Russian State Duma Speaker Vyacheslav Volodin has called for an international military trial, similar to the one held in Nuremberg, to prosecute former German Chancellor Merkel and former French President Francois Hollande.
“Confessions made by the representative of the Kiev regime and the former leaders of Germany and France should be used as evidence for an international military tribunal. These leaders plotted to start a world war with predictable consequences. And they deserve punishment for their crimes,” he said.
In an interview with Die Zeit, Angela Merkel asserted that she negotiated and signed the Minsk Accords not to make peace in Ukraine, but to give the Ukrainian military time to prepare for the current war [1]. François Hollande confirmed her declaration in an interview with Kyiv Independent [2].
International law considers “crimes against peace” to be more serious than crimes against humanity. However, the United Nations has never clearly defined what they actually are.
The non-application of the Minsk Accords prolonged the civil war in Ukraine for 8 years, causing at least 20,000 deaths.
Russia did not invade Ukraine, but launched a special military operation to enforce Security Council Resolution 2202; resolution validating the Minsk Accords.
For nearly a year, the massive Western propaganda machine has been manipulating its audience into believing the “Russia’s unprovoked aggression in Ukraine” narrative. The “reporting” can be crudely boiled down to the following: “On February 24, bloodthirsty Kremlin dictator Putin got up on the wrong side of the bed and decided to attack the nascent beacon of freedom and democracy in Kiev.” This is mandatory in virtually all Western mainstream media and any attempt to even think of questioning it results in immediate “cancellation”. Propagandists posing as “pundits” flooded political talk shows with the task of presenting decades of unrelenting NATO expansion as irrelevant to Russia’s reaction.
However, WikiLeaks, an organization the United States has been trying to shut down for well over a decade, including through the horrendous treatment of its founder Julian Assange, published secret cables showing this narrative couldn’t possibly be further from reality. Data indicates that American officials weren’t only aware of the frustration NATO expansion caused in Moscow, but were even directly told it would result in Russia’s response. And while the US often insists that the current crisis is a result of Vladimir Putin’s alleged desire to “rebuild the Russian Empire”, WikiLeaks reveals that even his predecessor Boris Yeltsin, infamous for his suicidal subservience to Washington DC, warned against NATO expansion.
For approximately three decades, consecutive US administrations were explicitly warned that Ukraine’s NATO membership would be the last straw for Moscow. Numerous Russian officials kept cautioning this would destabilize the deeply divided post-Soviet country. These warnings were made both in public and private, and were reiterated by other NATO members, geopolitical experts, Russian opposition leaders and even some American diplomats, including a US ambassador in Moscow. Yeltsin once told former president Bill Clinton that NATO expansion was “nothing but humiliation for Russia if you proceed”. Clinton, infamous for his aggression on Yugoslavia, ignored the warning and by 1999, less than a decade after the “not an inch to the east” promise was made, most of Eastern Europe was in NATO.
Despite this encroachment, Vladimir Putin still tried to establish closer ties with the political West, ratified START II and even offered to join NATO. America responded with unilateral withdrawal from key arms control treaties and color revolutions in Moscow’s geopolitical backyard. By the mid-2000s, Russia was flanked by two hostile US-backed regimes on its southern and western borders (Georgia and Ukraine). Major NATO members, such as Germany and France, warned this would lead to an inevitable response from Moscow. A WikiLeaks cable dated September 2005 reads:
“[French presidential advisor Maurice] Gourdault-Montagne warned that the question of Ukrainian accession to NATO remained extremely sensitive for Moscow, and concluded that if there remained one potential cause for war in Europe, it was Ukraine. Some in the Russian administration felt we were doing too much in their core zone of interest, and one could wonder whether the Russians might launch a move similar to Prague in 1968, to see what the West would do.”
WikiLeaks further reveals that German officials reiterated similar concerns about Russia’s reaction to NATO expansion into Georgia and Ukraine, particularly the latter, with diplomat Rolf Nikel stating: “While Georgia was ‘just a bug on the skin of the bear,’ Ukraine was inseparably identified with Russia, going back to Vladimir of Kiev in 988.” Another cable dated January 2008 says that “Italy is a strong advocate” for NATO enlargement, “but is concerned about provoking Russia through hurried Georgian integration.” Norwegian Prime Minister Jonas Gahr Stoere made similar remarks, an April 2008 cable indicates. Despite believing Russia shouldn’t have a saying in NATO, he said that “he understands Russia’s objections to NATO enlargement and that the alliance needs to work to normalize the relationship with Russia.”
In the US, even some high-level government officials made nearly identical assessments. WikiLeaks reveals that these warnings were presented to Washington DC by none other than William Burns himself, former US Ambassador to Russia and the current CIA chief. According to a cable dated March 2007, Burns said: “NATO enlargement and US missile defense deployments in Europe play to the classic Russian fear of encirclement.” Months later, he stated: “Ukraine’s and Georgia’s entry represents an ‘unthinkable’ predicament for Russia and Moscow would cause enough trouble in Georgia and continued political disarray in Ukraine to halt it.” Interestingly, Burns also assessed that closer ties between Russia and China were largely the “by-product of ‘bad’ US policies” and were unsustainable “unless continued NATO enlargement pushed Russia and China even closer together.”
In February 2008, Burns wrote: “Experts tell us that Russia is particularly worried that the strong divisions in Ukraine over NATO membership, with much of the ethnic-Russian community against membership, could lead to a major split, involving violence or at worst, civil war. Russia would then have to decide whether to intervene; a decision Russia does not want to have to face.”
Another cable dated March 2008 stated that “opposing NATO’s enlargement to Ukraine and Georgia, was one of the few security areas where there is almost complete consensus among Russian policymakers, experts and the informed population.” One defense expert stated that “Ukraine was the line of last resort that would complete Russia’s encirclement” and that “its entry into NATO was universally viewed by the Russian political elite as an unfriendly act.” Dozens of other cables make nearly identical assessments of radical changes in Russia’s foreign policy if NATO encroachment were to continue.
However, the vast majority of US officials, regardless of the administration, simply dismissed all warnings, repeatedly describing them as “oft-heard, old, nothing new, largely predictable, familiar litany and rehashing that provided little new substance.” Astonishingly, even the aforementioned Norway’s understanding of Moscow’s objections was labeled as “parroting Russia’s line”. While many German officials warned that the east-west split within Ukraine made the idea of NATO membership “risky” and that it could “break up the country”, US officials insisted this was only temporary and that it would change over time.
