the “medical armamentarium” from as far back as the sixth century BC through the present day.
In his important book Evidence of Harm, author David Kirby exposed the pharmaceutical industry’s controversial practice of including mercury preservatives in vaccines. Pointedly using the word “criminal,” Kirby wrote in the foreword to another book about mercury (The Age of Autism by Dan Olmsted and Mark Blaxill) that the “blind belief in a known poison” has been “misguided, immoral, and in some cases, patently criminal.”
The “Messianic” Benjamin Rush
In many ways, the medical practices and beliefs of U.S. Founding Father, physician, and University of Pennsylvania medical school professor Benjamin Rush may have set the stage for modern medicine’s stubborn adherence to dangerous protocols—despite clinical evidence of harm—and its silver-bullet fascination with vaccines “as substitutes for right living,” as Eleanor McBean put it in her 1957 book The Poisoned Needle: Suppressed Facts About Vaccination.
The reportedly “messianic” and “uncompromising” Rush’s late-1700s stock-in-trade was a radical protocol involving bloodletting and purging with—what else?—mercury, a practice that medical historians later dubbed “heroic medicine.” Rush had his own proprietary brand of laxative called “Thunderclappers,” consisting of approximately 60% mercury chloride (also called calomel), which he promoted as “a purgative of explosive power.” As Rush honed his clinical methods, he passed them on to a phalanx of enthusiastic students and disciples during yellow fever epidemics in Philadelphia, where he would bleed and purge up to 100 patients a day. Although use of calomel was not uncommon among doctors of that era, Rush prescribed up to 10 times more than his medical peers and also recommended the removal of huge amounts of patients’ blood, erroneously believing that the blood would replenish itself in a matter of a day or two. “A patient’s failure to respond to this disastrous therapy,” one historian wrote in 2004, “won [the patient] only another round of bleeding and purging.” In another modern writer’s colorful description, “So much blood was spilled in the front yard that the site became malodorous and buzzed with flies.”
No less a figure than George Washington underwent a rapid and gruesome death after Rush protégé Dr. Elisha Dick (and two other Johnny on-the-spot physicians) poisoned Washington with mercury and removed 40% of the beleaguered general’s total blood volume—a quantity that, to this day, “continues to amaze and appall laymen and physicians alike.” From many historians’ point of view, Washington’s doctors caused his death, a death that may well have changed the course of history.
Rush was enthusiastic about promoting his “heroic medicine” protocol, “proclaim[ing] the success of his cure to the public and his medical colleagues” in newspapers, advertisements, and brochures, and even “harangu[ing] people in the streets.” In addition, he was an early and explicit proponent of smallpox vaccination. In 1803, he joined with 30 other Philadelphia doctors in signing a public notice “expressing their confidence in vaccination and recommending it for general use.” Significantly, smallpox vaccination represented a turning point in the “medicalization of the general public” in both early nineteenth-century America and Europe, and a boon for the burgeoning medical profession:
Since the late eighteenth century, doctors had intensified their efforts to win government support for their plans to bring the whole population under medical control. . . . Thus Jenner’s method of cowpox vaccination presented medical practitioners with a new chance to increase their prestige and influence on public health affairs [bold added]. Doctors also foresaw an increase in their income through vaccination fees and hoped to establish themselves, with the help of the vaccine, among those classes of the population who had not consulted doctors before.
From 1813 to 1822, the young U.S. government appointed James Smith as the nation’s “federal vaccine agent,” charging him with “maintaining a supply of the smallpox vaccine and distributing it nationwide”; Smith had been a student of Rush’s at the University of Pennsylvania and was a fellow member of the “well-educated medical elite.” Although other physicians of the day argued that smallpox vaccination was both dangerous and ineffective, then—as now—defenders of the practice prevailed by using “more or less perverted statistics,” with one doctor urging his “professional brethren to be slow to publish fatal cases of small-pox after vaccination” and others passing off vaccine-induced fatalities as some other disease.
Reflecting on Rush’s medical legacy, U.S. Army medical officer P.M. Ashburn made remarks in 1929 that highlight one of the many reasons why Rush’s cautionary tale is still pertinent today. Ashburn wrote that by virtue of Rush’s “social and professional prominence, his position as teacher and his facile pen,” the Philadelphia physician “was more potent in propagation and long perpetuation of medical errors than any man of his day,” thereby “blacken[ing] the record of medicine.” This observation illustrates how social prestige—coupled with “unyielding devotion to dogma”—often helps practitioners of dangerous medicine beat back their critics.
In Rush’s time, those critics included fellow physician Elisha Barlett, who opined about Rush’s medical theories, “In the whole vast compass of medical literature, there cannot be found an equal number of pages containing a greater amount of utter nonsense and unqualified absurdities,” as well as feisty British journalist and pamphleteer William Cobbett, who dared to publish tracts asserting that Rush’s yellow fever treatments were both ineffective and dangerous—and “a perversion of nature’s healing powers.” In response, Rush sued Cobbett for libel and won, in “one of the largest libel awards in American history at the time.”
One of Cobbett’s fascinating observations—which reverberates uncannily in the COVID era—was that extreme fear (in this instance, of yellow fever) made members of the public far more willing to subject themselves to Rush’s “experiments” than they otherwise might have been. Cobbett wrote:
[Rush] seized, with uncommon alacrity and address, the occasion presented by the Yellow Fever, the fearful ravages of which were peculiarly calculated to dispose the minds of the panick-struck people to the tolerance, and even to the admiration, of experiments, which, at any other time, they would have rejected with disdain.
Interestingly, after Rush’s libel victory, Cobbett exacted a modicum of revenge by assembling data from municipal records (acknowledged today as “an epidemiological tour de force”), which pointed to a 56% mortality rate among Rush’s yellow fever patients that contrasted starkly with the physician’s own claim of a greater than 90% survival rate. When word of those dismal statistics got out to the public, Rush’s medical practice suffered. Undaunted, Rush went on to become Treasurer of the U.S. Mint under President John Adams. As the author of America’s first psychiatric textbook, he is also revered today as “the father of American psychiatry.” Rush proposed the same general treatments for madness that he favored for physical ailments, supplemented by straitjackets and other “modes of punishments” for tough cases.
For his part, in 1800, a disgusted Cobbett returned to London, where he continued to hold medicine’s feet to the fire, including condemning smallpox vaccination as “quackery.”
A “Patently Criminal” Model
Some modern medical historians are willing to go so far as to characterize medicine, in periods and places like 18th-century America, as “deplorable,” and to suggest that back then, “a doctor was just as likely to kill you as save you.” Most, however, frame medical barbarity as a thing of the past. Shielded by high-end machines, complex drug technologies, glossy scientific publications, and lingo like “rigorous” and “evidence-based,” the current medical-pharmaceutical-regulatory establishment and its hagiographers would have the public believe that “safe and effective” now rules the day.
There is ample evidence to show that pledges of safety often are either disingenuous or false, and there are indications that Kirby’s description of the medical model as sometimes “patently criminal” was squarely on the mark. At the level of individual medical practitioners, law firms specialized in malpractice note that if a doctor “appears to be indifferent to patients’ well-being or safety,” that indifference can be grounds for criminal liability. A search of the word “criminal” on the website of Medpage Today (a conventional news service that is generally protective of medicine’s reputation) brings up countless articles about doctors and other health care providers running “pill mill” operations, carrying out fraud, taking kickbacks, tampering with drugs, faking data, sexually assaulting or abusing patients, and engaging in other types of “unprofessional” and unethical conduct. The site’s “Investigative Roundups” feature stories (often formulated as questions to soften the impact) with titles like “Columbia protected predator doc?”, “Psychiatrist held patients against their will?”, “$15K surgery shakedown?” or “Doc pushed unneeded surgery?” Other Medpage Today headlines flamboyantly bandy about words like “deadly,” “loophole,” “games,” “tactics,” “unethical,” and “secretive.”
