Russia to kick out German state media after Berlin bans RT DE
RT | February 3, 2022
The Russian office of the German state broadcaster, Deutsche Welle (DW), is to be closed as part of the “first round” of a response to Berlin’s “unfriendly actions” against RT DE, the Russian Foreign Ministry said in a statement on Thursday.
The German outlet will also be barred from broadcasting in Russia via a satellite or through other means, the statement added. All staff members at DW’s Russian office are to be stripped of their press credentials, according to the foreign ministry.
Moscow has also launched a procedure which will recognize DW as a “foreign media outlet acting as a foreign agent” under Russian law.
Moscow also said it was compiling a list of German state and public entities believe t be linked to blocking RT DE in Germany and exerting pressure on the Moscow-based broadcaster. Representatives included on the list will be barred from entering Russia, the foreign ministry said, adding that it would release information about subsequent rounds of reciprocal measures “in due course”.
DW said it would challenge the decision of the Russian authorities in court and would also continue operating from the Moscow office until it receives a formal closure order. DW’s director, Peter Limbourg, denounced Moscow’s move as “absurd” and an “overreaction.” He also vowed to “significantly increase the coverage” of Russia.
The move comes a day after Germany’s top media regulator sided with a regional authority and upheld a ban on RT DE’s broadcast in Germany, citing the absence of a locally-issued license. The channel previously obtained a valid pan-European permit in Serbia but the German regulators declared that void.
RT DE now has four weeks to appeal the decision in court, which it is planning to do.
Different vaccines reveal different side effects
MHRA should release the raw data for public scrutiny
Health Advisory & Recovery Team | February 1, 2022
The MHRA Yellow Card reporting system is designed to provide a signal of possible problems with new drugs based on reports of suspected adverse reactions from qualified medical practitioners. The data collected could be of much more value if more details were published. The MHRA shares such information with the pharmaceutical industry but, despite its role being to protect the public and relying on public funding, this data is not put into the public domain.
To make the most of what information is available the reports on different vaccine types can be compared. Any side effects that are a result of the production of the spike protein itself may be similar between all vaccine types. However, if one vaccine type has a much higher rate of a particular adverse effect than other vaccine types then this is suggestive of a genuine causal relationship. Confounders such as age may account for part of these differences, which is why publishing the raw data is so important.
Data sharing
The Yellow Card scheme is administered by the MHRA, a government body funded, at least in part, by the public. The data for the scheme is collected largely by NHS staff, who are again funded by the public. However, despite public finance being crucial to the generation of Yellow Card data, the MHRA have refused to release the anonymised individual patient data from this scheme for independent analysis (FOI 21/640). The MHRA argue that release of these data would be too onerous, yet paradoxically these same data are passed on to the vaccine manufacturers for analysis as a matter of routine (FOI 21/942). All that the public can access from Yellow Card is a rudimentary summary of the total numbers of adverse events recorded for each vaccine type in particular medical categories.
The MHRA’s attitude to data sharing stands in stark contrast to the situation in the USA, where the VAERS reporting system [2] provides anonymised individual patient data, and the detailed analyses that this allows has been crucial for recognising important safety signals [3] — albeit US Regulators have been slow off the mark in making full use of the data available to them. We note that the MHRA’s refusal to share the information that they hold within the Yellow Card database would not be tolerated in the general science community where access to raw data is now a prerequisite for publication in peer reviewed journals.
Despite the intransigence of the MHRA over the issue of releasing raw data from the Yellow Card scheme to the general public, it is incumbent upon the scientific community to make the maximum use of the data released from the scheme to scrutinise the validity of the conclusions that the MHRA reach in their weekly reports. This is particularly important to achieve because, despite FOI requests to see the scientific analyses on which their conclusions are based, the MHRA have been unable to produce any such reports (FOI 21/942).
Comparing frequency of reports by vaccine type
The weekly data released from the Yellow Card scheme takes the form of the total number of doses of each of the vaccines given, the total number of reports filed for each vaccine type, and the total number of adverse reactions recorded for each of a huge range of medical conditions compiled separately for each of the vaccine types. What insights can we gain from analysis of this information?
A simple question that we can ask is whether the different vaccines elicit the same or different rates of reporting of adverse reactions or number of reactions per report. The answer is clear (Table 1). There is something about a Moderna injection that generates a higher frequency of adverse event reports with less reactions per report than an Astrazeneca vaccination, which in turn generates a higher frequency of reports and more reactions per report than a Pfizer injection. The figures involved are so huge that these differences cannot be due to chance. There is something important happening that needs to be explained.

Table 1. Percentage of vaccinations resulting in a Yellow card report, and mean number of adverse events per report for three covid-19 vaccines administered in the UK
Risk of misinterpretation
Unfortunately, however, our interpretation can never be secure. The results we see could be due to the vaccines themselves. Alternatively, they could also be due to some confounding factor like the differences in age profile of the patients who were injected with different vaccine types, or to certain vaccine types being injected predominantly as boosters, or some combination of such factors. Yet distinguishing between alternative explanations is vital. If the effects we see are indeed due predominantly to vaccine type, this would have serious implications for vaccination policy and optimum choice of vaccine for minimising adverse reactions. However, analysis of confounding effects can only be achieved if the raw, anonymised individual patient data from the Yellow Card scheme are released by MHRA.
Comparing type of report by vaccine type
The second type of question that we can address using the Yellow Card data is whether choice of vaccines affects the spectrum of medical conditions recorded as adverse reactions. To answer this question, we can first sum up the number of adverse events elicited by each vaccine under the broad headings Blood & Vascular, Cardiac, Immune, Reproductive & Breast, Respiratory, Skin, Nervous System, Eye, Muscle and Other. A simple test for heterogeneity indicates that the relative frequency with which these classes of adverse reactions occur is highly dependent on the type of vaccine administered (χ2(18) = 29508, P<<0.001). Figure 1 illustrates the percentage by which the observed numbers of adverse reactions differ from the number expected if all vaccines elicited the same spectrum of adverse reactions. It is clear from the figure that departures from expectations are particularly large in the categories Blood & Vascular, Cardiac, Reproductive & Breast, and Skin; the different vaccines are eliciting quite different relative frequencies of adverse reaction in these categories.
For the categories Blood & Vascular, Cardiac, and to a lesser extent Immune and Reproductive & Breast, much higher than expected numbers of adverse reactions are elicited when the mRNA vaccines are administered, and lower than expected numbers of adverse reactions are found when the virus vectored Astrazeneca vaccine is used. Given that the same spike protein is encoded in the mRNA and virus vectored vaccines, this suggests that differences in the observed spectra of adverse reactions may be related to the mode of delivery of the spike encoding nucleic acid sequence in the vaccine. This observation for the Cardiac category is in agreement with a recent case series analysis which found that the risk of myocarditis is greater following sequential doses of mRNA vaccine than sequential doses of the adenovirus vaccine [4]. The role of the mRNA vaccine delivery system itself in eliciting adverse reactions must therefore come under scrutiny.

