The American Cyber Stasi Will Suppress All Digital Dissent In Biden’s Dystopia
By Andrew Korybko | One World | May 7, 2021
The dystopian hellhole that I predicted would become a fait accompli following Joe Biden’s confirmation as President by the Electoral College is quickly becoming a reality after CNN’s recent report that the US’ security services are considering contracting the services of so-called “researchers” as a legal workaround for spying on average Americans. According to the outlet, these ostensibly independent contractors would be charged with infiltrating the social media circles of white supremacists and other supposedly terrorist-inclined domestic forces within the country. The report claims that the intent is to “help provide a broad picture of who was perpetuating the ‘narratives’ of concern”, after which “the FBI could theoretically use that pool of information to focus on specific individuals if there is enough evidence of a potential crime to legally do so”.
In other words, the US’ security services essentially want to establish a “Cyber Stasi” of “fellow” citizens who spy on one another and produce purported “evidence” of “potential crimes” for “justifying” the FBI’s “legal” investigations. CNN quoted an unnamed senior intelligence official who asked, “What do you do about ideology that’s leading to violence? Do you have to wait until it leads to violence?”, thereby hinting that this initiative might likely be exploited to stop so-called “pre-crime”, or crimes before they occur. Put another way, even those average Americans who practice their constitutionally enshrined right to the freedom of speech to peacefully dissent against the Democrats’ consolidation of their de facto one-party rule of the country might find themselves targeted by the security services depending on how the contracted “researchers” spin their words.
It should be remembered that even Americans’ constitutionally enshrined right to the freedom of assembly is nowadays under scrutiny depending on the stated reason behind their planned peaceful protests if they dare to propose gathering in opposition to last year’s alleged voter fraud for example. The events of 6 January were exploited as a game-changer by the security services in order to restrict Americans’ freedoms. It’s neither here nor there whether one sincerely believes that the election was stolen since the purpose in pointing these double standards out is to prove that average Americans are being politically discriminated against with the implied threat of legal intimidation when it comes to exercising their constitutional rights about “politically incorrect” issues of concern to them.
Although the reported purpose of the “Cyber Stasi” is to preemptively thwart emerging domestic terrorist plots, it can’t be discounted that the combination of political Russophobia and “mission creep” will combine to create additional objectives such as stopping the spread of so-called “Russian disinformation” throughout society. That phrase is actually just a euphemism for “politically incorrect” facts and interpretations thereof that contradict the Democrats’ official narrative of events, being intentionally vague enough to function as an umbrella under which to cover practically every alternative understanding possible. With this in mind, those average Americans who dare to share something “politically incorrect” – even in private chats amidst the presence of “deep state” infiltrators (“researchers” employed as “Cyber Stasi”) – might be targeted by the FBI.
The end effect is that the US’ security services might succeed in suppressing most expressions of digital dissent in the coming future. They’re inspired to do so by the ruling administration which wants to impose a syncretic system of economic leftism and social fascism onto the country. It’s not “communist” in the sense that the economic vision is more akin to state capitalism than traditional Marxism, but the social impact will certainly mirror that of East Germany during its darkest days of Stasi rule, though that’s precisely why many critics casually describe it as “communist” despite that not being economically correct (at least not yet). The US’ “researcher”-contracted “Cyber Stasi” will have a chilling effect how Americans interact with one another from here on out, all in order for Biden’s dystopian hellhole to avoid the fate of its predecessor, East Germany.
COVID-19: Just the Facts

By Will Jones | Lockdown Sceptics | May 9, 2021
Twelve key questions about COVID-19 and lockdowns answered. All answers fully referenced from peer-reviewed research and leading authorities.
How deadly is COVID-19?
Stanford Professor of Medicine and Epidemiology John P. A. Ioannidis in the European Journal of Clinical Investigation has reviewed data from studies globally and estimated that the infection fatality rate (IFR) of COVID-19 is around 0.15%. It varies considerably by region (for reasons such as demographics and prior susceptibility) and between countries within regions. In Europe and the Americas it is around 0.3%-0.4%. In Africa and Asia it is around 0.05%.
It also varies considerably between ages and depending on the presence of underlying conditions. Cambridge Professor of Statistics David Spiegelhalter has used the mortality data from the spring 2020 epidemic in England and Wales to show that the risk of dying from a COVID-19 infection roughly increases by 12-13% for each year older, doubles every 5-6 years and is around 10,000 times higher for the oldest compared to the youngest. It is also roughly equivalent to the normal risk of dying in a given year (though is mostly in addition to that normal risk). Men have around double the risk of death of women of the same age.

The average age of death from Covid in England and Wales in the spring epidemic was 80.4 according to the ONS, splitting 78.7 for men and 82.5 for women. The average age of death in the UK is 79.3 for men and 82.9 for women (though note these are modelled estimates of life expectancy at birth based on life tables, not the actual average age of those who die each year). Public Health England has estimated that life expectancy was reduced by 1.3 years for men and 0.9 years for women in 2020 due to the Covid and lockdown death tolls, though these figures are also modelled.
Economist John Appleby writing in the BMJ has shown that every year prior to 2009 was more deadly than 2020 in England and Wales once the size and age of the population is taken into account. The same analysis also shows that previous pandemics have not resulted in continued elevated death rates for more than a year or two despite not having vaccines for the diseases, indicating how the human immune system and the diseases adapt into a less deadly relationship.

A Swedish review of Covid deaths outside hospitals (i.e., in care homes and private homes) in one county found 85% were from a different underlying cause. In Northern Ireland, 38% of Covid deaths in spring 2020 were determined to be not primarily due to COVID-19. However, the same figure in England and Wales was 8%, suggesting significant differences in how Covid deaths are registered between jurisdictions.
How is COVID-19 spread?
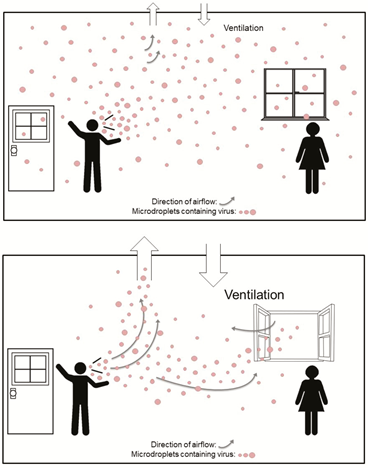
According to the most up-to-date data, COVID-19 primarily spreads via aerosols that build-up in the air of a room rather than via larger droplets or through contact with surfaces (fomites). This is why many of the measures taken to combat the spread of COVID-19, such as distancing, barriers, face masks (see below) and cleaning surfaces are ineffective. Outdoor transmission is very rare.
Public Health England has used data from the Government testing programme to show that the secondary attack rate (proportion of contacts who catch the virus from an infected person) in private homes is around 10.1%. An American study in JAMA found it was 16.6%.
The low secondary attack rate in the high-exposure context of private homes is indicative of high levels of pre-existing immunity to the disease, as discussed in the BMJ by Peter Doshi. Note that immunity is not binary – a person can be resistant on one occasion and not resistant on another, for a variety of reasons. Cross-reactive T-cells that provide a measure of immunity have been found in a number of studies in 20-50% of unexposed people. Exposure without detectable infection (detectable by a PCR test) has also been found to induce a degree of T-cell immunity.
Infection with COVID-19 has been shown in a number of studies, including one on U.S Marines published in the Lancet, to confer natural immunity that gives around 80% protection from re-infection and 90% protection from symptomatic re-infection, with ten times lower viral load (corresponding to infectiousness).
What about asymptomatic and pre-symptomatic transmission?
Asymptomatic infection is typically characterised by a much lower viral load and consequently much lower infectiousness. The study in JAMA on household secondary attack rate (SAR) cited above found that asymptomatic infections had a SAR of just 0.7% versus a SAR of 18% for symptomatic infection. The proportion of infections that are asymptomatic increases among those with immunity from previous infection or vaccination, showing that it is a characteristic of immunity.
People become infectious around two days prior to onset of symptoms as viral load peaks. This pre-symptomatic transmission is estimated to account for around 6.4% of spread, according to a study of actual transmission events from Singapore. Modelled estimates of the contribution of pre-symptomatic spread appear to go too high.
This means that people without symptoms, whether asymptomatic or pre-symptomatic, are not major drivers of the epidemic.
Do lockdowns work?
Restrictions on social contact, such as stay-at-home orders, business closures and gathering limits, have consistently been shown in peer-reviewed studies to have had no significant impact on outcomes such as Covid infections and deaths. Here is a sample, with a key quote from each.
- “Full lockdowns and wide-spread COVID-19 testing were not associated with reductions in the number of critical cases or overall mortality.” “A country level analysis measuring the impact of government actions, country preparedness and socioeconomic factors on COVID-19 mortality and related health outcomes” by Rabail Chaudhry, George Dranitsaris, Talha Mubashir, Justyna Bartoszko, Sheila Riazi. EClinicalMedicine (Lancet) 25 (2020) 100464, July 21st, 2020.
- “We find that shelter-in-place orders had no detectable health benefits, only modest effects on behaviour, and small but adverse effects on the economy.” “Evaluating the effects of shelter-in-place policies during the COVID-19 pandemic” by Christopher R. Berry, Anthony Fowler, Tamara Glazer, Samantha Handel-Meyer, and Alec MacMillen, Proceedings of the National Academy of Science of the USA, April 13th, 2021.
- “Stringency of the measures settled to fight pandemia, including lockdown, did not appear to be linked with death rate.” “Covid-19 Mortality: A Matter of Vulnerability Among Nations Facing Limited Margins of Adaptation” by Quentin De Larochelambert, Andy Marc, Juliana Antero, Eric Le Bourg, and Jean-François Toussaint. Frontiers in Public Health, November 19th, 2020.
- “Comparing weekly mortality in 24 European countries, the findings in this paper suggest that more severe lockdown policies have not been associated with lower mortality. In other words, the lockdowns have not worked as intended.” “Did Lockdown Work? An Economist’s Cross-Country Comparison” by Christian Bjørnskov. CESifo Economic Studies March 29th, 2021.
- “While small benefits cannot be excluded, we do not find significant benefits on case growth of more restrictive NPIs.” “Assessing Mandatory Stay‐at‐Home and Business Closure Effects on the Spread of COVID‐19” by Eran Bendavid, Christopher Oh, Jay Bhattacharya, John P.A. Ioannidis. European Journal of Clinical Investigation, January 5th, 2021.
Studies which conclude otherwise are invariably based on models rather than data.
Professor Simon Woods, a mathematician, has shown that infections were in decline prior to the start of all three lockdowns in England.

