“I Don’t Know of a Bigger Story in the World” Right Now Than Ivermectin: NY Times Best-Selling Author
So why are journalists not covering it?
By Nick Corbishley | Naked Capitalism | May 25, 2021
Michael Capuzzo, a New York Times best-selling author, has just published an article titled “The Drug That Cracked Covid”. The 15-page article chronicles the gargantuan struggle being waged by frontline doctors on all continents to get ivermectin approved as a Covid-19 treatment, as well as the tireless efforts by reporters, media outlets and social media companies to thwart them.
Because of ivermectin, Capuzzo says, there are “hundreds of thousands, actually millions, of people around the world, from Uttar Pradesh in India to Peru to Brazil, who are living and not dying.” Yet media outlets have done all they can to “debunk” the notion that ivermectin may serve as an effective, easily accessible and affordable treatment for Covid-19. They have parroted the arguments laid out by health regulators around the world that there just isn’t enough evidence to justify its use.
For his part, Capuzzo, as a reporter, “saw with [his] own eyes the other side [of the story]” that has gone unreported, of the many patients in the US whose lives have been saved by ivermectin and of five of the doctors that have led the battle to save lives around the world, Paul Marik, Umberto Meduri, José Iglesias, Pierre Kory and Joe Varon. These are all highly decorated doctors. Through their leadership of the Front Line COVID-19 Critical Care (FLCCC) Alliance, they have already enhanced our treatment of Covid-19 by discovering and promoting the use of Corticoid steroids against the virus. But their calls for ivermectin to also be used have met with a wall of resistance from healthcare regulators and a wall of silence from media outlets.
“I really wish the world could see both sides,” Capuzzo laments. But unfortunately most reporters are not interested in telling the other side of the story. Even if they were, their publishers would probably refuse to publish it.
That may explain why Capuzzo, a six-time Pulitzer-nominated journalist best known for his New York Times-bestselling nonfiction books Close to Shore and Murder Room, ended up publishing his article on ivermectin in Mountain Home, a monthly local magazine for the of the Pennsylvania mountains and New York Finger Lakes region, of which Capuzzo’s wife is the editor. It’s also the reason why I decided to dedicate today’s post to Capuzzo’s article. Put simply, as many people as possible –particularly journalists — need to read his story.
As Capuzzo himself says, “I don’t know of a bigger story in the world.”
Total News Blackout
On December 8 2020, FLCCC member Dr Pierre Kory gave nine minutes of impassioned testimony to the US Homeland Security Committee Meeting on the potent anti-viral, anti-inflammatory benefits of ivermectin. A total of 9 million people (myself included) saw the video on YouTube before it was taken down by YouTube’s owner, Google. As Capuzzo exhaustively lays out, both traditional and social media have gone to extraordinary lengths to keep people in the dark about ivermectin. So effective has this been that even in some of the countries that have benefited most from its use (such as Mexico and Argentina) many people are completely unaware of its existence. And this is no surprise given how little information is actually seeping out into the public arena.
A news blackout by the world’s leading media came down on Ivermectin like an iron curtain. Reporters who trumpeted the COVID-19 terror in India and Brazil didn’t report that Ivermectin was crushing the P-1 variant in the Brazilian rain forest and killing COVID-19 and all variants in India. That Ivermectin was saving tens of thousands of lives in South America wasn’t news, but mocking the continent’s peasants for taking horse paste was. Journalists denied the world knowledge of the most effective life-saving therapies in the pandemic, Kory said, especially among the elderly, people of color, and the poor, while wringing their hands at the tragedy of their disparate rates of death.
Three days after Kory’s testimony, an Associated Press “fact-check reporter” interviewed Kory “for twenty minutes in which I recounted all of the existing trials evidence (over fifteen randomized and multiple observational trials) all showing dramatic benefits of Ivermectin,” he said. Then she wrote: “AP’S ASSESSMENT: False. There’s no evidence Ivermectin has been proven a safe or effective treatment against COVID-19.” Like many critics, she didn’t explore the Ivermectin data or evidence in any detail, but merely dismissed its “insufficient evidence,” quoting instead the lack of a recommendation by the NIH or WHO. To describe the real evidence in any detail would put the AP and public health agencies in the difficult position of explaining how the lives of thousands of poor people in developing countries don’t count in these matters.
Not just in media but in social media, Ivermectin has inspired a strange new form of Western and pharmaceutical imperialism. On January 12, 2021, the Brazilian Ministry of Health tweeted to its 1.2 million followers not to wait with COVID-19 until it’s too late but “go to a Health Unit and request early treatment,” only to have Twitter take down the official public health pronouncement of the sovereign fifth largest nation in the world for “spreading misleading and potentially harmful information.” (Early treatment is code for Ivermectin.) On January 31, the Slovak Ministry of Health announced its decision on Facebook to allow use of Ivermectin, causing Facebook to take down that post and removed the entire page it was on, the Ivermectin for MDs Team, with 10,200 members from more than 100 countries.
