Seyed Mohammad Marandi is in Islamabad, where the negotiations between Iran and the US collapsed. Marandi explains why the negotiations failed and that there will likely be a return to war. In the US media, there are already threats to kill the Iranian leadership and delegation. Marandi is a professor at Tehran University and a former advisor to Iran’s Nuclear Negotiation Team. (
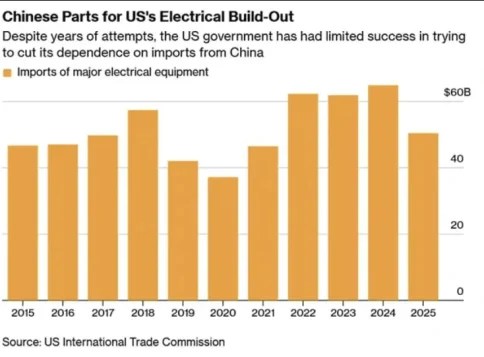
Apparently tomorrow morning, April 13, at 10 a.m. ET the blockade of Iran’s ports by the US will begin. Make no mistake, this is primarily pointed at Iran’s trade with China. The Trump team seem to still think they can kill two birds with one stone – bring down the Islamic Republic and also economically weaken China. In this article I will focus on China, in particular, one aspect of the US/China relationship that gets little attention but which can be a “nuclear bomb” for China. Much discussion in the US about the boom in data center construction, but far less discussion of the total reliance on Chiina for these builds.
It has been estimated by multiple sources that literally all of the US growth in the past year has been due to the AI boom, specifically, due to AI data center builds. Without this ,US growth would be flat, potentially even negative. Even without the Iran war and rising energy costs, data center construction in the U.S. is currently facing significant headwinds, resulting in delays and escalating costs. The primary driver is the strained supply chain, impacting the availability of critical components like switchgear, generators, and specialized cooling equipment. Lead times for these items have stretched considerably, pushing project timelines back by months, if not quarters.
There are other factors for the slow down, especially chip and labor shortages, regulatory hurdles, and the increasing costs of infrastructure. This isn’t the place to delve into all of the factors, but the point is this vital sector for the US economy is in an extremely fragile state. One small push and it can come tumbling down.
And it turns out that whether this sector continues to keep the US out of recession or not is entirely in China’s hands. Forget chips as the vital factor, especially as other US allies control most of the chip production. Just as real a bottleneck is in Chinese electrical components. There is currently a backlog of several years for many of these. Sure, potentially in the long run, there can be many sources for these components. But not tomorrow. Or the day after.
With just the flick of a switch, China stop exporting these components and the AI boom dies almost instantly. And with it, any hopes for real growth in the US economy over the coming months or years.
I obviously don’t know how China will react, or what measures it will enact, if the US navy does go through with its blockade tomorrow. What I outline here is just one of many potential levers the Chinese can pull (rare earths, pharma base ingredients, T-Bills, …)
But don’t expect the US blockade to impact China too severely any time soon.
Proving itself incapable of winning on any front, despite such vast power imbalances, the Zionist regime has developed various collective punishment doctrines over the years. This time, after getting battered by Iranian missiles and failing to achieve any strategic goal, it takes out its frustration on Lebanon and Gaza.
When the US-Israeli alliance launched its war of aggression against the Islamic Republic of Iran on February 28, the Zionist regime’s Premier Benjamin Netanyahu openly gloated about getting what he had wanted for over 40 years. However, the moment he had been pushing for decades to reach failed to render the results the Israeli leader had hoped for.
US President Donald Trump, having initially agreed to Iran’s 10-point plan, before later backtracking, decided to announce a two-week cessation of hostilities with Iran. Within hours, having freed up its Air Force that had been bogged down in Iran attack operations, the Israelis were already targeting civilians across Lebanon, including bombing an ambulance in Tyre, south Lebanon.
Hours after that came the horrifying Beirut massacre, during which the Israelis carried out over 100 airstrikes in 10 minutes, demolishing dozens of civilian buildings without any notice. The result was the mass slaughter of more than 300 people, with an additional 1,200 left injured across the country in less than a day.
This was evidently no accident; the Israeli leadership had been claiming throughout the 15-month Lebanon ceasefire – which they violated over 15,400 times according to UNIFIL – that Hezbollah had been defeated, that it posed no threat to the northern settlements and would easily be dealt with. In early March, the Israeli victory narrative collapsed completely.
There is a reason why 77% of Israelis polled, according to Hebrew media outlet Maariv, say they want a continuation of the war against Lebanon. That reason is that they understand well that Hezbollah is still a massive threat to them, and the occupation army they support has failed at deterring the Lebanese Party.
Over two years of genocide in the Gaza Strip, Hamas is still there, and none of the dozen Palestinian Resistance groups have been defeated, despite them taking blows. In Lebanon, the Zionist regime killed most of Hezbollah’s senior leadership, yet failed to deal any decisive blow to the organization. The largest blow that was dealt to Hezbollah was the way the 2024 assault on Lebanon reshaped the Lebanese government.
In Iran, twice, the Israeli-US alliance has assassinated a large number of the Islamic Republic of Iran’s leadership figures, but has failed to deliver any defeat to it. All of the statistics about the percentages of missiles and launchers that the Israelis claim to have destroyed are simply plucked out of thin air.
While the leadership in Tel Aviv may allege that they have come out of every confrontation with some kind of total victory, they also admit that the “war is not over”. This is an admission of failure, because if each war were a victory for them, they wouldn’t require another. The only thing that saves them each time is that they are granted ceasefires, which the Zionists use as a period in which they create new plots to attack once again. If the wars were all-out and total, they would eventually be drained and forced to submit.
So, as each lull in the fighting occurs – what some call “ceasefires” – the Israelis end the round with more treachery. This time around, as soon as the US announced that a two-week temporary ceasefire had been reached, Tel Aviv used the opportunity to concentrate its entire air force on striking civilian targets as a calibrated tactic.
The Gaza genocide was not done simply out of a desire to shed blood as a revenge blow, although this clearly played into it; the genocide was a message to the Palestinian people and the rest of the region. It was a desperate attempt to salvage the so-called “deterrence capacity” image that the Zionist regime had spent so long building up.
The Israelis did not want to directly go after the Palestinian resistance in Gaza because they knew that it would be costly, so they hid in their tanks and armored vehicles, entering areas with the intent of flattening infrastructure and knocking out major hospitals as the end goal of each operation.
In Lebanon, their tactics are very similar, but are complicated by the fact that Hezbollah is a far stronger military force to deal with. We immediately saw that Tel Aviv displaced a million Lebanese, bombed all the bridges allowing for civilian passage to the south of Lebanon, and then flattened entire towns and neighborhoods.
The mass slaughter of civilians in Beirut was also part of that strategy. The civilian populations of Gaza and Lebanon become a punching bag, with the end goal being the demoralization of the people, attempting to turn them against the resistance groups they overwhelmingly support.
