HOW IS THIS A THING? 27TH OF JUNE 2022
Sources:
Women’s Health and COVID-19: FLCCC Weekly Update (June 15, 2022): https://odysee.com/@FrontlineCovid19CriticalCareAlliance:c/Weekly_Webinar_June15#d
By Suzanne Burdick, Ph.D. | The Defender | July 1, 2022
The Biden administration today said it ordered 2.5 million more doses of Bavarian Nordic’s Jynneos monkeypox vaccine, bringing the total vaccine doses to be delivered in 2022 and 2023 to more than 4 million.
The news followed Tuesday’s announcement of the first phase of the U.S. government’s “national monkey vaccine strategy,” which will expand testing capabilities and make Bavarian Nordic’s Jynneos vaccines readily available to anyone exposed to the virus.
The U.S. Department of Health and Human Services (HHS) said the government’s “enhanced” nationwide strategy “will vaccinate and protect those at-risk of monkeypox,” as well as provide guidance to communities on how to respond to outbreaks.
“We are focused on making sure the public and healthcare providers are aware of the risks posed by monkeypox and that there are steps they can take — through seeking testing, vaccines and treatments — to stay healthy and stop the spread,” said Dr. Rochelle Walensky, director of the Centers for Disease Control and Prevention (CDC).
As part of the strategy, the CDC and HHS began shipping tests to five major laboratory companies across the country: Aegis Science, Labcorp, Mayo Clinic Laboratories, Quest Diagnostics and Sonic Healthcare.
The government, which for months has been buying more Jynneos doses to add to the national stockpile, is now distributing the vaccine. It’s currently making available 296,000 doses and expects to roll out 750,000 doses over the summer, with an additional 500,000 doses produced and released in the fall — for a total of 1.6 million doses this year.
The Jynneos vaccine is licensed for use in adults and is considered safer than Emergent BioSolutions Inc.’s ACAM2000 smallpox vaccine, which also can be used against monkeypox, the HHS said.
The vaccine will be made available to individuals “with confirmed and presumed monkeypox exposures,” said the HHS.
“This includes those who had close physical contact with someone diagnosed with monkeypox, those who know their sexual partner was diagnosed with monkeypox, and men who have sex with men who have recently had multiple sex partners in a venue where there was known to be monkeypox or in an area where monkeypox is spreading.”
Health officials seeking to expand use of monkeypox vaccine for kids, despite lack of safety data
U.S. health officials also are seeking to expand use of the monkeypox vaccine for children, Bloomberg reported.
The CDC is developing a protocol aimed at allowing use of the Jynneos vaccine in children “should cases in children occur,” Kristen Nordlund, a CDC spokesperson, said in an email to Bloomberg.
“I’m concerned about sustained transmission because it would suggest that the virus is establishing itself, and it could move into high-risk groups, including children, the immunocompromised, and pregnant women,” Tedros Adhanom Ghebreyesus, director-general of the World Health Organization (WHO) said in a Wednesday press briefing.
“We’re starting to see this with several children already infected,” he added.
There have been 350 cases so far of monkeypox in the U.S. — all adults — according to the CDC. The agency confirmed 5,115 cases worldwide.
The WHO confirmed two cases in children in the U.K. and said Wednesday it is following up on reports of cases in children in Spain and France.
No safety trials have been done in children for the Jynneos vaccine as of yet, partly because clinical research involving participants under the age of 18 must pose no more than “minimal risk” to children, which can be difficult for vaccine manufacturers to argue.
Commenting on the CDC’s actions, Dr. Meryl Nass, a member of the Children’s Health Defense scientific advisory committee, told The Defender, “It’s kind of extraordinary that they want to vaccinate everyone in the country before knowing what the safety issues are.”
Nass, an internist and biological warfare epidemiologist, said, “We don’t actually know” if the Jynneos vaccine prevents monkeypox in humans because it was developed as a smallpox vaccine, and prevention studies have been conducted using only animals.
“It is hard to believe that the [U.S. Food and Drug Administration (FDA)] gave this vaccine a license when you read the FDA reviewers’ comments in their own report,” Nass wrote in her June 23 substack newsletter.
“They could not test the vaccine for efficacy against smallpox because there is no smallpox, nor against monkeypox, because the disease is so rare,” Nass wrote. “So the FDA relied on neutralizing antibody titers.”
At the same time, the FDA admitted there is no established correlate of protection, Nass said.
“This means that there is no evidence that the titers represent actual immunity to infection,” Nass wrote. “So FDA relied on animal studies to simply guess the vaccine might be effective in humans.”
According to the FDA, the effectiveness of Jynneos for the prevention of monkeypox is “inferred from the antibody responses in the smallpox clinical study participants and from studies in non-human primates that showed protection of animals vaccinated with Jynneos who were exposed to the monkeypox virus.”
Jynneos, a replication-deficient live Vaccinia virus vaccine, was licensed in the U.S. in 2019, by the FDA for use in individuals 18 and over considered to be at high risk for smallpox or monkeypox.
In 2021, the CDC’s Advisory Committee on Immunization Practices (ACIP) voted to recommend Jynneos as a safer alternative to the ACAM2000 vaccine because of ACAM2000’s propensity to cause serious adverse effects, including myocarditis and pericarditis — i.e., inflammation of the heart.
However, Nass noted, Jynneos also was linked to heart inflammation, according to the FDA licensure review of the Jynneos smallpox-monkeypox vaccine which reported:
“Up to 18.4% of subjects in 2 studies developed post-vaccination elevation of troponin [a cardiac muscle enzyme signifying cardiac damage]. However, all of these troponin elevations were asymptomatic and without a clinically associated event or other sign of myopericarditis.”
These higher levels of troponin were not studied further, and the reviewers admitted they did not know if the Jynneos vaccine caused myocarditis, Nass said.
The Jynneos manufacturers said they would conduct an “observational, post-marketing study” in which they would “collect data on cardiac events that occur and are assessed as a routine part of medical care.”
But myocarditis — particularly asymptomatic forms of myocarditis that lack outer signs of the condition — could fly under the radar of the “routine part of medical care,” noted Nass.
The manufacturers would need to test for heightened troponin levels — something that is not typically done in “routine” check-ups.
The authors of a 2015 study reported evidence of heart injury following vaccination in a sample of 1,445 individuals who received a smallpox or trivalent influenza vaccine.
They found that chest pain, shortness of breath and/or palpitations occurred in 10.6% of those who received the smallpox vaccine SPX-vaccinees and 2.6% of those who received the trivalent influenza vaccine within 30 days of immunization.
Additionally, the study authors reported levels more than double the upper limit of troponin — a protein that flags cardiac injury — in 31 of the individuals who received the smallpox vaccine.
“Passive surveillance significantly underestimates the true incidence of myocarditis/pericarditis after smallpox immunization,” they concluded.
The authors added:
“Evidence of subclinical transient cardiac muscle injury post-vaccine immunization is a finding that requires further study to include long-term outcomes surveillance. Active safety surveillance is needed to identify adverse events that are not well understood or previously recognized.”
Suzanne Burdick, Ph.D., is an independent journalist and researcher based in Fairfield, Iowa.
© 2022 Children’s Health Defense, Inc. This work is reproduced and distributed with the permission of Children’s Health Defense, Inc. Want to learn more from Children’s Health Defense? Sign up for free news and updates from Robert F. Kennedy, Jr. and the Children’s Health Defense. Your donation will help to support us in our efforts.
By Francis Menton | Manhattan Contrarian | June 29, 2022
Just over six months ago, in December 2021, I asked the question that was on the tip of the tongue of everybody who follows the subject of the ongoing massive “green” transition to fossil-fuel-free energy. Actually, that’s a lie. The question I asked was not on the tip of the tongue of everybody who follows the subject, or even of most of the people who follow the subject, for reasons that to me are completely inexplicable. The question was : “Which Country Or U.S. State Will Be The First To Hit The Green Energy Wall?”
The candidates that I nominated in that post as potentially the first to hit the “green energy wall” were California, New York, the UK and Germany. At the time, I thought it was obvious that one of those jurisdictions would hit the wall sooner than almost anybody expected. Indeed, I was quite bold in the short time frame that I predicted:
A prolonged period of unfavorable weather (calm and overcast) could cause a serious energy crunch to hit one or both of Germany or the UK as soon as this winter. Or they could get lucky and go another year or two.
