MMR (Measles, Mumps and Rubella) – Vaccine Risk Statement
MMR Vaccine (Measles, Mumps, and Rubella) Is It Safer Than Measles, Mumps and Rubella?
Physicians for Informed Consent | December 2024
What Is the MMR Vaccine?
The measles, mumps, and rubella (MMR) vaccine is a live virus vaccine that was introduced in 1963. It has significantly reduced the incidence of reported cases of measles, mumps, and rubella infections; however, vaccine immunity wanes over time.1-3
What Are Side Effect of the MMR Vaccine?
Common side effects of the MMR vaccine include fever, mild rash, and swelling of glands in the cheeks or neck.4 A more serious side effect is seizure, which occurs in about 1 in 640 children vaccinated with MMR5 — about five times more often than seizure from measles infection.6
Although severe potential side effects have been observed following MMR vaccination, including neurological disorders (e.g., encephalopathy, meningitis, ataxia, transverse myelitis, optic neuritis, multiple sclerosis, Guillain-Barré syndrome, brachial neuritis, and hearing loss), autoimmune diseases (e.g., chronic arthritis), fibromyalgia, and chronic fatigue syndrome, the Institute of Medicine (IOM) states that “the evidence is inadequate to accept or reject a causal relationship between MMR vaccine” and those conditions.7 Additionally, the manufacturer’s package insert states, “M-M-R II vaccine has not been evaluated for carcinogenic or mutagenic potential or impairment of fertility.”8
How Are Risks of Vaccine Side Effects Measured?
Methods to measure vaccine risks include surveillance systems, clinical studies, and epidemiological studies.
How Accurate Is Surveillance of Adverse Events from the MMR Vaccine?
The government tracks reported cases of vaccine side effects through the Vaccine Adverse Event Reporting System (VAERS). Approximately 40 cases of death and permanent injury from the MMR vaccine are reported to VAERS annually.9 However, VAERS is a passive reporting system — authorities do not actively search for cases and do not actively remind doctors and the public to report cases. These limitations can lead to significant underreporting.10 The Centers for Disease Control and Prevention (CDC) states, “VAERS receives reports for only a small fraction of actual adverse events.”11 Indeed, as few as 1% of serious side effects from medical products are reported to passive surveillance systems,12 and as few as 1.6% of MMR-related seizures are reported to VAERS.13 In addition, VAERS reports are not proof that a side effect occurred, as the system is not designed to thoroughly investigate all cases.14 As a result, VAERS does not provide an accurate count of MMR vaccine side effects.
How Accurate Are Clinical Trials of the MMR Vaccine?
The CDC states, “Prelicensure trials are relatively small — usually limited to a few thousand subjects — and usually last no longer than a few years… Prelicensure trials usually do not have the ability to detect rare adverse events or adverse events with delayed onset.”10 For children under age 10 at normal risk (i.e., with normal levels of vitamin A and infected after birth), the pre-vaccine annual risk of death or permanent disability from measles, mumps, and rubella respectively was 1 in 1 million, 1 in 1.6 million, and 1 in 2.1 million.6,15-17 Therefore, the cumulative annual risk of a fatal or permanently disabling case of any of those diseases was about 1 in 500,000, and the risk over a 10-year span was 1 in 50,000. A few thousand subjects in clinical trials are not enough to prove that the MMR vaccine causes less permanent disability or death than measles, mumps, and rubella (Fig. 1). In addition, the lack of adequate clinical trials of the MMR vaccine resulted in the manufacturer’s package insert data to be reliant on passive surveillance for rates of MMR-related neurological adverse reactions, permanent disability, and death.8
How Accurate Are Epidemiological Studies of the MMR Vaccine?
Epidemiological studies are hindered by the effects of chance and possible confounders — additional factors that could conceivably affect the groups being studied. For example, there is a well-known 2002 Danish study published in the New England Journal of Medicine involving about 537,000 children that looked for an association between the MMR vaccine and certain adverse events.18 The raw data in the study was adjusted, in an attempt to account for potential confounders, and the study found no association between the MMR vaccine and the adverse events. However, because there is no evidence that the estimated confounders used to adjust the raw data were actually confounders, the study did not rule out the possibility that the MMR vaccine increases the risk of an adverse event that leads to permanent injury by up to 77%. Consequently, the study did not rule out the possibility that such adverse events might occur up to 21 times more often than death or permanent disability from measles, mumps, and rubella in children at normal risk (i.e., with normal levels of vitamin A and infected after birth): 1 in 2,400 compared to 1 in 50,000 (Fig. 2 and Table 1). The range of possibilities found in the study, between the adjusted data and the raw data, makes the result inconclusive; even large epidemiological studies are not accurate enough to prove that the MMR vaccine causes less death or permanent injury than measles, mumps, and rubella.
Is the MMR Vaccine Safer Than Measles, Mumps, and Rubella?
It has not been proven that the MMR vaccine is safer than measles, mumps, and rubella. The vaccine package insert raises questions about safety testing for cancer, genetic mutations, and impaired fertility. Although VAERS tracks some adverse events, it is too inaccurate to measure against the risk of measles, mumps, and rubella. Clinical trials do not have the ability to detect less common adverse reactions, and epidemiological studies are limited by the effects of chance and possible confounders. Safety studies of the MMR vaccine are particularly lacking in statistical power. A review of more than 60 MMR vaccine studies conducted for the Cochrane Library states, “The design and reporting of safety outcomes in MMR vaccine studies, both pre- and post-marketing, are largely inadequate.”19 Because permanent sequelae (aftereffects) from measles, mumps, and rubella are so rare (especially in children with normal levels of vitamin A and infected after birth),6,15-17 the level of accuracy of the research studies available is insufficient to rule out the possibility that the MMR vaccine causes greater death or permanent disability than measles, mumps, and rubella.
References
- LeBaron CW, Beeler J, Sullivan BJ, Forghani B, Bi D, Beck C, Audet S, Gargiullo P. Persistence of measles antibodies after 2 doses of measles vaccine in a postelimination environment. Arch Pediatr Adolesc Med. 2007 Mar;161(3):294-301. https://pubmed.ncbi.nlm.nih.gov/17339511/.
- Lewnard JA, Grad YH. Vaccine waning and mumps re-emergence in the United States. Sci Transl Med. 2018 Mar 21;10(433):2. http://stm.sciencemag.org/content/10/433/eaao5945.
- Davidkin I, Jokinen S, Broman M, Leinikki P, Peltola H. Persistence of measles, mumps, and rubella antibodies in an MMR-vaccinated cohort: a 20-year follow-up. J Infect Dis. 2008 Apr 1;197(7):955. https://pubmed.ncbi.nlm.nih.gov/18419470/.
- Centers for Disease Control and Prevention. Washington, D.C.: U.S. Department of Health and Human Services. Vaccines and immunizations: possible side effects from vaccines; [cited 2023 Dec 28]. https://physiciansforinformedconsent.org/cdc-vaccines-and-immunizations-possible-side-effects-from-vaccines/.
- Vestergaard M, Hviid A, Madsen KM, Wohlfahrt J, Thorsen P, Schendel D, Melbye M, Olsen J. MMR vaccination and febrile seizures: evaluation of susceptible subgroups and long-term prognosis. JAMA. 2004 Jul 21;292(3):356. https://jamanetwork.com/journals/jama/fullarticle/199117.
- Physicians for Informed Consent. Newport Beach (CA): Physicians for Informed Consent. Measles – disease information statement (DIS). 2017 Oct; updated 2024 Aug. https://physiciansforinformedconsent.org/measles.
- Institute of Medicine (IOM). Adverse effects of vaccines: evidence and causality. Washington, D.C.: National Academies Press; 2012. 119-217. https://www.ncbi.nlm.nih.gov/books/NBK190024/pdf/Bookshelf_NBK190024.pdf.
- Merck. Rahway (NJ): Merck and Co., Inc. M-M-R II (measles, mumps, and rubella virus vaccine live); revised 2023 Oct [cited 2024 Jan 27]. 8. https://www.merck.com/product/usa/pi_circulars/m/mmr_ii/mmr_ii_pi.pdf.
- Centers for Disease Control and Prevention. Washington, D.C.: U.S. Department of Health and Human Services. CDC wonder: about the Vaccine Adverse Event Reporting System (VAERS); [cited 2024 Feb 12]. https://wonder.cdc.gov/vaers.html. Query for death and permanent disability involving all measles-containing vaccines, 2011-2015.
