The WHO’s Proposed Amendments Will Increase Man-Made Pandemics
By Meryl Nass | Brownstone Institute | August 17, 2023
This report is designed to help readers think about some big topics: how to really prevent pandemics and biological warfare, how to assess proposals by the WHO and its members for preventing and responding to pandemics, and whether we can rely on our health officials to navigate these areas in ways that make sense and will help their populations. We start with a history of biological arms control and rapidly move to the COVID pandemic, eventually arriving at plans to protect the future.
Weapons of Mass Destruction: Chem/Bio
Traditionally, the Weapons of Mass Destruction (WMD) have been labelled Chemical, Biological, Radiologic, and Nuclear (CBRN).
The people of the world don’t want them used on us—for they are cheap ways to kill and maim large numbers of people quickly. And so international treaties were created to try to prevent their development (only in the later treaties) and use (in all the biological arms control treaties). First was the Geneva Protocol of 1925, following the use of poison gases and limited biological weapons in World War I, banning the use of biological and chemical weapons in war. The US and many nations signed it, but it took 50 years for the US to ratify it, and during those 50 years the US asserted it was not bound by the treaty.
The US used both biological and chemical weapons during those 50 years. The US almost certainly used biological weapons in the Korean War (see this, this, this and this) and perhaps used both in Vietnam, which experienced an odd outbreak of plague during the war. The use of napalm, white phosphorus, agent orange (with its dioxin excipient causing massive numbers of birth defects and other tragedies) and probably other chemical weapons like BZ (a hallucinogen/incapacitant) led to much pushback, especially since we had signed the Geneva Protocol and we were supposed to be a civilized nation.
In 1968 and 1969, two important books were published that had a great influence on the American psyche regarding our massive stockpiling and use of these agents. The first book, written by a young Seymour Hersh about the US chemical and biological warfare program, was titled Chemical and Biological Warfare; America’s Hidden Arsenal. In 1969 Congressman Richard D. McCarthy, a former newspaperman from Buffalo, NY wrote the book The Ultimate Folly: War by Pestilence, Asphyxiation and Defoliation about the US production and use of chemical and biological weapons. Prof. Matthew Meselson’s review of the book noted,
Our operation, “Flying Ranch Hand,” has sprayed anti-plant chemicals over an area almost the size of the state of Massachusetts, over 10 per cent of its cropland. “Ranch Hand” no longer has much to do with the official justification of preventing ambush. Rather, it has become a kind of environmental warfare, devastating vast tracts of forest in order to facilitate our aerial reconnaissance. Our use of “super tear gas” (it is also a powerful lung irritant) has escalated from the originally announced purpose of saving lives in “riot control-like situations” to the full-scale combat use of gas artillery shells, gas rockets and gas bombs to enhance the killing power of conventional high explosive and flame weapons. Fourteen million pounds have been used thus far, enough to cover all of Vietnam with a field effective concentration. Many nations, including some of our own allies have expressed the opinion that this kind of gas warfare violates the Geneva Protocol, a view shared by McCarthy.
A Biological Weapons Convention
Amid great pushback over US conduct in Vietnam, and seeking to burnish his presidency, President Nixon announced to the world in November 1969 that the US was going to end its biowarfare program (but not the chemical program). Following pointed reminders that Nixon had not eschewed the use of toxins, in February 1970 Nixon announced we would also get rid of our toxin weapons, which included snake, snail, frog, fish, bacterial, and fungal toxins that could be used for assassinations and other purposes.
It has been claimed that these declarations resulted from careful calculations that the US was far ahead technically of most other nations in its chemical and nuclear weapons. But biological weapons were considered the “poor man’s atomic bomb” and required much less sophistication to produce. Therefore, the US was not far ahead in the biological weapons arena. By banning this class of weapon, the US would gain strategically.
Nixon told the world that the US would initiate an international treaty to prevent the use of these weapons ever again. And we did so: the 1972 Convention on the Prohibition of the Development, Production and Stockpiling of Bacteriological (Biological) and Toxin Weapons and on their Destruction, or Biological Weapons Convention (BWC) for short, which entered into force in 1975.
But in 1973 genetic engineering (recombinant DNA) was discovered by Americans Herbert Boyer and Stanley Cohen, which changed the biological warfare calculus. Now the US had regained a technological advantage for this type of endeavor.
The Biological Weapons Convention established conferences to be held every 5 years to strengthen the treaty. The expectation was that these would add a method to call for ‘challenge inspections’ to prevent nations from cheating and would add sanctions (punishments) if nations failed to comply with the treaty. However, since 1991 the US has consistently blocked the addition of protocols that would have an impact on cheating. By now, everyone accepts that cheating occurs and is likely widespread.
A leak in an anthrax production facility in Sverdlovsk, USSR in 1979 caused the deaths of about 60 people. While the USSR tried a sloppy cover-up, blaming contaminated black market meat, this was a clear BWC violation to all those knowledgeable about anthrax.
US experiments with anthrax production during the Clinton administration, detailed by Judith Miller et al. in the 2001 book Germs, were also thought by experts to have transgressed the BWC.
It has taken over 40 years, but in 2022 all declared stocks of chemical weapons had been destroyed by the USA, by Russia, and the other 193 member nation signatories. The chemical weapons convention does include provisions for surprise inspections and sanctions.
Pandemics and Biological Warfare Receive Funding from Same Stream
It is now 2023, and during the 48 years the Biological Weapons Convention has been in force the wall it was supposed to build against the development, production, and use of biological weapons has been steadily eroded. Meanwhile, especially since the 2001 anthrax letters, nations (with the US at the forefront) have been building up their “biodefense” and “pandemic preparedness” capacities.
Under the guise of preparing their defenses against biowarfare and pandemics, nations have conducted “dual-use” (both offensive and defensive) research and development, which has led to the creation of more deadly and more transmissible microorganisms. And employing new verbiage to shield this effort from scrutiny, biological warfare research was renamed as “gain-of-function” research.
Gain-of-function is a euphemism for biological warfare research aka germ warfare research. It is so risky that funding it was banned by the US government (but only for SARS coronaviruses and avian flu viruses) in 2014 after a public outcry from hundreds of scientists. Then in 2017 Drs. Tony Fauci and Francis Collins lifted the moratorium, with no real safeguards in place. Fauci and Collins even had the temerity to publish their opinion that the risk from this gain-of-function research was ‘worth it.’
What does gain-of-function actually mean? It means that scientists are able to use a variety of techniques to turn ordinary or pathogenic viruses and bacteria into biological weapons. The research is justified by the claim that scientists can get out ahead of nature and predict what might be a future pandemic threat, or what another nation might use as a bioweapon. The functions gained by the viruses or other microorganisms to turn them into biological warfare agents consist of two categories: enhanced transmission or enhanced pathogenicity (illness severity).
1) improved transmissibility may result from:
a) needing fewer viral or bacterial copies to cause infection,
b) causing the generation of higher viral or bacterial titers,
c) a new mode of spread, such as adding airborne transmission to a virus that previously only spread through bodily fluids,
d) expanded range of susceptible organs (aka tissue tropism); for example, not only respiratory secretions but also urine or stool might transmit the virus, which was found in SARS-CoV-2,
e) expanded host range; for example, instead of infecting bats, the virus is passaged through humanized mice and thus acclimated to the human ACE-2 receptor, which was found in SARS-CoV-2,
f) improved cellular entry; for example, by adding a furin cleavage site, which was found in SARS-CoV-2,
2) increased pathogenicity, so instead of causing a milder illness, the pathogen would be made to cause severe illness or death, using various methods. SARS-CoV-2 had unusual homologies (identical short segments) to human tissues and the HIV virus, which may have caused or contributed to the late autoimmune stage of illness, impaired immune response and ‘long COVID.’
Funding for (Natural) Pandemics, Including Yearly Influenza, was Lumped Together with Biological Defense Funding
Perhaps the comingling of funding was designed to make it harder for Congress and the public to understand what was being funded, and how much taxpayer funding was going to gain-of-function work, which might lead them to question why it was being done at all, given its prohibition in the Biological Weapons Convention, and additional questions about its value. Former CDC Director Robert Redfield, a physician and virologist, told Congress in March of 2023 that gain-of-function research had not resulted in a single beneficial drug, vaccine, or therapeutic to his knowledge.
Nonprofits and universities like EcoHealth Alliance and its affiliated University of California, Davis veterinary school were used as intermediaries to obscure the fact that US taxpayers were supporting scientists in dozens of foreign countries, including China, for research that included gain-of-function work on coronaviruses.
Perhaps to keep the lucrative funding going, fears about pandemics have been deliberately amplified over the past several decades. The federal government has been spending huge sums on pandemic preparedness over the past 20 years, routing it through many federal and state agencies. President Biden’s proposed 2024 budget requested “$20 billion in mandatory funding across DHHS for pandemic preparedness” while the DHS, DOD, and the State Department have additional budgets for pandemic preparedness for both domestic and international spending.
Although the 20th century experienced only 3 significant pandemics (the Spanish flu of 1918-19 and 2 influenza pandemics in 1957 and 1968) the mass media have presented us with almost non-stop pandemics during the 21st century: SARS-1 (2002-3), avian flu (2004-on), swine flu (2009-10), Ebola (2014, 2018-19), Zika (2016), COVID (2020-2023), and monkeypox (2022-23). And we are incessantly told that more are coming, and that they are likely to be worse.
We have been assaulted with warnings and threats for over 2 decades to induce a deep fear of infectious diseases. It seems to have worked.
The genomes of both SARS-CoV-2 and the 2022 monkeypox (MPOX) virus lead to suspicion that both were bioengineered pathogens originating in laboratories. The group of virologists assembled by Drs. Fauci and Farrar identified 6 unusual (probably lab-derived) parts of the SARS-CoV-2 genome as early as February 1, 2020 and more have been suggested subsequently.
I do not know if these viruses leaked accidentally or were deliberately released, but I am leaning toward the conclusion that both were deliberately released, based on the locations where they first appeared, the well-orchestrated but faked videos rolled out by the mass media for COVID, and the illogical and harmful official responses to each. In neither case was the public given accurate information about the infections’ severity or treatments, and the responses by Western governments never made scientific sense. Why wouldn’t you treat cases early, the way doctors treat everything else? It seemed that our governments were trading on the fact that few people knew enough about viruses and therapeutics to make independent assessments about the information they were being fed.
Yet by August 2021, there was no corresponding course correction. Instead, the federal government doubled down, imposing vaccine mandates on 100 million Americans in September 2021 in spite of ‘the science.’ There has been no accurate statement yet from any federal agency about the lack of utility of masking for an airborne virus (which is probably why the US government and WHO delayed acknowledging airborne spread by COVID for 18 months), the lack of efficacy of social distancing for an airborne virus, and the risks and poor efficacy of 2 dangerous oral drugs (paxlovid and molnupiravir) purchased by the US government for COVID treatment, even without a doctor’s prescription.
Never have any federal agencies acknowledged the truth about the COVID vaccines’ safety and efficacy. Instead, the CDC turns definitional and statistical cartwheels so it can continue to claim they are “safe and effective.” Even worse, with all that we know, a third generation COVID vaccine is to be rolled out for this fall and the FDA has announced that yearly boosters are planned.
All this goes on, even a year after we learned (with continuing corroborations) that children and working age adults are dying at rates 25 percent or more above the expected averages, and the vascular side effects of vaccination are the only reasonable explanation.
Maiming with Myocarditis
Both of the two US monkeypox/smallpox vaccines (Jynneos and ACAM2000) are known to cause myocarditis, as do all 3 COVID vaccines currently available in the US: the Pfizer and Moderna COVID-19 mRNA vaccines and the Novavax vaccine. The Novavax vaccine was first associated with myocarditis during its clinical trial, but this was downplayed and it was authorized and rolled out anyway, intended for those who refused the mRNA vaccines due to the use of fetal tissue in their manufacture.
Here is what the FDA’s reviewers wrote about the cardiac side effects noted in the Jynneos clinical trials:
Up to 18.4% of subjects in 2 studies developed post-vaccination elevation of troponin [a cardiac muscle enzyme signifying cardiac damage]. However, all of these troponin elevations were asymptomatic and without a clinically associated event or other sign of myopericarditis. p. 198
The applicant has committed to conduct an observational, post-marketing study as part of their routine PVP. The sponsor will collect data on cardiac events that occur and are assessed as a routine part of medical care. p. 200
In other words, while the only way to cause an elevated troponin level is to break down cardiac muscle cells, the FDA did not require a specific study to evaluate the extent of cardiac damage that might be caused by Jynneos when it issued its 2019 license. How frequently does myocarditis occur after these vaccines? If you use elevated cardiac enzymes as your marker, ACAM2000 caused this in one in thirty people receiving it for the first time. If you use other measures like abnormal cardiac MRI or echo, according to the CDC it occurs in one in 175 vaccinees. I have not seen a study with rates of myocarditis for Jynneos, but there was an unspecified elevation of cardiac enzymes in 10 percent and 18 percent of Jynneos recipients in two unpublished prelicensure studies available on the FDA website. My guess for the mRNA COVID vaccines is that they cause myocarditis in this general range, the vast majority of which remain undiagnosed and probably asymptomatic.
Why would our governments push 5 separate vaccines all known to cause myocarditis on young males who have been at extremely low risk from COVID, and who simply get a few pimples for 1-4 weeks from monkeypox unless they are immunocompromised? It’s an important question. It does not make medical sense. Especially when the vaccine probably does not work—Jynneos didn’t prevent infection in the monkeys in whom it was tested nor did it do well in people. And the CDC has failed to publish its trial of Jynneos vaccine in the ~1,600 Congolese healthcare workers on whom the CDC tested it for efficacy and safety in 2017. The CDC made the mistake of announcing the trial, and posting it to clinicaltrials.gov as required, but has not informed its advisory committee that reviewed the vaccine, nor the public, of the trial’s results.
There can be no question about it: our health agencies are guilty of malfeasance, misrepresentation, and deliberate infliction of harm on their own populations. The health agencies first incited terror with apocalyptic predictions, then demanded patients be medically neglected, and finally enforced vaccinations and treatments that were tantamount to malpractice.
COVID Vaccines: The Chicken or the Egg?
The health authorities could have just been ignorant — that could possibly explain the first few months of the COVID vaccines’ rollout. But once they figured out, and even announced in August 2021 that the vaccines did not prevent catching COVID or transmitting it, why did our health authorities still push COVID vaccines on low-risk populations who were clearly at greater risk from a vaccine side effect than from COVID? Particularly as time went on and newer variants were less and less virulent?
Once you acknowledge these basic facts, you realize that maybe the vaccines were not made for the pandemic, and instead the pandemic was made to roll out the vaccines. While we cannot be certain, we should at least be suspicious. And the fact that the US contracted for 10 doses per person (review purchases here, here, here, here and here) and so did the European Union (here and here) and Canada should make us even more suspicious – there is no justification for agreeing to purchase so many doses for vaccines at a time when the vaccines’ ability to prevent infection and transmission was questionable, and its safety suspect or worrying.