Now here we are in June 2022, and I think it’s hard to deny that Germany has in fact hit the “green energy wall.” Let’s consider.
First, here is the definition of the “green energy wall” that I gave in the post:
[O]ne or another of [those states or countries] is highly likely to hit a “wall” — that is, a situation where the electricity system stops functioning, or the price goes through the roof, or both, forcing a drastic alteration or even abandonment of the whole scheme.
And here’s the reason I gave why one or another (or all) of the nominated jurisdictions would soon be hitting the “wall”:
All these places, despite their wealth and seeming sophistication, are embarking on their ambitious plans without ever having conducted any kind of detailed engineering study of how their new proposed energy systems will work or how much they will cost. Sure, a wind/solar electric grid can function with 100% natural gas backup, if you’re willing to have the ratepayers foot the bill for two overlapping and redundant generation systems when you could have had just one. But “net zero” emissions means no more fossil fuel backup. What’s the plan to keep the grid operating 24/7 when the coal and natural gas are gone?
As is (or should be) obvious to everyone, a predominantly wind/solar electricity generation system needs full backup from some source to keep the lights on 24/7. The options are few: fossil fuels plants (coal, oil or natural gas), nuclear, or storage (i.e., batteries). Germany has ruled out the fossil fuel and nuclear options. It never had much in the way of oil-fired electricity generation, and it spent the last ten-plus years phasing out its coal and nuclear plants. So, that leaves storage. Surely, you might think, having embarked on a multi-trillion dollar transition to a predominantly wind/solar electricity system, and having ruled out both fossil fuels and nuclear for backup, Germany must have been focused like a laser beam on the storage issues to make the whole thing work.
You would be wrong. It is truly unbelievable the extent to which Germany — seemingly the country with the most sophisticated engineering in the world — put its head in the sand and ignored the storage problem until it just ran its energy system into the wall.
Let’s compare how much energy storage Germany would need to back up its wind/solar electricity system to the amount of storage actually developed to date or in the pipeline. At this website, I have followed the energy storage question closely, and have discussed and linked to the most competent calculations of how much storage would be needed to back up a predominantly or fully wind/solar electricity system for various jurisdictions, including Germany. In this post in November 2018 I linked to and extensively discussed work by a man named Roger Andrews, who calculated the storage requirement for Germany to back up a fully wind/solar system as approximately 25,000 GWH. In that post, I also examined some reasons why Andrews’s calculation might be low — for example, Andrews assumed a 100% return from energy put into storage (which is unrealistic), and also based his calculations on actual generation and weather data for a particular year (2016), which could prove more favorable than another year. But that said, Andrews’s calculation appeared to me to be in the right ballpark. More recently, in a post in March 2022, I discussed and linked to work of two German scientists named Oliver Ruhnau and Staffan Qvist. Ruhnau and Qvist calculated a storage requirement for Germany to back up a fully wind/solar system as 56,000 GWH.
If you figure that Andrews may be on the low side, and Ruhnau/Qvist on the high side, that would put a good rough estimate of Germany’s need for grid-scale energy storage to back up a wind/solar system somewhere in the range of about 40,000 – 50,000 GWH.
So how much storage does Germany have currently existing or in the pipeline? Here is an April 11, 2022 piece from consultancy Wood Mackenzie reporting excitedly about Europe’s plans to solve the wind/solar intermittency problem with storage, “Europe’s grid-scale energy storage capacity will expand 20-fold by 2031.”:
Europe has set out some of the world’s most ambitious decarbonisation targets. And the pace of change is accelerating. . . . [T]he region’s nascent grid-scale energy storage segment is growing fast. We forecast that total capacity will expand 20-fold between now and 2031.
Here’s their chart showing what that “20-fold expansion” will mean by 2031:

For Germany, this enormous expansion will supposedly mean all of 8.81 GWH of grid-scale energy storage. Is there a decimal place error here? Unfortunately no. Against a requirement of 45,000 GWH +/- of grid-scale storage, they’re not planning on 9000 GWH, or even 900 GWH or 90 GWH, but 9. They’re off by a factor of around 5000 against what they would need.
In other words, they haven’t even begun to solve the storage problem that would need to be solved to make their wind/solar system work, and they will barely if at all have begun to solve it by 2031. Indeed, the problem may not be solvable at all, and as yet they haven’t really put any meaningful effort into trying to figure that out. The result, as we all know, is that they left themselves completely dependent on natural gas from Russia. Now the Russian gas is effectively unavailable, and other potential sources have seen insufficient supply and massive price spikes. Here are a few observations on Germany’s current energy predicament. From Walter Russell Mead in the Wall Street Journal, June 27, “End of the German Idyll”:
As recently as 2020, almost the entire world agreed with the smug German self-assessment that Germany had the world’s most successful economic model, [and] was embarking on the most ambitious—and largely successful—climate initiative in the world. . . . [Now we understand that] German energy policy is a chaotic mess, a shining example to the rest of the world of what not to do. . . . Green energy, despite massive German investment, will be unable to supply German industry with reliable and cheap power for a long time.
From Energy Intelligence Group, June 28, “King Coal Makes Comeback in Europe”:
[German] officials are working on emergency laws that would allow roughly 9-10 gigawatts of idle coal and lignite capacity to return to service until 2024, replacing some of the 16% market share now held by gas. The country is home to seven of the EU’s 10 most polluting power stations, according to NGO Ember. . . . Economy Minister Robert Habeck said laws allowing more coal use and less gas-fired generation should pass the Bundesrat — upper house of parliament — in early July. . . . The government says there are no plans to change the coal phase-out date, with the last units still earmarked for closure by 2030.
It’s a complete reversal of the prior policy of shutting down the coal plants. Economy Minister Habeck says that the reversal is temporary, and that they are still on track to close all the coal plants by 2030. And how exactly are they going to accomplish that, with all of 9 GWH of grid-scale energy storage? There is only one possible method, which is to go back to natural gas, either using alternative suppliers (U.S.?), or because Russia re-enters the good graces of the world. But using natural gas for backup is just as much a complete abandonment of the “net zero” fantasy as is using coal.
So I say that Germany has in fact hit the “green energy wall,” and will not be going back, no matter what they are saying at the moment. Time could prove me wrong, but I don’t see any realistic plans that they have in the works to do away with, or even meaningfully reduce, full fossil fuel backup of their wind and solar generators.
Computing Forever | July 1, 2022
Sources:
https://www.irishmirror.ie/news/irish-news/fifth-wave-latest-covid-19-27342285
Sources:
Women’s Health and COVID-19: FLCCC Weekly Update (June 15, 2022): https://odysee.com/@FrontlineCovid19CriticalCareAlliance:c/Weekly_Webinar_June15#d
By Megan Redshaw | The Defender | June 30, 2022
Three physicians are suing Twitter, alleging the company violated its own terms of service and community standards when it suspended their accounts for posting “truthful statements regarding COVID-19 policy, diagnosis and/or treatment.”
Drs. Robert Malone, Peter McCullough and Bryan Tyson on Monday filed the lawsuit in Superior Court in California, San Francisco County.
The complaint alleges Twitter breached the terms of its contract when it permanently suspended the plaintiffs’ accounts, silenced their voices and failed to provide them with “verified” badges.
Plaintiffs allege Twitter’s actions were a substantial factor in causing them harm, and are asking the judge to order Twitter to reactivate their accounts.
All three doctors are represented by attorneys Bryan M. Garrie and Matthew P. Tyson (no relation to the plaintiff, Bryan Tyson).
Matthew Tyson on May 12, sent a letter to the directors and managing agents of Twitter requesting the company reinstate the accounts of five physicians, including the plaintiffs, and provide them with “verified” badges. Twitter failed to respond.
In the letter, Matthew Tyson acknowledged Twitter is a “private company” and its terms state it can “suspend user accounts for any or no reason.”
“However, Twitter also implemented specific community standards to limit COVID-19 misinformation on the platform, and Twitter was bound to follow those terms,” he added.
According to the complaint, Twitter’s content-moderation terms included removal procedures for ineffective treatments and false diagnostic criteria, and measures for “labeling” information as “misleading.”
Twitter has a “five-strike policy” as part of its COVID-19 misinformation guidelines and community standards.
Twitter’s website states:
“The consequences for violating our COVID-19 misleading information policy depend on the severity and type of the violation and the account’s history of previous violations. In instances where accounts repeatedly violate this policy, we will use a strike system to determine if further enforcement actions should be applied.”
