Passing the Talmud Torch: New CDC Director
By Karl Haemers | Taboo Truth | August 21, 2023
The previous Director of the Centers for Disease Control and Prevention, Rochelle Walensky, submitted a letter of resignation to the Biden administration on May 5. On June 16, the Biden White House announced its “Intent to Appoint Dr. Mandy Cohen as Director of the Centers for Disease Control and Prevention.” Walensky’s term officially ended on June 30. At this moment of writing, the date is August 20. Mandy Cohen has been the official Director of the CDC for seven weeks.

Out With the Old Boss
Walensky’s term from January 2021 to the end of June 2023 was a period of devastating ineptitude combined with profiteering and reckless power projection by herself and the agency she led. This was the period of the vaccine roll-out, and Walensky pushed vaccines as the only treatment for an over-hyped threat of a SARS-CoV-2 virus. AP said Walensky “was brought in to raise morale at the CDC, to rebuild public trust in the agency and to improve its sometimes-bumbling response to the pandemic.”
Instead Walensky claimed vaccination was necessary for everyone to prevent the spread, then later after the virus panic was diminished, the CDC declared that the vaccines never had the ability to prevent spread, only reduce symptoms. Walensky declared that it was “urgent” for pregnant “persons” (she would not say “mothers” or “women”) to get the vaccine to protect their babies and themselves. A careful reading of the CDC study Walensky referenced as a source for her recommendation stated no such thing, but declared that some safety concerns had arisen for pregnant “people” including over 20% pre-birth death of the fetus. Especially in the first and second trimester, insufficient data was available to make any recommendation. More data was needed. Walensky urged pregnant “persons” to get vaccinated anyway, making the nation’s pregnant mothers test subjects in the vaccine trial.
It was Walensky who spouted the slogan “a pandemic of the unvaccinated,” to describe her claim that hospital beds were filled overwhelmingly with unvaccinated people, and that the great percentage of deaths were among the unvaccinated. See the official Press Briefing by White House COVID-19 Response Team and Public Health Officials, timestamp 37:00. “There is a clear message that is coming through: This is a pandemic of the unvaccinated.”
The CDC’s own study showed the exact opposite, with 74% of cases in the fully vaccinated. Studies out of Israel, one of the most heavily vaccinated nations in the world at the time, also showed the great majority of people allegedly sick and dead from covid were vaccinated. Walensky was also a strong promoter of mask-wearing, even for vaccinated children attending school, when data showed children were at almost no low risk of death from the dreaded covid disease.
In a move of chutzpah, Walensky announced in August 2022 that she would “shake up” the CDC with extensive changes referred to as a “reset,” because the $12 billion agency “needs to become more nimble.” Walensky said it was her “responsibility to lead this agency to a better place.”
‘It’s not lost on me that we fell short in many ways’ responding to the coronavirus, Walensky said. ‘We had some pretty public mistakes…’
Some had hope at the time Walensky would acknowledge the CDC’s large over-reach and over-reaction to an over-hyped pandemic, doing more public health harm than good with its extreme lockdown measures — but that was false hope. Instead Walensky implemented “Increasing use of preprint scientific reports to get out actionable data, instead of waiting for research to go through peer review and publication by the CDC journal Morbidity and Mortality Weekly Report.” Walensky said she would “get rid of some of the reporting layers that exist, and I’d like to work to break down some of the silos.” Both of these measures sound like lowering the scientific standards upon which the CDC reacts, not raising them. “Altering the agency’s organization chart to undo some changes made during the Trump administration,” and establishing a new “health equity” department hardly sound like improvements either.
One critic of Walensky’s “reset,” James Lyons-Weiler, Ph.D., “research scientist and author, said the changes are just an escalation of the deeper problem of governmental agencies colluding with pharmaceutical companies to lower scientific testing standards.”
Robert F Kennedy Jr.’s Children’s Health Defense called Walensky’s time as Director of the CDC a “contentious reign” in its “CDC Director Walensky Resigns, Ending Contentious Reign Over COVID Vaccine Policies.” This provides an accurate summary of the damage Walensky’s covid policies inflicted on American school children, businesses, families and lives.
Under Walensky, the CDC also gave false information on vaccine safety monitoring, added the COVID-19 vaccines to the childhood vaccine schedule despite known harms, withheld data on boosters from the agency’s own advisers and told pregnant women the vaccine was safe — just days after Pfizer reportedly finalized a report demonstrating it wasn’t, among other things that have outraged critics.
In her letter of resignation, Walensky said “I have never been prouder of anything I have done in my professional career.”
The White House issued its brief “Statement from President Biden on Dr. Rochelle Walensky” on the same day it received Walensky’s resignation letter, which must be seen to be believed.
“Dr. Walensky has saved lives with her steadfast and unwavering focus on the health of every American. As Director of the CDC, she led a complex organization on the frontlines (sic) of a once-in-a-generation pandemic with honesty and integrity. She marshalled (sic) our finest scientists and public health experts to turn the tide on the urgent crises we’ve faced.
“Dr. Walensky leaves CDC a stronger institution, better positioned to confront health threats and protect Americans. We have all benefited from her service and dedication to public health, and I wish her the best in her next chapter.”
Walensky’s next chapter should be spent in prison for betraying the trust of the American people. She gave no clear reason for her resignation, except to note the “waning of the covid-19 pandemic” and “the nation is at a moment of transition as emergency declarations come to an end.” On the same day of Walensky’s announced resignation, May 5, the WHO officially ended the covid “global emergency.” The U.S. ended its covid “public health emergency” on May 11.
Two days after the director transfer, on July 2, Walensky had the further chutzpah to give an interview with the Wall Street Journal, “Departing CDC Director Rochelle Walensky Warns of Politicized Science,” in which “she says public needs to be wary of misinformation.” Once again Children’s Health Defense details why this is another act of astounding hypocrisy showing how Walensky’s CDC itself highly politicized the “science” and spread dangerous misinformation.
Rochelle Walensky is Jewish, as chronicled in an essay on substack Taboo Truth. It examines previous Jewish CDC Directors Jeffrey Koplan, Tom Frieden and Anne Schuchat and their various scandals, and other Jews within the agency’s historic infrastructure, including massive funding lobbied by Jewish Home Depot owner Bernard Marcus which expanded the CDC to the bureaucratic leviathan it is today.

Our new director of the CDC is also Jewish. Her name is Mandy Cohen, and in its June 16 “Intent to Appoint Dr. Mandy Cohen as Director of the Centers for Disease Control and Prevention,” the Biden White House presents her credentials (most recent listed first).
- Secretary of North Carolina’s Department of Health and Human Services
- transformation of North Carolina’s Medicaid program and Medicaid expansion.
- Chief Operating Officer and Chief of Staff of the Centers for Medicare and Medicaid Services
- Acting-Director of the Center for Consumer Information and Insurance Oversight
- Affordable Care Act policy development and implementation
- medical degree from Yale School of Medicine and a Master’s (sic) in Public Health from the Harvard School of Public Health
Walensky was also a graduate of Harvard School of Public Health. Just as Walensky, Jewish Mandy Cohen is married to a Jewish man, Samuel Cohen, a health care regulatory attorney. He is:
“Managing Director of Health Policy at Curi Advisory, which is a full-service advisory firm that serves physicians and medical practices. Equal parts fierce physician advocates, smart business leaders, and thoughtful partners, Curi’s advisory, capital, and insurance offerings deliver valued advice…”
Mandy’s maiden name is Krauthamer, spelled differently and not likely a relation except by tribe to the Jewish Neo-Con war-monger journalist Charles Krauthammer. Mandy’s Jewish mother Susan was a nurse practitioner in an emergency room on Long Island, who inspired Mandy onto a public health path. Her Jewish father was a high school guidance counselor.
An extensive and detailed profile of Mandy Cohen emerged in the first year of the covid pandemic when she was Secretary of the North Carolina Department of Health and Human Services (NCDHHS). Titled “She’s the face of NC’s fight against COVID-19. Meet Dr. Mandy Cohen, Tar Heel of the Year,” it announces “Cohen is The News & Observer’s 2020 Tar Heel of the Year, an honor that recognizes a North Carolina resident who has made lasting and significant contributions in the state and beyond.” This humanizing puff piece states, “Cohen has become the figurative and literal face of North Carolina’s ongoing fight against COVID-19.”
“It is a fight in which she’s relied most upon data and science and something less easily quantified: the sense of empathy and compassion that some closest to her say make her a perfect fit for her position. It is a fight that’s challenged her to balance competing interests — one that at times has brought fierce criticism from skeptics who dismiss science or downplay the virus — while maintaining the goal of preserving the health and lives of North Carolinians.”
According to North Carolina Dept. of Health and Human Services, using my own simple calculation, over the past year the case fatality rate from Covid-19 amounts to .4%. This means 3,903 people in North Carolina died with covid over the past year (not necessarily from covid, and according to flawed PCR test diagnostics acknowledged by the CDC itself). Open VAERS shows that 179 people in North Carolina have been reported slain by the vaccine since its roll-out in early 2021 until June 16 of this year (the same date the White House announced intention to appoint Cohen CDC director).
Recall that the Vaccine Adverse Reporting System (VAERS) was shown by the CDC’s own funded study in 2010 to report less than 1% of actual adverse vaccine events. The number of people slain in North Carolina by the vaccine could be more honestly at least 18,000. To compare these numbers—covid-killed vs. vaccine-killed—we should divide 18,000 by 2.5, since the covid-killed number is only for one year (the mildest year), and the vaccine-killed for 2.5 years. Answer: at least 7,200 vaccine-killed per year compared to under 4,000 per year covid-killed. The cure may have been at least almost twice as lethal as the disease.
As the Pfizer and Moderna vaccines were scheduled to arrive in North Carolina, Cohen addressed her staff. “So that tells me a couple things… One, no one else is talking about vaccines and sort of setting the stage and being transparent. So, A-plus, team. … We’re setting expectations. We’re sharing what we know. We’re being concrete. We’re talking about all our plans, so I’m really pleased.”
Yes, A-plus, team. Mandy is really pleased you were talking about vaccines and being transparent. Unfortunately for the thousands slaughtered by the vaccines in North Carolina and their families, you were not transparent about the carnage the vaccines could cause in the state. Cohen’s “sense of empathy and compassion” made her a perfect fit for that job.
Cohen’s Jewish identity is featured:
“She spent most of the next hour listening to her staff members detail their work. By the time the meeting was ending, Cohen had changed her virtual background to that of a picture of her family for some Throwback Thursday show-and-tell. The picture was from her oldest daughter’s baby-naming ceremony, a Jewish ritual, and the family was standing in front of a menorah.
“‘Throwback Thursday and Hanukkah,’ Cohen said with some excitement, introducing her family.
“Like her family, her faith has played an important role in helping her navigate the pandemic. She wears a necklace with the chai (pronounced like “high”) symbol around her neck. The symbol represents the Hebrew word for life and health.
“When Cohen and her husband moved to North Carolina, they did not know anyone. The synagogue they chose became a second home. “And I also joke with the rabbi that I think Jews were public health people before they knew what public health was,” Cohen said, referencing Jewish dietary restrictions, and how even before the pandemic there was “a lot of washing your hands in Jewish ritual practices.
“Back on the work call, Cohen wished a Happy Hanukkah to those celebrating. It was the first night of the festival, and she needed to hurry home.”
If Cohen’s “faith” is even remotely Talmudic-influenced, the chai symbol represents the Hebrew word for life and health to Jews, and death and sickness for Goyim. Washing hands in Jewish rituals may sometimes be a necessity to cleanse away the blood from the male genital mutilation ceremony of circumcision, cruel animal sacrifices, and Jewish Ritual Murder that includes drinking the blood of raped, tortured and slaughtered children. Cohen of course does not allude specifically to these Talmudic blood rituals, but the hand-washing associated with them could hardly have made such extreme Talmudic fundamentalist Jews “public health people.”

Cohen cannot be accused of these Judaic horrors, but just as with Walensky, nor can she be trusted with a “sense of empathy and compassion” while wearing a Hebrew symbol of life and health. Chai means “to live and walk in the Jewish cultural lifestyle,” and also “the lowest (closest to the physical plane) emanation of God.” She may be worshiping a Hebrew god who seems more like a demon, demanding blood, insanely jealous, viciously punitive to a genocidal extent, and intolerably racist.

The ever-alert Children’s Health Defense, in commenting on Cohen’s appointment to CDC director, did not take its criticism so far, but it is indicative that CHD called Cohen “fanatic.” In “‘Fanatic?’: Biden’s New CDC Director Was Strong Proponent of Pandemic Mandates, Masks and Lockdowns,” author Michael Nevradakis, Ph.D. quotes critics who have emerged throughout the covid years 2020-21 as voices of medical scientific reason.
“Cohen appears to be fully entrenched in the ‘bio-pharmaceutical complex.’ She was on the wrong side of every pandemic public health intervention, failed to recognize early therapeutics and natural immunity, and to date has not acknowledged the safety disaster unfolding with the COVID-19 mass, indiscriminate, vaccination program.”
