The Davos World Economic Forum (WEF) is a premier forum for governments, global corporations and international entrepreneurs. Founded in 1971 by engineer and economist Klaus Schwab, the WEF describes its mission as “shaping global, regional and industry agendas” and “improving the state of the world”. According to its website, “moral and intellectual integrity is at the heart of everything it does.”
The WEF has been involved in the coronavirus pandemic in several ways.
First, the WEF was, together with the Gates Foundation, a sponsor of the prescient “Event 201” coronavirus pandemic simulation exercise, held in New York City on October 18, 2019 – the same day as the opening of the Wuhan Military World Games, seen by some as “ground zero” of the global pandemic. China itself has argued that US military athletes may have brought the virus to Wuhan.
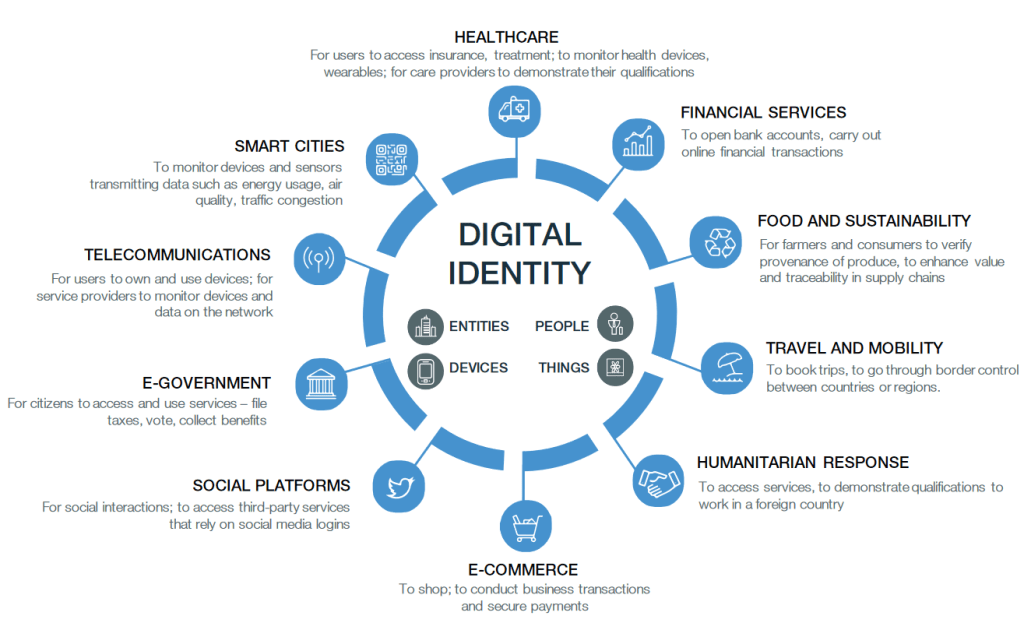
Second, the WEF has been a leading proponent of digital biometric identity systems, arguing that they will make societies and industries more efficient, more productive and more secure. In July 2019, the WEF started a project to “shape the future of travel with biometric-enabled digital traveler identity management”. In addition, the WEF collaborates with the ID2020 alliance, which is funded by the Gates and Rockefeller foundations and runs a program to “provide digital ID with vaccines”. In particular, ID2020 sees the vaccination of children as “an entry point for digital identity.”
Third, WEF founder Klaus Schwab is the author of the book COVID-19: The Great Reset, published in July 2020, which argues that the coronavirus pandemic can and should be used for an “economic, societal, geopolitical, environmental and technological reset”, including, in particular, advancing global governance, accelerating digital transformation, and tackling climate change.
Finally, the WEF has been running, since 1993, a program called “Global Leaders for Tomorrow”, rebranded, in 2004, as “Young Global Leaders”. This program aims at identifying, selecting and promoting future global leaders in both business and politics. Indeed, quite a few “Young Global Leaders” have later managed to become Presidents, Prime Ministers, or CEOs (see below).
During the coronavirus pandemic, several WEF Global Leaders and Global Shapers (a junior program of the Global Leaders) have played prominent roles, typically promoting zero-covid strategies, lockdowns, mask mandates, and ‘vaccine passports’. This may have been a (largely failed) attempt to protect public health and the economy, or it may have been an attempt to advance the global transformation agenda outlined above, or perhaps both.
In this regard, some notable Young Leaders include Jeffrey Zients (US White House Coronavirus Response Coordinator), Stéphane Bancel (CEO of Moderna), Jeremy Howard (founder of influential lobby group “Masks for All”), Leana Wen (zero-covid CNN medical analyst), Eric Feigl-Ding (zero-covid Twitter personality), Gavin Newsom (Governor of California, selected in 2005), Devi Sridhar (British zero-covid professor), Jacinda Ardern (Prime Minister of New Zealand), French President Emanuel Macron (selected one year prior to his election in 2017), Austrian Chancellor Sebastian Kurz, German Chancellor Angela Merkel (selected back in 1993), German Health Minister Jens Spahn, and former British Prime Minister Tony Blair (a leading proponent of ‘global vaccine passports’).
To get a full overview of their members, see Global Leaders for Tomorrow and Young Global Leaders on WikiSpooks (a Wiki focusing on covert power structures) as well as the official Young Global Leaders website. For an overview of some notable members in politics and the media, see below.
In conclusion, the Davos World Economic Forum has indeed been involved in the strategic management of the coronavirus pandemic, with a major emphasis on using the pandemic as a catalyst for digital transformation and the global introduction of digital identity systems.
Digital Identity: The vision of the World Economic Forum (WEF, 2018)
WEF “Young Global Leaders”
An overview of some WEF Young Global Leaders (2005-2021) and Global Leaders for Tomorrow (1993-2003) in politics and the media. The list is not exhaustive.
Jeffrey Zients (White House Coronavirus Response Coordinator since 2021, selected in 2003), Jeremy Howard (co-founder of lobby group “masks for all”, selected in 2013), California Governor Gavin Newsom (selected in 2005), Pete Buttigieg (selected in 2019, candidate for US President in 2020, US secretary of transportation since 2021), Chelsea Clinton (Clinton Foundation board member), Huma Abedin (Hillary Clinton aide, selected in 2012), Nikki Haley (US ambassador to the UN, 2017-2018), Samantha Power (US ambassador to the UN, 2013-2017, USAID Administrator since 2021), Ian Bremmer (founder of Eurasia Group), Bill Browder (initiator of the Magnitsky Act), Jonathan Soros (son of George Soros), Kenneth Roth (director of “Human Rights Watch” since 1993), Paul Krugman (economist, selected in 1995), Lawrence Summers (former World Bank Chief Economist, former US Treasury Secretary, former Harvard University President, selected in 1993), Alicia Garza (co-founder of Black Lives Matter, selected in 2020), Stéphane Bancel (Moderna CEO).
Media
CNN medical analyst Leana Wen (selected in 2018), CNN chief medical correspondent Sanjay Gupta, Covid Twitter personality Eric Feigl-Ding (a ‘WEF Global Shaper‘ since 2013), Andrew Ross Sorkin (New York Times financial columnist), Thomas Friedman (New York Times columnist, selected in 1995), George Stephanopoulos (ABC News, 1993), Lachlan Murdoch (CEO of Fox Corporation).
Technology and Social Media
Microsoft founder Bill Gates (1993), former Microsoft CEO Steven Ballmer (2000-2014, selected in 1995), Amazon founder Jeff Bezos (1998), Google co-founders Sergey Brin and Larry Page (2002/2005), former Google CEO Eric Schmidt (2001-2017, selected in 1997), Wikipedia co-founder Jimmy Wales (2007), PayPal co-founder Peter Thiel (2007), eBay co-founder Pierre Omidyar (1999), Facebook founder and CEO Mark Zuckerberg (2009), Facebook COO Sheryl Sandberg (2007).