The Strait of Hormuz is “under reasonable control and management” and open to passage by civilian vessels “in compliance with specific regulations,” the IRGC’s public relations department has announced.
This provision does not apply to military vessels, whose approach of the Strait “under any pretext will be considered a ceasefire violation and will be dealt with severely,” the IRGC warned.
The announcement comes on the heels of President Trump’s declaration on Sunday of a naval blockade of “any and all ships trying to enter, or leave, the Strait of Hormuz,” and threats to “blow” any Iranian forces that fire at US warships “to hell!”
Former United States State Department advisor and veteran West Asia negotiator Aaron David Miller sharply criticized Washington’s assumptions about the pace and substance of talks with Iran, arguing that the US misjudged Iran’s position.
“If Administration believed after only 21 hours of negotiations, Iran would give up enrichment which is what Vance implied, they totally misread the moment and the Iranian dominated IRGC,” Miller posted on X.
Gerard Araud, a high-ranking retired French diplomat who served as the Ambassador to the United States and the Permanent Representative to the United Nations, also pointed to the prowess of Iranian negotiators.
“The agreement we reached with Iran in 2015 was the result of hundreds of hours of negotiations with the support of experts of nuclear energy,” Araud explained.
“Negotiating with the Iranians is the equivalent of a diplomatic trenches war. Line by line, word by word.” he posted on X.
“From an Iranian point of view, the negotiations are not starting from scratch but after an agreement endorsed by the UNSC,” he added in another post.
“Any new negotiations have to take into account this precedent: words have already a significance and proposals a history,” he said.
Deadlock in Islamabad talks after 21 hours of negotiations
Negotiations between Iran and the US have ended without agreement following Pakistan-mediated diplomatic efforts in Islamabad, with core nuclear demands keeping both sides far apart after 21 hours of discussions.
The talks, aimed at narrowing differences over Iran’s nuclear program and related regional security arrangements, failed to produce convergence on key issues, including Iran’s right to uranium enrichment, the security regime of the Strait of Hormuz, and proposals linking any broader understanding to a ceasefire extending to Lebanon.
Expectations of a rapid breakthrough had been encouraged by US Vice President JD Vance, but were widely regarded as unrealistic given the depth of disagreement between Washington and Tehran. The 2015 nuclear agreement itself took nearly two years to finalize, while current conditions are further complicated by escalating regional confrontation.
Vance defends US position after talks collapse
Following the breakdown of negotiations, US Vice President JD Vance stated that Iran had rejected Washington’s terms, while leaving the door open for future engagement.
“They have chosen not to accept our terms,” Vance said in a brief news conference in Islamabad, though he left open the possibility that terms could still be reached.
“We leave here with a very simple proposal: a method of understanding that is our final and best offer,” he added.
“We’ll see if the Iranians accept it,” he asserted.
Australia calls for renewed negotiations and ceasefire
International reactions followed the collapse of the talks, with Australia urging both sides to return to diplomacy and maintain a ceasefire across the region.
Australian Foreign Minister Penny Wong described the outcome of the Islamabad talks as “disappointing” and called for an immediate resumption of negotiations.
“The priority now must be to continue the ceasefire and return to negotiations,” Wong said, adding it was “disappointing that the Islamabad talks between the United States and Iran have ended without agreement.”
Wong also warned that any further escalation “would impose an even greater human cost and further impact the global economy,” stressing the need for sustained diplomatic engagement.
As I expected, the negotiation between the US and Iran failed to reach an agreement. Although JD Vance headed the US team, he was never in control… I have heard from someone who was directly involved with this circus in Islamabad that Israeli agents — Steve Witkoff and Jared Kushner — made certain that JD Vance would not follow his instincts and accept the deal that Iran had laid on the table. Israel’s role in sabotaging the US delegation was evident in Vance’s statement announcing the failure of the negotiations, when he falsely accused Iran of refusing to give up its alleged quest for a nuclear weapon. This is just a rehashed piece of Zionist propaganda.
There were several Iranian conditions that the US refused to accept: Iranian control of the Strait of Hormuz, an end to Israel’s attack on Lebanon and Hezbollah, unfreezing of Iran’s assets and retaining sovereignty over its supply of enriched uranium. I have said repeatedly this past week during various interviews on the subject that Iran’s position on these issues was non-negotiable.
Here is the statement just released by the Iranian government:
The American enemy, which is vile, wicked and dishonest — attempted to achieve on the negotiating table what it could not achieve through war.
Among these demands are handing over enriched uranium and opening the Strait of Hormuz without confirmed Iranian sovereignty over it.
Iran has decided to reject these terms and continue the sacred defense of its fatherland by any means necessary, military or diplomatic.’
So what is next? For starters I hope that the Iranian delegation in Islamabad gets a return flight home on a Russian or Chinese flagged airplane. I do not discount the possibility of Israel and the US trying to destroy the Iranian airliner on its return flight to Tehran.
Iran will not initiate new military actions against Israel or the US… They will wait to absorb the first blow and then launch a massive retaliation. I think they now understand that the US is too much under the control of the Zionist lobby to act in the interest of the people of the United States.
Iran’s demand that the US vacate its bases in the Gulf will be achieved by force… Iran will hit the remaining bases and make them uninhabitable for the US military going forward. The Saudis and the UAE will have to make a choice this week… Seek reconciliation with Iran and survive or side with the US and Israel and face economic destruction.
The real action that will put the most pressure on Trump will start on Monday morning when the US stock market takes a nose dive… again… and the price of oil heads back up into triple digit territory. JD Vance actually did Iran a favor by breaking off first and walking away. This paints Iran in a very favorable light in the eyes of the global south, i.e., Iran was willing to negotiate, but the US refused to engage in good faith negotiations and bailed.
Here is my chat with Ed DeMarche of the Trends Journal from last Wednesday:Video Link
MOSCOW – US President Donald Trump said on Sunday that the United States would soon start the naval blockade of the Strait of Hormuz to prevent Iran from using what he described as “extortion.”
“The Blockade will begin shortly. Other Countries will be involved with this Blockade,” Trump wrote on Truth Social.
The US Navy will be blockading “any and all Ships trying to enter, or leave, the Strait of Hormuz,” until all are allowed to go in and out, he wrote.
“I have also instructed our Navy to seek and interdict every vessel in International Waters that has paid a toll to Iran. No one who pays an illegal toll will have safe passage on the high seas,” Trump also said.
The US leader added that he would not allow any country, especially his own, to be “extorted” by Iran.
Safe passage of vessels through the Strait of Hormuz will be possible if the United States complies with its obligations, Iranian Foreign Minister Abbas Araghchi said on Thursday.
Earlier, Araghchi announced the reopening of the Strait of Hormuz, which accounts for about 20% of the world’s oil, petroleum products, and LNG supplies.
