One Health: A Plan to ‘Surveil and Control Every Aspect of Life on Earth’?
This is part two of a two-part series on the One Health initiative. Read part one here.
By Michael Nevradakis, Ph.D. | The Defender | May 8, 2023
The World Health Organization (WHO) defines “One Health,” as “an integrated, unifying approach that aims to sustainably balance and optimize the health of people, animals and ecosystems,” as they are “closely linked and interdependent” — a concept that on the surface appears to promote noble goals interlinking human and environmental health.
However, some scientists and medical experts are concerned about One Health’s vague goals. Arguing that the concept has been “hijacked,” they question the intent of those involved with the development and global rollout of the concept — including the WHO, the Centers for Disease Control and Prevention (CDC) and the World Bank.
Experts who spoke with The Defender also raised questions about other aspects of the One Health concept, including a biosecurity agenda, a global surveillance system, vaccine passports and restrictions on human behavior.
While these goals are underpinned by a vaguely defined “Theory of Change,” experts told The Defender that major financial interests are at the heart of the One Health agenda, which appears to be closely linked to climate change and sustainable development initiatives promoted by the same global organizations.
One Health objectives include a ‘global takeover of everything’
In a May 1 article, Dr. Joseph Mercola connected the One Health concept, as promoted by global organizations, to the policies and restrictions pursued in response to COVID-19, describing it as an attempted “global takeover of everything.”
Mercola tied the One Health concept to key entities that have supported gain-of-function research. According to Mercola:
“Interestingly, the term ‘One Health,’ which was formally adopted by the WHO and the G20 health ministers in 2017, was first coined by the executive vice president of the EcoHealth Alliance, the same firm that appears to have had a hand in the creation of SARS-CoV-2.”
During the 2019 lecture “Can One Health Help Prevent the Next Pandemic?” EcoHealth Alliance President Peter Daszak, Ph.D., commissioner in The Lancet’s One Health Commission, said “emerging infectious diseases” are “a growing global threat.”
He also argued that many of these emerging diseases are “zoonotic — spread from animals to humans.”
Francis Boyle, J.D., Ph.D., professor of international law at the University of Illinois and a bioweapons expert who drafted the Biological Weapons Anti-Terrorism Act of 1989, questioned this narrative, telling The Defender :
“All these ‘emerging infectious diseases’ are emerging out of their offensive biological warfare weapons programs conducted in their BSL4 [biosecurity level 4] and BSL3 laboratories.
“If you look at the people on the WHO advisory committee dealing with ‘emerging infectious diseases,’ that’s exactly what they are doing — ‘emerging’ them from their labs.”
One example is that of Marion Koopmans, DVM, Ph.D., director of the WHO Collaborating Centre for emerging infectious diseases at Erasmus Medical Centre in the Netherlands and member of the WHO’s One Health High-Level Expert Panel (OHHLEP).
According to Boyle, “Erasmus is where this offensive Nazi biowarfare gain-of-function death science dirty work first became notorious under Fouchier, [who] started the entire controversy over his gain-of-function work there.”
Boyle was referring to Ron Fouchier, Ph.D., who also is deputy head of Erasmus’ Viroscience Department and who, according to Science, “alarmed the world” in 2011, after he and other researchers “separately modified the deadly avian H5N1 influenza virus so that it spread between ferrets” — an early example of gain-of-function research.
Dr. Meryl Nass, an internist and biological warfare epidemiologist who is a member of the Children’s Health Defense scientific advisory committee, said such objectives are kept deliberately vague. She referred to a CDC document that stated:
“Successful public health interventions require the cooperation of human, animal, and environmental health partners … Other relevant players in a One Health approach could include law enforcement, policymakers, agriculture, communities, and even pet owners.
“By promoting collaboration across all sectors, a One Health approach can achieve the best health outcomes for people, animals, and plants in a shared environment.”
Nass wrote on her blog, “I anticipate that One Health will be used to impose changes in the way humans and animals interact … most likely based on the needs of the WEF [World Economic Forum]/elites and not the needs of the people or the animals that will be affected.”
Reggie Littlejohn, founder and president of Women’s Rights Without Frontiers and co-chair of the Stop Vaccine Passports Task Force, told The Defender, “It’s not clear that One Health is prioritizing human health.”
Highlighting the “vague” language employed by the global organizations promoting One Health, Littlejohn said that one goal may be to “govern farm animal health in addition to human health,” through which “they could do things like forcing vaccines on livestock.”
One Health means ‘surveilling everything’
The experts who spoke with The Defender expressed concerns over the biosecurity agenda that is associated with the stated objectives of One Health.
According to Nass, this reflects how the WHO “has been changing into a biosecurity agency,” adding that “the justification, apparently, for the WHO’s director-general to take over jurisdiction of healthcare during pandemics, but also potentially ecosystems, animals and plants, is through One Health.”
Nass noted that One Health “is mentioned several times in the National Defense [Authorization] Act for Fiscal Year 2023” (NDAA), which includes 18 pages on “pandemic preparedness” and a formal definition of the “One Health approach” on page 952 of the act.
Independent journalist and researcher James Roguski also highlighted the prominent placement of One Health in the NDAA and noted that, by formally defining the concept within the act, it is now part of the Code of Federal Regulations.
However, Roguski said the NDAA goes even further:
“The U.S. has pledged a billion dollars a year to the World Bank Pandemic Fund in support of the global health security agenda. The WHO is one of 14 intermediaries who will receive and redistribute some of that billion dollars.
“Basically, it’s capitalism, it’s corruption, it’s an abomination from a health perspective. Let’s just throw money at pharmaceutical companies, build out the infrastructure in these nations and, if you’re making tons of products locally, you’re going to be able to convince the local government to stick them in people’s arms or shove it down their throat.
“And none of it really has shown to be of any health benefit. It’s damage to people’s health.”
Associated with the promotion of a global biosecurity agenda is the development of a global surveillance infrastructure that would purportedly protect human and animal health and the environment. An Oct. 3, 2022, WHO document states:
“The emergence of the SARS-CoV-2 virus that caused COVID-19 has underlined the need to strengthen the One Health approach, with a greater emphasis on connections to animal health and the environment …
“… It uses the close, interdependent links among these fields to create new surveillance and disease control methods. …
“We now have an unprecedented opportunity to strengthen collaboration and policies across these many areas and reduce the risk of future pandemics and epidemics while also addressing the ongoing burden of endemic and non-communicable diseases
“Surveillance that monitors risks and helps identify patterns across these many areas is needed.”
Remarking on this, Littlejohn said One Health’s proponents talk about “interoperable, integrated surveillance systems.” She told The Defender :
“I believe … these surveillance systems of people, animals, plants, and the environment are going to be coordinated by some kind of a global surveillance system that is interoperable globally and integrated.
“Whoever’s running this show, the WHO, the Chinese Communist Party … the Bill and Melinda Gates Foundation, who are the people who really appear to be running the show at the WHO, are going to be able to tap into and see all of our private information. Not just us, but animals and plants.”
Dr. David Bell, a public health physician and biotech consultant and former director of global health technologies at Intellectual Ventures Global Good Fund, told The Defender that what global organizations intend is “surveilling everything.” He said:
“It means surveilling everything, surveilling the climate for possible threats, surveilling animal population, surveilling wildlife, surveilling the soil to see if there’s new traces of virus or bacteria in river systems, et cetera.
“This allows you to ‘discover’ what we already know is nature, and then turn nature into a potential threat or into a threat. The more surveillance you have and the wider it is, the more inevitable ‘threats’ you’ll find … because you can make an argument that almost any new variant virus is a ‘threat.’
“It will allow them to keep a constant kind of fear which then allows you to introduce authoritarian controls such as central bank digital currencies and digital passports … that allow them to monetize the human population more effectively.”
Nass noted that global actors such as the WHO “talk about sharing of specimens during a pandemic … so they can try to make vaccines too. However, they don’t talk about performing surveillance on human beings. But what they did say, which let the cat out of the bag, is that they would want to get informed consent from countries for sharing of genomic data, rather than from individuals.”
Part of this surveillance infrastructure also would include vaccine passports, which figure prominently in the pandemic treaty and amendments to the International Health Regulations (IHR) currently under negotiation at the WHO.
According to Littlejohn:
“I believe that they laid the infrastructure during the COVID-19 crisis, and we’re having a little bit of a ‘break’ here between pandemics, but that structure, that infrastructure is going to snap shut with the next pandemic if we don’t stop it. That structure has to do with vaccine passports.
“It could be called a ‘smart health card’ or ‘digital health ID,’ or even a mandatory digital driver’s license can serve as the platform for a China-style social credit system. And there’s a new bill in front of the Senate right now … the Improving Digital Identity Act of 2023 … It’s a mandatory national ID that’s going to be interoperable, coordinated, integrated and can serve as the same platform as China’s social credit system … to surveil us.”
Restrictions on human behavior could lower humans to the level of animals
The WHO’s Oct. 3, 2022, document also claimed that “Some 60% of emerging infectious diseases that are reported globally come from animals, both wild and domestic,” adding that “human activities and stressed ecosystems have created new opportunities for diseases to emerge and spread.”
