Keira Bell: My Story

After a landmark court ruling in December, the name “Keira Bell” was cited worldwide, admiringly by some, with hostility by others. (Photo: Paul Cooper/Shutterstock)
By Keira Bell | April 7, 2021
From the earliest days, my home life was unhappy. My parents—a white Englishwoman and a black American who got together while he was in Britain with the U.S. Air Force—divorced when I was about 5. My mother, who was on welfare, descended into alcoholism and mental illness. Although my father remained in England, he was emotionally distant to me and my younger sister.
I was a classic tomboy, which was one of the healthier parts of my early life in Letchworth, a town of about 30,000 people, an hour outside London. Early in childhood, I was accepted by the boys—I dressed in typically boy clothing and was athletic. I never had an issue with my gender; it wasn’t on my mind.
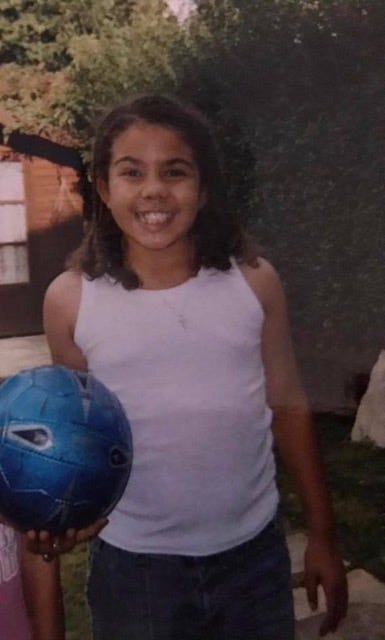
(Courtesy: Keira Bell)
Then puberty hit, and everything changed for the worse. A lot of teenagers, especially girls, have a hard time with puberty, but I didn’t know this. I thought I was the only one who hated how my hips and breasts were growing. Then my periods started, and they were disabling. I was often in pain and drained of energy.
Also, I could no longer pass as “one of the boys,” so lost my community of male friends. But I didn’t feel I really belonged with the girls either. My mother’s alcoholism had gotten so bad that I didn’t want to bring friends home. Eventually, I had no friends to invite. I became more alienated and solitary. I had been moving a lot too, and I had to start over at different schools, which compounded my problems.
By the time I was 14, I was severely depressed and had given up: I stopped going to school; I stopped going outside. I just stayed in my room, avoiding my mother, playing video games, getting lost in my favorite music, and surfing the internet.
Something else was happening: I became attracted to girls. I had never had a positive association with the term “lesbian” or the idea that two girls could be in a relationship. This made me wonder if there was something inherently wrong with me. Around this time, out of the blue, my mother asked if I wanted to be a boy, something that hadn’t even crossed my mind. I then found some websites about females transitioning to male. Shortly after, I moved in with my father and his then-partner. She asked me the same question my mother had. I told her that I thought I was a boy and that I wanted to become one.
As I look back, I see how everything led me to conclude it would be best if I stopped becoming a woman. My thinking was that, if I took hormones, I’d grow taller and wouldn’t look much different from biological men.
I began seeing a psychologist through the National Health Service, or NHS. When I was 15—because I kept insisting that I wanted to be a boy—I was referred to the Gender Identity Development Service, at the Tavistock and Portman clinic in London. There, I was diagnosed with gender dysphoria, which is psychological distress because of a mismatch between your biological sex and your perceived gender identity.
By the time I got to the Tavistock, I was adamant that I needed to transition. It was the kind of brash assertion that’s typical of teenagers. What was really going on was that I was a girl insecure in my body who had experienced parental abandonment, felt alienated from my peers, suffered from anxiety and depression, and struggled with my sexual orientation.
After a series of superficial conversations with social workers, I was put on puberty blockers at age 16. A year later, I was receiving testosterone shots. When 20, I had a double mastectomy. By then, I appeared to have a more masculine build, as well as a man’s voice, a man’s beard, and a man’s name: Quincy, after Quincy Jones.