The escalation of the conflict has virtually halted shipping through the Strait of Hormuz, a key supply route for global oil and LNG. As a result, fuel prices are rising in most countries.
There is growing expectation in Tehran that the Islamabad talks with the US may open the door leading into the rose-garden. But footfalls still echo in the memory, as the US has been an utterly unreliable and unscrupulous interlocutor.
The Islamabad talks on Saturday lasting 21 hours ended without a deal. The US Vice-President JD Vance, in a very short news conference at Islamabad, blamed Iran for not accepting American terms. As he put it, “We need to see an affirmative commitment that [Iran] will not seek a nuclear weapon, and they will not seek the tools that would enable them to quickly achieve a nuclear weapon. That is the core goal of the president of the United States, and that’s what we’ve tried to achieve through these negotiations.”
Iran’s Foreign Ministry spokesman Esmaeil Baqaei said that the two sides reached a consensus on some issues, but held different views regarding 2-3 important matters. Baqaei said the talks covered some new issues with their own complexities, such as the Strait of Hormuz, but stressed that diplomacy never ends, as it is a tool to preserve national interests, and “stands ready for all kinds of sacrifices.”
Baqaei later told Iran’s state television, “Naturally, from the beginning we should not have expected to reach an agreement in a single session. No one had such an expectation.” And Tehran is “confident that contacts between us and Pakistan, as well as our other friends in the region, will continue”.
On their part, Pakistani mediators called on the US and Iran to maintain the ceasefire. Foreign minister Ishaq Dar said Islamabad would try to facilitate a new dialogue between Iran and the US in the coming days.
Such tough situations have a history of grandstanding by protagonists but that hasn’t happened here, and gives hope that it is far too premature to write off that the peace track ended in a train crash. After all, the negotiations were initially expected to be indirect, but the two political leaderships are now engaging in direct discussions for the first time since the 1979 Islamic Revolution. Vance separately met Iranian parliamentary speaker Mohammad Baqer Qalibaf and foreign minister Abbas Araqchi for two hours.
Previously, the plan was for the two delegations to sit in separate rooms while Pakistani mediators relayed messages between them. “However, now, in a significant shift, our sources close to the mediators say that the two teams are holding direct talks with the presence of Pakistani intermediaries,” Al Jazeera reported.
Also, the negotiations have moved beyond general issues, and in some cases entered technical discussions. Iranian media reported that “specialists from both sides are now reviewing detailed aspects of unresolved matters, including the implementation of regional de-escalation measures and the assessment of the ceasefire in southern Lebanon.”
The talks are very important for Vance himself as he personally sought this role from Trump. Another reason for Trump’s selection was the deep mistrust between Tehran and Jared Kushner and Steve Witkoff following the US and Israeli attacks after two previous rounds of negotiations. Nevertheless, Witkoff and Kushner, both Jews with close ties to Israeli prime minister Benjamin Netanyahu, accompanied Vance.
At any rate, finalising an agreement may take weeks or months and will likely require extending the current two-week ceasefire. That requires patience and fortitude. Whereas, an inventory of the war highlights only Trump’s fickle-minded temperament and Netanyahu’s tenacity bordering on obsession. Netanyahu has admitted that the US-Israeli attacks on Iran were “something I’ve longed to do for 40 years.”
In the 13 months since Trump took office until the outbreak of the war, Netanyahu met with Trump on average every two months for face-to-face meetings (apart from multiple remote meetings), unmatched by any foreign leader.
According to the New York Times, Trump’s irreversible decision to go to war was reached on February 11, in the famous Situation Room at the White House, where Netanyahu and the head of Mossad delivered Trump a spectacular story of decapitation of Iranian leaders, with a happy ending.
The Times wryly noted that none of Trump’s close associates — Vance, secretary of state Rubio or the CIA director Ratcliffe saw Netanyahu’s presentation and his closing argument as anything more than a live steam for young children, and they were well aware that their boss might believe in fairy tales, yet, none of them was willing to resign in protest.
Vance disclosed in Islamabad yesterday that he spoke with Trump at least half a dozen times during the talks and noted, “The bad news is that we have not reached an agreement, and I think that’s bad news for Iran much more than it’s bad news for the United States of America.”
Herein lies the danger. Trump is notoriously prone to mood swings and has a propensity to believe in the last person he spoke with. It may seem child-like innocence but in this case, chaffing under public ridicule in the US as well as internationally for having ‘lost’ the war, Trump is under immense pressure to do something.
Meanwhile, the Zionist lobby that has easy access to Trump’s ears must be working overtime to block any US-Iran agreement. On the other hand, as the final hours ticked down, there was little indication that Iran was ready to agree to Trump’s ultimatum.
Li Haidong, professor at China Foreign Affairs University, told the Global Times last week that based on past patterns, when confronted with mounting pressure, the US has at times escalated tensions, while at other moments abruptly shifted course with tactical adjustments. This makes Washington’s next move highly unpredictable.
The Chinese professor noted that “the current dynamics suggest that Tehran is unlikely to make meaningful concessions, while Washington also faces significant constraints in altering its own position. Coupled with Israel’s role in shaping the conflict, this latest ultimatum [by Trump] thatIran could be ‘taken out’ if it did not meet his newly updated deadline is likely to unfold in a more dramatic and uncertain manner.”
But that does not mean the war can end only on Washington’s terms; war is more likely to become protracted. Iran no longer trusts the US and will only accept an end of the war with guarantees that it won’t be attacked again.
Above all, the resurgent IRGC remains confident that it would “deprive the US and its allies of the region’s oil and gas for years” if Trump carries out his threat to attack power plants and bridges. An Iranian official told the media that the process of preparing new infrastructure for managing vessel traffic in the Strait of Hormuz has been completed by Iran and more than 100 vessels of various nationalities have so far submitted written requests to transit the strait under the new protocol.
Max Blumenthal discusses why the consensus over the US-Israel partnership is unravelling as the intrusive influence of Israel is widely seen to undermine US interests. The disastrous Iran War has intensified the MAGA Civil War. Blumenthal is the editor-in-chief of The Grayzone, an award-winning journalist and the author of several books, including best-selling Republican Gomorrah, Goliath, The Fifty One Day War, and The Management of Savagery. He has produced print articles for an array of publications, many video reports, and several documentaries, including Killing Gaza.
Iran’s Tasnim News Agency reported on Sunday morning that US-Iran talks ended with no agreement due to “excessive US demands” that prevented the formation of a common framework.
The agency said Washington sought to secure concessions it had failed to achieve through military escalation, including demands related to Iran’s enriched materials and control over the Strait of Hormuz. According to Tasnim, the Iranian delegation attempted to advance toward a joint negotiating framework, but US demands ultimately stalled progress.
Tasnim reported that upon arriving in Islamabad, the Iranian delegation met with Pakistan’s army chief and prime minister to coordinate positions and raise concerns over what it described as US breaches of commitments.
