The World Health Organization (WHO) is proposing a set of recommendations for “social listening surveillance systems” designed to address what it describes as a “health threat” posed by online “misinformation.”
The WHO’s Preparedness and Resilience for Emerging Threats (PRET) initiative claims “misinformation” has resulted in an “infodemic” that poses a threat — even in instances where the information is “accurate.”
The latest draft of the pandemic treaty contains language on how WHO member states would commit to “social listening.” Under article 18(b), WHO member states would commit to:
“Conduct regular community outreach, social listening, and periodic analysis and consultations with civil society organization and media outlets to identify the prevalence and profiles of misinformation, which contribute to design communications and messaging strategies for the public to counteract misinformation, disinformation and false news, thereby strengthening public trust and promoting adherence to public health and social measures.”
Remarking on PRET’s “social listening” proposals, Michael Rectenwald, Ph.D., author of “Google Archipelago: The Digital Gulag and the Simulation of Freedom” and a former New York University liberal studies professor, told The Defender:
“The WHO’s PRET initiative is part of the UN’s attempt to institute global ‘medical’ tyranny using surveillance, ‘social listening’ and censorship. PRET is the technocratic arm of the WHO’s proposed pandemic treaty, which, if accepted by nation-states, would amount to the surrendering of national and individual sovereignty to this ‘global governance’ body.
“What better way to establish a one-world government than by using so-called global crises that must be addressed by nothing short of ‘global governance’? I remind readers that you cannot comply your way out of tyranny.”
WHO could use artificial intelligence to monitor social media conversations
A WHO document outlining the PRET initiative — “Module 1: Planning for respiratory pathogen pandemics, Version 1.0” — contains a definition of infodemic:
“Infodemic is the overabundance of information — accurate or not — which makes it difficult for individuals to adopt behaviors that will protect their health and the health of their families and communities.
“The infodemic can directly impact health, hamper the implementation of public health countermeasures and undermine trust and social cohesiveness.”
The document recommends that in response to the “infodemic,” countries should “incorporate the latest tools and approaches for shared learning and collective action established during the COVID-19 pandemic.”
According to the WHO document, this can be done if governments “establish and invest in resources for social listening surveillance systems and capacities to identify concerns as well as rumors and misinformation.”
Such resources include “new tools and approaches for social listening … using new technologies such as artificial intelligence to listen to population concerns on social media.”
According to the document:
“To build trust, it’s important to be responsive to needs and concerns, to relay timely information, and to train leaders and HCWs [healthcare workers] in risk communications principles and encourage their application.”
Risk communications “should be tailored to the community of interest, focusing on and prioritizing vulnerable groups,” the WHO said.
“Tailored” communication was a hallmark of public health efforts during the COVID-19 pandemic.
For instance, in November 2021, the Rockefeller Foundation, the National Science Foundation and the Social Science Research Council launched the Mercury Project, which aimed “to increase uptake of COVID-19 vaccines and other recommended public health measures by countering mis- and disinformation” — in part by studying “differential impacts across socio-demographic groups.”
Similarly, PRET states that it will “incorporate the latest tools and approaches for shared learning and collective action established during the COVID-19 pandemic.”
These “tools and approaches” could be deployed during “acute respiratory events,” according to the document, which recommends that governments:
“Develop and implement communication and behavior change strategies based on infodemic insights, and test them during acute respiratory events including seasonal influenza.
“This includes implementing infodemic management across sectors, and having a coordinated approach with other actors, including academia, civil society, and international agencies.”
This is not the first time the WHO has addressed the so-called “infodemic.”
A WHO review published Sept. 1, 2022, titled “Infodemics and health misinformation: a systematic review of reviews,” found that “infodemics and misinformation … often negatively impact people’s mental health and increase vaccine hesitancy, and can delay the provision of health care.”
In the review, the WHO concluded that “infodemics” can be addressed by “developing legal policies, creating and promoting awareness campaigns, improving health-related content in mass media and increasing people’s digital and health literacy.”
WHO, Google announce collaboration targeting ‘medical misinformation’
The WHO’s PRET proposals coincided with a new multi-year collaboration agreement with Google for the provision of “credible health-related information to help billions of people around the world respond to emerging and future public health issues.”
The agreement was announced on May 23 by Dr. Karen DeSalvo, Google’s chief health officer, on the company’s blog. She wrote:
“Information is a critical determinant of health. Getting the right information, at the right time can lead to better health outcomes for all. We saw this firsthand with the COVID-19 pandemic when it was difficult for people worldwide to find useful information online.
“We worked with the World Health Organization (WHO) on a range of efforts to help people make informed decisions about their health — from an SOS alert to surfacing locally relevant content about COVID-19 to YouTube policies on medical misinformation.”
One way Google will collaborate with the WHO is through the creation of more “knowledge panels” that will prominently appear in search results for health-related questions on the platform.
“Each day people come to Google Search looking for trustworthy information on various health conditions and symptoms,” DeSalvo wrote. “To help them access trustworthy information our Knowledge Panels cite content from reliable sources covering hundreds of conditions from the common cold to anxiety.”
“Working closely with WHO, we’ll soon expand to cover more conditions such as COPD [chronic obstructive pulmonary disease], hypertension, type 2 diabetes, Mpox, Ebola, depressive disorder, malaria and more,” she added.
Google will make these Knowledge Panels available in several languages, including English, Arabic, Chinese, French, Russian and Spanish.
DeSalvo’s May 23 post also addressed an ongoing collaboration between Google and the WHO, Open Health Stack (OHS), which “help[s] accelerate the digital transformation of health systems around the world” and “lower[s] the barrier to equitable healthcare.”
Google also awarded the WHO with more than $320 million “in donated Google Search advertising via ad grants” allowing the agency “to publish health topics beyond COVID-19, such as Mpox, mental health, flu, Ebola, and natural disasters.”
Google is slated to provide an additional $50 million in ad grants to the WHO this year.
According to Google, the ad grants to the WHO represent the company’s largest such donation to a single organization.
Separately, the U.S. Food and Drug Administration (FDA) tweeted on May 22 about the agency’s own efforts at combating purported “misinformation” and “disinformation.”
The tweet contains a 35-second video, which claims “misinformation” travels “six times faster than the facts,” while promoting the FDA’s “Rumor Control” initiative.
A top priority of FDA Commissioner Dr. Robert Califf, “Rumor Control” was launched in August 2022 and joins other agency initiatives to fight “misinformation” and “disinformation.”
“The growing spread of rumors, misinformation and disinformation about science, medicine, and the FDA, is putting patients and consumers at risk,” according to the FDA’s Rumor Control webpage. “We’re here to provide the facts.”
The initiative asks the public to do “three easy things” to “stop rumors from spreading”: “don’t believe the rumors,” “don’t pass them along” and “get health information from trusted sources like the FDA and our government partners.”
“Rumor Control” appears to have been inspired by an initiative developed by the Virality Project, “a coalition of research entities” from six institutions “focused on supporting real-time information exchange between the research community, public health officials, government agencies, civil society organizations, and social media platforms.”
Documents released as part of the “Twitter files” in March revealed that the Virality Project, based out of the Stanford Internet Observatory, also called for the creation of a disinformation board just one day before Biden announced plans to launch his government-run Disinformation Governance Board.
Similar to PRET’s recommendations to target “accurate” information that nevertheless contradicts establishment public health narratives, the Virality Project worked with Twitter and other social media platforms, recommending they “take action even against ‘stories of true vaccine side effects’ and ‘true posts which could fuel hesitancy.’”
These censorship efforts included at least one tweet by Robert F. Kennedy Jr., chairman on leave of Children’s Health Defense.
Michael Nevradakis, Ph.D., based in Athens, Greece, is a senior reporter for The Defender and part of the rotation of hosts for CHD.TV’s “Good Morning CHD.”
Democratic presidential candidate Robert F. Kennedy Jr recently said that if he becomes president, he will ban pharmaceutical advertising on US television.
“It’s not good to have pharmaceutical advertising on TV,” said Kennedy. “It’s good for the television stations, it’s good for the pharmaceutical companies, but it’s not good for public health.”
The US and New Zealand are the only two nations globally that allow drug companies to promote their products directly to the consumer – known as direct-to-consumer advertising (DTCA).
Kennedy said that because of pharmaceutical advertising in the US, Americans use more prescription drugs than anywhere else in the world, and yet, they have the worst outcomes.
Americans have the lowest life expectancy compared to other wealthy nations and the highest rate of avoidable deaths, despite spending nearly 18% of GDP on healthcare in 2021.
Kennedy told me he blames “the influence of the pharmaceutical lobby in Washington, and indirectly, the influence of media companies that earn some $18 billion in revenue annually from direct-to-consumer drug advertising.”
Drug advertising in the US
In the 80s, there were few prescription drug ads broadcast on US TV because the regulatory standard made it difficult to provide adequate information about drug labelling to consumers. David Kessler, FDA Commissioner between 1990 and 1997, also vigorously opposed DTCA.
But when Kessler left the agency, the new administration eased regulatory restrictions and the floodgates opened. Within a decade, DTCA went from US$2.1 billion in 1997 to US$9.6 billion in 2016.
“They do it because it works,” said Barbara Mintzes, professor of evidence-based pharmaceutical policy at the University of Sydney. “Drug companies would not be spending the money if it did not lead to expanded sales.”
Proponents argue that DTCA empowers the consumer with information about diseases and drug treatments by encouraging informed discussions between patients and their medical providers. But Mintzes is not convinced.
“I totally agree that people need information on medicines but getting that information from advertising is not the same as getting it from an unbiased source,” said Mintzes.
Mintzes has long argued against DTCA saying, “There is no public health rationale and no reliable evidence that it leads to better care, public or patient empowerment, or to the type of information needed for shared informed treatment choices.”
Many Americans are unaware of the persuasiveness of DTCA. A national FDA survey found that 29% of consumers believed that only completely safe medicines could be advertised on TV. In California, it was 42% of consumers.