- Centers for Disease Control and Prevention. Manual for the surveillance of vaccine-preventable diseases. 5th ed. Miller ER, Haber P, Hibbs B, Broder Chapter 21: surveillance for adverse events following immunization using the Vaccine Adverse Event Reporting System (VAERS). Atlanta: Centers for Disease Control and Prevention; 2011. 1,2,8. https://physiciansforinformedconsent.org/cdc-manual-for-the-surveillance-of-vaccine-preventable-diseases-5th-ed-chpt21-surv-adverse-events-2011.
- Centers for Disease Control and Prevention, Food and Drug Administration. Washington, D.C.: U.S. Department of Health and Human Services. Guide to interpreting VAERS data; [cited 2022 May 28]. https://vaers.hhs.gov/data/dataguide.html.
- Kessler DA. Introducing MEDWatch. A new approach to reporting medication and device adverse effects and product problems. JAMA. 1993 Jun 2;269(21):2765- https://www.sciencedirect.com/science/article/abs/pii/0163834394900515?via%3Dihub.
- Doshi P. The unofficial vaccine educators: are CDC funded non-profits sufficiently independent? [letter]. BMJ. 2017 Nov 7 [cited 2017 Nov 20];359:j5104. http://www.bmj.com/content/359/bmj. j5104/rr-13.
- Centers for Disease Control and Prevention. Washington, D.C.: U.S. Department of Health and Human Services. CDC wonder: about the Vaccine Adverse Event Reporting System (VAERS); [cited 2022 May 28]. https://wonder.cdc.gov/vaers.html.
- Magno H, Golomb B. Measuring the benefits of mass vaccination programs in the United States. Vaccines. 2020 Sep 29;8(4):4. https://pubmed.ncbi.nlm.nih.gov/33003480/.
- Physicians for Informed Consent. Newport Beach (CA): Physicians for Informed Consent. Mumps – disease information statement (DIS). Mumps: what parents need to know. 2024 Aug. https://physiciansforinformedconsent.org/mumps.
- Physicians for Informed Consent. Newport Beach (CA): Physicians for Informed Consent. Rubella – disease information statement (DIS). Rubella: what parents need to know. 2024 Aug. https://physiciansforinformedconsent.org/rubella.
- Madsen KM, Hviid A, Vestergaard M, Schendel D, WohlFahrt J, Thorsen P, Olsen J, Melbye M. A population-based study of measles, mumps, and rubella vaccination and autism. N Engl J Med. 2002 Nov 7;347(19):1477,1480. https://www.nejm.org/doi/full/10.1056/NEJMoa021134?url_ver=Z39.88-2003&rfr_id=ori%3Arid%3Acrossref.org&rfr_dat=cr_pub%3Dpubmed.
- Demicheli V, Rivetti A, Debalini MG, Di Pietrantonj C. Vaccines for measles, mumps and rubella in children. Cochrane Database of Syst Rev. 2012 Feb 15;(2). https://pubmed.ncbi.nlm.nih.gov/22336803/.
The silencing of scientific curiosity
Medical journals have became enforcers of orthodoxy—retracting genuine hypotheses while protecting proven fraud
By Maryanne Demasi, PhD | April 14, 2025
As a scientific writer and researcher, I’ve witnessed the decline of medical journals firsthand. Once forums for open debate and intellectual rigour, they’ve morphed into gatekeepers, more concerned with preserving a narrow orthodoxy than pursuing truth.
My previous work has exposed how journals suppress uncomfortable questions, avoid studies that challenge dominant narratives, and operate under a peer-review system distorted by bias and external influence.
But never have I seen a more absurd example of this decay than the retraction of a hypothesis paper—yes, a hypothesis—authored by Dr. Sabine Hazan in Frontiers in Microbiology.
Her 2022 article hypothesised that ivermectin might mitigate Covid-19 severity by promoting the growth of Bifidobacterium, reducing inflammation via the gut-lung axis.
She cited preliminary observations in 24 hypoxic patients who recovered without hospitalisation after combination therapy including ivermectin.

Dr Sabine Hazan, ProgenaBiome, Ventura, CA
She made no claims of definitive proof. Instead, she proposed a mechanism worth investigating. That’s the point of a scientific hypothesis.
But in May 2023—more than a year after the article was peer-reviewed and published—the journal retracted the paper following a series of complaints on PubPeer, offering only a vague explanation about “scientific soundness.”
Seeking clarity, I contacted both the journal’s editorial office and the editor who handled the paper, Professor Mohammad Alikhani at Hamadan University.

Prof Mohammad Alikhani, Department of Microbiology, Hamadan University
Specifically, I sought an explanation for retracting a ‘hypothesis’, but I did not receive a response.
This silence is damning.
Retraction is a serious step, historically reserved for cases of fraud or clear ethical misconduct. But here, no such claim was made—nor could one be substantiated.
The journal simply erased the paper, offering no transparent justification, no engagement with the scientific process, and no accountability.
In fact, it violated the very guidelines that journals are supposed to follow.
The Committee on Publication Ethics (COPE) advises that publications should only be retracted if they contain seriously flawed or fabricated data, or plagiarism that cannot be addressed through a correction.
Hazan’s paper was transparent about its speculative nature. In a January 2023 tweet, Hazan challenged her critics.
“It’s a hypothesis. PROVE ME WRONG,” she wrote.
After all, that’s the essence of science. But the journal’s decision to retract sends a message that even theoretical propositions are now intolerable.
Having tasted blood, Hazan’s critics kept digging. In January 2025, Future Microbiology retracted another of her studies—this one examining ivermectin-based multidrug therapy.
Hazan, her co-author Australian immunologist Dr. Robert L. Clancy, and others strongly disputed the decision after the journal failed to conduct a meaningful investigation into the alleged data integrity issues.
The irony is palpable.
While pundits argued over ivermectin’s efficacy during the pandemic, Hazan was one of the few actually doing the hard work to test its effects—collecting data, proposing mechanisms, engaging with the science. And yet she’s the one being silenced!
Which begs the question – why?
Is there professional jealousy in the microbiome space? Are pharmaceutical companies, threatened by low-cost alternatives like ivermectin, pressuring journals to kill competing narratives?
If so, the Securities and Exchange Commission (SEC) should investigate. Suppressing research that could affect investor decisions—by inflating the perceived value of antivirals or vaccines—could amount to securities fraud.
While there’s no definitive evidence, the pattern is hard to ignore: two retractions, no clear misconduct, and a growing campaign to discredit a scientist whose work challenges a profitable status quo.
Whether coordinated or not, the outcome is the same – the erasure of inconvenient data.
The spinelessness of journals in these episodes is unmistakable. Why do they capitulate so readily?
Just follow the money.
Many journals are financially entangled with the pharmaceutical industry—relying on drug ads, sponsorships, and profitable reprint sales. That financial tether distorts editorial independence.
Editors, often underpaid and overstretched, are understandably risk-averse. They fear litigation. They fear social media outrage. They fear becoming the next target.
Pharmaceutical companies, meanwhile, don’t hesitate to use legal threats to silence dissent because their pockets are deep—as in the case of Covaxin.
In July 2024, Bharat Biotech International Limited sued 11 authors—six of them students—and the editor of Drug Safety, Nitin Joshi, over a peer-reviewed article questioning the safety of their Covaxin vaccine.
The journal, under legal duress, retracted the paper. The authors were left to fend for themselves.
Journals are supposed to stand on principle. But, increasingly, they serve as enforcers of orthodoxy—vulnerable to financial pressure and online activists.
Let’s be honest, the trolls are part of the strategy. Anonymous complaints, often from individuals with no expertise, are weaponised to trigger retractions and smear reputations.
That’s not peer review. That’s mob rule.
The SEC must take a closer look at this ecosystem. If research is being suppressed to protect corporate revenue or manipulate investor confidence, that’s not just unethical—it’s illegal.
During his presidential campaign, Robert F. Kennedy Jr. addressed this very issue, declaring that journals colluding with pharmaceutical companies might be subject to charges under the Racketeer Influenced and Corrupt Organizations (RICO) Act.
“We’re gonna… file some racketeering lawsuits if you don’t start telling the truth in your journals,” he warned in 2023. It was provocative, yes—but it struck a chord with those of us watching the machinery of science betray its mission.
Retractions have become so casually executed, they’ve lost all meaning. What was once a mark of serious fraud is now a tool of reputational management.
Today, many papers are retracted not because they’re wrong, but because they’re inconvenient.
How else can one explain the demonstrably fraudulent studies funded by industry that remain published?