Great Britain, Canada, New Zealand
Professor Devi Sridhar (a leading ‘zero covid’ proponent, selected in 2020/21), former British Prime Ministers Tony Blair and Gordon Brown (both selected in 1993), BBC World Service journalist Dawood Azami, Lynn Forester de Rothschild (co-owner of The Economist), Nathaniel Rothschild (son of Lord Rothschild), historian Niall Ferguson (selected in 2005), William Hague (Foreign Secretary, 2010-2014), Charles Allen (CEO of ITV, 2004-2007; Chairman of EMI, 2008-2010).
New Zealand Prime Minister Jacinda Ardern (since 2017, selected in 2014), Canadian Deputy Prime Minister Chrystia Freeland (selected in 2001; former managing director of Reuters). Canadian Prime Minister Justin Trudeau is a WEF participant, but is not a confirmed Young Global Leader.
Germany
Chancellor Angela Merkel (selected in 1993, 12 years before becoming Chancellor), current Health Minister Jens Spahn and former Health Ministers Philipp Roesler and Daniel Bahr, current co-chair of the Green Party and failed Chancellor candidate Annalena Baerbock (selected in 2020), former co-chair of the Green Party Cem Özdemir (selected in 2002), media mogul and Axel Springer CEO Mathias Doepfner (selected in 2001), talk show host Sandra Maischberger, late Foreign Minister and Vice Chancellor Guido Westerwelle (1997), former German President Christian Wulff (selected in 1995, 15 years before becoming President), Reto Francioni (former CEO of Deutsche Boerse).
European Union
EU Commission Presidents Jose Manuel Barroso (2004-2014, selected in 1993) and Jean-Claude Juncker (2014-2019, selected in 1995), French President Emanuel Macron (since 2017, selected in 2016), former French President Nicolas Sakozy (2007-2012, selected in 1993), Austrian Chancellor Sebastian Kurz, former Italian Prime Minister Matteo Renzi (2014-2016, selected in 2012), former Spanish Prime Minister Jose Maria Aznar (1996-2004, selected in 1993), Klaus Regling (CEO of the European Financial Stability Mechanism since 2012), Guy Verhofstadt (former Belgian Prime Minister, Chair of the Brexit Steering Group), Danish Minister for the Environment Lea Wermelin, Finnish Prime Minister Sanna Marin, former Finnish Prime Minister Alexander Stubb, and Mark Leonard (founding director of the Soros-funded European Council on Foreign Relations).
Switzerland
Natalie Rickli (Director of Health of the Canton of Zurich, selected in 2012), former Presidents of the Swiss National Council Christa Markwalder (selected in 2011) and Pascale Bruderer-Wyss (selected in 2009), Geneva politician Pierre Maudet (selected in 2013), NZZ media group CEO Felix R. Graf (selected in 2007), former Swiss Justice Minister Ruth Metzler (selected in 2002), former Swiss television CEO Roger de Weck (2011-2017, selected in 1994), former UBS CEOs Peter Wuffli (selected in 1994) and Marcel Rohner (selected in 2003), former Credit Suisse CEO Tidjane Tiam (1998).
Video Annex
1) Bill Gates demanding “digital immunity proof” in March 2020
2) Edward Snowden warning of the “destruction of rights” (March 2020)
CALGARY: The Justice Centre today responded to the federal government announcement that unvaccinated Canadians will lose their right to move and travel freely within Canada, their right to leave Canada, and their right to earn a living and participate in society without discrimination.
“The government is seeking to have 100% of Canadians injected with the experimental mRNA vaccine, which has not been subjected to any long-term testing on humans,” states lawyer John Carpay, President of the Justice Centre.
With the Canada-U.S. land border closed to non-essential travel, this Covid-19 vaccine travel mandate will effectively prevent unvaccinated people from leaving Canada in any way. In addition to denying unvaccinated Canadians the right to travel by plane or train, the federal government has also announced that federal employees and contractors will lose their jobs unless they participate in the world-wide experiment with new mRNA vaccines.
“We were recently promised, this past summer, that life would go back to normal once 70% of Canadians were injected with mRNA. This high vaccination rate has been achieved but has not stopped the spread of the virus. The new mRNA vaccine also provides no guarantee against the Delta variant,” continues Mr. Carpay.
According to media reports, Prime Minister Trudeau declared that these discriminatory measures against unvaccinated Canadians are needed to keep people “safe,” including children.
“Government data and statistics from every Canadian province, and from countries around the world, tell us that children, teenagers and young adults face no serious threat from Covid, which makes the Prime Minister’s rhetoric about saving children highly misleading,” continues Mr. Carpay.
“Medical reports and scientific studies make it clear that both vaccinated and unvaccinated people spread Covid-19. There is no scientific basis for turning unvaccinated Canadians into second-class citizens,” stated Allison Pejovic, Justice Centre Staff Lawyer.
Currently, Canada’s provincial and federal governments accept two injections as enough to qualify for “full” vaccination. But this may soon change to requiring three, four and more injections to maintain one’s legal status as “fully” vaccinated, as has been demonstrated in Israel and the Netherlands.
“Governments throughout history have used the notion of ‘science’ to support their policies, along with various appeals to public health, safety, security, morality, and so on. No government will violate human rights without putting forward a good-sounding justification, such as the war on terrorism, communism, online hate, drugs, or a nasty virus,” continues Mr. Carpay.
The government’s own data and statistics tell us that Covid is much closer to the annual flu than to the Spanish Flu of 1918. This matters because the entire world was put into a state of panic by the dire predictions of Dr. Neil Ferguson of Imperial College, who claimed in March of 2020 that Covid would be like the Spanish Flu of 1918, killing tens of millions of people.
“Canada’s vaccine passports, and the creation of first-class and second-class citizenship, are founded on Neil Ferguson’s demonstrably false claim that Covid is an unusually deadly killer,” states Mr. Carpay.
“Covid is real. Fear of Covid is wildly exaggerated. Over the past 18 months, government-funded media have been very successful in persuading the majority that vaccine passports (and lockdown policies preceding them) are based on science. When people hear a message thousands of times, they believe it to be true,” continues Mr. Carpay.
“The Justice Centre is profoundly disturbed that these federal mandates will prevent unvaccinated Canadians from leaving the country. Such a mandate is an egregious and unacceptable infringement of Canadians’ constitutionally protected mobility rights. There is no scientific justification for this,” concludes Ms. Pejovic.
These new government restrictions on civil liberties are still announcements at this stage, and no law has been passed by Parliament or by way of cabinet regulation (Order-in-Council). So, no legal challenge is possible at this time. If the government intends to implement these vaccine travel mandates and give them the force of law, these policies can then be challenged in court.
In Oakville, Ontario in Canada, engaged couples will have to show a vaccine passport to attend a meeting for a marriage license. The only way around the requirement is to get married in a different town.
“Appointments for marriage licenses and ceremonies that have already been booked prior to September 22 will not require proof of full vaccination,” the city website says. “…however, any new appointments for marriage licences and ceremonies will be required. Ceremonies will be held inside town hall as of November 4, 2021.”
A marriage license is a requirement to be recognized as legally married in Canada. In Oakville, a marriage license cannot be obtained online.
“You must schedule an appointment to receive your marriage licence,” the city’s website says. “To be eligible for an appointment, please ensure that the intended date of your marriage is finalized and you have an officiant that has agreed to perform the marriage.”