(Courtesy: Keira Bell)
But the further my transition went, the more I realized that I wasn’t a man, and never would be. We are told these days that when someone presents with gender dysphoria, this reflects a person’s “real” or “true” self, that the desire to change genders is set. But this was not the case for me. As I matured, I recognized that gender dysphoria was a symptom of my overall misery, not its cause.
Five years after beginning my medical transition to becoming male, I began the process of detransitioning. A lot of trans men talk about how you can’t cry with a high dose of testosterone in your body, and this affected me too: I couldn’t release my emotions. One of the first signs that I was becoming Keira again was that—thankfully, at last—I was able to cry. And I had a lot to cry about.
The consequences of what happened to me have been profound: possible infertility, loss of my breasts and inability to breastfeed, atrophied genitals, a permanently changed voice, facial hair. When I was seen at the Tavistock clinic, I had so many issues that it was comforting to think I really had only one that needed solving: I was a male in a female body. But it was the job of the professionals to consider all my co-morbidities, not just to affirm my naïve hope that everything could be solved with hormones and surgery.
Last year, I became a claimant against the Tavistock and Portman NHS Foundation Trust in a judicial-review case, which allows petitioners in Britain to bring action against a public body they deem to have violated its legal duties. Few judicial reviews get anywhere; only a fraction obtain a full hearing. But ours did, with a panel of three High Court judges considering whether youths under treatment at the clinic could meaningfully consent to such medical interventions.
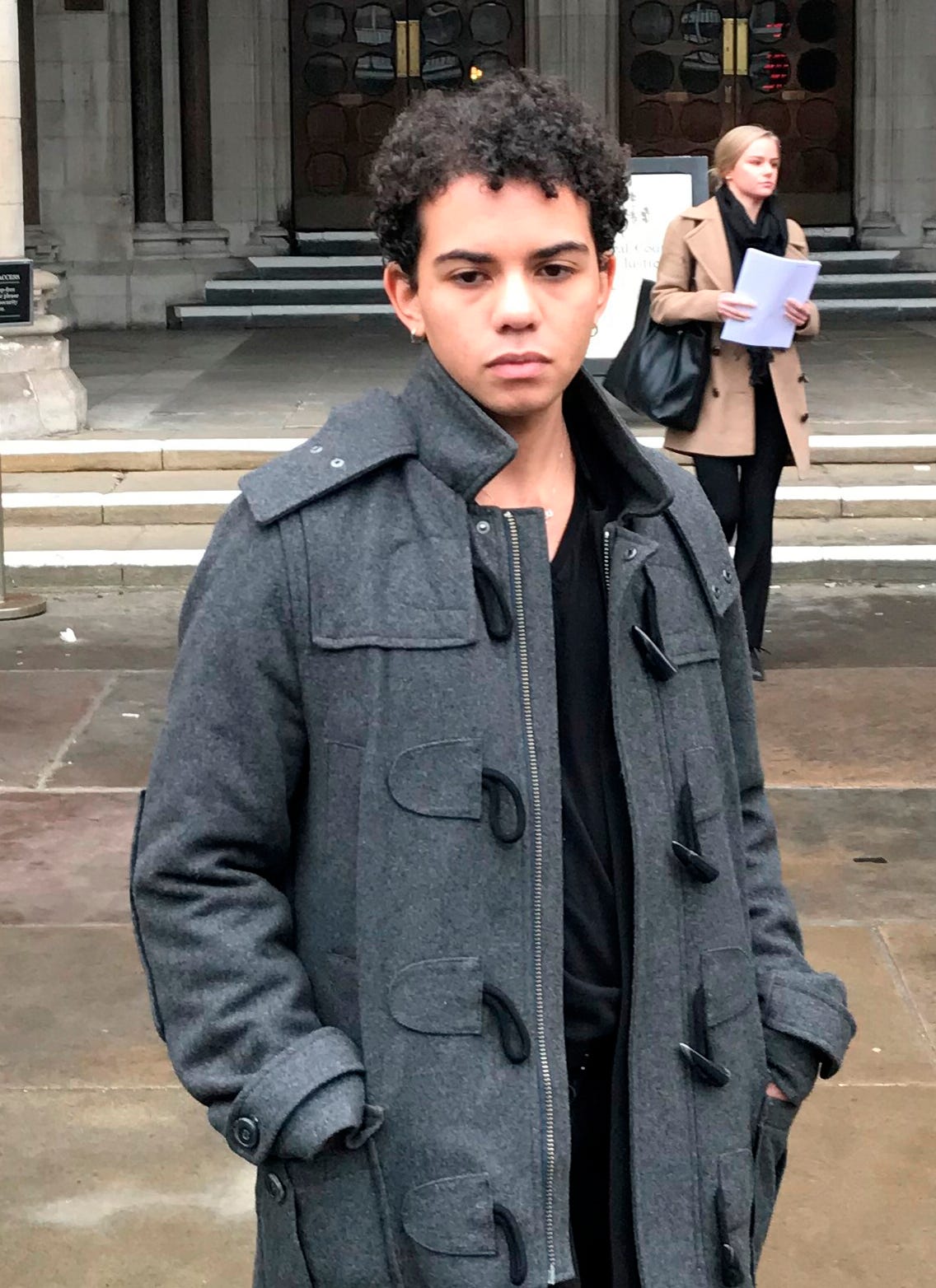
Bell in January 2020, after she brought legal action against the clinic. (Photo: Sam Tobin/PA Wire)
My team argued that the Tavistock had failed to protect young patients who sought its services, and that—instead of careful, individualized treatment—the clinic had conducted what amounted to uncontrolled experiments on us. Last December, we won a unanimous verdict. The judges expressed serious doubts that the clinic’s youngest patients could understand the implications of what amounted to experimental treatment with life-altering outcomes.
In their ruling, the judges repeatedly expressed surprise at what had been going on at the Tavistock, particularly its failure to gather basic data on its patients. They noted the lack of evidence for putting children as young as 10 years old on drugs to block puberty, a treatment that is almost universally followed by cross-sex hormones, which must be taken for life to maintain the transition. They also had concerns about the lack of follow-up data, given “the experimental nature of the treatment and the profound impact that it has.”