You can find a useful round-up of the studies showing lockdowns don’t work at AIER.
Does social distancing work?
Many studies (including some of those above) which conclude that lockdowns don’t work nonetheless add that voluntary social distancing practices do reduce infections or deaths by suppressing spread. However, this is typically stated without supporting evidence. In fact, the evidence on this is also quite weak.
An international comparison study in Nature by R.F. Savaris and colleagues found that actually staying at home (measured by mobile phone mobility data) made no significant difference to outcomes either. “We were not able to explain the variation of deaths per million in different regions in the world by social isolation, herein analysed as differences in staying at home, compared to baseline,” they wrote. “In the restrictive and global comparisons, only 3% and 1.6% of the comparisons were significantly different, respectively.”
The fact that transmission is mainly via aerosols that build-up in the air of a room means that keeping a physical distance from people makes little difference to risk. A study from MIT used a model of viral dynamics to show that physical distancing makes no significant difference to transmission risk in indoor spaces.
Social distancing doesn’t have a significant impact on infections or deaths for a number of reasons.
Firstly, much of the spread, especially which leads to serious infection and death, is nosocomial, i.e., it occurs in care homes and hospitals. According to data from the ONS, 39% of Covid deaths in England and Wales in spring 2020 were care home residents. According to Public Health Scotland, between half and two thirds of serious Covid infections during the winter were picked up in hospital.
Second, not everyone is staying at home, even when they’re unwell. ONS figures show that nearly half of people in the U.K. travelled to work during the January lockdown. A major survey from King’s College London found that less than half of those with symptomatic Covid fully self-isolated during their infectious period.
Because social distancing does not significantly suppress viral spread, there is no reason to expect a large new wave of infections when social distancing practices are eased or ended. This aligns with the experience of states in the U.S. such as Florida, Texas and South Dakota which ended restrictions or never imposed them and did not experience noticeably worse outcomes than states which maintained them.

Are lockdowns harmful?
Lockdowns are extremely harmful to human health and well-being, leading to large reductions in access to healthcare, education and sources of social support, and considerable reductions in economic activity resulting in large-scale losses of earnings and livelihoods.
A U.K. Government report estimated that the first lockdown would kill at least 63,000 people through missed medical care and worsened economic conditions. It argued this loss of life was justified because COVID-19 was predicted to kill directly up to 1.5 million people or around 2.2% of the population. However, this figure is many times higher than the death toll in any country on earth no matter how lax its response. The worst affected country as of May 8th 2021, Hungary, has lost less than 0.3% of its population with COVID-19 according to official data. Sweden, with looser restrictions, has lost less than 0.14%.
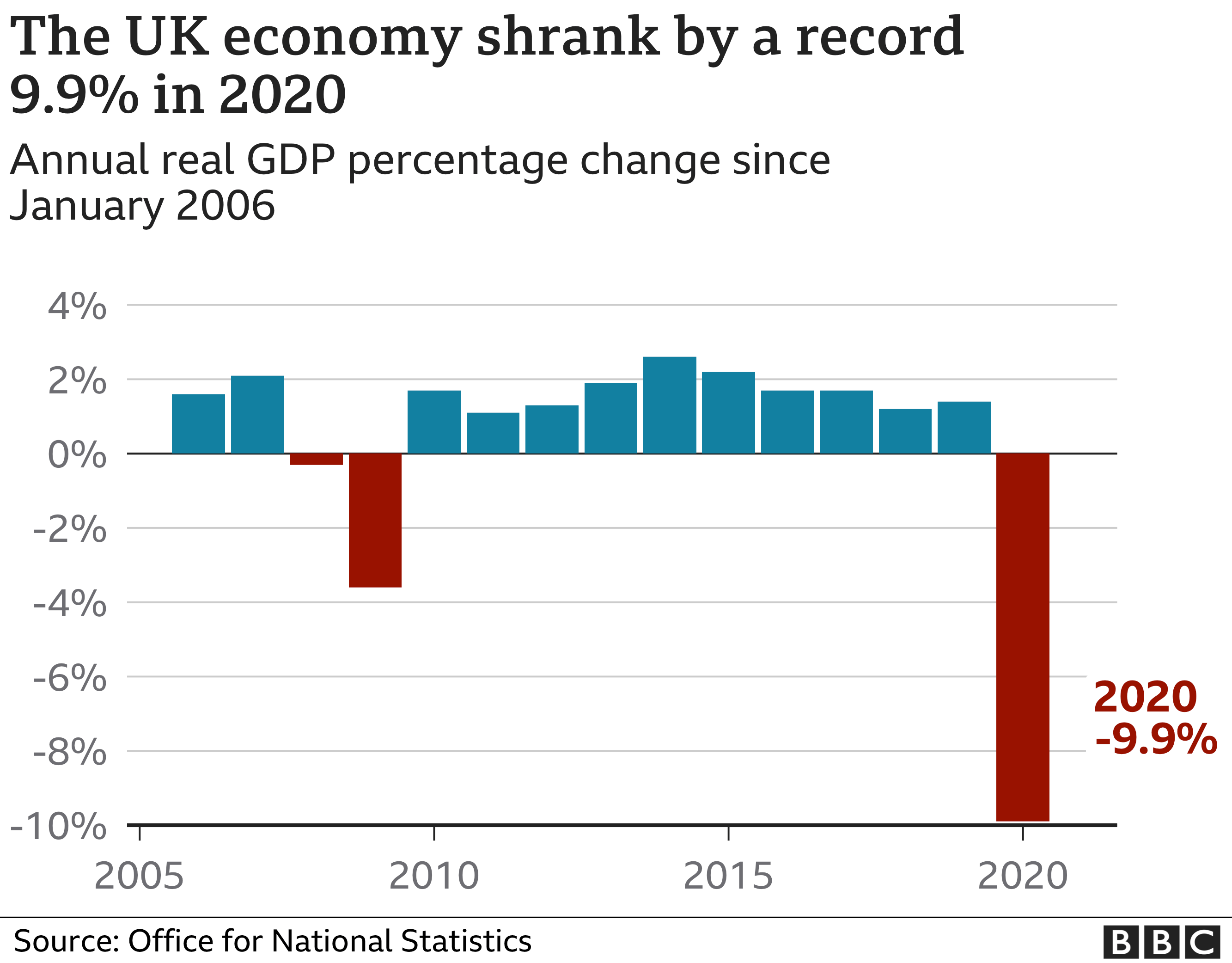
The UK economy shrank by almost 10% in 2020, the largest annual fall on record.
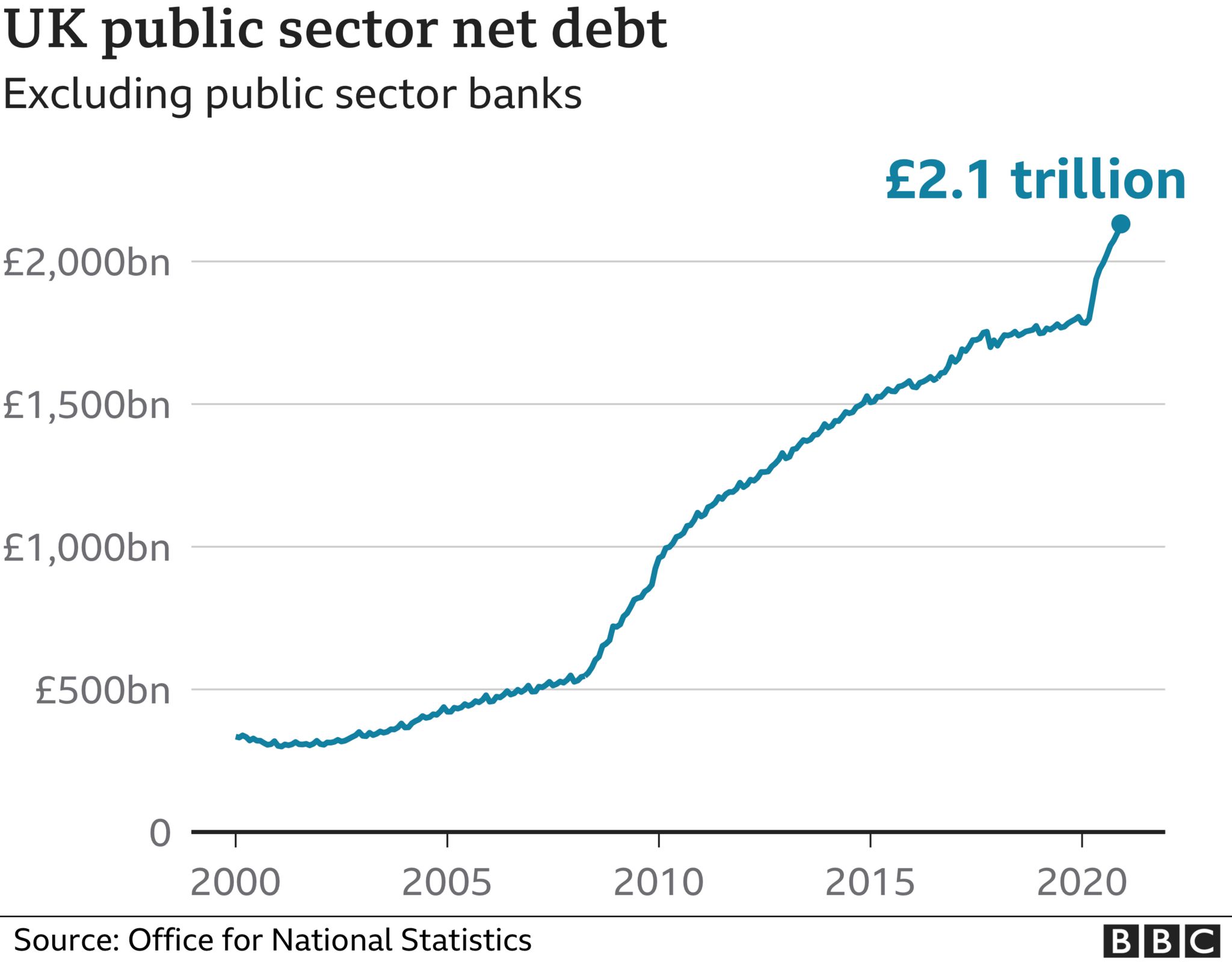
UK national debt has also jumped considerably during the pandemic to £2.1 trillion.
Lockdowns take a toll on mental health. The ONS estimates that the proportion of UK adults experiencing some form of depression is “more than double” what it was before the pandemic, increasing from 10% in 2019 to 21% in 2020.
The United Nations has estimated that disruption in healthcare services caused by government responses to COVID-19 in Afghanistan, Nepal, Bangladesh, India, Pakistan and Sri Lanka (home to some 1.8 billion people) may have led to 239,000 maternal and child deaths. Of these, an estimated 228,000 were children under five, who are at very low risk from the virus.
The United Nations has also estimated that an additional 207 million people could be pushed into extreme poverty over the next decade due to the long term impact of lockdowns.
A website has been created by the signatories of the Great Barrington Declaration to document some of the harms of lockdowns called Collateral Global.
Are the vaccines effective?
The vaccines, particularly the mRNA vaccines such as Pfizer’s, appear to be effective at preventing COVID-19 infection. They succeed in producing antibodies to SARS-CoV-2. They appear to give a level of protection comparable to that provided by infection (80-90%). A Public Health England study suggested they cut transmission rates in half after one dose.
However, among those groups who are most vulnerable to the virus they appear to be significantly less effective. A Danish study in nursing homes found that the Pfizer vaccine (often the best performing vaccine) was reduced to 64% effectiveness at preventing COVID-19 among fully vaccinated care home residents. A German study found a third of those over 80 fully vaccinated with the Pfizer jab did not generate antibodies.
Some coronavirus variants are showing signs of partial escape from vaccine-induced immunity. The AstraZeneca vaccine, for example, was found to be only 21.9% effective against the South African variant. The need for regular boosters tailored to new variants has been suggested.
Are the vaccines safe?
A number of safety concerns have been raised about the vaccines, some of which have led to some of the vaccines being restricted or removed in some countries.
The U.S. vaccine adverse effects reporting system (VAERS) has generated reports of deaths linked with Covid vaccinations at a rate 30 times greater than with flu vaccinations (although the number of deaths associated with flu vaccines is very low). Hundreds of serious adverse reactions have been reported in the UK.
A major study in the UK reported “an abundance of patients admitted to hospital within seven days of vaccination”.
The vaccines involve using genetic instructions to induce the body to produce the virus’s spike protein. However, there are concerns that the spike protein is itself pathogenic. One study reported that: ”The SARS-CoV-2 spike protein (without the rest of the viral components) triggers cell signalling events that may promote pulmonary vascular remodelling and pulmonary arterial hypertension as well as possibly other cardiovascular complications.” The spike protein by itself was shown to harm the lungs of mice.
There is also evidence that a Covid vaccination programme can cause a spike in infections. The association of vaccination programmes and Covid surges in a number of countries has been discussed in the pages of the BMJ. Dr. Clare Craig has argued against it being behaviour based (people letting their guard down) and pointed to the results from the vaccine trials which showed a reduction in white blood cells in the days following the jab that may indicate temporary immune suppression.