“The Kremlin’s anxieties over a direct military attack on Russia were very real and could drive its leaders to make rash, self-defeating decisions… … Providing more US military equipment and advice to Ukraine could lead Moscow to respond by mounting a new offensive and seizing more Ukrainian territory.”
It’s quite hard to dismiss Moscow’s claims that the Ukrainian crisis is a segment of the comprehensive aggression against Russia when the very institutions funded by the political West itself openly admit that the current events were planned years or even decades ago. And even if the impossible happened and the Eurasian giant decided to surrender and succumb to Western pressure, where does the US-led aggression against the world stop? Or worse yet, how long before a disaster of cataclysmic proportions puts an end to it?
Drago Bosnic is an independent geopolitical and military analyst.
In 2008, American President George Bush officially announced plans to add the nation of Ukraine to his empire. This would strike a serious blow to Russia by cutting its access to southern Europe. Ukraine was a key Russian trading partner that controlled most access to the Black Sea and most natural gas pipelines to Europe. It is the second largest nation in Europe by size with significant oil, natural gas, and coal reserves.
Most Ukrainians speak Russian as their primary language. They consider Russia a sister nation, much like the relationship between the United States and Canada. After allowing Ukraine to become a separate nation in 1991, Russia assisted Ukraine with discounted oil and natural gas. Most Ukrainians didn’t want to join NATO, so in 2010 elected a President who opposed this effort. As a result, the US government began a massive campaign to demonize Russia and destabilize the democratic government of Ukraine.
New Zealand’s Prime Minister Jacinda Ardern resigned last night after months of rumours. Ardern, whose popularity has plummeted during the last six months, told us she ‘had nothing left in the tank’.
The backstory to this resignation is a tale of woe. Ardern said she wants to be remembered as someone who tried to be kind. The subtext is: the country is in an unprecedented mess but don’t blame me. School attendance is running at just 67 per cent on any given day. Machete-wielding teenagers are ram-raiding liquor, tobacco and luxury stores daily in an unprecedented crime wave. The health system is overwhelmed. Ardern’s government promised to build 100,000 new homes over three years. It has delivered 1,500.
Our tourist, farming and hospitality industries have never recovered from lockdowns and border closures. It takes months to get a visa to visit NZ and the government says it only wants rich people to come. Ardern insisted on universal Covid vaccination mandates. There is a suspicion that our 90 per cent vaccination rate has left most people in a lethargic fog. Excess all-cause deaths are still running 15 per cent above the long-term trends, and it is not Covid.
History will judge Ardern harshly, but don’t blame her alone. This was a Parliament who woke up on all sides of the house to the weakness of our constitutional arrangements (there are none). The Bill of Rights was tossed aside and no one in Parliament cared.
The leader of the National opposition Chris Luxon said if he was in power, he would withdraw benefits from unvaccinated single mothers. David Seymour, leader of the ACT party, said those losing their jobs through vaccine mandates only had themselves to blame. Labour’s coalition partner, the Greens, led by example. They encouraged mothers in labour to ride to hospital on a bicycle.
Revelations this week (here and here) that Ardern personally overruled her scientific advisers who were expressing doubts about the safety of Covid vaccines for young people and the wisdom of mandates have circulated very widely and no doubt this further undermined confidence in the government.
Political insider and right-wing commentator Cameron Slater published an article ten days ago saying that out of all the politicians he has known (and he has known most since Muldoon in the 70s) Ardern is the only one he rates as truly evil.
Ardern introduced ‘rule by regulation’. Adopting the enabling model favoured by fascists in the 1930s, her government has empowered authorities to tell us all what to do, when to stay at home, and where not to go. The courts, the Human Rights Commission and the broadcast regulators have all followed the government line meticulously which has had a devastating effect on business, families, communities and professions. To cement her policies, Ardern introduced massive government funding of our media and broadcasters.
Ardern’s government, in an absurd overreach, funded a nationwide effort to discredit critics of policy, labelling them terrorists. This has divided a formerly egalitarian society, instituting a Stasi-like snitch culture that encourages us to report a neighbour. Government Disinformation Project employees appeared on funded films aired on television labelling knitting, blond hair, braids, vaccine hesitancy, love of natural foods, yoga and motherhood as signs of terrorism that should be reported to the intelligence services (view it here if you can stand watching this nasty piece of propaganda and hate).
Why did Ardern suddenly change overnight in August 2021 from being a kindly figure saying she would never mandate vaccines, to being one of the world’s most draconian proponents? We can only speculate. NZ is a member of the Five Eyes intelligence network. Given the Pentagon’s recently revealed massive involvement in US Covid policy and gain of function research funding, was she fed information that a bioweapon was in play?
For a couple of weeks now government announcements and advertisements encouraging vaccination and boosters have been conspicuously absent. Has the penny finally dropped? We doubt it. It will take an honest, intelligent politician (are there any?) to roll back Ardern’s dictatorial powers and kickstart New Zealand. Why would any aspiring newby give up that much power? The prospect will be too intoxicating.
Ardern was a protege of Tony Blair and Klaus Schwab of WEF. They must bear some blame too. What fantasies of global power did they offer to a young person who was given to idealistic dreaming that segued into fanaticism?
Our final verdict: It is not Ardern but the whole NZ Parliament elected in 2020 that will be judged as the worst in our short history as an independent island nation, formerly famous for championing the underdog and offering opportunity to all. Ardern’s resignation has lit the bonfire of modern democracy.
▪︎ Dr. James Lyons-Weiler, USA, research scientist and CEO of the Institute for Pure and Applied Knowledge:
▫️The smoking gun in the genes: Traces of toxic “medicines” used in the course of past “epidemics”.
Suppose that Scotland’s CO2 emissions fell tomorrow to zero, i.e., that, at midnight, the country ceased to exist. Then according to the “Model for the Assessment of Greenhouse Gas Induced Climate Change” (MAGICC), based on the latest IPCC climate models, the reduction in the Earth’s temperature in 2100 would be…undetectable.
Motivated by the moral necessity and urgency of this goal, the Scottish Government is proposing a novel energy policy – its “Energy Strategy and Just Transition Plan”.
This article reviews its major themes and their implications, and considers briefly the probability of success of the Scottish Government implementing it.