Sometimes, individuals who defend the medical status quo blame whichever reports of misbehavior manage to surface (many do not) on “a few bad apples.” Others, such as Harvard scientist and patient safety advocate Lucian Leape, do the reverse, shifting the blame from “bad people” to nebulous “bad systems;” Leape suggests that a cycle of disrespect is “learned, tolerated, and reinforced in the hierarchical hospital culture.” The fact is, however, that medical harms flow from both individuals and institutions. Most health care providers operate in broader organizational and corporate contexts—and it is policymakers and decision-makers at those levels who often give medical-pharmaceutical corruption and criminality a green light. This is illustrated by the phenomenon (for which there is even an academic field of study) called “clinicide,” defined as serial medical killers responsible for “the unnatural death of multiple patients in the course of treatment;” not infrequently, the killers’ host institutions countenance or “enable” this clinicide by choosing to ignore red flags.
As an extension of the “bad apples” argument, some upholders of the status quo point to the fines that the U.S. Department of Justice (DOJ) routinely levies on hospitals and pharmaceutical corporations, suggesting that these are an adequate mechanism to catch and punish players engaged in malfeasance. However, given that medical-pharmaceutical culprits not infrequently are criminal recidivists and that the fines generally amount to “little more than a slap on the wrist,” it is fair to ask “whether such a monetary punitive system really does much to prevent bad behavior.”
Moreover, DOJ rarely prosecutes or holds corporate leaders accountable, despite having a “powerful legal tool” at its disposal to go after the executives at the helm of medical misconduct; it has done so only 13 times since the year 2000. Instead, many signs point to a wink-and-a-nod sub rosa understanding between the various parties, with the penalties doing nothing to prevent future harms but instead furnishing a generous flow of kickbacks that prosecutors and regulators can funnel into various sectors of the federal budget (see Illegal But Profitable). In fact, under the False Claims Act, the U.S. Department of Health and Human Services (HHS) gets a 20 to 1 return on every dollar it “invest[s] in prosecutions and investigations.”
To our knowledge, a parent company has never been excluded from participation in Medicare and Medicaid for illegal activities, which endanger the public health and deplete taxpayer-funded programs. Criminal prosecutions of executives leading companies engaged in these illegal activities have been extremely rare. Much larger penalties and successful prosecutions of company executives that oversee systemic fraud, including jail sentences if appropriate, are necessary to deter future unlawful behavior. Otherwise, these illegal but profitable activities will continue to be part of companies’ business model.
Iatrogenocide Takes Center Stage
Even before COVID, available data indicated that 20th- and 21st-century Western medicine had failed to improve health in any meaningful way, instead trading off the industrial-age diseases of yore for modern chronic disease epidemics, many or most with iatrogenic causes or contributors. Unfortunately, recent events suggest that medicine—forging an unhealthy partnership with government—may now be more dangerous than it has ever been.
Until 2020, the Americans who were most concerned about medical risks and medical criminality belonged to groups already adversely affected, such as those injured by vaccines or opioids. However, with the advent of life-threatening COVID “countermeasures” and lethal protocols in U.S. hospitals and in other countries such as the UK, medical pharmaceutical gangsterism—seemingly occurring with government cognizance—has begun attracting more widespread notice. When governments began parlaying the dubious health “emergency” into an excuse to authorize and mandate the COVID vaccines and boosters—and proceeded full tilt even when unprecedented injuries and deaths immediately began piling up—some segments of the public saw the contours of an officially sanctioned medical crime.
As Holocaust survivor and human rights activist Vera Sharav communicated in her docuseries Never Again Is Now Global, medical coercion and the suspension of constitutional freedoms have never led anywhere good. Unfortunately, history shows that governments intent on “state repression, brutality and genocide” can usually count on the readiness of some doctors to serve as accomplices, even if their complicity has the potential to turn them into “mass murderers on an exponential scale.”
On November 14, 1986, Ronald Reagan signed the National Childhood Vaccine Injury Act into law.¹ The legislation ended more than a decade of tort litigation against vaccine manufacturers by transferring civil liability for injury and death from the companies producing the products to the American taxpayer. The pharmaceutical industry had threatened to leave the childhood vaccine market. Reagan’s signature ensured they would stay, at a price paid by parents who would never be told what had been arranged on their behalf.
Twenty-five years later, in Bruesewitz v. Wyeth, the Supreme Court closed the last remaining exit. The 2011 decision, written by Justice Antonin Scalia, held that federal law preempts all design-defect claims against vaccine manufacturers in state courts.² Justice Sotomayor’s dissent, joined by Justice Ginsburg, identified the practical effect: no federal agency, no state court, no jury of citizens would henceforth ensure that vaccine manufacturers accounted for scientific advances when designing their products. The manufacturers had been placed outside the accountability structure that governs every other industry in the United States.
The 1986 Act and the 2011 ruling together defined the shape of what now exists. Every function of the vaccine program — licensing, recommendation, purchase, safety monitoring, patent holding, research funding, injury adjudication, and courtroom defense — resides in the federal government. When the products kill a child, the state prosecutes the parents.
Leslie Manookian, founder of the Health Freedom Defense Fund, mapped this architecture in a twelve-point summary published to her readers.³ What follows walks through the machine she described, in five stages. Each stage encloses the next. By the fifth, the shape of the trap around the American parent becomes fully visible.
1. The License
The Food and Drug Administration licenses vaccines on the basis of clinical trials that do not use inert placebo controls. This fact is documented in the FDA’s own package inserts and in sworn testimony by the industry’s most senior figures.
In January 2018, attorney Aaron Siri deposed Dr. Stanley Plotkin in New Hope, Pennsylvania — the vaccinologist widely regarded as the industry’s founding figure and co-editor of the standard reference textbook Plotkin’s Vaccines.⁴ Under oath, Siri walked Plotkin through the pre-licensure clinical trials for each product on the recommended childhood schedule. The pattern that emerged was uniform.
The safety review period following each dose was 48 hours for the IPOL polio vaccine. 48 hours for ActHIB. Four days for Engerix-B, the hepatitis B vaccine administered to newborns on their first day of life. Five days for Recombivax HB, the other hepatitis B product. Siri produced, for comparison, the package insert for Enbrel — a drug given to adults with rheumatoid arthritis — and asked Plotkin to confirm that its pre-licensure clinical trials monitored patients for up to 80 months. Plotkin confirmed. A drug given to sick adults was studied for six and a half years. Vaccines given to healthy newborns were studied for 48 hours to five days.
Plotkin then confirmed, product by product, that these trials had no saline placebo control group. Not Recombivax HB. Not Engerix-B. Not IPOL, whose trial subjects received the polio vaccine concurrently with DTP, making it impossible to attribute any reaction to either product. Not ActHIB. The MMR II vaccine, which Plotkin himself was present for the licensure of, had, in his own words, no control group “for the studies that I’m recalling.” When the Hiberix Hib vaccine was later licensed, the manufacturer used ActHIB itself as the “placebo” — testing one Hib vaccine against another.
On the necessity of a saline control, Plotkin was direct: “Without a control group, if you’re looking for a phenomenon occurring in the vaccine group, you cannot judge that phenomenon without having a control group.” That is the industry’s founding figure, testifying under oath, describing the epistemic condition of the products his industry markets.
The pattern in the trials produces a specific consequence. When a new vaccine is tested against an existing licensed vaccine as its control, any injury rate common to both groups becomes invisible. The comparison measures relative difference, not absolute harm. If the existing vaccine produces seizures at a rate of 1 in 500, and the new vaccine produces seizures at a rate of 1 in 500, the trial reports no significant difference — and both products remain on the market.
The Gardasil trial illustrates what happens when a saline group is included but the result is inconvenient. Merck’s pre-licensure clinical trial for its HPV vaccine assigned 9,412 subjects to a “placebo” arm. Of these, only 594 received actual saline. The remaining approximately 8,800 received AAHS — the aluminum-containing adjuvant used in the Gardasil formulation itself. Merck reported the two groups combined, showing 2.3% of the “placebo” arm developing what the trial recorded as systemic autoimmune events, matched by 2.3% in the Gardasil arm. The vaccine was declared safe on the strength of no difference.
Siri produced the underlying trial data. Broken out separately, the saline placebo group of 594 girls and women showed zero such events. The aluminum group showed approximately 2.5%. Merck had recorded the difference and reported the combination.