Strike 1 is “no account-level action.” Strike 2 results in a 12-hour account lock. Strike 3 results in another 12-hour account lock. Strike 4 results in a seven-day account lock and five or more strikes lead to permanent suspension.
Plaintiffs claim they relied on Twitter to employ and enforce its terms in good faith and it was foreseeable to Twitter that plaintiffs would rely on the terms the company is obligated to follow.
According to the complaint, a “truthful tweet regarding COVID-19 policy, diagnosis and/or treatment” would not violate Twitter’s terms of service, community standards, content moderation policies or misinformation guidelines.
“None of these physicians posted false or misleading information, nor did they receive five strikes before suspension,” Matthew Tyson stated in his letter to Twitter.
“It’s no accident that Twitter violated its own COVID-19 misinformation guidelines and suspended the accounts of Drs. Zelenko, Malone, Fareed, Tyson and McCullough,” he wrote.
The letter stated:
“Twitter received express and implied threats from government officials to censor certain viewpoints and speakers, lest Twitter face the amendment or revocation of Section 230, or antitrust enforcement. This was a financial decision for Twitter.
“For the sake of profits, it chose to abandon its role as a neutral internet service provider and instead openly and intentionally collude with government to silence lawful speech.”
In an email to The Defender, lead attorney Garrie and co-counsel Matthew Tyson said:
“In this political climate, honesty is a rare commodity, and concerns over new and experimental vaccines and drug therapies and the safety and effectiveness of alternative outpatient treatments should be the subject of full and transparent public debate.
“Drs. Malone, Tyson and McCullough are highly qualified and credentialed physicians and scientists who posted truthful information on Twitter that contradicted the mainstream narrative regarding COVID-19 policy, diagnosis, and treatment.
“They shared fact-based information which furthered an important public interest as people around the world try to decide how to treat themselves and their loved ones for COVID-19. Twitter silenced them.
“Our clients seek to hold Twitter liable not as a Section 230 publisher, but as a counterparty to a contract, as a promisor who has breached the very terms it put in place to moderate tweets. We will hold Twitter accountable in court and prove the truth of our clients’ statements for the world to see.”
Twitter refused to verify physicians’ accounts
In addition to being suspended from Twitter, the company refused to verify the plaintiffs’ accounts even though the accounts met Twitter’s criteria for verification.
To be verified, an account must be “notable and active.”
Twitter defines a notable account to include “activists, organizers, and other influential individuals,” including “prominently recognized individuals.”
According to the complaint, Malone is an “internationally recognized scientist and physician” who completed a fellowship at Harvard Medical School as a global clinical research scholar and was scientifically trained at the University of California and Salk Institute Molecular Biology and Virology laboratories.
Malone is the “original inventor of mRNA vaccination technology, DNA vaccination and multiple non-viral DNA and RNA/mRNA platform delivery technologies,” and has “roughly 100 scientific publications, which have been cited more than 12,000 times.”
He holds an “outstanding” impact factor rating on Google Scholar and sits as a non-voting member on the National Institutes of Health [Accelerating COVID-19 Therapeutic Interventions and Vaccines] committee, which is tasked with managing clinical research for a variety of drug and antibody treatments for COVID-19.
The complaint states Malone used his Twitter account to post truthful statements regarding COVID-19 policy, diagnosis and/or treatment. He received no strikes for his content and he did not violate Twitter’s rules, yet his account was permanently suspended.
McCullough, according to the complaint, is a highly accomplished physician who is the founder and current president of the Cardiorenal Society of America.
He has been “published more than 1,000 times, made presentations on the advancement of medicine across the world and has been an invited lecturer at the New York Academy of Sciences, the National Institutes of Health, U.S. Food and Drug Administration and the European Medicines Agency.”
McCullough has also served on the editorial boards of multiple specialty journals and was a member or chair of data safety monitoring boards of 24 randomized clinical trials.
He was a “leader in the medical response to COVID-19, has more than 30 peer-reviewed publications on the infection, and has commented and testified extensively on COVID19 treatment, including before the U.S. Senate Committee on Homeland Security and Governmental Affairs,” the lawsuit states.
McCullough’s account was suspended, but Twitter allowed him to create a new account that is followed by more than 480,000 people. Yet, he is still unable to receive a “verified” badge.
In a June 28 tweet, McCullough said “trouble is on the horizon for the “common carrier” whose only role is to provide a platform for communications operations,” referring to the lawsuit.
Tyson is a licensed physician with15 years of hospital and emergency medicine experience. He practices with Dr. George Fareed, who also was suspended from Twitter for posting what he claimed was truthful COVID-19 information.
Tyson and Fareed have “gained international recognition for providing successful early treatment to more than 10,000 COVID-19 patients, with zero patient deaths when treatment was started within 7 days,” the complaint states.
Tyson testified in various proceedings about early treatment protocols and co-authored a book about COVID-19.
He also ran as a candidate for the U.S. House of Representatives for California’s 25th Congressional District, yet was not deemed a “notable figure of public interest” regarding COVID-19 policy, diagnosis and/or treatment, which prohibited him from obtaining a “verified” badge on Twitter.
Tyson says he posted only truthful statements about COVID-19 policy, diagnosis and/or treatment with his account, and none of his tweets were classified as a “strike” or violated Twitter’s terms of service.
Like Malone’s, Tyson’s and Fareed’s accounts were permanently suspended.
“In a nutshell, these are five [physicians] of the most knowledgeable and helpful voices in the world regarding COVID-19 treatment,” Matthew Tyson wrote in his letter. “Disturbingly, Twitter silenced all of them.”
Megan Redshaw is a staff attorney for Children’s Health Defense and a reporter for The Defender.
© 2022 Children’s Health Defense, Inc. This work is reproduced and distributed with the permission of Children’s Health Defense, Inc. Want to learn more from Children’s Health Defense? Sign up for free news and updates from Robert F. Kennedy, Jr. and the Children’s Health Defense. Your donation will help to support us in our efforts.
By Michael Nevradakis, Ph.D. | The Defender | June 30, 2022
Just a few months into the COVID-19 pandemic — and almost two years before global health officials warned of a food shortage crisis — the Rockefeller Foundation issued a report predicting the crisis and offering up solutions, including “shifts to online enrollment, online purchasing of food.”
In a report published July 28, 2020, “Reset the Table: Meeting the Moment to Transform the U.S. Food System,” the foundation described “a hunger and nutrition crisis … unlike any this country has seen in generations.”
The authors blamed the crisis on COVID-19.
The report concluded the crisis would have to be addressed not by strengthening food security for the most vulnerable, but by revamping the entire food system and associated supply chain — in other words, we would need to “reset the table.”
The Rockefeller Foundation called for this food system “reset” less than two months after the World Economic Forum (WEF), on June 3, 2020, revealed its vision for the “Great Reset.”
Some of the contributors to the Rockefeller Foundation report are WEF members; a few of which, along with other proponents of “resetting the table,” also have ties to entities pushing vaccine passports and digital ID schemes.
Rockefeller Foundation: ‘changes to policies, practices, and norms’ are needed
The WEF describes the Rockefeller Foundation as a “science-driven” philanthropic organization that “seeks to inspire and foster large-scale human impact that promotes the well-being of humanity around the world” and which “advances the new frontiers of science, data, policy and innovation to solve global challenges related to health, food, power and economic mobility.”
In the foreword to its 2020 “Reset the Table” report, foundation President Dr. Rajiv J. Shah, who is a former administrator of the U.S. Agency for International Development (USAID), states:
“America faces a hunger and nutrition crisis unlike any this country has seen in generations.
“In many ways, Covid-19 has boiled over long-simmering problems plaguing America’s food system. What began as a public health crisis fueled an economic crisis, leaving 33 percent of families unable to afford the amount or quality of food they want.
“School closures put 30 million students at risk of losing the meals they need to learn and thrive.”
The report did not explain how the Rockefeller Foundation was able to know about this food crisis mere months after the pandemic took hold — especially as the report states it was developed out of “video-conference discussions in May and June 2020.”
The report also didn’t provide any insight into the role pandemic countermeasures such as lockdowns — which the foundation championed along with the WEF — played in contributing to the food crisis.
In its report, the Rockefeller Foundation proposes a series of solutions, derived from “dialogues with over 100 experts and practitioners.”
One recommendation calls for moving away from a “focus on maximizing shareholder returns” to “a more equitable system focused on fair returns and benefits to all stakeholders — building more equitable prosperity throughout the supply chain.”