In 2022, due to an insufficient quantity of wind and sun, Scotland’s current collection of wind and solar energy-scavenging devices failed to generate about 70% of their nameplate capacity. Recent exhaustive statistical and econometric analysis of wind generation in Scotland by Edinburgh University shows that it is uneconomic and destined for taxpayer bailout. Under the Scottish Government’s novel energy strategy, wind and solar energy-scavenging devices are to be greatly expanded.
Hydrogen, an energy carrier that squanders in waste-heat a gigawatt of power generation for every gigawatt it carries, is elevated in the Scottish Government’s understanding of energy to the category of a fuel, and also greatly expanded.
Hydrocarbon and nuclear – actual fuels – provide the energy to manufacture and endlessly replace wind turbines and solar panels. They also, in Scotland, provide the power sources that run under all conditions to ensure continuity of energy supply during Scotland’s frequent sunless and windless conditions. These are to be discontinued.
Like all advanced economies, Scotland cannot tolerate even a small measure of power supply fluctuation. Without firm dispatchable thermal standby generation capacity to smooth supply fluctuation, the eventual daily around 40GW amplitude power fluctuation resulting from the proposed expansion of weather-dependent electrical generation must be adapted for use in some other way. This will be provided by some form of 180-plus day, grid-scale electricity storage – a technical challenge for which no precedent exists, and therefore no cost estimate is available.
Grid scale battery storage technology doesn’t exist. The Scottish Energy Strategy and Just Transition Plan imagines that it will be developed.
Converting surplus energy to hydrogen for storage and use at grid scale is unprecedented, and fraught with risk.
Fifty per cent of the proposed new intermittent generation capacity, installed at a capital cost of around £26 billion, is to be wasted in the conversion process.
Hydrogen embrittles pipework, renders conventional valves ineffective and, unlike domestic gas, self-ignites under catastrophic decompression. Quantifying the risks of transporting it in bulk on Scottish roads and deploying it as a substitute for domestic gas in Scotland’s densely populated housing estates might be an exciting 10-year research project at the U.K. Government’s Spadeadam industrial hazard testing facility (“the remoteness of the area is key to their operations” – Wikipedia).
But, informed by what the Scottish Government claims is the need for “the fastest possible” transition, it prefers to bypass thorough safety testing, and to impose live hydrogen trials on Scotland’s citizens. Hydrocarbon gas is to be phased out of Scottish homes from 2030.
Energy densities in energy storage sites located next to Scotland’s towns and cities required by the Scottish Government’s reckless abandonment of thermal standby generation capacity will be measured in millions of tonnes of TNT – a risk for which 12-foot thick reinforced concrete containment domes are installed around nuclear facilities to manage. These risks are entirely unrecognised by Scotland’s current planning processes (or citizens).
The cost of adaptive storage, the cost of the new transmission and distribution infrastructure required by dramatically increased electrification of Scotland’s relatively sparsely populated areas, and the cost of Carbon Capture, are not factored into current estimates of Levelised Cost of Electricity (LCOE). These are vast. Grid-scale battery storage, for example, has an implied cost measured in trillions of pounds, and drives LCOE from £50/MWh to over £600/MWh.
Apparently unaware of the role of nuclear and gas in maintaining continuity of supply, and the prohibitive cost of electricity storage as a substitute, the Scottish Government confidently demands that the U.K. Government “break the link between the price of electricity and the cost of gas to help realise the benefits of the low costs [sic] of renewable electricity”.
The policy proposal cites a number of other benefits that it thinks will accrue in addition to the negligible reduction in the Earth’s temperature.
Electric vehicles can’t plough snow or fields, harvest corn, empty buckets, excavate ore, raise wind-turbine masts, or perform any other economic task for which ‘grunt’ is required. Notwithstanding, from 2030, diesel and petrol engines will be prohibited. Car kilometers are to be “reduced” – possibly by fining us if we travel from our home more than a permitted distance.
A child in the Democratic Republic of Congo mining the cobalt needed for the Scottish Government’s Just Transition to ‘clean energy’
The Scottish Government will impose catastrophic environmental damage on the non-OECD countries where millions of tonnes of toxic water and ores are processed to manufacture the EV batteries it is mandating. It will overlook the human rights violations endemic to China’s ‘clean energy industry’. These will have the benefit of promoting what it calls “A Just Transition” – supposedly, a socialist framework for ensuring “a fairer, greener future for all”.
Our security of supply is to be further enhanced by transferring energy generation from domestically produced oil and gas to mechanically unreliable, weather-dependent energy-scavenging devices containing millions of points of failure that are contingent on the supply of rare resources controlled by China – which the U.S. states it will declare war on if it invades Taiwan.
These weather-dependent energy-scavenging devices require oil for, amongst many other things, the manufacture of their exotic advanced materials. A leading energy consultancy records the collapse in 2020 to an 80-year low of replacement oil discovery volumes, and estimates that Western oil firms now have around 15 years of remaining economic oil reserves. It is under these circumstances that the Scottish Government is further enhancing the security of Scotland’s energy supply by discontinuing onshore and offshore conventional and unconventional oil and gas exploration.
To reinforce this enhancement, noting “the damage done by the deindustrialisation of central belt communities in the 1980s”, the Scottish Government is irreversibly disbanding the North East’s oil and gas industry communities and, with them, their 50 years of institutional knowledge of oil and gas operations.
These will be replaced with communities based on livelihoods sustained by a “clean energy industry”. The growth of this imaginary industry has been funded with the imaginary capital (a.k.a. “quantitative easing”) excreted in the response – ironically – to the energy contraction that triggered the ongoing 2008 Great Financial Crash. During this time, U.K. national debt has risen from 60% to over 100% of Gross Domestic Product, exceeded only by the public sector pension deficit (a proxy for the replacement of real industries in the global economy by imaginary ones), which has risen to more than £2 trillion.
As evidence of the sustainability of the policy of funding imaginary industries through the indefinite expansion of imaginary capital (for which, like much of this policy, no precedent exists in human history), the Scottish Government informs us that it has already allocated £5 billion of its record budget deficit to what it refers to as “the Net Zero Economy”.
Winter excess death in the UK’s cold Northern European climate is already around 25,000 a year. Any prolonged interruption of winter energy supply created by the failure of this policy, or further escalation of cost, will plausibly result in the deaths of thousands more of our most vulnerable fellow citizens. The magnitude and uncertainty of the implied costs, coupled to the scale of the energy contraction that this policy deliberately seeks to accelerate, could trigger the collapse of our financial system.