Such stressors “include animal trade, agriculture, livestock farming, urbanization, extractive industries, climate change, habitat fragmentation and encroachment into wild areas,” according to the WHO.
“To the extent that carbon emissions due to transportation within cities would contribute to climate change, then the ‘15-minute city’ would be a way of addressing that,” Littlejohn said. “The danger is that they will enforce it by having surveillance cameras everywhere to make sure you don’t go outside of your district without permission.”
In a March 30 article, “Your Daughter for a Rat,” Bell cited a One Health editorial published in The Lancet stating that “all life is equal, and of equal concern.” In response, Bell suggested that One Health aims to lower humans to the level of animals.
The same Lancet article described One Health as “a call for ecological, not merely health, equity” and called for a “subtle but quite revolutionary shift of perspective” away from “anthropocentrism”: “All life is equal, and of equal concern.”
“It looks like this is going to be the justification for moving people down to the value of animals,” Nass said in response; a sentiment shared by Boyle, who said, “One Health relates the healthcare of human beings to the healthcare of animals and thus reduces healthcare for human beings to the level of healthcare for animals.”
According to Bell, “suggesting that we have a duty as a species on this planet to look after every species equally and treat them more equally [is] becoming sort of a religion or dogma. It defies what any rational society in the history of humanity” has practiced and is “a very unusual approach and potentially very scary.”
One Health: Follow the money
The WHO has attempted to give theoretical credence to the One Health concept by developing a so-called “Theory of Change” (ToC).
Although the WHO says the ToC is designed to provide “a conceptual framework” for “organisations, agencies and initiatives working towards similar One Health goals” and a “common narrative of coherence,” the theory itself does not appear to have a clear definition.
“They want to be able to do whatever they want,” Littlejohn said. “If you define it, then you can hold them to the definition … one of the tactics is just to be really obscure and incomprehensible.”
“This is a term that is used in these circles,” Bell added. “It’s stating the obvious, that if you do a certain act, you’ll have a certain outcome. It’s a fancy way of saying that.”
Bell also referred to the “fallacy that is being pushed that humans are having increasing contact with wildlife,” supposedly leading to “this threat of viruses jumping from wildlife to humans.”
Calling it a “ludicrous claim,” Bell said that “when humans move into wildlife habitats, the wildlife don’t start living with humans. They die out.”
Noting that “it used to be very common” for people to live with farm animals, Bell added that the claim that pandemics are becoming more common due to increased contact with animals is itself “not true,” but is “used to instill fear and to try to get people to buy into this One Health, constant health emergency agenda.”
Nass said One Health proponents “don’t actually have any evidence” to support their claims, offering the example of antimicrobial resistance in bacteria found in meat consumed by humans, as a result of antibiotics administered to livestock. “That’s been the hook that One Health has been hung on,” Nass said.
However, Nass said this problem “could be solved in a heartbeat if the U.S. Food and Drug Administration or the U.S. Department of Agriculture just told farmers they can’t put antibiotics into animal feed anymore, they can only use them when an animal gets sick.”
In his recent article, Mercola suggested following the money. “Private interests wield immense power over the WHO, and a majority of the funding is ‘specified,’ meaning it’s earmarked for particular programs. The WHO cannot allocate those funds wherever they’re needed most.”
As a result, this “massively influences what the WHO does and how it does it. So, the WHO is an organization that does whatever its funders tell it to do,” naming organizations such as the Gates Foundation as prime funders of the WHO.
Bell said that supporters of One Health include “those who have been pushing the COVID agenda … and enriching themselves from it,” including “private foundations who are on the bandwagon” and “corporations who stand to gain from controlling the food chain and controlling agriculture and pharmaceuticals, et cetera.”
“It’s corporate authoritarians that have benefited themselves from public health through COVID and the certainly inappropriate COVID response,” Bell added. “And it’s the same and it’s not disconnected with the climate emergency agenda.”
One prominent financial actor closely involved with the development of the One Health agenda is the World Bank, as WHO documents indicate.
At a November 2022 OHHLEP meeting, Franck Berthe, the World Bank’s senior livestock specialist, introduced the World Bank’s Financial Intermediary Fund, which would “allow countries to borrow funds to strengthen their health system and promote the OH [One Health] approach.”
According to Nass, “the WHO and the World Bank have helped form this financing operation for the biosecurity agenda,” while Boyle told The Defender, “There is nothing humanitarian about these backers and the WHO promoting the One Health agenda.”
Both Nass and Bell said the One Health agenda is closely tied to the UN’s Sustainable Development Goals and Agenda 2030. Bell said that the One Health agenda attempts to deal with a supposed “existential threat to human health” that “must be dealt with in a centralized way, rather than giving people a choice.”
One Health closely tied to WHO pandemic treaty, IHR amendments
Experts who spoke with The Defender also emphasized the connections between the One Health concept and the pandemic treaty and IHR amendments under negotiation.
Mercola wrote that through the One Health agenda, which recognizes “a very broad range of aspects of life and the environment [that] can impact health and therefore fall under the ‘potential’ to cause harm,” the WHO “will be able to declare climate change as a health emergency and subsequently require climate lockdowns.”
Roguski, who has extensively researched the pandemic treaty and IHR amendments, said that in amendments the EU recently proposed for the pandemic treaty, the term “One Health” appears 29 times, including calling upon countries to develop and regularly update pandemic prevention plans via the One Health approach.
Referring to the need to prevent potential “pandemic situations,” the proposals also call for strengthening global public health surveillance “using a One Health approach,” which will also “address the drivers of the emergence and re-emergence of disease at the human-animal-environment interface, including but not limited to climate change, land use change, wildlife trade, desertification and antimicrobial resistance.”
The proposals also suggest the One Health approach could be used “to produce science-based evidence, and support, facilitate and/or oversee the correct, evidence-based and risk-informed implementation of infection prevention and control,” and go as far as to suggest targets on “antimicrobial consumption/use.”
Roguski told The Defender that the latest draft of the pandemic treaty refers to One Health 13 times. Such language would “be used to take over complete control of our lives,” Roguski added.
For example, one proposal states, “Each Party shall, in accordance with national law, adopt policies and strategies, supported by implementation plans, across the public and private sectors and relevant agencies, consistent with relevant tools, including, but not limited to, the International Health Regulations, and strengthen and reinforce public health functions for: (c) surveillance (including using a One Health approach).”
Other proposals include:
“The Parties commit to strengthen multi-sectoral, coordinated, interoperable and integrated One Health surveillance systems … to identify and assess the risks and emergence of pathogens and variants with pandemic potential, in order to minimize spill-over events, mutations and the risks associated with zoonotic neglected tropical and vector-borne diseases, with a view to preventing small-scale outbreaks in wildlife or domesticated animals from becoming a pandemic.
“Each Party shall … develop and implement a national One Health action plan on antimicrobial resistance that strengthens antimicrobial stewardship in the human and animal sectors, optimizes antimicrobial consumption, increases investment in, and promotes equitable and affordable access to, new medicines, diagnostic tools, vaccines and other interventions, strengthens infection prevention and control in health care settings and sanitation and biosecurity in livestock farms, and provides technical support to developing countries.”
Roguski said the phrase “One Health” doesn’t directly appear in documents related to the proposed IHR amendments, but he added the WHO “is going to try to get them both to prevail,” referring to both the treaty and IHR amendments.
Littlejohn said, the One Health approach and the proposed language in the treaty “gives them the right to surveil and potentially control every aspect of life on earth.”
Noting that the proposed treaty also calls for a “commitment to counteract ‘misinformation,’ ‘disinformation,’ and ‘false news,’” Littlejohn added, “they’re going to surveil our social media … and if any of us steps out of line by contradicting what the WHO says, then we could be censored.”
“That’s what I think is in mind with this commitment to ‘coordinated, interoperable and integrated’ One Health surveillance systems,” Littlejohn added. “I think that’s how it could end up being deployed. Ultimately, globalist entities, such as the World Economic Forum and the UN are using the WHO as their way of establishing global control.”
“The reason that health is such a good pretext is that people can become terrified,” Littlejohn added. “To the extent that their minds are paralyzed if they think they could die or get really sick, they’re willing to give up freedoms that they would not be willing to give up in other contexts.”
Roguski told The Defender :
“They made a lot of bad decisions. They gave a lot of bad advice [and] they caused a lot of harm to a lot of people. You can’t just give those people more power, authority and control without looking at what they did and going, ‘no, you should not be in charge of any of this.’”
In turn, Mercola wrote that “The globalist takeover hinges on the successful creation of a feedback loop of surveillance for virus variants, declaration of potential risk followed by lockdowns and restrictions, followed by mass vaccinating populations to ‘end’ the pandemic restrictions, followed by more surveillance and so on.”
And according to Bell, One Health “is part of a much bigger picture of finding ways to pull apart the intrinsic ideas that most societies have been built on.”
“I think that this is part of a move to undo these sorts of ideas and to replace them with a sort of religion of fear of our surroundings and denigration of other humans that can then be used by very greedy people to increase their wealth and power,” Bell said. “It’s taken over public health to a large extent.”