Whistleblower Dr. Peter Wilmshurst has spent years trying to get the MIST trial retracted—published in Circulation. It’s riddled with false claims, undeclared conflicts, and unreported adverse events, yet the journal continues to protect it.
This exposes the rot. These decisions have nothing to do with science.
They are political, financial, and reputational tools—used selectively to punish dissent.
There’s a growing list of researchers penalised—not for bad science, but for exploring uncomfortable truths.
Journals must reclaim their role as platforms for robust scientific debate. COPE must enforce its standards, not just cite them. Editors must be held accountable for vague or retaliatory retractions. And if corporate suppression of research is distorting public markets, then the SEC must act.
Because what I’m witnessing isn’t scientific curiosity—it’s narrative control. And the death of curiosity is the death of science itself.
Pregnant women deserve better than “trust us” science
A major study has been used to reassure pregnant women that Covid-19 vaccines are safe. But the data behind the claim are fatally flawed.
By Maryanne Demasi, PhD | April 12, 2025
In medicine, few assurances carry more emotional weight—or greater responsibility—than the claim that something is “safe during pregnancy.”
Pregnant women are justifiably cautious about what they expose themselves to during this vulnerable time, and history has given them every reason to be.
The thalidomide disaster, diethylstilboestrol (DES), and other cautionary tales have shown what can happen when scientific rigour is sidelined in favour of commercial interests.
So, when a new study published in Pediatrics – the official journal of the American Academy of Pediatrics – claimed that Covid-19 vaccination in early pregnancy was safe, it came with an air of authority and reassurance.
News headlines followed suit, and public health recommendations continued to promote the vaccine’s safety in pregnancy.

But scratch the surface of this study, and something starts to unravel.
Not only are the data unverifiable and privately sourced, but the study contains a fatal flaw that renders its conclusions virtually meaningless.
The fatal flaw
The study analyzed 78,052 pregnancies that ended in a live birth—but left out 20,341 pregnancies that ended in miscarriage or other non-live outcomes.
That’s not a minor oversight.
The very purpose of studying vaccine safety in pregnancy is to assess whether exposure in utero leads to adverse outcomes—like miscarriage, birth defects, or foetal death. Yet one-fifth of the pregnancies were excluded from the analysis, removing exactly the kind of outcomes the study was supposed to detect.
This introduces what’s known as live-birth bias—a selection bias that arises when research includes only live births, disregarding the possibility that harmful effects may have caused some pregnancies to end prematurely.
Put plainly, if you only study babies who made it to birth, you’re ignoring the ones who didn’t—and any harm that may have played a role.
Even the study’s authors acknowledge this limitation, conceding that the exclusion “could lead to an underestimation of identified outcomes.” Still, they move forward to conclude there’s no association between the vaccine and birth defects.
Omitting over 20,000 pregnancies isn’t just a technicality – it’s a fatal flaw.
If even a small fraction of those pregnancies ended in miscarriage or birth defects linked to vaccination, the entire outcome could tip the other way.
Commercial data with no accountability
Then there’s the source of the data itself—a point entirely overlooked.
Rather than using clinical records from hospitals or national birth registries, the study relied entirely on a commercial database from Merative® MarketScan® Research Databases.
These databases are vast, aggregating de-identified insurance claims, prescriptions, lab results, and hospital records from more than 263 million Americans. But they are also privately owned, and their inner workings are entirely opaque.
Researchers using MarketScan data cannot verify whether the patients are real or theoretical, whether records have been altered, or how the data has been cleaned or processed before delivery.
In essence, they are working with a black box, one that comes with no guarantee of integrity.
Experts have already noted that the data from this unverified source shows signs of being unreliable.
The authors ran 93 separate statistical tests to look for differences in outcomes like birth defects. By chance alone, you’d expect a handful to be statistically significant. But none were.
The probability of that happening randomly is just 0.8%—a sign that the dataset may have been fabricated, or that its integrity is in question.
When two of the study authors – Dr Stacey Rowe and Dr Annette Regan – were asked if they had verified the authenticity of the MarketScan database—that is, if they could confirm these were ‘real’ patient data—they did not respond.

L: Dr Stacey Rowe, R: Dr Annette Regan
This isn’t a hypothetical problem.
The medical literature has already been rocked by the Surgisphere scandal, where fraudulent hospital datasets were used to produce papers in The Lancet and The New England Journal of Medicine.
Those papers were eventually retracted, but only after independent researchers demanded to see the raw data and were denied – the data were likely fabricated.
Reassurance without evidence
Despite these glaring problems, the study’s conclusions are being used to reassure pregnant women.
In Australia, for example, the government’s official guidance recommends Covid-19 vaccination in pregnancy, stating that the “recommendations for pregnant women are the same as the general population.”
This, despite the fact that pregnant women were excluded from the pivotal clinical trials and no randomised studies have ever been completed to assess the vaccine’s safety in early-pregnancy.
The result is a landscape where pregnant women are asked to make a “shared decision” with their doctors—based on scientific literature that’s increasingly built on unverifiable data, flawed assumptions, and little to no independent scrutiny.
We are drifting into a new era where conclusions are based on data that sit behind corporate firewalls. An era where trust is expected, but no longer earned.
The Pediatrics study is a case in point.
It carries the imprimatur of authority, published in the flagship journal of the American Academy of Pediatrics. But, in reality, the analysis was based on commercial datasets that cannot be independently verified, and a methodology that systematically excludes the very outcomes it was supposed to assess.
This isn’t just bad science—it’s misleading by design.
And when it comes to pregnancy, where the stakes are literally life and death, that kind of scientific chicanery is a betrayal.
Pregnant women deserve better than a “trust us” approach to medicine.
They need full access to the data, honest communication about uncertainties, and above all, respect for their right to make informed decisions based on real evidence, not selective reporting.
Until that happens, we should remain sceptical of any study that asks us to believe in the evidence without seeing it.
Did Head of CDC Vaccine Safety Office Delete COVID Vaccine Injury Records?
By Michael Nevradakis, Ph.D. | The Defender | April 11, 2025
A key official at the Centers for Disease Control and Prevention (CDC) responsible for monitoring vaccine safety and reports of vaccine injuries may have mishandled or deleted official records subpoenaed by Congress, Sen. Ron Johnson (R-Wis.) alleged earlier this week. The New York Post first reported the story on Thursday.
Dr. Tom Shimabukuro, director of the CDC Immunization Safety Office, maintained the records in question. Shimabukuro previously authored a key paper and participated in public messaging claiming the COVID-19 vaccines were safe and effective for pregnant women.
Johnson, chairman of the U.S. Senate Permanent Subcommittee on Investigations, requested the records in a subpoena sent in January to the U.S. Department of Health and Human Services (HHS). The subpoena pertained to an investigation into internal COVID-19 vaccine safety communications.
According to the New York Post, the subpoena led HHS to discover “potential discrepancies” in the emails maintained by Shimabukuro.
“HHS officials recently informed me that Dr. Shimabukuro’s records remain lost and, potentially, removed from HHS’s email system altogether,” Johnson wrote in a letter he sent earlier this week to U.S. Attorney General Pam Bondi, FBI Director Kash Patel and HHS Principal Deputy Inspector General Juliet Hodgkins.
Johnson called Shimabukuro’s possible mishandling of his official records “highly concerning.”
Journalist Paul D. Thacker, a former U.S. Senate investigator, said, “Every American should be concerned about government scientists deleting or hiding federal information to shape a political agenda. That information belongs to the taxpayers.”
Nebraska chiropractor Ben Tapper, whose questioning of the COVID-19 vaccines led the Center for Countering Digital Hate to add him in 2021 to its “Disinformation Dozen” list of the “leading online anti-vaxxers,” said he was “not surprised” by Johnson’s allegations.
“For years, I’ve seen patterns like this before regarding vaccine safety data. The public health establishment often prioritizes profits over people and continuously seems to protect the lies over the truth. The idea that critical records might vanish — whether through negligence or intent — fits a familiar playbook,” Tapper said.
California attorney Rick Jaffe said Johnson’s allegations are “troubling, but not surprising, given longstanding concerns about transparency at the CDC.”
In response to a Freedom of Information Act (FOIA) request last year, the CDC told Children’s Health Defense the agency has no records of certain internal email communications relating to the agency’s follow-up investigation of safety signals associated with COVID-19 vaccines.
HHS, CDC and Johnson’s office did not respond to requests for comment.
