Reports of Deaths, Injuries After COVID Vaccines Climb Steadily
By Megan Redshaw | The Defender | February 11, 2022
The Centers for Disease Control and Prevention (CDC) today released new data showing a total of 1,103,893 reports of adverse events following COVID vaccines were submitted between Dec. 14, 2020, and Feb. 4, 2022, to the Vaccine Adverse Event Reporting System (VAERS). VAERS is the primary government-funded system for reporting adverse vaccine reactions in the U.S.
The data included a total of 23,615 reports of deaths — an increase of 466 over the previous week — and 188,135 reports of serious injuries, including deaths, during the same time period — up 4,824 compared with the previous week.
Excluding “foreign reports” to VAERS, 753,482 adverse events, including 10,747 deaths and 70,746 serious injuries, were reported in the U.S. between Dec. 14, 2020, and Feb. 4, 2022.
Foreign reports are reports foreign subsidiaries send to U.S. vaccine manufacturers. Under U.S. Food and Drug Administration (FDA) regulations, if a manufacturer is notified of a foreign case report that describes an event that is both serious and does not appear on the product’s labeling, the manufacturer is required to submit the report to VAERS.
Of the 10,747 U.S. deaths reported as of Feb. 4, 18% occurred within 24 hours of vaccination, 23% occurred within 48 hours of vaccination and 60% occurred in people who experienced an onset of symptoms within 48 hours of being vaccinated.
In the U.S., 541.5 million COVID vaccine doses had been administered as of Feb. 4, including 318 million doses of Pfizer, 205 million doses of Moderna and 18 million doses of Johnson & Johnson (J&J).

Every Friday, VAERS publishes vaccine injury reports received as of a specified date. Reports submitted to VAERS require further investigation before a causal relationship can be confirmed. Historically, VAERS has been shown to report only 1% of actual vaccine adverse events.
U.S. VAERS data from Dec. 14, 2020, to Feb. 4, 2022, for 5- to 11-year-olds show:
- 7,724 adverse events, including 170 rated as serious and 3 reported deaths.
The most recent death involves a 7-year-old girl (VAERS I.D. 1975356) from Minnesota who died 11 days after receiving her first dose of Pfizer’s COVID vaccine when she was found unresponsive by her mother. An autopsy is pending.
- 16 reports of myocarditis and pericarditis (heart inflammation).
- 29 reports of blood clotting disorders.
U.S. VAERS data from Dec. 14, 2020, to Feb. 4, 2022, for 12- to 17-year-olds show:
- 28,793 adverse events, including 1,651 rated as serious and 38 reported deaths.
The most recent deaths involve a 13-year-old male (VAERS I.D. 2042005) from an unidentified state who died from a sudden heart attack seven months after receiving his second dose of Moderna, and a 17-year-old female from an unidentified state (VAERS I.D. 2039111) who died after receiving her first dose of Moderna. Medical information was limited and it is unknown if an autopsy was performed in either case.
- 68 reports of anaphylaxis among 12- to 17-year-olds where the reaction was life-threatening, required treatment or resulted in death — with 96% of cases attributed to Pfizer’s vaccine.
- 629 reports of myocarditis and pericarditis with 617 cases attributed to Pfizer’s vaccine.
- 155 reports of blood clotting disorders, with all cases attributed to Pfizer.
U.S. VAERS data from Dec. 14, 2020, to Feb. 4, 2022, for all age groups combined, show:
- 19% of deaths were related to cardiac disorders.
- 54% of those who died were male, 41% were female and the remaining death reports did not include the gender of the deceased.
- The average age of death was 72.6.
- As of Feb. 4, 5,038 pregnant women reported adverse events related to COVID vaccines, including 1,615 reports of miscarriage or premature birth.
- Of the 3,531 cases of Bell’s Palsy reported, 51% were attributed to Pfizer vaccinations, 40% to Moderna and 8% to J&J.
- 858 reports of Guillain-Barré syndrome (GBS), with 40% of cases attributed to Pfizer, 30% to Moderna and 28% to J&J.
- 2,316 reports of anaphylaxis where the reaction was life-threatening, required treatment or resulted in death.
- 1,576 reports of myocardial infarction.
- 12,981 reports of blood clotting disorders in the U.S. Of those, 5,780 reports were attributed to Pfizer, 4,627 reports to Moderna and 2,527 reports to J&J.
- 3,950 cases of myocarditis and pericarditis with 2,427 cases attributed to Pfizer, 1,343 cases to Moderna and 169 cases to J&J’s COVID vaccine.
Pfizer and BioNTech delay request to authorize vaccine for children under 5
Pfizer and BioNTech announced today they are delaying their request to the FDA to authorize the Pfizer-BioNTech COVID vaccine for children under five years old, citing not enough data on the efficacy of a third dose.
The FDA said its advisory panel meeting scheduled for next week will be postponed. Pfizer was originally expected to publish an analysis of its data today.
Pfizer said it will wait for its data on a three-dose series of the vaccine — expected in April — because it believes three doses “may provide a higher level of protection in this age group.”
Pfizer said in December 2021 that two doses of its Pfizer-BioNTech vaccine failed to generate a strong immune response during its clinical trial of children ages 2 to 4.
For children aged 6 months to 5, Pfizer’s vaccine has a dosage of 3 micrograms. For children ages 5 to 11, the dosage is 10 micrograms.
Despite the results of its trial, the company asked the FDA this month to authorize these first two doses, with a plan to submit additional data in the coming weeks on a third dose, NBC reported.
As The Defender reported Wednesday, some experts speculate the push to expand the authorization to the younger age group would lay the groundwork for subsequently folding COVID shots into the childhood vaccine schedule — thereby ensuring “liability protection forever.”
6-year-old gets myocarditis, can’t walk, after receiving COVID vaccine
Milo Edberg, 6, has been intubated and hospitalized since receiving his COVID vaccine on Dec. 10, Alpha News reported.
