Dr. Malone Versus The World: Why Is He At War With Everyone?

Vigilant News Network | December 28, 2023
Dr. Malone’s latest Substack just dropped. Once again, the theme of the blog post is that a series of people and organizations within the medical freedom movement are actively working against him.
The pioneer in mRNA vaccine technology seems to have a pattern of lashing out against anyone who levels the slightest criticism of him and has attempted to diminish his critics by claiming that they “appear to be getting compensated in some way for actively promoting hate.”
It is clear, though, that what Dr. Malone describes as “hate” can run the gamut from indifference or perceived slights to mild criticism — or a stark difference of opinion. Dr. Malone’s volatile responses to criticisms have led some to think that he is connecting dots against his critics that aren’t real.
Dr. Malone’s Naughty List

Image via NTD News
Dr. Malone’s limited tolerance for criticism, along with his emphatic responses, has led to an increasing number of individuals and organizations subjected to his public denunciation.
The list below, derived from Dr. Malone’s past X and Substack posts, details these entities:
• Dr. Peter Breggin and Ginger Breggin
• Dr. Mike Yeadon
• Sasha Latypova
• Karen Kingston
• Matthew Crawford
• Dr. Ben Marble
• Dr. Judy Mikovitz
• George Webb
• Sage Hana on Substack
• America Out Loud
• Dr. Jane Ruby
• Red Voice Media
• Stew Peters
• Catherine Austin Fitts (The Solari Report)
• J. J. Couey
• Mary Holland (President of Children’s Health Defense)
• The Wellness Company and its founder Foster Coulson
• Dr. Paul Alexander
• The Washington Post
• Alex Berenson
• Dr. Peter McCullough
• And more. “The list goes on and on,” Dr. Malone has stated.
Lawsuits
On October 30, 2022, Dr. Malone filed a lawsuit seeking $25 million in damages from Dr. Peter Breggin, Ginger Breggin, America Out Loud, Dr. Jane Ruby, and Red Voice Media (Stew Peters). This was described as a “shocking defamation lawsuit,” which Diana West called “an anti-personnel weapon of free-speech-destruction” and a “heat-seeking lawfare missile targeting financial ruin.”
 After a lengthy legal battle, Judge Norman K. Moon dismissed Dr. Malone’s $25 million defamation lawsuit on December 11, 2023, stating it “has not met his burden of proof as to jurisdiction.”
After a lengthy legal battle, Judge Norman K. Moon dismissed Dr. Malone’s $25 million defamation lawsuit on December 11, 2023, stating it “has not met his burden of proof as to jurisdiction.”
In a separate case, On September 28, 2023, Judge Norman K. Moon also struck down Dr. Malone’s defamation lawsuit against The Washington Post. Judge Moon directed the court clerk to “strike this case from the docket.” He said at the time, “If Plaintiff [Dr. Malone] continues to bring defamation actions like those that have been dismissed, there will come a time when his lawsuits might fairly be deemed frivolous and awarding attorney fees is appropriate.”
Dr. Malone vs. Dr. Yeadon
 Dr. Michael Yeadon
Dr. Michael Yeadon

In response to Dr. Malone’s op-ed, “FDA Fails to Address DNA Adulteration Concerns,” Dr. Michael Yeadon, ex-chief scientist and vice president of Pfizer’s allergy and respiratory research division, also found himself on the wrong side of Dr. Malone.
Dr. Yeadon wrote:
“He [Dr. Malone] knows these aren’t regulated pharmaceutical products at all but countermeasures under a public health emergency. It’s not a side issue. For proof, see Substacks of Katherine Watt and Sasha Latypova. There is zero possibility that Malone doesn’t know this.”
Rather abrasively, Dr. Malone responded that Dr. Yeadon “does not understand what is going on” and that he “should just STFU (shut the f*ck up).”
 Former pharma insider Sasha Latypova replied:
Former pharma insider Sasha Latypova replied:

Image Source
“I think Dr. Yeadon understands very well what is going on, and think he understands too well for Robert Malone’s liking, and that’s why the response full of, let’s say – hate and hyperbole – but no actual rebuttal or an explanation of what exactly is incorrect.”
Read more on that here.
Dr. Malone’s Grudge Extends to Dr. Peter McCullough.

Dr. Peter McCullough
Dr. Malone once spoke of renowned cardiologist Dr. Peter McCullough as “a good friend.” However, it seems that the passage of time has altered the dynamics of their relationship, especially after Dr. McCullough accepted the position of Chief Scientific Officer of The Wellness Company, a business specializing in alternative healthcare solutions that Dr. Malone suggests is “yet another CIA cutout organization.”
 Dr. McCullough has refrained from engaging in public criticism of Dr. Malone on social media platforms like X. Conversely, Dr. Malone has, on multiple occasions, publicly scorned Dr. McCullough.
Dr. McCullough has refrained from engaging in public criticism of Dr. Malone on social media platforms like X. Conversely, Dr. Malone has, on multiple occasions, publicly scorned Dr. McCullough.
In June 2023, Dr. Robert Malone expressed disappointment over a perceived bias at Senator Ron Johnson’s “COVID-19 Vaccines: What They Are, How They Work, and Possible Causes of Injuries” event, which Dr. McCullough helped organize. Malone indicated a division between McCullough and himself, noting that they are “no longer on the same team.” Malone also accused McCullough of prioritizing profits over people, stating, “He [McCullough] works for ‘The Wellness Company’ selling vitamins. I work for my substack subscribers.”
 On November 25, 2023, Dr. Malone stated that he and Dr. McCullough no longer attend the same venues. He referenced an instance where he received a standing ovation at a conference, and McCullough did not, which he suggested led to jealousy.
On November 25, 2023, Dr. Malone stated that he and Dr. McCullough no longer attend the same venues. He referenced an instance where he received a standing ovation at a conference, and McCullough did not, which he suggested led to jealousy.
He further alleged that Dr. McCullough compensates someone to attack him on social media and accused Dr. Paul Alexander of acting as Dr. McCullough’s “surrogate” to “obsessively” attack him “hundreds of times.”
 Furthermore, Dr. Malone paradoxically seemed to harbor hopes that the FDA, an agency he has consistently accused of corruption, would take stringent action against The Wellness Company:
Furthermore, Dr. Malone paradoxically seemed to harbor hopes that the FDA, an agency he has consistently accused of corruption, would take stringent action against The Wellness Company:
“These [supplements] are mislabeled as therapeutics. Peter [McCullough] know[s] this but will not act to object. Eventually, they will get called out by the FDA. Surprising, this has not happened yet.”
 Who Is Defaming Who?
Who Is Defaming Who?
Dr. Malone says, “I am constantly amazed by the self-styled social media ‘independent journalists’ who obsessively attack me” while having a long history of obsessively attacking others.
 There’s a saying that what goes around comes around. However, Dr. Malone characterizes what is likely an organic backlash to his own degrading statements as “compensated” attacks or “yet another CIA cutout organization” looking to cause division in the medical freedom movement.