Figure 1. Percentage deviation of observed number of adverse reactions from the number expected if the spectrum of adverse events was the same for all vaccines. Data from nine different categories of adverse events are shown
While this example shows that the Yellow Card data may be helpful for generating ideas and supporting other studies, the inadequacy of the partial information currently released by the MHRA means that our interpretation of such data will always be compromised. Again, we do not possess the means to control for possible confounding factors (age and sex of individual, vaccine dose number etc.) that could contribute to the results observed. Nevertheless, in this example, the sheer size of the apparent effects of vaccine type on the spectrum of adverse effects indicates that a thorough investigation is essential. If the vaccine effect were confirmed, this would have serious real-world implications for the Covid-19 vaccination programme and the safety and health of the UK population.
Conclusion
The data we need to carry out the necessary analysis to maximise the usefulness of the Yellow Card scheme has already been collected at the public expense and is currently held by the MHRA. We call upon the MHRA immediately to release the raw, anonymised, individual patient data from the Yellow Card reporting scheme to enable rigorous scrutiny of Covid-19 vaccine adverse events by doctors, researchers and the public. This echoes the recent call by BMJ editors for immediate release of raw data from trials conducted by vaccine manufacturers [5].
2. https://www.cdc.gov/vaccinesafety/ensuringsafety/monitoring/vaers/index.html
3. https://jessicar.substack.com/p/a-report-on-myocarditis-adverse-events
4. https://www.medrxiv.org/content/10.1101/2021.12.23.21268276v1
5. Doshi P, Godlee F, Abbasi K. Covid-19 vaccines and treatments: we must have raw data, now BMJ 2022; 376 Covid-19 vaccines and treatments: we must have raw data, now | The BMJ
Am I immune to Omicron if I have already become infected with the Delta variant?
Q&A #12 with Geert Vanden Bossche | February 3, 2022
Question
“Those who became infected with the Delta variant are therefore not immune to the Omicron,” says Frank Vandenbroucke, Minister of Public Health Belgium. Is this correct? Will my T cells then not recognize the coronavirus? Or will my antibodies not protect me? Or maybe I will be infected asymptomatically and thus not get sick and then this is equivalent to “after vaccination”?
Answer
When you get infected with another variant there is always a chance that you will get sick. However, if you are in good health, the chance that SARS-CoV-2 will make you seriously ill is negligible. We owe this to our innate immunity which – especially in young people – is the first line of defense to clean up and eliminate large amounts of the virus (vacuum cleaner!). Young people, but even all healthy people who are in excellent health (e.g. no excess weight and regular exercise / sport), will often not even get sick or at best develop some vague, mild symptoms. If the first line of defense is broken, then our acquired immune system rushes to the rescue whereby our T cells ensure that the sick, virus-infected cells are eliminated. This allows us to recover from illness.
But whenever our innate immune system is exposed and eliminates the virus (with or without the help of the acquired immune system) it also immediately learns to recognize the virus better in the future. While it continues to recognize all SARS-CoV-2 variants (and even all CoVs), it now does so with more efficiency/affinity. This phenomenon is called “training” of the innate immune system. It is a form of adaptive immunity caused by epigenetic changes that effect a reprogramming of immune cells that secrete innate antibodies. That is, with subsequent exposure to the virus, there is an increasing chance that that person will develop an asymptomatic infection and actually not get sick at all, even if the virus undergoes antigenic drift (antigenic drift). If the virus undergoes an antigenic shift (i.e., severe change due to multiple mutations as in the case of Omicron), then the innate immunity will have to train again for a while before being able to withstand an infection with such a variant without giving rise to illness.
A pandemic is of course an excellent opportunity to train the innate immune system against SARS-CoV-2. However, it also means that if a variant with an antigenic shift (e.g. Omicron) dominates, more people may become ill anyway and within a short period of time the virus will be under pressure due to the induced natural antibodies, which are not able to suppress the virus at high infection pressure. Reducing the infection pressure is possible via (one-time) antiviral chemoprophylaxis. On the contrary, continued vaccination will increase the immune pressure and ensure that the vicious circle of the pandemic is maintained.
Thus, trained innate immunity to SARS-CoV-2 is not equivalent to COVID-19 vaccination but is superior because
- It is effective against all variants
- It has a sterilizing effect in contrast to vaccine antibodies
- Because of its non-varying character it does not lead to the selection of more infectious or resistant variants.
In other words, it benefits both individual and public health. It is the only way to acquire group immunity (independent of the circulating SARS-CoV-2 variant) and thus to move the pandemic into the endemic phase.
Former Pfizer VP Michael Yeadon demands apology from media over ‘lies’ asserting vaccine safety