Edberg’s mother, Carrie, said her son was at M Health Fairview’s Masonic Children’s Hospital in Minneapolis, Minnesota for a minor procedure when a doctor recommended he receive the COVID vaccine.
Carrie said she followed the advice of her doctor, who told her the vaccine was “safe and harmless.”
“I went against my gut and said OK, do it,” she said.
Carrie said the evening after receiving the shot, her son was gasping for air. She dialed 911. Edberg was transported back to the hospital, was intubated and diagnosed with myocarditis.
He was “perfectly fine and then he wasn’t,” Carrie said. He was “eating on his own [but] now he can’t even swallow his saliva.”
Doctors have no answers and cannot explain her son’s affliction, Carrie said. They haven’t even been able to provide a timeline for when her son might return home or whether he will regain any quality of life — and they “won’t bring up the vaccine” when discussing Edberg’s situation.
Carrie filed a VAERS report in January and said her son received a 10-15 minute visit from an infectious disease specialist who said they would file a report with the CDC and and Pfizer early in his hospital stay. She has heard nothing since.
The CDC maintains most cases of myocarditis after COVID vaccines are “mild” and patients recover quickly.
Not all doctors agree. As Dr. Steven Pelech of the University of British Columbia explained last August:
“Contrary to what a number of people have said, there is no such thing as ‘mild myocarditis.’ It’s the destruction of the myocytes, the heart cells that contract. When those cells die, they are not replaced in your body and are instead replaced by scar-tissue, which is from fibroblasts — skin cells which don’t have contractile activity …Every time you get an inflammatory response, you lose more of that contractility and have a greater chance of heart attack and other problems later in life.”
A New Zealand writer observed that “mild” clinical manifestations in the present are meaningless for interpreting longer-term risks.
Using magnetic resonance imaging (MRI) scans with gadolinium contrast — capable of showing “damaged heart areas undetectable by any other means” — studies of children and adolescents who developed myocarditis following COVID vaccination revealed, in the vast majority, a “potentially poor prognosis despite the heart seeming to have returned to normal.”
Kansas woman died from allergic reaction to Moderna’s COVID vaccine
Jeanie Evans, 68, of Effingham, Kansas, died of “anaphylaxis due to COVID-19 vaccination,” according to her autopsy report acquired by the Topeka Capital-Journal.
Evans died March 24, 2021, one day after her first dose of Moderna’s vaccine.
According to the autopsy report, Evans said her airway felt blocked about 15 to 20 minutes after she received her first dose on March 23, 2021. She was taken by ground ambulance at 5:21 p.m. to Stormont-Vail hospital, where she died at 11:55 a.m. the next day.
Evans had a medical history of hypertension, environmental allergies, allergic disorders and reactive airway disease. She previously experienced an anaphylactic reaction to the drug Albuterol, the report said.
Colt Umphenour, one of Evans’ sons, said the family plans to file a lawsuit.
Denmark officials see no reason to continue COVID vaccine program
Health authorities in Denmark announced Friday they are considering “winding down the entire general vaccination program later in the spring.”
According to the Associated Press, officials see no reason to administer a booster dose to children or a fourth shot to residents at risk of severe COVID.
The Danish Health Authority said in a statement the third wave of COVID was waning “due to the large population immunity,” and the country can cope with increasing infection without getting serious illness.
The agency said it would continue to follow the epidemic closely should there be a fourth spring wave or new worrying variants.
Denmark ended most of its pandemic restrictions earlier this month after officials said they no longer considered COVID “a socially critical disease.”
Children’s Health Defense asks anyone who has experienced an adverse reaction, to any vaccine, to file a report following these three steps.
Megan Redshaw is a freelance reporter for The Defender. She has a background in political science, a law degree and extensive training in natural health.
© 2022 Children’s Health Defense, Inc. This work is reproduced and distributed with the permission of Children’s Health Defense, Inc. Want to learn more from Children’s Health Defense? Sign up for free news and updates from Robert F. Kennedy, Jr. and the Children’s Health Defense. Your donation will help to support us in our efforts.
The extraordinary story of how patient access to COVID treatments were denied
Eventually involving witch hunts of physicians who dared to treat patients
By Meryl Nass, MD | February 11, 2022
In 2020, I compiled a list of over 50 ways authorities and pharma companies in multiple countries stopped the use of the chloroquine drugs for COVID. This was (and is) a stunning collection,which has been widely read and reproduced on many websites. When you read it, you are astounded to learn that all the US (and many international) public health agencies took many different actions to increase deaths and destruction from COVID and prolong the pandemic. “Avoiding the Trump drug” served as a great cover story. Taking hydroxychloroquine for COVID was equated to drinking bleach.
But here’s the kicker: the authorities knew all about chloroquine and other treatments for COVID before there was a COVID… because they had figured it out for the 2002 SARS epidemic and the 2012 MERS epidemic, both caused by related coronaviruses. But they hushed it up.
Five CDC (US government) scientists published a paper, along with three Canadian government scientists, showing that chloroquine was an effective drug against SARS coronaviruses, in 2005. European scientists had shown the same thing in 2004.
Here is the CDC paper:

and here is its conclusion:

It looked very promising for both prevention and treatment of the first SARS. After all, it has been used for many decades both to prevent and to treat malaria. (I took it for prevention, and later for treatment, 50 years ago.)
Nine years later, In 2014, scientists in Tony Fauci’s NIAID showed the same thing. Not only did chloroquine work in vitro against the MERS coronavirus, but dozens of existing drugs, which could have been tested in patients as soon as the pandemic started, were also effective against SARS and MERS coronaviruses.
Here is the paper from Fauci’s NIAID:

And this is what the NIAID authors said:
Here we found that 66 of the screened drugs were effective at inhibiting either MERS-CoV or SARS-CoV infection in vitro and that 27 of these compounds were effective against both MERS-CoV and SARS-CoV. These data demonstrate the efficiency of screening approved or clinically developed drugs for identification of potential therapeutic options for emerging viral diseases and also provide an expedited approach for supporting off-label use of approved therapeutics.