Advertised drugs offer little benefit
The decision about which drugs are advertised is not made on public health grounds, but on what will maximise profits.
“It’s a marketing decision,” says Mintzes. “Often, it’s a small, select group of drugs that are very expensive, on patent, and are not necessarily the best available treatments in terms of effectiveness or safety.”
According to a recent study published in JAMA, most of Big Pharma’s spending (68%) on the top-selling prescription drugs in 2020, were of ‘low added benefit’ for patients.
The study’s lead author Michael DiStefano, a researcher at Johns Hopkins said it’s probably a strategy of the pharmaceutical industry to “drive patient demand for drugs that clinicians would be less likely to prescribe.”
“When a consumer sees these advertisements on TV or social media, they should really question if it’s the best drug for them and have a conversation with their provider,” said DiStefano.
Poor FDA oversight of DCTA
The FDA regulates the promotion of medicines and the content of DTCA, under the authority of the Federal Food, Drug and Cosmetic Act (FFDCA). It requires that advertising is accurate, and only promotes the drug for approved conditions, clearly stating harms and ways to get more information.
However, the agency lacks the resources to police it properly.
A 2002 Government Accountability Office report found the FDA’s oversight of DTCA was lacking. The agency had allowed some drug companies to repeatedly disseminate new misleading advertisements for the same drug.
Further, a change in the FDA’s procedures for reviewing draft regulatory letters led to a significant lag in issuing letters to demand the removal of misleading advertising – some regulatory letters were not even issued until after the advertising campaign had run its course.
Vioxx ads led to unnecessary deaths
From 1999 to 2004, Vioxx was among the most aggressively advertised medicines in the US. Merck spent more than US$100 million per year in advertising to consumers and generated annual sales of more than US$1 billion.
But Merck ran a deceptive advertising campaign, which misrepresented the safety of Vioxx and improperly concealed the drug’s increased risk of stroke. Vioxx was estimated to have caused 88,000–140,000 heart attacks in the USA alone – 44% of which were fatal.
A significant proportion of those people who died, took Vioxx after seeing it advertised on TV.
FDA promoted covid products
During the pandemic, the FDA began promoting covid-19 products – antivirals and vaccines – something that is not in the agency’s remit.
FDA commissioner Robert Califf, for example, repeatedly advertised the benefits of Pfizer’s antiviral drug paxlovid and covid-19 vaccines for reducing the risk of long covid.
“The FDA commissioner can’t tweet like this,” wrote Vinay Prasad, a practicing haematologist-oncologist at the University of California San Francisco. “How does the FDA preserve the authority to regulate truthful marketing, when the FDA commissioner is a billboard for Pfizer? These claims are not validated by the highest methods. This is unbelievable.”
In addition, director of the FDA’s vaccine division Peter Marks, featured in multiple videos on the FDA’s website, encouraging people to take the newly authorised bivalent boosters.
“It always feels odd to see the FDA promote products,” said Jessica Adams, a regulatory affairs expert. “The agency used to go out of its way to respect patient-provider decision-making and not interfere with the practice of medicine.”
In fact, the FDA’s own homepage was promoting the covid-19 vaccines.
“The FDA acts like a cheerleading or marketing arm of pharma companies, not a regulatory agency” said Aaron Siri, attorney at Siri & Glimstad law firm. “By promoting these shots, the FDA has hopelessly conflicted itself from later admitting these products have serious issues.”
“It is not the role of the FDA to promote vaccines or advise people to get them. Its role is to objectively assess whether they are safe and effective to its standard,” added Siri.
FDA’s revolving door
Kennedy has renewed calls to put an end to the FDA→Big Pharma “revolving door” which leads to undue influence over the agency.
Ten of the last 11 commissioners have gone on to secure roles with the pharmaceutical or biotech industries they once regulated – most within a year or two of leaving the FDA (see table).
Califf was announced as FDA commissioner on 17 Feb 2022 (his second time). SEC filings indicate that he resigned from the board of directors of Centessa Pharmaceuticals, the day before the announcement.
“That is an indication of just how completely industry has captured this agency,” said Kennedy vowing to shake up the system if he becomes president.
“We will institute new rules extending the waiting period before former officials can enter industry, consulting, and lobbying. We want real public servants in positions of public trust,” he added.
Kennedy believes the key to reforming the FDA will be to put qualified people in positions from outside the pharmaceutical industry, and to call on whistle-blowers, dissidents, and other people of integrity from within the FDA.
The FDA did not comment on the agency’s ‘revolving door’, nor did it answer whether the agency had considered instituting an extended waiting period between the time officials leave the FDA and enter industry.
Nobody believes in Remdesivir anymore. How can you possibly make a case for it? Remdesivir is so lethal it got nicknamed “Run Death Is Near” after it started killing thousands of Covid patients in the hospital. The experts claimed that Remdesivir would stop Covid; instead, it stopped kidney function, then blasted the liver and other organs.
As word got around, some patients started showing up in the emergency room with signs saying, “NO REMDESIVIR” and refusing to take it. (Not that their refusal helped: many were given it anyway, often without their knowledge.)
When I heard that Remdesivir is still being used, I couldn’t believe it. How could hospitals be so brazen as to push this killer drug, even after the lawsuits started flying? Fourteen California families are now suing three hospitals, claiming their loved ones suffered wrongful deaths from what they call “the Remdesivir protocol.” Expect other lawsuits to follow, because the Remdesivir carnage was nationwide.
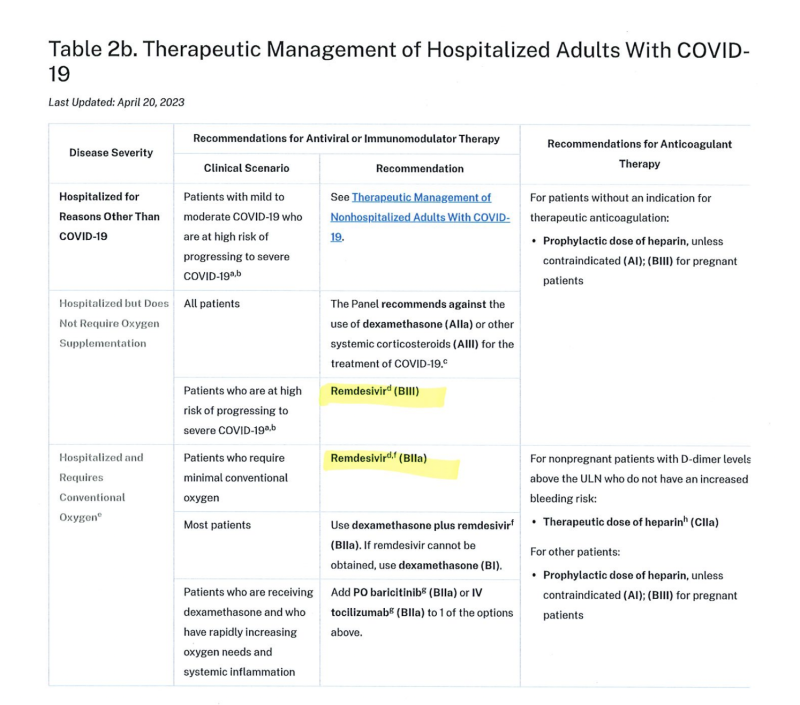
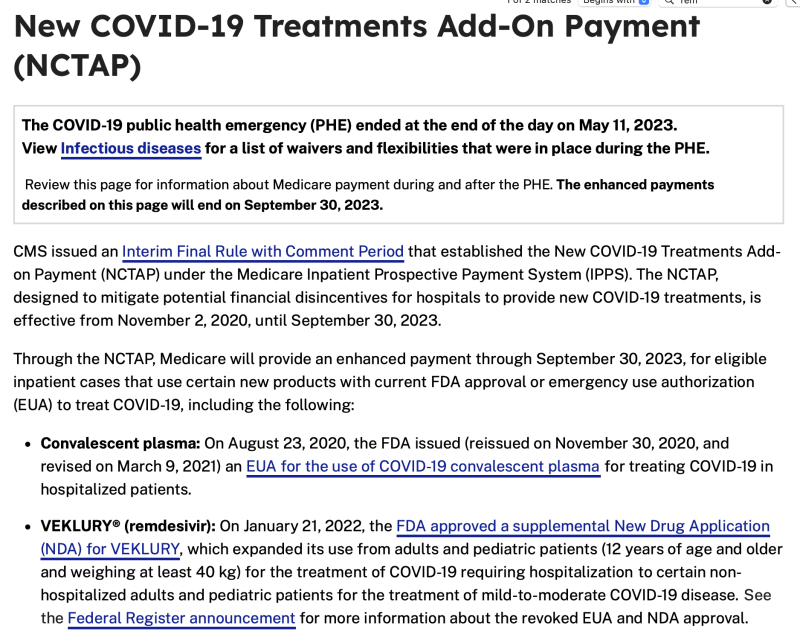
I began to poke around to see if hospitals are still giving Remdesivir and I think I’ve found the smoking gun. Two smoking guns, in fact. First, it’s still listed on the NIH web site as its standard of care for Covid. Second (and in my opinion, more importantly), the CMS.gov official website says, “The COVID-19 public health emergency (PCE) ended at the end of the day on May 11, 2023.” Two sentences later, it states, “The enhanced payments described on this page will end on September 30, 2023.” And there it is, listed in bold: Remdesivir.
Allow me to translate the bureaucratese. “Even though we acknowledge the Covid emergency is over, the federal government will continue to pay lavish bonuses to hospitals who kill their patients with Remdesivir through the end of the fiscal year.”
Money; it all comes down to money. There’s SO much money in the Covid con game. The CARES Act of 2020 slathered $2 trillion across the country to deal with Covid, and lots of it went to hospitals. The 20 largest hospitals enjoyed a 62 percent increase in their combined net assets during those glorious Covid years, providing many top executives with a $10 million salary or more.