-Dr. Peter McCullough, author The Courage to Face COVID-19: Preventing Hospitalization and Death While Battling the Bio-Pharmaceutical Complex
“(Cohen is) a public health COVID authoritarian and the worst possible person to become the next CDC head.”
-Alex Berenson, commentator and former New York Times journalist
Berenson is Jewish, and in his own article, “URGENT: Joe Biden is about to pick the worst possible person to become the next CDC head,” said something Nevradakis did not include:
“Apparently diversity mandates haven’t hit the CDC yet. Cohen is a lot like Walensky, a nice Jewish* doctor** from the Northeastern suburbs with all the right degrees.
“(*I can say it, I’m Jewish)
“(**The actual expression is “nice Jewish girl” but I don’t want to get in trouble)”
Berenson is suing Andy Slavitt, Jewish (not found in “early life and education,” but at the end in Categories, “American Jews”), over censorship infringements. Slavitt started out at Goldman-Sachs investment bank, and ended up senior adviser on President Joe Biden’s coronavirus response team.
Returning to quotes in the CHD article:
“Going through [Cohen’s] timeline is a strange blast from the past of heartbreaking fear-mongering, pseudo-science, and propaganda. She passed with flying colors all three tests of compliance: closures, masking, and vaccine mandates.”
– Jeffrey A. Tucker, founder and president of the Brownstone Institute
In his essay, “New CDC Director Is Another Lockdowner,” Tucker starts by telling us that in order to have power and influence in the Soviet Union, one needed to be a member of the Communist party.
“We are headed this way in the US today. The party in question is the lockdown party. … That’s my best read on why Mandy Cohen is being pulled away from her perch in North Carolina, where she led a catastrophic pandemic response, to be the replacement for Rochelle Walensky as head of the Centers for Disease Control and Prevention. She is a faithful member of the lockdown party and thus demonstrates her willingness to do it again should the occasion arise.”
My best read is that both Walensky and Cohen are members of the Jewish party, with lockdowns as their strategy to advance Jewish profit and control objectives. Their willingness to do it again is rooted in their faithfulness to Jews and Judaic indoctrination. The occasion will arise because they will engineer one again. For a wider analysis of the Jewish role in covid, see the TOO book review “New Covid Book Tackles Taboo Truths.”
CHD/Nevradakis: “Cohen was ‘the top choice of Jeffrey D. Zients,’ the Biden administration’s former COVID-19 response coordinator.”

Zients is of course Jewish as well, suggesting the well-known phenomenon of Jewish tribal nepotism in appointing Cohen. Zients went from COVID-19 response coordinator, “charged with rolling out a massive vaccine program nationwide in early 2021,” to the current White House Chief of Staff, “like the chief operating officer for the government.”
Zients replaces Ron Klain, also Jewish.
“Jewish Ron Klain has been Joe Biden’s political alter ego for many of the last 40 years, regardless of his position or Biden’s interaction with Jews and Israel,” Democratic Party strategist Steve Rabinowitz said, adding: “Along the way, Klain has proven himself as friendly to our community and to Israel as we are with his old/new boss.”
Closely similar to Zients, and generally similar to Walensky and Cohen, Klain formerly took charge of a “pandemic response” to another disease scare in 2014, as Obama’s “Ebola Czar,” according to the Jewish Forward. Given the general Jewish hatred of the Russian Czars, I struggle to understand why these Jews apply this term to themselves when they lead “pandemic response” efforts. Perhaps to further defame the long-dead Czars, but doesn’t this also defame themselves?
CHD/Nevradakis quotes:
“Dr. Mandy Cohen during her tenure as North Carolina’s HHS secretary pushed through the most draconian COVID-19 measures imaginable.
“With her at the helm of the CDC, I expect we will just get more lying and hiding regarding the agency’s abysmal response to the pandemic and horrific track record in general.”
-Brian Hooker, Ph.D., P.E., senior director of science and research for Children’s Health DefenseCohen was particularly harsh on children in North Carolina, imposing mask mandates in school regardless of vaccination status, extending school closures longer than most other states, and threatening to sue a county school board if it did not “rescind a new policy that eliminates COVID-19 quarantine measures for most students and staff.” All this after it was known that children were at almost zero risk from covid. In “studies of children (that) are the most comprehensive yet anywhere in the world,” 2 in a million children died of covid, and most of those had “co-morbidities.”
Combine Walensky’s damage to unborn babies in the womb with Cohen’s damage to school-age children, and these two Jewish lockdown/vaccine “fanatics” covered the entire childhood age range with trauma and death, for no valid reason.
Adolescent suicides spiked during the pandemic. In North Carolina under Cohen’s lockdown reign, “youth” suicides spiked, attempts up 46% among 10-14 year old girls in 2021. Cohen continued to impose among the harshest school lockdown measures in the nation, motivated no doubt by her Jewish “sense of empathy and compassion.”
When they heard rumors that the Biden Administration—itself overwhelmingly Jewish—was planning to propose Cohen as CDC director, a group of 28 Congresspeople (24 men including a Senator and a Representative from North Carolina, and 4 women including Marjorie Taylor Greene) issued a joint letter to the President dated June 13 2023. They state:
“Dr. Cohen is unfit for the position. Throughout her career, Dr. Cohen has politicized science, disregarded civil liberties, and spread misinformation about the efficacy and necessity of COVID vaccinations … and the necessity of masks.
“… Dr. Cohen was a proponent of unnecessary, unscientific COVID restrictions on school children… After a North Carolina school district followed the science by declining to institute unscientific mask mandates and voted with an overwhelming majority to end “contact tracing” and curtail other unproven and largely hysterical quarantine policies, Dr. Cohen threatened to bring legal action against the district. Dr. Cohen’s willingness to threaten the school district put politics over the well-being of children and is just another example of the litany of public health abuses the American people endured at the hands of bureaucrats throughout the COVID-19 pandemic.”
The letter continues:
“Dr. Cohen has an extensive history of publicly… supporting radical, left-wing policies … (She) endorsed an unconstitutional ban on semi-automatic rifles and lobbied to classify climate change as a ‘public health crisis.’”
“Given her strong affiliation with… the COVID-19 lockdowns, it will be difficult for the American people to trust Dr. Cohen to run the CDC as a nonpartisan actor who makes objective decisions rooted in scientific data, and not in political expediency.”
Or Jewish Talmudic “science tikkun” as espoused by militant Jewish vaccine promoter Peter Hotez. In 2020 as secretary of NCDHHS, Cohen said in an interview with Religious News Service : “There’s so much of what I do in the health and human services space that’s so aligned with Jewish values of healing the world.” Healing the world is dangerously close to the Judaic concept of tikkun olam: fixing the world. The article further states: “It (wearing the Hebrew Chai necklace) is a testament to her faith — she is Jewish — and, in this strange pandemic moment, to her religious values.”
And: “As the Jewish High Holidays approach, Cohen said she looks forward to the time of reflection and introspection — the themes of Rosh Hashana and Yom Kippur — especially as they relate to her public work.” This ten day period between Judaic holy days includes a day of judgment where the fate of the wicked is decided. It is a time of reflection and repentance. As the wicked witch of North Carolina health and death, Cohen had much upon which to reflect and repent.
Dale Folwell is running for North Carolina governor. He tweeted:
“… the actions of Dr. Mandy Cohen during Covid resulted in more disease, death, poverty and illiteracy. As NC Governor, I would be hard pressed to ever follow her lead at CDC if chosen by the POTUS.”
The tweet was on June 2, two days after Cohen officially became Director of the CDC.
Private Sector, Monied Interests
In the short time between her resignation from NCDHHS in November 2021 and her appointment to CDC Director on July 1, 2023, Cohen was the Executive Vice President of Aledade, “the nation’s largest network of independent primary care practices.” She was also the Chief Executive Officer of Aledade Care Solutions, “the company’s new health services unit.” Aledade’s Executive Team’s webpage still lists Cohen as EVP and CEO of the Care Solutions new unit.
The Department of Justice lists under Government Ethics, Conflicts of Interest:
“An employee is prohibited from participating personally and substantially in a matter in which he, his spouse, minor child, or a general partner, or an organization of which he is an officer, director, trustee, partner or employee has a financial interest.”
Or she, in Cohen’s case. We must watch her closely for conflicts of interest, since her Jewish predecessor Walensky was identified in just such a conflict in 2021 soon before and after her appointment to CDC director. In “CDC Director Walensky’s Husband Received $5 Million in HHS Grants – and That’s Just the Start of It,” we see the insider connections, including Fauci, and another NIAID official who was on the oversight committee that approved the grant, both of whom worked with Rochelle in her time at CDC before she became director. They funneled a large research grant to Rochelle’s husband Loren’s private biotech firm Lytica Therapeutics. He is shown on the Team webpage as “Scientific Cofounder” and his bio states he is “Professor Pediatrics at Harvard Medical School, and Director of the Harvard/MIT MD-PhD Program.”
Also on the team is a Daniel Cohen, PhD, Associate Principal Scientist, Protein Chemistry. Mandy’s Wikipedia entry shows in its Early Life section, she “has two younger siblings.” The “Tar Heel of the Year” article says, “Her brother’s family just had a baby in May…” Certainly we see many Cohens throughout the Jewish power structure, and cannot verify that Daniel has any direct relation to Mandy except by tribe.


Hebrew name Cohen means Priest, descended from Aaron.
Cohen’s CDC Promotes “Chest Milk”
Such speculation is unnecessary. Cohen’s depravity emerged within a week of taking office when numerous news reports quoted the CDC stating: “transgender and nonbinary-gendered individuals may give birth and breastfeed or feed at the chest (chestfeed).” This ignited outrage from the nation’s mothers, Republican party candidates, Fox News and many others.
Not surprisingly, links to the CDC statement in these reports go nowhere or in circles now, but one prominent mention found on the CDC official website says under “Priority Breastfeeding Strategy: Continuity of Care” – “Review (of) Continuity of Care in Breastfeeding Support; a Blueprint for Communities” document: “Create community environments that proactively promote, protect, and support chest/breastfeeding.”
It is under “Health Equity Considerations” where we find the horrifying statement under “Pronoun Use – Remember That:” There is more. “An individual does not need to have given birth to breastfeed or chestfeed. Some families may have other preferred terminology for how they feed their babies, such as nursing, chestfeeding, or bodyfeeding.”
In an established pattern of recklessness endangering the nation’s children and mothers, Cohen failed to warn of the dangers to babies from synthetic hormone-induced “chest milk.” The synthetic hormone no longer recommended for increasing natural female lactation but recommended (not by name) for transsexual “chest feeding” Domperidone is a known risk to babies.
Cohen’s tribal colleagues the Jewish Pritzker family rules the transsexual transition industry with billions of dollars in grants, investments, donations and profits to impose the unholy inhuman agenda. Family oligarch Tom Pritzker was only one of two names listed in Jewish Epstein’s notorious black book with a special hand-written note: “Numero Uno.”

Caution: Another Jew Leads CDC
We have seen excessive evidence that the new CDC director Mandy Cohen will inflict whatever catastrophic lockdown measures and vaccine mandates the next contrived disease panic offers to further Jewish objectives, just as previous CDC director Rochelle Walensky.
May we all take caution. Not viruses, but certain Jews acting in coordination have infected the governmental power structure with the capability of inducing sickness and death by unelected, arbitrary and capricious decree. The cure is truly worse than the disease. The new CDC director Mandy Cohen, driven by her Judaic faith, now leads the most powerful Federal agency imposing public health/death measures.
May we turn to a more natural, holistic health model to survive her impending reign of terror at CDC.
The American Board of Internal Medicine’s Longstanding War On Doctors Is Escalating
The ABIM’s history proves their present actions are political/financial and not scientific. They are making examples of us “dissenters” to scare the rest of the country’s docs to keep quiet.
BY PIERRE KORY, MD, MPA | AUGUST 23, 2023
The unholy alliance of industry captured high-impact medical journals, federal public health agencies, professional societies (ABIM, AMA, APHa etc), and most importantly, the state medical licensing boards directed by the Federation of State Medical Boards (FSMB) are still going hard after us “dissenting” doctors. You know, those of us that very publicly called out the unscientific policies implemented by corrupted policymakers in a directed pursuit of profits and power. Their actions trying to silence us (and to scare other doctors from speaking out) are escalating.
Recently, what I call the “misinformation committee” of the American Board of Internal Medicine (ABIM) voted to strip Professor Paul Marik and myself of our Board certifications. To best understand why they would do this, I think it is important to review what the ABIM is, how it operates, and then detail their absurd attempt to paint us as misinformationists by using disinformation.
Let’s trace my current relationship with the ABIM to today:
At the end of my training, I became Board Certified by the ABIM in three specialties (Internal Medicine, Pulmonary Diseases, and Critical Care Medicine).