It said talks with the Pakistani leadership preceded negotiations with the US side, which began at the level of main delegations before shifting to technical teams and lasted more than 21 hours.
The agency added that Tehran presented what it described as reasonable proposals, stressing that responsibility now rests with Washington to respond realistically. It also said the US administration has miscalculated both militarily and in its negotiating approach, noting that the status of the Strait of Hormuz will not change without a “reasonable agreement.”
No date or venue has been set for a potential new round of talks.
Meanwhile, Al Mayadeen’s bureau chief in Pakistan reported that the US delegation had departed Islamabad following the conclusion of the talks.
Additionally, a source close to the Iranian negotiating team told Fars News that the US delegation appeared to be looking for a pretext to exit the talks. The source added that Iran currently has no plans to engage in a new round of negotiations.
The source further said the Iranian team, representing the Iranian people, sought to safeguard the gains achieved on the ground, arguing that Washington was in greater need of the talks to repair its standing on the international stage.
US leaves Islamabad without an agreement
US Vice President JD Vance announced on Sunday at dawn that negotiations with Iran lasted 21 hours, but ultimately ended without reaching an agreement, failing to produce a satisfactory outcome as the US delegation headed back to Washington.
Vance alleged that core objectives were not achieved despite what he claimed was “significant flexibility” from the US side, claiming that Iran “chose not to accept our terms,” saying the proposal is a “method of understanding that is our final and best offer. We’ll see if the Iranians accept it.”
Of 18,426 patients enrolled in 71 antidepressant trials — 67,319 pages of clinical data, a stack seven metres high, obtained from drug regulators and read for the first time by Peter Gøtzsche’s research group — 12 percent more dropped out while taking the drug than while taking placebo.¹
The psychiatrists’ position is that these drugs do more good than harm. The patients, through their behaviour, delivered the opposite verdict. They preferred the sugar pill.
Nobody who takes a psychiatric drug and reports feeling better is lying. The experience is real. But what produced it, what it is made of, and what it costs — none of this is what the patient was told. Six mechanisms account for almost everything people attribute to their medication. None of them require the drug to be treating a disease.
The Prescription
A person in distress sits across from a doctor. Fifteen minutes later they leave with a diagnosis and a prescription. They are told they have a chemical imbalance that the drug will correct. They may be told depression runs in families — that there is a genetic predisposition, a biological vulnerability they inherited. They are told to give it a few weeks.
The chemical imbalance theory has been abandoned by every serious researcher in the field.² No gene or set of genes for depression has ever been identified despite decades of searching and billions in funding. As Peter Breggin observed, there is no substantial scientific evidence that depression is genetic in origin — and telling patients otherwise leaves them convinced they are stuck with an innate defect, dependent on experts, and resigned to lifelong medication.⁴⁵ The drug was approved on the basis of trials lasting five to six weeks.³ Long-term effects have never been properly studied.⁴ And the condition being treated has a spontaneous remission rate so high that the head of the NIMH’s depression section once observed that most depressive episodes “will run their course and terminate with virtually complete recovery without specific intervention.”⁵
The patient knows none of this. They go home, swallow the pill, and wait.
The First Weeks: Time Heals What the Pill Takes Credit For
Depression, before pharmacology claimed it, was understood to be self-limiting. NIMH psychopharmacologist Jonathan Cole wrote in 1964: “Depression is, on the whole, one of the psychiatric conditions with the best prognosis for eventual recovery with or without treatment. Most depressions are self-limited.”⁶ His colleague Nathan Kline: “In the treatment of depression, one always has as an ally the fact that most depressions terminate in spontaneous remissions. This means that in many cases regardless of what one does the patient eventually will begin to get better.”⁷
Cole and Kline were not dissidents. They were among the most prominent figures in American psychopharmacology.
A study tracking eighty-four patients through untreated depressive episodes found that 23 percent recovered within one month, 67 percent within six months, and 85 percent within a year.⁸ Mark Posternak, the researcher, noted that his results confirmed Kraepelin’s century-old observation that untreated depression typically clears within six to eight months. Dean Schuyler, who headed the NIMH’s depression section, recognised the problem as early as 1974: spontaneous recovery rates were so high that it was difficult to “judge the efficacy of a drug, a treatment or psychotherapy in depressed patients.”⁹
Antidepressants take four to six weeks to produce their claimed effect. Spontaneous recovery begins immediately and continues at roughly 2 percent per week.¹⁰ A person who starts a drug during a depressive episode is beginning treatment at the moment when natural recovery is already underway. A month later, they feel better. The drug gets the credit. The calendar does not.
The Side Effects That Sell the Cure
In the NIMH’s review of all antidepressant studies, well-controlled trials showed 61 percent of drug-treated patients improved versus 46 percent on placebo — a net benefit of 15 percent.¹¹ Irving Kirsch, reviewing FDA data on Prozac, Effexor, Serzone, and Paxil, found the drug-placebo difference on the Hamilton Rating Scale was 1.8 points. The UK’s National Institute for Clinical Excellence had established 3 points as the minimum for clinical significance.¹² The best Danish meta-analysis found a difference of 2 points, and the smallest effect that can actually be perceived on this scale is 5 to 6 points.¹³
That is the margin on which billions of prescriptions rest.
Breggin identified why even this margin exists. He called it the “enhanced placebo effect.” A patient on a sugar pill senses, consciously or not, that nothing powerful has entered their system. An antidepressant produces noticeable physical effects — dry mouth, nausea, drowsiness, sexual dysfunction, weight change. The patient feels these and concludes, reasonably, that they are taking potent medicine. The side effects convince the patient the drug is real. This conviction amplifies the placebo response.¹⁴
Investigators tested this in at least seven studies comparing tricyclic antidepressants to “active” placebos — chemicals that produce unpleasant side effects like dry mouth but have no antidepressant properties. In six of the seven, there was no difference in outcomes.¹⁵ When both pills cause side effects, neither is superior. A Cochrane review confirmed the finding.¹⁶
The entire marginal advantage of antidepressants over placebo may be an artefact of broken blinding. Patients and clinicians can guess who is on the drug and who is on the sugar pill, because the drug has obvious physical effects. This knowledge contaminates every rating, every assessment, every reported outcome.
The NIH-funded St. John’s wort trial demonstrated this by accident. Because St. John’s wort causes side effects similar to an antidepressant, this trial was genuinely blinded — neither patients nor clinicians could tell who was taking what. Results: 24 percent of the herbal group had a full response, 25 percent of the Zoloft group, 32 percent of the placebo group. Zoloft did not outperform placebo. The investigators concluded that the herb was ineffective and neglected to mention that their own drug had failed the same test.¹⁷
The Flattening
Psychiatric drugs produce their effects the same way in patients, healthy volunteers, and laboratory animals. Gøtzsche, drawing on clinical trial data, lists what these effects actually are: numbing of feelings, emotional blunting, drowsiness, reduced concern about oneself and others, diminished capacity for sexual function and romantic attachment.¹⁸
These are not side effects. They are the effects. The drug does not selectively remove depression while leaving everything else intact. It reduces the brain’s capacity to generate emotional intensity across the board. A person who was in anguish may interpret this flattening as recovery. A clinician observing calmer behaviour will rate the patient as improved. Both are observing something real. Neither is observing the treatment of a disease.