Alas, the federal government insisted that if hospitals wanted to get paid, they had to treat Covid patients with Remdesivir. The fact that this drug was made by their good friends at Gilead Science and everybody was getting rich from the deals they cut had absolutely nothing to do with it, of course. It was all done for love of the people. But just to make sure that Remdesivir could attain its current billion-dollar status, the feds incentivized hospitals with a 20 percent boost to the entire hospital bill of patients treated with Remdesivir.
And here’s the kicker: the feds did not allow hospitals to even consider using safe, cheap drugs like ivermectin.
“Remdesivir caused a lot of renal failures,” Ralph Lorigo told me. Mr. Lorigo is a lawyer in Buffalo who spent last year helping families rescue loved ones who were trapped inside hospitals that were killing them. “If you got Covid, the hospital put you on this government protocol and didn’t even check if you have kidney disease. There was a real lack of monitoring.”
“I was surprised when the FDA approved it, even though The World Health Organization (WHO) had advised against using it. But Big Pharma had the strength to push it through.”
He added, “Hospitals had stopped doing elective cases, which is how they made money. So now they made money giving people Remdesivir and putting them on ventilators, which the government also paid big bonuses for. Every day you’re on a vent, it’s damaging you. When I managed to get people out of the hospital and off the vent and they got ivermectin, they lived. When I couldn’t get into court or lost the case, they died.”
It’s way past time for there to be a hard stop on the use of Remdesivir. And we must work fast to save the children. “In late April 2022, the FDA even approved remdesivir as the first and only COVID-19 treatment for children under 12, including babies as young as 28 days, an approval that boggles the mind, considering COVID-19 is rarely serious in children while remdesivir is ineffective and carries a risk of serious, and deadly, side effect,” writes Dr. Joseph Mercola.
In all my reporting on the Hospital Death Protocol, I’ve never heard a single person say, “You’re wrong. My mother perked right up when they gave her Remdesivir and the ventilation made her bounce out of bed. They saved her life!”
Instead, my inbox and Twitter feed are filled with messages that would make you break down and cry. The Bereaved Army in America needs an investigation into exactly who shattered their lives and why.
Stella Paul is the pen name of a writer in New York who has covered medical issues for over a decade. In 2021, she lost her husband in a locked down nursing home in New York City where he had been brutally isolated for almost a year. He died one week after getting the vaccine. Stella is focused on exposing the Hospital Death Protocol to honor her husband’s memory and to support thousands of bereaved families.
When the Covid-19 vaccines rolled out, public health officials took great pains to downplay how the vaccines spread from the injection site. Articles with language like this were common: “Most of the mRNA vaccine stayed in the injection site muscle—where you get the shot.”
We now know the truth. The lipid nanoparticles, or LNPs, travel widely throughout the body. These LNPs carry the Frankenstein mRNA that causes the cells to produce spike proteins.
We initially got tissue biodistribution data from Japan which showed that significant lipid concentrations were found in the adrenal glands, bone marrow, liver, ovaries, spleen (and more) for at least 48 hours after injection.
And from the lawsuit that we brought against the FDA demanding the release of the Pfizer documents, we now know that this same data was also provided to the FDA. What is really troubling, however, is that this document was dated November 9, 2020—meaning, prior to any Emergency Use Authorization or public use of Pfizer’s Covid-19 vaccine.
Having LNPs release their cargo into the cells of critical organs is very concerning. This is because many scientists will tell you that the spike protein produces an immune response, including inflammation. It is one thing to have inflammation in one’s bicep, but it is quite another to have it in your heart muscle, liver, ovaries, etc.
This is again why the government should not be in the business of promoting, let alone mandating, any product. It becomes impossible to acknowledge safety issues without self-incrimination. How often do you hear the government say, “Oops, you know that thing we told every American to inject into their body? Well, it actually can cause serious harm to a lot of people—our bad!” No. That rarely happens.
CONCLUDING REMARK
As I have written in the past, the lack of respect for individual and civil rights has wrought more harm on humanity than anything else. The American experiment was a rebellion against the idea that you must cede your rights to some overseers who know better and will make decisions on your behalf.
To that end, as I also often repeat, please send the following proposed legislation to your legislative representatives:
No law may require or coerce a person to receive or use a medical product, or impose a penalty or deprive a benefit for refusing a medical product or refusing to disclose whether a person has received a medical product.
Medical freedom is freedom. If you cannot get a job, go to school, or otherwise participate in civil society because you refuse a medical product, you are not free. What good are your rights if you can only exercise them at home by yourself? That is why medical freedom is a fundamental right that must be permanently fixed into the law of every civilized nation.
We are, as provided in the Declaration of Independence, indeed “endowed by [our] Creator with certain unalienable Rights” and to safeguard those rights “we mutually pledge to each other our Lives, our Fortunes, and our sacred Honor.” We must never yield to the tyranny of permitting others to dictate what can or must be placed, administered, or injected onto or into our bodies. For once that right is ceded, none truly remain.
Advisers to the U.S. Food and Drug Administration (FDA) on Thursday recommended, by a vote of 10 to 4, that the agency approve Pfizer’s respiratory syncytial virus (RSV) vaccine for pregnant women, despite questions about the vaccine’s safety.
During Thursday’s Vaccines and Related Biological Products Advisory Committee (VRBPAC) meeting, committee members and medical experts raised concerns about premature births identified during Pfizer’s clinical trials.
The FDA is expected to issue a final decision on the vaccine in August. If approved, it would become the first RSV vaccine authorized for pregnant women.
The Centers for Disease Control and Prevention (CDC) must “sign off” on Pfizer’s vaccine for pregnant women prior to it becoming available to the public.
Dr. Meryl Nass, an internist, biological warfare epidemiologist and member of the Children’s Health Defense (CHD) scientific advisory committee, told The Defender that while the FDA is not obliged to follow the recommendations of its advisory committees, “it almost always does so.”
The appeal of a maternal vaccine like Pfizer’s is “the way it would create neutralizing antibodies in pregnant women that can be transferred to infants in the womb,” Axios reported.
However, “there are health risks, including preterm births,” Axios added, noting that GlaxoSmithKline Biologicals’ (GSK) recently halted its trial of a similar RSV vaccine for infants. According to NBC News, the GSK vaccine “showed a higher preterm birth rate among some vaccine recipients.”
Commenting on the FDA’s recommendation of Pfizer’s RSV vaccine, Dr. Peter McCullough, a cardiologist, told The Defender :
“This product represents an unprecedented attempt to vaccinate mothers for no benefit to them and only theoretical efficacy in babies. In the trial, less than 2% of infants at any time point contracted RSV, which is easily treatable with nebulizers.
“Pregnancies should not be threatened with novel vaccines for uncommon and low-risk infantile illnesses.
“Widespread use of this reactogenic vaccine can be expected to cause fetal loss in some unfortunate women. A single case of pregnancy termination would not be worth the population being vaccinated.”
The positive recommendation from the VRBPAC comes two weeks after the FDA approved Arexvy, the first vaccine authorized for RSV. That vaccine, produced by GSK, is intended for adults 60 years of age and older.
It also comes as Pfizer is expecting an FDA decision later this month for its RSV vaccine for adults 60 and over, with the same formulation as the one for pregnant women. The VRBPAC recommended the vaccine for this age group in February.
Pfizer is also “evaluating how its shot performs in other age groups,” Axios reported.
‘A sad day for babies and mums’
According to CNBC, Pfizer’s RSV vaccine, marketed as Abrysvo, will be administered as a single dose to pregnant women in their second or third trimester.
NBC News reported that the shot would be given to pregnant women at 24 to 36 weeks gestation and that the “protective antibodies transfer to infants through the placenta.”
The FDA advisory panel found that data from Abrysvo’s clinical trial “supports the safety of the vaccine” for pregnant women, while the same panel voted unanimously “that available data supported the vaccine’s efficacy for giving the shot to women in their second or third trimesters of pregnancy.”
An FDA briefing document said safety data from Abrysvo clinical trials was “generally favorable.”
According to the trial data, Abrysvo “had an 81.7% efficacy at protecting newborns in the first three months of life against severe illness and a 69.4% efficacy through the first six months,” Axios reported.
The trial consisted of nearly 7,400 participants, according to NBC News, adding that Abrysvo “also lowered the risk of developing respiratory disease from RSV that required doctors’ visits by 51% within about six months.”
“After that, however, the vaccine didn’t appear to make a big difference,” according to the NBC News report, which also reported that “a slightly higher rate of preterm births — defined as before 37 weeks’ gestation — among people who received the vaccine (5.7%) versus those who got a placebo (4.7%)” was identified.
“The difference wasn’t statistically significant, however, so it’s unclear whether it was vaccine-related,” NBC News added. CNBC reported that both percentages were below the overall percentage for preterm births in the general population (10%).
According to CNBC, the clinical trial for Abrysvo “reported 18 peripartum fetal deaths.”
However, the FDA said these deaths were “unlikely” to be related to the shot. According to Axios, “The fetal deaths present in the vaccine group (0.3%) were not related to Pfizer’s vaccine … Similarly, 4 out of 5 infant deaths were considered unrelated to the shot, with one being possibly connected to the shot, although that remains unclear.”
Data reported by Pfizer to the CDC indicated that 14% of pregnant women who participated in Pfizer’s trial sustained an adverse event, with 4.2% sustaining a “serious” adverse event, 1.7% experiencing a “severe” adverse event and 0.5% suffering a “life-threatening” adverse event.
Similarly, the same data showed that 37.1% of infants whose mothers received the experimental Pfizer vaccine experienced adverse events within one month of birth — with 15.5% classified as “serious,” 4.5% as “severe” and 1% as “life-threatening,” while efficacy waned within months of vaccination.
According to the National Vaccine Information Center (NVIC), “The RSV clinical trial data also included the death of one pregnant woman, 18 stillbirths (10 in vaccinated pregnant women and eight in unvaccinated pregnant women), and 17 infant deaths (five from the vaccinated pregnancy group and 12 in unvaccinated pregnancy group).”
