Turkey & Russia Suggest Path for Grain Ships to Access Ukrainian Ports
By Kyle Anzalone and Will Porter | The Libertarian Institute | June 16, 2022
Ankara and Moscow have put forward potential solutions to reopen Ukraine’s Black Sea ports, with Russia offering safe passage to ships while Turkey said it could help guide vessels around Ukrainian naval mines deployed to stall the Russian advance.
Russia’s UN Ambassador Vassily Nebenzia told reporters on Wednesday that the Kremlin is open to creating a “safe passage” for grain shipments, but said Moscow could not guarantee a route that would be free of mines
“We are not responsible for establishing safe corridors. We said we could provide safe passage if these corridors are established,” he said. “It’s obvious it’s either de-mine the territory, which was mined by the Ukrainians, or ensure that the passage goes around those mines.”
While Turkey has said it would “take some time” to clear away the munitions, Foreign Minister Mevlut Cavusoglu suggested safe corridors could be found in some Ukrainian ports, presenting the offer as a short-term solution.
“Since the location of the mines is known, certain safe lines would be established at three ports,” the FM said earlier on Wednesday, adding that ships could “come and go safely to ports without a need to clear the mines.”
Cavusoglu went on to say that Ankara has not received a response from the Kremlin on the proposal, but is currently working with the United Nations on a plan. UN spokesman Stephane Dujarric confirmed that discussions were underway, though noted that an agreement from both Ukraine and Russia would be needed to move forward.
Turkey’s National Defense Minister Hulusi Akar, meanwhile, told TRT that the three nations recently created an “emergency communication mechanism” to resolve the problem and reopen Ukraine’s ports, but it’s not yet clear whether any progress had been made in negotiations. Last Sunday, President Recep Tayyip Erdogan also announced that he plans to hold a three-way dialogue on the issue with his Russian and Ukrainian counterparts sometime in the coming weeks, after Ankara hosted several rounds of lower-level peace talks.
Kiev, however, has signaled that it will not accept the Russian or Turkish proposals. Speaking at an event in Washington on Wednesday, David Arakhamia, a lawmaker and the head of Ukraine’s negotiation team, said “Our military people are against [de-mining the ports], so that’s why we have very, very limited optimism for this model.”
The UN has warned that the disruption of grain exports from Ukraine could have a massive impact on global food supplies. Together, Moscow and Kiev provide up to 40% of Eastern Europe’s grain purchases, and make up an even greater part of some countries’ total imports.
While Ukrainian and American officials have repeatedly blamed Russia for the shortages, Moscow has rejected the charge, instead pinning the scarcities on US sanctions and the explosives still deployed at key Ukrainian seaports. The Kremlin previously offered to help establish a safe route for shipping vessels in exchange for sanctions relief, but Washington refused to take up the deal.
The US and its Western partners have attempted to cripple the Russian economy through heavy sanctions in response to the invasion, some pledging outright embargoes on the country’s energy exports. While the penalties initially sent the ruble tumbling, it has since made a significant comeback and is now among the best performing currencies against the dollar in 2022. Meanwhile, the White House is now quietly pushing US shipping companies to do business with Russian fertilizer suppliers.
The conflict raging in Eastern Europe has not severed all business ties between Moscow and Kiev, as Ukraine’s state-run Naftogaz has continued to work with its Russian equivalent, Gazprom. Though the two firms have reportedly done hundreds of millions of dollars in trade since the war kicked off in February, the shaky truce could soon fracture, as Naftogaz is now pursuing a lawsuit against Gazprom for alleged underpayment.
Google, Twitter, Meta, TikTok and more just signed the EU’s “anti-disinformation” code
By Dan Frieth | Reclaim The Net | June 16, 2022
Big Tech companies have signed a new version of the European Union’s “anti-disinformation” code. Some of the companies that signed include Google, Twitter, Meta, TikTok, and Twitch – but also smaller players such as Vimeo and Clubhouse.
There are 34 signatories in total:
- Adobe
- Avaaz
- Clubhouse
- Crisp Thinking
- Demagog
- DOT Europe
- European Association of Communication Agencies (EACA)
- Faktograf
- Globsec
- Interactive Advertising Bureau (IAB Europe
- Kinzen
- Kreativitet & Kommunikation
- Logically
- Maldita.es
- MediaMath
- Meta
- Microsoft
- Neeva
- Newsback
- NewsGuard
- PagellaPoltica
- Reporters without Borders (RSF)
- Seznam
- The Bright App
- The GARM Initiative
- TikTok
- Twitch
- Vimeo
- VOST Europe
- WhoTargetsMe
- World Federation of Advertisers (WFA)
Apple declined to sign.
The “code of practice on disinformation,” will require online platforms to show how they are tackling “harmful content.”
It will also require platforms to fight “harmful misinformation” by forming partnerships with fact-checkers and developing tools. They will be forced to include “indicators of trustworthiness” on information verified independently on hot-button issues like COVID-19 and Russia’s invasion of Ukraine.
Perhaps the most notable requirement is providing their efforts to tackle harmful content and disinformation on a country-by-country basis. The move was opposed by online platforms, but national regulators demanded that they need more specific data to better address the spread of disinformation.
The EU’s vice president for values and transparency Věra Jourová, who is in charge of the code, said “to respond to disinformation effectively, there is a need for the country- and language-specific data. We know disinformation is different in every country, and the big platforms will now have to provide meaningful data that would allow to understand better the situation on the country level.”
“Russia’s actions have informed to shape the anti-disinformation code,” she said. “Once the code is operational, we will be better prepared to address disinformation, also coming from Russia.”
The new code also requires online platforms to provide other data, including the AI systems deployed to tackle “disinformation,” number of bots removed, and the number of content moderators in each country.
The code applies immediately but allows for a six-month implementation period for platforms to adhere to the strict rules.
Russia to export agricultural products to ‘friendly countries’ only
Samizdat | June 16, 2022
Russian Minister for Agriculture Dmitry Patrushev said on Thursday that the country’s grain harvest could reach 130 million tons this year, which would be enough to cover both domestic needs and ensure export potential.
Speaking on the sidelines of the St. Petersburg International Economic Forum (SPIEF), he pointed to numerous challenges including broken supply chains and difficulties with financial calculations.
Patrushev said Russia has to overcome these obstacles in order to provide food to the countries that need it most. “Our [agricultural] products will be on foreign markets, but only in those countries that are friendly to us, that do not create hurdles and difficulties for us,” he told reporters.
Russia is expecting a bumper grain crop this year, including a record wheat harvest, President Vladimir Putin said last month. He added that a number of countries are facing the threat of famine, stressing that the blame for this situation lies entirely with “the Western elites.”
The grain crisis is being felt across the globe as wheat prices have surged to record highs over the past two months. The global food market, already affected by weather and the Covid pandemic, was dealt another blow due to the Russia-Ukraine conflict and Western sanctions on Moscow. This has sparked fears of global food insecurity and hunger.
Nord Stream Can Stall Completely in the Event of New Turbine Problems: Russian UN Envoy
Samizdat | 16.06.2022
The pipeline, which supplies a significant proportion of the natural gas imported by Germany, reduced its output to just 60% after its operator failed to receive one of the turbines that pump the gas from maintenance in Canada due to anti-Russia sanctions. The warnings of a further reduction in the capacity prompted a 25% spike in EU gas prices.
