A new study published in the New England Journal of Medicine has demonstrated that people who are triple-vaccinated (boosted) against COVID recover significantly more slowly from COVID infection and remain contagious for longer than people who are not vaccinated at all.
The study did not deal with the severity of illness with or without a vaccine.
Researchers swabbed infected people and cultured the swabs, repeating the process for over two weeks until viral replication was not observed.
At five days post-infection, less than 25 percent of unvaccinated people were still contagious, whereas around 70 percent of boosted people were still carrying viable virus particles. For those partially vaccinated, around 50 percent were still contagious at this point.
Even more strikingly, at ten days post-infection, one-third of boosted people (31 percent) were found to still be carrying live, culturable virus. By contrast, just six percent of unvaccinated people were still contagious at day 10.
In other words, people who have received a booster shot are five times more likely still to be contagious at ten days post-infection than are unvaccinated people.
The findings go a long way to explaining why Paxlovid, Pfizer’s anti-viral medication, is often not effective for people who have been vaccinated against COVID, with many experiencing a recurrence of symptoms along with a positive COVID test after completing the five-day regimen (as recently occurred with quadruple-vaccinated Dr. Anthony Fauci). This phenomenon is known as COVID rebound.
Meanwhile, Israeli Health Ministry data shows that in the older population (those over the age of 60), having submitted to more COVID shots often correlates to a greater likelihood of becoming infected with COVID.
Israel Ministry of Health
The blue line represents the unvaccinated; light-green is the partially-vaccinated; dark-green is those who have received a booster shot within the past six months.
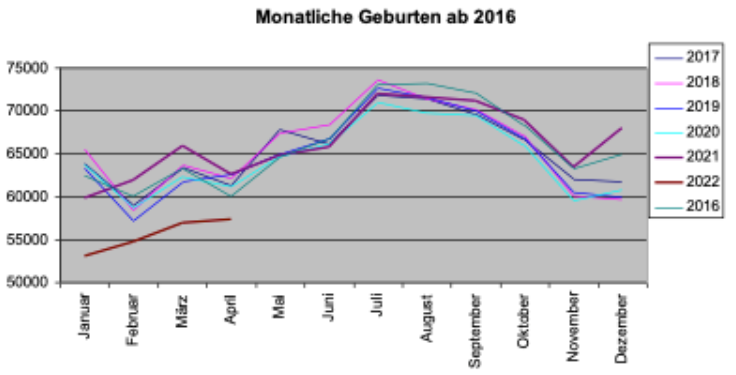
Germany has seen a “dramatic drop” in birthrate during the first 4 months of 2022, according to transitionnews.de, leading to rising suspicions over COVID vaccine safety.
“Compared to the previous year, the number of births has fallen by 12 percent – that’s about 25,000 fewer births in the first four months of 2022,” reports Sternfried Müller of transitionnews.de.
The above chart shows the number of births for the January-April period each year since 2018. During the Corona years of 2020 and 2021, Germany saw a rise in the number of births, climbing to 250,000 births. But in 2022, the number of births mysteriously plummeted a whopping 12%!
Something unusual must have triggered the phenomenon. Going back 9 months prior to the January-April 2022 period takes us to the April to July 2021 period, which coincides to COVID vaccination of younger adults in earnest. Remarkably, Germany’s media have been silent on the latest published statistics, issued by the German Federal Statistical Office (Destatis).
The next transitionnews.de chart shows the monthly number of births and just how dismally 2022 lags so far compared to the previous years:
A number of reasons have been proposed to explain the dramatic decline, among them fewer marriages. But that remains highly doubtful.
There are increasing suspicions that it is vaccine linked, as some studies already suggest: see here and here.
For the time being German authorities obstinately continue to remain in denial mode when it comes the the adverse effects of the COVID vaccines. Currently the Ministry of Health is gearing up to roll out another mass wave of vaccinations and restrictions in the run-up to the fall flu season.
A former Washington State University football coach is seeking $25 million from the university for wrongful termination after he was fired last year for refusing to get vaccinated against COVID-19, The Seattle Times reported Tuesday.
A tort claim was filed April 27 on behalf of Nick Rolovich with the state’s risk management office. Filing a claim is a prerequisite to filing a lawsuit against a state agency.
There’s a 60-day waiting period between when a claim is filed and when the claimant can file a lawsuit. As of Wednesday, a spokesperson for Attorney General Bob Ferguson said no suit had been filed, according to The Washington Post.
After denying Rolovich’s request for a religious exemption from Gov. Jay Inslee’s COVID-19 vaccine mandate for state employees, the university in October 2021 fired Rolovich.
At the time of his firing, Rolovich was subject to a five-year contract with three seasons remaining and was paid $3.2 million per year — the highest public salary in the state. He had coached 11 games with the Cougars over two seasons.
Rolovich’s attorney, Brian Fahling, said at the time his client would take legal action for religious discrimination. He filed a 34-page letter with the university appealing the university’s decision to fire Rolovich, but the appeal was denied.
Rolovich, a Catholic, is not the first person to file a claim for wrongful termination or religious discrimination over an employer’s failure to grant a religious exemption to a COVID-19 vaccine mandate.
Liberty Counsel on July 29 settled the nation’s first class action lawsuit on behalf of healthcare workers who were unlawfully discriminated against and denied religious exemptions to the COVID-19 vaccine mandate by their employer, Chicago-based NorthShore University HealthSystem.