The risk-benefit calculation for Covid vaccination has been acknowledged by leading figures including Chief Medical Officer Chris Whitty to be different for those who are at lower risk from the disease, particularly the young. In the U.K., the AstraZeneca vaccine is no longer recommended for those under 40.
Do masks work?
Because transmission of COVID-19 is primarily via aerosols building up in the air of indoor spaces, face masks have little to no impact on risk of infection or transmission. This is because even surgical masks do not filter out enough infected aerosols to be considered respiratory protection devices. In addition, aerosols routinely escape with breath around the sides of the mask.
Accordingly, studies consistently find no significant benefit from wearing masks. The Danmask-19 randomised controlled trial (RCT) found that surgical masks provide no significant protection for the wearer from COVID-19 infection. This is in line with other RCTs for other similar viruses. One, published in autumn 2020, concluded face masks “did not seem to be effective against laboratory-confirmed viral respiratory infections nor against clinical respiratory infection”.
The Government’s scientific advisers admit masks are little use to the wearer, saying they “may provide a small amount of protection to an uninfected wearer; however, this is not their primary intended purpose”. Rather they are “predominantly a source control” (preventing transmission). The advisers cite the findings of a study by Brainard et al, which reviews a number of RCTs and concludes surgical masks provide the wearer with protection from just 6% of infections. The same study’s review of RCTs for masks as source control finds no evidence above low quality.
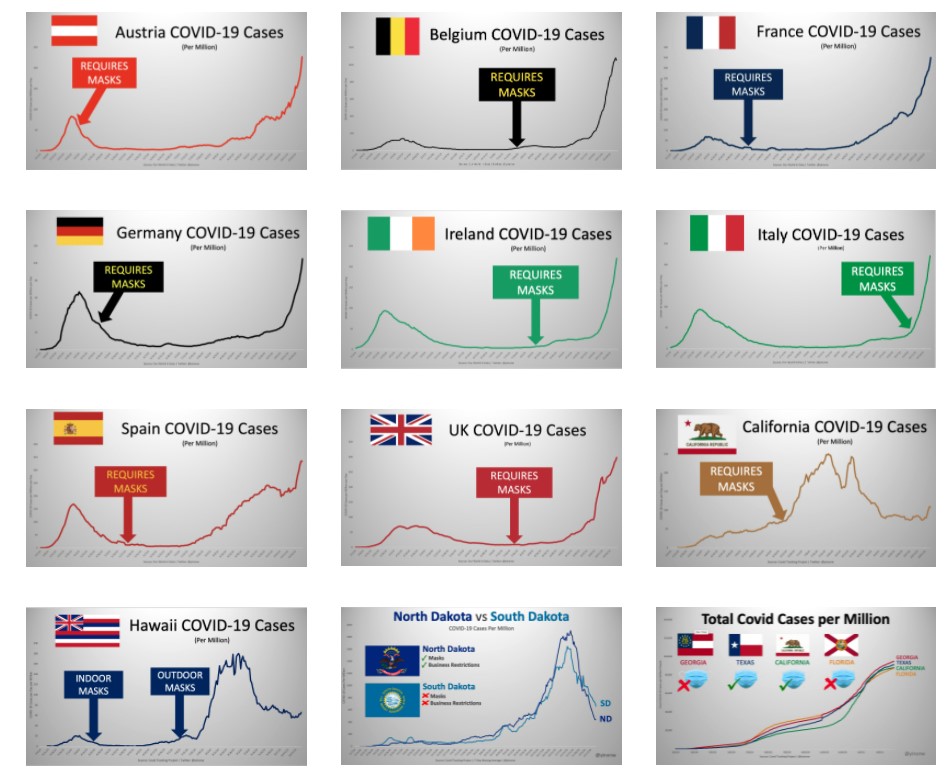
Yinon Weiss has plotted real-world data to show there is no sign of mask mandates altering the course or size of Covid epidemics in countries and states around the world.
Are masks safe?
A number of studies raise concerns about the safety of face masks used daily and for long periods.
A study in Water Research has called for a “full investigation” into the safety of face masks, after detecting easily detached particles of microplastics and heavy metals. “The toxicity of some of the chemicals found and the postulated risks of the rest of the present particles and molecules, raises the question of whether DPFs [disposable plastic face masks] are safe to be used on a daily basis.”

