Five people injured by COVID-19 vaccines, along with a father whose 16-year-old son died from vaccine-induced cardiac arrest, are suing the Biden administration and top U.S. public health officials.
In a lawsuit filed Monday, the plaintiffs — including Brianne Dressen who suffered severe nerve damage after taking the AstraZeneca COVID-19 vaccine — allege the U.S. government colluded with social media companies to censor them when they posted stories about their personal vaccine injury experiences.
Defendants include President Biden and top-ranking White House officials, the Centers for Disease Control and Prevention and the U.S. Department of Homeland Security.
This is the first lawsuit brought by U.S. citizens injured by the COVID-19 vaccines.
Dressen — a preschool teacher from Saratoga Springs, Utah — volunteered to participate in AstraZeneca’s clinical trial for its COVID-19 shot. Now, she says, she is “collateral damage of the pandemic.”
Dressen co-chairs React19, a “science-based non-profit offering financial, physical, and emotional support for those suffering from longterm COVID-19 vaccine adverse events globally.”
After receiving the AstraZeneca shot, Dressen experienced extensive adverse effects — including doubled and blurry vision, severe sensitivity to sound and light, heart and blood pressure fluctuations and intense brain fog — that worsened over time.
She said Facebook, YouTube, TikTok, GoFundMe, Reddit and Instagram removed content she posted about her injuries.
According to Dressen, the plaintiffs’ experiences of censorship “pale in comparison to the thousands of Americans we know who all have experienced the same thing.”
“There is nothing scarier than reaching out for help only to be silenced,” Dressen told The Defender. “It was as scary as the vaccine reaction itself.
“Our constitutional freedoms must be protected, regardless of whether or not we are in a national emergency,” Dressen added.
Dressen — who now experiences “permanent disability” with “ups and downs” — said she and the other plaintiffs are “not fighting this fight for a select few” but are fighting on behalf of the “tens of thousands who are experiencing the same kind of censorship.”
The New Civil Liberties Alliance (NCLA) filed the suit on behalf of Dressen and the other plaintiffs, who include Kristi Dobbs, Nikki Holland, Suzanna Newell and Ernest Ramirez.
All but Ramirez experienced COVID-19 vaccine-related injuries. Ramirez received the Moderna vaccine with no adverse effect — but his 16-year-old son died of vaccine-induced cardiac arrest five days after receiving the Pfizer vaccine.
Newell is a former triathlete from St. Paul, Minnesota, who was diagnosed with an autoimmune disease after she got the vaccine and who now relies on a walker or cane to get around.
Case challenges ‘shocking’ government mass-censorship
According to the complaint, the plaintiffs experienced “heavy and ongoing censorship” on social media platforms — including Facebook, Instagram, YouTube, Twitter, TikTok and GoFundMe — “when they attempted to share “ their personal experiences after they, or a loved one, were medically harmed after taking the vaccine.”
For instance, TikTok on multiple occasions removed Holland’s video posts in which she shared her personal experiences related to her COVID-19 vaccine-related injuries and recovery process.
TikTok said the videos violated “Community Guidelines” for posting “violent and graphic content” and for “integrity and authenticity” concerns.
According to the complaint:
“This case challenges the government’s mass-censorship program and the shocking role that it has played (and still plays) in ensuring that disfavored viewpoints deemed a threat to its agenda are suppressed.
“This sprawling censorship enterprise has involved the efforts of myriad federal agencies and government actors (including within the White House itself) to direct, coerce, and, ultimately, work in concert with social media platforms to censor, muffle, and flag as ‘misinformation’ speech that conflicts with the government’s preferred narrative — including speech that the government explicitly acknowledges to be true.”
Kim Mack Rosenberg, the Children Health Defense’s (CHD) acting outside general counsel, said the new lawsuit is important because it exists “at the intersection” of COVID-19 vaccine injury and COVID-19 censorship.
“The complaint here alleges — as have other cases — a massive censorship program to control the narrative and promote the government’s COVID-19 propaganda,” Mack Rosenberg told The Defender.
She added:
“Silencing those who have been injured, like the plaintiffs in this case, by the very product promoted — and in some cases mandated — by the government is particularly egregious and causes further, albeit, different injury to those individuals, whose First Amendment rights have also been violated.
“Moreover, censoring these injured individuals injures the public, depriving them of important information and discourse on these issues.”
Missouri and Louisiana in May 2022 filed a landmark lawsuit against top-ranking Biden administration officials for allegedly colluding with social media giants to suppress free speech on topics like COVID-19 and election security.
Former Missouri attorney general Eric Schmitt alleges the Biden administration led “the largest speech censorship operation in recent history” by working with social media companies to suppress and censor information later acknowledged as truthful.”
In March, CHD Chairman on Leave Robert F. Kennedy Jr. and CHD filed a class action lawsuit against Biden, Dr. Anthony Fauci and other top administration officials and federal agencies, alleging they “waged a systematic, concerted campaign” to compel the nation’s three largest social media companies to censor constitutionally protected speech, including facts and opinions about the COVID-19 vaccines.
Commenting on the new lawsuit, Peggy Little, senior litigation counsel for NCLA, said in a statement:
“Americans injured by experimentally approved Covid vaccines are being deplatformed, silenced, suppressed, defamed and cancelled by their own government for reaching out to others simply to share and receive information critical to their physical and mental well-being.
“Government actors have bullied, threatened and coerced social media companies to strip these plaintiffs of their First Amendment rights of association and speech. Suppression of speech critical of the government by the very government actors mandating the vaccine is frightening.
“NCLA’s lawsuit seeks to restore these plaintiffs’ civil liberties and the free flow of information guaranteed by the First Amendment for all Americans. We must never again lose our constitutional bearings in a pandemic.”
Casey Norman, one of the NCLA lawyers representing Dressen and the other plaintiffs, agreed. He said that the government claims it suppresses “so-called misinformation” for the sake of “public safety and welfare.”
“Fortunately,” Norman added, “the First Amendment says otherwise: the government may neither censor our clients nor induce others to do so.”
Suzanne Burdick, Ph.D., is a reporter and researcher for The Defender based in Fairfield, Iowa. She holds a Ph.D. in Communication Studies from the University of Texas at Austin (2021), and a master’s degree in communication and leadership from Gonzaga University (2015). Her scholarship has been published in Health Communication. She has taught at various academic institutions in the United States and is fluent in Spanish.
This article was originally published by The Defender — Children’s Health Defense’s News & Views Website under Creative Commons license CC BY-NC-ND 4.0. Please consider subscribing to The Defender or donating to Children’s Health Defense.
May 24, 2023
Posted by aletho |
Civil Liberties, Full Spectrum Dominance | COVID-19 Vaccine, Facebook, GoFundMe, Human rights, Instagram, TikTok, Twitter, United States, YouTube |
Leave a comment
The COVID-19 vaccines have provided a once-in-a-lifetime opportunity to answer this question
A major problem I see throughout the scientific and political sphere is that people cannot maintain a perspective that allows them to see the whole picture; rather they tend to focus or fixate on things they have some type of emotional or subconscious priming to focus on (this has been an issue throughout history). This is why you can have someone be around an individual they like and they primarily register the one good thing the individual did (while ignoring all the bad things) and conversely why they will ignore all the good things another individual they don’t like is trying so hard to do and focus on the one bad thing that individual did.