Why would governments want ten doses per person? Three maybe. But ten? Even if yearly boosters were expected, there was no reason to sign contracts for enough vaccine for the next nine years for a rapidly mutating virus. Australia bought 8 doses per person. By December 20, 2020 New Zealand had secured triple the vaccines it needed, and offered to share some with nearby nations. No one has come forward to explain the reason for these excessive purchases.
Furthermore, you don’t need a vaccine passport (aka digital ID, aka a phone app that in Europe included a mechanism for an electronic payments system) unless you are giving out regular boosters. Were the vaccines conceived of as the means for putting our vaccinations, health records, official documents–and most importantly, shifting our financial transactions online, all managed on a phone app? This would be an attack on privacy as well as the enabling step to a social credit system in the West. Interestingly, vaccine passports were already being planned for the European Union by 2018.
A Pandemic Treaty and Amendments: Brought to You by the Same People who Mismanaged the Past 3 Years, to Save us from Themselves?
The same US and other governments and the WHO that imposed draconian measures on citizens to force us to be vaccinated and take dangerous, expensive, experimental drugs, withheld effective treatments, and refused to tell us that most people who required ICU care for COVID were vitamin D-deficient and that taking vitamin D would lessen COVID’s severity–decided in 2021 we suddenly needed an international pandemic treaty. Why? To prevent and ameliorate future pandemics or biological warfare events… so we would not suffer again as we did with the COVID pandemic, they insisted. The WHO would manage it.
To paraphrase Ronald Reagan, the words, “I’m from the WHO, and I’m here to help” should be the most terrifying words in the English language after the COVID fiasco.
What the WHO and our governments conveniently failed to mention is that we suffered so badly because of their medical mismanagement and our governments’ merciless economic shutdowns and mismanagement. According to the World Bank, an additional 70 million people were forced into extreme poverty in 2020 alone. This was due to policies issued by our nations’ rulers, their elite advisers and the World Health Organization, which came out with guidance to shut down economic activity that most nations adopted without question. The WHO is acutely aware of the consequences of economic lockdowns, having published the following:
Malnutrition persisted in all its forms, with children paying a high price: in 2020, over 149 million under-fives are estimated to have been stunted, or too short for their age; more than 45 million – wasted, or too thin for their height…
Starvation may have killed more people than COVID, and they were disproportionately the youngest, rather than the oldest. Yet the WHO prattles on about equity, diversity, and solidarity—having itself caused the worst food crisis in our lifetime, which was not due to nature but was man-made.
How can anyone take seriously claims by the same officials who mishandled COVID that they want to spare us from another medical and economic disaster–by using the same strategies they applied to COVID, after they masterminded the last disaster? And the fact that no governments or health officials have admitted their errors should convince us never to let them manage anything ever again. Why would we let them draw up an international treaty and new amendments to the existing International Health Regulations (IHR) that will bind our governments to obey the WHO’s dictates forever?
Those dictates, by the way, include vaccine development at breakneck speed, the power to enforce which drugs we will be directed to use, and which drugs will be prohibited, and the requirement to monitor media for “misinformation” and impose censorship so that only the WHO’s public health narrative will be conveyed to the public.
The WHO’s Pandemic Treaty Draft Requires the Sharing of Potential Pandemic Pathogens. This is a Euphemism for Bioweapons Proliferation.
Obviously, the best way to spare us from another pandemic is to immediately stop funding gain-of-function (GOF) research and get rid of all existing GOF organisms. Let all nations build huge bonfires and burn up their evil creations at the same time, while allowing other nations to inspect their biological facilities and records.
But the WHO in its June 2023 Bureau Text of the Draft Pandemic Treaty has a plan that is the exact opposite of this. In the WHO’s draft treaty, which most nations’ rulers appear to have bought into, all governments will share all viruses and bacteria they come up with that are determined to have “pandemic potential” — share them with the WHO and other governments, putting their genomic sequences online. No, I am not making this up. (See screenshots from the draft treaty below.) Then the WHO and all the Fauci’s of the world would gain access to all the newly identified dangerous viruses. Would hackers also gain access to the sequences? This pandemic plan should make you feel anything but secure.
Fauci, Tedros, and their ilk at the WHO, and those managing biodefense and biomedical research for nation states are on one side, the side that gains access to ever more potential biological weapons, and the rest of us are on the other, at their mercy.
This poorly conceptualized plan used to be called proliferation of weapons of mass destruction—and it is almost certainly illegal. (For example, see Security Council resolution 1540 adopted in 2004.) But this is the plan of the WHO and of many of our leaders. Governments will all share the weapons.
The Genomic Sequencing Conundrum
And governments are to commit to building biolabs that must include genomic sequencing. No explanation has been forthcoming about why each nation needs to install its own genome sequencing laboratories. Of course, they would sequence the many viruses that will be detected as a result of the pathogen surveillance activities nations must perform, according to the WHO treaty draft. But the same techniques can be used to sequence human genomes. The fact that the EU, UK, and US are currently engaged in projects to sequence about 2 million of their citizens’ genomes provides a hint they may want to collect additional genomes of Africans, Asians, and others.
This might fly as simply sharing state-of-the-art science with our less-developed neighbors. But it is curious that there is so much emphasis on genomics, compared to an absence of discussion about developing repurposed drugs for pandemics in the draft treaty or IHR amendments.
But we can’t forget that virtually all developed nations, in lockstep, restricted the use of safe generic hydroxychloroquine, ivermectin, and related drugs during the pandemic. In retrospect, the only logical explanation for this unprecedented action was to preserve the market for expensive patentable drugs and vaccines, and possibly to prolong the pandemic.
Genomes offer great potential profits, as well as providing the substrate for transhumanist experiments that could include designer babies.
The latest version (aka the WHO Bureau draft) of the pandemic treaty can be accessed here. I provide screenshots to illustrate additional points.
Draft pages 10 and 11:




The WHO Treaty Draft Incentivizes Gain-of-Function Research
What else is in the Treaty? Gain-of-Function research (designed to make microorganisms more transmissible or more pathogenic) is explicitly incentivized by the treaty. The treaty demands that administrative hurdles to such research must be minimized, while unintended consequences (aka pandemics) should be prevented. But of course, when you perform this type of research, leaks and losses of agents can’t always be prevented. The joint CDC-USDA Federal Select Agent Program (FSAP) which keeps track of research on potential pandemic pathogens collects reports of about 200 accidents or escapes yearly from labs situated in the US. The FSAP annual report for 2021 notes:
“In 2021, FSAP received 8 reports of losses, 177 reports of releases, and no reports of thefts.”
Research on deadly pathogens cannot be performed without risks both to the researchers and the outside world.
Draft page 14:

Vaccines Will be Rolled Out Speedily Under Abbreviated Future Testing Protocols
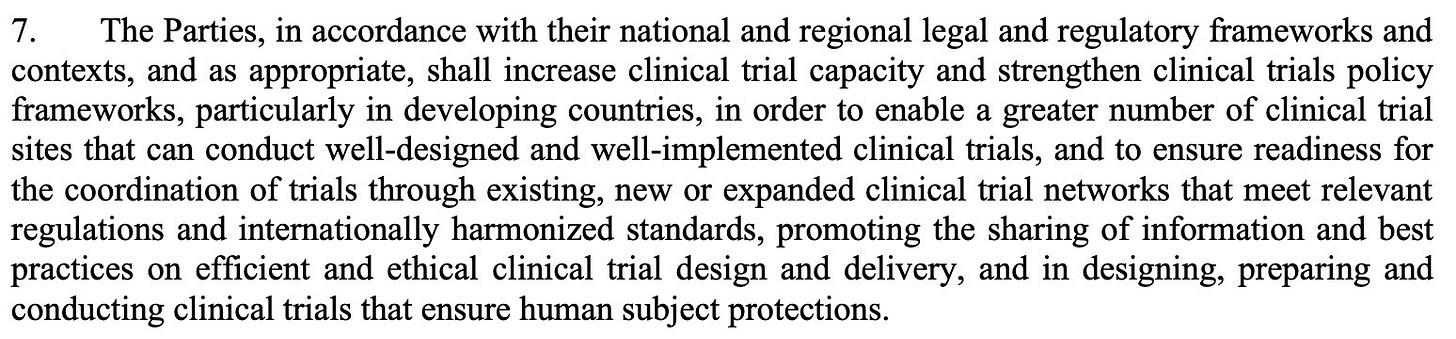
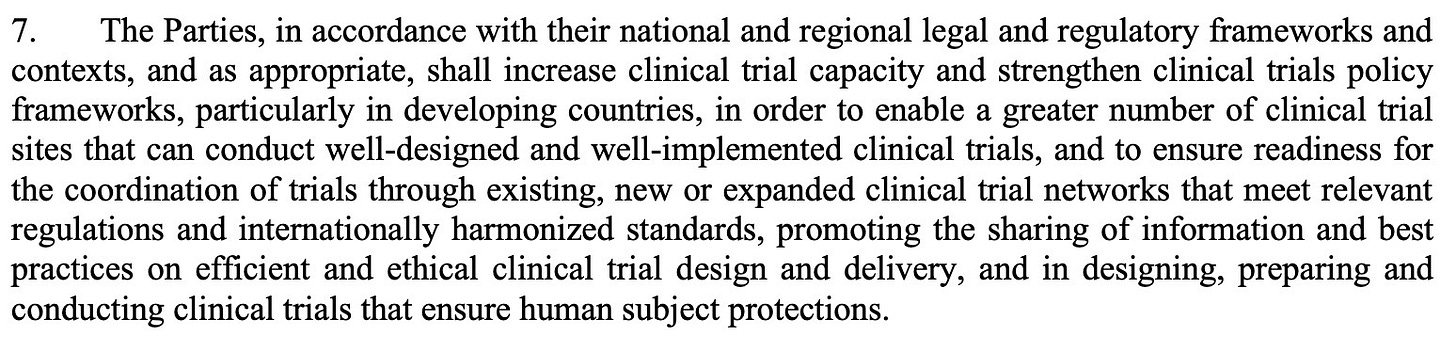
Vaccines normally take 10-15 years to be developed. In case you thought the COVID vaccines took too long to be rolled out (326 days from availability of the viral sequence to authorization of the first US COVID vaccine) the WHO treaty draft has plans to shorten testing. There will be new clinical trial platforms. Nations must increase clinical trial capacity. (Might that mean mandating people to be human subjects in out-of-the-way places like Africa, for example?) And there will be new “mechanisms to facilitate the rapid interpretation of data from clinical trials” as well as “strategies for managing liability risks.”
Draft page 14:
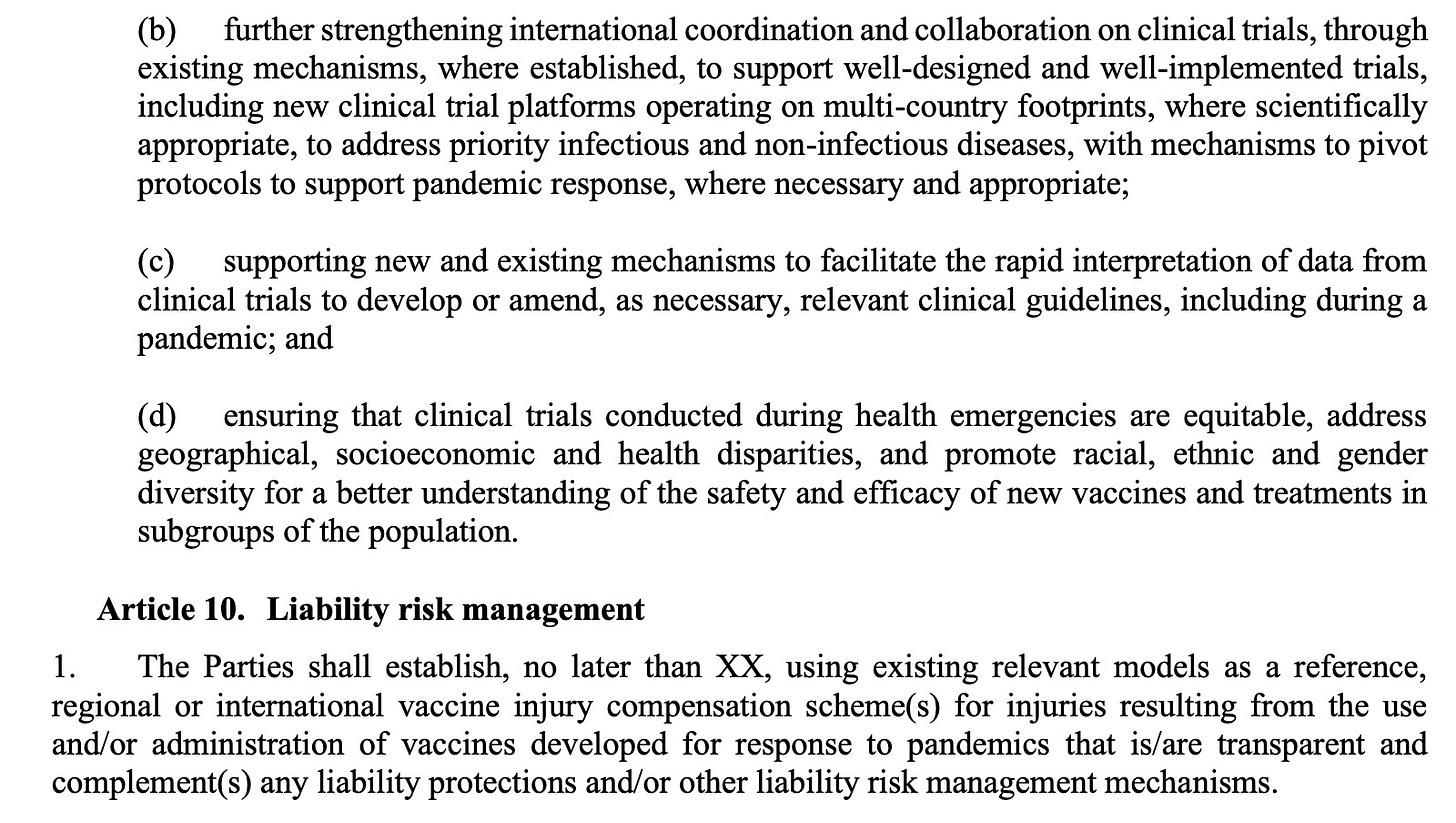
Manufacturer and Government Liability for Vaccine Injuries Must be “Managed”
Nations are supposed to use “existing relevant models” as a reference for compensation of injuries due to pandemic vaccines. Of course, most countries do not have vaccine injury compensation schemes, and when they do the benefits are usually minimal.
Is the US government’s program to be a model of what gets implemented internationally?