Attorney, journalist and podcaster Daniel Horowitz, in an article published Monday in the Conservative Review, quoted Phase 2 trial data for Abrysvo. He wrote: “Pfizer reported 3 out of 116 (2.6%) premature births in the placebo group and 6 out of 114 (5.3%) in the group that received the vaccine that was chosen as Pfizer’s final product,” adding that Pfizer “was studying preterm birth as an ‘adverse event of special interest.’”
According to NBC News, “The most common side effects of the shot reported among pregnant women were fatigue, headache, muscle pain and injection site pain.”
Nass told The Defender there were essentially three problems with the Abrysvo clinical trial data, “two of which were identified by Pfizer and the FDA.” She said:
“There were about 20% more preterm babies and low birth weight babies in the group, whose mothers had been vaccinated versus the group whose mothers had received a placebo. This was very concerning but was disregarded by most of the committee.
“It was unclear to me whether Pfizer had collected enough information on the health of the pregnant women after vaccination. It is hard to tell when you were studying, newborns and babies, whether they have had a side effect from their mothers’ vaccination. The children weren’t studied for long enough to compare their intellectual ability or other parameters.”
The third problem reflected concerns arising from the problems GSK’s candidate vaccine for pregnant women encountered, Nass said. However, “the FDA claimed the GSK clinical trial data were proprietary, and they were unable to provide them,” even though it was pointed out that these findings had been published and were in the public domain.”
“No one questioned the veracity of the data Pfizer presented, despite the fact that Pfizer repeatedly presented data on its COVID vaccine efficacy to this committee that made the vaccines appear much more efficacious than they turned out to be,” Nass said.
McCullough, writing on his Substack, also questioned the Abrysvo clinical trial data. “Pfizer has aggressively advanced RCTs [randomized controlled trials] into the pregnant population with no assurances on long term outcomes. There is no direct benefit to the mothers.”
“Furthermore, the sponsors moved the goal posts to make it easier to have a successful trial. We should demand long-term safety, high efficacy … and at least one year of durability, for such a rare and easy-to-treat condition in babies,” he added.
Calls for ‘tougher scrutiny’ of the RSV vaccine ignored
Some health experts called for “tougher scrutiny” of Abrysvo leading up to Thursday’s VRBPAC meeting, Axios reported, “after trials for GlaxoSmithKline halted trial for a similar shot over increased risks of preterm births and neonatal deaths.”
“Pfizer has not reported similar safety concerns, but some health experts told the British Medical Journal [BMJ] that they hope FDA staff will take the GlaxoSmithKline results into consideration when reviewing the vaccine,” according to Axios.
“Results have raised concerns about a possible increase in preterm births, and experts are calling for further analyses of the data and for post-approval monitoring of the vaccine, should the FDA approve it,” The BMJ analysis stated.
Horowitz said the “formulations of most of these shots are likely very similar, so red flags from one cohort of the study should inform us on the problems with the other.”
According to Nass, who live-blogged the meeting, one VRBPAC member, Dr. Henry H. Bernstein, a professor of pediatrics at Hofstra University, said during the meeting “he does not want another rotavirus vaccine repeat, in which the signal was known when licensed, but was not statistically significant.”
The rotavirus vaccine was pulled within one year because of intussusception, she said. Intussusception is a life-threatening illness that occurs when a portion of the intestine folds like a telescope, with one segment slipping inside another segment. This causes an obstruction, preventing the passage of food that is being digested through the intestine.
Dr. Paul Offit, a pediatrician at Children’s Hospital of Philadelphia and VRBPAC panelist, was quoted by CNBC as saying that the problems with GSK’s trial are “hanging over” Pfizer’s RSV shot for pregnant women and infants.
“If GSK truly abandons a program on a similar, almost identical vaccine, that is going to hang over [Pfizer’s] program. I think it needs to be addressed,” Offit added.
Offit separately told Reuters “I worry that if preterm births are in any way a consequence of this vaccine that would be tragic in many ways.”
Science magazine quoted FDA medical officer Dr. Yugenia Hong-Nguyen, who said the rate of premature births was “not statistically significant and lower than background incidence rates in the general population.”
Other VRBPAC members were less concerned. Dr. Daniel Feikin, a Johns Hopkins University epidemiologist and “temporary voting member”, said, “I’m not convinced that there’s a clear causal relationship between this vaccine and preterm birth,” Reuters reported.
Another VRBPAC panelist, Dr. Jay Portnoy, a pediatrics professor at the University of Missouri-Kansas City, said, “If the vaccine actually lives up to the data that we’ve seen today, I can guarantee that many infants and their parents will breathe easier in the coming years.”
Pfizer representatives also sought to downplay concerns with Abrysvo. According to CNBC, Dr. William Gruber, Pfizer’s senior vice president of vaccine clinical research and development, said, “Certainly in our eyes, there is no definitive evidence to suggest that there is a risk of prematurity.”
“So, the question is, do you hold hostage the potential benefits of the vaccine for something which you have no statistical significance at this point?”
Dr. Anthony Fauci also raised concerns about vaccines for respiratory illnesses, Horowitz wrote in a May 4 article. A paper co-authored by Fauci and published in January in Cell Host & Microbe stated that the challenges for RSV and flu vaccines were “many and complex” and that RSV vaccines were not good at providing immunity.
In a November 2022 episode of “RFK Jr. The Defender” podcast, Robert F. Kennedy Jr., then-chairman and chief litigation counsel for CHD (now chairman on leave), described RSV as “a vehicle for re-implementing the COVID-19 playbook all over the country and responding with vaccines.”
Nass characterized Thursday’s VRBPAC approval of Abrysvo as “a sad day for babies and mums,” adding, “Is there a reason to trust Pfizer’s data on its RSV vaccine, when we could not trust its COVID vaccines?”
“Currently, pregnant women are advised (not by me!) to get the flu, TdaP [tetanus-diphtheria-pertussis] and COVID vaccines during pregnancy. This would be a fourth pregnancy vaccine,” Nass wrote.
Nass said Thursday’s VRBPAC meeting was held with four temporary members.
“Did FDA stuff the meeting with four new temporary members in order to get the majority yes votes it wanted?” Nass asked.
Horowitz noted in his article published Monday that Pfizer vaccines have previously been approved despite concerns about their impact on pregnant women, citing trial data from the Pfizer-BioNTech COVID-19 vaccine.
Pfizer seeks to ‘offset declining revenue from its COVID-19 products’
According to Reuters, “Pfizer is counting on new medicines and vaccines to help offset declining revenue from its COVID-19 products,” noting that the market for RSV vaccines is expected to surpass $10 billion by 2030 and that Pfizer is “ready to launch” its RSV vaccines for both pregnant women and older adults “later this year.”
Pfizer CEO Albert Bourla said he expects increased revenue for the company in the coming years from the company’s RSV and flu shots.
On her Substack, Nass noted:
“As a consequence of the 21st Century Cures Act of 2016, all vaccines recommended by CDC for pregnant women have all manufacturer liability waived, and are placed in the national vaccine injury compensation program. This improves profitability and may result in mandates.”
Several other Big Pharma drugmakers are now clamoring to enter the potentially lucrative RSV vaccine market, after decades of failed attempts to develop a vaccine.
Moderna is developing an mRNA RSV vaccine for older adults. According to Axios, it “was found to be 83.7% effective in preventing RSV with one or two more symptoms” and “The company plans to apply for FDA approval this quarter.”
Bavarian Nordic, known for its development of a vaccine in response to last year’s monkeypox outbreak, is also developing an RSV vaccine for adults 60 and over,” expecting to release Phase 3 clinical trial data by midyear.
AstraZeneca and Sanofi also are seeking FDA approval for a monoclonal antibody treatment for RSV that would be administered to infants and toddlers up to age 2. Sanofi says the antibody, nirsevimab, was found to be 83.2% effective in reducing RSV-related hospitalizations.
However, the NVIC reported that the effectiveness of nirsevimab “is not known beyond 150 days” and it is unclear if the drug prevents ICU stays or deaths.
In all, “Eleven RSV vaccines (including GSK’s approved shot) are being actively studied in U.S. trials,” NBC News reported. “Six are for older adults, and five are designed to protect infants or children.”
Michael Nevradakis, Ph.D., based in Athens, Greece, is a senior reporter for The Defender and part of the rotation of hosts for CHD.TV’s “Good Morning CHD.”
Less than a year after successfully winning the fight to force Pfizer to release their COVID-19 vaccine trial data that the FDA was attempting to block for 75 years, ICAN’s Lead Counsel, Aaron Siri, Esq., joins Del with a new, updated ruling, and great news about what this ruling means for Pfizer and Moderna’s COVID vaccine trial data.
Biden’s new pick for Head of the NIH, Monica Bertagnolli, received more than 290 million in grants from Pfizer. This appointment comes more than a year after former director, Francis Collins, left the beleaguered agency. With deep ties to Pfizer and the cancer industry, she joins a roster of agency heads with questionable conflicts of interest, contributing to a growing distrust of our health agencies now seemingly beyond repair.
Previously, I wrote about Makena, a synthetic hormone given to millions of pregnant woman, to prevent premature birth. It was highly controversial because there was no robust proof that it was safe or effective, despite having FDA-approval.
Last month, after many years of use, the FDA finally decided to withdrawMakena from the market.
Adam Urato, a maternal-foetal medicine specialist at MetroWest Medical Centre, Massachusetts welcomed the decision, but said it took the FDA far too long.
“I cannot believe we’ve been injecting this hormone into pregnant women for 20 years, all the leading medical organisations recommended it, the FDA approved it – and it took this long to finally acknowledge the drug did not work,” he said.
Urato opposed the use of Makena from the start. He testified before the FDA, he wrote in the media and in medical journals, and helped petition the FDA to withdraw the drug from the market.
Adam Urato, maternal-foetal medicine specialist, MetroWest Medical Centre, Massachusetts.
Preterm birth is a major issue in obstetrics. In the US, one in 10 babies are born prematurely, and accounts for most of the neonatal morbidity and mortality.
Physicians were desperate for a solution, and Makena seemed to hold promise.