Missing records ‘could contain unfiltered insights’ into vaccine adverse events
Citing an unnamed aide from Johnson’s office, the New York Post said it is unclear which specific records are missing. But according to Johnson’s letter, Shimabukuro’s role included “monitoring adverse events relating to the COVID-19 vaccines.”
Tapper said Shimabukuro may have been “handling sensitive data on adverse events linked to the COVID-19 vaccines,” including data from the U.S. government-run Vaccine Adverse Event Reporting System (VAERS) and the V-safe database, as well as studies, raw data and internal communications on vaccine-related safety signals.
Tapper said:
“These records could contain unfiltered insights into side effects that were downplayed or unresolved during the pandemic. For example, I’ve seen cases in my practice where patients developed symptoms like persistent fatigue or heart palpitations post-vaccination, yet struggled to get clear answers from authorities.
“Missing records could hide similar signals, undermining efforts to validate patient experiences or refine vaccine protocols.”
Internal medicine physician Dr. Clayton J. Baker said, “Such records would likely be very damning to all CDC officials who perpetuated the false ‘safe and effective’ narrative about the COVID-19 vaccines from 2021 until the present.”
“Given how damning any evidence of ignored or falsified safety signals would be, I think it is highly likely that Biden-era officials might try to destroy such records if they could. Better to be accused of destruction of federal records than to be charged as an accessory to mass negligent homicide,” Baker said.
In an April 2023 presentation to the CDC Advisory Committee on Immunization Practices, Shimabukuro claimed that surveillance conducted by international regulatory and public health partners “has not detected a safety concern for ischemic stroke following bivalent COVID-19 mRNA booster vaccination.”
Yet, a peer-reviewed study published in November 2024 found that mRNA COVID-19 vaccines pose a 112,000% greater risk of brain clots and strokes than flu vaccines, and a 20,700% greater risk of those symptoms than all other vaccines combined. The study called for a global moratorium on mRNA vaccines.
In 2021, Shimabukuro was the lead author of a study in The New England Journal of Medicine (NEJM) on the safety of COVID-19 vaccines for pregnant women. The study concluded that “preliminary findings did not show obvious safety signals among pregnant persons who received mRNA Covid-19 vaccines.”
However, a peer-reviewed study published in 2022 showed that the authors of the NEJM study performed a “statistical sleight-of-hand” that substantially lowered the miscarriage rate in pregnant women, presenting it as 12.6% instead of 82%.
In a Substack post, epidemiologist Nicolas Hulscher said Shimabukuro’s “potential involvement in the deliberate manipulation of critical safety data on COVID-19 mRNA injections during pregnancy carries grave implications — resulting in immeasurable harm to mothers and their unborn children worldwide.”
Shimabukuro ‘may have violated multiple federal laws’
According to a press release from Johnson’s office, Shimabukuro’s actions, if proven to have occurred, “may have violated multiple federal laws.”
Those laws include the Federal Records Act, which requires federal employees to preserve materials “made or received by a Federal agency under Federal law or in connection with the transaction of public business,” the New York Post reported.
Johnson wrote that the destruction of records subpoenaed by Congress may also be “grounds for contempt of Congress,” which, according to the New York Post, is punishable by up to a six-figure fine and 12 months in prison.
Jaffe said Shimabukuro may also face other penalties. He said:
“Under federal law, he could be charged with obstruction of justice or destruction of official records — risking fines, restitution and up to 20 years in prison. His federal pension could also be garnished to satisfy any judgment against him.
“Beyond criminal penalties, he faces permanent disqualification from federal service and career-ending reputational harm.”
In addition, if records relating to vaccine-injured people are missing or destroyed, impairing their legal cases, “courts could impose evidentiary sanctions or presume the destroyed records were unfavorable to the government,” Jaffe said.
Johnson’s letter also referred to Dr. David Morens, an employee of the National Institute of Allergy and Infectious Diseases who was a close aide of the agency’s former director, Dr. Anthony Fauci. Morens allegedly deleted emails and instructed colleagues to contact him at a personal email account to sidestep FOIA rules.
In his letter, Johnson accused HHS of a “lack of transparency” and failure to investigate the allegations against Morens.
“I had always suspected that Dr. Morens was not the sole evader of federal record-keeping requirements at HHS,” Johnson wrote. “The extent to which HHS officials systemically mishandled, deleted, or destroyed their communications, data, and other information relating to the COVID-19 pandemic and the vaccines must be thoroughly investigated.”
Johnson’s letter asks the FBI, the U.S. Department of Justice and the HHS Inspector General’s Office to investigate the matter, including whether records were intentionally destroyed to “avoid or subvert Congressional oversight or the Freedom of Information Act.”
The letter builds on Johnson’s efforts to investigate COVID-19 vaccine safety.
Earlier this week, Johnson sent letters to the heads of four COVID-19 vaccine manufacturers, requesting they turn over records related to the development and safety of the COVID-19 vaccines and their communications with Big Tech platforms about vaccine-related adverse events.
In November 2024, Johnson wrote a letter to HHS, CDC and FDA, asking the agencies to “preserve all records referring or relating to the development, safety, and efficacy of the COVID-19 vaccines.”
In an October 2023 letter to the then-heads of CDC and FDA, Johnson accused the agencies of an “appalling” lack of transparency regarding COVID-19 vaccine safety signals, depriving Americans of “the benefit of informed consent.”
During the Biden administration, Johnson wrote over 70 letters to HHS officials and its health agencies requesting information on COVID-19 vaccine adverse events and related communications, according to a Jan. 29 press release.
Last year, Johnson hosted a congressional roundtable to discuss the risks of COVID-19 vaccines. Medical experts, political figures, journalists and whistleblowers were among the participants.
This article was originally published by The Defender — Children’s Health Defense’s News & Views Website under Creative Commons license CC BY-NC-ND 4.0. Please consider subscribing to The Defender or donating to Children’s Health Defense.
The Media Playbook for Measles Looks a Lot Like Its COVID Playbook — This Time, Kids Are the Pawns
By Mary Holland, J.D. | The Defender | April 8, 2025
There are moments in the history of a movement that test its resolve. For the medical freedom movement, this is one of those moments.
We are in the midst of another full-on attack by the pharmaceutical-industrial complex, aided and abetted by a beholden mainstream media united around its allegiance to a $69 billion vaccine industry.
Five years ago, we fought back as our government, Big Media and Big Pharma orchestrated and executed a COVID-19 fear campaign — a campaign built on lies, deception and censorship — and then parlayed the public’s fear into dangerous and deadly medical mandates and hospital protocols that continue to cause profound harm.
The upside to COVID-19 global disaster?
It opened the eyes of millions more people to the dangers of shoddily tested vaccines, regulatory agency hubris and one-size-fits-all “medicine.”
As our movement has grown exponentially, so has our threat to Big Pharma.
In response, we’re seeing the same tactics rolled out again. This time, it’s measles. This time, children are the pawns in pharma’s playbook.
Children’s Health Defense (CHD) stood strong and stayed true to our mission during COVID. We’re standing just as strong now. We remain just as committed now to the truth, informed consent and medical freedom as we were during the pandemic.
As pharma ramps up its measles playbook, our No. 1 job is to dismantle the vaccine industry’s lies — broadcast far and wide through the industry’s most reliable and faithful megaphone: mainstream media.
The media would have you believe that measles is a “deadly” disease. But any suggestion that MMR (measles-mumps-rubella) vaccines are safer than measles infection isn’t supported by facts.
In fact, between 2000 and 2024, nine measles-related deaths were reported to the CDC. During the same period, 141 deaths following MMR or MMRV vaccination were reported in the U.S. to the Vaccine Adverse Event Reporting System (VAERS) — suggesting the MMR vaccine can be deadlier than measles.
The media echo the same familiar refrain: The MMR vaccine is “overwhelmingly safe.”
In fact, the MMR vaccine is associated with serious health risks. The package insert for Merck’s MMRII says, “M-M-R II vaccine has not been evaluated for carcinogenic or mutagenic potential or impairment of fertility.”
Research also shows the MMR vaccine causes febrile seizures, anaphylaxis, meningitis, encephalitis, thrombocytopenia, arthralgia and vasculitis. In 2004, researchers at the Centers for Disease Control and Prevention found that boys vaccinated with their first MMR vaccine on time were 67% more likely to be diagnosed with autism compared to boys who got their first vaccine after their 3rd birthday.
The media insist there’s no viable treatment for measles — hence prevention, with the MMR vaccine, is the sole solution.