Plotkin was asked why the two groups had been combined for that analysis when they were broken out separately for local reaction analysis on the preceding pages. His response, verbatim: “So going into the study, they just assumed aluminum wouldn’t cause autoimmunity and so that’s how they proceed in designing it.” A pre-licensure trial for a product administered to schoolgirls declared the vaccine safe by defining the aluminum adjuvant as inert, then combining subjects receiving that adjuvant with subjects receiving nothing.
Once a vaccine reaches the schedule, the failure to test it against saline becomes permanent. For each product Siri walked Plotkin through, he asked whether a proper placebo-controlled study could now be conducted. Plotkin confirmed, product by product, that it could not — running such a trial would be “unethical” in children whose vaccines are already recommended. The absence of a control group at the point of licensure becomes the reason no control group can ever be introduced. The regulatory record is locked at the point of the initial deception.
When a Freedom of Information Act request submitted by the Informed Consent Action Network in 2018 asked the Department of Health and Human Services to produce the biennial vaccine safety reports required by Section 300aa-27 of the 1986 Act, HHS was forced to respond that it had not produced a single such report in the thirty-two years since Reagan signed the law.⁵ The statutory obligation to review safety had been ignored for the entire life of the program.
The FDA license then triggers the second function. The Centers for Disease Control and Prevention convenes the Advisory Committee on Immunization Practices, which votes on whether to add the newly licensed vaccine to the recommended childhood schedule. ACIP members are drawn from the same institutional networks that developed and defended the products. Once added, the vaccine appears on the schedule that is distributed to every state health department in the country. The recommendation is not a mandate. It becomes one at the next stage.
Under oath in the same deposition, Plotkin acknowledged that he had served as medical and scientific director of Sanofi Pasteur in the 1990s, that he operated a personal consulting entity called Vaxconsult, and that he had received payments over the preceding two decades from Merck, GSK, Pfizer, Sanofi, and, in his own phrasing, “essentially all of the major manufacturers.” He had also consulted for the FDA. The industry’s founding figure had confirmed the case against the products his industry markets. He was also paid by every major manufacturer of those products.
The federal government does not directly mandate childhood vaccines. That function is delegated to the states.
Every state in the union has passed legislation requiring specified vaccines for school attendance. The specific list varies. The mechanism is uniform. Parents who wish to enroll their children in public school — and in many states private school — must produce documentation that their children have received the vaccines on the state’s list. The state list is drawn from the CDC schedule; the CDC schedule from the ACIP recommendation; the ACIP recommendation from the FDA license. The FDA license rests on trials that were never controlled against a genuine placebo.
The chain is complete before the parent enters the pediatrician’s office.
Under the Vaccines for Children program, established in 1993, the federal government purchases half of all childhood vaccines administered in the United States. Recent VFC spending has exceeded $5 billion annually.⁶ The federal government is the largest single purchaser of the products it licenses, the products it recommends, and the products the states mandate.
This creates a market structure without parallel elsewhere in American pharmaceutical policy. The maker of a blood pressure medication faces market discipline. Doctors may prescribe it or not, patients may fill the prescription or not, insurance may cover it or not. The maker of a childhood vaccine faces no equivalent constraint. The state compels administration; the federal government guarantees a buyer; demand is legislated. Revenue is secured before a single dose is delivered.
The mandate has hardened as it has aged. Every state at some point permitted medical, religious, and in some cases philosophical exemptions from the vaccine schedule. Over the past decade, state legislatures have moved to close them. California eliminated its personal belief exemption in 2015 through SB 277 following the Disneyland measles cluster. In 2019, New York eliminated its religious exemption; Maine followed the same year. Connecticut eliminated its religious exemption in 2021. The pattern has been consistent: a highly publicised incident, a legislative response drafted with industry input, and the removal of the exit ramp. The federal government does not need to mandate. The state legislatures have been prevailed upon to do it, and to progressively narrow the terms under which the mandate can be refused.
Leslie Manookian, in the interview she gave me,¹⁹ described the shape of what has been built here. “When we succeed and thrive outside the extant medical paradigm, we pose an existential threat to the medical complex which is why the main actors fight our information, experiences, and independence so fervently.” The compelled purchase is what makes the mandate machinery operate. Without it, the products would compete on their merits. With it, they do not compete at all.
The 1986 Act shielded manufacturers from every category of liability that governs other industries. The immunity covered injuries caused by design choices themselves — the composition of the product, the adjuvants used, the decisions about testing. A safer alternative product could exist and the manufacturer could refuse to adopt it, and the injured child’s family could not sue.
Justice Scalia’s opinion in Bruesewitz addressed a case brought by Robalee Bruesewitz on behalf of her daughter Hannah, who had suffered residual seizure disorder and developmental delay after receiving the DPT vaccine manufactured by Wyeth. The Bruesewitz family had exhausted the Vaccine Injury Compensation Program. They then attempted to sue Wyeth in state court, arguing that a safer alternative vaccine design existed and Wyeth had refused to adopt it. The Supreme Court held that federal law preempts such claims. The manufacturer’s choice to continue producing a design that injured children could not be litigated.
Sotomayor’s dissent identified the consequence. Vaccine manufacturers now occupy a regulatory space in which no external mechanism — regulatory agency, court, or jury — holds them accountable for design decisions. This is not an inference. It is a description of the legal structure the majority created.
Behind the shield sits a further conflict. The Department of Health and Human Services — the parent agency of the FDA, the CDC, the National Institutes of Health, and the Health Resources and Services Administration that runs the injury compensation program — holds patents on multiple childhood vaccines. HHS scientists Douglas Lowy and John Schiller developed the recombinant protein technology underlying Merck’s Gardasil and receive royalties on its sale.⁷ Similar patent and royalty arrangements extend to other products in the childhood schedule. The regulator collects revenue on the products it approves.
The research infrastructure that would produce independent safety findings is subject to a parallel capture. Studies funded by the CDC, the NIH, or by the manufacturers themselves consistently produce findings favorable to the schedule. The vaccinated-versus-unvaccinated comparison studies that would settle the fundamental question about long-term outcomes have not been funded. When independent researchers attempt them — Anthony Mawson’s 2017 study of homeschooled populations,⁸ Paul Thomas’s cohort analysis of his own pediatric practice⁹ — the results are attacked, retracted, or ignored, and the researchers face professional consequences.
The capture extends inside the agencies themselves. In August 2014, Dr. William Thompson, a senior epidemiologist at the CDC and co-author of the 2004 DeStefano study widely cited to reject any link between the MMR product and neurodevelopmental injury, submitted a statement through his attorney acknowledging that he and his co-authors had “omitted statistically significant information” from the published paper and had disposed of documents to conceal the omission.¹⁰ The withheld data showed an elevated risk of neurodevelopmental injury among African American boys who received the injection before thirty-six months of age. Thompson’s disclosure was made under whistleblower protection. Congress has never subpoenaed him to testify. The DeStefano paper remains uncorrected.
Merck faced a parallel qui tam action from two of its own virologists, Stephen Krahling and Joan Wlochowski, who alleged in a federal filing that Merck had falsified mumps vaccine efficacy data submitted to the FDA over the course of a decade.¹¹ The case, filed in 2010, moved slowly through the courts. The Department of Justice declined to intervene. Merck retained its exclusive contract to supply mumps vaccine to the U.S. government. The plaintiffs’ allegations of test manipulation entered the public record and produced no regulatory action.
The shield is a network. Liability preemption from Congress protects the manufacturer. Patent revenue aligns the regulator with the products it approves. Captured research funding directs the studies that might identify harm away from the questions that would find it. Judicial preemption then blocks any citizen who attempts to litigate the design decisions the products embody. Each layer supports the others. The whole structure is invisible to the parent standing in a pediatrician’s office being told the shot is safe.
The Centers for Disease Control and Prevention operates the Vaccine Adverse Event Reporting System. It also runs the promotional campaigns that place vaccination on the pediatric schedule. The agency responsible for detecting harm from the products is the same agency responsible for driving their uptake.
The conflict is not theoretical. Harvard Pilgrim Health Care, under a grant from the Agency for Healthcare Research and Quality within HHS, conducted an internal study of VAERS reporting rates in a Massachusetts patient population between 2007 and 2010. The study found that fewer than 1% of vaccine adverse events were being captured by the reporting system.¹² When the researchers attempted to communicate their findings to the CDC in order to develop improved reporting mechanisms, the agency stopped responding to their emails. The grant ended. The improved reporting system was never built.