Michael Nevradakis, Ph.D., based in Athens, Greece, is a senior reporter for The Defender and part of the rotation of hosts for CHD.TV’s “Good Morning CHD.”
This article was originally published by The Defender — Children’s Health Defense’s News & Views Website under Creative Commons license CC BY-NC-ND 4.0. Please consider subscribing to The Defender or donating to Children’s Health Defense.
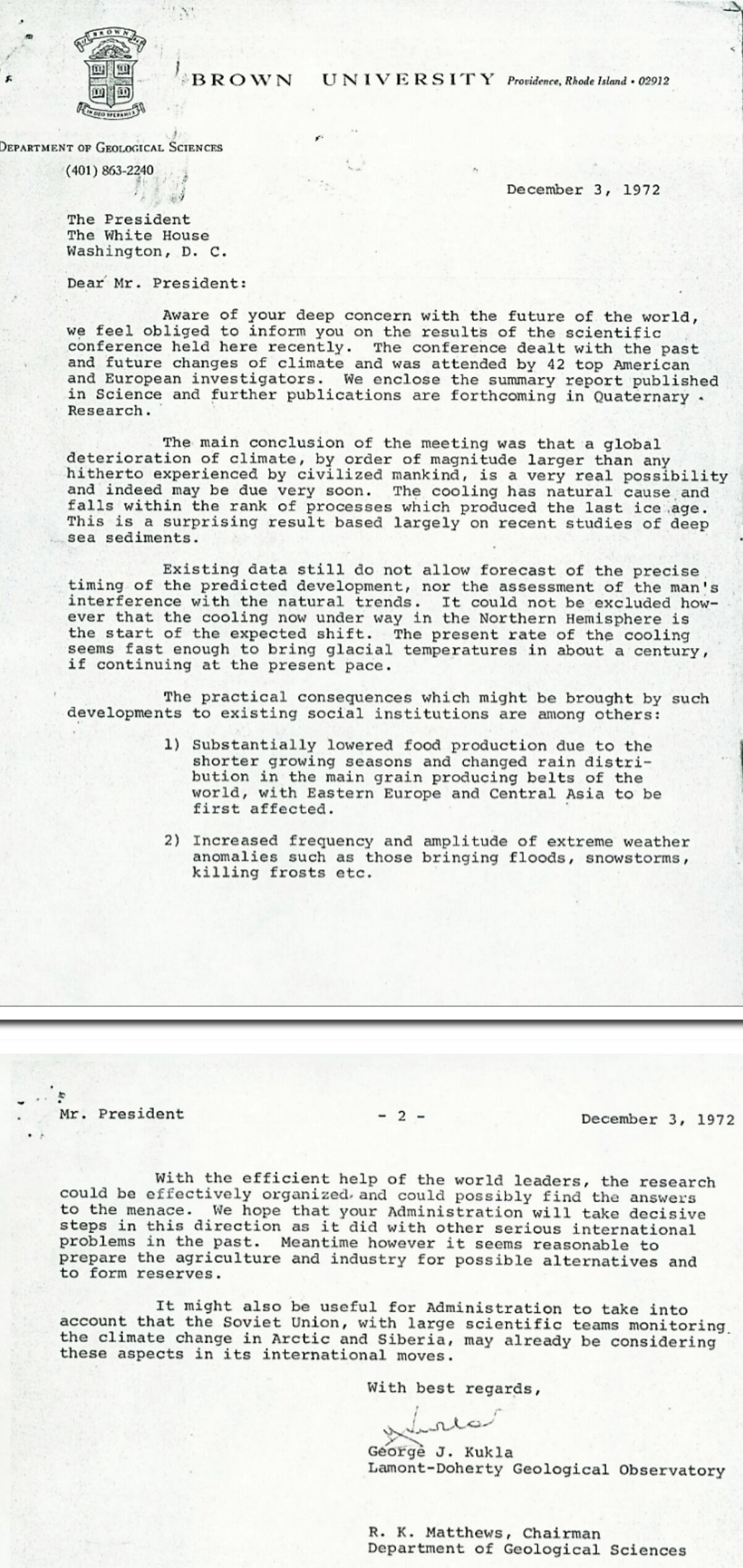
Global Cooling Alert! (1972)
By Robert Bradley Jr. | MasterResource | March 8, 2023
——————–
For various posts at MasterResource on the experts’ global cooling scare, see here.
Facebook Censoring The Inconvenient Truth About Antarctic Temperatures
By Paul Homewood | Not A Lot Of People Know That | May 6, 2023
This post came up on my Facebook today:

https://www.facebook.com/william.dunn.1238/posts/pfbid036joG1b82T95G59BVS3uTQT1wYL26XMEBFVyMWto8CdzfBhTWBQ7YecGyr9GREWxol
When you click on SEE WHY, this comes up:

And this is the story the Facebook censors don’t want you to see:

Quite why Facebook would want to rely on the USA Today for its source of science is a mystery. Perhaps they should have actually checked what real scientists are saying:

Abstract
The Antarctic continent has not warmed in the last seven decades, despite a monotonic increase in the atmospheric concentration of greenhouse gases.
In this paper, we investigate whether the high orography of the Antarctic ice sheet (AIS) has helped delay warming over the continent. To that end, we contrast the Antarctic climate response to CO2-doubling with present-day orography to the response with a flattened AIS. To corroborate our findings, we perform this exercise with two different climate models. We find that, with a flattened AIS, CO2-doubling induces more latent heat transport toward the Antarctic continent, greater moisture convergence over the continent and, as a result, more surface-amplified condensational heating. Greater moisture convergence over the continent is made possible by flattening of moist isentropic surfaces, which decreases humidity gradients along the trajectories on which extratropical poleward moisture transport predominantly occurs, thereby enabling more moisture to reach the pole. Furthermore, the polar meridional cell disappears when the AIS is flattened, permitting greater CO2-forced warm temperature advection toward the Antarctic continent. Our results suggest that the high elevation of the present AIS plays a significant role in decreasing the susceptibility of the Antarctic continent to CO2-forced warming.

https://www.nature.com/articles/s41612-020-00143-w
I’ll post this on Facebook and see how long it takes for the censors to strike!
WHO Denies Pandemic Treaty Will Reduce Sovereignty of States – But it’s Pure Propaganda
BY DR DAVID BELL | THE DAILY SCEPTIC | MAY 6, 2023
The Director General of the World Health Organisation (WHO) reassures us that the WHO’s ‘pandemic accord’ (or ‘treaty’) won’t reduce the sovereignty of Member States. The WHO trusts that these words will serve as a distraction from reality. Those driving the perpetual health emergency agenda are planning to give WHO more power, and states less. This will happen whenever WHO designates a ‘Public Health Emergency of International Concern’ (PHEIC), or considers we may be at risk of one.
The WHO’s proposed treaty, taken together with its ‘synergistic’ amendments to the International Health Regulations (IHR), aim to undo centuries of democratic reform that based sovereignty with individuals, and by extension their state. The discomfort of facing this truth and the complexities it raises is providing the cover needed to push these changes through. This is how democracy, and freedom, wither and die.
Why it’s hard to acknowledge reality
Our society in the West is built on trust and a feeling of superiority – we built the institutions that run the world and they, and we, are good. We consider ourselves humanitarians, the public health advocates, the unifiers, and anti-fascist freedom-lovers. We consider our system is better than the alternatives – we are ‘progressive’.
It takes quite a step for comfortable, middle-income, Left-leaning professionals to believe that the institutions and philanthropic organisations we have admired all our lives might now be pillaging us. Our society relies on having ‘trusted sources’, the WHO being one of them. Among others are our major media organisations. If our trusted sources told us we were being misled and pillaged, we would accept this. But they are telling us these claims are false, and that all is well. The WHO’s Director General himself assures us of this. Anyone who thinks rich corporate and private sponsors of WHO and other health institutions are self-interested, that they might mislead and exploit others for their own benefit, is a conspiracy theorist.
We are all capable of believing the rich and powerful of past ages would exploit the masses, but somehow this is hard to believe in the present. For proof of their benevolence, we rely on the word of their own publicity departments and the media they support. Somehow, malfeasance on a grand scale is always a figment of history, and now we are smarter and enlightened.
Over recent decades we have watched individuals accumulate wealth equivalent to medium-sized countries. They meet our elected leaders behind closed doors at Davos. We then applaud the largesse they bestow on the less fortunate, and pretend all this is fine. We watch as corporations expand across national borders, seemingly above the laws that apply to ordinary citizens. We allowed their ‘public-private partnerships’ to turn international institutions into purveyors of their commodities. We ignored this descent because their publicity departments told us to, becoming apologists for obvious authoritarians because we want to believe they are somehow doing a ‘greater good’.
Whilst a schoolchild might see through this facade to the conflicted greed beyond, it is much harder for those with years of political baggage, a peer network, reputation and career to admit they have been duped. The behavioural psychologists that our governments and institutions now employ understand this. Their job is to keep us believing the trusted sources they sponsor. Our challenge is to put reality above right-think.