This may sound like a good idea, until one considers “stakeholders” in this case refers to “stakeholder capitalism” — a concept heavily promoted by the very same large corporations that have been beneficiaries of the shareholder capitalist system.
The WEF also heavily promotes “stakeholder capitalism,” defining it as “a form of capitalism in which companies seek long-term value creation by taking into account the needs of all their stakeholders, and society at large.”
For some context, economic fascism, as personified by the regimes of Nazi Germany and fascist Italy, encompassed government-mandated “partnerships” between business, government and unions organized by a system of regional “economic chambers,” and a philosophy where “the common good comes before the private good.”
It is, of course, unclear how the “needs [of] society at large” are determined — or by who.
The Rockefeller Foundation report declares, “Success will require numerous changes to policies, practices, and norms.”
What does such “success” entail? The report names three main objectives:
The report describes the lack of universal broadband access in this context as “a fundamental resiliency and equity gap.”
These objectives, dressed up in “inclusive” language, are further described in the report as being beneficial to human health, ensuring “healthy and protective diets” that “will allow Americans to thrive and bring down our nation’s suffocating health care costs.”
The report goes as far as to describe this as a “legacy” of COVID-19, even predicting that doctors will “prescribe” produce for patients.
According to the report:
“One of Covid-19’s legacies should be that it was the moment Americans realized the need to treat nutritious food as a part of health care, both for its role in prevention and in the treatment of diseases.
“By integrating healthy food into the health care system, doctors could prescribe produce as easily as pharmaceuticals and reduce utilization of expensive health services that are often required because of nutrition insecurity.”
But as Dr. Joseph Mercola pointed out, despite this purported emphasis on healthy, nutritious food, the words “organic,” “natural” and “grass fed” do not appear in the report.
What does appear is the phrase “alternative proteins,” in this case referring to proteins derived from the consumption of insects — another concept promoted by the WEF.
In 2021, for instance, the WEF published a report titled “Why we need to give insects the role they deserve in our food systems,” suggesting that “insect farming for food and animal feed could offer an environmentally friendly solution to the impending food crisis.”
Yet again, an “impending food crisis” is forecast, which may lead some to ask how entities such as the Rockefeller Foundation and the WEF even knew what was coming.
As stated by Mercola:
“COVID was declared a pandemic March 11, 2020, so by the time this Rockefeller report was published, the pandemic had only existed for four months, and while certain high-risk groups did experience food insecurity, such as children whose primary meal is a school lunch, widespread food shortages, in terms of empty shelves, were not widely prevalent or particularly severe in the U.S.
“It seems nothing escapes the prophetic minds of the self-proclaimed designers of the future. They accurately foresee ‘natural disasters’ and foretell coincidental ‘acts of God’. They know everything before it happens.
“Perhaps they truly are prophets. Or, perhaps they’re simply describing the inevitable outcomes of their own actions.”
Mercola suggests such crises are inevitable because they are part of “an intentional plan” by the very same actors.
The Rockefeller Foundation’s amazing ‘predictions’ of future crises, and its ties with Big Tech and Big Pharma
Lending credence to Mercola’s view, and as recently reported by The Defender, the Rockefeller Foundation, WEF and other entities accurately predicted a remarkable number of crises that then came to pass.
For instance, Event 201, held in October 2019 and co-organized by the Rockefeller Foundation, accurately “predicted” the global outbreak of a coronavirus.
Similarly, the Nuclear Threat Initiative (NTI), which co-organized a “tabletop simulation” predicting the global outbreak of monkeypox in March 2021, with an imaginary start date of May 2022, has received $1.25 million in grants from the Rockefeller Foundation since January 2021.
In turn, the other co-organizer of the monkeypox “tabletop simulation,” the Munich Security Conference, in May 2022 held a roundtable with the Rockefeller Foundation on “Transatlantic cooperation on food security.”
Among the suggestions arising from this roundtable include a “focus on transforming the global food system and making it more resilient to future shocks, with steps taken now and over the long term.”
The Rockefeller Foundation is also a partner and board member and donor to GAVI: The Vaccine Alliance — alongside the WEF, the Bill & Melinda Gates Foundation and the Johns Hopkins Bloomberg School of Public Health, which hosted Event 201.
As previously reported by The Defender, the GAVI Alliance proclaims a mission to “save lives and protect people’s health,” and states it “helps vaccinate almost half the world’s children against deadly and debilitating infectious diseases.”
GAVI is also a core partner of the World Health Organization (WHO).
The GAVI Alliance — and the Rockefeller Foundation — also work closely with the ID2020 Alliance. Founded in 2016, ID2020 claims to advocate in favor of “ethical, privacy-protecting approaches to digital ID,” adding that “doing digital ID right means protecting civil liberties.”
As reported previously by The Defender, ID2020’s founding partners include the Rockefeller Foundation, GAVI, UNICEF, Microsoft, the Bill & Melinda Gates Foundation and the World Bank, while general partners of ID2020 include Facebook and Mastercard.
For the past two years, the Rockefeller Foundation and entities such as ID2020 and the WEF have been closely involved with the push for digital “vaccine passports.”
For instance, on July 9, 2020, the Commons Project, itself founded by the Rockefeller Foundation, launched “a global effort to build a secure and verifiable way for travelers to share their COVID-19 status” — that is, a vaccine passport.
The Commons Project also was behind the development of the CommonPass, another vaccine passport initiative, developed in tandem with the WEF.
In turn, the Good Health Pass was launched by ID2020, as part of a collaboration between Mastercard, the International Chamber of Commerce and the WEF. It was endorsed by embattled former U.K. Prime Minister Tony Blair, now executive chairman of the Tony Blair Institute for Global Change.
Other members of the Good Health Pass Collaborative include Accenture, Deloitte and IBM — which developed New York’s “Excelsior Pass” vaccine passport system.
The Rockefeller Foundation, along with the Bill & Melinda Gates Foundation, also funded an August 27, 2021 document issued by the WHO titled, “Digital documentation of COVID-19 certificates: Vaccination status.”
The document is described as follows:
“This is a guidance document for countries and implementing partners on the technical requirements for developing digital information systems for issuing standards-based interoperable digital certificates for COVID-19 vaccination status, and considerations for implementation of such systems, for the purposes of continuity of care, and proof of vaccination.”
And in another remarkably prescient “prediction,” the Rockefeller Foundation, in 2010, published a report — “Scenarios for the Future of Technology and International Development” — which presented four future scenarios.
One of these hypothetical scenarios was “Lock Step” — described as “[a] world of tighter top-down government control and more authoritarian leadership, with limited innovation and growing citizen pushback.”
The description of this “Lock Step” scenario goes on to state:
“Technological innovation in ‘Lock Step’ is largely driven by government and is focused on issues of national security and health and safety.
“Most technological improvements are created by and for developed countries, shaped by governments’ dual desire to control and to monitor their citizens.”
This scenario also predicted “smarter” food packaging:
“In the aftermath of pandemic scares, smarter packaging for food and beverages is applied first by big companies and producers in a business-to-business environment, and then adopted for individual products and consumers.”
Moreover, the “Lock Step” scenario remarkably predicted China would fare better than most countries in a hypothetical pandemic, due to the heavy-handed measures it would implement:
“However, a few countries did fare better — China in particular.
“The Chinese government’s quick imposition and enforcement of mandatory quarantine for all citizens, as well as its instant and near-hermetic sealing off of all borders, saved millions of lives, stopping the spread of the virus far earlier than in other countries and enabling a swifter post-pandemic recovery.”
The Rockefeller Foundation’s involvement in public health is not new.
Going back more than a century, the foundation heavily promoted “scientific medicine” and formalized medical practice based on the European model on a global scale, at the expense of homeopathy and other traditional and natural remedies.
The foundation’s “philanthropic” activities have been described as “de facto colonialism in countries including China and the Philippines.”
Moreover, the foundation helped give rise to the first global public health entities, the International Health Commission (1913-16) and the International Health Board (1916-1927).
It also helped finance the earliest public health programs at universities such as Harvard and Johns Hopkins — today home to the Johns Hopkins Bloomberg School of Public Health.
Michael Nevradakis, Ph.D., is an independent journalist and researcher based in Athens, Greece.