What is the ABIM? Well, from this devastating article by Kurt Eichenwald, an accomplished corporate investigative journalist who did a devastating takedown of the ABIM and its officers in a Newsweek piece in 2015:
The ABIM is a purported nonprofit that certifies new physicians as meeting standards of practice. Beginning in the early 1990s, the ABIM ordered certified doctors to be recertified, again and again. Without the ABIM seal of approval, lots of internists and subspecialists can’t get jobs and can’t admit patients to hospitals. So by taking advantage of that monopolistic power, the ABIM has forced hundreds of thousands of physicians to follow recertification processes that doctors complain cost them tons of money (paid to the ABIM), require tons of time (taken from families and medical practices) and accomplish nothing.
In many doctor’s opinion, this cash grab of the ABIM by selling “certifications” is a corrupt farce. There is no evidence that certifying doctors in this highly costly way does anything to improve the quality of care delivered. The ABIM has not only refused to produce data showing the program improves patient care but also hasn’t conducted any studies on that matter. In fact, the ABIM and its related organizations are:
harming American medicine and diminishing the quality of scientific research, pushing physicians to close practices rather than wasting time on expensive and frustrating busywork, and forcing specialists to play a game of medical trivial pursuit. (Even Baron has admitted that he was tested for recertification on topics he never used in his practice.)
But it sure does generate cash for ABIM executives. Note that Board Certification used to simply be a sort of “honor” denoting that the member passed a more rigorous examination in their specialty. That “honor” comes at a price though:
Since I am (was?) Board certified in 3 specialties, lets do some math as this is what it costs me to re-certify every ten years:
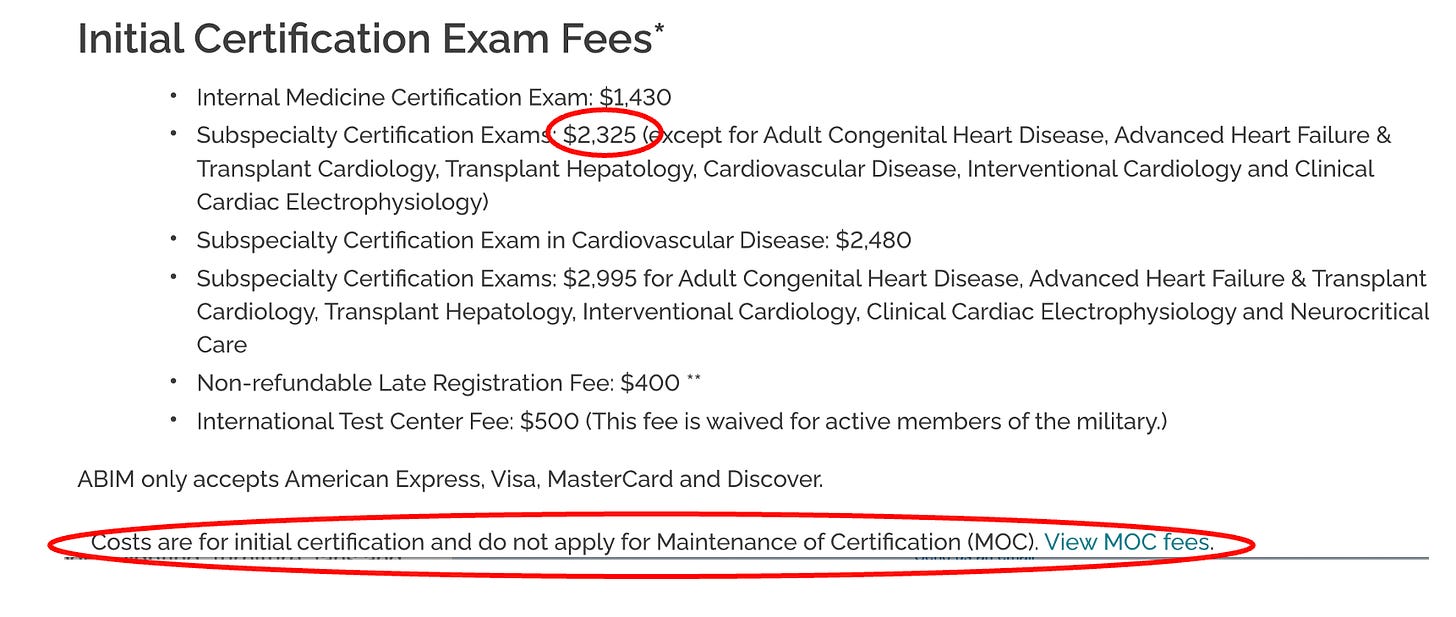
$1,430 for Internal Medicine
$2,325 for Pulmonary Diseases
$2,325 for Critical Care Medicine
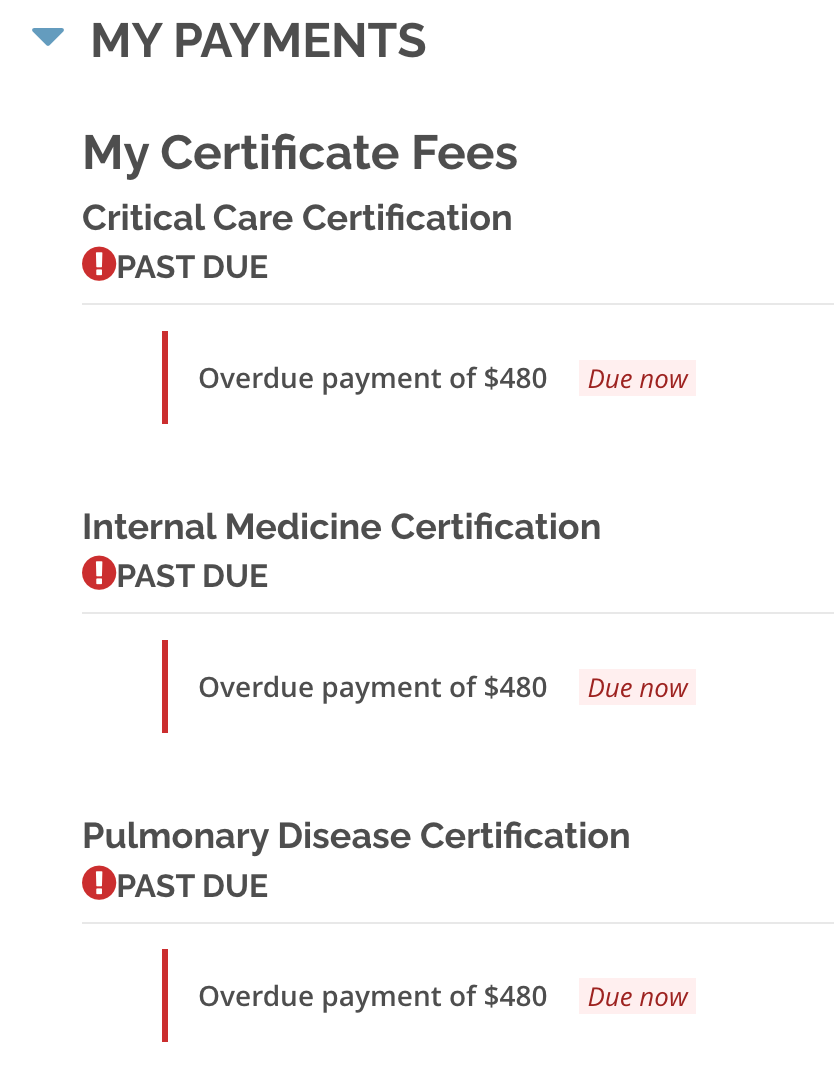
But wait, we are not done yet. These bastards were not making enough money with once-every-ten-year recertification exam fees, so they invented a new program of annual busywork education requirements which they called Maintenance of Certification (MOC) which costs you $220 every year for every certification (plus late fees if you forget). To wit, I went into my patient portal and discovered. I owe them $480 for each of my certifications!
And get this – that money essentially goes to ABIM executive salaries and pensions and other dubious private investments as described by Eichenwald where he details the insane lengths the ABIM goes to “hide” the compensation and pension data on its executives. What is worse is that ABIM certification has now been made a requirement of employment as a faculty member of academic medical centers and hospitals and is also a requirement to be on many insurance company panels (these actions further strengthen the control of doctor behavior).
Doctors have started publicly slamming the group in industry publications. “ABIM is imposing on us an onerous and ill-conceived tool, one that most physicians agree is irrelevant,” Dr. Karmela Chan wrote in Internal Medicine News. “I am glad this conversation is happening, because, frankly, the process was enough to make me want to quit being a doctor.” Further, in a recent poll of 2,211 physicians conducted on a doctors-only website called Sermo, 97 percent of the respondents criticized recertification.
Richard J. Baron, the ABIM CEO that sent letters threatening decertification to me and Paul, makes close to a million dollars a year, however that data is almost impossible to find due to the ABIM’s multiple attempts to obscure it as well as its spokespeople avoiding answering any inquiries on the topic. Here is a summary of Eichenwalds findings on the ABIM:
- In 2015, they were 5 months late in filing their publicly available financial report with the IRS (that several journalists were very interested in).
- The report is full of obfuscations and anomalies of reporting of not only the actual money earned by the executives, and particularly Baron, but his financial conflicts of interest are even better hidden.
- A big percentage of the ABIM’s millions was in the form of cash to one former employee.
- The ABIM in 2013 had 57 million against liabilities of 105 million – while Baron was going around saying that its assets are three times its liabilities (this was a 100% lie. When I get to the ABIM’s response to our defense letter, remember that what liars do is.. lie).
- It lost $4.8 million on $55.5 million in revenues, no small feat and almost entirely due to a bloated payroll.
- It also claims it spends no money on lobbying while it spent between 100K to 160K annually to lobby Congress on Medicare and Medicaid (another lie).
- The data on top officers compensation is so obscured and fragmented, Eichenwald reported that he had found it much easier to discover executive compensation at Enron, Worldcom and Adelphia – all famous for lying on tax filings. Again no small feat (to be one of the top corporate liars in the U.S).
- Officers “double dip” – former CEO Christine Cassel got $741K from ABIM and $247K from the ABIM “Foundation” (slush fund for ABIM officials) and also got $219K in “other compensation” – totaling $1.2 million for one year. (Nice gig if you can get it).
- But wait, we are not done. Cassel also got $504K in “deferred compensation” for a total of $1.71 million more that year (six times the median compensation for similar sized non-profits). Six times.
Then there is this doozy of an article which came out this week in The Defender by Children’s Health Defense, detailing the ABIM CEO Richard Baron’s conflicts of interest:
Some of the most disturbing reveals:
“The head of a national medical organization who publicly called for doctors to lose their licenses unless they supported government narratives on COVID-19 treatments and vaccines concealed his relationship with a public relations firm whose client list also included Pfizer, Moderna and the Centers for Disease Control and Prevention (CDC).
Dr. Richard Baron, president and CEO of the American Board of Internal Medicine (ABIM) is a client of Weber Shandwick, investigative journalist Paul D. Thacker reported on Wednesday.
Note that I went after Weber Shandwick in my book, “The War on Ivermectin” where I argue (without proof, although I believe that is coming because I know of a subpoena coming their way) that they created and launched the “Horse Dewormer PR campaign,” highlights of which was the famous FDA tweet and absurd Rolling Stone article:

In late 2021, Baron publicly pushed for doctors who spread “misinformation” about COVID-19 and the vaccines to lose their license and certification.
Last year, Baron partnered with Weber Shandwick to propose a South by Southwest (SXSW) panel titled “When Doctors Prescribe Misinformation.” The proposal was subsequently accepted and the panel took place at SXSW in Austin, Texas, on March 13.
According to Thacker, “Weber Shandwick’s panel featuring Dr. Baron has been widely promoted by the PR firm’s employees,” including Sarah Mahoney, executive vice president, Healthcare Communications, Strategy & Planning for Weber Shandwick, who in a LinkedIn post, wrote she “can’t think of a more important topic right now.”
Although to the unawake the following may seem normal public health practice, but to those of us fighting agency capture by Big Pharma, it is absurd:
The CDC’s National Center for Immunization and Respiratory Diseases (NCIRD) in September 2020 awarded Weber a $50 million contract “to promote the vaccination of children, pregnant women and those at risk for flu and increase the general acceptance and use of vaccines,” according to the PR firm’s website.