Further problems with the repair and maintenance of turbines that pump the gas flowing through the Nord Stream pipeline could bring a halt to its operation, Russia’s Permanent UN Ambassador Vladimir Chizhov has warned in his speech at the St. Petersburg International Economic Forum (SPIEF).
Such scenario would be a disaster for Germany, which significantly depends on gas supplies from this pipeline, Chizhov added.
“We should ask [the turbine’s manufacturer] Siemens, why the turbines must undergo maintenance in Canada. […] I don’t want to give any advice, but I think they could have learnt by now how to repair [turbines] themselves”, Chizhov said.
The UN envoy further called EU plans for a seventh sanctions package against Russia a “strategic mistake”. He added that Russia will start dealing with its consequences once the sanctions package is adopted.
The anti-Russia sanctions are the reason why German giant Siemens can’t return Russia’s Nord Stream turbines, which had been sent to Canada for maintenance. Siemens said that it was looking into ways to solve the problem.
While the German company is looking for a solution, the Russian company Gazprom announced on 14 June that Nord Stream’s output capacity had fallen to 60% due to an inability to retrieve the turbine which had undergone maintenance. Its output dropped to 100 million cubic metres versus 167 million per day at peak. The company warned that it would be further reduced on 16 June to 67 million cubic metres per day for the same reason.
On the news of a further reduction in Nord Stream output capacities, the price of gas in Europe jumped 25% in one day (15 June) exceeding $1,300 per thousand cubic metres. On the trading day’s opening the price was up 2% compared to around $1,069 per thousand cubic metres as of the close of the previous day’s trading.
Should the patient really get the drug?
By Sebastian Rushworth, M.D. | June 14, 2022
I recently gave a lecture to 70 primary care physicians here in Stockholm, titled “should the patient really get the drug?”. The lecture seemed to generate quite a bit of cognitive dissonance among some in the audience, based on the somewhat aggressive discussion that followed the lecture, which suggests to me that much of what I was saying was stuff they had literally never been exposed to before – not at any point in medical school, and not at any point during their careers after medical school either. Cognitive dissonance is good. It’s the first step towards change.
I thought it would be interesting to re-write the lecture as an article, so that more people can hopefully achieve similar levels of cognitive dissonance. Please feel free to share it with any doctors you know that you think might benefit from an expanded perspective. Anyway, here we go.
Let’s imagine a common patient. Every primary care physician meets this patient, or someone much like her, on an almost daily basis. She’s 75 years old, and overweight. She experienced a wrist fracture two years ago, and was subsequently diagnosed with osteoporosis. She has high cholesterol levels, but she’s never had a heart attack or other “cardiovascular event”. On top of that, she has type 2 diabetes, chronic knee pain due to osteoarthritis, and high blood pressure. She was diagnosed with depression a few years ago, after her husband died.
Our patient takes seven drugs every day:
- Alendronate, because of her weak bones.
- Atorvastatin, because of her high cholesterol levels.
- Sertraline, because of her depression.
- Metformin, because of her type 2 diabetes.
- Insulin, also because of her type 2 diabetes.
- Paracetamol (a.k.a. acetaminophen), because of her knee pain.
- Enalapril, because of her high blood pressure.
So, the question is, are these drugs doing her any good?
Well, to answer that question, we need to consider NNT (Number Needed to Treat). NNT is the number of patients who need to take a drug for one patient to achieve a noticeable benefit.
For alendronate, the NNT is 20, i.e. if you treat 20 people for a couple of years, you prevent one fracture. For atorvastatin the NNT is 200, i.e. you need to treat 200 people for five years or so in order to prevent one heart attack. For sertraline, the NNT is 7, which means that you need to treat seven people in order to have a noticeable effect on depression in one patient. Note that this doesn’t mean that one out of seven gets cured of their depression, it just means that there is a noticeable difference on a rating scale for depression.
For metformin, the NNT is 14 – If you treat 14 type 2 diabetics with metformin for ten years, you prevent one death. For enalapril, the NNT is 70 – If you treat 70 people with high blood pressure with enalapril for five years or so, you prevent one stroke.
For insulin, however, there is no NNT, because insulin has not been shown to result in any benefit on any clinically relevant outcome, even though big studies have been carried out that have included thousands of patients and followed them for five or ten years. Note here that we’re talking about insulin for type 2 diabetics. When it comes to type 1 diabetes, insulin is pretty much magical – you don’t even need to do a randomised trial in order to show benefit. People with type 1 diabetes virtually return from the dead when treated with insulin. But when it comes to type 2 diabetes, there is no benefit, at least not to any hard outcomes. All insulin has been shown to do is reduce blood sugar, but it’s never been shown to result in any meaningful patient oriented benefit for type 2 diabetics.
The same is true for paracetamol/acetaminophen. When it comes to patients with knee pain due to osteoarthritis, the drug doesn’t provide any benefit whatsoever.
Ok, so we have seven drugs, and we know what their NNT’s are. If we plus the probabilities of benefit together, then we get the probability that our 75-year old woman will benefit in some way from at least one of the drugs she’s taking. So, what probability of benefit do we get?
We get 30%. Only 30%.
What that means is that there is a 70% probability that this woman doesn’t benefit at all from any of the seven drugs that she takes every day for years on end!
If you told her, I’d say there are pretty good odds she’d decide to stop taking her pills. Seven drugs a day, every day, and two to one odds of zero benefit.
And we haven’t even talked about harms yet. Because none of these pills are inert. All have widespread biological effects. And all can cause harms. So any rational treatment decision must include not just the potential benefits, but also the potential harms.
For figuring out harms, we have NNH (Number Needed to Harm), which is the counterpoint to NNT. NNH is the number of patients who need to get a drug for one to be harmed. Like I said, the drugs all have widespread biological effects, so there isn’t just one NNH – there is an NNH for each possible harm. That means that there are multiple NNH’s for each drug.
With our 75-year old woman and her seven drugs, we don’t have time to go through the NNH for every possible side effect, so we’re just going to look at a few, and put them side by side with the NNT, to get a somewhat more complete picture of benefits vs harms. I’ve tried to make sure that the NNH numbers apply to the same time period as the NNT numbers, since otherwise it’s an apples to oranges comparison.
If we do that, we get something like this:
Alendronate
NNT: 20 (fractures)
NNH: 200 (esophagitis), 260 (atrial fibrillation), 4,000 (osteonecrosis)
Atorvastatin
NNT: 200 (cardiac infarction)
NNH: 20 (myalgia), 20 (type 2 diabetes)
Sertraline
NNT: 7 (depression)
NNH: 2 (sexual disturbance), 10 (hyponatremia)
Metformin
NNT: 14 (death)
NNH: 2 (stomach upset), 5 (B12 deficiency), 1,000 (lactic acidosis)
Enalapril
NNT: 70 (stroke), 125 (death)
NNH: hyperkalemia (10), acute kidney failure (100)
Insulin
NNT: 0 (no benefit to clinically relevant outcomes)
NNH: severe hypoglycemia (5), weight gain (1)
Paracetamol/acetaminophen
NNT: 0 (no benefit to clinically relevant outcomes)
NNH: Hypertension (30), liver damage (?)
It’s possible to quibble here about specific NNT and NNH numbers. Different studies show different things. And many of the numbers come from studies carried out by pharmaceutical companies, which generally means that the risk of a certain side effect is massively underestimated (as we will discuss shortly). The point here isn’t to get hung up on any of the specific numbers. It’s to illustrate that we quickly end up with a very complex equation, where it in many cases isn’t clear at all whether the benefits outweigh the harms.
