Should people who have recovered from COVID take a vaccine?
By Marc Girardot | Trial Site News | July 6, 2021
Epidemiology1 , immunology2 and the clinical data3 all say a clear “No!”.
There is no good reason to vaccinate the recovered.
________________________________________________________________________
A British friend, recovered from COVID, decided to get vaccinated despite being naturally immune. This is the email he recently sent me:
“Marc I suffered a mild stroke on Wednesday 8 days after taking the Astrazeneca 2nd dose. Since I am a marathon runner I am a very ‘rare case’. I don’t smoke, have high blood pressure, high cholesterol, family history or come into any of the risk categories for blood clots…
You did warn me against taking the second dose and I wished I’d heeded your advice. I’ve taken a totally unnecessary risk with my life and I bitterly regret doing it.”
Contrary to most, Tony was informed; he had been told about the power of natural immunity, about the long—if not lifelong—duration of immunity, of the risk inherent to any medical procedure (Yes, vaccination is a medical procedure!), as well as of the rising levels of adverse events. He admitted he hadn’t imagined it could happen to him…
Though it is hard to assess precisely the actual severity and breadth of vaccine-related adverse events, it is very clear that vaccination against COVID-19 isn’t as harmless4 as pharmaceutical companies, mainstream media, academia, health authorities and the medical community have been saying. And, in contrast to high risk individuals who are still susceptible, recovered people have no real benefit to balance the additional risks of vaccination.
2021 Adverse Events Reporting
| VAERS US | EUROVIGILANCE EUROPE | YELLOW CARDS UK | |
| Date | 18/06/2021 | 04/06/2021 | 16/06/2021 |
| Fully Vaccinated (Mn) | 148.46 | 137.44 | 30.68 |
| Deaths | 6,136 | 4,572 | 1,356 |
| Incidents | 387,288 | 316,925 | 73,944 |
| Death per 100,000 | 4.1 | 3.3 | 4.4 |
For over a year, mainstream media, health authorities as well as many “experts” have been downplaying the power of the immune system, dismissing natural immunity5 and proclaiming that immunity to COVID-19 was short-lived6. Simultaneously, vaccines have been portrayed as the silver bullet to this crisis, an incidental procedure with no risk whatsoever. The data shows a different picture and many are coming forward7 8, to challenge the official narrative. We will demonstrate that the official narrative is a dangerous fallacy.
The human immune system is one of the most sophisticated achievements of evolution. The survival of our species has depended on it for millenia. Today, we still very much rely on it. For the record, 99% of people infected with SARS-CoV-2 recover without treatment. Only 1% of SARS-CoV-2 patients, who did not receive early home-based treatment, end up hospitalized9. In other words, the immune system overwhelmingly protects. Even vaccines are entirely dependent on the immune system: vaccines essentially teach our immune systems what viral markers to be prepared for, they are not cures per se. Without a functional immune system, there can be no effective vaccine10.
On the waning immunity fallacy
Once recovered, the immune response recedes, notably via a decrease in antibodies. It is not only natural; it is indispensable to restore the body to a normal, balanced state. Just as a permanent state of fever is harmful, a high number of targetless antibodies or T-cells constantly circulating throughout the body could create serious complications, such as autoimmune diseases11. Taking an evolutionary perspective, only those whose antibody and T-cell count waned post-infection survived. So, a decreasing number of antibodies and T-cells is reassuring, even healthy.
Antibody Levels during infection and post infection

Redline= antibodies – Blue-line= Memory B cells | Credit: Nature
But this decrease in T-cells and antibodies doesn’t mean that immunity is lost . It means the immune system has adapted to the new situation, and is now just on sentinel mode: Memory B- and T-cells, circulating in the blood and resident12 in tissues, act as vigilant13 and effective sentinels for decades:
- survivors of the Spanish Flu epidemic were tested for their immunity to the 1918 influenza virus 90 years later –14,15 and still demonstrated immunity;
- people who had recovered from the 2003 SARS infection demonstrated robust T-Cell responses seventeen years later16.
- the wide-spread prevalence of high cross-immunity17,18,19— gained from past common cold infections—further demonstrates the resilience of natural immunity for coronaviruses.
Indeed, all recent studies show that specific anti-SARS-CoV-2 immunity remains effective20,21,22,23, possibly for a lifetime24. Our immune system is a modular platform, it can combine in an infinite number of ways to address a multitude of threats in a variety of contexts. As such it is neutral to the viral threats it faces. In other words, there is absolutely no reason to believe that those recovered from Covid-19 would lose their immunity over the years, or even the decades25 to come.
On the reinfection fallacy
You might have also heard of people becoming reinfected by SARS-CoV-2. Indeed, immunity, natural or vaccine-induced, isn’t the impenetrable shield described by many. Essentially harmless and asymptomatic reinfections do take place. That is, in fact, the very mechanism by which adaptive immunity is triggered.
However, symptomatic reinfections are very rare26,27. Like an army that adapts its response to the size and the progression of its enemy forces, adaptive immunity provides a specific, rapid and resource-optimized response. As such reinfections are mostly asymptomatic28 and recovered patients are protected from severe disease.
In fact, innocuous reinfections can play a positive public health role by acting as continuous immune updates29 for the population. They can help form a seamless and progressive adaptation to emerging variants and strains. And indeed a recent study showed that couples with children were more frequently asymptomatic than couples without, most likely because children act as natural and harmless immunisation vehicles. The most likely reason why high density countries mostly have very low death tolls is that they have asymptomatic reinfections that regularly and widely update the population’s immunity.
On the variant fallacy
As demonstrated by the low numbers of symptomatic reinfections mentioned above, and also by multiple studies31,32, variants have thus far not escaped acquired immunity. Just as Americans can speak and interact seamlessly in England, unhindered by a few word variants33, natural immunity is unhindered by variants, possibly more so than vaccine-induced immunity. There is ample evidence of the sophistication and breadth of the human immune system, and it is clear that a few minor gene changes in the virus cannot evade its arsenal .