The $10,337,500 settlement, filed in the federal Northern District Court of Illinois, compensates NorthShore employees who were “punished for their religious beliefs against taking an injection associated with aborted fetal cells.”
As part of the settlement agreement, NorthShore also will change its unlawful “no religious accommodations” policy to make it consistent with the law and must provide religious accommodations in every position across its numerous facilities.
In addition, employees who were terminated because they refused to receive a COVID-19 vaccine on religious grounds will be eligible for rehire if they apply within 90 days of the final settlement approved by the court, and they will retain their previous seniority level.
The amount of individual payments from the settlement fund will depend on how many valid and timely claim forms are submitted during the claims process.
If the settlement is approved by the court and nearly all of the affected employees file valid and timely claims, it is estimated employees who were terminated or resigned because of their religious refusal of a COVID-19 vaccine will receive approximately $25,000 each.
Also under the settlement, employees who were forced to get the shot against their religious beliefs to keep their jobs will receive approximately $3,000 each.
The 13 healthcare workers who are lead plaintiffs in the lawsuit will receive an additional approximate payment of $20,000 each for their role in bringing this lawsuit and representing the class of NorthShore healthcare workers.
Lawsuits over denied exemptions or insufficient accommodations to COVID-19 vaccine requirements began last September after the U.S. Food and Drug Administration granted full approval to the Pfizer-BioNTech Comirnaty vaccine, allowing more employers to enact vaccine mandates.
Workers as of May 19, 2022, had filed at least 66 lawsuits since September 2021 against private employers for refusing to grant exemptions to COVID-19 vaccine requirements, according to Bloomberg Law.
Judges rejected workers’ requests for immediate court orders blocking enforcement of mandates in 22 cases.
In one case involving United Airlines Inc., the airline changed its policy allowing accommodations rather than contest the lawsuit.
According to Bloomberg Law, 59% of lawsuits filed over COVID-19 vaccine mandates are related to an employer’s response to faith-based requests for accommodation.
About 22% of lawsuits involve contesting a company’s handling of both religious and disability requests and 5% involve health-related accommodations.
Megan Redshaw is a staff attorney for Children’s Health Defense and a reporter for The Defender.
Twitter will start censoring “disputed claims,” “potentially harmful and misleading information,” and “false” information about the 2022 US midterms from today under its “Civic Integrity Policy.”
Tweets that fall foul of this policy will be removed or labeled with links to “credible information” or “helpful context.” Labeled tweets aren’t amplified or recommended by Twitter and the platform also dissuades or prevents users from liking and sharing labeled tweets. Twitter also noted that its latest label design reduces likes by 10%, reduces replies by 13%, and reduces retweets by 10%.
Users who have tweets removed or labeled under this policy are subject to Twitter’s five strikes system. The account owner is given two strikes if their tweet is deleted and one strike if their tweet is labeled. 2-4 strikes results in a temporary account lock and five strikes results in a permanent account suspension.
In addition to censoring tweets, Twitter will also start artificially boosting content that it deems to be “reliable” by displaying this content prominently on the “Home” and “Search” tabs and promoting it in the “Explore” tab.
Twitter’s Civic Integrity Policy resulted in mass censorship in the run-up to the 2020 US presidential election. The rule banning “disputed claims that could undermine faith in the process itself, such as unverified information about election rigging, ballot tampering, vote tallying, or certification of election results” was used to justify much of this censorship with users that discussed election discrepancies often targeted.
Many of former President Trump’s statements about the election were censored under this policy before he was permanently banned. This same policy was also used to mass censor other users and tweets before and after the 2020 election.
The World Economic Forum is becoming a little concerned. Unapproved opinions are becoming more popular, and online censors cannot keep up with millions of people becoming more aware and more vocal. The censorship engines employed by Internet platforms, turned out to be quite stupid and incapable. People are even daring to complain about the World Economic Forum, which is obviously completely unacceptable.
So, WEF author Inbal Goldbergercame up with a solution: she proposes to collect off-platform intelligence from “millions of sources” to spy on people and new ideas, and then merge this information together for “content removal decisions” sent down to “Internet platforms”.
To overcome the barriers of traditional detection methodologies, we propose a new framework: rather than relying on AI to detect at scale and humans to review edge cases, an intelligence-based approach is crucial.
By bringing human-curated, multi-language, off-platform intelligence into learning sets, AI will then be able to detect nuanced, novel abuses at scale, before they reach mainstream platforms. Supplementing this smarter automated detection with human expertise to review edge cases and identify false positives and negatives and then feeding those findings back into training sets will allow us to create AI with human intelligence baked in. Thismore intelligent AI gets more sophisticated with each moderation decision, eventually allowing near-perfect detection, at scale.
What is this about? What’s new?
The way censorship is done these days is that each Internet platform, such as Twitter, has its own moderation team and a decision making engine. Twitter would only look at tweets by any specific twitter user, when deciding on whether to delete any tweets or suspend their authors. Twitter moderators do NOT look at Gettr or other external websites.
So, for example, user @JohnSmith12345 may have a Twitter account and narrowly abide by Twitter rules, but at the same time have a Gettr account where he would publish anti-vaccine messages. Twitter would not be able to suspend @JohnSmith12345’s account. That is no longer acceptable to the WEF because they want to silence people and ideas, not individual messages or accounts.
This explains why the WEF needs to move beyond the major Internet platforms, in order to collect intelligence about people and ideas everywhere else. Such an approach would allow them to know better what person or idea to censor — on all major platforms at once.