The passive reporting infrastructure that captures under 1% of injuries then becomes the basis for the CDC’s public assurances that adverse events are rare.
The injury table itself has been subject to steady contraction. When the Vaccine Injury Compensation Program began in 1988, the injury table included a broader range of conditions presumed to be caused by vaccination, with corresponding timelines within which onset would qualify a case for compensation.¹³ Over the following decades, categories were removed or narrowed. Sudden Infant Death Syndrome, initially compensable when it followed vaccination within a specified window, was removed. Neurodevelopmental injury, briefly acknowledged as a category during the 1990s when concerns about the MMR product and other injections emerged, was removed. The seizure timelines were narrowed. Encephalopathy definitions were tightened.
The 1995 amendment illustrates the pattern. Residual seizure disorder — a category under which many families of children who had suffered seizures after DPT vaccination had successfully claimed compensation — was removed. Encephalopathy criteria were revised in ways that made the diagnosis nearly impossible to satisfy. The Advisory Commission on Childhood Vaccines, which recommended the changes, drew a majority of its membership from the same medical-institutional networks that administered and defended the vaccine schedule. Petitioners whose cases had been filed under the earlier table found themselves adjudicated under the new one. Cases that would have succeeded were denied.
Each removal reduced the number of compensable claims. The fund benefited. So did the manufacturers whose products would otherwise be more clearly implicated in the injury pattern.
The Institute of Medicine, tasked periodically with reviewing whether specific vaccines cause specific injuries, has repeatedly concluded that the evidence is insufficient to accept or reject a causal relationship for a majority of the injury-outcome pairs it examines.¹⁴ This finding — insufficient evidence — is then used in the injury compensation courtroom to deny claims. The absence of evidence functions as evidence of absence, produced by the very research infrastructure that would have to fund the studies to end the insufficiency.
The industry’s founding figure confirmed the position under oath in the same deposition. Asked directly whether he could make the scientific statement that childhood vaccines do not cause autism, Plotkin answered: “As a scientist, I would say that I do not have evidence one way or the other.” The IOM had found no study establishing that the DTaP or Tdap products do not cause autism. Plotkin acknowledged that no such study existed and that he personally held no evidence to support the claim his industry has spent three decades making.
The parent whose child seized within twelve hours of vaccination, developed encephalopathy, and never recovered enters a system that was prepared for her arrival. The injury table’s timeline for seizure onset has been shortened past the point where her child’s case qualifies. The IOM has declared the evidence insufficient. VAERS captured her report and did nothing with it. The monitor was never separate from the promoter.
5. The Court and the Blame
The Vaccine Injury Compensation Program is administered by the U.S. Court of Federal Claims. It is not a court in the ordinary sense. The proceedings involve no juries, no meaningful discovery, and no Article III judges — no judges appointed for life under the constitutional protections designed to insulate the judiciary from executive influence.
Cases are heard by “Special Masters,” Article I officers appointed by the Chief Judge of the Court of Federal Claims to seven-year terms. The Special Masters are drawn from a pool of attorneys with prior government experience. The Department of Justice provides the attorneys who defend against injury claims. HRSA administers the fund. The petitioner’s attorneys are paid from the same fund out of which awards are made.
Every party in the courtroom — the judge, the government’s defense attorneys, the fund itself, and the petitioner’s legal counsel — is paid by the federal government. The injured child’s family stands before a tribunal in which no independent party has an interest in a finding of injury.
The statistics reflect the structure. The majority of petitions filed with the VICP have been dismissed rather than compensated over the life of the program.¹⁵ Of the cases that succeed, the majority are settled rather than adjudicated on the merits, with no admission that the vaccine caused the injury. The compensation cap for a vaccine-caused death — $250,000 — has not been raised since the statute was passed in 1986.
The excise tax that funds the program is $0.75 per antigen per dose. The fund now holds over $4 billion.¹⁶ The families whose children were injured cannot access it through the ordinary legal system because the ordinary legal system has been closed to them.
This is the structure Leslie Manookian described in her twelve-point summary. Her exact phrasing on the final function is worth returning to: “So, parents who’ve already suffered an unimaginable tragedy are up against a govt court staffed by govt paid special masters and attorneys with no due process defending a govt licensed and govt mandated product for which they blame the victims for harm.”
The final phrase — “they blame the victims for harm” — describes the twelfth function of the machine. When a child collapses after vaccination with the sudden onset of retinal hemorrhages, subdural hematoma, and cerebral edema — the triad — the diagnosis assigned in emergency departments and coroner’s offices is “shaken baby syndrome” or its rebranded successor, “abusive head trauma.” The triad is presumed diagnostic of parental abuse. The parents are arrested.
The vaccine reaction that produces the identical triad — through encephalopathy, elevated intracranial pressure, and hemorrhagic events following injection — is not considered in the differential diagnosis.¹⁷ The diagnostic criteria for “shaken baby syndrome” were developed without accounting for it. The emergency physician, the coroner, and the child protective services investigator have all been trained within an institutional framework in which vaccine injury of this magnitude does not exist.
Alan Yurko’s ten-week-old son died in November 1997 shortly after receiving a round of childhood vaccinations. Yurko was convicted of first-degree murder in 1999 on the basis of the triad diagnosis and sentenced to life plus ten years in Florida state prison. He was released in 2004 after independent medical review of the case demonstrated that the shaking diagnosis could not be sustained and post-conviction proceedings established alternative medical explanations for the child’s injuries.¹⁸ Yurko is one documented case. There are others. The precise number is unknown because the diagnostic framework prevents the question from being asked.
A parent whose child dies after vaccination faces a compound structure. The vaccine that caused the death is licensed by the federal government, recommended by the federal government, purchased by the federal government, and defended in the injury court by the federal government. The manufacturer is shielded from civil liability by federal statute and Supreme Court precedent. The injury table does not recognize the death as vaccine-caused. The state, meanwhile, has assigned the triad diagnosis and turned the case over to the district attorney. The parent must now prove — in a criminal court, against the state — that the child was not shaken.
Robalee Bruesewitz spent nearly two decades in litigation on behalf of her daughter. The Supreme Court’s ruling denied her family relief and closed the door behind them for every family that would come after. The 1986 Act had shifted liability from the manufacturer to the taxpayer. Bruesewitz confirmed that the shift was permanent and that no design decision made by the manufacturer could be challenged in any court open to ordinary Americans.
This is the position in which the American parent now stands. Her child’s pediatric visit will produce a recommendation to administer products licensed on the basis of trials that were never controlled against saline. The state will require their administration for school attendance. When injury results, over 99% of adverse events never reach VAERS at all, and the reports that do reach it change nothing. A family that attempts compensation will petition a court in which every party is paid by the federal government to defend the products or administer the fund. And when death occurs with the triad present, the emergency department’s diagnostic framework will not include vaccine reaction in the differential, and the parent enters the criminal jurisdiction as the presumed cause of the child’s death.
There is no exemption from this structure that carries no cost. State legislatures have progressively narrowed medical and religious exemptions; declining vaccines removes a child from school; injury bars a family from ordinary civil courts. And when death is accompanied by the triad, the state prosecutes the parent for the death.
Leslie Manookian described this arrangement, at the close of her twelve-point post, as “crony capitalism at best and pure evil fascism at worst.” The characterization is precise. A private industry produces the product. The state compels its administration, indemnifies the manufacturer against claims of harm, and prosecutes the parent when the harm arrives.
The machine’s design serves the flow of money and the concentration of power. Every safeguard the ordinary citizen might rely on — informed consent, product liability, judicial review, jury trial, prosecutorial restraint — has been removed at the point where the childhood vaccine schedule intersects with the American family. The parent who accepts the recommendation and whose child is injured has no meaningful path to redress. Refusal costs school access. Death with the triad opens the parent to criminal prosecution for a killing they did not commit.
This is the environment in which every American child is now born. The machine was assembled piece by piece across four decades, ratified by every institution that could have prevented it, and defended by the same institutions today. What Leslie Manookian named as crony capitalism at best and fascism at worst describes a working system, operating as designed, in a country that once organised its politics around the presumption that no such system could be permitted to form.