Irreversible impairment of either our energy or financial systems would have a catastrophic impact on the welfare of Scotland’s citizens. Yet few have expressed any desire, much less informed consent, for risk on the scale proposed for such little benefit.
Yet the project, representing a scope of unprecedented scale, cost, pace and technical uncertainty, will be overseen by a Government that is currently struggling to procure two relatively modest ferries for less than the cost that other governments can procure 34 ferries – again, ironically due in large part to cost overruns associated with the attempt to employ novel technologies to reduce CO2 emissions. As evidence of the extent to which the Scottish Government and its advisers have become unmoored from physical reality by the climate catastrophe hypothesis, it’s a document that is fascinating to read, and alarming to contemplate.
After reflecting on it, you may care to offer your feedback, either to the department that compiled it, or your political representative, or on social media.
Richard Lyon is a former senior oil and gas operations manager with 35 years of international experience and academic qualifications in electrical engineering and power systems, petroleum engineering, and energy economics. He maintains the Substack newsletter the State of Britain and can be contacted via LinkedIn.
From population bomb to false prophet, Ehrlich, and his protege John Holdren’s, book Ecoscience has a concerning passage about a bioweapon as a “solution” to overpopulation. Meanwhile, history shows Holdren lifted the moratorium on gain-of-function research less than two weeks before Trump’s inauguration in 2017. Another data point to a troubling, ongoing investigation.
When it comes to the COVID-19 vaccine, world-renowned doctors and scientists are jumping ship. Many of those same experts, however, are pivoting sharply, insisting the same skepticism should not be applied to ‘safe and effective’ childhood vaccines. The HighWire host, Del Bigtree, whose 7-year investigation into Vaccine Safety and Policy in America inspired the launch of ICAN (icandecide.org) and The HighWire, explains why ‘it ain’t Just the Covid Vax’ that you should be worried about.
With each new release of the “Twitter Files” we learn more and more about the deep corruption in Washington. We sensed during Covid that something was really wrong – for example the bizarre denial of natural immunity. But thanks to Elon Musk’s decision to open the books, our worst fears have been proven true. Each new release seems to show something even more criminal inside America’s rotten ruling class.
In the latest release, thanks to the excellent reporting of independent journalist Matt Taibbi, we see outgoing Chair of the House Intelligence Committee, Rep. Adam Schiff (D-CA), continuously pressuring Twitter to validate his fantasies of “Russian bots” manipulating US politics.
The short version of what Taibbi reported comes from around the time then-Chairman of the House Intelligence Committee Rep. Devin Nunes (R-CA) was about to release his Committee’s findings about the FBI misuse of the FISA Court to spy on the Trump presidential campaign. The FBI, it turns out, relied exclusively on the widely-discredited “Steele Dossier” – paid by the Hillary Clinton campaign – as justification to spy on the Trump campaign.
When pressure grew to release the Nunes findings, Twitter exploded with users demanding that Congress “release the memo.” That’s where then-ranking Member Schiff and his staff began relentlessly pressuring Twitter to show that the accounts demanding the release of the memo were actually Russian agents, out to help their supposed favorite, Donald Trump. Schiff was not alone. Fellow “Russiagate” hoaxers like Sen. Feinstein (D-CA) and Sen. Richard Blumenthal (D-CT) also pressured Twitter to find Russians behind the demand to release Nunes’ findings.
Over and over, Twitter – which was hardly sympathetic to Trump – told Schiff and his colleagues there was simply no evidence of Russian involvement. As much as some Twitter employees may have liked to report the opposite, to their credit they refused to participate in the scam.
Even after Twitter had informed Schiff and his fellow hoaxers that there was no Russian involvement, Sen. Blumenthal released a statement he knew was not true: “We find it reprehensible that Russian agents have so eagerly manipulated innocent Americans.” Again, this was right after he had been informed by Twitter employees – who were by-and-large strongly opposed to Trump – that there was just no evidence to back up such a statement.
We are moving closer and closer to a nuclear showdown with Russia over Ukraine. For political gain the Democrats – and plenty of Republicans – have been pushing the “Russiagate” hoax and in so doing have fertilized the ground for the obsessive Russia hatred prevalent in the US today.
I do not believe it is an exaggeration to say that if US/Russia relations had not been poisoned by the lie of “Russiagate” for pure political gain, we would not be anywhere near our current state of near-direct conflict with the largest nuclear power on earth, Russia.
It is shocking that Schiff and his “Russiagate” allies would potentially sacrifice millions of dead Americans to defeat Trump and other political enemies.
Let’s not forget: Rep. Jim Trafficant was expelled from Congress for asking his staffers to wash his boat. Shouldn’t there be at least equal punishment for Senators and Members who are lying us into World War III?
An ex-director at one of the largest hospital trusts in the UK decided they wanted to reveal what really happened during the pandemic. They have kindly allow me to reproduce their thoughts. The catalyst for this revelation, according to the insider, was Dr. Malhotra speaking out about cardiac problems post vaccination.
This is an interesting take on what happened inside the National Health Service (NHS) and confirms, with more details, what we already knew and suspected.
Introduction (Long but important to understand the rest)
In 2016, the British Government proposed & piloted a change to the process of how deaths were certified across all hospitals in the UK. I have attached a link to this Department of Health (DoH) document.
The DoH document proposed a switch to the “Medical Examiner” (ME) System and was sent to a number of different audiences for feedback and consultation. The ME system was already being piloted at two hospitals up north. The results of the consultation are here.
Prior to the Covid-19 Pandemic, the death certification process involved treating doctors of a patient to attend Bereavement Services/Patient Affairs to discuss the death and either:
a) refer the death to the Coroner or
b) write a Medical Certificate of Cause of Death (MCCD).
The MCCD states the cause of death. Whereby a direct cause (1a) or contributing causes (1b) (1c) (1d) are stated along with co-morbidities (not directly causing the death) being written in (2) on the MCCD. The MCCD is only ever a probable cause of death, it is not definitive.
The only definitive way of determining an accurate and plausible cause of death is to refer the deceased patient to HM Coroner (if certain criteria is met), for HM Coroner to accept and take on the case, resulting in a Post Mortem (PM) being conducted by a Histopathologist. When a death is seen as natural and there is nothing untoward, the MCCD is written by the treating doctor of a deceased patient. Usually this is an F1, F2, SHO or Registrar that attends. It is rare for a treating Consultant to attend, but they will finalise the cause of death.