Additionally, a couple might not get married if they do not pass a screening at the city’s building.
“When you arrive at Town Hall for your scheduled appointment, you will be required to complete a COVID-19 self-assessment,” the city said. “If you do not successfully meet the screening criteria, you will not be allowed to enter the building and your appointment will be canceled.”
The city’s requirement for proof of vaccination for marriages is in line with the vaccination mandate implemented in Ontario last month.
Three US medical certifying boards have warned doctors that they risk losing their certification and licence if they spread covid vaccine misinformation.
Internists, family doctors, and paediatricians received an email on 9 September that quoted a warning from the Federation of State Medical Boards in July1 which read: “Providing misinformation about the covid-19 vaccine contradicts physicians’ ethical and professional responsibilities, and therefore may subject a physician to disciplinary actions, including suspension or revocation of their medical licence.”2
Richard Baron, president and chief executive of the American Board of Internal Medicine (ABIM), told The BMJ that the move was an attempt to establish a standard of care. “As standard setting organisations, we thought it was important to be on record, in a public way, to make clear that putting out flagrant misinformation is unethical and dangerous during a pandemic.” Baron said that the statement has been well received—“4 to 1 positive.” But community physicians contacted by The BMJ thought differently.
“When I got that email I thought I’d better not put anything on social media about vaccines,” said Shveta Raju, a community physician in the Atlanta, Georgia, area, who has treated covid patients and led the vaccination effort at her outpatient clinic.
“The email was sent more as a veiled threat to keep doctors on the official, established narrative, and that’s what I find chilling,” said a paediatrician who pseudonymously blogs under the name Elizabeth Bennett. “Pandemic or no, there is a problem with having an ill defined concept of misinformation that’s tied to public health messaging that hasn’t been consistent. How are physicians supposed to figure out what is misinformation when public health messaging swings so wildly?” Bennett asked.
Undefined offence
Baron said that the statement was also intended to signal the certifying boards’ support for physicians “trying to do the right thing.”
“We wanted to support that group and say ‘hey, we do have a standard of care here and you are doing the right thing when you uphold it,’” he said.
Raju responded, “If that was their intent, they should have defined misinformation. By leaving it undefined, the message was that we can’t talk about this at all.” She said that physicians are, by and large, a conservative group. “If they’re not sure what can be deemed misinformation, physicians would rather be quiet.”
Bennett concurred: “The thing I find most alarming is that they don’t define misinformation, but if they strip you of your board certification, you would lose your means of earning a living.”
Doctors spreading misinformation?
Official and social media company efforts to target “vaccine misinformation” predate the pandemic.3 But the new statement from ABIM, the American Board of Family Medicine, and the American Board of Paediatrics is one of several recent statements putting doctors in the spotlight for the first time.
In Canada, warnings about physician information began earlier, when in April the College of Physicians and Surgeons of Ontario declared that physicians “have a professional responsibility not to communicate anti-vaccine, anti-masking, anti-distancing, and anti-lockdown statements or promote unsupported, unproven treatments for covid-19.”4
The Canadian statement triggered an outcry, leading to a clarification that the statement was “not intended to stifle a healthy public debate about how best to address aspects of the pandemic.” But concerns continued. In June, a Canadian member of parliament held a press conference on censorship of Canadian clinicians and scientists. YouTube removed the video of the meeting.56
The BMJ asked ABIM about the size of the problem of board certified physicians spreading misinformation.
“We don’t have a sense of numbers of physicians spreading misinformation,” Baron said. “We’re at the beginning.” He believed it was only a “small number of doctors.” The medical boards opted to send the statement to all doctors, he said, because focusing on just the offending individuals would “miss the impact they’re having because of how much their voices are being amplified.”
As an example of “unprofessional or unethical behaviour,” Baron cited the case of a Florida doctor offering medical exemptions from mask wearing for $50 (£37; €43).7
Personalised medicine—or one-size-fits-all?
The BMJ asked whether physicians expressing doubt about the need for booster doses or vaccination of patients with natural immunity—two matters that have been the subject of debate and changing official guidance—would qualify as misinformation.8 “I don’t think we have concerns with doctors wrestling with areas where the science is unclear,” Baron said, “but there is no debate about whether people should get a primary vaccination series.”
Raju worries about the impact on personalised care. “The job of physicians is to take guidelines and apply them to the patient in front of them.” But now “physicians are basically being told that when it comes to covid vaccines it’s one-size-fits-all.”
Baron said, “We’re not trying to stifle conversations between doctors and patients. We understand that different people may look at evidence in different ways, but when you have an overwhelming preponderance of medical consensus in a certain area, you need at least to tell patients that there is an overwhelming professional consensus here.”
Cautious approach
Jeffrey Flier, former dean of Harvard Medical School, said that in the context of the pandemic, he was “not opposed to certain levels of misinformation triggering a decision to question somebody’s licence.” He said, “I can see this being an appropriate remedy at a time of public health emergency.
“But this is not how the system for licensure and certification has traditionally worked, and creates many opportunities for mistaken judgment about what is and is not misinformation, and those decisions would have to be rendered with extreme caution.”
Flier added, “We have to remember that there are legitimate areas of debate, and such matters should not fall within the scope of disciplinary actions.”
“There are reasons to be concerned that state boards might be unprepared for these kinds of decisions at a time when so many aspects of covid policy have been enmeshed with political views.”
Footnotes
This article was updated on 4 October to make clear that it was medical certifying boards, rather than licensing boards, that emailed physicians. The email quoted an earlier warning from the Federation of State Medical Boards.
Competing interests: PD gave a public statement at a 17 September 2021 FDA advisory committee to discuss covid-19 vaccines, where he highlighted the joint statement. The views and opinions expressed here are those of the author and do not necessarily reflect official policy or position of the University of Maryland.
Provenance: commissioned; not externally peer reviewed.
This article is made freely available for use in accordance with BMJ’s website terms and conditions for the duration of the covid-19 pandemic or until otherwise determined by BMJ. You may use, download and print the article for any lawful, non-commercial purpose (including text and data mining) provided that all copyright notices and trade marks are retained.
OWEN SOUND, Ontario – Dr. Rochagné Kilian recently resigned as an emergency room and family practice physician due to her concerns that the Ontario health system and Grey Bruce Health Services (GBHS) crossed ethical lines throughout the pandemic.
In a virtual meeting that included GBHS CEO Gary Sims and other staff members, Dr. Kilian asked Sims a series of questions about what she believes is unethical behaviour on behalf of the Ontario health system at all levels. Sims appeared to be unprepared for difficult questions pertaining to the ongoing rollout of vaccination mandates and vaccine segregation restrictions the Ontario heath system is championing.
Kilian estimated that 80 percent of the patients she saw in the ER during the past month who had inexplicable symptoms were “double vaxxed.”
Dr. Kilian relocated to Owen Sound – a small city in Grey County, Ontario – from South Africa after previously working in British Columbia. When she resettled in Owen Sound with her family, she expressed to a local paper how happy she was to live there: “Our recruitment to Owen Sound might have been by chance, but our choice to settle here was definitely not. Our four months in Owen Sound have been blessed. A little town with lots of soul, surrounded by beautiful landscapes, filled with welcoming residents and businesses, and exciting festivals, programs and activities. We truly feel fortunate to raise a family here.”
The first issue that Dr. Kilian brought up during the meeting was informed consent regarding the COVID jab and what she considered to be a coercive mentality of pressuring people to accept medications that she pointed out are still in “clinical trials.”
An GBHS administrator did not answer her question directly, but instead passed the buck to the provincial government and stated they do not have “oversight or input” regarding consent mechanisms presented to patients.