Just in case you think these papers were flukes, two unrelated groups of European scientists found essentially the same thing. The 2014 European paper was published back to back with the NIAID paper above. I have cited the 2004 European paper elsewhere, and these citations can also be found in Bobby Kennedy’s book The Real Tony Fauci, which according to Amazon has now sold over 800,000 copies. Please read it. OTOH, If you are seeking misinformation on COVID, I’d recommend Fauci’s own book, Expect the Unexpected.
I have to repeat myself, because the information is so shocking and I don’t want you to miss it: our governments already knew of options for treating COVID before it appeared, but instead of immediately trying these already identified, safe, cheap, and available repurposed drugs, and offering early treatments, they did everything they could to stop people obtaining the chloroquine drugs. Look up the articles I linked to above. Read my long article on this suppression. Or the two articles I wrote here and here about how patients were administered borderline lethal doses of hydroxyhcloroquine to give the drug a black eye. Check the links. Verify that what I have just written is correct. Human beings planned and carried out these medical crimes against humanity. Who are those humans? What are they doing now?
This has to be be investigated and justice attained, to prevent such crimes from happening to patients ever again.
The “Why?” and “How could this be?!!” requires people to take a huge leap in order to understand the world we live in. Many don’t have the fortitude to dissect their world view and rebuild it in accord with the facts that have spilled out over the last two years.
But I am about to present some more facts that I hope you can assimilate into your understanding of the world. It might require a stiff drink, or perhaps some chocolate. Whatever it takes, read on, as it might save your life or someone else’s.
Ivermectin
Ivermectin had not been identified in the studies I mentioned above as a potentially useful coronavirus drug.
But some people knew it was likely to work in early 2020, because the French MedInCell company, supported by Bill Gates, was working on an injectable (which would make it patentable) version of ivermectin for COVID, issuing a press release about this on April 6, 2020 and an informational paper on April 23, 2020. There was a brief run on the veterinary drug at this time in the US, according to an FDA warning issued on April 10, 2020, indicating some people knew it might be an effective COVID treatment and were acquiring it. But there was not a lot of buzz and sales did not take off at that time.
Here is what FDA said on April 10, 2020:
FDA is concerned about the health of consumers who may self-medicate by taking ivermectin products intended for animals, thinking they can be a substitute for ivermectin intended for humans… Please help us protect public health by alerting FDA of anyone claiming to have a product to prevent or cure COVID-19 and to help safeguard human and animal health by reporting any of these products
In December 2020, a full eight months later, Ron Johnson held a Senate hearing that was focused on ivermectin’s benefits for COVID. Intensive care specialist Dr. Pierre Kory, originally a New Yorker, gave a particularly compelling speech. People began paying attention to the drug. YouTube then removed Kory’s speech–censoring a Senate hearing!
I think the authorities were initially scared to repeat the same tricks with ivermectin they had used to beat down the chloroquine drugs. And because ivermectin has efficacy late in the disease as well as at the start, and is not toxic at several times the normal dose, some of the tricks used against chloroquine (giving it too late in the disease course or overdosing patients) simply would not work with ivermectin. The authorities kept quiet.
But then ivermectin’s popularity started exploding. CDC published a report in late August showing that ivermectin prescriptions had quadrupled in a month, and the drug was now selling at 25 times the pre-COVID rate.
IVERMECTIN PRESCRIPTIONS SOLD by WEEK, 2019-21

Apparently this terrified the powers-that-be. What if the pandemic got wiped out with ivermectin? It worked too well! Would that be the end of vaccine mandates, boosters, vaccine passports and digital IDs? The end of the Great Reset? Something had to be done, and fast. It had to be big. It had to be effective. They couldn’t simply take the drug off the market; that would require a long process and a paper trail.
What to do? There was probably only one option: Scare the pants off the doctors. Loss of license is the very worst thing you can do to a doctor. Threaten their licenses and they will immediately fall into line. You can’t get a prescription if there is no doctor to write it.
The method had been tested in the Philippines.
The powers-that-be could also scare the pharmacies. This required stealth. No paper trails. Intimidation was required, backed by a one-two punch: actually suspending doctors’ (annd maybe pharmacists’) licenses. You couple that with a huge media offensive, and threats from an industry of medical “non-profits.” You suddenly invent “misinformation” as a medical crime, studiously failing to define it. You make people think the legal prescribing of ivermectin and hydroxychloroquine is a crime, even though off-label prescribing is entirely legal under the federal Food, Drug and Cosmetic Act.
Did Fauci give the order? Walensky? Acting FDA Commissioner Woodcock? It was probably some combination, plus the public relations professionals managing the messaging and the media.
Here’s what happened.
1. Senator Ben Ray Lujan (D, NM) and several other Senators introduced the “Health Misinformation Act” in July 2021 because “misinformation was putting lives at risk,” he said. A huge supporter of COVID vaccinations, the 49 year old Senator suffered a stroke on February 1, 2022.
2. The pharmacies suddenly could not get ivermectin from their wholesalers. No reason was given except ‘supply and demand.’ But it seemed the supply was cut off everywhere. Ivermectin was dribbled out by the wholesalers, a few pills a week per pharmacy, not enough to supply even one prescription weekly. Some powerful entity presumably ordered the wholesalers to make the drug (practically) unavailable. With no shortages announced. I called the main manufacturer in the US, Edenbridge, and was told they were producing plenty.
Hydroxychloroquine had been restricted in a variety of ways, determined by each state, since early 2020. It had also been restricted by certain manufacturers in 2020. Suddenly, in September 2021, it too became considerably harder than it already was to obtain.
3. In late August, CDC sent out a major warning about ivermectin, but only gave 2 examples of anyone having a problem with the drug: one person overdosed on an animal version and one overdosed on ivermectin bought on the internet. This should not have been news. However, pharmacists and doctors read between the lines and knew this was code for “verboten.” Almost all stopped dispensing ivermectin at that time. It should be of interest to everyone that our health agencies now speak in coded messages to doctors and pharmacies, presumably to avoid putting their threats on paper and being accountable for them. What a way for government to do business.