For a Six-Year-Old
There is a big company that makes shots.
The government helps the company make the shots and sell them. The government tells your school that you have to get the shots before you can come to school.
Nobody checks the shots very well. The people who are supposed to check work with the company. So the shots go out into the world before anyone really knows if they are safe.
When a child is hurt by a shot, the family cannot go to a normal judge. There is a special room where a different kind of judge decides. That judge is paid by the government. The lawyers on the other side are paid by the government. The government made the shot rules. The government bought the shots. And the government decides whether the shot hurt you.
Most families are told the shot did not hurt their child, even when it did.
When a shot makes a baby die, the doctors sometimes think the mother or father shook the baby. The parents can be arrested. They can go to prison. For what the shot did.
The company that made the shot never gets in trouble. The company keeps making the shots. Your school keeps requiring them. The next family goes through the same door.
That is the machine.
References
¹ National Childhood Vaccine Injury Act of 1986, Public Law 99-660, 42 U.S.C. § 300aa-1 et seq.
² Bruesewitz v. Wyeth LLC, 562 U.S. 223 (2011).
³ Leslie Manookian, twelve-point summary post, X (@LeslieManookian), July 3, 2026, status/2072712451800625369.
⁴ Deposition of Stanley A. Plotkin, M.D., taken January 11, 2018, in Matheson v. Schmitt, State of Michigan, Circuit Court for the County of Oakland, Family Division, Case No. 2015-831539-DM; transcript published via Informed Consent Action Network.
⁵ ICAN v. HHS, correspondence dated July 9, 2018, in response to FOIA request; HHS acknowledged no biennial reports produced under 42 U.S.C. § 300aa-27(c).
⁶ Vaccines for Children Program expenditure data, Centers for Disease Control and Prevention; annual VFC purchasing figures.
⁷ U.S. Patents 5,437,951 and related — Lowy, Schiller et al., “Self-Assembling Recombinant Papillomavirus Capsid Proteins,” assigned to the United States Department of Health and Human Services; licensed to Merck & Co. for Gardasil.
⁸ Mawson AR et al., “Pilot comparative study on the health of vaccinated and unvaccinated 6- to 12-year-old U.S. children,” Journal of Translational Science, 2017.
⁹ Thomas JL, Lyons-Weiler J, “Relative Incidence of Office Visits and Cumulative Rates of Billed Diagnoses Along the Axis of Vaccination,” International Journal of Environmental Research and Public Health, 2020.
¹⁰ Statement of William W. Thompson, Ph.D., through counsel Rick Morgan, August 27, 2014; documentation regarding DeStefano DA et al., “Age at first measles-mumps-rubella vaccination in children with autism and school-matched control subjects: a population-based study in metropolitan Atlanta,” Pediatrics, 2004.
¹¹ United States ex rel. Krahling and Wlochowski v. Merck & Co., Inc., No. 2:10-cv-04374, U.S. District Court for the Eastern District of Pennsylvania, complaint filed 2010.
¹² Lazarus R et al., “Electronic Support for Public Health–Vaccine Adverse Event Reporting System (ESP:VAERS),” Grant Final Report, Harvard Pilgrim Health Care, Inc., 2011 (AHRQ Grant ID R18 HS 017045).
¹³ Vaccine Injury Table history, Health Resources and Services Administration; successive amendments to 42 C.F.R. § 100.3.
¹⁴ Institute of Medicine (now the National Academy of Medicine), Adverse Effects of Vaccines: Evidence and Causality (2011) and predecessor reports.
¹⁵ Health Resources and Services Administration, VICP claim adjudication statistics.
¹⁶ Vaccine Injury Compensation Trust Fund monthly balance report, U.S. Department of the Treasury.
¹⁷ Michael Innis, “Vaccines, Apparent Life-Threatening Events, Barlow’s Disease, and Questions about ‘Shaken Baby Syndrome,’” Journal of American Physicians and Surgeons, 2006; Harold Buttram and Alan R. Yurko, “Shaken Baby Syndrome or Vaccine-Induced Encephalitis?” Medical Sentinel, subsequent case documentation.
¹⁸ State of Florida v. Alan R. Yurko, Ninth Judicial Circuit, 1999; post-conviction proceedings and release 2004; contemporaneous medical review including Harold E. Buttram, M.D.
¹⁹ Unbekoming, “Interview with Leslie Manookian, Health Freedom Defense Fund,” Lies are Unbekoming, Substack, April 13, 2024.
“We are basically given a piece of paper that says when the vaccines are due and when to give them.”
Dr. Suzanne Humphries: “You may not know this, but doctors are not taught about vaccines in medical school. We are not taught what is in vaccines, the adjuvants, we are not taught how vaccines are manufactured, as far as what kind of animals go into them, we are not taught the potential dangers of vaccination, we are basically given a piece of paper that says when the vaccines are due and when to give them.”
There is your 30 seconds of Vaccine Education. You now have the amount of Education as the average doctor. Congratulations!
Don’t you think there is a purpose to keeping doctors in the DARK?
Then Dr. Humphries did her own research on what she was told about Smallpox Vaccines and Polio Vaccines – two diseases she said she was “continuously told were eradicated by vaccination.”
Dr. Humphries found out that this was a total LIE. She wrote this in her book
She found that populations that stopped Vaccinating for Smallpox had a DECLINE in smallpox.
She says the Polio vaccination did not make polio go away and this story is a more complicated one.
Today Dr. Humphries spends 6 to 8 hours every single day researching immunology and everything she needs to know about vaccinations – the “deeper details of vaccinations.”
Dr. Humphries says that medical authorities use fear to get populations to get vaccinated and the authorities tell doctors to persuade you to get vaccinated, to use fear if necessary and even to kick you out of the office if you refuse to get vaccinated.
Nothing better than the “Doctor knows Best” attitude.
Vaccines are Safe & Effective and they Need to be Given.
The medical “authorities” do not want doctors or their patients looking into the data, they just want both to comply and they use the doctors as your higher authority, but the doctors don’t know any more than you do, they are just TOLD that the vaccines are safe and effective and are told to tell you that.
That’s how the vaccine game is played and that’s how they are setting children up for a lifetime of illnesses, diseases and a much shorter lifespan than their parents and grandparents.
What is ONE Question that a Doctor should Ask EVERY Single time someone comes in their office?
Doctors should ask “When was the last time you were vaccinated and what vaccine(s)?”
Do they? NOPE.
Their superiors would have a cow if they knew they were doing this and connecting some common sense dots.
They don’t want you to know and they don’t want your doctor to know. Just follow the orders, keep your mouth shut and don’t question the narrative.
Doctors actually believe what they are told most of them get vaccinated themselves.
What better way to get the masses to get vaccinated when the doctors themselves are taking the jabs?
Doctors do not have the time to educate themselves, they are too busy and they choose to do other things on their days off.
They certainly are not going to receive this education from med school.
There are TWO Sciences here – one by the Private Medical Industry and one by Independent Scientists and Researches. One has Big Pharma Interest and the other doesn’t.
Big Pharma Science has a MAJOR “Conflict of Interests.” They can design studies by word trickery that make them reach any endpoint they desire. That is how it is done. 100%.
Don’t worry about the Thimerosal (49% Mercury) and the Aluminum in the jabs, just trust the final headliners that say the vaccines are safe and effective.
Dr. Humphries goes over some date with Unvaccinated vs Vaccinated and the picture is very clear.
Then she goes over Tetanus Vaccines – one jab you do not want to take. You can watch the full video in the source #1 below.
Improvements in lifestyles, good hygiene and nutrition had more to do with the decline of death and the incidences of diseases than both antibiotic intervention and vaccinations.
“Israel’s” military aggression in southern Lebanon has damaged or destroyed heritage sites across the region, including UNESCO-listed landmarks, historic towns, religious sites, and archaeological monuments, Lebanon’s Culture Minister Ghassan Salame told Reuters, warning that authorities have yet to assess the full extent of the destruction due to the continued Israeli military presence in parts of southern Lebanon.
According to Salame, Israeli forces remain stationed in an approximately 10-kilometer-deep zone inside southern Lebanon despite the ceasefire that came into effect a week ago, preventing officials from conducting comprehensive damage assessments. “We cannot work under the shadow of occupation,” he said.