The remaking of WHO
When the WHO was set up in 1946 to help coordinate responses to major health issues, the world was emerging from the last great bout of fascism and colonialism. Both these societal models were sold on the basis of centralising power for a greater good. Those who considered themselves superior would run the world for those less worthy. The WHO once claimed to follow a different line.
Since the early 2000s WHO’s activities have been increasingly dictated by ‘specified funding’. Its funders, increasingly including private and corporate interest, tell it how to use the money they give. Private direction is fine for private organisations promoting their investors’ wares, but it is obviously a non-starter for an organisation seeking to mandate medicines, close borders and confine people. Anyone with a basic understanding of history and human nature will recognise this. But these powers are exactly what the amendments to the International Health Regulations and the new treaty intend.
Rather than consider alternate approaches, WHO is seeking censorship of opinions not fitting its narrative, publicly denigrating and demeaning those who question its policies. These are not the actions of an organisation representing ‘we the people’, or confident in its ability to justify its actions. They are the trappings we have always associated with intellectual weakness and fascism.
WHO’s impact on population health
In its 2019 pandemic influenza recommendations, WHO stated that “not in any circumstances” should contact tracing, border closures, entry or exit screening or quarantine of exposed individuals be undertaken in an established pandemic. It wrote this because such measures would cause more harm than good, and disproportionately harm poorer people. In 2020, in conjunction with private and national sponsors, it supported the largest wealth shift in history from low to high income by promoting these same measures.
In abandoning its principles, WHO abandoned millions of girls to nightly rape through child marriage, increased teenage pregnancies and child mortality, reduced childhood education, and grew poverty and malnutrition. Despite most of these people being too young to be troubled by Covid and already having immunity, they promoted billions of dollars of mass vaccination whilst traditional priorities such as malaria, tuberculosis and HIV/AIDS deteriorate. Western media have met this with silence or empty rhetoric. Saving lives does not turn a profit, but selling commodities does. The WHO’s sponsors are doing what they need for their investors, whilst WHO is doing what it needs to keep their money flowing.
The new powers of WHO
The IHR amendments will reduce the sovereignty of any WHO Member State that fails to actively reject them, giving a single person (the Director General) direct influence over health policy and the freedom of its citizens is indisputable. It is what the document says. Countries are required to “undertake” to follow the WHO’s “recommendations”, which are no longer simply suggestions or advice. Whilst the WHO does not have a police force, the World Bank and IMF are on board, and control much of your money supply. The U.S. Congress passed a bill last year recognising that the U.S. Government should address countries that do not comply with the IHR. We are not witnessing toothless threats; most countries, and their people, will have little choice.
The real power of the WHO’s proposals is in their application for any health-related matter they proclaim to be a threat. The proposed amendments state this explicitly, whilst the ‘Treaty’ expands the scope to ‘One-Health‘, a hijacked public health concept that can mean anything perceived to be affecting human physical, mental or social well-being. Inclement weather, crop failures or the promulgation of ideas that cause people stress – everyday things that humans have always coped with, now become reasons to confine people and impose solutions dictated by others.
In essence, those sponsoring WHO are manufacturing crises of their own desiring, and are set to get wealthier from other’s misery, as they did during Covid. This under the guise of ‘keeping us safe’. As WHO implausibly insists, “no one is safe until all are safe”, so removal of human rights must be broad and prolonged. Behavioural psychology is there to ensure that we comply.
Facing the future
We are building a future in which compliance with authoritarian dictates will win the return of stolen freedoms, whilst censorship will suppress dissent. People who wish to see evidence, who remember history or insist on informed consent will be designated, in WHO parlance, far-Right mass killers. We have already entered this world. Public figures who claim otherwise are presumably not paying attention, or have other motivations.
We can meekly accept this new disease-obsessed world, some may even embrace the salaries and careers it bestows. Or we can join those fighting for the simple right of individuals to determine their own future. At the very least, we can acknowledge the reality around us.
Dr. David Bell is a clinical and public health physician with a PhD in population health and background in internal medicine, modelling and epidemiology of infectious disease. Previously, he was Programme Head for Malaria and Acute Febrile Disease at FIND in Geneva, and coordinating malaria diagnostics strategy with the World Health Organisation. He is a member of the Executive Committee of PANDA.
Unrepentant Corona arch-villain Christian Drosten re-emerges to give the vaccines credit for ending the pandemic
Insists that lockdowns and school closures remain policy options in the future

Virus-understander-in-chief Christian Drosten posing as a scrappy compassionate avatar of The Science, rather than the conniving and perpetually wrong loser that he is.
eugyppius: a plague chronicle | May 6, 2023
That eternal turd who will not flush, Christian Drosten, has resurfaced with an odious media interview, demanding that the vaccines receive credit for ending the pandemic and that oppressive non-pharmaceutical interventions like lockdowns and school closures remain on the table for future pandemics.
From Tagesspiegel :
The measures taken by the federal and state governments in the Corona pandemic proved highly controversial and triggered fierce debates. The Berlin Charité virologist Christian Drosten, among the advocates of harsh restrictions, has now warned against drawing the wrong conclusions. The “fundamental, ideological exclusion of lockdowns and school closures” is foolhardy, Drosten told the newspapers of the Funke Mediengruppe.
“Not all pathogens have the same characteristics. A virus could surface that is especially dangerous for children, for example, or that triggers insidious sequelae despite a harmless initial infection.”
“The school closures in 2020 and 2021 were a mistake, but please don’t take away our power to close schools again in the future! The next virus might really be dangerous to children! We don’t always cry wolf, except when we do!”
Infections such like mumps and measles have caused brain inflammation, diabetes or infertility, the director of the Institute of Virology added. “If such a virus developed into a highly transmissible pandemic pathogen, politicians would inevitably have to take measures. You can’t categorically rule out things like lockdowns and school closures, that’s neither realistic nor responsible.”
Yes, you can categorically rule out lockdowns and school closures. We literally never did any of this before at this scale or for this duration in response to any virus, nor were lockdowns or other invasive measures ever even contemplated until the Chinese gave you guys a bunch of evil ideas three years ago. What’s more, all of your interventions were utter, abject failures; they did nothing.
Drosten also criticised the public debate on Covid vaccinations, which “is often still destructive.” The fact that further Covid vaccinations for children and many adults are now no longer recommended “does not prove that vaccines have always been unnecessary,” the Charité professor emphasised.
“Rather, with the help of vaccinations, we have mitigated the impact of infections and developed a high level of immunity in the population. This is the only reason that the vaccine recommendations could now be changed.”
Had we vaccinated not a single soul, we’d have identical levels of immunity in the population right now from Omicron. We also wouldn’t have all those awkward vaccine injury headlines.
In case you’re not yet angry enough, though, it gets worse:
The director of the Institute for International Health at Charité, Beate Kampmann, warned against vaccine scepticism. “Vaccination is not only about the well-being of the individual, but also about the health of society as a whole, that is public health, and that also means solidarity,” she told the newspapers.
“Sometimes people forget that they contribute to the protection of everyone with their personal decision. That was true for Corona, but it’s also true for measles, for example.”
Why are these assholes always lying, I want to know. The vaccines were not intended to stop transmission, the trials weren’t designed to show whether they would stop transmission, and we’ve known beyond all doubt since the summer of 2021 that they don’t stop transmission. Nobody who was vaccinated against Corona contributed to anybody else’s health at all, this is all just a straight-up untruth.
The pandemicists aren’t going away. They have amassed a great toolkit of new powers, and they will be slinking around for decades waiting for the next opportunity to try them out all over again. Now that the virus hysteria has boiled off and some minimal standards of rationality have returned to the discussion, it should be a priority to discredit every last one of these virus pests, Corona astrologers, modellers, and panic mongerers, now and for all time. Otherwise we’re at great risk for getting the same thing all over again.
How to fight for Covid truth

By Guy Hatchard | TCW Defending Freedom | May 6, 2023
The writer is in New Zealand.
Every day brings more news of extreme efforts to promote biotech vaccines and cancel those asking questions.
For example Dr Mark Tykocinski, an immunologist with a spotless academic record who is president of Thomas Jefferson University in Philadelphia may be about to lose his job. His sole mistake appears to be liking tweets by former New York Times journalist Alex Berenson who questions vaccine safety.
British MP Andrew Bridgen has been expelled from the Conservative Party. According to Bridgen, a senior UK politician has privately admitted to him that he may well be right about Covid vaccine harms, but said the government is expecting to suppress public information about Covid vaccine adverse effects for the next 20 years, citing ‘lack of political appetite’ for a public disclosure.
Statistician Professor Norman Fenton was locked out of his Twitter account following a complaint that he had broken German law by claiming Covid data manipulation was creating the appearance of vaccine efficacy, when in fact there was none. The German government is the main sponsor of BioNTech, the co-creator of the Pfizer mRNA Covid vaccine. Fortunately the complaint was not upheld and Fenton was reinstated.