© 2022 Children’s Health Defense, Inc. This work is reproduced and distributed with the permission of Children’s Health Defense, Inc. Want to learn more from Children’s Health Defense? Sign up for free news and updates from Robert F. Kennedy, Jr. and the Children’s Health Defense. Your donation will help to support us in our efforts.
That’s why PAXLOVID does not work for them
By Igor Chudov | June 30, 2022
A new study just came out:

It looked at how long “culturable virus” (that is, virus capable of infecting people) is present in Covid patients after the first positive test. The authors literally cultured swabs of patients, on various days past-diagnosis, and counted how many patients, by vaccination status, are still carrying live, replication-competent virus.
The result is shocking:

What this chart shows is that one-third of boosted people still carried live, culturable virus at 10 days after the beginning of the infection. This is contrasted with unvaccinated people, who had only 6% of persons still contagious at Day 10.
This means that the share of boosted people who are still contagious (31%) is over five times greater, than the share of still-contagious unvaccinated people (6%).
In other words: out of 100 boosted persons who catch Covid, fully one-third will be still carrying LIVE VIRUS on Day 10. Out of 100 unvaccinated persons, only one out of 16 would test positive on Day 10 — over five TIMES fewer people.
As a word of warning, the study involved a relatively small amount of people, so statistical significance is probably not quite what we’d like it to be — but it shows what we saw all along in other news.
It also means that boosted people, who might feel better in a few days, would be contagious for a few MORE days after recovery, thus becoming silent superspreaders of Covid. So much for “stopping the spread”!
This is why Paxlovid does Not Work for the Boosted
This study explains why Paxlovid does not work in vaccinated (and boosted) people. For the introduction into my paxlovid series, see the sad story of double-boosted Dr. Fauci, who relapsed on Paxlovid, with links to my Paxlovid articles shown chronologically:
What Paxlovid is, is a biomolecular “snooze button” that suspends viral replication for 5 days. However, as we can see, one-third of the boosted people still carry live virus at 10 days due to delayed, or disabled, immune responses. Those persons would be likely to rebound on Paxlovid.
The numbers also match other calculations: my guesstimate of unvaccinated Paxlovid rebound was 12% — that is not too far from 6% of unvaccinated people in this study who carried live virus on Day 10. 31% of boosted people who still have live virus on Day 10, matches Twitter reports of 40-50% rebound rates in vaccinated people.
In other words, while we had fairly certain evidence that Paxlovid does not work for vaccinated people, and suspected the vaccine, we were missing the most crucial proof: that of live virus not clearing in the boosted. The study I mentioned above, provides this proof.
It also exposes vaccines as merely “increasing tolerance” to Sars-Cov-2, as opposed to generating robust immune response that leads to rapid viral clearance.
Molnupiravir
I personally have not paid close attention to Merck’s Molnupiravir, due to it being a dead-end, mutagenic, cancer-causing, variant-generating, toxic-to-bones drug from hell, which is, fortunately, seeing little use. Our friend Modern Discontent discovered that Molnupiravir is also snake oil and does not work in vaccinated people.
Getting boosted is a great way to become unable to clear a Covid infection in 10 days and become a Covid superspeader.
Samizdat | July 1, 2022
The state of Alabama has called on a federal court to uphold a ban on so-called gender-affirming medical treatments for transgender youths, citing a recent Supreme Court ruling that allowed state governments to prohibit abortions.
In a 76-page brief filed with the 11th US Circuit Court of Appeals on Monday, Alabama Attorney General Steve Marshall insisted that a previous injunction on the state’s ban of transgender treatments should be overturned, since such care is not protected under the 14th amendment to the US Constitution as it is not “deeply rooted in the nation’s history and traditions.”
“The Legislature determined that transitioning treatments in particular are too risky to authorize, so it is those treatments Plaintiffs must show the Constitution protects,” the brief says. “But no one –adult or child– has a right to transitioning treatments that is deeply rooted in our nation’s history and tradition.”
The state’s argument closely resembles the reasoning behind the recent US supreme court decision to overturn Roe v. Wade, which removed federal abortion protections and placed the responsibility for legalizing or banning the procedure on individual states and their citizens.
Supreme Court judges that ruled in favor of overturning the legislation argued that terminating a pregnancy was not a fundamental constitutional right because it was not explicitly mentioned in the US constitution and was not “deeply rooted in this nation’s history and tradition.”
In the brief, Marshall goes on to insist that the Constitution reserves to the state, and not courts or medical interest groups, the authority to determine that “sterilizing interventions” are too dangerous for minors, adding that the State has a right to regulate or prohibit such interventions for children “even if an adult wants the drugs for his child.”
The Attorney General also noted that research regarding these “novel interventions” was poor and that they were unproven to offer lasting relief to children suffering from gender-related distress. “What research does exist is already outdated – a remarkable fact given that the seminal study on transitioning children was published less than a decade ago and has not been replicated,” he added.
Marshall also drew attention to the fact that gender-related distress has become “a tsunami” as clinics offering “‘transitioning’ treatments on kids are seeing their patient loads increase by thousands of percent,” noting that the new trend was “troubling.”
In April, Alabama governor Kay Ivey signed into law a bill which made it a felony to provide gender-affirming treatments to minors, and sought a 10-year prison sentence and a $15,000 fine for anyone providing puberty blockers, hormones or surgical procedures to transgender youths under the age of 19.
However that legislation was partially blocked one month later by a federal judge, who dismissed the state GOP leader’s claim that puberty blockers were “experimental,” and insisted that transitioning medications were “well-established, evidence-based treatments for gender dysphoria in minors” endorsed by “at least 22 major medical associations.”
By Megan Redshaw | The Defender | June 29, 2022
The U.S. Food and Drug Administration’s (FDA) vaccine advisory panel on Tuesday voted 19 to 2 to recommend new COVID-19 booster shots that include the Omicron variant this fall.
The FDA’s Vaccines and Related Biological Products Advisory Committee (VRBPAC) did not issue guidance on whether additional data would be needed to recommend an updated composition of the primary-series vaccines authorized for emergency use in the U.S., or whether it would be appropriate to continue to use a primary-series vaccine as a booster.
It is the first time VRBPAC has suggested vaccine makers modify their vaccines to target a different variant, according to CNBC, which also reported the FDA will likely accept the committee’s recommendation.
If so, the FDA would be authorizing a vaccine change without requiring additional data showing a bivalent vaccine — containing both the original 2019 Wuhan variant and one of the Omicron variants — is safe and effective for those age groups that are already authorized to receive a booster dose.
The FDA plans to decide by early July whether vaccines will target the now-dominant BA.4 and BA.5 Omicron subvariants or the BA.1 Omicron variant that led to a surge in infections last winter, Reuters reported.
At the beginning of the meeting, Dr. Peter Marks, director of the FDA’s Center for Biologics Evaluation and Research, suggested a newly designed shot could begin in October, adding that it takes manufacturers around three months to choose a vaccine design and begin producing doses.
Dr. Paul Offit, director of the Vaccine Education Center and professor of pediatrics in the Division of Infectious Diseases at Children’s Hospital of Philadelphia, and Dr. Hank Bernstein, professor of pediatrics at Zucker School of Medicine, were the only two members who broke from the panel to vote against the initiative.
Offit acknowledged there’s a benefit to providing a booster in the fall to some age groups, but questioned whether Omicron was the right strain. He said the move to new-variant vaccines was happening too fast, with too little data.
“I think as a new product it should be handled as a new product,” Offit said. “I think we need a higher standard than what we’ve been given. …“I’m not comfortable enough to support the risk of a new product.”
Bernstein expressed concern over the lack of data used to justify changing the strain, and the potential that by the time a subsequent booster is approved, it will contain outdated strains.
“So, in sum, I think including an Omicron strain in the vaccine seems to have some potential, but data especially for BA.4 and BA.5 are limited at this time, and that’s why I’m struggling to even make a strain change at this time,” Bernstein said.
Bernstein also said he didn’t see a need to change the strain as the current vaccine being used is shown to be effective against severe disease — a claim made just two weeks earlier at a prior VRBPAC meeting.
Bernstein said the strain change would need to be supported by data showing improved vaccine effectiveness and he “didn’t think we really have the data to be able to say that” even though the panel looked at the immune response.
Dr. Ofer Levy, VRBPAC member and an infectious disease physician at Boston Children’s Hospital, voted “yes” to change the computation of COVID-19 boosters, despite Pfizer’s admission there is “no established correlate of protection,” referring to the level of antibodies needed to confer protection.