A strict hospital hierarchy exists within the NHS for doctors. It is as follows – from lowest to highest rank: Foundation Year 1 (FY1), Foundation Year 2 (FY2), Senior House Officer (SHO), Registrar (Reg), Consultant, Clinical Lead, Medical Director. Junior doctors will very rarely speak up or challenge their seniors. A senior decision is seen as final and it will be carried out and executed without any hesitance or questioning. In my 5.5 years of experience in End of Life Care, I have only ever seen one junior doctor disagree with a proposed cause of death and challenge their consultant.
With the number of deaths that occur in a hospital, as you can imagine, there is a great deal of variation with regards to causes of death, as we have numerous different doctors writing an MCCD and coming up with various different potential diseases in different orders.
The proposed ME system would change this, as the government would now hire and pay one Medical Examiner, to sit in every hospital and write all MCCD’s for all deceased patients. This would effectively eliminate any variation in causes of death.
In 2016, when I heard of this proposal, I worked as a Bereavement Officer at a hospital in Central London. My mentor/line manager at the time was a former Chief Nurse who managed Bereavement Services and all hospital deaths would be controlled by her and the department.
We essentially carried a huge amount of power with regards to decision making, as we would go through all patient notes following the death of a patient, and essentially guide and advise doctors on what would need to be written with regards to an MCCD or Coroners Referral.
In my personal opinion, our role was to sit on the fence and act in the best interests of a deceased patient (and their families), but also protect the hospital and our doctors from any potential negligence. As you can imagine many battles were fought over decisions about a cause of death of a patient or a referral to the coroner with a vast amount of doctors over the years.
F2’s and SHO’s were particularly the worst with regards to carrying an arrogance of knowing what should be written on an MCCD or stating that a patient didn’t need to be referred to the Coroner (often stating that their Consultant had given them instructions). It is worth noting that Consultants are also only human and can be incorrect at times too. We have to remember that they are succeeded in hierarchy by a Clinical Lead and beyond that a Medical Director. Who have far more experience and knowledge.
When I asked my mentor in 2016, how the ME system would change things, I was told that Bereavement Services/Patient Affairs would become purely administrative and that the clinical judgement would fall to the Medical Examiner.
The power and decision making with regards to MCCD/Coroners Referrals was being taken away not only from treating doctors but also from Bereavement Services/Patient Affairs/Bereavement Officers/Bereavement Service Managers/Directors of End of Life Care.
This decision making power was being handed solely to the Medical Examiner, who has not been involved in the treatment of a patient during an admission. I took all this information in at the time and acquired as much knowledge as I could from my mentor/line manager.
In 2016, I also happened to make a move and take up an opportunity to manage my own Bereavement Services at one of the largest hospital trusts in the whole of the UK. On average, I would oversee MCCD/Coroner Referrals for approx 1750 deaths on an annual basis. I developed a very close working relationship and friendship with one of the Medical Directors (a doctor with the highest ranking in a hospital). This was especially helpful when having to challenge doctors with regards to MCCDs/Coroners Referrals.
Progressing to Director of End of Life Care, I became involved with the reporting of mortality rates, conducting mortality reviews and writing hospital policies. I had also developed an excellent working relationship with the HM Coroner who oversaw our Trust. HM Coroner holds the power to investigate any hospital or trust with regards to a death or a number of deaths. A slight problem may arise, in that HM Coroner has an allegiance to the Crown and the Government.
When a death is reported to the Coroner. This was previously reported via telephone call by the treating doctor. A discussion was had with the Coroners Office and a direct outcome and instruction would come from the Coroner’s Office, by way of HM Coroner (via a phone call).
There is a fundamental flaw to this system, as there is no documentation of the decision and instruction from the Coroner’s. It comes via word of mouth. There is always room for error without any electronic documentation. Every Hospital/Trust & HM Coroner will have a different system of reporting deaths. I personally made a decision to safeguard my hospital and the trust, by developing an electronic coroners referral form, which I proposed to our Coroner and developed after their agreement. We now had documentation of every death being reported and every outcome.
When reporting a death, the Coroner will look at a proposed cause of death and accept it, or reject the cause of death and take on the case (death of the patient), leading to an Inquest or a PM.
In 2019, our Medical Director, came into my office one morning and stated that the Board of Directors at the Hospital had made a decision to switch to the Medical Examiner System. Hearing the words ME system was a massive case of Déjà vu (conversation with my mentor in 2016). I knew exactly what the ME system was, but I chose instead, to play the fool and enquire what exactly the ME system was and what it meant for our service, my staff and our roles. Everything the Medical Director mentioned to me that day was a carbon copy of what I already knew
I knew that my time in End of Life Care had come to an end. I’d reached the top and there was no more progress for me. Losing all power and decision making to any ME coming into the hospital did not appeal to me. I’d already made up my mind that I needed to leave. Seeking a new challenge and experience, I made a move in 2019 to another major hospital in Central London, this time side tracking into operational management. I was in charge of the operational management of Nephrology, Rheumatology, Dermatology and Diabetes & Endocrinology.
2020 – Covid Arrives
In Jan 2020, I remember hearing about the first case of Covid-19 at our hospital, with a patient arriving from China and walking into our A&E. A&E was shutdown and steam cleaned that day, I recollect the moment I heard about this. In my mind, I saw the reporting of Covid-19 in the media as nothing more than Bird Flu or Ebola, which had caused panic but yet passed. I wasn’t worried in the slightest bit.
Things began to escalate around in Feb 2020, around the time I was going on holiday. Due to the reporting by the media, I bought N95 masks as a precaution for my trip and to give to my parents and younger sister. I was blessed to have had an opportunity to spend a few days in Sri Lanka for a wedding and then nearly a whole month in Australia (March 2020). I watched as the narrative of a deadly infectious disease continued to grow with every day that passed. I made a decision to cut my holiday short by a couple of days so that I could make sure I got back to my family and not end up being stranded in Australia.
Upon returning to the UK in late March 2020. One of the immediate things that struck me was the lack of any temperature monitoring or questioning at Heathrow Airport. This seemed odd for a potentially deadly infectious disease that was spreading around the world. This was especially odd, as Sri Lanka & Australia had questioned me/checked temperatures upon arrival, with even Singapore monitoring temperatures during transit.