In fact, as CHD reported, doctors in West Texas are successfully treating measles with budesonide and vitamin A. Even the World Health Organization recommends vitamin A.
Yet some hospitals and doctors are refusing to treat measles patients with budesonide. Texas health officials rejected pleas by a treating physician to endorse the treatment and get the word out to hospitals about its effectiveness.
Sound familiar?
We saw this identical playbook with COVID. Media parroted public health officials’ claim that the vaccine alone would save us — while discouraging, ridiculing and even outright sanctioning the use of ivermectin, hydroxychloroquine, budesonide and other treatments known to reduce COVID severity and death.
Last month, a 6-year-old child in West Texas died after developing pneumonia while recovering from measles. Media seized the opportunity to disparage the parents, members of a Mennonite community, for not vaccinating their child.
As our science and CHD.TV teams uncovered — after enlisting experts to review the child’s medical records — the little girl died not “from” measles, as media claimed, but from a tragic medical error.
In fact, the hospital properly diagnosed the little girl’s pneumonia — a community-acquired pneumonia that, when treated properly is not life-threatening. Unfortunately, the doctors failed to use the standard antibiotic indicated for treating her pneumonia until it was too late.
Even after CHD exposed the accurate cause of death, The New York Times reported the 6-year-old died from measles — and accused us of making “unfounded claims” about the death.
Last week, a second child in West Texas died. The media and Texas health officials reported the death as “measles pulmonary failure.” CHD is working with the child’s parents to analyze her medical records. We will report, accurately, on what we find.
The media have accused CHD and the health freedom movement — or “anti-vaxxers” as reporters love to call us — of “weaponizing” the tragic death of the 6-year-old who died because of a medical error. (We should point out that death by medical error is not uncommon in the U.S. It’s estimated that at least 250,000 people die every year as a result of the wrong diagnosis or treatment, making it the third-leading cause of death).
The death of any child, for any reason, is heartbreaking. But in this case, who are the real “weaponizers?”
If media are genuinely concerned about children’s lives, where are the reports on children’s injuries and deaths from COVID-19 vaccines? From MMR vaccines? From the other 14 shots on the CDC-recommended schedule?
Last month, CHD reported on the senseless death of a 1-year-old roughly 12 hours after the child’s pediatrician insisted on administering six shots of 12 vaccines at once.
Where were the headlines deploring this child’s death, denouncing the child’s pediatrician? Where were the reports on the known dangers of “catching up” babies and children on vaccines?
As the media remain radio silent on the carnage inflicted on innocent children by a powerful, greedy industry and its minions in Congress, CHD is honoring the legacy of these children by reporting the facts, telling the truth and insisting on the rights of parents to make independent, informed medical decisions.
This latest round of attacks on the health freedom movement is a measure of pharma’s fear. We are winning. Pharma knows it.
We have no intention of backing down from the facts: Vaccines cause serious injuries, including death. As Big Pharma and Big Media wage a renewed battle for the hearts and minds of parents, we must strengthen our resolve, we must stay true to our mission.
Our children deserve nothing less.
This article was originally published by The Defender — Children’s Health Defense’s News & Views Website under Creative Commons license CC BY-NC-ND 4.0. Please consider subscribing to The Defender or donating to Children’s Health Defense.
US-Funded “Anti-Misinformation” Groups Are Still Quietly Active
By Didi Rankovic | Reclaim The Net | April 9, 2025
Despite the big and open push that came in with the new US administration to end the practice of the government funding third-party groups to effectively act as its censorship proxies – some of these arrangements continue to be operational.
Most appear to be working to strengthen previously established “preferred” narratives around health issues – as ever, with “combating misinformation” given as the declarative, overarching purpose behind the effort.
But critics say, that was/remains a smokescreen meant to manipulate public opinion.
The Federalist reports that the National Science Foundation (NSF) – one of the US government’s “independent agencies” designed to channel federal funds – had a number of programs under its “anti-misinformation” umbrella, the Convergence Accelerator.
Among the ones who continue to this day are Chime In, Analysis and Response Toolkit for Trust (ARTT), and Expert Voices Together (EVT).
Chime In’s original name was Course Correct. It was set up at the University of Wisconsin-Madison – with $5 million coming from NSF in 2022 – to provide “anti-misinformation” resources for journalists.
True to the era, its original “mission” was to persuade (Covid) vaccine skeptics to take the jab; and then it went into advocating (“misinformation detecting”) in favor of persuading people there was no reason to be skeptical about genetically modified (GMO) foods, Covid narratives, and vaccines in general, as well as issues like sunscreen product and raw milk safety.
ARTT, meanwhile, came up with its own “AI” chatbot, that focused on political discourse, but according to the Federalist, once again, heavily tied to vaccine hesitancy.
From 2021, ARTT received close to $750,000 from the NSF, and a further $5 million, “to develop practical interventions to build trust and address vaccine hesitancy.”
Another controversial tie-in concerning ARTT was the organization’s plans to partner with, among others, the Children’s Hospital of Philadelphia, which the article describes as being “infamous for performing transgender surgeries on, and administering opposite-sex hormones to minors.”
ARTT – now operating as Discourse Labs, a non-profit – was, while one of the groups incubated by NSF’s Convergence Accelerator, backed up by the World Economic Forum (WEF), Wikimedia Foundation, Google, Mozilla, and Meta.
EVT’s “new home” as of 2025 is “the leftist group Right To Be,” the report says.
Some of the issues covered by this group are named, “Bystander Intervention To Support The LGBTQIA+ Community,” “Conflict De-Escalation In Protest Spaces,” and “Bystander Intervention To Stop Police Sponsored Violence and Anti-Black Racism.”
But the Federalist reported earlier that, “a representative from Right To Be” previously told the site EVT “remains under the direction of George Washington University (and) direct inquiries there.”
Lawmakers say RFK Jr. is spreading misinformation about psychiatric drugs
The real threat may be their attempt to silence the debate
By Maryanne Demasi, PhD | April 9, 2025
The Make America Healthy Again (MAHA) Commission, established by Executive Order, convened its first meeting last month.
Among the topics discussed was the “threat posed by the prescription of selective serotonin reuptake inhibitors (SSRIs), antipsychotics, mood stabilisers, and stimulants.”
Shortly thereafter, a group of legislators issued a strongly worded letter to Health Secretary Robert F. Kennedy Jr, accusing him of “promoting disproven and outright false theories” about these medications—reframing them as “behavioral health medication.”
They argued that even suggesting these drugs might pose a “threat” would “stigmatize” Americans with mental health conditions and potentially deter them from seeking medical care.
But labelling something a “threat” in a policy discussion is not a condemnation; it is an invitation to assess risk—a fundamental responsibility of medical oversight.
The letter, led by Senator Tina Smith, urged Kennedy to “adhere to the well-established and widely accepted scientific and medical consensus” on the matter.
Consensus? This is precisely the problem—they are appealing to authority to shut down inquiry rather than fostering critical examination.
The FDA itself has placed a black box warning on SSRIs, cautioning that studies have shown these drugs double the risk of suicidal ideation and behaviour in certain populations.
Should that warning be revoked for fear of discouraging treatment?
Are we now at a point where simply discussing the risks of medications is considered dangerous? What happened to informed consent?
And if we are to insist on evidence – as the legislators say – where is their study that suggests educating people about the harms and benefits of medication prevents them from seeking treatment?
It does not exist.
In many cases, psychotherapy should be prioritised over medication, as it is safer, more effective in the long run, and aligns with what most patients prefer.
Neither the MAHA Commission nor Kennedy has advocated for anyone to stop taking medication abruptly—a well-known risk—but rather to investigate the full scope of these drugs’ effects.
The legislators cited CDC statistics showing that “43 percent of children between the ages of 3 and 17 took medication for an emotional, concentrational, or behavioral condition,” then immediately noted that “youth mental health needs have only increased in the past five years.”
The contradiction is glaring—if these medications were the solution, why is the problem worsening? This is precisely what Kennedy seeks to investigate.
One of the most contentious points was Kennedy’s claim that SSRIs have been linked to school shootings in the U.S.
The legislators cited studies such as an analysis of FBI data on “educational shootings” from 2000-2017, which concluded that the majority of school shooters had not been previously treated with psychotropic medication.
However, these data are incomplete. Privacy laws restrict access to shooters’ full medical histories, making definitive conclusions about many of these analyses difficult.
Meanwhile, a 2015 study published in PLOS One by Moore et al. found a disproportionate association between certain psychotropic drugs and violent behaviour in the FDA’s adverse event reporting system.
