FBI Contractor Created Fake Online IDs to Join Chatrooms Run by Groups Organizing Against Vaccine Mandates
By Brenda Baletti, Ph.D. | The Defender | May 12, 2023
An FBI surveillance contractor infiltrated the chatrooms of two airline industry groups opposed to vaccine mandates to collect intelligence on the groups’ organizing activities, investigative journalist Lee Fang reported.
The contractor, Flashpoint, which in the past infiltrated Islamic terror groups, now focuses on “anti-vaccine” groups and other domestic political organizations, according to Fang.
In a webinar presentation for clients last year, which Fang analyzed on his Substack, Flashpoint analyst Vlad Cuiujuclu demonstrated his company’s methods for identifying and entering encrypted Telegram chat groups.
He explained how the company attempted to join chatrooms of transportation workers resisting the COVID-19 vaccine mandates.
Fang described the presentation:
“‘In this case, we’re searching for a closed channel of U.S. Freedom Flyers,’ said Cuiujuclu. ‘It’s basically a group that opposed vaccination and masks.’
“As he clicked through a database, Cuiujuclu showed a chat group on Telegram sponsored by Airline Professionals For Justice, another group formed by airline industry workers opposed to the mandate. The forum, he added, provided useful insights, including Zoom links for meetings of the grassroots organization.
“‘Private chats,’ said Cuiujuclu, ‘require for you to have an invite link,’ which he noted can often either be found by scrolling through public forums or by ‘engag[ing] the admin of that channel.’”
Flashpoint also offers clients artificial intelligence and internet scraping tools.
According to Fang, the firm is a leader in the “threat intelligence industry,” a growing number of security and surveillance firms that create fake online identities to infiltrate Discord chats, WhatsApp groups, Reddit forums and dark web message boards to gather information for clients, including corporations and the FBI, to monitor potential threats.
Joshua Yoder, president of US Freedom Flyers, said he is aware that Flashpoint infiltrated private chat groups associated with his organization.
Yoder told The Defender :
“Tradecraft and other strategies are often used to gain inside knowledge of conservative organizations with the intent to disrupt, mislead and otherwise thwart effective campaigns.
“Infiltration is a tactic used by the deep state to prevent the truth from being told by attempting to destroy the advancement of the message. The team at US Freedom Flyers has been successful in recognizing these attacks and we have taken decisive actions to protect the organization and our members.”
Aviation industry workers were some of the most vocal and organized against COVID-19 vaccine mandates.
They wrote an open letter to the aviation industry signed by thousands of organizations, physicians and pilots. They also organized research on the risks of vaccines for pilots, spoke publicly about the “culture of fear and intimidation” around the mandates in the industry, and filed multiple lawsuits in Canada, the Netherlands, and the U.S.
US Freedom Flyers brought a lawsuit against Atlas Air, one of the largest air cargo carriers in the aviation industry, in May 2022.
Fang told The Defender the targeting of American citizens resisting the vaccine mandates fits into a long history of surveillance being used to subvert democracy. He said:
“There is a long sordid history of informants and surveillance contractors working to undermine democratic engagement in this country.
“The push against regular citizens opposed to COVID-19 vaccine mandates has come in many forms: censorship, demonization and in this case, surveillance.”
The growing market for spying on domestic dissent
Flashpoint advertises its surveillance success on its website, providing examples of its work undermining environmental activism, G20 protests and protests against the aviation industry.
The webpages describing these activities were taken down after Fang published his investigation, but they can be found on the Wayback Machine internet archive.
For example, Flashpoint described its capacity to monitor activists organizing against pollution and the aviation industry. The website said:
“By monitoring the situation and assessing tactics, techniques, and procedures (TTP’s), Flashpoint was able to assess the impact of upcoming protests, and determine that these groups would likely continue to protest and attempt to impede airport construction and expansion projects through direct action. …
“Based on this information, Flashpoint customers were able to take actions to help control the impact to business operations, and to ensure the safety of their employees and facilities as well as the safety of those protesting.”
Flashpoint was founded by Evan Kohlmann, former NBC News contributor who investigated Islamic terror groups and whom The Intercept described as “the U.S. government’s go-to expert witness in terrorism prosecutions.”
Jack Poulson of Tech Inquiry, a group that researches the surveillance industry, told Fang that “Flashpoint has been selling its chatroom infiltration services to companies and governments for years.”
But, he said, it has shifted its focus from “surveilling Muslims after September 11” and “followed the money into both the Pentagon’s information warfare programs and the business of monitoring domestic protest groups.”
Last year, Flashpoint acquired Echosec Systems, another intelligence contractor, and last month it formalized a partnership with Google Cloud.
These acquisitions come in addition to “a steady stream of contracts to Flashpoint in recent years from the FBI, the Department of Defense, Treasury Department, and Department of Homeland Security, among other agencies,” Fang wrote.
Fang also spoke to Jay Bhattacharya, M.D., Ph.D., professor of medicine at Stanford University, research associate at the National Bureau of Economics Research and one of the authors of the Great Barrington Declaration.
Bhattacharya said:
“This kind of domestic spying violates the implicit protection Americans have in these kinds of settings.
“This isn’t terrorism, this doesn’t have anything to do with national security.
“This is a private set of employees, workers who are trying to maintain their jobs in the face of unscientific demands for COVID vaccinations.”
Brenda Baletti Ph.D. is a reporter for The Defender. She wrote and taught about capitalism and politics for 10 years in the writing program at Duke University. She holds a Ph.D. in human geography from the University of North Carolina at Chapel Hill and a master’s from the University of Texas at Austin.
This article was originally published by The Defender — Children’s Health Defense’s News & Views Website under Creative Commons license CC BY-NC-ND 4.0. Please consider subscribing to The Defender or donating to Children’s Health Defense.