Kilian added that having more input into what patients are consenting to is something that GBHS “should consider,” especially in light of enacting the government-recommended vaccination mandates with their own staff.
Referring to informed consent and mandating experimental vaccines that been linked to thousands of deaths and injuries, Sims explained that because of the “pandemic,” certain procedural normalities will not take place.
“In a pandemic, some of those pieces that you think would be there [mechanisms of informed consent from the government] when you have lots of time to review stuff … in a pandemic, they’re going to pass mandates, and they’re going to pass laws, and they’re going to pass directives as needed to manage that pandemic,” he said. “And some of the things … will feel like they’re infringing on or taking short cuts … they are doing that directly to save lives.”
Sims then stated that there is a “massive scientific group” that has reviewed all the issues pertaining to the vaccines and their usage and rollout. This meeting took place August 23. Since then, the Ontario government has admitted that at least one of the vaccines pushed on the public has caused serious heart problems in young men, who are at virtually no statistical risk of suffering severely from COVID.
Dr. Kilian pressed Sims about claims that protocols of informed consent can be skirted due to an emergency, and clarified that the Tri-Council Policy Statement stipulates that an emergency situation does not warrant skirting protocols that protect the population from being put at risk due to medical experimentation. The Tri-Council Policy Statement is a Canadian guideline for the ethical conduct of research involving humans and/or human biological materials. As the vaccinations are still technically under experimental trial, they are being implemented under a research-based framework on the population.
It was Kilian’s opinion that the ethical framework is being ignored, thus health workers and citizens are being forced to take something against their will that is not proven to be safe or effective in the long term, as a result of vaccination mandates.
Sims reacted sharply to Kilian and said, “Nobody is forcing you to do this, you have a right to say no, but the reality is the government has the right to say that you’re not employed.”
“When the law looks at it, the law is saying you have the right to do it [enforcing vaccine mandates],” he added.
Dr. Byram Bridle, a University of Guelph professor, recently released a letter he sent to the president of his university that called into question the legitimacy of vaccine mandates, both from a medical and legal perspective. He stated in the letter that he is “confident there will be lawyers willing to test this in court.”
Dr. Kilian asked a final question in the virtual meeting about the claims that Sims and others at GBHS have made about the majority of COVID-associated cases in the region being among the unvaccinated. She asked if there was a detailed database that could be shared to prove this point. Sims stated that the vaccination status of the individuals who have been admitted in his region could not be released due to privacy reasons, but that the provincial government would have the information.
He then claimed that provincially, “less than 0.7 percent of people who ended up in ICUs were vaccinated.”
He referred to the “third wave” of COVID in Ontario that he said was due to the Delta variant, and stated that “it was all unvaccinated” who fell seriously ill at that time. The third wave in Ontario is reported to have happened in April and May. The vast majority of Ontarians had not received their second dose of any COVID jab by that point, and the province has made it clear in numerous places that a person only counts as “full vaccinated” for clinical purposes after 14 days have passed since they have received their second dose.
During the month of May in the Grey Bruce region, there were a total three confirmed hospitalizations with COVID-19. Five people in the region died that month with a COVID-positive diagnosis, and two of the deaths were residents who died outside of the county.
Sims said on the call that a minimum “80 percent” and up to “97 percent” of ICU patients with COVID across the province were unvaccinated. It is impossible to reach that number given the Grey Bruce statistics because there are too few people for calculations to be mathematical doable.
He then intimated that there will be great fears among pediatric physicians regarding autumn COVID numbers “if children start to die.” There is no evidence to suggest that COVID is dangerous to children in any statistically significant way.
Dr. Kilian resigned from her position while on the call with GBHS administration and spoke about her situation on the The Strong and Free TruthCast, where she criticized the state of health care in Canada. She expressed that care for the individual patient has gone by the wayside during the “farce that we have been living through.”
She said that throughout the entire time that the pandemic has been declared, she has only admitted two patients to the ICU that tested positive for COVID. She then clarified that this did not mean they were in the ICU due to COVID, but only that they had tested positive. She stated that her emergency department was “dead” throughout all of the declared waves of COVID, and that she took pictures of the official numbers to prove that they “had nothing to do” with lack of patients.
Dr. Kilian added that since the rollout of COVID jabs, she has seen a striking uptick in patients who have been admitted with heart issues and do not fit risk categories. She stated that as more and more people have received the jab, she has seen a host of strange events in her patients. She spoke of “people coming with newly diagnosed high blood-pressure, diabetics that was controlled that are no longer controlled – their sugars are either through the roof or they’re down in the ground … The only factor … constant that changed in their life was the injection of an experimental biologic.”
Covid-19 came to Saskatchewan (pop 1,179,906) on March 12, 2020. This highly infectious, deadly disease devastated 0.05 percent of the population; miraculously sparing 99.95 percent.
Officially, Covid killed 658 Saskatchewanians. Persons aged 80-and-over account for 298 (45 percent) of fatalities. 60-and-overs account for 85 percent.
304,000 Saskatchewanians are aged 19-and-under.
Covid allegedly killed three of them.
Annually, Covid culls 0.00049 percent of Saskatchewan youth. Accidental drownings kill more kids than Covid.
In the year ending December 31, 2021, a total of 10,107 Saskatchewanians died (up slightly from 2019). Typically, 0.8 percent of Saskatchewanians die annually.
Year-to-year fluctuations render Covid’s signal undecipherable.
Tens of thousands of Saskatchewanians suffer chronic respiratory and/or immune malfunction.
Chest infections finish-off many of these people. Most Covid fatalities rested on death’s brink, pre-Covid.
Still, Covid killed only a tiny percentage, even of this frail cohort.
Covid cases to date: 63,875.
Active cases: 4,715.
Resolved cases (dead or recovered): 59,160.
Covid’s official survival rate: 98.9 percent.
Testing programs undercount cases.
15 percent of Saskatchewanians have had Covid.
Covid’s real survival rate: 99+ percent.
Of 4,715 active cases, 273 are hospitalised.
94 percent of Covid cases self-medicate and self-police their quarantine.
They’re clearly not in distress.
Furthermore, letting 4,442 infected patients roam free means authorities don’t believe their own hype about Covid’s contagiousness and lethality.
The shocking revelation that the armed forces implemented a secret information campaign in 2020 to brainwash people over the pandemic is proof of deliberate intent to quash critical and independent thought and freedoms.
As a Canadian citizen who recovered from Covid and acquired natural immunity and antibodies without the anti-Covid vaccine, the government doesn’t much appreciate my narrative.
Proof lies in the fact that when I arrived back home in Vancouver from my work base in Europe in August, the federal government demanded that I pay for my own three-day imprisonment in a government mandated facility at a cost of up to $2,000. Refusal resulted in being ordered in writing to immediately get back on a plane and leave my own country under threat of penalties up to and including imprisonment. All because my acquired immunity didn’t jibe with the government’s “one size fits all” two-jab narrative.
Now I’ve learned that the Canadian military was deployed against unconventional and inconvenient narratives like mine in favor of lockstep groupthink. Does that make me an enemy of the state?
The Canadian military’s Joint Operations Command implemented a propaganda campaign in April 2020 with the intent to manipulate unsuspecting Canadians into falling in line with the federal government’s official positions on Covid-19. The brainwashing operation’s termination was ordered a month later, but in the meantime, it “relied on propaganda techniques similar to those employed during the Afghanistan war,” according to the Ottawa Citizen’s exclusive report on documents obtained under Access to Information.
The operation’s aim, according to the military, was to “head off civil disobedience by Canadians during the coronavirus pandemic and to bolster government messages about the pandemic.”