This human tendency ends up becoming a huge problem because the media will emotionally condition the public to focus on the one side on an issue which favors its corporate sponsors. This in turn leads to these people getting up in arms about that one point when individuals who dissent against the corporate narrative try to highlight the issues that greatly outweigh any purported benefit of the narrative.
This is particularly common with complex issues (which are difficult to understand to begin with) and one of my longstanding frustrations has been that despite the harms of vaccines greatly outweighing their benefits, many of you can only register the danger of the (often insignificant disease) the vaccine allegedly protects against. In my eyes, one of the upsides about COVID-19 is that this selective reframing of reality and the media lies to maintain it went to such an extreme extent, much of the public became able to realize it was absurd and started taking the time to try and fully understand the subject.
One of the common questions I get from readers relates to another complex question—which vaccines are safe for their kids, and which ones are a bad idea? This is surprisingly difficult to answer because you must weigh the likelihood of an adverse event from a vaccination vs. the likelihood of suffering a complication from the disease that the vaccine would prevent you from getting and compute a figure that takes the weighted average of each into consideration.
In order make this determination, you need to consider all of the following:
Disease Risk
How likely is it for a person to get the disease?
Some diseases we vaccinate against are incredibly rare (e.g., tetanus).
How likely is the disease to cause a negligible, minor, moderate, severe, or fatal complication?
It is very important to distinguish between these categories because, for most infections, the risk of you catching it and then it becoming a severe condition is extremely low. For example, a Neisseria meningitidis infection (which can cause septic meningitis) is really bad and can progress very quickly, but also is very rare for people to develop (one in ten people are asymptomatic carriers whereas approximately one in a million get it a year).
How likely is it that the severity of the disease can be improved with an existing medical treatment?
Most of the infections we vaccinate against are very easy to treat. Unfortunately, the focus is always on vaccinating against the disease rather than providing treatment for it (especially if the treatment is something more unorthodox than an antibiotic). In the case of COVID-19, while severe complications represent the minority of cases, they (and the more minor ones) can in most cases easily be prevented by early outpatient treatment. Unfortunately, the Federal government has refused to disclose to the public what the effective treatments are for it (presumably because it would make it impossible to continue making money off COVID-19).
How likely is it that you will have access to the necessary treatment before you get seriously ill?
Although I dislike the vaccine approach, I have to acknowledge that this is one of the strongest arguments for it. For rapidly progressing diseases, for those in isolated areas, for those unable to recognize their need to seek medical care, and for those of limited economic means, they often cannot get the necessary treatment for the disease before it is too late to prevent a severe complication.
In general, it’s very rare that a vaccine-preventable disease has both a significant likelihood that you will get it and a significant likelihood that it will develop into a severe condition. Many of those believed to fall into this category are no longer an issue in the United States (e.g., polio or smallpox), regardless of whether or not you are vaccinated, but people who look at this question are often fixated on the past presentations of the disease when it was more pathogenic or when we did not have a way to treat it.
Vaccine Efficacy
How likely is the vaccine to be effective in preventing the disease, and do the presence of vaccine antibodies correlate with a decreased risk of the disease?
Many vaccines fail to do one or both of these. COVID-19 has provided the greatest red pill in history on this topic, especially since successive COVID-19 vaccines actually increase your risk of catching the disease.
How likely is the vaccine to be effective at preventing severe complications of the disease?
The human papillomavirus vaccine (which “prevents” cervical cancer) is an excellent example of a vaccine that does not live up to its promise to do so because it’s promise was based on a series of erroneous (and wishful) assumptions.
How long does the vaccine’s protection last following immunization?
Many vaccines suffer from the problem of declining immunity, hence needing repeated boosters to be given which re-expose the recipient to the risks of the vaccine. COVID-19 again has provided the greatest red pill in history on this topic, as the immunity from it wanes approximately 3 months after the most recent injection.
How likely will it be for the vaccine to prevent you from getting the disease when you need to be protected?
The hepatitis B vaccine is routinely given at birth, and then twice more very early in life. This is nonsensical for two reasons. First, at the time of birth, infants lack an immune system that can mount a proper antibody response to the vaccine. Second, hepatitis B is spread by blood-to-blood contact (e.g., sharing heroin needles or having unprotected sex), both things very unlikely to happen in childhood. This is important because the hepatitis B vaccine typically only lasts for around 6-7 years (estimates vary). The best explanation I have seen for why the vaccine is given immediately following birth (despite being completely unjustifiable) is that it habituates parents to come in for regular well child vaccination visits starting at two months.
How long does it take for the vaccine to create a selective pressure that causes the pathogen to no longer be covered by the vaccine?
This is a huge problem for any vaccine that “works”, because it rapidly creates selective pressure for variants not covered by the vaccine’s antigen. The only vaccines that do not suffer from this issue are the ones where the vaccine does not create selective pressures against the vaccine (e.g., the non-contagious tetanus bacteria toxin) and live attenuated vaccines since they contain so many different antigens [note: except for tuberculosis, all live attenuated vaccines are viruses]. Live attenuated vaccines, unfortunately, can cause infections of the vaccine strain in the immunocompromised host, and are frequently contaminated with other viruses that were present in the medium used to cultivate the virus.
Because this is a longstanding problem, many theorized that the COVID-19 vaccine (due to it only containing a single antigen in a rapidly mutating part of the spike protein) would rapidly trigger the production of more pathogenic variants. This is, of course, what happened soon after it hit the market.
Does the vaccine have other benefits besides preventing the disease?
Some live attenuated vaccines broadly stimulate the immune system. In third world countries with a high infectious disease burden, this actually saves lives (this has been shown with the measles-mumps-rubella vaccine [MMR] and the tuberculosis vaccine [BCG]) because the immune system is better able to fight off those otherwise fatal infections modern medical care is not available for.
Note: conversely, other vaccines like DPT, when studied were found to do the opposite and broadly increase the risk of death due to the immune suppression they create.
Population Immunity
Assuming that the vaccine “works”:
Does vaccination create a selective pressure for vaccine resistant variants to produce more or less dangerous variants?
With certain vaccines, the strains created by the selective pressure of the vaccine are more dangerous than those that preceded them, and they affect different age groups. This has primarily been shown with the childhood vaccines for bacterial infections.
Does developing a population-wide vaccine immunity to a disease improve or worsen the disease’s consequences?
Two of the best examples of this were the chickenpox vaccine and the measles vaccine (two relatively benign diseases in the era preceding vaccination due to a robust herd immunity).
If you get chickenpox as a child, it is benign, but if you get it as an adult, it can often give you a horrible (and sometimes recurrent) case of shingles. The CDC eagerly expected rolling out the chickenpox vaccine would decrease shingles, but the opposite instead happened (so they, of course, suppressed the data). The researcher who conducted those studies, with a good basis for doing so, theorized that this happened because the reduction of chickenpox in the population prevented people from having their immune response to it be periodically boosted by natural exposure.