Notably, a growing wave of girls has been seeking treatment for gender dysphoria. In 2009-10, 77 children were referred to the Gender Identity Development Service, 52% of whom were boys. That ratio started to reverse a few years later as the overall number of referrals soared. In England in 2018-19, 624 boys were referred and 1,740 girls, or 74% of the total. Over half of referrals were for those aged 14 or under; some were as young as 3 years old. The court noted the practitioners at the Tavistock did not put forward “any clinical explanation” for the dramatic rise in girls, and expressed surprise at its failure to collate data on the age of patients when they began puberty blockers.
The ruling does not completely prevent a minor from beginning a medical transition. But the judges recommended that doctors consider getting court permission before starting such treatment for those 16 to 17; they concluded it was “very doubtful” that patients aged 14 and 15 could have sufficient understanding of the consequences of the treatment to give consent; and that it was “highly unlikely” for those aged 13 and under.
In response, the NHS said that the Tavistock had “immediately suspended new referrals for puberty blockers and cross-sex hormones for the under-16s, which in future will only be permitted where a court specifically authorizes it.” The Tavistock appealed the ruling, and the court will hear its appeal in June.
The puberty blockers that I received at 16 were designed to stop my sexual maturation: The idea was that this would give me a “pause” to think about whether I wanted to continue to a further gender transition. This so-called “pause” put me into what felt like menopause, with hot flushes, night sweats, and brain fog. All this made it more difficult to think clearly about what I should do.
By the end of a year of this treatment, when I was presented with the option of moving on to testosterone, I jumped at it—I wanted to feel like a young man, not an old woman. I was eager for the shots to start, and the changes this would bring. At first, the testosterone gave me a big boost in confidence. One of the earliest effects was that my voice dropped, which made me feel more commanding.
Over the next couple of years, my voice deepened further, my beard came in, and my fat redistributed. I continued to wear my breast binder every day, especially now that I was completely passing as male, but it was painful and obstructed my breathing. By the time I was 20, I was being treated at the adult clinic. The testosterone and the binder affected the appearance of my breasts, and I hated them even more. I also wanted to align my face and my body, so got a referral for a double mastectomy.