Dr Michael Yeadon, former Pfizer vice president and co-founder of Doctors for COVID-19 Ethics
By Patrick Delaney | LifeSiteNews | February 2, 2022
After being excoriated by mainstream media outlets regarding his concern that COVID-19 gene-based vaccines could cause fertility issues in young women, Dr. Michael Yeadon is now requesting contrition on the part of media outlets as leaked data from the U.S. military indicates heavy spikes in these tragic outcomes.
“I’m not vindictive, but I want some humility and contrition from the BBC and all other media outlets that lied to their audiences,” said the former Pfizer vice president and Chief Scientist for allergy and respiratory.
Yeadon, who spent 32 years in the industry leading new medicines research and retired from the pharmaceutical giant with the most senior research position in his field, was an author of a submitted petition to the European Medicines Agency (EMA) in December 2020 that raised substantial concerns regarding a lack of sufficient testing of the experimental COVID-19 gene-based vaccines, prior to their emergency use authorizations.
With regard to the possibility of the shots endangering the fertility of women, Yeadon and his colleague, Dr. Wolfgang Wodarg, wrote, “There is no indication whether antibodies against spike proteins of SARS viruses would also act like anti-Syncytin-1 antibodies. However, if this were to be the case this would then also prevent the formation of a placenta which would result in vaccinated women essentially becoming infertile.”
Such a possibility would need to be ruled out through standard experimentation prior to imposing such substances onto the entire population, according to the doctors.
“It’s important to note that none of these gene-based agents had completed what’s called ‘reproductive toxicology,’” Yeadon wrote in his recent statement. “Over a year later, this battery of tests in animals still has not been done. So there was and still is no data package supporting safety in pregnancy or prior to conception.”
Media response to valid concerns: attacks, smears, vilifications
“As a society, we’ve practiced the precautionary principle most assiduously in relation to conception and pregnancy ever since the tragedy of thalidomide, over 60 years ago. So we had hoped that some at least in the media would take this [concern] with the seriousness it deserved,” he wrote.
“Did that happen? No. Instead, we were attacked, smeared and vilified in every medium, from Twitter to the BBC,” the British national wrote. “[M]ajor broadcasters actively lied to the public, explicitly stating that these agents were completely safe in pregnancy.”
Indeed, Reuters excoriated the doctors for making their inquiry “without providing evidence, that the vaccines could cause infertility in women,” shifting the burden of proof onto the petitioners from the regulators whose job it is to ensure proper safety trials are completed before the release of such drugs.
The article quoted an anonymous spokesman for Britain’s Department of Health & Social Care, saying, “These claims are false, dangerous and deeply irresponsible.”
Reuters later attempted to “fact-check” Yeadon as well over several concerns including the danger to fertility, to which he simply reiterated common ethical principles with regard to human experimentation: “No one in their right mind thinks giving experimental treatments to pregnant women is other than reckless. Especially when reproductive toxicity testing is incomplete.”
Of special note for Yeadon was BBC Radio talk show hostess Emma Barnett, who “directly attacked me by name on air in the most unpleasant terms,” which also led to his charging the program with slander. In response, after a bit of investigation, the program editor conceded, apologized to Yeadon, and cut their false representation of the former Pfizer scientist from their recorded podcast.
“[Barnett] also had her guest, who was from the Royal College of Obstetrics and Gynecology, repeat the lies that it was perfectly safe for young women to be injected,” Yeadon called out in his statement.
Preprint paper reveals placental-damaging antibodies increased 2.5 fold after shots
Also of note for the former executive was a preprint study published last May that appeared to attempt a rebuttal of his concern that anti-Syncytin-1 antibodies could be developed due to the shots, but instead reinforced them showing a 2.5 fold increase of the placental-damaging antibodies in days 1 to 4 after COVID-19 gene-therapy injections.
The paper, which claimed a conflict of interest in being funded by Johnson & Johnson, went on to explain that though they had observed this major increase, they did not examine its “clinical significance,” thus admitting they didn’t know if these higher levels of the antibody flagged an actual safety problem with regards to fertility and miscarriage.
At the same time, the study’s authors acknowledged data showing “spontaneous miscarriage as the most common obstetric outcome after COVID-19 mRNA vaccination.”
Based on the outcome of this study alone, Yeadon said “all of these experimental products as a class should have been completely contraindicated in women younger than menopause.”
Pfizer & Moderna ‘definitely knew’ these mRNA products would ‘accumulate in the ovaries’
An additional source of concern regarding fertility was that “the mRNA products (Pfizer and Moderna) would accumulate in ovaries,” the British national explained.
“An FOI request to the Japanese Medicines Agency revealed that product accumulation in ovaries occurred in experiments in rodents. I searched the literature based on these specific concerns and found a 2012 review [here], explicitly drawing attention to the evidence that the lipid nanoparticle formulations as a class do, in fact, accumulate in ovaries and may represent an unappreciated reproductive risk to humans. This was ‘a well-known problem’ to experts in that field,” Yeadon explained.
“I’ll say that again. The pharmaceutical industry definitely knew, in 2012, that formulating these agents in lipid nanoparticles would lead them to accumulate in the ovaries of women to whom these were given.
“No one in the industry or in leading media could claim ‘they didn’t know about these risks to successful pregnancy,’” he emphasized.
Results from the U.S. military leak confirm damage done to unborn children and fertility
“So it’s with tremendous anger and sorrow that I heard of military physicians blowing the whistle about the evidence of harms in pregnancy that their proprietary safety monitoring database had thrown out,” Yeadon said, referring to last week’s revelations during a U.S. Senate panel discussion.
“In the intervening months since journalists (including but definitely not limited to Emma Barnett) chose to downplay or downright lie about our concerns, we learned that women in the U.S. military were experiencing 3X normal rates of miscarriage,” he explained.
In fact, these data leaks, given by three “decorated high-ranking soldiers who are doctors and public health officials,” in sworn declarations under penalty of perjury, show several increases in negative impacts upon fertility, including spontaneous abortion, among this military population where enforcement of an experimental COVID gene-vaccine mandate is strictly observed.
As presented by these soldiers, the following 2021 increases only include the first 10 months of the year (January through October) and are compared with the full five-year average of figures taken from 2016 through 2020.
- Miscarriages — increase of 279%
- Female infertility – increase of 471%
- Male infertility — increase of 344%
- Congenital malformations (birth defects) – increase of 156%
And considering most children conceived after these injections had not been born before November 2021, the final figure of birth defects is likely to significantly increase as well.
Journalists, regulators and manufacturers: ‘You are way out over thin ice and deep water’
After Yeadon’s request for contrition from the BBC and other media outlets, he went on to implore readers, “please do not get injected with these inherently dangerous and ineffective experimental products. Warn anyone you know about the risks to pregnancy, now confirmed by whistleblowers from physicians in the U.S. military.
“Please also tell them there are likely to be other reproductive health consequences, even in young girls, because of accumulation [of lipid nanoparticles] in their ovaries.“
Having originally alerted the EMA of several other possible toxic outcomes due to the injections, Yeadon highlighted that he and Dr. Wodarg were sadly also right about their warning of “allergic, potentially fatal reactions to the vaccination,” citing examples from the UK of emergency interventions and tragic deaths.
“Having had two of two serious harms we warned about, prior to regulatory authorisations, come to pass,” he said. “I humbly recommend that governments and journalists everywhere recognise what you’ve done and lobby for or directly decide to immediately and completely withdraw all these experimental products from the market, before some of the other specified concerns (or issues we didn’t think of) show up in the safety monitoring systems.”
“Journalists, regulators, healthcare professionals and politicians, as well [as], of course, the manufacturers, you are way out over thin ice and deep water. I don’t know how you’re planning to get out from under this before the wider public more fully appreciates what you’ve done,” Yeadon wrote.
“One possibility is that you won’t be able to hide your complicity in the massed harms you’ve done to millions of people. In this case, I look forward to giving evidence against you in a court of law,” he concluded.
Dr. Yeadon’s full statement can be accessed here.
These 5 Studies Reveal a Disturbing Trend — Researchers Presenting Conclusions That Don’t Match the Data
By Josh Mitteldorf, Ph.D. and Madhava Setty, M.D. | The Defender | February 2, 2022
It was January 2020, the very beginning of COVID, when news articles began appearing that connected the genetics of the virus with gain-of-function research on bat coronaviruses at the Wuhan Institute of Virology.
These speculations were put to rest by an authoritative statement in the prestigious journal Nature Medicine, echoed by a summary in Science and an unusual affidavit in the Lancet signed by an impressive list of prominent scientists.
The message in the Nature Medicine article was dispositive: “Our analyses clearly show that SARS-CoV-2 is not a laboratory construct or a purposefully manipulated virus.”
But where was the support for this confident conclusion in the article itself?
The 2,200-word article in Nature Medicine (Anderson, et al) contained a lot of natural history and sociological speculation, but only one tepid argument against laboratory origin: that the virus’s spike protein was not a perfect fit to the human ACE-2 receptor.
The authors expressed confidence that any genetic engineers would certainly have computer-optimized the virus in this regard, and since the virus was not so optimized, it could not have come from a laboratory. That was the full content of their argument.
Most readers, even most scientists, take in the executive summary of an article and do not wade through the technical details. But for careful readers of the article, there was a stark disconnect between the Cliff Notes and the novel, between the article’s succinct (and specious) conclusion and its detailed scientific content.
This was the beginning of a new practice in the write-up of medical research. Recent revelations in the Fauci/Collins emails shed light on the origins of this tactic and the motives behind it.
In the past, if a company wanted, for example, to make a drug look more effective than it really was, it would choose a statistical technique that masked its downside, or it would tamper with the data.
What companies would not do, in the past, was describe the results of a statistical analysis that proves X is false, then publish it with an Abstract that claims X is true.
But this strange practice has become more common in the last two years. Academic papers are being published in which the abstract, the discussion section and even the title flatly contradict the content within.
Why is this happening? There are at least three possibilities:
- The authors cannot understand their own data.
- The authors are being impelled by the editorial staff to arrive at conclusions that match the ascendant narrative.
- The authors and editors realize the only way to get their results into publication is to avoid a censorship net that gets activated by any statement critical of vaccination efficacy or safety.
Before reaching any conclusions, let’s take a closer look at some examples of this troubling phenomenon arising in what should be the foundation of what is known: published scientific data.
In this article, we present five different published studies. Each to varying degrees exemplifies a disconnect between the data and the conclusions.
Example 1: ‘Phase I Study of High-Dose L-Methylfolate in updates Combination with Temozolomide and Bevacizumab in Recurrent IDH Wild-Type High-Grade Glioma’
This example is unrelated to the pandemic, but it typifies a common practice in the pharma-dominated world of medical research. If a remedy is cheap and out of patent, there is no one motivated to study its efficacy.
But research practice has gone well beyond neglect. In fact, investigators are skewing statistics to make cheap, effective treatments look ineffective if they are in competition with expensive pharma products.
This is ridiculously easy to do — all it requires is incompetence. Using the wrong statistical test, using a weak test when a stronger one applies — or just about any mistake in parsing the data — is far more likely to make compelling data appear random than the opposite.
Is it always incompetence? Or is it more often a well-thought-out deception that uses seemingly erudite analysis to lead the undiscerning reader into believing the wrong conclusion?
In the case of this article, a simple B vitamin (L-Methylfolate) was shown to double the life expectancy of 6 out of 14 brain cancer patients who received it, while showing no benefit (and no harm) to the other half of the patients.