Robert Kennedy Jr. is the only presidential candidate to still be banned from Instagram
By Tom Parker | Reclaim The Net | May 12, 2023
Robert Kennedy Jr., a Democratic candidate for the 2024 United States presidential election, revealed that his account is till banned from Instagram and accused the tech giant of preventing him from accessing the site, despite him being a contender for the White House.
This makes him the only 2024 US presidential candidate that’s unable to post to the influential social media platform and currently being subjected to direct Big Tech censorship.
Former President Donald Trump, who is running for president in 2024 as a Republican candidate, was suspended from Instagram on January 6, 2023 and banned on January 7. However, his ban was lifted on January 25, 2023.
The other 2024 presidential candidates, Joe Biden (D), Marianne Williamson (D), Larry Elder (R), Nikki Haley (R), Asa Hutchinson (R), Vivek Ramaswamy (R), and Corey Stapleton (R), all have active Instagram accounts.
Kennedy was banned from Instagram in February 2021 for violating the platform’s strict speech rules related to the coronavirus and vaccines. The ban came after several Democratic senators and 12 state attorneys general demanded that Kennedy and other Covid vaccine skeptics be deplatformed by Big Tech. Before the ban, Kennedy had over 800,000 Instagram followers.
Instagram’s failure to reinstate Kennedy since announcing his presidential campaign means that he won’t be able to directly post his message to the social media platform’s sizeable audience of two billion monthly active users.
COVID Was Not Dangerous to Unvaccinated Pregnant Women
BY IGOR CHUDOV | MAY 11, 2023
Remember the endless media hysterics about COVID being “dangerous to unvaccinated pregnant women”?

A recent report MBRRACE-UK throws doubt on such statements. It covers 2018-2020, so the year of 2020 was a part of the COVID pandemic.
In the UK, in 2020 (before COVID vaccines), only NINE women died from (or with) COVID-19 during pregnancy or up to six weeks after giving birth.

Remember that in 2020, all pregnant women in the UK were unvaccinated. COVID was at its worst in 2020.
COVID was quite rampant in the UK at the time. According to Our World in Data, the UK had 94,194 COVID deaths in 2020. However, only nine deaths out of those involved pregnant women.
ONS reports that England and Wales had 613,936 live births in 2020.

So,
- Pregnant women’s COVID deaths (9 total) were less than one in ten thousand overall COVID deaths.
- Pregnant women’s deaths (9 total) were less than one in 68,000 (sixty-eight thousand) births.
- In other words, for every pregnant woman who died of COVID in 2020, over 68,000 did NOT die.
Every death is a tragedy, especially those of future mothers. Those nine deaths were tragic for the families involved. I am very sorry for each of the nine women who died with COVID in the UK in 2020. I am relieved, however, that the number of deaths among pregnant women was far less than what the media intimated.
Was COVID a great danger to pregnant women? The numbers above suggest that the chance of dying from COVID for unvaccinated women in 2020 was very remote, as there was less than one COVID death per 68,000 births.
To me, this cannot be considered “particularly dangerous.” Pregnant women are young (most are under 40), and Covid is not particularly deadly to that age category.
So, those who believed that COVID-19 puts future mothers’ lives at tremendous risk were lied to. Pregnant women were given false information to nudge them to get vaccinated.
We finally have the proof.
Pfizer trial data showed danger for babies but health czars recommended jabs to pregnant women anyway
By Guy Hatchard | TCW Defending Freedom | May 11, 2023
A PREPRINT paper published this month highlights just how many unknowns we are dealing with when it comes to assessing the long-term outcomes of mRNA vaccination. It shows that IgG4 antibodies are present in umbilical cord blood of infants born to vaccinated mothers, meaning a theoretical risk to newborns of an ineffective response to Covid infection.
But was this really unknown to those recommending that mRNA vaccination was safe for pregnant women? Documents released by Pfizer under court order reveal that Pfizer and the US Food and Drug Administration (FDA) were well aware of clinical trial results indicating appalling outcomes for babies of pregnant women.
Watch this 20-minute video where dozens of so-called experts in New Zealand are recorded telling us that the mRNA Covid vaccines are completely safe for pregnant women in direct contradiction of Pfizer trial results available in April 2021. These results indicated an unfolding disaster for babies including miscarriage, premature birth, cardiac arrest, toxic breast milk and spike protein crossing the placenta.
In the video, their comments are juxtaposed with scientists exposing the highly disturbing content of the Pfizer trials of pregnancy outcomes.
Was the NZ government aware of this information? Certainly the contractual arrangements that our government had made with Pfizer would have required Pfizer to fully inform the Ministry of Health of all the results of vaccine trials. But the MoH has completely ignored the information which has become public knowledge. Since the start of this month they are again encouraging pregnant and breastfeeding mothers from 16 and up to get a further booster shot. Why? Especially considering the increased incidence of miscarriages and stillbirths since the NZ vaccine rollout began.
I can’t imagine at this time a more important video to watch than this 20-minute film of our experts lining up to misinform prospective mothers of safety. Were they misled by Pfizer, by the MoH, by politicians, by the FDA, or by all of the above? Or did they just decide to promote a safety rating without any evidence to back up their statements? We may never know, but the lesson of this video is clear: we will not be able to trust the medical czars again.
Covid jabs the big picture: Part 1
Overview of evidence prior to rollout
Health Advisory & Recovery Team | May 10, 2023
HART have been asked to submit evidence to module 3 of the Covid-19 Public Inquiry. That module is about the impacts on healthcare but we were specifically asked to include evidence around deaths in males aged 15-18 years of age and so provided an overview of the full impact these novel products have had on the healthcare system. What follows are some of the highlights. There will be three parts to this series. Here the evidence on what was known before rollout will be presented. Part two covers the evidence after rollout (excluding deaths) and part three the evidence on deaths.