It wasn’t cheap though. Makena was 5,200% more expensive than generic versions of the same medication.
Large amounts of public money in the Medicaid program and other health insurance dollars were used to pay for the weekly shots at a total cost of $30,000 per pregnancy.
How it began
The drug maker sought fast-track approval of Makena, citing a 2003 study that was so flawed, the FDA’s own statistical reviewer commented that the drug was not worth approving.
The FDA approved it anyway on the basis that the drugmaker conduct more in-depth research into the medication’s effectiveness.
Then, in 2019 a confirmatory trial found the drug did not work. And by this stage, there were documented harms including gestational diabetes, depression, blood clots and a non-statistical doubling in stillbirths.
But instead of pulling the drug off the market, the FDA allowed Makena to be licensed for another four years.
“It should’ve been pulled immediately,” said Urato. “There were substantial profits for the drug company even after a confirmatory trial found it did not work, so it’s no wonder it was dragging its feet.”
It begs the question…
How is it even possible that a drug, which was neither safe nor effective for pregnant women, was allowed to be on the market for so long?
Urato says it’s a direct symptom of the medical-industrial complex – an entanglement of big pharma, medical organisations, and regulatory agencies – that creates an underlying motive to bolster profits, over health.
“For two decades the drug brought in billions in profits, and that money was used to fund physicians, researchers, professional medical societies, and academic institutions,” said Urato.
This makes it exceedingly difficult, if not impossible, for patients to navigate the healthcare system and know who to trust.
“We need elected officials that are going to put the interests of patients and the public first, and not be tainted, or corrupted by industry. We need to separate our politics and our regulatory bodies from industry funding,” he added.
Lesson learned?
Urato feels vindicated for his work, but says it’s no time for a victory lap. Instead, the Makena fiasco should provide us with tangible lessons to safeguard us against such scientific transgressions in the future.
“We must ‘first do no harm’ and follow the precautionary principle,” insisted Urato.
“When you’re exposing developing babies to synthetic chemical compounds, you can’t just assume it’s safe, until harm is proven. You must assume that the chemicals are having chemical effects on the foetus, because that’s what chemicals do.”
The Diethylstilbestrol (DES) disaster should have been a reminder to all obstetricians about the harms of giving synthetic hormones to pregnant women without sufficient data. But once Makena was rolled out, Urato said, “it was like everyone forgot the past.”
“I counselled my patients on my concerns about exposing them and their babies to a synthetic hormone with unknown short and long-term effects, so I guess I could have been accused of peddling ‘misinformation’,” said Urato cognisant that he was going against medical consensus.
“But what is considered misinformation today, may be scientific fact tomorrow. I helped to prevent a generation of mums and babies in my community from being exposed to a useless drug. That’s why it’s so important that doctors have freedom of speech to express their views,” said Urato.
It’s estimated that hundreds of thousands of pregnant mothers and babies were exposed to the ineffective and risky synthetic hormone over the past 2 decades.
“Time and time again, drugs and devices are pulled off the market for safety issues. If the FDA approves a drug, it does not mean that it will be proven to be safe and effective over time. The FDA has lost the public’s trust,” Urato said.
The history of the CDC during covid has been, at best, a checkered one.
Given what we now know about the complete failure of covid vaccines to provide sterilizing immunity, stop infection, or stop spread as well as the fact that such issues were not even tested for in the drug trials that approved them, certain questions would seem overdue in the asking:
Just what was this “Data from the CDC today” that suggested that “Vaccinated people do not carry the virus?”
Was there, in fact, any data at all?
Or was this a completely fabricated claim used to underpin the mass rollout of a product that failed so spectacularly right out of the gates and:
There seems to be an awfully large body of claims made by CDC that appear to have lacked foundation in fact or data. Both Dr Walensky and her predecessor Robert Redfield would seem to have a great deal to answer for here.
This talking point was simply everywhere all at once.
Pfizer CEO Albert Bourla certainly pushed this narrative. Presumably, the fact that he was allowed to do so (itself quite an exceptional situation) implies the acquiescence of FDA, CDC, and other regulators.
Upon what was this seemingly widespread consensus based?
The matter appears to have never even been studied at the time the claims were made.
Why were the usually strict and fastidious US regulators so sanguine about such unusually aggressive and certain statements?
This is a most unusual situation and such an extraordinary outcome would seem to demand an extraordinary explanation.
Yet none seems forthcoming.
“The mRNA and the spike protein do not last long in the body” constitutes another key early safety claim similarly rooted in opaque or absent evidence or perhaps simply assumed or invented. (before being quietly retracted later).
This claim also proved extravagantly incorrect.
Wherever one looks, it seems one finds that these grand claims of safety and efficacy were underpinned by a paucity or utter absence of supporting evidence.
Even the definitions themselves such as “Any positive for trace covid from a PCR test at a 40 Cycle Threshold is covid” or “No disease outcomes from vaccines are to be counted until 2 weeks after the second (or third) dose” which left a large window (4-6 weeks) during a period of known immune suppression from the jabs uncounted or even, in many cases, attributed to the unvaccinated in a manner that can make placebo look like high efficacy preventative are so unusual and inconsistent with past practice or sound science as to demand the most pointed of questions as to how such practices came to be and who the decision makers who put them in place were.
This series of unfounded claims and distortionary definitions seems both a poor and a deeply dangerous practice for Public Health.
If we are to have any hope of restoring faith in this field, we must ask and answer the pointed questions of “How did this happen?” and “At whose behest?”
Someone made these choices for some reason. Who and why would seem to be the bare minimum of post mortem here.
It is oft opined that a bad map is worse than no map at all and in this, I must wholeheartedly agree. The public health agencies in America have become the most calamitous of cartographers.
If we would seek to have the agents of public health act as something other than a marketing arm and apologist for the revolving door of Pharma with whom they seem to so regularly swap staff and sinecure then it must once more be turned to serve the public. It may do so only if it regains the public trust and such trust, once lost, may only be restored by asking the hard questions and diligently following the answers wherever so they may lead until we may understand what went wrong, hold the malefactors to account, and effect the means to prevent this from happening again.
Please make no mistake, if nothing is done and this is swept beneath some august Congressional rug or societal memory hole, it will happen again. And soon. This is not a choice I would have for America and one I do not believe you should countenance.
Describing it as the “future of how we need to feed people,” a group of scientists and researchers from Washington State University (WSU) enjoyed some “smoky, and mildly salty” pork sausage earlier this month — derived from gene-edited pigs.
The WSU research team recently received approval from the U.S. Food and Drug Administration (FDA) to allow pork meat from gene-edited pigs into the human food supply — resulting in the celebratory barbecue featuring sausage with “a good snap to the casings … just like regular pork.”
The FDA approval, which does not appear on the agency’s website, is investigational and limited to the specific pigs raised by the research team for this purpose. It is touted as evidence that “gene-editing livestock to quickly produce desirable traits for improved food production is a viable strategy for helping feed the planet’s growing population.”
However, some scientists and food safety advocates question the safety of the gene-editing technology — CRISPR (clustered regularly interspaced short palindromic repeats) — used by the WSU researchers and backed by investors like Bill Gates, and wonder if the products produced by the technology are really safe for human consumption.
‘Gene-edited meats could be mass produced for human consumption in 10 years’
Put differently, this technology allows scientists to edit sections of DNA by “snipping” specific portions of it and replacing them with new segments. Gene editing is not a new concept, but CRISPR technology is viewed as being cheaper and more accurate than other gene-editing technologies.
The WSU research team, led by Jon Oatley, Ph.D., associate dean for research for the College of Veterinary Medicine and tenured professor in the School of Molecular Biosciences, used CRISPR “to improve genetic traits in livestock.”
According to Nextgov, Oatley sought “to demonstrate that food made from the [gene-edited] animals is safe to eat and that it is possible for an academic institution to achieve this type of FDA authorization.”
“Gene-editing can make changes in an organism’s DNA that could occur in nature or through selective breeding but would take much longer without a tool like CRISPR,” Nextgov writes.
Oregon Public Broadcasting reported that WSU “is also studying CRISPR gene editing on cattle and sheep,” and wrapped up a goat study last year. “If all goes as planned … gene-edited meats could be mass produced for human consumption in 10 years.”
FDA’s investigational authorization is limited to five pigs. A WSU announcement described the work by Oatley and his team as “essentially a high-tech form of selective breeding,” adding that the pigs were originally gene-edited in a way that “would enable researchers to use them to sire offspring with traits from another male pig.”
According to WSU:
“Known as surrogate sires, this technology first gene-edits male animals to be sterile by knocking out a gene called NANOS2 that is specific to male fertility. These animals can then be implanted with another male’s stem cells that create sperm with that male’s desired traits to be passed on to the next generation.”
The research “has the potential to not just improve meat quality but the health and resilience of livestock in the face of changing environmental conditions, a critical goal for increasing protein sources in developing nations,” WSU said.
According to the university’s announcement, Oatley said:
“It’s important for a university to set the precedent by working with federal regulators to get these animals introduced into the food supply. … If we don’t go through that process, all of the research we’re doing is for naught because it will never make it out into the public.”
“The original intent in making these animals was to try to improve the way that we feed people,” Oatley said. “And we can’t do that unless we can work with the FDA system to get these animals actually into the food chain.”
WSU’s announcement did not mention Oatley’s membership on the Gene Editing in Agriculture Task Force, a collaboration of the American Association of Veterinary Medical Colleges and the Association of Public and Land-grant Universities created in June 2020.
“The next frontier in devising strategies to effectively feed a growing global human population will be defined by genetic enhancement; gene editing technologies are a key component in this endeavor.”
According to WSU, “The surrogate sires’ progeny, which are themselves not gene-edited, have not yet been reviewed by the FDA for possible inclusion in the food chain.” However, the original pigs “were processed at the WSU Meat Lab, and the U.S. Department of Agriculture inspected the meat as it does with all meat products.”
The meat “will be used in catering services that raise travel funds for the student members of the WSU Meat Judging team,” WSU said.