There’s a saying that what goes around comes around. However, Dr. Malone characterizes what is likely an organic backlash to his own degrading statements as “compensated” attacks or “yet another CIA cutout organization” looking to cause division in the medical freedom movement.
It’s time for Dr. Malone to reflect and take a look in the mirror. He sought $25 million in legal damages for “defamation” while issuing disparaging comments to those who dared criticize him.
Dr. Malone, a line must be drawn. You have done better, and you can do better. The world wants a return to the principled physician who courageously opposed vaccine mandates and the use of experimental gene-based products in children, rather than the one persistently embroiled in drama. Please choose a path of greater dignity and resolve these online disputes with grace.
 EDITORIAL NOTES:
EDITORIAL NOTES:
• Vigilant News Network reached out to Dr. Malone for comment regarding allegations made in his Substack and online, but Dr. Malone declined to respond.
• The founder of Vigilant News Network, Foster Coulson, is also the founder of The Wellness Company. Coulson has no control over the day-to-day operation of Vigilant News. The decision to run this article – an article we have worked on for over a month and an article that has been subjected to our rigorous journalistic standards – was 100% the decision of the news division for Vigilant News Network.
This post is sponsored content and Zerohedge has been compensated for its publication.
New FOIA’ed Data Reveal NY Vaccine Clinics Called Ambulances To Be “On Standby”
Data reveal a shocking number of vaccine emergency calls as well
BY PIERRE KORY, MD, MPA | DECEMBER 27, 2023
Right before the recent Christmas holiday, I received a call from a friend and colleague named Louis Conte regarding a “contact” of his with knowledge of the inner workings of Emergency Medical Services in Westchester County, New York.
Louis’s contact had been monitoring EMS dispatches in Westchester County and saw, subsequent to the jab rollout in early 2021, what he felt was a frightening number of calls from vaccine clinics or homes where general or specific “vaccine reactions” were cited as the cause of the need for an ambulance.
Last year, the contact decided to submit a FOIL (Freedom of Information Law) request—similar to a FOIA—to the Westchester County EMS (and the adjoining Dutchess County EMS) asking for a record of all calls whose transcripts mentioned either the word “vaccine” or “Covid-19 vaccine” in 2021.
Louis asked me to look at the documents. As difficult as it is at this point to further distress me with data on the toxicity and lethality of the mRNA platform, this dataset still managed to do this.
Before I review the data, let’s review what we know about ambulance calls timed with the roll-out of the vaccination campaign, because this issue is NOT new.
For instance, we already know from ICAN and Aaron Siri’s FOIA request of the CDC’s V-Safe data that 7.9% of all 10.1 million vaccine recipients reported requiring medical care to treat a vaccine adverse effect. Of those requiring medical care, almost 11% (87,700 people) visited the emergency room or hospital. How many travelled for this high level of urgent /emergent care by ambulance is unknown, but historically, about 15% of ER patients arrive by ambulance, so this would come out to about 13,000 patients among a population of 10 million vaccinated.
Further, an article published in the journal Nature reported:
- There was an increase of more than 25% in the number of ambulance calls in response to cardiac arrests (CA) and acute coronary syndromes (ACS or “heart attacks”) for young people in the 16–39 age group during the COVID-19 vaccination rollout in Israel (January–May, 2021) compared with the same period of time in prior years (2019 and 2020).
- They also found a robust and statistically significant association between the weekly CA and ACS call counts and the rates of 1st and 2nd vaccine doses administered to this age group. Note they found no observed statistically significant association between COVID-19 infection rates and the CA and ACS call counts.
- They report that their findings aligned with previous studies showing that increases in overall CA incidence were not always associated with higher COVID-19 infection rates at a population level, and that the stability of hospitalization rates related to myocardial infarction throughout the initial COVID-19 wave compared to pre-pandemic baselines in Israel.
- Their findings above also mirrored reports of increased emergency department visits with cardiovascular complaints during the vaccination rollout in Germany as well as increased EMS calls for cardiac incidents in Scotland.
In line with the above, anecdotal data from social media described the following:
The import of the above data/anecdotes was further supported by new, massive demands for ambulances across the world, evidenced by this compilation of TV news and print reports of shortages, compiled in another favorite substack of mine by Marc Crispin Miller. Note that although some reports blame the issue on shortages of staff and ambulance parts, the vast majority also mention… increases in the number of calls for ambulances.
And then there’s even more anecdotal data by someone who has earned my deep trust in regards to accuracy of events on the “inside of the system” (recall she is a nurse colleague of mine that works at a major academic medical center who I referred to as “My Spy On The Inside” [MSOTI] in my prior multi-part series of posts called “Nursing Reports From the Front Lines of The Vaccine Catastrophe”).
During one of her shifts referring to the ambulance/emergency services issue:

So, with the above publications and observations in mind, let’s review this new “data dump.” Maybe what it reveals is not as statistically damning as what the New Zealand Whistleblower exposed but you will see that it is equally, if not even more alarming. To me, the most shocking discovery I made when reviewing the documents, is that I found evidence of 5 different occasions where calls were made to Westchester County EMS dispatch to have ambulances “on standby”:
1. 2021-02-21 07:38:16.000 E2105940 NOTIF EMS 355 PELHAM RD NE _ROCHELLE: @WILLOW TOWERS NEW_ROCHELLE ‘WILL BE ADMINISTERING THE COVID-19 VACCINE TODAY TO 220 PEOPLE’
2. 2021-03-20 08:19:58.000 E2108926 STAND-BY EMS 210 N BROADWAY SLEEPY HOLOW: @HIGH SCHOOL- SLEEPY HOLLOW “‘73B2 & 36M3 ON STANDBY FOR VACCINE DETAIL
3. 2021-03-20 08:46:43.000 E2108930 STAND-BY EMS 168 W BOSTON POST RD MAMARONECK_V : @STT HOMAS EPISCOPALC HURCH MAMARONECK_V “‘VACCINE STANDBY UNTIL APPROX 1300HRS’
4. 2021-05-20 09:07:15.000 E2115997 STAND-BY EMS 950 PALMER A MAMARONECK_V: @MAMARONECK HIGH SCHOOL-PALMER AVE MAMARONECK_V “‘EMS STAND-BY FOR VACCINE CLINIC
5. 2021-05-20 14:09:41.000 E2116032 ALS 950 PALMER AVE MAMAR @MAMARONECK HIGH SCHOOL-PALMER AVE SIDE MAMARONEC _V “‘EMS STANDBY FOR VACCINE CLINIC
Are you kidding me? Employees at vaccine clinics in Westchester County, as early as Feb 21, 2021, were calling EMS “to be on standby?” For “vaccine detail?” One caller informed EMS dispatch that they “will be administering vaccines to 220 people today?” Note they did that as early as February 21, 2021. That is how fast some front-line workers knew how dangerous the vaccines were.
Also note how, on 5/20/21, two calls from the Mamaroneck High School clinic asked for ambulances to be on standby, the first call was made at 9:07 AM and a later one was made at 2:09 PM. For a “safe and effective” vaccine?