Te Whatu Ora (Health New Zealand) has announced that from May 1, pregnant people (!) aged 16 to 29 years can now get an additional Covid-19 booster. They don’t seem to have noticed that stillbirths and miscarriages rose following the Covid vaccine rollout, or the absence of any data to confirm ‘safety’ assurances for pregnant women – quite the reverse, in fact.(See this article.) Is it possible that the NZ government have a lot of boosters left over after a poor response to their latest bivalent vaccine campaign and are now trying to offload them via deceptive advertising to mothers who naturally want to do the best for their child?
Highly vaccinated Portugal has seen a 73 per cent rise in emergency callouts for heart attacks. This mirrors the 83 per cent rise in heart attack hospitalisation in Wellington, NZ.
The continuing attacks from the media and vaccine advocates mean that some people must be seriously worried that the scientific data about vaccine harms is beginning to resonate with a wider audience. We are winning the argument.
Last week I reported correspondence from our Minister of Statistics Dr Deborah Russell MP in which she downplayed the significance of rising excess deaths in New Zealand. This appeared to be the result of misinformed policy rather than real statistics. Does the New Zealand government, in line with the UK, wish to hide Covid vaccine adverse effect statistics from the public until it becomes a matter of distant history? You tell me.
Should we be protesting on the streets?
In fact both the vaccinated and unvaccinated have been injured by government policy and experimental biotechnology. Even the pro-vaccine, pro-zoonotic origin NY Times has conceded that evidence is mounting that Covid came from a lab leak. We have a common cause.
It would certainly suit those who wish the pandemic gravy train and the biotech boom to continue, if the population were to remain polarised and the adverse effects hidden. At this time, it is my belief that launching ad hominem attacks, participating in lawful protests or expressing violent sentiments (never a good idea) will simply play into the hands of those from the media, corporates, medical professions and governments who are hoping that public concern can continue to be managed, marginalised and cancelled.
But this doesn’t mean remaining silent, we should be raising our voices and using our pens. I do believe we should always talk rationally and factually about issues that matter. This is an election year in New Zealand, when there is a higher chance of being heard. We can talk to candidates and demand answers, or even become candidates. In an election year, politicians know that all votes will matter. We can raise a voice of reasoned intelligence, express ourselves calmly, cite research, and send letters to our politicians. Politicians cannot find papers to back their views; published research is now firmly on our side of the debate. Our points cannot be dismissed.
Again and again I come back to ‘knowledge matters’. It might still be possible to nip dictatorial control in the bud before it gains more traction.
Scientists Against Science: RCTs Which Give the Wrong Answer on Masks Are “the Worst Way to Answer the Question”
BY DR ROGER WATSON | THE DAILY SCEPTIC | MAY 5, 2023
Paradigm shifts in science are rare, but it seems we may have just had one. The RCT (randomised controlled trial), an experimental method used to test if medical procedures and drugs work, has long been considered the gold standard method of establishing the relationship between cause and effect. But it may just have been knocked off its perch and usurped by a new approach to seeking evidence.
Based on the first such study by James Lind in 1774 when he rid the Royal Navy of scurvy, the method in its simplest form involves giving one group of people a treatment and withholding it from another group and seeing if the treatment group fares better than the other (control) group. There is no evidence that Lind randomised the sailors on which he tested lemons as a cure for scurvy; randomisation, to avoid bias in who does and who does not receive treatment, was introduced much later. There are many modern variations on the theme of the RCT but, essentially, they are all designed to achieve the same thing.
As an experimental method for trying to settle whether treatments worked, the clinical trial took a while to catch on with the first RCT being published in 1948. Until that time, what was purported to work was based on power and opinion and, therefore, largely on who said it. Other, weaker designs based on observation and correlation abounded but, eventually, were superseded by the RCT.
Of course, not every RCT produces the same results due to an annoying phenomenon called ‘regression to the mean’ whereby observed effects are often obtained one day and inverse effects are obtained on another day. To account for regression to the mean, it is considered necessary to combine the results of similar studies to be able to pinpoint, at any time, where the true effect lies. Thus, the science of meta-analysis arose which does precisely that and the most rigorous repository of such analyses is considered to be the Cochrane Collaboration.
Well, forget all the above. It seems we have been following the wrong lines of investigation — especially when it comes to the use of face masks to prevent the spread of respiratory infections (e.g. COVID-19) — and that we should simply have asked the experts what they thought all along. In view of what we have witnessed in the past few years, what could possibly go wrong?
I may be doing them a disservice, but that is my interpretation of a recent article in STAT of May 2nd titled: ‘Do masks work? Randomised controlled trials are the worst way to answer the question.’ STAT is a newsletter that purports to be “Reporting from the frontiers of health and medicine” and the authors of the article are Baruch Fischhoff, Howard Heinz University Professor in the Department Engineering and Public Policy and Institute for Politics and Strategy Carnegie Mellon University, Martin Cetron an infectious disease epidemiologist who has worked for the CDC and Katelyn Jetelina, an epidemiology, data scientist, and science communicator who publishes a Substack, Your Local Epidemiologist.
Such is their faith in experts (and I assume they see themselves as such), with respect to RCTs on the use of face masks they “believe that many of these studies should never have been done at all, reserving resources for studies that could improve health outcomes”. The recent pair of Cochrane meta-analyses of studies on the use of face masks concluded that:
Pooled results of RCTs did not show a clear reduction in respiratory viral infection with the use of medical/surgical masks. There were no clear differences between the use of medical/surgical masks compared with N95/P2 respirators in healthcare workers when used in routine care to reduce respiratory viral infection.
Our paradigm-shifting team is not impressed, however: “Both meta-analyses have been widely misinterpreted as showing that face masks don’t work.” I cannot be certain but, had the Cochrane review shown a positive result regarding the use of face masks, my guess is that they would have been proclaiming that from the rooftops.
With apologies for lengthy quotes, they also say that:
What if it is so difficult to conduct scientifically sound randomised trials of mask wearing that even the best studies reveal little? Such studies can confuse people who want to know how effective face masks are, while emboldening people who are already completely convinced that face masks are ineffective — and are looking for grounds to sow doubt about them.
Clearly they see themselves as being above the misinterpretation of data to satisfy their own predilections; being “convinced” can work both ways.
With reference to the much-quoted and much-maligned DANMASK study where the difference observed between mask mandates and no mask mandates was “not statistically significant”, they conclude — presumably as the outcome, inconveniently, did not fit their prejudices – that “The designs of most clinical trials are too weak to answer the question that they pose — namely, whether an intervention succeeded”. Plus: “RCTs have value only when researchers can be sure that the treatment is administered as intended.” Perhaps they meant to say: “RCTs have value only when they show us what we want to see.” Besides, knowing whether an intervention works in practice rather than when done perfectly is valuable information from a public health point of view.
However, they do not leave us with no hope and inform us that: “Today, we have strong evidence regarding the effectiveness of face masks in the form of laboratory studies, theoretical analyses and RCTs that involved health care personnel. It has not come from RCTs of face masks distributed to the general public.” They do not trouble us ignoramuses with any details of this strong evidence, unless their hypertexted link to some words in an earlier sentence are meant to do the job. I guess they did not expect many people to go past the various subsequent links to read the material. It is fascinating stuff. The link eventually enables the explorer to download a ‘Rapid Expert Consultation on the Effectiveness of Fabric Masks for the COVID-19 Pandemic (April 8th 2020)’. This is a document written by experts which relates a series of studies on the likely effectiveness of face masks. No method is applied to the selection of studies which show a 100% publication bias. They have all been ‘cherry-picked’ to show exactly what the authors want them to show: that face masks could work.
Conveniently, the authors of the STAT article fail to refer to Cochrane reviews of precisely the kind of studies they advocate. A 2015 review of studies titled ‘Gloves, gowns and masks for reducing the transmission of meticillin‐resistant Staphylococcus aureus (MRSA) in the hospital setting’ concluded: “The effects of gloves, gowns and masks in these circumstances have yet to be determined by rigorous experimental studies.” In a 2016 review of studies titled ‘Disposable surgical face masks for preventing surgical wound infection in clean surgery’, the authors concluded: “From the limited results it is unclear whether the wearing of surgical face masks by members of the surgical team has any impact on surgical wound infection rates for patients undergoing clean surgery.”
Naturally, readers of the Daily Sceptic have the humility to admit that absence of evidence is not conclusive – though a null result from an RCT is not really absence of evidence but evidence of absence within the bounds of the trial’s limitations. In these circumstances, is it acceptable to impose a costly, polluting and potentially harmful intervention on the public? I think not.
Dr. Roger Watson is Academic Dean of Nursing at Southwest Medical University, China. He has a PhD in biochemistry.
The climate scaremongers: How the ‘world disaster’ figures lie
By Paul Homewood | TCW Defending Freedom | May 5, 2023
According to AP last year:
‘A disaster-weary globe will be hit harder in the coming years by even more catastrophes colliding in an interconnected world, a United Nations report issued Monday says. If current trends continue the world will go from around 400 disasters per year in 2015 to an onslaught of about 560 catastrophes a year by 2030, the scientific report by the United Nations Office for Disaster Risk Reduction said. By comparison from 1970 to 2000, the world suffered just 90 to 100 medium to large scale disasters a year, the report said.
