Scientist at center of lab leak controversy to lead the Lancet’s task force to investigate virus origin
By Steve Watson | Summit News | June 4, 2021
Revered scientific journal The Lancet has created a ‘task force’ to investigate the origins of the coronavirus that caused a global pandemic, yet it has decided to employ as its leader the very guy who funded the dangerous gain of function research at the Wuhan lab and subsequently allegedly ‘bullied’ other scientists into avoiding looking into the lab as a potential source of the outbreak.
In the wake of renewed scrutiny of the lab leak hypothesis, the Lancet’s task force will reportedly “focus on analyzing data on all of the theories put forward on the origins of COVID, on the reasons why SARS-CoV-2 was able to break out of Wuhan and spread globally, and on the most plausible strategies to prevent future pandemics.”
It also states that “The Task Force will review thoroughly and objectively all publicly available evidence, particularly the peer-reviewed literature, and conduct interviews with key leaders in science, medicine, policy and civil society.”
‘Objectively’. Right.
Dr Peter Daszak, who is heading up this task force, is perhaps the least suitable scientist on the planet to objectively analyse the data, given his track record.
Daszak, as President of the EcoHealth Alliance, shovelled at least $600,000 to the Wuhan Institute of Virology in the past few years to play around with coronaviruses inside the lab through the now infamous ‘gain of function’ research.
Daszak, who also works for the World Health Organisation, is on record admitting that he was involved with manipulating coronaviruses. Here is a video of him talking in DECEMBER 2019 about how ‘good’ the viruses are for altering in a lab:
Daszak notes that “coronaviruses are pretty good… you can manipulate them in the lab pretty easily… the spiked proteins drive a lot about what happens. You can get the sequence you can build the protein, we work with Ralph Baric at UNC to do this, insert into the backbone of another virus and do some work in a lab.”
No wonder then that Daszak as lead investigator for the WHO investigation determined within 3 hours of visiting the Wuhan lab in February 2021 that there was ‘nothing to see here’?
Recently released emails now document that Daszak thanked Dr Fauci for dismissing the lab leak theory before any scientific research had been done on the possibility.