They want to collect intelligence from “millions of sources”, and train their “AI systems” to detect thoughts that they do not like, to make content removal decisions handed down to the likes of Twitter, Facebook, and so on. This is a major change from the status quo of each platform deciding what to do based on messages posted to that specific platform only.
For example, in addition to looking at my Twitter profile, WEF’s proposed AI would also look at my Gettr profile, and then it would make an “intelligent decision” to remove me from the Internet at once. It is somewhat of a simplification because they also want to look for ideas and not only individuals but, nevertheless, the search for wrongthink becomes globalized.
This sounds like an insane conspiracy theory from hell: WEF collecting information on everyone everywhere, and then telling all platforms what posts to remove, based on a global decision-making AI engine that sees everything and can identify individual people and ideas beyond any given platform.
If someone ever told me that it would be contemplated, I would probably think that this person is insane. It sounds like a sick technological fantasy. Unfortunately, this crazy stuff is real, is in a WEF agenda proposal that is officially posted on their website’s “WEF Agenda” section. And WEF is not messing around.
France is an important factor in Europe’s energy supply. But the country is planning on shutting down more than half of its nuclear reactors. The reason given is that they supposedly need maintenance.
The energy exporter is going to have to access energy from abroad. But that can turn out to be more difficult than planned with the European energy crisis expanding. Is a mega blackout looming?
Some 56 nuclear reactors at 18 locations normally supply France with electricity. But 18 of these reactors are already shut down. Long-term maintenance work is to be carried out. That had been planned for a long time, authorities said. But then France also had to shut down 12 more reactors last week.
Damage caused by corrosion is said to be the reason for this. The supply in Europe’s power grid seems all the more uncertain in winter.
In many places, the European power grid is dependent on the energy security of the neighboring country. If a country fails over a large area, other states are drawn into the blackout. France has been an important factor in European energy supply in recent years. But the Grande Nation itself may have to switch to energy imports.
Any ‘Plan B’ in the talks on the Iranian nuclear program would violate a “consensus decision” of the UN Security Council on the issue and have “unavoidable negative consequences” for the entire Middle East, the Russian Foreign Ministry warned on Thursday.
“Any departure [from the original 2015 deal] or ‘Plans B’ that some people like to speculate about would run counter to the consensus decisions of the [UN] Security Council,” said Ivan Nechaev, the ministry’s deputy spokesman, referring to a 2015 UNSC resolution supporting that year’s agreement on the Iranian nuclear program.
The revival of the existing 2015 deal through the ongoing talks in Vienna is the only “reasonable and effective way” forward, Nechaev told journalists during a briefing. He also welcomed the latest round of indirect talks between the US and Iranian delegations in Vienna, which resulted in some “progress” on issues that had earlier been a stumbling block in the negotiations.
“A positive result of the talks is… achievable,” Nechaev said, adding that “there are no irreconcilable differences between the parties. Further progress would solely depend on each side’s “political will,” the diplomat said.
At the same time, Moscow slammed the EU for what it called the bullying tactics. “The language of ultimatums does not work in such a sensitive and high-stakes issue,” Nechaev said as he particularly criticized Peter Stano, the spokesman for EU diplomatic chief Josep Borrell.
Earlier this week, Stano told journalists that “everything that could be negotiated has been incorporated into the final version of the text” compiled after the latest round of talks between Tehran and Washington, which was mediated by the EU. “It’s yes or no,” Stano insisted, adding that “there is no more room for other compromises.” Borrell himself also called the document “the final text” at that time.
On Thursday, the Russian Foreign Ministry responded by saying Stano had no authority to make such statements on behalf of all parties involved in the talks. The Iranian deal, also known as the Joint Comprehensive Plan of Action (JCPOA), was built on “carefully measured balance of interests” and not “crude political pressure,” it added.
The work on reviving the deal will only end “when interests of all parties involved are properly taken into account,” Nechaev told journalists on Thursday.
Last week, Washington said it developed a proposal for a mutual return to the nuclear deal with Iran. Tehran responded by saying the revival of the agreement relies primarily on the US’ “will” and that Washington must show its readiness to achieve a long-term result.
The Western media have also been publishing pieces calling on Washington and Brussels to work out a ‘Plan B’ that can be used if the Vienna negotiations yield no results. Some of the pieces openly called on Western governments to ditch the talks in favor of this option, which has apparently yet to be devised. “Enough of the ‘tenuous’ Iran nuclear deal – it’s time for Plan B,” read an opinion piece The Hill published in early July. “Biden Should Show Iran What ‘Plan B’ Looks Like,” another piece published by the Washington Post in mid-June suggested.
The deal signed in 2015 by Iran, the US, the UK, France and Germany – as well as Russia, China and the EU – involved Tehran agreeing to certain restrictions on its nuclear industry in exchange for the lifting of economic sanctions and other incentives.
The agreement has been in limbo since 2018 when it was torpedoed by the US under then-President Donald Trump, who unilaterally withdrew from it. In response, Iran started gradually reducing its commitments under the accord, such as the level of enriched uranium it produces.
On August 1, Tehran announced it has “the technical ability to build an atomic bomb,” adding, however, that such a program “is not on the agenda.”
Canada’s RCMP and its commissioner Brenda Lucki are fending off requests to reveal if the police force used malware to also spy on members of the country’s parliament (MPs).