Professor Michael Braungart, head of the Hamburg Environmental Institute, has warned: “Many of them are made of polyester, so you have a microplastic problem. If I have the mask in front of my face, then of course I inhale the microplastic directly and these substances are much more toxic than if you swallow them, as they get directly into the nervous system,”
The World Health Organisation highlights a number of potential harms and risks of prolonged mask use in its guidance, including contamination, skin lesions and headaches.
A study in Clinical Research in Cardiology, “Effects of surgical and FFP2/N95 face masks on cardiopulmonary exercise capacity“, finds significant impact on lung function from wearing a mask during exercise: “The pulmonary function parameters were significantly lower with mask… the ventilation was significantly reduced with both face masks… Peak blood lactate response was reduced with mask. … Participants reported consistent and marked discomfort wearing the masks.”
Face masks have been found to be a transmission risk, with infectious virus remaining on the mask for several days.
There are also important psychological consequences from frequent and widespread mask wearing.
Are effective treatments available?
A number of treatments have been used by clinicians around the world that appear to have some beneficial impact on treating COVID-19. Among the most promising are Ivermectin, as detailed in the American Journal of Therapeutics, and Budesonide, as detailed in the Lancet. The safety profile of these well-established drugs is well-known and not controversial.
What should governments have done?
The UK Government has a Pandemic Preparedness Strategy, drafted in 2011 in line with international ethical norms and scientific evidence. It is primarily for an influenza pandemic, but also envisages a SARS-like pandemic and anticipates up to 315,000 deaths, most in the space of a few weeks. It primarily recommends hand hygiene and self-isolation of the infected. It does not recommend school closures, border closures, business closures, face masks in the community or bans on large gatherings. It aims to encourage “business as usual”, stating:
During a pandemic, the Government will encourage those who are well to carry on with their normal daily lives for as long and as far as that is possible, whilst taking basic precautions to protect themselves from infection and lessen the risk of spreading influenza to others. The UK Government does not plan to close borders, stop mass gatherings or impose controls on public transport during any pandemic. …
Large public gatherings or crowded events where people may be in close proximity are an important indicator of ‘normality’ and may help maintain public morale during a pandemic. The social and economic consequences of advising cancellation or postponement of large gatherings are likely to be considerable for event organisers, contributors and participants.
The Government should have followed this strategy, as it was doing until around March 16th 2020, and not been pressured into deviating from it. It should have recognised that no pandemic has caused elevated mortality for more than a year or two and maintained a sense of proportion.
That said, the strategy is notably silent on the role of hospitals and care homes in spreading the virus (nosocomial spread). It includes no special provisions for protecting care home residents, hospital patients, or any other vulnerable category. It could therefore be improved by considering how focused protection, as advocated in the Great Barrington Declaration, could reduce deaths among the vulnerable. It could also give more consideration to how infected patients could be more effectively isolated from uninfected patients in hospitals.
It should also place more emphasis on quickly finding effective treatments besides vaccines, especially repurposed drugs which are readily available and whose safety profile is known.
Dr Mike Yeadon – “Please warn everyone not to go near top-up vaccines”
THE DAILY EXPOSE • MAY 9, 2021
We spoke to Dr Mike Yeadon about his views on the experimental Covid-19 vaccines, the medicine regulators approving them and his fears for the future.
From the outset, Dr. Yeadon said “I’m well aware of the global crimes against humanity being perpetrated against a large proportion of the worlds population.
“I feel great fear, but I’m not deterred from giving expert testimony to multiple groups of able lawyers like Rocco Galati in Canada and Reiner Fuellmich in Germany.
“I have absolutely no doubt that we are in the presence of evil (not a determination I’ve ever made before in a 40-year research career) and dangerous products.
“In the U.K., it’s abundantly clear that the authorities are bent on a course which will result in administering ‘vaccines’ to as many of the population as they can. This is madness, because even if these agents were legitimate, protection is needed only by those at notably elevated risk of death from the virus. In those people, there might even be an argument that the risks are worth bearing. And there definitely are risks which are what I call ‘mechanistic’: inbuilt in the way they work.
“But all the other people, those in good health and younger than 60 years, perhaps a little older, they don’t perish from the virus. In this large group, it’s wholly unethical to administer something novel and for which the potential for unwanted effects after a few months is completely uncharacterized.
“In no other era would it be wise to do what is stated as the intention.
“Since I know this with certainty, and I know those driving it know this too, we have to enquire: What is their motive?
“While I don’t know, I have strong theoretical answers, only one of which relates to money and that motive doesn’t work, because the same quantum can be arrived at by doubling the unit cost and giving the agent to half as many people. Dilemma solved. So it’s something else. Appreciating that, by entire population, it is also intended that minor children and eventually babies are to be included in the net, and that’s what I interpret to be an evil act.
“There is no medical rationale for it. Knowing as I do that the design of these ‘vaccines’ results, in the expression in the bodies of recipients, expression of the spike protein, which has adverse biological effects of its own which, in some people, are harmful (initiating blood coagulation and activating the immune ‘complement system’), I’m determined to point out that those not at risk from this virus should not be exposed to the risk of unwanted effects from these agents.”
The Israel Supreme Court decision last week cancelling COVID flight restrictions said: “In the future, any new restrictions on travel into or out of Israel need, in legal terms, a comprehensive, factual, data-based foundation.”
In a talk you gave four months ago, you said –
“The most likely duration of immunity to a respiratory virus like SARS CoV-2 is multiple years. Why do I say that? We actually have the data for a virus that swept through parts of the world seventeen years ago called SARS, and remember SARS CoV-2 is 80% similar to SARS, so I think that’s the best comparison that anyone can provide.
“The evidence is clear: These very clever cellular immunologists studied all the people they could get hold of who had survived SARS 17 years ago. They took a blood sample, and they tested whether they responded or not to the original SARS and they all did; they all had perfectly normal, robust T cell memory. They were actually also protected against SARS CoV-2, because they’re so similar; it’s cross immunity.
“So, I would say the best data that exists is that immunity should be robust for at least 17 years. I think it’s entirely possible that it is lifelong. The style of the responses of these people’s T cells were the same as if you’ve been vaccinated and then you come back years later to see if that immunity has been retained. So I think the evidence is really strong that the duration of immunity will be multiple years, and possibly lifelong.”
In other words, previous exposure to SARS – that is, a variant similar to SARS CoV-2 – bestowed SARS CoV-2 immunity.
The Israel government cites new variants to justify lockdowns, flight closures, restrictions, and Green Passport issuance. Given the Supreme Court verdict, do you think it may be possible to preempt future government measures with accurate information about variants, immunity, herd immunity, etc. that could be provided to the lawyers who will be challenging those future measures?
Yeadon: “What I outlined in relation to immunity to SARS is precisely what we’re seeing with SARS-CoV-2.The study is from one of the best labs in their field.” So, theoretically, people could test their T-cell immunity by measuring the responses of cells in a small sample of their blood. There are such tests, they are not “high throughput” and they are likely to cost a few hundred USD each on scale. But not thousands. The test I’m aware of is not yet commercially available, but research only in U.K.
“However, I expect the company could be induced to provide test kits “for research” on scale, subject to an agreement. If you were to arrange to test a few thousand non vaccinated Israelis, it may be a double edged sword. Based on other countries experiences, 30-50% of people had prior immunity & additionally around 25% have been infected & are now immune.
“Personally, I wouldn’t want to deal with the authorities on their own terms: that you’re suspected as a source of infection until proven otherwise. You shouldn’t need to be proving you’re not a health risk to others. Those without symptoms are never a health threat to others. And in any case, once those who are concerned about the virus are vaccinated, there is just no argument for anyone else needing to be vaccinated.”
My understanding of a “leaky vaccine” is that it only lessens symptoms in the vaccinated, but does not stop transmission; it therefore allows the spread of what then becomes a more deadly virus.
For example, in China they deliberately use leaky Avian Flu vaccines to quickly cull flocks of chicken, because the unvaccinated die within three days. In Marek’s Disease, from which they needed to save all the chickens, the only solution was to vaccinate 100% of the flock, because all unvaccinated were at high risk of death. So how a leaky vax is utilized is intention-driven, that is, it is possible that the intent can be to cause great harm to the unvaccinated.
Stronger strains usually would not propagate through a population because they kill the host too rapidly, but if the vaccinated experience only less-serious disease, then they spread these strains to the unvaccinated who contract serious disease and die.
Do you agree with this assessment? Furthermore, do you agree that if the unvaccinated become the susceptible ones, the only way forward is HCQ prophylaxis for those who haven’t already had COVID-19?
Would the Zelenko Protocol work against these stronger strains if this is the case? And if many already have the aforementioned previous “17-year SARS immunity”, would that then not protect from any super-variant?
“I think the Gerrt Vanden Bossche story is highly suspect. There is no evidence at all that vaccination is leading or will lead to ‘dangerous variants’. I am worried that it’s some kind of trick.
“As a general rule, variants form very often, routinely, and tend to become less dangerous & more infectious over time, as it comes into equilibrium with its human host. Variants generally don’t become more dangerous.
“No variant differs from the original sequence by more than 0.3%. In other words, all variants are at least 99.7% identical to the Wuhan sequence.
“It’s a fiction, and an evil one at that, that variants are likely to “escape immunity.”
“Not only is it intrinsically unlikely – because this degree of similarity of variants means zero chance that an immune person (whether from natural infection or from vaccination) will be made ill by a variant – but it’s empirically supported by high-quality research.
“The research I refer to shows that people recovering from infection or who have been vaccinated ALL have a wide range of immune cells which recognize ALL the variants.
“This paper shows WHY the extensive molecular recognition by the immune system makes the tiny changes in variants irrelevant.
“I cannot say strongly enough: The stories around variants and need for top up vaccines are FALSE. I am concerned there is a very malign reason behind all this. It is certainly not backed by the best ways to look at immunity. The claims always lack substance when examined, and utilize various tricks, like manipulating conditions for testing the effectiveness of antibodies. Antibodies are probably rather unimportant in host protection against this virus. There have been a few ‘natural experiments’, people who unfortunately cannot make antibodies, yet are able quite successfully to repel this virus. They definitely are better off with antibodies than without. I mention these rare patients because they show that antibodies are not essential to host immunity, so some contrived test in a lab of antibodies and engineered variant viruses do NOT justify need for top up vaccines.
“The only people who might remain vulnerable and need prophylaxis or treatment are those who are elderly and/or ill and do not wish to receive a vaccine (as is their right).
“The good news is that there are multiple choices available: hydroxychloroquine, ivermectin, budesonide (inhaled steroid used in asthmatics), and of course oral Vitamin D, zinc, azithromycin etc. These reduce the severity to such an extent that this virus did not need to become a public health crisis.”
Do you feel the MHRA does a good job regulating ‘big pharma’? In what ways does ‘big pharma’ get around the regulator? Do you feel they did so for the mRNA jab?
“Until recently, I had high regard for global medicines regulators. When I was in Pfizer, and later CEO of a biotech I founded (Ziarco, later acquired by Novartis), we interacted respectfully with FDA, EMA, and the MHRA.
Always good quality interactions.
“Recently, I noticed that the Bill & Melinda Gates Foundation (BMGF) had made a grant to the Medicines and Healthcare products Regulatory Agency (MHRA)! Can that ever be appropriate? They’re funded by public money. They should never accept money from a private body.
“So here is an example where the U.K. regulator has a conflict of interest.” The European Medicines Agency failed to require certain things as disclosed in the ‘hack’ of their files while reviewing the Pfizer vaccine.
“You can find examples on Reiner Fuellmich’s “Corona Committee” online.
“So I no longer believe the regulators are capable of protecting us. ‘Approval’ is therefore meaningless.
“Dr. Wolfgang Wodarg and I petitioned the EMA Dec 1, 2020 on the genetic vaccines. They ignored us.
“Recently, we wrote privately to them, warning of blood clots, they ignored us. When we went public with our letter, we were completely censored. Days later, more than ten countries paused use of a vaccine citing blood clots.
“I think the big money of pharma plus cash from BMGF creates the environment where saying no just isn’t an option for the regulator.
“I must return to the issue of ‘top up vaccines’ (booster shots) and it is this whole narrative which I fear will he exploited and used to gain unparalleled power over us.
“PLEASE warn every person not to go near top up vaccines. There is absolutely no need to them. As there’s no need for them, yet they’re being made in pharma, and regulators have stood aside (no safety testing), I can only deduce they will be used for nefarious purposes.
“For example, if someone wished to harm or kill a significant proportion of the worlds population over the next few years, the systems being put in place right now will enable it.
“It’s my considered view that it is entirely possible that this will be used for massive-scale depopulation.”
Update on ivermectin for covid-19
By Sebastian Rushworth, M.D. | May 9, 2021
Back in January I wrote an article about four randomized controlled trials of ivermectin as a treatment for covid-19 that had at that time released their results to the public. Each of those four trials had promising results, but each was also too small individually to show any meaningful impact on the hard outcomes we really care about, like death. When I meta-analyzed them together however, the results suddenly appeared very impressive. Here’s what that meta-analysis looked like:

It showed a massive 78% reduction in mortality in patients treated with covid-19. Mortality is the hardest of hard end points, which means it’s the hardest for researchers to manipulate and therefore the least open to bias. Either someone’s dead, or they’re alive. End of story.
You would have thought that this strong overall signal of benefit in the midst of a pandemic would have mobilized the powers that be to arrange multiple large randomized trials to confirm these results as quickly as possible, and that the major medical journals would be falling over each other to be the first to publish these studies.
That hasn’t happened.
Rather the opposite, in fact. South Africa has even gone so far as to ban doctors from using ivermectin on covid-19 patients. And as far as I can tell, most of the discussion about ivermectin in mainstream media (and in the medical press) has centred not around its relative merits, but more around how its proponents are clearly deluded tin foil hat wearing crazies who are using social media to manipulate the masses.
In spite of this, trial results have continued to appear. That means we should now be able to conclude with even greater certainty whether or not ivermectin is effective against covid-19. Since there are so many of these trials popping up now, I’ve decided to limit the discussion here only to the ones I’ve been able to find that had at least 150 participants, and that compared ivermectin to placebo (although I’ll add even the smaller trials I’ve found in to the updated meta-analysis at the end).
As before, it appears that rich western countries have very little interest in studying ivermectin as a treatment for covid. The three new trials that had at least 150 participants and compared ivermectin with placebo were conducted in Colombia, Iran, and Argentina. We’ll go through each in turn.
The Colombian trial (Lopez-Medina et al.) was published in JAMA (the Journal of the American Medical Association) in March. There is one thing that is rather odd with this study, and that is that the study authors were receiving payments from Sanofi-Pasteur, Glaxo-Smith-Kline, Janssen, Merck, and Gilead while conducting the study. Gilead makes remdesivir. Merck is developing two expensive new drugs to treat covid-19. Janssen, Glaxo-Smith-Kline, and Sanofi-Pasteur are all developers of covid vaccines. In other words, the authors of the study were receiving funding from companies that own drugs that are direct competitors to ivermectin. One might call this a conflict of interest, and wonder whether the goal of the study was to show a lack of benefit. It’s definitely a little bit suspicious.
Anyway, let’s get to what the researchers actually did. This was a double-blind randomized controlled trial that recruited patients with mildly symptomatic covid-19 who had experienced symptom onset less than 7 days earlier. Potential participants were identified through a statewide database of people with positive PCR-tests. By “mildly symptomatic” the researchers meant people who had at least one symptom but who did not require high-flow oxygen at the time of recruitment in to the trial.
Participants in the treatment group received 300 ug/kg body weight of ivermectin every day for five days, while participants in the placebo group received an identical placebo. 300 ug/kg works out to 21 mg for an average 70 kg adult, which is quite high, especially when you consider that the dose was given daily for five days. For an average person, this would work out to a total dose of 105 mg. The other ivermectin trials have mostly given around 12 mg per day for one or two days, for a total dose of 12 to 24 mg (which has been considered enough because ivermectin has a long half-life in the body). Why this study gave such a high dose is unclear. However, it shouldn’t be a problem. Ivermectin is a very safe drug, and studies have been done where people have been given ten times the recommended dose without any noticeable increase in adverse events.
The stated goal of the study was to see if ivermectin resulted in more rapid symptom resolution than placebo. So participants were contacted by telephone every three days after inclusion in the study, up to day 21, and asked about what symptoms they were experiencing.
398 patients were included in the study. The median age of the participants was 37 years, and they were overall very healthy. 79% had no known co-morbidities. This is a shame. It means that this study is yet another one of those many studies that will not be able to show a meaningful effect on hard end points like hospitalization and death. It is a bit strange that studies keep being done on young healthy people who are at virtually zero risk from covid-19, rather than on the multi-morbid elderly, who are the ones we actually need an effective treatment for.
Anyway, let’s get to the results.
In the group treated with ivermectin, the average time from inclusion in the study to becoming completely symptom free was 10 days. In the placebo group that number was 12 days. So, the ivermectin treated patients recovered on average two days faster. However, the difference was not statistically significant, so the result could easily be due to chance. At 21 days after inclusion in the study, 82% had recovered fully in the ivermectin group, as compared to 79% in the placebo group. Again, the small difference was not statistically significant.
In terms of the hard end points that matter more, there were zero deaths in the ivermectin group and there was one death in the placebo group. 2% of participants in the ivermectin group required “escalation of care” (hospitalization if they were outside the hospital at the start of the study, or oxygen therapy if they were in hospital at the start of the study) as compared with 5% in the placebo group. None of these differences was statistically significant. But that doesn’t mean they weren’t real. Like I wrote earlier, the fact that this was a study of healthy young people meant that, even if a meaningful difference does exist in risk of dying of covid, or of ending up in hospital, this study was never going to find it.
So, what can we conclude?
Ivermectin does not meaningfully shorten duration of symptoms in healthy young people. That’s about all we can say from this study. Considering the conflicts of interest of the authors, my guess is that this was the goal of the study all along: Gather together a number of young healthy people that is too small for there to be any chance of a statistically significant benefit, and then get the result you want. The media will sell the result as “study shows ivermectin doesn’t work” (which they dutifully did).
It is interesting that there were signals of benefit for all the parameters the researchers looked at (resolution of symptoms, escalation of care, death), but that the relatively small number and good health status of the participants meant that there was little chance of any of the results reaching statistical significance.
Let’s move on to the next study, which is currently available as a pre-print on Research Square (Niaee et al.). It was randomized, double-blind, and placebo-controlled, and carried out at five different hospitals in Iran. It was funded by an Iranian university.
In order to be included in the trial, participants had to be over the age of 18 and admitted to hospital because of a covid-19 infection (which was defined as symptoms suggestive of covid plus either a CT scan typical of covid infection or a positive PCR test).
150 participants were randomized to either placebo (30 people) or varying doses of ivermectin (120 people). The fact that they chose to make the placebo group so small is a problem, because it makes it very hard to detect any differences even if they do exist, by making the statistical certainty of the results in the placebo group very low.
The participants were on average 56 years old and the average oxygen saturation before initiation of treatment was 89% (normal is more than 95%), so this was a pretty sick group. Unfortunately no information is provided on how far along people were in the disease course when they started receiving ivermectin. It stands to reason that the drug is more likely to work if given ten days after symptom onset than when given twenty days after symptom onset, since death usually happens around day 21. If you, for example, wanted to design a trial to fail, you could start treating people at a time point when there is no time for the drug you’re testing to have a chance work, so it would have been nice to know at what time point treatment started in this trial.
So, what were the results?
20% of the participants in the placebo group died (6 out of 30 people). 3% of the participants in the various ivermectin groups died (4 out of 120 people). That is an 85% reduction in the relative risk of death, which is huge.
So, in spite of the fact that the placebo group was so small, it was still possible to see a big difference in mortality. Admittedly, this is a pre-print (i.e. it hasn’t been peer-reviewed yet), and the absolute numbers of deaths are small, so there is some scope for random chance to have created these results (maybe people in the placebo group were just very unlucky!). However, the study appears to have followed all the steps expected for a high quality trial. It was carried out at multiple different hospitals, it used randomization and a control group that received a placebo, and it was double-blinded. And death is a very hard end point that is not particularly open to bias. So unless the researchers have falsified their data, then this study constitutes reasonably good evidence that ivermectin is highly effective when given to patients hospitalized with covid-19. That’s great, because it would mean that the drug can be given quite late in the disease course and still show benefit.
Let’s move on to the third trial (Chahla et al.), which is currently available as a pre-print on MedRxiv. It was carried out in Argentina, and funded by the Argentinean government. Like the first trial we discussed, this was a study of people with mild disease. It literally boggles my mind that so many researchers choose to study people with mild disease instead of studying those with more severe disease. Especially when you consider that these studies are all so small. A study of people with mild disease needs to be very large to find a statistically significant effect, since most people with covid do well regardless. The risk of false negative results is thus enormous. If you’re going to do a small-ish study, and you want to have a reasonable chance of producing results that reach statistical significance, it would make much more sense to do it on sick hospitalized patients.
The study was randomized, but it wasn’t blinded, and there was no placebo. In other words, the intervention group received ivermectin (24 mg per day), while the control group didn’t receive anything. This is a bad bad thing. It means that any non-hard outcomes produced by the study are really quite worthless, since there is so much scope for the placebo effect and other confounding factors to mess up the results. For hard outcomes, in particular death, it should be less of a problem (although we wouldn’t expect any deaths in such a small study of mostly healthy people with mild disease anyway).
The study included people over the age of 18 with symptoms suggestive of covid-19 and a positive PCR test. The average age of the participants was 40 years, and most had no underlying health issues. A total of 172 people were recruited in to the study.
The researchers chose to look at how quickly people became free of symptoms as their primary endpoint. This is enormously problematic, since the study, as already mentioned, wasn’t blinded and there was no placebo. Any difference between the groups could easily be explained by the placebo effect and by biases towards treatment benefit among the researchers.
Anyway, the study found that 49% in the treatment group were free of symptoms at five to nine days after the beginning of treatment, compared with 81% in the control group. However, the lack of blinding means that this result is worthless. The methodology is just too flawed.
No data is provided on the number of people who died in each group. Since it isn’t reported, I think it’s safe to assume that there were no deaths in either group. Nor is any data provided on the number of hospitalizations in each group.
So, what does this study tell us?
Absolutely nothing at all. What a waste of time and money.
Let’s move on and update our meta-analysis. The reason we need to do a meta-analysis here is that none of the trials of ivermectin is large enough on its own to provide a definitive answer as to whether it is a useful treatment for covid-19 or not. For those who haven’t heard of meta-analyses before, basically what you do is just take the results from all different studies in existence that fulfill your pre-selected criteria, and then put them together, so as a to create a single large “meta”-study. This allows you to produce results that have a much higher level of statistical significance. It is particularly useful in a situation where all the individual trials you have to work with are statistically underpowered (have too few participants), as is the case here.
In this new meta-analysis, I’ve included every double-blind randomized placebo-controlled trial I could find of ivermectin as a treatment for covid. Using only double-blind placebo-controlled trials means that only the highest quality studies are included in this meta-analysis, which minimizes the risk of biases messing up the results as far as possible. In order to be included, a study also had to provide mortality data, since the goal of the meta-analysis is to see if there is any difference in mortality.
I was able to identify seven trials that fulfilled these criteria, with a total of 1,327 participants. Here’s what the meta-analysis shows:

What we see is a 62% reduction in the relative risk of dying among covid patients treated with ivermectin. That would mean that ivermectin prevents roughly three out of five covid deaths. The reduction is statistically significant (p-value 0,004). In other words, the weight of evidence supporting ivermectin continues to pile up. It is now far stronger than the evidence that led to widespred use of remdesivir earlier in the pandemic, and the effect is much larger and more important (remdesivir was only ever shown to marginally decrease length of hospital stay, it was never shown to have any effect on risk of dying).
I understand why pharmaceutical companies don’t like ivermectin. It’s a cheap generic drug. Even Merck, the company that invented ivermectin, is doing it’s best to destroy the drug’s reputation at the moment. This can only be explained by the fact that Merck is currently developing two expensive new covid drugs, and doesn’t want an off-patent drug, which it can no longer make any profit from, competing with them.
The only reason I can think to understand why the broader medical establishment, however, is still so anti-ivermectin is that these studies have all been done outside the rich west. Apparently doctors and scientists outside North America and Western Europe can’t be trusted, unless they’re saying things that are in line with our pre-conceived notions.
Researchers at McMaster university are currently organizing a large trial of ivermectin as a treatment for covid-19, funded by the Bill and Melinda Gates foundation. That trial is expected to enroll over 3,000 people, so it should be definitive. It’s going to be very interesting to see what it shows when the results finally get published.
The Biden Administration Wants to Partner with Criminals to Spy on You
By Thomas Knapp | CounterPunch | May 6, 2021
“The Biden administration,” CNN reports, “is considering using outside firms to track extremist chatter by Americans online.”
Federal law enforcement agencies are legally and constitutionally forbidden to monitor the private activities of citizens without first getting warrants based on probable cause to believe those citizens have committed, or are committing, crimes. The feds can browse public social media posts and so forth, but secretly trawling private groups and hacking encrypted chats is off-limits.
Private companies and nonprofit civic organizations, not being government entities, don’t need warrants or probable cause to access those private discussion areas. The administration’s bright idea is that through partnership with these non-government entities, they can get around legal and constitutional barriers: “WE didn’t collect the information. THEY collected the information, then gave it to us.”
There are several flies in that ointment. Here’s a big one:
It’s entirely understandable that — to use an entirely hypothetical example — someone with the Southern Poverty Law Center might impersonate a fictional white supremacist to get into a private Ku Klux Klan chat room and see what those people are up to.
But the US Department of Justice says it’s illegal (under the Computer Fraud and Abuse Act) to evade terms of service with false identities.
A government partnership with an organization that gathers information in that way is no different than the government partnering with a burglar to find out what you have in your house, without the bother of convincing a judge there’s probable cause to issue a search warrant. It is, quite simply, criminal conspiracy.
As with so many political and social issues arising in the Internet age, we’re coming up against a big question that urgently needs answering:
At what point does “working with” government amount to “being part of” government?
Much of the “private” tech sector makes big money on government contracts. NBC News reports, based on a 2020 Tech Inquiry expose, that Microsoft enjoys thousands of subcontracts with the US Department of Defense and federal law enforcement. Amazon has more than 350 such subcontracts with agencies like ICE and the FBI. Google, more than 250.
What about the “nonprofit” sector? According to the National Council of NonProfits, 31.8% of nonprofit revenues are tied to government grants and contracts.
When these entities do things FOR government, they should be held to the same standards and limits AS government. And those standards and limits should put our freedom and privacy first.
Thomas L. Knapp is director and senior news analyst at the William Lloyd Garrison Center for Libertarian Advocacy Journalism (thegarrisoncenter.org).
Prominent American “Anti-Racist” Jews Are Funding Racist Gangs Attacking Arabs In Israel