Daszak was later employed as an ‘expert fact checker’ by Facebook when it was monitoring and removing ‘misinformation’ about the origins of COVID on its platform, much of which was credible scientific research. Facebook has since reversed the policy of banning any posts containing information suggesting COVID-19 was “man-made”.
Daszak’s Twitter profile is basically one long ‘it came from bats not a lab’ thread, much to the annoyance of some other scientists:
Why does this guy keep getting put in charge of investigations, task forces and ‘fact checking’, when it’s abundantly clear that he has the biggest motive to dismiss the lab leak notion?
As microbiologist Professor Richard Ebright has noted, “Daszak was the contractor who funded the laboratory at the Wuhan Institute of Virology that potentially was the source of the virus with subcontracts from $200million [£142million] from the US Department of State and $7million [£5million] from the US National Institutes of Health and he was a collaborator and co-author on research projects at the laboratory.”
Daszak has already lied about the type of research that was being conducted at the Wuhan lab, claiming, after the outbreak happened, that he didn’t know if it was gain of function or not. His own previous statements, and the Fauci emails prove he knew full well what was going on in the lab.
In addition, as reported by The Daily Mail and other outlets, Daszak “orchestrated a ‘bullying’ campaign and coerced top scientists into signing off on a letter to The Lancet aimed at removing blame for Covid-19 from the Wuhan lab he was funding with US money.”
Daszak used his influence to get the journal to publish the letter, which stated that to even suggest the lab leak theory had any credibility was equal to spreading “fear, rumours, and prejudice.”
It effetely shut down discussion among the scientific ‘consensus’ of the lab leak potential for a whole year until intelligence findings brought the matter back to the attention of the mainstream media.
WHO scientific advisor Jamie Metzl described Daszak’s letter as “scientific propaganda and a form of thuggery and intimidation.”
“By labelling anyone with different views a conspiracy theorist, the Lancet letter was the worst form of bullying in full contravention of the scientific method,” Metzl added.
The letter further stated that “We stand together to strongly condemn conspiracy theories suggesting that Covid-19 does not have a natural origin,” and even had the audacity to state that “We declare no competing interests.”
Indeed, Daszak had made sure that the letter would be devoid of any link to EcoHealth, and even considered leaving his own name off it, emails released via the Freedom of Information Act have revealed.
To make matters worse, the other members of The Lancet’s task force are practically all minions of Daszak, some of whom helped him draft the letter that unequivocally stated the lab leak theory was dangerous, and others who either worked with him on ‘fact checking’ for Facebook, or were cited as sources during that activity.
Taking all this into account, it is obvious what the outcome of The Lancet’s inquiry will be, and it should not and cannot be used as credible evidence against the lab leak theory.
Why Is There Such Reluctance to Discuss Natural Immunity?
By Jon Sanders | AIER | June 4, 2021
If you’re among those of us who aren’t tribally invested in Covid politics but would like good information about when life will resume as normal, chances are you’re interested in herd immunity. You’re likely not interested in having to rely on the Internet Archive for good information on herd immunity. Alas, it’s become a go-to place for retrieving, as it were, previously published information on herd immunity that became inconvenient post-vaccine and then virtually Memory-Holed.
Over the past 15 months, the litany of Experts’ True Facts and Science regarding various aspects of SARS-CoV-2 has changed more often than the starting lineup of a bad minor league ball club. Covid-19 is spread by droplets, especially from asymptomatic people, until one day it was airborne all along and people who weren’t sick in all likelihood weren’t even sick. Stay at home, you’re safer indoors, even stay away from parks and beaches; well, actually, outdoors is the place to be. Masks don’t work against viruses and are actually unhealthy to wear if you’re not sick, then suddenly they did work and without one you might as well be shooting people. Everyone knows and PolitiFact verified that the virus couldn’t have been created in the prominent infectious disease lab doing gain-of-function research on coronaviruses in bats coincidentally at Covid Ground Zero until, one day, PolitiFact had to retract the entire “Pants on Fire!” article. And so forth.
Unfortunately, information about herd immunity has also not been immune to this kind of meddling. Until recent months, people readily understood that active immunity came about either by natural immunity or vaccine-induced immunity. Natural immunity comes from battling and defeating an actual infection, then having your immune system primed for the rest of your life to fight it off if it ever shows up again. This immunity is achieved at a sometimes very high personal price.
Vaccine-induced immunity is to prime your immune system with a weaker, non-threatening form of the invading infection, so that it’s ready to fight off the real thing should you ever encounter it, and without your having first to risk severe illness or death.
Those interested in herd immunity in itself likely don’t have a moral or political preference for one form of immunity to the exclusion of the other. Immunity is immunity, regardless of whether a particular person has it naturally or by a vaccine. All immunity contributes to herd immunity.
Others, however, are much less circumspect. They seem to have forgotten the ultimate goal of the public campaign for people to receive vaccination against Covid-19. It’s not to be vaccinated; it’s to have immunity. People with natural immunity — i.e., people whose immune systems have faced Covid-19 and won — don’t need a vaccine.
They do, however, need to be considered in any good-faith discussion of herd immunity. There are two prongs to herd immunity, as we used to all know, and those with natural immunity are the prong that’s being ignored. It’s not just mere oversight, however. Fostering such ignorance can lead to several bad outcomes:
- People with natural immunity could be kept from employment, education, travel, normal commerce, and who knows what other things if they don’t submit to a vaccine they don’t need in order to fulfill a head count that confuses a means with the end
- The nation could already be at herd immunity while governors and health bureaucrats continue to exert extreme emergency powers, harming people’s liberties and livelihoods
- People already terrified of Covid — including especially those who’ve already had it — would continue to live in fear, avoiding human interaction and worrying beyond all reason
- People could come to distrust even sound advice from experts about important matters, as they witness and grow to expect how what “the experts” counsel diverges from what they know to be wise counsel while it conforms to and amplifies the temporary needs of the political class
Those of us wanting good information certainly don’t want any of those outcomes. But others seem perfectly fine to risk them. They include not only elected officials, members of the media, political talking heads, self-important bureaucrats, and their wide-eyed acolytes harassing shoppers, but strangely also highly prominent health organizations.
For example, late last year Jeffrey Tucker showed that the World Health Organization (WHO) suddenly, and “for reasons unknown,” changed its definition of “herd immunity.” Using screenshots from a cached version on the Internet Archive, Tucker showed how the WHO altered its definition in such a way as to erase completely the role of natural immunity. Before, the WHO rightly said it “happens when a population is immune either through vaccination or immunity developed through previous infection.” The WHO’s change stated that it happens “if a threshold of vaccination is reached.” Not long after Tucker’s piece appeared, the WHO restored natural immunity to its definition.
The Food and Drug Administration (FDA), seemingly apropos of nothing, on May 19 issued a “safety communication” to warn that FDA-authorized SARS-CoV-2 antibody tests “should not be used to evaluate immunity or protection from COVID-19 at any time.” The FDA’s concern appears to be that taking an antibody test too soon after receiving a vaccination may fail to show vaccine-induced antibodies, but why preclude its use for “identifying people with an adaptive immune response to SARS-CoV-2 from a recent or prior infection?” Especially after stating outright that “Antibody tests can play an important role in identifying individuals who may have been exposed to the SARS-CoV-2 virus and may have developed an adaptive immune response.”
Then there is the National Institute of Allergy and Infectious Diseases director, Dr. Anthony Fauci, that ubiquitous font of fatuous guidance. He had told people that herd immunity would be at 60 to 70 percent immunity, and then he started publicly cinching those numbers up: 75 percent, 80 percent, 85 percent, even 90 percent (as if Covid-19 were as infectious as measles). He is quoted in the New York Times admitting to doing so deliberately to affect people’s behavior:
“When polls said only about half of all Americans would take a vaccine, I was saying herd immunity would take 70 to 75 percent,” Dr. Fauci said. “Then, when newer surveys said 60 percent or more would take it, I thought, ‘I can nudge this up a bit,’ so I went to 80, 85.“
Now — or better put, as of this writing — Fauci has taken to arguing herd immunity is a “mystical elusive number,” a distracting “endgame,” and therefore not worth considering. Only vaccinations are worth counting. As he put it recently, “We don’t want to get too hung up on reaching this endgame of herd immunity because every day that you put 2 million to 3 million vaccinations into people [it] makes society be more and more protected.”
While composing an article about natural immunity and herd immunity for my home state of North Carolina, I happened to notice that the Mayo Clinic had removed a compelling factoid about natural immunity. It’s something I had quoted in an earlier discussion of the matter and wanted to revisit it.
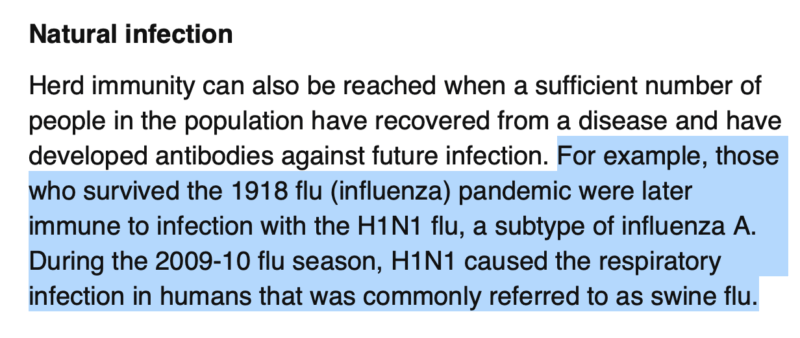
Here’s what the Mayo Clinic once wanted people to know in its page on “Herd Immunity and COVID-19” with respect to natural immunity: “[T]hose who survived the 1918 flu (influenza) pandemic were later immune to infection with the H1N1 flu, a subtype of influenza A.” The Mayo Clinic pointed out that H1N1 was during the 2009-10 flu season, which would be 92 years later. That finding attested to just how powerful and long-lived natural immunity could be.
As can be seen from the Internet Archive, however, sometime after April 14 the Mayo Clinic removed that compelling historical aside:
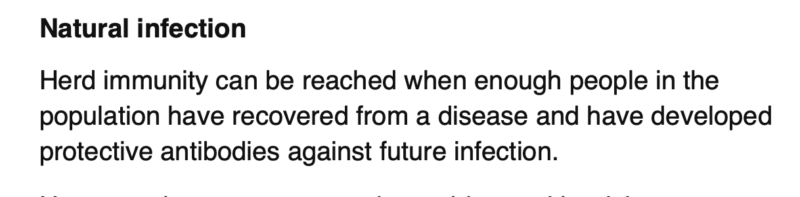
The Mayo Clinic also reoriented its page to feature vaccination over “the natural infection method” (method? ) and added a section on “the outlook for achieving herd immunity in the U.S.” This new section stated that “it’s not clear if or when the U.S. will achieve herd immunity” but encouraged people nonetheless that “the FDA-authorized COVID-19 vaccines are highly effective at protecting against severe illness requiring hospitalization and death … allowing people to better be able to live with the virus.”
Why, from people who know better, is there so much interest in downplaying or erasing natural immunity?
Is it because it’s hard to quantify how many people have natural immunity? Is it out of a mix of good intentions and worry, that discussing natural immunity would somehow discourage (“nudge,” in Fauci’s term) people from getting vaccines who otherwise would? Is it simple oversight, being so focused on vaccinations that they just plain forgot about natural immunity? Or is something else at work?
Whatever the reason, it’s keeping Americans in the dark about how many people have active immunity from Covid-19. It’s keeping people needlessly fearful and suspicious of each other. It’s empowering executive overreach. Worst of all, it’s tempting people to consider government and business restrictions on the unvaccinated, regardless of their actual immunity.
Jon Sanders is an economist and the senior fellow of regulatory studies and research editor at the John Locke Foundation in Raleigh, North Carolina.
The real conspirators who lied about Covid’s origin, funded fraudulent trials of therapeutics, and controlled the Covid pandemic are the top public health leaders
By Meryl Nass, MD | June 3, 2021
In very early 2020 there was a lot of chatter about where the virus, later named SARS-CoV-2, actually came from. In an excellent, detailed article for the Bulletin of the Atomic Scientists, former NY Times science writer Nicholas Wade describes how two short pieces published in The Lancet and Nature Medicine in Feb-March 2020 determined how this chatter would be channeled.
These two extraordinarily influential pieces, each simply titled as a “Correspondence,” were parroted by the mainstream media for a year. Each was plainly intended to shut down any discussion of a possible lab origin.
I happened to read both Correspondences in March 2020 and it was immediately apparent to me that each was designed as a propaganda tool. Neither had anything to do with science. In fact, the Andersen Correspondence butchered the science. Each had an unusual concatenation of authors.
I was so intrigued by these articles that I kept searching the net to understand them, and discovered that Francis Collins, the NIH Director, had blogged on March 26 about the Nature Medicine Correspondence, suggesting it should put an end to conspiracy theories about lab origin.
I further found the letter from the 3 heads of the US National Academy of Science, Engineering and Medicine, which had been referred to by the Lancet Correspondence authors. But it had not yet been published when the Lancet correspondence was written, suggesting again some hidden connection (or mutual effort) involving the author(s) of the National Academies letter and the Lancet Correspondence author(s).
I wondered why 5 otherwise credible scientists would sign their names to the Nature Medicine Correspondence, when the arguments made in the paper were nonsensical. I concluded that they had been put up to it by a ‘hidden hand,’ and when I was interviewed for the film that became Plandemic 2: Indoctornation I said so. (The film has been banned and shadowbanned, as have many of my writings, so it is impossible to find using google or a standard search engine. Here it is on Bitchute, using the Ecosia search engine.)
Months ago, in another email drop obtained by US Right to Know, we learned that Peter Daszac, CEO of the nonprofit EcoHealth Alliance, was the primary but hidden author of the Lancet Correspondence. He was also the primary beneficiary, since his organization had been used as the pass through to send money from the NIAID to the Wuhan coronavirus lab. (Some might consider this method of giving out grants as a fancy way of money laundering.) Daszac, like Fauci, earned over $400,000/year. He was also a member of the WHO Covid origins investigative team, and had been selected as the head of the Lancet Covid origins investigative team. But the Lancet-sponsored investigation looks like it is now dead in the water. The WHO and the Lancet thus seem to be co-conspirators, choosing the fox (Daszac) to guard the henhouse (the natural origin theory of Covid).
Today, I was sent a link to a specific one of Fauci’s emails, and the mystery of why 5 well known scientists coauthored drivel, which the venerable Nature Medicine journal published, and which was then used as the foundation supporting the claim of Covid’s natural origin, was solved. Here’s the email.