In the case of measles, if there is no pre-existing immunity and poor living conditions (e.g., widespread vitamin A deficiency), the disease can be horrible (e.g. measles killed 10% of Native Americans it infected in one outbreak). In the past, infants received antibodies from their mother’s milk (the importance of breast feeding is discussed here), which provided them sufficient protection to build up permanent natural immunity once they were exposed to the virus. The population-wide herd immunity we used to have does not exist now, and periodic measles outbreaks still occur despite the majority of the population being vaccinated. Because we lack that immunity, many are vulnerable to measles, which is always addressed by vaccinating even more people for the disease.
Is there a benefit to developing the disease naturally that is prevented by vaccination?
One of the lesser known facts about diseases is that childhood infections are often critical for helping the immune system develop. A variety of diseases that are much more severe in adults than their corresponding “vaccine preventable” childhood infections are observed to result from not catching the disease in childhood. Some examples include:
-Not having a chickenpox infection increasing your risk of glioblastoma (a horrible brain cancer) later in life.
-Not having a mumps infection increasing your risk of ovarian cancer (one of the most deadly cancers for women).
Note: research substantiating these links and more can be found here.
Vaccinating While Infected
If you are already infected at the time you receive the vaccine, does this improve or worsen your response to the infection?
This was a major problem with the human papillomavirus (HPV) vaccine, as it was shown in the study data that Merck submitted to the FDA that if you had a pre-existing HPV-16 or -18 infections, your risk of developing a cancerous lesion was increased by 44.6% following vaccination. I also have now seen many things which suggest that getting a vaccine while you are infected with COVID-19 significantly worsens the infection.
If an existing infection worsens following vaccination, how practical is it to test for the infection prior to vaccination, and vaccinate at a later time?
As far as I know, a pre-existing infection is never tested for before vaccination. I presume that this is because public health authorities never want to do anything which might encourage vaccine hesitancy. This is particularly absurd with COVID-19 because we are continually passing out free tests and encouraging people to test multiple times per week…except when they are going to be vaccinated.
Vaccine Side Effects
How likely is the vaccine to cause a minor, moderate, severe, or fatal side effect?
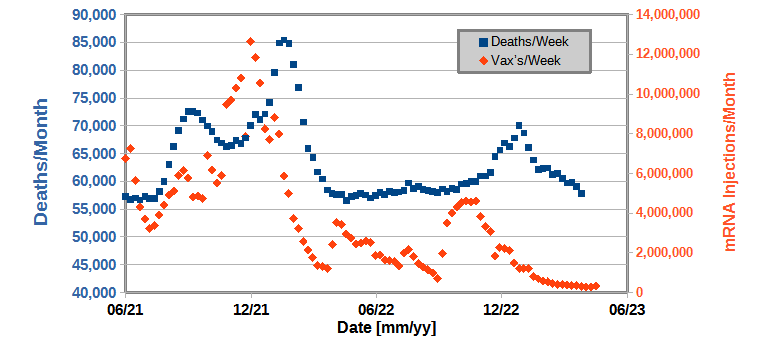
One of the important things to understand about toxins is that their side effects distribute on a bell curve, which means that their side effects become increasingly rarer as they increase in severity. Although the severe reactions are the most noticeable (e.g., the rapid progression to lifelong autism or sudden infant death syndrome), less severe chronic complications are much more common, and in my opinion, create the greatest burden to society (this is very well illustrated by Edward Dowd’s figures below).
An explosion of chronic illness (particularly of neurological and autoimmune nature) in our society has paralleled the mass vaccination of society. This has been most apparent at three times in history: the period of the smallpox vaccines, after 1986 when Fauci passed legislation to shield manufacturers from liability for producing dangerous vaccines (which led to a rapid increase in the number of childhood vaccinations and no motivation to ensure their safety), and following the COVID-19 vaccines. In each case, we’ve tragically become acclimated to an increase in baseline levels of chronic illness which never existed in the past, and we have simply assumed that the current disease burden is normal, when in reality it is not.
Similarly, although the sudden deaths from the COVID-19 vaccine are tragic, many less severe but debilitating or disabling reactions are much more common.
How easy is it to recognize that these effects occurred?
Given how difficult it is to get doctors to acknowledge the most extreme reactions to a childhood vaccine, it should come as no surprise that the more subtle issues go mostly unrecognized or are dismissed (to the point that members of the societal orthodoxy commonly produce memes making fun of anti-vaxxers who blame their various health issues on vaccines).
One of the struggles I have experienced throughout my career in medicine is the fact that I can notice right away that a vaccine injury has occurred while sadly, most of my peers cannot. Most of the signs that scream out to me are rarely detected by my colleagues, and the symptoms either don’t register or they give some type of innocuous explanation for them (e.g., it’s a behavioral thing that requires an SSRI to treat—something I do not support). Furthermore, if I try to point them out, all it accomplishes is undermining my credibility.
This has been particularly fascinating to watch with COVID-19, as countless patients are all developing the same symptoms after vaccination, and yet most doctors ardently insist they have nothing to do with the vaccines. Fortunately, this does appear to be beginning to change, as the medical field’s eyes are opening up to the issue (largely because many healthcare workers have also been injured).
How consistent and safe is the vaccine’s manufacturing process?
Because vaccine manufacturers are exempt from liability for unsafe products they produce, many corners often end up getting cut with the production process so more money can be made by the manufacturer (to this point America’s facilities that make our vaccines have been plagued with production concerns such as potential contamination) the FDA has done almost nothing to address. Additionally, since many vaccines are grown in cell cultures, contamination from things already present in the cells (e.g., retroviruses) is inevitable, and some believe this is a key issue with the vaccines.
With the COVID-19 vaccines, it has been demonstrated that much less due diligence was done with producing the vaccines (likely due to Operation Warp Speed enabling this malfeasance) and as a result, there is immense variation in what is present in each vaccine. Presently, this is the best explanation I have found for why people react so differently to the vaccines and why “hot lots” exist.
Does the vaccine priming your immune system to target one pathogen reduce its ability to respond to other pathogens or cancerous cells within the body?
This is a frequent but underappreciated consequence of vaccination. As far as I know, the worst offender in this regard has been the COVID-19 vaccines, which have been linked to both an explosion of cancers and unusual diseases typically only seen in immune-suppressed individuals.
Does the vaccine impair circulation and cause microstrokes in the body?
I believe that this is one of the primary mechanisms of harm done by vaccines, and frequently what must be focused on when treating these patients (e.g., we have seen miraculous results for individuals with COVID-19 vaccine injuries who we treated with simple methods for addressing their zeta potential). As this is a complex but critically important subject to understand, I put together an article explaining it here, and a series explaining how it affects the body and how to treat it here.
Does the vaccine cause the immune system to attack the body and give rise to chronic illnesses?