4. Also last August, various “nonprofit” medical organizations started issuing warnings, in concert, regarding doctors prescribing ivermectin or hydroxychloroquine, and spreading misinformation, especially about COVID vaccines. These organizations included the Federation of State Medical Boards, the American Medical Association, the American Pharmacy Association, and several specialty Boards. Here is an example of the AMA’s language:
“A handful of doctors spreading disinformation have fostered belief in scientifically unvalidated and potentially dangerous “cures” for COVID-19 while increasing vaccine hesitancy…”
These organizations told doctors they could lose their licenses or board certifications for such “crimes.” Mind you, none of these so-called nonprofit organizations has any regulatory authority. Nor do I believe they have any authority to claw back a Board Certification. They were blowing smoke. And they were probably paid to do so. Who paid?
5. Over the course of 3 days at the end of August, national media reported on 4 doctors in 3 states whose Boards were investigating them for the use of ivermectin.
Hawaii’s Medical Board went after Hawaii’s chief medical officer:
The Hawaii Medical Board has filed complaints against Maui’s top health official and a Valley Isle physician following reports that they backed COVID-19 treatments that state and federal health agencies advise against.
They really wanted to make an example by going after the state’s chief medical officer, who had had the guts to treat COVID patients. Clearly the orders are coming from high up on the food chain.
Here were some of the other August headlines about doctors who legally prescribed a fully approved drug off-label:

6. The Federation of State Medical Boards (FSMB) is an organization that assists 71 state and territorial medical boards with policies, training, etc. Members pay dues and the organization accepts donations. It has its own foundation, too. Its President earns close to $1,000,000/year, not bad for a backwater administrative job at an organization headquartered in Euless, Texas. After the FSMB instructed its members that misinformation was a crime, somewhere between 8 and 15 of its member boards began to take action. (Media have reported that 8, 12 or 15 boards of its 71 member Boards did so, according to the FSMB, which is closely monitoring this.)
7. On February 7, 2022 the Department of Homeland Security issued its own dire warning about the spread of misinformation, disinformation and a neologism, malinformation.
“The United States remains in a heightened threat environment fueled by several factors, including an online environment filled with false or misleading narratives and conspiracy theories, and other forms of mis- dis- and mal-information (MDM) introduced and/or amplified by foreign and domestic threat actors. These threat actors seek to exacerbate societal friction to sow discord and undermine public trust in government institutions to encourage unrest, which could potentially inspire acts of violence. Mass casualty attacks and other acts of targeted violence conducted by lone offenders and small groups acting in furtherance of ideological beliefs and/or personal grievances pose an ongoing threat to the nation.
Thus it appears that Misinformation and Disinformation have been selected to play an important role in a newly developing narrative, as the Pandemic restrictions and narrative come to an end.
8. I presume the majority of the 71 Medical Boards’ attorneys knew something about the Constitution, knew that every American has an inalienable right to freedom of speech, and simply ignored the FSMB’s exhortation to go after misinformatin spreaders. The Maine Board, however, went along. Three doctors in Maine have recently had their licenses suspended or threatened for writing waivers for COVID vaccines, spreading misinformation, and/or prescribing ivermectin and hydroxychloroquine. (All three of which are legal activities for doctors.). But Boards have broad powers to intervene, and are shielded from liability as agents of the state. So they went after a chronic Lyme doctor several years ago, who found, as expected, that it would be too onerous to fight back, and he gave up his license.
9. Here is what the Board claims about me:
“The board noted that Ivermectin isn’t Food and Drug Administration “authorized or approved” as a treatment for COVID-19 in the suspension order.”
“The board said that her continuing to practice as a physician “constitutes an immediate jeopardy to the health and physical safety of the public who might receive her medical services, and that it is necessary to immediately suspend her ability to practice medicine in order to adequately respond to this risk.”’
I am 70 years old, and my medical practice was set up as a service, so that everyone could access COVID drugs who wanted them. My fee was $60 per patient for all the COVID care they needed.
I am sure the Board had calculated that given all the above, I would not challenge the Board’s suspension and would simply surrender my license, since it would probably cost hundreds of thousands of dollars to fight the Board’s actions in court.
On the day my license was suspended, there was massive national publicity about my case. The story was on the AP wire, covered from the San Francisco Chronicle to the Miami Herald. And for some reason, it was not behind the usual paywall. The Hill, Newsweek, the Daily Beast and many other publications all ran hit pieces about me.
I realized that my situation was bigger than just a Maine issue: it had been selected to serve as an example to physicians nationwide who might be thinking for themselves and prescribing early treatment for COVID. Once I realized I was to be made an example of, as part of a national purge of doctors who think independently, I decided to fight back. Fortunately, Children’s Health Defense is helping with my legal expenses, which is what allows me to mount a strong attack against the bulldozing of free speech, patient autonomy and the doctor-patient relationship. Please join me in the fight!
Try as They Might, Facebook ‘Fact-Checkers’ Cannot Refute the Dire Scottish Vaccine Data
By Thorsteinn Siglaugsson | The Daily Sceptic | February 10, 2022
Ever since I realised the devastating effects lockdowns would have all over the world, I have actively fought them. My first task, in October 2020, was hosting an interview with world-renowned epidemologist Martin Kulldorff, one of the authors of the Great Barrington Declaration, which argues for focused protection instead of blanket lockdowns.
Incidentally, Kulldorff was involved also in my first really memorable encounter with the so-called fact-checkers. Last summer the Icelandic Chief Epidemiologist said in an interview he believed herd immunity would never be reached by vaccination, only through infections. I posted a link to the interview on LinkedIn. Kulldorff shared my post, and the next thing he knew his reshare had been removed. Clearly a fact-checker hadn‘t liked what our Chief Epidemiologist said, and decided the public shouldn‘t know.