Breggin made the point precisely: antidepressants reduce emotional responsiveness generally, which is why they are prescribed not only for depression but for anxiety, panic attacks, obsessive-compulsive behaviour, bulimia, chronic pain, and aggression. They are not treating different diseases through different mechanisms. They are producing the same blunting effect across all of them.¹⁹
The rating scales used to measure “improvement” cooperate with this illusion. The Hamilton Depression Rating Scale — the standard instrument — scores items like sleep quality, appetite, and psychomotor behaviour. A sedated patient who sleeps more and eats more registers as improved. Breggin observed that psychiatric improvement standards are often behavioural (”sleeps better,” “gaining weight”) rather than psychological (”feels better about life,” “actively building a better future”).²⁰ A tranquillised patient and a recovered patient score identically.
Patient self-ratings tell a different story. In Greenberg and Fisher’s meta-analysis of newer antidepressants, patient self-ratings showed virtually no benefit beyond placebo.²¹ The doctors see improvement. The patients, asked directly, do not.
In Denmark, researchers surveyed patients on antidepressants. Half agreed the drugs altered their personality and that they had less control over their thoughts and feelings. The psychiatrists who received these results refused to believe what their own patients told them, called the patients ignorant, and recommended “psychoeducation.”²² The patients’ relatives, independently surveyed, agreed with the patients.
Breggin described a further mechanism operating in some patients: mild organic brain syndrome. Antidepressants, through their general toxicity, can produce a delirium characterised by memory difficulties, confusion, impaired judgment, and mood instability. A patient in this state may experience artificial euphoria or generalised apathy and be evaluated as “improved” — because depression requires a relatively intact brain to sustain itself. Damage the brain sufficiently and the depression lifts, not because the distress has been addressed, but because the capacity to experience it has been impaired.²³ A Yale study found this drug-induced delirium appeared two to four weeks after starting treatment — the exact interval when “therapeutic response” is expected — in more than one-third of patients over age forty.²⁴
The Attempt to Stop
Months pass. Perhaps years. The patient decides to stop. They feel well. They are tired of the side effects. They may have read something that unsettled them.
Within days: headaches, dizziness, nausea, insomnia, agitation, anxiety, confusion, fatigue, flu-like symptoms, electric shock sensations. As many as 50 percent of patients who stop antidepressants experience these withdrawal effects.²⁵
The symptoms vanish when the drug is restarted. The trap closes.
Patient and doctor both conclude that the return of distress proves the drug was treating a real condition. The depression has “come back.” The drug is “needed.” But the symptoms are not relapse. They are withdrawal. The brain, having adapted to the presence of a chemical that altered its neurotransmitter activity, protests the chemical’s removal.
Gøtzsche coined a term for this: “abstinence depression.” A depression that occurs in a patient who is not currently depressed but whose drug is stopped too quickly. Its hallmark: symptoms appear rapidly after discontinuation and disappear within hours when the full dose is resumed. A real depressive episode does not respond to a pill within hours. The speed of response is the diagnostic marker that separates withdrawal from genuine relapse.²⁶
He demonstrated this with a cold turkey trial. Stable, well patients were secretly switched to placebo for 5 to 8 days. Twenty-five of 122 patients on sertraline or paroxetine met criteria for depression during that window. Gøtzsche calculated the expected number of genuine relapses in such a short period, based on known relapse rates from an adolescent depression study: 0.03. Effectively zero. Every one of the twenty-five “relapses” was a withdrawal reaction.²⁷
The profession does not call these symptoms “withdrawal.” It calls them “discontinuation syndrome.” Gary Greenberg described this renaming for what it is: in any other context, a malaise that appears when you stop a drug and disappears when you restart it is called dependence with withdrawal. Calling it “discontinuation syndrome” keeps antidepressants at a comfortable distance from alcohol, benzodiazepines, and opioids.²⁸
The clinical consequences are specific. Breggin described the vicious circle: a patient attempts to stop the drug and experiences withdrawal. The treating professionals mistake withdrawal for relapse. The drug is reinstated. The patient — who might have recovered fully without the medication — is now physiologically dependent on a chemical they were told was safe to stop at any time.²⁹ A study of twenty-two children withdrawn from the tricyclic Tofranil documented this pattern: staff attributed the children’s withdrawal symptoms to “mental illness,” to stress, to allergies, even to viral illness. Antidepressants were restarted in children who were “mistakenly diagnosed as relapsing during the withdrawal period.”³⁰
Gøtzsche reviewed the five most-used psychiatry textbooks in Denmark and found that their withdrawal guidance is wrong and frequently dangerous. Doctors taper too quickly and in linear fashion rather than the exponential taper the drugs’ pharmacology demands. None of the textbooks acknowledged that withdrawal symptoms and disease symptoms are often identical.³¹
The Long Decline
European psychiatrists began noticing the pattern in the 1960s. German physician H. P. Hoheisel reported in 1966 that antidepressant exposure appeared to be “shortening the intervals” between depressive episodes. A Yugoslavian doctor observed the drugs were causing “chronification” of the disease. Bulgarian psychiatrist Nikola Schipkowensky agreed: the tricyclics were inducing “a change to a more chronic course.”³²
Dutch physician J. D. Van Scheyen examined ninety-four depressed patients over five years. Long-term antidepressant medication, he found, “exerts a paradoxical effect on the recurrent nature of the vital depression” — the drugs increased the rate of recurrence and shortened the time between episodes.³³
In 1994, Italian psychiatrist Giovanni Fava forced the question into the open. The drugs, he argued, perturb neurotransmitter systems in ways that produce compensatory brain changes. When the drug is stopped, these changes operate unopposed, producing withdrawal and increasing vulnerability to relapse. The longer someone takes the drug, the worse this becomes. Antidepressants, Fava concluded, “may propel the illness to a more malignant and treatment unresponsive course.” He raised the possibility that the drugs cause “irreversible receptor modifications” that “sensitize” the brain to depression.³⁴
Ross Baldessarini of Harvard confirmed it: half of all patients withdrawn from antidepressants relapsed within fourteen months, and the longer a person had been on the drug, the higher the relapse rate upon withdrawal.³⁵
The profession’s response was not investigation. Donald Klein of Columbia University told Psychiatric News: “The industry is not interested, the NIMH is not interested, and the FDA is not interested. Nobody is interested.”³⁶
Instead, the history was rewritten. The pre-drug studies showing that depression was episodic and self-limiting were declared “flawed.” The 1999 APA Textbook of Psychiatry stated that it was previously believed “most patients would eventually recover from a major depressive episode. However, more extensive studies have disproved this assumption.” Depression was now “a highly recurrent and pernicious disorder.”³⁷
The drugs worsen the long-term course of the illness. Rather than withdraw the drugs, the profession rewrote the natural history of the illness to match the drug-damaged outcomes.