Across the world34, multiple studies demonstrate high levels of pre-existing cross-reactive T-cells35 and antibodies to SARS-CoV-2. In other words, many were already largely immune via other coronaviruses. This is the most likely explanation for the unexpectedly high level of asymptomatic infections during the pandemic. More importantly, this demonstrates that even with large genetic differences, prior immunity to related coronaviruses is sufficient to avoid severe COVID-19. Therefore, it is quite evident that variants are of no concern to the recovered population.
On the vaccine better-than-natural-immunity fallacy
You might have heard people stating that vaccines provide better protection than natural immunity. That is an interesting way of bending reality. How can a vaccine be more effective at immunisation than the disease it is trying to mimic?
Theoretically, there are several reasons explaining why natural immunity is better than vaccine-induced immunity:
- Fewer immune targets: mRNA/DNA vaccines present only a fraction of the virus genetic code (5-10%). For example, they don’t utilize the ORF1 highly immunogenic epitopes36. Therefore, the immune system recruits a smaller number of T-cells by tapping into a narrower repertoire and consequently mounts a less effective response37. The logic: Imagine you lose a number of key players for a football tournament, you might still win, but it will be harder.
- Longer immune trigger time: The smaller number of epitope targets also means that the alarm to the immune system will be delayed. This is a key driver of success in the COVID-19 battle. The wider the target repertoire, the faster the encounter between dendritic cells and identifiable antigens.
The logic: Like a party you go to, you can start partying much faster when you have ten friends there than when you have only one. They are just easier to find. - Inappropriate delivery location: The intramuscular delivery of current vaccines unfortunately doesn’t mimic viral penetration and propagation at all. Coronaviruses don’t enter the body via muscles. They do so via the respiratory tract, often infecting cell-to-cell. Contrary to muscle-delivered vaccines, natural immunity places a strong sentinel force of memory resident cells at the portals of entry38 and shuts the body entrance to the virus preemptively. From an evolutionary standpoint, this makes perfect sense.
The logic: it’s much easier to stop an army coming through a narrow gorge than on the beaches of Normandy.
Recent research confirms this logic. One comparative study39 in Israel found the protection from severe disease to be 96·4% for Covid-19 recovered individuals but 94.4% for vaccinated ones, and concluded “Our results question the need to vaccinate previously-infected individuals.” Another reference comparative study40 by a team at New York University highlighted a faster, wider and more impactful humoral and cytotoxic reaction in recovered immunity versus vaccine-induced.
There is ample evidence that vaccinating people recovered from COVID-19 doesn’t bring any benefit. It quite possibly does the opposite, because of the risk of building tolerance to elements of the virus43 translating into reduced immune potency.
On the vaccine innocuity fallacy
Without denigrating the incredible contribution of vaccines to modern medicine and public health, one needs to acknowledge that vaccines are a medical procedure. As such, vaccines should never be considered lightly. They are neither neutral, nor trivial, all the more so when they are injected into billions of people.
By their very nature, vaccines tinker with the sophisticated balance of one’s immune system. That in itself demands respecting rigid safety protocols. Though we have made considerable progress in our understanding of immunology, we are still very far from understanding its intricacies and subtleties, especially when it comes to novel mRNA and DNA technologies. Because of the risk of anaphylactic44 shock, auto-immune diseases, unforeseen interactions, design flaws, deficient quality protocols, over-dosage, and so on, vaccines have traditionally been strictly regulated.
History teaches us to be watchful45 with vaccines, from the botched inactivation of polio vaccines that ended infecting 40,000 kids46 with polio in 1955, to the 1976 swine flu vaccine47 which caused 450 to develop Guillain-Barré syndrome, to the more recent vaccine-induced outbreak of polio in Sudan48. The recent rejection49 by Brazilian health authorities of the Bharat’s Covaxin is a clear reminder of how rigorous and independent our health authorities need to be if vaccines are to promote, not hinder, public health.
Map of Vaccine Symptoms
316,925 reports (date: 06/20/21)

credit: Wouter Aukema – source: CDC
After 6 months of vaccination and a year of research, a number of red flags should be alerting the would-be vaccinated and health authorities:
- Wandering nanoparticles: The lipid nanoparticles, the carriers of the mRNA, were supposed to remain in the muscle, but ended up broadly distributed throughout the body50, notably in the ovaries51, the liver52 and possibly the bone marrow.
- Anaphylactic PEG: A number of concerns had been raised regarding the novel use of PEG adjuvant53. Notably, prior research had raised the risk of cardiac anaphylaxis at second injection54.
- Sensitive locations: ACE-2 receptors susceptible to binding to the spike protein are highly expressed in blood vessel lining cells of highly sensitive areas, such as the brain, the heart, the lungs, the liver and both male and female reproductive systems.
- Toxic circulating spikes: The spike proteins induced by mRNA/DNA vaccines have been shown to be pathogenic55,56,57,58 and highly inflammatory59, notably because of the similarity of a spike sequence to that of Staphylococcal Enterotoxin B60. It has also been found to be directly causing blood clots through platelet activation61,62. One researcher said, “Our findings show that the SARS-CoV-2 spike protein causes lung injury even without the presence of an intact virus”.
- BBB disruption – A recent study highlights the risk of disruption of the blood-brain barrier63, a fundamental filter mechanism to protect the brain64,65. The spike protein has also been found to cross the BBB and create inflammation in the brain,.
- High adverse events: Even though most likely under-reported66, the overall number of serious adverse events versus other traditional vaccines remains very high. The 6,000+ deaths67 seen [in the US] in six months exceed all the vaccine-related deaths in 30 years. This is quite disquieting, and tends to confirm the aforementioned red flags..
- Children more at risk: The Covid-19 vaccines seem to be more harmful to children and teens, notably with a growing number of myocarditis68,69 events. The fact that vaccine doses are not adjusted for body weight is notably a cause for concern given the discovery of circulating nanoparticles and spike toxicity.