By Eric Striker | National Justice | May 8, 2021
American Jews are bankrolling Zionist paramilitary groups that have been assaulting and terrorizing random Arabs on the streets of East Jerusalem.
Two weeks ago, 100s of Israelis chanted “Death To Arabs” as they attacked non-Jewish men, women and children during a demonstration organized by Lehava.
Lehava describes itself as a group militantly opposed to race-mixing and openly calls for the killing and expulsion of Christians and Muslims alike.
According to a recent investigation into the groups funding, a number of wealthy Jews who support pro-Israel and liberal causes in the United States have been funding Lehava’s activities.
Two names that stand out are Adam Milstein, a real estate speculator, and the Falic family, which controls all the duty free shops that operate in US airports.
Milstein’s support for violent extremist Jewish groups is known, yet he retains his seats on the boards of “mainstream” Jewish groups as diverse as the American Israel Public Affairs Committee (AIPAC), which lobbies Washington on behalf of Israeli interests, and the Jewish Funders Network, which supports a number of liberal and “anti-racist” causes, including Roberta Kaplan’s ongoing Charlottesville lawsuit and the Anti-Defamation League.
Milstein’s most egregious hypocrisy is displayed with his Canary Mission project, which blacklists nationalists, Muslims, and leftists that are critical of Zionism or Jewish power in the name of “fighting hate.” Recently Canary Mission put the spotlight on this author, labeling me a “white supremacist journalist” with a profile attached that falsely and dishonestly links me to a supposed conspiracy to kill Jews by giving them COVID.
As for the Falics, their massive investments into illegal Israeli settlements has not impacted their Duty Free America airport business monopoly in the least. During the Trump years, the Falics were able to get high profile US officials such as Mike Pompeo to travel to these criminal operations and help grant them legitimacy.
Jewish organizations such as the Anti-Defamation League have been forced to publicly condemn some of the more overt acts of racial violence unfolding in Israel, but Jonathan Greenblatt does not appear interested in curtailing the cash going to extremist groups in his homeland. The ADL is intimately connected to Milstein, who is a regular ADL donor.
Whatever superficial differences they project to the public, liberal Jews and more virulent Kahanist Jews retain their racial synergy and solidarity against Gentiles, whether its oppressing whites in America or beating and killing Arabs in Israel, they are thick as thieves.
Leaked documents prove UK funded anti-Damascus groups: Assad’s top aide
Press TV – May 9, 2021
A senior aide to Syrian President Bashar al-Assad has accused the United Kingdom of funding anti-Damascus groups to stoke further unrest in the Arab country and said Western states were exerting pressure on Syrian officials to dissent from the government.
Bouthaina Shaaban, Assad’s political and media adviser, made the remarks in a video conference organized by the German Schiller Institute on Saturday, entitled “The Moral Collapse of the Trans-Atlantic World Cries Out for a New Paradigm,” Syria’s official news agency SANA reported.
Shaaban said Syria has been waging a “double-edged” war over the past decade, one on the ground against terrorists wreaking havoc in the country and the other against a Western-backed drive for inciting dissent within government ranks.
“All that happened in Syria of destruction, death, and displacement, were because of Western intelligence institutions which, in cooperation with Turkey, trained thousands of terrorists to achieve a single goal which is destroying Syria,” the presidential aide said, adding that the West was dealing with Syria as if it were still under their colonization, ignoring its deep-rooted history and values.
Shaaban also said leaked British documents revealed that the United Kingdom “officially funded” groups of Syrian dissidents who called themselves “witnesses” to launch street movements and provide news for Western media outlets.
Assad’s political and media adviser told the video conference that, “Western governments were pressing Syrian officials to dissent and bribing some of them with money to join those against the Syrian government, assuring them the political system is going to fall and collapse.”
Syrian government troops and their allies have managed to retake some 80 percent of the war-ravaged Arab country’s territory from the Takfiri terrorists.
The Syrian army is fighting to drive out the remaining militants, but the presence of US and European forces in addition to Turkish troops has slowed down its advances.
The United States has also imposed crippling sanctions on Damascus. The Syrian government has repeatedly denounced Washington’s unilateral sanctions as “crimes against humanity,” saying the Western sponsors of terrorism must pay the price for their atrocities against the Syrian nation.
USAID was ‘key tool’ for Washington undermining the Venezuelan government, official review reveals
By Kit Klarenberg | RT | May 9, 2021
Allegations that the US government’s leading aid provider is in fact a ‘trojan horse’ for regime change have circulated for years but were always strenuously denied. Now though, Washington appears to have confirmed it in writing.
On April 16, the oversight division of the US Agency for International Development (USAID) quietly published a review of the organization’s activities in Venezuela from January-April 2019. Its seismic findings were almost universally ignored by the mainstream media, although the Grayzone certainly took notice.
During that chaotic period, Juan Guaido declared himself the country’s acting and rightful leader, challenging the legitimacy of elected President Nicolas Maduro, leading to fiery upheaval engulfing the streets of Caracas. In a widely publicized incident on February 23, trucks carrying USAID “humanitarian commodities” from Colombia into Venezuela were stopped at border crossings and set ablaze.
Western news outlets and politicians were quick to blame the arson on government forces, framing the action as a dastardly attempt to prevent vital supplies reaching citizens desperately in need.
However, journalist Max Blumenthal was actually on the ground in Venezuela at the time, and compiled compelling evidence the fires were started by anti-Maduro activists. Two weeks later, the New York Times published video evidence proving this was in fact the case, without acknowledging Blumenthal had already busted the ploy wide open.
The event is specifically referenced in the USAID review, and while the language is highly euphemistic, reading between the lines it appears the aid was never intended to reach Caracas, and the incendiary episode was, in effect, a Washington-directed “false flag” event.
In interviews with investigators, senior USAID staff admitted the agency’s programs are “subject to foreign policy guidance from the National Security Council and State Department,” guidance which may “impact USAID’s ability to adhere to humanitarian principles and mitigate operational risks.”
In other words, no matter what positive ends its distribution of aid may achieve in some areas, the agency is ultimately answerable to the US military and intelligence agencies, while also engaging in activities that are anything but philanthropic at their behest as a result.
The review notes that it was in response to such “directives” – which included “taking actions that deviated from humanitarian principles and heightened security and fiduciary risks” – USAID dispatched those trucks to the Venezuelan border.
The State Department and National Security Council is reported to have specifically approached USAID for the purpose after the US government in January and February 2019 “identified USAID’s humanitarian assistance for Venezuelans as also serving as a key tool to elevate support” for Guaido’s illegitimate “interim government” and “increase pressure on the Maduro regime.”
Though it’s striking to see USAID’s shadowy nature spelled out in an official report intended for public consumption, the agency’s wide-ranging, insidious role in US efforts to reverse Venezuela’s Bolivarian revolution has been clear since 2010. That year, WikiLeaks published a US embassy cable from 2006 that was transmitted from Caracas to US diplomatic missions the world over – including Vatican City.
It noted that in August 2004, the US ambassador outlined his team’s “five point strategy” in Venezuela, which included “penetrating [Hugo] Chavez’ political base,” “dividing Chavismo,” “protecting vital US business,” and “isolating Chavez internationally.” USAID’s Office of Transition Initiatives (OTI), which “provides fast, flexible, short-term assistance targeted at key political transition” – i.e. facilitates regime change – was said to be central to these efforts.
OTI’s activities in Venezuela included supporting over 300 NGOs across the country “with technical assistance, capacity building, connecting them with each other and international movements, and financial support upwards of $15 million.”
Many of the NGOs which included initiatives “dealing with the rights of the handicapped,” and countering “revolutionary ideology” via “civic education” were said to have been specifically launched off the back of OTI funding. Quite some trojan horse, although USAID’s destabilization efforts aren’t always conducted under the bogus banner of democracy and human rights.
For example, in 2014 it was revealed that OTI had established ZunZuneo, a ‘Cuban Twitter’, in order to stir unrest in Havana. It was constructed via a nexus of secret shell companies and financed by foreign banks.
Tens of thousands of Cubans registered accounts on the social network over the course of two years. The plan was to build a receptive audience, then push them toward unseating the government of Raul Castro. Users were entirely unaware it was created by USAID, and that their sensitive personal data was surreptitiously being gathered in service of a prospective future coup.
In response to the scandal, then-White House press secretary Jay Carney said, “USAID is a development agency not an intelligence agency.” Allegations to the contrary have swirled for decades, and quite understandably. From 1962-1974, a core division of the agency was the Office of Public Safety (OPS), which tutored thousands of police officers in 49 countries over the course of its existence, and provided them with weapons and pacification equipment worth millions.
Its director was Byron Engle, a veteran of the Central Intelligence Agency (CIA). The OPS provided cover for its operatives overseas, helped Langley plant staff in the local police forces of countries of interest to Washington, and also worked as a prospective agent talent spotter. In the late 1960s, it became the subject of negative congressional scrutiny due to allegations equipment it provided and personnel it had trained were linked to torture, murder and disappearances across Latin America.
A US Government Accountability Office report on the OPS, published two years after it shuttered, concluded the unit “encouraged or condoned police brutality, taught or encouraged use of terror and torture techniques, and promoted creation of police states” – charges which government officials, perhaps unsurprisingly, denied.
That report also exposed how extensive support was provided to police forces in countries notorious for their brutal treatment of political dissidents today, including Indonesia, the Philippines, Saudi Arabia, Thailand, and Vietnam. Mercifully, no one seems to have been tortured or killed as a result of USAID’s cloak-and-dagger machinations in Venezuela, although the oversight review was far from glowing in its appraisal of the agency’s National Security Council and State Department-directed activities there.
For instance, USAID’s implementers in Colombia “did not assess the risks of fraud or develop risk mitigation strategies with anti-fraud control activities,” meaning untold funds and “humanitarian commodities” may have been pilfered by Guaido and his interim government.
After all, in June 2019, it was revealed the would-be leader’s entourage, including hundreds of defectors from the Venezuelan armed forces, had spent vast sums of aid money on expensive dinners, nightclubs and shopping trips in Bogota, as they awaited the downfall of Maduro. Said to have an appetite for “prostitutes, alcohol and violence,” the hotels they and their families stayed in went unpaid for three months despite Guaido’s promises to bankroll them, prompting their eviction.
Given the effort to remove the legitimate government of Venezuela remains abortive as of May 2021, it’s likely the ramshackle administration-in-exile has racked up an even bigger bill. Who will ultimately pick up that hefty tab is anyone’s guess.
Kit Klarenberg is an investigative journalist exploring the role of intelligence services in shaping politics and perceptions.
Texas Medical Doctors Testify Before State Senate to Oppose Mandatory COVID Shots
By Brian Shilhavy | Health Impact News | May 8, 2021
This past week the Texas Senate Committee on State Affairs took testimony from Texas physicians regarding SB 1669: Stop Forced Vaccination and Vaccine Passports in Texas.
SB 1669 was sponsored by Senator Bob Hall.