All vaccines work by provoking the immune system to go into overdrive to attack the vaccine antigen that is present. The downside to this is that it typically also causes the immune system to attack other proteins in the vicinity (e.g., a mice study showed that mice develop allergies to pollen that is in the air at the time of their vaccination). Autoimmunity is especially likely to happen if the vaccine shares antigen sequences with human tissue (homologies) and contains a very strong adjuvant (the vaccine component which stimulates the immune system). Before the COVID-19 vaccines (which have a remarkable number of homologies with human tissue), Gardasil (the HPV vaccine) was the greatest offender here as it had to use a very strong adjuvant and had homologies to human tissue.
If a vaccine causes negative reactions, does the risk increase if multiple vaccines are given concurrently?
Everything I have seen has shown that the more vaccines that are given (especially if they are received at the same time), the more likely people are to develop a severe reaction to the vaccine. This, for example, is why Sudden Infant Death Syndrome has been correlated to receiving multiple vaccines simultaneously, why many parents have observed their child developing autism after multiple vaccinations, and why some doctors advocate for not following the CDC schedule and spacing out the required vaccinations.
Similarly, if the same vaccine is provided multiple times (especially if it has tissue homology) each successive time it is given, it is more likely to create an autoimmune condition. Although I have seen this with other vaccines, this effect has been by far the most dramatic with the COVID-19 vaccines because their risk of a severe adverse event increases significantly with each successive vaccination.
Although increased autoimmune priming likely plays a role, the best model I have to explain the cumulative toxicity with vaccines is largely due to them successively impairing the zeta potential of the body, which creates catastrophic consequences once a critical threshold is passed. Analogously, I often see the worst responses to vaccines in individuals who already have an impaired zeta potential and cannot tolerate the additional reduction created by one more vaccine.
Unfortunately, since vaccines are considered “safe and effective” their potential harms are never considered. This is why individuals who try to propose very simple measures that could greatly mitigate the harm of the vaccination schedule (like spacing out vaccines) are relentlessly attacked under the justification that “they are not following CDC guidelines” and thus creating vaccine hesitancy.
At this point, we have never had a study performed on the cumulative effects of children receiving the entire vaccine schedule. Anyone who tries to do so is attacked for unethically experimenting on children, since the placebo group (who are not vaccinated) are placed at a “great and unjustified” risk because they are being denied life-saving vaccines (for diseases they will never get).
Since these studies have thus far never been completed, a variety of less controlled ones (e.g., comparing vaccinated and unvaccinated children in the same medical practice) are published. While these studies show a massive number of complications arise from vaccination, they are typically dismissed as not being valid since they weren’t a controlled study, and in many cases, the authors are attacked (e.g., consider what happened to Paul Thomas). Similarly, I and many colleagues can often immediately recognize children who were never vaccinated (as they are healthier in the body, mind and spirit), yet the changes vaccination create have become so normalized in our society, most doctors now lack the ability to recognize the currently accepted baseline is not normal.
If the vaccines cause negative reactions, who is the most susceptible to them?
There is a huge variation in responses to vaccines. Typically, individuals who have had a bad reaction to a vaccine are more likely to have bad reactions in the future, and there are a variety of other signs that predict the likelihood of a bad reaction to vaccines (e.g., previous adverse reactions, pre-existing autoimmune conditions, poor physiologic zeta potential, genetic metabolic defects, having previously had the infection the vaccine is for).
Unfortunately, since vaccines are considered 100% safe, virtually nothing qualifies as an exemption to them (which California has used as a justification to revoke the licenses of anyone who writes exemptions, hence leading to it now being almost impossible to get vaccine exemptions there). To highlight the absurdity of it, I had a friend who had a documented anaphylactic reaction to the Moderna vaccine they had to go to ER for, and was simply told that they needed to get a different COVID vaccine. I have also heard of a case where someone hospitalized in a California ICU for a vaccine reactions and could not find a doctor in the state who was willing to write a medical exemption for their employer.
The Public Health Perspective
One of the largest issues with public health is that it does not see people as individuals, and instead uses theoretical constructs (that are often wrong) and applies them to the entire population. I believe that this is done because it is the most practical way for a centralized bureaucracy to affect the health of a large swath of people with whom it has no direct contact with.
This approach is a huge problem because many individuals behave differently from others (e.g., some derive no benefit from the intervention and some react poorly to the interventions). Unfortunately, for the centralized public health approach to work, the public’s diversity must be ignored, and dissent must be forcefully suppressed when members of the public complain.
Many issues in life I believe ultimately come down to people being lazy and taking the easy way out when addressing a complex problem. For example, in the recent series on SSRI antidepressants (this article and this article), one way the entire debacle could be summarized is that patients with mental health issues require a therapeutic relationship with a counselor who can help them navigate their issues, but this is far too time consuming for most doctors in practice.
Psychiatric medications offer an easy way out; you can just give the drug for the symptom, feel like you solved it, and not have to deal with the patient. Unfortunately, this often doesn’t work, and the medications make the patients worse. At this point, the choice to do one’s job properly or default to a lazy approach again comes up. The doctor can actively monitor the patient for adverse reactions to their drug and intervene before those effects are catastrophic, or gaslight the patient, tell the patient the drug works and just give them more of it or another drug. Most of the catastrophic events I’ve heard about from SSRI-injured patients happened because the doctors took the lazy approach to handle their issues.
Similarly with public health, if a contagious disease is present that the system believes needs to be addressed, there are two options:
• Adopt comprehensive public health measures that contain and mitigate the spread of the disease and encourage practices that increase the natural immunity of the population.
• Add a vaccine for it to the vaccine schedule and mandate it so everyone takes it.
Since the second approach takes much less work, it’s a foregone conclusion that it will happen. Similarly, since the approach will inevitably fail to prevent many people from catching the disease, excuses will be made for why this happens that ultimately boils down to “not enough vaccines were given.”
Likewise, it’s inevitable that injuries will occur from these campaigns (which often outweigh any benefit achieved by the vaccines). When this happens, those injuries are written off by the centralized public health administrators as “necessary collateral damage” for the greater good that the vaccine creates and system-wide policies will be adopted to conceal those injuries and gaslight the injured.
Typically, once it becomes clear that the vaccine is not completely “safe and effective” the justification provided to the public is that the vaccines create “herd immunity” to the disease, and that this benefit outweighs the negative consequences of the vaccine. Unfortunately, in most cases (for many of the reasons listed above) the vaccines do not create herd immunity and instead become a product the population needs to take indefinitely while the disease continues to persist.
Note: for those interested in this subject, I discussed how vaccines consistently fail to prevent disease transmission here, and how we watched this unfold with the COVID-19 vaccines here.
Which Vaccines Should Be Avoided?
For each vaccine, as we consider the risk of its disease, the efficacy of the vaccine, the effects of developing vaccine immunity within a population, the issues with vaccinating while infected, and vaccine side effects, it should become clear that this is an immensely complex question to answer. There are so many potential risks and benefits of different magnitudes that combining them into a weighted average borders on the impossible.
This helps to illustrate some of the major issues that arise when you provide an intervention with known harms as a preventative for a potential risk that may or may not happen (note: the same can also be said for statins). My own belief is that if a therapy has known harm, the benefit for it needs to be concrete (e.g., all antibiotics are to some extent toxic, but most would agree that toxicity is outweighed if someone has a dangerous infection the antibiotic will treat). In the case of vaccination, there are a few vaccines that can be given therapeutically (BcG, rabies, and ones made from the patient’s own serum) so that a clear discussion can be made about the relative risks and benefits of each, but that is not the case for virtually every other vaccine on the market.