Take alendronate, as an example. We know that it decreases fractures in elderly osteoporotic women. But it doesn’t decrease hospitalisations. The only reasonable conclusion is that the reduction in hospitalisations that is seen due to the reduction in fractures is made up for by an increase in hospitalisations due to the many and varied side effects. So at the end of the day the only way to decide whether or not to take the drug is to have a detailed discussion with the patient and get them to decide which set of risks they’d rather be taking.
Hippocrates is supposed to have said “primum non nocere”, which is latin for “first, do no harm”. Actually he didn’t say that, and couldn’t have even if he wanted to. Hippocrates was greek, and didn’t speak latin. The quote comes from a 19th century American physician, Worthington Hooker.
Of course, as doctors, we all know that “first, do no harm” is completely unrealistic. Every intervention we do carries some measure of risk. If our primary guiding principle was to never do harm, we literally would never be able to do anything. A more reasonable principle is “only do something if the benefits clearly outweigh the risks”. If it isn’t clear to you that the benefits of a drug outweigh the harms, then don’t give it to the patient.
That’s a good general rule to stick by. However, it probably isn’t enough, for a few reasons we’re now going to discuss.
A study was published in JAMA Internal Medicine in 2021 that sought to establish how good physicians are at estimating the likelihood that a patient has a certain disease. 500 primary care physicians in the US were asked to consider various hypothetical scenarios, and then answer what they thought the probability of disease was. Here’s an example of a scenario that they were asked to consider:
Ms. Smith, a previously healthy 35-year-old woman who smokes tobacco presents with five days of fatigue, productive cough, worsening shortness of breath, fevers to 102 degrees Fahrenheit (38.9 degrees centigrade) and decreased breath sounds in the lower right field. She has a heart rate of 105 but otherwise vital signs are normal. She has no particular preference for testing and wants your advice.
How likely is it that Ms. Smith has pneumonia based on this information? ___%
Ms. Smith’s chest X-ray is consistent with pneumonia. How likely is she to have pneumonia? ___%
Ms. Smith’s chest X-ray is negative. How likely is she to have pneumonia? ___%
Go ahead and make your own guesses in relation to each of the three questions.
Once you’ve done that, you can take a look at the table below, and the answers will be revealed.

So, for our pneumonia example above, we see that the actual initial risk of disease based on the presented information was around 35%. If we then move along and look at what the doctors answered, they thought the risk was 80-85%. In other words, they thought pneumonia was more than twice as likely as it actually was!
The same phenomenon was seen in all clinical scenarios tested. The doctors consistently overestimated the initial risk, and they continued to overestimate the risk after both a positive and a negative test result. In some cases the difference between reality and what the doctors thought was huge, with the doctors overestimating risk by a factor of ten or more.
What can we conclude from this?
Doctors consistently overestimate disease risk.
Hold that thought, as we move on to take a quick look at another study, which was published in BMJ Open in 2015. This study sought to do something about a problem inherent in statin trials (and for that matter, all trials in medicine), which is that the results they produce, in the form of percent absolute risk, percent relative risk, and NNT, are so abstract that they’re completely meaningless to patients (and for that matter, to doctors as well). We know that statins have an NNT of 200 when used for primary prevention (to prevent a heart attack in someone who has risk factors but hasn’t already has a heart attack), and 40 when used for secondary prevention (to prevent additional heart attacks in someone who has already experienced a heart attack). But what do those numbers actually mean? Are they good or bad?
What the patient really wants to know is “how much longer will I live if I take this drug?”
So, what the researchers did was gather together data from all the big randomised trials of statins, and use the survival curves provided to estimate how much longer the patients actually lived. Here’s what they came up with:

All the big statin trials are included here. What’s interesting to do is look at the NNT provided, and then compare that with the number to the right of it, which is how much longer the patients actually lived, on average. So, for the ALLHAT trial, to take the topmost example, we have an NNT (for primary prevention) of 250, which comes down to a postponement of death of 4.96… well, 4.96 what?
Is it years? No.
Is it months? No
The patients in the statin group lived 4.96 days longer than the patients in the placebo group. That is what the NNT of 250 means in real terms.
Let’s look instead at 4S, which was published in 1994 and is the statin trial that has produced the best results of any statin trial ever. It’s the trial that initiated the massive boom in statin prescribing that we still see today. In 4S, the NNT (for secondary prevention) is 27.8. So, in other words, one in 27.8 patients benefited from the treatment.
But what does that actually mean in terms of life extension?
It means 27 days.
Not as impressive as you would have thought, right?
When the researchers put all the data together, from all the trials, in order to get an overall average, what they found was that when statins are used for primary prevention they prolong life by 3 days. When they are used for secondary prevention, they prolong life by 4 days.
I can imagine quite a few patients turning down the offer of a statin if they knew that it will on average only prolong their life by days.
The purpose of bringing up this study was to illustrate the following general point:
Doctors consistently overestimate the benefit of the drugs they prescribe.
Hold that thought in your mind as we move on and look at a third study.
This one was published in The Lancet Healthy Longevity in 2021. It compared the rate of serious side effects seen in randomised trials with that seen in the real world. If randomised trials give us good information about what to expect in reality, then the rate of serious side effects in the trials should be the same as that seen in reality.
But that isn’t what the researchers found. What they found was that serious side effects were three to four times more common in reality than they are in the randomised trials! Three to four times!
How is this possible?
Well it’s important to remember that the randomised trials are funded and run by the drug companies, and the drug companies want to sell their drugs, so they will do what they can to make side effects appear as rare as possible.
Why is this a problem? Because it’s the randomised trials that doctors mostly use as a basis for determining whether a drug is safe to give to a patient or not.
So, what can we conclude from the study?
Doctors consistently underestimate side effects of drugs.
Ok, so we have three conclusions, that are all pointing us in the same direction:
- Doctors consistently overestimate disease risk.
- Doctors consistently overestimate drug benefit.
- Doctors consistently underestimate drug harm.
What does this lead to?
Massive overprescribing of drugs.
Peter Gotzche, a founding member of the Cochrane Collaboration and former director of the Nordic Cochrane Center, has estimated that prescription drugs are now the third biggest cause of death in the western world, after heart disease and cancer.
That on its own should lead to massive humility among all doctors about our drug prescribing. It should make us much more careful every time we think about prescribing a drug to a patient.
Ok, so we’ve identified the problem. The causes of this problem are many and complex, so I’m just going to bring up one that each of us as doctors can actually do something about – industry sponsored meals.
A study was published in JAMA Internal Medicine in August 2016 that sought to estimate the extent to which physicians are influenced by partaking in industry sponsored meals, which often take the form of a lecture about a specific drug given by an drug company salesperson, which the physician is supposed to sit and listen to in return for getting a free meal. Industry sponsored meals are very common. Most physicians probably take part in at least a couple of these per year, and many take part in far more than that.
As the saying goes, “there’s no such thing as a free lunch”. The drug companies are not charities whose goal it is to keep starving doctors alive. If they spend vast sums of money of sponsored meals, it’s because they’re pretty damn sure that it increases sales of their drugs, and thereby their profits.
So, anyway, the study sought to estimate the extent to which industry sponsored meals influence physician prescribing patterns, by comparing participation in such meals with later prescribing behaviour. Here’s what they found:

They looked at four different drugs. As I think is clear from the tables, participation in industry sponsored meals increased prescribing of the drug the meal was about, and the more such meals a doctor participated in, the more often he or she prescribed that drug.
