COVID SHOTS FLAGGED FOR PARALYTIC SYNDROME
The Highwire with Del Bigtree | June 2, 2022
BY WILL JONES | THE DAILY SCEPTIC | JUNE 16, 2022
Former United Nations Assistant Secretary-General Ramesh Thakur has warned in the Spectator of the coming massive expansion of the international pandemic bureaucracy and the powers of the WHO to press countries towards authoritarian public health measures. The WHO’s track record during COVID-19 hardly merits reward with further powers, he says.
Health includes mental health and wellbeing and is highly dependent on a robust economy, yet the WHO-backed package of measures to fight Covid has been damaging to health, children’s immunisation programs in developing countries, mental health, food security, economies, poverty reduction, social and educational wellbeing of peoples. Their worst effects were grievous assaults on human rights, civil liberties, individual autonomy and bodily integrity. To make it worse, in promoting these policies the WHO violated, without providing any justification beyond China’s example, (1) the guidance from its own report in October 2019 that summarised a century’s worth of worldwide experience and science; and (2) its own constitution which defines health as “a state of complete physical, mental and social well-being and not merely the absence of disease or infirmity”. The vaccine push has similarly ignored accumulating safety signals about the scale of adverse reactions, on the one hand, and rapidly dwindling efficacy after successive doses, on the other.
Euro-U.S. efforts, backed by Australia, to amend legally binding international health regulations and adopt a new pandemic convention would confer extraordinary powers on the WHO to declare public health emergencies of international/regional concern and command governments to implement their recommendations. WHO inspectors would have the right to enter countries without consent and check compliance with their directives. They would lock in the lockdowns-vaccines narrative and preempt rigorous independent retrospective reviews of their costs and efficacy. The ‘reforms’ amount to a WHO power grab at the behest of Big Pharma and Big Donors. Whether approved as two separate instruments or folded into one overarching new treaty, the changed architecture will greatly strengthen the WHO’s core capabilities on public health surveillance, monitoring, reporting, notification, verification and response. The rush to amend the existing international health regulations encountered significant pushback last month from developing countries, China and Russia but will come up again for discussion and approval shortly. The new treaty under negotiation will be presented to the World Health Assembly in 2024.
The proposed reforms to international health agreements will only make things worse, he says.
On January 24th, Director-General Tedros Adhanom Ghebreyesus said an urgent priority was to “strengthen WHO as the leading and directing authority on global health”, for: “We are one world, we have one health, we are one WHO.” On April 12th, he said the Covid crisis had “exposed serious gaps in the global health security architecture”; the new treaty would be “a generational agreement” and “a gamechanger” for global health security. If adopted, it will consolidate the gains of those who have benefitted from COVID-19, concentrating private wealth, increasing national debts and decelerating poverty reduction; expand the international health bureaucracy under the WHO; shift the centre of gravity from common endemic diseases to relatively rare pandemic outbreaks; create a self-perpetuating global biopharmaceutical complex; shift the locus of health policy authority, decision-making and resources from the state to an enlarged corps of international technocrats, creating and empowering an international analogue of the administrative state that has already thinned national democracies. It will create a perverse incentive: the rise of an international bureaucracy whose defining purpose, existence, powers and budgets will depend on outbreaks of pandemics, the more the better.
The massive propaganda campaign which led doctors to disassociate from the reality of widespread vaccine injuries is slowly weakening in impact
By Pierre Kory, MD, MPA | Medical Musings | June 13, 2022
I recently posted a deeply referenced compilation of evidence detailing the historic humanitarian catastrophe that has slowly unfolded within most advanced health economies across the world. Caused by a global mass vaccination campaign led by the Pharma masters of BMGF/WHO/CDC that illogically (but profitably) targeted a rapidly mutating coronavirus. They did it with what turned out to be the most toxic protein used therapeutically in the history of medicine. In vials mixed with lipid nano-particles, polyethylene glycol and who knows what else.
I cited studies and reports showing massive increases in cardiovascular deaths and neurologic (and other) disabilities amongst working age adults, beginning in 2021 only. A disturbing signal screaming from the original clinical trials data , VAERS data, life insurance data, disability data, reports of cardiac arrests of professional athletes, rises in ambulance calls for cardiac arrests in pre-heart attack age young people, and the massive increases in illnesses and data manipulations in Department of Defense databases.
As these events become more and more recognized by the average citizen (and occasional journalist), a new pathetic “Disinformation Campaign” was launched in response trying to blame all the young people dying as simply a need for increased awareness of the rare condition called Sudden Adult Death Syndrome (SADS), rather than examples of the legions dying from the vaccines. The fact checkers also came out in support of this narrative, branding anyone who thinks the vaccines are the cause of SADS as a conspiracy theorist. Like this self-appointed social media watchdog. Mentions of SADS are popping up from many countries… all in the last few weeks. Here, here, here, here and.. oh whatever. This article even listed a dozen such publicized deaths in the past few weeks from all over the world… but blamed them all on SADS. You get it. What is nauseating is the tone of purported good intention within these articles, informing folks that if you are related to someone young who died suddenly you should go see a cardiologist to make sure you don’t have an abnormal EKG. After it turns out normal, they will assuredly tell you to get vaccinated, an absurdity atop a mountain of absurdities caused by our bio-medical-media industrial complex over the past 2+ years.
Ugh, lets move on. In this post, I will move away from numbers and data and studies to give a more qualitative view of how the vaccines’ impacts are manifesting in the “belly of the beast,” (i.e. on the inside of a major academic medical center).
I want to first share a comment made in response to another recent post of mine, by my new partner in our COVID/Long Haul/Vax Injury specialty tele-health practice. Scott Marsland is both a COVID-expert and a Nurse Practitioner Extraordinaire (you should see the reviews he gets by his patients – they are over-the-top). Anyway, Scott wrote:
The most profound reflection of this last week came from a patient who is a physician and therapist. She was hospitalized recently for non-COVID reasons and observed: “I think many of the physicians are exhibiting dissociation. It takes an enormous amount of energy to maintain their narrative and hold off the reality hitting them in the face every day.” I thought of this reading the recent piece you referenced from The Annals of Emergency Medicine.
Wikipedia:“The major characteristic of all dissociative phenomena involves a detachment from reality, rather than a loss of reality as in psychosis. Research has suggested that dissociation is inversely related to mindfulness, which is a potential treatment.“
TY PK for this dose of mindfulness.