Again, calls with requests of this nature were being made from clinics in New Rochelle, Sleepy Hollow, and two different ones in Mamaroneck? If I was living in Westchester County at the time, I damn well would have wanted to know these calls were being made (as an aside, I lived in that county from 2008-2015 and still have lots of friends with children there).
My sense is that these calls were made by employees who were secretly, or at least, somewhat anonymously, trying to alert authorities as to how dangerous the vaccines were but without doing so in a way that would make them a target as an “anti-vaxxer” or cause them to lose their job. They were clearly smart enough to know the consequences of a more public call-out of vaccine toxicity. So instead, they called EMS to have them “on standby.” Although the attempt was well-intentioned, should they be absolved of responsibility for any subsequent injuries which occurred on their watch at that clinic? They were actively injecting people with an experimental vaccine… after calling EMS to have them “on standby”?
After I shared this article with A Midwestern Doctor, he sent me this commentary:
One of the biggest challenges people have had throughout the vaccine rollout has been coming to terms with the fact that so many people could have been complicit in letting a bad vaccine be pushed on the world (which hence leads many of them to believe the only possible explanation is that the vaccine was not in fact dangerous).
Sadly, I’ve seen numerous tragic cases of the same thing that has happened in the past. Much of this is explained by an effect in psychology known as the bystander effect:
The bystander effect occurs when the presence of others discourages an individual from intervening in an emergency situation, against a bully, or during an assault or other crime. The greater the number of bystanders, the less likely it is for any one of them to provide help to a person in distress. People are more likely to take action in a crisis when there are few or no other witnesses present.
In turn, throughout my life, I’ve found that if something is happening I know is wrong and no one is speaking out about it (e.g., because its not politically correct to do so), I can reliably predict that if I don’t speak out against it, no one will. So for this reason, I often “break” the bystander effect (once one person speaks out, others will often feel safe to do so as well) as I know otherwise it won’t happen. Likewise, I’ve seen this same thing occur again and again within organizations, especially when people’s financial livelihoods are on the line for speaking out.
One of the best illustrations of the point Kory is making here can be found within the data of vaccination deaths leaked by the brave New Zealand whistleblower Barry Young (who now faces a seven year prison sentence for his leaking). Within that data, Young noticed that there were about a dozen vaccinating doctors and a dozen vaccination sites which had a very high rate of deaths in those they vaccinated.

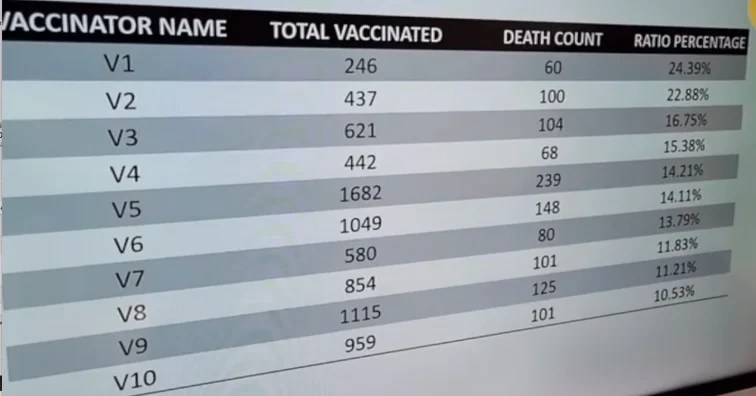
Barry, in turn, raised a very simple question—how could something like this happen?
Sadly, as this summary of EMS calls shows, the bystander effect can be a very real thing, especially when everyone else in a large institution going along with something makes those who want to challenge it feel even more powerless to speak out.
I believe the vaccine clinic employees who called EMS in Westchester should get some credit for, in my interpretation, trying to blow a whistle, but they did so too “softly.” Instead, as per the bystander effect, they simply hoped that “someone else,” i.e. EMS personnel or leadership would take note of these calls, and “do something” about them.
Remember, May 2021 (the day of the two calls from Mamaroneck High School) was nearing the height of the global “psy-ops” propaganda campaign where the unvaccinated and/or the vaccine hesitant were demonized and attacked widely across all mainstream media and social media. Even those who already got the vaccine and were trying to share the horrible stuff happening to them were being attacked. Never, ever forget that occurred, and more importantly, never forget just how successful that propaganda was. So, while I get the clinic employee’s hesitation, I cannot forgive their ultimate behavior.
Walking off the job would have been another option, but if there is anything I have learned in Covid and the immense, multi-faceted fraud that has occurred and keeps occurring, is that there were and are far too few real whistleblowers. The desire to remain employed is paramount to the concern for the welfare of others. Period.
Anyway, these data points above are beyond shocking, even to me at this point in my research journey. If anyone has a different or more benign interpretation of these five EMS transcripts above than I do, I am all ears. If I find such an interpretation more compelling or corrective, I will do a follow-up post.
Now, let’s review the rest of the transcripts from EMS dispatch. One set of data is from Westchester County EMS. First, know that Westchester County has a population of about 1 million, but these EMS calls do not include the City of Yonkers which has a population of about 200,000. So, for 800,000 people, the total EMS calls which specifically mentioned the vaccine as a cause of distress in 2021 was 165 calls. For Dutchess County, population of 295,000, the number of calls was an almost equally proportionate 55 calls.
However, these 220 calls across these two counties likely represent a small subset of the severe, ambulance requiring vaccine reactions because sudden death was likely never reported as a vaccine reaction and many people calling ambulances may not have initially related their medical issue with the vaccine or, even if suspected, may not have mentioned it to dispatch – thus, this dataset represents only the most tightly “temporally associated” events, ones where it was more than 100% obvious the vaccine was causative, like when it happened within minutes or hours or 1-2 days of the vaccine being administered.
What was the nature of these “reactions” which triggered calls for an ambulance? Well, from the transcript log posted at the end of this post, most simply say “reaction to Covid-19 vaccine” or “vaccine reaction” but there are also many disturbingly detailed reactions such as seizures, inability to ambulate, unresponsiveness, altered mental status, etc.