These are essentially just the short-term effects of these novel vaccines. There is no long-term clinical data regarding the implications of these vaccines, notably regarding autoreactive antibodies (antibodies that target one’s own body creating autoimmune diseases).
To conclude, we question why anyone healthy and recovered from COVID-19 would want or be advised to take any risk—even the most remote—in getting vaccinated given that:
- those who have recovered from COVID-19 enjoy robust immunity,
- natural immunity duration is decades-long, probably lifelong,
- natural immunity effectiveness is better than vaccine-induced,
- variants are not an immunological concern, presenting no risk of immune escape,
- vaccines are medical interventions which should never be taken lightly, especially when still experimental,
- there is no benefit for COVID-19 recovered and
- COVID-19 vaccines are obviously not as safe as stated initially by the manufacturers.
- The 2021 seasonal peak in Europe started down on January 22 when only 0.13% of the population was fully vaccinated.
- “Comprehensive analysis of T cell immunodominance and immunoprevalence of SARS-CoV-2 epitopes in COVID-19 cases” by Alessandro Sette et al, Cell, February 2021
- “No point vaccinating those who’ve had COVID-19: Findings of Cleveland Clinic study” by Dr. Sanchari Sinha Dutta, June 2021
- “Pfizer-BioNTech vaccine is “likely” responsible for deaths of some elderly patients, Norwegian review finds” by Ingrid Torjesen, British Medical Journal, May 2021
- “Why COVID-19 Vaccines Offer Better Protection Than Infection” by Brian W. Simpson, John Hopkins School Of Public Health Expert Insights, May 2021
- “Study Finds People Have Short-Lived Immunity to Seasonal Coronaviruses” by Dr. Francis Collins, CDC’s Director Blog, September 2020
- “Are Covid Vaccines Riskier Than Advertised? There are concerning trends on blood clots and low platelets, not that the authorities will tell you” by Joseph A. Ladapo and Harvey A. Risch, The Wall Street Journal, June 2021
- “Why we petitioned the FDA to refrain from fully approving any covid-19 vaccine this year” by Peter Doshi et al, The British Medical Journal Opinion, June 2021
- “Phase 3 trial shows REGEN-COV™ (casirivimab with imdevimab) …” show 4.1% of at risk Placebo (non treated) patients are hospitalized, or 1% of the general population
- “Coronavirus vaccines may not work in some people. It’s because of their underlying conditions.” by Ariana E. Cha, The Washington Post, May 2021
- “Determinants and outcomes of accelerated arteriosclerosis: Major impact of circulating antibodies” by Alexandre Loupy, Circulation Research, June 2015
- “Peripheral and lung resident memory T cell responses against SARS-CoV-2” by Meritxell Genescà et al, Nature, May 2021
- “Tissue-Resident Memory T Cells and Fixed Immune Surveillance in Nonlymphoid Organs” by Francis R. Carbone, Journal of Immunology, July 2015
- “Flu survivors still immune after 90 years” by Ed Yong, National Geographic
- “Neutralizing antibodies derived from the B cells of 1918 influenza pandemic survivors” by James E. Crowe Jr., Nature
- “SARS-CoV-2-specific T cell immunity in cases of COVID-19 and SARS, and uninfected controls” by Le Bert et al, Nature, July 2020
- “Targets of T Cell Responses to SARS-CoV-2 Coronavirus in Humans with COVID-19 Disease and Unexposed Individuals” by A.Sette et al, Cell, June 2020
- “A majority of uninfected adults show pre-existing antibody reactivity against SARS-CoV-2” by Pascal M. Lavoie et al, JCI Insight, March 2021
- “Cross-reactive antibody immunity against SARS-CoV-2 in children and adults” by Todd Bradley et al, Nature, May 2021
- “Robust SARS-CoV-2-specific T cell immunity is maintained at 6 months following primary infection” by Paul Moss, Nature Immunology, May 2021
- “Naturally enhanced neutralizing breadth against SARS-CoV-2 one year after infection” by Michel C. Nussenzweig, Nature, June 2021
- “A long-term perspective on immunity to COVID” by ” by A.Radbruch & H-D.Chang
- “SARS-CoV-2 natural antibody response persists up to 12 months in a nationwide study from the Faroe Islands” by Peter Garred et al, 2021
- “SARS-CoV-2 infection induces long-lived bone marrow plasma cells in humans” by Ali H. Ellebedy et al, Nature, May 2021
- “Immunity to the Coronavirus May Last Years, New Data Hint” by Apoorva Mandavilli, New York Times, November 2020
- “Prior SARS-CoV-2 infection is associated with protection against symptomatic reinfection” by Christopher J.A. Duncan, Journal of Infection, December 2020
- “What we know about covid-19 reinfection so far” by Chris Stokel-Walker, British Medical Journal, January 2021
- “Antibody Status and Incidence of SARS-CoV-2 Infection in Health Care Workers” by Thomas G. Ritter, et al, New England Journal of Medicine, December 2020
- “Development of potency, breadth and resilience to viral escape mutations in SARS-CoV-2 neutralizing antibodies” by Paul D. Bieniasz et al, March 2021
- Get article on
- “Comprehensive analysis of T cell immunodominance and immunoprevalence of SARS-CoV-2 epitopes in COVID-19 cases” by A.Tarke et al… – Cell – 16-02-2021
- “Landscape of epitopes targeted by T cells in 852 individuals recovered from COVID-19: Meta-analysis, immunoprevalence, and web platform” by Matthew R. McKay et al, Cell, May 2021
- “How Broad is Covid Immunity?” by M.Yeadon/M.Girardot, Panda, March 2021
- Countries: Canada, Ecuador, Gabon, Germany, India, Singapore, Sweden, UK, USA, Tanzania, Zambia
- “Cross-reactive CD4+ T cells enhance SARS-CoV-2 immune responses upon infection and vaccination” by Claudia Giesecke-Thiel, April 2021
- “Profiling SARS-CoV-2 HLA-I peptidome reveals T cell epitopes from out-of-frame ORFs” by Pardis C. Sabeti, Cell, June 2021
- “The landscape of antibody binding in SARS-CoV-2 infection” by Irene M. Ong et al, PLOS biology, June 2021
- “Adaptive immunity to SARS-CoV-2 and COVID-19” by Alessandro Sette & Shane Crotty, Cell, January 2021 – page 866
- “Protection of previous SARS-CoV-2 infection is similar to that of BNT162b2 vaccine protection: A three-month nationwide experience from Israel” by Amit Hupper et al, April 2021
- “Discrete Immune Response Signature to SARS-CoV-2 mRNA Vaccination Versus Infection” by Sergei Koralov, Cell, May 2021
- “We observe striking expansion of circulating plasmablasts in COVID-19 patients relative to healthy volunteers”
- “In COVID-19 (recovered) patients, we observed an expansion of cytotoxic populations and a dramatically elevated cytotoxic signature in NK cells, CD4 and CD8 T cells, and γδ T cells.”