The bombshell question was posed in a request filed by the House of Commons Standing Committee on Access to Information, Privacy, and Ethics – but Lucki’s response provided no useful response.
When it comes to wiretapping MPs and other employees of the parliament – “this information will not be provided by the RCMP,” Lucki brushed the question off, according to media reports out of Canada.
Earlier, these reports noted that the RCMP have been using spyware for a decade now (on-device investigation tools, ODITs, that not only record communications, but are installed on the targeted mobile devices) – to access cameras and microphones; and the law enforcement agency confirmed it.
Naturally, those holding public office in Canada, particularly those from the ranks of the opposition, then wanted to know if they, by any chance, had been subjected to this type of surveillance via government-deployed spyware.
Public Safety Minister Marco Mendicino reportedly avoided responding, unlike Lucki who’s now unapologetically suggesting that Canada’s democracy doesn’t stretch quite as far as providing this type of information to its legislators.
Opposition Conservatives are rattled by the whole affair. MP Pat Kelly noted that a parliamentary committee should have unfettered powers to request these documents.
“A blanket refusal to a committee is troubling,” Kelly is quoted as saying.
And a troubling development of this kind in any parliamentary democracy raises so many questions. One came from a Bloc Québécois MP – who asked RCMP commissioner for national security Mark Flynn if the office of the Federal Privacy Commissioner was involved in evaluating if the spyware in question was in compliance with Canada’s Privacy Act.
Flynn’s response was, “No.”
But one of Canada’s former privacy commissioners, Daniel Therrien, was far more forthcoming when he commented on RCMP’s collection of citizens’ personal data via ODITs to call that an extremely intrusive practice.
The authorities’ persistent policy of obscuring the details of the spyware-utilizing surveillance tools is “a crisis of accountability” – that’s how the Canadian Civil Liberties Association non-profit described the situation.
Transparency around such issues in Canada these days apparently goes as far – and no further – than the government stating that it is “not using NSO’s Pegasus.”
The media stopped describing the search of Donald Trump’s Mar-a-Lago estate as a “raid” after a top former FBI agent complained about the wording during an appearance on MSNBC.
Federal agents ransacked Trump’s Florida home, even going through his wife Melania’s wardrobes, in a bid to find classified records Trump allegedly took from the White House.
Trump supporters assert that the boxes recovered during the raid contain files that were already declassified by the time Trump left office.
The raid was carried out after an FBI informant had infiltrated Mar-a-Lago and discovered the precise location of where the files were being kept.
Despite widespread anger at the raid from both Trump supporters and Republicans in general, one former FBI agent tried to language police by insisting that the raid, timed for when the feds knew Trump wouldn’t be home, was not in fact a raid.
“Agents, by the way, don’t like the word raid, they don’t like it,” former FBI Assistant Director Frank Figliuzzi told MSNBC.
“It sounds like it’s some kind of, you know, extra judicial non legal thing. It’s the execution of a search warrant. It’s a court authorized search warrant,” he added.
Figliuzzi insisted that the FBI would want the incident described as them having “executed a search warrant” and that calling it a “raid” helped Trump define what happened as “prosecutorial misconduct.”
Almost instantly, the media followed orders.
“MSNBC changed their chyron, from “FBI Raids Trump’s Mar-A-Lago Home,” to “FBI Executes Search Warrant At Trump’s Mar-A-Lago,” moments after Figliuzzi’s appearance, notes Jack Hadfield.
The New York Times also changed the word “raid” to “search”.
Twitter’s trending tab description of the incident was also changed to omit the word “raid”.
Meanwhile, Trump himself said on Truth Social last night that the FBI had already visited Mar-a-Lago in June to view the records after they asked Trump to secure them with an extra lock.
“Then on Monday, without notification or warning, an army of agents broke into Mar-a-Lago, went to the same storage area, and ripped open the lock that they had asked to be installed,” wrote Trump.
I joined the Tavistock Clinic in North London as a clinical nurse therapist in 2003. Back then, Tavistock was prestigious—known all over the world for its professional seminars and specialized psychological treatments for mental-health patients. Before I ever worked there, I would attend lectures and training workshops to hear from renowned psychoanalysts, who were considered some of the best in the field.
A lot can change in a decade.
Last week, the National Health Service ordered that the gender youth clinic at Tavistock to shut its doors by next spring. And I am part of the reason why.
The story of what happened at Tavistock is the story of how a small group of whistleblowers—doctors, nurses, parents and patients, together with the help of journalists and reporters—were able to relentlessly expose activist-driven medicine that they knew was irresponsible. It’s also an object lesson for others who are deeply concerned about a one-size-fit-all approach to transgender healthcare and wonder what they should do about it.
I was delighted when I started working at Tavistock back in the early 2000s. My role as senior clinical lecturer was to devise and deliver training courses for mental-health staff. Shortly after I joined, I took on another part-time role working with children and adolescents in what was called the Gender Identity Development Service.
There were, as I recall, seven of us on the team back then. We would have clinical meetings each week in which we would discuss our referrals and caseloads. Back then we had fewer than 100 referrals per year in the entire country and they were mostly biological boys.
Sometime during my first few weeks we were discussing a newly referred patient, a 16-year-old boy with a complex history, who felt he had been born in the wrong body. My colleague took on the case. Four months later, the boy’s name came up again in the meeting, and my colleague announced that she was recommending him for puberty blockers (gonadotropin-releasing hormone agonists), which are used to suppress the further development of secondary-sex characteristics like breast tissue in females or facial hair in males. Puberty blockers are almost always followed by cross-sex hormones (testosterone or estrogen).