The purpose of these meals is not to educate us, or make us better doctors. It’s the opposite – the purpose is to make us do a specific profit-driven company’s bidding. And it works.
If you’re a doctor, and you think you don’t get influenced by participating in industry sponsored meals, then you are very naive. The more industry sponsored meals we participate in, the worse doctors we become.
Doctors in general massively underestimate the extent to which their thoughts, beliefs, and opinions are influenced by the pharmaceutical industry. We like to think that we are evidence based. But the truth is that much of what we think we know is not based on sound scientific knowledge, but on pharmaceutical industry propaganda, which quickly becomes clear to anyone who starts going through the studies in detail themselves.
On that note, I strongly recommend reading these three books, all written by physicians, to help get some perspective on the scale of the problem we face in relation to the pharmaceutical industry.
- Bad Pharma by Dr. Ben Goldacre
- Doctoring data by Dr. Malcolm Kendrick
- Deadly medicines and organised crime by Dr. Peter Gotzsche
There is one very simple thing every doctor can do, to at least partially free themselves from the onslaught of drug company propaganda, and that is to refuse to take part in industry sponsored lunches, and all other forms of industry sponsored “education”. Just say No.
Ok, so, that’s number one: refuse to take part in industry sponsored lunches.
What else can you do as a doctor?
Well, something that was once considered standard, but has fallen by the wayside in recent decades, is to never have a patient on more than five drugs at the same time. With drugs, as with everything else, there is a state of diminishing returns – the more you add, the less benefit (and more harm) each additional drug confers. So try to keep a patient on at most five simultaneous drugs. If you want to add a sixth, then rank them all, and get rid of the one that you think is least important. Most likely, the sixth least important drug in a list of six is not going to do anything useful for the patient anyway, just increase their risk of harm.
Ok, so that’s number two: try to avoid having your patients on more than five drugs simultaneously.
Number three: go through the patient’s drug list with them once a year, and get rid of anything that isn’t clearly conferring a benefit. As any doctor will know, it’s common for patients to stay on drugs for years, even though the original reason they were put on the drug resolved itself a long time ago. The patient often doesn’t remember why they were put on the drug in the first place, but they keep taking it dutifully. Drug lists require regular pruning or they will become increasingly bloated as the years go by, which is one reason why so many elderly people are on 15 simultaneous drugs or more.
Number four: only prescribe a drug if the benefits clearly outweigh the harms. This should be obvious, but it requires a deep knowledge of the size of both potential benefit and potential harm, which unfortunately most doctors lack. And what they think they know is often incorrect because it’s based more on pharma propaganda than real science.
As a doctor, the only way to get around this is to start doing your due diligence and getting in to the weeds of the scientific studies. Do that for the ten drugs you prescribe most commonly, so that you’re an expert on those ten drugs, and you’ve already done a lot. If a patient asks you about the probability of benefit and the probability of harm, you should be able to answer that question correctly, at least for the ten drugs you use most frequently. It requires an up-front investment of time, but it will pay massive dividends to your patients over the remainder of your career.
Ok, so that was number four: only prescribe a drug if the benefit clearly outweighs the harm.
Here’s number five: prioritise lifestyle changes. Most of the diseases that doctors spend most of their time dealing with are caused by poor lifestyle choices. And most can be rectified by switching to good lifestyle choices, which invariably produce greater benefits than any drug can, with less risk of harm.
Doctors can accomplish a lot with their patients with simple lifestyle coaching. To take one example, a primary care clinic in the UK decided to try putting their type 2 diabetic patients on a ketogenic diet, since the drugs they were using clearly weren’t making the patients better. They published their six year follow up results in BMJ Nutrition, Prevention, and Health in 2020.
Over six years, the patients following the ketogenic diet decreased their median HbA1c (a measure of average blood sugar over the preceding few months) from 66 to 48. Normally, that would be unheard of. HbA1c doesn’t decrease over time in a type 2 diabetic. It increases. Yet here it was far better at the end of the six years than at the beginning. The same goes for body weight. Normally it goes up over time. But here the median decreased from 99 kg to 91 kg. And on top of that, median systolic blood pressure dropped from 152 to 141.
All this just with a simple diet intervention. Thanks to the improvements in all health markers, the patients were able to get off a lot of their drugs. This meant that after six years, the clinic was spending less than half as much money on anti-diabetic drugs as the other primary care clinics in the region.
To take another example of a simple lifestyle intervention, a randomised trial published in BMJ in 2021 that was carried out in nursing homes in Australia found that a diet high in protein has an effect on fracture risk that is equivalent to that seen with bisphosphonates.
There is a massive amount that can be accomplished with simple lifestyle interventions, and since they are much less risky than drugs, and actually treat the underlying problem rather than just putting a patch on top of it, they should be the primary intervention we use whenever possible. Drugs should be viewed as a complement to lifestyle interventions. It shouldn’t be the other way around.
Ok, so that was my fifth and final point. I’ll repeat the five points here again. These are five things that you as a doctor can do about the situation we currently find ourselves in, where prescription drugs are the third biggest killer in the western world:
- Refuse to participate in industry sponsored lunches and other industry sponsored “education”.
- Try to avoid having your patients on more than five drugs simultaneously.
- Go through the patient’s drug list with them once a year, and get rid of anything that isn’t clearly conferring a benefit.
- Only prescribe a drug if the benefits clearly outweigh the harms.
- Prioritise lifestyle changes.
Senators want DHS chief Mayorkas to answer for “misleading” testimony about disinformation board
By Dan Frieth | Reclaim The Net | June 15, 2022
In a letter to Senate Homeland Security Committee Chairman Gary Peters, senate Republicans are demanding that Department of Homeland Security Secretary Alejandro Mayorkas answer for his testimony about the paused Disinformation Governance Board that contradicts newly-discovered documents.
We obtained a copy of the letter for you here.
According to the letter, Senators Josh Hawley and Chuck Grassley obtained documents from a whistleblower with detailed information about the disinformation board that contradicts what Mayorkas testified.
According to the documents, the disinformation board was created to to monitor online speech about “conspiracy theories about the validity of elections” and “disinformation related to the origins of effects of COVID-19 vaccines or the efficacy of masks.” It also said that the controversial board wanted to partner with Twitter to suppress certain speech and wanted to meet with Twitter executives to determine how this could be done.
Under oath on May 4, Mayorkas said that the disinformation board had not yet started working. Speaking to media outlets, Mayorkas said that the board would focus on cartels and foreign adversaries and would not spy on Americans, something that was contradicted by the leaked documents.
The letter demands that Mayorkas testify again to clear the contradictions between his previous testimony, his public statements, and the documents provided by the whistleblower.
The letter states: “We are deeply concerned that documents recently obtained by Senators Josh Hawley and Chuck Grassley contradict the Secretary’s testimony and public statements about the Board. The American public deserves transparency and honest answers to important questions about the true nature and purpose of the Disinformation Governance Board and it is clear that Secretary Mayorkas has not provided them – to the public or this Committee.
“Therefore, we request you hold a hearing with Secretary Mayorkas and join us in insisting that all records related to the Board be provided to the Committee prior to the hearing.”
Developmental Disorders in Babies born to Vaccinated Mothers?
Pfizer wants Babies to be Exposed to SIX Vaccine Shots!