The purple jagged line extending out to the right represents 40% of patients who lived dramatically longer when treated with L-Methylfolate (LMF).
The abstract reports that “LMF-treated patients had median overall survival of 9.5 months [95% confidence interval (CI), 9.1–35.4] comparable with bevacizumab historical control 8.6 months (95% CI, 6.8–10.8).”
The increase in median survival time is just a few months and not statistically significant. But the average survival time of the folate-treated group was more than double, and the difference was statistically significant (by my calculation, not in the article).
But the average is what is more commonly reported, and most readers don’t understand the difference between average and median.
The longest surviving patient on the B vitamin was still alive at the end of the study (3.5 years) when every one of the patients treated only with traditional chemo was dead before 1.5 years.
There were three different dosages in the study, (30, 60, 90 mg) and it was not reported whether the longest-living patients were receiving the highest dosages.
This is, in fact, a hugely promising pilot study about treating a common, fatal cancer with a simple vitamin. If it were an expensive chemotherapy drug instead of a cheap vitamin, you can be sure it would have been hailed as a breakthrough.
But this study will not create much excitement, and few oncologists will even know to prescribe methylfolate for their glioma patients.
Example 2: ‘Preliminary Findings of mRNA Covid-19 Vaccine Safety in Pregnant Persons’
Earlier this year, MacLeod et al used data from a prominent Centers for Disease Control and Prevention (CDC) study to calculate that for women in their first trimester, the rate of miscarriage following administration of an mRNA COVID vaccine was an alarming 82%.
On Jan. 7, the CDC released a report designed to dispel our misgivings about vaccinating pregnant women. Its conclusions were unequivocal:
“These data support the safety of COVID-19 vaccination during pregnancy. CDC recommends COVID-19 vaccination for women who are pregnant, recently pregnant, who are trying to become pregnant now, or who might become pregnant in the future.”
The Defender reported on the numerous flaws in this study. The most egregious deficiency was the dearth of pregnant women in the study who were vaccinated early in their pregnancy (less than 2%).
The authors admit their study could not quantify the risk of vaccine exposure in the first trimester: “First trimester vaccinations are not included in analyses stratified by trimester because few exposures occurred…”
How then can they recommend COVID vaccination for women who are “recently pregnant” if their analyses excluded women in their first trimester?
This report serves a purpose. People who read it superficially will find the reported results reassuring — including front-line doctors who don’t have time to evaluate the research critically.
The CDC chose to paint over troubling safety concerns with reassuring words that are unsupported by clear science.
Example 3: ‘Public Health Scotland COVID-19 & Winter Statistical Report’
There is a section of this report comparing vaccinated and unvaccinated rates of disease, preceded by a warning to the reader not to take the data at face value.
“PLEASE READ BEFORE REVIEWING THE FOLLOWING TABLES AND FIGURES There is a large risk of misinterpretation of the data presented in this section due to the complexities of vaccination data …”
The data the authors don’t want us to misinterpret say that people who have been vaccinated with one shot or three shots are 50% more likely to contract COVID-19 compared to people who are unvaccinated.
People who receive two shots are more than twice as likely to contract COVID-19. This is according to the authors’ own method of calculating age-standardized disease rates.

The authors emphasize it’s not about case numbers — it’s about severe outcomes, hospitalizations and deaths:
“Evidence suggests the COVID-19 vaccines are 90% effective at preventing a severe outcome of COVID-19. COVID-19 hospitalizations and deaths are strongly driven by older age, with most deaths occurring in those over 70 years old and having multiple other illnesses. But overall, you are less likely to be hospitalized if you are vaccinated with a booster.”
What data are they talking about? Here are results from their own data table:
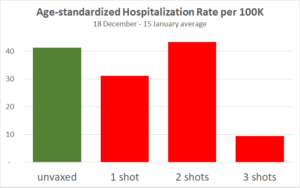
The only substantial reduction is from people who received the third shot, which has only recently been available in Scotland. But for the three-shot cohort only, vaccination effectiveness is declining over the four weeks.
This adds to previous evidence that protection from the vaccine is short-lived, and each injection provides a shorter window of protection than the previous one. Also, note the hospitalization statistics may have been gamed.
Since the publication of this article, England but not Scotland has backed off requirements for vaccination IDs.
Example 4: ‘Clinically Suspected Myocarditis Temporally Related to COVID-19 Vaccination in Adolescents and Young Adults’
Myocarditis, or inflammation of the heart, is a severe and life-shortening disease. It is virtually unknown in young people, but it is a recognized side effect of the COVID vaccines, especially in boys and young men.
This article summarizes the experience of 139 young patients (ages 12 to 20) who were hospitalized for myocarditis following vaccination.
19% of them were taken into intensive care.
Two required infusions of pressors and inotropes (potent intravenous drugs used to raise critically low blood pressure).
Every patient had an elevated Troponin I level. Troponin is an enzyme specific to cardiac myocytes. Levels above 0.4 ng/ml are strongly suggestive of heart damage. These young patients had a median Troponin I level of 8.12 ng/ml — over 20 times greater than the levels found in people suffering heart attacks.
“Conclusions: Most cases of suspected COVID-19 vaccine myocarditis occurring in persons <21 years have a mild clinical course with rapid resolution of symptoms.”
“Mild clinical course” — We suppose this refers to the 81% who did not go to the ICU or the fact that none died or required ECMO (Extracorporeal Membrane Oxygenation, a desperate means to keep the body oxygenated when a patient’s heart or lungs have completely failed).
In any case, every single person in this study was hospitalized. When does a “mild clinical course” require hospitalization for a two-day median length of stay?
“Rapid resolution of symptoms” — How would anyone know this? Myocarditis in older patients doubles the probability of death for the long term.
We don’t know what it will do to young boys in the long term, especially since every patient had some damage to their heart as evidenced by significantly abnormal troponin levels. And we don’t fully understand the mechanism by which the vaccines cause myocarditis.
Example 5: ‘Increases in COVID-19 are unrelated to levels of vaccination across 68 countries and 2947 counties in the United States’
This is the title of a paper by two statisticians from the Harvard School of Public Health, published on Sept. 30, 2021, in the European Journal of Epidemiology.
The title makes the important claim that there is no public health benefit from vaccination. COVID-19 is spreading at the same rate in different populations, unrelated to whether the population is mostly vaccinated or mostly unvaccinated.
It’s a powerful counterpoint to the ubiquitous demand that more people should undergo vaccination for the sake of their community.
The paper completely undermines the requirement of vaccination to attend meetings, concerts, theater and other public gatherings. It says there is no legitimacy to the creeping government vaccine mandates for travel.