Typically speaking, to analyze complex questions like this, we depend on large clinical trials. The problem with such trials is that since they are industry-funded, they always omit most of the adverse events that arise (e.g., they reclassify a severe event as something nebulous, they use a toxic placebo to mask the increase in adverse events seen amongst the vaccinated, or they only monitor subjects for a brief period of time, which is not long enough for most of the vaccine side effects to appear). Generally speaking, the only way to get around this issue is to assess the total number of people who die in each group (as there is no way to reclassify death), and when this metric is looked at in the trials for the worst vaccines (e.g., Gardasil or Pfizer’s COVID-19 vaccine) the total death rate is shown to be increased by vaccination.
The other option is to look at population statistics. Sadly, while these consistently show vaccines cause significant harm, public health officials tend to ignore this data.
When I approach this question I use the following algorithm, where each item takes precedence over the ones after it.
1. Does the vaccine have an unusually high degree of toxicity?
2. Does the vaccine potentially provide an important benefit?
3. Does the vaccine have other reasons to make me concerned about its potential side effects?
4. Does the vaccine actually work?
5. Does the vaccine still work?
I will now briefly discuss some of the vaccines on the current CDC schedule that I feel are the worst offenders.
First, let’s consider the HPV vaccine and the benefits it created by “preventing cervical cancer.”


While I have seen datasets (when stratified by age) showing Gardasil (and other HPV vaccines) actually increased the cervical cancer death rate in those vaccinated, I will give it the benefit of the doubt here. As the graph shows, cervical cancer rates were already approaching 0 before Gardasil, so it is difficult to say if any of the lives saved were due to it (at this point I believe the cancer prevention attributed to Gardasil is false).
Note: many other diseases whose decline was attributed to vaccination also actually had most of their decline occur prior to a vaccine being available.
However, assuming all lives were saved by Gardisil, in England, each year it has saved 6 lives per 100,000 (0.0006%) people, and in the United States, 2 lives per 100,000 (0.0002%) people. Conversely in the clinical trials, 133 per 100,000 (0.13%) participants died (in comparison, the average death rate at the time for those the same age as the trial participants was 43.7 per 100,000). This means, in the best case scenario for the vaccine, for 100,000 people you traded killing 89.3 of vaccine recipients in return for saving 2.
Even though this is terrible, the greater issue is that in the original HPV clinical trial, between 2.3% to 49% of the individuals who received Gardasil developed a new autoimmune condition. We do not know exactly where in that range the total number of new autoimmune disorders was, as Merck classified many autoimmune disorders simply as “new medical conditions” (industry trials always reclassify something they don’t want to show up in the final trial with vague labels like this), but other investigations have concluded the 2.3% figure significantly underestimated the rate of new autoimmune conditions.
So, in return for saving 2 lives per 100,000 people while killing 89.3, you are also giving 2300 (and likely many more) a new life-altering autoimmune condition. All in all, I would not say this represents the best risk-to-benefit ratio. Unfortunately, because Gardasil is so profitable, nothing has been done about this despite numerous red flags being set off and many petitions being made to the FDA to address it.
Diphtheria, Pertussis and Tetanus (DPT)
I am not a fan of the DPT vaccine for the following reasons:
• It is the vaccine most clearly linked to infant deaths (I summarized the extensive degree of evidence substantiating the link that has accumulated over the last century here).
• The vaccine frequently causes permanent brain damage (especially the older version of it). In addition to hearing this from many parents, this happened to two members of my extended family who received the slightly older and more toxic version of it.
• I believe it is one of the primary causes of childhood ear infections (one of the most common complaints parents see their pediatricians for). Many doctors have observed this link, and the best example I heard of came from a doctor and medical missionary who decided to vaccinate an ashram (Indian temple) he was staying in. Before the vaccines, ear infections were non-existent, immediately afterward a large number of children came down with them.
Conversely, I believe the benefit is minimal because:
• The vaccine does not prevent the colonization of any of these bacteria. This is why pertussis outbreaks occur in fully vaccinated populations.
• Diphtheria is now non-existent in the United States, so there is no reason to vaccinate against it (additionally it can be treated with modern antibiotics).
• Tetanus is now very rare (there are approximately 30 cases a year) and it’s actually difficult to say how much the vaccine antibodies protect a person from tetanus (studies have shown that the vaccine produced antitoxin does not prevent tetanus).
Note: it is impossible to get a vaccine that is only for tetanus. Anyone who tells you otherwise is lying. For example, I’ve had multiple family members who went to the ER for a laceration, were told they needed to get a tetanus vaccine, agreed to on the condition it only had tetanus, but not diphtheria or pertussis, and when I reviewed their medical records, they had received the DPT vaccine.
Hepatitis B
As stated above, I do not believe childhood hepatitis B vaccines can be justified. Additionally, the vaccine does create complications and has been repeatedly associated with neuromuscular autoimmune conditions. I believe that this is most likely due to the fact that the antigen used shares a homology with myelin (the coating of nerves), but it may be for other reasons as well.
In adults who are at risk of a hepatitis B infection (e.g., healthcare workers who can accidentally get poked with infected needles), there is a stronger justification for this practice. I do not know how reliable my approach to this problem has been, but each time I have been exposed to potentially infected fluids (including from a hepatitis patient), I avoided the medications and vaccinations offered to me and instead immediately got an ozone or ultraviolet blood irradiation treatment. I am not sure if that was necessary, but I have never developed one of those infections.
In the most memorable instance, my team worked with a patient who exposed many of us to his fluids, and after a preliminary HIV test came back positive, everyone was given antiretroviral medications. I declined them (which everyone made fun of me for) since I knew they were dangerous and I thought it was extremely unlikely he had infected any of us. Later, a few of the healthcare workers told me they had experienced significant complications from the antiretrovirals, which they thought might have been the early stages of HIV, and later still we were told that the test the patient had gave a false positive and he did not, in fact, have HIV.
Measles, Mumps, Rubella (MMR)
As discussed above, it is a bit of a debate if the MMR vaccine decreases measles rates, since while regular vaccination does reduce measles rates, permanent immunity to it disappears within the population, and outbreaks will still occur within the vaccinated population. Sadder still, deaths from measles had almost completely disappeared at the time the vaccine for it was introduced (so there was essentially no justification for introducing it), and in effect by creating the vaccine we turned a non-existent problem into a permanent one by doing so. From my perspective, the greatest problem with the MMR vaccine is its frequent association with autism, something I believe is much worse than developing measles and something you are at a much higher risk for than the infection itself.
Polio
Two types of polio vaccines exist. The inactivated polio vaccine (currently used in the USA) and the live attenuated one (frequently used in poorer nations). The inactivated one does not prevent you from catching polio, but does to some extent (I don’t know how to calculate the exact figure) prevent a polio infection from causing polio-like paralysis. Since it does not prevent infection, it has no effect on transmission. The live polio vaccine does prevent you from becoming infected with polio, but has the unfortunate side effect of sometimes causing polio in the recipient and spreading the weakened polio virus into the environment.