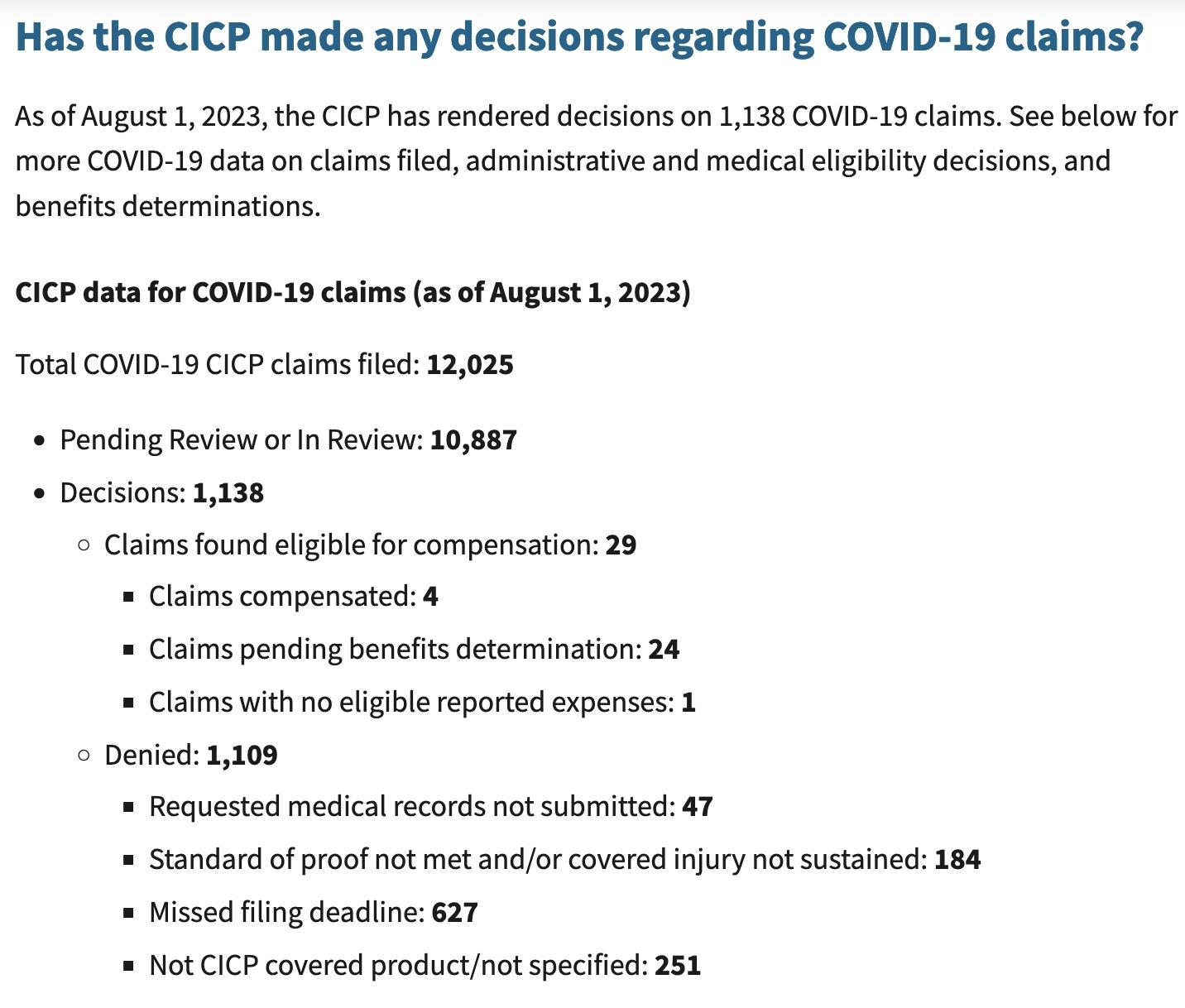
The US government scheme for injuries due to COVID pandemic products (the Countermeasures Injury Compensation Program or CICP) has compensated exactly 4 (yes, four) of the 12,000 claimants for COVID product-related injuries as of August 1, 2023. All pandemic EUA drugs and vaccines convey a liability shield to the government and manufacturers (this includes monoclonal antibodies, pre-licensure remdesivir, paxlovid, molnupiravir, some ventilators and all COVID vaccines) and the only avenue for injury compensation is through this program.
Slightly over 1,000 of the 12,000 claims have been adjudicated while 10,887 are pending review. Twenty claims were deemed eligible and await a benefits review. Benefits are only paid for uncovered medical expenses or lost income. A total of 983 people, or 98 percent of those whose claims have been adjudicated had their claims denied, many because they missed the brief one-year statute of limitations. Below are the latest data from this program:
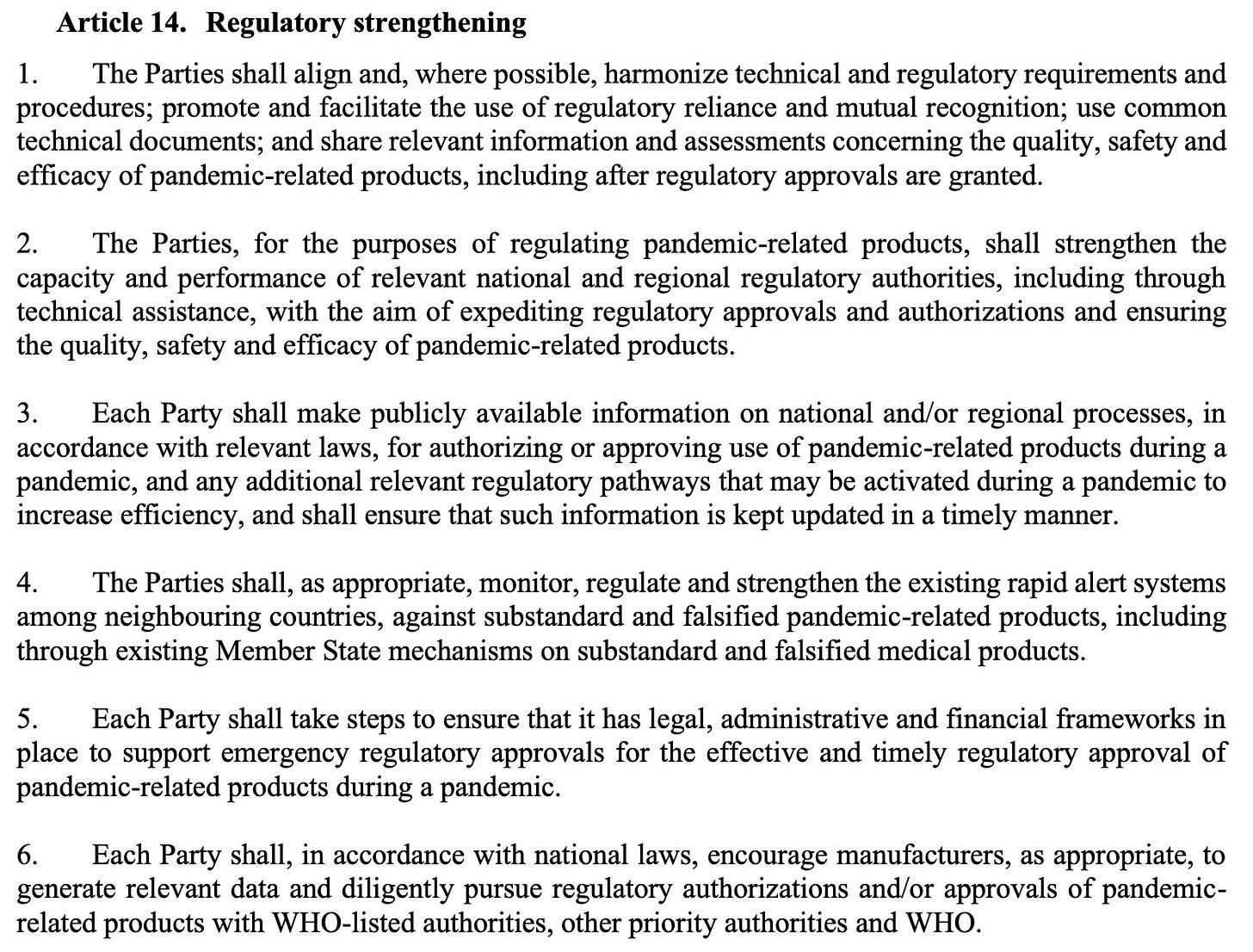
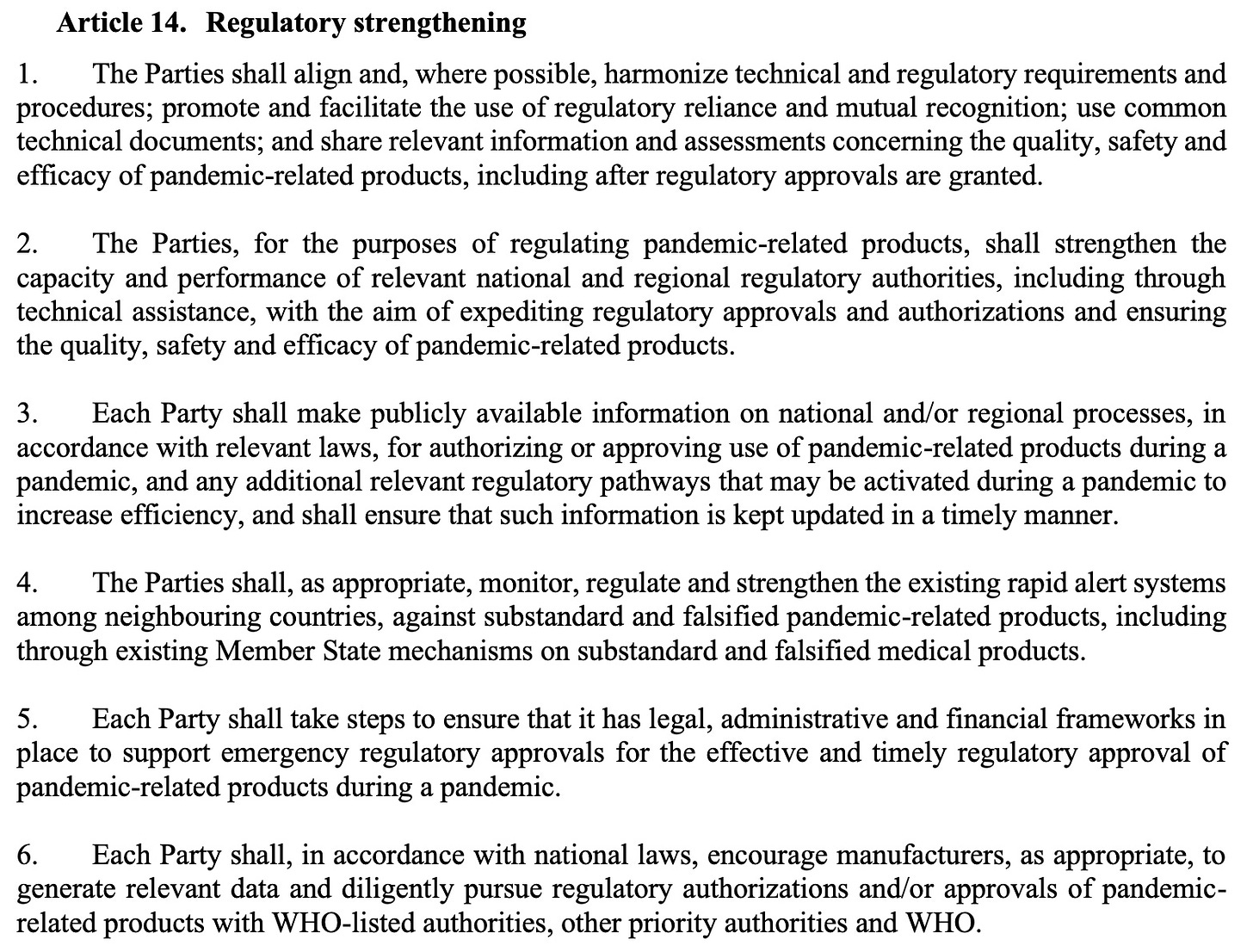
The treaty draft also demands weakening the strict regulation of medical drugs and vaccines during emergencies, under the rubric of “Regulatory Strengthening.” As announced in the UK last week, where ‘trusted partner’ approvals will be used to speed licensure, this is moving toward a single regulatory agency approval or authorization, to be immediately adopted by other nations (p 25).
Next Up: Vaccines Developed in 100 Days
A plan to develop vaccines in 100 days and have them manufactured in 30 additional days has been widely publicized by the vaccine nonprofit CEPI, founded in 2017 by Sir Dr. Jeremy Farrar, who is now the WHO’s Chief Scientist. The plan has been echoed by the US and UK governments and received some buy-in from the G7 in 2021. This timeframe would only allow for very brief testing in humans, or would, more likely, limit testing to animals. Why would any country sign up for this? Is this what we the people want?
The plan furthermore depends on the vaccines only being tested for their ability to induce antibodies, which is termed immunogenicity, rather than being shown to actually prevent disease, at least for the initial rollout. My understanding of FDA regulation was that antibody levels were not an acceptable surrogate for immunity unless they had been demonstrated to actually correlate with protection. However, the FDA’s recent vaccine decisions have scrapped all that and vaccines are now being approved based on antibody titers alone. The FDA’s vaccine advisory committee has asked it for better indicators of efficacy than this, but the advisers have also voted to approve or authorize vaccines in the absence of any real measures showing that they work. I learned this because I watch the FDA vaccine advisory meetings and provide a live blog of them.
We all know how long it took for the public to become aware that the COVID vaccines failed to prevent transmission and only prevented cases for a period of weeks to months. The US government has still not officially admitted this, even though CDC Director Rochelle Walensky told CNN’s Wolf Blitzer the truth about transmission on August 6, 2021.
It is critical for the public to understand that safety testing can only be accomplished in human beings, as animals react differently to drugs and vaccines than humans do. Therefore, limited testing in animals would mean there was no actual safety testing. But testing vaccines in humans for only short periods is also unacceptable.
Testing vaccines during brief trials in humans (the Pfizer trials only followed a “safety subset” of trial subjects for a median of two months for safety) allowed COVID vaccines to be rolled out without the public being aware they could cause myocarditis and sudden deaths, most commonly in athletic young males in their teens and twenties, or a myriad of other conditions.
Finally, following this rapid manufacturing plan, thorough testing for potential failures in the manufacturing process could not be performed. With the current plan for far-flung, decentralized manufacturing facilities that are said to be necessary to achieve vaccine equity for all, there are nowhere near enough regulators who could inspect and approve them.
Will the WHO Respect Human Rights?
The need to respect “human rights, dignity, and freedom of persons” is embedded in the current International Health Regulations (IHR), as well as other UN treaties. However, the language guaranteeing human rights, dignity, and freedom of persons was peremptorily removed from the proposed IHR Amendments, without explanation. The removal of human rights protections did not go unnoticed, and the WHO has been widely criticized for it.
The WHO apparently is responding to these criticisms, and so the language guaranteeing human rights that was removed from the drafts of the International Health Regulations has been inserted into the newest version of the pandemic treaty.