I list the more specific and disturbing ones below (or you can also just read through the actual EMS transcripts that are at the end of this post):
- 2-16-21 92 YO F abnormal breathing from 2nd covid-19 vaccine
- 2-17-21 69 YO M unable to ambulate secondary to covid vaccine
- 2-21-21 73 YO unable to ambulate, reaction to Covid-19 vaccine
- 2-17-21 female reaction to vaccine – altered mental status (AMS)
- 2-22-21 88 YO F low oxygen saturation, possible reaction to Covid vaccine
- 3-10-21 unresponsive, reaction to vaccine
- 3-19-21 fever and confusion post covid vaccine
- 3-27-21 56 YO M cancer patient possible reaction to vaccine, altered mental status (AMS)
- 3-27-21 2nd vaccine, sudden hypertension (HTN), back and abdominal pain
- 4-2-21 46 YO M disoriented, recent covid vaccine
- 3-24-21 56 YO F abnormal breathing from 2nd Covid vaccine
- 6-18-21 12 YO F experiencing chest pain after 2nd vaccine
- 7-11-21 13 YO F feeling weak, reaction to vaccine
- 4-7-21 27 YO M possible seizure
- 4-2-21 passed out/ reaction to Covid vaccine
- 4-22-21 38 Y.O female not breathing secondary to recent vaccination
- 4-32-21 50 YO F passing out/covid vaccine
- 5-13-21 49 YO M labored breathing/reaction to recent vaccination
- 5-19-21 89 YO M weak/speech problems
- 5/24/21 27 YO F fell by pharmacy
- 6-17-21 39 YO F difficulty breathing from 2nd vaccine
- 8-31-21 31 YO difficulty breathing
- 11-19-21 18 YO M anxiety attack, difficulty breathing from a covid vaccination
- 46 YO F chest pain/labored breathing, body numbness/covid-19 vaccine booster yesterday
- 11-19-21 18 YO F leg numbness
- 12-21-21 46 YO F chest pain, labored breathing, body numbness – covid 19 booster
- 86 YO F low 02, chest pain radiating to the left arm post 2nd covid vaccine shot
- 4-11-21 50 YO M syncope (passing out)
- 4-18-21 57 YO F severe edema (i.e swelling, water retention) possible reaction to vaccine
- 5-22-21 16 YO reaction to vaccine shot, semi-responsive
- 5-31-21 48 YO M reaction to the 2nd vaccine, difficulty breathing, right sided numbness
- 6-2-21 passed out after receiving Covid vaccine
- 6-2-21 29 YO F reaction to vaccine, unconscious
- 6-18-21 12 YO F experiencing chest pain after 2nd vaccine
- 9-24-21 44 YO M seizures after vaccine
- 9-25-21 Male unconscious after getting covid vaccine
- 11-6-21 5 YO M difficulty breathing post vaccine
- 11-13-21 58 YO M reaction to covid vaccine, syncope and difficulty breathing
- 11-3-21 81 YO M Unable to ambulate post vaccine
- 12-8-21 syncope (passing out) post covid shot
- 2-11-21 73 YO M, reaction to Covid vaccine, unable to ambulate
- 4-21-21 reaction to vaccine AMS (altered mental status)
Again, these were just a subset of the 220 calls in 2021 amongst a population of approximately 900,000. I am reasonably certain that there is no data to accurately estimate what a “safe” ambulance call rate per number of vaccines administered should be but that is also because I have never even heard of a threshold being established for a “safe” ambulance call rate per number of vaccines administered.
I would instead simply argue that the ambulance call rate per vaccination should be no more than one in a million or if I were generous in estimating its ability to protect people from severe disease, maybe even one per 100,000, but in reality should be zero.
I say this because vaccines are not a treatment for someone suffering from an active disease, it is an intervention given to generally healthy, functional people to theoretically protect them from becoming ill (i.e. I don’t think the dying need vaccines). An intervention which causes a generally healthy, functional person to need an ambulance directly contradicts any belief of utility or safety in this regard.
These data, to me, are simply another outrageous Covid era example of the deplorable failure of a Public Health Agency to protect the population whose literal mission it is to protect. Obtaining the data by FOIA means that no one in Westchester EMS or Dutchess County EMS leadership acted in response to paramedics or EMTs reporting repeated calls for urgent medical attention to those recently vaccinated?
Don’t you think that you, the average citizen, would have wanted to be informed if this was happening in your community? That vaccine clinics were asking for ambulances to be “on standby?” What other kinds of events request ambulances “on standby” or to be present? I have heard of having them on-site for judo tournaments, Evil Knievel stunts, American football games, (which require two on site), but never for an alleged preventative health measure.
From the webpage of a company that provides ambulance coverage for sports events:
![]()
So, apparently, vaccine clinic employees in Westchester quickly came to the perception that vaccinating people was more dangerous than a charity walk or fun run.
Here is the thing though: to many of us who are deeply studied on the data showing immense toxicity and lethality of the mRNA vaccine platform, this changes nothing about what we already know. To those still in the “safe and effective” camp, I ask how you can explain away the above in a way that can somehow still support that position. Happy to read your comments.
Finally, before we get to the EMS transcripts, for any of you who are as troubled by these data as I am, I suggest you FOIA the same from your local EMS service. I promise you that my colleagues and I are interested in studying this further.
They are covering their tracks
December 23, 2023
“More than 300 medical journal articles have disappeared within the last year.” – Dr. Scott Jensen
@drscottjensen
Canada Reports 300% Increase in ‘Unspecified Causes’ of Death, Sparking Calls for Investigation
By Mike Capuzzo | The Defender | December 13, 2023
As life expectancy plummets in Canada, a new government report claims “unspecified causes” have become the fifth leading cause of death in the country after cancer, heart disease, COVID-19 and accidents.
According to the Statistics Canada report, “unspecified causes” in 2022 passed strokes, aneurysms, chronic bronchitis, emphysema, asthma, diabetes, influenza and pneumonia, chronic liver disease and cirrhosis, Alzheimer’s and suicide as causes of death.
Statistics Canada, also known as StatCan, released the report on Nov. 27 in The Daily, the agency’s online news bulletin.
The report generated a slew of nearly identical headlines — provided by Canada’s national news service — in Canada’s leading newspapers along the lines of this one in the Toronto Sun : “Life expectancy for Canadians fell for third straight year in 2022, StatCan says,” followed by the subhead: “More people died of COVID-19 in 2022 than in any other year since the pandemic began, report says.”
Andre Picard, health columnist at The Globe and Mail in Toronto, Canada’s newspaper of record, called the life expectancy drop — to 81.3 years in 2022 from 82.3 years in 2019 — “a big deal.”
“It’s only the second time this sharp a drop has happened in Canada in the past century,” Picard said. “In fact, life expectancy has been climbing steadily for decades: 71 in 1960, 75 in 1980, 79 in 2000 and 82.3 in 2019.”
COVID-19 deaths in Canada decreased to 14,466 in 2021 from 16,313 in 2020, the report shows. Canada is on track for about 7,000 COVID-19 deaths in 2023, Picard said.
COVID-19 deaths can’t account for Canada’s 7.3 % increase in total deaths in 2022 compared with 2021 — or for the country’s 17% increase in total deaths over the historic norm of 2019, or the historic drop in life expectancy in Canada and worldwide, Picard said.
Like many mainstream journalists and public health officials in the U.S. examining the U.S. drop in life expectancy, Picard blamed chronic diseases, drug overdoses, opioid deaths, smoking, unhealthy diets and “indifference” for the decline in Canada. “There are virtually no mitigation measures like masking any more, and vaccination rates have fallen sharply,” he wrote.
But Drs. Pierre Kory and Peter McCullough told The Defender they believe the most important and startling fact contained in the report is the 300% increase from 2019 to 2022 in “unspecified causes” of death in Canada.
McCullough, a highly published cardiologist who developed a widely used early treatment protocol for COVID-19, said the dramatic rise in deaths from “unspecified causes” in Canada represents a seismic and disturbing shift in Western medicine.