In Argentina, Professor and doctor Hector Carvallo, whose prophylactic studies are renowned by other researchers, says all his scientific documentation for Ivermectin is quickly scrubbed from the Internet. “I am afraid,” he wrote to Marik and his colleagues, “we have affected the most sensitive organ on humans: the wallet…” As Kory’s testimony was climbing toward nine million views, YouTube, owned by Google, erased his official Senate testimony, saying it endangered the community. Kory’s biggest voice was silenced.
“The Most Powerful Entity on Earth”
Malcom X once called the media “the most powerful entity on the earth.” They have, he said, “the power to make the innocent guilty and to make the guilty innocent, and that’s power. Because they control the minds of masses”. Today, that power is now infused with the power of the world’s biggest tech and social media companies. Together social and traditional media have the power to make a medicine that has saved possibly millions of lives during the current pandemic disappear from the conversation. When it is covered, it’s almost always in a negative light. Some media organizations, including the NY Times, have even prefaced mention of the word “ivermectin” — a medicine that has done so much good over its 40-year lifespan that its creators were awarded the Nobel Prize for Medicine in 2015 — with the word “controversial.”
Undeterred, many front-line doctors have tried to persuade their respective health regulators of the unparalleled efficacy and safety of ivermectin as a covid treatment. They include Dr. Tess Lawrie, a prominent independent medical researcher who, as Capuzzo reports, evaluates the safety and efficacy of drugs for the WHO and the National Health Service to set international clinical practice guidelines:
“[She] read all twenty-seven of the Ivermectin studies Kory cited. The resulting evidence is consistent and unequivocal,” she announced, and sent a rapid meta-analysis, an epidemiolocal statistical multi-study review considered the highest form of medical evidence, to the director of the NHS, members of parliament, and a video to Prime Minister Boris Johnson with “the good news… that we now have solid evidence of an effective treatment for COVID-19…” and Ivermectin should immediately “be adopted globally and systematically for the prevention and treatment of COVID-19.”
Ignored by British leaders and media, Lawrie convened the day-long streaming BIRD conference—British Ivermectin Recommendation Development—with more than sixty researchers and doctors from the U.S., Canada, Mexico, England, Ireland, Belgium, Argentina, South Africa, Botswana, Nigeria, Australia, and Japan. They evaluated the drug using the full “evidence-to-decision framework” that is “the gold standard tool for developing clinical practice guidelines” used by the WHO, and reached the conclusion that Ivermectin should blanket the world.
“Most of all you can trust me because I am also a medical doctor, first and foremost,” Lawrie told the prime minster, “with a moral duty to help people, to do no harm, and to save lives. Please may we start saving lives now.” She heard nothing back.
Ivermectin’s benefits were also corroborated by Dr. Andrew Hill, a renowned University of Liverpool pharmacologist and independent medical researcher, and the senior World Health Organization/UNITAID investigator of potential treatments for COVID-19. Hill’s team of twenty-three researchers in twenty-three countries had reported that, after nine months of looking for a COVID-19 treatment and finding nothing but failures like Remdesivir— “we kissed a lot of frogs”— Ivermectin was the only thing that worked against COVID-19, and its safety and efficacy were astonishing—“blindingly positive,” Hill said, and “transformative.” Ivermectin, the WHO researcher concluded, reduced COVID-19 mortality by 81 percent.
Why All the Foot Dragging?
Yet most health regulators and governments continue to drag their feet. More evidence is needed, they say. All the while, doctors in most countries around the world have no early outpatient medicines to draw upon in their struggle against the worst pandemic in century. Drawing on his own experience, Capuzzo describes the absence of treatments for COVID-19 as a global crisis:
When my daughter Grace, a vice president at a New York advertising agency, came
down with COVID-19 recently, she was quarantined in a “COVID hotel” in Times Square with homeless people and quarantining travelers. The locks on her room door were removed. Nurses prowled the halls to keep her in her room and wake her up every night to check her
vitals—not to treat her, because there is no approved treatment for COVID-19; only, if her oxygen plummeted, to move her to the hospital, where there is only a single eective approved treatment for COVID-19, steroids that may keep the lungs from failing.
There are three possible explanations for health regulators’ refusal to allow the use of a highly promising, well-tolerated off-label medicine such as ivermectin:
- As a generic, ivermectin is cheap and widely available, which means there would be a lot less money to be made by Big Pharma if it became the go-to early-stage treatment against covid.
- Other pharmaceutical companies are developing their own novel treatments for Covid-19 which would have to compete directly with ivermectin. They include ivermectin’s original manufacturer, Merck, which has an antiviral compound, molnupiravir, in Phase 3 clinical trials for COVID-19. That might explain the company’s recent statement claiming that there is “no scientific basis whatsoever for a potential therapeutic effect of ivermectin against COVID-19.
- If approved as a covid-19 treatment, ivermectin could even threaten the emergency use authorisation granted to covid-19 vaccines. One of the basic conditions for the emergency use authorisation granted to the vaccines currently being used against covid is that there are no alternative treatments available for the disease. As such, if ivermectin or some other promising medicine such as fluvoxamine were approved as an effective early treatment for Covid-19, the vaccines could be stripped of authorisation.
This may explain why affordable, readily available and minimally toxic drugs are not repurposed for use against Covid despite the growing mountains of evidence supporting their efficacy.