Part of my activities as an active lockdown sceptic has been managing a large and fast-growing local Facebook group, dedicated to providing a broad view of the Covid situation, including negative effects of lockdowns, and later on, growing concerns with the effectiveness and safety of mass-vaccination. This is a difficult task as we must always be very careful not to accept posts that for some reason contain material that doesn‘t comply with the worldview of the fact-checkers. We get a few strange conspiracy theories of course, but mostly the material we have to reject is simply inconvenient facts or well-argued opinions, even by respected scientists, that just happen to go against the official narrative.
Fact-checking is nothing new, and until recently it was just that, checking for facts. But since very early in the pandemic, fact-checkers have become less concerned with facts, but more, and in some cases exclusively, with censoring anything that goes against their own opinions. Every day, hundreds of such articles are published and then used to justify censorship. The following example is a typical one.
Recently, official Scottish data has shown COVID-19 infections, hospitalisations and deaths are becoming more frequent among the double-vaccinated than the unvaccinated. The latest report shows the infection rate among the double-jabbed is now double the rate for the unjabbed, and 50% higher for the triple-jabbed. Hospitalisations are higher among the double-jabbed than the unjabbed and the death rate is double. This is a concerning development and has garnered some attention from those who follow such statistics. I wrote a short Facebook post on this the other day, quoting an article discussing this development. A few days later the familiar warning of ‘false information’ had been slapped on my post.
I decided to follow up on the ‘fact check’ referred to in the warning, an article by Mr. Dean Miller, managing editor at Lead Stories, one of the agencies that frequently publish articles used to justify censorship. Mr. Miller holds an undergraduate degree in English and seems to have no science training whatsoever.
Mr. Miller begins by claiming there is a consensus among health statisticians “working independently” that vaccination reduces the probability of hospitalisation and death, and that as the vaccinated tend to be older than the unvaccinated, “amateur statisticians” often reach false conclusions based on official data. Mr. Miller then quotes an epidemiologist who suggests various factors that “may” affect the numbers. First, that the vaccinated are more likely to get tested, quoting test and trace data but providing no reference. Second, that the vaccinated tend to be older than the unvaccinated and therefore more vulnerable in general. Third, that the vaccinated may behave differently from the unvaccinated when it comes to social interactions. Fourth, that the unvaccinated are more likely to have been previously infected by the virus.
None of this is necessarily untrue. But the article provides no references showing that vaccinated people behave differently from unvaccinated people, which would make them more likely to come into contact with infected persons. We also have no way of determining if the opposite is true. In other words, this is pure speculation, for which no evidence is provided. Whether vaccinated people are more likely to get tested is speculative also and there is no data provided to back up this claim. The same goes for the claim that the unvaccinated are more likely to have been previously infected. In fact, as numerous studies have already demonstrated that infection provides strong and lasting protection, this suggestion seems highly unlikely.
So, three of Mr. Miller‘s arguments are pure speculation, unquantified and not supported by any evidence. But what about the last argument, that the vaccinated tend to be older and therefore more likely to be hospitalised or to die? This certainly looks like a valid point, since we know it is primarily the elderly who become seriously ill with COVID-19. But how valid, or relevant is this really?
To start with, being vulnerable to serious illness or death if infected has nothing to do with the probability of infection. Rather than increasing it, it might rather decrease it, as a vulnerable person might be more likely to avoid situations where they are likely to get infected. As for hospitalisation and death, the data presented in the Public Health Scotland reports is in fact age-standardised. This means the age-related probability of death is already accounted for in the statistics. Mr. Miller‘s key argument, and the only one that isn‘t purely speculative, is therefore simply invalid. It seems he either failed to familiarise himself with the methodology used, or did not understand what it entails.
The weakness of Mr. Miller‘s argumentation does not however stop him from categorically denying that comparison of infection rates is a valid indicator of vaccine effectiveness. And of course it does not prevent the media and social media using his claim, based on speculation and lack of basic understanding of the data, to censor the discussion of a disturbing development that most certainly calls for thorough investigation.
When I showed the data to a Scottish friend recently, he suggested it was of no relevance for other nations, as the Scots were genetically different from other people due to a long-standing diet of nothing but chips, Marlboros and Irn-Bru. I can only say his explanation makes just as much sense as Mr. Miller‘s do.
But Scotland is not the only country experiencing this disturbing trend. A couple of weeks ago I published an article in the Daily Sceptic discussing a similar trend in Iceland: early January data showed the double-vaccinated to be twice as likely to get infected as the unvaccinated. This undermines the aforementioned dietary explanation, as in Iceland we boil our potatoes, smoke Camels rather than Marlboros and Irn-Bru has never been available. No ‘fact check’ has yet been published trying to invalidate this data. However the already published infection rate for the unvaccinated suddenly rose by 20%, without explanation, soon after this development was pointed out.
Unfortunately Mr. Miller‘s article is not the only example of a ‘fact check’ that ignores or distorts the facts, or counters hard data with pure speculation. This sloppy kind of reporting seems to be the fact-checkers’ standard way of working when it comes to the pandemic. Some have even admitted their fact-check labels are nothing but opinion. And the general press is no exception. For example, the Scottish Herald recently published an article on this subject, also failing to acknowledge the fact that the data is age-standardised.
It is a noble endeavour to try to make sure facts rather than fiction influence public opinion. But unfortunately, it looks as if the champions of ‘fact-checking’ have little respect for facts. Most of the material they produce consists of low quality, highly opinionated articles, lacking not only references, but more importantly the clarity of thinking that must be required of anyone who takes upon themselves the important and difficult task of deciding what is true and what isn‘t.
Thorsteinn Siglaugsson is an economist who lives in Iceland. Find him on his blog.
Lawmakers take heat for flip-flopping on mask mandates
RT | February 10, 2022
Republican lawmakers have slammed their Democratic opponents for suddenly speaking in favor of lifting mask mandates, especially in schools, saying that the switch is just an attempt to boost their chances in the midterm elections.