The occupied zone includes the medieval Beaufort Castle and centuries-old border villages that were home to Christian, Shiite Muslim, and Sunni Muslim communities, along with their places of worship. Salame said entire villages had been erased, adding, “There are villages that have been completely bulldozed.”
Beyond the occupied areas, Israeli airstrikes also struck historic cities including Tyre, Nabatieh, and Tebnin. Salame expressed concern that Tebnin’s Crusader-era fortress may have sustained damage during the bombardment.
“Heritage is not only Roman and Phoenician antiquities,” Salame said. “Heritage is also historic buildings, archaeological sites, and buildings with a cultural function.”
Among the sites affected was the UNESCO World Heritage city of Tyre, where a crown was blown off an ancient Roman column. A pilgrimage site revered by both Muslims and Christians was reportedly destroyed in another southern town, while Israeli strikes heavily damaged the Mamluk-era market in Nabatieh and razed centuries-old villages along the border.
In response to Reuters‘ questions, the Israeli military said it does not seek “to cause excessive damage to civilian infrastructure and strikes only out of military necessity, with consideration for the safety of its citizens.” It added that operations involving “sensitive sites” undergo “a rigorous approval process as required.”
The Israeli military has also accuse
Modern-day Lebanon contains archaeological and historical sites reflecting civilizations including the Phoenicians, Byzantines, Mamluks, and Crusaders. Tyre, whose origins date back nearly 5,000 years, remains one of the country’s most significant cultural landmarks and is recognized as a UNESCO World Heritage Site.
Following months of Israeli bombardment, large parts of Tyre have been reduced to rubble. Protective barriers erected around the archaeological site to shield it from strikes and debris were themselves destroyed during the attacks.
“Look at the damage that happened to it, it’s as if it all exploded from underneath, as if an earthquake hit it,” Adnan Istanbouli of Lebanon’s antiquities department told Reuters while inspecting damage near a Roman mosaic.
Tyre’s Deputy Mayor Alwan Charafeddine said the city should have been protected under international conventions.
“It is supposed to be one of the cities that is internationally protected, or that should never be targeted in any way, in any conflict,” he said.
UNESCO voices concern over cultural destruction
Last month, UNESCO expressed concern over the condition of Tyre, which is listed as a World Heritage Site under enhanced protection status. The agency also said it was “deeply alarmed” by reports of damage to a citadel in the southern town of Chama and by fighting around Beaufort Castle, while condemning what it described as “unlawful attacks against cultural property.”
Following Israeli strikes on Tyre, Salame requested that UNESCO classify the city as a World Heritage Site in Danger, a designation that would trigger additional international protection measures. The request has not yet been approved.
Salame also pointed to earlier remarks by Israeli War Minister Israel Katz, who said during the conflict that Israeli forces would destroy all houses along Lebanon’s border.
Warning of the long-term consequences, Salame said the destruction threatens to erase centuries of Lebanon’s cultural identity.
“There is something systematic: a systematic destruction of villages, hamlets, and entire towns,” he told Reuters.
The FDA began reevaluating sunscreen chemical safety in 2019, yet millions are still told to apply these products every day. Jefferey looks at what happens when sunscreen chemicals enter the bloodstream, and why new research on sun exposure, vitamin D, and cancer is challenging old assumptions.
For three thousand years, Crocus sativus — saffron — has been threaded into the food, ritual, and medicine of Persia, India, and the Mediterranean. What is new is not the plant. What is new is the clinical record: a growing body of randomized, controlled research showing that saffron can perform comparably to several conventional psychiatric medications for depression, obsessive-compulsive disorder, and ADHD — often with fewer adverse effects (GreenMedInfo overview; a 2024 systematic review).
This is not a claim that pharmaceuticals never help (indeed, the active placebo effect alone is to generate a perceived positive effect in the majority of treatments). It is something more uncomfortable: strong evidence that the dominant drug-centered model has quietly ignored a lower-risk botanical option with a far older record of human use — and called it folklore while doing so.
“If a patented molecule matched Prozac, fluvoxamine, or Ritalin with fewer side effects, it would be called a breakthrough. Because saffron is an ancient spice, it is treated like a footnote.”
It should also be noted that the adverse effects of psychiatric medications have been downplayed, especially their connection to violent episodes. We have explored this problem in greater depth in the article below.
I. Older Than Memory: The Spice at the First Chapter of Medicine
The truth is that we saythree thousand yearsout of habit. The origin of saffron is far stranger, and far older. Pigments derived from saffron have been identified in cave paintings in what is now northwest Iran, dated to roughly fifty thousand years ago — meaning the human bond with this flower predates agriculture, predates writing, predates nearly everything we call civilization (documented at GreenMedInfo). The relationship is, as nearly as we can tell, as old as our species’ capacity for wonder.
By the Bronze Age the flower had become sacred. On the Aegean island of Thera, frescoes painted some 3,500 years ago show a goddess enthroned above attendants gathering saffron — presiding, the imagery suggests, over both the harvest and the medicinal use of the spice. When researchers finally decoded the scene, The New York Times reported that they had effectively rewritten the first chapter in the history of medicine (Honan, The New York Times, 2004). Long before the pharmacy, there was the crocus — and a goddess watching over it.
And it has never surrendered its mystery cheaply. Each Crocus sativus bloom offers only three crimson threads, and it takes roughly one hundred and fifty flowers to yield a single gram — every stigma drawn by hand, the plant having refused mechanization for the whole of its history. Ounce for ounce it has long rivaled gold. The world calls it red gold, and not as flattery.
The deeper mystery is biochemical. A single thread carries more than 150 aromatic compounds and acts on more than fifty biological pathways in the body — a symphony so layered that its medicinal power remains, in a real sense, refractory to the reductionist gaze of modern pharmacology. This is the paradox the rest of this essay lives inside: a medicine humanity has trusted since the Ice Age, whose biochemistry we are only now learning to read — and which, read at last, turns out to stand toe to toe with the patented drugs of the present day.
I. The Promise Psychiatry Keeps Failing to Keep
The public was sold a simple story: depression is a chemical imbalance (e.g. serotonin deficiency), OCD requires heavy serotonergic correction, and ADHD needs stimulants to normalize performance. But real-world outcomes are often mixed. Incomplete response, relapse, dose escalation, withdrawal difficulty, sexual side effects, sleep disruption, appetite suppression, and emotional blunting are all widely documented in the literature (depression meta-analysis; adult ADHD adjunctive trial).
This does not mean medication has no role, especially in emergency medicine. It means the standard model has often demanded a punishing trade: partial symptom control in exchange for physiological, emotional, and financial costs that patients are expected to normalize.
II. Saffron for Depression: The Ancient Spice That Stood Up to Antidepressants
Clinical trials and pooled analyses suggest saffron is significantly better than placebo for mild to moderate depression and may be comparable to standard antidepressants in symptom reduction (meta-analysis). GreenMedInfo’s summary of six saffron studies emphasizes trials in which saffron matched or exceeded common antidepressants while maintaining a cleaner tolerability profile (GreenMedInfo).
In one line of research, saffron at around 30 mg per day was comparable to fluoxetine (aka Prozac) for major depressive disorder over several weeks — similar improvement on standard depression scales, fewer problematic adverse effects in the study populations.
GreenMedInfo also highlights a postpartum depression study in which saffron outperformed escitalopram on response and remission measures — underscoring that this is not merely an adjunctive wellness story, but a direct challenge to antidepressant assumptions.
“Saffron does not merely suppress symptoms. The broader literature suggests it may support a healthier terrain: oxidative balance, neuroprotection, and inflammatory regulation.”
III. OCD: Where Saffron Matched a Front-Line Pharmaceutical
Obsessive-compulsive disorder is usually treated with SSRIs at substantial doses. Yet a randomized, double-blind study found saffron comparable to fluvoxamine in mild to moderate OCD, using standard symptom scoring over eight weeks (randomized clinical trial).
The significance is not only clinical parity, but the implication that a botanical intervention may achieve similar benefit without extending the same burden of side effects.
That matters because OCD patients are often told they must accept a harsh medication profile as the cost of functioning. Saffron’s performance here suggests the “no alternative” framing is far weaker than many patients have been led to believe.