It is worth remembering how cautious people were about any novel products that might claim to prevent covid. In February 2020, Chris Whitty said,
“The rate limiting steps are late clinical trials for safety & efficacy, & then manufacturing. For a disease with a low (for the sake of argument 1%) mortality a vaccine has to be very safe so the safety studies can’t be shortcut. So important for the long run.”
He was right.
The belief that vaccines were safe had led to a circular belief that vaccines required fewer safety checks than other novel therapies. Novel vaccines take a decade or more to go through safety checks. Flu vaccines don’t. These novel drugs were treated like flu vaccines for regulatory purposes.
The regulators failed us in numerous ways as set out in The Perseus Report. Examples include:
- Companies were allowed to skip testing for gene and cancer toxicity and even studies showing how much spike is produced, for how long and where in the body it reaches. Pfizer said these studies were “not considered necessary.” Even while their trial info sheet said “Due to the urgent need for a vaccine against Covid-19, with agreement from the MHRA, some of the tests usually required for a newly manufactured vaccine have been modified, in order to make the vaccine available more quickly for assessment.”
- They did not demand these studies were done after rushed emergency approvals either. No human studies were carried out to see what happened to the synthetic modified RNA – no-one knows how long it takes to be removed from the body. There is evidence that in some it lasts between at least 28 days and 4 months in the blood.
- The regulators let the pharma companies get away with terminating the placebo arm of the study after ~3months by offering them all the novel products.This was despite us knowing that narcolepsy caused by Pandemrix vaccine took on average of 8 months to be diagnosed.
- The lipid nanoparticles that deliver the modified synthetic mRNA are themselves toxic. This mechanism of delivery was shelved in 2016 for gene therapy to treat inherited genetic conditions because of the multiple doses needed. It was claimed it could still be used in vaccine technology because that only requires one dose…
- The viral vector used for delivering the AstraZeneca DNA message was reported in 2007 to cause platelet activation, which can lead to blood clots.
- There were many more points made including failings in investigating deaths, failing to listen to patients, problems with manufacturing processes and problems with accountability and governance all of which are in the report.
Since 2005 there have been concerns about the regulator losing “sight of the need to protect and promote public health.” The CEO of the MHRA, Dame June Raine, claims the MHRA is now an “enabler” not a “watchdog.” Even before there was political capture there were pre-existing conflicts of interest.
The spike protein is the most toxic part of the virus. It damages lungs, vessel walls and causes clots. Part of the sequence is identical to a region of a bacterial sequence that can bind directly to a particular type of white blood cells resulting in lethal cytokine storms. This part of the sequence was heavily mutated in the Omicron variant making it less lethal. However, even the most recent injections contained the original Chinese spike sequence with this dangerous sequence.
The manufacturers decided to use the WHOLE chinese spike sequence rather than parts of it, or peptides, which have been shown to be safer for vaccine design. Some manufacturers modified the spike so that it could not bind to the receptor and enter a cell. This might have reduced some harm from receptor binding but not from the action of spike within cells. The spike was delivered into cells so spike was produced INSIDE the cells in the first place. AstraZeneca did not modify the sequence. From November 2020 it was clear that parts of AZ spike could be shed outside of cells.
The Pfizer and Moderna clinical trial data shows a higher rate of serious adverse reactions from the treatment group (12.5 per 10,000) than any reduction in serious events from covid (2.3 and 6.4 per 10,000 for Pfizer and Moderna respectively). Yet the claim of 90%+ efficacy was all that was reported and all that Dame June Raine claimed she needed to see in order to approve the drugs.
AZ issued a press release claiming 100% efficacy against hospitalisation and death after only two severe covid hospitalisations and one death in the placebo arm. This claim was repeated widely and was believed.
At the time, the priority was to protect the old and vulnerable who accounted for 98% of covid deaths. There were going to be 15 million jabs to freedom:

The evidence presented is damning. The failures of the regulators to adequately test the safety and efficacy of these novel vaccines are shocking. The circular belief that vaccines required fewer safety checks than other novel therapies is a dangerous assumption that has put the lives of millions at risk. The fact that serious adverse reactions were higher in the treatment group than any reduction in serious events from covid is deeply concerning. We must demand accountability from the regulators and demand that the safety and wellbeing of the public is always the top priority, not profit or political gain. There was total regulatory failure in allowing these products to be given to anyone, which was compounded by not withdrawing them promptly once evidence these issues were clinically relevant became clear.
Andrew Bridgen MP Joins Reclaim Party and Announces He is Suing Matt Hancock for Defamation

BY WILL JONES | THE DAILY SCEPTIC | MAY 10, 2023
Ex-Tory MP Andrew Bridgen, who was expelled from the party for criticising the Covid vaccines, has announced he’s joining Laurence Fox’s Reclaim Party, making him its first member of Parliament. At a press conference today Bridgen said he would be standing at his North West Leicestershire constituency at the next General Election. He also confirmed he would be suing Matt Hancock MP for defamation over an allegation of antisemitism.
At the press conference this morning Bridgen confirmed he has decided not to appeal his expulsion and blasted the Conservative Party. He said:
Even if I were to be given a fair hearing, which I doubt, I would not wish to rejoin the party after the treatment received by myself and my family over the past few years.
I feel now that the party no longer represents the people of this great country. If I am to represent my constituents and countrymen it must be from outside the party which I have served dutifully for many decades.
I will be standing again in North West Leicestershire at the next election. Not as a Conservative, but as a Member of the Reclaim Party. More than anything, the Reclaim Party stands for freedom of speech.
I will cross the floor today, Wednesday May 10th, and sit on the opposition benches as the first Member of Parliament for the Reclaim Party. I say first because I have no doubt I will not be the last. This is just the beginning.
If the Conservative Party wishes to contest my seat it can do so at the next General Election.