Generally, government intelligence operations rely on ear-bending friendly journalists and think-tank analysts to publish the state’s talking points in mainstream publications or online. Washington Post journalist Carl Bernstein, best-known for breaking the Watergate scandal, wrote in a Rolling Stone magazine article titled “The CIA and the Media,” back in 1977, how the CIA used “journalist-operatives” to “plant subtly concocted pieces of misinformation.”
He further noted: “There are perhaps a dozen well known columnists and broadcast commentators whose relationships with the CIA go far beyond those normally maintained between reporters and their sources. They are referred to at the Agency as ‘known assets’ and can be counted on to perform a variety of undercover tasks; they are considered receptive to the Agency’s point of view on various subjects.”
Another known tactic used by military intelligence to manipulate its own country’s citizens is to send out retired generals to spew talking points on various media platforms. In 2008, the Los Angeles Times wrote of the Pentagon’s Iraq War era “message multipliers” program. At the time, Democratic Congressman Paul Hodes had introduced an amendment – overwhelmingly adopted – to investigate the Pentagon’s public opinion manipulation program, unveiled by the New York Times as “cultivating former military officers who became regulars on Fox News, CNN and the broadcast networks.”
“They were fed administration talking points, believing they were getting independent military analysis,” Hodes said at the time of the public manipulation campaign.
So despite the Ottawa Citizen’s reporting that the program was officially quashed one month after its deployment, we really don’t know how much damage was done and to what extent the propaganda distribution it sparked may have since become autonomous and taken on a life of its own.
Canadians now need to know exactly what “government messages” were propagandized and where, and what “enemy narratives” were targeted for smears. Only then is it possible for the public to assess how much of the current conventional wisdom is the result of deliberate boosting or suppressing.
It’s a sad fact that the Canadian military has seen fit to use similar techniques to those that US intelligence has long deployed on foreign opponents. Declassified US intelligence manuals drafted in 1987 show that both the Pentagon and the CIA used similar propaganda techniques in Latin America, with the aim of indiscriminately brainwashing both civilians and guerrillas to support the US-backed movements. And like with the Canadian military campaign, it involved monitoring innocent people for their thoughts and beliefs while minimizing consideration of both basic human rights and the rule of law.
Lest we forget that Canadians were also victims of some of the most egregious brainwashing experimentation under the CIA-led MK-Ultra program to test various mind control methods, including LSD, sensory deprivation, and electroshock therapy, on unwitting Canadians at the Allan Memorial Institute in Montreal between 1957 and 1964.
We really have no idea how deep the rabbit hole goes with this recent revelation that Canadians were once again treated as experimental guinea pigs – this time in the interest of quashing critical thinking or dissent amid the pandemic. What we do see, however, it’s probably just the tip of the iceberg, and that its aim of creating a compliant citizenry has been successful.
More than three in four double-jabbed Canadians consider their unjabbed fellow citizens selfish and irresponsible, according to a new Leger poll. If they’re jabbed, and they have so much confidence in the jab preventing them getting ill, then what do they care what anyone else does? How much has the Canadian military and government propaganda played a role in shaping their views?
The whole truth about the extent of this psychological abuse of innocent Canadian civilians needs to come out – if only so the manipulated can see to what extent they were coerced into turning against their fellow citizens for simply making a different personal choice in what, after all, is supposed to still be a free and democratic country.
Rachel Marsden is a columnist, political strategist and host of an independently produced French-language program that airs on Sputnik France. Her website can be found at rachelmarsden.com
A listener writes in with a straightforward (but important) question: why do I use the term “scamdemic”? Here’s my (equally important and meticulously documented) answer!
The plan, devised by the Canadian Joint Operations Command, relied on propaganda techniques like those used during the Afghan war. What on earth is going on in the upper echelons of Ottawa?
High-up elements of the Canadian Forces have been waging psychological operations on the public over Covid-19 to manipulate their emotions and thoughts, and to gauge their reactions. While this is not uncommon around the world, getting caught is.
A new article in Canada’s National Post states that the Canadian Joint Operations Command used “propaganda techniques similar to those employed during the Afghanistan war” on the Canadian public.
The Post cites a December 2020 investigation by retired Major-General Daniel Gosselin, who was asked to look into it by then-Chief of the Defence Staff General Jon Vance.
According to the article, the federal government was innocent and not aware of the plan – a claim I find unbelievable, considering the amount of gaslighting and knowingly pointless regulations the government has subjected Canadians to since the start of the pandemic scare.
The plan involved “shaping” and “exploiting” information, the Post noted, to “head off civil disobedience by Canadians” and “bolster government messages about the pandemic.”
Among the stranger aspects was scaring Canadians with stories of a wolf invasion.
This, according to the Post, involved Canadian Forces’ military information operations staff forging a letter from the Nova Scotia government warning about wolves on the loose, in September 2020.
The Post claims the letter’s release was inadvertent, and basically ran with the Canadian Forces’ claim that this was down to a few bad apples, reservists who “lacked formal training and policies governing the use of propaganda techniques.”
Canadian journalist Dan Dicks, who was among the first to report on and analyze the wolves story, noted at the time that it was a classic example of a psychological operation.
Dicks has also pointed out what the National Post omitted, highlighting:
“They created a fake letter from the government saying there are dangerous wolves, and they set up loudspeakers in the area, projecting out wolf noises. This isn’t just research, this isn’t just a training exercise, they’re actively engaging in this psychological operation to scare people using loudspeakers.
‘Psyops’, he noted, is a term used “to denote any action which is practiced mainly by psychological methods with the aim of evoking a planned psychological reaction in other people,” and they are “aimed at influencing a target audience’s value system, belief system, emotions, motives, reasoning, or behaviour.”
Canadian journalist James Corbett likewise commented on this at the time, pointing out how a rumour is floated to see how the public reacts:
“This entire coordinated campaign to convince an entire public of a threat that doesn’t exist, in order to test how they will react to that, what will the public respond to and how will they respond? That really speaks volumes to the world we are living in. And you really think they are going to do all of that, but they are never going to use that for any nefarious purposes?”
An article in the Ottawa Citizen noted at the time that Canada’s Department of National Defence claimed: “The fake letter wasn’t meant to be released to the public and an investigation is underway to determine how that happened. The letter was an aid for the propaganda training.”
The department also claimed to not know why the loudspeaker was set up to transmit wolf sounds.
I guess a member of the public who read the letter must have taken it upon themselves to set up the loudspeaker then, hey?
The same Ottawa Citizen article cites Bard College professor Emma Briant, who specializes in researching military propaganda, calling the stunt a “major violation of ethics.”
UK “anti-masker” razor-blade poster hoax
The “shaping” and “exploiting” of information on Covid-19 to gauge and shape the public mood is, of course, not unique to Canada. To give another example, in May 2020, the UK Column obtained a leaked internal document of the Scientific Advisory Group for Emergencies (SAGE) from March 26, 2020, which advised:
“Use the media to increase the sense of personal threat. Use the media to increase the sense of responsibility of others. Use the media to promote positive messaging around actions. Tailor the messaging and use and promote social approval for desired behaviours.”
I recently spoke to UK-based journalist Iain Davis on a variety of issues pertaining to fear porn and media hype around the issue of Covid-19.
In our interview, Davis spoke of another hoax that appeared on the BBC last July: a Cardiff woman who claimed she had been cut by a razor blade allegedly stuck on the back of an ‘anti-mask’ poster.
What the BBC did not bother investigating was that the poster in question was laminated, thus stiff, and the razor blade stuck flat to the back of it, making it virtually impossible that the woman had actually cut herself.