“Prior to the pandemic, death in Western countries was well understood,” McCullough said, with 40% due to known cardiovascular, 40% due to terminal neoplastic disease (cancer) and 20% due to other known causes such as homicide, suicide, drug overdoses and accidents.”
He added:
“Since the roll-out of the COVID-19 vaccines, we have witnessed unprecedented deaths without antecedent disease. A large autopsy series published by Hulscher et al, found that 73.9% of the deaths after COVID-19 vaccination were due to problems caused by the shots.”
McCullough cited the hundreds of studies examining post-vaccine, spike-protein-related injuries and deaths and the millions of deaths and injuries reported by citizens in the U.S. and Europe to their governments following mRNA vaccination.
“All deaths should be categorized according to the doses and dates of COVID-19 vaccination,” McCullough said. “Unless proven otherwise, ‘unspecified death’ should be attributed to a fatal COVID-19 vaccine injury syndrome,” McCullough said.
Kory, the former University of Wisconsin professor of medicine and president of the Front Line COVID-19 Critical Care Alliance, told The Defender the evidence is overwhelming that the COVID-19 mRNA shots caused more deaths and injuries across the Western world than any prior drug or vaccine in history.
“The answer as to why ‘unspecified causes’ are now a leading cause of death is plain and simple,” Kory said. “That cause is the one medical intervention that the world’s governments and media have championed since the start [of the pandemic]. … The mRNA platform technology is and has been a colossal failure in both efficacy and safety.”
Kory and journalist Mary Beth Pfeiffer on Tuesday published an opinion piece in The Hill calling on governments and public health officials to study and address the problem of a global historic rise in mortality thus far not recognized by officials and not reported by mainstream journalists.
On Dec. 13, the essay was trending as the first or second most popular story on The Hill’s website, which claims 32.5 million monthly unique visitors.
U.S. Food and Drug Administration (FDA) Commissioner Robert Califf on Nov. 30 published an extraordinary thread of posts on X (formerly Twitter) calling for a society-wide “all hands on deck” approach to solve the problem of the “catastrophic” decline in U.S. life expectancy.
“JAMA Internal Medicine published earlier this month that our overall life expectancy has dropped to 76 years, and remarkably, that male life expectancy in the U.S. has dropped to 73 years,” Califf wrote.
But Kory said the FDA commissioner’s post, “which hit on smoking, diet, chronic illness and healthcare, ignored the obvious: People are dying in abnormally high numbers even now and long since COVID waned. Yet public health agencies and medical societies are silent.”
The FDA and mainstream media are ignoring the fact that life insurers have been “sounding the alarm over these unexpected or, ‘excess,’ deaths, which claimed 158,000 more Americans in the first nine months of 2023 than in the same period in 2019,” Kory wrote.
“That exceeds America’s combined losses [wounded?] from every war since Vietnam. Congress should urgently work with insurance experts to investigate this troubling trend.”
Amy Kelly, COO of DailyClout and the program director of the Pfizer Documents Analysis Project, said that for an autopsy to reach a proper diagnosis of an mRNA-vaccine-caused death, “histopathological examination of tissues from all over the body is necessary. Most of the time, even if an autopsy is performed, the histopathological examination of tissues is not.”
She cited an interview with Dr. Arne Burkhardt, who describes the types of testing the coroners must perform but seldom do.
Dr. Robert Chandler, a Los Angeles orthopedic surgeon who taught at the University of Southern California medical school, identified “entire new disease categories” he calls “CoVax Diseases” in his study of Pfizer’s 450,000 pages of COVID-19 vaccine documents, documents the FDA was forced to release via a court order, Kelly said.
“It makes sense that the unspecified causes of death have increased so much,” Kelly said. “When a patient dies with either multiple diseases all at one time or with a previously unseen disease state, both of which happen with ‘CoVax Diseases’ Dr. Chandler has identified, I would imagine many doctors and/or coroners don’t know how to categorize those causes of death. That would lead to ‘cause unknown’ categorization of deaths.”
According to Naomi Wolf, author of “Facing the Beast: Courage, Faith and Resistance in a New Dark Age,” “In the preindustrial world, people died mysteriously. But in the modern Western world, there are no mystery deaths. Every death has a death certificate which by law must identify a cause of death.”
“A minor rise in unattributed deaths is a problem that needs investigation,” Wolf said. “A major rise, such as you’ve identified, does not indicate a mass mystery to doctors and coroners, but rather it is evidence of a problem with state record-keeping — some bureaucratic malfeasance at a grand scale.”
Mike Capuzzo is a reporter for The Defender. He is a former prize-winning reporter for The Philadelphia Inquirer and The Miami Herald, a science writer, and a regional magazine founding editor and publisher who has won more than 200 journalism awards as a writer, editor and publisher.
This article was originally published by The Defender — Children’s Health Defense’s News & Views Website under Creative Commons license CC BY-NC-ND 4.0. Please consider subscribing to The Defender or donating to Children’s Health Defense.
Where are they now? White House Covid Task Force members cashed in on pandemic panic
Almost 4 years later, things are going swimmingly for the virus panic corps.
By Jordan Schachtel | The Dossier | December 13, 2023
The White House Coronavirus Task Force was spun up on January 29, 2020. Shortly thereafter, the federal government began to deploy countless billions of dollars to pharmaceutical companies with the ostensible hopes to mitigate a much-hyped incoming pandemic.
Now, almost four years later, our hindsight presents a much clearer picture to the fog of virus mania we experienced in realtime.
Instead of mobilizing an effective public-private response to the advertised problem, Operation Warp Speed and the Task Force served as a vehicle for further panic and the facilitating of taxpayer cash that ended up enriching the pharmaceutical industry. These taxpayer-funded, Covid-related slush funds ballooned to astronomical heights across two presidencies, delivering record profits to Pharma companies that took pains to bring themselves onsides with the people in charge in Washington, D.C.
Tragically, the government-backed mechanical (ventilators) and pharmaceutical (remdesivir, mRNA shots, etc) interventions didn’t work to remedy the respiratory illness problem. Instead, they added an additional layer of chaos on top of the virus mania that had captured the world.
Operation Warp Speed and the resulting Task Force operation was, by all objective accounts, a catastrophic blunder, but that didn’t stop many of its members from parlaying their roles on the high visibility government detail into successful post service gigs.
So we thought now would be a good time to take a look at some of the healthcare/pharma-related government officials responsible for some of those fateful decisions, and where they are today.

Mike Pence:
He was primarily responsible for staffing the Trump Administration’s Covid response team. Pence launched his presidential bid in June, but gave up by October. He is perhaps the only Task Force member who did not benefit from the operation, as his political career is effectively over.
Anthony Fauci:
The most notorious member of the Task Force, Fauci’s wealth increased multiple times over while serving as the Pharma kingmaker over at the National Institute of Allergy and Infectious Diseases (NIAID). He recently took a no-show professorship at Georgetown University and is said to be working on a book.

Deborah Birx:
The second most infamous member of the Task Force, Birx, a protege of the Bill Gates network, has also cashed in on her time in the spotlight. She has since joined multiple pharmaceutical boards and wrote a book attempting to generate even more virus hysteria.