“You have a lot of data now,” Levy told Pfizer. “What is your relative protection?”
“I would say there is no established correlate of protection,” Kena Swanson, Ph.D., vice president of viral vaccines at Pfizer, told Levy.
Levy circled back during the meeting:
“I would like to hear from FDA what their overall approach will be around improving our understanding of correlate protection. We spend a good amount of time reviewing antibody data. We have no doubt antibody data is important. We don’t have a level of antibody that anybody is comfortable stating is correlated [with] protection.
“So yes, the antibodies are important but so are the T cells. We heard from Dr. Weir, yes, T-cell assays are trickier and they’re more diverse, but it’s not going to happen without federal leadership to have a standardization of the T-cell assay and encourage or in fact require the sponsors to gather that information.”
“So what is the effort to standardize the pre-clinical assays?” Levy asked. “This is an effort that’s critical not just now but for future cycles of vaccine revision. If we aren’t able to define a standard for correlate protection we are fighting with one arm behind our back.”
Marks acknowledged the importance of Levy’s question, but said T-cell-mediated immunity was “difficult to study” initially.
“We have been having conversations with our colleagues at the NIH [National Institutes of Health] and throughout government about how we might move forward here,” Marks said. “It is something that we don’t have an answer to yet.”
Marks said as vaccines are developed in the future, it will “become even more important” to define a standard of correlate protection because “we won’t be able to have a large naive population to vaccinate with newer vaccines.”
“We will need to understand the T-cell response better,” Marks said. “I take your point, it’s just that we haven’t solved the problem yet.“
Dr. Meryl Nass, a member of the Children’s Health Defense scientific advisory committee, told The Defender that in her opinion, Tuesday’s meeting was a “vote to essentially approve a future framework — the future framework being a dearth of evidence required to change the booster, without clinical evidence and without a correlation of protection.”
Nass added:
“They voted on using an Omicron variant in the next booster iteration — which could contain any Omicron variant and could be either mono- or bi-valent.
“But most likely they will keep the current version and add another — which might double the amount of mRNA, or not.”
The new formulation might be for adults alone or adults and children, or only older adults and the immunocompromised, Nass said.
Brian Hooker, Ph.D., Children’s Health Defense chief scientific officer and professor of biology at Simpson University, told The Defender :
“The proposed move by VRBPAC will increase the harm to the U.S. public to unprecedented levels, as this action will further circumvent necessary clinical trials even beyond the slapdash testing of COVID-19 vaccines under Emergency Use Authorization.
“This adds to a foundation of lies used to authorize the original COVID-19 vaccines without anywhere near proper testing.”
Dr. Cody Meissner, VRBPAC panel member and professor of pediatrics at Tufts University, expressed concern about the financial risk pharmaceutical companies “are taking by making these vaccines.”
“If there’s a low likelihood the vaccines will be recommended, then they could incur significant loss,” he said.
Marks responded:
“I guess I would say that I would make recommendations here knowing the vaccine manufacturers will be kept whole by the United States government at least for some vaccines. I could be wrong but I think that’s a reasonable assumption.”
During the meeting, Moderna told the panel it would be ready with a “couple of hundred million” bivalent, or double-targeted, vaccines designed to combat BA.1 by September, but it would be late October or early November if the company needs to design a new vaccine targeting subvariants.
Pfizer said it and partner BioNTech have a significant amount of vaccine doses designed for the BA.1 variant ready and are already preparing to produce a large number of doses targeting BA.4 and BA.5 Omicron subvariants.
Pfizer said either could be ready for an early October rollout.
Multiple concerns raised during the public comment session
During the public comment session of the meeting, experts raised concerns that were largely ignored by the advisory panel.
Dr. Dustin Bryce, with Interest of Justice, said the FDA, Centers for Disease Control and Prevention (CDC) and the World Health Organization are “usurping Congress’ definition of a vaccine — which is any substance designed for the prevention of one or more disease.”
“FDA actually classifies mRNA as gene therapy, which they say is to treat or cure an existing disease by modifying your genes,” Bryce said. “Gene therapies are still being studied and are experimental at this time.”
Citing FDA documents, Bryce said gene therapy, unlike a vaccine, is so inherently unsafe the FDA says it requires 15 years of research to follow up on safety due to known risks of antibody-dependent enhancement, alteration of DNA and delayed adverse effects, such as cancer.
Bryce said:
“FDA says that gene therapy use in the mass population represents an unreasonable risk and they should limit the number of subjects who might be exposed to risk. We require due process and forbid the FDA from authorizing the proposed changes.
“We are demanding that EUA [Emergency Use Authorization] is promptly revoked because unreasonable risks are inherent in gene therapy products, as evidenced by large numbers of reports of adverse serious events linked to or suspected of being caused by an EUA product, product failure and product ineffectiveness.”
Bryce said COVID-19 vaccines fail to meet the requirements of EUA because not a single mRNA vaccine has been found to be effective for the prevention or treatment of an existing disease.
Michael Briskin pointed out in his public comment that the FDA receives approximately 75% of its budget from pharmaceutical companies, which he believes represents a conflict of interest.
Briskin challenged the use of the phrase “safe and effective” to describe COVID-19 vaccines, given the FDA has done no long-term testing to determine whether these products are safe.
Briskin presented data showing a significant rise in reported deaths among working-age Americans following COVID-19 vaccine mandates.
He said:
“In the short-term, 2021 was a very interesting year. We saw a stark increase [in death] among working-age adults from 18 to 64 and specifically in Q3 and into Q4, so something new for the working-age demographic partly through 2021 would be the clear correlation.
“With comparable trends in BLS [Bureau of Labor Statistics] data, children’s health insurance data, Israeli ambulance data, and of course we have the [Vaccine Adverse Event Reporting System (VAERS)] data — which the CDC tried to minimize but a recent FOIA [Freedom of Information Act] request forced them to reveal that they never once did the PRR calcification that was supposed to be their tool for spotting safety signals, according to their posted documents.”
“And what do we do when people get injured from these vaccines?” Briskin asked the panel. “We leave them in the mud.”
Briskin chastised the panel for authorizing boosters for infants two weeks earlier when data showed two doses weren’t effective and only 10 cases were used to assess efficacy.
“Three-quarters of the severe COVID in the trial was in the vaccine arm, as was the only hospitalization case which was accompanied by a seizure,” Briskin said. “And Moderna is so dangerous in young people Nordic countries won’t allow it to be used in anyone under the age of 30.”
Briskin said:
“In fact, the director of health of Denmark just admitted that vaccinating children was a mistake, whereas our officials only ever doubled down. And now we’re about to double down so hard we are about to lose the pretense of holding these pharmaceutical companies to any statistically meaningful regulatory standards for formula modification.
“For people following at home, what this agency is proposing is not just modifying the genetic code in the vaccine and the structure of the proteins produced to chase variants, but even things like doubling the microgram count for Pfizer — all without doing any statistically powered safety studies.”
“And to be clear,” Briskin added, “the companies we’re giving carte blanche to include Pfizer, the world’s largest criminal organization having paid the world’s largest criminal fine, and Moderna, which never made a safe product before we did away with long-term safety testing.”
Dr. Eric Feintuch, a chiropractor, asked the FDA if the agency knows how long mRNA from COVID-19 vaccines and the spike protein stay in the body, whether they know what the rate of protein production is and whether the FDA is aware of the consequences of the methylpseudouridine substitutions at the codon optimization step.
“For anyone on this panel who says it doesn’t go anywhere, tell me what proof you have of that,” Feintuch said, referring to the spike protein.
Feintuch said COVID-19 vaccines are associated with prion disease, noting 26 people have reported experiencing sudden onset of a severe and fatal brain disorder within one month of the second mRNA vaccine dose.
“This information needs to be researched and seen,” Feintuch said.
“A thousand peer-reviewed studies question the safety of COVID-19 vaccines. Doesn’t anyone see the safety signals? Is there anyone here who will stand up?” he asked. “Some of you know this, you need to stand up and you need to help us.”
Dr. David Wiseman, a research scientist with a background in pharmacy, pharmacology and experimental pathology, said VRBPAC is once again being asked to opine on inadequate information.
Wiseman said the FDA recently waived efficacy requirements for COVID-19 vaccines and has ignored its experts, notably Levy, who “has called for federal efforts to validate and standardize a correlate of protection.”