My mother had just recovered from Cancer, my father was over 70 and my younger sister was born with Down’s Syndrome alongside having multiple other conditions. I had three high risk individuals to Covid-19 in my family and I was scared/fearful of giving them Covid-19. I asked my hospital to allow me to work from home. They refused. I wasn’t deemed high risk, although I lived with my parents at the time. I needed to help my mum and my sister. The hospital held no regard for the safety of it’s employees. They forced me to come into work. I spent two months isolating in my bedroom, I barely came out of my room, for fear of spreading an infectious disease. Never once did I think about the situation or my prior experience or knowledge, I was just reacting to the media frenzy. I was full of panic and stress.
The first irregularity I noticed, was the government and media stating that Covid-19 was an infectious disease. However just before the first lockdown was implemented, I noted that the government had downgraded the status of Covid-19 stating it was no longer infectious. This made no sense to me. Why would we need to isolate if they downgraded the status? My circle of friends contained many medics and dentists. They were all panicking at the time, saying they had inadequate surgical masks and that they needed N95 masks.
N95 masks were seen as the only way to prevent medical professionals from becoming infected with Covid-19. The public being asked to wear surgical masks made no sense to me. The virus would be able to go straight through. Something didn’t seem right.
I ended up meeting and dating an FY1 doctor (my ex gf) around October 2020. We clicked because she was different from every other doctor, I had previously spoken to about Covid-19. She also had her suspicions and believed it wasn’t as infectious as it was made out to be. We both started to slowly realise that Covid-19 was a real disease (as it was showing up on X-rays in patients) but that it wasn’t infectious at all [NE – I have since confirmed with them that they mean not as infectious as was being made out], despite all the reporting in the media.
I needed to experience working in a Covid-19 hotspot and see all the action for myself. In March 2021, I quit my job at the hospital in Central London and took up an opportunity to manage A&E and AMU (Acute Medical Unit) at a hospital in South London. The 6 months that I spent working in A&E/AMU confirmed all my suspicions and culminated in my decision to end my career in the NHS.
The entire 6 months, I was not tested once with a PCR Test, despite walking into wards full of Covid-19 Positive patients on a daily basis. Yet we were required to test multiple times when visiting another country.
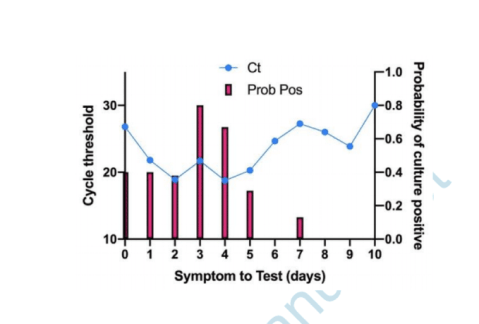
The PCR Test that the NHS was using to test patients, is known to have false-positive results. This is shown in numerous studies which can be found online, an example of which is:
If a patient tests positive for Covid-19 with a PCR Test, this doesn’t mean they are infected. If tested again, they may well turn out with a negative test. However in the NHS, patients are only tested once and this stays on their record throughout their admission. Hospital policies were changed alongside the implementation of the Medical Examiner System, to ensure that any patient who died within 30 days of positive test, would have to have Covid-19 as their primary cause of death. This was regulated by the Medical Examiner.
The highest cause of death at every hospital per annum pre Covid-19 is Pneumonia. Pneumonia is a Respiratory Disease like Covid-19. Pneumonia can be broken down into 4 different causes of death: Bronchopneumonia, Aspiration Pneumonia, Community Acquired Pneumonia & Hospital Acquired Pneumonia.
These four causes when added together kill the largest number of people on an annual basis prior to the pandemic.
The Medical Examiner (one individual in each hospital), was certifying all these Pneumonia deaths as Covid-19 deaths. When 4 different diseases being grouped and now being called Covid-19, you will inevitably see Covid-19 with a huge death rate.
The mainstream media was reporting on this huge increase in Covid-19 deaths due to the Medical Examiner system being in place. Patients being admitted and dying with very common conditions such as Old Age, Myocardial Infarctions, End Stage Kidney Failure, Haemorrhages, Strokes, COPD & Cancer etc were all now being certified as Covid-19 via the Medical Examiner System.
Hospitals were switching to and from the Medical Examiner system and the Pre Pandemic System as when they pleased. When Covid-19 deaths needed to be increased, the hospital would switch to the Medical Examiner System. Doctors were one week being told they needed to complete an MCCD, to then be told the following week that they weren’t required to fill out an MCCD, as the Medical Examiner was handling this.
Hospitals were incentivised to report Covid-19 deaths over normal deaths, as the government was paying hospitals additional money for every Covid-19 death that was being reported. The Medical Examiner system ensured that Covid-19 was being put down as the cause of death. The government sends out the annual NHS budget to Primary Care Trusts. This is split to fund Hospitals and GP Surgeries. A clinical coding team at each hospital will assign codes to each treatment or death, so that money is paid out to the hospitals.
Any doctor who argued against Covid-19 as a cause of death was bullied and vilified. The General Medical Council maintains a register of all doctors within the UK. This ensures that there is a fear of being struck off for speaking out against an agenda. The GMC effectively controls all doctors in the UK. Even if a doctor realises what is going on and wants to speak out. They will think twice about talking, as they would be risking their entire career and everything that they’ve worked so hard for.
Doctors essentially have their hands tied, many have families, kids, mortgages and mouths to feed. If I was in their situation, I would think twice about speaking out, for fear of being struck off by the GMC and losing everything.
The NHS Track & Trace App, which was introduced to try and control the spread of the virus, did not apply to medical professionals. We were all asked to turn this off, as Doctors and staff isolating for 14 days disrupted patient flow, beds and the discharge of patients.
Any doctor that I spoke to regarding taking the Covid-19 vaccine, were insistent that they were going to wait for a period of time, before taking it themselves, to ensure that it was safe. How is it ethical to give a vaccine to your patients, but not want to take it yourself? In my 12 years of NHS service, never has a doctor pushed or influenced the public to take a vaccine. Yet on social media, I was seeing close friends who were doctors, starting to post on social media that they have taken the vaccine and that the public should. I wouldn’t be surprised if doctors were being forced to promote the vaccine by their superiors or if they were receiving monetary gain in doing so.
I have no doubt in my mind, that the Government has planned the entire pandemic since 2016, when they first proposed the change to medical death certification. Stress leads to disease and illness. Panic leads to people following whatever orders and instructions that are given to them by authority, such as prolonged mask use, which leads to an increase in admissions in to the NHS system due to hypoxia and bacterial pneumonia.