I thought his comment was the perfect introduction to this post, where I will share disturbing “insider info,” compiled largely from recent correspondences with a senior ICU and ER Nurse, both via email and phone. Although she is not working full-time in ICU’s or ER’s anymore, she still does shifts on occasion, particularly night shifts. Night shifts, although brutal, are WAY more fun and relaxed than day shifts. That is, most of the time, unless you get slammed due to less staff being around. Although the worst shifts of my career were night ones, thankfully they were rare.
What is great about night shifts is the camaraderie and closeness that develops among staff that choose to primarily work nights. The pool of such folks is small, and they choose night shifts for various but often similar reasons (preference, child care responsibilities, other jobs, hatred of day shifts etc). The general atmosphere is more “intimate,” as you end up having conversations, longer and deeper than you would or could in the middle of a hospital day. This is because at night there are no families around, no administrators, most patients are sleeping (sort of), no masses of swirling ancillary specialists like dietitians, physical therapists, occupational therapists, speech therapists, physician sub-specialists, transporters, social workers, food service workers, maintenance folks etc.
Anyway, this was the first email I received from her (editorial note: I wrote out or translated all her abbreviations but made no other edits to substance – I had to do it as her writing style clearly reflected someone who has been writing myriad nursing notes her whole career :).
On May 12, 2022, at 7:47 PM, L. <XXXX> wrote:
I wish I could have you as my doc. Nurse of 20 yrs + ICU – cardiac, neuroICU/ neurosurgical ICU mostly, and ED at Level 1. Vax injured from 2 Pfizer doses mandated by my major University hospital system. Clotting issues, open bleeding, spontaneous with no ability to stop, weeping down arms and legs. Severe leg clot post-surgery in March. Had to get D-Dimer ordered by force at little ED I was in, and use my own portable doppler I brought in from work, b/c they had no Ultrasound techs or equipment access – TPA (clot buster med) finally. Cervical lymph nodes enlarged since vax especially, for over 1.5 yrs. Cannot biopsy at least one as it sits on my Left carotid, now wrapped around it, . Got Covid originally while working ED in March 2020. “N antibody” still high as of Nov 2021. Hit neuro, never respiratory. Had same issues with H1N1 vaccine which was also mandated and then I got Guillain Barre Syndrome and neurological weakness – out of work 5 months. Will not get any boosters or vaccines this year, but have no exemption as all docs took to the “deer in headlight” look and said nothing. I will lose my career this winter if I refuse. Functional med/family practitioner – she has a long wait list and I have no idea how she sits with this data on vaccine injured. My VAERS report – it was deleted. Pharmacist never entered as required so I did. It has vanished. My batch numbers – significant for bad neurologic responses, clotting. I lost my Hematologist-Oncologist doctor to vaccine injury – he is out and never to practice again – in his early 40s. He was a “true believer” and in denial until it was him who was the injured patient. Our cancer hospital – know most of the case managers and many doctors since they were residents. They now have case loads in the 1000s rather than 250-400 over any given quarter. Not enough bed or infusion space for the cancer patients as outpatients. Radiation treatment backlog. All at a huge cancer hospital monstrosity itself. All kinds – brain, lymph, stomach, pancreas, blood, AND EYE CANCERS – orbital especially in younger people recently vaxxed. Microvascular ischemia on rise in vaxxed younger people. Strokes way up in no-risk, no co-morbidities, young to younger-ish. Ask me anything. I’ll tell you inside scoop from the floors and suites. This has to stop. They need to admit the fraud and crime and STOP. The liability must be lifted, mandates ended. They KNOW NOW and many KNEW THEN. Don’t know if you’ll even read this, but I follow all of you on substack and Twitter – those not banned yet! – and read ALL the data. I’ve been a lab rat myself from an issue from a car accident yrs back – I know the process. So much fraud. Keep going. Never give up. Never, never, never give up. Thank you for all you do, hope that you inspire and the confirmation of that little voice in me, that said NO way back, everything was off. I did not have an option or data then. I have data now, and it will keep coming. The option is NO.
Follow up:
Lost 4 practitioners to serious side effects of “strongly encouraged” boosters. 2 hospitalized, one in MICU. The irony is, for most staff, completely lost … All in early 30s to mid 40s. They had no need for boosters while BEING OUTSIDE ALL WEEKEND even if they truly believed in efficacy of them. All had Covid previous, N antibodies fully measurable. One female, one male, both inpatient. Female still nursing newborn.
On Fri, May 13, 2022 at 11:27 AM Pierre Kory <> wrote:
I am stunned by your email. Stunned. We know it’s bad, like real bad but this is the worst inside look I have heard yet. I am on the outside and don’t talk to most former colleagues so don’t have a feel. We should talk. Would you be interviewed on a VSRF (Kirsch’s organization) webinar? I assume not, but who knows, maybe anonymously like with altered voice and blurry screen? This needs to get out. Send me contact… and name? First name is fine… Thanks for this – Pierre
She wrote again before we talked, it was this email below that prompted me to ask her number so we could discuss in more depth:
It’s the inside folks who talk to each other, and you have to speak another language depending on who’s listening. That has been a skill set unto itself. It’s texting, the phone calls from area to area with back stories on patient issues. I was getting texts from my old stat team covering cardiac catheterization lab – the clots. The clots stunned everyone…it continues. My cardiac units – where I spent the bulk of my nursing years – lung and heart transplant included – have so many anomalies presented with patients that never existed before. Re-writing the script for each new problem never encountered. The constant codes (cardiac arrests). Can’t keep up.
Lost quite a few coworkers to either VAX injury itself – took them out of the work force, OR they resigned/accepted firing or retired once mandates were settled. It’s the phone calls I have with my cohorts in the other areas of the system. The real story is in those conversations. The doctors now admitting to injury is growing, but they can’t tell their patients why they are no longer practicing. Losing specialists is big problem not easily solved.
The signaling coming from management MD/PhD administrators has not been towards what winter will bring, but is focused on congratulating everyone on clinical excellence during the last 2 yrs. I think there is great trepidation in their approach because they see the data, they know the inside info on injury, disability/death of faculty and staff not from Covid itself, but the forced vax. We lost only a few to original Covid, with underlying co-morbidities that made outcomes a given in many cases.
I can’t come on a public show, but I can share info. My name is Linda (not her real name). In my current position, I read many charts and see in depth info – so much boosting and reboosting and not following other protocols – it’s a given now that the explosions in diagnosis of the cancers and cardiac issues especially come from these decisions. In some cases, the first thing you see on a chart is huge letters stating VAXXED alongside the pt’s diagnosis, treatments thus far, which is usually at odds with normal disease course, age and projected outcome, etc. They’re pushing the vax status, in bright letters, to the top of the list so it can be considered – not for every patient, but the “challenging cases” … That may be for research purposes.