Usually, when new patients arrived at the service, they would come in for an hour or so once a month for the first few months. So I was surprised to hear that my coworker was recommending drugs when, in my view, no meaningful understanding of his internal world could have been reached. I knew from my experience in working with adolescents that any diagnostic assessment arrived at after such a short time span would have been superficial.
It’s worth pointing out that Tavistock specialized in therapy—talking through problems with patients—and that we did not generally prescribe drugs. For that reason, I had expected the same approach when it came to treating children and teens with gender dysphoria. But it seemed that, even back then, certain staff didn’t hesitate to recommend puberty blockers—even for vulnerable kids contending with anxiety, autism, internalized homophobia or other challenges.
I had also noticed that senior clinicians in the service would regularly meet with Mermaids, a transgender patient-advocacy group. At the time, various patient-advocacy groups were springing up alongside mental-health services so that patients would have a voice in the examination room. At first, I viewed all of this as an overdue development. But as time progressed, it seemed clear that groups like Mermaids were exerting influence over doctors and clinicians in the service—sometimes dictating the expectations of care for our patients.
One small anecdote: I was once instructed by a superior to rewrite a letter I’d written to a male patient’s referring doctor—making sure to use the patient’s chosen, female name and new pronouns. I understood the sensitivities around this subject, but I pointed out that using a female name and female pronouns might be confusing to the clinical team, since we had been talking about a male child with gender dysphoria..
I was informed that failure to use the right name and pronouns might result in problems or even litigation for me and the gender clinic at Tavistock.
The external influence of the advocacy groups increased. Instead of being a clinical, research-focused service where we were learning and developing ideas, it felt like it was a fait accompli that we had to go along with what Mermaids and patients wanted—even if we, the mental-health-care professionals, had legitimate questions about the appropriateness of the treatments that patients and patient advocates were demanding.
For example, a weird paradox arose at a conference on transgender health care hosted by Tavistock around 2005: the opening speaker declared that we were no longer supposed to think of gender dysphoria as a mental illness. But we were a mental-health team working at a mental-health facility. What were we supposed to be doing if not treating patients with psychological conditions?
Remember, this was all before the internet took hold of an entire generation of teenagers. There were no online groups dedicated to gender affirmation and coaching kids on what to say to their providers to secure cross-sex hormones. We mostly saw younger boys who believed themselves to be girls from an early age and a few teenagers who felt like they were trapped in the wrong bodies. So, although I felt aware of the gathering force of thinking around the area of gender dysphoria and transgender identity, it was hard to foresee the slow-motion avalanche that would hit over the next two decades.
Yet even what I saw in those years worried me deeply and working on the Gender Identity Development Service started to affect my personal well-being. I would come home with a headache on the days that I worked in the unit, and my heart would beat quickly when I went in the next morning. It felt like every time I raised a concern about us rushing prematurely to prescribe drugs that would have permanent effects on our patients, I’d be met with an eye roll and the unstated “Oh, here she goes again,” or “Can’t she just fit in?”
There were a few colleagues who shared my views. One colleague, Dr. Az Hakeem, would also speak up at team meetings. But for the most part I felt alone, and I felt very anxious about some of the children who had been referred for body-altering medications. I began to feel as though I might be part of something unethical. I tried to take on only children who were legally too young to commence the blockers, which would allow me more time to do long-term therapeutic work while avoiding the dilemma of the fact I worked in a so-called “gateway service” to medicalization.
I spoke a lot to my husband, Marcus, who is a psychoanalyst and who was by now a senior member of staff in the Adult Department of Tavistock. He suggested I go to the clinical director at theTavistock, which I did. She listened and took my concerns seriously. I later learned that she reached out to Dr. David Taylor, the Medical Director of the Trust, who was asked to launch an investigation into the work of the gender clinic. That was issued in 2006.
I do not remember being shown the report then, and don’t recall any in depth discussion about the contents of it or how the recommendations would be implemented. The only change that I remember was that a senior staff member from the more general Adolescent Department began overseeing our work. That oversight petered out when this staff member retired.
It was only in 2019 that I saw the full report when Hannah Barnes, a BBC journalist, obtained it via a Freedom of Information request. It confirmed all the disturbing things I had reported: Our data was poor; it wasn’t being stored properly; and there were not sufficient follow-ups with patients once they left the service—meaning we didn’t know how our patients were faring unless they voluntarily wrote to us.
As we have now learned from more recent whistleblowers, the recommendations in the report were buried, and when any criticism or difficult questions arose in the press, the Tavistock management would repeat the same mantra about how they were “a world-class service.” It’s important to acknowledge that there might have been some staff still struggling to deliver thoughtful, measured care, but the noise around our standards was growing louder.
I had tried hard to help the Gender Identity Development Service from the inside, but it felt like I was swimming against a stronger and stronger tide. I didn’t want to be part of something that felt wrong, and I knew that each time I spoke up I was being cast in a darker shadow of suspicion by my colleagues.
So in 2007, I quit.
After I left the gender clinic, I continued to work in other departments at Tavistock. I continued my clinical lecturing and practiced psychoanalytic psychotherapy. Life was satisfying and busy, and I tried to put the experience out of my mind.
But it became increasingly impossible to ignore.