I have more confidence that I will win my seat than the vast majority of sitting Conservative MPs, so I welcome the challenge should the Prime Minister and Parliamentary Party wish to take it.
Bridgen was accused of antisemitism for agreeing in a tweet with an anonymous heart doctor he quoted that the Covid vaccine rollout was “the biggest crime against humanity since the Holocaust”.
He has denied the allegation – which we at the Daily Sceptic agree is spurious and an example of a weaponised antisemitism allegation to achieve political ends. This morning Bridgen confirmed that he will be suing ex-Health Secretary Matt Hancock for defamation after the Conservative MP tweeted in January that he was spouting “antisemitic, anti-vax, anti-scientific conspiracy theories”.
In a YouTube video Bridgen said he has submitted a “defamation claim to the Royal Court of Justice against Matthew Hancock MP”. The basis of the claim is that Hancock’s accusation of antisemitism is “a false slur to deliberately try and shut down valid concerns raised by me on behalf of constituents and thousands of others around the world about the safety and efficacy of the experimental COVID-19 injections”.
Matt Hancock in the dock: that’s a court case to look forward to.
You can donate to Andrew Bridgen’s legal fund here.
Andrew Bridgen and Fraser Myers clash in fiery debate on Covid vaccine harms
GBNews | May 8, 2023
Andrew Bridgen, a Member of Parliament in the UK, has been vocal about vaccine harms and the origins of Covid.
Fraser Myers, deputy editor of Spiked online, published an article called “The delusions of Andrew Bridgen – Conspiratorial thinking corrodes reason, democracy and humanism”.
The pair joined Andrew Doyle on GB News in a fiery debate.
One Health: A Plan to ‘Surveil and Control Every Aspect of Life on Earth’?
This is part two of a two-part series on the One Health initiative. Read part one here.
By Michael Nevradakis, Ph.D. | The Defender | May 8, 2023
The World Health Organization (WHO) defines “One Health,” as “an integrated, unifying approach that aims to sustainably balance and optimize the health of people, animals and ecosystems,” as they are “closely linked and interdependent” — a concept that on the surface appears to promote noble goals interlinking human and environmental health.
However, some scientists and medical experts are concerned about One Health’s vague goals. Arguing that the concept has been “hijacked,” they question the intent of those involved with the development and global rollout of the concept — including the WHO, the Centers for Disease Control and Prevention (CDC) and the World Bank.
Experts who spoke with The Defender also raised questions about other aspects of the One Health concept, including a biosecurity agenda, a global surveillance system, vaccine passports and restrictions on human behavior.
While these goals are underpinned by a vaguely defined “Theory of Change,” experts told The Defender that major financial interests are at the heart of the One Health agenda, which appears to be closely linked to climate change and sustainable development initiatives promoted by the same global organizations.
One Health objectives include a ‘global takeover of everything’
In a May 1 article, Dr. Joseph Mercola connected the One Health concept, as promoted by global organizations, to the policies and restrictions pursued in response to COVID-19, describing it as an attempted “global takeover of everything.”
Mercola tied the One Health concept to key entities that have supported gain-of-function research. According to Mercola:
“Interestingly, the term ‘One Health,’ which was formally adopted by the WHO and the G20 health ministers in 2017, was first coined by the executive vice president of the EcoHealth Alliance, the same firm that appears to have had a hand in the creation of SARS-CoV-2.”
During the 2019 lecture “Can One Health Help Prevent the Next Pandemic?” EcoHealth Alliance President Peter Daszak, Ph.D., commissioner in The Lancet’s One Health Commission, said “emerging infectious diseases” are “a growing global threat.”
He also argued that many of these emerging diseases are “zoonotic — spread from animals to humans.”
Francis Boyle, J.D., Ph.D., professor of international law at the University of Illinois and a bioweapons expert who drafted the Biological Weapons Anti-Terrorism Act of 1989, questioned this narrative, telling The Defender :
“All these ‘emerging infectious diseases’ are emerging out of their offensive biological warfare weapons programs conducted in their BSL4 [biosecurity level 4] and BSL3 laboratories.
“If you look at the people on the WHO advisory committee dealing with ‘emerging infectious diseases,’ that’s exactly what they are doing — ‘emerging’ them from their labs.”
One example is that of Marion Koopmans, DVM, Ph.D., director of the WHO Collaborating Centre for emerging infectious diseases at Erasmus Medical Centre in the Netherlands and member of the WHO’s One Health High-Level Expert Panel (OHHLEP).
According to Boyle, “Erasmus is where this offensive Nazi biowarfare gain-of-function death science dirty work first became notorious under Fouchier, [who] started the entire controversy over his gain-of-function work there.”
Boyle was referring to Ron Fouchier, Ph.D., who also is deputy head of Erasmus’ Viroscience Department and who, according to Science, “alarmed the world” in 2011, after he and other researchers “separately modified the deadly avian H5N1 influenza virus so that it spread between ferrets” — an early example of gain-of-function research.
Dr. Meryl Nass, an internist and biological warfare epidemiologist who is a member of the Children’s Health Defense scientific advisory committee, said such objectives are kept deliberately vague. She referred to a CDC document that stated:
“Successful public health interventions require the cooperation of human, animal, and environmental health partners … Other relevant players in a One Health approach could include law enforcement, policymakers, agriculture, communities, and even pet owners.
“By promoting collaboration across all sectors, a One Health approach can achieve the best health outcomes for people, animals, and plants in a shared environment.”
Nass wrote on her blog, “I anticipate that One Health will be used to impose changes in the way humans and animals interact … most likely based on the needs of the WEF [World Economic Forum]/elites and not the needs of the people or the animals that will be affected.”
Reggie Littlejohn, founder and president of Women’s Rights Without Frontiers and co-chair of the Stop Vaccine Passports Task Force, told The Defender, “It’s not clear that One Health is prioritizing human health.”