‘The number of extreme heat waves in 2030 will be three times what it was in 2001 and there will be 30 per cent more droughts, the report predicted. It’s not just natural disasters amplified by climate change, it’s Covid-19, economic meltdowns and food shortages. Climate change has a huge footprint in the number of disasters,’ report authors said.’
The UN report included this graph, showing how the number of disasters were now five times as high as in the 1970s:

https://www.undrr.org/media/79595
Last week it was the turn of the World Meteorological Organisation (WMO) to bang the climate change drum. Their State of the Global Climate 2022 report commented: ‘From mountain peaks to ocean depths, climate change continued its advance in 2022 . . . Droughts, floods and heatwaves affected communities on every continent and cost many billions of dollars. While greenhouse gas emissions continue to rise and the climate continues to change, populations worldwide continue to be gravely impacted by extreme weather and climate events.’
The WMO is, of course, a UN body, so unsurprisingly this report has little to do with science and everything to do with politics.
But have natural disasters become so much more common in recent years? A closer look at that graph above reveals that the number of disasters has actually been declining since 2000, a fact which should immediately cast doubt on the ‘global warming is making everything worse’ meme.
The real reason for the ‘increase’ is that many natural disasters in years past were never officially logged in the UN database, called EM-DAT, which is compiled by CRED, the Center for Research on the Epidemiology of Disasters. The database was not created until 1998, and CRED relied on informal reports for disasters prior to that year.
CRED has acknowledged that many events were missed by them in the past. In their 2006 report, they warned that earlier data was incomplete and should not be used for comparing long-term trends. In particular, over the past 30 years development in telecommunications, media and increased international cooperation has played a critical role in the number of disasters reported. In addition, increases in humanitarian funds have encouraged reporting of more disasters.
In fact the unreliability of the database in earlier years is much worse than we thought. Take a look, for example, at the official data for the number of deaths from floods in the UK:

https://ourworldindata.org/natural-disasters
Now look again, and see if you can spot what is missing. Yes, the North Sea floods in 1953, recognised as one of the worst natural disasters ever to hit Britain, and which left 307 dead on the east coast alone. The death toll in 1952, by the way, reflects the Lynmouth disaster, which killed 34.
How any supposedly reputable database can omit an event like the 1953 flood and still claim to be credible is beyond me. Other bad flooding events have also been missed, such as those in Somerset in 1968 which killed 15 people.
Flooding events in the UK have been thoroughly recorded as far back as the 19thC and beyond. If CRED cannot even get accurate data for the UK, what chance is there of compiling full and accurate data for the rest of the world?
The truth about the looming energy shortage
UK FIRES is a five-year research programme funded by £5million of government money, a collaboration between the universities of Cambridge, Oxford, Nottingham, Bath and Imperial College London. Its job is to look at what Net Zero means in practical terms for the economy.
The researchers have a habit of revealing the harsh realities of Net Zero which are deliberately hidden from us by the government and its advisers. For instance, in their 2019 report, called Absolute Zero, they calmly informed us that we would all have to drive less, use less energy, and stop eating beef and lamb. All UK airports except for Heathrow, Glasgow and Belfast would have to close by 2030, and those three would also have to go by 2050. All shipping to and from Britain would have to be phased out as well.
Their report on the construction sector last November told us that no bricks, cement or glass would be allowed in our bright new future. Instead we would have to make do with recycled materials, along with stone, earth and timber. A sort of cross between Fred Flintstone and Mad Max!
Their latest analysis came out last month, looking at the prospect for UK energy supplies under current emission reduction targets. The government has pledged to reduce emissions by 68 per cent from 2018 levels by 2035.
According to UK FIRES, to do this we need to be constructing 14GW of low carbon generation every year until 2035, whereas the current rate is only about 2GW. (They do not tell us, by the way, how we can build wind farms and nuclear plants without cement and steel!)
One problem is that it is now taking more than 20 years to build a large nuclear power station. It seems unlikely therefore that we will see Sizewell C before the 2040s, even if contracts were signed today.
According to UK FIRES, they have been pointing out this energy shortfall for a while, but government and the civil service prefer to stick their heads in the sand. Not that UK FIRES are concerned either, because they just want us to drastically cut the amount of energy we use instead.
Over the next eight years, they say, we must cut our car mileage by a fifth, consume a third less beef, lamb, milk and cheese, replace millions of gas boilers with heat pumps, and spend tens of billions that we have not got on insulating our homes.
Industry must halve its use of construction materials, such as cement and steel, and shut half of the county’s blast furnaces. With all this and more, we will be able to reduce the country’s energy use by 30 per cent. All in the next eight years; after that it really gets tough!
For years, successive governments, along with the Committee on Climate Change, other advisers, and the complicit media, have lied to us, pretending that we could chart a path to Net Zero without any real cost or consequences. Thanks to UK FIRES, we are beginning to get a glimpse of the truth. And the public will be horrified and extremely angry when they discover they have been duped.
FDA Approves First RSV Vaccine, But Some Experts Say Weak Safety, Efficacy Data Suggest Benefits Don’t Outweigh Risks
By Michael Nevradakis, Ph.D. | The Defender | May 4, 2023
Describing it as a “long-sought scientific achievement,” the U.S. Food and Drug Administration (FDA) on Wednesday approved Arexvy, the first vaccine for respiratory syncytial virus (RSV).
GlaxoSmithKline Biologicals (GSK) developed Arexvy under the FDA’s Priority Review designation. The FDA approved it for people ages 60 and older.
According to CNBC, the U.S. “suffered an unusually severe RSV season” this past winter. The New York Times reported on a “tripledemic” involving RSV, flu and COVID-19, “that swamped children’s hospitals and some I.C.U. wards.”
One U.S. county — Orange County, California — declared a local health emergency and issued a proclamation of local emergency in November 2022, citing rising RSV cases among children in the region.
GSK described results from clinical trials for Arexvy as “positive,” and the company said the U.S. launch of the vaccine is planned before the 2023-24 RSV season.
Other RSV vaccines, including one produced by Pfizer, are in the pipeline and expectations are that the FDA will approve them.
During clinical trials for both the GSK and Pfizer vaccines, several participants were diagnosed with rare conditions such as Guillain-Barré syndrome (GBS) and acute disseminated encephalomyelitis (ADEM). One of the individuals who developed ADEM later died, according to the FDA.
Aside from concerns over potential serious adverse events related to RSV vaccines, some experts have questioned the need for such a vaccine in the first place.
According to the journal Science, “RSV is a common respiratory infection” with symptoms “similar to a cold,” adding that “The majority of individuals recover within a few days from an uncomplicated RSV infection, although occasionally the virus can cause lower respiratory infections requiring medical attention.”
Dr. Peter McCullough, a cardiologist, told The Defender:
“Respiratory syncytial virus is a negligible threat to even the most frail elderly adults. The effort of widespread vaccination is simply not worth it. Even rare side effects will outweigh any theoretical benefit.”
And in a November 2022 episode of “RFK Jr. The Defender” podcast, several medical and public health experts expressed concerns about RSV vaccines.
“We have to stop these shots,” said Dr. Meryl Nass, an internist and biological warfare epidemiologist. “It’s just extraordinary that we’re still vaccinating people … we have a lot of work to do.”
Robert F. Kennedy Jr., then-chairman and chief litigation counsel for Children’s Health Defense (now chairman on leave), described RSV as “a vehicle for re-implementing the COVID-19 playbook all over the country and responding with vaccines.”
And according to the National Vaccine Information Center (NVIC), “Cost analysis data presented to the ACIP [Advisory Committee on Immunization Practices] did not show the RSV vaccines to be cost-effective at reducing the burden of costs associated with RSV illness.”
Nevertheless, more RSV vaccines are expected to receive FDA approval this year — including a Pfizer RSV vaccine for pregnant women that led to a high incidence of adverse events for both the women and their infants during clinical trials, as well as several deaths and stillbirths.
Arexvy approval ushers in new ‘highly competitive and lucrative vaccine market’
The RSV vaccine market is estimated to be worth up to $10 billion by 2030.
According to Endpoints News, the FDA’s approval of Arexvy ends “half a century of failed efforts against the elusive, shape-shifting virus” and “officially start[s] what analysts expect will be a highly competitive and lucrative new vaccine market.”
In getting Arexvy approved, “GSK beat a crowded field of competitors to cross the finish line first.”
Arexvy “showed strong efficacy in stopping lower-respiratory tract infections as well as more severe disease” and will be administered as a single dose, according to Endpoints News.
STAT reported that a “vaccine that was developed by Pfizer and aimed at the same demographic [adults 60 and over] is expected to be approved by the end of the month,” while other RSV vaccines and therapeutics, including some intended for children and pregnant women, are in the pipeline and also are close to receiving FDA approval.
The FDA’s approval of Arexvy came after an FDA advisory panel reviewed data from GSK’s and Pfizer’s clinical trials on March 1. The panel unanimously agreed that GSK’s vaccine is effective and, in a 10-2 vote, deemed it “safe,” according to The Washington Post.