The long-term studies are unambiguous. British researchers found that never-medicated depressed patients experienced a 62 percent symptom reduction in six months; drug-treated patients, 33 percent.³⁸ A WHO study found that patients diagnosed and treated with psychiatric drugs fared worse — in both depressive symptoms and general health — over one year than those not exposed to the drugs.³⁹ In a five-year study of 9,508 depressed patients, those on antidepressants were symptomatic nineteen weeks per year, versus eleven weeks for those on no medication.⁴⁰ An NIMH study found the eighteen-month stay-well rate was highest for cognitive therapy (30 percent) and lowest for antidepressants (19 percent).⁴¹
The STAR*D trial — $35 million of NIMH money, over four thousand “real-world” patients — was announced with the claim that about 70 percent of those who stayed in the study “became symptom-free.” Ed Pigott and colleagues spent more than five years analysing the actual data. The real figure: 3 percent of patients who entered the trial remitted, stayed well, and remained in the study during the one-year follow-up. Confronted with the 3 percent number, investigator Maurizio Fava acknowledged it was accurate. The investigators had known all along.⁴²
The Patients Vote
Those 18,426 patients across Gøtzsche’s 71 trials voted with their feet. Twelve percent more chose to stop taking the drug than chose to stop taking placebo.¹ The finding is worse than it appears, because some of the patients randomised to placebo were suffering cold turkey withdrawal from drugs they had been taking before the trial. Even with this handicap, the placebo group was more willing to continue.
Gøtzsche’s team attempted to assess quality of life — the outcome that matters most to patients. The data was virtually non-existent. Out of 131 studies, three had published quality-of-life results. The data was not missing because it was not collected. It was missing because the results were unfavourable.⁴³
A Danish parliamentarian asked the Minister of Health whether it was reliable to conclude that antidepressants improved quality of life when only three of 131 studies had published data on the question. The minister referred the question to the drug agency, which replied that an effect on quality of life had been found in the studies where it was measured. Quality of life was measured in far more studies than those that published their findings.⁴⁴
What Was Not Disclosed
The feeling was real. It was produced by the natural passage of time and the body’s tendency toward spontaneous recovery. By the placebo effect of receiving treatment from an authority figure. By the enhanced placebo effect of a pill that produces noticeable physical sensations. By emotional blunting that reduced the capacity to feel distress along with the capacity to feel everything else. And in some patients, by a mild organic brain dysfunction that made the sustained experience of depression temporarily impossible.
When it came time to stop, the drug produced withdrawal symptoms indistinguishable from the original condition. Patient and doctor both interpreted this as proof that the disease had returned and the medication was needed for life. The dependence was renamed “discontinuation syndrome.”
For those who stayed on, the drug altered brain chemistry in ways that increased vulnerability to future episodes, shortened the intervals between them, and converted an episodic, self-limiting condition into a chronic one. This conversion was attributed not to the treatment but to a revised understanding of the disease. The textbooks were rewritten to match the drug-damaged outcomes.
At no point was the patient given accurate information. Not about the spontaneous remission rate. Not about the drug’s negligible advantage over placebo. Not about the blunting. Not about the withdrawal. Not about the long-term prognosis.
Three percent of STAR*D patients recovered and stayed well. The investigators announced 70 percent. Sixty-seven thousand pages of clinical trial data sat unread until one research group opened them and discovered that patients preferred placebo. Quality of life data was collected and buried. The profession was told the drugs were sensitising the brain to depression and responded that nobody was interested in investigating.
The patient was told they had a chemical imbalance. They were told the drug would correct it. They were told depression ran in their family and that they were genetically predisposed. They were told to give it a few weeks. Every element of that narrative has been contradicted by the profession’s own research.
The feeling was real. What produced it was not what they said.
References
Sharma, T., et al. “Drop-out rates in placebo-controlled trials of antidepressant drugs.” Int J Risk Saf Med 30 (2019): 217–232. Discussed in Gøtzsche, P.C. “Is psychiatry a crime?” (2024), p. 21.
Moncrieff, J., et al. “The serotonin theory of depression: a systematic umbrella review of the evidence.” Molecular Psychiatry (2022). See also Lacasse, J.R., Leo, J. “Serotonin and Depression: A Disconnect between the Advertisements and the Scientific Literature.” PLoS Med (2005).
Breggin, P.R. Toxic Psychiatry. New York: St. Martin’s Press, 1991, pp. 160–163.
Deshauer, D., et al. “Selective serotonin reuptake inhibitors for unipolar depression.” Canadian Medical Association Journal 178 (2008): 1293–1301.
Schuyler, D. The Depressive Spectrum. New York: Jason Aronson, 1974. Cited in Whitaker, R. Anatomy of an Epidemic. New York: Broadway Paperbacks, 2010, p. 150.
Cole, J. Cited in Whitaker, Anatomy of an Epidemic, p. 150.
Kline, N. Cited in Whitaker, Anatomy of an Epidemic, p. 150.
Posternak, M.A., et al. “The naturalistic course of unipolar major depression in the absence of somatic therapy.” J Nerv Ment Dis 194 (2006): 324–329. Cited in Whitaker, Anatomy of an Epidemic, pp. 163–164.
Schuyler, D. Cited in Whitaker, Anatomy of an Epidemic, p. 150.
Posternak, J Nerv Ment Dis (2006).
NIMH review of antidepressant studies. Cited in Whitaker, Anatomy of an Epidemic, p. 151.
Kirsch, I., et al. “Initial severity and antidepressant benefits.” PLoS Medicine 5 (2008): e45. Cited in Whitaker, Anatomy of an Epidemic, pp. 152–153.
Jakobsen, J.C., et al. “Selective serotonin reuptake inhibitors versus placebo.” BMC Psychiatry 17 (2017): 58. Leucht, S., et al. “What does the HAMD mean?” J Affect Disord 148 (2013): 243–248. Cited in Gøtzsche, “Is psychiatry a crime?” p. 19.
Breggin, P.R. Toxic Psychiatry, pp. 159–160.
Whitaker, Anatomy of an Epidemic, p. 151.
Moncrieff, J., Wessely, S., Hardy, R. “Active placebos versus antidepressants for depression.” Cochrane Database Syst Rev (2004): CD003012.
Hypericum Depression Trial Study Group. “Effect of Hypericum perforatum in major depressive disorder.” JAMA 287 (2002): 1807–1814. Cited in Whitaker, Anatomy of an Epidemic, p. 153.