CRISPR: ‘It’s not precise and it’s not breeding’
The public often holds “many misconceptions about gene-editing,” Oatley said, adding:
“There’s a trust that comes with university-based research. … At WSU, we’re all about the science. We just want to make sure the research is valid, and the animals we produce are healthy.”
However, other experts have previously raised questions about the potential safety risks of inserting gene-edited and lab-grown meat into the human food supply and using tools such as CRISPR for this purpose.
In October 2022 interviews with The Defender, Michael Antoniou, Ph.D., head of the Gene Expression and Therapy Group at King’s College London, and Claire Robinson, managing editor of GMWatch, explained why they believe the risks of developing gene-edited meats and using CRISPR in this process outweighs the benefits.
Though CRISPR is often described as a “precision” gene-editing technology, Antoniou told The Defender, “It is not precise and it’s not breeding.”
Robinson told The Defender :
“These were also risks with the old-style GMOs [genetically modified organisms], and they are still risks with these gene-edited GM plants and animals.
“The risks, if you’re gene editing them … are that there will be knock-on effects on the animals, welfare or health that we can’t anticipate, such as deformities or changes in the function of certain genes in the animal.”
Antoniou warned that there may be unintended or unforeseen effects arising from this process. He said:
“Innately, gene editing also can bring about unintended DNA damage … even at the site of your intended edit or elsewhere in the DNA of your target cells, with unknown downstream consequences.
“None of these products … have been tested properly.”
A report published in the Journal of Genetics and Genomics in 2020 found that CRISPR gene-editing in rice resulted in numerous unintended and undesirable on-target and off-target mutations.
However, major investors like Gates see significant potential in foods created via gene editing and CRISPR.
According toBusiness Insider, Gates has said, “Researchers are studying ways to modify the genes of livestock animals … to make them produce milk more like dairy cows” and “make dairy cattle more resilient in hot weather.”
Gates and other proponents of CRISPR also claim that such tools — and the development and production of gene-edited meats — can serve as a solution to increased food demand due to a growing global population.
Robinson, in her October 2022 remarks, disputed such claims. She said:
“There’s no shortage of food in the world. Even in those countries where there are terrible hunger problems, they are producing food and it is available for those to buy if you have money.
“But the problem with hunger is, of course, poverty. The failure of infrastructure, the fact that you cannot get food to the hungry people. But mostly it’s inequality, things like wars and conflicts that are going on in some countries that mean that supply chains are disrupted. So really, there is no shortage of food and there isn’t ever likely to be.”
Instead, Robinson said that major corporate interests lie behind the use of CRISPR for the development of gene-edited food products.
“What we want to avoid,” said Robinson, “is a situation where the food supply ends up entirely patented, owned by big corporations … The patents on CRISPR are mostly owned by Corteva. Another patent owner used to be Monsanto, now owned by Bayer.”
Robinson added:
“The technology is patented; the products are patented. Therefore, it is all about increasing corporate control of the food supply.”
More FDA approvals of gene-edited meats likely coming soon
The FDA has approved only one other organization’s gene-edited animal for entering the food supply, according to WSU. The company, Acceligen, produces “slick-haired cattle,” which are gene-edited to grow coats that increase their resilience to higher temperatures.
The FDA’s March 7, 2022, announcement about the approval stated that “the intentional genomic alteration (IGA) does not raise any safety concerns” and that this was the agency’s “first low-risk determination for enforcement discretion for an IGA in an animal for food use.”
“We expect that our decision will encourage other developers to bring animal biotechnology products forward for the FDA’s risk determination in this rapidly developing field, paving the way for animals containing low-risk IGAs to more efficiently reach the marketplace,” said Dr. Steven M. Solomon, director of the FDA’s Center for Veterinary Medicine.
In recent years, the FDA also approved — or is close to granting full approval to — other gene-edited meat products for human consumption.
On Dec. 14, 2020, the FDA approved “a first-of-its-kind intentional genomic alteration (IGA) in a line of domestic pigs, referred to as GalSafe pigs, which may be used for food or human therapeutics. This is the first IGA in an animal that the FDA approved for both human food consumption and as a source for potential therapeutic uses.”
According to the FDA, the IGA in GalSafe pigs is intended to eliminate alpha-gal sugar on the surface of the pigs’ cells. “People with Alpha-gal syndrome (AGS) may have mild to severe allergic reactions to alpha-gal sugar found in red meat,” the FDA said, adding that the potential environmental impact “is no greater than from conventional pigs.”
The FDA also said it noted “no animal safety concerns” for GalSafe pigs “beyond those that would be expected in well-managed, commercial swine operations,” and “the microbial food safety risk is low and is mitigated by the low number of GalSafe pigs entering the food supply and the ongoing surveillance for antimicrobial resistance, among other factors.”
And in November 2022, the FDA declared lab-grown chicken meat developed by Upside Foods, a California-based firm, safe for human consumption, as part of its completion of a pre-market consultation that will likely lead to full FDA approval.
The FDA’s Nov. 16, 2022, announcement described this development as “a food revolution” that enables “food developers to use animal cells obtained from livestock, poultry, and seafood in the production of food, with these products expected to be ready for the U.S. market in the near future.”
The lab-grown chicken appears to have been developed using a process involving CRISPR. In 2019, it was reported that Memphis Meats — the former name of Upside Foods prior to a 2021 rebrand — was employing CRISPR as part of its process for curating lab-grown meat, and even received a patent for this purpose.
Michael Nevradakis, Ph.D., based in Athens, Greece, is a senior reporter for The Defender and part of the rotation of hosts for CHD.TV’s “Good Morning CHD.”
As you may recall, we obtained a court order in January 2022 forcing FDA to produce all of its data on Pfizer’s covid vaccine for those 16 years and older at a rate of 55,000 pages per month, as opposed to the 75 years FDA sought. That production should be completed in a few more months.
In a second lawsuit we brought, the same judge just ordered FDA to produce the documents it relied on to license and Moderna’s covid vaccine AND Pfizer’s covid vaccine for 12-to-15-year-olds at an average rate of at least 180,000 pages per month.
In this second lawsuit, this time also on behalf of the parents of Maddie de Garay, a young girl grievously injured in Pfizer’s clinical trial for 12-to-15-year-olds, we explained to the Court the importance of timely production. Once again, FDA claimed it would be “impractical” to release the estimated 4.8 million pages at more than between 1,000 to 16,000 pages per month, or in other words at least 23.5 years. We countered, demanding FDA produce all documents by mid-2025.
The federal judge, in an amazing decision, started by stating that “Democracy dies behind closed doors” andordered them to produce the files – millions of pages – in just 2 years, amounting to a rate of at least 180,000 pages per month.
Indeed, it is another blow for transparency and accountability. The Judge’s decision is just that good that I am including below a copy of the entire decision – it is a short four pages.
GlaxoSmithKline Biologicals (GSK) developed Arexvy under the FDA’s Priority Review designation. The FDA approved it for people ages 60 and older.
According to CNBC, the U.S. “suffered an unusually severe RSV season” this past winter. The New York Times reported on a “tripledemic” involving RSV, flu and COVID-19, “that swamped children’s hospitals and some I.C.U. wards.”
One U.S. county — Orange County, California — declared a local health emergency and issued a proclamation of local emergency in November 2022, citing rising RSV cases among children in the region.
GSK described results from clinical trials for Arexvy as “positive,” and the company said the U.S. launch of the vaccine is planned before the 2023-24 RSV season.
Other RSV vaccines, including one produced by Pfizer, are in the pipeline and expectations are that the FDA will approve them.
Aside from concerns over potential serious adverse events related to RSV vaccines, some experts have questioned the need for such a vaccine in the first place.
According to the journal Science, “RSV is a common respiratory infection” with symptoms “similar to a cold,” adding that “The majority of individuals recover within a few days from an uncomplicated RSV infection, although occasionally the virus can cause lower respiratory infections requiring medical attention.”
“Respiratory syncytial virus is a negligible threat to even the most frail elderly adults. The effort of widespread vaccination is simply not worth it. Even rare side effects will outweigh any theoretical benefit.”
And in a November 2022 episode of “RFK Jr. The Defender” podcast, several medical and public health experts expressed concerns about RSV vaccines.
“We have to stop these shots,” said Dr. Meryl Nass, an internist and biological warfare epidemiologist. “It’s just extraordinary that we’re still vaccinating people … we have a lot of work to do.”
Robert F. Kennedy Jr., then-chairman and chief litigation counsel for Children’s Health Defense (now chairman on leave), described RSV as “a vehicle for re-implementing the COVID-19 playbook all over the country and responding with vaccines.”
And according to the National Vaccine Information Center (NVIC), “Cost analysis data presented to the ACIP [Advisory Committee on Immunization Practices] did not show the RSV vaccines to be cost-effective at reducing the burden of costs associated with RSV illness.”
Nevertheless, more RSV vaccines are expected to receive FDA approval this year — including a Pfizer RSV vaccine for pregnant women that led to a high incidence of adverse events for both the women and their infants during clinical trials, as well as several deaths and stillbirths.
Arexvy approval ushers in new ‘highly competitive and lucrative vaccine market’
The RSV vaccine market is estimated to be worth up to $10 billion by 2030.
According to Endpoints News, the FDA’s approval of Arexvy ends “half a century of failed efforts against the elusive, shape-shifting virus” and “officially start[s] what analysts expect will be a highly competitive and lucrative new vaccine market.”
In getting Arexvy approved, “GSK beat a crowded field of competitors to cross the finish line first.”
Arexvy “showed strong efficacy in stopping lower-respiratory tract infections as well as more severe disease” and will be administered as a single dose, according to Endpoints News.
STAT reported that a “vaccine that was developed by Pfizer and aimed at the same demographic [adults 60 and over] is expected to be approved by the end of the month,” while other RSV vaccines and therapeutics, including some intended for children and pregnant women, are in the pipeline and also are close to receiving FDA approval.