Moncef Slaoui
Technically not a member of the Task Force but the leader of Operation Warp Speed. Slaoui succeeded in delivering preferential treatment to Moderna, where he had a board seat and $10 million in stock options. Moderna stock would jump 20x from January of 2020 to late 2021. Slaoui left Operation Warp Speed in January 2021 to join a GSK-owned pharmaceutical company. He was later fired due to a sexual harassment claim.
Alex Azar
A former president at Eli Lily, he briefly chaired the White House Task Force. As the head of the U.S. Department of Health and Human Services (HHS), Azar facilitated billions of dollars in funding to vaccine companies. Like his colleagues, Azar has since joined several pharmaceutical and healthcare boards.
Jerome Adams
After leaving the White House, the former Surgeon General became Purdue University’s “Executive Director of Health Equity Initiatives,” sporting a salary of half a million dollars a year for the gig. He also joined the boards of half a dozen healthcare and pharmaceutical companies. The hyper woke activist just penned a book casting himself as a “front line hero” in the fight against Covid-19.
Brett Giroir
The Trump Administration’s assistant secretary for health (succeeded by the transgender identifying admiral “Rachel” Levine) spun right through the revolving door with his colleagues. He now serves as CEO and a member of the board of a respiratory virus treatment company. He also wrote a book on “fighting Covid from the front lines to the White House.”
Stephen Hahn
Hahn served as the FDA commissioner and a member of the Task Force. Only six months after authorizing the Moderna mRNA shot, he went on to serve as the chief medical officer of Flagship Pioneering, the venture capital firm behind Moderna. He has since joined multiple ventures seeking to get products approved for FDA clearance.
Robert Redfield
The former CDC director who once declared masks as superior to vaccines has joined quite a few boards related to Pharma and healthcare.
Seema Verma
As CMS Director, this Task Force member issued the infamous memo leaning on healthcare systems to suspend non elective procedures. After her tenure in the Trump Administration, Verma joined the boards of several healthcare firms and became a Senior Vice President at Oracle Corporation.
New Zealand whistleblower released on bail, meanwhile scientists debate meaning of leaked vaccine data
By Michael Nevradakis, Ph.D. | The Defender | December 12, 2023
Scientists and statisticians continue to review and debate the accuracy and completeness of a large database of COVID-19 vaccine-related deaths released less than two weeks ago by a New Zealand Ministry of Health whistleblower.
Meanwhile, the whistleblower — Barry Young — was charged by New Zealand authorities with “accessing a computer system for dishonest purposes.” The 56-year-old appeared in Wellington District Court on Dec. 4. and was released on bail the next day.
Young, who also has used the pseudonym “Winston Smith,” was a computer systems programmer for New Zealand’s Ministry of Health, administering a computer payment system for certain vaccine administrators.
Police raided Young’s home on Dec. 3, and arrested him. Police raided the home of an associate the same day.
Young, who was reportedly offered two safehouses in New Zealand and one overseas but refused the offers, now faces at least seven years’ imprisonment. According to Newsweek, Young shouted “freedom” as he departed the courtroom on Dec. 4.
Young released the anonymized data with the assistance of Liz Gunn, a former lawyer, television journalist and candidate for public office for the NZ Loyal Party.
According to mathematician Igor Chudov, who analyzed the data, the database included information on the vaccine type, batch number, dose number, vaccination date, age, date of birth and date of death of the anonymized vaccine recipients.
The dataset was related to so-called pay-per-dose providers, such as individual doctors and drugstores. It did not include data on vaccinations administered at mass vaccination centers and by mobile vaccination clinics.
Data raise questions government ‘can’t ignore’
According to the New Zealand Herald, Health New Zealand, the national public health system also known as Te Whatu Ora, has opened an investigation and attempted to discredit the whistleblower, claiming Young “had no clinical background or expert vaccine knowledge.” Some analysts noted Young’s expertise in data administration.
Health New Zealand’s public messaging has centered around the security of personal data. “What [Young] is claiming is completely wrong and ill-informed … We take the security of the information we hold extremely seriously, and this is a significant breach of trust,” said Margie Apa, Health New Zealand’s chief executive.
In an interview with The Defender, Australian attorney Katie Ashby-Koppens said Health New Zealand was also granted an injunction from New Zealand’s Employment Relations Authority, prohibiting the publication of the leaked data.
Ashby-Koppens, who worked with New Zealand groups promoting medical freedom and transparency, questioned the legality of this injunction, which reportedly was used to pressure hosting providers to remove copies of the leaked data stored on their servers, leading some providers to remove accounts hosting the anonymized data.
Minister of Health Shane Reti sought to reassure the public about vaccine safety.
“There are many conspiracy theorists out there who unfortunately disseminate harmful disinformation, however, as Minister and as a physician, the public can and should continue to have confidence in vaccines,” he said. “I am reassured by experts confirming that there is no evidence supporting the allegations that have been made.”
According to the New Zealand Doctors Speaking Out with Science (NZDSOS) media team, consisting of Dr. Cindy de Villiers, Dr. Alison Goodwin, Dr. Matt Shelton and Anna McLoughlin, such statements are a continuation of official COVID-19 narratives.
“The official mainstream media narrative is that New Zealand did very well during the pandemic, having negative excess mortality,” a spokesperson for NZDSOS told The Defender. “The New Zealand government and media have adopted a ‘shoot the messenger’ approach and then studiously ignored the issue, such that the average person on the street probably is unaware of what is happening in New Zealand.”
Yet, members of the public “who know what is happening absolutely support the whistleblower,” NZDSOS said, noting that “the media is so controlled and captured that large chunks of the population remain unaware of the data release or its significance.”
New Zealand authorities acknowledge only four COVID-19 vaccine-related deaths.
“The data has been very controversial, with people finding opposing things from their analysis of the data, despite being on the same side of the COVID debate,” Ashby-Koppens said. “The data is not complete [but] it raises a lot of questions, questions that the new New Zealand coalition government can’t ignore.”
Norman Fenton, Ph.D., a mathematician and professor emeritus at Queen Mary University of London, also examined the leaked data. He told The Defender the reaction of New Zealand’s authorities to the leak was “very strange.” He added:
“I understand that releasing confidential medical records is a criminal offense, but … the whistleblower only released an anonymized version of the data.
“Given the advanced publicity by people like Steve Kirsch about what the data revealed, I would have thought the New Zealand government would have been better advised to do nothing rather than raiding homes, arresting the whistleblower and erasing files from people who had gained access to the data. It is almost as if they wanted to get more publicity for both the data breach and what the data revealed.”
Presenting one possible reason supporting such an explanation, Fenton said:
“Not surprisingly, this has also led to conspiracy theories of which the most notable is that the government knew that this particular dataset did not contain (as some have claimed) any ‘smoking gun’ on vaccine safety and therefore it was deliberately released so it could be used to discredit ‘anti-vaxxers’ who claimed it did, and also act as a warning against any others who had access to more incriminating data to shut up.”
But for Kirsch, the founder of the Vaccine Safety Research Foundation who examined the data and publicly claimed it proves that the COVID-19 vaccines killed 1 in 1,000 people globally, Young “is a hero.”