The same panel also approved Pfizer’s candidate vaccine, Abrysvo, but with a 7-4 vote.
On June 21 or 22, ACIP, which advises the Centers for Disease Control and Prevention (CDC), will convene to “make recommendations on the appropriate use of the vaccine in the U.S.,” according to GSK’s announcement. The ACIP must recommend the vaccines before they are marketed.
According to STAT, there is a likelihood that ACIP may not approve Arexvy for its intended age group, stating:
“Though Arexvy’s approval is for adults 60 and older, it remains to be seen if the CDC will recommend it for that entire group.
“At an advisory committee meeting in February, members of a work group studying the adult vaccines that will soon come before ACIP indicated that at present, they don’t believe the vaccine would be cost-effective in people aged 60 to 64 and they would not recommend to the wider committee that it include people 60 to 64 in its recommendation for the use of the vaccine. (The group held the same position for the Pfizer RSV vaccine.)”
In April, the European Medicines Agency (EMA) issued its own recommendation for Arexvy, for adults 60 and over, according to the Times. However, a final EMA regulatory decision is anticipated later this year. GSK is also awaiting licensure for Arexvy in Australia, China, Japan and other countries, STAT reported.
In an earnings presentation April 26, GSK said it has “millions of doses” of Arexvy “ready to be shipped.”
“GSK’s RSV vaccine works by using a small piece of the virus: a protein that sticks out on its surface called the fusion, or F, protein, which helps the virus glom onto and infect cells in the body’s upper airways. The protein pieces in the vaccine are made in a lab, using cells specially programmed to manufacture them.”
CNN noted that the vaccine “builds on a pivotal discovery made a decade ago” by National Institutes of Health researchers, “including some of the same scientists who helped make the COVID-19 vaccines.” Specifically, the researchers figured out how to freeze the otherwise “wiggly” F protein, “in the shape it takes before it fuses onto a cell.”
STAT, quoting Phil Dormitzer, GSK senior vice president and global head of vaccines research and development, reported that although Arexvy “contains only one of the two RSV subtypes, RSV A,” studies showed that it is “virtually equally protective against both RSV A and RSV B” as the F protein on both subtypes is similar.
Dormitzer acknowledged natural immunity, telling STAT, “because older adults have all had RSV probably multiple times by the time they get [the vaccine], they’re primed against both A and B. So you’re able to get very solid boosting against both subtypes with a single adjuvanted F antigen.”
According to GSK, the Arexvy vaccine does not use mRNA technology, but “contains a recombinant subunit prefusion RSV F glycoprotein antigen (RSVPreF3) combined with GSK’s proprietary AS01E adjuvant.”
GSK, FDA claim Arexvy clinical trial data show vaccine is ‘safe and effective’ but annual shot may be needed
The FDA announcement stated:
“The safety and effectiveness of Arexvy is based on the FDA’s analysis of data from an ongoing, randomized, placebo-controlled clinical study conducted in the U.S. and internationally in individuals 60 years of age and older.”
According to the FDA, “approximately 12,500 participants … received Arexvy and 12,500 participants … received a placebo. Among the participants who have received Arexvy and the participants who have received a placebo, the vaccine significantly reduced the risk of developing RSV-associated LRTD [lower respiratory tract disease] by 82.6% and reduced the risk of developing severe RSV-associated LRTD by 94.1%.”
LRTD was “defined as two or more symptoms including shortness of breath, wheezing, cough, increased mucus production, crackles, low oxygen saturation, or need for oxygen supplementation,” according to CNBC, while according to CNN, “People were considered to have severe disease if they needed supplemental oxygen or needed mechanical help to breathe, like a ventilator.”
According to the FDA, half of the 25,000 participants received Arexvy, while the other half received a placebo.
The results of GSK’s clinical trials for Arexvy were published in the New England Journal of Medicine on Feb. 16.
FDA and GSK officials provided glowing reviews of the new vaccine. Peter Marks, M.D., Ph.D., director of the FDA’s Center for Biologics Evaluation and Research, said in a statement:
“Older adults, in particular those with underlying health conditions, such as heart or lung disease or weakened immune systems, are at high risk for severe disease caused by RSV.
“Today’s approval of the first RSV vaccine is an important public health achievement to prevent a disease which can be life-threatening and reflects the FDA’s continued commitment to facilitating the development of safe and effective vaccines for use in the United States.”
Tony Wood, GSK’s chief scientific officer, described Arexvy’s approval as “a turning point in our effort to reduce the significant burden of RSV,” adding that “Our focus now is to ensure eligible older adults in the U.S. can access the vaccine as quickly as possible and to progress regulatory review in other countries.”
In turn, Dormitzer said, “There’s just the broad excitement of finally, after all these years, having good options emerging for RSV,” describing this as a “triumph of the basic science.”
While GSK is first out of the gate in the RSV vaccine race with Arexvy, Pfizer’s candidate vaccine has also completed clinical trials, which found it to be “nearly 67 percent effective in preventing R.S.V. – related illness,” according to the Times.
The FDA and GSK announcements did not mention the vaccines’ waning effectiveness. An analysis by the NVIC found that the effectiveness of the GSK vaccine peaked after two months and offered no protection after one year. This may result in recommendations for adults to receive annual doses of the vaccine.
Trial participant died from a rare inflammatory condition, others developed GBS
Despite positive comments from FDA and GSK officials, clinical trial data for Arexvy revealed instances of GBS and other rare conditions.
In its announcement Wednesday, GSK claimed:
“The vaccine was generally well tolerated with an acceptable safety profile. The most frequently observed solicited adverse events were injection site pain, fatigue, myalgia, headache, and arthralgia. These were generally mild to moderate and transient.”
The announcement did not mention GBS.
According to the FDA announcement Wednesday:
“The most commonly reported side effects by individuals who received Arexvy were injection site pain, fatigue, muscle pain, headache and joint stiffness/pain.
“Among all clinical trial participants, atrial fibrillation within 30 days of vaccination was reported in 10 participants who received Arexvy and 4 participants who received placebo.”
However, the FDA noted that in two other Arexvy studies involving approximately 2,500 participants 60 and over, “two participants developed acute disseminated encephalomyelitis (ADEM), a rare type of inflammation that affects the brain and spinal cord, seven and 22 days, respectively, after receiving Arexvy and the influenza vaccine.”
“One of the participants who developed ADEM died,” according to the FDA.
In another Arexvy study conducted by GSK, “one participant developed Guillain-Barré syndrome (a rare disorder in which the body’s immune system damages nerve cells, causing muscle weakness and sometimes paralysis) nine days after receiving Arexvy,” the FDA stated.
According to an FDA briefing document cited by CNBC:
“A 78-year-old woman in Japan was diagnosed with Guillain-Barré syndrome nine days after receiving GSK’s vaccine … She was hospitalized for six months before being released.”
CNBC reported that GSK claimed in February “There is insufficient evidence to confirm the woman got Guillain-Barre as a result of GSK’s shot.” However, the FDA “considers the case to be related to GSK’s vaccine.”
According to the FDA’s announcement:
“The FDA is requiring the company to conduct a postmarketing study to assess the signals of serious risks for Guillain-Barré syndrome and ADEM. In addition, although not an FDA requirement, the company has committed to assess atrial fibrillation in the postmarketing study.”
According to the Times, “Once the shots become available to the public, the agency said it would require GSK to monitor the incidence of Guillain-Barré and another rare condition that was possibly related to the shot.”
The FDA similarly flagged GSK “as a potential safety issue with Pfizer’s RSV vaccine for older adults,” CNBC reported after two clinical trial participants developed GBS. According to the Post, both participants — one man and one woman — were 66 years old.
CNBC in February reported that Pfizer “will conduct a safety study to further address Guillain-Barré syndrome if the FDA approves its vaccine.”
GSK’s chief commercial officer, Luke Miels, said the vaccine would cost upwards of $120 a dose, according to the Post, which also reported that private insurers may cover “many costs” associated with the vaccine, while Medicare patients with Part D coverage “won’t pay anything out of pocket” for the vaccine.
“Shares of GSK rose nearly 2% Wednesday following the approval,” CNBC reported.
GSK is also pressing forward with “A clinical trial that aims to expand the population who may benefit from RSV vaccination into adults aged 50-59, including participants with underlying comorbidities,” according to the company’s Wednesday announcement, with results “expected in 2023.”
Is there a need for an RSV vaccine?
According to the FDA:
“RSV is a highly contagious virus that causes infections of the lungs and breathing passages in individuals of all age groups. RSV circulation is seasonal, typically starting during the fall and peaking in the winter.
“In older adults, RSV is a common cause of lower respiratory tract disease (LRTD), which affects the lungs and can cause life-threatening pneumonia and bronchiolitis (swelling of the small airway passages in the lungs).”
The FDA cited CDC figures claiming each year in the U.S., RSV leads to approximately 60,000-120,000 hospitalizations and 6,000-10,000 deaths among adults 65 years of age and older.”
STAT reported that “RSV season has been unpredictable in the wake of the COVID-19 pandemic, though some experts believe RSV activity is moving back toward the seasonality seen in the pre-COVID days,” noting that “there was little transmission in 2020, when people were wearing masks and social distancing.”