By Igor Chudov | June 10, 2022
I will explain that
- Children of Covid vaccinated mothers were never tested for developmental disorders
- CDC recently revised and lowered developmental milestones, and removed some entirely
- Newly born babies will be exposed to SIX doses of mRNA vaccines if the FDA’ approves the Pfizer vaccine.
An interesting article came out:
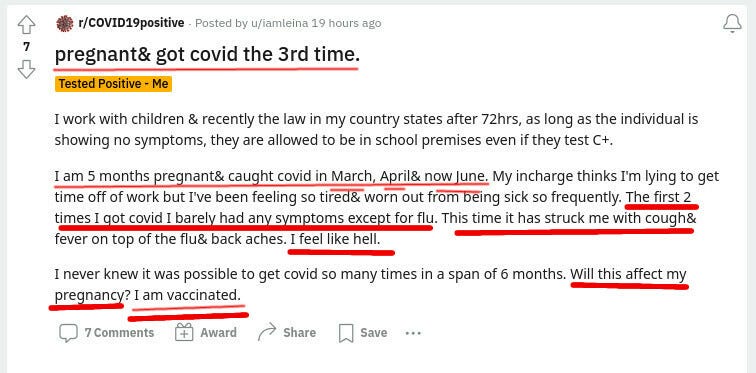
This article found that at one year of age, babies born to mothers who had COVID (not vaccine), had a roughly twice-higher rate of neurodevelopmental disorders:
those born to the 222 mothers with a positive SARS-CoV-2 polymerase chain reaction test during pregnancy were more likely to receive a neurodevelopmental diagnosis in the first 12 months after delivery, even after accounting for preterm delivery.
Considering that COVID is a bad disease for a sizable minority of people, there is no surprise. Covid is bad and gives people all sorts of problems. Then I started thinking: a lot of adverse effects of Covid vaccines mimic the adverse effects of Covid. The younger is the vaccine recipient, the worse some effects of vaccination (such as myocarditis) are.
A great number of expectant mothers received up to three Covid vaccine shots during pregnancy. Did anyone bother testing one-year-old children of vaccinated and boosted (during pregnancy) women for neurodevelopmental disorders, before approving this vaccine for all pregnant women?
The question is, obviously, rhetorical, since “mRNA Babies” of triple-vaxed-during-pregnancy mothers are only beginning to get born right now and are at most a few months old. Not one such baby reached a year of age. So nobody tested them for developmental disorders at one year of age, before approving the three vaccine shots for expectant mothers.
The usual argument of vaccinators that “since Covid does it too, you should take the vaccine” does not hold water. To a woman who decided to take the vaccine, the probability of getting a vaccine is 100%. The probability of her getting Covid is much less. In the above study, out of 7,772 births, only 222 (2.8%) were exposed to Covid during pregnancy. So while vaccination is 100% guaranteed for those who elect to vaccinate, the chance of Covid is over 30 times less likely. And the “vaccine” does not prevent Covid anyway and does not even reduce the viral load.
There is literally zero data on one-year-old children of triple-vaccinated mothers because the oldest ones are 3-4 months old as of today.
However, there are disturbing developments regarding newborns. Vaccination does seem to have an effect on births and pregnancies.
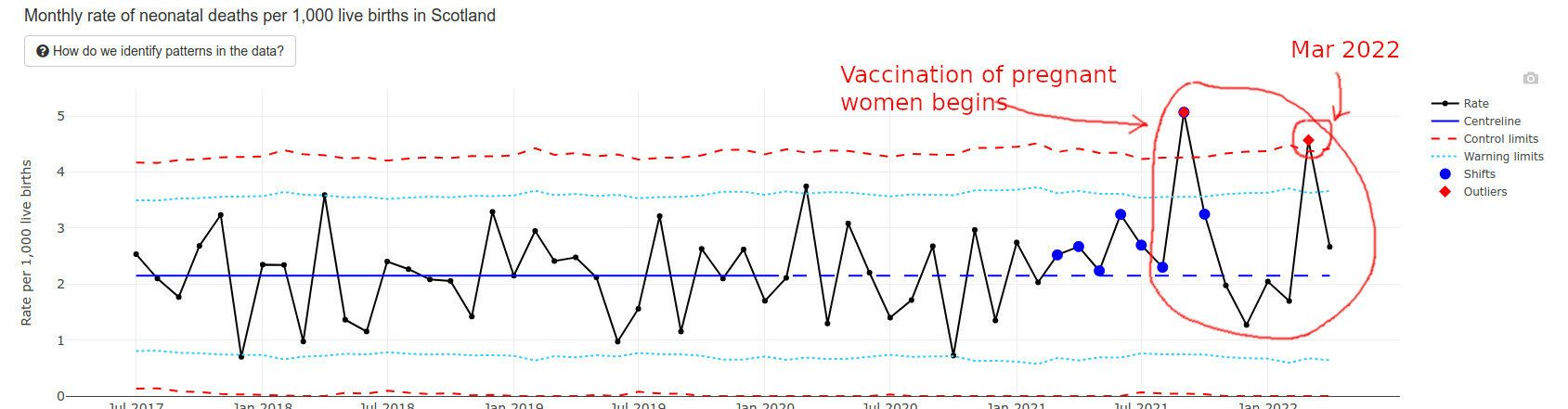
The best data I found regarding recently born newborns happens to come from Scotland. They have an interesting “wider impacts” page that I am quoting below.
Infant deaths are way above average and exceeded “Alert Limits” twice.