The FDA’s approval of Arexvy came after an FDA advisory panel reviewed data from GSK’s and Pfizer’s clinical trials on March 1. The panel unanimously agreed that GSK’s vaccine is effective and, in a 10-2 vote, deemed it “safe,” according to The Washington Post.
The same panel also approved Pfizer’s candidate vaccine, Abrysvo, but with a 7-4 vote.
On June 21 or 22, ACIP, which advises the Centers for Disease Control and Prevention (CDC), will convene to “make recommendations on the appropriate use of the vaccine in the U.S.,” according to GSK’s announcement. The ACIP must recommend the vaccines before they are marketed.
According to STAT, there is a likelihood that ACIP may not approve Arexvy for its intended age group, stating:
“Though Arexvy’s approval is for adults 60 and older, it remains to be seen if the CDC will recommend it for that entire group.
“At an advisory committee meeting in February, members of a work group studying the adult vaccines that will soon come before ACIP indicated that at present, they don’t believe the vaccine would be cost-effective in people aged 60 to 64 and they would not recommend to the wider committee that it include people 60 to 64 in its recommendation for the use of the vaccine. (The group held the same position for the Pfizer RSV vaccine.)”
In April, the European Medicines Agency (EMA) issued its own recommendation for Arexvy, for adults 60 and over, according to the Times. However, a final EMA regulatory decision is anticipated later this year. GSK is also awaiting licensure for Arexvy in Australia, China, Japan and other countries, STAT reported.
In an earnings presentation April 26, GSK said it has “millions of doses” of Arexvy “ready to be shipped.”
“GSK’s RSV vaccine works by using a small piece of the virus: a protein that sticks out on its surface called the fusion, or F, protein, which helps the virus glom onto and infect cells in the body’s upper airways. The protein pieces in the vaccine are made in a lab, using cells specially programmed to manufacture them.”
CNN noted that the vaccine “builds on a pivotal discovery made a decade ago” by National Institutes of Health researchers, “including some of the same scientists who helped make the COVID-19 vaccines.” Specifically, the researchers figured out how to freeze the otherwise “wiggly” F protein, “in the shape it takes before it fuses onto a cell.”
STAT, quoting Phil Dormitzer, GSK senior vice president and global head of vaccines research and development, reported that although Arexvy “contains only one of the two RSV subtypes, RSV A,” studies showed that it is “virtually equally protective against both RSV A and RSV B” as the F protein on both subtypes is similar.
Dormitzer acknowledged natural immunity, telling STAT, “because older adults have all had RSV probably multiple times by the time they get [the vaccine], they’re primed against both A and B. So you’re able to get very solid boosting against both subtypes with a single adjuvanted F antigen.”
According to GSK, the Arexvy vaccine does not use mRNA technology, but “contains a recombinant subunit prefusion RSV F glycoprotein antigen (RSVPreF3) combined with GSK’s proprietary AS01E adjuvant.”
GSK, FDA claim Arexvy clinical trial data show vaccine is ‘safe and effective’ but annual shot may be needed
“The safety and effectiveness of Arexvy is based on the FDA’s analysis of data from an ongoing, randomized, placebo-controlled clinical study conducted in the U.S. and internationally in individuals 60 years of age and older.”
According to the FDA, “approximately 12,500 participants … received Arexvy and 12,500 participants … received a placebo. Among the participants who have received Arexvy and the participants who have received a placebo, the vaccine significantly reduced the risk of developing RSV-associated LRTD [lower respiratory tract disease] by 82.6% and reduced the risk of developing severe RSV-associated LRTD by 94.1%.”
LRTD was “defined as two or more symptoms including shortness of breath, wheezing, cough, increased mucus production, crackles, low oxygen saturation, or need for oxygen supplementation,” according to CNBC, while according to CNN, “People were considered to have severe disease if they needed supplemental oxygen or needed mechanical help to breathe, like a ventilator.”
According to the FDA, half of the 25,000 participants received Arexvy, while the other half received a placebo.
FDA and GSK officials provided glowing reviews of the new vaccine. Peter Marks, M.D., Ph.D., director of the FDA’s Center for Biologics Evaluation and Research, said in a statement:
“Older adults, in particular those with underlying health conditions, such as heart or lung disease or weakened immune systems, are at high risk for severe disease caused by RSV.
“Today’s approval of the first RSV vaccine is an important public health achievement to prevent a disease which can be life-threatening and reflects the FDA’s continued commitment to facilitating the development of safe and effective vaccines for use in the United States.”
Tony Wood, GSK’s chief scientific officer, described Arexvy’s approval as “a turning point in our effort to reduce the significant burden of RSV,” adding that “Our focus now is to ensure eligible older adults in the U.S. can access the vaccine as quickly as possible and to progress regulatory review in other countries.”
In turn, Dormitzer said, “There’s just the broad excitement of finally, after all these years, having good options emerging for RSV,” describing this as a “triumph of the basic science.”
While GSK is first out of the gate in the RSV vaccine race with Arexvy, Pfizer’s candidate vaccine has also completed clinical trials, which found it to be “nearly 67 percent effective in preventing R.S.V. – related illness,” according to the Times.
The FDA and GSK announcements did not mention the vaccines’ waning effectiveness. An analysis by the NVIC found that the effectiveness of the GSK vaccine peaked after two months and offered no protection after one year. This may result in recommendations for adults to receive annual doses of the vaccine.
Trial participant died from a rare inflammatory condition, others developed GBS
Despite positive comments from FDA and GSK officials, clinical trial data for Arexvy revealed instances of GBS and other rare conditions.
“The vaccine was generally well tolerated with an acceptable safety profile. The most frequently observed solicited adverse events were injection site pain, fatigue, myalgia, headache, and arthralgia. These were generally mild to moderate and transient.”
“The most commonly reported side effects by individuals who received Arexvy were injection site pain, fatigue, muscle pain, headache and joint stiffness/pain.
“Among all clinical trial participants, atrial fibrillation within 30 days of vaccination was reported in 10 participants who received Arexvy and 4 participants who received placebo.”
However, the FDA noted that in two other Arexvy studies involving approximately 2,500 participants 60 and over, “two participants developed acute disseminated encephalomyelitis (ADEM), a rare type of inflammation that affects the brain and spinal cord, seven and 22 days, respectively, after receiving Arexvy and the influenza vaccine.”
“One of the participants who developed ADEM died,” according to the FDA.
In another Arexvy study conducted by GSK, “one participant developed Guillain-Barré syndrome (a rare disorder in which the body’s immune system damages nerve cells, causing muscle weakness and sometimes paralysis) nine days after receiving Arexvy,” the FDA stated.
“A 78-year-old woman in Japan was diagnosed with Guillain-Barré syndrome nine days after receiving GSK’s vaccine … She was hospitalized for six months before being released.”
CNBC reported that GSK claimed in February “There is insufficient evidence to confirm the woman got Guillain-Barre as a result of GSK’s shot.” However, the FDA “considers the case to be related to GSK’s vaccine.”
According to the FDA’s announcement:
“The FDA is requiring the company to conduct a postmarketing study to assess the signals of serious risks for Guillain-Barré syndrome and ADEM. In addition, although not an FDA requirement, the company has committed to assess atrial fibrillation in the postmarketing study.”
According to the Times, “Once the shots become available to the public, the agency said it would require GSK to monitor the incidence of Guillain-Barré and another rare condition that was possibly related to the shot.”
The FDA similarly flagged GSK “as a potential safety issue with Pfizer’s RSV vaccine for older adults,” CNBC reported after two clinical trial participants developed GBS. According to the Post, both participants — one man and one woman — were 66 years old.
CNBC in February reported that Pfizer “will conduct a safety study to further address Guillain-Barré syndrome if the FDA approves its vaccine.”
GSK’s chief commercial officer, Luke Miels, said the vaccine would cost upwards of $120 a dose, according to the Post, which also reported that private insurers may cover “many costs” associated with the vaccine, while Medicare patients with Part D coverage “won’t pay anything out of pocket” for the vaccine.
“Shares of GSK rose nearly 2% Wednesday following the approval,” CNBC reported.
GSK is also pressing forward with “A clinical trial that aims to expand the population who may benefit from RSV vaccination into adults aged 50-59, including participants with underlying comorbidities,” according to the company’s Wednesday announcement, with results “expected in 2023.”
Is there a need for an RSV vaccine?
According to the FDA:
“RSV is a highly contagious virus that causes infections of the lungs and breathing passages in individuals of all age groups. RSV circulation is seasonal, typically starting during the fall and peaking in the winter.
“In older adults, RSV is a common cause of lower respiratory tract disease (LRTD), which affects the lungs and can cause life-threatening pneumonia and bronchiolitis (swelling of the small airway passages in the lungs).”
The FDA cited CDC figures claiming each year in the U.S., RSV leads to approximately 60,000-120,000 hospitalizations and 6,000-10,000 deaths among adults 65 years of age and older.”
STAT reported that “RSV season has been unpredictable in the wake of the COVID-19 pandemic, though some experts believe RSV activity is moving back toward the seasonality seen in the pre-COVID days,” noting that “there was little transmission in 2020, when people were wearing masks and social distancing.”
But RSV “returned abnormally early in 2021,” STAT reported, but without an explanation for why this occurred, despite widespread masking and social distancing that year, too.
In the U.S., pediatric deaths from RSV are not common but the infection is the No. 1 cause of hospitalizations for children under the age of 1, STAT reported. Globally, however, it is the second leading cause of death in children under 1, after malaria.
According to STAT, “All but the youngest of children have had RSV multiple times, but few of us would know with any certainty that this bad cold was caused by that bad virus.”
Nevertheless, Pfizer is proceeding with the development of an RSV for infants as young as 6 months — “the age group at highest risk of being hospitalized with RSV,” STAT reported, noting that the vaccine for this age group is expected to gain FDA approval later this year and will be administered to pregnant women “to generate antibodies that protect both the pregnant person and their newborn.”