“Recent vaccine decisions were based on irrelevant Wuhan immunobridging,” Wiseman said. “Omicron assays are unvalidated and unverified by FDA.”
Wiseman said safety questions surrounding COVID-19 vaccines remain unanswered:
“We have shown correlations between vaccination and all-cause mortality. FDA says VAERS is under- and misreported. A FOIA disclosure reveals that CDC has not conducted safety signal analyses, which we have provided to FDA. Neurologic adverse events are finally being acknowledged [but there are] still no cancer studies.”
Wiseman further pointed out that FOIA requests show vital studies involving the spike protein have not been done:
“A Stanford study in [the journal] Cell showed vaccine message and antigen persisting for at least eight weeks. Does spike accumulate? Is this why myocarditis rates after boosting match or best primary series rates for some ages?
“Does spike persistence contribute to immune suppression, imprinting and negative efficacy? What is the toxicity of multiple doses? How will sameness of the manufacturing process be defined? Are the guidelines talking about monovalents or bivalents?”
Pfizer has dismissed concerns about the spike protein as “academic,” Wiseman said, “but it is certainly not.”
Booster formulation should be changed to combat waning efficacy, committee said
During the meeting, which occurred two weeks after the panel signed off on the primary COVID-19 vaccine series for the nation’s youngest children, a change in booster composition was deemed necessary due to waning effectiveness.
Dr. Mahesh Shenai, neurosurgeon and data analyst, said in a tweet:
“After many months of extolling benefits of vax and booster, now they are criticizing its efficacy and durability. . . to set the stage for a new updated booster!?”
In a briefing document published ahead of Tuesday’s meeting, FDA officials predicted a major COVID-19 outbreak will occur in the fall “due to the combination of waning immunity, further evolution of variants and increased indoor activity.”
A similar committee that advises the WHO recently suggested COVID-19 vaccines be reformulated to include both the original SARS-CoV-2 Wuhan variant and the first version of Omicron, BA.1 — although this variant has since been replaced by other strains of BA.4 and BA.5.
Moderna and Pfizer studied Omicron-specific vaccines in preparation for fall boosters, but efforts have been complicated by new subvariants.
If the government decides it wants a booster shot that targets BA.4 and BA.5 — two strains derived from the Omicron variant that are becoming dominant — vaccine manufacturers will have to race to produce the doses by fall, The New York Times reported.
Vaccines produced by Pfizer, Moderna, Novavax and Johnson & Johnson were developed against the original Wuhan COVID strain that emerged in 2019, but as the virus has rapidly evolved, these vaccines have become less effective.
COVID-19 vaccines target the spike protein the SARS-CoV-2 virus uses to invade human cells, but as the virus mutates away from the original strain, it has trouble “recognizing and attacking the spike,” CNBC reported. The Omicron variant has more than 30 mutations.
Marks said during the meeting he hopes changing the booster will “convince people to go get that booster,” adding the FDA plans to begin a booster campaign in October.
Megan Redshaw is a staff attorney for Children’s Health Defense and a reporter for The Defender.
© 2022 Children’s Health Defense, Inc. This work is reproduced and distributed with the permission of Children’s Health Defense, Inc. Want to learn more from Children’s Health Defense? Sign up for free news and updates from Robert F. Kennedy, Jr. and the Children’s Health Defense. Your donation will help to support us in our efforts.
BY WILL JONES | THE DAILY SCEPTIC | JUNE 28 2022
Here we go again. It’s the middle of summer and the leading opinion piece in the Guardian today calls for the return of restrictions in response to rising infections and hospitalisations. In a piece introduced with, “a few small changes would make a big difference to millions of vulnerable people”, journalist Frances Ryan writes:
If you’re reading this in the U.K., odds are that by now you’ve had coronavirus: seven in 10 of us have watched the dreaded red line appear. You may have been stuck in bed with it twice or even three times by now; by April 2022, England alone had recorded almost 900,000 reinfections. When the public asked to “return to normal”, I’m not sure a regular hacking cough was what they had in mind.
Almost 900,000 reinfections? How will 1.6% of the population have coped with getting another cold?
Ryan continues:
It is an odd situation. Last week, Covid infections were reported to have soared by 43%, while hospitalisation from the virus rose by 23%. An estimated 1.7 million people in the U.K. tested positive over those seven days. Two million of us now have long Covid, with about two in five of those – or 826,000 people – having symptoms for at least a year.
What Ryan fails to mention is that Long Covid studies frequently find small to negligible numbers of additional symptoms compared to a control group, meaning the quoted figure is unlikely to be an accurate picture of the real impact of COVID-19.
Ryan again:
Back in February, Johnson said the Government had created a plan to start “living with Covid”, but what it really did was form a plan to catch and spread Covid. After all coronavirus prevention measures were dropped on April 1st – from the legal obligation to isolate if you had Covid, to the end of most free testing – the public were left wide open to mass infection. Even hospitals were told by ministers to ditch mask mandates, though some worried trusts have defied the rules and kept them. That all precautions were pulled back just when most people’s vaccine immunity was beginning to fade, and the virus was evolving to be more transmissible, gives a hint at how little logic ministers applied.
Since Ryan accepts that vaccine protection wanes, she evidently intends restrictions, sorry, precautions to continue indefinitely. Indeed, the plummeting of the infection fatality rate makes no difference to her argument, as “excessive focus” has been placed on deaths, she says.
One of the biggest problems facing Britain’s attempts to quell the virus is that this Government doesn’t really want to. There is hope – the number of people dying from Covid has reduced since its peak – but excessive focus on this has long hidden the fact that loss of life has never been the only thing that matters: how many people are infected with the virus matters too. A strategy that lets the virus rip through the population increases the risk we all face, be it from surges, new dangerous variants, or in developing long Covid. Fundamentally, it means accepting a reality where it is deemed normal for many of us to be (possibly severely) sick, from a virus whose long-term effects – and the effects of repeated reinfection – we still know little about.
Once again, the plight of the vulnerable is deployed to justify indefinite restrictions on everyone – a logic which would destroy most freedoms given the opportunity, as we have seen in the last two and a half years.
There will be few greater casualties though than the 3.7 million clinically extremely vulnerable people, especially the 500,000 who are immunocompromised and can’t get much or any benefit from a booster jab. Trying to avoid the virus in a country that has forgone all safety measures means risking your life when you pop to the shops. Ministers who are content for repeated coronavirus infection to just become part of British life are content for isolation to be part of clinically vulnerable people’s.
What does Ryan propose? The reinstatement of free lateral flow tests – as though there isn’t an economic crisis on, and we haven’t spent enough over-testing ourselves for colds; the return of the legal requirement to isolate for those with a positive test – a measure extremely disruptive to education, employment, health care and everything else; and financial help such as sick pay for those isolating – more magical money. Plus more of the vaccines she has acknowledged don’t work for long.
And, inevitably, masks: “Wearing masks in busy and enclosed spaces again is the right thing to do; just under half of Britons (48%) reported wearing a face covering when outside their home last month, down from about 95% during the January Omicron wave.”
From a sceptical point of view, it’s depressing that nearly half of people still say they’re wearing a mask – though since far fewer than half the people I see out and about are actually wearing a mask, this poll probably reveals more about the biases of polls (and what people say to them) than the reality on the ground.
Then Ryan lays it on thick:
Unless we wish to sign up to getting repeatedly sick for the foreseeable future, and to the risk of long-term disability from long Covid, we are going to have to bring back low-effort protective measures to curb it. A recent public health campaign in Ireland, which encourages people to think of clinically vulnerable people in their daily interactions, shows how easy it is to do things differently.
Former Deputy Chief Medical Officer Jonathan Van-Tam recently said the rise in infections was nothing to worry about and that even he had stopped wearing his face mask. But will he think again now, if respectable opinion starts to shift in the direction Frances Ryan and others would like?
Let’s hope this is just an anomalous op-ed and not the start of a trend. After all, if this is what they’re saying in June, what will they be saying in December?