Highlighting the “vague” language employed by the global organizations promoting One Health, Littlejohn said that one goal may be to “govern farm animal health in addition to human health,” through which “they could do things like forcing vaccines on livestock.”
One Health means ‘surveilling everything’
The experts who spoke with The Defender expressed concerns over the biosecurity agenda that is associated with the stated objectives of One Health.
According to Nass, this reflects how the WHO “has been changing into a biosecurity agency,” adding that “the justification, apparently, for the WHO’s director-general to take over jurisdiction of healthcare during pandemics, but also potentially ecosystems, animals and plants, is through One Health.”
Nass noted that One Health “is mentioned several times in the National Defense [Authorization] Act for Fiscal Year 2023” (NDAA), which includes 18 pages on “pandemic preparedness” and a formal definition of the “One Health approach” on page 952 of the act.
Independent journalist and researcher James Roguski also highlighted the prominent placement of One Health in the NDAA and noted that, by formally defining the concept within the act, it is now part of the Code of Federal Regulations.
However, Roguski said the NDAA goes even further:
“The U.S. has pledged a billion dollars a year to the World Bank Pandemic Fund in support of the global health security agenda. The WHO is one of 14 intermediaries who will receive and redistribute some of that billion dollars.
“Basically, it’s capitalism, it’s corruption, it’s an abomination from a health perspective. Let’s just throw money at pharmaceutical companies, build out the infrastructure in these nations and, if you’re making tons of products locally, you’re going to be able to convince the local government to stick them in people’s arms or shove it down their throat.
“And none of it really has shown to be of any health benefit. It’s damage to people’s health.”
Associated with the promotion of a global biosecurity agenda is the development of a global surveillance infrastructure that would purportedly protect human and animal health and the environment. An Oct. 3, 2022, WHO document states:
“The emergence of the SARS-CoV-2 virus that caused COVID-19 has underlined the need to strengthen the One Health approach, with a greater emphasis on connections to animal health and the environment …
“… It uses the close, interdependent links among these fields to create new surveillance and disease control methods. …
“We now have an unprecedented opportunity to strengthen collaboration and policies across these many areas and reduce the risk of future pandemics and epidemics while also addressing the ongoing burden of endemic and non-communicable diseases
“Surveillance that monitors risks and helps identify patterns across these many areas is needed.”
Remarking on this, Littlejohn said One Health’s proponents talk about “interoperable, integrated surveillance systems.” She told The Defender :
“I believe … these surveillance systems of people, animals, plants, and the environment are going to be coordinated by some kind of a global surveillance system that is interoperable globally and integrated.
“Whoever’s running this show, the WHO, the Chinese Communist Party … the Bill and Melinda Gates Foundation, who are the people who really appear to be running the show at the WHO, are going to be able to tap into and see all of our private information. Not just us, but animals and plants.”
Dr. David Bell, a public health physician and biotech consultant and former director of global health technologies at Intellectual Ventures Global Good Fund, told The Defender that what global organizations intend is “surveilling everything.” He said:
“It means surveilling everything, surveilling the climate for possible threats, surveilling animal population, surveilling wildlife, surveilling the soil to see if there’s new traces of virus or bacteria in river systems, et cetera.
“This allows you to ‘discover’ what we already know is nature, and then turn nature into a potential threat or into a threat. The more surveillance you have and the wider it is, the more inevitable ‘threats’ you’ll find … because you can make an argument that almost any new variant virus is a ‘threat.’
“It will allow them to keep a constant kind of fear which then allows you to introduce authoritarian controls such as central bank digital currencies and digital passports … that allow them to monetize the human population more effectively.”
Nass noted that global actors such as the WHO “talk about sharing of specimens during a pandemic … so they can try to make vaccines too. However, they don’t talk about performing surveillance on human beings. But what they did say, which let the cat out of the bag, is that they would want to get informed consent from countries for sharing of genomic data, rather than from individuals.”
Part of this surveillance infrastructure also would include vaccine passports, which figure prominently in the pandemic treaty and amendments to the International Health Regulations (IHR) currently under negotiation at the WHO.
According to Littlejohn:
“I believe that they laid the infrastructure during the COVID-19 crisis, and we’re having a little bit of a ‘break’ here between pandemics, but that structure, that infrastructure is going to snap shut with the next pandemic if we don’t stop it. That structure has to do with vaccine passports.
“It could be called a ‘smart health card’ or ‘digital health ID,’ or even a mandatory digital driver’s license can serve as the platform for a China-style social credit system. And there’s a new bill in front of the Senate right now … the Improving Digital Identity Act of 2023 … It’s a mandatory national ID that’s going to be interoperable, coordinated, integrated and can serve as the same platform as China’s social credit system … to surveil us.”
Restrictions on human behavior could lower humans to the level of animals
The WHO’s Oct. 3, 2022, document also claimed that “Some 60% of emerging infectious diseases that are reported globally come from animals, both wild and domestic,” adding that “human activities and stressed ecosystems have created new opportunities for diseases to emerge and spread.”
Such stressors “include animal trade, agriculture, livestock farming, urbanization, extractive industries, climate change, habitat fragmentation and encroachment into wild areas,” according to the WHO.
“To the extent that carbon emissions due to transportation within cities would contribute to climate change, then the ‘15-minute city’ would be a way of addressing that,” Littlejohn said. “The danger is that they will enforce it by having surveillance cameras everywhere to make sure you don’t go outside of your district without permission.”
In a March 30 article, “Your Daughter for a Rat,” Bell cited a One Health editorial published in The Lancet stating that “all life is equal, and of equal concern.” In response, Bell suggested that One Health aims to lower humans to the level of animals.