The harms of antidepressants are often downplayed—even in the medical literature.
Comparisons between published studies and confidential regulatory documents have revealed significant discrepancies, including underreporting of suicide attempts and aggressive behaviour.
My point is, Kennedy is not asserting causation—he is calling for more research. The legislators’ dismissal of his concerns as “disproven” serves only to suppress an important discussion that demands further scrutiny.
At his confirmation hearing, Kennedy remarked, “I know people, including members of my family, who’ve had a much worse time getting off of SSRIs than getting off of heroin.”
Legislators strongly objected to the comparison in the letter, but Kennedy was referring to the well-documented difficulties of SSRI discontinuation—affecting about half of those who take them, even though their dependency profile differs from that of opioids.
What most people don’t realise is that psychiatrists who specialise in tapering patients off antidepressants report that SSRI-withdrawal can last far longer than withdrawal from heroin.
In fact, some patients remain on SSRIs indefinitely—not by choice, but because withdrawal symptoms are so severe that stopping is unbearable. The legislators’ letter conveniently ignores this reality.
Instead of engaging with the substance of his arguments, Kennedy’s critics attacked his qualifications, claiming he was “unqualified” to weigh in on mental health or addiction.
True, Kennedy is not a psychiatrist—or even a physician. But as a lawyer who has spent decades exposing the failures of public health institutions, he understands where scrutiny is needed.
Moreover, Kennedy is not issuing medical directives—he is demanding accountability in a system that too often fails to critically examine the long-term effects of the medications it prescribes.
As Danish physician Peter Gøtzsche has shown, prescription drugs are a leading cause of death, surpassing even heart disease and cancer—and psychiatric medications alone are the third leading cause of death.
Why are these legislators so adamantly defending what is widely acknowledged as the rampant over-prescription of psychiatric drugs? Could it have anything to do with their deep ties to Big Pharma lobbyists?
Their eagerness to silence dissent suggests that the interests being protected may not be those of the public, but rather those of the industry that funds their campaigns.
I have been writing about this issue for years, exposing the pharmaceutical industry’s role in shaping narratives around psychiatric drugs while downplaying their harms.
The pattern is always the same — suppress uncomfortable discussions, attack those who raise legitimate concerns, and protect the status quo.
How fragile do these legislators think people are, that they shouldn’t be trusted with the full truth about the medications they take? And more disturbingly, what gives them the authority to control what information the public is allowed to access?
Kennedy pledged that “nothing is going to be off limits” in his effort to Make America Healthy Again—this is what he meant.
Raising questions is not misinformation. And shutting down debate is not science.
If policymakers are confident in the safety and efficacy of these drugs, they should welcome scrutiny—not suppress it.
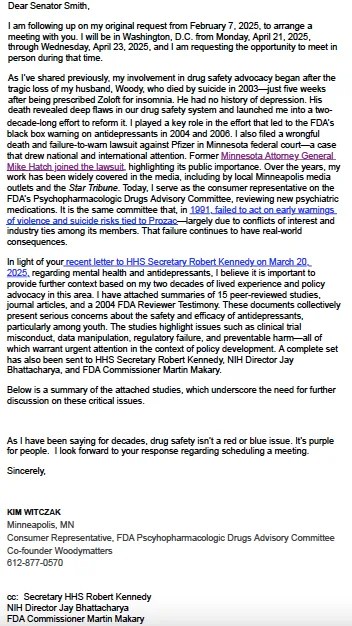
Below is a letter from Kim Witczak, a drug safety advocate – addressed to Senator Tina Smith. It requests a meeting to discuss mental health and antidepressant safety concerns, referencing Witczak’s personal experience, attaching 15 studies highlighting issues like clinical trial misconduct and regulatory failures
How Big Pharma Weaves Its Web
By Kim Witczak | Brownstone Institute | April 5, 2025
Inever set out to be an advocate. I wasn’t a doctor, scientist, or policy expert. I was just a regular person who, like so many, blindly trusted that our healthcare system was designed to protect us.
But life has a way of pulling us into the arena when we least expect it.
After the tragic and unexpected loss of my husband Woody to the antidepressant Zoloft he was prescribed for insomnia, I was thrust into a world I never imagined—one where medicine wasn’t solely about healing, but deeply entangled in a system that prioritizes profit over safety, buries harms, and keeps the public in the dark.
For over two decades, I’ve had a front-row seat to how this system truly operates—not the illusion of rigorous oversight we see in medical journals or glossy pharmaceutical ads, but the reality of how industry influence is woven into every stage.
I’ve met with regulators, testified before the FDA and Congress, filed a wrongful death and failure-to-warn lawsuit against Pfizer, and earned a seat on the FDA’s Psychopharmacologic Drugs Advisory Committee as a consumer representative.
I’ve also spoken at and participated in global conferences like Selling Sickness, Too Much Medicine, and the Harms in Medicine meeting in Erice, Italy—where some of the world’s leading experts acknowledge what few in mainstream medicine dare to say:
Our healthcare system isn’t about health—it’s about business.
And in this business, harm isn’t an accident. It’s built into the system.
The more I uncovered, the more I realized:
We aren’t just patients. We are customers.
And we are all trapped in Big Pharma’s spiderweb of influence.
The Spiderweb of Influence
The more I learned, the more I saw just how deeply embedded the pharmaceutical industry is—not just in drug development and marketing but in every corner of our healthcare system.
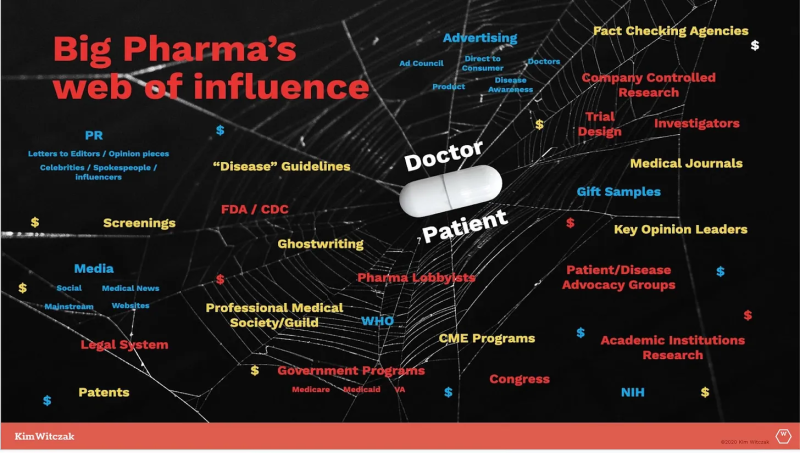
That’s why I created the Big Pharma Spider Web of Influence—to visually map out how the system is designed not to prioritize health but to sell sickness while minimizing, downplaying, or outright hiding harms.
From clinical trial design to regulatory approval, from direct-to-consumer advertising to medical education, from controlling medical journals to silencing dissenting voices, the industry has built an intricate and self-reinforcing web—one that traps doctors, patients, and even regulators in a cycle of pharmaceutical dependence.
How the Web Works
- Clinical trials are often designed, funded, and controlled by the very companies that stand to profit. They manipulate data to exaggerate benefits and obscure risks, ensuring that negative results are buried, spun, or never published at all.
- Regulatory agencies like the FDA are deeply entangled with the industry they’re supposed to oversee. More than 50% of the FDA’s budget comes from industry-paid user fees, and a revolving door ensures that many key decision-makers come from—and later return to—pharmaceutical companies.
- Medical journals depend on pharmaceutical funding through advertising, reprint sales, and industry-sponsored studies—severely limiting independent scrutiny of drug safety. Many studies are ghostwritten or crafted by paid “key opinion leaders” (KOLs) who serve as pharma’s trusted messengers.
- Doctors receive education through industry-funded programs, learning “best practices” based on treatment guidelines crafted by the very system that profits from overprescription.
- Patient advocacy groups, once independent grassroots organizations, have been co-opted by industry money, ensuring that the loudest voices often serve pharma’s interests rather than patients’ needs. I call them “astroturf” patient groups—they look like real grassroots organizations, but they’re anything but.
- Screenings and guidelines continuously expand the definitions of disease, turning more people into lifelong customers.
This isn’t about one bad actor or isolated corruption—it’s a systemic issue. The entire structure is designed to push more drugs onto the market, medicalize normal human experiences, and only acknowledge harm when it becomes too big to ignore.
It’s a brilliant business model—but a catastrophic public health strategy.