Democrat-led New Jersey, New York, California, Oregon, Connecticut, and Delaware announced plans to roll back their mask requirements on Tuesday and Wednesday, with Illinois soon expected to join them.
The issue has been a major bone of contention between the two rival American parties during the pandemic. The Democrats have always defended face coverings as an essential measure to stop the spread of Covid-19, while the Republicans insist that the measure is of little use, especially for students, who face a much lesser risk of serious coronavirus infection due to their young age.
“I’d love to see whatever internal polling went around the Democrat Party last week – it’s certainly no coincidence that Democrat-run states are dropping mandates as fast as they can,” Rep. Kevin Hern, R-Okla., told the Daily Mail about the plans by Democratic governors to lift their mask requirements.
Hern was fully backed by Rep. Lisa McClain, R-Mich., who claimed that “the Democrats continually follow the political science instead of the actual science.”
“We’ve known for months that masking has been detrimental to our children. The science hasn’t changed in the last several months, the only change has been the overwhelming uproar over government mandates,” she said.
Rep. Andy Biggs, R-Ariz, said it was “no surprise” that the Democrats have now decided to give up on mask mandates. “They had every intention of using Covid mandates to their advantage – especially when it comes to the polls – and have perfected playing politics in our everyday lives.”
However, Rep. Dan Bishop, R-N.C., suggested that the switch will likely be too little, too late. “Democrats forced masks on kids for two years and now they’re hoping that the rest of America will suddenly forget.”
The midterm elections, scheduled to take place in the US in November, are expected to be a tough test for the Democratic Party. Last month, a poll by Gallup revealed that 47% of Americans identified themselves as Republicans, compared to 42% as Democrats. The news figures contradicted the historic trend of Democrats outnumbering GOP supporters in the country.
The Centers for Disease Control (CDC) said earlier this week that the number of cases and hospitalization in the US was still “too high” to think about lifting Covid-19 restrictions, adding that it continued to endorse universal masking in schools.
On Tuesday, CNN’s medical analyst, Dr. Leana Wen, who has always been a strong supporter of mask mandates, urged the CDC to follow the example of the Democratic states and lift the curbs.
“The CDC has already lost a lot of trust and credibility. This is their time to rebuild and remove restrictions as quickly as they were put in,” she argued.
Wen defended her new stance on face coverings by claiming that “circumstances have changed. Case counts are declining. Also, the science has changed.”
She faced a harsh backlash online, with prominent journalist Glenn Greenwald, who was among the critics, insisting that behavior like Wen’s was the reason behind the public loss of trust in what the medical experts have to say.
“As others noted, there is nothing in The Science™ that changed to justify Dem politicians suddenly ending mask mandates. All that changed is the political fear they have. Conflating ‘The Science’ with politics like this is a key reason many lost trust in public health experts.”
Valieva ‘repeatedly passed doping tests’ before and after positive result – ROC

RT | February 11, 2022
Figure skater Kamila Valieva passed doping tests in the period before and after the positive result announced on Friday, including returning negative tests at the Beijing Olympics, the Russian Olympic Committee (ROC) has said.
Valieva is fighting for the right to remain at the Beijing Games after the International Testing Agency (ITA) announced that the 15-year-old had tested positive for a banned substance detected in a sample from December 25.
The sample was taken during the Russian national championships, and was sent to a laboratory in Stockholm accredited by the World Anti-Doping Agency (WADA).
Tests found the presence of the banned heart medicine trimetazidine, but the result was only reported on February 8 – one day after Valieva had won gold with the ROC in the figure skating team event in Beijing.
Valieva was provisionally suspended by the Russian Anti-Doping Agency (RUSADA), but had that decision reversed upon appeal on February 9, freeing her to train and compete.
However, the International Olympic Committee (IOC) and International Skating Union (ISU) are both challenging the ruling with the Court of Arbitration for Sport (CAS), which is set to hear the case before Valieva is due to compete in the ladies’ singles event in Beijing on Tuesday.
In a statement on Friday, the ROC confirmed the positive test, but affirmed that it had taken place outside the Beijing Games.
“The doping test of the athlete [Valieva] who tested positive does not apply to the period of the Olympic Games,” read an ROC message.
“At the same time, the athlete [Valieva] repeatedly passed doping tests before and after December 25, 2021, including at the European Championships [in January] and already in Beijing during the figure skating tournament. All the results were negative.”
The ROC added that due procedure had been followed when the disciplinary commission of the Russian Anti-Doping Agency (RUSADA) decided to lift the initial suspension, but noted that the IOC and ISU also have the right to appeal that decision with CAS.
“At present, the athlete has the right to train and compete in full without restrictions until the Court of Arbitration for Sport decides otherwise regarding her status in relation to the Olympic Games,” the ROC added.
Concerning the status of the ROC’s gold medal in the figure skating team event – where the medal ceremony has been delayed – the Russian statement added: “Given that the athlete’s positive doping test was not taken during the Olympic Games, the results of the athlete and the results of the team tournament during the Olympic Games are not subject to automatic review.”
Separately, ROC president Stanislav Pozdnyakov has questioned the timeframe surrounding Valieva’s case, asking why it took until after the figure skating team event in Beijing for the result to be announced, when the sample was taken back in December.
Led by Valieva, the ROC team had beaten the USA and Japan to gold in China, with Canada down in fourth.
A CAS panel is expected to hold an expedited hearing on Valieva’s case ahead of the ladies’ singles event on Tuesday.
The drug in question, trimetazidine, is used to treat angina or chest pain, but has been on the WADA banned list since 2014.
In an advisory note in 2018, WADA noted that trimetazidine – also known as TMZ – could be detected in urine samples as a false positive for lomerizine, a migraine medication which is permitted.
Some have questioned how trimetazidine could be used as a performance-enhancing drug, particularly in a sport like figure skating.
“Why it’s being considered as doping is not clear to me,” Yaroslav Ashikhmin, a member of the European Society of Cardiology and the American Heart Association, told RT.