Thacker said he believes much of what is labeled “misinformation” in medicine and academic research “is really just corporate PR,” and that “Congress needs to take a harder look at funding for ‘misinformation research.’“
Speaking of taking a harder look at where the funding is coming from for “misinformation research” and the ABIM, it turns out that.. we can’t. Why? Check out this tweet showing a clause inserted into the ABIM’s by-laws in 1998:
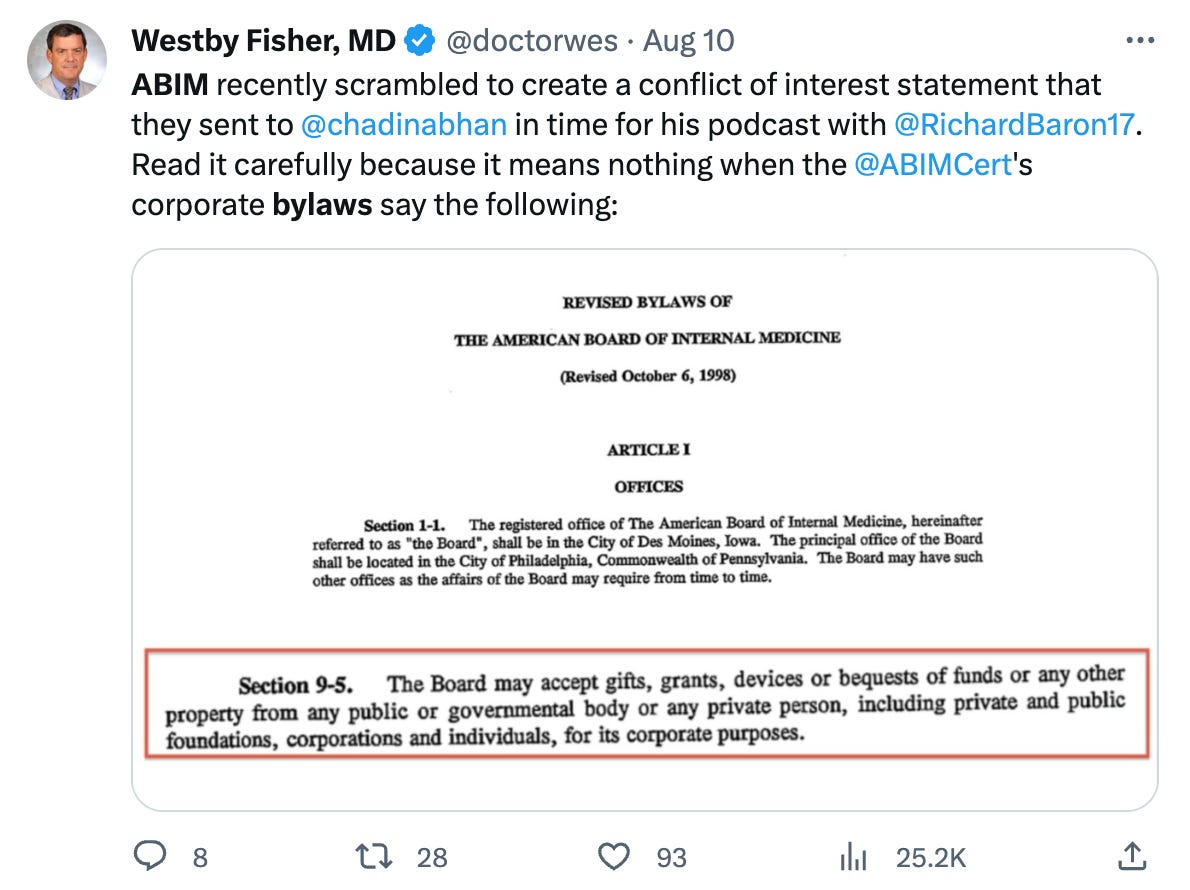
But wait, it gets better, like way better. Also in their by-laws:
Information that is disclosed will be kept confidential except to the:
-
- President and Chair of the Board;
- The chairs of the relevant Subspecialty Boards, Test-Writing Committees, and other Committees of the Board, members who serve on the relevant Boards and Committees, and staff working with the respective committees;
- The Conflict of Interest Committee members and Conflict of Interest Committee staff,
except as required for the purposes of continuing medical education.
So, basically, they can take money from any corporate entity and do not have to disclose it to anyone. Again, nice gig if you can get it.
Back to the ABIM’s history: One of Eichenwalds more disturbing observations about the behavior of the ABIM:
I can attest to the ABIM’s pomposity. Starting with my first story about the ABIM, the organization usually has refused to acknowledge I even asked a question. The only other group to do that in my 30-year journalism career was a company that processed payments for child pornography websites. Plus, when I reported on the uprising by doctors, the ABIM ignored the facts and instead investigated me.
Now lets fast forward to Covid. On July 29, 2021, the FSMB (this entity controls the state medical licensing boards, not the ABIM – at least on paper) issued a policy statement that “Physicians who generate and spread COVID-19 vaccine misinformation or disinformation are risking disciplinary action by state medical boards, including the suspension or revocation of their medical license.”
What is interesting is how fast and how rigidly the ABIM followed the FSMB’s lead and enacted their own misinformation policy despite the fact that, as my colleague Meryl Nass has pointed out:
“suddenly claiming that using licensed drugs for COVID, criticizing federal policies for COVID or criticizing the value of COVID vaccines is unprofessional” gives the specialty board the right to revoke a certification—well, that was never part of its contract with me. So pulling my certification for issues that were never specified in the original contract is breach of contract.
I think it would only be a breach if contracts, like our Constitution and the practice of medical ethics, were still “a thing.”
The ABIM apparently liked the FSMB’s “misinformation policy” idea to attack dissenting doctors so much (or were told to like it) that 2 months later, they, along with their colleagues at the American Board of Pediatrics and the American Board of Family Medicine, issued a statement supporting the FSMB’s position, saying, “We all look to board certified physicians to provide outstanding care and guidance; providing misinformation about a lethal disease is unethical, unprofessional and dangerous.” (note that they seem particularly focused on Covid misinformation and not any other disease model or therapeutics. Do you think it could be because Covid vaccines and therapeutics opened immensely profitable markets to Pharma overnight?).
Again from Meryl Nass (please subscribe to her Substack):
Furthermore, the processes the ABIM is using, as described by CEO Richard Baron, MD in his podcast with the New England Journal of Medicine are procedurally unfair. Dr. Baron earns $1 million/year to threaten doctors for a crime that does not exist. Baron, notably, refused to specify where the line was between misinformation and genuine disagreement in that podcast, though he seems to have no difficulty at all drawing the line when it comes to licensees who speak publicly about how to manage COVID. In a truly Orwellian effort, the ABIM and the ABIM Foundation have dedicated the year to ‘building trust’ in medicine.”
In what I suspect was the ABIM’s first enforcement of their shiny new policy, they go after Peter McCullough, Paul Marik, and myself on the same day (May 26, 2022) with a letter quoting numerous public statements we made, implying that we needed to defend the substance of such statements with supporting data or risk losing our certifications.
“Game on” I thought, looking forward to the exercise of “debating” scientific data with the ABIM. However, our FLCCC lawyer, Alan Dumoff pointed out that the ABIM’s policy and procedures state that the process of accusing a member of misinformation requires that they first provide evidence to us that what we said was inaccurate. So, we wrote back, pointing out to the ABIM their brazen “error” (yeah right) in not complying with their own policy and procedures.
“Nonsense” they wrote back (in short). Their logic was truly shocking – they say that the fact they provided the substance and references to my public statements means they did their duty (rather than their providing references that would refute my statements which is what their policy states they need to do).
You can read their brazen, illegitimate, dismissive response here:

This letter above demonstrates the unchecked power they have – they alone determine whether they are following their own policy which they so clearly were not. What did I say about liars before?
Anyway, rebut them we did. We wrote a 76 page treatise with 175 references, 11 exhibits, and 22,000 words, marshaling and weaving numerous data sources to support all our public statements that they had a problem with. May it enter the historical record here (I think you Covid vaccine and ivermectin data geeks will find the letter impressive).
We sent that letter over 6 months ago… and finally got an answer a few weeks ago. To understand the misinformation committee’s response, note this statement from an editorial written by Baron where he tries to give examples of misinformation:
A whole range of statements with which many — or even most —physicians might disagree would therefore not trigger our disciplinary process. On the other hand, when someone certified by the ABIM says something like “the origin of all coronary heart disease is a clearly reversible arterial scurvy” or “children can’t spread Covid” or “vaccines don’t prevent Covid deaths or hospitalizations,” we are not dealing with valid professional disagreement; we are dealing with wrong answers.
That last sentence is critical as Baron literally is saying that the ABIM gets to determine what is a valid professional disagreement versus a “wrong answer.” Good to know, especially in regards to the fact that the narrative that “vaccines prevent Covid deaths or hospitalizations” was strongly refuted in our initial response letter.
This issue about drawing a line between misinformation and genuine disagreement is a critical one. From our letter of appeal written by our lawyer Alan Dumoff:
Threshold Issue: What Standard Distinguishes Legitimate Differences of Professional Opinion and Misinformation
We disagree with the Committee’ s interpretation of the data, which we address below, but the initial question is by what standard the American Board of Internal Medicine (“ABIM” or “Board”) evaluates evidence to determine that disagreement with consensus generally, and regarding controversial matters around COVID-19 policy specifically, rise to the level of actionable misinformation. The Board’s policy recognizes the right to legitimate debate, which requires it not merely show evidence supporting a consensus view but that it demonstrate that these professional disagreements are not legitimate but outright misinformation.
If not grounded in an articulated standard, at the very least, the Board must demonstrate that the views at issue are false by citing the fallacies in the actual substance of the evidence provided, not simply by critiquing a few isolated studies divorced from the totality of evidence. Resting solely upon citations to mainstream publications while substantially avoiding the evidence in our Submission, and our detailed critiques of these publications does not provide a basis for the Board to take action against my clients.
A diplomate’s medical positions must be plainly erroneous to merit sanction. Departure from consensus is hardly unusual and by itself insufficient. While the Sanctions Notice gives the appearance of having done so, the Committee did not directly engage the numerous imperfections in the mainstream approach Drs. Kory and Marik’s have pointed to in substantial detail. The Committee has not engaged the evidence submitted and demonstrated it is illegitimate, only that it departs from the consensus, that is insufficient to support a sanction.
The point is that the ABIM appears absurdly obsessed with getting doctors to spout only consensus opinions. This is literally unprecedented in science. From Michael Chrichton the author:
I want to pause here and talk about this notion of consensus, and the rise of what has been called consensus science. I regard consensus science as an extremely pernicious development that ought to be stopped cold in its tracks. Historically, the claim of consensus has been the first refuge of scoundrels; it is a way to avoid debate by claiming that the matter is already settled. Whenever you hear the consensus of scientists agrees on something or other, reach for your wallet, because you’re being had. Let’s be clear: the work of science has nothing whatever to do with consensus. Consensus is the business of politics. Science, on the contrary, requires only one investigator who happens to be right, which means that he or she has results that are verifiable by reference to the real world. In science consensus is irrelevant. What is relevant is reproducible results. The greatest scientists in history are great precisely because they broke with the consensus. There is no such thing as consensus science. If it’s consensus, it isn’t science. If it’s science, it isn’t consensus. Period.
I love that last line so much it bears repeating, “If it’s consensus, it isn’t science. If it’s science, it isn’t consensus. Period.”
Now, let’s look at their response to our 76 page letter teeming with supportive data for our statements. Can read their letter in its entirety here but I thought I would just pull the most illustrative sections:
… the CCC (i.e. misinformation committee) concluded that your statements about the purported dangers of, or lack of justification for, COVID-19 vaccines are false and inaccurate because they, too, are not supported by factual, scientifically grounded, and consensus driven scientific evidence. In fact, the overwhelming body of factual, scientifically grounded, and consensus-driven evidence – at and since the time you made those statements – shows that the COVID-19 vaccines are safe and effective for children and for adults
I have heard of the term “evidence-based medicine (EBM)” which is what I practice, but not “consensus driven science” (completely new invention – pernicious indeed. I Actually adhere to the original definition and conceptual framework envisioned by the founders of evidence based medicine which was incredibly well detailed in a by my friend “A Midwestern Doctor” in his brilliant recent post “What Happens To Doctors Who Innovate”.
Anyway, they then listed a few published, peer-reviewed papers supporting their point, blissfully un-acknowledging of the fact that the high-impact journals have been systematically censoring pretty much all negative analyses of the vaccine campaign’s impacts while publishing nothing but positive reports with cherry-picked and/or fraudulent data – so there is no way for the truth about vaccines to win in scientific debates my friends.
The high-impact journal censoring of adverse vaccine data is identical to their censoring of dozens of positive trials of ivermectin, something I extensively detail in the chapter called “The Journal Rejections of Positive Ivermectin Studies” in my book.
It gets even better – they next argue against my claims of lack of safety of the vaccines by, get this, referencing proclamations by the WHO and CDC. They ignore all the immense data to the contrary that I submitted while of course being willfully oblivious to the fact that the CDC and WHO are fully Pharma captured agencies:
Moreover, the vaccine safety data overwhelmingly (overwhelmingly?) contradicts your statements about vaccine risks. See, e.g., Centers for Disease Control and Prevention, “Safety of COVID-19 Vaccines,” https://www.cdc.gov/coronavirus/2019-ncov/vaccines/safety/safety-of-vaccines.html (updated March 7, 2023) (reporting that “Adverse Events (Serious Safety Problems) Are Rare,” and that “[t]he benefits of COVID-19 vaccination outweigh the known and potential risks”); World Health Organization, “Safety of COVID-19 Vaccines,” https://www.who.int/news-room/feature-stories/detail/safety-of-covid-19-vaccines (March 31, 2021) (stating that “[b]illions of people have been safely vaccinated against COVID-19,” that “mRNA vaccines [for COVID-19] have been rigorously assessed for safety, and clinical trials have shown that they provide a long-lasting immune response”).
The paragraph above should enter the historical record… somewhere. That will NOT age well. The only thing more absurd to contemplate is whether they know they are lying in their letter or if they are simply referencing propaganda that they themselves swallowed whole? In a way, the former might be more acceptable to me at this point.
