‘Fox guarding the henhouse’: AMA, Vaccine Integrity Project to conduct their own vaccine safety and efficacy reviews
By Suzanne Burdick, Ph.D. | The Defender | February 11, 2026
The American Medical Association (AMA) is teaming up with the Vaccine Integrity Project to conduct its own review of vaccine safety and efficacy, claiming that advisers to the Centers for Disease Control and Prevention (CDC) are no longer doing a good enough job.
The groups said Wednesday in a press release that “for decades,” the CDC’s Advisory Committee on Immunization Practices (ACIP) had “served as the engine of evidence-based vaccine policy” for the U.S. “That system has now effectively collapsed.”
U.S. Department of Health and Human Services (HHS) Press Secretary Emily G. Hilliard told The Defender the claim that ACIP’s evidence-based process has collapsed is “categorically false.” She said:
“ACIP continues to remain the nation’s advisory body for vaccine use recommendations driven by gold standard science. While outside organizations continue to conduct their own analyses and confuse the American people, those efforts do not replace or supersede the federal process that continues to guide vaccine policy in the United States.”
The Vaccine Integrity Project, based at the University of Minnesota’s Center for Infectious Disease Research and Policy (CIDRAP), says it is dedicated to “safeguarding vaccine use in the U.S.”
The AMA will work with the project to review vaccines for the 2026-2027 respiratory virus season. These include immunizations against COVID-19, influenza and respiratory syncytial virus (RSV), according to the press release.
CIDRAP Director Michael Osterholm said in a statement that the goal is “to restore peace of mind for clinicians and patients by ensuring that experts are continuously evaluating vaccine safety and effectiveness using transparent, evidence-based methods.”
Children’s Health Defense (CHD) General Counsel Kim Mack Rosenberg said it’s unlikely that the groups will restore people’s peace of mind about vaccines. She said:
“Unfortunately, the AMA and the Vaccine Integrity Project support a narrative about vaccines that is being exposed more and more as problematic and contradicted by what people are seeing with their own eyes.
“The system is broken and efforts to prop it up from the inside are being exposed for conflicts of interest and flawed analyses.”
The groups’ review process looks similar to how the ACIP traditionally worked, but they won’t issue recommendations. Instead, they will share their review results with medical societies, which can write recommendations for their patient demographic.
The AMA and the Vaccine Integrity Project said they will also involve medical societies and public health and healthcare organizations to craft policy questions.
Review members will disclose “relevant” conflicts of interest, according to the press release. However, “relevant” was left undefined.
The AMA and Vaccine Integrity Project said in a statement:
“The goal of this work is to ensure a deliberative, evidence-driven approach to produce the data necessary to understand the risks and benefits of vaccine policy decisions for all populations — the approach traditionally used by the federal government.”
The effort may generate more confusion among Americans who are torn between looking to the federal government or medical societies for vaccine guidance, according to Trial Site News.
“The country is no longer operating with a single, uncontested center of vaccine-policy gravity,” Trial Site News wrote.
‘Like asking the fox to guard the henhouse’
The Vaccine Integrity Project, launched in April 2025, is funded by an unrestricted gift from iAlumbra, a nonprofit founded by Walmart heiress and philanthropist Christy Walton.
The Robert Wood Johnson Foundation, The Greenwall Foundation and Lasker Foundation are also listed among the project’s funders.
The Vaccine Integrity Project declined The Defender’s request for a list of donation amounts and names of any individual donors.
Former CDC Director Rochelle Walensky serves as the Vaccine Integrity Project’s adviser of medical affairs. In 2022, Walensky admitted the CDC gave false information about COVID-19 vaccine safety monitoring.
Already, the Vaccine Integrity Project released a review of the hepatitis B vaccine that supported vaccinating all newborns at birth, rather than delaying when the mother has tested negative for hepatitis B. The project is currently reviewing the human papillomavirus (HPV) vaccine.