Conclusions
As long predicted by science fiction, our bio- and cyber-scientific achievements have finally gotten away from us. We can produce vaccines in 100 days and manufacture them in 130 days–but there will be no guarantees that the products will be safe, effective, or adequately manufactured. And we can expect large profits but no consequences for the manufacturers.
Our genes can be decoded, and the fruits of personalized medicine made available to us. Or perhaps our genes will be patented and sold to the highest bidder. We might be able to select for special characteristics in our children, but at the same time, a human underclass could be created.
Our electronic communications can be completely monitored and censored, and uniform messaging can be imposed on everyone. But for whom would this be good?
New biological weapons can be engineered. They can be shared. Maybe that will speed up the development of vaccines and therapeutics. But who really benefits from this scheme? Who pays the price of accidents or deliberate use? Wouldn’t it be better to end so-called gain-of-function research entirely through restrictions on funding and other regulations, rather than encouraging its proliferation?
These are important issues for humanity, and I encourage everyone to become part of the conversation.
Dr. Meryl Nass, MD is an internal medicine specialist in Ellsworth, ME, and has over 42 years of experience in the medical field. She graduated from University of Mississippi School of Medicine in 1980.
How the current version of the WHO’s Pandemic Treaty (aka Bureau Text) encourages rather than prevents pandemics
BY MERYL NASS | AUGUST 5, 2023
Weapons of Mass Destruction: Chem Bio
Traditionally, Weapons of Mass Destruction (WMD) were Chemical, Biological, Radiologic and Nuclear (CBRN).
The people of the world don’t want them used on us—they are cheap ways to kill and maim lots of people at once. And so international treaties were created to try to prevent their development (sometimes) and use. First was the Geneva Protocol of 1925, banning the use of biological and chemical weapons in war. The US and many nations signed it, but it took 50 years for the US to ratify it, so we believed we were not bound by it.
The US used chemical weapons subsequently. The US probably used biological weapons in the Korean War, and perhaps in Vietnam, which experienced an odd outbreak of plague during the war. The use of napalm, white phosphorus, agent orange (with its dioxin excipient causing massive numbers of birth defects and other tragedies) and possibly other chemical weapons led to much pushback, especially since we had signed the Geneva Protocol and we were supposed to be a civilized nation.
In 1968, a young Seymour Hersh wrote a book about the US chemical and biological warfare program. In 1969 Congressman Richard D. McCarthy wrote the book “Ultimate Folly” about the US production and use of chemical and biological weapons. Prof. Matthew Meselson’s review of the book noted,
Our operation, “Flying Ranch Hand, ” has sprayed anti-plant chemi-
cals over an area almost the size of the state of Massachusetts, over
10 per cent of it cropland. “Ranch Hand” no longer has much to do with
the official justification of preventing ambush. Rather, it has become
a kind of environmental warfare, devastating vast tracts of forest in
order to facilitate our aerial reconnaisance. Our use of “super tear
gas” (it is also a powerful lung irritant) has escalated from the originally
announced purpose of saving lives in “riot control-like situations” to the
full-scale combat use of gas artillery shells, gas rockets and gas bombs
to enhance the killing power of conventional high explosive and flame
weapons. Fourteen million pounds have been used thus far, enough
to cover all of Vietnam with a field effective concentration. Many
nations, including some of our own allies have expressed the opinion
that this kind of gas warfare violates the Geneva Protocol, a view
shared by M cCarthy.
A Biological Weapons Convention
Amid great pushback over US conduct in Vietnam, in November 1969 President Nixon announced to the world we were going to end the US biowarfare program (but not the chemical program). In February 1970 Nixon announced we would also get rid of our toxin weapons (snake, snail, frog, fish, bacterial and fungal toxins that could be used for assassinations, etc.). Furthermore, Nixon said the US would initiate an international treaty to prevent the use of these weapons ever again. And we did: the 1972 Convention on the prohibition of the development, production and stockpiling of bacteriological (biological) and toxin weapons and on their destruction, or Biological Weapons Convention (BWC) for short, which entered into force in 1975.
The BWC established conferences to be held every 5 years to strengthen the Convention. The expectation was that these would add a method to call for ‘challenge inspections’ to prevent cheating and would add sanctions (punishments) if nations did not comply with the treaty. However, the US has consistently blocked the addition of protocols that would have an impact on cheating. By now, everyone knows that cheating occurs and is likely widespread.
A leak in an anthrax production facility in Sverdlovsk, USSR in 1979 caused the deaths of about 60 people. A clear BWC violation. US experiments with anthrax production during the Clinton administration, detailed by Judith Miller et al. in the 2001 book Germs were also thought by experts to have transgressed the BWC.
In 1997 a Chemical Weapons Convention came into force. It took over 20 years, but all official stocks of chemical weapons have been destroyed by the USA and by Russia and the other 193 member nation signatories.
Pandemics or Biological Warfare?
So here we are. It is 2023 and the WHO Director General has declared 2 pandemics (the current terminology is ‘Public Health Emergency of International Concern’) over the past 3 and a half years: COVID-19 and monkeypox, which was renamed MPOX to “avoid stigma.” I am sure the monkeys were relieved by the name change.
I have previously (in my substack) described why I believe both SARS-CoV-2 and MPOX were bioengineered pathogens that came from labs. I do not know if they leaked or were deliberately released, but I am leaning toward deliberately released for both of them, based on where they appeared, how they spread, and in particular the official responses to each—neither of which was explained accurately to the public, and yet we never changed course, even when the lack of efficacy with masks, social distancing, EUA drugs and vaccines had become clear.
Vaccines: the Chicken or the Egg?
Both the monkeypox vaccines (there are two, Jynneos and ACAM2000) are known to cause myocarditis, as do the two COVID-19 mRNA vaccines and the Novavax vaccine. The Novavax vaccine was first associated with myocarditis during its clinical trial in Australia. I have written about all this previously on substack.
How frequently does myocarditis occur after these vaccines? If you use elevated cardiac enzymes as your marker, ACAM2000 caused this in one in thirty people receiving it for the first time. If you use other measures like abnormal cardiac MRI or echo, according to the CDC it occurs in one in 175 vaccinees. We do not know the number for Jynneos, but there was some degree of elevation of cardiac enzymes in 10% and 18% of recipients in two small prelicensure studies. My guess for the mRNA vaccines is that they are somewhere in this range. I don’t know about Novavax’ vaccine.
Why would our governments push 5 separate vaccines all known to cause myocarditis on young males who have been at extremely low risk from COVID, and who simply get a few pimples for 1-4 weeks from monkeypox unless they are immunocompromised? It’s an important question. It does not make medical sense. Especially when the vaccine probably does not work — Jynneos didn’t on the monkeys in whom it was tested. And CDC has clammed up about the 2,000 Congolese healthcare workers on whom CDC tested it for efficacy and safety in 2017. (I have detailed this too in earlier substacks.)
The health authorities could have just been ignorant—that could explain the first 8 months of the COVID vaccines’ rollout. But once they figured out, and even announced in August 2021 that the vaccines did not prevent catching COVID or transmitting it, why did they still push it on low risk populations who were clearly at greater risk from a vaccine side effect?
Once this is acknowledged, you realize that maybe the vaccines were not made for the pandemic, and instead the pandemic was made to roll out the vaccines. I’m not sure. But I’m suspicious. And the fact that multiple countries contracted for 10 doses per person makes me even more suspicious—for vaccines whose safety and efficacy had not been established. WHY would you want ten doses apiece? Three maybe. But ten?
Furthermore, you don’t need a vaccine passport aka digital ID aka justification to convert to all-electronic money unless you are giving out regular boosters. Were the vaccines conceived of as the pathway to getting our vaccinations, health records, official documents and financial transactions all online—as Ukraine has already done?
A Pandemic Treaty and Amendments: Brought to you by the same people who mismanaged the past 3 years, to save us from themselves?
The same US government and western governments that imposed draconian measures on their citizens to force us to be vaccinated and take dangerous, expensive, experimental drugs and withheld the good drugs, decided in 2021 we needed a pandemic treaty to prevent and ameliorate future pandemics or biological warfare events… so we would not suffer as we did with the COVID pandemic.
Except COVID was a disaster due to its mismanagement (or should I say dismanagement or malmanagement?) by our nations’ rulers, their bosses and the WHO. Hundreds of millions of our fellow human being were slammed into extreme poverty—by nations following guidelines issued by the WHO, whose main job it was to protect exactly those people. Tens of millions died from starvation as a result. Yet the WHO blathers on about equity, diversity and solidarity—having itself caused the worst (manmade) food crisis in our lifetimes. Have you heard any apology or explanation?
How can anyone with a brain believe the public health officials who messed up COVID so badly want to spare us from another medical and economic disaster, after they imposed the last one on us? And the fact that no governments or health officials will admit their mistakes — especially how they made it nearly impossible to obtain the cheap and safe drugs that effectively treat COVID — why would we let them plan anything, let alone an international treaty that will bind our governments to obey the WHO’s dictates? How thoughtful of these officials to want to spend a king’s ransom of our money to prevent the next government-caused disaster.
We are fed up with secret vaccine contracts, waivers of liability for junk medical products, and spikes in sudden deaths and chronic disabilities. No more secret negotiations. Please shove your pandemic planning where the sun…
The Gain of Function farce
Obviously, the best way to spare us from another pandemic is to immediately stop funding “Gain of Function”* research, and get rid of what has already been funded and created. Let all the nations make big bonfires and burn up their evil creations at the same time, while allowing other nations to inspect their biological facilities and records.
But the WHO in its Bureau Text of the draft Pandemic Treaty has a plan that is the exact opposite of this. In the WHO’s world, which almost all nations’ rulers have bought into, all the governments will share any and all viruses and bacteria they come up with that have “pandemic potential” — share them with all the other governments. They are supposed to sequence them and then put the sequence online. No kidding. Then the WHO and all the Faucis of the world would gain access to every Frankenstein virus, at once. Presumably a bunch of hackers would also gain access to the sequences. Does this make you feel more secure?
The WHO Treaty draft incentivizes Gain Of Function research
At least this plan makes clear whose side everyone is on. Fauci, Tedros and their ilk at the WHO, and those managing biodefense and biomedical research for nation states are on one side, the side that gains access to even more biological weapons, and the rest of us are on the other, at their mercy.
This crazy plan used to be called proliferation of weapons of mass destruction—and it is almost certainly illegal. But it is their plan. Governments will all share the weapons. And they are to put a lot more money into biolabs, and especially into genomic sequencing. Presumably so they can make even better weapons, and maybe they will even get around to cures or antidotes. But who will get the cures? It wasn’t us during the COVID-19 pandemic. Here is where you can read the current Treaty draft:
https://apps.who.int/gb/inb/pdf_files/inb5/A_INB5_6-en.pdf
Pages 10 and 11:




What else is in the Treaty? Gain of Function research (designed to make pathogens more transmissible or more virulent) is explicitly incentivized. Administrative hurdles to it must be minimized, while unintended consequences (pandemics) should be prevented: (page 14)

Vaccines will be rolled out speedily under future testing protocols
Just in case you thought the COVID vaccines took too long to be rolled out, the WHO has plans to shorten testing. There will be new clinical trial platforms. Nations must increase clinical trial capacity. (Might that mean mandating people to be human subjects in out-of-the-way Africa, for example?). And there will be new “mechanisms to facilitate the rapid interpretation of data from clinical trials” as well as “strategies for managing liability risks.” (page 14)
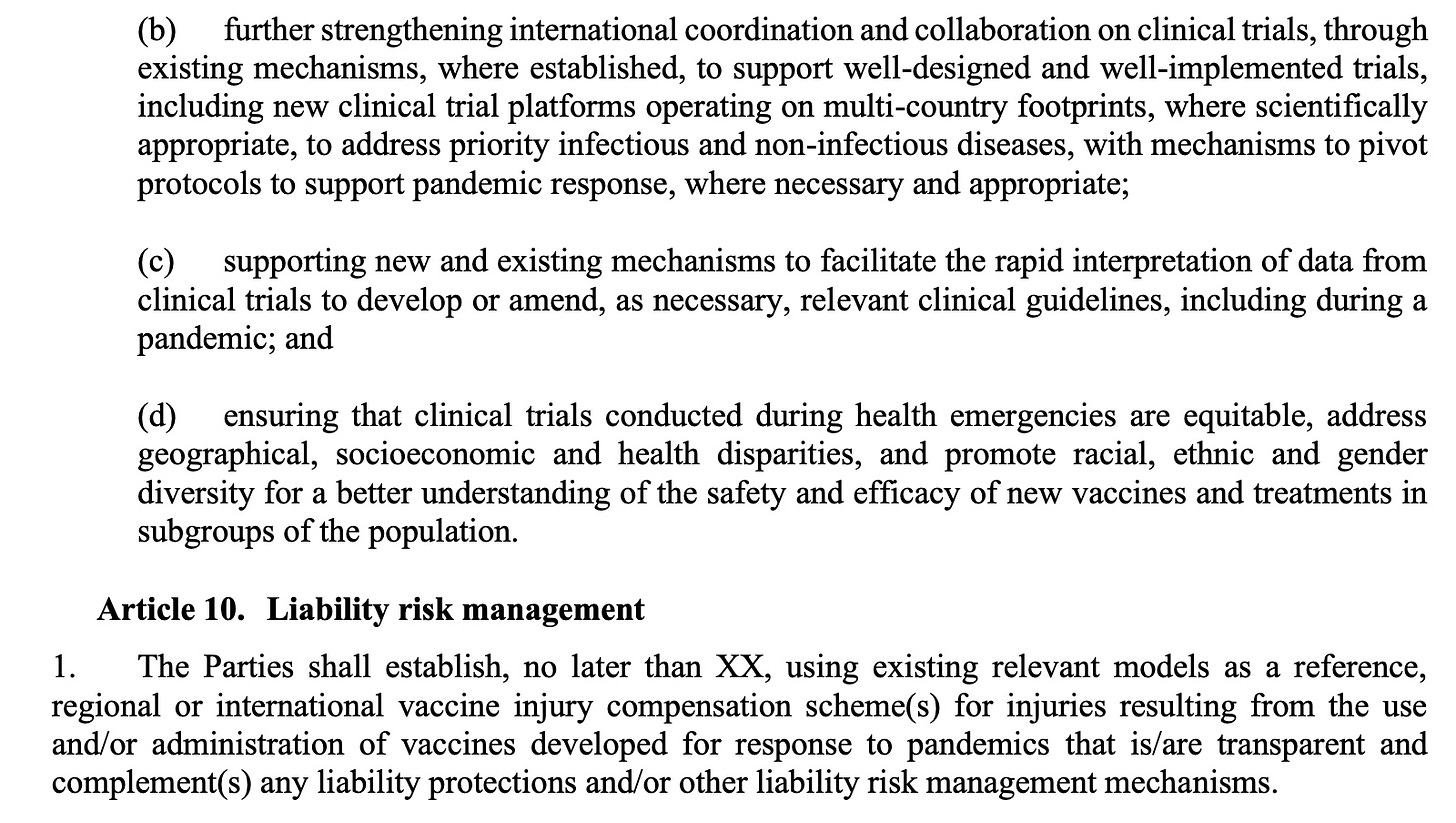
Manufacturer and government liability will be “managed”
Nations are supposed to use existing models as a reference for compensation of injuries due to pandemic vaccines. Of course, most countries do not have vaccine injury compensation schemes, and when they do the benefits are usually minimal. The US government scheme for injuries due to COVID pandemic products (the Countermeasures Injury Compensation Program or CICP) has compensated 4 (yes, FOUR) people as of July 1, 2023. All pandemic EUA drugs and vaccines fall into this program (monoclonal antibodies, early remdesivir, paxlovid, molnupiravir, some ventilators and all COVID vaccines). There have been nearly 12,000 claims made to the CICP related to a COVID product. Slightly over 1,000 have been adjudicated while 10,886 are pending review. Twenty claims were deemed eligible and are waiting to see whether they can collect. A total of 983 people, or 98% had their claims denied. About 90% of all claimants filed for a vaccine injury.