You can learn more about this bill at the National Vaccine Information Center’s Advocacy Portal (registration required.)
Here is some of the text provided to the public regarding Senate Bill 1669:
Contact your Texas State Legislators and Demand No Forced Vaccination, No Vaccine Passports, No Exceptions – Support SB 1669
Mandated vaccination in Texas with COVID-19 vaccines will be the reality unless the legislature takes decisive action now. In fact, it has already started happening.
Houston Methodist Hospital has told its 26,000 employees to get vaccinated by June 7th or get fired. Atria Senior Living, which has 16 facilities in Texas, is requiring all employees to receive 2 COVID-19 vaccines by May 1, 2021 as a condition of employment or face termination.
The city of Farmer’s Branch, Texas is requiring COVID-19 vaccination to access the city run facility called The Branch Connection. Forget taking a cruise with Royal Caribbean from Texas unless you’ve been COVID-19 vaccinated. St. Edwards University in Austin became one of the first colleges to mandate COVID-19 vaccines.
This is just the beginning.
Governor Abbott’s Executive Order Prohibiting COVID-19 Vaccine Passports Falls Short at Protection
Texas Governor Greg Abbott has been quoted saying that in Texas, COVID-19 vaccines “are always voluntary and never forced.”
The truth is Executive Order GA 35 falls short at preserving the right of law-abiding Texas citizens to be able to function normally in society without having to show proof of a COVID-19 vaccination.
EO GA 35 only prohibits the government, or public or private entities funded by the government, from requiring documentation of an individual’s COVID-19 vaccination status. This does nothing to prohibit businesses not receiving government funding from banning customers who don’t have a COVID-19 vaccine. Also, this executive order fails to give any protection to employees whose employers are requiring COVID-19 vaccination as a condition of employment.
In addition, the limited protections offered in EO GA 35 will be short lived because the order only applies to “Emergency Use Authorization” (EUA) COVID-19 vaccines. Once a vaccine has received full FDA approval, the EUA designation no longer applies and therefore neither will any protection in this executive order including the ban on forced vaccination by the government. Full FDA approval will be soon. Moderna, the manufacture of one of the 3 available COVID-19 vaccines, is already seeking full FDA approval, and Pfizer, one of the other manufacturers, announced it would seek full approval in the first half of 2021.
Governor Abbott’s executive order also falls short when compared to Florida Governor Ron DeSantis’s executive order banning vaccines passports which additionally prohibits all business from requiring COVID-19 vaccination status or post infection recovery status to gain access to or service from the business, and it applies to all COVID-19 vaccines instead of expiring after full FDA approval is achieved. It also protects personal privacy rights by prohibiting the government from publishing or sharing a person’s COVID-19 vaccination status to third parties.
Texans Need a Law Passed to Protect them From Forced Vaccination and Vaccine Passports (If you want to immediately see what you can do to help pass SB 1669 into law in Texas scroll down to “Action Needed)”
We are grateful to announce that Texas history has been made with the filing of
SB 1669 in the Texas Legislature by Senator Bob Hall.SB 1669 prohibits discrimination or segregation based on vaccination or immune status and prohibits forced vaccination in all areas of your life.
We need your help getting SB 1669 moving as the bill is currently stalled awaiting a hearing in the Senate State Affairs Committee. Legislators need to be educated about the shortcomings in Governor Abbott’s executive order and the vulnerabilities for mandated vaccination in Texas based on current law so they can pass this bill or amend parts of it onto other bills.
This is by far the most comprehensive bill prohibiting mandated vaccination in all areas that could affect your life including government orders, employment, healthcare, education, access to businesses, access to events and venues like sports and concerts, long-term care, nursing homes, insurance, and childcare.
Read more at the National Vaccine Information Center’s Advocacy Portal.
Senator Bob Hall, in his opening statements at the Senate hearing this week stated:
The chief responsibility and Constitutional role of our government is to protect the rights of the individual. Employees can take off their helmets, masks, and uniforms at the end of the work day, but they cannot remove a vaccine.

Dr. Richard Bartlett was the first physician to testify in favor of SB 1669 to Stop Forced Vaccination and Vaccine Passports in Texas.
Dr. Bartlett has over 28 years of medical practice experience and is a veteran primary care and emergency room doctor in West Texas.
Dr. Bartlett is best known since the COVID crisis started as a doctor who has cured many patients using an older, already FDA approved drug, called budesonide, which is an inhaled corticosteroid. (Learn more here.)
During his testimony, Dr. Bartlett explained that there are existing treatments already available to treat COVID patients, making it unnecessary to mandate experimental new “vaccines.”
He pointed to a recent Oxford University study just published that showed 90% success rate in using inhaled budesonide with COVID patients in preventing long-term care or hospitalization.
From the Oxford study:
The STOIC study found that inhaled budesonide given to patients with COVID-19 within seven days of the onset of symptoms also reduced recovery time. Budesonide is a corticosteroid used in the long-term management of asthma and chronic obstructive pulmonary disease (COPD).
Findings from the phase 2 randomised study, which was supported by the NIHR Oxford Biomedical Research Centre (BRC), were published on the medRxiv pre-print server.
The findings from 146 people – of whom half took 800 micrograms of the medication twice a day and half were on usual care – suggests that inhaled budesonide reduced the relative risk of requiring urgent care or hospitalisation by 90% in the 28-day study period. Participants allocated the budesonide inhaler also had a quicker resolution of fever, symptoms and fewer persistent symptoms after 28 days. (Source.)
Dr. Bartlett works in the Emergency Room, and he stated that there are very few patients coming in now with COVID, but “I am now seeing more people come in (to the ER) who are having complications from the COVID shot.”
And Dr. Bartlett points out that these are mostly younger people who were in excellent health before the shot, since Dr. Bartlett works in Lubbock, Texas, which is a college town.

Dr. Ben Edwards of Veritas Medical in Lubbock, Texas, was the next physician to give testimony in favor of SB 1669 to Stop Forced Vaccination and Vaccine Passports in Texas.
Dr. Edwards received his degree from Baylor University, and later graduated from UT-Houston Medical School. He moved to Waco to complete his training at the Waco Family Practice Residency Program where he was Chief Resident. He now operates three clinics in West Texas.
Dr. Edwards stated his concern that “the forced and coerced COVID-19 vaccinations would, in my opinion, be a violation of the Nuremberg Code,” as well as several other international codes on bioethics and human rights.
He cited the fact that the CDC is now reporting 4,178 deaths reported to VAERS, while for the previous 20 years combined there were 4,182 deaths recorded from all vaccines.
He also pointed out that a Harvard Study has previously estimated that only about 1% of all adverse reactions to vaccines are ever reported to VAERS. Two other subsequent studies showed the same thing.
In his own practice, Dr. Edwards stated that he has received “numerous reports within hours of receiving the COVID vaccines that people have suffered strokes, heart attacks, pulmonary embolisms (blood clots), and sudden death.”
Dr. Edwards went on to cite research which shows that those with natural immunity to COVID (they already had it) will see a 2 to 3 fold increase risk of adverse reactions from the COVID shots.
Over half of Texans now have this natural immunity. He stated:
On a personal note, I believe that God gave us an amazingly robust immune system, and I don’t think you can improve on God.

The next physician to testify in favor of SB 1669 to Stop Forced Vaccination and Vaccine Passports in Texas was Dr. Amy Offutt from St. Marble Falls, TX.
Dr. Offutt is trained in Integrative Medicine. She was recently appointed by Governor Greg Abbott to the Pediatric Acute-Onset Neuropsychiatric Syndrome Advisory Council. In addition, she serves on the Board of Directors for ILADS (International Lyme and Associated Diseases Society).
Dr. Offutt is another physician who has been successfully treating COVID patients with existing early treatment protocols.
She testified:
As of last Friday, my practice has treated 579 acutely ill patients as old as 98 years of age, with only ten hospitalizations and one dead.
The man who died presented on the 12th day of illness was a transplant patient and had already been to the ER multiple times before seeking care from us. This was such an unnecessary tragedy.
Dr. Offutt believes that “informed consent is the core to shared decision making in medicine.”

The next physician to testify in favor of SB 1669 to Stop Forced Vaccination and Vaccine Passports in Texas was Dr. Angelina Farella from Webster, TX.
Dr. Farella is a pediatrician with over 25 years experience. She started out her testimony to the Senate Committee by stating:
I am here today to protect our children in Texas. This is a very scary situation that we are in right now.
Dr. Farella stated that as a pediatrician she has given out tens of thousands of vaccines, and that she is not “anti-vaccine,” but:
I am against this COVID vaccine, if we can even call it that (a vaccine.)
What we are doing to our children with this vaccine is actually criminal.
All of these physicians are “frontline physicians” who actually treat patients, but their clinical experiences in treating COVID patients is being censored by the corporate media, and ignored by the government and Big Pharma, in favor mass vaccination instead.
Here is their testimony. This is from our Rumble Channel, and it is also on our Bitchute Channel.
Featured Video

American Aerial Massacres in Germany
or go to
Aletho News Archives – Video-Images
From the Archives
“Democratic Institutions?” – 10 Lessons from history that will destroy your trust in the CIA
By Kit | OffGuardian | July 20, 2018
… At every corner, we are urged to simply believe what we are told. Whether it is about believing Porton Down and MI6 about “novichok”, or believing the White Helmets about Sarin, or believing the FBI about “collusion”, we are presented with no facts, just assertions from authority. Those who question those assertions are deemed “bots” at best or “traitors” at worst.
Well here, fellow traitors, are the Top Ten reasons to question anything and everything the CIA – or any intelligence agency – has ever told you. … Read full article
Blog Roll
 Aletho News
Aletho News- Israeli forces launch fresh ground incursions into Syria’s Quneitra, interrogate locals
- Syria ‘unwilling, unprepared’ to attack Lebanon despite US pressure: Report
- Hezbollah thwarts Israeli advances into Kfar Tebnit-Ali al-Taher
- The final war or final deal: Why the MoU?
- Iran declares victory over US
- Iran reveals full text of war-ending MoU signed with US
- Belarusian children wounded in deadly Ukrainian drone strike
- US, EU authorize production of ‘deep strike’ missiles inside Ukraine
- Trump leverages illegally frozen Palestinian funds to force normalization, halt legal cases against Israel
- Call for Hamas de-proscription
- If Americans Knew
- An error has occurred; the feed is probably down. Try again later.
- No Tricks Zone
- New Study: Chile’s Relative Sea Level Was 3.2 Meters Higher Than Today During The Mid-Holocene
- Beyond The Pitch: Why FIFA’s World Cup Is One Of Humanity’s Best Investments
- Climate Alarmists Now Using Natural Phenomena To Support Their Claims
- New Study: Significant CO2 Fluxes From Non-Volcanic Sources Are Largely Neglected In Carbon Budgets
- Women Climate Scientists Being Harassed, Insulted By Skeptics, Claims Berkeley Earth Researcher
- Germany’s Longterm Spring Climate Data Show “No Climate Trend”
- New Study: Solar Photovoltaic, Wind Power Fail To Meet Annual Energy Demands 62% Of The Time
- Germany’s Die Welt: “Too Much Is Too Much” … Green Energies Are Cannabalizing Each Other!
- Germany’s Ecological Holocaust… Once Fairy Tale Forests Getting Cleared For Wind Turbines
- A Grand Solar Minimum Has Arrived…Global Cooling Of At Least 1°C Is Expected By The 2030s, 2040s