IV. ADHD: A Challenge to the Stimulant Monopoly
Several studies and reviews suggest saffron may improve ADHD symptoms in children and adults, either alone or as an adjunct, with an acceptable safety profile (systematic review).
A pediatric trial found saffron performed comparably to methylphenidate — the molecule sold as Ritalin — for core ADHD symptoms over six weeks (pediatric trial).
An adult adjunctive randomized trial also reported benefits when saffron was added to existing treatment, suggesting value even within conventional care rather than only outside it (randomized trial).
This should force a bigger question: why is a controlled-substance framework treated as normal first-line thinking when a non-patented botanical with human-trial support has been relegated to the margins?
“When a flower can compete with a stimulant, the problem is no longer lack of evidence. The problem is what the system is willing to see.”
V. Why Saffron May Work Differently
The broader neuropsychiatric literature points to multiple active constituents in saffron — including crocin and safranal — with effects on serotonin, dopamine, oxidative stress, inflammation, and neuroprotection (mechanistic review; Frontiers review).
This multi-target profile may help explain why saffron appears to improve mood and attention without reproducing the full burden of conventional drug toxicity.
Unlike a single-target pharmaceutical narrative, saffron appears to work more like a systems-level intervention. That does not make it magical. It makes it biologically plausible in a way reductionist psychiatry often is not.
VI. Safety, Accessibility, and Price
One of the strongest arguments for saffron is not only efficacy but proportionality. At studied doses, saffron has generally shown good tolerability across trials — especially relative to medications associated with sexual dysfunction, insomnia, appetite suppression, cardiovascular concerns, or difficult discontinuation syndromes (depression meta-analysis; 2024 systematic review).
It is also accessible. Standardized saffron extracts are widely available without a prescription, and although high-quality saffron is not cheap by weight, the clinically studied extract doses are small enough that monthly use may compare favorably with branded psychiatric medications — and with the downstream cost of managing their side effects.
This does not prove saffron is always cheaper in every market. But it strengthens the case that a lower-tech option may deliver better value with less harm.
VII. A Balanced Position on Medication
Some people benefit meaningfully from antidepressants, from SSRIs for OCD, or from stimulant medications for ADHD. Abrupt discontinuation can be dangerous, and saffron should not be presented as a simplistic replacement for every patient in every context.
But balance cuts both ways. A fair reading of the literature no longer allows the claim that pharmaceuticals are the only serious evidence-based option. Saffron now belongs in the main conversation: as a first consideration in some mild to moderate cases, as an adjunct in others, and as a serious object of informed discussion between patients and clinicians.
VIII. The Real Scandal
The real scandal is not that saffron works. The scandal is that patients have been taught to regard an ancient, clinically validated spice as quaint — while accepting a cascade of pharmaceutical harms as modern medicine.
A model built on failed promises deserves scrutiny. A medicine with deep cultural roots, growing scientific support, broad accessibility, and a gentler risk profile deserves a place at the center of the discussion.
If the psychiatric model were judged by the standards imposed on natural medicine, it would have to explain far more than saffron ever did.
IX. The Benevolent Superfluity: Why a Flower Heals
Chemistry tells us how saffron works. It does not tell us why a flower, of all things, should be the one to outperform the molecules built in the lab. For that we have to go underneath pharmacology — to the strangest fact about the plant we have been discussing: that before it is a medicine, it is a flower, and the flower is the most extravagant, least necessary, most beautiful gesture the living world makes.
A flower feeds nothing on its own. It shelters no one. By the cold logic of survival it is extravagant waste — energy poured into color, scent, symmetry, and form when sturdier roots would have been the rational investment. And yet every human culture on every continent has tended flowers for at least five thousand years, with, as one Rutgers study dryly noted, no known reward for this costly behavior. When the researchers measured what a flower actually does to a person, the result was without precedent in the literature of emotion: a gift of flowers produced the involuntary Duchenne smile — the true smile, the one that cannot be faked — in one hundred percent of recipients. No gift of candy or money had ever reached that number. In the elderly it lifted mood and sharpened memory; in a crowded elevator a single bloom dissolved the reflex of stranger-avoidance and made people speak (Haviland-Jones et al., Evolutionary Psychology, 2005).
I have argued elsewhere that this is no accident of neural wiring, but a disclosure about the nature of reality itself — what I have called the benevolent superfluity of the universe (A Benevolent Superfluity). The cosmos did not stop at hydrogen, or carbon, or the first living cell. It kept going, overshooting bare function and landing in beauty — the spiral of the nautilus, the lattice of the honeycomb, the five-fold symmetry of the wild rose. Beauty, in this reading, is not decoration laid over a grey and functional world. Beauty is the structure of reality expressing itself. The flower is that structure made flesh — made petal, made scent, made color. The superfluous turns out to be the sacred, and the sacred turns out to be exactly what the body recognizes in an instant, before thought, with a yes.
Now hold saffron against that backdrop. If the flower is the universe’s gratuitous beauty made incarnate, saffron is that gesture brought to its most concentrated pitch: the crimson heart of the crocus, three threads to a bloom, a hundred and fifty flowers spent for a single gram, more than a hundred and fifty aromatic compounds folded into each thread. It is the flower distilled to its most lavish and most superfluous expression — and it carries, in that concentration, the same healing ontology the Duchenne study caught on film.
This is why the contest with the synthetic drug was never quite fair to the drug. A laboratory molecule is a stranger to the body — a foreign key for which the body has no lock, which it must labor to detoxify, paying the tax in the gut, the liver, the nervous system. Saffron is not a stranger. It is kin — the flower, the oldest object of human tenderness, a form the body has been answering with a yes since before we had language for it. The drug subtracts as it acts. The flower, even as medicine, adds — because it is continuous with the beauty that makes a nervous system want to go on living at all. That continuity is not a metaphor laid over the pharmacology. It is the ground the pharmacology stands on.
A note on practice
This essay is a reading of what the clinical literature reveals, not medical advice. Do not stop a prescribed antidepressant, SSRI, or stimulant abruptly — discontinuation of these drugs can be dangerous, and some require careful, supervised tapering. If you are looking for support in withdrawing from psychiatric medicines, consult the Inner Compass initiative. Saffron is not a blanket substitute for every patient in every situation, and it is not free of interactions: it can have additive effects with serotonergic medications and acts on the same mood-regulating pathways, so it warrants the same respect as any active compound. Pregnancy, bipolar disorder, and combination with prescription psychiatric drugs all call for a knowledgeable practitioner’s oversight. Honor the power of this plant by respecting it — and make these decisions with a clinician who will actually read the evidence with you.
The Holocaust: Myth and Reality, Overview of the book by Dr. Nicholas Kollerstrom
BY ANTONY C. BLACK • UNZ REVIEW • APRIL 17, 2022
Heresy In the 21st Century
Never in my long journalistic career have I ever hesitated to put pen to paper – until now. Indeed, I have delayed writing this overview of Dr. Kollerstrom’s remarkable book for going on six years.[1] Up until now no subject had been too controversial, too sensitive, too beyond the pale as to warrant more than a passing moment’s consideration of consequences. But this is different. In some sixteen countries in Europe one can be put in prison for doing what I am doing now, or even for expressing ‘holocaust denialism’ on social media. In Germany some fifteen thousand people are tried each year for Thought Crime, i.e., for so-called ‘right-wing extremism’. Here in North America it is somewhat better; one merely risks losing one’s job, friends and family – and possibly being blacklisted as a writer from virtually every venue one might have formerly been associated with. No small potatoes.
Dr. Kollerstrom, himself, stumbled rather more naively into this punitive quagmire in 2008 when, after merely reviewing a scientific paper analyzing samples taken from the walls of the alleged ‘gas chambers’ at Auschwitz, – a paper authored by one Germar Rudolf, a young scientist working at the time at the Max Planck Institute – he found himself summarily dismissed from his erstwhile position as historian and philosopher of science at University College, London (UCL), “the sole member of staff…ever to have been expelled for ideological reasons”. As he recounts,
“I became ethically damned, thrown out of polite, decent groups, banned from forums and denounced in newspapers…..I felt as if some Mark of Cain had been branded onto my forehead. I had done something so awful that we could not even discuss the matter. The Medieval crime of Heresy was back alive and well…”
Heresy, of course, implicates the notion of taboo, and what a society makes taboo is what it feels to be sacred, and what is sacred is beyond question. When dealing with the ‘Holocaust’, then, we are, Kollerstrom assures us, dealing not with historical science, but, essentially, with a religion; the Holo-religion. And as the author repeatedly points out, “There can be no science where doubt is prohibited.” … continue
This site is provided as a research and reference tool. Although we make every reasonable effort to ensure that the information and data provided at this site are useful, accurate, and current, we cannot guarantee that the information and data provided here will be error-free. By using this site, you assume all responsibility for and risk arising from your use of and reliance upon the contents of this site.