- “Differential Effects of the Second SARS-CoV-2 mRNA Vaccine Dose on T Cell Immunity in Naïve and COVID-19 Recovered Individuals” by Jordi Ochando et al, Cell, March 2021
- “Suspicions grow that nanoparticles in Pfizer’s COVID-19 vaccine trigger rare allergic reactions” by Jop de Vrieze, Science, December 2020
- “Historical Vaccine Safety Concerns”, CDC
- “The Cutter Incident: How America’s First Polio Vaccine Led to a Growing Vaccine Crisis” by Michael Fitzpatrick, Journal of the Royal Society of Medicine, 2006
- “The Public Health Legacy of the 1976 Swine Flu Outbreak” by Rebecca Kreston, 2013
- “UN says new polio outbreak in Sudan caused by oral vaccine” by Maria Cheng, Associated Press, September 2020
- “Anvisa denies certificate of good practice to Bharat Biotech, which produces Covaxin” by Enzô Machida and Murillo Ferrari, CNN, March 2021
- “Organ bio distribution study undertaken by the Japanese regulator”
- “Potential adverse effects of nanoparticles on the reproductive system”by Shao LQ, DovePress, September 2018
- “Synthetic Lipid Nanoparticles Targeting Steroid Organs” by Bertrand Tavitian, The Journal of Nuclear Medicine, 2013
- “PEGylated liposomes: immunological responses” by Tatsuhiro Ishida et al, Science and Technology of Advanced Materials Vol 20, 20219
- “Pseudo-anaphylaxis to Polyethylene Glycol (PEG)-Coated Liposomes: Roles of Anti-PEG IgM and Complement Activation in a Porcine Model of Human Infusion Reactions” by János Szebeni et al, ACS Nano, 2019
- “Superantigenic character of an insert unique to SARS-CoV-2 spike supported by skewed TCR repertoire in patients with hyperinflammation” by Ivet Bahar et al, PNAS, October 2020
- “SARS-CoV-2 spike protein induces inflammation via TLR2-dependent activation of the NF-κB pathway” by Hasan Zaki et al, March 2021
- “SARS-CoV-2 Spike Protein Impairs Endothelial Function via Downregulation of ACE 2” by John Y-J. Shyy, Circulation Reseacrh, MArch 2021
- “Single intratracheal exposure to SARS-CoV-2 S1 spike protein induces acute lung injury in K18-hACE2 transgenic mice” by Pavel Solopov et al, The FASEB Journal, May 2021
- “SARS-CoV-2 spike protein interacts with and activates TLR4” by Fuping You et al, December 2020
- “Bacterial Toxins—Staphylococcal Enterotoxin” by Bettina C. Fries & Avanish K. Varshney
- “A prothrombotic thrombocytopenic disorder resembling heparin-induced thrombocytopenia following coronavirus-19 vaccination” by Sabine Eichinger et al, The New England Journal of Medicine, April 2020
- “Acquired Thrombotic Thrombocytopenic Purpura: a rare disease associated Acquired with BNT162b2 vaccine” by Dorit Blickstein et al, Journal of Thrombosis and Haemostatis, June 2021
- “The SARS-CoV-2 spike protein alters barrier function in 2D static and 3D microfluidic in-vitro models of the human blood–brain barrier” by Sergio H. Ramirez, Neurobiology of Disease, December 2020
- “The S1 protein of SARS-CoV-2 crosses the blood–brain barrier in mice” by William A. Banks et al, NAture Neuroscience, December 2020
- “Guillain-Barré syndrome following ChAdOx1-S/nCoV-19 vaccine” by Boby Varkey Maramattom et al, June 2021
- “Underreporting of Side Effects to VAERS” by Vincent Iannelli, Vaxopedia, September 2017
- Open VAERS data
- “The C.D.C. is investigating nearly 800 cases of rare heart problems following immunization.” by Apoorva Mandavilli, New York Times, June 11, 2021
- “Israel reports link between rare cases of heart inflammation and COVID-19 vaccination in young men” by Gretchen Vogel & Jennifer Couzin-Frankel, Science, June 2021
French City Fair Drops Covid Measures In Victory For People Power!
By Richie Allen | July 7, 2021
On Friday last, the historic city of Tours in France opened its annual fair. It’s normally a very big deal. This year is even more special as the fair celebrates its centenary. However, organisers and traders were shocked on Friday, when hardly anyone turned up.
Attendees and staff were told that they would need a “sanitary pass” to attend. To get a pass, a visitor or worker needed to show proof of vaccination or take a PCR test at the entrance. Throughout Friday, the fair was a ghost town and only 4 per cent of the staff had shown up.
Panic ensued. Traders, having spent thousands of euros for their pitches started screaming bloody murder. Others started buying and selling products among themselves. It was grim. Punters were walking away in their thousands. No-one wanted anything to do with the PCR tests piled high at the entrances.