“When you took it off the wall, it would have been like a card, not a piece of paper you could scrunch up, it would have been a stiff card,” David said.
Nor did the BBC question why she threw away the ‘evidence’ instead of turning it over to the police she had contacted. They didn’t look into her apparent history of outlandish and improbable claims, like being disemboweled and walking to hospital holding her intestines in, nor her admitted history of self-harming, lending credence to the likelihood she staged the sliced-hand photo.
While this story seemingly originated from an unstable individual, it was pushed unquestioningly by British state-owned media.
Further, as Davis noted, the nonsensical razor poster story re-emerged two months later, this time with London transport warning of “anti-mask posters with razor blades.”
In this story, the Rail, Maritime and Transport (RMT) union cited by the BBC actually said it wasn’t aware of any razor-blade incidents. Yet the BBC ran with the claims nonetheless (using the previous unstable person’s photo to support the claims).
These were not the first razor-blade poster stories, though. In 2020, the BBC and other media ran stories claiming razor blades (and needles) had been put behind anti-5G posters, again not providing any actual evidence to back the claims.
Anti-mask, anti-5G… and ‘razor-blade posters’. Clearly, this looks like another psyop to indoctrinate the public into equating people who have legitimate and science-based concerns about particular issues as being not only bat-s**t crazy, but dangerous, a menace to society.
But these stories are being cooked up in underhand ways by some powerful forces that shouldn’t be engaged in these matters, while the masses actually concerned about these issues are raising their concerns in peaceful manners: petitions, peaceful demonstrations, scientific papers… All that is easily obscured by a few tabloid stories with screaming headlines.
According to Davis, the point is “to seed the idea into the public imagination to associate people that question vaccines with extremism, ultimately with terrorism. There is a lineage going back quite a few years where you can see this narrative being seeded into the public consciousness. It has really ramped up in the last couple of months.”
Indeed, in November 2020, the Ottawa Citizenrevealed the Canadian Forces’ desire to “establish a new organization that will use propaganda and other techniques to try to influence the attitudes, beliefs and behaviours of Canadians,” noting they’ve already spent over $1 million to “train public affairs officers on behaviour modification techniques of the same sort used by the parent firm of Cambridge Analytica.”
While noting nominal opposition and concern by the defence minister, the Citizen reported that “work is already underway on some aspects of the plan and some techniques have been already tested on the Canadian public,” as well as that “a series of town halls were already conducted last week for a number of military personnel on the strategies contained in the draft plan.”
Dan Dicks, in his commentary on the wolves scare story, aptly opined, “It frustrates me so much that the government is actively trying to silence me as being ‘fake news’ or putting out ‘false information’, when they are actively engaged in propaganda campaigns to distribute false information designed to scare Canadians.”
Indeed, we who speak out on uncomfortable issues are censored, ostracized, and labeled as ‘conspiracy theorists’, while governments are actively spewing misinformation and manipulating the masses.
This week, the Australian Federal Health Minister announced a commitment to COVID-19 vaccines for kids aged 5 to 11 years pending TGA-approval, after Pfizer claimed, in a press release, that it had obtained “favourable” results.
Pfizer’s ongoing Phase 2/3 trial apparently showed the vaccine “was safe, well tolerated and showed robust neutralising antibody responses”. However, the results were not submitted to the drug regulator, nor were they published in a medical journal, so for now, we must take their word for it.
Pfizer registered the trial plan, showing that it tested a lower dose (10µg) as well as two higher doses (20µg and 30µg) in 5- to 11-year-olds. Whether the vaccine can provide protection against symptomatic disease or severe COVID-19 remains to be seen.
The manufacturer also claimed that the vaccine had a “favourable safety profile”, however, it is important to note that the trial has not enrolled enough children (2,268) to detect any rare but serious harms that might arise from the vaccine
Only healthy kids were recruited in the trial – children with known or suspected immunodeficiency, a history of autoimmune disease, any condition associated with prolonged bleeding, anyone receiving treatment with immunosuppressive therapy or corticosteroids were excluded from the trial.
Notably, these are the same cohort of children who have been prioritised for the vaccine.
Despite little to no data available for its safety and efficacy, the Israeli Ministry of Health gave the green light to start vaccinating high risk 5- to 11-year olds with the lower-dose (10µg) of the vaccine.
Pfizer senior vice-president Dr Bill Gruber said he felt “a great sense of urgency” in the process, and Pfizer’s CEO Albert Bourla said trial data would be submitted to the various international drug regulators for “immediate authorisation.”
The language of Pfizer executives, the frenzied press coverage, and the political will of Governments, is all designed to pressure drug agencies to fast-track authorisations.
Younger than 5 years old?
Pfizer announced that trial data involving children under 5 are expected later this year.
Last week, Cuba began vaccinating toddlers as young as 2, using its homegrown vaccine, the Soberana 02, from the Finlay Vaccine Institute administered at adult doses. To my knowledge, there has been no data from Phase III trials published in the peer-reviewed literature in children as young as 2 with this vaccine.
China’s drug agency has cleared three COVID-19 vaccines produced by Sinopharm and Sinovac and is vaccinating children aged 3 years and older, under emergency use authorisation.
12- to 15-year-olds
Most major western nations have authorised COVID-19 vaccines for those aged 12 years and older.
In Australia for example, children aged 12 to 15 years began receiving the mRNA vaccines last week. According to the NSW Premier, 20% of children in the state of NSW have already had their first jab.
They require a two-dose regimen, the same dose given to adults, which aligns with the US FDA and Health Canada advisories on vaccines for this age group. (See my previous analysis for 12-15yr olds)
This does not align with the UK’s more cautious approach. After significant political and media pressure, UK chief medical officers recommended a single dose of the Pfizer vaccine, because of concerns about rare side effects such as heart inflammation.
Brazil appears to be an outlier at the moment. It was reported that the Minister for Health called for the suspension of the COVID-19 immunisation of people aged 12 to 17 after the death of a 16-year old girl named Isabelli Borges Valentim, eight days after she received the Pfizer shot. Authorities are still investigating the incident but the drug regulator denies any link to the vaccine.
Myocarditis/Pericarditis
This issue has stirred up some heated debate.
Now that real world data is becoming widely available, myocarditis (inflammation of the heart muscle) and pericarditis (inflammation of the membrane surrounding the heart) are being reported as rare harms related to the Pfizer & Moderna mRNA vaccines.
Israel, because of its fast vaccine roll-out, was first to raise the alarm – 148 cases of myocarditis were reported within 30 days of immunisation, more commonly after the second jab. It prompted the Israeli Ministry of Health to launch an investigation into any possible link between these cases of myocarditis and vaccination.
Since then, other countries such as the UK, the US and Canada have corroborating data.
In June, the US FDA decided that the link between the mRNA vaccines and myocarditis, particularly in young males, was sufficiently clear that it revised its vaccine fact sheets to include a warning.
The CDC released data showing the incidence of “expected” versus “observed” incidences of myocarditis and pericarditis and found a significant increase in the observed rates. The graph shows the higher rates in red (see table numbers circled in red).
Another study, published in JAMA which looked at data from 40 hospitals in the US showed a similar pattern to the CDC, although at higher incidences, suggesting that the vaccine’s adverse events were being underreported.
Researchers then took a more granular look at the database for reported adverse events (VAERS database) between 1 January and 18 June, and found boys aged 12-15 years vaccinated with their second shot of the mRNA vaccine, with no underlying medical conditions were 4 to 6 times more likely to develop a cardiac adverse event, than ending up in hospital with COVID-19.