But the data in the paper don’t show that vaccination and spread of COVID-19 are “unrelated.” In fact, there is a paradoxical relationship, an insidious relationship: The more vaccinated countries had more new COVID-19 cases (during the week when the survey was conducted). The correlation is significant (p=0.04).
Still, the authors conclude by explicitly recommending propagandizing of the unvaccinated: “In summary, even as efforts should be made to encourage populations to get vaccinated it should be done so with humility and respect.”
It may sometimes be wrong to promote flawed health policy, but apparently, it’s a good thing, so long as it is done with humility and respect.
Why would these researchers take the trouble to publish data that is so damning to the vaccine narrative, and then pull punches in the title and in the conclusions?
Are we to assume that these authors who have assiduously extracted data from 68 different countries and nearly 3,000 U.S. counties were unable to notice their meticulous scatter plot unequivocally demonstrates high vaccination uptake is associated with higher (NOT lower) prevalence of COVID-19?
This seems to be a different case from the first example, where shills for the pharmaceutical industry set out to create a deceptive narrative. We think it’s probable that in this case, soft-pedaling the implications of these glaring data may not have been the authors’ choice, but rather a decision by the journal’s editors.
We know from personal experience how difficult it is to get an article through peer review at most “reputable” medical journals when the results are out of sync with the COVID narrative.
It may well be that these authors fought hard to get their subversive message into print, and in order to get past peer review, they softened the language, especially, the title.
Conclusions
The church was once the most trusted institution in Europe. Then the bishops started selling indulgences — a kind of get-out-of-hell-free pass for rich sinners.
Today the most trusted institution is science.

Sources: Gallup, Gallup, Gallup, Pew
This is true despite the fact that scientists are human, subject to error and to corruption.
Medical journals have become financially dependent on their advertisers, which are almost exclusively the pharmaceutical giants.
For several decades now, the “Church of Science” has been selling indulgences. With enough money, you could buy a scientific study that says what you want it to say.
Darell Huff’s book, “How to Lie with Statistics,” first published in 1954, remains the all-time best-seller in its field.
Recently, Gerald Posner documented the way in which the pharmaceutical industry has used its profits to affect science at every level, from medical researchers to journal editors to government regulatory agencies to the journalists who interpret science for the public.
Pressure is being placed on independent researchers by the journal editors and peer reviewers, many of whom have ties to Big Pharma. Valid studies, honestly reported, can be rejected for publication if they send a message that threatens corporate profits.
In the age of COVID, we see three reasons that an article’s conclusions might become detached from its statistical findings:
- Scientists have suddenly abandoned basic logic and reason. This is an implausible explanation because, as has been demonstrated above, these examples demonstrate diligence in gathering data. There is no reason why they would abandon diligence in arriving at reasonable conclusions.
- Shortcuts by pharmaceutical companies and their shills in academia. Rigging clinical trials the old-fashioned way is expensive and time-consuming. It’s also uncertain. Sometimes the truth rears its head even if a study is designed to conceal it. Even a study that is designed to fail might succeed when the inconvenient truths are sufficiently stubborn. How much easier it is to report the results and then tack on an abstract and a discussion section that say what you want to say, regardless of the data tables in the body of the article!
- Scientist authors are well aware of the pernicious censorship in scientific publication that has emerged in recent days. This is perhaps the most intriguing possibility. If researchers behind the study have some prestige and some influence, they still may find they have to soften their rhetoric in order to pass peer review. However, what we are witnessing today is more than a tendency to be “diplomatic” in their choice of words. What does it mean when their conclusions do not match the findings? Are they trying to tell us that they are gagged? Are they silently screaming at us to look at the data and not their interpretation of them?
The Nature Medicine article on the origins of the SARS-CoV-2 virus (reviewed first) seems to be an example of researcher corruption.
The article in the European Journal of Epidemiology (Example 5), which relates vaccination rates to COVID prevalence, is more likely an example of corruption by journal editors and peer reviewers.
In this instance, the data and conclusions are so disparate that it begs us to reconsider the cynical position that all scientists have been corrupted. Is there a better way for conscientious scientists to signal their community that they are being censored than by compiling solid data that tell a compelling story and then arriving at a nonsensical conclusion? Are they imploring us to read between the lines?
For the other four articles reviewed above, we leave it to your judgment — how do you think the conclusions came to be so disconnected from the statistical findings in these same articles?
Obviously, this blatant distortion of scientific write-ups is not a long-range strategy, but the world is moving fast, and people who count on their ability to shape scientific conclusions to their financial interests will be successful for long enough to do a great deal of mischief.
What will be the damage to the credibility of science when the dust clears?
Josh Mitteldorf, Ph.D., has a background in theoretical physics. Since the 1990s, he is best known for his contributions to the biology of aging, including many articles and two books.
Madhava Setty, M.D. is senior science editor for The Defender.
© 2022 Children’s Health Defense, Inc. This work is reproduced and distributed with the permission of Children’s Health Defense, Inc. Want to learn more from Children’s Health Defense? Sign up for free news and updates from Robert F. Kennedy, Jr. and the Children’s Health Defense. Your donation will help to support us in our efforts.
How Many Pregnant Women Have Actually Died of COVID-19?
The Daily Sceptic | February 3, 2022
There follows a guest post by a Daily Sceptic reader, who wishes to remain anonymous, who, being pregnant, was following closely the advice and studies concerning pregnant women. However, her own analysis of the reports on the deaths of pregnant women with COVID-19 suggested that the alarming statistics about Covid in pregnancy she was being provided with did not stack up.
As a pregnant woman, I have been following advice and studies that concern this group closely. Unfortunately, it is becoming increasingly difficult to find any balanced information amongst the blatant propaganda. I am so sick of being told at every turn that ICU is full of unvaccinated pregnant women. Below is an example of the stuff that gets shared online by my local maternity team.