At the 11th hour, the city backed down and all restrictions were lifted. The traders had been bombarding the local authority all day with texts and emails, threatening retribution if the sanitary pass wasn’t kicked to the kerb.
The city blinked and the fair was mobbed over the rest of the weekend. The PCR tests are still rotting at the entrances. The people of Tours stood up.
Vive La France! That’s the way it’s done. That’s people power. The French never let you down. Let it be a lesson to the businesses of the UK and Ireland.
We are sick to the back teeth of this scamdemic. We want our lives back. We want to frequent shops, theaters, cafés, cinemas, bars and restaurants again. We’ll fill your tills.
Just remember, whether we have been jabbed or not is none of your business. Same goes for face muzzles. The ball is now firmly in your court. I can’t wait to see you again.
Global Vaccine Passports Have Arrived Courtesy of Google, EU
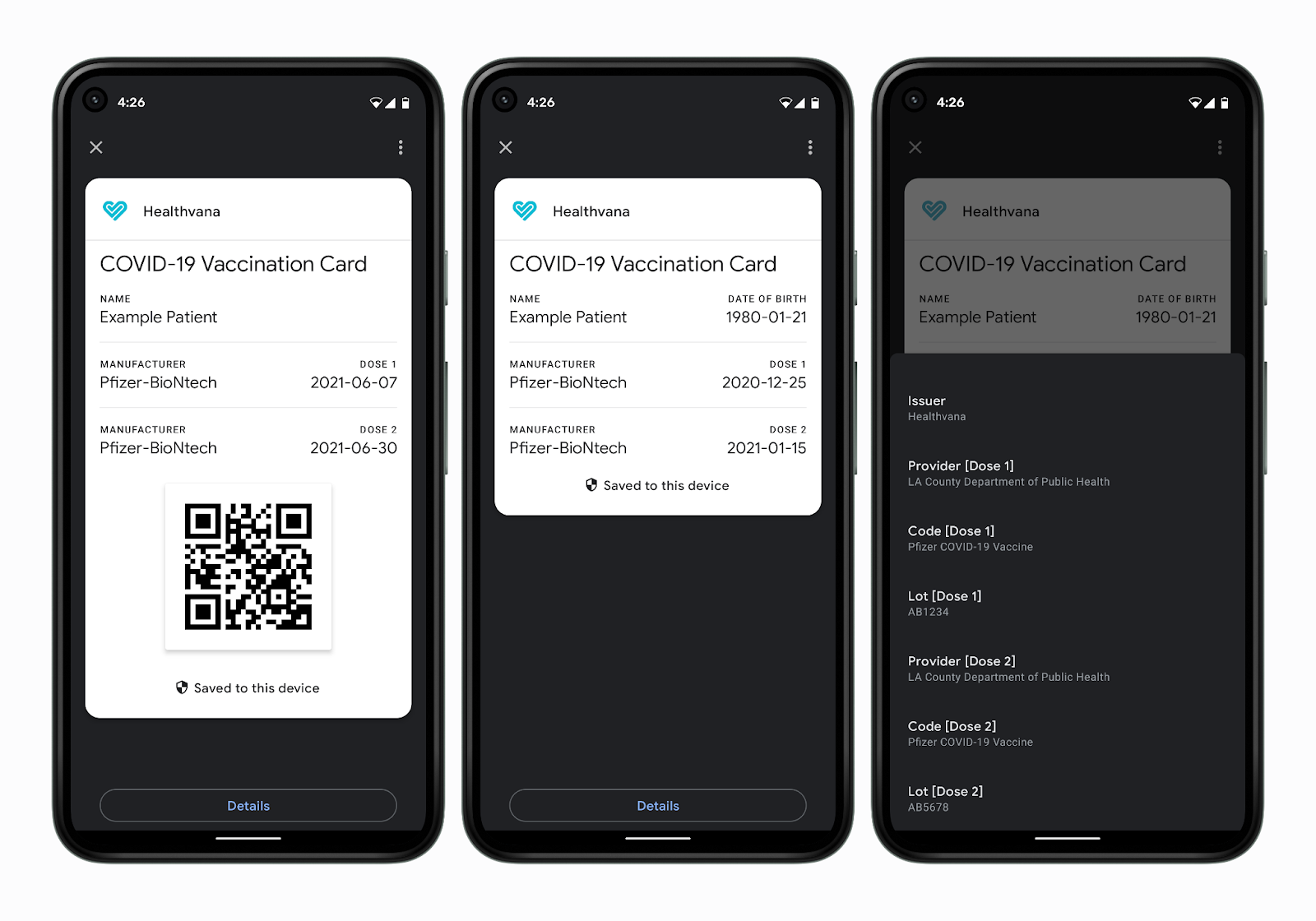
Image Credits: Google
Privacy To Go | July 8, 2021
On June 30th, 2021, the Google Developers blog announced the launch of vaccine passports in Android through its Passes API.
Less than 24 hours later, the European Union, long mired in a sea of national standards for digital jab records, rolled out its EU-wide vaccine passport.
Two completely different vaccine passport schemes unveiled on the same day, encompassing the whole of the Western world? What are the odds!
Exceedingly low, of course. This level of coordination belies yet another blitz in the ongoing rollout of a global, technofeudal control grid. The EU has arguably been at the forefront of this rollout – its standardized digital jab certificate is little more than an aggregator for the draconian technology now operating at the Nation-State level.
Adoption of this unified standard is already approaching 100% of EU Member States. Doublethink rhetoric of restoring the Schengen Area’s “freedom of movement” abounds, even as additional barriers to travel are erected.
In this sense, Google and the US are playing catch-up. While de facto vaccine passports have been implemented sparingly in places like New York, California, and Hawaii, an ever-expanding number of States have banned the notion outright.
Yet herein lies the insidiousness of the public-private partnership model: Technocrats can use governments where it suits them, corporations where it does not, and an increasingly bizarre fusion of the two where necessary. Even the propaganda rollout surrounding jab passports is bifurcated by this model, with the EU using official government bulletins while Google syndicates the news via trendy tech blogs.