The first author of the Nature Medicine paper thanks 3 incredibly important people for their “advice and leadership” regarding the paper. All 3 are MD researchers, and they dole out more money for medical research than anyone else in the world, perhaps excepting Bill Gates. Fauci runs the NIAID; Collins is the NIH Director (nominally Fauci’s boss) and Sir Jeremy Farrar is the director of the Wellcome Trust. Jeremy also signed the Lancet letter. And he is the Chair of the World Health Organization R&D Blueprint Scientific Advisory Group, which put him in the driver’s seat of the WHO’s Solidarity trial, in which 1000 unwitting subjects were overdosed with hydroxychloroquine in order to sink the use of the drug for Covid. Jeremy had worked in Vietnam, where there was lots of malaria, and he had also been involved with SARS-1 there. He additionally was central in setting up the UK Recovery trial, where 1600 subjects were overdosed with hydroxychloroquine. I think he had some idea of the proper dose of the chloroquine drugs from his experience in Vietnam. But even if he didn’t, Farrar, Fauci and Collins would have learned about such overdoses after Brazil told the world about how they mistakenly overdosed patients in a trial of chloroquine for Covid, published in the JAMA in mid April 2020. Thirty-nine percent of the subjects in Brazil who were given high doses of chloroquine died, average age 50.
Yet the Solidarity and Recovery hydroxychloroquine trials continued into June, stopping only after their extreme doses were exposed.
Fauci made sure to control the treatment guidelines for Covid that came out of the NIAID, advising against both chloroquine drugs and ivermectin. Fauci’s NIAID also cancelled the first large-scale trial of hydroxychlorquine treatment in early disease, after only 20 of the expected 2,000 subjects were enrolled.
What does all this mean?
- There was a conspiracy between the five authors of the Nature Medicine paper and the heads of the NIH, NIAID and Wellcome Trust to cover up the lab origin of Covid.
- There was a conspiracy involving Peter Daszac, Tony Fauci and others to push the natural origin theory.
(See other emails in the recent drop.)
- There was a conspiracy involving Daszac to write the Lancet letter and hide its provenance, to push the natural origin theory and paint any other ideas as conspiracy theory. Collin’s blog post is another piece of this story.
- Farrar was intimately involved in both large HCQ overdose trials (in which about 500 subjects total died).
- Farrar, Fauci and Collins withheld research funds that could have supported quality trials of the use of chloroquines and ivermectin and other repurposed drugs that might have turned around the pandemic.
- Are the 4 individuals named here intimately involved in the creation of the pandemic, as well as the prolongation and improper treatments used during the pandemic?
Below are my two early posts on this subject from March and April 2020, and a snippet from the Lancet Correspondence, with a list of signatories.
I don’t want to take credit improperly. Dan Sirotkin noticed the Nature Medicine article before I did, and wrote lucidly about it. I did not see his writing until much later.
Thursday, March 26, 2020
There are many ways the novel coronavirus may have come about/ Nass
Nature Medicine ran a 3 page article that claimed to explain why the novel coronavirus is not a lab construct. USA Today wrote a summary piece explaining it:
“If someone were seeking to engineer a new coronavirus as a pathogen, they would have constructed it from the backbone of a virus known to cause illness,” the report said. “But the scientists found that the SARS-CoV-2 backbone differed substantially from those of already known coronaviruses and mostly resembled related viruses found in bats and pangolins.”—USAT
Yet it turns out to be a specious argument, relying on the fact that the novel coronavirus backbone sequence was not already known in the open virology literature.
- While starting from a known RNA sequence is one easy way to create a pathogen, it is certainly not necessary to do so.
- Nor is it likely that biodefense/biowarfare programs share knowledge of all their creations. They never have before.
- a) Finally, it is relatively easy to detect the human hand when a chimera of known virulence factors is strung together.
- b) But because plausible deniability is a critical component of a bioweapons attack, I doubt that a chimera using known sequences is the path that would have been followed by a modern biowarrior.
I will briefly mention some of the old techniques for creating bioweapons, none of which require that a known, published RNA backbone would be required to build a novel, virulent coronavirus:
- China has unique bats. So do other countries. Unique bats likely harbor unique viruses. Bits of these viruses can be strung together, while no outside parties are aware that these particular RNA threads exist in nature.
- You take an already virulent RNA virus, subject it to high rates of mutation via chemical or radiological exposure, and test the viruses that survive for the acquisition of new virulence characteristics.
- You simply passage the virus through tens, hundreds or thousands of lab animals or cell cultures and test the results for acquisition of new virulence characteristics.
- You mix different viruses together with different virulence characteristics, allow them to grow together, and seek recombinants that have obtained the desired new mix of virulence factors.
All these possibilities result in viruses that are hard to pin on lab production. I dare the Nature Medicine scientists to dismiss these scenarios.
Still, I doubt that any national program would deliberately release this coronavirus onto the people of the earth, because it is so hard to control.
Historically, bio-weaponeers have required their creations to be controlled at all costs. In one well-documented example of biowarfare, unleashing African swine fever on a Caribbean island was associated with no spread beyond the island. In another, anthrax spores were used because they stay put– their use did not cause anthrax cases beyond the borders of Rhodesia (now Zimbabwe).
So why do we have a coronavirus epidemic now?
An accidental biowarfare laboratory release is the best current hypothesis, in my opinion. Such accidental releases have been documented for many decades, throughout the world. But I could certainly be wrong.
Update April 29: Newsweek has been delving into “gain of function” (which means increasing the virulence of a pathogen) coronavirus research in Wuhan, China which might have contributed to the formation of SARS-CoV-2… and the interesting fact (which I posted about here) that the US government provided financial support for this research. Newsweek’s pieces were posted April 27, and 29. My other pieces questioning the origin of SARS-CoV-2 are here and here.
Thursday, April 2, 2020
Why are some of the US’ top scientists making a specious argument about the natural origin of SARS-CoV-2?
- I know about biological warfare/biodefense. I am the first person in the world (according to publicly available literature) to have analyzed an epidemic and demonstrated that the epidemic was due to biological warfare. (1992 study of the 1978-1980 Rhodesian anthrax outbreak, published in Medicine and Global Survival, aka Physicians for Social Responsibility Quarterly (name changed), hosted by International Physicians for the Prevention of Nuclear War).
https://www.ippnw.org/pdf/mgs/psr-2-4-nass.pdf
- Prior to genetic engineering techniques being developed (1973) and widely used (since late 1970s), more ‘primitive’ means of causing mutations, with the intention of developing biological weapons, were employed. Such methods were used by the Japanese beginning in the 1930s, by the US beginning in the 1940s, and by a number of other countries. They resulted in biological weapons that were tested, well-described, and in some cases, used. Such methods were also used subsequent to the 1970s.
- These methods can result in biowarfare agents that lack the identifiable signature of a microbial agent constructed in a lab from known RNA or DNA sequences. In fact, it would be desirable to produce such agents, since it would be difficult to prove they were deliberately constructed in a lab. Here are just a few possibilities for how one might create new, virulent mutants:
- a) exposing microorganisms to chemical or radiological agents that cause high mutation rates and selecting for desired characteristics
- b) passaging virus through a number of lab animals or tissue cultures
- c) mixing viruses together and seeking recombinants with a new mix of virulence factors
- Top scientists circled their wagons to protest against “conspiracy theories suggesting that COVID-19 does not have a natural origin,”in a statement published in the LancetMarch 7. (It was published earlier online.) Their reported aim was to “stand with” public health professionals and scientists in China. Many who signed the statement have worked in biodefense. Signers include Rita Colwell, former director of the National Science Foundation, and James Hughes, former director of CDC’s National Center for Infectious Diseases and former assistant Surgeon General.
https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(20)30418-9/fulltext
Science magazine wrote an article in support of these scientists, which included the following:
The authors of The Lancet statement note that scientists from several countries who have studied SARS-CoV-2 “overwhelmingly conclude that this coronavirus originated in wildlife,” just like many other viruses that have recently emerged in humans. “Conspiracy theories do nothing but create fear, rumours, and prejudice that jeopardise our global collaboration in the fight against this virus,” the statement says.
Five additional scientists soon provided the “scientific evidence” to back up the natural origin claim. These 5 scientists have been affiliated with signers of the statement above, they too have worked in biodefense, and their article was published in Nature Medicine (in the print version) on March 17, 2020.
https://www.nature.com/articles/s41591-020-0820-9
These scientists set up a straw man to knock down: they claimed that had the novel coronavirus (SARS-CoV-2 is the official name of the virus) been created in a lab: “if genetic manipulation had been performed,” then a known coronavirus backbone would have been used. But because no known backbone forms part of SARS-CoV-2, “the evidence shows that SARS-CoV-2 is not a purposefully manipulated virus.”
As USA Today summarized this:
“If someone were seeking to engineer a new coronavirus as a pathogen, they would have constructed it from the backbone of a virus known to cause illness,” the report said. “But the scientists found that the SARS-CoV-2 backbone differed substantially from those of already known coronaviruses and mostly resembled related viruses found in bats and pangolins.”
Their work was then discussed by Francis Collins, the current director of the NIH.
https://directorsblog.nih.gov/2020/03/26/genomic-research-points-to-natural-origin-of-covid-19/
Dr. Collins says,
“Some folks are even making outrageous claims that the new coronavirus causing the pandemic was engineered in a lab and deliberately released to make people sick. A new study debunks such claims by providing scientific evidence that this novel coronavirus arose naturally…
this study leaves little room to refute a natural origin for COVID-19…
Finally, next time you come across something about COVID-19 online that disturbs or puzzles you, I suggest going to FEMA’s new Coronavirus Rumor Control web site…”
I know that the groups of scientists who wrote these pieces in the Lancet and Nature Medicine, as well as NIH Director Dr. Francis Collins, know that you don’t need genetic engineering methods to create a bioweapon. Like me, they are old, they recall a world before genetic engineering, they know the history of biowarfare, and they know the score. Why then are they participating in this charade?
https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(20)30418-9/fulltext
Statement in support of the scientists, public health professionals, and medical professionals of China combatting COVID-19
published online February 19, 2020
CORRESPONDENCE| VOLUME 395, ISSUE 10226, E42-E43, MARCH 07, 2020
- Charles Calisher
- Dennis Carroll
- Rita Colwell
- Ronald B Corley
- Peter Daszak
- Christian Drosten
- Luis Enjuanes
- Jeremy Farrar
- Hume Field
- Josie Golding
- Alexander Gorbalenya
- Bart Haagmans
- James M Hughes
- William B Karesh
- Gerald T Keusch
- Sai Kit Lam
- Juan Lubroth
- John S Mackenzie
- Larry Madoff
- Jonna Mazet
- Peter Palese
- Stanley Perlman
- Leo Poon
- Bernard Roizman
- Linda Saif
- Kanta Subbarao
- Mike Turner
… The rapid, open, and transparent sharing of data on this outbreak is now being threatened by rumours and misinformation around its origins. We stand together to strongly condemn conspiracy theories suggesting that COVID-19 does not have a natural origin. Scientists from multiple countries have published and analysed genomes of the causative agent, severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2),
and they overwhelmingly conclude that this coronavirus originated in wildlife,
,
,
,
,
,
,
,
,
as have so many other emerging pathogens.
,
This is further supported by a letter from the presidents of the US National Academies of Science, Engineering, and Medicine
and by the scientific communities they represent. Conspiracy theories do nothing but create fear, rumours, and prejudice that jeopardise our global collaboration in the fight against this virus.
Counting Covid’s Deceptive Deaths
A look at the unorthodox way in which Covid-19 deaths are registered shows the numbers don’t add up
By Bernard Marx | OffGuardian | June 2, 2021
Four-thousand, nine-hundred and forty one. And rising. This number can only increase or, at best, stay the same. It can never go down.
Of all the innovations that governments and media around the world have come up with, seemingly independently of each other, during the ongoing Covid period, perhaps the most insidious is the daily running total of deaths.
As I write, the number given for Ireland stands at 4,941. And rising.
I have often wondered what the purpose of this number is. At a time when we are frequently told by our betters in the media and in the halls of government to ‘follow the science’, what could be more unscientific than a figure which, even when nobody is dying, looms above us as a warning that danger is ever present and nothing has improved. Bow down before its power, there’s nothing else to be done.
Take the number of people who are unemployed. Here’s a figure that has reached terrifying proportions without any sophistry or assistance from the behavioural science people. In fact, a lot of effort is expended on massaging this number down from the actual amount to levels which are considered more palatable for public consumption.
But imagine that we calculated the number of people who are unemployed by concocting a total of all the people who have been unemployed, at any time and for any duration, during the past 14 months? Or since unemployment began, a running total of all the people who have been unemployed ever?
What function would that number serve? Might it help prevent future unemployment? Might it better inform us of the skills and training required for our workforce? Might it be useful for analysis and reporting? As Frankie Howerd used to say, “Nay, nay, and thrice nay.” I wager any civil servant who proposed such an idea would soon be on their way to early retirement, as popular with politicians as those Gardai who do breathalyzer duty outside Leinster House.
Yet that’s exactly what we do with the running death total (and its near-twin the running case total). If the purpose of this number was to show us where we currently stand amidst the ebbs and flows of the pandemic, then surely a monthly or a weekly total would do the job better. We could then, as we do with the unemployment figure, compare this month to last (or this week to last) and judge which way we’re going. Are we moving steadily forwards? Are we tumbling hopelessly backwards? You get the idea.