In the past decade, there has been an explosion in referral numbers to the gender clinic at the Tavistock—over 3,000 in 2019—and the service came under mounting pressure to get through the long waiting lists. This resulted in even more children getting fast-tracked and put on blockers if they expressed a wish for them.
The profile of the patients changed significantly, too. Many were adolescent girls who had never exhibited signs of gender dysphoria. Often, their feelings of wanting to be a boy developed along with their breasts, or when they got their period. They were horrified by their bodies, and they wanted control over the changes taking place in them.
Between then and now, there were more whistleblowers, like Dr. David Bell, a psychiatrist and psychoanalyst at Tavistock, who issued yet another report on the service in 2018 that raised a lot of the same concerns that I had raised back in 2005. Sonia Appleby, whose job title was Safeguarding Children Lead, spoke out in November 2019, claiming that she was being blocked from doing her job by management. By then, the political pressure, the institutional capture, and the influence of social media had become much more intense, and about 40 people were working on the youth gender care team. Shortly after Dave’s report came out, my husband Marcus resigned from the Tavistock Board.
His resignation gained national publicity, and Marcus was invited to present at a 2019 House of Lords meeting, which I attended with him. A representative of the Tavistock Trust who was also at the meeting read a statement claiming that no one was being rushed through treatment, that Tavistock was a best-in-class facility. This was my second Damascene moment. I raised my hand to speak. “Look, that is not correct,” I said. “I worked there. And I saw that children were being pushed to transition very quickly.”
After that meeting, a group of us met, and we learned that a mother of a girl with autism and gender dysphoria was seeking support as a claimant in a judicial review of Tavistock’s practice of giving puberty blockers to minors. (Adults who transition are also prescribed blockers prior to starting on cross-sex hormones.) She had contacted a lawyer and he arranged a meeting with several of us who had attended the House of Lords meeting. The mother was worried about her daughter’s referral to the Gender Identity Development Service, as she did not feel that her daughter would be able to fully understand the ramifications of the treatment and give informed consent to it. She needed to remain anonymous and, therefore, needed a co-claimant who could afford to go public. Dave was still at Tavistock and was being threatened by the administration there. My husband had his hands full with his own patients. I did not relish the idea of sticking my neck out, but I knew I had to get back into the ring. By now, the whistleblowers’ reports felt grave. I signed onto the suit.
Almost no one in the U.K. wanted to get involved, so I set about finding expert witnesses in the United States, Australia and Scandinavia. Gradually, we put together statements and evidence to support our claim that children could not give fully informed consent to an experimental treatment with lifelong, as yet unknown consequences. I found, among many others, Kiera Bell through a journalist, and I was immediately taken by her story.
Keira is a young woman who went on puberty blockers at 16, testosterone at 17, and then had a double mastectomy—only to realize, at 21, that she wasn’t, in fact, a man trapped in a woman’s body. She argued that, as a minor, she hadn’t been able to consent in any meaningful way to the treatment. Eventually, she became a co-claimant in the case against Tavistock.
In December 2020, we won. The court ruled that minors under 16 could not give informed consent to having their puberty blocked. The ruling came as a great relief. I thought, Finally, people will have to pay attention and examine the evidence base for treatment of childhood gender dysphoria.
It’s hard to deal with the feeling of being hated. I’m aware how contentious this area is, and while I was only ever trying to do my best for our young patients, there was a loud group of people who would only hear my concerns as transphobia or bigotry or that I was a proponent of conversion therapy. The win felt like such a victory—not just legally, but culturally. It felt like an honest conversation was finally beginning to happen.
But then, in September 2021, we lost on appeal. It was awful—deflating.
The only thing that softened the blow was the fact that the government commissioned yet another report into Tavistock. And the results were devastating. It vindicated everything we had been saying for years.
But this time, the NHS decided they were going to do something about it. On July 28, the NHS announced that Tavistock Gender Identity Development Service would be closed and that, from now on, regional clinics would handle cases of transgender kids. I was blown away. I still can hardly believe it. The aim is that the new services should be more holistic, taking into consideration the whole child, and adopt better clinical standards according to the new report’s findings.
I didn’t seek any of this. It has been a pretty stressful few years. When I get a letter from patients or parents from around the world, and they tell me, “Well done, thank you for speaking up, you didn’t give up,” I sometimes get a lump in my throat. It’s been hard to be suspected of being prejudiced when all I wanted was safer clinical practice, more scrutiny and evidence collecting, and improved data storage.
Because what I am is a nurse. And my job as a nurse is to treat all my patients with respect and an open mind. I try to think about who they are as people, and to relate to their experience and empathize with them. I also believe we need to keep an open and curious clinical mind when something is occurring in society that seems novel or not yet fully understood. It should never be that doctors and nurses are unable to question diagnoses and prescriptions.
If my actions all those years ago have made a contribution, then I am proud. I made the right decision to raise my hand to ask another unwanted question.
Sue and Marcus Evans run a private psychotherapy practice in London. They are the authors of “Gender Dysphoria: A Therapeutic Model for Working with Children, Adolescents and Young Adults,” which you can buy here.
Richard Smith, editor of the British Medical Journal (BMJ) until 2004 posted an interesting opinion piece in the BMJ last year.
I have posted it below for you to read.
Time to assume that health research is fraudulent until proven otherwise?