The treaty draft also demands weakening the regulation of medical drugs and vaccines during emergencies under the rubric of Regulatory Strengthening. As announced in the UK last week, where ‘trusted partner’ approvals will be used to speed licensure, this is moving toward a single regulatory agency approval or authorization, to be immediately adopted by other nations (p 25)
Why would any developed country sign up for this? Is this what we the people want?
The WHO did sweeten the pot, however. Remember how the need to respect “human rights, dignity, and freedom of persons” was removed in the WHO’s draft IHR Amendments that are being negotiated? Well, WHO apparently did not like us pointing that out—so the old human rights language that was removed from the International Health Regulations draft has been added to this newest version of the Treaty.
There is much more I could say about problems with this draft of the Treaty, but I will save them for another time.
Please share this brief analysis of the WHO’s Pandemic Treaty. We must EXIT the WHO.
*Gain of Function is a euphemism for biological warfare reserch or germ warfare research. It is so foolhardy that it was banned in the US for SARS coronaviruses and avian flu viruses from 2014-2017 due to public outcry by scientists. Then in 2017 Fauci and Collins lifted the moratorium, claimed they were putting safeguards in place, which were just a handwaving exercise, and off we were to the races: creating new bioweapons. Fauci and Collins had the nerve to publish their opinion that the risk was ‘worth it.’
‘Health Program or Military Program’? White House Taps Military Official to Lead New Pandemic Policy Office
By Michael Nevradakis, Ph.D. | The Defender | July 26, 2023
Just weeks after ending the COVID-19 national and public health emergencies and the resignation of COVID-19 Response Coordinator Ashish Jha, the White House launched its Office of Pandemic Preparedness and Response Policy (OPPR).
Retired Major General Paul Friedrichs, a military combat surgeon, will lead the office, the White House said.
According to the White House, the OPPR will be “a permanent office in the Executive Office of the President (EOP) charged with leading, coordinating, and implementing actions related to preparedness for, and response to, known and unknown biological threats or pathogens that could lead to a pandemic or to significant public health-related disruptions in the United States.”
The OPPR will take over the duties of President Biden’s COVID-19 and monkeypox response teams, including “ongoing work to address potential public health outbreaks and threats from COVID-19, Mpox, polio, avian and human influenza, and RSV [respiratory syncytial virus],” the announcement stated.
The OPPR also will oversee efforts to “develop, manufacture, and procure the next generation of medical countermeasures, including leveraging emerging technologies and working with HHS [U.S. Department of Health and Human Services] on next generation vaccines and treatments for COVID-19 and other public health threats.”
According to The New York Times, Friedrichs, set to take office Aug. 7, will have the authority to “oversee domestic biosecurity preparedness.” He will work on the development of next-generation vaccines, ensure adequate supplies in the Strategic National Stockpile and “ramp up surveillance to monitor for new biological threats.”
Several medical, biosecurity and civil liberties experts questioned the selection of a career military and biosecurity individual to head a new office charged with pandemic preparedness.
They also told The Defender they saw parallels between the White House’s establishment of the OPPR and ongoing United Nations (U.N.) efforts to draft a global declaration on Pandemic Prevention, Preparedness and Response (PPPR).
‘Is OPPR a health program or a military program?’
Friedrichs, a board-certified physician, is currently a special assistant to the president and senior director for Global Health Security and Biodefense at the National Security Council.
He previously served as joint staff surgeon at the U.S. Department of Defense (DOD) and as medical adviser to the Pentagon’s COVID-19 task force.
Throughout his career, the White House said, Friedrichs worked closely with federal, state, tribal, local and territorial government partners, as well as industry and academic counterparts.
According to the White House:
“As the United States’ representative to the North Atlantic Treaty Organization Committee of Military Medical Chiefs, he worked closely with many of America’s closest allies and partners throughout the pandemic and in developing medical support to the Ukrainian military.”
In his previous roles at the National Security Council and DOD, Friedrichs was a strong proponent of COVID-19 vaccines and countermeasures.
The Times reported that, in a February speech, Friedrichs said, “The military health system became the pinch-hitter that stepped in to help our civilian partners as we collectively struggled to work through that pandemic.”
In a February 2022 podcast, Friedrichs praised the COVID-19 vaccines and also appeared to blame those who were unvaccinated for placing “stress on our system.”
And in remarks shared in January 2022 with the Association of the United States Army, Friedrichs asked military families to continue holding off on gatherings so that service members are “able to do the things that our nation depends on them to do.”
Does Friedrichs’ appointment signal more vaccine mandates?
Describing Friedrichs’ appointment as “a joke and a fraud,” Francis Boyle, J.D., Ph.D., a bioweapons expert and professor of international law at the University of Illinois who drafted the Biological Weapons Anti-Terrorism Act of 1989, told The Defender :
“DOD has routinely enforced experimental medical vaccines on U.S. Armed Forces, in gross violation of the Nuremberg Code on Medical Experimentation — that is, a Nuremberg crime against humanity — from today’s COVID-19 ‘vaccines’ and going all the way back in recent history to the ‘vaccines’ that produced Gulf War sickness starting in 1990-1991, when Friedrichs was a U.S. Military medical doctor.
“Of 500,000 U.S. troops inoculated, 11,000 died and 100,000 were disabled. I do not recall that Friedrichs was among the handful of courageous and principled military medical doctors who refused, as a matter of principle, to inflict Nuremberg crimes on our own troops. Did he? That needs to be investigated.”
Michael Rectenwald, Ph.D., author of “Google Archipelago: The Digital Gulag and the Simulation of Freedom,” said the selection of Friedrichs, who supported military vaccine mandates, may signal similar future mandates for the general public.
“We should not forget that the DOD mandated the COVID-19 vaccine for service members,” Rectenwald said. “The OPPR will mandate vaccines for the nation.”
And writing on her blog, Dr. Meryl Nass, an internist, biological warfare epidemiologist and member of the Children’s Health Defense scientific advisory committee, questioned if the OPPR plans “to use the military’s OTA [other transaction] authority again to bypass the FDA [U.S. Food and Drug Administration] and vaccinate us with untested junk that turned out to be poison, like it did for COVID.”
Is OPPR “a health program or a military program?” Nass wrote.
Nass told The Defender that if the main purpose of the OPPR was to respond to pandemics and pandemic threats, an epidemiologist or infectious disease doctor would have been tapped to head the office instead of a military general.
Similarly, Dr. David Bell, a public health physician, biotech consultant and former director of Global Health Technologies at Intellectual Ventures Global Good Fund, told The Defender :
“COVID-19 demonstrated that the sort of interventions envisioned by the pandemic preparedness lobby such as lockdowns and coerced mass vaccination, have poor public health outcomes.
“Public health should be concentrated on informing the public to make personal decisions about health, rather than the population-control approaches we saw for COVID-19 that are most profitable to the corporate world. We must hope this new health bureaucracy is more independent of vested interests, and will take an evidence-based approach.”
Nass suggested that Friedrich’s selection belies a broadly encompassing biosecurity agenda, which would include censorship of non-establishment medical information, surveillance and mass, or mandatory, vaccination, tied to U.N. and World Health Organization (WHO) “pandemic preparedness and response” efforts.
A ‘WHO globalist worldwide medical and scientific police state’ here in the U.S.?
Other experts also noted the similarities between the name of the OPPR, the U.N.’s draft PPPR and a similar recent agreement among WHO member states.
Still in “zero draft” form, the PPPR is scheduled to be discussed by the U.N. General Assembly in September 2023. It would also be tied to the WHO’s proposed pandemic treaty and amendments to the International Health Regulations.
Similarly, a June 28 document from the WHO said, “Member States … have agreed to a global process to draft and negotiate a convention, agreement or other international instrument under the Constitution of the World Health Organization to strengthen pandemic prevention, preparedness and response.”
And a separate but similar set of proposals — part of the U.N.’s “Pact for the Future” and “Our Common Agenda” — would give the U.N. secretary-general unprecedented emergency powers not only for pandemics but seemingly for an unlimited range of other potential crises. The U.N. will discuss these proposals in September 2024.
Boyle told The Defender the OPPR is “obviously being coordinated with the U.N. [and] the Biden administration to establish the effective functioning of a WHO globalist worldwide medical and scientific police state here in the United States.”
“You need the mentality of an unprincipled military medical major general to do that,” Boyle said. “All the trains will run on time.”
Rectenwald drew similar connections, telling The Defender the OPPR and Friedrichs’ selection:
“Signifies the militarization of pandemic responses in the U.S., in line with the ‘global governance’ measures outlined by the U.N.’s Pandemic Preparedness, Prevention and Response declaration.
“This new wing of the executive branch is the means by which this ‘global governance’ (read: one-world totalitarian system) is being introduced to the U.S., using pandemic preparedness as the pretext.”
Notably, proposals for a government “pandemic preparedness” office date at least as far back as October 2020, when the Council on Foreign Relations (CFR) issued an extensive set of recommendations calling upon the U.S. government to “adopt a robust strategy for domestic and global pandemic preparedness.”
The report recommended that the U.S. “finally treat pandemics as a serious national security threat, translating its rhetorical support for pandemic preparedness into concrete action.”
According to the CFR, this would entail “bolstering the White House’s leadership role in preparing for and responding to pandemics, improving congressional input into and oversight over executive branch efforts, reforming the CDC so that it can perform more effectively, and clarifying the often confused division of labor across federal, state, and local governments in pandemic preparedness and response.”
“The president should designate a focal point within the White House for global health security, including pandemic preparedness and response,” the report added. “This office would have lead responsibility for coordinating the multiple federal departments and agencies in anticipating, preventing, and responding quickly to major disease outbreaks.”
OPPR reports to Congress required only every 5 years, not annually
The establishment of the OPPR resulted from the passage of the PREVENT Pandemics Act in December 2022.
The bill, introduced by Sen. Patty Murray (D-Wash.) and the now-retired Sen. Richard Burr (R-N.C.), passed as part of an omnibus spending bill, contained a requirement for the creation of a White House pandemic preparedness and response office.
Though the bill was passed in December 2022, the White House was unable to immediately establish a pandemic preparedness office and name a director.
A Politico report in May said these efforts were “hindered by concerns over whether [the office] will have the influence within the administration and the financial resources needed to fulfill its broad mission — especially as COVID plummets down the list of political priorities.”
According to the White House announcement, OPPR will “Develop and provide periodic reports to Congress” as required by law, including drafting and delivering to Congress “a biennial Preparedness Review and Report and Preparedness Outlook Report every five years.”
On her blog, Nass wrote, “Instead of the more customary yearly reports, the reporting to Congress is being delayed considerably, perhaps until after many of us have died from the countermeasures — a great way to evade oversight.”
In a separate blog post, Nass also observed that the Centers for Disease Control and Prevention requested $20 billion for “pandemic preparedness” in its fiscal year 2024 budget.
Michael Nevradakis, Ph.D., based in Athens, Greece, is a senior reporter for The Defender and part of the rotation of hosts for CHD.TV’s “Good Morning CHD.”
This article was originally published by The Defender — Children’s Health Defense’s News & Views Website under Creative Commons license CC BY-NC-ND 4.0. Please consider subscribing to The Defender or donating to Children’s Health Defense.
The appropriations committee marked up their bill and the budget for the WHO remains at zero!
MERYL NASS | JULY 13, 2023
Furthermore, there is also in the bill no money for operationalizing the Pandemic Treaty unless it goes through the Senate for approval:

Can the WHO and the United Nations impose sanctions on your country for non-compliance?
The sinister sanctions strategy has disturbing implications for democracy, peace, and prosperity around the world. It’s time for us to defund and exit.
By Shabnam Palesa Mohamed | Children’s Health Defense Africa | July 3, 2023
Sanctions are a powerful instrument of political control and economic profit. One of the rare but critical topics relevant to the international campaign to #ExitTheWHO is whether the World Health Organisation and the United Nations can impose, influence or recommend specific sanctions. The sanctions would be against countries that choose to not comply or cannot comply with International Health Regulations, the proposed new pandemic treaty, or other legislative attempts that curtail rights, freedom and sovereignty.
The accelerating and profitable globalist march towards unprecedented levels of ‘1984’ style totalitarianism – using censorship, vaccine passports, 15 minute cities, and CBDC’s continues. It is plausible that the WHO and the UN will move to impose, influence or recommend sanctions against countries that do not want to or cannot comply with its centralised health agenda and undemocratic legislative attempts.
At last year’s World Health Assembly 75, the 47 nation African bloc voted surprisingly, against most amendments to the International Health Regulations, stating that they were broad, rushed, and can pose a threat to national sovereignty. Since then, no doubt with persuasive behind the scenes manoeuvres, some of the most disturbing amendments are being proposed by African countries. Many relate to financing for the cost intensive provisions of IHR amendments and the proposed pandemic treaty or accord. Africa cannot afford more debt slavery.
Countries that could be sanction targets for non-compliance with the WHO and the UN, include but are not limited to, those in the steadily growing BRICS initiative: Brazil, Russia, India, China and South Africa. Iran and Malaysia are reported to have expressed reservations to the proposed IHR amendments at last year’s World Health Assembly 75. Russia is making decisive moves in the international arena and could possibly exit the WHO. In addition, India raised serious audit concerns on irregularities with WHO financials, including missing assets.

World Health Assembly, Geneva, Switzerland
The ambit of the overwhelmingly privately funded WHO, contained in its extensive constitution, can be interpreted as overly broad and sweeping, and thus, unknown to non-participants, has always posed a potential threat to individual health and national sovereignty.
The WHO’s constitution states in Chapter 2 – Functions – Article 2: In order to achieve its objective, the functions of the Organization shall be: (v) generally to take all necessary action to attain the objective of the Organization. However Article 21 of the WHO’s constitution is specific about making (non-binding) regulations, limiting the WHO to just five areas.