“Trusting the AMA and the Vaccine Integrity Project to objectively review vaccine safety feels a lot like asking the fox to guard the henhouse,” said Nebraska chiropractor Ben Tapper.
Mack Rosenberg said the repeated failures of such organizations to “truly and comprehensively” analyze vaccine safety data have led to “increasing distrust among the public — and with good reason.”
AMA ‘a political force,’ not a ‘neutral medical association’
In 2025, the AMA spent nearly $24 million on lobbying, making it one of the top 10 groups trying to influence government policy, according to OpenSecrets.
“This is not the behavior of a neutral medical association. It is the strategy of a political force,” wrote Jason Altmire in an op-ed for RealClearHealth.
Altmire, a former hospital and health insurance executive who served in the U.S. House of Representatives, is an adjunct professor of healthcare management at the Texas Tech University Health Sciences Center.
Tapper questioned whether the AMA and the Vaccine Integrity Project would sufficiently assess the safety of vaccines.
For many people, the concern isn’t that vaccines can have benefits, he said. “The concern is whether safety data is fully transparent, whether adverse event reporting is thoroughly investigated, whether conflicts of interest are disclosed and whether risk-benefit analyses are stratified appropriately by age and health status.”
The AMA, which touted 2024 revenues of $546 million, was criticized during the COVID-19 pandemic for deferring to political ideology rather than medical facts.
Its “AMA COVID-19 Guide: Background/Messaging on Vaccines, Vaccine Clinical Trials & Combatting Vaccine Misinformation” encouraged doctors to use certain words and avoid others. For instance, “stay-at-home order” replaced “lockdown,” and “deaths” replaced “hospitalization rates.”
The AMA in August 2025 was disinvited from the CDC’s vaccine advisory committee’s workgroups.
This article was originally published by The Defender — Children’s Health Defense’s News & Views Website under Creative Commons license CC BY-NC-ND 4.0. Please consider subscribing to The Defender or donating to Children’s Health Defense.
AAP, AMA Booted From CDC Vaccine Advisory Working Groups
By Brenda Baletti, Ph.D. | The Defender | August 8, 2025
The American Academy of Pediatrics (AAP), the American Medical Association (AMA) and six other major medical associations will no longer participate in advising the Centers for Disease Control and Prevention (CDC) on vaccine policy, Bloomberg reported.
The associations said they were informed via email last week that their vaccine experts were being disinvited from the workgroups that report to the CDC’s vaccine advisory committee.
The Advisory Committee on Immunization Practices (ACIP) decides which vaccines should be recommended to the public, who should take them and how often. Its recommendations help determine which vaccines will be covered by the CDC’s Vaccines for Children Program and insurers, and will be mandated by states for daycare and school attendance.
The medical association members will no longer be invited to participate in the working groups that review data and form policy recommendations. However, they will be able to participate in the open public meetings, like the rest of the public.
They are being eliminated because they are “special interest groups and therefore are expected to have a ‘bias’ based on their constituency and/or population that they represent,” according to one U.S. Department of Health and Human Services (HHS) email reported by The Associated Press.
HHS spokesperson Andrew Nixon confirmed the decision in an email. He said:
“Under the old ACIP, outside pressure to align with vaccine orthodoxy limited asking the hard questions. The old ACIP members were plagued by conflicts of interest, influence, and bias. We are fulfilling our promise to the American people to never again allow those conflicts to taint vaccine recommendations.
“Experts will continue to be included based on relevant experience and expertise, not because of what organization they are with.”
Groups call decision ‘irresponsible, dangerous’ to public health
The organizations responded in a joint statement, claiming the decision is “irresponsible, dangerous to our nation’s health, and will further undermine public and clinician trust in vaccines.” They called on the Trump administration to reconsider the decision.