Ivermectin has already been approved as a covid-19 treatment in more than 20 countries. They include Mexico where the mayor of Mexico City, Claudia Scheinbaum, recently said that the medicine had reduced hospitalisations by as much as 76%. As of last week, 135,000 of the city’s residents had been treated with the medicine. The government of India — the world’s second most populous country and one of the world’s biggest manufacturers of medicines — has also recommended the use of ivermectin as an early outpatient treatment against covid-19, in direct contravention of WHO’s own advice.
Dr Vikas P. Sukhatme, the dean of Emory School of Medicine, recently wrote in a column for the Times of India that deploying drugs such as ivermectin and fluvoxamine in India is likely to “rapidly reduce the number of COVID-19 patients, reduce the number requiring hospitalization, supplemental oxygen and intensive care and improve outcomes in hospitalized patients.”
Four weeks after the government included ivermectin and budesonide among its early treatment guidelines, the country has recorded its lowest case count in 40 days.
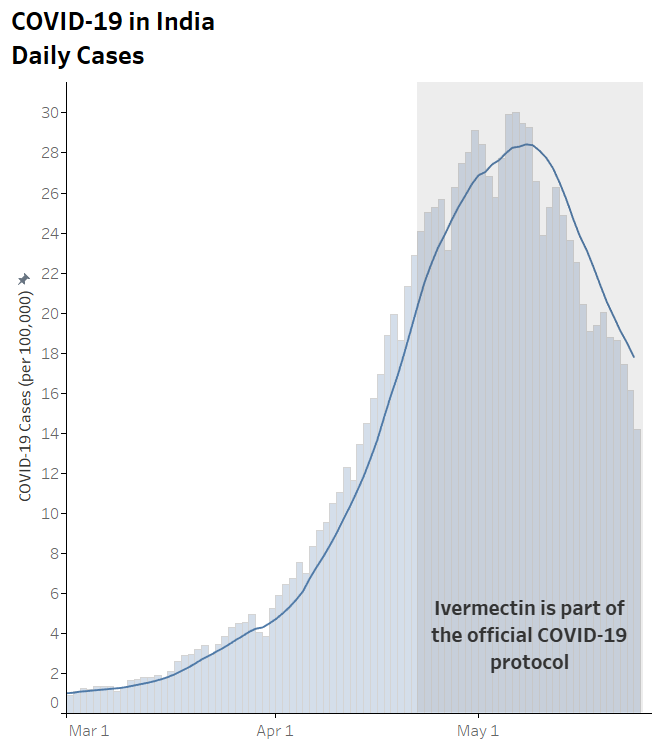
In many of India’s regions the case numbers are plunging in almost vertical fashion. In the capital Delhi, as in Mexico City, hospitalisations have plummeted. In the space of 10 days ICU occupancy fell from 99% to 70%. Deaths are also falling. The test positivity ratio slumped from 35% to 5% in just one month.
One of the outliers of this trend is the state of Tamil Nadu, where cases are still rising steeply. This may have something to do with the fact that the state’s newly elected governor, MK Stalin, decided to exclude ivermectin from the region’s treatment protocol in favor of Remdesivir. The result? Soaring cases. Late last week, Stalin reversed course once again and readopted ivermectin.
For the moment deaths in India remain extremely high. And there are concerns that the numbers are being under-reported. Yet they may also begin to fall in the coming days. In all of the countries that have used ivermectin widely, fatalities are the last thing to fall, after case numbers and hospitalizations. Of course, there’s no way of definitively proving that these rapid falloffs are due to the use of ivermectin. Correlation, even as consistent as this, is not causation. Other factors such as strict lockdowns and travel restrictions no doubt also play a part.
But a clear pattern across nations and territories has formed that strongly supports ivermectin’s purported efficacy. And that efficacy has been amply demonstrated in three meta-analyses.
India’s decision to adopt ivermectin, including as a prophylaxis in some states, is already a potential game-changer. As I wrote three weeks ago, if case numbers, hospitalizations and fatalities fall in India as precipitously as they have in other countries that have adopted ivermectin, it could even become a watershed moment. But for that to happen, the news must reach enough eyes and ears. And for that to happen, reporters must, as Capuzzo says, begin to do their job and report both sides of this vital story.
New Paper: Masks Achieve Nothing In Terms Of Spread
By Damian D. Guerra and Daniel J. Guerra | medrxiv.org | May 29, 2021
Latest analysis shows yet again – yet again – what we already knew from 40 years of published research. And also empirically from simply glancing over the past year’s real-world data. Masks don’t work!
Our main finding is that mask mandates and use are not associated with lower SARS-CoV-2 spread among US states. 80% of US states mandated masks during the COVID-19 pandemic.
Mandates induced greater mask compliance but did not predict lower growth rates when community spread was low (minima) or high (maxima). We infer that mandates likely did not affect COVID-19 case growth [15], as growth rates were similar on all days between actual or modeled issuance dates and 6 March 2021. Higher mask use (rather than mandates per se) has been argued to decrease COVID-19 growth rates [11].
While compliance varies by location and time, IHME estimates are robust (derived from multiple sources [17]) and densely sampled (day-level precision). Higher mask use did not predict lower maximum growth rates, smaller surges, or less Fall-Winter growth among continental states.