The same Lancet article described One Health as “a call for ecological, not merely health, equity” and called for a “subtle but quite revolutionary shift of perspective” away from “anthropocentrism”: “All life is equal, and of equal concern.”
“It looks like this is going to be the justification for moving people down to the value of animals,” Nass said in response; a sentiment shared by Boyle, who said, “One Health relates the healthcare of human beings to the healthcare of animals and thus reduces healthcare for human beings to the level of healthcare for animals.”
According to Bell, “suggesting that we have a duty as a species on this planet to look after every species equally and treat them more equally [is] becoming sort of a religion or dogma. It defies what any rational society in the history of humanity” has practiced and is “a very unusual approach and potentially very scary.”
One Health: Follow the money
The WHO has attempted to give theoretical credence to the One Health concept by developing a so-called “Theory of Change” (ToC).
Although the WHO says the ToC is designed to provide “a conceptual framework” for “organisations, agencies and initiatives working towards similar One Health goals” and a “common narrative of coherence,” the theory itself does not appear to have a clear definition.
“They want to be able to do whatever they want,” Littlejohn said. “If you define it, then you can hold them to the definition … one of the tactics is just to be really obscure and incomprehensible.”
“This is a term that is used in these circles,” Bell added. “It’s stating the obvious, that if you do a certain act, you’ll have a certain outcome. It’s a fancy way of saying that.”
Bell also referred to the “fallacy that is being pushed that humans are having increasing contact with wildlife,” supposedly leading to “this threat of viruses jumping from wildlife to humans.”
Calling it a “ludicrous claim,” Bell said that “when humans move into wildlife habitats, the wildlife don’t start living with humans. They die out.”
Noting that “it used to be very common” for people to live with farm animals, Bell added that the claim that pandemics are becoming more common due to increased contact with animals is itself “not true,” but is “used to instill fear and to try to get people to buy into this One Health, constant health emergency agenda.”
Nass said One Health proponents “don’t actually have any evidence” to support their claims, offering the example of antimicrobial resistance in bacteria found in meat consumed by humans, as a result of antibiotics administered to livestock. “That’s been the hook that One Health has been hung on,” Nass said.
However, Nass said this problem “could be solved in a heartbeat if the U.S. Food and Drug Administration or the U.S. Department of Agriculture just told farmers they can’t put antibiotics into animal feed anymore, they can only use them when an animal gets sick.”
In his recent article, Mercola suggested following the money. “Private interests wield immense power over the WHO, and a majority of the funding is ‘specified,’ meaning it’s earmarked for particular programs. The WHO cannot allocate those funds wherever they’re needed most.”
As a result, this “massively influences what the WHO does and how it does it. So, the WHO is an organization that does whatever its funders tell it to do,” naming organizations such as the Gates Foundation as prime funders of the WHO.
Bell said that supporters of One Health include “those who have been pushing the COVID agenda … and enriching themselves from it,” including “private foundations who are on the bandwagon” and “corporations who stand to gain from controlling the food chain and controlling agriculture and pharmaceuticals, et cetera.”
“It’s corporate authoritarians that have benefited themselves from public health through COVID and the certainly inappropriate COVID response,” Bell added. “And it’s the same and it’s not disconnected with the climate emergency agenda.”
One prominent financial actor closely involved with the development of the One Health agenda is the World Bank, as WHO documents indicate.
At a November 2022 OHHLEP meeting, Franck Berthe, the World Bank’s senior livestock specialist, introduced the World Bank’s Financial Intermediary Fund, which would “allow countries to borrow funds to strengthen their health system and promote the OH [One Health] approach.”
According to Nass, “the WHO and the World Bank have helped form this financing operation for the biosecurity agenda,” while Boyle told The Defender, “There is nothing humanitarian about these backers and the WHO promoting the One Health agenda.”
Both Nass and Bell said the One Health agenda is closely tied to the UN’s Sustainable Development Goals and Agenda 2030. Bell said that the One Health agenda attempts to deal with a supposed “existential threat to human health” that “must be dealt with in a centralized way, rather than giving people a choice.”
One Health closely tied to WHO pandemic treaty, IHR amendments
Experts who spoke with The Defender also emphasized the connections between the One Health concept and the pandemic treaty and IHR amendments under negotiation.
Mercola wrote that through the One Health agenda, which recognizes “a very broad range of aspects of life and the environment [that] can impact health and therefore fall under the ‘potential’ to cause harm,” the WHO “will be able to declare climate change as a health emergency and subsequently require climate lockdowns.”
Roguski, who has extensively researched the pandemic treaty and IHR amendments, said that in amendments the EU recently proposed for the pandemic treaty, the term “One Health” appears 29 times, including calling upon countries to develop and regularly update pandemic prevention plans via the One Health approach.
Referring to the need to prevent potential “pandemic situations,” the proposals also call for strengthening global public health surveillance “using a One Health approach,” which will also “address the drivers of the emergence and re-emergence of disease at the human-animal-environment interface, including but not limited to climate change, land use change, wildlife trade, desertification and antimicrobial resistance.”
The proposals also suggest the One Health approach could be used “to produce science-based evidence, and support, facilitate and/or oversee the correct, evidence-based and risk-informed implementation of infection prevention and control,” and go as far as to suggest targets on “antimicrobial consumption/use.”
Roguski told The Defender that the latest draft of the pandemic treaty refers to One Health 13 times. Such language would “be used to take over complete control of our lives,” Roguski added.
For example, one proposal states, “Each Party shall, in accordance with national law, adopt policies and strategies, supported by implementation plans, across the public and private sectors and relevant agencies, consistent with relevant tools, including, but not limited to, the International Health Regulations, and strengthen and reinforce public health functions for: (c) surveillance (including using a One Health approach).”