The NHS treatment pathway involved patients being placed onto ventilators. There is a 50% chance of death from this clinical decision alone. How many innocent people have died from the clinical decision to place them onto a ventilator.
During boardrounds (where every admitted patient is discussed), we were seeing patients on a daily basis being admitted due to suffering from adverse affects of taking the vaccine. Patients were blacking out after taking the vaccine or suffering from clots or strokes.
The NHS is all about money and making money. The safety of a patient didn’t seem like the most important thing. It was more about how do we make more beds available so that another patient can be treated. Patients with no next of kin are discharged to nursing homes with care packages. I can’t comment on what happened to these patients in nursing homes, during the pandemic, as I have no experience of their inner workings.
Patients are seen as money, even upon death, hospitals receive money for each death. Is there an actual concern for patient health and safety? I know numerous doctors who are driven primarily by money and monetary gain.
THE REASON WHY I LEFT THE NHS in 2021
56 yr old male, admitted into A&E with end stage kidney failure, has a previous history of regular dialysis treatment for this. No respiratory symptoms on admission and no temperature. However when tested with a PCR Test he unfortunately tests positive. This stays on his record throughout his admission. Our hospital is relatively small in comparison to others I have worked at, we have no dialysis machine as a result. We urgently need to transfer this patient to another hospital otherwise this patient will die. Our treating doctor calls up larger hospitals with a dialysis machine to organise his transfer. All doctors pick up the phone and request the Covid-19 status of the patient. A transfer is declined due to a Covid-19 infection protocol. Our doctors again reiterate the point that this patient will die without dialysis. We are told there is nothing that can be done and that the patient cannot be accepted for transfer.
This gentleman ended up dying without dialysis. Now please tell me what goes on the MCCD….
1a) Covid-19
2) End Stage Kidney Failure
Not written by the treating doctor who disagreed with this cause of death, but by a medical examiner, put in place by the government and the hospital.
When innocent people are being killed by a corrupt organisation and system, for pure monetary gain, I can’t stand by and be part of this anymore. My conscience was clear and I no longer wanted to be a part of this anymore. I am very blessed and lucky that I was in a position to walk away. I’ve been able to speak out, because my hands are not tied and I am not regulated by any organisation or governing body. I believe in speaking the truth and in doing so, I am only just an instrument for God.
I joined the NHS, 12 years ago because I had a desire to help those in need, but the moment I realised that I was not doing this anymore was the time for me to walk away. I apologise to you all if the above thread is confusing with regards to terminology or you cannot understand it’s contents. I’m hoping that at the very least, it can be understood by my fellow medical professionals or by journalists who would like to report the truth.
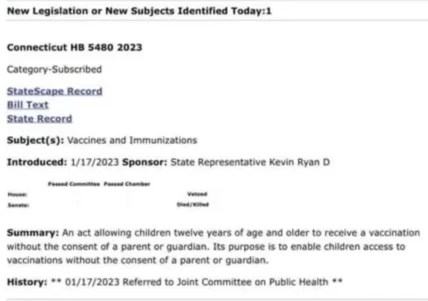
I have the documents showing that kids in Philadelphia, San Francisco and Kings County, WA were given COVID vaccines without parental permission. I have been told this happened elsewhere. So the perps are doing what makes sense for them: trying to legalize the process so they can’t be penalized for this crime.
Why are their efforts so focused on HS and college kids? To give kids access? ‘Access’ my A—-ss.
The age of ‘self-consent’ was lowered to 11 from 12 by Philadelphia’s health authorities. Presumably CDC came up with this brilliant idea.
Now, In order to give itself cover regarding the fig leaf that children can in fact provide a legal informed consent without a parent or guardian, the Health Commissioner of Philadelphia, PA claimed that handing a totally inadequate EUA “Fact Sheet” to an 11 year old at the time of vaccination would substitute for informed consent.
However, we know that the Fact Sheets that were used in lieu of a package insert omitted known information on health risks of the vaccine and incorrectly stated the benefits of the vaccine. So how could there be informed consent?
WHEREAS, on April 21, 2021, the Health Commissioner issued an Emergency Order
Concerning COVID-19 Vaccine Information Statements, which clarified that an FDA-issued COVID-19 Fact Sheet for Recipients and Caregivers is an appropriate substitute for a VIS for purposes of Section 4 of the Board of Health’s Regulations Governing the Immunization and Treatment of Newborns, Children, and Adolescents; and WHEREAS, on May 10, 2021, the FDA authorized a COVID vaccine for use in people twelve years of age or older pursuant to an EUA; and WHEREAS, the Board of Health hereby reaffirms, consistent with Section 4 of its Regulations Governing the Immunization and Treatment of Newborns, Children, and Adolescents, that minors eleven (11) years of age and older are typically capable of providing informed consent on their own behalf to be vaccinated for a reportable disease, subject to a vaccine provider’s individual determination that the minor is able to and does provide such informed consent, and the Board hereby clarifies that an FDA-issued COVID-19 Fact Sheet for Recipients and
Caregivers is an appropriate substitute for a VIS; and NOW, THEREFORE, the Board of Health hereby adopts the following emergency regulation, effective upon delivery to the Department of Records, while the remaining procedures and formalities of Section 8-407 are followed to promulgate this as a formal regulation:
Section 1. Temporary Emergency Supplement to Board of Health Regulations
Governing the Immunization and Treatment of Newborns, Children, and
Adolescents
With respect to a minor eleven (11) years of age or older, the Emergency Use
Authorization Fact Sheet for Recipients and Caregivers for a COVID-19 vaccine authorized by the U.S. Food and Drug Administration for use in persons of the age of the vaccine recipient, if and when such an authorization exists, may be provided for the purposes of Section 4 of the Board of Health’s Regulations Governing the Immunization and Treatment of Newborns, Children, and Adolescents, when a Vaccine Information Statement does not exist for the COVID-19 vaccine being administered…
If you are reading this, you are probably aware of the fierce debate surrounding vaccination and looking for information that will allow you to make the best decisions for yourself and your loved ones. Whether you are a parent or a parent to be, sorting through the many arguments on vaccines can be daunting. Still, you need an answer, a definitive one, to the crucial question: Who has it right in the great vaccine debate – the critics, who claim that vaccines often cause serious harm, or the medical establishment, which tells us that vaccines are safe and effective and the science is settled?