So I thought I would look at what stats MBRRACE had released lately. They have two reports that caught my eye in particular: one on maternal Covid deaths March-May 2020 (10 women) and another covering the period June 2020-March 2021 (17 women).
Despite being such a small group of people, I feel that each case is a fascinating story that paints a dramatically different picture to that portrayed by the media and the NHS. Here are some points that stood out to me from each report
March-May 2020 (10 deaths)
- None of the women who died received any actual treatment, just support.
- Three of the ten women died because they were too scared to go to hospital.
- Four women died of suicide and not being able to access help was a factor (I don’t think they were included in the ten deaths, but the insinuation is that Covid restrictions contributed to their deaths).
- Two women were murdered by their partners, with health services already knowing they were at risk (again, I don’t think they were included in the ten, but the insinuation about restrictions is there again).
- The quote “pregnancy [sic] and postpartum women do not appear to be at higher risk of severe COVID-19 than non-pregnant women” seems telling.
- Only two women were classified as having received “good care”.
June 2020-March 2021 (17 deaths)
- Three women did not even have Covid but died as a result of the side effects of restrictions.
- Four women tested positive but died of unrelated causes – two of these women received poor care because of their Covid status.
- 60% of the women who actually died from Covid were obese and a further 20% were overweight.
- 50% had pre-existing mental health conditions (personally I believe that this both prevents women from being able to speak up for themselves and creates a stigma that they are ‘difficult patients’).
- One woman died at home of a urinary tract infection because no translator was available for her telephone appointment.
- Four women died because they were too scared to go to hospital – one of these women sought no antenatal care at all and died after giving birth at home.
- One woman died after being given painkillers for backache – she was only seen remotely by a GP so he or she couldn’t see she was both heavily pregnant and had sepsis.
- Another woman died of sepsis from a miscarriage because doctors assumed she just had (asymptomatic) Covid.
- A woman died of obvious kidney/liver problems shortly after birth because again, doctors bizarrely assumed she was actually suffering from Covid following a positive routine test.
- 90% of the women who died had “care” that was not managed by the RCOG guidelines.
- One woman was not given treatment despite poor clinical indications, as she did not “look sick”.
- Three women who were very poorly and were considered for ECMO were denied this despite not having any contraindications.
- One woman died from a pulmonary embolism at home after her GP’s online triage system did not recognise either her Covid status or recent pregnancy as risk factors and didn’t give her an urgent appointment.
- Only 10% of the women received “good care”, and in 70% improvements in care may have meant they survived.
The reports are heartbreaking and I do not wish to diminish the pain that these women’s families must be suffering, but it is abundantly clear that very few of these women died from actual Covid – many appear to be victims of the restrictions and fear – and the handful that did had significant confounding factors.
Jordan Peterson Compares Climate Model Errors to Compounding Interest
By Chris Morrison | The Daily Sceptic | February 2, 2022
It’s been all Canada on Joe Rogan’s popular Spotify podcast of late. First, crinkly rockers Neil and Joni threw their guitars out of the pram when Rogan dared to broadcast a number of different opinions on Covid and vaccines. Then fellow Canadian Dr. Jordan Peterson said climate models compounded their errors, just like interest. Green activists and zealots (often known in the climate change business as ‘scientists’) clutched their responsibly sourced pearls and whined, “Lawks a-mercy, it’s outrageous!” and “Banning’s too good for them!”. The septuagenarian songsters briefly found themselves out of the headlines as the mainstream media rushed to quell a growing sceptical climate debate and rubbish a troublesome competitor.
Dr. Peterson suggested that the climate was too complex to be modelled. Such notions were said to be a “word salad of nonsense,” reported a distraught Guardian. Dr. Sarah Perkins-Kirkpatrick of the University of Canberra added Peterson had “no frickin’ idea”. Professor Michal Mann of Penn State University said Peterson’s comments – and Rogan’s “facilitation” of them – was an “almost comedic type of nihilism” that would be funny if it wasn’t so dangerous.
This of course is the same Michael Mann who produced the infamous temperature hockey stick that was at the centre of the 2010 Climategate scandal. The graph was used for a time in IPCC reports and showed a 1,000 year straight temperature line followed by a recent dramatic rise. This startling image was helped by the mysterious disappearance of the medieval warming period and subsequent little ice age. Discussion about the graph led to Mann pursuing a U.S. libel suit against the broadcaster and journalist Mark Steyn. In court filings, Mann argued that it was one thing to engage in discussion about debatable topics, but it was quite another to “attempt to discredit consistently validated scientific research through the professional and personal defamation of a Nobel Prize recipient”. He is not himself a Nobel Prize recipient, but perhaps he was referring to someone else.
Independent minded communicators like Joe Rogan and take-no-prisoner intellectuals such as Dr. Peterson command a worldwide audience and they are difficult to cancel. The battle between Neil Young and Joni Mitchell and Joe Rogan, sitting on a $100m Spotify contract, had only one free speech winner – at least for the moment. Meanwhile, the Guardian’s default position when faced with something unsettling like the ‘settled’ science of anthropogenic climate change is to declare it will not “lend” its credibility to its critics by engaging in debate. That was obviously not possible with Peterson’s remarks being plastered all over social media, although it could be argued that the Guardian reporting the vulgar abuse users posted in response is not much of a substitute for the usual lofty disdain.
Dr. Peterson attacked climate models on a number of fronts. In particular, he noted that as you stretch out the models across time “the errors increase radically”. In its way, this refers to the biggest problem that lies at the heart of the 40-year track record of climate model failures. To make a prediction, climate models are fed a guess of the increase in the global mean surface temperature that follows a doubling of atmospheric CO2. Nobody actually knows what this figure is – the science for this crucial piece of the jigsaw is missing, unsettled you may say. The estimates run from 1°C to as high as 6°C and of course the higher the estimate, the hotter the forecasts run.
As they don’t say in the climate and Covid modelling business – Garbage In, Garbage Out.
Meanwhile back in the real world, global warming has been running out of steam over the last two decades. Satellite temperatures, which have been available since 1979, provide a more accurate measurement of global warming (or cooling) than flawed and frequently massaged surface measurements.
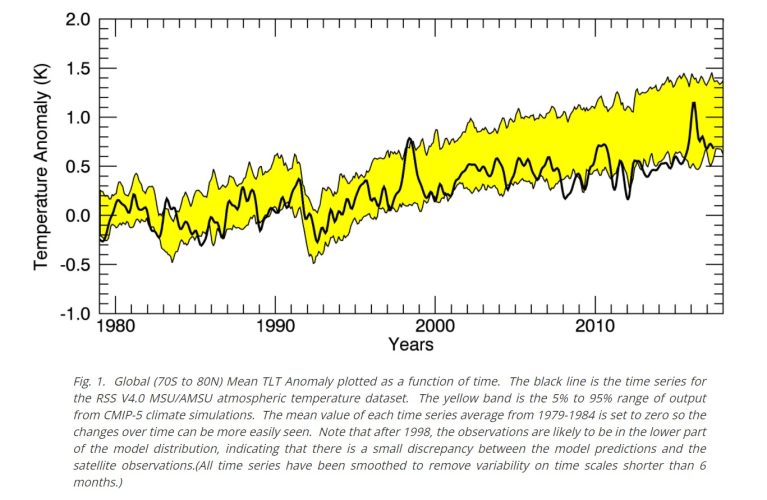
The graph above from Remote Sensing Systems demonstrates the lack of warming measured by satellites and is displayed by the black line. Forecasts from climate models, contained within the yellow area, started to diverge significantly from the late 1990s, backing Dr. Peterson’s claim that over time they magnify their own errors. As with epidemiological models, there seems little incentive to tone down the inputs – it’s difficult to make a reputation, and secure grants, by saying that few people will die. In the case of climate models, there are also 204,000,000,000,000 reasons to exaggerate – this being the £204 trillion that McKinsey recently said must be spent to achieve the political goal of global Net Zero by 2050.
The ‘pure’ science around climate change is thin on the ground in the fast-growing Earth Science university faculties, more often than not a rebranding of the old Geography departments. The real science surrounds the effect of adding CO2 to the atmosphere, where an advanced knowledge of chemistry and physics is essential. Within such academic circles, there are growing doubts about the unproven hypothesis that humans cause all or most global warming by burning fossil fuel. While CO2 has been rising recently from a geologically ultra-low base, there is little correlation between the gas and temperature movement in almost any timeframe. Again Dr. Peterson is right to note that the climate is too complex to model accurately since there are almost countless other natural factors at work in a chaotic atmosphere.
Professor William Happer of Princeton has suggested that CO2 becomes “saturated” once it reaches a certain level, since it reflects heat back to Earth only within certain bands of the infrared spectrum. Increases in CO2 beyond current levels will have little effect on future warming, or cooling. Far from being harmful, the extra CO2 is highly beneficial for plant growth and food.
Recently, a group of physics professors from the University of Massachusetts led by Kenneth Skrable examined the carbon isotope trail released by fossil fuel burning. They found the amount of CO2 released was “much too low to be the cause of global warming”. The German physicist Dr Frank Stefani looked at the effect of the Sun and geomagnetic forces on the planet and concluded that the Sun alone accounted for between 30-70% of recent planetary warming.
About two years ago, 48 Italian science professors wrote an open letter to their Government noting that the “advanced alarmist forecasts” of climate models “were not credible”. Natural variability, it was said, “explains a substantial part of global warming observed since 1850”. Catastrophic predictions “are not realistic”. The letter was signed by a number of distinguished academics including Antonino Zichichi, Emeritus Professor of Physics, a past president of the World Federation of Scientists and the discoverer of nuclear antimatter. Not that the folks who write for the Guardian would ever “lend” their credibility by talking about the climate with these 48 ‘denier’ scientists.
Relax, Wisconsin Public Radio, Climate Change Isn’t Making Human Health Worse
By H. Sterling Burnett | ClimateRealism | January 28, 2022
A story run by Wisconsin Public Radio (WPR) today claims climate change poses a threat to human health. Disease and mortality data show this is false. During the recent period of modest warming, deaths resulting from extreme heat and weather have declined sharply, and research indicates climate change is not contributing to pandemics or parasite borne diseases.
WPR’s story, titled “Wisconsin health providers say climate change is a medical issue,” features input from the climate activist group, Wisconsin Health Professionals for Climate Action. WPR writes:
“Heat waves, cold spells could harm people, along with dangerous flooding, according to Wisconsin Health News panelists. Last year, top medical journals warned that climate change, not COVID-19, was the greatest threat to public health.”
“In the Midwest, climate change is likely to bring extreme temperatures and flooding, along with more mosquito and tick diseases, according to the Centers for Disease Control and Prevention (CDCP).”
While many top medical journals and the politically controlled CDCP have claimed climate change is causing worsening health and increasing incidences of premature mortality, hard data presented in peer reviewed literature proves this is false.
Data from the U.N. Intergovernmental Panel on Climate Change and the National Oceanic and Atmospheric Administration presented in Climate at a Glance articles disprove claims that heat waves, cold spells, and incidences of flooding have increased during the recent period of modern warming.
If instances of extreme heat or cold, and flooding events aren’t increasing, or are in fact declining, they can’t be causing an increase in adverse health events, which is precisely what the data establish.
As detailed in Climate Realism, here, deaths resulting from climate related events have fallen to a historic low, having fallen by more than 99 percent over the past 100 years.
On July 1, 2021 The Lancet published what is arguably the largest study ever to examine excess mortality associated with temperature. The study’s authors, 68 scientists representing universities and research institutes in 33 countries spanning all regions of the world, came to two very clear conclusions: Cold temperatures contribute to far more deaths each year than warmer temperatures; and deaths associated with extreme temperatures, hot or cold, are declining.
This study confirms what research previously published in The Lancet, the Southern Medical Journal, and other outlets, has consistently shown: Cold is the biggest temperature related killer, not heat, and as he earth warms the number of deaths related to extreme temperatures is falling dramatically.
Also, contrary to the impression given in the WPR story, there is no evidence insect borne tropical diseases are expanding their range or sickening, or claiming the lives of greater numbers of people as the earth has warmed.
The vast body of scientific literature referenced in Chapter Seven of Climate Change Reconsideree II: Biological Impacts and Chapter Four of Climate Change Reconsidered II: Fossil Fuels fails find any link between global warming and the spread of Lyme disease, malaria, Dengue fever, West Nile virus, and other vector-borne diseases are either grossly overstated or outright false.
For example, a 2010 study in the peer-reviewed science journal Nature:
“[C]compared historical and contemporary maps of the range and incidence of malaria and found endemic/stable malaria is likely to have covered 58% of the world’s land surface around 1900 but only 30% by 2007. They report, ‘even more marked has been the decrease in prevalence within this greatly reduced range, with endemicity falling by one or more classes in over two-thirds of the current range of stable transmission.’ They write, ‘widespread claims that rising mean temperatures have already led to increases in worldwide malaria morbidity and mortality are largely at odds with observed decreasing global trends in both its endemicity and geographic extent.’”
Also, in a 2008 article in the Malaria Journal, Pasteur Institute of Paris professor Paul Reiter wrote:
“Simplistic reasoning on the future prevalence of malaria is ill-founded; malaria is not limited by climate in most temperate regions, nor in the tropics, and in nearly all cases, ‘new’ malaria at high altitudes is well below the maximum altitudinal limits for transmission, [continuing] future changes in climate may alter the prevalence and incidence of the disease, but obsessive emphasis on ‘global warming’ as a dominant parameter is indefensible; the principal determinants are linked to ecological and societal change, politics and economics.”
Despite numerous claims to the contrary, claims parroted by WPR without citing any hard evidence, human health is not being threatened by climate change. Indeed, on every health indicator: human lifespan, premature mortality, premature births, infant mortality, hospitalizations linked to extreme temperatures or weather events, hunger, and malnutrition, to name the most often discussed health indicators, humans are living better, longer, healthier, lives than ever before.
Omicron did not “slam labor markets.” Covid policy did. And it was entirely avoidable.
el gato malo – bad cattitude – february 2, 2022
CNBC would appear to wish to have us believe that the drop in jobs was caused by “the variant” as though this was some act of nature instead of an act of government.
it is not. this is a deeply misleading framing intended to obscure causality rather than reveal it.