“He knew he would risk his life and could spend the rest of his life in jail, but he made the courageous move to expose the data for all to see,” he wrote.
According to NZDSOS, Young is due to appear in court again on Dec. 18 to submit a plea and is “represented by a large legal firm in New Zealand.”
Whistleblower noticed ‘really big safety signals’ in the data
In his Nov. 30 interview with Gunn accompanying the release of the data, Young said he helped build the very database from which the data were leaked. Access to such data led him to note items of concern that he decided to go public with, he said.
“I helped build it. I implemented it,” he said. “When I was looking up the data, I noted discrepancies with the dates of death. People were dying almost straight away after being injected and that sort of prompted my curiosity and I dug a little deeper.”
According to Young, he previously was vaccinated, but said that whether he’d get another dose was “a different story.” He added that he “believe[s] in fundamental freedoms of humans and [that] we shouldn’t have a procedure forced on us because of a mandate,” calling this “a huge overreach by the government.”
Following his release on bail, Young granted an interview to Infowars producer and host Alex Jones, stating that he noticed “really big red flags” and “really big safety signals” in the data. “Statistically, it may be killing people,” he said.
“I just looked at the data and what I was seeing, since the rollout, it just blew my mind. I was just seeing more and more people dying who shouldn’t have been dying. It was just obvious,” Young said. “I want people to analyze this … We need to open it up and the government needs to have an inquiry about it. Just bring it to the public’s attention.”
According to New Zealand police, Young’s post-bail interview with Infowars did not breach his bail conditions. He has since granted other interviews.
Scientists disagree on significance of data
According to NZDSOS, the leaked data “cover[s] vaccines that were administered as pay-per-dose. There are 2.2 million people and approximately 4 million doses included.” This compares to a total of 12.78 million doses administered in New Zealand.
Statistical consultant William Briggs is one of the analysts who reviewed the data. On his Substack, he wrote that “we cannot tell for sure” what the data definitively indicates, as there are important items of information missing.
“There was no cause of death given for anybody,” Briggs said. “Just death date for those who had at least one shot and died in this window. There can therefore be no certain proof of any cause of death,” he wrote.
Briggs added:
“An insurmountable problem in ascribing cause is the lack of data on people who did not get any shots. Their death and age data is missing. There is no comparison group for the people who got shots. …
“… this means there is no natural comparison group and nothing about cause, therefore, can be said with certainty.”
Briggs said that the data indicated a small increase in deaths among young people soon after receiving the first and second dose, but said this may be “because the young tended to get fewer shots.”
The analysis that has perhaps garnered the most analysis, though, comes from Kirsch, who wrote, “There is no confusion any longer: the vaccines are unsafe and have killed, on average, around 1 person per 1,000 doses.”
Kirsch noted that this figure “is consistent with other careful analyses,” such as one by Canadian scientist Denis Rancourt.
According to Kirsch, one safety signal he identified in the data is a “mortality hump that peaks around 6 months after a dose is given.”
“The data from New Zealand is not perfect; it is not a complete sample,” Kirsch conceded. “But, by using a cohort time-series analysis, it doesn’t matter. There is no possible way that this data is consistent with a safe vaccine.”
Fenton, who analyzed the data on his Substack, took a different position, telling The Defender, “The dataset is a very large subset of those vaccinated in New Zealand, and is potentially one of the most important publicly available datasets for examining COVID vaccine safety. But I don’t believe it is the ‘smoking gun’ as some have claimed.”
He noted the absence of a control group (the unvaccinated) and that “the age profile seems higher than the national age profile of [the] vaccinated, so there is some bias.”
However, he said the data “does provide some evidence of lack of safety of the vaccine, in particular supporting our own previous observations (from U.K. data) that in older age groups, all-cause mortality is higher in the vaccinated than the unvaccinated.”
“What is less clear is the claim concerning batches with exceptionally high mortality rates,” Fenton said. “The claim that these batches were especially deadly due to the contents of the vaccine or its delivery is confounded by their very different age and time of vaccination profiles,” he added.
Chudov, in a pair of posts on Substack, also presented his analysis of the data. In his initial post, he suggested the public “be wary” of the data and noted that Gunn “is misinterpreting it by trying to pass normal nursing home deaths as evidence of ‘super deadly batches’ and ‘mass vaccine casualties.’”
In a follow-up post, Chudov acknowledged that some of his original questions about the completeness of the data were subsequently addressed, stating his belief that “Barry Young was more likely to be sincere than insincere in his intentions and actions.” Yet, he said his questions “about nursing home deaths and data quality still apply.”
Some analysts also pointed to official data indicating that excess deaths in New Zealand continue to be significantly above the long-term average — 17% in September and early October 2023, according to data from the Organisation for Economic Co-operation and Development. Some also pointed to data indicating sharp increases in the incidence of heart attacks in New Zealand.
Yet, Apa said, “We assure people there is no evidence whatsoever that vaccination is responsible for excess mortality in New Zealand and that they can continue to have confidence in the vaccine,” in remarks quoted by the New Zealand Herald.
“We hope that additional independent assessment of the data by credible analysts will lead to further scrutiny of the vaccine rollout in [New Zealand] and that the whistleblower will not have risked everything for nothing,” activist group Voices for Freedom wrote.
Political questions surrounding the data leak, subsequent government actions
According to Voices of Freedom, Young reached out to them “a couple of years ago” and had reached out to several other organizations during this period, prior to telling Gunn about the data and releasing it with her assistance.
Voices of Freedom, as well as some other analysts, have nevertheless raised questions as to whether Gunn handled the release appropriately.
Young and Gunn told Infowars they attempted to contact Winston Peters, leader of the New Zealand First political party and current deputy prime minister and foreign minister, regarding the data, but were unsuccessful in doing so.
But according to analyst Tony Mobilifonitis, Peters “most likely is limited in what he can do because of the delicate politics of the three-party coalition.” Analyst Markus Mutscheller wrote that while Peters had previously “aligned with the NZ freedom movement … His priority is always to keep his position of power in the cabinet. Without it, he can’t do anything.”
NZDSOS told The Defender, “So far, there has been no public comment by NZ First or the ACT party, both of which championed a broader inquiry,” adding that Reti “is from the National Party, which firmly backs the use of mandated vaccines.”
“The Associate Minister of Health, Casey Costello, is from NZ First, who is well aware of what is happening. However, ministers are not able to comment on cases that are before the court,” NZDSOS added.
According to the New Zealand Herald, an inquiry examining New Zealand’s COVID-19 pandemic response has been convened. However, according to NZDSOS, it is unlikely to examine the leaked data, as the inquiry “specifically excludes vaccine efficacy and does not include vaccine safety.” Instead, it aims to “strengthen … preparedness for, and response to, any future pandemic.”
According to NZDSOS, “The new coalition government has promised a broader public inquiry, but terms and conditions have not been decided upon to date. It is not clear whether there will be additions to the existing inquiry or whether a completely new inquiry will commence. Our preference is for a brand-new inquiry.”