My relationship with my parents continued to be difficult. I was no longer speaking to my mother. My father had kicked me out of his apartment shortly after I turned 17, and I went to live in a youth hostel. He and I were still in touch, though he was adamantly opposed to my transition. Reluctantly, he took me for the surgery. I was a legal adult when it took place, and I don’t relieve myself of responsibility. But I had been put on a pathway—puberty blockers to testosterone to surgery—when I was a troubled teen. As a result of the surgery, there’s nerve damage to my chest, and I don’t have sensation the way I used to. If I am able to have children, I will never breastfeed them.
Around the end of that first year post-surgery, something started happening: My brain was maturing. I thought about how I’d gotten where I was, and gave myself questions to contemplate. A big one was: “What makes me a man?”
I started realizing how many flaws there had been in my thought process, and how they had interacted with claims about gender that are increasingly found in the larger culture and that have been adopted at the Tavistock. I remembered my idea as a 14-year-old, that hormones and surgery would turn me into someone who appeared to be a man. Now, I was that person. But I recognized that I was very physically different from men. Living as a trans man helped me acknowledge that I was still a woman.
I also started to see what I was living out was based on stereotypes, that I was trying to assume the narrow identity of “masculine guy.” It was all making less and less sense. I was also concerned about the effect my transition would have on my ability to find a sexual partner.
Then there was the fact that no one really knew the long-term effects of the treatment. For instance, the puberty blockers and testosterone caused me to have to deal with vaginal atrophy, a thinning and fragility of the vaginal walls that normally occurs after menopause. I started feeling really bad about myself again.
I decided to stop, cold turkey. When I was due for my next testosterone shot, I canceled the appointment.
After I came to this decision, I found a subreddit for detransitioners. The number of people on it started rising, as if all these young women had come to a collective realization of the medical scandal we had been a part of. It was a place we could talk about our experiences and support each other. I felt liberated.
What happened to me is happening across the Western world. Little of my case was a surprise to those paying attention to the Tavistock whistle-blowers who in recent years have spoken out in alarm to the media, sometimes anonymously. Some have left the service because of these concerns. But the transgender issue is now highly political and wrapped up in questions of identity politics. It can be perilous to raise questions or doubts about young people’s medical gender transitions. Some who have done so have been vilified and had their careers threatened.
At the Tavistock, practitioners provide “gender affirmative care”—in practice, this means that when children and teens declare a desire to transition, their assertions are typically accepted as conclusive. Affirmative care is being adopted as a model in many places. In 2018, the American Academy of Pediatrics released a policy statement on the treatment of young people who identify as transgender and gender diverse that advocated for “gender-affirmative care.”
But former Tavistock practitioners have cited varied problems suffered by the kids who sought help, such as sexual abuse, trauma, parental abandonment, homophobia in the family or at school, depression, anxiety, being on the autism spectrum, having ADHD. These profound issues, and how they might be tied up with feelings of dysphoria, have often been ignored in favor of making transition the all-purpose solution.
As the High Court found, much of the clinic’s treatment is not even based on solid evidence. At the time our case was accepted, the NHS was asserting that the effects of puberty blockers are “fully reversible.” But recently, the NHS reversed itself, acknowledging “that ‘little is known about the long-term side-effects’ on a teenager’s body or brain.” That didn’t stop them from prescribing these drugs to people like me.
Dr. Christopher Gillberg, a professor of child and adolescent psychiatry at Gothenburg University in Sweden and a specialist in autism, was an expert witness for our case. Gillberg said in his court statement that over his 45 years of treating children with autism, it was rare to have patients with gender dysphoria—but their numbers started exploding in 2013, and most were biological girls. Gillberg told the court that what was happening at the Tavistock was a “live experiment” on children and adolescents.