Other proposals include:
“The Parties commit to strengthen multi-sectoral, coordinated, interoperable and integrated One Health surveillance systems … to identify and assess the risks and emergence of pathogens and variants with pandemic potential, in order to minimize spill-over events, mutations and the risks associated with zoonotic neglected tropical and vector-borne diseases, with a view to preventing small-scale outbreaks in wildlife or domesticated animals from becoming a pandemic.
“Each Party shall … develop and implement a national One Health action plan on antimicrobial resistance that strengthens antimicrobial stewardship in the human and animal sectors, optimizes antimicrobial consumption, increases investment in, and promotes equitable and affordable access to, new medicines, diagnostic tools, vaccines and other interventions, strengthens infection prevention and control in health care settings and sanitation and biosecurity in livestock farms, and provides technical support to developing countries.”
Roguski said the phrase “One Health” doesn’t directly appear in documents related to the proposed IHR amendments, but he added the WHO “is going to try to get them both to prevail,” referring to both the treaty and IHR amendments.
Littlejohn said, the One Health approach and the proposed language in the treaty “gives them the right to surveil and potentially control every aspect of life on earth.”
Noting that the proposed treaty also calls for a “commitment to counteract ‘misinformation,’ ‘disinformation,’ and ‘false news,’” Littlejohn added, “they’re going to surveil our social media … and if any of us steps out of line by contradicting what the WHO says, then we could be censored.”
“That’s what I think is in mind with this commitment to ‘coordinated, interoperable and integrated’ One Health surveillance systems,” Littlejohn added. “I think that’s how it could end up being deployed. Ultimately, globalist entities, such as the World Economic Forum and the UN are using the WHO as their way of establishing global control.”
“The reason that health is such a good pretext is that people can become terrified,” Littlejohn added. “To the extent that their minds are paralyzed if they think they could die or get really sick, they’re willing to give up freedoms that they would not be willing to give up in other contexts.”
Roguski told The Defender :
“They made a lot of bad decisions. They gave a lot of bad advice [and] they caused a lot of harm to a lot of people. You can’t just give those people more power, authority and control without looking at what they did and going, ‘no, you should not be in charge of any of this.’”
In turn, Mercola wrote that “The globalist takeover hinges on the successful creation of a feedback loop of surveillance for virus variants, declaration of potential risk followed by lockdowns and restrictions, followed by mass vaccinating populations to ‘end’ the pandemic restrictions, followed by more surveillance and so on.”
And according to Bell, One Health “is part of a much bigger picture of finding ways to pull apart the intrinsic ideas that most societies have been built on.”
“I think that this is part of a move to undo these sorts of ideas and to replace them with a sort of religion of fear of our surroundings and denigration of other humans that can then be used by very greedy people to increase their wealth and power,” Bell said. “It’s taken over public health to a large extent.”
Michael Nevradakis, Ph.D., based in Athens, Greece, is a senior reporter for The Defender and part of the rotation of hosts for CHD.TV’s “Good Morning CHD.”
This article was originally published by The Defender — Children’s Health Defense’s News & Views Website under Creative Commons license CC BY-NC-ND 4.0. Please consider subscribing to The Defender or donating to Children’s Health Defense.
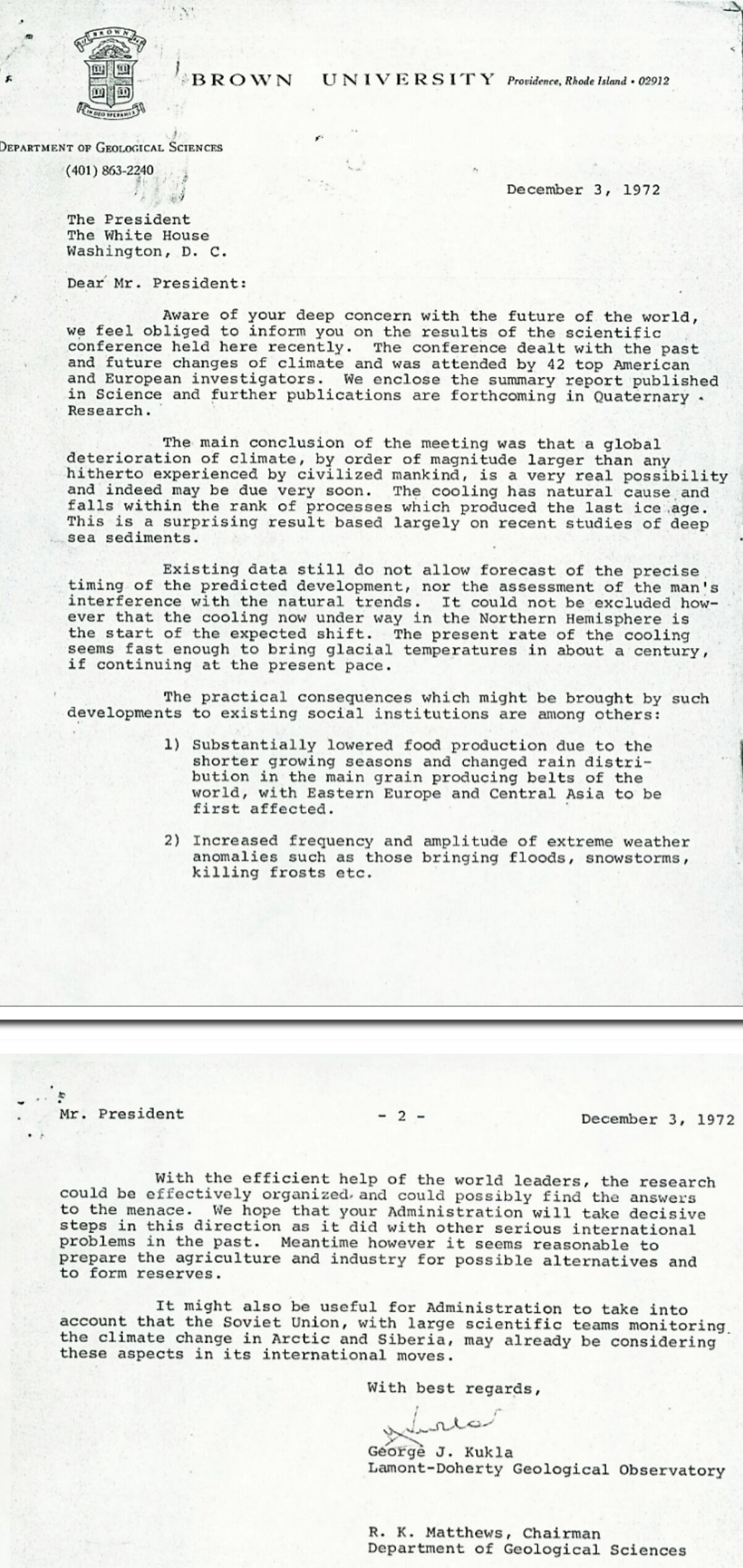
Global Cooling Alert! (1972)
By Robert Bradley Jr. | MasterResource | March 8, 2023
——————–
For various posts at MasterResource on the experts’ global cooling scare, see here.