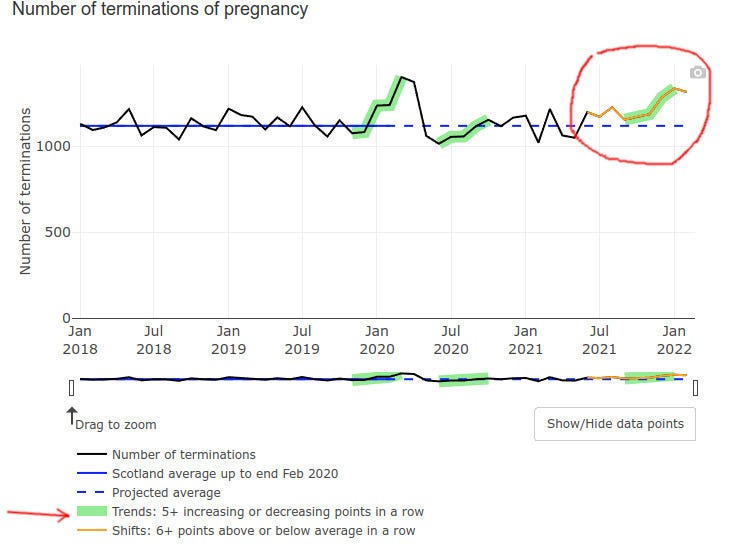
Even pregnancy terminations went up at the end of 2021, possibly but not certainly explained by prenatal vax problems:
Low Apgar score births (for those readers who do not have kids, Apgar score is how healthy is the baby at birth, the best being a score of 10) triggered a green alarm signal:
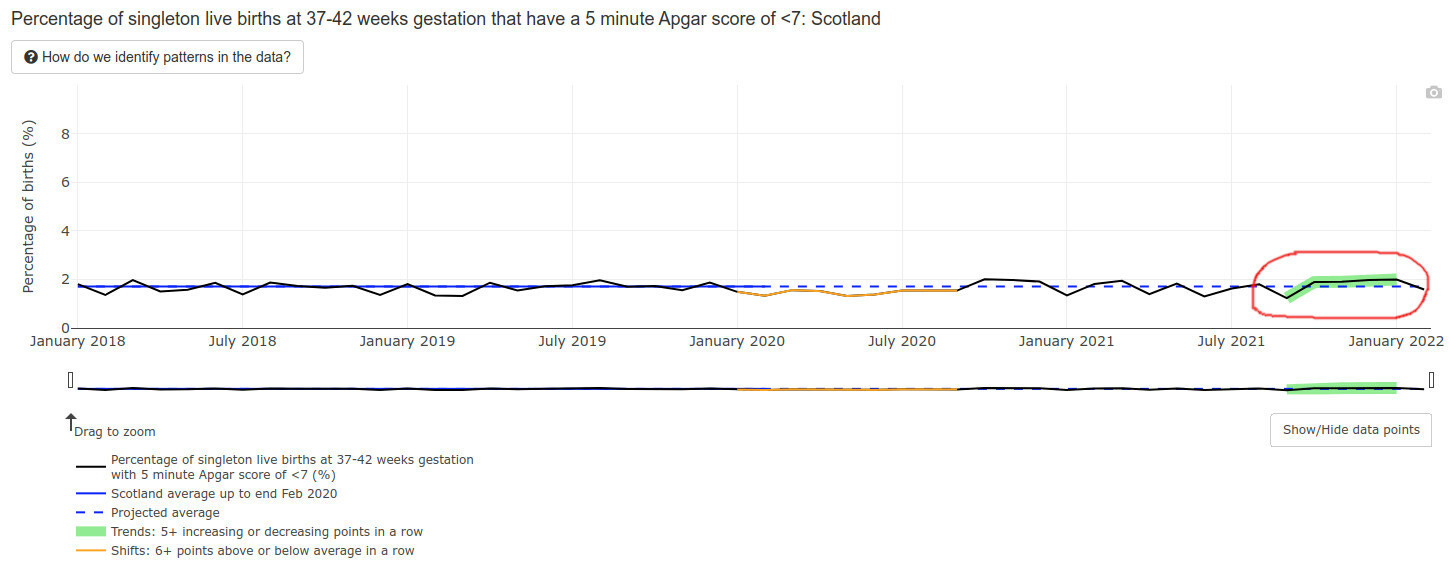
Mind you, an Apgar score is also a developmental evaluation of sorts — at 5 minutes after birth. What will happen to the developmental milestones of those lucky babies of vaccinated mothers, who survived the pregnancies, did not die postnatally, and lived to one year of age? I literally have no idea and nobody else in the world does — the time has not passed yet.
The data we have is NOT encouraging.
CDC Solution: Remove and Lower Milestones
The CDC possibly caught a whiff of this, because in February of 2022 they literally removed half the developmental milestones, bumped some others to higher ages, and lowered standards for yet more of them. (Hat tip @CLesterwood)
About one-third of milestones like fine motor skills have been bumped up to older ages. Because of the setback, children may worsen their developmental delay, making it harder to provide early intervention, explains Jessica Hatfield, MS, OTR/L, a pediatric occupational therapist for TheraTree Pediatric Therapy.
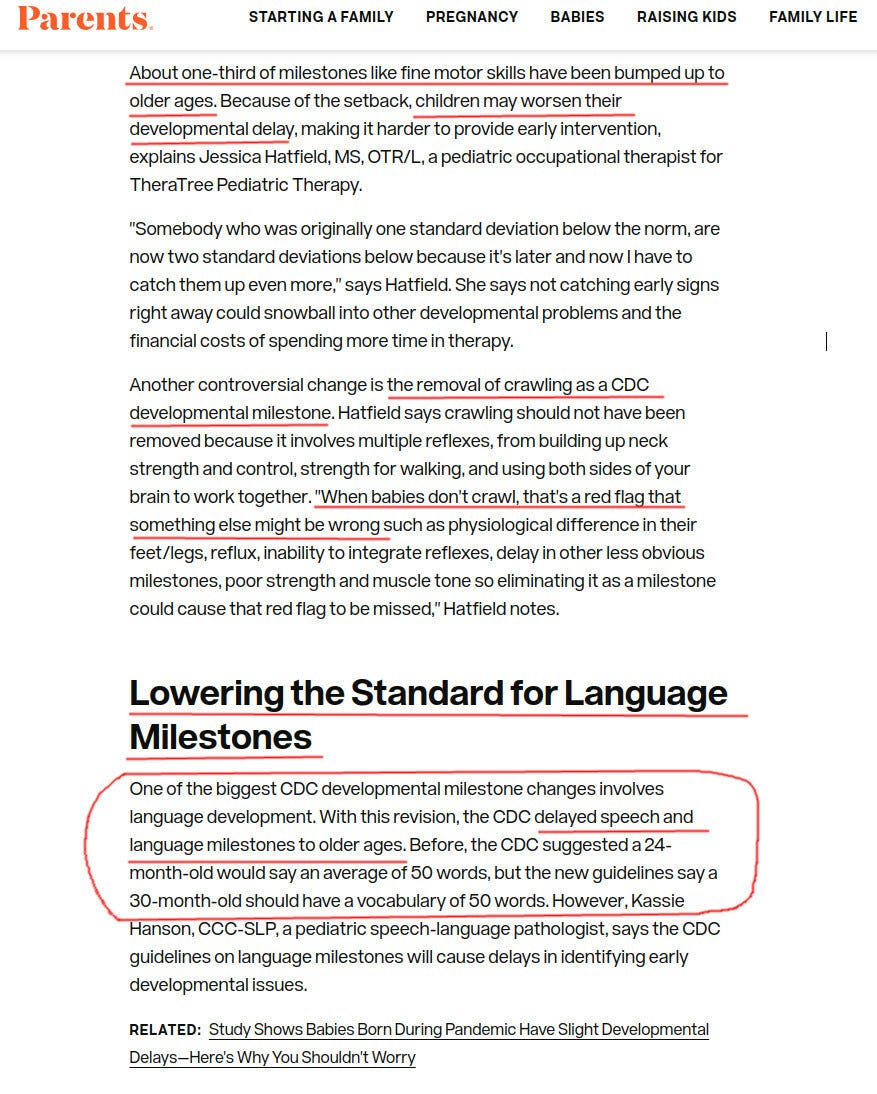
Removing crawling as a milestone??? Are you kidding us? For those of my readers who are parents, do you think that crawling is unimportant as a milestone?
Vaccinated Infants Exposed to SIX Doses of Covid Vaxx in a Year!
Imagine a vaccine enthusiast mother, who gets three doses during her pregnancy. Say, two doses during month 4 and one during the last week of pregnancy. The unborn baby is, obviously, exposed to all that.
Then the baby is born.
If the June 14-15 FDA meeting goes as planned, FDA will approve a three-dose Pfizer vaccine for infants and toddlers. So shortly after being exposed to THREE doses of mRNA vaccines prenatally, the recently born 6 months old baby will get THREE MORE Pfizer mRNA shots.
That’s a total of, drumroll, six spike protein, and nanoparticle exposures. For a tiny newborn, all during one first year of her life.
And what if the mom has several Covids while being pregnant and vaccinated?
They will ask the mom to vaccinate the baby regardless of those covid infections. This literally amounts to six doses within a year or close to, without even counting actual covids that the vaxed moms have. Pfizer will make $132 from these six shots. Not sure if the baby will eventually need much more expensive treatments.