“To Sell to Everyone:” The Business Model of Medicine
If this sounds like a conspiracy, consider the bold admission made by Henry Gadsden, former CEO of Merck, in a 1976 interview with Fortune Magazine:
“The problem we have had is limiting the potential of drugs to sick people. We could be more like Wrigley’s Gum…it has long been my dream to make drugs for healthy people. To sell to everyone.”
– Former Merck CEO Henry Gadsden
Let that sink in.
This wasn’t about curing disease—it was about expanding markets. Gadsden’s vision wasn’t just to treat illness, but to medicalize everyday life—creating a cradle-to-grave model where every person, healthy or sick, became a customer for life. Just like selling a variety of gum—something for everyone. Juicy Fruit, Big Red, Doublemint, Spearmint, and so on.
And that’s exactly what happened.
Today, we live in a system where:
- Everyday emotions—sadness, worry, shyness—are rebranded as medical conditions requiring treatment.
- Preventive medicine often means lifelong prescriptions, not lifestyle changes.
- Drugs are marketed to the “worried well”, turning normal human experiences into diagnoses.
This isn’t just theory—it’s well documented. In Selling Sickness: How the World’s Biggest Pharmaceutical Companies Are Turning Us All into Patients, Ray Moynihan and Alan Cassels expose how pharmaceutical companies create diseases, expand diagnostic criteria, and convince the public that normal life experiences require medical intervention.
The goal?
Make medication the default—not the last resort.
Harms Are Always an Afterthought
Harms from medication are not rare, nor are they unexpected.
But in this system, they are treated as acceptable collateral damage—something to be dealt with only after the damage is done, after lives are lost or forever changed.
I’ve sat in FDA Advisory Committee meetings, reviewing new drug applications, and have seen firsthand how safety concerns are often dismissed in favor of “innovation” or “unmet medical need.”
I’ve heard industry representatives and advisory committee members argue that safety signals can be addressed post-market, meaning after a drug is already in circulation and causing harm or a required REMS (Risk Evaluation and Mitigation Strategies) program upon approval.
But by the time post-market safety issues are acknowledged, it’s often too late.
We’ve seen this play out over and over:
- Opioids—marketed as “non-addictive” and pushed aggressively onto patients, leading to an epidemic of addiction and death.
- SSRIs and antidepressants—long linked to increased risks of suicide and violence, particularly in young people, yet downplayed or dismissed for decades. Other hidden harms include withdrawal syndromes and Post-SSRI Sexual Dysfunction (PSSD), conditions that many patients were never warned about.
- Antipsychotics—widely prescribed for off-label use, leading to severe metabolic and neurological side effects.
- Covid-19 vaccines—an experimental mRNA platform rushed to market, mandated, and imposed on society despite limited long-term safety data and growing concerns over harms.
Every time, the pattern is the same:
The industry sells the benefits while downplaying the risks—until those risks become too big to ignore.
By then, the drug is a blockbuster, billions have been made, and the system moves on to the next new “breakthrough.”
More Than Degrees: The Truth of Lived Experience
One of the biggest lessons I’ve learned in this fight is that real-world experience matters just as much as credentials.
Over the years, I’ve been invited to speak at medical schools, PhD programs, and universities, thanks to brave academics willing to challenge the narrative. I share my journey as an accidental advocate—someone who didn’t have a medical degree but discovered America’s broken drug system the hard way.
But let’s be honest—the medical world is driven by credentials. Or, as I like to say, the alphabet soup.
At conferences, attendees wear name tags listing their titles—MD, PhD, JD, MPH. It’s a quick way to size someone up, to assess credibility before even speaking. And I’ve seen it happen: people glance at my name tag, see no impressive letters after my name, and walk right by.
Years ago, I was speaking at the Preventing Overdiagnosis Conference and noticed my badge read: Kim Witczak, BA.
I was horrified. Was that really necessary? Did my name tag need to remind everyone that I only had a BA?
Later, I was telling the story to a doctor friend, and he laughed.
“Next time, tell them BA stands for Bad Ass.”
And he was right.
Because real expertise doesn’t always come from an advanced degree—it comes from lived experience, from asking the right questions, from refusing to accept the status quo.
The Counterargument: But Don’t We Need Experts?
Of course, some will argue that only experts with MDs and PhDs should be trusted to shape healthcare policy.
But that assumes that the system they operate in is free from bias, conflicts of interest, or financial incentives.
The reality is that many of those with the most letters after their names are also the ones benefiting from pharma funding—whether through consulting fees, research grants, or advisory roles.
Meanwhile, patients and their families—the ones living with the consequences—are too often ignored.
That needs to change.
Asking Better Questions: Reclaiming Our Power
If there’s one thing I’ve learned on this journey, it’s this: no one is coming to save us. The institutions meant to protect us are too entangled in the web to act with true independence.
My late husband, Woody, used to say: “Follow the money.” And when you do, the truth becomes impossible to ignore. Pharmaceutical profits—not patient well-being—drive the system. That’s why the only way to create real change is through awareness, transparency, and fundamentally shifting how we think about medicine and health.
That starts with asking better questions:
- Who funded this research?
- Does this person or institution have financial ties, intellectual bias, or self-interest that could impact their recommendations?
- Who benefits from this treatment?
- What aren’t we being told?
- What are the long-term consequences of this drug or intervention?
- Are there safer, non-drug alternatives being ignored because they aren’t profitable?
But asking the right questions isn’t enough.
We have to stop outsourcing our health to a system built on financial incentives and guided by corporate interests.
We must demand full transparency, challenge the status quo, and recognize that sometimes the best medicine isn’t a pill but a deeper understanding of what our bodies truly need.
Because once you see the web, you can’t unsee it.
And once you recognize how deeply medicine has been shaped by profit, you’ll realize the most important question isn’t just “What can I take?”—it’s “Who benefits if I do?”
Final Thoughts: Tearing Down the Web
I never wanted to be in this fight, but once you see the web, you can’t unsee it. That’s why I continue to speak out, to challenge the system, and to push for real accountability.
Because the stakes aren’t theoretical. They’re deeply personal.
For me, this fight began over two decades ago with Woody. But for countless others, it begins the moment they or someone they love is caught in the web—trusting a system that was never truly designed to protect them.
It’s time to tear down the web.
And it starts with seeing it for what it really is.