Mask-growth rate correlation was only evident at minima. This may be an artifact of faster growth at fewer normalized cases, as well as regional differences in case prevalence early in the pandemic. States in the high mask quintile grew at similar rates as states in the low mask quintile after maxima (when interstate total case differences were smaller than before minima).
In addition, mask use did not predict normalized cases at minima, and low mask growth curves trailed those of high mask (particularly Northeast) states before minima. Growth maxima and Fall-Winter surges did not differ between Northeast and other states. Northeast states exhibited the highest seroprevalence up to at least July 2020 [24] and constituted 80% of the top quintile of mask use, which may explain their comparatively lower Summer growth.
Overall, mask use appears to be an intra-state lagging indicator of case growth. There is inferential but not demonstrable evidence that masks reduce SARS-CoV-2 transmission. Animal models [25], small case studies [6], and growth curves for mandate-only states [16] suggest that mask efficacy increases with mask use [11]. However, we did not observe lower growth rates over a range of compliance at maximum Fall-Winter growth (45-83% between South Dakota and Massachusetts during maxima) [17] when growth rates were high.
This complements a Danish RCT from 3 April to 2 June 2020, when growth rates were low, which found no association between mask use and lower COVID-19 rates either for all participants in the masked arm (47% strong compliance) or for strongly compliant participants only [8].
Masks have generally not protected against other respiratory viruses. Higher self-reported mask use protected against SARS-CoV-1 in Beijing residents [26], but RCTs found no differences in PCR confirmed influenza among Hong Kong households assigned to hand hygiene with or without masks (mask use 31% and 49%, respectively) [27].
Medical and cloth masks did not reduce viral respiratory infections among clinicians in Vietnam [9] or China [10], and rhinovirus transmission increased among universally masked Hong Kong students and teachers in 2020 compared with prior years [28].
These findings are consistent with a 2020 CDC meta-analysis [29] and a 2020 Cochrane review update [30].
Our study has implications for respiratory virus mitigation. Public health measures should ethically promote behaviors that prevent communicable diseases. The sudden onset of COVID-19 compelled adoption of mask mandates before efficacy could be evaluated.
Our findings do not support the hypothesis that SARS-CoV-2 transmission rates decrease with greater public mask use.
As masks are required in public in many US states, it is prudent to weigh potential benefits with harms. Masks may promote social cohesion as rallying symbols during a pandemic [31], but risk compensation can also occur [32]. Prolonged mask use (>4 hours per day) promotes facial alkalinization and inadvertently encourages dehydration, which in turn can enhance barrier breakdown and bacterial infection risk [33].
British clinicians have reported masks to increase headaches and sweating and decrease cognitive precision [34]. Survey bias notwithstanding, these sequelae are associated with medical errors [35]. By obscuring nonverbal communication, masks interfere with social learning in children [36]. Likewise, masks can distort verbal speech and remove visual cues to the detriment of individuals with hearing loss; clear face-shields improve visual integration, but there is a corresponding loss of sound quality [37, 38].
Future research is necessary to better understand the risks of long-term daily mask use [30]. Conversely, it is appropriate to emphasize interventions with demonstrated or probable efficacy against COVID-19 such as vaccination [39] and Vitamin D repletion [40]. In summary, mask mandates and use were poor predictors of COVID-19 spread in US states. Case growth was independent of mandates at low and high rates of community spread, and mask use did not predict case growth during the Summer or Fall-Winter waves.
Strengths of our study include using two mask metrics to evaluate association with COVID-19 growth rates; measuring normalized case growth in mandate and non-mandate states at comparable times to quantify the likely effect of mandates; and deconvolving the effect of mask use by examining case growth in states with variable mask use. Our study also has key limitations. We did not assess counties or localities, which may trend independently of state averages.
While dense sampling promotes convergence, IHME masking estimates are subject to survey bias. We only assessed one biological quantity (confirmed and probable COVID-19 infections), but the ongoing pandemic warrants assessment of other factors such as hospitalizations and mortality. Future work is necessary to elucidate better predictors of COVID-19 spread. A recent study found that at typical respiratory fluence rates, medical masks decrease airway deposition of 10-20μm SARS-CoV-2 particles but not 1-5μm SARS-CoV-2 aerosols [41].
Aerosol expulsion increases with COVID-19 disease severity in non-human primates, as well as with age and BMI in humans without COVID-19 [42]. Aerosol treatment by enhanced ventilation and air purification could help reduce the size of COVID-19 outbreaks.
Don’t Be Stupid – Inform Your Decisions
By Gillian Dymond | OffGuardian | May 28, 2021
Are you tired of having to watch everything you say, in case you’re accused of “hate speech”? Do you frequently have to bite back innocently-spoken words, when someone claims to be “offended” by them? Have you become used to avoiding lively debate or expressing frank opinions on social media, for fear of finding police officers on your doorstep?
If so, you’ll be glad to know that at last there is a whole class of people you may attack with impunity; people who may be derided, slandered and ostracised to your heart’s content; people so selfish and stupid that you are fully entitled to incite hatred against them with the full blessing of your government.
These are the Great Unclean: the “anti-vaxxers” who are not just nasty spoilsports, standing between you and the ever-deferred reopening of society, but who continue to waft death and disease through a world which can only be made safe by universal, and repeated, “jabbing”.