I will explain the above – what Linda is saying is that practitioners are starting to call out the patient’s vaccination status more clearly on the first screen of the medical record in those cases where they know or suspect the vaccine is related to the patients’s new “mysterious” or “complex” problem. Let’s be clear though, the doctor’s don’t necessarily or explicitly include vaccines as a possible cause in their reasoning/impression/plan section of the patient note. But it seems the nurses and junior docs are now calling it out in some small/large way. Disassociation breaking, ever so slowly?
It makes me just stop, and by end of the week, take into account cases of say, ocular orbital cancer in 20-somethings. Have had 6 in last 2 weeks with no Family History or other indicators. Out of the blue, some with brain mets now. All vaxxed unwillingly, all had Covid and recovered fine prior to employer forced vax. The employers, the areas the patients reside in….nothing in common other than the previous. The actuaries are correct. Excess mortality, let along whatever-life-left disability. Stunning numbers.
I ended up talking to Linda.. about lots of things. She is clearly a fellow spirit, highly experienced in ICU and Emergency medicine, and she told me even more disturbing developments, like the fact that on some night shifts, nurse teams are seeing more cardiac arrests in a single shift than ever before and in unprecedented younger age patients. On some shifts, they have had so many that the “crash carts” are rolled straight from one arrest to another because Pharmacy, especially on night shifts, are not able to re-stock fast enough. This situation has happened maybe once in my whole career… when two arrests happened on the same floor or unit within a short time period.
She also told me that night nurses are more openly discussing the vaccine as the cause of what they are seeing (much more than during day shifts apparently). However, they do this largely in text, and they use “code”. Their code word for a vaccination injury or cause is “that issue,” i.e. in reference to a 22 year old who suddenly arrested on the hospital ward, “he is having that issue.” Note these are nurses.. not the docs.. but some of the docs are talking to her, like the one above who performed 6 enucleations (eyeball removals) this year already in young people (very rare to have to do this, especially in this age group). She also told me about how her interventional cardiologist nurse friends related that some patients are coming in with massive heart attacks, and during the angiogram the interventional cardiologists are seeing such extensive thrombi filling the entire artery (as documented by some embalmers), that they say “I can’t stent or remove this, this guy needs surgery, like now.”
In that conversation with Linda, I was also finally able to confirm a fraud that I had suspected was occurring within U.S hospitals regarding the accuracy (or willful inaccuracy) of the vaccination status listed in the medical record of a patient newly admitted to the hospital. It has long been my strong belief that this fraud drove the U.S data used to support some of the last remaining false narratives (i.e narratives #6 and $7 below) . Note these ever-shifting narratives were all directed at combatting vaccine hesitancy, which as some of you may know, was the primary military objective of the vaccinators.
![]()
BMGF/WHO/NIH et al. had clearly identified vaccine hesitancy as the main enemy in the battle plans they drew up and distributed after their viral pandemic simulation exercises over the past decade. In this prominent medical journal publication on addressing viral pandemics, they state “the World Health Organization has listed vaccine hesitancy among the greatest threats to global health, calling for research to identify the factors associated with this phenomenon.” Vaccine hesitancy is why the HHS gave $1 Billion to U.S media to support a relentlessly positive public relations campaign supporting the uptake of vaccines.
Now let’s get back to this fraud. First, note that during all of 2021, (well, up until late November when I was let go from my last pandemic ICU job on a completely fabricated accusation), I had only taken care of one ICU patient that was officially documented in their medical record as “fully vaccinated.” I knew that it could simply not be true that only one patient that I took care of the entire year was fully vaccinated. I knew this was false based on data from countries that more transparently (mistakenly?) reported vaccination status and hospital outcomes. In multiple reports starting in February 2021, the majority of hospitalizations and deaths (even when adjusted to rates per 100,000) had long been the vaccinated.
One of the more ridiculous attempts to cover this fraud up in the U.S was a media narrative launched in June/July of 2021, created from statements by Fauci and Wollensky, that 99% of patients in hospital and dying were the unvaccinated. They literally did this with a straight face, knowing that they were including in their numerator all the deaths that occurred prior to the start of the vaccination campaign. Yup, if you died in 2020, you were reported as dying in an unvaccinated status. Not subtle. But that was not the only lie. We must never forget the famous slip by the NY times.. when they suddenly and surprisingly called out the CDC for “withholding large amounts of COVID data” throughout the pandemic. Umm.. their actual job is to collect and disseminate data. Not subtle. Even crazier is that at the time of that narrative launch, during a lecture, a CDC slide deck mistakenly showed a slide which revealed that 26% of patients in U.S hospitals were vaccinated. But this number was falsely and fraudulently lower than the actual number. By a long shot.
Here is how I think they falsely suppressed the real rate of vaccinated patients entering U.S hospitals and dying:
In the most popular electronic medical record system in the U.S (EPIC), on the sidebar of every page in the chart are the name, demographics, room number, provider team, and COVID vaccination status of the patient. What I found weird from the outset was that, in EPIC, there were only two categories under the COVID-19 vaccine status section, “Vaccinated” or “Unknown.” There was no “Unvaccinated” status. Also realize that “Unknown” was interpreted by all providers and official data as akin to being “Unvaccinated”. Everyone I took care of in the ICU in 2021, except one, had an “Unknown” vaccination status. How could that be? How come only one ICU patient of mine in the entire year was reported as being “fully vaccinated?” Even if the vaccines worked really well (which I knew they didn’t), something was off, like really off.
There was only one hypothesis I could come up with to reconcile these observations. I suspected that during the admission process to the hospital, there must have been some sort of barrier to deeming someone “vaccinated.” I hypothesized that in order to be documented as vaccinated on admission, you had to have received the vaccine from a primary care physician’s clinic who worked for that same hospital system in a system office, and that they had already documented in the electronic medical record. If you got a vaccine from anywhere else outside that hospital system’s clinic, you were assigned an “Unknown”, i.e. “Unvaccinated” status in the electronic medical record.
And lo and behold, Linda confirmed this was the case in one major health system she worked at. What I found most striking is that she worked in two different hospital systems, in one (the smaller one) it was very easy to document a patient in the record as vaccinated. The admitting nurse could accept any documentation, from a Walgreen’s card to even a verbal report from the patient or family and they could put it in the record on admission and the patient would show up as “vaccinated” on the main screen sidebar.