The study was published as a pre-print online but it ignited a twitter storm, with critics claiming the study ‘over-estimated’ the risk and it was biased because one of the authors belonged to a group that did not support making vaccines compulsory.
Sceptics say that most of the myocarditis cases are mild, and that children recover quickly from hospitalisation. Others are not so quick to dismiss the potential risk of ‘sub-clinical disease’ (myocarditis without symptoms) in children.
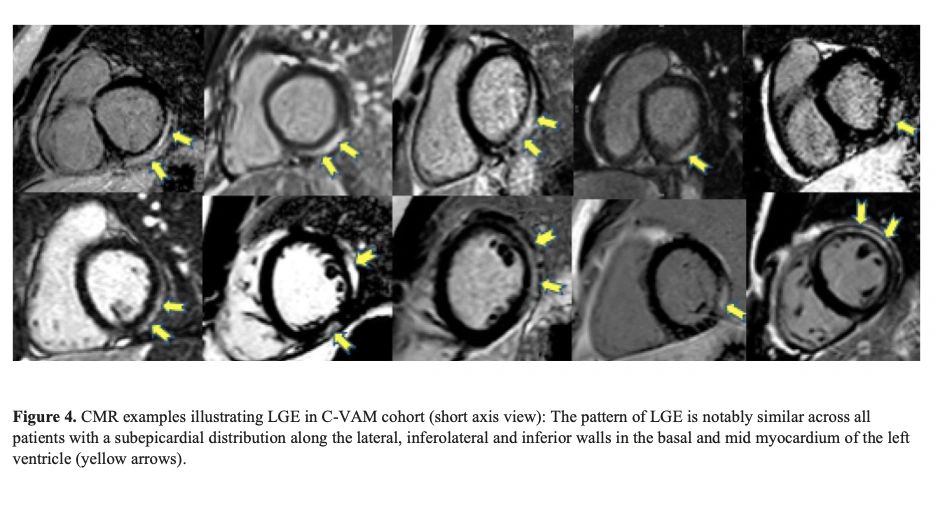
Notably, a retrospective multi-centre study across 16 US hospitals including patients <21 years of age with a diagnosis of myocarditis following COVID-19 vaccination, found concerning abnormalities in heart tissue (the left ventricle) (See image with yellow arrows).
Jain SS, et al doi: 10.1542/peds.2021-053427.
Careful monitoring is required to see if these abnormalities lead to fibrosis, which can have long-term implications for young patients.
Early findings suggest that post-vaccination myocarditis could be mediated by the toxicity of ‘spike protein’ on heart muscle cells or from circulating spike proteins in plasma after vaccination.
The risk of myocarditis associated with contracting COVID-19 infection may be higher than that after vaccination, but more research is needed to weigh harms against benefit.
If we don’t vaccinate kids, what about long COVID?
The fear of long-COVID has been a major impetus behind vaccinating kids.
A recent review by Monash University, analysing 14 international studies on long COVID in children and adolescents, found no difference in the symptoms reported by those who had experienced COVID-19 and those who had not.
Lead researcher on the study, Professor Nigel Curtis told newsGP the review’s findings should be reassuring for parents and carers.
Similarly, a webinar hosted by The BMJ revealed the results of the largest citizen-scientist participation study to date in young children. It used a smartphone app to monitor the illness and symptoms of children after testing positive to COVID-19.
The researchers found that the median duration of illness was 6 days. Only 4.4% of children had illness duration >28 days and 1.8% had symptoms >56 days. Encouragingly, their symptom ‘burden’ was greatly reduced by this time (none became worse) with the most common symptoms being headache and fatigue.
The researchers looked at neurological symptoms such as epileptic seizures, convulsions, impaired attention and concentration, but none were reported.
Lead investigator on the study, Prof Emma Duncan from Kings College in London concluded “Long illness duration of COVID-19 in children is uncommon.”
Vaccine Mandates for kids
Despite COVID-19 vaccine mandates for teachers in places such as New York and Australia (Victoria and New South Wales), no Federal government has announced plans to make the vaccines compulsory for children (yet).
Canadian and English professors have argued that making COVID-19 vaccines mandatory for children, will “encourage uptake”.
U.S. Surgeon General Vivek Murthy has also suggested that COVID-19 vaccine mandates for students could happen at the state and local level in the US, once they have been approved for paediatric use by the US FDA.
In a surprise announcement this week, the Los Angeles public school system said students aged 12 and older will now have to be double-vaccinated by the end of the year, to attend classes on campus or take part in sports and other extracurricular activities. It remains to be seen whether other school districts will follow.
Consent from kids
Before the age of 14, minors are generally thought to lack the cognitive capacity and maturity to make rational judgments about their health.
In fact, most US state laws presume that minors lack medical decision-making capacity and therefore require parental consent for most health care decisions, including vaccination, with some exceptions.
However, in the case of COVID-19, under what is termed ‘Gillick competency’, those under 16 years can make independent decisions about a medical treatment if they can demonstrate they have the capacity to consent, even if their parent withholds consent.
This applies to every Australian state and territory as part of the ‘common law’ and in the UK.
The Victorian government has produced ‘communication packs’ for teachers and educators on how to ‘promote’ COVID-19 vaccines to minors.
Hopefully, the conversations about COVID-19 vaccines, between health professionals and minors, are conducted without coercion, pressure or judgment.
Not surprisingly, this has raised the age-old question about who is better placed to determine the best medical treatment for a child – a parent or a Government minister?
The debate will continue and experts will need to wade through muddy waters to find a balance between protecting children’s health and the uncertainty over the long-term harms of the vaccine.
Between 29 November and 1 December 2021, member states are meeting in a special session with the World Health Organisation to discuss, possibly sign, a new treaty on pandemic preparedness and response.
This decision was taken in March 2021 and backed by 26 nations, among which Australia, Canada, Iceland, Norway, Republic of Korea, South Africa, Ukraine, United Kingdom, United States, Uruguay and Member States of the European Union.1
To be noted is the absence of Russia, China, and India among these 26.
The International Health Regulations (2005)[i] signed by 196 countries already provide States the legal right to:
“– review travel history in affected areas;
– review proof of medical examination and any laboratory analysis;
– require medical examinations;
– review proof of vaccination or other prophylaxis;
– require vaccination or other prophylaxis;
– place suspect persons under public health observation;
– implement quarantine or other health measures for suspect persons;
– implement isolation and treatment where necessary of affected persons;
– implement tracing of contacts of suspect or affected persons;
– refuse entry of suspect and affected persons;
– refuse entry of unaffected persons to affected areas; and
– implement exit screening and/or restrictions on persons from affected areas.”
In other words, all the measures applied round the world since 2020, including mandatory vaccination, are in effect legal under this former treaty.
In particular, it critically changes the definition of “quarantine” from that in the 1969 IHR. There, it is used only in the expression “in quarantine” defined to be a “state or condition during which measures are applied by a health authority to a … means of transport or container, to prevent the spread of disease, reservoirs of disease or vectors of disease from the object of quarantine”.[i]
The 2005 revised IHR use the term by itself, and define it as “the restriction of activities and/or separation from others of suspect persons who are not ill or of suspect baggage, containers, conveyances or goods in such a manner as to prevent the possible spread of infection or contamination”.
This represents a subtle but critical shift from protection of the community to restriction of individual liberties.
The implementation of quarantine and other coercive measures on all, including surveillance and vaccination, is legalized: the expression “suspect persons” criminalizes every individual, both healthy and unhealthy.
Indeed, it covers anyone “considered by a State Party as having been exposed, or possibly exposed, to a public health risk and that could be a possible source of spread of disease”. Of significance is the use of “possibly” and “possible”, hence not just anyone definitely known to be a risk factor.