The opportunity to indulge in virtuous hate speech has been seized with zest by household names and obscure Twitterati alike.
“Love the idea of covid vaccine passports for everywhere,” enthuses Piers Morgan, “restaurants, clubs, football, gyms, shops etc. It’s time covid-denying, anti-vaxxer loonies had their bullshit bluff called and bar themselves from going anywhere that responsible citizens go.”
Edwina Currie has emerged from political oblivion to agree:
I hear what you say about someone exercising their freedom not to have a vaccination and they’re perfectly healthy. I don’t want them sitting next to me in the theatre. I don’t want them standing next to me at the theatre bar. I don’t want them next to me or anywhere near me or even in the same carriage on the train. So they can exercise their freedom by staying at home.”
As for the chorus of the immunologically saved on social media, here’s a sample meme:
If you’re antivax and you see me making fun of antivax people, I just want to say I’m talking about you personally and I hope you’re offended because you’re fucking stupid.”
Just try substituting one of a whole range of tenderly protected diversities for “antivax people” or “anti-vaxxers”, and watch the frisson of outrage creeping down any bien-pensant spine. But as the State extends its tolerance, even its encouragement, to our abusers, we covid sceptics, it seems, are fair game.
For there is no quarter from the government for those who are standing aloof from the stampede to get “shots into arms”, as believers in the WHO’s revised definition of herd immunity so crudely like to put it.
This is, after all, a government which, spurred on by behavioural psychologists and with malice aforethought, has industriously stirred up and exploited social disapproval as a potent means of shaming dissent and achieving maximum compliance.
Be kind, they urge you, and deprive yourself and your children of oxygen for your neighbour’s sake. Be responsible, and roll up your sleeve to receive the magic injection that will not only make you immortal but demonstrate your selfless concern for others. Don’t be stupid! Remember, having no symptoms doesn’t mean you’re not a silent super-spreader.
But do sceptics really deserve the contempt being dished out to them so freely?
Are they really so stupid?
Would any self-respecting “anti-vaxxer”, for instance, have been silly enough to come out with the nonsense spouted by the UK’s secretary of state for health, when he told us that:
If you think about it, the vaccine is a tiny bit of the virus in order to get your body to be able to respond.”
Really, Mr Hancock? Are you sure that’s what’s actually on offer here?
Perhaps Mike Yeadon, former head of respiratory research at Pfizer, can set you straight. As he pointed out to James Delingpole recently, “a tiny bit of the virus” is not what goes into these novel treatments – perhaps because, when it comes down to brass tacks, “no-one’s got any”.
What is actually being pumped into millions of arms throughout the world with such careless abandon is not, he says, “just a vaccine”. Although these gene-based medications do “ultimately raise an immune response … the way they do it is completely different from any vaccine we’ve used before … they induce the body, the cells of your body, to actually manufacture a piece of this pathogen, this infective agent. And you respond to that.”
“Anti-vaxxers” could have told you that, Mr Hancock, because they’ve done their own research, and they understand the difference between the traditional idea of a vaccine and what is currently being held up as the golden ticket to freedom. So please stop feeding us blatant untruths about what is actually being injected into all those trusting arms and making its insidious way around millions of bloodstream.
Let’s have the facts that would enable everyone to make a truly informed decision. It really doesn’t help when you fuel sectarian hatred by standing up in parliament and declaring that:
those who promulgate lies about the dangers of vaccines that are safe and have been approved … are threatening lives …”
The obvious response to that is, “those who promulgate lies about the safety of novel and incompletely tested gene therapies doled out on emergency approval only are threatening lives.”
The life of Peter Meadows, for instance: a superlatively healthy seventy-six-year-old, who, trusting government and NHS assurances that the “vaccines” were “safe and effective”, suffered an unprecedented heart attack within hours of receiving the Pfizer jab, and died a few days later: just one of over a thousand post-vaccine fatalities officially logged in the UK’s Yellow Card system to date – or perhaps, as the evidence is increasingly suggesting, of thousands of vaccine-related deaths which, unlike those ascribed to Covid, are not in line with natural mortality profiles.
It seems that those castigated for being “anti-vaxxers” are, in fact, far from stupid. On the contrary, they are the ones sensible enough to take the time and trouble to research and weigh up risks versus benefits before exposing their bodies to any of the novel gene therapies currently being hawked around as “vaccines”.
It is those who don’t search out the facts for themselves who are not using their intelligence, and who are thereby laying themselves open to the smooth sales talk of drug pushers in high places. Peter Meadows and his wife were apparently not handed even the minimal information supplied by the NHS regarding possible side effects they might suffer until after they had received their shots.
They had no idea that the “vaccines” so confidently touted by Matt Hancock were not fully tested for immediate, let alone medium- or long-term, safety, and were issued under the “black triangle” system – ie, were still “subject to intensive safety monitoring”, with the proviso that a record should be kept of all adverse reactions experienced by those acting effectively as human guinea pigs on behalf of the pharmaceutical companies.
What is more, a “high volume” of such adverse reactions were anticipated by the apparently unconcerned UK government before the roll-out began.