Health research is based on trust. Health professionals and journal editors reading the results of a clinical trial assume that the trial happened and that the results were honestly reported. But about 20% of the time, said Ben Mol, professor of obstetrics and gynaecology at Monash Health, they would be wrong. As I’ve been concerned about research fraud for 40 years, I wasn’t that surprised as many would be by this figure, but it led me to think that the time may have come to stop assuming that research actually happened and is honestly reported, and assume that the research is fraudulent until there is some evidence to support it having happened and been honestly reported. The Cochrane Collaboration, which purveys “trusted information,” has now taken a step in that direction.
As he described in a webinar last week, Ian Roberts, professor of epidemiology at the London School of Hygiene & Tropical Medicine, began to have doubts about the honest reporting of trials after a colleague asked if he knew that his systematic review showing the mannitol halved death from head injury was based on trials that had never happened. He didn’t, but he set about investigating the trials and confirmed that they hadn’t ever happened. They all had a lead author who purported to come from an institution that didn’t exist and who killed himself a few years later. The trials were all published in prestigious neurosurgery journals and had multiple co-authors. None of the co-authors had contributed patients to the trials, and some didn’t know that they were co-authors until after the trials were published. When Roberts contacted one of the journals the editor responded that “I wouldn’t trust the data.” Why, Roberts wondered, did he publish the trial? None of the trials have been retracted.
Later Roberts, who headed one of the Cochrane groups, did a systematic review of colloids versus crystalloids only to discover again that many of the trials that were included in the review could not be trusted. He is now sceptical about all systematic reviews, particularly those that are mostly reviews of multiple small trials. He compared the original idea of systematic reviews as searching for diamonds, knowledge that was available if brought together in systematic reviews; now he thinks of systematic reviewing as searching through rubbish. He proposed that small, single centre trials should be discarded, not combined in systematic reviews.
Mol, like Roberts, has conducted systematic reviews only to realise that most of the trials included either were zombie trials that were fatally flawed or were untrustworthy. What, he asked, is the scale of the problem? Although retractions are increasing, only about 0.04% of biomedical studies have been retracted, suggesting the problem is small. But the anaesthetist John Carlisle analysed 526 trials submitted to Anaesthesia and found that 73 (14%) had false data, and 43 (8%) he categorised as zombie. When he was able to examine individual patient data in 153 studies, 67 (44%) had untrustworthy data and 40 (26%) were zombie trials. Many of the trials came from the same countries (Egypt, China, India, Iran, Japan, South Korea, and Turkey), and when John Ioannidis, a professor at Stanford University, examined individual patient data from trials submitted from those countries to Anaesthesia during a year he found that many were false: 100% (7/7) in Egypt; 75% (3/ 4) in Iran; 54% (7/13) in India; 46% (22/48) in China; 40% (2/5) in Turkey; 25% (5/20) in South Korea; and 18% (2/11) in Japan. Most of the trials were zombies. Ioannidis concluded that there are hundreds of thousands of zombie trials published from those countries alone.
Others have found similar results, and Mol’s best guess is that about 20% of trials are false. Very few of these papers are retracted.
We have long known that peer review is ineffective at detecting fraud, especially if the reviewers start, as most have until now, by assuming that the research is honestly reported. I remember being part of a panel in the 1990s investigating one of Britain’s most outrageous cases of fraud, when the statistical reviewer of the study told us that he had found multiple problems with the study and only hoped that it was better done than it was reported. We asked if he had ever considered that the study might be fraudulent, and he told us that he hadn’t.
We have now reached a point where those doing systematic reviews must start by assuming that a study is fraudulent until they can have some evidence to the contrary. Some supporting evidence comes from the trial having been registered and having ethics committee approval. Andrew Grey, an associate professor of medicine at the University of Auckland, and others have developed a checklist with around 40 items that can be used as a screening tool for fraud (you can view the checklist here). The REAPPRAISED checklist (Research governance, Ethics, Authorship, Plagiarism, Research conduct, Analyses and methods, Image manipulation, Statistics, Errors, Data manipulation and reporting) covers issues like “ethical oversight and funding, research productivity and investigator workload, validity of randomisation, plausibility of results and duplicate data reporting.” The checklist has been used to detect studies that have subsequently been retracted but hasn’t been through the full evaluation that you would expect for a clinical screening tool. (But I must congratulate the authors on a clever acronym: some say that dreaming up the acronym for a study is the most difficult part of the whole process.)
Roberts and others wrote about the problem of the many untrustworthy and zombie trials in The BMJ six years ago with the provocative title: “The knowledge system underpinning healthcare is not fit for purpose and must change.” They wanted the Cochrane Collaboration and anybody conducting systematic reviews to take very seriously the problem of fraud. It was perhaps coincidence, but a few weeks before the webinar the Cochrane Collaboration produced guidelines on reviewing studies where there has been a retraction, an expression of concern, or the reviewers are worried about the trustworthiness of the data.
Retractions are the easiest to deal with, but they are, as Mol said, only a tiny fraction of untrustworthy or zombie studies. An editorial in the Cochrane Library accompanying the new guidelines recognises that there is no agreement on what constitutes an untrustworthy study, screening tools are not reliable, and “Misclassification could also lead to reputational damage to authors, legal consequences, and ethical issues associated with participants having taken part in research, only for it to be discounted.” The Collaboration is being cautious but does stand to lose credibility—and income—if the world ceases to trust Cochrane Reviews because they are thought to be based on untrustworthy trials.