it’s way past the point where even these people could possibly be this ignorant of baseline reality.
this is, instead, a clear bet that you are.
this drop in jobs was not “unexpected” at least not by anyone paying attention. this is the direct, proximate effect of imposing vaccine mandates as a precondition to work. the OSHA mandate fell, but the federal mandate for contractors did not. thousands of mandates for health care workers imposed by states and hospital systems did not. requirements for many truckers and teachers and hospitality workers did not. many employers went ahead and imposed these anyway. they waited until after the holidays, but here we are.

we also cut off the flow of travel and of patronage. we closed businesses (again). we limited capacity. we mandated vaccination as a pre-requisite for going out to eat or staying in hotels. and like clockwork, it choked off the flow of tourists and local patrons alike because people HATE this and hate playing officious games and pretending that the made up “covid physics” of “wear your mask to the table then take it off when you sit” make any sense at all. they hate having some hostess demand “their papers.” maybe not everyone does, but enough people do that it has savaged businesses.
we’re living though needless damage to no useful effect at all.
this is NOT the virus.
it’s the predictable and unavoidable output of deeply stupid public health policy.
the damage since this began has been acute and severe. “2 weeks to flatten the curve” was, as many of us were screaming right from the beginning, the commencement of the nastiest economic hit to jobs and small business per unit time in US history and probably in global history.
in the US, we dropped 20 million jobs in 2 months. that is so far outside any precedent it’s staggering.
the entire 2008 recession and financial crisis led to a job reduction of 8 million over 24 months…
and we have NOT recovered to previous levels. current job levels are about the same as jan 2018.
they are 4 million jobs below the level from early 2020.
they are 9 million below where we would be had job growth continued as before. (added in red)
might job growth have slowed anyway? yes, perhaps, but this gives us a set of fairly reasonable bookends to assess the scope of what this has cost in terms of private nonfarm employment.
we’re 4-9 million jobs short of where we would likely have been without this public health response and claims that the US jobs market looks strong are pretty iffy.
(keep in mind that the unemployment rate drops when people drop out of the labor force/stop looking for work. it does not mean they found jobs.)