Gøtzsche, P.C. “Is psychiatry a crime?” (2024), p. 9.
Breggin, P.R. Toxic Psychiatry, pp. 163–164.
Ibid., pp. 160–161. Fisher, S. and Greenberg, R. The Limits of Biological Treatments for Psychological Distress. Hillsdale, NJ: Erlbaum, 1989.
Greenberg, R., et al. Meta-analysis of newer antidepressant drugs. Cited in Breggin, P.R. Talking Back to Prozac. New York: St. Martin’s Press, 1994, pp. 89–92.
Kessing, L., et al. “Depressive and bipolar disorders: patients’ attitudes and beliefs towards depression and antidepressants.” Psychological Medicine 35 (2005): 1205–1213. Cited in Gøtzsche, “Is psychiatry a crime?” p. 21.
Breggin, Toxic Psychiatry, pp. 164–166.
Davies, R., et al. “Confusional Episodes and Antidepressant Medication.” American Journal of Psychiatry (July 1971). Cited in Breggin, Toxic Psychiatry, pp. 165–166.
Greenberg, G. Manufacturing Depression. New York: Simon & Schuster, 2010, pp. 281–282.
Gøtzsche, “Is psychiatry a crime?” pp. 104–105.
Rosenbaum, J.F., et al. “Selective serotonin reuptake inhibitor discontinuation syndrome.” Biol Psychiatry 44 (1998): 77–87. Analysis in Gøtzsche, “Is psychiatry a crime?” pp. 104–105. Expected relapse rate calculated from Lewinsohn, P.M., et al. J Am Acad Child Adolesc Psychiatr 33 (1994): 809–818.
Greenberg, Manufacturing Depression, pp. 281–282.
Breggin, P.R. Toxic Psychiatry, pp. 169–171.
Law, W., III, et al. American Journal of Psychiatry (May 1981). Cited in Breggin, Toxic Psychiatry, pp. 169–170.
Gøtzsche, “Is psychiatry a crime?” pp. 104–105. See also Gøtzsche, P.C. Mental Health Survival Kit and Withdrawal from Psychiatric Drugs. Ann Arbor: L H Press, 2022.
Hoheisel, Schipkowensky, and others cited in Whitaker, Anatomy of an Epidemic, pp. 155–156.
Van Scheyen, J.D. Cited in Whitaker, Anatomy of an Epidemic, p. 156.
Fava, G. “Do antidepressant and antianxiety drugs increase chronicity in affective disorders?” Psychotherapy and Psychosomatics 61 (1994): 125–131. Fava, G. “Holding on: depression, sensitization by antidepressant drugs, and the prodigal experts.” Psychotherapy and Psychosomatics 64 (1995): 57–61. Cited in Whitaker, Anatomy of an Epidemic, pp. 157–159.
Viguera, A. “Discontinuing antidepressant treatment in major depression.” Harvard Review of Psychiatry 5 (1998): 293–305. Cited in Whitaker, Anatomy of an Epidemic, p. 156.
“Editorial sparks debate on effects of psychoactive drugs.” Psychiatric News, May 20, 1994. Cited in Whitaker, Anatomy of an Epidemic, p. 159.
Hales, R., ed. Textbook of Psychiatry. Washington, DC: American Psychiatric Press, 1999, p. 525. Cited in Whitaker, Anatomy of an Epidemic, pp. 159–160.
Ronalds, C., et al. “Outcome of anxiety and depressive disorders in primary care.” British Journal of Psychiatry 171 (1997): 427–433. Cited in Whitaker, Anatomy of an Epidemic, p. 162.
Goldberg, D., et al. “The effect of detection and treatment on the outcome of major depression in primary care.” British Journal of General Practice 48 (1998): 1840–1844. Cited in Whitaker, Anatomy of an Epidemic, p. 168.
Whitaker, Anatomy of an Epidemic, pp. 168–169.
Shea, M.T., et al. “Course of depressive symptoms over follow-up.” Archives of General Psychiatry 49 (1992): 782–787. Cited in Whitaker, Anatomy of an Epidemic, p. 156.
Pigott, H.E., et al. “Efficacy and effectiveness of antidepressants.” Psychother Psychosom 79 (2010): 267–279. Gøtzsche, “Is psychiatry a crime?” pp. 27–28.
Paludan-Müller, A.S., et al. “Extensive selective reporting of quality of life in clinical study reports and publications of placebo-controlled trials of antidepressants.” Int J Risk Saf Med 32 (2021): 87–99. Discussed in Gøtzsche, “Is psychiatry a crime?” pp. 21–22.
Gøtzsche, “Is psychiatry a crime?” p. 22.
Breggin, P.R. Talking Back to Prozac. New York: St. Martin’s Press, 1994, pp. 73–74. See also Breggin, Toxic Psychiatry, pp. 109–141 (chapter on genetics of psychiatric disorders).
The mental health system is failing children by treating everyday struggles as “chronic illness requiring lifelong pharmaceutical treatment,” former psychiatric patient Laura Delano told lawmakers this week.
Delano said many challenges people face are “rooted in nutrition, sleep, stress, trauma, substance use, relationships, vocation, environment, economics, meaning, faith and purpose.” Yet the system often reduces those issues to medical diagnoses, she said.
Drawing on her own 14 years in the mental health system, Delano told lawmakers her experience reflects a broader trend.
Now the founder of Inner Compass Initiative and author of “Unshrunk: A Story of Psychiatric Treatment Resistance,” Delano said more Americans are seeking mental healthcare than ever, but outcomes — including suicide rates among young people — continue to worsen.
‘Two meds became three, four, five. My life unraveled’
Delano said she began treatment at 13. She was diagnosed with bipolar disorder and told she would need medication for life.
“You’re told this is an incurable illness. You’ll have this for the rest of your life. It’s manageable with medications, but you will never not have it,” she said. “And that’s the story that many, many people are being told about these conditions, which is simply not true.”
Over time, her diagnoses expanded and her prescriptions multiplied.
“Two meds became three, four, five,” she said. “My life unraveled.”
She said she gained weight, developed chronic health issues and became “increasingly anxious and suicidal.”
“Eventually, I couldn’t work or take care of myself,” she said.
“Nobody told me” that many psychiatric drugs were approved based on trials lasting “on average 6 to 12 weeks,” or that the long-term effects of taking multiple drugs together have “never been properly established.”
She said she wasn’t warned that medications could cause “serious physical health problems,” impair sexual function or, in some cases, increase suicidal thoughts.
When she tried to stop taking the drugs, she said she experienced withdrawal symptoms, but was told it was a relapse.
“Nobody told me that what I experienced … was withdrawal,” she said. “Instead, I was told that my worsening state meant my illness was so severe that it was now resistant to any treatment.”
At 25, Delano said she believed there was no hope. She attempted suicide.