In the other, larger, major (and I mean major) health system she worked in, if the patient received the vaccine from anywhere but an employed provider’s clinic within the health system (even if the patient had a vaccine card on them), she was forced to put it in an “open field” buried on page 2 of the initial nursing assessment not where nobody, and certainly no physician looked for it. All these patients were automatically documented on the main screen as “Unknown”, i.e “Unvaccinated”, even if the dates of each shot were entered into that nursing note field.
This process is what led the vast majority of U.S doctors to become convinced that the only people dying in hospitals were the unvaccinated. Which made perfect sense, I mean, the vaccinators did not want anyone to know the vaccines were not preventing hospital or death, so it would be helpful to their mission if they could make everyone think that all hospital patients were unvaccinated. This way, all the health care workers would get vaccinated out of fear of dying and would also aggressively insist that all their patients and family members get vaccinated. Which is what happened. It is also why a large percentage of the population (at least the ones I meet at lectures, conferences, and symposia) no longer want to see a “system doctor” or go to a “system hospital,” no matter how grand their brand/reputation once was. Fun fact: a long-time donor of large annual gifts to the Mayo clinic.. decided to direct their donation to the FLCCC this year because they felt the Mayo Clinic had departed from their founding principles and mission. Go FLCCC.
The system docs behaved this way because they saw with their own eyes, “the (false) reality” of what would happen if you were unvaccinated. This, combined with the medical journal propaganda publishing only favorable and selective analyses of vaccine efficacy and safety drove nearly all the nation’s doctors to go completely mad.
Their fervor to vaccinate everyone and everything, even in patients who just recovered from COVID, was something to behold. I saw overt hectoring, harassment and even rage. Twitter was one of the most terrifying places to watch doctors arrogantly propagate the need to be vaccinated.. even for folks who had (often hard-earned) natural immunity. I almost feel bad for some of those docs as history will not judge them kindly. Forgive them for they know not what they do. They were literally screaming across Social Media, Media, and Medical Journal editorials, that you will be OK if you just get vaccinated. The high profile docs were the worst, except I have little sympathy for them as some/many/most were likely complicit in the deception rather than just fooled like the rest. Folks like Eric Topol, Peter Hotez, Alastair McAlpine, Tom Friedan (who I used to deeply admire as NYC Health Department Commissioner), Eric Feigl-Ding-(bat), Jeremy Faust (probably the biggest ignoramus on Twitter, having taken an early lead in that competition since the pandemic broke in 2020), and Monica Gandhi. Leana Wen deserves particular ire as she is the most active prostitute for the Pharma-captured federal health agencies on mass media. A media darling as it were.
Then you started to see doctor walk-outs protesting the unvaccinated, increasing numbers of doctors publicly stating they would start refusing to see unvaccinated patients, heck, the Pharma controlled outlet called Medscape even got an ethicist to argue that it was OK to refuse to treat the unvaccinated. Yup. Crazy town. Clown World. One of my patients who is a hospital pharmacist even told me that at her hospital, the hospitalists were vaccinating patients admitted for COVID..as they were being discharged from the hospital. That’s right, as the patients were being discharged after having recovered from COVID, they were recommending and administering vaccines for the same illness. I even heard of one case where a team of clinicians decided to vaccinate a severely ill COVID patient in the ICU.
I also witnessed aggressive attacks in one of the nation’s largest medical-centers staff physician email forum. Doctors “screaming” that everything would be fine if everyone just got the damn vaccine. Deriding anyone bringing forth arguments about untested safety, suspicious efficacy data, and concerns about mandates violating patient autonomy and medical ethics. Anyone who brought forth “adverse data” towards the vaccines were treated with dismissal and a retaliatory posting of selectively favorable data with the imprimatur of the Pharma captured agencies and Pharma captured journals. I will never forget this time in the history of medicine. Ever.
Some other “insights” into the medical system I haver come across, from another ER nurse:
I have no research to offer but first hand experience from working as an RN
in an ER.Ringing in ears and hallucinations have followed vaccinations in 3 of my
patients. Family members at a loss. I mention the vaccine but most don’t
even hear it…The gentleman with the ringing in the ears (just had his 4th booster the day
before) I suggested he didn’t get any more boosters as ringing in the ears
is an adverse reaction to the vaccine. His wife looked at me and yelled
“his doctor told him he won’t survive the anti-virals for COViD” I was
speechless. The patient continued on and told me about his experience with
the vaccines 1st shot-he had a seizure, doctor recommended 2nd shot. After
2nd shot he was very sick, doctor recommended 3rd shot and he was
hospitalized 4th shot ringing in ears, abdominal bloating and months away
from dialysis. Wife added that she also had seizure after first vaccine and
she had that attitude that it was no big deal.I have said this before, it’s criminal what is happening. I have cried on
my way home from shifts, I tell whoever will listen. The information I have
collected over the last 7 months (time of vaccine/booster in relation to
chief complaint) is jaw dropping.I took a break from working for the summer but continue to keep in touch
with the nurses…My friend told me about an 80yr old man, 4 strokes in the last year and
they all line up with his 4 shots but the doctors response is “he’s 80,
he’s going to have strokes”Has anyone come across research in regards to GI bleeds and low hgb? I have
a lot of this patients, GI bleeds out of the blue… and they are young!I had 28yr old black obese young woman… new diagnosis of enlarged heart
and CHF. Vaccine was roughly 1 month prior to ER admit and I suggested no
more vaccines for COViD and her response was “my doctor told me this
happened because I got the vaccine and a tattoo on the same day”60ish lady…….just got over COViD (after have 3 COViD vaccines) and she told
me she was going in for second booster next week!!!!!!Kids are having random seizures and are put on anti-seizure medication for
2 years…when I ask parents what caused the seizure, the neurologist has no
idea. All these children vaccinated for COViD-100%. NO ONE CONNECTS THE
DOTS.The screenshot below is of 3 days I worked and I’m in the ER for 12 hours
and don’t see all admits. I’m also super busy so it’s hard to check status
of all admit patients… of course this is very limited information but a lot
of the patients have some issue 2-3 months post vaccine/booster.