Parents who are reluctant or even alarmed about starting their children on a medical transition may be warned, “Would you rather have a dead daughter or a live son?” (Or vice versa.) I had suicidal thoughts as a teen. Suicidal thoughts indicate serious mental health problems that need assessment and proper care. When I told them at the Tavistock about these thoughts, that became another reason to put me on hormones quickly to improve my well-being. But after the court ruling, the Tavistock released an internal study of a group of 44 patients who had started taking puberty blockers at ages 12 to 15. It said that this treatment had failed to improve the mental state of patients, having “no significant effect on their psychological function, thoughts of self-harm, or body image.” Additionally, of those 44 patients, 43 went on to cross-sex hormones. This suggests blocking puberty isn’t providing a pause. It is giving a push.
Before beginning on testosterone, I was asked if I wanted children, or if I wanted to consider freezing my eggs because of the possibility that transition would make me infertile. As a teenager, I couldn’t imagine having kids, and the procedure wouldn’t have been covered by the NHS. I said I was fine if I couldn’t, and I didn’t need to freeze my eggs. But now as a young adult, I see that I didn’t truly understand back then the implications of infertility. Having children is a basic right, and I don’t know if that has been taken from me.
As part of its defense, the Tavistock put forth statements from a few young trans people who are happy with their care. One is S, a 13-year-old trans boy who got puberty blockers from a private provider because the waiting list at the Gender Identity Development Service was so long. S told the court that he had “no idea what me in the future is going to think” about being able to have children and that since he has never been in “a romantic relationship,” the idea of one is not “on my radar at the moment.”
Lots of teenagers, when contemplating future sexual relationships, feel baffled and even disturbed at the thought. Those same people, when adults, often feel very differently. I know, because this happened to me. I’d never been in a sexual relationship at the time of my transition, so I didn’t truly understand what the transition would mean sexually.
S’s statement demonstrates how difficult it is for minors to give consent for procedures they can’t yet understand. As the judges wrote, “There is no age-appropriate way to explain to many of these children what losing their fertility or full sexual function may mean to them in later years.”

Bell speaking to the media after the court ruling last December. (Photo: Sam Tobin/PA Wire)
Today, at 24, I’m in my first serious relationship. My partner is very supportive of everything I do, and I am the same for her. She has a large group of female friends who accept me; it’s been very healing. For now, I don’t speak to either of my parents or have a relationship with them.
I still get taken for male sometimes. I expect that, and I’m not angry about it. I know that I will live with that for the rest of my life. What I am angry about is how my body was changed at such a young age. People want to know if I’m going to have reconstructive surgery of my breasts or do other things to make me look more female. But I haven’t fully processed the surgery I had to remove my breasts. For now, I want to avoid more such surgical procedures.
When I joined the case, I didn’t realize how big it would become. What has happened since the ruling has been a rollercoaster. Many people have thanked me. I have also been attacked online. If you’re someone who regrets transitioning and decides to speak out about your experiences, you’re considered a bigot. You may be told that you’re trying to take away trans rights, that children know what’s best for themselves and their bodies, and that you’re ruining kids’ lives.
But I am focused on what is best for distressed young people. A lot of girls are transitioning because they’re in pain, whether it’s from mental-health disorders, or life trauma, or other reasons. I know what it’s like to get caught up in dreaming that transitioning will fix all of this.
Although sharing my story has been cathartic, I still struggle, and have yet to receive appropriate therapy. As I go on with my life, I plan to continue to be an activist on behalf of this cause. I want the message of cases like mine to help protect other kids from taking a mistaken path. This year, I helped create the first Detrans Awareness Day, on March 12. I hope that, in years to come, this day can be a beacon to empower others.
I do not believe in rigid gender expression. People should be comfortable and feel accepted if they explore different ways of presenting themselves. As I said in my statement after the ruling, this means stopping the homophobia, the misogyny, and the bullying of those who are different.
I also call on professionals and clinicians to create better mental health services and models to help those dealing with gender dysphoria. I do not want any other young person who is distressed, confused, and lonely as I was to be driven to conclude transition is the only possible answer.
I was an unhappy girl who needed help. Instead, I was treated like an experiment.