Research fraud is often viewed as a problem of “bad apples,” but Barbara K Redman, who spoke at the webinar insists that it is not a problem of bad apples but bad barrels if not, she said, of rotten forests or orchards. In her book Research Misconduct Policy in Biomedicine: Beyond the Bad-Apple Approach she argues that research misconduct is a systems problem—the system provides incentives to publish fraudulent research and does not have adequate regulatory processes. Researchers progress by publishing research, and because the publication system is built on trust and peer review is not designed to detect fraud it is easy to publish fraudulent research. The business model of journals and publishers depends on publishing, preferably lots of studies as cheaply as possible. They have little incentive to check for fraud and a positive disincentive to experience reputational damage—and possibly legal risk—from retracting studies. Funders, universities, and other research institutions similarly have incentives to fund and publish studies and disincentives to make a fuss about fraudulent research they may have funded or had undertaken in their institution—perhaps by one of their star researchers. Regulators often lack the legal standing and the resources to respond to what is clearly extensive fraud, recognising that proving a study to be fraudulent (as opposed to suspecting it of being fraudulent) is a skilled, complex, and time consuming process. Another problem is that research is increasingly international with participants from many institutions in many countries: who then takes on the unenviable task of investigating fraud? Science really needs global governance.
Everybody gains from the publication game, concluded Roberts, apart from the patients who suffer from being given treatments based on fraudulent data.
Stephen Lock, my predecessor as editor of The BMJ, became worried about research fraud in the 1980s, but people thought his concerns eccentric. Research authorities insisted that fraud was rare, didn’t matter because science was self-correcting, and that no patients had suffered because of scientific fraud. All those reasons for not taking research fraud seriously have proved to be false, and, 40 years on from Lock’s concerns, we are realising that the problem is huge, the system encourages fraud, and we have no adequate way to respond. It may be time to move from assuming that research has been honestly conducted and reported to assuming it to be untrustworthy until there is some evidence to the contrary.
In this in-depth interview series with Kirsten Murfitt of NZLSOS, we highlight the key points and outline the crucial yet-to-be-answered questions from Kirsten’s excellent Open Letter to Parliament, which she penned on 22 July 2022. This is Part 1.
Please share this interview. Please also utilise the steps involved at the end of the interview in order to put pressure on the government to answer our important questions:
The 3 main questions are:
1.) Why doesn’t the Government require mandatory reporting of deaths and serious adverse reactions, following the administration of a vaccine which has only provisional approval?
2.) Why does the Government refuse to investigate the safety and contents of the vaccine, given both the emerging overseas data and the court-ordered release of Pfizer’s documents?
3.) Why did the Government market the vaccine as “Safe and Effective”, when it knew that neither of those statements was true?
Establishment historians state that Adolf Hitler made a mistake when he declared war on the United States. For example, British historian Andrew Roberts wrote:[1]
“It seems an unimaginably stupid thing to have done in retrospect, a suicidally hubristic act less than six months after attacking the Soviet Union. America was an uninvadable land mass of gigantic productive capacity and her intervention in 1917-18 had sealed Germany’s fate in the Great War.”
Historian Martin Gilbert wrote in regard to Germany’s declaration of war on the United States:[2]
“It was perhaps the greatest error, and certainly the single most decisive act, of the Second World War.”
In this article I will explain why Hitler was forced to declare war on the United States. … continue
This site is provided as a research and reference tool. Although we make every reasonable effort to ensure that the information and data provided at this site are useful, accurate, and current, we cannot guarantee that the information and data provided here will be error-free. By using this site, you assume all responsibility for and risk arising from your use of and reliance upon the contents of this site.
This site and the information available through it do not, and are not intended to constitute legal advice. Should you require legal advice, you should consult your own attorney.
Nothing within this site or linked to by this site constitutes investment advice or medical advice.
Materials accessible from or added to this site by third parties, such as comments posted, are strictly the responsibility of the third party who added such materials or made them accessible and we neither endorse nor undertake to control, monitor, edit or assume responsibility for any such third-party material.
The posting of stories, commentaries, reports, documents and links (embedded or otherwise) on this site does not in any way, shape or form, implied or otherwise, necessarily express or suggest endorsement or support of any of such posted material or parts therein.
The word “alleged” is deemed to occur before the word “fraud.” Since the rule of law still applies. To peasants, at least.
Fair Use
This site contains copyrighted material the use of which has not always been specifically authorized by the copyright owner. We are making such material available in our efforts to advance understanding of environmental, political, human rights, economic, democracy, scientific, and social justice issues, etc. We believe this constitutes a ‘fair use’ of any such copyrighted material as provided for in section 107 of the US Copyright Law. In accordance with Title 17 U.S.C. Section 107, the material on this site is distributed without profit to those who have expressed a prior interest in receiving the included information for research and educational purposes. For more info go to: http://www.law.cornell.edu/uscode/17/107.shtml. If you wish to use copyrighted material from this site for purposes of your own that go beyond ‘fair use’, you must obtain permission from the copyright owner.
DMCA Contact
This is information for anyone that wishes to challenge our “fair use” of copyrighted material.
If you are a legal copyright holder or a designated agent for such and you believe that content residing on or accessible through our website infringes a copyright and falls outside the boundaries of “Fair Use”, please send a notice of infringement by contacting atheonews@gmail.com.
We will respond and take necessary action immediately.
If notice is given of an alleged copyright violation we will act expeditiously to remove or disable access to the material(s) in question.
All 3rd party material posted on this website is copyright the respective owners / authors. Aletho News makes no claim of copyright on such material.