“but it was the virus! most of this would have happened anyway!”
this is a predictable claim, but seems out of step with reality. fortunately, we have a control group.
compare this damage to a place like sweden who did not lock down and freak out.
sweden’s payrolls figure is much more seasonally variable than the US, but looking through this seeming cardiac rhythm the overall difference in outcome is unavoidably obvious.
the dip was extremely minor in comparison. it was extremely short in comparison. and, despite the effects of many neighbors locking down, tourism and travel dropping, and global supply chain issues, their jobs figures currently look indistinguishable from 2019 and pre pandemic 2020.
employment today is higher than dec 2019 or jan 2020.
the US is nowhere close.

it’s really very simple: places that locked down harder got no better outcomes on covid. but they got much, much worse outcomes on economic and societal damage.
this was all known and knowable.
the base prior for pandemics was to never, never do this.
it’s what the guidelines said.
i did a ton of work on this back in the twitter days. it was obvious right from the start that drops in google mobility data (measuring actual human behavior from cell phone tracking) had zero effect on bending any epidemiological curve. it was clearly doing nothing at all. this was already glaring. and so was the harm.
i pulled this data from BLS way back in 2020:
it was more than a little apparent that it was predominantly politics and policy, not covid putting people out of work.
the no lockdown states were back at baseline by the fall.

the relationship was not subtle:

at this stage of the game and with this much clear data at one’s disposal, it’s pretty absurd to still be trying to blame upon a virus that which’s fault lies with public health response.
to do so is neither economically or epidemiologically accurate.
these are choices, not happenstance.
and it’s long past time to be making different ones.
Major Study Says Lockdowns Did More Harm Than Good – Well D’uh!

By Richie Allen | February 3, 2022
Lockdowns did far more harm than good. A new study published by Johns Hopkins University, in the US, Lund University, in Sweden and Denmark’s Centre for Political Studies found that lockdowns prevented just 0.2 per cent of deaths compared to letting people get on with their lives.
According to The Telegraph :
Researchers from Johns Hopkins University, in the US, Lund University, in Sweden and the Centre for Political Studies, in Denmark, said the costs to society far outweighed the benefits and called for lockdown to be “rejected out of hand” as a future pandemic policy.
The team even found that some lockdown measures may have increased deaths by stopping access to outdoor space, “pushing people to meet at less safe places” while isolating infected people indoors, where they could pass the virus on to family members and housemates.
“We do find some evidence that limiting gatherings was counterproductive and increased Covid-19 mortality,” the authors concluded. “Often, lockdowns have limited people’s access to safe outdoor places such as beaches, parks, and zoos, or included outdoor mask mandates or strict outdoor gathering restrictions, pushing people to meet at less safe indoor places.”
This isn’t earth-shattering. In March 2020, when the first lockdown was implemented, many doctors and healthcare workers warned that locking down would be ineffective against an airborne virus and that the measure would be devastating for public health.
They weren’t just ignored, they were banned by the mainstream media. I featured many of them on The Richie Allen Show.
Look, the government and its scientific advisers knew that lockdowns would be ineffective and dangerous. The policy wasn’t pursued in the interest of public health, rather it was implemented in the interest of public coercion.
The events of the last 22 months have nothing to do with a virus and all to do with mRNA drugs. They grossly exaggerated the threat of covid-19 and forced the world into lockdown after lockdown, to push their experimental jabs.
The major new study on the ineffectiveness and danger of lockdowns concludes thus:
“Lockdowns during the initial phase of the Covid-19 pandemic have had devastating effects. They have contributed to reducing economic activity, raising unemployment, reducing schooling, causing political unrest, contributing to domestic violence and undermining liberal democracy.
These costs to society must be compared to the benefits of lockdowns, which our meta-analysis has shown are marginal at best. Such a standard benefit-cost calculation leads to a strong conclusion: lockdowns should be rejected out of hand as a pandemic policy instrument.”
Featured Video

Seyed M. Marandi: Morocco Invades Spain?
or go to
Aletho News Archives – Video-Images
Book Review
Truth Lost, Truth Found
A Review of “Finding Treblinka” by Caroline Sturdy Colls
By David Skrbina • Unz Review • July 30, 2026
Long ago, there was a small place in the Polish countryside where, it was said, up to 1 million human beings met their demise over the course of some 10 months. This small place, comprising only around 50 acres of land, was located about 1.5 miles from the small village of Treblinka (population circa 300). At this remote location, a handful of Germans built a facility in 1942—a transit camp, they called it—intended to temporarily house people undesirable to the German state, to disinfest them of dangerous disease-bearing pests, and then to ship them onward to various locations distant from that state; some of these people died in the camp, some would later be put to forced labor, and others would be simply released in far-flung regions. Sadly, due to the tremendous military struggle of that time and to the eventual defeat of the German state, nearly all of these people were lost to the Western world, never to be heard from again.
As a result of these unfortunate events, the Treblinka Durchgangslager became known to the world as the Treblinka “death camp”—a place where as many as 1 million people (nearly all Jews) were said to have been killed by engine exhaust in specially-designed “gas chambers.” This action, it was said, was a direct consequence of an alleged German policy to kill every Jew in Europe. Thus, this small encampment became a central aspect of the (Jewish-designated) “Holocaust” in which, it is said, some 6 million Jews perished at the hands of the evil Germans.
It is a remarkable story. But is it true? … continue
Blog Roll
 Aletho News
Aletho News- Iran’s Petrochemical Industry Turns Sanctions Into Domestic Manufacturing Boom
- Iranian precision drones cripple US Patriot shield in Erbil, forcing a hasty American pullout
- Brazil approaches NATO and Israel to modernize its armed forces
- US punished Colombia’s outgoing leader for calling Gaza war ‘genocide’ – FM
- Claims of Iran agreeing to reopen Hormuz Strait are false: Report
- Ditch the Chemicals: 14 Herbal Oils Offering 50-87.5% UV Protection (SPF)
- The folk recipe that outperformed the leading pharmaceutical cough syrup in a randomized trial
- Seyed M. Marandi: Morocco Invades Spain?
- Big Tech On The Path To Net Zero — 2026 Edition
- Singapore police open probe over Palestinian flag displayed at Massive Attack concert
- If Americans Knew
- Settler violence is state violence in the West Bank
- In July, Israel killed 152 Gazans, more than any other “ceasefire” month – Daily Update
- As Gazans suffer, Israel says No to ceasefire package – Daily Update
- The Satanic Hazing Rituals of the IDF
- Israel Is Paying Millions to Train AI Chatbots How to Talk About Gaza. It’s Working.
- Right now, it’s all about what “Netanyahu wants” – Daily Update
- The Killing of Awdah Hathaleen: Beyond a Settler Crime
- Republican Voters are Turning against the Iran War
- Haley Stevens Is an Enemy of International Law
- Were the first Zionists Christian? A review.
- No Tricks Zone
- Analysis: Robert Koch Institute’s Heat Death Model Is “A Joke”… Deaths “Assumed” To Be Due To Heat
- New Research Finds Increasing CO2 Induces Cooling In The Lower Atmosphere Over The Arctic
- Germany’s Industrial Suicide… Grid Agency Prepares Secret Power Rationing Plans Amid Electric Power Bottlenecks
- ECMWF Models Throwing Cold Water On Extreme Germany Heat Wave Forecast Next Week
- Greenland’s Ice Sheet Was Supposed To Be Rapidly Melting Away. It Hasn’t Been.
- Global Temperature Trend Has Cooled Over The Past 6500 Years, Scientists Have Found
- Wind Energy Means Going Back To The Middle Ages, Says German Professor Horst-Joachim Lüdecke
- New Study: A 40-Fold Increase In Earth’s Main Greenhouse Gas Contributes To Cooling The Ocean
- New Study Highlights The ‘Dominant Role’ Of Aerosol/Cloud Interactions In Shaping Climate
- Munich’s First-Ever Green Party Mayor Declares First Ever City Water Use Restrictions… Fines Up to 50,000 €!