Proposed amendments to the new pandemic treaty include a dangerous clause that would change the WHO’s role from a UN agency that shares recommendations, to a rogue agency whose elitist and secretive attempts at legislation are binding and mandatory on member states, violating fundamental human rights and freedoms. However, health freedom advocates agree that WHO has no actual authority in the law.
In effect therefore, with both IHR amendments and the proposed new treaty, the WHO is acting ultra vires in its Big Pharma driven power grab, in collusion with naïve or compromised member state delegates. Ultra vires is defined in the law as: acting beyond the scope or in excess of legal power or authority. Ultra vires acts of impunity by the WHO could accelerate a mass defund and exit of the agency.

WHO’s negotiating body on a proposed pandemic treaty
Health is no longer just health, as it is defined in the WHO’s constitution. Through Covid-19, and other controversially declared pandemics, health is now a multi-billion dollar health security industry. With it, creeps in the tyranny of secrecy, surveillance, vaccine certificates, forced quarantines, and the undemocratic censorship of free speech. Given the absence of public participation, the WHO is a strategic spear for oligarchs and corporations, and given international resistance to its power grab, it may become desperate and argue or push for sanctions.
Reported in 2021: “In 2021, German Health Minister Jens Spahn called for sanctions against countries that hide information about future outbreaks. Citing the World Trade Organization’s power to sanction countries for non-compliance, Spahn said “there must be something that follows” if countries fail to live up to commitments under a new pandemic treaty that the World Health Assembly will take up in November.”
Further, it is entirely under reported that controversial “World Health Organization Director-General Tedros Adhanom Ghebreyesus also urged countries to consider the idea as they take up the treaty, a legally binding tool. The treaty should “have all the incentives, or the carrots” to encourage transparency, Tedros said, appearing at a press conference with Spahn in Berlin. “But maybe exploring the sanctions may be important,” he added.”
Also reported in 2021: “Speaking at the WHA in June, Mike Ryan, WHO Health Emergencies Programme Executive Director, also spoke out in favour of the treaty, despite the fact that WHO technical staff have historically avoided taking positions on controversial policy choices before member states. “My personal view is that we need a political treaty that makes the highest-level commitment to the principles of global health security — and then we can get on with building the blocks on this foundation.”
I engaged renowned international law expert Professor Francis Boyle about the possibility of sanctions via the WHO. He had no doubt “They will pursue sanctions against countries that do not comply with their orders, coming from Geneva. Both economic and political sanctions. However, they will only have the power to pursue sanctions if we accept their authority. We cannot. We must exit the WHO.”
With far less public scrutiny currently than the WHO, the United Nations is also seeking exponential new powers and stronger “global governance” mechanisms to deal with what they define as international emergencies. In March 2023, the UN released a policy brief , astonishingly titled “To Think and Act for Future Generations – Our Common Agenda. Strengthening the International Response to Complex Global Shocks – An Emergency Platform”
These all encompassing areas of expanded UN power include:
- climate or environmental events;
- environmental degradation;
- pandemics;
- accidental or deliberate release of biological agents;
- disruptions in the flow of goods, people, or finance;
- disruptions in cyberspace or “global digital connectivity;”
- a major event in “outer space;”
- and “unforeseen risks (‘black swan’ events)
There are several types of sanctions imposed through the United Nations:
- Economic sanctions – typically a ban on trade, possibly limited to certain sectors such as armaments, or with certain exceptions (such as food and medicine)
- Diplomatic sanctions – the reduction or removal of diplomatic ties, such as embassies.
- Military sanctions – military intervention
- Sport sanctions – preventing one country’s people and teams from competing in international events.
- Sanctions on the environment – since the declaration of the United Nations Conference on the Human Environment, international environmental protection efforts have been increased gradually.
- Economic sanctions are distinguished from trade sanctions, which are applied for purely economic reasons, and typically take the form of tariffs or similar measures.
It is plausible that the UN’s controllers realise that the world is pushing back against the WHO’s overreach, or find it irrelevant to real health. Given that sovereign nations will choose to exit the WHO, the UN decided to launch plan B and ascribe to itself even greater powers. Technically, there is no legislation to exit the United Nations within the UN Charter. Again, this is a critical issue of national sovereignty.
The United Nations Children’s Fund or UNICEF’s 2020 Annual Report highlights USD 717 million in donations from the private sector, which is 21 percent of income overall. Lucrative corporate partnerships include Unilever, Louis Vuitton, and Microsoft, while foundation partners include Bill and Melinda Gates Foundation and Mastercard Foundation. It also prides relationships with the World Economic Forum and the International Chamber of Commerce. National committees fundraise from individual donors and corporations at the national level, to support UNICEF globally. The UN’s programmes therefore are heavily dependant on private funding. Funding crowns influence.

UN secretary general Antonio Guterres with WHO director general Adhanom Tedros Ghebreyesus
The WHO is an agency of the United Nations.
- In 2015, on punishing member states who violate the IHR, as reported: “United Nations health officials said they want to impose sanctions on countries that do not comply with public health regulations meant to avoid the spread of dangerous epidemics, such as the Ebola outbreak that killed more than 9,000 people and ravaged domestic health care systems in West Africa last year. World Health Organization Director Margaret Chan said she is investigating ways to reprimand countries that disobey the International Health Regulations (IHR) — a set of rules adopted in 2005 and mandate that countries set up epidemiological surveillance systems, fund local health care infrastructure and restrict international trade and travel to affected regions deemed unsafe to the public, among other provisions. Chan is on a panel set up by U.N. Secretary General Ban Ki-moon, who instructed the group to think of ways to hold countries accountable for how they manage public health crises and punish those who violate the IHR.”
- In 2022, according to commentators in a policy article: “In order to enforce compliance, some commentators have recommended concluding the treaty at the United Nations level. However, we fear that it has been already decided with the INB (mandated by WHASS) that a treaty will be developed under the roof of WHO. They added: “To move on with the treaty, WHO therefore needs to be empowered — financially, and politically. If international pandemic response is enhanced, compliance is enhanced. In case of a declared health emergency, resources need to flow to countries in which the emergency is occurring, triggering response elements such as financing and technical support. These are especially relevant for LMICs, and could be used to encourage and enhance the timely sharing of information by states, reassuring them that they will not be subject to arbitrary trade and travel sanctions for reporting, but instead be provided with the necessary financial and technical resources they require to effectively respond to the outbreak. High-income settings may not be motivated by financial resources in the same way as their low-income counterparts. An adaptable incentive regime is therefore needed, with sanctions such as public reprimands, economic sanctions, or denial of benefits.”
* Tweet CHD Africa if you agree that sanctions are possible and must be opposed internationally. Use the #StopSanctions

United Nations headquarters in Geneva, Switzerland
In 2000, Kofi Annan, former Secretary General of the UN said: “However, just as we recognize the importance of sanctions as a way of compelling compliance with the will of the international community, we also recognize that sanctions remain a blunt instrument, which hurt large numbers of people who are not their primary targets. Further, sanctions need refining if they are to be seen as more than a fig leaf in the future. Hence, the recent emphasis on targeted sanctions which prevent the travel, or freeze the foreign bank accounts, of individuals or classes of individuals – the so-called ‘smart sanctions’.”
Do sanctions work? “UN targeted sanctions, which are packages of sanctions imposed by the UN Security Council, have been successful in leading to intended policy change only 10% of the times, and limited the policies they intended to change in 28% of cases, but led to a reduced life expectancy in the targeted countries by 1.2–1.4 years. Economic sanctions have also been criticised for the potential collateral damage to third states they can cause. For this reason, some authors suggest that economic sanctions should be banned, as they are having detrimental effects on health and nutrition of civilians.”
Countries themselves can and do impose dangerous sanctions. A 2022 UN security council meeting on sanctions recorded: “Unilateral sanctions, which are sanctions imposed by (groups of) states and not by the UN Security Council, are particularly controversial. Unilateral sanctions have also been criticised for being disproportionately imposed on low-income and middle-income countries by wealthier countries, for example, by the Kenyan representative in a Security Council debate on sanctions on 7 February 2022: ‘The frequency and reach of unilateral sanctions have led to a growing view that they are the weapons of the strong against the vulnerable or weak’.”
- The Universal Declaration of Human Rights, in its first article, states that ‘all human beings are |…| equal in dignity and rights’, which includes the right to health. Article 25 specifies that ‘everyone has the right to |…| health and well-being |…| including medical care’.
- In the UN Convention on the Rights of the Child, article 24 states that ‘state parties recognize the right of the child to |…| the highest attainable standard of health and to facilities for the treatment of illness and rehabilitation of health. State parties shall strive to ensure that no child is deprived of his or her right of access to such health care services’.
- General Comment No.14 of the UN Committee on Economic, Social and Cultural Rights (CESCR) on the right to the highest attainable standard of health, the right to health is a fundamental human right which is necessary for all other human rights to exist and be exercised.
- “The use of sanctions designed to hurt a country’s healthcare sector is clearly incompatible with respecting citizens’ right to health. Accordingly, the general comment No. 14 of the CESCR calls on states to refrain ‘at all times’ from sanctions on medicines and medical equipment. However, sanctions on other healthcare products and, in fact, other non-healthcare products may as well interfere with the right to health, and, thus, need to be subject to scrutiny.”

WHO’s World Health Assembly 75
South African Precious Matsoso, co-chair of the International Negotiating Body (INB), formed to negotiate the terms of the proposed pandemic treaty or accord, admitted openly that punitive measures have not been shown to work “anywhere” in the world. However, she said, there must be accountability measures while recognizing countries’ sovereignty. “We have to recognize that they’re sovereign, and they keep on reminding us that they are sovereign states.” It is positive to note that more states do recognise the real threat to sovereignty.
Not all states are considered equal. Smaller countries are at a distinct disadvantage in participating, negotiating and making decisions at the hierarchical WHO. Significantly, Matsoso was transparent about failures in equal participation. “A number of smaller delegations have always expressed concerns about organizations of multiple meetings, where they have to travel from afar, and not even having the capacity to participate in the negotiations,” Matsoso said. “And they have repeatedly requested that you must avoid parallel sessions.” To little avail.
Given the rapidly growing distrust in the WHO, its historical failures and harms, Covid-19 failures and harms, and the fact that it cannot maintain independence because it is a largely privately funded entity; it is plausible that the WHO and/or the UN will move to impose or influence sanctions via the World Trade Organisation, ahead of Agenda 2030. This act of aggression weaponises the WHO and/or the UN against countries that influential funders and unethical stakeholders have an interest in destabilising for power and resource control.
This sinister strategy has disturbing implications for democracy, peace, and prosperity around the world. Freedom faces an existential risk through unelected bureaucratic entities. Nations can and must protect their sovereignty by defunding and exiting WHO, and, by critically assessing the true nature, value, and risks of continued membership in the 78 year old United Nations. Not to do so, means ignoring the risks of UN peacekeepers, who are known to commit crimes with impunity, being deployed in your country to enforce UN and WHO dictates.
Shabnam Palesa Mohamed is executive director and chapter coordinator for Children’s Health Defense Africa. She is an activist, journalist, lawyer, and mediator, with over 20 years of experience in human rights work. To share information, Twitter: @ShabnamPalesaMo
Follow CHD Africa on 6 social platforms for news, action alerts, and updates:
– Telegram: t.me/CHDafrica
– Twitter: https://twitter.com/CHD_Africa
– Instagram: https://www.instagram.com/af.childrenshealthdefense/
– Facebook: https://www.facebook.com/CHDafricachapter
– Rumble: https://rumble.com/user/ChildrensHealthDefenseAfrica
– Tiktok: https://www.tiktok.com/@chdafrica?is_from_webapp=1…
James Corbett Testifies at the National Citizens Inquiry
Corbett • 06/12/2023
Podcast: Play in new window | Download | Embed
On May 18, 2023, James Corbett testified to the National Citizens Inquiry in Ottawa on the subject of the WHO’s looming global pandemic treaty, the proposed amendments to the International Health Regulations, and the One Health approach that is being used to justify an even greater centralization of power in the hands of unaccountable institutions in the name of “global health.” The presentation also includes information on the prospect of Canada or other member states withdrawing from the WHO, information on the technocratic roots of the One Health agenda, how states of exception are used to undermine constitutional rights, and much, much more.
For those with limited bandwidth, CLICK HERE to download a smaller, lower file size version of this episode.
Watch on Archive / BitChute / Odysee / Rokfin / Rumble / Substack / Download the mp4
DOCUMENTATION
| National Citizens Inquiry – #SolutionsWatch | |
| Time Reference: | 00:47 |
| National Citizens Inquiry homepage | |
| Time Reference: | 01:17 |
| Quotations from WHO Constitution | |
| Time Reference: | 05:19 |
| Zero draft of the WHO CA+ for the consideration of the Intergovernmental Negotiating Body at its fourth meeting | |
| Time Reference: | 10:12 |
| WHO says COVID emergency is over. So what does that mean? | |
| Time Reference: | 13:20 |
| WHO chief declares monkeypox an international emergency after expert panel fails to reach consensus | |
| Time Reference: | 20:55 |
| Newsweek: PHEIC gives WHO widespread powers, up to and including “mobilizing NATO military assets” | |
| Time Reference: | 21:40 |
| Council of Europe: The handling of the H1N1 pandemic: more transparency needed | |
| Time Reference: | 23:01 |
| BMJ: WHO and the pandemic flu “conspiracies” | |
| Time Reference: | 23:04 |
| Proposed Amendments to the International Health Regulations (2005) submitted in accordance with decision WHA75(9) (2022) | |
| Time Reference: | 23:33 |
| Quote on Global Digital Health Certification Network from Implementation of the International Health Regulations (2005) |
|
| Time Reference: | 25:07 |
| CDC page on One Health | |
| Time Reference: | 33:27 |
| Quadripartite Secretariat for One Health | |
| Time Reference: | 35:24 |
| Sovereignty Coalition Press Conference: Get the US out of the W.H.O. | |
| Time Reference: | 40:12 |
| Biosecurity and Politics (Giorgio Agamben) | |
| Time Reference: | 43:15 |
| State of Exception by Giorgio Agamben | |
| Time Reference: | 51:33 |
| Universal Declaration of Human Rights | |
| Time Reference: | 51:59 |
| Lab-grown meat could be 25 times worse for the climate than beef | |
| Time Reference: | 55:21 |
| Shock: Elon Musk’s Grandfather Was Head Of Canada’s Technocracy Movement | |
| Time Reference: | 57:44 |
| Exploring Biodigital Convergence – Policy Horizons Canada | |
| Time Reference: | 01:01:04 |
| Denis Rancourt on excess mortality during the scamdemic | |
| Time Reference: | 01:15:40 |
| The Independent Panel: “Pandemic Preparedness” scores vs. death rates | |
| Time Reference: | 01:16:31 |
Pandemic and Panopticon: The Rise of the Biomedical Security State
By Janet Levy | American Thinker | April 20, 2023
The pandemic of 2020 saw the imposition of shocking restrictions. For the first time, healthy people were confined to their homes. Vaccines cleared for emergency use – meaning not rigorously tested – were forced on all citizens. Debate, even by scientists, was censored. Refusal to obey these arbitrary impositions could mean arrest, legal action, or, as Dr. Aaron Kheriaty found out, losing one’s job.