‘This is the next opiate crisis, and I think it’s bigger’
Delano’s testimony comes as mental health outcomes worsen, even as diagnoses and prescriptions keep rising.
From 2007 to 2021, the suicide rate among people ages 10-24 increased by 62%. In 2023, over 49,000 Americans died by suicide — the highest number on record, and about 20,000 more than in 2000.
Among adolescents in 2024, 2.6 million reported serious suicidal thoughts, 1.2 million made a plan, and 700,000 attempted suicide.
At the same time, diagnoses have surged. Today, about 23.4% of U.S. adults — roughly 61.5 million people — experienced mental illness. This includes more than 36% of young adults.
Medication use has climbed alongside those numbers.
Since 2006, the use of SSRIs in children has more than doubled. A December 2025 report found that 6.1 million U.S. children ages 17 and under are taking at least one psychiatric drug.
“This is the next opiate crisis, and I think it’s bigger,” Delano said.
Doctors are increasingly medicalizing ‘normal human unhappiness’
Other experts at the roundtable raised similar concerns about diagnosis and treatment.
Dr. Sally Satel, a psychiatrist and senior fellow at the American Enterprise Institute, said clinicians often blur the line between clinical depression and life challenges.
“I can’t tell you how many people … once got a diagnosis [of depression], but their diagnosis is really demoralization,” she said.
“Do we need medications for that?” Satel asked. In some cases, what patients need to hear is, “Your life is difficult. You’re actually having a rational response to a difficult life,” she said.
Satel also said psychiatrists do not prescribe most psychiatric medications.
Primary care providers and midlevel practitioners write many of the prescriptions, she said. “That’s definitely … a problem.”
“We are overdiagnosing,” she added. “We’re turning … normal human unhappiness into … diagnoses that we then prescribe medications for that probably won’t work.”
‘Doubling down on what we’re doing … is not going to get us anywhere’
Dr. David Hyman, a physician and legal scholar, drew a similar distinction.
“Sadness and depression are two different things,” he said. Treatment — and not necessarily with medication — should focus on the latter, he added.
He also warned against a system that increasingly defaults to prescribing. “Doubling down on what we’re doing, which isn’t working, is not going to get us anywhere better than where we are,” he said.
While medications must show safety and efficacy to gain approval, he said, there is no consistent system to study the long-term effects or what happens when patients stop taking them.
“There’s not a mechanism or systematic reevaluation of things after they’ve been approved,” he said.
Tapering can take ‘not just months, but years’
Delano said that gap is especially clear when patients try to taper off medications.
Asked how often patients receive full information about their diagnosis and medications, she said: “From what I’ve seen, never.”
“It took 13 years to realize I needed to get out,” Delano said. But getting off the drugs is “incredibly difficult.”
“We have a system set up that makes it incredibly easy to start these drugs that were really only ever studied for … short-term use,” she said. “Yet, most people stay on them long term for years and have zero safe off-ramps.”
Without clear guidance, people often stop too quickly, feel worse and assume they need the drugs indefinitely, she said.
Delano called for updated drug labels, public education and clinical guidelines for gradual tapering.
She stressed that these medications can create physical dependence. “Not addiction, it’s different than addiction,” she said. It’s a biological effect that can make stopping difficult.
“It sounds so unfathomable that a capsule … might require chipping away … over not just months, but years,” she said. Yet for some patients, that level of gradual tapering is necessary, she added.
Now 16 years off psychiatric medications, Delano said her experience drives her work.
“It’s urgent that we better understand what is happening in people’s brains and bodies from using these medications long term and from trying to get off them,” she said.
Watch an excerpt from the subcommittee hearing here:
During World War I, for security reasons the Australian Government pursued a comprehensive internment policy against enemy aliens living in Australia.
Initially only those born in countries at war with Australia were classed as enemy aliens, but later this was expanded to include people of enemy nations who were naturalised British subjects, Australian-born descendants of migrants born in enemy nations and others who were thought to pose a threat to Australia’s security.
Australia interned almost 7,000 people during World War I, of whom about 4,500 were enemy aliens and British nationals of German ancestry already resident in Australia.
During World War II, Australian authorities established internment camps for three reasons – to prevent residents from assisting Australia’s enemies, to appease public opinion and to house overseas internees sent to Australia for the duration of the war.
Unlike World War I, the initial aim of internment during the later conflict was to identify and intern those who posed a particular threat to the safety or defence of the country. As the war progressed, however, this policy changed and Japanese residents were interned en masse. In the later years of the war, Germans and Italians were also interned on the basis of nationality, particularly those living in the north of Australia. In all, just over 20 per cent of all Italians resident in Australia were interned. … continue
This site is provided as a research and reference tool. Although we make every reasonable effort to ensure that the information and data provided at this site are useful, accurate, and current, we cannot guarantee that the information and data provided here will be error-free. By using this site, you assume all responsibility for and risk arising from your use of and reliance upon the contents of this site.
This site and the information available through it do not, and are not intended to constitute legal advice. Should you require legal advice, you should consult your own attorney.
Nothing within this site or linked to by this site constitutes investment advice or medical advice.
Materials accessible from or added to this site by third parties, such as comments posted, are strictly the responsibility of the third party who added such materials or made them accessible and we neither endorse nor undertake to control, monitor, edit or assume responsibility for any such third-party material.
The posting of stories, commentaries, reports, documents and links (embedded or otherwise) on this site does not in any way, shape or form, implied or otherwise, necessarily express or suggest endorsement or support of any of such posted material or parts therein.
The word “alleged” is deemed to occur before the word “fraud.” Since the rule of law still applies. To peasants, at least.
Fair Use
This site contains copyrighted material the use of which has not always been specifically authorized by the copyright owner. We are making such material available in our efforts to advance understanding of environmental, political, human rights, economic, democracy, scientific, and social justice issues, etc. We believe this constitutes a ‘fair use’ of any such copyrighted material as provided for in section 107 of the US Copyright Law. In accordance with Title 17 U.S.C. Section 107, the material on this site is distributed without profit to those who have expressed a prior interest in receiving the included information for research and educational purposes. For more info go to: http://www.law.cornell.edu/uscode/17/107.shtml. If you wish to use copyrighted material from this site for purposes of your own that go beyond ‘fair use’, you must obtain permission from the copyright owner.
DMCA Contact
This is information for anyone that wishes to challenge our “fair use” of copyrighted material.
If you are a legal copyright holder or a designated agent for such and you believe that content residing on or accessible through our website infringes a copyright and falls outside the boundaries of “Fair Use”, please send a notice of infringement by contacting atheonews@gmail.com.
We will respond and take necessary action immediately.
If notice is given of an alleged copyright violation we will act expeditiously to remove or disable access to the material(s) in question.
All 3rd party material posted on this website is copyright the respective owners / authors. Aletho News makes no claim of copyright on such material.