“I personally use it extremely rarely, even in treatment, since its effect is not strong enough, it just slightly affects the heart function. You can say that it is a heart vitamin. Of course, it is a complete mess with doping control if this drug is identified as doping.”
The Russian figure skating federation said it has “no doubts” that Valieva is a clean athlete, adding that it will “make every effort to clarify the circumstances of the incident.”
Meanwhile, Valieva continues to train along with teammates Alexandra Trusova and Anna Shcherbakova, ignoring questions from the media after completing a session on Friday.
The UK wants to criminalize “misinformation” online as its own health service gets caught posting falsehoods
By Dan Frieth | Reclaim The Net | February 11, 2022
Less than a week after the UK proposed criminalizing the posting of some types of “knowingly false” information online, England’s National Health Service has taken down a social media video over inaccurate information.
Last week, NHS England posted a video on its Twitter account with more than half-a-million followers to promote vaccination in kids.
The video claimed that 1% of children will be hospitalized because of Covid, 136 kids in the UK had died because of Covid, and 117,000 children have “long Covid.”
The video went viral attracting comments and retweets from some of the most popular influencers in the health category.
But some, including Dr. Robert Hughes, a clinical research fellow at the London School of Hygiene & Tropical Medicine, questioned the accuracy of the data.
“As both a parent and scientist who has been involved in research on symptom duration and severity of covid in children, the cited statistics didn’t make sense to me,” Hughes wrote in an article in UnHerd. “The idea that 1% of children with Covid are hospitalized for it didn’t pass the ‘sniff test.’”
The video also shared the story of a kid aged 11 that was suffering from long Covid. According to Hughes, the story contradicted the vaccination guidance in the UK, as it does not even recommend vaccination for that age group.
Additionally, there is not yet any substantial evidence to support that the vaccine prevents long Covid.
Hughes also notes that NHS England was silent when he and others questioned the accuracy of the data.
“Several people agreed with me, sharing their working for why these numbers are at best long outdated, may be orders of magnitude out, and risk undermining confidence in vaccine communications and uptake.
“But others seemed to dig in, praising both the content and tone of the messaging when challenged, and directing the discussion into an important, but different, one about the merits of extending Covid vaccination to children rather than the need for accurate and honest communication about vaccination,” Dr. Hughes wrote for UnHerd.
Hughes contacted the Office of the Statistics Regulator about the numbers. The Statistics Regulator agreed that it was important that the NHS provides accurate figures.
“It is important that figures provided by NHSE&I are accurate and reliable,” the Office of the Statistics Regulator said. “In this case the claim made in the video fell short of these expectations – we contacted NHSE&I and it acknowledged that the data were historic and had methodological shortcomings. We are therefore glad that the content has now been removed from Twitter.”
Before its removal, the video had already been widely shared.
News articles on heart attacks. Why are there so many recently?
The Naked Emperor’s Newsletter | February 7, 2022
Why are there so many articles on heart attacks recently?
There have always been articles, now and then, discussing strenuous activities that can cause heart attacks. However, in recent weeks there seems to have been a flurry of them.
Are there more heart attacks happening? Are they being caused by Covid? Lack of care during lockdowns? Lockdowns themselves? Vaccines?
Do you have access to any cardiac data and what do you think is causing them, if there are in fact more? (To be fair, looking at my recent energy bills did make me fill a bit funny).
A selection of the articles I am talking about:

Wales Online – Energy bill price rise may cause heart attacks and strokes