Justice Department Accused of Taking Attorney-Client Material at Mar-a-Lago
By Jonathan Turley | August 14, 2022
Fox News is reporting that the FBI seized boxes containing attorney-client privileged and potentially executive privileged material during its raid Mar-a-Lago. When the raid occurred, I noted that the legal team had likely marked material as privileged at the residence and that the collection could create an immediate conflict over such material. Now, sources are telling Fox that the Justice Department not only took attorney-client material but has refused Trump requests for a special master to review the records.
The request for a special master would seem reasonable, particularly given the sweeping language used in the warrant. It is hard to see what material could not be gathered under this warrant.
Attachment B of the warrant has this provision:
“Any physical documents with classification markings, along with any containers/boxes (including any other contents) in which such documents are located, as well as any other containers/boxes that are collectively stored or found together with the aforementioned documents and containers/boxes; b.. Information, including communications in any form, regarding the retrieval, storage, or transmission of national defense information or classified material”
Thus, the agents could not only take an entire box if it contained a single document with classification markings of any kind but could then take all boxes around that box.
It is not surprising that dozens of boxes were seized.
Given that sweeping language (and the various lawsuits and investigations facing Trump), it would seem reasonable to request a special magistrate. That is why the reported refusal is so concerning. What is the harm from such a review? The material is now under lock and key. There is no approaching deadline in court or referenced grand jury.
Moreover, many have accused the Justice Department of using this search as a pretext. While saying that they were seeking potential national security information, critics have alleged that the real purpose was to gather evidence that could be used against Trump in a prosecution over his role in January 6th riot. I have noted that such a pretext would be deeply disturbing given the documented history of Justice Department officials misleading or lying to courts in prior Trump-related investigations. The continuation of such subterfuge could be disclosed in a later oversight investigation.
The use of a special master could have helped quell such claims of a pretextual search. Conversely, the denial of such a protective measure would fuel even greater concerns.
The refusal to take this protective measures is almost as troubling as the sweeping language in the search warrant itself. We need to see the affidavit that led to this search warrant. I am not going to assume that the search was unwarranted until I see that evidence. However, in the interim, Attorney General Merrick Garland could have allowed accommodations for this review to assure not just the Trump team but the public that the search was not a pretext for seeking other evidence like January 6th-related material.
Did the BBC unwittingly reveal the true proportion of unvaccinated as at least 20%
Norman Fenton | August 12, 2022
In the BBC2 documentary “Unvaccinated” it was claimed that only 8% of the UK adult population is unvaccinated.
This is the ONS figure and we challenged this: https://www.normanfenton.com/post/bbc…
But for the programme itself the BBC commissoned a large survey which, we show, revealed that 26% were unvacinated.
To understand why it is so critical to get an accurate estimate of the proportion of unvaccinated see this 2 minute accompanying video: https://youtu.be/8It4qI9yhzQ
A Drought In Germany Gets The Media Overexcited
By Paul Homewood | Not A Lot Of People Know That | August 14, 2022
There is a drought in Germany, and naturally the media has gone into hyperdrive to link it to global warming:
Drought hits Germany’s Rhine River: ‘We have 30cm of water left’
This report is all over the media, and all with virtually the same wording, suggesting a carefully coordinated, manufactured story, almost certainly from one of the well funded, climate misinformation organisations.
The BBC headline is grossly misleading, as the 30cm is the water under the boat; As Captain Kempl comments, the river depth is actually 1.5m.
The river gauge measurement of 42cm at Kaub is also widely reported, but is equally misleading, as this measurement is taken near the river bank, rather than at the deepest part of the stream.
In none of the dozens of reports I have read is there any actual historical data to compare against this event, whether rainfall or water level data. We are told this is the lowest water level since 2018, as if this means anything at all. There is no evidence presented to show that this drought is in any way unprecedented, or that droughts are becoming more extreme; merely this claim that appears in most of the articles:
“HGK and other shipping companies are preparing for a “new normal” in which low water levels become more common as global warming makes droughts more severe, sapping water along the length of the Rhine from the Swiss Alps to the North Sea.