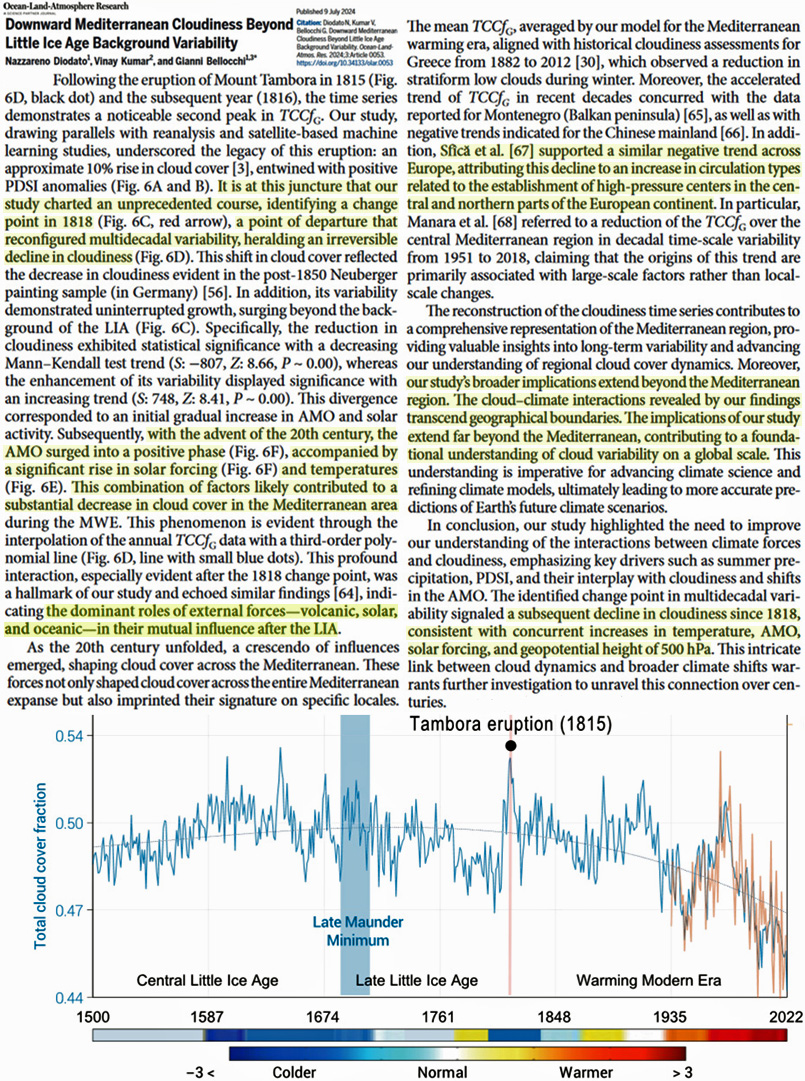
New Study: Recent ‘Unprecedented’ Cloud Cover Decline Driving Modern (And Past) Climate Change
By Kenneth Richard | No Tricks Zone | March 25, 2025
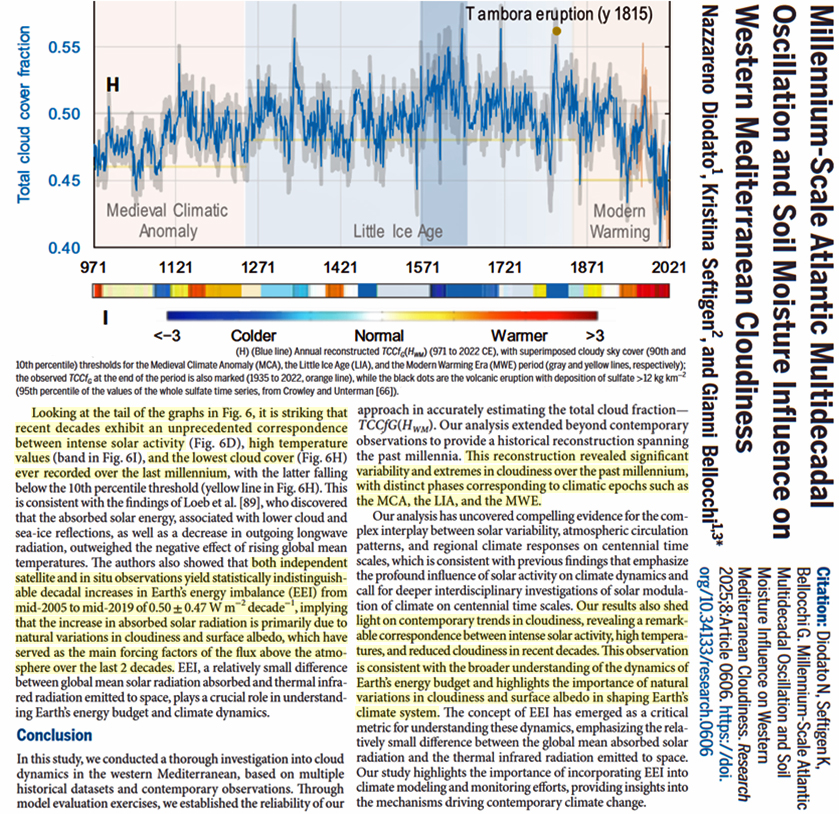
“[T]he increase in absorbed solar radiation is primarily due to natural variations in cloudiness and surface albedo, which have served as the main forcing factors of the flux above the atmosphere over the last 2 decades.” – Diodato et al., 2025
It is commonly accepted that there has been a satellite-observed (CERES) cloud cover albedo decline that has led to an increase in solar radiation absorbed by the Earth’s oceans. This increasing trend in absorbed solar radiation (ASR) explains the post-2000 global-scale temperature increase (Dübal and Vahrenholt, 2021, Loeb et al., 2021, Stephens et al., 2022, Koutsoyiannis et al., 2023, Loeb et al., 2024, Nikolov and Zeller, 2024).
And now, in two new studies (Diodato et al., 2024 and Diodato et al., 2025), scientists have begun formulating reconstructions of cloud cover over the Mediterranean region that can be dated all the way back to the Medieval Warm Period, or 970 CE.
The authors suggest their reconstructions of cloud cover may be representative of more than just this region, as it is a product of large scale processes that may “transcend geographical boundaries.” In other words, what happens in the Mediterranean region may well have global implications.
Their reconstructions indicate the modern declining cloud cover trend may not only have been occurring since 2000, but, except for a brief increasing period from about 1945 to 1980 (that coincided with a global cooling trend), it has been ongoing for over 200 years. The “turning point” years were 1815-1818, following the eruption of Mount Tambora. From that point on there has been a precipitous decline in cloud cover that departs from multi-decadal variability.
The authors suggest the “dominant” factors linked to the post-1800s warming trend include solar forcing, volcanic forcing, and the Atlantic Multi-decadal Oscillation (Diodato et al., 2024).
In other words, the modern warming as well as the past climate changes may be “primarily due to natural variations in cloudiness and surface albedo, which have served as the main forcing factors” (Diodato et al., 2025).
IDAHO GOV VETOES MEDICAL FREEDOM BILL
The HighWire with Del Bigtree | April 3, 2025
A sweeping bill to ban forced medical interventions in Idaho, including vaccines and masks, passed both chambers only to be vetoed by Governor Brad Little, who ironically cited “medical freedom” in his opposition. Now, a political clash brews as Attorney General Raul Labrador urges lawmakers to override the veto and defend Idahoans from future mandates.
Featured Video
The Iran War has destroyed fertilizer markets and farmers everywhere, almost
or go to
Aletho News Archives – Video-Images
From the Archives
Truth, History and Integrity
By Gilad Atzmon | March 13, 2010
… As devastating as it may be, at a certain moment in time, a horrible chapter was given an exceptionally meta-historical status. Its ‘factuality’ was sealed by draconian laws and its reasoning was secured by social and political settings. The Holocaust became the new Western religion. Unfortunately, it is the most sinister religion known to man. It is a license to kill, to flatten, no nuke, to wipe, to rape, to loot and to ethnically cleanse. … Read full article
Blog Roll
 Aletho News
Aletho News- Iran rejects US assassination claim, says Washington trying to whitewash its own crimes against Iranians
- The Iran War has destroyed fertilizer markets and farmers everywhere, almost
- Capitulate or Die: The Gaza ‘peace process’ and Western propaganda
- FSB Blows Lid on Western Plot to Hack Russian Officials’ Phones — But Here’s the Shocker
- Do Palantir’s bosses have blood on their hands over the Starobelsk massacre?
- US Eyes Spreading its Nuclear Footprint Deeper into Europe – Report
- Kiev admitted it launched drones at NATO member – media
- Russia Raises Alarm Over Ukraine’s Surging Black Sea Terrorist Activity
- ‘Luring Russia into war’
- Russia accuses France and the UK of piracy over cargo ship seizure
- If Americans Knew
- Israeli settlers, soldiers, gov’t go all out against West Bank Palestinians – Daily Update
- A Slow-motion Execution of the West Bank Health System
- The Palestinian journalists held in Israel’s ‘cemeteries for the living’
- Super PAC Network Backing Connie Chan Received Hundreds of Thousands from AIPAC
- Israel’s Solution to the Gaza Problem Is Well Underway
- UK Bans Prominent Commentators Over Their Statements on Israel
- Israel’s killing machine deepens its invasion into Lebanon – Daily Update
- ‘To call it a ceasefire is a joke’: Israeli soldiers share rare accounts from Gaza with AP
- Israeli Espionage: How Israel and its American agents stole US uranium
- From Paul Findley to Thomas Massie: How the Israel Lobby Purges Republican Dissenters
- No Tricks Zone
- Germany’s Ecological Holocaust… Once Fairy Tale Forests Getting Cleared For Wind Turbines
- A Grand Solar Minimum Has Arrived…Global Cooling Of At Least 1°C Is Expected By The 2030s, 2040s
- European “Expert Commission” Urges COVID-19-Like Global Climate State Of Energency!
- Real-World Observations Do Not Support The Position That Climate Change Is Human-Caused
- Germany’s AfD Party Calls Debunked Climate Scenarios “Greatest Fraud In Human History”
- Researchers Find Rapid Global Warming Phase At End Of Last Ice Age (Ca.18,000 Years Ago)
- Even The DNA Of Single-Celled Plankton Can Upend Alarmist Arctic Sea Ice Melt Claims
- Scandal: Although Climate Panic Is Canceled By IPCC, Europe’s Policymakers Continue With Their Crushing Policies
- How Once Hardcore Climate Alarmist Lucy Biggers Realized It Was All A Scam, Brainwashing
- German Expert: “No Climate Crisis” …”Warming Generally Better For Humanity”