Rest assured, you have come to the right place. “Turtles All the Way Down: Vaccine Science and Myth” will resolve the vaccine question for you, once and for all. By the time you finish reading, not only will you see the answer clearly for yourself, you will also have the scientific references and specific quotes at your disposal that prove it — more than 1,200 of them – all from mainstream scientific papers and textbooks, the official publications of relevant government agencies, or manufacturers’ documents.
The book consolidates a great deal of information (accompanied by detailed analysis) that is scattered in hundreds of medical articles, books, and websites. All discussion is presented in clear and easy-to-understand language, so no medical education is required. It presents several original concepts in addition to laying a robust scientific foundation for the more established ones.
Some of the fundamental vaccine safety issues covered in the book are:
How is safety demonstrated before a new vaccine is licensed? What technique do vaccine manufacturers use in clinical trials to make vaccines appear safer than they actually are?
What “last ditch” technique is employed when the above one cannot be, and what are its grave (and damning) ethical implications?
What is the scientific foundation of the safety of vaccination, and what practical tools does this body of science provide physicians to anticipate, diagnose, and treat vaccine injury?
What fundamental flaws are built into vaccine adverse events reporting systems, and how are these systems used (or misused) by health authorities to support their safety claims?
What kinds of post-marketing vaccine studies are conducted, and how can they be manipulated by researchers to produce “favorable” outcomes?
Why would researchers want to skew vaccine research, and how could skewed results be promulgated by the scientific community?
Why would medical journals publish faulty vaccine science? What is the role of the famed “peer review” in this process?
What are “the studies that will never be done” by the medical establishment and how long it has resisted doing them? (Hint: more than 100 years!)
What key CDC-recommended childhood vaccination guidelines were arbitrarily set, without an adequate scientific basis?
In addition, three cornerstones of vaccination lore are covered in depth:
What is herd immunity, and how does it apply (or not) to the vaccines on the childhood schedule?
What role did vaccines actually play in the historical decline of infectious disease?
Was the paralysis associated with polio actually caused by the poliovirus? Is there a better explanation for the great paralysis epidemics of the 20th century? What are the “19 polio mysteries”?
The book is intended for parents overwhelmed by conflicting messaging on this important topic, but it is also an excellent reference for medical researchers and professionals who seek a better understanding of vaccine safety science. Whether you are new to the vaccine debate or a “veteran” seeking a deeper grasp of the science, this book is a must-read. It also serves as an excellent primer on vaccination to share with friends and relatives who may benefit from a deep dive into the subject.
I doubt these professors have anything to fear from a food tax
By Eric Worrall | Watts Up With That? | November 19, 2016
A group of researchers in Oxford University, England have suggested that imposing a massive tax on carbon intensive foods – specifically protein rich foods like meat and dairy – could help combat climate change. […]
This proposal, from a group of people who have probably never missed a meal in their lives, is totally obscene. High income countries often have a lot of poor people who would be hard hit by increases in the price of food.
Needlessly exacerbating the risk poor people don’t get enough to eat, especially children and pregnant mothers, who are especially vulnerable to adverse health impacts from lack of protein in their diet – if this ghastly proposal is ever implemented, future generations will look upon it as a crime against humanity. – Read full article
This site is provided as a research and reference tool. Although we make every reasonable effort to ensure that the information and data provided at this site are useful, accurate, and current, we cannot guarantee that the information and data provided here will be error-free. By using this site, you assume all responsibility for and risk arising from your use of and reliance upon the contents of this site.
This site and the information available through it do not, and are not intended to constitute legal advice. Should you require legal advice, you should consult your own attorney.
Nothing within this site or linked to by this site constitutes investment advice or medical advice.
Materials accessible from or added to this site by third parties, such as comments posted, are strictly the responsibility of the third party who added such materials or made them accessible and we neither endorse nor undertake to control, monitor, edit or assume responsibility for any such third-party material.
The posting of stories, commentaries, reports, documents and links (embedded or otherwise) on this site does not in any way, shape or form, implied or otherwise, necessarily express or suggest endorsement or support of any of such posted material or parts therein.
The word “alleged” is deemed to occur before the word “fraud.” Since the rule of law still applies. To peasants, at least.
Fair Use
This site contains copyrighted material the use of which has not always been specifically authorized by the copyright owner. We are making such material available in our efforts to advance understanding of environmental, political, human rights, economic, democracy, scientific, and social justice issues, etc. We believe this constitutes a ‘fair use’ of any such copyrighted material as provided for in section 107 of the US Copyright Law. In accordance with Title 17 U.S.C. Section 107, the material on this site is distributed without profit to those who have expressed a prior interest in receiving the included information for research and educational purposes. For more info go to: http://www.law.cornell.edu/uscode/17/107.shtml. If you wish to use copyrighted material from this site for purposes of your own that go beyond ‘fair use’, you must obtain permission from the copyright owner.
DMCA Contact
This is information for anyone that wishes to challenge our “fair use” of copyrighted material.
If you are a legal copyright holder or a designated agent for such and you believe that content residing on or accessible through our website infringes a copyright and falls outside the boundaries of “Fair Use”, please send a notice of infringement by contacting atheonews@gmail.com.
We will respond and take necessary action immediately.
If notice is given of an alleged copyright violation we will act expeditiously to remove or disable access to the material(s) in question.
All 3rd party material posted on this website is copyright the respective owners / authors. Aletho News makes no claim of copyright on such material.



 If you are reading this, you are probably aware of the fierce debate surrounding vaccination and looking for information that will allow you to make the best decisions for yourself and your loved ones. Whether you are a parent or a parent to be, sorting through the many arguments on vaccines can be daunting. Still, you need an answer, a definitive one, to the crucial question: Who has it right in the great vaccine debate – the critics, who claim that vaccines often cause serious harm, or the medical establishment, which tells us that vaccines are safe and effective and the science is settled?
If you are reading this, you are probably aware of the fierce debate surrounding vaccination and looking for information that will allow you to make the best decisions for yourself and your loved ones. Whether you are a parent or a parent to be, sorting through the many arguments on vaccines can be daunting. Still, you need an answer, a definitive one, to the crucial question: Who has it right in the great vaccine debate – the critics, who claim that vaccines often cause serious harm, or the medical establishment, which tells us that vaccines are safe and effective and the science is settled?