So Why The Need For A New Treaty?
The answer was given by WHO Director-General Tedros Adhanom Ghebreyesus. “It’s the one major change, Tedros said, that would do the most to boost global health security and also empower the World Health Organization.”[i]
The 2005 revised IHR still leave some authority to States and require certain conditions for a health event in a particular State to be considered sufficiently serious globally for the State to be forced to communicate it to WHO. Once communicated, it becomes the prerogative of the director general of WHO to determine whether it “constitutes a public health emergency”, but in collaboration with that particular State.
Although it should be added that in case of disagreement, the director general decides after consultation with the emergency committee of WHO, and passed a certain period no State can reject or emit reservations about the IHR or any later amendments. Still, to some extent, measures implemented remain the result of a dialogue between “IHR focal points” in each country and “WHO IHR contact points”.
What is particularly important is that the above listed measures, although rendered legal by the IHR, can under this treaty, only be recommended by the WHO, not imposed, and that it is up to the States to proceed towards their imposition, and to verify they are followed by means already existing in their respective countries.[ii]
The new treaty would address the above “weaknesses” of the IHR as they are considered to be, by ensuring “independent verification, monitoring, and compliance”. Given the clearly expressed end of empowering the WHO, should one conclude that “independent” means under the authority of WHO rather than the States themselves?[i]
Further the IHR cover “public health hazards and public health emergencies of international concern”, whereas the treaty will concern “all hazards”, not just pandemics. In the latter case, it would take over from the IHR once a pandemic is officially declared by the WHO.[ii]
This said, the treaty would presumably also make clear the idea expressed in the 2007 CDC “Interim Pre-pandemic planning guidance”,[i] namely overruling the need of a pandemic to implement restrictive measures. All that would be needed would be for an event to be declared a “public health emergency of pandemic potential”.
Given that any future event is always hypothetical, does this enable the maintenance of the measures for an indeterminate period? For it can always be claimed that a pandemic will occur especially were the measures lifted. This raises many questions, all the more so as the event would no long need to be of “international concern as in the current IHR”. “Measures”, as advised, should also go beyond the current scope of IHR”, in particular to cover the production and supply of vaccines, diagnostics, and treatments”.[ii]
The treaty would unlike the IHR also go beyond sanitary issues and allow the implementation of measures against “social and economic disruptions” as well as “broader disaster risk”.[i]
Would this in effect not only make it legal to put an end to criticisms, and thus to the freedom of expression, and make it possible to control any public antagonism against restrictive measures through “urgent international assistance”,[ii] namely not just by national police or military forces, but international ones?
In short, would the treaty not provide the international legal framework for derogation from the civil and political rights guaranteed “even in time of emergency threatening the life of the nation” by The Syracuse Principles on the Limitation and Derogation Provisions in the International Covenant on Civil and Political Rights drafted in 1984,[iii] namely:
“the right to life; freedom from torture, cruel, inhuman or degrading treatment or punishment, and from medical or scientific experimentation without free consent; freedom from slavery or involuntary servitude; the right not be be imprisoned for contractual debt; the right not to be convicted or sentenced to a heavier penalty by virtue of retroactive criminal legislation; the right to recognition as a person before the law; and freedom of thought, conscience and religion. These rights are not derogable under any conditions even for the asserted purpose of preserving the life of the nation”?
For the Syracuse Principles only ensure that “No state party shall” in any circumstance “derogate from the Covenant’s” above guarantees”. However, according to the new treaty, would the WHO, possibly together with the help of other international bodies, not become an occupying planetary power, with each State a collaborating subservient unit, like France in 1940, and hence without any power to ensure that non-derogable rights are protected?
Last but not least, “[t]rying to revise the IHR would be a long process and take several years. … In addition, any amendment made to the IHR will enter into force only two years after its adoption. A world in crisis cannot afford to wait this long.”[i] Why such a rush to get the treaty ratified?
It should not be forgotten that among the main contributors of WHO are the Bill and Melinda Gates foundation and the vaccine alliance (GAVI). It established in 2000 and whose initial funding it essentially provided – a “unique public-private partnership … bring[ing] together key UN agencies, governments, the vaccine industry, private sector and civil society”.[i]
Through the introduction of the ICU and Critical Care Ward, hospitals have been subverted by cold, calculating technicians who do not care about individual patients. **TO SUPPORT MY WORK PLEASE CLICK HERE: https://amazingpolly.net/contact-support.php THANK YOU ** read more…
Video is in 4 parts;
Part 1: My takedown of “Trusted Voice” of the Pandemic, Michael Warner.
Part 2: What is an Intensivist and how have they ruined Hospitals?
Part 3: The history of Critical Care – some shady characters emerge in the wake of WW2.
Part 4: Who benefits from this? Who forced the hiring of Intensivists in thousands of hospitals? Is this part of a darker agenda of population control and eugenics?
By Kit Klarenberg | Mint Press News | January 28, 2025
Ever since Tel Aviv’s 1948 creation, much has been said and written about ‘Greater Israel’ – the notion Zionism’s ultimate end goal is the forcible annexation and ethnic cleansing of vast swaths of Arab and Muslim lands for Jewish settlement, based on Biblical claims this territory was promised to Jews by God. The mainstream media typically dismisses this concept as antisemitic conspiracy theory, or at most the fringe fantasy of a minuscule handful of extremist Israelis.
This site is provided as a research and reference tool. Although we make every reasonable effort to ensure that the information and data provided at this site are useful, accurate, and current, we cannot guarantee that the information and data provided here will be error-free. By using this site, you assume all responsibility for and risk arising from your use of and reliance upon the contents of this site.
This site and the information available through it do not, and are not intended to constitute legal advice. Should you require legal advice, you should consult your own attorney.
Nothing within this site or linked to by this site constitutes investment advice or medical advice.
Materials accessible from or added to this site by third parties, such as comments posted, are strictly the responsibility of the third party who added such materials or made them accessible and we neither endorse nor undertake to control, monitor, edit or assume responsibility for any such third-party material.
The posting of stories, commentaries, reports, documents and links (embedded or otherwise) on this site does not in any way, shape or form, implied or otherwise, necessarily express or suggest endorsement or support of any of such posted material or parts therein.
The word “alleged” is deemed to occur before the word “fraud.” Since the rule of law still applies. To peasants, at least.
Fair Use
This site contains copyrighted material the use of which has not always been specifically authorized by the copyright owner. We are making such material available in our efforts to advance understanding of environmental, political, human rights, economic, democracy, scientific, and social justice issues, etc. We believe this constitutes a ‘fair use’ of any such copyrighted material as provided for in section 107 of the US Copyright Law. In accordance with Title 17 U.S.C. Section 107, the material on this site is distributed without profit to those who have expressed a prior interest in receiving the included information for research and educational purposes. For more info go to: http://www.law.cornell.edu/uscode/17/107.shtml. If you wish to use copyrighted material from this site for purposes of your own that go beyond ‘fair use’, you must obtain permission from the copyright owner.
DMCA Contact
This is information for anyone that wishes to challenge our “fair use” of copyrighted material.
If you are a legal copyright holder or a designated agent for such and you believe that content residing on or accessible through our website infringes a copyright and falls outside the boundaries of “Fair Use”, please send a notice of infringement by contacting atheonews@gmail.com.
We will respond and take necessary action immediately.
If notice is given of an alleged copyright violation we will act expeditiously to remove or disable access to the material(s) in question.
All 3rd party material posted on this website is copyright the respective owners / authors. Aletho News makes no claim of copyright on such material.