At this point, the polio virus is mostly extinct, and from 2017 onwards, more cases of polio have resulted from the vaccine than polio itself (note: one of my friend’s relatives developed polio from the vaccine). One of the most tragic examples occurred in India where Bill Gates diverted their health budget to aggressively vaccinating against polio, which resulted in 491,000 children developing a “polio-like” illness.
Given that there is no reason to vaccinate against polio, there is no benefit to outweigh the vaccine’s risks. The risk from this vaccine is harder to quantify as I have met many people who have had bad reactions to it, but they did not have a consistent pattern to the injuries (which I often see with other vaccines).
Influenza
There is presently no evidence that the (often mandated) influenza vaccine prevents an individual from getting the flu (which, in most cases, is a relatively benign infection) or transmitting it to others. Additionally, there is evidence that the vaccine increases your likelihood of developing a severe case of influenza and developing influenza in the subsequent year. Furthermore, many individuals have developed injuries from the influenza vaccine.
Meningococcal
Initially, due to the severity of a Neisseria meningitidis infection, I initially thought the meningococcal vaccine would probably be a vaccine you could make a strong case for. Unfortunately, there are multiple dangerous strains of this bacteria, and one of those strains (strain B) is very difficult to make a vaccine for, since it has homology with tissue of the human body.
Not surprisingly, this has created a selective pressure on the bacteria and now the majority of infections are caused by strain B, which until recently, the scheduled vaccine did not cover (and at this point I am unsure how effective this newer vaccine is). Furthermore, as discussed above, many people carry this bacteria and are asymptomatic—the infection is very rare and the primary group at risk are those with pre-existing susceptibilities, not the general population.
Conversely, the vaccine has a variety of potential autoimmune complications. By far the most common one I encounter is that it causes Crohn’s disease (typically a few months after vaccination), and I think this side effect alone outweighs any potential benefits from the vaccine.
For those wishing to learn more about this subject, I would suggest reading this article on why vaccines consistently fail to create herd immunity, Miller’s Review of Critical Vaccine Studies (especially in regard to the HiB and Pneumococcal vaccines), and the textbook Vaccines and Autoimmunity. Peter Gøtzsche (one of my heroes) has also written a good review of the evidence surrounding the vaccines, Vaccines: Truth, Lies, and Controversy, which highlights many issues with them but also has the typical pro-vaccine bias and contains certain conclusions I do not agree with (but makes it an excellent book for opening the eyes of more conventional physicians). Finally, Turtles All The Way Down also does a deeper dive on many of these vaccines.
Pneumococcal and Haemophilus influenzae type B (HiB)
These two are probably the most difficult routine vaccines to have a clear-cut position on. This is because:
• These two infections, especially HiB are the vaccine-preventable illnesses that are the most likely to cause severe complications in children. For example, when the HiB vaccine came out, pediatricians around the country noticed a significant decline in the rates of infants with meningitis, which is a big deal. Similarly, in modern-day pediatrics, many of the most common concerning infections doctors encounter are pneumococcal.
• Although these vaccines have adverse effects, they are not as dangerous as those of many other vaccines.
• Because these vaccines work but target an easily mutable part of the bacteria, their adoption triggers their target bacteria to mutate, become resistant to the vaccines, and, in some cases, affect different populations. For example, the pneumococcal vaccine is continually being updated and re-released, with additional strains being covered in each successive version (and I’ve seen multiple vaccinated children with potentially life-threatening pneumococcal infections who had been vaccinated). In the case of the HiB vaccine, it selected for the A strain (HiA), which in some areas was more deadly than HiB, and also selected for strains that affected adults (typically HiB only affects children), leading to severe HiB infections becoming a disease of adults and the elderly.
Note: studies supporting the contentions in this section can be found within this excellent book.
The Risks and Benefits of the COVID Vaccines
Although many tragic things have happened with the COVID-19 vaccines, the circumstances around them have also made it possible to shed light on the actual risks and benefits of a vaccine, a topic that is typically far too obfuscated for anyone to make sense of. The clarity this time around is primarily because:
• The novel vaccines were rapidly rolled out onto the entire population at the start of 2021. This makes it possible to compare numerous existing yearly trends to before and after the deployment of the COVID vaccines.
• A lot of people strongly objected to how the vaccines were pushed onto the population, and did a lot of work to prove that the risks from these vaccines greatly outweighed their benefits in almost every aspect that was examined.
For example, many people are aware of this dataset:

Recently two things became available, which I believe help to clearly illustrate the poor risk-to-benefit ratio of the COVID-19 vaccines.
Rasmussen Reports
The first was a recent poll from Rasmussen Reports. Before discussing it, I would like to share the results from two of their prior polls on this issue:


Both of these reports serve to highlight that the damage from the COVID vaccines is on a scale that the general public is fully aware of, despite the massive amounts of propaganda telling them otherwise. Let’s now look at Rasmussen’s recent results:


There are a few important takeaways from these polls:
• Although Democrats tend to believe that the COVID virus is dangerous and that vaccines are safe relative to Republicans, they have now seen so much evidence to the contrary that the gap between them is much smaller. This is especially true for the vaccine deaths, which will likely have immense political repercussions for the party that forced them on America.[
• In the public’s perception, the same number of people have died from COVID-19 as from the vaccines. Given that many of the COVID-19 deaths occurred before the vaccines, many of those deaths were not actually due to COVID-19, and that the vaccines do not offer complete protection against COVID-19, this is a strong argument that the benefits of the vaccines do not outweigh their risks, especially when you factor in their much more common complications which disable but do not kill the recipient.
• Many respondents likely did not understand what “household” meant (and likely instead interpreted it to just mean someone they knew). This is because nowhere near 11% of US households have had a COVID-19 or vaccine death in them.
Note: Many people disparage Rasmussen and claim they have a right-wing bias. I, however, consider them to be one of the most accurate political polling firms in the country.
Edward Dowd has taken an innovative approach to red-pilling the public—showing the financial costs of the vaccine program for the country and making people feel like chumps for investing in fields that are being adversely affected by those costs. Since everyone can relate to money, this makes the concept much easier for individuals to grasp, and more importantly, since money is the most important thing to the upper class, they are likely to be motivated to act against the vaccination program in order to protect their assets.
Dowd has assembled a team of experienced analysts that has done a lot of work to calculate the costs of the vaccine program. Recently they released a report which speaks for itself:

When I reviewed Dowd’s report, I realized that there were a lot of issues that I know have human and economic costs that it was not counting, presumably since they are impossible to calculate. This means he had to underestimate the harms that have been caused by the vaccine program.
Because things like this are so difficult to estimate, you have to err on the conservative side and avoid claiming things you cannot quantify or are unsure of. Similarly, I have the same experience each time I write an article here, and do not mention a lot of things I am passionate about after I realize I can’t actually back them up.