I’m still shocked we don’t have a “vaccine team” monitoring all the
patients as they come into the ER but no one cares. Not the ER medical
director, not the doctors, not the COViD response team…..no one. Nurses see
it and they are talking but many are fearful of getting fired.Thank you for all that you are doing! Although I can’t read all the emails,
I am just happy to know that there are others out there that are in the
same boat as I am.I’m disgusted with the AMA and AAP. I don’t trust a thing they say. I don’t
trust them with my four children as they have not protected our children
over the past 2 years.Thank you!
And another:
May 26 05:28PM -0400
Katie (not her real name),
Thank you for sharing your story! This is what I live every day and I tell my husband how hard it is to see so much damage. I have had more patients diagnosed with aggressive cancers than I have seen in the last two decades.
… I’ve been so especially concerned about the clotting effects with Total joints treated with Tranexamic Acid. I’ve been keeping track of my patients (that I would consider) have had mild/moderate vax injury. i.e. – reactivation of latent viruses, (oral herpes (not just one or two lesions, but their whole mouth broke out – something that had never happened before) shingles – affecting their eyes, that took more treatment than normal) – Histoplasmosis; *blood clots/Cardiac problems – Stroke from new onset Atrial fib in a patient on blood thinners within 12 hr post injection, Atrial fibrillation in a healthy, athletic 34 yr old male, new onset hypertension without prior history; * Persistent cough, months of diarrhea, migraine, neuropathy of upper extremity to the extent she could not write/type – all extensively checked out without cause. But, all within a few days/weeks/couple months of injection. All my practitioners are still advocating the Vax!!! What do you think we should do??? I’ve got to get the guts to gently visit with our Chief of Staff. CRNA, Colorado
Last one, from a colleague:
Just had dinner with my friend, a colleague friend of his here, Dr XXX renowned YY Physician . PRO Vaccine. Was adamant all physicians should get the vaccine and should not be able to practice without it. Was a trailblazer for the vaccine here. He got boosted around Christmas time, had a stroke less than a week after, lost his eyesight in one eye, lost his practice, cannot be a doctor any longer, and said undoubtedly it was from the Pfizer vaccine and encouraged all of his doctor friends to max out their disability insurance to protect themselves. I know not surprising to you, but this guy was so pro vaccine and clearly admits his stroke and his loss of eyesight from the vaccine!!
And then there is this doozy – another nurse sent me a case history below of an elderly woman whose blood thinner was highly “supra-therapeutic” (i.e. very thin blood at risk of major bleeding), yet she had a massive stroke caused by a blood clot. This simply does not happen.
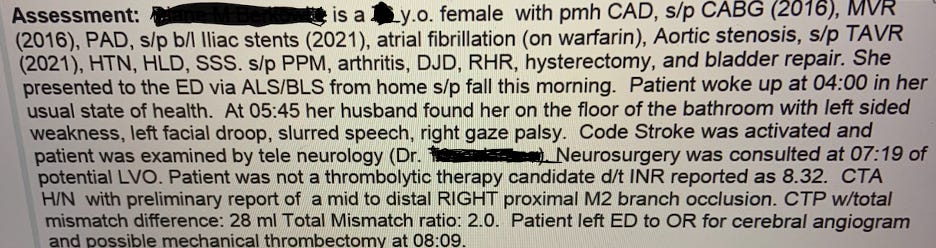
El Fin.

The Counter Signal | June 7, 2022
Speaking on behalf of the World Health Organization (WHO), International Council of Nurses CEO Howard Catton claimed that climate change is the ”grandmother of all health threats.”
“I talk to nurses around the world every week who tell me about how they see the impacts of climate change on the health of people they care for every single day in their practice,” Catton said. “There are 45 million-plus healthcare professionals who are witnesses to the health emergency that is unfolding in plain sight.”
“Their voice must be heard and acted on.”
He continues, conflating the damage caused by poor air quality and pollution — likely in places like China and India, not the developed countries of the West — with the supposed damage caused by minute rising temperatures. WHO Director-General Tedros Adhanom, of course, agrees with this radical climate change position.
“They see and work with young people struggling and old people struggling with respiratory disorders caused or exacerbated by poor air quality and pollution. People who can’t go out, who are struggling with their tasks of daily living, who are losing function, whose independence undermined,” Catton said.
“They support people who are not coping with extreme temperature changes from heat stroke and exhaustion to hypothermia. Many of these people are [the] most vulnerable, with underlying conditions, such as cardiovascular disease, which is made worse.”
According to Climate.gov, the global average temperature has risen by 1 degree Celsius over the last 40 years… This is the “extreme temperature” change that Catton speaks of, without going into the fact weather trends fluctuate and we, in the broader scheme of things, just came out of a little ice age, which probably should just be labelled a light cooling period between 1500-1850 AD (starting before the Industrial Revolution and ending as it was kicking off).
Catton continues, blaming the 1-degree Celsius change in global temperatures for natural occurrences like flooding and forest fires, which he says perpetuates the spread of disease.
For these reasons, Catton says that climate change is one of the greatest risks to global health and that health needs “to be at the centre of all our policies: energy, transport, agriculture, water, and food.”

By Paul Joseph Watson | Summit News | May 30, 2022
Billionaire Bill Gates says there’s a 50 per cent chance the next pandemic will be caused by man-made climate change or be deliberately released by a bio-terrorist.
The Microsoft founder made the comments during an interview with Spanish news outlet El Diario.
Asserting that the next major pandemic is likely to occur within 20 years, Gates said, “It could be a virus made by man, by a bioterrorist who designed it and intentionally circulated it. That is a very scary scenario because they could try to spread it in different places at once.”
“Or it could be something that makes the leap from the natural world. The human population is growing and we are invading more and more ecosystems. That is why I calculate that there is a 50% chance that we will have a pandemic of natural origin in the next 20 years, as a consequence of climate change,” he added.
The prediction that climate change will cause a virus which will then require another global vaccine rollout is somewhat convenient for Gates given that he is heavily invested in both areas.
Gates reiterated the call made in his recent book to pump billions of dollars into researching future pathogens by creating a 3,000-strong team of specialists under the control of the World Health Organization, which would require a 25% budgetary increase.
Commenting on the recent outbreak of monkeypox, Gates said “there is very little chance” it will have an impact anything like coronavirus, although he cautioned that it could mutate into something significantly nastier.
Gates infamously warned of a coming super-virus five years before the emergence of COVID-19 during a 2015 TED talk.
As we highlighted earlier this month, Gates warned that COVID was not over and that there is likely to be an “even more fatal” variant of the virus coming.
During an event at the Munich Security Conference back in February, Gates said that “sadly” Omicron is a “type of vaccine” and has “done a better job getting out to the world population than we have with vaccines” by providing natural immunity.