And though many States in the US have passed legislation or executive action to curb the implementation of vaccine passports, Google could care less.
Google Passes: Vaccine passports for all, regulation be damned
Like the contact tracing API before it, political resistance alone is proving ineffective against the technological implements of the Great Reset. Even the staunchest State level opponents to this agenda have done nothing to halt the hyperactive Bluetooth surveillance grid running on Android and iOS devices – on the contrary, many have used taxpayer money to help finance its data harvesting operations.
Similar political action against digital vaccine passports will not halt Google’s rollout via the Passes API, either.
In fact, Google’s selection of the Passes API to implement vaccine records is telling in its own right, given the information it already stores: Boarding passes for airlines. Travel tickets. Event tickets.
While legislative action in States like Florida may allow you to attend a Miami Dolphins game with your biological privacy intact, the same may not be said for travel. The battle over Federalization of airline travel was lost on November 19th, 2001 with the creation of the Transportation Security Administration, whose influence has been expanding ever since – the latest privacy affront being the REAL ID Act, which mandates highly insecure RFID technology for interstate air travel.
Even more dangerous are biometric companies with government contracts, like CLEAR, whose terminals are already widely used at TSA PreCheck terminals and event centers.
Google Passes and other digitized jab certificates are simply a competing product. One that is already in the pocket of 85% of Americans alone, with similar adoption levels in Europe.
Products marketed for “convenience” like TSA PreCheck biometrics will, over time, become mandatory – the REAL ID Act itself is a perfect example of this Fabian creep. Passed all the way back in 2005, its full implementation has been pushed back multiple times due to individual State holdouts, most recently until 2023.
But these delays are immaterial – the framework’s existence is all that matters, as despite not being enforced, privacy-violating RFID technologies are now the norm for US driver’s licenses. Jab certificates like Google Passes will be no different. Once in place, they will be utilized – if not immediately, then in the future.
Not only can the Passes API integrate with third-party pharmaceutical companies to track jab history, it is also capable of storing results from dubious PCR tests. This level of biodigital convergence sets an unsettling precedent, as Silicon Valley’s expectation is that your medical history will now be in your pocket at all times, integrated with their servers, and subject to whatever authority may ask for it.
Passes is not an isolated product, either – it’s a development suite within the broader Google Pay SDK.
There are technical reasons why Google may have chosen to use the Pay SDK as opposed to a health-focused API like Google Fit – QR code generation, limited use passes, and encrypted keyrings are already present in the Passes API. However, despite Google Pay’s scant consumer use at present, the long-term intent is crystal clear: Access to financial services and medical records will be intertwined.
In Closing
The post-2020 era has pushed humanity to the precipice of a longstanding dream of our would-be comptrollers. Whether it is Newt Gingrich’s Age of Transitions or the late Zbignew Brzezinski’s Between Two Ages, the kind of biodigital convergence represented by digitized medical passports has been at the forefront of the Technocratic agenda for decades.
As Silicon Valley attempts to bridge the “last mile” of mandated biometric surveillance, resistance to these aims on an individual level remain multivariate – ditch your smartphone, or at least utilize a privacy-respecting alternative that is incompatible with Google or iOS services. Starve the business of travel and entertainment industries that would see us become serfs in exchange for bread and circuses.
If you’re in the EU, use paper records instead of digital equivalents, or better yet, refuse to comply at all.
Educate well-meaning policymakers to the threats represented by the pseudo-private sector and impress upon them that the dangers of State surveillance are rapidly being outpaced by Terms and Conditions mandated by smartphone companies.
Neofeudal Technocracy is desperately trying to extract humanity’s consent to these draconian efforts before the next phase of the so-called Great Reset.
Don’t let them.
US neocons Bolton & PNAC lay down weapons of war for protest signs with their new ‘Turkish Democracy Project’

By Helen Buyniski | RT | July 5, 2021
The aging neocons who have been practicing regime change ops in the Middle East for decades are now launching a project targeting Turkey – perhaps in honor of the deceased Don Rumsfeld.
Erdogan’s Turkey has long been something of a thorn in Washington’s paw, given its ongoing refusal to buy inferior US military equipment (it was booted from the US’ F-35 program for insisting on buying Russian S-400 missiles, making the Americans who still store their nukes at Incirlik somewhat nervous), its refusal to place the good of Israel above its own benefit, and its rumblings of discontent regarding the US’ pleas for support (or at least safe passage) to its Syrian ‘moderate rebel’ militant groups, which Ankara considers to be little more than terrorists.
Under the government of President Recep Tayyip Erdogan, Turkey has become quite recalcitrant indeed, far from the ideal domesticated state keen to babysit American nukes and stage American missiles in exchange for coveted membership in the deteriorating NATO structure (not long ago fetchingly described by French President Emmanuel Macron as “brain dead”). Clearly what it needs is a shot in the bottom from that great big needle marked ‘Democracy’ – and who better to deliver that than the good old boys from the Project for a New American Century, many of them the old same men who led and lied the US, blindfolded, into the chaos of Iraq.
Enter the Turkish Democracy Project, a non-profit organization which – it should be clear from the name – has nothing to do with democracy or, really, Turkishness. The group’s website is about as subtle as a nuclear bomb, blaming President Recep Tayyip Erdogan for “dramatically alter[ing] Turkey’s position in the international community and its status as a free and liberal democracy” and calling for “a nonprofit, non-partisan, international policy organization that opposes its destabilizing behavior, supports genuine democratic reform, and holds the forces of corruption and oppression within Turkey to account.” In other words: “We want a piece of your country. Resist and be annihilated.”
It’s not that the US thinks Turkey is stupid. But they believe, and are likely correct, that the US will never have as good a time as now to strike. With its military still feared by many parts of the world (even though its bark is at this point far worse than its bite, and its image still suitably ferocious to put much of the actual war-fighting business to fleeing instead of fighting), the main business must be – if the US expects to do something other than flee home with its tail between its legs – “shock and awe.”