Why haven’t we ever had a running total of deaths from cancer, heart attacks or diabetes? If we’d started even a year ago, these numbers would be at impressive levels now. They’d give the Covid tally a run for its money. There’d be opportunities for new betting markets based around causes of mortality, although spread bets might be distasteful for the contagious diseases.
I’m surprised Worldometer hasn’t tried to do something like this. To many of us, Worldometer is the central hub of running Covid death totals. At this very moment, it trumpets a formidable 609,767, deaths for the United States, a daunting 127,782 for the United Kingdom and, as mentioned at the start, a not inconsiderable 4,941 for Ireland.
But what do these frightening numbers refer to? Well, they refer to the number of Covid-19 deaths. So what’s all the fuss about? The fuss is about what constitutes a Covid-19 death. And what is meant, exactly, by a Covid-19 death? Ah, now that’s where it starts to get a bit complicated.
On 16th April 2020, the World Health Organisation (WHO) issued a document entitled “International Guidelines for Certification and Classification (Coding) of Covid-19 as Cause of Death”. This document provided strict rules for the registration of Covid-19 deaths, rules which were fundamentally different to those which were in place for the registration of deaths from other causes.
Some doctors expressed concern about what they felt would give a misleading picture of causes of mortality. These rules, they said, were unprecedented: they would lead to the overreporting of deaths from Covid-19 and the underreporting of deaths from other causes. Their warnings went unheeded and, for the most part, unreported. There was no place for prudence and common sense amid the frenzy and hysteria of the early days of the pandemic.
Since then, however, more and more medical professionals have added their voices to this dissenting chorus. The latest is Patrick O’ Connor, coroner for Mayo and public information officer of the Coroners Society of Ireland.
O’Connor has expressed his discomfort at official reporting of Covid-19 deaths in this country: “I think numbers that are recorded as Covid deaths may be inaccurate and do not have a scientific basis”, he said earlier this month.
Let’s take a look at the International Medical Certificate of Cause of Death (MCCD). For this section I am indebted to Dr. No, the author of the ‘Bad Medicine’ blog, for his succinct explanation of how the MCCD works and how, in practice, the WHO guidelines affect this process. I recommend you read his article about this if you would like a more detailed understanding of the topic.
The MCCD was introduced by the WHO in 1948. Its purpose was to create an international standard for the recording of deaths and to describe the sequence of events which led to a death, rather than just the immediate cause (as was common in many countries at that time).

Frame A (above) is the most important part of the MCCD. It is here that all significant information about a death is recorded. As you can see, Frame A has 2 boxes. Box 1 is for recording the cause of death, Box 2 is for recording contributing conditions. Box 1, the cause of death box, has four lines: the first line records the immediate cause of death, the remaining lines record any conditions which led to the immediate cause of death, with the last line containing the underlying cause of death. The idea is to record the sequence of events which led to the death.
To give an example. A person with diabetes dies from a heart attack, which was caused by heart disease.

So the first line in Box 1 contains ‘Myocardial Infarction’ (the clinical name for a heart attack) because a heart attack was the immediate cause of death. The second line contains ‘Ischaemic Heart Disease’ (the clinical name for heart disease) because this is the underlying cause of death. This is the condition which initiated the sequence of events which culminated in the person’s death: the heart disease led to a heart attack.
The remaining lines in Box 1 are left blank because this person had no other conditions which contributed to the sequence of events leading to their death. Diabetes is recorded in Box 2 because this is a contributing condition, rather than being a part of the sequence of events which led to death. This death will be registered as ischaemic heart disease (or simply heart disease) because this is the underlying cause of death.
Another example. A person dies from internal bleeding due to a ruptured artery as the result of a road traffic accident.

The first line in Box 1 contains ‘Internal Bleeding’ because this is the immediate cause of death. The second line contains ‘Ruptured Artery’ because this is what led to the internal bleeding. The third line contains ‘Road Traffic Accident’, as this was the underlying cause of death: it was a road traffic accident which initiated the sequence of events that led to the death.
In this instance, Box 2 is left blank as there were no contributing conditions. So, the road traffic accident led to the ruptured artery which led to the internal bleeding. This death will be registered as a road traffic accident.
The WHO’s guidelines define a Covid-19 death as “a death resulting from a clinically compatible illness, in a probable or confirmed COVID-19 case, unless there is a clear alternative cause of death that cannot be related to COVID disease (e.g. trauma).” This is an extremely vague definition and one which allows for a rather broad interpretation of what can be considered a Covid-19 death.
As can be seen from the HSE’s website or that of the UK’s NHS, there is a large overlap between the symptoms of Covid-19 and those of any number of other respiratory conditions or Influenza Like Illnesses (ILIs). Any of these other conditions can be considered a “clinically compatible illness”.
You will note that Covid does not have to be confirmed: a “probable” case is sufficient for inclusion as a death. As Dr. No puts it, “If it looks like Covid-19, it is Covid-19.”
The guidance goes on:
A death due to COVID-19 may not be attributed to another disease (e.g. cancer) and should be counted independently of preexisting conditions that are suspected of triggering a severe course of COVID-19.”
This is very important. What physicians are being told here is that, when they have identified a Covid-19 death (using the loose “if it looks like Covid” definition), then regardless of any pre-existing conditions which may have triggered severe Covid-19, the death must be registered and counted as a Covid-19 death. This goes against all conventions for identifying the cause of death.
So how does this relate to our MCCD form? Well, in our earlier examples of somebody dying from a heart attack and somebody dying in a road traffic accident, there should be no difference in the way the deaths are recorded. In fairness to the WHO, they are quite clear in their guidance that these two types of death should not be recorded as Covid-19.
(Unfortunately, this has not stopped overzealous authorities around the world from registering heart failure, motor accidents, suicides and murders as Covid deaths).
However, when it comes to most other types of death, we start getting into murky waters.Take the example of a person who dies from pneumonia, caused by immobilisation, which itself was caused by multiple sclerosis.

In this case, the underlying cause of death is multiple sclerosis. Why? Because multiple sclerosis led to immobilisation which led to pneumonia. So this death will be registered as multiple sclerosis.
Now, let’s imagine this person had tested positive for Covid-19.

Notice anything strange? Because of the WHO guidelines, the underlying cause of death is no longer multiple sclerosis, but is instead Covid-19. Multiple sclerosis (and immobilisation) gets moved to Box 2, it’s now been relegated to a contributing condition. This death will be registered as Covid-19. Remember the WHO said in their guidelines:
A death due to Covid-19 may not be attributed to another disease and should be counted independently of pre-existing conditions.”
A further issue with the above example is that the presence of Covid-19 is determined solely on the basis of a positive PCR test result.
According to the WHO’s clinical coding instructions, a death must be registered as Covid-19 if the patient received a positive test result, even if they never displayed any symptoms.
I’ll be looking at the problems with PCR testing in a future article, but it’s sufficient to say here that they are notoriously unreliable, with even the WHO themselves warning of their tendency to produce false-positive results.
So here we have the case of an unfortunate individual whose multiple sclerosis, over many years, caused them to become immobile. Immobility, sadly, can lead to pneumonia which, especially for the aged and/or immunocompromised, often results in death. However, because of the WHO guidance, the presence of a positive PCR result alone means that all of their medical history, the entire chain of events which led up to the person’s death, is cast aside and replaced by the misleading explanation of Covid-19.
But the issue goes even deeper. You’ll recall that the WHO’s definition of a Covid-19 death includes “probable” cases as well as “confirmed” ones. Our final example describes an individual who dies from acute respiratory distress syndrome (ARDS), caused by pneumonia, which itself was caused by chronic obstructive pulmonary disorder (COPD).