Meanwhile India discovers irregularities in WHO financial audit
By Shabnam Palesa Mohamed | Take Back Power | May 27, 2022
Africa Day, 25 May, has made an impact. In a rare show of African power and solidarity, several African member states objected to proposed International Health Regulations amendments, discussed at the World Health Assembly 75 this week – a move many believe might shake up the World Health Organization’s dominance.
A well placed source shared: “The resolution on IHR amendments was not passed at the WHA, as African countries were concerned that there was inadequate consultation amongst member states, and the process was being rushed. Botswana read the statement on behalf of the 47 AFRO members and I was personally present.”
According to Reuters, “if Africa continues to withhold support, it could block one of the only concrete reforms expected from the meeting, fraying hopes that members will unite on reforms to strengthen the U.N. health agency’s rules as it seeks a central role for itself in global health policy.”
The IHR seeks to define and detail WHO members’ obligations around public health emergencies and other health matters. The United States government proposed 13 controversial IHR amendments, which give the WHO DG Tedros unilateral power to declare actual or potential health emergencies and expect a response in 48 hours.
The draft proposal yet to be formally decided also aims to change article 59 of the IHR, and would accelerate the implementation of future amendments.
Bear in mind, a few countries at the WHA submitted draft resolutions to the IHR, which would need, at least according to the WHO process, four months to be considered. These countries are Australia, Bosnia and Herzegovina, Colombia, European Union and its Member States, Japan, Monaco, Republic of Korea, United Kingdom of Great Britain, Northern Ireland and the United States of America.
The African #WHA75 delegation expressed reservations about these IHR amendments, saying all reforms should be tackled together as part of a “holistic package” at a later stage.
“The African region shares the view that the process should not be fast tracked…,” Moses Keetile, deputy permanent secretary in Botswana’s health ministry, told the assembly on Tuesday on behalf of the Africa region.
“We find that they are going too quickly and these sorts of reforms can’t be rushed through,” said a concerned African delegate in Geneva. The U.S. mission in Geneva did not respond to a Reuters request for comment.
BRIMI emerges: Brazil, Russia, Iran, Malaysia and India
Brazil and Russia form part of the BRICS initiative with Brazil, Russia, India, China and South Africa. Iran and Malaysia are reported to have also expressed reservations to the proposed IHR amendments, while Russia and Brazil seem set to make big moves on international health policies, or possibly even exit the WHO. Meanwhile, India raised audit concerns on irregularities with WHO financials.
A civil society World Health Assembly monitor shared “Just for your interest, from the external audit done by India team, who yesterday during the financial comittee stated that they feel very disappointed that their audit has been ignored by WHO.”

Time line, duplication, and waste of funding resources
The IHR amendments discussions are parallel to talks on a potential new pandemic treaty (#PandemicAccord) , raising concerns over duplication and waste of funding handed to the WHO.
Given the trajectory, it appears that both the IHR amendments and the new pandemic accord, if successful, will converge on the world in 2024, unless countries decide to curtail the WHO’s power and take charge of their health.
This 2024 date was highlighted in the working group on IHR amendments: “Delegates welcomed the final report of the Working Group on strengthening WHO preparedness and response to health emergencies which, among other things, proposed a process for taking forward potential amendments to the IHR (2005). They agreed to continue the group, with a revised mandate and name (the “Working Group on IHR amendments” (WGIHR)) to work exclusively on consideration of proposed IHR amendments. Member States also requested the Director-General to convene an IHR Review Committee to make technical recommendations on the proposed amendments that may be submitted. The Working Group will propose a package of targeted amendments for consideration by the Seventy-seventh Health Assembly.”
“Several developing countries have said that the WHO has too many platforms for negotiation, and it is simply not manageable,” said Nithin Ramakrishnan, consultant for the Third World Network.
US senators start to push back on WHO overreach
According to the Daily Caller
Republican senator Ron Johnson … introduced legislation Thursday that would push back against the World Health Organization’s (WHO) overreach and ensure the Senate has power over its pandemic treaty.
The Daily Caller first obtained the legislation, titled the No WHO Pandemic Preparedness Treaty Without Senate Approval Act, which was spearheaded by Johnson and has 15 cosponsors. The bill mentions the WHO creating an intergovernmental negotiating body (INB) and, if passed, would require any agreement produced by the INB to be submitted to the Senate as a treaty in an effort to provide more transparency on the administration.
The lawmakers believe they need to start fighting to prevent the WHO from creating an INB.
“The World Health Organization, along with our federal health agencies, failed miserably in its response to COVID-19. Its failure should not be rewarded with a new international treaty that would increase its power at the expense of American sovereignty. What the WHO does need is greater accountability and transparency,” Johnson told the Daily Caller prior to officially introducing the legislation.
“This bill makes clear to the Biden administration that any new WHO pandemic agreement must be deemed a treaty and submitted to the Senate for ratification. The sovereignty of the United States is not negotiable,” Johnson continued.
Also in the US, Senator Sen. Rick Scott, R-Fla., is introducing legislation aimed at curtailing the power of the World Health Organization (WHO). This is welcome but ironic, as the amendments were proposed by the US Department of Health and Human Services. The bill, introduced Thursday, would prevent U.S. officials from being bound to orders or Republican directives given by the WHO or it’s branches. “In addition, it would require U.S. officials to oppose changes to the WHO charter until the House and the Senate agree to adopt the change in a joint resolution of Congress.”
Fact checkers spinning denial of sovereignty threat
Meanwhile, there is a clear spin attempt from establishment media against opposition to the IHR amendments and the WHO in general. A FactCheck article states “The World Health Organization can make recommendations after the declaration of a global emergency, but it has no control over any nation’s decisions. Yet conservatives in the U.S. falsely claim that amendments proposed by the Biden administration to existing global health regulations, and a new WHO pandemic treaty, will threaten U.S. sovereignty.”
It is not clear whether the writer fully understands the implications of the proposed IHR amendments, a new #PandemicAccord, sanctions for non-compliance, or the clear erosion of personal autonomy, national sovereignty, and democratic values.
The WHO and the IHR were spotlighted at the World Council for Health’s successful Better Way Conference, and a video presentation by WHO expert Dr Astrid Stuckelberger will soon be released. Dr Stuckelberger reminded the audience that the WHO is a small part of a much bigger UN/WEF machine.