A psychiatry professor in good standing at the University of California at Irvine (UCI), Dr. Kheriaty became persona non grata when he demurred to the mandatory vaccine policy, claiming natural immunity as a Covid-recovered individual. Not caring for scientific debate, the university declared him a “threat to the health and safety of the community,” suspended him without pay, barred him from campus, and eventually fired him.
It did not matter that his psychiatry clerkship was the highest rated clinical course at UCI’s medical school; that he’d been chosen keynote speaker to address incoming medical students; and that when the pandemic broke out, he had risked his life to work long hours at the hospital, often uncompensated, while many colleagues stayed home in safety.
Uncowed, Dr. Kheriaty sued the university. In a more far-reaching action, he authored The New Abnormal: The Rise of the Biomedical Security State, a sober analysis and exposure of the tyranny of pandemic policies and the devastation they wrought. The book traces the roots of state interference in, and control of, the biomedical aspects of citizens’ lives to utilitarian ideas that began with Galton and Darwin, and trickled into eugenics, which he says is falsely viewed as entirely a creation of the Nazis when in fact American states were enforcing sterilization from the 1900s to the 1960s.
The core idea, he says, is this: the freedom of a citizen to make health and life decisions can be annulled by the state for the greater good, especially during emergencies. The questions it raises are: Who makes these decisions and on what basis? Who decides what is the greater good? Who is to be held responsible for errors of judgement? What checks and balances do we have, then, against the dictatorial inclinations of the powerful? Ancillary to the idea, he says, is the dangerous circular logic of the state of exception: those who declare an emergency in which citizens’ rights – including the right to question the declaration – stand suspended will believe that in that instance it is morally and politically justified!
We saw all that playing out during the pandemic. Kheriaty observes that the global elite and other political entities, in unbridled collaboration with intelligence and police powers, promoted the acceptance of biomedical surveillance. None of the extreme measures – lockdown, school closure, mandatory masking, vaccine mandates and passports – were subject to debate. No benchmarks were set to justify the emergency or identify when it would end. In fact, America continues to remain in a state of emergency (until May 11th).
Compliance was achieved through propaganda, policing, and surveillance. Guilt – Don’t Kill Granny – and Mao-style rousing – 15 Days to Stop the Spread – were deployed. Six-foot social distancing and curtailment of gatherings to no more than 10 people were imposed with no explanation of where these magic numbers came from. Human contact was redefined as a source of contagion. Exposure could build natural immunity, but this wasn’t acknowledged, for it would have potentially halved the profits of the $100 billion Covid vaccine industry.
Kheriaty identifies the characteristics of the biosecurity paradigm:
- a hypothetical risk, magnified to worst-case scenario to adduce grounds for maximum behaviorial control;
- systematic imposition of control on the entire citizenry, instead of vulnerable subsets;
- catastrophizing, in order to justify intrusive surveillance and the use of police and military action; and
- a merging of public health and the military-intelligence-industrial complex in developing and implementing tracking and data-mining capabilities.
Surveillance is the backbone of dictatorial regimes, and it was no different during the pandemic. In 2021, evidence emerged that the CIA had used digital surveillance to gather information on Americans sans judicial oversight or congressional approval. There were no safeguards to protect civil liberties. Such scenarios have long been envisioned – as far back as 1999, a possible smallpox outbreak was studied. Exercises such as Dark Winter, Atlantic Storm, Clade X, and Event 201 followed. They simulated imposition of martial law, detention of citizens, control of messaging, censoring dissent, enforcing mandates, and surveillance during public health crises. Recommendations to increase state power and use police or military intervention were subsequently embodied in the 2002 U.S. Public Health Security & Bioterrorism Preparedness & Response Act.
The religion of scientism took hold as Dr. Anthony Fauci, former chief medical advisor to the President, reframed the narrative on Covid, shifting the focus from the virus to viewing humanity as a vector. Fauci and a set of scientists and technocrats with broad powers arrogated to themselves a monopoly on knowledge and expertise. Lacking rational explanation, they used force, defamation of critics, and dubious promises of future outcomes to obtain public conformity to the security and surveillance measures.
The vast influence of Big Pharma over governments, the research establishment, and media, says Kheriaty, cannot be understated. Pfizer and Johnson & Johnson are wealthier than most countries, with vast sums available for lobbying. In 2020, 72 senators and 302 congressional representatives cashed campaign checks from the pharmaceutical industry. Biomedical researchers and medical journal editors receive payments from pharma. In a nine-year-period, two-thirds of all FDA reviewers took positions in the industry they regulated. The National Institute of Health, which owns half of the Moderna vaccine patent, chose to conduct internal testing of the vaccine rather than leave it to independent university-based researchers. Media acquiescence was achieved through $1 billion-worth of vaccine advertisements, paid for in taxpayer dollars!
Kheriaty goes so far as to assert that the lockdown was driven by an economic agenda disguised as public health protocol. It helped Big Pharma, multinationals, and the global elite who control them achieve the largest transfer of wealth in history by eliminating competition and spelling doom for small business.
The ultimate plan, devised by the global elite, is for a new world order, shifting government authority from sovereign states to powerful NGOs like the World Economic Forum (WEF), the International Monetary Fund (IMF), and the World Health Organization (WHO). Plans are afoot for a WHO-driven international pandemic treaty tied to a digital ID system, while IMF is promoting central bank digital currency (CBDC), which will allow complete tracking of monetary transactions. WEF chairman Klaus Schwab nurses transhumanist dreams, saying “we will not change what we do” but “who we are,” through gene- and bio-engineering.
The concluding chapter suggests ways of avoiding totalitarian emergencies and the abyss of the biomedical security state. He suggests strict limits on the declaration and control of emergencies, incorporating more checks and balances if necessary. He calls for substantive institutional reform that will eliminate the revolving door between Big Pharma and federal agencies. Besides, he says, the NIH monopoly must be broken, perhaps by distributing research grants to 50 state institutes of health that will focus on issues of local concern. Other ideas include provision of accurate, comprehensive information to allow people to give informed consent; allowing doctors to prescribe off-label or repurposed drugs and provide individualized care; holding Big Pharma accountable by bringing back product liability.
Freedom is at stake, as we discovered during the pandemic. Dr. Kheriaty lost his job, without a chance to defend himself, for daring to dissent. This – or much worse – can happen to any of us if we allow America to become the biomedical security state the global elite want to transform the world into.
WHO Member Says Agency Needs To “Nullify The Conspiracies” About Covid Vaccines
By Tom Parker | Reclaim The Net | June 13, 2023
In 2020, as people challenged the “expert guidance” on Covid during the first few months of the pandemic, the use of the term “misinformation” in news articles almost doubled. This rapid increase in the use of the term by legacy media outlets was followed by an equally rapid rollout of new Big Tech misinformation rules which targeted content that questioned the Covid guidance being pushed by authorities.
Fast forward to 2023 and the first signs of this censorship pattern are starting to play out again.
The WHO, an unelected global health agency, is less than a year away from finalizing an international pandemic treaty/accord and amendments to the International Health Regulations (2005). These two instruments will collectively give the World Health Organization vast new powers to target misinformation and increase its surveillance powers.
And as this WHO power grab faces mounting criticism and pushback, several representatives of this unelected global health agency decided to use the recent seventy-sixth World Health Assembly (WHA) (the annual meeting of the WHO’s decision-making body) to claim that dissent is misinformation and call for more action against dissenting voices.
During a WHA committee meeting, the WHO representative for the Bahamas said “dissenting voices can clutter the airwaves and derail the public health good with disinformation and misinformation.” She added that “more is needed to nullify the conspiracies.”
Professor Peter Piot, a former Director of the London School of Hygiene & Tropical Medicine and a Handa Professor of Global Health, urged the WHO to do more to combat so-called “fake news” during the opening of the seventy-sixth WHA. Specifically, he said the declining trust in science, technology, and the actions of public health groups is “very damaging for health of the people” and called for the WHO to “invest with the same energy as those who are spreading the fake news and are undermining all these efforts.”
And during the closing of the seventy-sixth WHA, the WHO’s Director-General, Dr. Tedros Adhanom Ghebreyesus, said:
“We must work hard to counter the mis and dis-information about the accord that’s circulating in many member states. We cannot mince words. The idea that this accord will cede authority to WHO is simply fake news.
This is an accord by member states, for member states, and will be implemented in member states in accordance with their own laws.”
Although the pandemic treaty won’t “cede authority to WHO,” it does recognize “the central role of WHO, as the directing and coordinating authority on international health work, in pandemic prevention, preparedness, response and recovery of health systems.”
While these WHO members are railing against what they deem to be misinformation, the WHO itself is infamous for pushing misleading information during the early stages of the Covid pandemic. In a January 2020 tweet, the global health agency amplified a claim from Chinese authorities that there was “no clear evidence of human-to-human transmission” of the coronavirus.
Despite repeating these misleading claims from China, the WHO has gained major power over online speech since 2020 via partnerships with YouTube, Facebook, and Wikipedia. On YouTube alone, over 800,000 videos were deleted for contradicting the WHO. Many of the deleted videos shared perspectives that health officials have now admitted to be true. And Google recently renewed its partnership with the WHO.
But the WHO doesn’t appear to be satisfied with the increased influence it has gained in just a few short years and hopes that the pandemic treaty and amendments to the International Health Regulations (IHR) will give it more powers to target speech.
If these instruments are finalized, WHO member states will be instructed to “tackle false, misleading, misinformation or disinformation, including through promotion of international cooperation” and combat “infodemic[s]” (infodemic is a WHO buzzword that describes “too much information including false or misleading information in digital and physical environments during a disease outbreak”).
The WHO hopes to finalize both instruments by May 2024 and both will be legally binding under international law. The instruments have the full support of the US, Canada, and France.
The COVID-19 Pass is Dead, Long Live the Global Digital Health Certification Network
It was never going away
NAKED EMPEROR | JUNE 6, 2023
You didn’t really think the Covid Pass had disappeared did you? Knowing my readers, I’m guessing you didn’t.
Yesterday, it was announced that the World Health Organization (WHO) has entered into an agreement with the European Union (EU) to use their digital COVID-19 certification system. This will be in order to establish a global system to “help facilitate global mobility and protect citizens across the world from on-going and future health threats, including pandemics”.
Going by the last few years, “global mobility” most likely means restricting the mobility of the unvaccinated and “protecting citizens” means only allowing vaccinated passengers to travel together.
The WHO says this is just the first building block in their Global Digital Health Certification Network (GDHCN). WHO Director-General, Dr. Tedros Adhanom Ghebreyesus wants to offer all WHO Member States access to this digital health tool, which is based on “the principles of equity, innovation, transparency and data protection and privacy”.
Equity is an immediate red flag word, whilst transparency probably means telling everyone whether you are vaccinated or not.
Since the EU Covid Pass was launched it has issued more than 2.3 billion certificates. The certificates don’t only cover vaccination but also include tests and recovery. The EU claim it facilitated safe travel for citizens and supported Europe’s hard-hit tourism industry. It says that the passes allowed the coordinated lifting of restrictions from the moment it was possible.
The EU Digital COVID Certificate Regulation was set to expire at the end of June but never one to let a good crisis go to waste, the WHO has jumped in and will takeover the system this month. It then aims to progressively develop the system in the coming months.
Some might think that this will only be used for more regular vaccines. Think again. One of the first things the WHO will do with the new system is to converge digital COVID-19 certificates. This will mean all certificates will meet EU standards, validating digital signatures to prevent fraud.
The WHO says it won’t have any access to underlying personal data but national governments will.
Commenting on the latest news, Christine Anderson MEP said “During COVID, we have all been made into “potential threats” whose individual freedoms and rights must be curtailed to “protect society”!
Rob Roos MEP said “The #Coronapas is a discriminatory instrument that has only created a false sense of safety.”
and George Orwell said “Bloody hell, guys. It’s worse than I thought”.
Dear World – Writers Write
This was never going away was it. The amount of money spent on it was one thing but the temptation to retain such a huge piece of bio-control over the population was another.
We wondered why the unvaccinated ICD-10 codes had been implemented. Another conspiracy theory come true.
WHO Initiative Would ‘Promote Desired Behaviors’ by Surveilling Social Media
By Michael Nevradakis, Ph.D. | The Defender | May 30, 2023
The World Health Organization (WHO) is proposing a set of recommendations for “social listening surveillance systems” designed to address what it describes as a “health threat” posed by online “misinformation.”
The WHO’s Preparedness and Resilience for Emerging Threats (PRET) initiative claims “misinformation” has resulted in an “infodemic” that poses a threat — even in instances where the information is “accurate.”
PRET has raised eyebrows, at a time when the WHO’s member states are engaged in negotiations on two controversial instruments: the “pandemic treaty” and amendments to the International Health Regulations (IHR).
The latest draft of the pandemic treaty contains language on how WHO member states would commit to “social listening.” Under article 18(b), WHO member states would commit to:
“Conduct regular community outreach, social listening, and periodic analysis and consultations with civil society organization and media outlets to identify the prevalence and profiles of misinformation, which contribute to design communications and messaging strategies for the public to counteract misinformation, disinformation and false news, thereby strengthening public trust and promoting adherence to public health and social measures.”
Remarking on PRET’s “social listening” proposals, Michael Rectenwald, Ph.D., author of “Google Archipelago: The Digital Gulag and the Simulation of Freedom” and a former New York University liberal studies professor, told The Defender :
“The WHO’s PRET initiative is part of the UN’s attempt to institute global ‘medical’ tyranny using surveillance, ‘social listening’ and censorship. PRET is the technocratic arm of the WHO’s proposed pandemic treaty, which, if accepted by nation-states, would amount to the surrendering of national and individual sovereignty to this ‘global governance’ body.
“What better way to establish a one-world government than by using so-called global crises that must be addressed by nothing short of ‘global governance’? I remind readers that you cannot comply your way out of tyranny.”
WHO could use artificial intelligence to monitor social media conversations
A WHO document outlining the PRET initiative — “Module 1: Planning for respiratory pathogen pandemics, Version 1.0” — contains a definition of infodemic:
“Infodemic is the overabundance of information — accurate or not — which makes it difficult for individuals to adopt behaviors that will protect their health and the health of their families and communities.
“The infodemic can directly impact health, hamper the implementation of public health countermeasures and undermine trust and social cohesiveness.”
The document recommends that in response to the “infodemic,” countries should “incorporate the latest tools and approaches for shared learning and collective action established during the COVID-19 pandemic.”
According to the WHO document, this can be done if governments “establish and invest in resources for social listening surveillance systems and capacities to identify concerns as well as rumors and misinformation.”
Such resources include “new tools and approaches for social listening … using new technologies such as artificial intelligence to listen to population concerns on social media.”