These recent publications (and the datasets that Dowd’s estimate is based upon) show clearly and unambiguously that the risks of the COVID vaccines greatly outweigh any possible benefit they might have. Given that much of the country is beginning to see this now, it will be very interesting to see how this issue unfolds in the coming years as our institutions struggle to rebuild the trust they spent decades creating in America. My hope is that this process will allow us to also critically examine the entire vaccine program, which has by and large enjoyed complete immunity to scrutiny, due to both the difficulty in comprehensively assessing it and our institutions’s adamant protection of them.
One of the themes of my articles here has been to discuss the progressively evolving pleas for COVID amnesty, which in the space of slightly under a year have gone from “the experts were wrong, but you should still trust them rather than your gut” to “America’s COVID-19 response was based on lies.” Recently, the author of one plea (I did not completely agree with) posted something I felt made an excellent conclusion to this article.

At this point, I believe that all vaccines can cause harm frequently enough that the harm must always be considered when evaluating the vaccine. For this reason, I always feel very torn on what to do when people ask me to provide them with a way to protect themselves from the harms of a vaccine they have to get (note: the two best approaches I know of are taking a lot of vitamin C beforehand, and doing whatever you can to strengthen your zeta potential).
This is because regardless of what you do, you will still always have patients who are harmed by taking the vaccine, and I hate being complicit in what happens. To this point, I have had times where I repeatedly warned a patient against vaccinating where I felt they were at risk of an adverse reaction, and they had one anyway, and then they suffered a permanent complication and I was left having to try to help them get better.
I also believe that natural immunity is always superior to vaccine immunity. For this reason, I believe that the correct approach to handling almost all diseases you can vaccinate against is to accept the inherent risk of getting it as an unvaccinated individual and be familiar with what treatment protocol you need to implement if you got the infection so that you can clear the infection and develop natural immunity. Just imagine how different the world would be now if we had followed that approach instead of suppressing every single treatment for COVID-19 and mandating a deadly and ineffective vaccination on the population.
May 21, 2023
Posted by aletho |
Science and Pseudo-Science, Timeless or most popular | COVID-19 Vaccine, HPV vaccine, United States |
Leave a comment

Ralph Marxen Jr. had just turned 70 and was enjoying life with his wife of 49 years, Lynda, and his adult children and grandchildren. The Minnetonka, Minnesota, native was in good health and, according to his daughter, Nicole Riggs, walked long distances daily and wasn’t on any medications.
In August 2021, several members of Riggs’ household contracted COVID-19, including, presumably, her parents. A week later, while most family members were recovering, Marxen’s condition deteriorated leading him to be admitted to Abbott Northwestern Hospital in Minneapolis on Aug. 23, 2021.
Marxen would never leave the hospital — he died there on Sept. 7, 2021.
During his stay, Marxen, who had not received a COVID-19 vaccine, was administered more than 50 medications, including remdesivir, vancomycin, fentanyl and midazolam, and in the days prior to his death, he was placed on a ventilator.
At the time of his death, Marxen had “multiple organ system failure including renal failure, endocarditis, hyperkalemia, MRSA [methicillin-resistant Staphylococcus aureus] pneumonia, MRSA bacteremia and sepsis,” Riggs said.
Riggs told The Defender the treatments she and her family requested for Marxen, including ivermectin, monoclonal antibodies and vitamins, were refused.
She said she did not believe her father’s refusal of the COVID-19 vaccines played a role in his illness — in fact, she argued that her father’s non-vaccinated status — and the COVID-19 protocols prescribed by the Centers for Disease Control and Prevention (CDC) and the National Institutes of Health (NIH) — were factors in the treatment he received from the hospital and its medical staff.
‘Is this a hospital or a prison?’
“My dad went to the ER seeking help for dizziness and nausea,” Riggs said. “He was 70 years old and took no daily meds. He was unvaccinated and refused to take their unreliable PCR tests.”
In a separate interview with Minnesota’s Alpha News, Riggs said that two of her father’s friends had gotten vaccinated “and they both got vax-injured.” As a result, “He was adamant that he was not going to get the vaccine.”
“I think this played a part in him not getting good care,” Riggs told The Defender.
Riggs recounted the chain of events that led her father to end up in the hospital.
“In the middle of August 2021, my household of four, plus my parents, became ill with fever and fatigue, and a few of us had chest congestion,” Riggs said. “Myself, my husband and my two boys were spit-tested for COVID and were all told we were positive for COVID. We assumed my parents had the same.”
But after a week of being sick, she said they noticed that her father “didn’t seem to be bouncing back like the rest of us. He was having trouble walking to the bathroom because he was so weak and dehydrated.”
Due to his older age, his family “decided to call the ambulance and get him checked out,” Riggs said. Paramedics recommended Marxen go to the hospital for further evaluation, so he was admitted on Aug. 23, 2021, after an ER visit.
“From the beginning, the medical records indicate they wanted to get him on remdesivir even though they couldn’t get him to PCR test,” Riggs said.
“Within a day, a friend of the family who had been working with COVID patients for the past year told us to call the hospital and request that my dad be given monoclonal antibodies (a.k.a. Regeneron),” Riggs said. However, the nurse treating her father said he “had never heard of that before, and that was the end of that discussion.”
“That seemed strange to me, but I still trusted them at that time,” Riggs said.
The day after her father was admitted to the hospital, her mother also was admitted, after her oxygen levels dropped to the low 90s.
“My parents were soon hospital room neighbors,” Riggs said. “COVID medications were started, which we later learned was hospital protocol with remdesivir and dexamethasone.”
Despite being in neighboring rooms though, Riggs’ parents could not visit each other. “My mom wanted to go see my dad since he was in the room right next door, but she realized that her bed had an alarm that sounded when she tried to get up. She also learned that both of them were locked in their rooms as well,” Riggs said.
She added:
“My mom’s nurse thought ‘it wasn’t appropriate,’ and refused to let her go see my dad. They had to wait until that nurse was off her shift before the doctor would OK my mom to go into my dad’s room for a short visit.
“Is this a hospital or a prison?”
It wasn’t long before Riggs began to receive more disturbing updates about the treatment her parents were receiving in the hospital.
She told The Defender :
“My brother started a CaringBridge site to keep our whole family updated. It wasn’t long before I started to receive unsettling messages from people I knew and trust. One was from my dad’s old neurological chiropractor, saying ‘no remdesivir and no ventilator, that’s asking to die.’ He also sent me information on how to get a lawyer involved.
“It was then that I started to research and realize the dangers of the deadly hospital protocols put in place by the NIH and CDC, especially for those on Medicare, as the hospital is given a 20% bonus payment if certain steps are followed with those patients, starting with a positive COVID PCR test.”
According to Riggs, this was evident in her father’s medical records.
“One of the doctors actually wrote this in the medical records: ‘I don’t think it’s impossible to use remdesivir without a PCR positive,’” Riggs said, adding, “My dad initially refused a nasal PCR test because he knew they could be inaccurate and wanted to be treated by symptoms, not a PCR positive COVID test result.”
However, the hospital told Marxen and his family this was not possible. According to Riggs, the doctor said, “Certain treatments may not be available without PCR-proven COVID, and that if his condition worsened such that he required intubation, we would run the nasopharyngeal swab.”