As you can see, the underlying cause of death is COPD, which led to pneumonia, which led to ARDS. This death will, of course, be registered as COPD.
But what if this person had had contact with someone known to have Covid-19 or even with a person suspected of having it? Here’s what would happen to the MCCD:

The underlying cause of death is now ‘suspected Covid-19’, which, in the figures we see on the nightly news and in the vast majority of statistics made available by governments, is treated in exactly the same way as a confirmed Covid-19 death. The WHO’s clinical coding instructions insist that it is, so long as the deceased had “contact with (a) confirmed or probable case.” The COPD which caused this person’s pneumonia is cast aside, no longer considered to have played a part in the sequence of events that led to their death.
This is absurd. Yet this is how deaths around the world are now being recorded and registered.
If somebody is dying of heart disease, liver disease, respiratory disease, cancer, dementia or any other terminal illness, and they have a positive PCR test or have simply been in contact with somebody suspected of having Covid, their death is now registered and counted as a Covid-19 death.
Any pre-existing condition, no matter how serious and no matter what part it played in their ultimate demise, is moved to Box 2 of the MCCD and not recorded as the underlying cause of death. The WHO guidelines state, in the section entitled “Comorbidities”, that “if the decedent had existing chronic conditions…they should be reported in Part 2 of the medical certificate of cause of death.”
Conditions which for more than seventy years, since the introduction of the MCCD form, have been understood as underlying causes of death, are now rebranded as contributing factors. All to make way for the mighty Covid.
The result is a massive inflation of the numbers of Covid-19 deaths. As Patrick O’Connor, the Mayo coroner, says, when speaking about terminally ill patients,
If they prove to be Covid positive in a test, it is that (Covid) which is recorded as the principal cause of death — even though that person may have been terminally ill with a short life-expectancy prior to such testing.”
And, as we have seen, a test is not even necessary, as the WHO’s guidelines instruct physicians to include “probable” with “clinically compatible” illnesses in the tallies.

Patrick O’Connor
Even before the WHO issued their guidelines on 16th April last year, Italian authorities had been using a similar method to register Covid deaths, with 88% of patients there (up to 20th March 2020) having at least one comorbidity and many having two or three.
In addition to hugely inflating the number of deaths from Covid-19, this bizarre way of counting also distorts the mortality rate of the disease, making it seem far more deadly than it actually is.
In 2020, a total of 73,444 people died in England and Wales with Covid-19 recorded as their underlying cause of death. In response to a freedom of information request, on 29th March 2021, the UK’s Office for National Statistics revealed that only 9,400 (12.8%) of that number were recorded without pre-existing conditions.
On July 3rd last, Ireland’s then acting Taoiseach, Leo Varadkar, tweeted,
In Ireland we counted all deaths in all settings, suspected cases even when no lab test was done, and included people with underlying terminal illnesses who died with Covid but not of it”
… revealing that the numbers of Covid-19 deaths in Ireland were vastly exaggerated and in no way reflected the lethality of the disease in this country.
Although the complete death statistics for 2020 have not yet been made available for Ireland, two weeks ago Kildare coroner Professor Denis Cusack published a report analysing deaths in that county during the pandemic. Of 230 deaths recorded with Covid-19 as the underlying cause, 228 (99.13%) had pre-existing conditions.
I would have thought that this was a significant finding, that fewer than 1% of the people who died from Covid-19 in County Kildare did not have comorbidities. But, like anything else that doesn’t fit in with their campaign of terror against the Irish people, the Irish media was having none of it.
While both RTE and The Irish Times gave coverage to Professor Cusack’s report, neither had anything to say about the 99.13% of Kildare’s Covid dead who had pre-existing medical conditions. Nor was there a mention of the average age of death in this cohort being 82.2 years of age.
Both news services instead chose to focus on selected aspects of the report which they used to support the ‘lethal virus’ narrative they have long favoured. Is this censorship? Maybe it’s just extremely poor journalism.
The running total of deaths is one of the pillars that supports this whole charade. The narrative of a deadly pandemic would never have worked without the impression of huge numbers of fatalities, countless lives ‘lost to Covid’. The unprecedented changes in the way deaths are counted allowed this to happen.
You would imagine such a fundamental change, one which has had such a colossal impact on every man, woman and child on the planet, would be widely reported and discussed. Yet it is almost impossible to find a mention of it anywhere in the mainstream media.
Although most of us have suffered under the heel of draconian Covid regulations, and will continue to suffer, some have profited greatly from this fiasco. We have seen how health scares have been manipulated for gain in the past, none more so than the Swine Flu pandemic that never was, in 2009, when governments, the WHO and pharmaceutical corporations colluded to profit at our expense.
There needs to be an urgent investigation, on a global scale, to find out how the Covid pantomime was allowed to happen. And we need one in Ireland, to determine who knew what and when, and exactly who has benefitted.

The current narrative being spun in Ireland is that we are close to ‘finding a way out’ of lockdown and that, if we behave ourselves, we might be permitted some limited freedoms during the summer. This is hardly surprising. We’re coming to the end of coronavirus season, which means it’s so much harder to inflate ‘cases’. And because mortality rates in the northern hemisphere are typically at their lowest during the summer months, it’s not as easy to attribute huge numbers of deaths to Covid-19. It was the same last summer.
But the government has been preparing for this. Already, there are 5 walk-in testing centres in operation in Ireland, with many more planned – a perfect way to boost the numbers up and keep us on our toes for the summer months. And, of course, the government reserves the right, at any moment, to slap us all back into lockdown.
At the same time, it has been made abundantly clear that whatever limited freedoms we might be permitted will be contingent on mass vaccination and, before long, vaccine passports and digital identity.
And don’t forget, coronavirus season comes around again in September. But, as we have seen, the lethality of this disease, for which we’ve radically changed the way we live and have forsworn so much of our freedom, has been blown out of all proportion by the fraudulent way in which deaths are registered.
We suffered under austerity for a decade. It’s hard to believe that the same politicians who decimated our health service, causing untold hardship and death, now want to protect us.
Do we trust they are spending our money honestly and wisely? How much is being spent on mass vaccination, testing, tracing, the vaccine passport infrastructure? And what is the cost of the Covid period to our economy? The whole circus makes a mockery of the years of austerity and of every person who suffered because of them.
Then there is the cost to our health.
Many have lost their lives because of this deception, but you don’t see a running total of their deaths on the news every night. How many have died due to a lack of primary health care, which has been sidelined and neglected, sacrificed at the altar of Covid? How many cancelled surgeries and missed screenings? What about those in urgent need of treatment who were too frightened to attend a hospital? And those who were turned away before they even reached a hospital, because Gardai at a checkpoint deemed their need not sufficiently urgent?
The mental health of our nation has taken a nosedive, not due to Covid but because of lockdowns and other unwarranted sanctions against our people. Loneliness, depression and despair have all taken their toll. The US Centres for Disease Control and Prevention (CDC), hardly a radical anti-lockdown stronghold, has estimated that one third of all excess mortality in the United States during 2020 was due to reasons other than Covid-19.
We’ve been deceived. When important facts are left out of a narrative in order to foster a misconception, we call it lying by omission. We have been lied to by politicians, public health officials, wealthy media barons and the stooges who write for them. And we have paid a terrible price. In the twilight of our freedom, it’s time for us to stand up for the truth.
Bernard Marx is the pseudonym used by a writer and teacher based in Ireland. Bernard’s areas of interest include history, politics and popular music. You can read more his work are Notes from the New Normal
Do SAGE Members Calling for Lockdown to be Extended Beyond June 21st Not Believe the Vaccines Work?
By Will Jones • Lockdown Sceptics • June 1, 2021
So do the vaccines not work then? That’s certainly the impression you’d get from the way various members of SAGE are carrying on, warning of new waves and new variants and the need to delay the end of lockdown even further (completely ignoring the fact that half of America is now open without any problems so far).
As Sherelle Jacobs asks in the Telegraph, why is the debate continuing as though nothing has changed despite half the country – the most vulnerable half – being vaccinated?
Instead of discussing how quickly vaccines could spell the end of restrictions, the commentariat fixates on the risk of another wave as if absolutely nothing has changed. Somehow, despite low deaths, the Indian variant rather than the vaccine has become the game changer.
We have become wearily used to these media interventions from SAGE members in the build-up to key decisions around lockdowns, usually pushing some skewed version of the scientific evidence to frighten the public and pile pressure on the Government to tighten or maintain restrictions. This was bad enough in the autumn before the vaccines were on the scene, but now it leaves you wondering if they know something we don’t about how well the vaccines prevent death and serious disease.
The Government has been continually putting out new research showing how effective the vaccines are, including against the Indian variant, and while I have written on a number of occasions about the shortcomings of these studies, I had been assuming that the vaccines do work, or at least that the Government and its scientists believe they work. With all this talk of third waves and extending lockdown, you have to wonder.
The latest line to justify extending the lockdown is from NERVTAG member Professor Ravi Gupta, who argues for just a few more weeks to let more people get vaccinated, saying there are signs an “explosive” third wave is on the horizon.
Yet according to the latest figures, 51.3% of the adult population has now had one vaccine dose and 31.4% has had two. Over 90% of the over-70s are now fully vaccinated.