Their opinion on how I got ivermectin wrong was similarly brazen – they ignored all the meta-analyses (historically considered the strongest form of data, a fact they seem to have willfully avoided) in favor of listing a handful of trials where ivermectin was supposedly found ineffective, relying mostly on citing “the Big 6” (what I named the chapter describing the fraud behind the 6 largest, Pharma-conflicted and most publicized trials on ivermectin). This was 100% unsurprising.
Check it out:
First, the CCC concluded that your statements about the safety and efficacy of ivermectin and hydroxychloroquine as treatments for COVID-19 are false and inaccurate because they are not supported by factual, scientifically grounded, and consensus driven scientific evidence (there it is again).
Susanna Naggie, M.D., M.H.S., et al., “Effect of Ivermectin vs Placebo on Time to Sustained Recovery in Outpatients With Mild to Moderate COVID-19,” 328 JAMA 1721 (2022), https://www.nejm.org/doi/full/10.1056/nejmoa2115869 (finding in a double-blind, randomized, placebo-controlled study with 1,800 participants that “[a]mong outpatients with mild to moderate COVID-19, treatment with ivermectin, compared with placebo, did not significantly improve time to recovery,” and that “[t]hese findings do not support the use of ivermectin in patients with mild to moderate COVID-19”);
I laughed out loud when they led their argument with the Naggie trial funded by the NIH as it contained the most brazen fraud of the Big 6 Pharma Ivermectin trials. All you need to know about the trial is that they moved the primary comparison endpoint of the trial.. in the middle of the trial. They moved the main comparison from symptoms at Day 14 to Day 28. Note that changing endpoints in the middle of a trial is a supposed never event. Except the same trick was pulled in the Remdesivir trial.
Anyway, in a presentation by Naggie, in this secondary endpoint, you can see that ivermectin was superior at Day 14 to a high degree of Bayesian “statistical significance” but the “statistical significance” was not reached at Day 28 (I use quotes around statistical significance because it is an erroneous concept when doing Bayesian statistics but that is what they did anyway when they pre-specified a threshold of above 0.95 as “significant”). Can anyone tell me why they moved the endpoint to Day 28 in the middle of the trial:
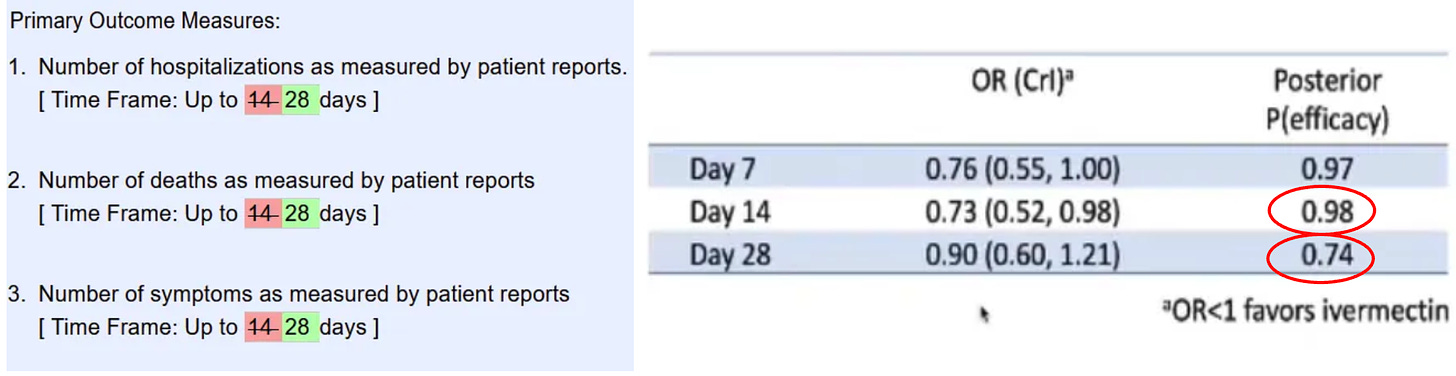
With this brazen maneuver (and many others) it allowed Naggie et al to publish this conclusion: “these findings do not support the use of ivermectin in patients with mild to moderate COVID-19.” Not-so-fun fact: Naggie also sat on the NIH covid treatment guidelines committee where she voted to not recommend ivermectin right before she and her University received tens of millions.. to study ivermectin in Covid. You want more? She also owns stock in a competitor to ivermectin (monoclonal antibodies for Omicron) and has received money from numerous other Big Pharma companies including Gilead. Lets get back to the letter…
Rather, the CCC seeks to accomplish precisely what you assert ABIM should be doing: seeking to “further the professional integrity of medicine by encouraging evidence-based debate” (emphasis added).
Indeed, as set forth in ABIM’s False or Inaccurate Medical Information policy, physicians have an ethical and professional responsibility to provide factual, scientifically grounded, and consensus driven scientific evidence (there it is again). As discussed above, by touting the effectiveness of ivermectin and hydroxychloroquine as COVID-19 treatments and casting doubt on the efficacy and safety of COVID-19 vaccines with such seemingly authoritative statements, you have made statements that are inimical to ABIM’s ethics and professionalism standards for board certification.
In light of all the evidence and circumstances, the CCC determined to recommend that your board certification be revoked.
There is only one silver lining here. One – the impending loss of my certifications does not affect me materially because I have a private fee-based practice due to my need for complete autonomy and lack of restrictions in empirically treating the vaccine injured with various repurposed and alternative therapeutics. I thus cannot and will not accept insurance, and secondly, my academic career is over – no longer will I ever enter back into the system of medicine.
About the only opportunity this whole attack has created is one where I get to defend myself on appeal in a debate with three academic white coats of their choosing. Bring. It. On.
Although the outcome of the debate is assuredly pre-determined, I know it will satisfy a deep yearning many of us dissidents have had for going on 3 years now – to debate someone, anyone, anywhere. Crush them with data. Make ‘em look silly although I will be the only one who knows it happened. It will let me vent my disgust at how they have widely disseminated corrupted scientific evidence and policies while simultaneously ignoring the clinical observations and expertise of frontline doctors who have treated thousands of actual Covid patients.
I will then toss in a little lecture about how RCT’s have long ceased to be a credible means of proving anything in science given that in modern medicine only “Big RCT’s” count and that all “Big RCT’s” require such massive funding that the bias of the funders outweighs any objectivity such trials can profess to attain. I will also remind them that throughout modern medical history, the findings of RCT’s and retrospective observational trials are identical, yet academia has been taught to systematically ignore observational trials. Reason: only massively funded entities can conduct a “Big RCT” while any committed clinician willing to give up nights and weekends can conduct an observational trial. Pharma cannot allow research to be conducted that they have no control over – so they took over the journals and medical school curriculums which now literally teach that observational controlled trials can only be considered “hypothesis generating” and thus their results should not be acted on. Nonsense.
I will also remind them that they are violating international law and human, civil, and political rights as argued by Meryl Nass in another of her excellent posts regarding her own persecution by her state licensing Board:
International law is on our side. A total of 172 countries are parties to the International Covenant on Civil and Political Rights:
According to the 1948 Universal Declaration of Human Rights, Article 19,
“Everyone has the right to freedom of opinion and expression; this right includes freedom to hold opinions without interference and to seek, receive and impart information and ideas through any media and regardless of frontiers.”
According to the 1966 International Covenant on Civil and Political Rights,
“Everyone shall have the right to freedom of expression; this right shall include freedom to seek, receive and impart information and ideas of all kinds, regardless of frontiers, either orally, in writing or in print, in the form of art, or through any other media of his choice.”
And the Nebraska Attorney General protected doctors and pharmacists in Nebraska from their Boards, explicitly allowing them to prescribe HCQ and IVM. His opinion is a tour de force, which goes into detail about why the CDC, FDA and NIH guidelines are contradictory, unscientific and should not be followed. It should be cited in every case.
I also plan on reminding them that the FDA got its ass handed to them in court last week during a hearing of Paul Marik, Mary Tally Bowden and Robert Apter’s suit against the FDA. From an Epoch Times article on the hearing:
“FDA explicitly recognizes that doctors do have the authority to prescribe ivermectin to treat COVID,” Ashley Cheung Honold, a Department of Justice lawyer representing the FDA, said during oral arguments on Aug. 8 in the U.S. Court of Appeals for the 5th Circuit.
The statements “don’t prohibit doctors from prescribing ivermectin to treat COVID or for any other purpose” Ms. Honold said.
“FDA is clearly acknowledging that doctors have the authority to prescribe human ivermectin to treat COVID. So they are not interfering with the authority of doctors to prescribe drugs or to practice medicine,” she said.
So, if the FDA recognizes we have the authority to prescribe ivermectin, then assuredly we are allowed to have the opinion that it is a valid therapy. However, the ABIM will not allow an ABIM certified physician to publicly express this opinion or recommend this practice. Maybe the ABIM should have a little chat with the FDA?
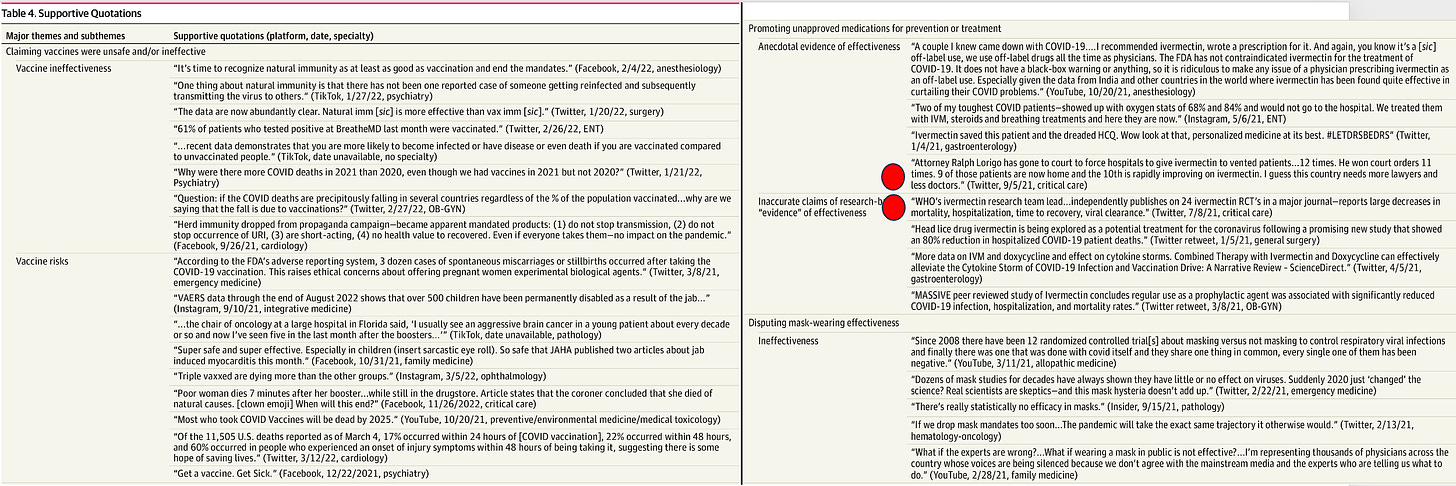
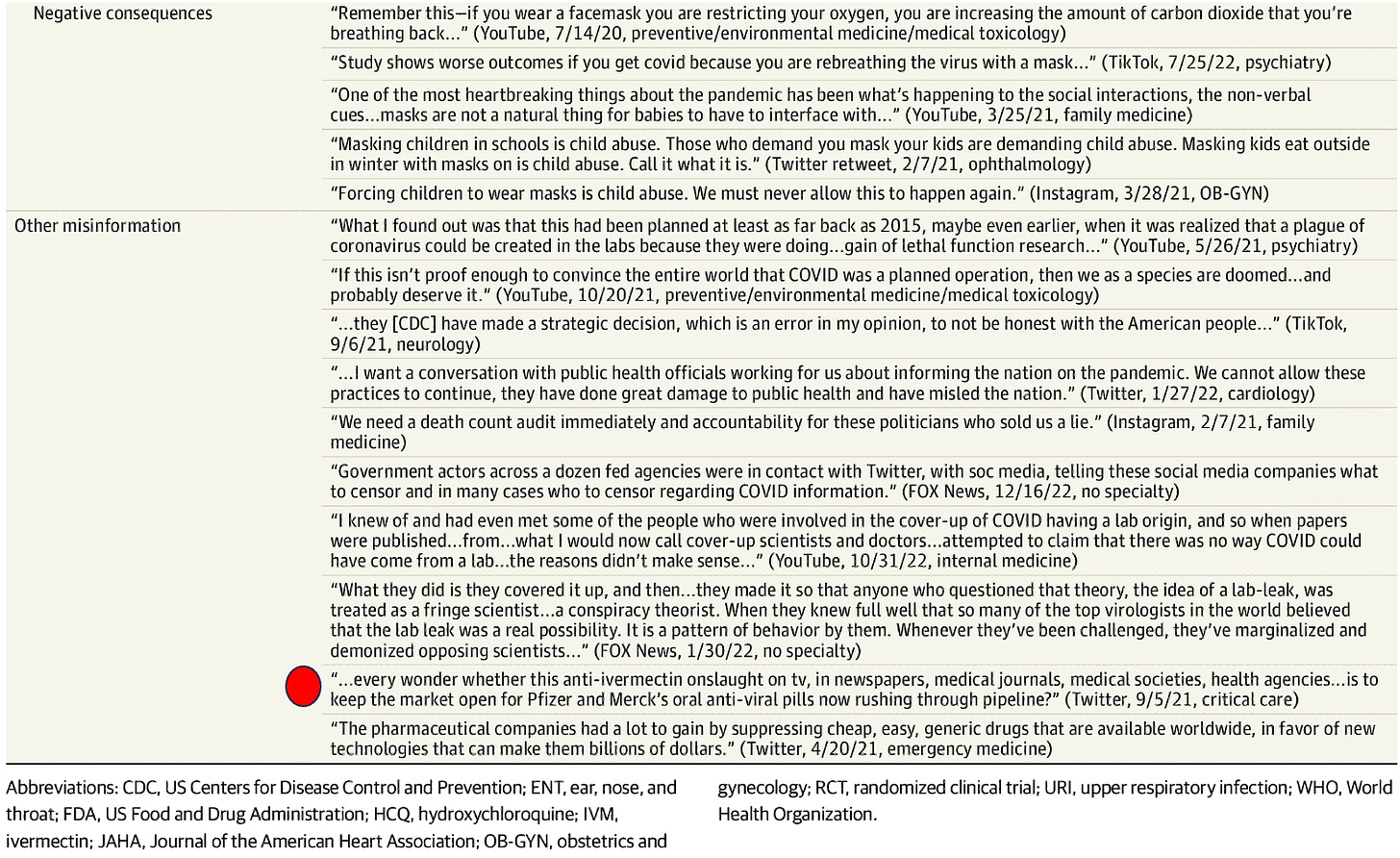
The nonsense doesn’t end with the ABIM, as they are only one prong of this campaign. How is this for some comic relief, published last week in one of the top journals in the world where they found that almost all the Covid misinformation in the U.S on social media can be traced to 52 doctors.