According to the document:
“To build trust, it’s important to be responsive to needs and concerns, to relay timely information, and to train leaders and HCWs [healthcare workers] in risk communications principles and encourage their application.”
Risk communications “should be tailored to the community of interest, focusing on and prioritizing vulnerable groups,” the WHO said.
“Tailored” communication was a hallmark of public health efforts during the COVID-19 pandemic.
For instance, in November 2021, the Rockefeller Foundation, the National Science Foundation and the Social Science Research Council launched the Mercury Project, which aimed “to increase uptake of COVID-19 vaccines and other recommended public health measures by countering mis- and disinformation” — in part by studying “differential impacts across socio-demographic groups.”
Similarly, PRET states that it will “incorporate the latest tools and approaches for shared learning and collective action established during the COVID-19 pandemic.”
These “tools and approaches” could be deployed during “acute respiratory events,” according to the document, which recommends that governments:
“Develop and implement communication and behavior change strategies based on infodemic insights, and test them during acute respiratory events including seasonal influenza.
“This includes implementing infodemic management across sectors, and having a coordinated approach with other actors, including academia, civil society, and international agencies.”
This is not the first time the WHO has addressed the so-called “infodemic.”
A WHO review published Sept. 1, 2022, titled “Infodemics and health misinformation: a systematic review of reviews,” found that “infodemics and misinformation … often negatively impact people’s mental health and increase vaccine hesitancy, and can delay the provision of health care.”
In the review, the WHO concluded that “infodemics” can be addressed by “developing legal policies, creating and promoting awareness campaigns, improving health-related content in mass media and increasing people’s digital and health literacy.”
And a separate, undated WHO document advises the public on how we can “flatten the infodemic curve.”
WHO, Google announce collaboration targeting ‘medical misinformation’
The WHO’s PRET proposals coincided with a new multi-year collaboration agreement with Google for the provision of “credible health-related information to help billions of people around the world respond to emerging and future public health issues.”
The agreement was announced on May 23 by Dr. Karen DeSalvo, Google’s chief health officer, on the company’s blog. She wrote:
“Information is a critical determinant of health. Getting the right information, at the right time can lead to better health outcomes for all. We saw this firsthand with the COVID-19 pandemic when it was difficult for people worldwide to find useful information online.
“We worked with the World Health Organization (WHO) on a range of efforts to help people make informed decisions about their health — from an SOS alert to surfacing locally relevant content about COVID-19 to YouTube policies on medical misinformation.”
One way Google will collaborate with the WHO is through the creation of more “knowledge panels” that will prominently appear in search results for health-related questions on the platform.
“Each day people come to Google Search looking for trustworthy information on various health conditions and symptoms,” DeSalvo wrote. “To help them access trustworthy information our Knowledge Panels cite content from reliable sources covering hundreds of conditions from the common cold to anxiety.”
“Working closely with WHO, we’ll soon expand to cover more conditions such as COPD [chronic obstructive pulmonary disease], hypertension, type 2 diabetes, Mpox, Ebola, depressive disorder, malaria and more,” she added.
Google will make these Knowledge Panels available in several languages, including English, Arabic, Chinese, French, Russian and Spanish.
DeSalvo’s May 23 post also addressed an ongoing collaboration between Google and the WHO, Open Health Stack (OHS), which “help[s] accelerate the digital transformation of health systems around the world” and “lower[s] the barrier to equitable healthcare.”
Google also awarded the WHO with more than $320 million “in donated Google Search advertising via ad grants” allowing the agency “to publish health topics beyond COVID-19, such as Mpox, mental health, flu, Ebola, and natural disasters.”
Google is slated to provide an additional $50 million in ad grants to the WHO this year.
According to Google, the ad grants to the WHO represent the company’s largest such donation to a single organization.
Separately, the U.S. Food and Drug Administration (FDA) tweeted on May 22 about the agency’s own efforts at combating purported “misinformation” and “disinformation.”
The tweet contains a 35-second video, which claims “misinformation” travels “six times faster than the facts,” while promoting the FDA’s “Rumor Control” initiative.
A top priority of FDA Commissioner Dr. Robert Califf, “Rumor Control” was launched in August 2022 and joins other agency initiatives to fight “misinformation” and “disinformation.”
“The growing spread of rumors, misinformation and disinformation about science, medicine, and the FDA, is putting patients and consumers at risk,” according to the FDA’s Rumor Control webpage. “We’re here to provide the facts.”
The initiative asks the public to do “three easy things” to “stop rumors from spreading”: “don’t believe the rumors,” “don’t pass them along” and “get health information from trusted sources like the FDA and our government partners.”
“Rumor Control” appears to have been inspired by an initiative developed by the Virality Project, “a coalition of research entities” from six institutions “focused on supporting real-time information exchange between the research community, public health officials, government agencies, civil society organizations, and social media platforms.”
Documents released as part of the “Twitter files” in March revealed that the Virality Project, based out of the Stanford Internet Observatory, also called for the creation of a disinformation board just one day before Biden announced plans to launch his government-run Disinformation Governance Board.
Similar to PRET’s recommendations to target “accurate” information that nevertheless contradicts establishment public health narratives, the Virality Project worked with Twitter and other social media platforms, recommending they “take action even against ‘stories of true vaccine side effects’ and ‘true posts which could fuel hesitancy.’”
These censorship efforts included at least one tweet by Robert F. Kennedy Jr., chairman on leave of Children’s Health Defense.
Michael Nevradakis, Ph.D., based in Athens, Greece, is a senior reporter for The Defender and part of the rotation of hosts for CHD.TV’s “Good Morning CHD.”
This article was originally published by The Defender — Children’s Health Defense’s News & Views Website under Creative Commons license CC BY-NC-ND 4.0. Please consider subscribing to The Defender or donating to Children’s Health Defense.
The not-so-heroic lockdown critic
By James Delingpole | TCW Defending Freedom | June 2, 2023
Dan Hannan has written another piece reminding us how heroically outspoken he was during lockdown. He writes in the Sunday Telegraph: ‘A handful of columnists – and it really was a handful, you could count us on your fingers – had argued from the beginning that the restrictions were excessive. We were almost universally howled down as murderers who wanted to cull the population . . .’
I’m sure many of us will remain eternally grateful for Lord Hannan’s selfless courage. But rather than resting on his laurels over what he may or may not have written three years ago, might not the noble lord more usefully direct his talents towards addressing the much more pressing problems of the present?
Foremost among these problems, I would suggest, is the looming WHO Pandemic treaty and the proposed amendments to the International Health Regulations (2005). If implemented they would give the World Health Organisation unprecedented powers over sovereign states. These powers would include the right to mandate all manner of highly restrictive measures: lockdowns, masks, quarantines, border closures, travel restrictions, medication of individuals including vaccination and medical examinations.
For full details I recommend the excellent summary by Dr Elizabeth Evans of the UK Medical Freedom Alliance published by TCW under the headline ‘Fight this sinister power grab by the unelected, unaccountable WHO’. What becomes clear if you read the article and follow the links is that the threat posed by the WHO is very real. If its plans are implemented – as currently appears more likely than not – it will represent arguably the most egregious assault on human freedom in the history of the world.
Never before, after all, has an unelected, supranational body been given such power over the lives of pretty much every single person on the planet. The WHO won’t just be able to decide on freedom of movement (whether, for example, it is permissible to keep them under house arrest or in quarantine camps, as happened during lockdown) but even whether or not they live or die or spend the rest of their days as cripples as a result of a compulsory ‘vaccine’ programme.
So let’s read what that doughty freedom fighter Dan Hannan has to say on the subject, shall we? Here he is, further down his hero-of-the-lockdown article: ‘Even more incredibly, some leaders would suggest we set up an international ‘pandemic treaty’, potentially giving the World Health Organisation binding powers on such matters – almost as if they were trying to validate the conspiracy theorists.’
Hmm. I’ve read that sentence a number of times and still I can’t quite make sense of what he is saying. Why is he trying to turn a real problem into a merely theoretical one? Surely, verifiably, unquestionably the case is that the World Health Organisation IS pressing ahead with its treaty, and that sovereign nations around the world will probably sign up to it. Yet instead of acknowledging this fact, Hannan has chosen to dress it up as something highly improbable – ‘incredibly’ – being mooted by certain, unidentified silly politicians or newspaper columnists. Then, as if to pull the rug from under the possibility that this nonsense should ever come to pass, he adds that curious, distancing phrase ‘almost as if they were trying to validate the conspiracy theorists’.
Well, yes, indeed, it would unarguably make ‘conspiracy theorists’ more credible because they have been warning of this threat for quite some time. But would their being proved right really be such a bad thing? In Hannan’s view, it appears, yes it would because – as he hints in a subsequent paragraph – he has a bit of an axe to grind on this score.
‘Two people I know have been pushed by all this into conspiracist paranoia. They went from asking (perfectly reasonably) why young people needed to be jabbed for a disease that posed no danger to them to doubting the efficacy of all vaccines. Then they started muttering about Bill Gates and Klaus Schwab. Now they are parroting the Kremlin line on Ukraine.’
I’m not quite sure what the relevance of Ukraine is to lockdowns. But I think what Hannan is telling us from his lofty perch in the House of Lords is that there is a right way to think about things and a wrong way to think about things – and that he clearly knows which is which, whereas these paranoid conspiracists are so away with the fairies that their every argument can be dismissed.
But are they? Are they really? On the subject of vaccines, for example, there is a perfectly lucid and reasonable case to be made that they are not the medical miracle but a gigantic con trick which has done far more harm than good to the health of the public.
As for the dismissive line about Bill Gates and Klaus Schwab, this is plain dishonest. The Bill and Melinda Gates Foundation is the second-biggest funder of the World Health Organisation after the US. Klaus Schwab wrote and published a book in 2020 called Covid-19: The Great Reset, spelling out how the global pandemic was a beneficial crisis which political leaders groomed by his World Economic Forum could use to make a new world order in which we would own nothing and be happy. Using a dismissive word such as ‘muttering’ doesn’t magically vanish these men away into a paranoid fantasy world where they pose no threat to our real one. Rather, it suggests a writer who is using rhetorical tricksiness to lead his readers away from the truth.
On lockdown, he concludes: ‘It would be comforting to pin the responsibility on someone: autocratic politicians, cowardly bureaucrats, sensational broadcasters. But the horrible truth is that, as a country, we did this to ourselves; and, in all likelihood, we would do it again tomorrow.’
The deception here is worth of Iago. ‘Politicians’ pushed the lockdown and vaccine agenda not because they were ‘autocratic’ but because they were corrupt, spineless and under the thumb of supranational institutions such as the World Economic Forum and the WHO. Bureaucrats pushed it not because they are cowardly but because as Deep State functionaries that was precisely their job. Broadcasters and newspapers like the one Hannan writes for pushed it not out of sensationalism but because they were either bought and paid for – or bullied and cowed – by the government to pump out relentless Covid propaganda while suppressing inconvenient truths such as vaccine injury.
At no point in his piece does Hannan address the fact that the primary driver responsible for all those things he so laments about lockdown Britain (‘taped-off playgrounds’, ‘power-crazed coppers’, ‘listless moody teenagers’) was the military-grade, state-orchestrated propaganda campaign designed to brainwash the public into believing that a fairly routine flu bug was the worst thing since the Black Death. The public would never have overreacted in the way it did if it hadn’t been bullied, cajoled, bribed, blackmailed and tricked into doing so by the political class of which Lord Hannan is a card-carrying member.
Featured Video
Seyed M. Marandi: Negotiations Collapsed – Return to War
or go to
Aletho News Archives – Video-Images
From the Archives
The US-Iran Scenario That Most Scares Israel
By Ali Haydar | Al-Akhbar | October 9, 2013
Israeli Prime Minister Benjamin Netanyahu issued a series of threats toward Iran and its interlocutors in the West, including the US, as serious negotiations on Iran’s nuclear program seem more plausible.
As a possible rapprochement looms between the US and Iran, Netanyahu has attempted to impose impossible Israeli conditions on the negotiators, such as the full dismantling of Iran’s nuclear program, not to mention threatening military force.
Whatever the deal that could materialize between Iran and the West, Israel is going to find itself before an open-ended path. One can foresee three possible scenarios… continue
Blog Roll
 Aletho News
Aletho News- UK, Spain reject Trump’s new scheme to blockade Hormuz Strait
- Russian frigate ‘resurfaces’, chases off NATO pirates days after Kiev ‘sank’ it
- Ukraine Targets Russian Merchant Fleet With NATO Intel Support – Presidential Aide
- Russia’s ‘shadow fleet’ makes mockery of UK naval power
- Ukraine plans to attack Russian ships with Norwegian support
- US’s ‘Very Foolish’ Double Blockade of Hormuz Strait Makes Absolutely No Sense: Here’s Why
- China issues rules on countermeasures against foreign states’ unlawful extraterritorial jurisdiction
- Seyed M. Marandi: Negotiations Collapsed – Return to War
- Tomorrow’s naval blockade showdown
- ‘Israel’ attacks civilians to hide its embarrassing military failures & out of pure sadism
- If Americans Knew
- Critical shortages in Gaza, Lebanon in ruins, “piracy” in Iran – Daily Update
- US-Iran ceasefire negotiations make zero progress – Daily Update
- Pro-Israel ‘Thinktanks’ and Individuals who Influence U.S. Foreign Policy
- Mearsheimer reveals how Israel dictates US policies on Iran, Gaza – video
- After killing 350+, Israel still has a “score to settle” with Lebanon before ceasefire – Daily Update
- Military aid to Israel emerges as the latest political litmus test for Democrats
- The only Palestinian children’s rights organization closes following years-long Israeli campaign against it
- ‘I Can’t Forget the Smell’: Lebanese Reel After Israel Kills Over 300 in Single Day
- DNC Shoots Down Resolutions Calling Out AIPAC and Limiting Arms to Israel
- TCN: Is Israel Blackmailing President Trump?
- No Tricks Zone
- Cave Discovery Reveals Today’s Desert Climates Were Recently Far Warmer, Wetter, Teeming With Life
- German Expert: Heat Dome Led To Record Temps In Western USA…Warmer In 1934, 1936
- New Study: No Linear Warming Or Glacier Retreat Along Northern Antarctic Peninsula Since 1980s
- An Inconvenient Tree: Uncovered In Alps… Europe Much Warmer Than Today 6000 Years Ago
- New Study Reports A 60% Slowdown In Greenland’s Ice Loss Rate In The Last Decade
- Low Intensity Tornado Wrecks Major Solar Farm, Creating A Potential Toxic Dump
- New Study Finds Warming Saves Lives…Cold Temperatures 12 Times More Deadly Than Excess Heat
- German Science Blog Accuses PIK Climate Institute Of Hallucinating Climate Tipping Points
- Devastating Assessment Of Comirnaty Vaccine By Former Senior Pfizer Europe Toxicologist
- New Study: CO2 Is ‘Effectively Negligible’ As An Explanatory Climate Change Factor Since 2000