But given that these shock and awe tactics will be taking place in the Middle East, an area which has seen the worst the US can throw at its enemies over the last 20 years of perpetual warfare and realizes all the money in the world can’t give even the largest military on Earth the stamina of the gods, it’s likely these dyed-in-the-wool bloodshed-artists will have to change with the times. To invade a militarily competent nation like Turkey – especially one which, inconveniently, happens to be backed by NATO – is unlikely to be a walk in the park, no matter how many phony war crimes the PNAC crew manage to cook up. Gas attacks have become cliche, and any talk of “weapons of mass destruction” will elicit a chortle at best.
So the TDS, if recent events are any indication, has instead gotten to work with the kind of color revolution-style events that have largely replaced shock and awe in other regime-change hotspots. They’re cheap, they’re easy, and in this case – a protest in Istanbul against Turkey’s withdrawal from the Istanbul Convention? – they require exactly zero imagination. It’s much easier to con the rest of NATO if you don’t have to make them think.
Thousands of activists took to the streets on Thursday, either on their own or hailing from various NGOs, denouncing Turkey’s withdrawal from the European human rights treaty known as the Istanbul Convention. Erdogan’s executive order removing Turkey from the treaty, first adopted back in March, argued the country’s women are protected by domestic laws rather than the international human rights treaty – which he argued had been “hijacked” by the LGBTQ+ community.
The hoary old PNAC boys behind the TDS likely couldn’t believe their luck when something like this fell into their lap. But will they be able to modernize?
The group’s CEO is Mark Wallace, who’s also the CEO of United Against Nuclear Iran – another unsubtly named regime-change operation (and a regime change that has failed repeatedly). An old hand at overthrowing Middle Eastern nations the old-fashioned way, Wallace held several positions with the George W. Bush administration while the nation was attempting to crush Iraq (apparently shocked the children had run forward with IEDs instead of handfuls of wildflowers to welcome their new rulers).
Indeed, numerous fellow veterans of the Iraq regime change effort and abortive attempts to overthrow Iran have bubbled up in the swamp gas to give regime change in Turkey a go. Wallace is joined by other bottom-feeders like former Connecticut senator Joe Lieberman and UANI intel chief Norman Roule, as well as glorified mustache-carrier, would-be thug, and former Trump national security adviser John Bolton. Former Bush adviser Frances Townsend is there, as is former associate deputy director of operations for the CIA (and Blackwater vet) Robert Richer. At least a few members of the shadowy pro-Israel Foundation for the Defense of Democracies were listed and then memory-holed, and Bush’s brother Jeb is there, a speech bubble forever hovering above his head reading “please clap.”
Oddly enough, however, the only currently listed actual employee aside from CEO Wallace is a (presumably) former assistant English professor at Princeton University. No, that’s not suspicious at all. Carry on, I’m sure Turkey will welcome you (and your desired partitioning of the country) with open arms!
With Erdogan still trustingly paying his country’s NATO dues, Ankara is unlikely to expect any sort of real attack, though the leader is likely on guard, given former President Trump’s on-again, off-again announcement to clear out US soldiers from Syria. He is likely to be on the lookout for foreign meddlers among the protesters, however. And Erdogan’s allies with their ears to the ground both inside and outside Turkey have already pegged this absurd attempt at bringing back ‘democracy’ for what it really is. While some have linked it to the infamous Gulen movement, referring to the cleric who most recently was accused of trying to overthrow Erdogan in 2016, Gulen’s movement itself seems to have ties to the same ‘Greater Israel’ plan to redraw the lines on the map of the Middle East, a plan Israeli military strategist Oded Yinon devised decades ago (and which the neocons appear to have used as their foreign policy guide ever since). Former Turkish opposition lawmaker Aykan Erdemir, senior director for Turkey at the FDD, was accused of being connected to Gulen in 2017 and had his assets seized, strengthening the case for the connection between Gulen’s organization and the notoriously pro-Israel FDD.
But with all of NATO’s heads turned to this human rights drama, surely the other countries in the alliance also participating in the drawing-and-quartering of Syria won’t expect a military attack on Turkey as well – not without some warning. The map of Greater Israel shows Turkey losing a mere corner of their land compared to Syria, which takes quite a beating – one which Turkey clearly expects to be a part of, having already staked its claim effectively to certain border regions of Syria under the logic of keeping the Kurdistan Workers’ Party (PKK) away. But this is all temporary, and eventually the region must settle into its new form. An Israel-first arrangement will not go down well with any of the other combatants, and, unlike the US and its European partners, Turkey won’t just sit on its hands and sigh wistfully while its share of the Syrian pie is handed to the US by way of Tel Aviv.
Because that’s who the ultimate beneficiary of this mess is supposed to be. Named after the Israeli military strategist who devised it, the Yinon project hopes to balkanize the Middle East and assemble the shards into a single nation consisting of the choicest morsels of those countries in between the Euphrates and the Nile rivers. Iraq has already been cut in half, Syria has shrunk dramatically even as the war goes on, and Egypt is run by a pliant leader who will do what the US and Israel tell him – as General Wesley Clark said over a decade ago, the plan was to take out seven countries in five years. They’re running a bit behind, but never underestimate the abilities of a bunch of old war criminals with nothing to lose.
Helen Buyniski is an American journalist and political commentator at RT. Follow her on Telegram.
Stringency Index Is Not Associated With COVID-19 Death Rate Across US States, but IS Associated With Higher Unemployment
By Noah Carl • Lockdown Sceptics • July 5, 2021
Some people oppose lockdown on principle, arguing that the government should never infringe on fundamental liberties like the freedom to leave our home or open our business, regardless of the impact this may have on disease transmission.
It’s a reasonable position, but I’m more drawn to the consequentialist case against lockdowns. This can be summed up as “benefits small, costs large”. In other words, even if lockdowns do reduce mortality from COVID-19 (under some circumstances), they don’t do so by anywhere near enough to justify their costs.