“Basically, my dad was told he wouldn’t get access to ‘certain treatments’ until he submitted to their request to be PCR tested,” Riggs said. “And if he got bad enough, they would test him anyway.”
The hospital also told them if Marxen’s condition deteriorated enough that they needed to put him on a ventilator, they would do the test without his permission.
Her father finally “relented” and tested positive for COVID-19. That’s when the hospital administered remdesivir “and many other harmful drugs,” Riggs said, and denied their request for safer alternatives.
‘It all happened so fast’
From this point forward, “It all happened so fast,” Riggs said. Her father was transferred to progressive care on Aug. 26, 2021, and to the ICU the next day.
“My dad was denied visitation by anyone under the guise of ‘COVID isolation,’” Riggs said. “Even my mom, who was in the same hospital with COVID.”
Marxen’s condition quickly deteriorated. “My dad was told he needed to get on the ventilator so he could get relief and a feeding tube,” Riggs said. “By this time, my dad hadn’t slept in two days and hadn’t eaten in five days.”
“After two days in the ICU, he was freaking out, pulling off his mask and pulling out his IV,” Riggs said. “They got him ‘reoriented’ and brought in the doctor. If you knew my dad, you would know that this was totally out of character for him. He was the kindest, most loving man and father. He was one of my best friends.”
“Soon, he felt he had no other option but to be put on a ventilator,” Riggs said. “A decision he had to make scared and alone because we were kept from him … They had finally got him desperate enough to submit to getting on a ventilator.”
Marxen was intubated on Aug. 29, 2021, and placed on fentanyl and propofol, Riggs said, “even though, reading the records, they knew that wasn’t the solution, but they did it anyway.”
Riggs said she and her family again requested monoclonal antibodies be administered, “but were denied because it was too late in the progression of the disease to be a benefit.”
They also requested “vitamin C, vitamin D, zinc, hydroxychloroquine, ivermectin,” but were denied “and told they refused to go off of protocol, ‘because the one time we did that, the patient died,’” Riggs added.
“My dad’s medical records indicate vitamin D was ‘deemed not appropriate during this admission,’” Riggs noted. “We asked them to take him off vancomycin because that can make you retain fluid and he was already doing that. They told us no, and that the drug was ‘the gold standard.’”
‘He was kept from everyone that truly loved him’
According to Riggs, she would call the hospital every day at 6 p.m. for updates, and her brother would do so daily at 6 a.m. This continued until Sept. 7, 2021, the day her father would be placed “off quarantine” and allowed to see family members again.
However, “on Sept. 7, we were told that the ‘infectious disease team’ said he needed another seven days of quarantine,” Riggs said. “This decision was not even made by his ICU doctor.”
Instead, Riggs and her family were told “the nurses would set up a Facetime for us for the evening of Sept. 7,” Riggs said. “After that call, I was crying and pacing in my house. My thoughts were, ‘Are we going to just leave him in there to die alone?’ I needed to actually do something.”
Riggs said she decided to request her father’s medical records from the hospital, “so I could see exactly what was going on there.” However, she was told the records could not be released “unless he signed the release form” — even though her father was sedated and on a ventilator “and it wasn’t possible for him to sign anything.”
In response, the hospital told Riggs that she “would need to provide his death certificate for the records if we hadn’t already set up power of attorney.”
“So, he had to die before I could access his records?” Riggs asked. “How did this nightmare become our reality?”
Within a few hours of this exchange, Riggs received a call that her father was “actively dying” and if they wanted to see him, they needed to do it soon, because he would pass away during that night.
“Now that he was dying, we were able to come see him — but hours before we couldn’t? This made zero sense to me,” Riggs said.
On arriving at the hospital, she and other family members “were required to wear space-like soft helmets, which made it impossible to even kiss my dad goodbye.”
According to Riggs, she and her family “gave the OK to remove him from the ventilator so we could pray scripture over him through his transition.”
“I thought removing him from the ventilator would cause him to pass away because he couldn’t live without it,” Riggs said. “But I can’t help but wonder if that’s really how it went down. His records show that he was given fentanyl at 5:10 p.m. and midazolam at 5:32 p.m. He passed away at 6:22 p.m.”
Riggs said the “official” cause of death was determined to be “respiratory failure with underlying COVID-19.”
When her father died, he had multi-system organ failure. Riggs said she did not believe her father died of COVID-19, but instead due to the CDC- and NIH-approved protocols.
“He was isolated and kept from everyone that truly loved him for 16 days,” Riggs said. “Then, under the guise of ‘palliative care,’ he was finished off with fentanyl and midazolam.”
According to Alpha News, the price tag from the hospital for the treatment her father received during those 16 days was $1.2 million.
A statement provided by Abbott Northwestern to Alpha News said the following:
“Allina Health respects the privacy of its patients and is unable to comment on specific patient care.
“We have great confidence in the exceptional care our medical teams provide to our patients, which is administered according to evidence-based practices by our talented and compassionate care teams.”
‘To honor my dad, I have put my grief into action’
Riggs said her father’s death had knock-on effects on her and her family.
“Now my mom, who survived remdesivir, can’t afford to keep their home,” Riggs said. “She had to sell almost all of their possessions accumulated over 50 years to move into one of the bedrooms of my two-bedroom home. Two of my boys … now share a bedroom in our living room.”
“She can hardly make the bed without being out of breath and she struggles mentally with what they endured and getting a grasp on her new life without my dad in it,” Riggs added.
Despite these challenges, Riggs said that “to honor my dad, I have put my grief into action,” getting involved in activism for victims of hospital protocol deaths.
Riggs is now the Minnesota chair of the FormerFedsGroup Freedom Foundation, a national coalition that has documented cases involving COVID-19 care protocols at hospitals.
“I don’t want the families … to be isolated and alone in their pain of losing their loved one,” Riggs said, adding that she has launched weekly Zoom calls for Minnesota families and survivors of hospital protocols, and is also launching in-person meetups.
Riggs also recently attended the Halt Hospital Homicide rally, which she described as the “first national rally for hospital protocol deaths.”
She drew parallels with those who died of COVID-19 vaccine injuries. “The vax-injured are ignored and not believed, just like those of us who have had a family member die or get injured by the hospital protocols,” she said.
“My dad, Ralph, will go on in our memories as a wonderful husband of 50 years, dad, grandpa and great-grandpa, as well as a fun fisherman and the best homemade French fry maker around.”
Michael Nevradakis, Ph.D., based in Athens, Greece, is a senior reporter for The Defender and part of the rotation of hosts for CHD.TV’s “Good Morning CHD.”
This article was originally published by The Defender — Children’s Health Defense’s News & Views Website under Creative Commons license CC BY-NC-ND 4.0. Please consider subscribing to The Defender or donating to Children’s Health Defense.
May 16, 2023
Posted by aletho |
Science and Pseudo-Science, Timeless or most popular, War Crimes | CDC, Covid-19, COVID-19 Vaccine, Human rights, NIH, United States |
Leave a comment







{kind=link}