Vaccine failure in one map
eugyppius | June 28, 2022
Behold the latest map of 7-day Corona incidence across the Federal Republic of Germany:
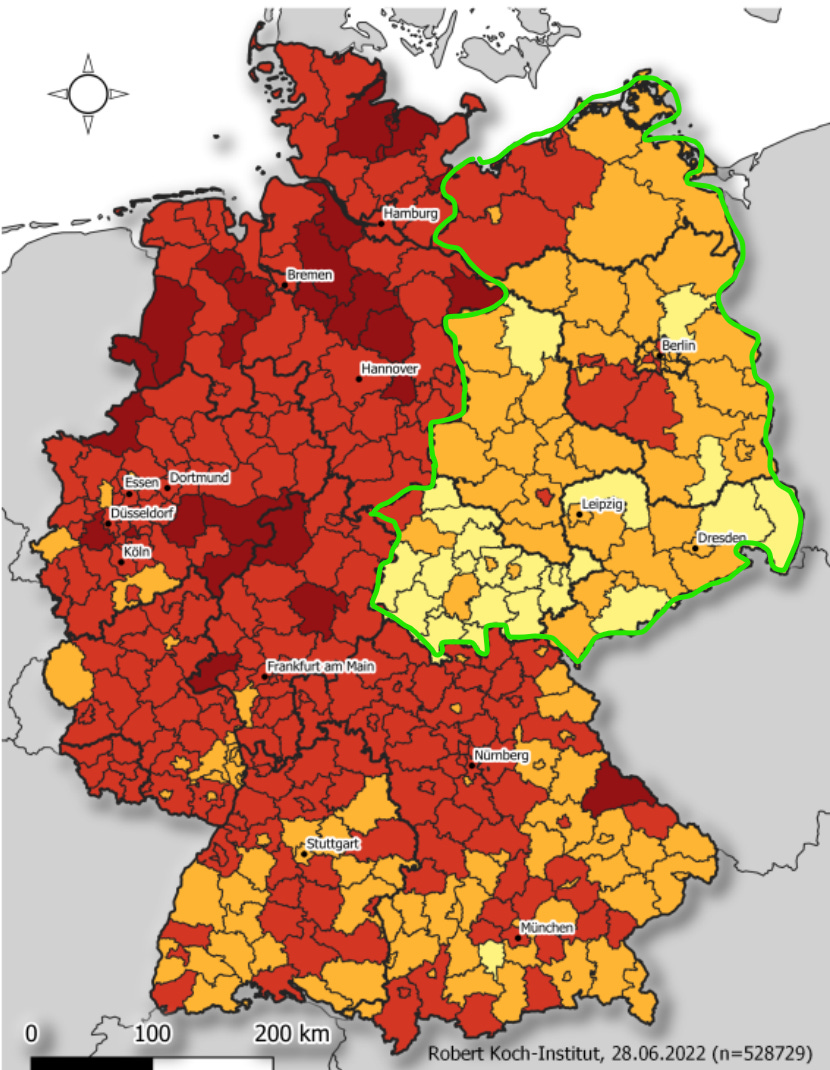
This is the Omicron BA.5 wave in central Europe, and it is attended by a curious phenomenon: Every day, you can see more clearly the borders of the old DDR in the district-level data. I’ve traced these in green just to make the phenomenon clearer.
Yes yes, there are systematic demographic differences between East and West Germans, and there are probably some differences in testing rates, but above all, there is an important difference in vaccine uptake. In this map of triple vaccination rates across my country, the old DDR borders are also evident:
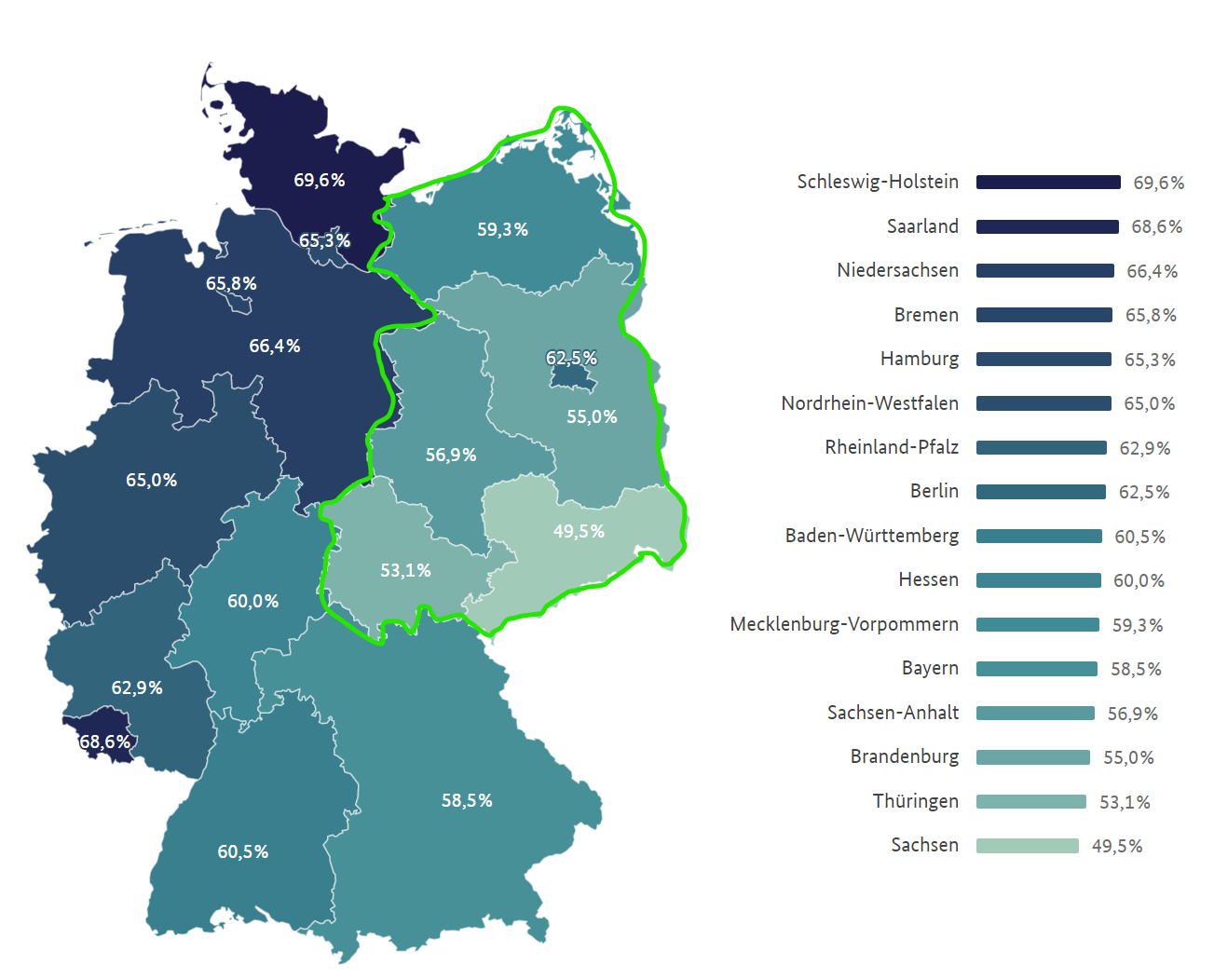
East Germans have direct experience with government propaganda, and have proven more resistent to the vaccination campaign than Westerners. Their reward, after being much maligned by state media, is now higher levels of natural immunity and lower rates of BA.5 infection, which appears to prefer vaccinated populations.
As the effects of vaccine failure grow clearer, you have to wonder how long the pandemicists will be able to publish even simple infection statistics, without raising extremely awkward questions.
See the follow up in depth critique of the theory.

or go to
Aletho News Archives – Video-Images
Involuntary servitude is good for business
By Kurt Nimmo | Another Day in the Empire | April 20, 2026
In 2025, Alex Karp, the CEO of government and military tech contractor Palantir, published The New York Times best-seller, The Technological Republic: Hard Power, Soft Belief, and the Future of the West. The Wall Street Journal praised the book as a cri de coeur, a passionate appeal “that takes aim at the tech industry for abandoning its history of helping America and its allies,” while Wired praised the book as a “readable polemic that skewers Silicon Valley for insufficient patriotism.”
On April 18, 2026, Palantir posted twenty-two points to social media summarizing the book. In addition to taking Silicon Valley to task for insufficient patriotism, advocating a role for AI in forever war, and denouncing the “psychologization of modern politics,” the Palantir post on X declares: “National service should be a universal duty. We should, as a society, seriously consider moving away from an all-volunteer force and only fight the next war if everyone shares in the risk and the cost.”
National conscription, a form of involuntary servitude, and the wars it portends, is good for business, especially for corporations within the orbit of the Pentagon, the CIA, and the national security state. Palantir fits comfortably within this amalgamation. … continue