As I noted recently, several cost-benefit analyses of the UK’s lockdowns have been published, and each one concluded that the costs almost certainly outweighed the benefits. (Which may explain why the Government has thus far refrained from publishing any estimates itself.)
A rather elegant demonstration of the consequentialist case against lockdown was provided back in May, in the form of a Twitter thread by the data scientist Youyang Gu.
Comparing the 50 US states, Gu obtained data on the COVID-19 death rate, the change in unemployment rate, and the average Government Stringency Index. The latter is a measure of the number and severity of restrictions imposed during the course of the pandemic (school closures, stay-at-home orders, etc.). Gu’s two main charts are shown below:

He found that the Stringency Index was not associated with the COVID-19 death rate (left-hand chart), but was strongly associated with an increase in unemployment (right-hand chart). In other words, US states with longer and more stringent lockdowns haven’t had fewer COVID-19 deaths, but they have seen higher unemployment.
In the replies to Gu’s thread, some critics argued that restrictions were often imposed in response to large outbreaks, so you can’t assume that causation only goes from restrictions to deaths and unemployment. However, Gu points out that the relative ordering of restriction levels is fairly constant over time, so this is unlikely to be a major issue.
His analysis adds to a large body of evidence indicating that – for the vast majority of Western states – the benefits of lockdown were small, but the costs were very large. Gu’s thread is worth reading in full.
Featured Video
Prof. Ted Postol: Iran Already Achieved Nuclear Deterrence Against Israel
or go to
Aletho News Archives – Video-Images
From the Archives
How the occupied mentality syndrome works
Saudi Arabia on the American chessboard – Part 3
By B. J. Sabri | American Herald Tribune | June 27, 2016
Read part 2: “The occupied mentality Syndrome“
Previously I argued whether Saudi Arabia’s repeated involvements in U.S. interventions and wars stem from free national will or in response to a specific condition. For starters, in Saudi Arabia there is no national will. In Saudi Arabia, the national will is the will of the Al Saud clan. Still, when a major Arab state allies itself with a superpower that committed unspeakable crimes against humanity in almost every Arab country, then something is wrong. This fact alone should compel us to examine the U.S.-Saudi relation for one exceptional reason. As a result of the U.S.-Saudi wars, hundreds of thousands of people in Afghanistan, Iraq, Iran, Libya, Syria, Yemen, and Somalia have lost their lives. Millions became displaced in their own homelands. And millions more rendered refugees.
Attributing the Saudi policies to the bonds of “partnership” with the U.S. is frivolous. There are no bonds between these two thugs except those of business, military deals, secret plots, and wars. Proving this point, bonds such as these have no space for the American and Saudi peoples to share significant cultural or societal exchanges. If partnership is not the reason for the Saudi contribution to the U.S. strategy of empire and imperialism, then another reason must exist.
This leads to three possibilities. … continue
Blog Roll
 Aletho News
Aletho News- NIAID/NIH and USDA Fund Bioengineered Chimeric Influenza Viruses Built Using Pandemic H1N1 Components: Journal ‘Science Advances’
- Hezbollah hits Israeli warship off Lebanon’s coast, sets it aflame
- Iran slams US strikes on B1 bridge, Mahshahr petrochemical plants as ‘blatant acts of state terrorism’
- In letter to UN chief, Araghchi warns of dire consequences of US-Israeli attacks on Iran’s nuclear facilities
- Why the CIA conspiracy to invade Iran with Kurdish militias failed
- Why Are Upbeat US Claims About Mission to Rescue Pilot ‘Highly Questionable’?
- Aircraft destroyed during US ‘rescue’ of downed F-15 pilot cost more than $100 million each
- Washington University removes professor who condemned US-Israeli war on Iran
- Russia Warns of Retaliation as UK Authorizes Seizure of Vessels
- Serbia thwarts plot to bomb Russia-Hungary gas pipeline – Vucic
- If Americans Knew
- In Iran, Israel-US take aim at “reason, research, and freedom of thought” – Daily Update
- US loses planes over Iran, Israel downgrades Lebanon war goals – Daily Update
- Israel Is Blocking Palestinians from Easter at Church Where Jesus Resurrected
- Plot to assassinate Palestinian activist follows harassment campaign promoted by Zionist groups and elected officials
- Prominent New York synagogue hosts presentation on why U.S. Jews should support the ethnic cleansing of Gaza
- Tapper vs. Piker: Is the CNN Anchor Auditioning for David Ellison?
- Shouldn’t Democrats Be Able to Condemn Genocide?
- Israel-US kill negotiators, destroy civilian structures, but Iran’s military capabilities still largely intact – Daily Update
- ‘War crime’: Global condemnation as Israeli ministers celebrate death penalty law targeting Palestinian prisoners
- 7 Ways Israel Is Turning Lebanon Into Gaza
- No Tricks Zone
- An Inconvenient Tree: Uncovered In Alps… Europe Much Warmer Than Today 6000 Years Ago
- New Study Reports A 60% Slowdown In Greenland’s Ice Loss Rate In The Last Decade
- Low Intensity Tornado Wrecks Major Solar Farm, Creating A Potential Toxic Dump
- New Study Finds Warming Saves Lives…Cold Temperatures 12 Times More Deadly Than Excess Heat
- German Science Blog Accuses PIK Climate Institute Of Hallucinating Climate Tipping Points
- Devastating Assessment Of Comirnaty Vaccine By Former Senior Pfizer Europe Toxicologist
- New Study: CO2 Is ‘Effectively Negligible’ As An Explanatory Climate Change Factor Since 2000
- Former Pfizer Toxicologist Dr. Helmut Sterz Tells Bundestag Hearing Pfizer Vaccine Should Have Never Been Approved
- Energy Expert: Germany’s Nuclear Phaseout Was A “500 Billion Euro Mistake”
- New Research: South Australia’s Mid-Holocene Sea Surface Temperatures Were 4°C Warmer Than Today