Data reported by Pfizer to the CDC indicated that 14% of pregnant women who participated in Pfizer’s trial sustained an adverse event, with 4.2% sustaining a “serious” adverse event, 1.7% experiencing a “severe” adverse event and 0.5% suffering a “life-threatening” adverse event.
Similarly, the same data showed that 37.1% of infants whose mothers received the experimental Pfizer vaccine experienced adverse events within one month of birth — with 15.5% classified as “serious,” 4.5% as “severe” and 1% as “life-threatening,” while efficacy waned within months of vaccination.
According to the NVIC, “The RSV clinical trial data also included the death of one pregnant woman, 18 still births (10 in vaccinated pregnant women and 8 in unvaccinated pregnant women), and 17 infant deaths (five from the vaccinated pregnancy group and 12 in unvaccinated pregnancy group).”
In its report to the CDC, Pfizer claimed the deaths were unrelated to the vaccine.
According to the Times, “Moderna is also developing an RSV vaccine for adults 60 and over, with authorization expected in the first half of this year. The Times referenced clinical trial data released by Moderna claiming 82% efficacy, with “no safety concerns identified.”
Bavarian Nordic, known for its development of a vaccine in response to last year’s monkeypox outbreak, is also developing an RSV vaccine for adults 60 and over,” expecting to release Phase 3 clinical trial data by midyear, according to the Post and CNN.
AstraZeneca and Sanofi also are seeking FDA approval, but for nirsevimab, a monoclonal antibody treatment for RSV that would be administered to infants and toddlers up to age 2, according to the Times, which referenced clinical trial results claiming a reduction of illness of up to 75%.
According to the Post, nirsevimab “is already approved in Europe, the United Kingdom and Canada.”
However, the NVIC reported that the effectiveness of nirsevimab “is not known beyond 150 days” and it is unclear if the drug prevents ICU stays or deaths. It is being reviewed by ACIP, which according to the NVIC, is “a federal advisory committee charged with making vaccine use recommendations.”
“It is unclear why the ACIP … has chosen to go beyond its charge of making vaccine use recommendations,” NVIC states.
Safety concerns related to RSV vaccines nevertheless linger. According to CNN, an RSV vaccine developed in the 1960s for children initially delivered promising results during trials in children and animals.
However, once administered to children in the general population, “many of the children who were vaccinated required hospitalization and got more severe RSV disease than what would have normally occurred” — and two of the initial trial participants died.
Michael Nevradakis, Ph.D., based in Athens, Greece, is a senior reporter for The Defender and part of the rotation of hosts for CHD.TV’s “Good Morning CHD.”
Robert Califf, commissioner of the Food and Drug Administration (FDA) is hell bent on ridding the internet of misinformation.
In a series of public appearances, Califf has claimed that “misinformation is now our leading cause of death.”
When I asked the FDA for evidence to support his claim, the agency drew a blank, admitting that Califf’s statement “cannot be proven.”
Califf has since made attempts to tweak his public statement.
This week, CBS News reporter Alexander Tin pressed him for an explanation, to which Califf replied, “I want to modify my statement. And I’ll keep working on this, to try to get it right. I would say I actually believe it is the leading cause of premature death…”
Jessica Adams, an expert in drug regulatory affairs said, “It’s ironic. Califf is spreading misinformation about the leading cause of premature death in the US, while promoting the need to counter misinformation.”
“It’s unbelievable for him to make these assertions with no scientific backing,” she added.
Adams said it’s not the FDA’s job to police medical misinformation online.
“The FDA should be assessing drug approvals, overseeing post-marketing studies and ensuring product labels are up to date – not promoting vaccines and antivirals as if it’s the marketing arm of the drug industry,” said Adams.
The FDA sent me its website providing Califf’s reasoning for why he believes misinformation is the leading cause of premature death. It states:
“Most of the COVID-19 deaths since vaccines and antivirals became available were preventable if people had gotten updated on their vaccination status and, if high risk and infected, had they been treated with an authorized antiviral.”
“He’s failed to cite any sources to substantiate his claims and Califf keeps saying that it is just his ‘belief’…Are we supposed to just accept that?” said Adams, criticising his “obsession” over the boosters.
“It’s as if the FDA thinks that people don’t want the vaccines because they are misinformed, when it might just be that they are not persuaded by the data,” she added.
Adams also said the FDA is misinforming the public by “over-inflating” the benefit of the more recent bivalent vaccines.
“They’re now promoting the bivalent boosters which are based on much less data than the original [monovalent] vaccines and authorised on the basis of antibodies, which is not a fully validated correlate of protection,” said Adams.
This is not the first time the FDA has made misleading scientific claims to the public.
In August 2021, the FDA attempted to dissuade people from using ivermectin as an off-label, early treatment for COVID-19 by suggesting it was a livestock drug. The agency tweeted “You are not a horse. You are not a cow. Seriously, y’all. Stop it.”
But critics were quick to condemn the misinformation by pointing out that ivermectin is not only a medicine used to deworm livestock, it is also FDA-approved for parasitic treatment in humans.
Califf also spread misinformation in a Nov 2022 tweet which stated, “preliminary epidemiological findings point to the distinct possibility of the bivalent vaccines and antivirals reducing risk of long Covid.”
Vinay Prasad, Professor of Epidemiology and Biostatistics, and a practicing Haematologist Oncologist at San Francisco General Hospital wrote a scathing criticism of the tweet.
“For bivalent vaccines, he’s making things up. There are no relevant clinical data in human beings for bivalent vaccines, certainly not for the end points of long covid symptoms. Ergo that claim is 100% false; essentially a lie,” wrote Prasad.
“For antivirals, such as Paxlovid, this endpoint has not been assessed in randomized control trials. There are some poorly done observational studies that conflate ICD-10 codes with long covid symptoms and make bold, unsupported claims, but there is no robust evidence,” he added.
Traditionally, the FDA has regulated health misinformation to protect consumers from misbranded and adulterated products, but this new proposed “misinformation oversight” seems to extend to overseeing any online health-related issue.
“The FDA has always maintained that it does not want to regulate the practice of medicine, but lately it’s behaving as if it’s the Surgeon General – America’s doctor – making drug recommendations and promoting vaccines,” said Adams.
If the FDA wants to curb the spread of misinformation, it should start by looking at its own behaviour.
Despite the criticism, Califf remains defiant. Recently, he boasted to a crowd of journalists that he is “relatively impervious to critique.”
Staggering Health Consequences of Sugar on Health of Americans
By Dr. Gary Null | Global Research | February 3, 2014
In September 2013, a bombshell report from Credit Suisse’s Research Institute brought into sharp focus the staggering health consequences of sugar on the health of Americans. The group revealed that approximately “30%–40% of healthcare expenditures in the USA go to help address issues that are closely tied to the excess consumption of sugar.”[1]The figures suggest that our national addiction to sugar runs us an incredible $1 trillion in healthcare costs each year. The Credit Suisse report highlighted several health conditions including coronary heart diseases, type II diabetes and metabolic syndrome, which numerous studies have linked to excessive sugar intake.[2]
Just a year earlier in 2012, a report by Dr. Sanjay Gupta appearing on 60 Minutes featured the work of Dr. Robert Lustig, an endocrinologist from California who gained national attention after a lecture he gave titled “Sugar: The Bitter Truth” went viral in 2009. Lustig’s research has investigated the connection between sugar consumption and the poor health of the American people. He has published twelve articles in peer-reviewed journals identifying sugar as a major factor in the epidemic of degenerative disease that now afflicts our country. The data compiled by Lustig clearly show how excessive sugar consumption plays a key role in the development of many types of cancer, obesity, type II diabetes, hypertension, and heart disease. His research has led him to conclude that 75% of all diseases in America today are brought on by the American lifestyle and are entirely preventable.[3]
Until the airing of this program, no one in the “official” world acknowledged anything wrong with sugar, here is a sampling of some the latest research available to them if they chose to look… continue
This site is provided as a research and reference tool. Although we make every reasonable effort to ensure that the information and data provided at this site are useful, accurate, and current, we cannot guarantee that the information and data provided here will be error-free. By using this site, you assume all responsibility for and risk arising from your use of and reliance upon the contents of this site.
This site and the information available through it do not, and are not intended to constitute legal advice. Should you require legal advice, you should consult your own attorney.
Nothing within this site or linked to by this site constitutes investment advice or medical advice.
Materials accessible from or added to this site by third parties, such as comments posted, are strictly the responsibility of the third party who added such materials or made them accessible and we neither endorse nor undertake to control, monitor, edit or assume responsibility for any such third-party material.
The posting of stories, commentaries, reports, documents and links (embedded or otherwise) on this site does not in any way, shape or form, implied or otherwise, necessarily express or suggest endorsement or support of any of such posted material or parts therein.
The word “alleged” is deemed to occur before the word “fraud.” Since the rule of law still applies. To peasants, at least.
Fair Use
This site contains copyrighted material the use of which has not always been specifically authorized by the copyright owner. We are making such material available in our efforts to advance understanding of environmental, political, human rights, economic, democracy, scientific, and social justice issues, etc. We believe this constitutes a ‘fair use’ of any such copyrighted material as provided for in section 107 of the US Copyright Law. In accordance with Title 17 U.S.C. Section 107, the material on this site is distributed without profit to those who have expressed a prior interest in receiving the included information for research and educational purposes. For more info go to: http://www.law.cornell.edu/uscode/17/107.shtml. If you wish to use copyrighted material from this site for purposes of your own that go beyond ‘fair use’, you must obtain permission from the copyright owner.
DMCA Contact
This is information for anyone that wishes to challenge our “fair use” of copyrighted material.
If you are a legal copyright holder or a designated agent for such and you believe that content residing on or accessible through our website infringes a copyright and falls outside the boundaries of “Fair Use”, please send a notice of infringement by contacting atheonews@gmail.com.
We will respond and take necessary action immediately.
If notice is given of an alleged copyright violation we will act expeditiously to remove or disable access to the material(s) in question.
All 3rd party material posted on this website is copyright the respective owners / authors. Aletho News makes no claim of copyright on such material.