Although the Royal Pharmaceutical Society is quick to state that the black triangle label “does not indicate that the product is unsafe for use in patients”, the common-sense response to such a claim, after careful examination of the Yellow Card data, must surely be, “Oh yeah? And now pull the other one!”
In fact, a Pubmed paper advising the US as to whether or not the black triangle system does indeed promote “more judicious prescribing” of new medications, concludes that, “Accelerated drug approvals could cause more uncertainty about drug effectiveness and safety, but specific labeling of newly approved medicines is unlikely to promote more judicious prescribing.”
How much more accelerated could approval be, than the emergency approval accorded to the new coronavirus “vaccines”? And how much less judicious their prescribing, encompassing, as it does, the wholesale jabbing of populations throughout the world, including young people and children, who are at little to no risk of succumbing to the disease, let alone dying of it? It is depressing to learn that Peter Meadows’ daughters had understood enough about the uncertain nature of the hastily concocted “vaccines” to urge their parents not to have the jabs.
Unfortunately, like so many others, the couple were swayed by a longing to return to their old normal, and by peer pressure whipped up by the likes of Matt Hancock and SAGE, rather than by the reasonable concerns raised by their daughters after careful scrutiny of the facts.
So, once more: just how stupid are anti-vaxxers? Interestingly, a recent paper by a team at the Massachusetts Institute of Technology, Viral Visualizations: How Coronavirus Skeptics Use Orthodox Data Practices to Promote Unorthodox Science Online found that, contrary to their popular denigration as “covidiots”, and to the embarrassment of the researchers themselves, covid sceptics “practice a form of data literacy in spades”.
Many of them “express mistrust for academic and journalistic accounts of the pandemic, proposing to rectify alleged bias by ‘following the data’ and creating their own data visualisations.” What they value is “unmediated access to information” and they “privilege personal research and direct reading over ‘expert’ interpretations.” And “Most fundamentally,” say the MIT team, “the groups we studied believe that science is a process, and not an institution.”
Exactly.
In which case, their dismissal of the WHO’s presumption, in claiming to be custodians of “The Science”, is hardly surprising. Nonsense, say the sceptics. Science can never be above questioning. It is not a bundle of rubber-stamped, government-approved dogmas, handy for facilitating some political or commercial agenda.
Like all forms of human knowledge, science remains eternally incomplete, the evolving construction of many minds researching truth in a continuing process of discovery: forming hypotheses, and attempting by all means possible to disprove those hypotheses; seeking to explain or resolve anomalies, but never holding any theory sacrosanct which further investigation might yet prove false; adapting to the gradual unfolding of new perspectives, as fresh evidence shakes the foundations of old paradigms.
It is the alleged “covidiots” and “anti-vaxxers” who, while they may not be scientists themselves, understand the principles on which the scientific method is based. As the MIT study admits, to complain that these irritating people “need more scientific literacy is to characterize their approach as uninformed and inexplicably extreme. This study shows the opposite: they are deeply invested in forms of critique and knowledge production they recognise as scientific expertise.”
All the same, the authors of the study seem to find the concessions they are compelled to make disturbing. “(H)ow do these groups diverge from scientific orthodoxy,” they wonder, “if they are using the same data?” Since all right-minded facts should show decent respect for the statutory consensus, surely anyone inducing them to defect in support of alternative, unsanctioned conclusions must be employing underhand methods?
“We have identified a few sleights of hand that contribute to the broader epistemological crisis we identify between these groups and the majority of scientific researchers,” the defenders of the true faith plead: and they shake their heads at the way “these groups skillfully manipulate data to undermine mainstream science,” quoting as examples the sceptics’ “outsize emphasis on deaths versus cases” and their suspicion of the officially promoted confusion of deaths “with” and “of” covid: both very good reasons, less partial analysts might say, for questioning the figures being spewed out ceaselessly by the government-funded mainstream media, and taken by a terrorised public to be gospel truth.
Yet it’s not just annoying amateurs, with their absurd claims that actual facts should trump any institutionally-coerced consensus, who question the official “narrative” – and, indeed the very existence of a pandemic, as traditionally understood before the WHO decided to “re-imagine” the term, on 4th May 2009, in anticipation of the projected swine-flu apocalypse (in the event, a damp squib, but a useful practice-run for the present resounding success).
After accumulating hard evidence in interviews with over a hundred eminent scientists and other experts, the Corona Investigation Committee, a team headed by Dr Reiner Fuellmich, are likewise challenging the means – essentially, a fraudulent PCR test capable of manufacturing cases on demand and fuelling the myth of the “asymptomatic superspreader” – by which the global coup and its predestined outcome, the push to “get jabs into arms”, have been so artfully engineered.
Dr Fuellmich – a lawyer qualified to practise in both the States and Europe – has already taken on such giants as Deutschebank and Volkswagen. We can only hope that the evidence which he and the rest of the Committee have gathered so painstakingly over the past year and shared with lawyers all over the world will continue to result in court cases where facts will triumph over consensus, vindicating the unvaccinated of “stupidity” before they are forced by the uninformed to wear yellow stars and find themselves rounded up in camps for the unclean.