“There’s no denying climate change and the industry is adjusting to it,”
However, annual rainfall trends at Mainz, which is just upstream of Kalb, show that while recent years have been drier than the 1980s and 90s, they are no drier than the 1950s. We also see exactly the same trends with April to September rainfall:


And finally, WUWT offers an insight to some of the megadroughts in Germany in the past, notably in 1540.
There is therefore nothing to suggest that this is not just another weather event.
Featured Video

BIRX POINTS THE FINGER AT FAUCI, DENIES LOCKDOWN BLAME
or go to
Aletho News Archives – Video-Images
From the Archives
There are ZERO Amish kids suffering from cancer, diabetes or autism – WHY IS THAT?
YourDestinationNow | July 8, 2023
The current population of Amish folks in America is quickly approaching 400,000, with the largest concentrations of 90,000 in Pennsylvania and 82,000 in Ohio. Amish have settled in as many as 32 US states, and have an average of 7 kids per family, so the population is growing rapidly. In a brand new, comprehensive study (as of June 2023), presented by Steve Kirsch to the Pennsylvania State Senate, it was calculated that for Amish children, who are strictly 100 percent not vaccinated (fully unvaccinated), typical chronic conditions barely exist, if any at all. … continue
Blog Roll
 Aletho News
Aletho News- BIRX POINTS THE FINGER AT FAUCI, DENIES LOCKDOWN BLAME
- Russian Strike on US Drone Factory in Kiev Makes Clear – NATO’s Overseas MIC Footprint Is Fair Game
- Merz readies secret plan to move German troops to Russian border – media
- With Karim Khan’s dismissal, the elimination of the war crimes court is near-complete
- UK charges over 1,500 people over signs opposing Israel’s genocide of Palestinians in Gaza
- Islamic Jihad says reported deal between Palestinian factions, Israel ‘inaccurate’
- Israeli army detonates 700 tons of explosives near Lebanon’s historic Beaufort Castle
- Ceuta crisis sparks online speculation over Israel’s role in pressuring Spain
- Saudi Arabia preps for ‘major’ land, sea operations against Ansarallah in Yemen: Report
- Iran Army hits US base in Kuwait as satellite images show fresh damage
- If Americans Knew
- The Satanic Hazing Rituals of the IDF
- Israel Is Paying Millions to Train AI Chatbots How to Talk About Gaza. It’s Working.
- Right now, it’s all about what “Netanyahu wants” – Daily Update
- The Killing of Awdah Hathaleen: Beyond a Settler Crime
- Republican Voters are Turning against the Iran War
- Haley Stevens Is an Enemy of International Law
- Were the first Zionists Christian? A review.
- Ben Gvir’s crocodiles are the latest weapon in Israel’s animal warfare on Palestinians
- CIA Assessment Details Israel’s Race to Make the U.S.-Israel Alliance Irreversible
- How much is your support for Israel worth? Try $1 billion.
- No Tricks Zone
- Germany’s Industrial Suicide… Grid Agency Prepares Secret Power Rationing Plans Amid Electric Power Bottlenecks
- ECMWF Models Throwing Cold Water On Extreme Germany Heat Wave Forecast Next Week
- Greenland’s Ice Sheet Was Supposed To Be Rapidly Melting Away. It Hasn’t Been.
- Global Temperature Trend Has Cooled Over The Past 6500 Years, Scientists Have Found
- Wind Energy Means Going Back To The Middle Ages, Says German Professor Horst-Joachim Lüdecke
- New Study: A 40-Fold Increase In Earth’s Main Greenhouse Gas Contributes To Cooling The Ocean
- New Study Highlights The ‘Dominant Role’ Of Aerosol/Cloud Interactions In Shaping Climate
- Munich’s First-Ever Green Party Mayor Declares First Ever City Water Use Restrictions… Fines Up to 50,000 €!
- Experimental Lab Research: The Climate Sensitivity To A 400-Fold Increase In CO2 Is 0.1°C
- Fatal Snobbery: In France, It’s Better To Die From A Heatwave Than To Do As Americans