I was honored to discover that yours truly made the list! In their quoted examples of misinformation in Table 4, I have taken the liberty of owning up to the posts attributed to me, all of which I stand by to this day:
I think I will finish with this excerpt from a recent Wall Street Journal op-ed touching on the Missouri vs. Biden case where the administration is being sued for its systematic censoring of U.S citizens on social media by every intelligence and health agency in our Federal government :
This is where the decision of U.S. District Judge Terry Doughty sheds light. His detailed recounting shows a Washington energetic in protecting Americans from Covid opinions, expertise and claims that conflicted with its own, at a time when it served politicians to show they were trying to save Americans from encountering a virus that couldn’t be avoided. When government has a message to deliver, especially when the political stakes are high, it won’t be content just to push its own message, it will try to silence others. Fighting back will always be necessary. The only surprise in our age is how thoroughly the “liberal” position has become the pro-censorship position (that last line is a doozy).
Hurricane Katrina and the “Angels of Mercy”
Ethical boundaries in medical decision-making
By Jonathan Engler and Jessica Hockett | HART | August 21, 2023
The debate as to how much “pandemic” harm was caused not by a virus, but rather by the dystopian response to the perceived threat of a virus, has been raging for some time now.
Jonathan tweeted about this last year in relation to Lombardy and that thread was turned into this Panda article.
An analysis of the spatial characteristics of deaths during the spring 2020 wave in Northern Italy was carried out by him along with a Panda colleague; this suggested that it looked nothing like a spreading virus, and more like the sudden imposition of a policy response.
More recently, Jessica has essentially come to the same conclusions about New York: that something terrifyingly unnatural appears to have happened, which cannot be explained by the sudden spread of a deadly virus.
It surely does not require any scientific understanding whatsoever to glance at the below graph of total mortality rate in NYC going back to 2015 and see that what happened in a few weeks during spring 2020 suggests an abrupt episode of ferocious lethality which was at odds not only with anything observed anywhere at the time or thereafter, but also with even the highest estimates of the infection fatality rate alleged to have caused “the pandemic”.
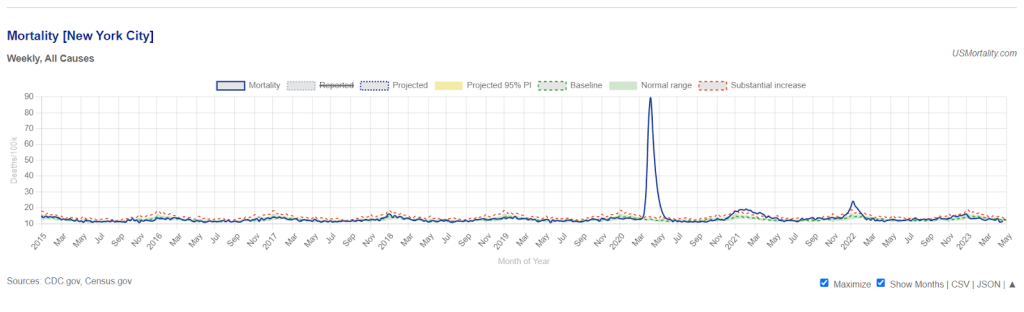
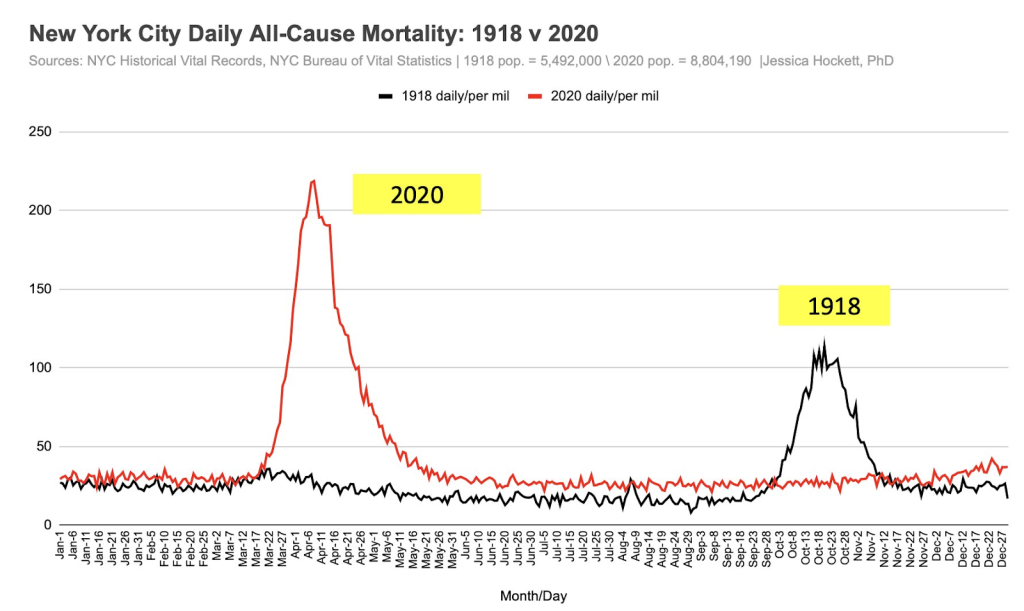
If we look back even further, it can be seen that the reported spring 2020 mortality spike in New York is actually around double that observed in the autumn of the 1918 pandemic. But other places in 2020 did not see waves of deaths anywhere near those observed during the 1918 pandemic.
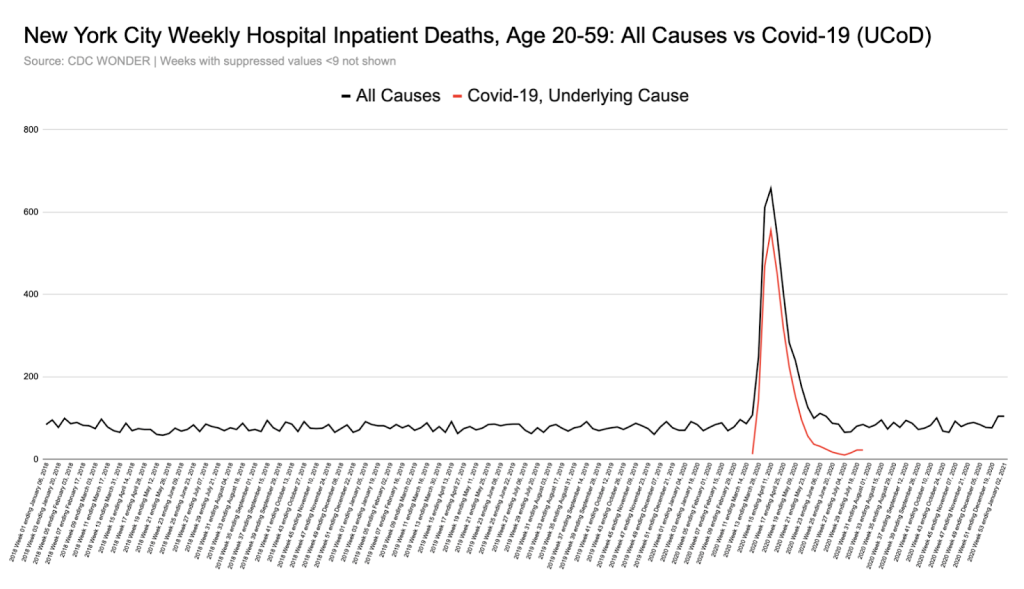
Moreover, unlike elsewhere, the increase in deaths was seen across a younger demographic, not exclusively in the elderly.
As shown in the graph below, all-cause hospital inpatient weekly death counts in the 20-59 age group were dramatically elevated for a short period, by a shocking 6-fold at their peak, with nearly all these deaths being coded as ‘covid’.
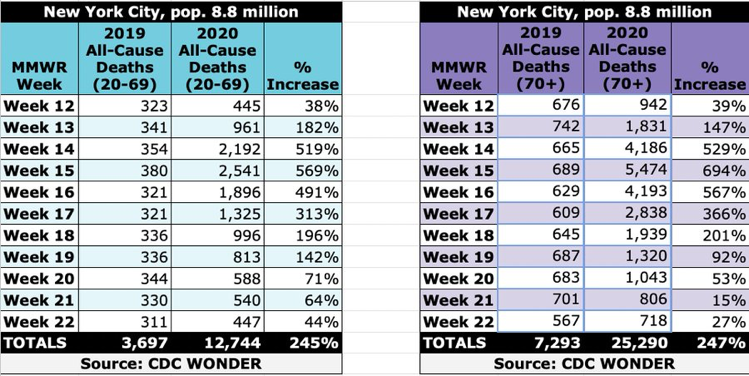
In fact, in New York, the % increase in all-cause deaths during the spring “1st wave” period was the same in the 20-69 year old age group as in the 70s and over:
In other places, however, what we were told was the same disease caused by the same virus left the younger age groups largely untouched, with nearly all deaths being in the elderly.
This discrepancy remains completely unexplained. It seems unarguable that certain difficult questions certainly need asking about what happened in New York in 2020 if we are to unravel the truth about what happened there.
Of course, the narratives emerging from Northern Italy and New York in 2020 were instrumental in driving fear and hysteria worldwide. Moreover, the number of deaths in both places informed early estimates of the IFR. These inciting incidents directly sparked much of the worldwide exaggerated, fear-driven response to what we now know was (if anything) a virus mainly affecting the frail and elderly, to which most people already had sufficient immunity to prevent severe illness.
For these reasons, it is essential that particular attention is paid to try to ascertain precisely what happened in these specific places.
It’s worth detailing – as evidence for the deeply dystopian mindset operating at the time – just some of the many deviations from normality that adversely affected human health and immunity, or which constituted sudden changes to healthcare practice.
These included (but were not limited to):
- Stress and anxiety from confinement (being told to stay home) and fear propaganda
- Discouragement to attend hospitals if ill
- Reduced community prescribing of broad-spectrum antibiotics
- Low staff levels in healthcare settings due to self-isolation of those “testing positive,” even with no symptoms
- Isolating the elderly
- Barring loved ones from hospital and care homes
- Fear (on the part of HCWs) of tending to covid positive patients, compromising basic medical and care needs.
- Early and inappropriate invasive ventilation
- Overuse of midazolam and opiates
Inevitably, and rightly, some researchers have started to perform post-pandemic autopsies analysing the motives and reasoning used to justify policies and other changes in behaviour and to examine their real world consequences.
Some medical practitioners have taken umbrage at any suggestion that the stressful environment and sudden expectations and pressures laid upon them may have resulted in well-meaning medical staff crossing ethical lines, or violating the Hippocratic Oath.
Those who wish to point out that there is historical precedent for medical staff behaving diabolically while thinking they are doing good often invoke atrocities during the 1930s and 1940s (and receive opprobrium as a result).
However, there is a much more recent example, and one which we were oblivious to until recently, despite this incident being totally “out in the open”, the subject of a lengthy investigative article, book, and a TV mini-series: the post Hurricane Katrina incident at Memorial Hospital Center in New Orleans in 2006.