Do you think that it is a little bit too much? Do you think Pfizer or the FDA care?
All of Greece turned into ‘huge US base,’ Greek lawmaker warns
Press TV – June 15, 2022
The Greek government has turned the whole country into a “huge US base,” a local lawmaker warned on Tuesday, amid attempts by Washington to expand its access to military zones across the European country.
Kleon Grigoriadis, in a speech in the Greek parliament on Tuesday, lambasted the government of Prime Minister Kyriakos Mitsotakis over its foreign policy for allowing the United States to turn the whole of Greece into a massive American base.
“At the moment, American soldiers, not Turkish soldiers, are wandering in Crete, Alexandroupoli, Larisa, and other areas left by (the left-wing party) Syriza’s old comrades to the United States. Let’s be clear: Greece has now turned into a huge US base,” said the lawmaker, who is a deputy of the left-wing MeRA25 party,” he remarked.
Grigoriadis warned that an atmosphere of war with Turkey has been created in the press. He said Greek citizens have been intimidated by such a perception in an attempt to make acceptable the conversion of Greece into an American military base.
The lawmaker said the Greek people should learn from history lest their country turns into a tool for big powers.
“History shows that big powers use small powers as tools and use them for their own interests regardless of the pain they may cause, as in 1922,” Grigoriadis said.
Grigoriadis’s comments almost echoed last week’s remarks by Turkish President Recep Tayyip Erdogan, who objected to the presence of US bases in Greece.
“Currently, nine US military bases have been established in Greece. Whom have they been deployed against? They say that against Russia. But we won’t buy that,” Erdogan said at the time.
Turkey and Greece have been at loggerheads for years over hydrocarbon resources and naval influence in the eastern Mediterranean.
In May, Erdogan said there were nearly ten American bases in Greece, asking: “Who is being threatened with these bases? Why are these bases being established in Greece?”
Back in November 2021, he warned that Greece itself had become a US military base. “At the moment, I can’t count all the American bases in Greece, there are so many. … It almost looks like Greece itself is a US base.”
The Greek authorities recently seized a tanker carrying Iranian oil in its territorial waters, under US pressure. The oil cargo was later transferred to the US, a move denounced by Iran as an “act of piracy”.
On Tuesday, Iran’s Ports and Maritime Organization (PMO) said in a statement that an Iranian-flagged tanker seized in April was released by Greek authorities.
“The Greek government finally issued an order and we are now witnessing the lifting of the ship’s seizure and the return of its cargo to its owner,” it said.
Iran’s foreign ministry had condemned the unacceptable surrender of Greece to Washington’s illegal pressure and reiterated that the seizure was an example of international piracy.
The seizure of the Iranian oil tanker took place at a time when the US administration claims it seeks the revival of the Joint Comprehensive Plan of Action (JCPOA), commonly known as the Iran deal. So far, talks for the revival of the 2015 deal have come to a standstill.
Days after the seizure, Iran’s Islamic Revolution Guards Corps (IRGC) seized two Greek oil tankers in the Persian Gulf over violations.
Iran vs. UAE – ‘Russia and Ukraine Gulf edition’ coming soon?
By Gavin O’Reilly | OffGuardian | June 15, 2022
Although receiving miniscule media coverage, Thursday’s announcement that Israel had deployed military infrastructure to the UAE and Bahrain in the shape of radar systems, ostensibly to counter an alleged missile threat from nearby Iran, should be a cause for concern amongst onlookers.
Coming in the same 24 hour period in which Israeli Prime Minister Naftali Bennett paid a surprise visit to the Emirates, and in which Israeli Forces bombed Damascus International Airport, the announcement that both Abu Dhabi and Manama had agreed to host Israeli military infrastructure should be seen as the first step towards current tensions between Tel Aviv and Tehran being placed on a possibly irreversible path towards conflict in the region.
Indeed, Israeli encirclement of Iran via Tel Aviv-allied Arab states possibly triggering a war between Tehran and both the UAE and Bahrain bears a stark similarity to the nine-year long build-up of provocations which would ultimately led Russia to launch a military intervention into neighbouring Ukraine in February of this year.
In November 2013, following the decision by then-Ukrainian President Viktor Yanukovych to suspend a trade deal with the EU in order to pursue closer ties with Russia, a CIA-orchestrated regime change operation, known as ‘Euromaidan’, would be launched in order to depose Yanukovych’s leadership and replace him with the pro-Western Petro Poroshenko – whose coalition government would contain rabid far-right sympathisers hostile to Moscow.
Indeed, such was the anti-Russian sentiment amongst the new US-backed Kiev government that the predominantly ethnic-Russian Donbass region in the east of the country would breakaway to form the independent republics of Donetsk and Luhansk in April 2014, following the previous month’s successful reunification of the Crimean Peninsula with the rest of Russia.
The establishment of these two pro-Russian Republics however, would spark a near eight-year long conflict in the eastern European country, in which Kiev would use neo-Nazi paramilitaries such as Azov Battalion and Right Sector to wage an ethnic cleansing campaign against the inhabitants of the Donbass.
In spite of Western media descriptions of ‘Russian aggression’ however, Moscow had sought to resolve the conflict in Donbass through peaceful mean via the Minsk Agreements – which would see both Republics granted a degree of autonomy whilst still remaining under the rule of Kiev.
With 14,000 dead in the Donbass conflict, NATO failing to honour a post-Cold War agreement not to expand eastwards, and the subsequent confirmation that US-funded labs were developing bioweapons in Ukraine however, Moscow’s hand was ultimately forced in February of this year when a Russian military intervention was launched into Ukraine in order to remove neo-Nazi elements from power and to destroy any military infrastructure that would ultimately have been used by NATO had Kiev gone on to become a member.
This is where the similarities with Iran and the neighbouring Gulf states of the UAE and Bahrain come into play, with both countries having formalised diplomatic links with Tel Aviv via the September 2020 US-brokered Abraham Accords.
Lauded as a ‘peace deal’ by the then-administration of Donald Trump, despite Israel, the UAE and Bahrain never actually being at war, the ‘normalisation’ agreements, coming eight months after the US had nearly triggered a new Gulf war with the assassination of Iranian Quds Force commander Qasem Soleimani in a drone strike, were seen by many geopolitical observers as a means to contain Iran within the region, a long-time foreign policy aim shared by both Washington and Tel Aviv.
Indeed, despite the relationship between Israel and both states initially starting off on a purely diplomatic basis, the announcement that Israeli radar systems are to be moved into both the UAE and Bahrain marks a dangerous step towards a scenario were Israeli military infrastructure is placed within striking distance of Iran – a situation that would likely lead to a major regional conflict, one that could reach far beyond the Persian Gulf.
Gavin O’Reilly is an Irish Republican activist from Dublin, Ireland, with a strong interest in the effects of British and US Imperialism; he was a writer for the American Herald Tribune from January 2018 up until their seizure by the FBI in 2021, with his work also appearing on The Duran, Al-Masdar, MintPress News, Global Research and SouthFront. He can be reached through Twitter and Facebook and supported on Patreon.
Nuclear-armed states spent $82.4bn on nukes in 2021, US topped list: Report
Press TV – June 15, 2022
The world’s nine nuclear-armed countries – led by the US – spent $82.4 billion upgrading their atomic arsenal in 2021, eight percent more than the previous year, an anti-nuke campaign group has unveiled.