The vaccines are supposed to be up to 90% effective at preventing symptomatic infection, including in the over-65s. They are also claimed to be a 90% effective at preventing hospitalisation or death (though presumably their efficacy is reduced somewhat in the frail elderly). This means any new “surge” will have something like one tenth of the infections of earlier waves, while hospitalisations and deaths should be up to a hundred times less – a non-event in infectious disease terms. While these are likely overestimates of vaccine effectiveness, especially among those most susceptible to the disease, there is also naturally acquired immunity and prior immunity that will help to bring the disease burden down.
However you look at it, if the vaccines are going to do their thing then they are already doing it and there’s no point postponing the unlocking. If they’re not working then there’s nothing we can do about it now anyway so we might as well get back to living fully. Either way, the SAGE prophets of doom should be roundly ignored.
COVID Corruption: Assaulting Human Norms

By Omar Khan | Uncommon Wisdom | May 31, 2021
Well, the seminal errors of the Covidian narrative stockpile so fetidly, you keep thinking one day, the stench will be so overpowering, that even those who have essentially put their critical faculties into suspended animation, will rally, finding that this reeks to high Heaven. Some restoratives surely, we think, will thaw their frozen wits.
I keep meandering back through the history of this ill begotten assault on life and liberty.
Imagine this being designated a “novel” Coronavirus. Well, if it was “massaged” in a Wuhan lab as it now seems all the craze to assert, perhaps there was some novelty to it. Otherwise, as we are advised, there are numerous coronaviruses parading around. Even C-19 is now relegated to only being the fourth most widespread in the US.
And now we find, from antibody tests and more, that some varietal was already doing the circuit in 2019. At any rate, some prior immunity exists. And if this is truly the descendant or even Frankensteinian stepchild of SARS, then as former Chief Medical Officer of Pfizer, Michael Yeadon has reminded us, though it is 80% identical, the immune systems of those exposed to SARS seem to “recognize” SARS-CoV-2, even these 17 years hence. Novelty therefore takes another nosedive.
So, this first assertion, right out of the gate, meant to terrorize us by suggesting an unknown pathogen without parallel, that could hoodwink our immune system completely, was poppycock. And we knew soon enough, it was far more infectious than SARS, but far less lethal. And mortality is where we should have kept our eyes fixed, not the delusions of asserted “cases” from unreliable tests. So, no, not so “novel” at least in impact.
Then, you have to wonder, if even mistaken as “novel,” surely there would be extraordinary curiosity, not fixated dogmatism, about this pathogen. However, it took only a few months, before torrential disdain was showered on any who raised questions as to whether we were over-reacting.
There was censorious outrage lavished on some of the world’s most eminent research experts in meta-analysis like John Ioannidis of Stanford, when he pointed out the lethality seemed less than was being forecasted for example, or when the Diamond Princess Cruise Ship kindly offered itself up as a floating case study, or when Knut Wittowski “sacrilegiously” suggested sunshine and fresh air are lethal to viruses with seasonality as a fairly evident way to corroborate that, and so many others. They were literally chased from the public sphere.
They have been only vindicated since, and why rationally, anyone actually interested in public health as a leader, wouldn’t have wanted a big tent of diverse views, a kind of Manhattan Project to tackle this virus and grapple with providing care, cannot be logically answered, except by accepting they were engaged in a charade of public health only, and other agendas were afoot that could brook no dissent.
In fact, if you consider it, how could they know who to censor? In other words, how with a “novel” coronavirus, could you have so readily stress tested alternatives to arrive at any credible consensus by then? Surely if genuinely interested in leadership and health, immensely experienced and credible experts indicating we may be overzealous, that this may be less deadly, more treatable and more manageable, would be manna from heaven. Such views would surely be welcomed, and would be carefully assessed, with trials done before the world was blown up, and irrevocable harm done to urban centers, small businesses, people needing desperate attention for other health issues, and before children’s lives and educations were turned topsy turvy. Yes, “if.”
By the way, it wasn’t even just Ioannidis and Wittowski. Similar alarms were raised and alternatives suggested by luminaries as diverse as Dr. Sucharit Bhakdi, specialist in microbiology and one of the most cited research scientists in Germany; Dr. Pietro Vernazza, Swiss specialist on Infectious Diseases at the Cantonal Hospital St. Gallen; Professor Hendrik Streek, Professor of virology and director of the Institute of Virology and HIV Research at Bonn University; Dr. David Katz founding director of the Yale University Prevention Research Center; Dr. Peter Goetzsche, Professor of Clinical Research Design and Analysis at the University of Copenhagen; Dr. Sunetra Gupta, Professor of Theoretical Epidemiology at the University of Oxford and later co-author of The Great Barrington Declaration; Dr. Anders Tegnell, that sainted man, Swedish State Epidemiologist who showed the world all of these contrary views were essentially right; Dr. Pablo Goldschmidt, Argentine-French virologist, Professor of Molecular Pharmacology at Universite Pierre et Marie Curie Paris; Dr. Jay Bhattacharya, Professor of Medicine and Public Health at Stanford and later co-author of The Great Barrington Declaration; Dr. Tom Jefferson, British epidemiologist based in Rome; Dr. Michael Levitt, Professor of Biochemistry at Stanford; German Network of Evidence Based Medicine… and so many more (distillations of their points can be found archived on Off-Guardian who collated these remarkable instances of “informed lack of consent.”)
When such a phalanx of experience, talent and credibility speaks at a seemingly desperate time, how could jurisdiction after jurisdiction, pillory them, ostracize them, mischaracterize what they had to say? Why that, rather than be desperately curious, and gratefully keen to explore their insights?
This is particularly so as you cannot possibly imagine that this constellation of talent had any motivation other than wishing to save and serve our global and local cultures, lives and livelihoods. And that they have continued to do so, despite media attacks, smears, economic disincentives, renders every word more plausible. After all, we know there are evident incentives of being proponents of the prevailing mythos. We cannot assert any incentive other than integrity and genuine conviction for refusing to acquiesce to the pervasive gaslighting and whitewashing.
Mass Manipulation
While stifling what should have been real life-lines, and once more we are seeing virtually all of their assessments vindicated today, we were run over by a freak-show of blatant stupidities.
With constant panic porn flashing incessantly, a multi-billion dollar industry of fraudulent tests is pushed through a 2-day peer review, by Dr. Doom (Drosten, who helped create the application of the test, sat on the review board of the publication “validating it” and profits from the tests that were mysteriously ready for production and shipping almost ahead of need). We were to ignore demonstrations of false positives, the need for amplification settings to be below 30 (WHO and others initially set them between 35 and 45, at the latter, a papaya fruit tested positive), as well as clarifications the test is not meant to be diagnostic (as per its inventor and as per the literature found in each test and finally “confessed” to post Trump by WHO as well).
And in one of the greatest bits of medical fraud, in plain sight, known by all, but still glossed over, a “case” was converted from someone who had symptoms to “someone who tested positive.”
The latter could be manipulated by the above settings, further counted on to be magnified via false positives, which ironically get worse in percentage terms as incidence goes down. The whole world held hostage to the vagaries of a non-diagnostic test, whereas had we focused on the symptomatic, no one would even have known we were in more than a really ugly influenza season.
Next, we were invited to ignore the age stratification, as the median age of death was over 80. So, lest people be cut down in the bloom of their 70’s and 80’s (and even there we can improve their odds with early treatment, which has been scrupulously avoided, or again smeared, or else “slow walked” almost catatonically en route to being reviewed), we were ready, for the first time in history, to quarantine the healthy!
We asserted “asymptomatic transmission” of which no credible instance has been found in over 14 months, being confirmed again and again even with the recent UK trials done with 9 large, teeming events that barely scraped together 16 “cases” from 60,000 people applying no COVID protocols, including a football FA Club Final and Brit Awards. You will have noticed, a very appreciable lack of media coverage of this “welcome” news. And the US CDC, now in the “vaccine selling” business has instructed clinics to only count as an instance of post-vaccination reinfection, those who, wait for it, have “symptoms.” The blood curdles at these fork tongued guideposts.
So, when the authors of The Great Barrington Declaration pointed out that when risk profiles are so vastly different, we should address and target care accordingly, there was howling and venting and the attacks were unleashed far and wide. They had pointed out this particular pathogen seems to focus on the elderly and so this pandemic tracks normal mortality and therefore in terms of both population size and adjusting for age, is considerably less lethal than the Hong Kong Flu of 1968 and the Asian Flu of the late 50’s, saying nothing of the epochal Spanish Flu in 1918 which infected one third of the global population of that time of which 10% perished!
By comparison, the current Indian death tally after all the shamefully imbalanced reporting is about 325,000 (despite the most egregious liberties with death certificates there, reported on by 161 doctors from N.I.C.E, National Influenza Care Experts, on May 24th in a letter to Prime Minister Modhi claiming guidelines given to them indicate that if PCR test is positive, even if someone died of accidents or clearly of other causes, the cause of death is to be recorded as C-19). Yet applying conventional death certificates, where only direct causation led to an entry, India lost 20 million in the Spanish Flu.
Painfully but necessarily, life went on. High time to adjust our hackles… and self-imposed shackles.
The Indian instance cited above is simply symptomatic of another fraud we embarked upon early on, taking liberties with how death certificates were filled out. Riddle me this, if truly so lethal, why was this necessary suddenly, after norms of indicating primary cause of death were the mainstay of medical practice for decades?
Why did we have to, in the US, incentivize via insurance, labeling COVID deaths? Why in the UK did we originally say anyone tested positively in the last 6 months, irrespective of comorbidities was a COVID death? This shrieks of outright dark comedy or at least ludicrous parody. But that was “fixed” to only doing that for those who tested positive in the last 28 days! So no one knows. Families have howled outrage, reported of course in secondary media, about their loved one being mis-tagged in this way, when they clearly passed from other causes. Who cares? Can’t interfere with the noxious narrative. In parts of South Asia, with cancer and blood poisoning along with a positive test on the death certificate, you guessed it, COVID wins the prize!
And the booby traps for sanity abounded. And the question to be asked is, why? For example,
why do we “lock down”?
This is a penal remedy, never applied before, disdained in public health literature until 2020, indicated in a 2019 report by WHO to
“not be done in any circumstances.”
One month in Wuhan blows up centuries of experience? Really? Are we welding doors shut next? Or staging collapsed bodies on streets with people in alien suits standing over them (you wondered about all those UFO sightings… voila!)?