But RSV “returned abnormally early in 2021,” STAT reported, but without an explanation for why this occurred, despite widespread masking and social distancing that year, too.
In the U.S., pediatric deaths from RSV are not common but the infection is the No. 1 cause of hospitalizations for children under the age of 1, STAT reported. Globally, however, it is the second leading cause of death in children under 1, after malaria.
According to STAT, “All but the youngest of children have had RSV multiple times, but few of us would know with any certainty that this bad cold was caused by that bad virus.”
Nevertheless, Pfizer is proceeding with the development of an RSV for infants as young as 6 months — “the age group at highest risk of being hospitalized with RSV,” STAT reported, noting that the vaccine for this age group is expected to gain FDA approval later this year and will be administered to pregnant women “to generate antibodies that protect both the pregnant person and their newborn.”
Data reported by Pfizer to the CDC indicated that 14% of pregnant women who participated in Pfizer’s trial sustained an adverse event, with 4.2% sustaining a “serious” adverse event, 1.7% experiencing a “severe” adverse event and 0.5% suffering a “life-threatening” adverse event.
Similarly, the same data showed that 37.1% of infants whose mothers received the experimental Pfizer vaccine experienced adverse events within one month of birth — with 15.5% classified as “serious,” 4.5% as “severe” and 1% as “life-threatening,” while efficacy waned within months of vaccination.
According to the NVIC, “The RSV clinical trial data also included the death of one pregnant woman, 18 still births (10 in vaccinated pregnant women and 8 in unvaccinated pregnant women), and 17 infant deaths (five from the vaccinated pregnancy group and 12 in unvaccinated pregnancy group).”
In its report to the CDC, Pfizer claimed the deaths were unrelated to the vaccine.
The FDA’s Vaccines and Related Biological Products Advisory Committee will meet virtually on May 18 to discuss approval of this vaccine. The meeting is open to the public, and a public comment period is open until May 17. A final FDA decision is expected in August.
According to the Times, “Moderna is also developing an RSV vaccine for adults 60 and over, with authorization expected in the first half of this year. The Times referenced clinical trial data released by Moderna claiming 82% efficacy, with “no safety concerns identified.”
Bavarian Nordic, known for its development of a vaccine in response to last year’s monkeypox outbreak, is also developing an RSV vaccine for adults 60 and over,” expecting to release Phase 3 clinical trial data by midyear, according to the Post and CNN.
AstraZeneca and Sanofi also are seeking FDA approval, but for nirsevimab, a monoclonal antibody treatment for RSV that would be administered to infants and toddlers up to age 2, according to the Times, which referenced clinical trial results claiming a reduction of illness of up to 75%.
According to the Post, nirsevimab “is already approved in Europe, the United Kingdom and Canada.”
However, the NVIC reported that the effectiveness of nirsevimab “is not known beyond 150 days” and it is unclear if the drug prevents ICU stays or deaths. It is being reviewed by ACIP, which according to the NVIC, is “a federal advisory committee charged with making vaccine use recommendations.”
“It is unclear why the ACIP … has chosen to go beyond its charge of making vaccine use recommendations,” NVIC states.
Safety concerns related to RSV vaccines nevertheless linger. According to CNN, an RSV vaccine developed in the 1960s for children initially delivered promising results during trials in children and animals.
However, once administered to children in the general population, “many of the children who were vaccinated required hospitalization and got more severe RSV disease than what would have normally occurred” — and two of the initial trial participants died.
Michael Nevradakis, Ph.D., based in Athens, Greece, is a senior reporter for The Defender and part of the rotation of hosts for CHD.TV’s “Good Morning CHD.”
This article was originally published by The Defender — Children’s Health Defense’s News & Views Website under Creative Commons license CC BY-NC-ND 4.0. Please consider subscribing to The Defender or donating to Children’s Health Defense.
After years of mandates, German Health Ministry admit they have no idea whether or to what degree masks work at all
Pandemic mythology continues its slow decay
eugyppius: a plague chronicle | May 3, 2023
As on several prior occasions, liberal Bundestag vice-president Wolfgang Kubicki has used his parliamentary prerogatives to put a question to the German Health Ministry, and compel an answer. He asked what study results the Ministry could cite to demonstrate the efficacy of face masks. Lauterbach’s crack team of virus understanders responded that, uh, it is a very complicated problem, and, in truth, well, actually, nobody really knows what effect masks really have. This is because “the effectiveness of individual measures … cannot be examined in isolation, but only in conjunction with the other measures in place at any given time.”
In other words: they got nothing. After years of making kids mask for hours on end in school, and imposing arbitrary but quite obnoxious mandates on airplanes and public transit and clinics, they have no idea whether it did anything, and no plans even to find out whether it did anything. Suddenly all that manic masking enthusiasm has just evaporated.
The response comes several weeks after Anthony Fauci’s statement to the New York Times that “at the population level, masks work at the margins, maybe 10 percent.” This is itself a baseless claim, but it’s another important walk-back of the insane doctrines that medical bureaucrats have been spinning about masks since 2020.
You have to think of propaganda like a big machine. Somebody has to plug it in and it draws a lot of electricity, but with the right inputs it can dazzle a lot of people. The problem is that sooner or later the deception isn’t worth anybody’s time or energy anymore, and so somebody must also shut it off. It looks like nobody bothered with any kind of messaging exit strategy, and so we’ve entered a very weird period, wherein the public health leviathan has ceased rehearsing its crazy pandemic myths, leaving the ever-shrinking minority of deranged Covidians to their own devices.
Now and again the fact-checkers still throw them a bone, so there’s that.
Featured Video

Larry Johnson: U.S. Desperation Grows as Iran Is Winning
or go to
Aletho News Archives – Video-Images
From the Archives
Alarmist climate science as a textbook example of groupthink
By Paul MacRae | May 1, 2012
A while ago, I received an email from a friend who asked:
How can many, many respected, competitive, independent science folks be so wrong about [global warming] (if your [skeptical] premise is correct). I don’t think it could be a conspiracy, or incompetence. … Has there ever been another case when so many ‘leading’ scientific minds got it so wrong?
The answer to the second part of my friend’s question—“Has there ever been another case where so many ‘leading’ scientific minds got it so wrong?”—is easy. Yes, there are many such cases, both within and outside climate science. In fact, the graveyard of science is littered with the bones of theories that were once thought “certain” (e.g., that the continents can’t “drift,” that Newton’s laws were immutable, and hundreds if not thousands of others).
Science progresses by the overturning of theories once thought “certain.” … continue
Blog Roll
 Aletho News
Aletho News- Larry Johnson: U.S. Desperation Grows as Iran Is Winning
- Why don’t UK media mention the Israel lobby?
- New US shipment of 6,500 tons of military aid arrives in Israel
- Military aid to Ukraine vital for ‘US hegemony’ – Republican senator
- Zelensky’s favorite drone company at center of Ukrainian corruption alert
- The Broken Contract
- US CENTCOM’s Request for Dark Eagle Missiles Shows Shortage of Weapons and Limited Options
- Iran consolidates Strait of Hormuz control in post-war power shift, leaving US in dark
- A pause, not a ceasefire: Washington stalls, Tehran recalibrates
- US blockade crumbles as Iran turns to overland routes
- If Americans Knew
- US ships 6,500 tons of munitions, equipment to Israel in 24 hours
- A New Library in Gaza Rises From the Ashes of Destruction
- Israel’s top Jewish religious body ‘refuses to condemn’ smashing of Jesus statue
- Nun assaulted in Jerusalem amid ‘pattern’ of anti-Christian attacks by Israelis
- Former Tik Tok official describes massive pressure from Israel lobby
- Amid ceasefire violations and genocide, Israel commits piracy – Daily Update
- Five Laws and Standards That Require the US Cut Off Weapons to Israel
- Israel’s diabolical killing machine and how it targets journalists.
- The Global Sumud Flotilla to Gaza — A cry at sea to the world’s dormant conscience
- Politico’s powerful parent company tells Politico they must support Israeli narrative
- No Tricks Zone
- Oversupply Of Volatile Solar Energy Leads To Record NEGATIVE Prices!
- New Study: Extreme Heat Records, Heatwaves, Extreme Cold Records Declining Across US Since 1899
- It’s The Cold, Stupid! Cold 20 Times More Lethal Than Heat, Multiple Studies Show
- European Institute For Climate And Energy: “Climate Debate is Seldom About Science”
- New Study: The Climate May Be 5 Times More Sensitive To Solar Forcing Than Commonly Assumed
- EV Industry Reached $70 Billion In Losses In 2024 Due To Delusional Green Ideologies
- Reality Check: Maldives Have Actually Grown In Size Or Remained Stable Over Recent Decades
- Abrupt Climate Change Also Occurred NATURALLY In The Past …25 Times During Last Ice Age
- Cave Discovery Reveals Today’s Desert Climates Were Recently Far Warmer, Wetter, Teeming With Life
- German Expert: Heat Dome Led To Record Temps In Western USA…Warmer In 1934, 1936