And that those behind the coup, along with all who enabled and enforced their unlawful actions by “just following orders”, are brought to justice before an international tribunal, to be charged with what the Corona Committee describes as “the greatest crime against humanity ever committed.”
Switch to Remote Learning Caused Large Increases in School Dropout and Learning Losses in Brazil
By Noah Carl • Lockdown Sceptics • May 28, 2021
Back in April, I wrote about a study published in Proceedings of the National Academy of Sciences, which found that Dutch students made “made little or no progress while learning from home”. Now researchers have reported a similar finding in Brazil.
As in the Dutch study, the researchers used rigorous methods to gauge the impact of remote learning on student outcomes. In other words, they didn’t just compare outcomes in 2020 to those the year before.
In São Paulo State (where the study was based) state schools switched to remote learning only at the end of the first quarter, and they continued to teach remotely thereafter. This allowed the researchers to compare the change in outcomes between the first and last quarters of 2020 to the change in outcomes between the same two quarters of 2019.
They looked at two different outcomes: high dropout risk (i.e., whether the student had any math and Portuguese grades on his school record in the relevant quarter), and standardised test scores.
When comparing the change in 2020 to the change in 2019, the researchers found large increases in school dropout and learning losses.
Furthermore, they exploited a natural experiment to gauge the impact of switching back to in-person learning. In the fourth quarter of 2020, some municipalities allowed high-schools but not middle-schools to switch back. This allowed the researchers to compare middle- and high-schools in those municipalities with respect to the change in 2020 versus the change in 2019.
Consistent with the previous result, they found that switching back to in-person learning was associated with higher standardised test scores.
In the authors’ own words, their results show that “the societal costs of keeping schools closed in the pandemic are very large”. As such, they argue that “the public debate should move from whether schools should be open or not to how to reopen them safely”.
MORE Flagrant Data Manipulation from the CDC
New report is further evidence the CDC is deliberately hiding post-vaccine “breakthrough cases”
By Kit Knightly | OffGuardian | May 26, 2021
A new report, published just yesterday, has provided yet more evidence that the CDC is manipulating data to conceal the number of “breakthrough infections”.
A “breakthrough infection” (or “breakthrough case”) is defined as a person who tests positive for Sars-Cov-2 infection, despite already being fully vaccinated. And this new report finds that the CDC’s official record of breakthrough cases is:
likely a substantial undercount.
Going on to explain:
The national surveillance system relies on passive and voluntary reporting, and data might not be complete or representative. Many persons with vaccine breakthrough infections, especially those who are asymptomatic or who experience mild illness, might not seek testing.
Which is partially accurate, but also a pretty major lie by omission.
It is probably true that vaccinated people with no symptoms are unlikely to seek testing, but it is also true that, on March 17th, the CDC updated their advice on testing policy to specifically exclude such people from testing protocols:

Screencap of CDC’s testing guidelines
So, while it’s certainly true that “breakthrough cases” are likely a substantial undercount, it is dishonest to pretend that this is just an accident of the system. Rather, the system is specifically designed to hide such cases.
Of course, this report only goes up to the end of April, the “undercount” will only have gotten worse since then, because the CDC changed their rules AGAIN to make it even harder to keep an accurate count of breakthrough cases.
As we wrote last week, as of May 1st the CDC will no longer be counting mild or asymptomatic cases as “breakthrough infections”, choosing to focus only on hospitalisations and deaths.
According to the CDC’s own report, though, over a quarter (27%) of breakthrough infections were asymptomatic, and a further 61% were only mildly ill. Conversely, only 10% of them were ever hospitalised, and only 2% died:
Based on preliminary data, 2,725 (27%) vaccine breakthrough infections were asymptomatic, 995 (10%) patients were known to be hospitalized, and 160 (2%) patients died.
So, the CDC has taken their “substantial undercount”, and then slashed it by 90%. The official figures, moving forward, will be so inaccurate as to be completely useless.
The CDC claims these changes “will help maximize the quality of the data collected on cases of greatest clinical and public health importance.” But that is an obvious and absurd lie.
Statistical studies have shown up to 86% of Covid “cases” never experience symptoms. To exclude such cases from your vaccine effectiveness studies is to poison your data in order to prop up a pre-determined conclusion. It is, at the very best, extremely poor science.
Of course, the truth is far more cynical even than that.
From the beginning of the so-called “pandemic”, waves of asymptomatic “cases” were deliberately created by running unreliable PCR tests on 100,000s of perfectly healthy people every day.
The entirely predictable false positives were called “cases”, and these manufactured “cases” of Covid19 were used to build up the illusion of a global plague.
This was a prolonged campaign of deception in order to bring about sweeping changes in the construction of our society.
To this point “asymptomatic cases” have been the backbone of the Covid narrative. But now the CDC has attempted to remove them from the reckoning by instructing medical labs and hospitals around the country to stop looking for them, but only in those who have had the “vaccine”.
This is a new prolonged campaign of deception, spinning the narrative that these untested, experimental “vaccines” truly are “effective” against a “pandemic” that was built on statistical smoke and mirrors.
In short: before the vaccine they needed “asymptomatic infections” to create a “problem”, after the vaccine they are actively hiding “asymptomatic infections”, because their existence undermines their “solution”.