This site and the information available through it do not, and are not intended to constitute legal advice. Should you require legal advice, you should consult your own attorney.
Nothing within this site or linked to by this site constitutes investment advice or medical advice.
Materials accessible from or added to this site by third parties, such as comments posted, are strictly the responsibility of the third party who added such materials or made them accessible and we neither endorse nor undertake to control, monitor, edit or assume responsibility for any such third-party material.
The posting of stories, commentaries, reports, documents and links (embedded or otherwise) on this site does not in any way, shape or form, implied or otherwise, necessarily express or suggest endorsement or support of any of such posted material or parts therein.
The word “alleged” is deemed to occur before the word “fraud.” Since the rule of law still applies. To peasants, at least.
Fair Use
This site contains copyrighted material the use of which has not always been specifically authorized by the copyright owner. We are making such material available in our efforts to advance understanding of environmental, political, human rights, economic, democracy, scientific, and social justice issues, etc. We believe this constitutes a ‘fair use’ of any such copyrighted material as provided for in section 107 of the US Copyright Law. In accordance with Title 17 U.S.C. Section 107, the material on this site is distributed without profit to those who have expressed a prior interest in receiving the included information for research and educational purposes. For more info go to: http://www.law.cornell.edu/uscode/17/107.shtml. If you wish to use copyrighted material from this site for purposes of your own that go beyond ‘fair use’, you must obtain permission from the copyright owner.
DMCA Contact
This is information for anyone that wishes to challenge our “fair use” of copyrighted material.
If you are a legal copyright holder or a designated agent for such and you believe that content residing on or accessible through our website infringes a copyright and falls outside the boundaries of “Fair Use”, please send a notice of infringement by contacting atheonews@gmail.com.
We will respond and take necessary action immediately.
If notice is given of an alleged copyright violation we will act expeditiously to remove or disable access to the material(s) in question.
All 3rd party material posted on this website is copyright the respective owners / authors. Aletho News makes no claim of copyright on such material.
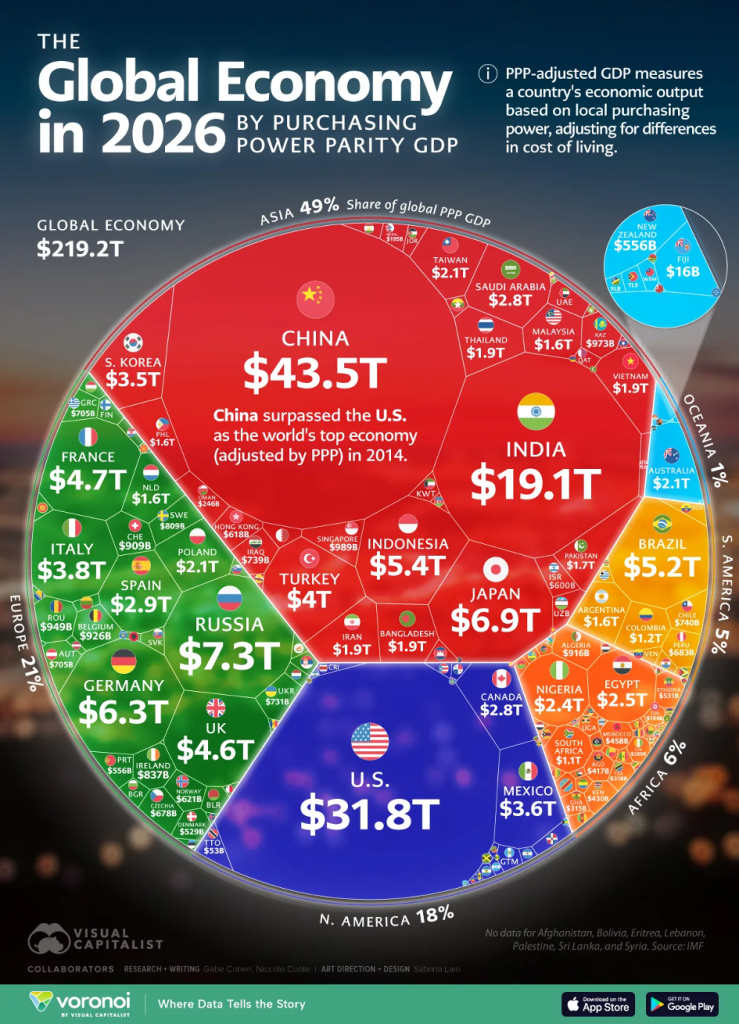
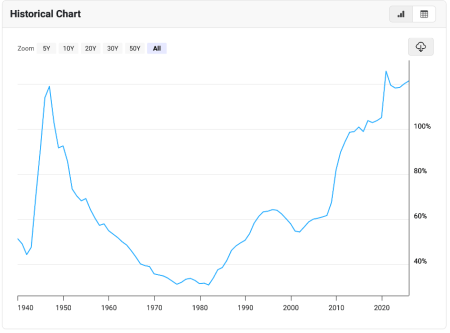
 Source: Macrotrends
Source: Macrotrends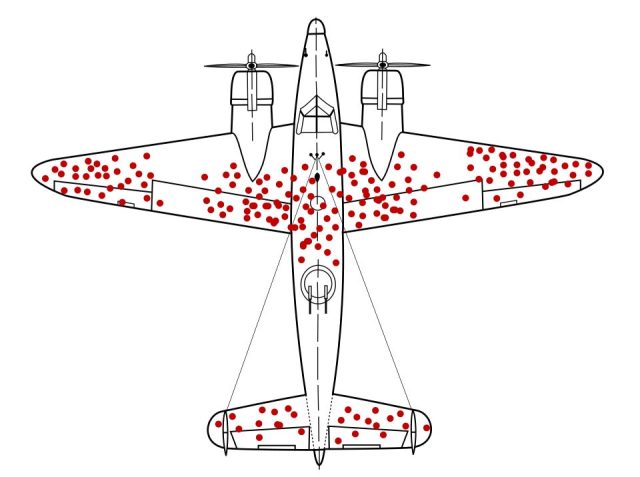



 Never in my long journalistic career have I ever hesitated to put pen to paper – until now. Indeed, I have delayed writing this overview of Dr. Kollerstrom’s remarkable book for going on six years.[1] Up until now no subject had been too controversial, too sensitive, too beyond the pale as to warrant more than a passing moment’s consideration of consequences. But this is different. In some sixteen countries in Europe one can be put in prison for doing what I am doing now, or even for expressing ‘holocaust denialism’ on social media. In Germany some fifteen thousand people are tried each year for Thought Crime, i.e., for so-called ‘right-wing extremism’. Here in North America it is somewhat better; one merely risks losing one’s job, friends and family – and possibly being blacklisted as a writer from virtually every venue one might have formerly been associated with. No small potatoes.
Never in my long journalistic career have I ever hesitated to put pen to paper – until now. Indeed, I have delayed writing this overview of Dr. Kollerstrom’s remarkable book for going on six years.[1] Up until now no subject had been too controversial, too sensitive, too beyond the pale as to warrant more than a passing moment’s consideration of consequences. But this is different. In some sixteen countries in Europe one can be put in prison for doing what I am doing now, or even for expressing ‘holocaust denialism’ on social media. In Germany some fifteen thousand people are tried each year for Thought Crime, i.e., for so-called ‘right-wing extremism’. Here in North America it is somewhat better; one merely risks losing one’s job, friends and family – and possibly being blacklisted as a writer from virtually every venue one might have formerly been associated with. No small potatoes. Aletho News
Aletho News
{kind=link}