Two years after the disastrous mismanagement of Coronavirus, it’s time the world thinks about and acts on a better way for health than giving power away to the WHO, which ignores its own standards on necessity, reasonableness, and proportionality.
That time is now. KeNako.
By Justin Hart | Rational Ground | May 26, 2022
Every year humans endures a “flu season” – a period denoting the high-water mark of that year’s wave of respiratory viral pathogens. Believe it or not we still have strains of the 1889 Russian flu, the 1918 Spanish flu, the 1957 Asian flu, the 1968 Hong Kong Flu, the 2009 H1N1 virus – all these various strains of nasty bugs rear their head every single year.
In late 2019, a new “novel” pathogen appeared on the scene – a bug from the “Coronavirus” family (“corona” describing the spike-like structure of the particles.) The official title was SARS-CoV-2. SARS = “severe acute respiratory syndrome”; CoV-2 = “Coronavirus 2.” This particular virus can cause a disease called COVID-19 (“Coronavirus Disease 2019”). The disease is thought to have originated in China and found significant human-to-human transmission. It is thought to be “novel” because prior infections of other pathogens do not seem to create anti-bodies to tackle this newfound disease within the human body.
Officials raised alarms about the potential mortality witnessed from COVID-19. Governments across the world scrambled to address and protect their populations from what quickly became a pandemic. Efforts ranged from stringent to downright authoritarian. Results were mixed to say the least. In early 2022, it was thought that SARS-Cov-2 and COVID-19 would join the panoply of viruses and diseases we experience during the annual ebb and flow of life.
That’s the short sterile version of what transpired.
Here’s what actually happened:
All of this was designed to latch onto a virus that many assert has unnatural origins. The ramifications of a man-made virus set loose upon the world by accident or on purpose should frighten us more than the virus itself. Someone was playing god and it appears they are just getting started.
My book, Gone Viral: How Covid Drove the World Insane comes out in September.
By Eamon McKinney | Strategic Culture Foundation | May 26, 2022
The green economy, de-industrialisation, digital health passports, Central Bank digital currencies, these are all core components of the Globalists’ plan for the Great reset. The WEF has painted a picture of their proposed future via Klaus Schwab and his acolytes. “We will have nothing, own nothing and be happy”. The main obstacle to this grand vision is that not surprisingly very few countries wish to go along with it. The Globalists know their game is coming to an end and the Great Reset is their way of ensuring that the same financial cabal that has brought the world to its current lamentable state will continue to rule over all in the next world order. The most prominent objectors to this insidious plan are of course Russia and China. Unlike their western counterparts both have strong leaders who enjoy popular support, have strong economies and are optimistic about future prospects for growth. Neither intends to sacrifice their countries so that Western elites can maintain their control over the Global economic system and impose their self-serving will on weaker nations. Which in its simplest terms is why both countries need to be destroyed, at least economically before the Great Reset can be imposed on the world. Time, however, is not on the Globalists’ side, recent events have demonstrated that they are aware of this and are accelerating their timelines.
The Great Reset and its stated objectives have been in the planning for several years, those plans however are now seriously behind schedule. The election of Trump in 2016 wasn’t supposed to happen. He was to Washington the ultimate “Black Swan” event. An outsider without the backing of a political party and with seemingly the entire mainstream media against him, his victory was considered all but impossible. Yet win he did, and it seemed he spent the entire four years of his presidency battling against the Globalist faction, both internationally and within America. Washington felt cheated, not only was Trump an “outsider” he was also a disrupter. Opinions on the divisive Trump aside, he was indisputably an “America First Nationalist”, he was anti-NATO. and a vocal anti-Globalist. There would be no Great Reset under Trump, he was an obstacle to the agenda and had to be removed. Which in 2020 in a blatantly fraudulent election he was. Should Trump run again in 2024 and all indications are that he will, he would likely win an honest election in a landslide. The return of Trump would provide another major obstacle to the Globalist agenda. Expect that all efforts will be expended to prevent another Trump presidency. With an angry populace and increased electoral scrutiny next time around, they may have to turn to other measures to foil a Trump return. Should Trump re-enter the White House in 2024, the notoriously vindictive Trump is expected to seek accountability against those who he believes robbed him of his rightful election. Nerves are frayed in Washington and they know the clock is ticking.
Trump set the agenda back four years and they are now playing against the clock to make up for lost time, all evidence suggests that they are getting increasingly desperate. The recent invitations issued to Sweden and Finland to “fast track” NATO membership is yet another provocation to Russia. Putin wants to end the Ukraine conflict on his own terms and withdraw, not get bogged down in a quagmire that would drag on for years. NATO wants exactly that. Wooing Sweden and Finland is their attempt to ensure years of conflict and tension. Putin understands this all too well. As they lurch from one bad idea to another, attention should be paid to the indecent haste in which they are moving. It appears they are making things up as they go along, all without any obvious sense of consequence.
The prospect of Trump 2.0 is not the only time sensitive issue facing the Globalists. The global economy is on the brink of implosion. Sri Lanka has recently defaulted on its international debts. This will immediately create at least a $500 billion hole in the global economy. Alarmingly, according to the World Bank more than 70 other countries are in a similarly perilous economic condition. For most their debts are un-payable, and the IMF solution of structural adjustment (austerity) privatisations, and cuts to government services, would consign these countries to generations of deprivation and social unrest. Or, they could repudiate the debt completely and abandon the Western banking model. Both China and Russia have alternatives to SWIFT and welcome countries who want to escape the neo-liberal financial plantation. Both offer investment for development, non-interference and respect for countries’ sovereignty. All things valued by every country, but unachievable under Western domination. Decisions will very soon be made by countries throughout the Global south about who they want to align their futures with.
A new proposal being put before the UN on May 22nd essentially requires all nations to surrender their sovereignty to the WHO in the event of another pandemic. That they would even think that post-Covid the WHO enjoys that level of confidence, is delusional. This transparent power grab is easily recognised for what it is, in the unlikely event that it gains enough traction, expect another pandemic to follow shortly after. The cabal still has the tools to cajole, bribe and threaten countries to submit, and doubtless it will try, but outside of the captured western countries, such a desperate move will garner scant support. Covid failed to usher in the Great Reset but it unleashed a wave of destruction on the global economy that may take generations to repair. Many questions on the criminal mismanagement of Covid remain unanswered. There are few nations that don’t harbour deep resentment towards the notoriously corrupt and inept WHO and its genocidal Sugar Daddy Bill Gates. The sheer audacity of the proposal stinks of desperation. The upcoming vote is likely to give the Globalists another stark reminder of its waning power and influence.