‘Still no letup’ in narrative that COVID vaccines are ‘safe and effective’
Several scientists, analysts and activists have called on the New Zealand government to release full, anonymized COVID-19 vaccine data and its own analysis.
“They should release the data on the unvaccinated so that a full direct comparison can be made,” Fenton said. “We also need all the (anonymized) patient-level data on new health conditions/hospitalizations since 2021, for both vaccinated and unvaccinated, so that we can determine the true level of vaccine adverse reactions.”
Similarly, NZDSOS said, “The best approach would be to release all the data in an anonymized form and for the Ministry of Health to discuss their analysis.”
Kirsch wrote, “Nobody will debate me on this,” adding that New Zealand authorities “should be releasing the full [12 million-person] record dataset to remove all doubt and prove to the world the vaccines are safe.”
“Clinical outcomes are never improved by keeping public health data hidden from public view,” Kirsch wrote. “Yet every health authority in the world has kept this critical record-level safety data hidden from view.”
In a subsequent Substack post, Kirsch wrote, “Health New Zealand: Where is your analysis of your data? Why aren’t you publishing it?”
Voices for Freedom called on New Zealand authorities “to be transparent with NZ’s vaccination data,” noting that “There appears to be no official denial of the accuracy of the downloaded Health NZ data set.”
NZDSOS said that New Zealand authorities have a history of not being transparent, telling The Defender that Official Information Act requests are fraught with “often lengthy delays and redaction of data” and the system “is not particularly functional.”
“Some of these requests have been acknowledged, but the length of time in releasing information of this kind in any form has been delayed time and time again … We have not heard of any data/information releases that have come out yet,” NZDSOS said.
Fenton said New Zealand authorities are not being forthcoming regarding the data because it would likely “reveal much more evidence on just how ineffective and unsafe the vaccines have been and on how it likely has led to increased all-cause mortality in all age groups who have taken it.”
“There is still no letup in attempts by governments and pharma companies to close down all discussion and evidence of vaccine harms and to maintain the ‘official’ line that these vaccines are ‘safe and effective’ and need to continue to be given,” he added.
“It appears that the measures taken to silence Barry and avoid discussing the data are designed to deter others from doing the same thing,” NZDSOS said. Similarly, Fenton shared his belief that “the very public actions taken against the whistleblower [were] likely intended to dissuade other whistleblowers everywhere, not just in New Zealand.”
NZDSOS said that prospective whistleblowers should nevertheless not be dissuaded.
“Do what will allow you to sleep at night. It is not about any legal advice, as we know that it is likely that the legal system is compromised. It is about doing what is right,” NZDSOS said. “Evil triumphs when good men do nothing.”
Michael Nevradakis, Ph.D., based in Athens, Greece, is a senior reporter for The Defender and part of the rotation of hosts for CHD.TV’s “Good Morning CHD.”
This article was originally published by The Defender — Children’s Health Defense’s News & Views Website under Creative Commons license CC BY-NC-ND 4.0. Please consider subscribing to The Defender or donating to Children’s Health Defense.
Featured Video
Laith Marouf: Hezbollah’s position on US-Iran ceasefire
or go to
Aletho News Archives – Video-Images
From the Archives
The Dirty Little Secret behind the “Global Terrorism Index”
The Omission of Israeli Terrorism in the Occupied Palestinian Territories
By Karin Brothers | Global Research | December 6, 2014
… The Israeli settlements — all of which are illegal – have been identified as a major impediment to peace. The refusal of a major “global” terrorism report to name the Israeli settlers as one of the groups most responsible for terrorism not only misrepresents a major source of regional violence but exposes the Global Terrorism Index as a propaganda tool that supports a U.S. agenda.
In recent years, governments have been attempting to thwart terrorism by blocking supportive fund-raising. When it comes to Israeli settlements, however, the US and Canada actually encourage fund-raising by giving organizations (such as Christian Friends of Israeli Communities (CFOIC) and the Jewish National Fund) financial support in the form of donor tax-deductions.
Charities which provide funds for the Israeli settlements should be regarded as terror-financing organizations. They should not only lose their tax-deductible status, but they should be banned because they support the violation of international humanitarian law. The terror-financing laws that are being strictly enforced for Muslim charities should be applied to Christian and Jewish charities as well. … Read full article
Blog Roll
 Aletho News
Aletho News- How UK Regulator Ofcom Quietly Bypassed International Law to Police American Speech
- The Black Cube Files: How Former Mossad Operatives Flipped a Nation
- Laith Marouf: Hezbollah’s position on US-Iran ceasefire: What you’re not being told
- Israel’s priority lies in destroying chances of peace between Iran, US: Ex-UN nuclear chief
- Ceasefire for all or for none: Iran shuts Hormuz over Lebanon attacks
- Strait of Hormuz is Iran’s ‘nuclear weapon’ that forced US retreat: Medvedev
- Energy crisis will last for months – Kremlin envoy
- Europe’s quiet role in the war on Iran
- Forty days that shook the Empire: How Iran turned the tables on US and prevailed
- Netanyahu unilaterally declares Lebanon outside of ceasefire deal
- If Americans Knew
- Gazans face a triple crisis: severe shortages of water and bread, healthcare in tatters
- NY Times reports how Netanyahu took the US into Iran War
- A sigh of relief over Iran, but Gaza and Lebanon in dire straits – Daily Update
- Thousands dead and neighborhoods razed to the ground: Aid agencies fear southern Lebanon is becoming the new Gaza
- The war the US is fighting for Israel could cost trillions
- ‘Cigarette Burns, Nail Wounds’: Toddler Tortured in Gaza to Coerce Father
- Trump Says US Sent ‘a Lot of Guns’ to Protesters in Iran
- Israeli forces destroy 17 UN peacekeeper cameras in south Lebanon
- US-Israeli strikes ‘completely destroy’ synagogue in Tehran
- Archbishop for US Military Says Iran War Is Unjust Under Catholic Teaching
- No Tricks Zone
- An Inconvenient Tree: Uncovered In Alps… Europe Much Warmer Than Today 6000 Years Ago
- New Study Reports A 60% Slowdown In Greenland’s Ice Loss Rate In The Last Decade
- Low Intensity Tornado Wrecks Major Solar Farm, Creating A Potential Toxic Dump
- New Study Finds Warming Saves Lives…Cold Temperatures 12 Times More Deadly Than Excess Heat
- German Science Blog Accuses PIK Climate Institute Of Hallucinating Climate Tipping Points
- Devastating Assessment Of Comirnaty Vaccine By Former Senior Pfizer Europe Toxicologist
- New Study: CO2 Is ‘Effectively Negligible’ As An Explanatory Climate Change Factor Since 2000
- Former Pfizer Toxicologist Dr. Helmut Sterz Tells Bundestag Hearing Pfizer Vaccine Should Have Never Been Approved
- Energy Expert: Germany’s Nuclear Phaseout Was A “500 Billion Euro Mistake”
- New Research: South Australia’s Mid-Holocene Sea Surface Temperatures Were 4°C Warmer Than Today