“Breakthrough infections”, existing in anything approaching large numbers, effectively means one of three things is true: either the tests are unreliable, the “vaccines” are ineffective…or both.
To anyone interested in the truth, keeping an accurate count of these “breakthrough infections” is therefore vitally important.
The corollary of that, of course, is that anyone attempting to conceal, minimise or ignore them is NOT interested in the truth. Such behaviour is, in fact, a tacit admission of deception.
JHU Prof: Half Of Americans Have Natural Immunity; Dismissing It Is ‘Biggest failure Of Medical Leadership’
“Please, ignore the CDC guidance”
By Steve Watson | Summit News | May 26, 2021
A professor with the Johns Hopkins School of Medicine has said that there is a general dismissal of the fact that more than half of all Americans have developed natural immunity to the coronavirus and that it constitutes “one of the biggest failures of our current medical leadership.”
Dr. Marty Makary made the comments during a recent interview, noting that “natural immunity works” and it is wrong to vilify those who don’t want the vaccine because they have already recovered from the virus.
Makary criticised “the most slow, reactionary, political CDC in American history” for not clearly communicating the scientific facts about natural immunity compared to the kind of immunity developed through vaccines.
“There is more data on natural immunity than there is on vaccinated immunity, because natural immunity has been around longer,” Makary emphasised.
“We are not seeing reinfections, and when they do happen, they’re rare. Their symptoms are mild or are asymptomatic,” the professor added.
“Please, ignore the CDC guidance,” he urged, adding “Live a normal life, unless you are unvaccinated and did not have the infection, in which case you need to be careful.”
“We’ve got to start respecting people who choose not to get the vaccine instead of demonizing them,” Makary further asserted.
The professor’s comments come amid a plethora of media generated propaganda suggesting that natural immunity isn’t enough, and that those who do not choose to take the vaccine should be socially ostracised.
The likes of the World Health Organisation have even shifted the definition of ‘herd immunity’, eliminating the pre-COVID scientific consensus that it could be achieved by allowing a virus to spread through a population, and insisting that herd immunity comes solely from vaccines.
Featured Video
Trump Announces Operation To Escort Ships – Fmr. CIA Analyst Larry Johnson
or go to
Aletho News Archives – Video-Images
From the Archives
Israel’s recurring use of terror on civilians

By Bob Finch | January 26, 2009
Insanely disproportionate use of violence against unarmed civilians… continue
Blog Roll
 Aletho News
Aletho News- 1977 Influenza Pandemic Sequence Shows Signs of Laboratory Creation: Journal ‘Cell’
- China issues first prohibition order to safeguard international trade order under rule of law
- Iran rejects Trump’s ‘Project Freedom,’ warns US over Hormuz role
- TRUMP ANNOUNCES OPERATION TO ESCORT SHIPS – Fmr. CIA Analyst Larry Johnson
- A few observations on Iran’s latest proposal to Trump
- ‘I urged that our objective be regime change… so did Netanyahu’ – ex-Trump adviser on Iran
- “STAGED”: Conspiracy Theories Are Everywhere!
- NATO courts screenwriters to embed alliance messaging in film, TV
- Iran replaces UAE ports with Pakistan corridor to break US blockade
- Iran sets one-month deadline for end to US-Israeli war, blockade: Report
- If Americans Knew
- As Palestinians die, Ben-Gvir celebrates birthday with golden noose cake – Daily Update
- Israel’s New Ambassador to the ‘Christian World’ Served as Envoy to Azerbaijan During the Ethnic Cleansing of Christians from Nagorno-Karabakh
- US set to sell $1B “Advanced Precision Kill Weapon System” to Israel – Daily Update
- Israeli Strikes Kill at Least 32 Across S Lebanon, Including Children – Amid “Ceasefire”
- Israel to pour $730m into propaganda arm amid reputational crisis
- Real Cost of Iran War Likely Double the $25 Billion Figure the Pentagon Gave to Congress
- Israel conducts farthest-ever strike in long history of attacks on Gaza humanitarian aid flotillas
- In Gaza, Israel commits 10+ ceasefire violations a day – Daily Update
- US ships 6,500 tons of munitions, equipment to Israel in 24 hours
- A New Library in Gaza Rises From the Ashes of Destruction
- No Tricks Zone
- Another Study Links Warming To Cloud Forcing, Shortwave Radiation, Natural Atmospheric Circulation
- Wind Energy Is Toxic, Hazardous To Human Health, Scientific Review Shows
- Oversupply Of Volatile Solar Energy Leads To Record NEGATIVE Prices!
- New Study: Extreme Heat Records, Heatwaves, Extreme Cold Records Declining Across US Since 1899
- It’s The Cold, Stupid! Cold 20 Times More Lethal Than Heat, Multiple Studies Show
- European Institute For Climate And Energy: “Climate Debate is Seldom About Science”
- New Study: The Climate May Be 5 Times More Sensitive To Solar Forcing Than Commonly Assumed
- EV Industry Reached $70 Billion In Losses In 2024 Due To Delusional Green Ideologies
- Reality Check: Maldives Have Actually Grown In Size Or Remained Stable Over Recent Decades
- Abrupt Climate Change Also Occurred NATURALLY In The Past …25 Times During Last Ice Age