New York Post – The little-known heart attack that’s striking ‘fit and healthy’ women as young as 22
The Sun – How the weather is HARMING your health – from heart attacks to stroke and gout
The Times – Rise in heart attacks attributed to pandemic stress and poor diet
BBC – Devoted football fans experience ‘dangerous’ levels of stress
The Sun – HIDDEN RISK Urgent warning as 300,000 Brits living with stealth disease that could kill within 5 years
Express – Heart attack: The drink that could trigger a ‘sudden’ cardiac arrest – ‘catastrophic’
Express – Heart attack: Does skipping breakfast increase your risk?
Times of India – Why are heart attacks becoming common in ‘seemingly’ fit people?
Mining Journal – Sports can break your heart in more ways than one
Daily Mail – Expert warns that shovelling snow can be a deadly way to discover underlying cardiovascular conditions as straining the heart with physical activity could cause sudden death
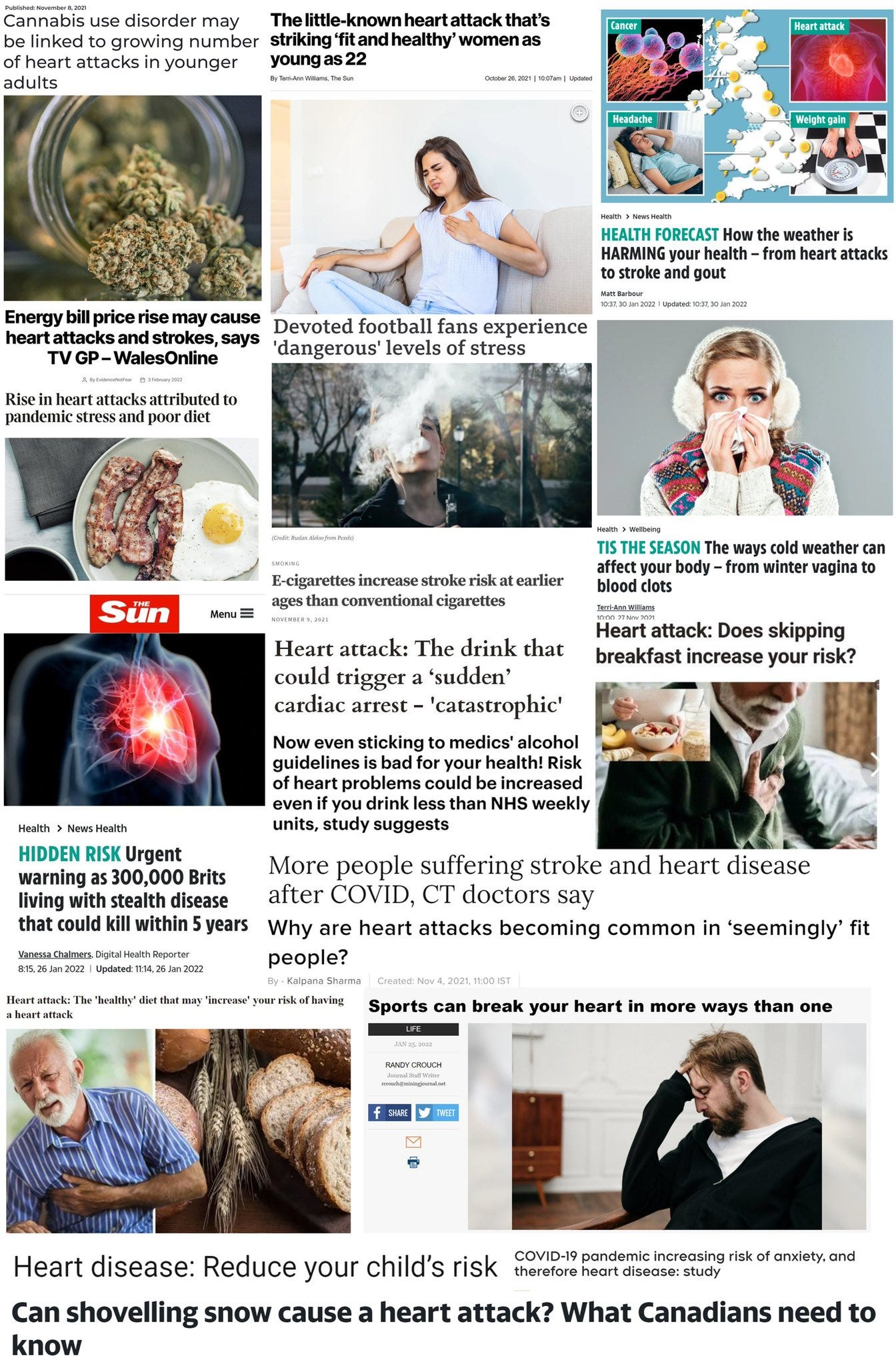
Daily Mail – Popping a paracetamol each day could raise your risk of a deadly heart attack or stroke by a FIFTH, study warns
Heart – Cannabis use disorder may be linked to growing number of heart attacks in younger adults
Featured Video

American Aerial Massacres in Germany
or go to
Aletho News Archives – Video-Images
From the Archives
“Democratic Institutions?” – 10 Lessons from history that will destroy your trust in the CIA
By Kit | OffGuardian | July 20, 2018
… At every corner, we are urged to simply believe what we are told. Whether it is about believing Porton Down and MI6 about “novichok”, or believing the White Helmets about Sarin, or believing the FBI about “collusion”, we are presented with no facts, just assertions from authority. Those who question those assertions are deemed “bots” at best or “traitors” at worst.
Well here, fellow traitors, are the Top Ten reasons to question anything and everything the CIA – or any intelligence agency – has ever told you. … Read full article
Blog Roll
 Aletho News
Aletho News- Strategic Ambiguity (If We Must)
- Finland shreds nuclear weapons ban
- Kiev turns to ‘systematic killing’ of Zaporozhye plant staff – Russia’s nuclear chief
- Censored Lavrov article Politico refused to publish (FULL TEXT)
- Israel’s censor silenced 5,700 reports in 2025
- After US-Iran deal, Israeli minister threatens war on Syria ‘sooner or later’
- When the Iran War is over: Why the West Bank may be Netanyahu’s next front
- Israeli forces launch fresh ground incursions into Syria’s Quneitra, interrogate locals
- Syria ‘unwilling, unprepared’ to attack Lebanon despite US pressure: Report
- Hezbollah thwarts Israeli advances into Kfar Tebnit-Ali al-Taher
- If Americans Knew
- Netanyahu’s Mouthpieces Turn on Trump, Revealing a Deeper Israeli Ingratitude
- Senate wants to force US to share sensitive intel with Israel
- Trump ended his idiotic Iran war. Good.
- Khanna Becomes First in Congress to Sign ‘Peace Pledge’ Promising to Reject AIPAC Funds
- Look who’s losing it over Trump’s Iran deal
- Israel has killed over 1,000 Gazans during 8-month “ceasefire” – Daily Update
- REVEALED: Former Top DEA Official Says Israel Spies on US Law Enforcement
- What would happen if US actually cut off military aid to Israel?
- Western Media Normalize Ethnic Cleansing of Lebanon by Viewing It Through Israel’s Eyes
- Behind the Screen, Netanyahu Is Annexing Gaza ‘Step-by-Step’
- No Tricks Zone
- New Study: Chile’s Relative Sea Level Was 3.2 Meters Higher Than Today During The Mid-Holocene
- Beyond The Pitch: Why FIFA’s World Cup Is One Of Humanity’s Best Investments
- Climate Alarmists Now Using Natural Phenomena To Support Their Claims
- New Study: Significant CO2 Fluxes From Non-Volcanic Sources Are Largely Neglected In Carbon Budgets
- Women Climate Scientists Being Harassed, Insulted By Skeptics, Claims Berkeley Earth Researcher
- Germany’s Longterm Spring Climate Data Show “No Climate Trend”
- New Study: Solar Photovoltaic, Wind Power Fail To Meet Annual Energy Demands 62% Of The Time
- Germany’s Die Welt: “Too Much Is Too Much” … Green Energies Are Cannabalizing Each Other!
- Germany’s Ecological Holocaust… Once Fairy Tale Forests Getting Cleared For Wind Turbines
- A Grand Solar Minimum Has Arrived…Global Cooling Of At Least 1°C Is Expected By The 2030s, 2040s