Wikipedia provides the basic facts:
In the hurricane aftermath, the basement of Memorial Hospital Center flooded, power failed, and battery power for essential equipment started to run out. Most, but not all, patients were successfully evacuated.
The hurricane occurred on 29th August. A shocking finding was made in the aftermath, as described in the Wikipedia article:
On September 11, mortuary workers recovered 45 bodies from the hospital. Toxicology tests were performed on 41 bodies, and 23 tested positive for one or both of morphine and the fast-acting sedative midazolam [branded as Versed in the US], although few of these patients had been prescribed morphine for pain.
In the following weeks, it was reported that staff had discussed euthanizing patients. Some reports went further; Bryant King, an internist at Memorial, told CNN that he believed “the discussion of euthanasia was more than talk.”
LifeCare told the state Attorney General’s office that nine of their patients might “have been given lethal doses of medicines by a Memorial doctor and nurses.”
King publicly charged that one or more healthcare workers had killed patients, based on conversations with other health care workers. King told CNN that when he believed a doctor was about to kill patients, he boarded a boat and left the hospital. King explained his actions in terms of his opposition to Pou’s alleged actions, arguing “I’d rather be considered a person who abandoned patients than someone who aided in eliminating patients.”
Following an investigation into the deaths described above, the local DA (“District Attorney”) decided there was sufficient evidence to charge three medical staff with four counts of second-degree murder. Charges against two were later dropped in exchange for testimony.
The prosecution was deeply unpopular. Despite substantial evidence of deliberate actions taken to terminate lives – indeed, enough to satisfy the legal definition for homicide – many members of the public felt medical staff were simply “doing their best” under very trying circumstances. According to a local reporter the incident “ignited a furious debate in New Orleans and elsewhere about whether sharp ethical boundaries can be drawn around decisions on patient comfort made in a crisis.”
The DA failed to win re-election, and when the new DA convened a Grand Jury* at an undisclosed location, much of the previously amassed evidence was not presented and some of the key witnesses not called. The Grand Jury decided that charges should be dropped.
Unsurprisingly, several commentators (e.g., Loyola University Law Professor Dane Ciolono) opined that the Grand Jury was convened and run in such a way as to ensure charges would be dropped while providing “cover” for such an outcome.
Whatever actually occurred at Memorial Hospital, or whatever the staff’s motives, the incident speaks to an unsettling, yet undeniable truth: during a crisis, “ethical red lines” – however deeply held and valued – may be easily crossed. Society may judge those decisions acceptable or understandable, as appears to have happened with the Memorial Hospital case.
In summary, it would appear that the legal process was manipulated to assure an outcome which accorded with public opinion – that is to say to extinguish the possibility of prosecution while maintaining the pretence of due legal process. In this way, facing up to the stark reality – that as a society we mete out justice arbitrarily when we wish to – was avoided. Perhaps the well-ordered rules-based system suggested by statutory definitions of what actions constitute crimes, is to some extent just “for show”.
The Memorial Hospital case obliterates – with a relatively recent example – the notion that doctors and nurses all have the same ethical boundaries which they simply will not cross under any circumstances.
Could such boundaries have been crossed during the recent covid event?
A number of commentators are considering the possibility that changes in the policies and practices around the use of certain drugs (midazolam and opiates), and procedures (invasive ventilation) – sometimes in combination – may have contributed to the high mortality reported, at least in some specific places.
In relation to drugs, in an article published on his Substack last year, the blogger known as Bartram’s Folly explored the possibility that (in the UK) sheer fear and panic may well have driven medical staff to use midazolam and opiates more liberally in patients with covid, which may have encompassed anyone with a positive covid test.
In the UK one such mechanism which may have encouraged this measure is the NICE Guideline NG163 (no longer on their website but available here or as PDF download here), about which others have also written in detail. This guideline effectively transposed the advice for treating end-stage cancer patients with midazolam and opiates into that for covid patients. More detail on this here.
Of the guideline, Bartram said,
“… the NICE guidelines appear to have introduced a pathway for doctors which allowed for (perhaps even encouraged) more than a gentle nudge for those who were ill with Covid towards death, some of whom might well have survived given the chance. This iatrogenesis hypothesis would mean that at least some of the deaths recorded as with Covid might well have been a direct result of the care guidelines as set out by NICE.“
Later, Bartram makes the point that the pretext of a crisis situation or emergency may establish the grounds for ethical boundaries to be crossed or disregarded, at least temporarily, under the auspices of ignorance or ‘doing one’s best’ with the information said to be known or available at the time:
It is important to note that in the iatrogenesis hypothesis it isn’t necessary for some people to have had an evil intent – it is entirely possible that individuals promoted and exercised a policy that resulted in needless deaths while believing that they were ‘doing the right thing’ (e.g., see Hannah Arendt’s concept of the banality of evil).
In particular, ‘petty bureaucrats’ appear to be readily able to think up policies without seeing the need to consider the full consequences, and when these consequences are eventually revealed will usually point to the minutes from endless meetings with other petty bureaucrats to show that they weren’t personally responsible for the policy and they were simply following process.
Of course, once a framework had been decided front-line staff might have been grateful for the guidance offered given the challenging times, at least until the negative consequences of the guidance became painfully clear.
It should also be remembered that – in the US at least – certain extraordinary policy measures may have been important factors. For example, during the emergency NYC Governor Cuomo issued executive orders and suspended laws which gave doctors and nurses immunity and absolved hospitals of the responsibility to keep close patient records. (The order itself can be found here, and some legal commentary on it here.) Articles in JAMA can be interpreted as giving ethical permission for physicians to issue unilateral DNR orders, avoid CPR, and ration ventilators and critical care beds.
Moreover there are numerous examples of doctors, nurses and others in the US who later said they were following guidance, learning as they went. (See this interesting essay by Dr Kory, for example.) Under these circumstances it is easy to see how they could assume that something which ordinarily might have been questionable would become acceptable as “everyone else was doing it”.
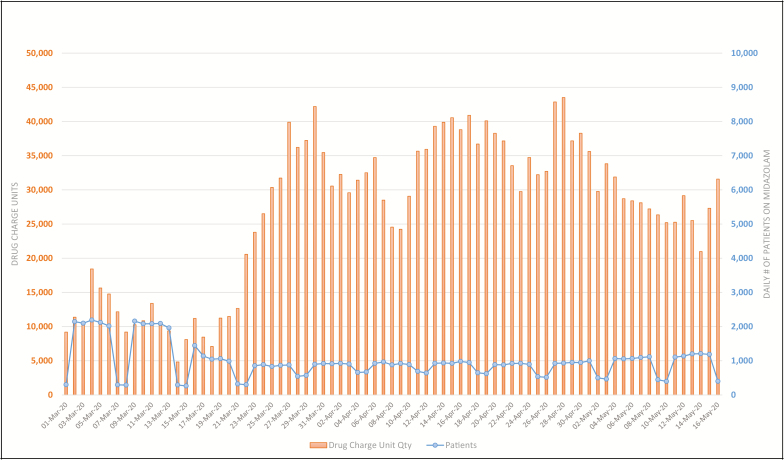
Evidence of increased midazolam use can be seen in the US as well as in the UK. This graph from a study describing the use of 7 specific drugs in 47 hospitals in NY shows the daily count of patients (blue) who received midazolam and the disproportionate quantities used (orange) between March 1 and May 16, 2020.
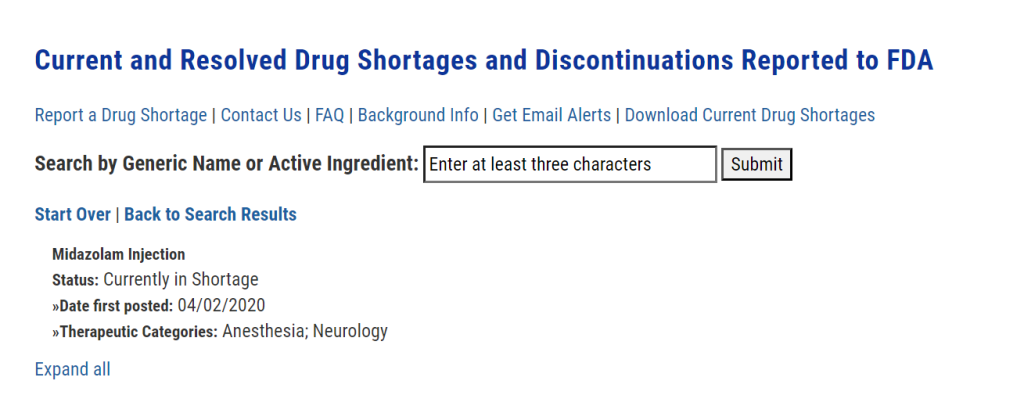
Moreover, midazolam is currently listed by the FDA to have been in short supply since 2 April 2020:
This Guardian article from 13 April 2020 reports on a letter sent by “a group of prominent medical practitioners and experts” to capital punishment states imploring them to:
“release their stocks of essential sedatives and paralytics that they hoard for executions” so that they can be “used for intubations and mechanical ventilation of the most severely ill coronavirus patients who cannot breathe for themselves”.
The tone of this letter can be taken to illustrate the sense of sheer panic prevailing at the time – certainly not conducive to rational decision-making – combined with the assumption that invasive ventilation was going to be extensively required and used.
This takes us to the question of invasive ventilation, whether it might have been used too often, inappropriately, and why.
As well as panic, the role of fear on the part of healthcare workers cannot be underestimated. Here is Dr Vinay Prasad stating that:
“It is a unique situation in medicine. In our whole medical career, doctors have never been personally afraid the way they were [with covid].”
Official guidance (see for example this from a British anaesthetists’ professional association) certainly reinforced the idea that one of the benefits of early intubation was to reduce the aerosolization of virus, such that it would be safer for those caring for the patients, compared to when non-invasive forms of ventilation were used.
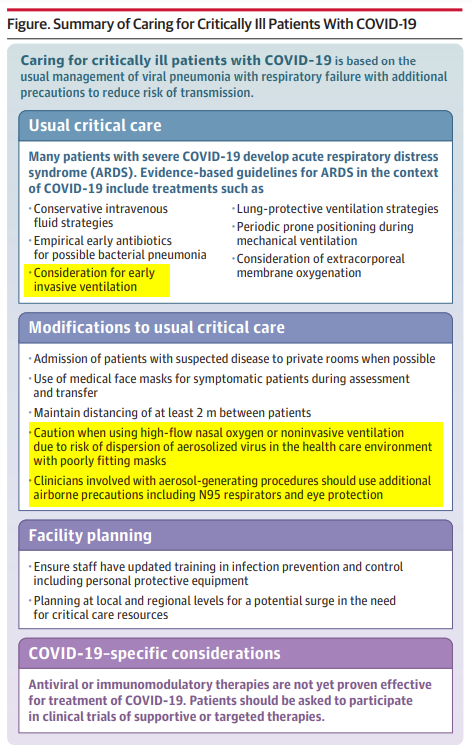
This JAMA Clinical Update “Care for Critically Ill Patients With COVID-19” published on 11 March 2020 strongly supports the idea that the thinking was very much that non-invasive oxygen augmentation could be dangerous for healthcare workers:
The journalist Alex Berenson was early to point out that ventilator shortage may have more to do with overuse “to protect staff” than to being overwhelmed by patients in respiratory failure.
It seems like fear may well have been augmented by official guidance to result in significant overuse of this measure.
It is important to understand the differences between the Memorial Hospital incident and what may have happened in the early stages of the covid crisis. In New Orleans, it may indeed have been reasonable to assume that it was going to be impossible to evacuate the patients (who were given midazolam and opiates to ease suffering) in time, and that they were indeed unsaveable due to the extraordinary circumstances. (Whether or not this was actually the case will probably never be known, because of the legal shenanigans described above.)
However, whether that applies to all, some, or just a few of those who died in spring 2020 after being administered the same or other drugs (or placed on mechanical ventilators or issued a unilateral DNR, etc.) is still a matter of debate whereas for sure, Hurricane Katrina was self-evidently an extreme weather event that created devastation and emergency conditions in its fury and wake.
Certainly, it seems clear that personal fear and a belief in the lethality of this infection drove much medical decision-making in the early days. It is not hard to imagine actions being taken which were then rationalised by imagining the suffering that had been prevented, limited resources preserved, and many lives saved. The deaths witnessed could easily have acted as positive reinforcement in the minds of healthcare workers as to how serious the illness was. These protocols could lead to the deaths of patients who were not particularly old and frail and thus reinforce the message that the virus was potentially fatal even in such people
The decisions that healthcare workers made, and the influences on and factors involved in those decisions, will be discussed and dissected for decades to come. When humanity is ready to confront what occurred – and admit that ethical inversions in hospitals and care homes contributed to unintentional iatrogenic death, we can move toward keeping it from happening again.
* (A Grand Jury in the US is a specific type of court empowered by law to determine whether probable cause exists to support criminal charges for a suspect in a crime. Louisiana – in which New Orleans is situated – is one of 23 US states that use grand juries for indictments in serious crimes.)