As Dr. Risch of Yale has pointed out, with such tonic simplicity, “locking down” is not even coherent once the pathogen has spread! It’s fairly obvious once that’s pointed out. And it’s airborne, and almost all infections are in tight indoor spaces. Anyone not pledging fealty to a cult religion, can work this out. And in the face of non locked down jurisdictions with open societies and economies (US States, Sweden, Bulgaria) flourishing, and 30+ studies confirming no benefit from this illogical imposition, and the Oxford Stringency Index showing an inverse relationship between degree of shutdown and health outcomes, we are truly “stoned” on some narcotic to keep invoking this. Oh, and the belligerence if you question it, as if some canonical certainty was being desecrated.
Masking was not recommended by Fauci or WHO, and suddenly realizing that it could be a signature of totemic compliance, it was asserted, though study after study and simply common sense indicates it is a life leeching absurdity, to have you inhale your own waste, while choking off your oxygen supply. As one eminent, also censored, once tenured professor of Physics, Denis Rancourt says,
“The magical ‘one way mask’, which does not protect the wearer but acts as ‘source control’, is an invention of propaganda. It is contrary to the physics of breathing aerosol particles suspended in the fluid air. It is ridiculous fantasy.”
Frankly, the size of the particles are so small as to make this beyond fantasy. And if we truly believed they captured viral particles, would we blithely be leaving these masks lying around, or even throwing them in the open trash, so their harvest can waft at will? The boxes the cloth masks come in, have disclaimers to confess they don’t protect you against C-19. After all, they have openings so you can breathe and see. And there is no correlation between masking or its absence and COVID results. Again, the open US States have put that to rest. But thou must not question! “They say,” is the holy homily, and it must prevail.
So the round-up is: stifle dissent (which admits we have an agenda), create a “test” that doesn’t test and which can be manipulated, change all the guidance based on one month in Wuhan and Italian nursing home deaths (of which later authorities said 12% only could be directly ascribed to C-19), “order” indefinite mass incarceration, and decide without debate that this one source of harm, this one consideration, trumps everything else in the world: health, wealth, family, work, education, poverty, everything.
Why? Who says? A few models. Hmm. Sounds pretty sane. I’m ready to jettison everything I worked for, lived for, my city, culture, neighborhood, travel, way of life, on “asserted apocalypse” without discussing less destructive mitigation with a slew of the world’s most eminent doctors and scientists who say, based on data, we can do better. No agenda there. And if you don’t want the above poison pill, you’re out to kill everyone!
You’re out to kill me, the holy, carcass preserving, center of all global paranoia, me!
Vaccinating Sense
I don’t want to go over past ground to make the necessary point here. As medical luminaries like Dr. Peter McCullough and Dr. Pierre Kory and many others have pointed out, we know there are clearly effective, preventive treatments, and even some real treatments post hospitalization far more effective than the ‘wait and see’ nihilism that so many of these doctors at the forefront of treatment consider “medical malpractice.”
Of course, these treatments were slandered, fraudulently attacked, even though these are widely in use, no side effects, with multiple studies and numerous countries where they’ve been shown to work magnificently (Mexico, India, Zimbabwe, South Africa, parts of the US and more). But since our so called “vaccines”, perhaps the real “point” of this whole inhuman grotesquerie, are only approved tentatively for “emergency use” (safety trials won’t be complete until 2023), then other treatments if established, would remove “the emergency necessity” and that would jeopardize the whole scabrous scam.
Serial entrepreneur Steve Kirsch has even offered $2 million to anyone who can demonstrate that all the randomized trials and global as well as research evidence is wrong, and that the NIH and WHO concern about Fluvoxamine and Ivermectin is justified. A straight $2 million windfall or grant. No one has taken him up on it. His credibility as a medical entrepreneur and philanthropist is unimpeachable.
A few points. You don’t have to remotely be an “anti-vaxxer” (those who oppose them on principle) to be concerned by any or all of the following:
Safety protocols are incomplete
The mRNA treatments are not “vaccines” they are symptom suppressors. Since the vulnerable were not part of the clinical trials, and those trials had such a small subset of the population anyway (‘nominal’ is a generous term), we really don’t know how well they do for the elderly, the vulnerable, etc. And how in that period could we know anything about “safety” and “efficacy?” Booster shots are already being discussed.
All of them have blood clotting issues, 4,000 deaths plus in the US, 10,000 in Europe, both very likely an undercount, as only a small percentage make it into the adverse effects database, and we have swelling evidence, of doctors extremely reluctant to link “anything” to a vaccine, even if a healthy person, within days, dies. Of course you can say, “healthy people also die.” But since in tabulating COVID lethality the norms were at the other extremity, where a “whiff” of COVID put it on the death certificate, we can clearly see again, wanton inconsistency, and again narrative protection at all costs. These deaths are more than the cumulative recorded death from all other vaccines combined, for an illness you have to be tested for to even know you have!
Re-infection has been rife, and mass surges in cases and deaths after mass vaccination in populations (Israel, UK, Gibraltar, Seychelles, Maldives), and now with the Chinese vaccines, Bahrain, Chile and UAE, either no improvement or serious spikes in cases and deaths.
How can anyone call this normal? And so people are opting out, and mania has set in. To induce you to get vaccinated, free ice cream, drinks, the NYC Mayor offering free burgers, lotteries linked to vaccination, dating apps linked to incentivize sexual license.
Yet, as noted, we hear people are getting re-infected? Doesn’t matter, speed past that, just get a jab in every arm. And children? They have no risk, they don’t transmit the disease, shown over and over, Sweden had no deaths in schools with schools open throughout. But suddenly, a 12-year-old can consent in North Carolina to being “jabbed”? Can they also vote, drive, have sex, smoke and drink while they’re at it?
Can anyone call this remotely normal? Experimental gene therapy asserting “safety” you cannot possibly even know (Salk Institute Study indicates that the spike proteins being injected themselves, without even a virus involved, can cause the virus). Future impact is unknown, people are understandably spooked. How is this anywhere close to “informed consent” by the Nuremberg standards?
And what has happened to the EU? But for a few standouts like Denmark and Sweden, they are ready to require “vaccine passports” thereby ignoring those who have recovered and don’t need experimental substances in their body, or those below 60 and healthy with no statistical risk, or children with a truly non-existent risk profile (symptoms easily treatable for them), and with abundant, far safer, preventive treatments? With plummeting numbers, no “pandemic” in Europe, no excess mortality for 2020, what in God’s name is the panic to just jab everything and everyone in sight, including innocent children we are conducting “human trials” on?
This is horror movie material, but chillingly real.
By the way, despite a nominal surge (large in a relative sense as their numbers are so tame), Japan still has among the lowest numbers of deaths per million in the world. 1% of the population is vaccinated.
None of it makes sense, none of it is plausible, any more than the face diapers, penal lock ups, fake non-diagnostic tests, death certificate manipulation, avoiding treatment that reduces hospitalization risk by over 85%, censoring new insights from the most credible experts. All this while blowing up the economy, magnifying poverty, killing children through hunger and awaiting the reckoning when all the currency printing eventually comes home to roost.
So, we have to stop “asking” for relief and move to “demanding” it. And we have to stop acquiescing and trying to “persuade.” No one is this villainously stupid. Villainous maybe. So you can’t “persuade” someone out of a pathology or a psychosis. We can be respectfully, lawfully, civilly disobedient, and make our voices heard, in concert, and purposefully.
This isn’t Life
C.J. Hopkins, writing from “New Normal” Germany describes this version of “living”:
“Perfectly healthy, medical-masked people are lining up in the streets to be experimentally ‘vaccinated’.”
Lockdown-bankrupted shops and restaurants have been converted into walk-in “PCR test stations.” The government is debating mandatory “vaccination” of children in kindergarten. Goon squads are arresting octogenarians for picnicking on the sidewalk without permission.” Sound appealing?
Should I await docilely to be told when to go out, where to go out, what experimental substance to have shot into my body and that of my family? Should I welcome no stimulus, no abandon, no real laughter or mirth, no experiencing of human aptitudes, or going freely to other lands and immersing in other cultures or relishing the world as a part of my birthright? Is it really all right for us to have these political scavengers pick on the remains of our autonomy?
Poet laureate Seamus Heaney writes so unforgettably:
“History says, don’t hope
On this side of the grave.
But then, once in a lifetime
The longed-for tidal wave
Of justice can rise up,
And hope and history rhyme.”
Time to see if we can’t catch one of those waves.
The prose, the poetry, the rhymes, the chimes, of our lives are at stake. And there we must all decide to take a stand, however, whenever and wherever we can, for the future we seek.
Canadian doctor removed from hospital duty after speaking out about COVID vaccine side effects
By Anthony Murdoch | LifeSiteNews | May 26, 2021
LYTTON, British Columbia — A Canadian family doctor says he has been punished by his local health authority because he raised concerns about side effects he observed in some of those who had received the Moderna COVID-19 jab within his community.
“I am no longer allowed to work in the ER,” British Columbia Dr. Charles Hoffe said, according to a True North News report.
Hoffe added that his suspension from the ER came at the end of April, after his local health authority “suspended” his clinical privileges “for the crime of causing ‘vaccine hesitancy,’ for speaking out about my vaccine injured patients.”
In an April 5 letter, Hoffe had written to British Columbia Provincial Health Officer Bonnie Henry that he was “quite alarmed at the high rate of serious side effects from this novel treatment,” in reference to Moderna COVID-19 injections given to 900 mostly Indigenous people in Lytton, British Columbia.
Hoffe said he had observed one patient death, “numerous” allergic reactions, along with three individuals who had “disabling” neurological deficits completed with chronic pain, which persisted “for more than 10 weeks after their first vaccine.”
“So in short, in our small community of Lytton, BC, we have one person dead, and three people who look as though they will be permanently disabled, following their first dose of the Moderna vaccine. The age of those affected ranges from 38 to 82 years of age,” wrote Hoffe.
Following his letter, Hoffe said, he is no longer allowed to work in the ER department of St. Bartholomew’s Health Centre due to his views on the COVID injection. He still can work in his private practice.
“I am still permitted to see patients in my private practice, which is not under the jurisdiction of the Interior Health authority,” Hoffe said. Losing the ability to work in the ER has resulted in his income being slashed by half, which he explained is “the price of advocating for the safety of my patients.”
A community note which was posted on the Lytton Medical clinic door states that Hoffe’s “suspension” by the local health authority will “likely” mean that the “emergency room in Lytton will be closed for at least two weeks out of every month.”
In a recent statement, the College of Physicians and Surgeons of British Columbia (CPSBC) and the First Nations Health Authority (FNHA) said they were aware of “public statements from physicians that contradict public health orders and guidance [being] confusing and potentially harmful to patients.”
CPSBC registrar and CEO Dr. Heidi Oetter threatened to take action against doctors who speak out against the government narrative, saying in the statement that those who “put the public at risk with misinformation may face an investigation by the College, and if warranted, regulatory action.”
Featured Video
Trump Announces Operation To Escort Ships – Fmr. CIA Analyst Larry Johnson
or go to
Aletho News Archives – Video-Images
From the Archives
Israel’s recurring use of terror on civilians