Featured Video

Rewriting the risk? Inside the government’s vaccine safety messaging
or go to
Aletho News Archives – Video-Images
Book Review
“Davos Can Really Replace the UN”
Inside the book that maps the architecture behind global governance — from the Epstein files to the Pact for the Future
Lies are Unbekoming | April 1, 2026
On June 13, 2019, the United Nations and the World Economic Forum signed a partnership deal to “accelerate the implementation of the 2030 Agenda for Sustainable Development.” That same evening, WEF president Börge Brende — Norway’s former Foreign Minister — had dinner with Jeffrey Epstein at Epstein’s Manhattan townhouse. The Epstein files, released January 2026, contain an exchange between the two from the previous year. Epstein to Brende: “Davos can really replace the UN. C21, cyber, crypto . genetics… intl coordination.” Brende back to Epstein: “Exactly — we need a new global architecture. World Economic Forum (Davos) is uniquely positioned — public private.”
The next day, the UN General Assembly adopted the framework for restructuring global governance.
That sequence — the partnership signing, the Epstein dinner, the candid admission about replacing the UN with a public-private architecture, and then the formal adoption — opens Jacob Nordangård’s The Digital World Brain. Pages two and three. Footnoted to the UN resolution number, the Epstein files, and the General Assembly record.
I keep coming back to it because it captures what this book does that almost nothing else in the independent research space manages. I’ve followed Jacob’s work for years now and interviewed him about his research. Each book peels back another layer of the same institutional architecture, and each time I think he’s reached the limit of what can be documented, the next one goes further. Nordangård doesn’t speculate. He doesn’t editorialize much. He lays institutional actions next to each other in chronological order and lets the pattern announce itself. … continue
Blog Roll
 Aletho News
Aletho News- What’s Behind U.S./Israeli Strikes On Iranian Pistachio Factories?
- Seyed M. Marandi: U.S. Military DIVIDED? Iran’s Secret Defense EXPOSED
- How I fell foul of the BBC thought police
- The End of NATO
- 37 days of war on Iran cost US staggering $42bln, tracker shows
- Baghdad tells Asian refiners, traders to begin loading Iraqi crude amid Iranian exemption
- Under fire, Moscow and Tehran close ranks
- Iran, US receive Pakistan-mediated plan for ceasefire then final deal
- Iran submits demands for end to war as mediators scramble ahead of Trump deadline
- Iran Threatens Retaliatory Strike on Stargate AI Project in UAE
- If Americans Knew
- U.N. experts demand Israel release prominent Gaza doctor after reports of ‘severe torture’
- Israel’s Latest Genocide Is Against the Shias of Lebanon. Why Is the World Silent?
- How Eliot Cohen’s influence over U.S. war-making paved the way for Trump’s war crimes in Iran
- Israelis don’t pay for the weapons we ‘sell’ to them — US taxpayers do
- While Distancing from AIPAC, Most 2028 Democratic Hopefuls Are Still Embracing Israel
- A brief history of the Israeli nuclear program, the open secret at the heart of the Iran war
- Israeli Settlers Killed a Palestinian Farmer on His Own Land, in Front of His Father. Yes, Again
- The US-Israeli War on Science is an Assault on our Future
- 100+ International Law Experts Say US Strikes on Iran Violate UN Charter, Could Be War Crimes
- ‘Vile, Horrifying, Evil’: Trump Threatens to Bomb Nation of 90 Million People ‘Back to the Stone Ages’
- No Tricks Zone
- An Inconvenient Tree: Uncovered In Alps… Europe Much Warmer Than Today 6000 Years Ago
- New Study Reports A 60% Slowdown In Greenland’s Ice Loss Rate In The Last Decade
- Low Intensity Tornado Wrecks Major Solar Farm, Creating A Potential Toxic Dump
- New Study Finds Warming Saves Lives…Cold Temperatures 12 Times More Deadly Than Excess Heat
- German Science Blog Accuses PIK Climate Institute Of Hallucinating Climate Tipping Points
- Devastating Assessment Of Comirnaty Vaccine By Former Senior Pfizer Europe Toxicologist
- New Study: CO2 Is ‘Effectively Negligible’ As An Explanatory Climate Change Factor Since 2000
- Former Pfizer Toxicologist Dr. Helmut Sterz Tells Bundestag Hearing Pfizer Vaccine Should Have Never Been Approved
- Energy Expert: Germany’s Nuclear Phaseout Was A “500 Billion Euro Mistake”
- New Research: South Australia’s Mid-Holocene Sea Surface Temperatures Were 4°C Warmer Than Today