The largest spender by far was the United States, which accounted for more than half the total expenditures on nuclear weapons – followed respectively by China, Russia, Britain, France, India, the Israeli regime, Pakistan and North Korea – the International Campaign to Abolish Nuclear Weapons (ICAN) stated in its annual report, titled “Squandered: 2021 Global Nuclear Weapons Spending.”
“Nuclear-armed states spent an obscene amount of money on illegal weapons of mass destruction in 2021, while the majority of the world’s countries support a global nuclear weapons ban,” the group said in the report, noting that the massive spending nevertheless failed to prevent a war in Europe.
“This spending failed to deter a war in Europe and squandered valuable resources that could be better used to address current security challenges, or cope with the outcome of a still raging global pandemic,” ICAN said. “This corrupt cycle of wasteful spending must be put to an end.”
The group said atomic arms producers had further spent millions of dollars on political lobbying efforts, saying that every $1 spent on lobbying had led to an average of $256 in new contracts involving nuclear weaponry.
“The exchange of money and influence, from countries to companies to lobbyists and think tanks, sustains and maintains a global arsenal of catastrophically destructive weapons,” it said.
The US spent $44.2 billion on atomic weaponry in 2021, followed by China’s $11.7 billion, Russia’s $8.6 billion, the UK’s $6.8 billion, and France’s $5.9 billion, according to the report. India led the more recent nuclear arms developers in expenditures on the mass-destructive weaponry, spending $2.3 billion, followed by the Israeli regime’s $1.2 billion, Pakistan’s $1.1 billion and North Korea’s $642 million.
The report came a week after US-led NATO alliance declared that it did not offer a guarantee to Russia that it would not deploy nuclear weapons on the territories of its two prospective new members, Finland and Sweden.
ICAN’s report further confirmed a statement released by the prominent Stockholm International Peace Research (SIPRI) a day earlier in which it had warned that all the nine nuclear-armed states were increasing or upgrading their arsenals, and that the risk of deployment of such weapons appeared higher now than at any time since the height of the Cold War.
While there is no official confirmation on the amount North Korea spends on nuclear weapons or its arsenal, SIPRI estimates that it possesses as many as 20 warheads.
The Israeli regime, along with India, Pakistan, and South Sudan have never joined the Treaty on the Non-Proliferation of Nuclear Weapons (NPT), an international treaty purportedly established to prevent the spread of nuclear weapons.
As of August 2016, 191 states have become parties to the NPT, though North Korea, which acceded in 1985, announced its withdrawal from the treaty in 2003, following detonation of nuclear devices in violation of core obligations.
Critics of the treaty insist, however, that the NPT cannot stop the proliferation of nuclear arms or the motivation to acquire them, arguing that the biggest possessors and developers of atomic weapons are leading members of the global accord. Officials of the treaty have been selective in enforcing nuclear disarmament, imposing sanctions on observant member nations, such as Iran, while ignoring certain atomic arms possessor and developers such as India, Pakistan, and the Israeli regime, which is widely believe to possess at least 300 nuclear warheads.
Featured Video
Prof. Ted Postol: Iran Already Achieved Nuclear Deterrence Against Israel
or go to
Aletho News Archives – Video-Images
From the Archives
How the occupied mentality syndrome works
Saudi Arabia on the American chessboard – Part 3
By B. J. Sabri | American Herald Tribune | June 27, 2016
Read part 2: “The occupied mentality Syndrome“
Previously I argued whether Saudi Arabia’s repeated involvements in U.S. interventions and wars stem from free national will or in response to a specific condition. For starters, in Saudi Arabia there is no national will. In Saudi Arabia, the national will is the will of the Al Saud clan. Still, when a major Arab state allies itself with a superpower that committed unspeakable crimes against humanity in almost every Arab country, then something is wrong. This fact alone should compel us to examine the U.S.-Saudi relation for one exceptional reason. As a result of the U.S.-Saudi wars, hundreds of thousands of people in Afghanistan, Iraq, Iran, Libya, Syria, Yemen, and Somalia have lost their lives. Millions became displaced in their own homelands. And millions more rendered refugees.
Attributing the Saudi policies to the bonds of “partnership” with the U.S. is frivolous. There are no bonds between these two thugs except those of business, military deals, secret plots, and wars. Proving this point, bonds such as these have no space for the American and Saudi peoples to share significant cultural or societal exchanges. If partnership is not the reason for the Saudi contribution to the U.S. strategy of empire and imperialism, then another reason must exist.
This leads to three possibilities. … continue
Blog Roll
 Aletho News
Aletho News- NIAID/NIH and USDA Fund Bioengineered Chimeric Influenza Viruses Built Using Pandemic H1N1 Components: Journal ‘Science Advances’
- Hezbollah hits Israeli warship off Lebanon’s coast, sets it aflame
- Iran slams US strikes on B1 bridge, Mahshahr petrochemical plants as ‘blatant acts of state terrorism’
- In letter to UN chief, Araghchi warns of dire consequences of US-Israeli attacks on Iran’s nuclear facilities
- Why the CIA conspiracy to invade Iran with Kurdish militias failed
- Why Are Upbeat US Claims About Mission to Rescue Pilot ‘Highly Questionable’?
- Aircraft destroyed during US ‘rescue’ of downed F-15 pilot cost more than $100 million each
- Washington University removes professor who condemned US-Israeli war on Iran
- Russia Warns of Retaliation as UK Authorizes Seizure of Vessels
- Serbia thwarts plot to bomb Russia-Hungary gas pipeline – Vucic
- If Americans Knew
- In Iran, Israel-US take aim at “reason, research, and freedom of thought” – Daily Update
- US loses planes over Iran, Israel downgrades Lebanon war goals – Daily Update
- Israel Is Blocking Palestinians from Easter at Church Where Jesus Resurrected
- Plot to assassinate Palestinian activist follows harassment campaign promoted by Zionist groups and elected officials
- Prominent New York synagogue hosts presentation on why U.S. Jews should support the ethnic cleansing of Gaza
- Tapper vs. Piker: Is the CNN Anchor Auditioning for David Ellison?
- Shouldn’t Democrats Be Able to Condemn Genocide?
- Israel-US kill negotiators, destroy civilian structures, but Iran’s military capabilities still largely intact – Daily Update
- ‘War crime’: Global condemnation as Israeli ministers celebrate death penalty law targeting Palestinian prisoners
- 7 Ways Israel Is Turning Lebanon Into Gaza
- No Tricks Zone
- An Inconvenient Tree: Uncovered In Alps… Europe Much Warmer Than Today 6000 Years Ago
- New Study Reports A 60% Slowdown In Greenland’s Ice Loss Rate In The Last Decade
- Low Intensity Tornado Wrecks Major Solar Farm, Creating A Potential Toxic Dump
- New Study Finds Warming Saves Lives…Cold Temperatures 12 Times More Deadly Than Excess Heat
- German Science Blog Accuses PIK Climate Institute Of Hallucinating Climate Tipping Points
- Devastating Assessment Of Comirnaty Vaccine By Former Senior Pfizer Europe Toxicologist
- New Study: CO2 Is ‘Effectively Negligible’ As An Explanatory Climate Change Factor Since 2000
- Former Pfizer Toxicologist Dr. Helmut Sterz Tells Bundestag Hearing Pfizer Vaccine Should Have Never Been Approved
- Energy Expert: Germany’s Nuclear Phaseout Was A “500 Billion Euro Mistake”
- New Research: South Australia’s Mid-Holocene Sea Surface Temperatures Were 4°C Warmer Than Today