By Bob Finch | January 26, 2009
Insanely disproportionate use of violence against unarmed civilians… continue
Blog Roll
 Aletho News
Aletho News- 1977 Influenza Pandemic Sequence Shows Signs of Laboratory Creation: Journal ‘Cell’
- China issues first prohibition order to safeguard international trade order under rule of law
- Iran rejects Trump’s ‘Project Freedom,’ warns US over Hormuz role
- TRUMP ANNOUNCES OPERATION TO ESCORT SHIPS – Fmr. CIA Analyst Larry Johnson
- A few observations on Iran’s latest proposal to Trump
- ‘I urged that our objective be regime change… so did Netanyahu’ – ex-Trump adviser on Iran
- “STAGED”: Conspiracy Theories Are Everywhere!
- NATO courts screenwriters to embed alliance messaging in film, TV
- Iran replaces UAE ports with Pakistan corridor to break US blockade
- Iran sets one-month deadline for end to US-Israeli war, blockade: Report
- If Americans Knew
- As Palestinians die, Ben-Gvir celebrates birthday with golden noose cake – Daily Update
- Israel’s New Ambassador to the ‘Christian World’ Served as Envoy to Azerbaijan During the Ethnic Cleansing of Christians from Nagorno-Karabakh
- US set to sell $1B “Advanced Precision Kill Weapon System” to Israel – Daily Update
- Israeli Strikes Kill at Least 32 Across S Lebanon, Including Children – Amid “Ceasefire”
- Israel to pour $730m into propaganda arm amid reputational crisis
- Real Cost of Iran War Likely Double the $25 Billion Figure the Pentagon Gave to Congress
- Israel conducts farthest-ever strike in long history of attacks on Gaza humanitarian aid flotillas
- In Gaza, Israel commits 10+ ceasefire violations a day – Daily Update
- US ships 6,500 tons of munitions, equipment to Israel in 24 hours
- A New Library in Gaza Rises From the Ashes of Destruction
- No Tricks Zone
- Another Study Links Warming To Cloud Forcing, Shortwave Radiation, Natural Atmospheric Circulation
- Wind Energy Is Toxic, Hazardous To Human Health, Scientific Review Shows
- Oversupply Of Volatile Solar Energy Leads To Record NEGATIVE Prices!
- New Study: Extreme Heat Records, Heatwaves, Extreme Cold Records Declining Across US Since 1899
- It’s The Cold, Stupid! Cold 20 Times More Lethal Than Heat, Multiple Studies Show
- European Institute For Climate And Energy: “Climate Debate is Seldom About Science”
- New Study: The Climate May Be 5 Times More Sensitive To Solar Forcing Than Commonly Assumed
- EV Industry Reached $70 Billion In Losses In 2024 Due To Delusional Green Ideologies
- Reality Check: Maldives Have Actually Grown In Size Or Remained Stable Over Recent Decades
- Abrupt Climate Change Also Occurred NATURALLY In The Past …25 Times During Last Ice Age

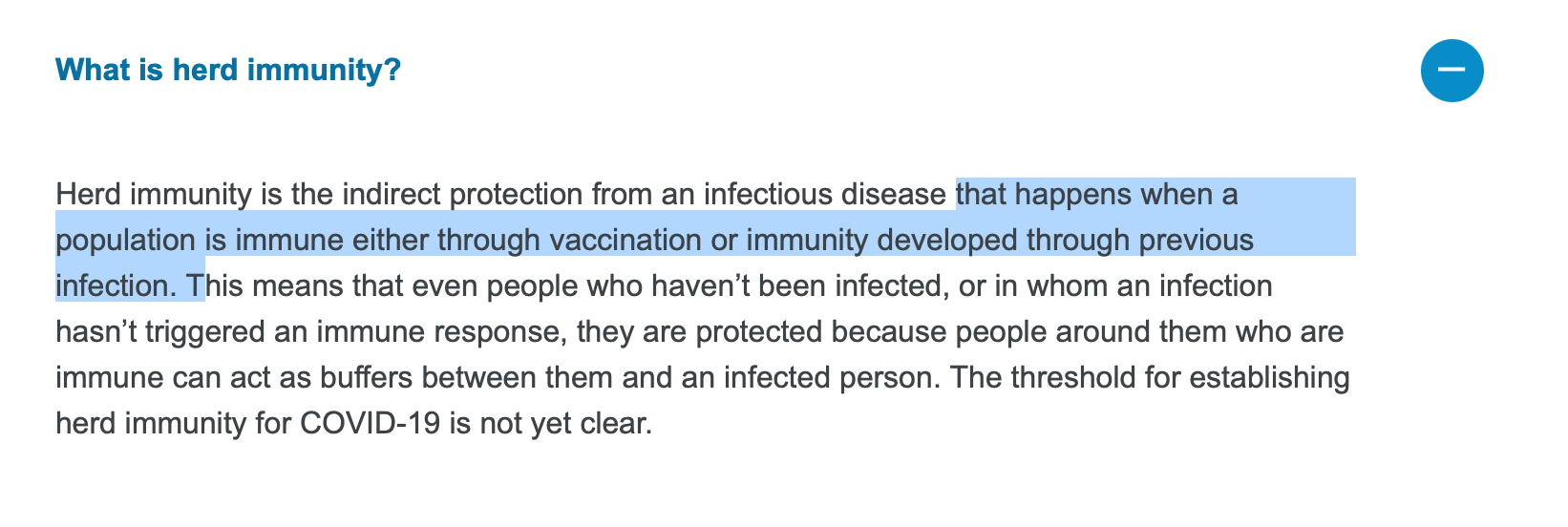{kind=link}
{kind=link}
{kind=link}