A Great Reset will happen, just not the one intended by the Globalists. They may have to settle for the Great Decoupling instead. As Western influence continues to diminish at a rapid pace the trend of countries flocking to the China/Russia orbit is bound to increase. The NWO that they have been lusting after for generations is likely to be restricted to Western Europe and North America, or about 15% of the World’s population. The effects of the disastrous Ukraine provocation and the failed sanctions will soon become undeniable. Food and energy shortages together with uncontrollable inflation, will make even this smaller NWO harder to control. The Emperor has no clothes, as all can now see, their game is old, tired and predictable, and they have no new ideas. The Globalists may not have to worry about a Trump return in 2024. It is highly likely that the clock will have run out on them by then. It could happen any day.
Press TV – May 25, 2022
A senior Iranian health ministry official says the country has publicly declared its opposition to a US-led proposal to reform the International Health Regulations (IHR).
Mohammad Hassan Niknam, a special aide to the Iranian health minister, said on Wednesday that an Iranian delegation attending the World Health Organization’s annual assembly in Geneva had rejected a proposal put forward by the United States and other countries to speed up the implementation for future IHR reforms from 24 to 12 months.
“The Islamic Republic of Iran officially distanced itself from accepting any commitment on this proposal during the assembly,” said Niknam.
Media reports on Tuesday suggested Iran and Malaysia had expressed reservations about the IHR reforms while a delegate representing African countries had entirely rejected the move.
Niknam said, however, that Iran has publicly announced that it is opposed to fast tracking future IHR reforms.
He said Iranian health minister Bahram Einollahi had declared the opposition during his speech to the WHO assembly while delegates representing the country in committee discussions had also opposed the move.
The Iranian health system has suffered from the impacts of American sanctions on the country during the spread of the coroanvirus pandemic.
Iran was forced to rely on home-grown capacities to tackle one of the largest outbreaks of the disease in the Middle East as the sanctions hampered its access to foreign supplies of vaccines, medicines and medical equipment.
US officials have repeatedly claimed that Iran’s humanitarian needs have been exempt from the sanctions. That comes as foreign suppliers and banks have refused to process Iranian requests for medical supplies under pressure from Washington.
By Dr Deborah Ancell | TCW Defending Freedom | May 25, 2022
Dear Prime Minister,
It’s the Davos World Economic Forum (WEF) season and conspiracies about World Government abound. I have a new one for you.
You might recall my letter concerning the opaqueness of the first international tax, the United Nations Carbon Offsetting Reduction Scheme for International Aviation (CORSIA)
CORSIA offsets aircraft carbon dioxide emissions and it’s hidden in the environmental provisions of the UN’s International Civil Aviation Organisation. CORSIA empowered the UN to raise taxes – something which appears to have escaped notice in signatory sovereign nations.
My concerns were that firstly, CO2 is not a pollutant and secondly, CORSIA is a Trojan horse for similar UN taxes on other industries such as shipping and information technology.
Taxation is the tool of national governments. When nations surrender tax powers to an international body, they undermine their sovereignty. CORSIA enables independent, non-political, commercial funding of UN development projects in developing nations and reduces their reliance on UN member-government funding.
CORSIA also provides developing world reparations, since it offsets (unevidenced) claims that underdevelopment results from historical emissions incurred during developed world industrialisation. As the first international tax, it’s an example of UN overreach which undermines national sovereignty.
Now another UN arm – the World Health Organisation – might also be attempting overreach. WHO is proposing a new ‘pandemic treaty’ to encourage more information-sharing in the event of another global health crisis.
The treaty would apparently give WHO ‘unprecedented, undemocratic jurisdiction over its 194 member nations, including the UK’. There would be almost unlimited authority to ‘order mandatory vaccines, digital health IDs, lockdowns, isolation, testing regimes, no-jab-no-job rules, or anything else it decided as policy, irrespective of dissenting voices’.
The treaty will not be voted on until the World Health Assembly in 2023. If the UK agreed to this, health sovereignty could also be undermined.
Combine these two sovereignty concessions and you have the beginnings of an independently-funded and legislating World Government. This prospect was promoted by now-deceased luminaries as diverse as discredited socialist millionaire Maurice Strong and capitalist banker David Rockefeller.
Strong, a promoter of CO2 as a cause of environmental harm, profoundly believed that the UN had the potential to be the World Government. Any such World Government would undermine democracies.
Similarly, Rockefeller founded and led the Trilateral Commission with its aim of a ‘New World Order’ to control population and resources. He is reported as stating that ‘the supranational sovereignty of an intellectual elite and world bankers is surely preferable to the national auto-determination (democracy) practised in past centuries.’ Scary!
Conspiracy theorists believe that today’s WEF, with its agenda to counter natural and anthropogenic climate change and its call for a Great (economic) Reset has a similar, shadowy agenda to these precursor pursuits.
As conspiracy theories go, this one is far-fetched – but can you assure me I’m wrong? Do you think that World Government is on the agenda at Davos today?
Yours sincerely,
Deborah Ancell

or go to
Aletho News Archives – Video-Images

By Irfan Chowdhury | Palestine Chronicle | July 18, 2020
… Israel has been carrying out the longest-running military occupation in modern history and the longest-running siege in modern history. These two facts alone render Israel unique in terms of the scope of its brutality and criminality.
There are other respects in which Israel stands out from other countries in its use of terror and violence; for example, it is one of the most aggressive countries in the world, having waged wars of aggression against Lebanon in 1978, 1982, 1993, 1996 and 2006, and against Gaza in 2004, 2006, 2008/9, 2012 and 2014, killing huge numbers of civilians in the process (all while issuing threats and carrying out various covert attacks against Iran, which are all in violation of the UN Charter). … continue
| Richard Ong on Israeli forces arrest writer a… | |
| Bill Francis on How reporting facts can now la… | |
| Gemma on Israel’s diamond industr… | |
| Bill Francis on Victoria Moves to Force Online… | |
| papasha408 on The Empire of Lies: How the BB… | |
| loongtip on US Weighs Port Restrictions on… | |
| Bill Francis on Chris Minns Defends NSW “Hate… | |
| Sheree Sheree on I was canceled by three newspa… | |
| Richard Ong on Czech–Slovak alignment signals… | |
| John Edward Kendrick on Colonel Jacques Baud & Nat… | |
| eddieb on Villains of Judea: Ronald Laud… | |
| rezjiekc on Substack Imposes Digital ID Ch… |