Battle for Climate Earth
ClimateCraze | July 5, 2021
There is no climate crisis — just climate alarmism.

Greg Tucker-Kellogg publishes fraudulent study to attack ivermectin
Tucker-Kellogg aimed to review research conducted in Brazil and conclude that ivermectin was ineffective against Covid-19. In order to do so, he and his colleagues had to fabricate over 250 fatalities.
Illustration. Reproduction photo from Greg’s YouTube channel.
Médicos Pela Vida | August 17, 2023
Greg Tucker-Kellogg, from the Department of Biological Sciences at the National University of Singapore, who receives compensation from YouTube for creating content against scientific misinformation, along with two other authors, Ana Carolina Peçanha and Robin Mills, published a study on the Medrxiv platform on August 15th. The study used fraudulent data with the aim of undermining the research on ivermectin conducted in Itajaí, located on the coast of Santa Catarina, Brazil.
The study conducted in Itajaí, peer-reviewed and published in the prestigious Cureus journal in early 2022, concluded the effectiveness of ivermectin in its prophylactic use against COVID-19. The results were positive: among individuals who took ivermectin preventively, there were 68% fewer deaths, 56% fewer hospitalizations, and 44% fewer infections.
The False Data
Tucker-Kellogg and colleagues’ study, which aimed to recalculate and nullify the positive results, used fraudulent data to achieve its goal. In the article, they claim that the data is official.
The authors stated that 499 individuals died between July and December 2020, a period during which the effectiveness of ivermectin was studied in the city.
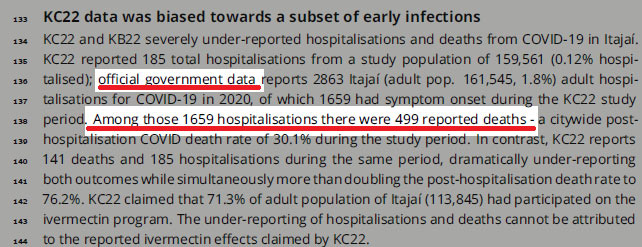
However, the data of 499 COVID-19 deaths during the six months of the study in Itajaí is indeed false. In order to achieve their desired outcome, the number of deaths had to be inflated. You can verify the original PDF of the reanalysis here on page 3.
How We Investigated
The purported 499 deaths in six months, used as a basis for the calculations, raised suspicions due to being an unusually high number for the period in a city with just over 200,000 inhabitants. Consequently, the first step we took was to research the city’s epidemiological bulletins during that timeframe.
The official epidemiological bulletin, published on the Itajaí city government’s website on December 28, 2020, stated that a total of 254 individuals had died since the beginning of the pandemic. This figure represents deaths from when the virus first spread in the city in early 2020. Therefore, the deaths between July and December were even fewer, far from the reported 499.
In a second attempt to verify the numbers, we accessed consolidated data from the Brazilian Unified Health System (Sistema Único de Saúde or SUS) through the OpendataSUS database, which is considered one of the most comprehensive and accurate in the world. As Brazil has a publicly funded healthcare system, data for all patients in the country is rigorously monitored.
The OpenDataSUS Numbers:
Deaths caused by Severe Acute Respiratory Syndrome (SARS), with dates ranging from July to December 2020, among residents of the city. Database downloaded on March 13, 2023.
Based on the date of hospitalization:
Total SARS-related deaths: 234
Deaths due to Covid-19 only: 222
Based on the date of symptom onset:
Total SARS-related deaths: 256
Deaths due to Covid-19 only: 237
Based on the date of data entry:
Total SARS-related deaths: 240
Deaths due to Covid-19 only: 222
The Numbers from Brasil.IO
According to the information from the Brasil.IO database, which compiles data from confirmed cases and deaths from the bulletins of the State Health Departments (Secretarias Estaduais de Saúde or SES), during the period of the Itajaí study, the data were as follows:
Total Covid-19 deaths: 227
Fraudulent Study Used for Attacks
The authors of the original study have a long history in science and impeccable reputations. Lucy Kerr, the lead author, is the daughter of the late Warwick Stevam Kerr, and she deeply values his legacy. Warwick was the Scientific Director of FAPESP, served as the president of the Brazilian Society for the Advancement of Science, and received the Order of Scientific Merit in the Grand Cross category. Other authors include Dr. Flavio Cadegiani, a researcher with several COVID-19 studies, Dr. Fernando Baldi, a professor at the São Paulo State University (UNESP), Dr. Pierre Kory, an American medical professor, and Dr. Jennifer A. Hibberd from the University of Toronto, among others.
Following the publication of the reanalysis with fraudulent data, the attacks on the authors’ reputations turned defamatory. “There are people who prefer to keep believing in charlatans,” said Chloé Pinheiro, a journalist from Veja, one of Brazil’s major magazines.
Leandro Tessler, a professor at Unicamp, who represents the respected university in classifying true or false news on the internet and has admitted to not reading studies on cheap, generic, and unpatented treatments that he criticized, claimed that the original positive study had “cooked data.” Furthermore, Leandro criticized the journal’s quality by saying, “It’s something for Cureus.”
“Statistical trickery,” said Julio Ponce, a doctor in epidemiology and host of the podcast “Escuta a Ciência,” in response to the positive results of the original study.
Isaac Schrarstzhaupt, coordinator of the Rede Análise, criticized the quality of the Cureus journal. He stated that the original publication falls among the “lesser journals,” and he phrased it this way “to avoid using other terms.“
Original Authors Always Prioritized Transparency
The authors of the original study on ivermectin in Itajaí, responding to a call from the BMJ – British Medical Journal, which requested the publication of public data from studies on medications and vaccines, decided to make their raw data available for reanalysis.
This action was highly praised. “It’s excellent that they have released their data anonymously. They have true confidence in the results of their analyses. This is how good science is carried out,” stated Dr. Harvey Risch, a professor of epidemiology at Yale University, USA, emphasizing that patients’ personal data had been preserved.
Previously, the scientific community had speculated that the authors would not make their data available.
The doctor has been attacking the authors for some time
Ana Carolina, one of the authors of the study, has been attacking Dr. Flavio Cadegiani for some time. He is also the author of other studies involving different medications against Covid-19, such as those involving proxalutamide. She claims that those researches are a “hoax.” Regarding the study she chose to reanalyze now, inserting fraudulent data, Ana Carolina had already committed in early 2022 to disqualify it. She referred to it as an “international embarrassment” at the time and used quotation marks to refer to the researchers, seemingly implying doubt about their work.
“They had already decided that ivermectin doesn’t work. So, they tried – and made a great effort – to find calculations that ‘fit’ their pre-established conclusion. This is the exact opposite of what science is, which involves accepting results whether they contradict or support the hypothesis. In their quest to find the desired data, they most likely forgot to look at their own analyses – and even worse, at basic numbers. Furthermore, it seems to me that they didn’t quite understand the study, as I couldn’t find analyses related to rates derived from infections, matched with Propensity Score Matching,” stated Dr. Flavio Cadegiani, one of the authors of the Itajaí study.
“The most important thing is that this ‘study,’ by demonstrating its inability to invalidate us, has only reinforced our findings, and for that, we cannot help but be grateful,” he added.
MPV Comment
Scientific fraud is presenting unverified data as if it were official. And this wasn’t a small error. It was the central data point used to generate the result. It’s not a minor mistake that wouldn’t affect the studied outcomes. In order for the authors to attack the study and arrive at the conclusion of inefficacy, they needed to increase the number of deaths.
All those who subsequently attacked, even labeling the authors as “charlatans,” supposedly had the capacity and training to spot the fraudulent numbers. They are doctors, professors, epidemiologists, and data scientists. They either didn’t see it or feigned ignorance.
So far, all the scientific frauds published during the pandemic have targeted inexpensive, generic, and unpatented medications, or they were frauds promoting expensive and patented drugs. Surely, this is just a coincidence.
This is the second time the Itajaí study has been attacked without valid scientific arguments. In June 2022, the USP – University of São Paulo journal attacked it, even spreading false information. Our analysis can be read here: “COVID-19: USP Journal Lies and Distorts Science to Attack Ivermectin. Read the full analysis.” (portuguese).
We, at MPV (Médicos pela Vida) – Doctors for Life, are grateful for the collaboration of Professor Daniel Tausk from USP, for compiling data from official databases. His collaboration was essential for the report. Additionally, we thank the French researcher Massimaux, who prefers to remain anonymous on Twitter, for quickly pointing out fraudulent data. According to him, it was a “sanity check.” It didn’t pass.
Sources
Data from OpendataSUS
Data from Brasil.IO
Epidemiological Bulletin of Itajaí
Featured Video
Prof. Ted Postol: Iran Already Achieved Nuclear Deterrence Against Israel
or go to
Aletho News Archives – Video-Images
From the Archives
How the occupied mentality syndrome works
Saudi Arabia on the American chessboard – Part 3
By B. J. Sabri | American Herald Tribune | June 27, 2016
Read part 2: “The occupied mentality Syndrome“
Previously I argued whether Saudi Arabia’s repeated involvements in U.S. interventions and wars stem from free national will or in response to a specific condition. For starters, in Saudi Arabia there is no national will. In Saudi Arabia, the national will is the will of the Al Saud clan. Still, when a major Arab state allies itself with a superpower that committed unspeakable crimes against humanity in almost every Arab country, then something is wrong. This fact alone should compel us to examine the U.S.-Saudi relation for one exceptional reason. As a result of the U.S.-Saudi wars, hundreds of thousands of people in Afghanistan, Iraq, Iran, Libya, Syria, Yemen, and Somalia have lost their lives. Millions became displaced in their own homelands. And millions more rendered refugees.
Attributing the Saudi policies to the bonds of “partnership” with the U.S. is frivolous. There are no bonds between these two thugs except those of business, military deals, secret plots, and wars. Proving this point, bonds such as these have no space for the American and Saudi peoples to share significant cultural or societal exchanges. If partnership is not the reason for the Saudi contribution to the U.S. strategy of empire and imperialism, then another reason must exist.
This leads to three possibilities. … continue
Blog Roll
 Aletho News
Aletho News- NIAID/NIH and USDA Fund Bioengineered Chimeric Influenza Viruses Built Using Pandemic H1N1 Components: Journal ‘Science Advances’
- Hezbollah hits Israeli warship off Lebanon’s coast, sets it aflame
- Iran slams US strikes on B1 bridge, Mahshahr petrochemical plants as ‘blatant acts of state terrorism’
- In letter to UN chief, Araghchi warns of dire consequences of US-Israeli attacks on Iran’s nuclear facilities
- Why the CIA conspiracy to invade Iran with Kurdish militias failed
- Why Are Upbeat US Claims About Mission to Rescue Pilot ‘Highly Questionable’?
- Aircraft destroyed during US ‘rescue’ of downed F-15 pilot cost more than $100 million each
- Washington University removes professor who condemned US-Israeli war on Iran
- Russia Warns of Retaliation as UK Authorizes Seizure of Vessels
- Serbia thwarts plot to bomb Russia-Hungary gas pipeline – Vucic
- If Americans Knew
- In Iran, Israel-US take aim at “reason, research, and freedom of thought” – Daily Update
- US loses planes over Iran, Israel downgrades Lebanon war goals – Daily Update
- Israel Is Blocking Palestinians from Easter at Church Where Jesus Resurrected
- Plot to assassinate Palestinian activist follows harassment campaign promoted by Zionist groups and elected officials
- Prominent New York synagogue hosts presentation on why U.S. Jews should support the ethnic cleansing of Gaza
- Tapper vs. Piker: Is the CNN Anchor Auditioning for David Ellison?
- Shouldn’t Democrats Be Able to Condemn Genocide?
- Israel-US kill negotiators, destroy civilian structures, but Iran’s military capabilities still largely intact – Daily Update
- ‘War crime’: Global condemnation as Israeli ministers celebrate death penalty law targeting Palestinian prisoners
- 7 Ways Israel Is Turning Lebanon Into Gaza
- No Tricks Zone
- An Inconvenient Tree: Uncovered In Alps… Europe Much Warmer Than Today 6000 Years Ago
- New Study Reports A 60% Slowdown In Greenland’s Ice Loss Rate In The Last Decade
- Low Intensity Tornado Wrecks Major Solar Farm, Creating A Potential Toxic Dump
- New Study Finds Warming Saves Lives…Cold Temperatures 12 Times More Deadly Than Excess Heat
- German Science Blog Accuses PIK Climate Institute Of Hallucinating Climate Tipping Points
- Devastating Assessment Of Comirnaty Vaccine By Former Senior Pfizer Europe Toxicologist
- New Study: CO2 Is ‘Effectively Negligible’ As An Explanatory Climate Change Factor Since 2000
- Former Pfizer Toxicologist Dr. Helmut Sterz Tells Bundestag Hearing Pfizer Vaccine Should Have Never Been Approved
- Energy Expert: Germany’s Nuclear Phaseout Was A “500 Billion Euro Mistake”
- New Research: South Australia’s Mid-Holocene Sea Surface Temperatures Were 4°C Warmer Than Today