“We are deeply disappointed and alarmed that our organizations are being characterized as ‘biased’ and therefore barred from reviewing scientific data and informing the development of vaccine recommendations that have long helped ensure our nation’s vaccine program is safe, effective, and free from bias,” they wrote.
In addition to the AAP and the AMA, the statement was signed by the American Academy of Family Physicians, American College of Physicians, American Geriatrics Society, American Osteopathic Association, Infectious Diseases Society of America and the National Medical Association.
The decision was the latest attempt by U.S. Health Secretary Robert F. Kennedy Jr. to address the problem of industry influence over ACIP.
In June, Kennedy announced that HHS was retiring all 17 members of ACIP to eliminate conflicts of interest. At the time, most members had financial ties to pharmaceutical companies marketing vaccines, or had worked with public health agencies to promote controversial vaccines, including the COVID-19, RSV and HPV shots.
Two days later, Kennedy named eight researchers and physicians to replace approximately half of the members. One nominee declined to participate.
At the first meeting of the new ACIP committee, the members voted to stop recommending flu shots that contain thimerosal, a mercury-based preservative linked to neurodevelopmental disorders. The AAP, which criticized the decision, maintains that thimerosal is “safe.”
The committee also voted to recommend Merck’s new RSV monoclonal antibody shot for newborns.
Every group kicked out of ACIP takes corporate money from Big Pharma
In July, several of the medical associations removed last week from the ACIP working groups sued Kennedy and other public health officials and agencies over the changes to COVID-19 vaccine recommendations for children and pregnant women.
The groups’ lead lawyer, Richard Henry Hughes IV, was vice president of public policy at Moderna from 2020-2022, when the vaccine maker developed and marketed the Spikevax COVID-19 vaccine, which has netted the company billions of dollars over the last four years. He also previously worked for Merck.
Last month, the AAP also called for an end to religious and philosophical vaccine exemptions for children attending daycare and school in the U.S.
In an updated policy statement published in Pediatrics, the AAP said universal immunization is necessary to keep children and employees safe. The organization said there is a place for “legitimate” medical exemptions, but nonmedical exemptions — part of the fundamental constitutional right to freedom of religion — are “problematic.”
In addition to working with lobbyists like Hughes, every organization expelled from the ACIP working group is funded by the pharmaceutical industry.
The AAP, the major professional organization representing 67,000 pediatricians in the U.S., has overseen the rising rates of chronic illness and medication of American children over recent decades. It is also a lobbying organization that, over the previous six years, has spent between $748,000 and $1,180,000 annually advocating for its members, according to the government website Open Secrets.
The organization’s funding for that work comes, in part, from annual contributions from corporate sponsors, including vaccine manufacturers Moderna, Merck, Sanofi, Abbott Laboratories, GSK and CSL Seqirus.
The AMA is also funded in part by corporate sponsorships. In the past, it came under fire for taking more than $600,000 from pharmaceutical companies to finance a $1 million campaign to promote ethical guidelines discouraging doctors from accepting expensive gifts from drug companies, The Lancet reported.
AMA funding also comes from the AMA Foundation, which is funded by “Roundtable members” from the pharmaceutical industry. Its largest donor is PhRMA, the primary lobbying organization for the industry — which spent a record $12.88 million lobbying for the industry in the first quarter of 2025.
Other AMA sponsors include Agmen, Bristol-Myers Squibb, Eli Lilly, Genentech, GSK, Merck, Novartis, Pfizer, Sanofi and others.
The National Medical Association takes funding from Eli Lilly, Gilead, Regeneron, Pfizer, Merck, Amgen, Novo Nordisk, Vertex, AstraZeneca and others.
The Infectious Diseases Society of America partners with Abbvie, AstraZeneca, Gilead, GSK, Merck, Moderna, Pfizer, Sanofi and others.
A similar list of Big Pharma companies funds the American Academy of Family Physicians, which also partners with Amazon Pharmacy.
Pharma giants, including Pfizer and Johnson & Johnson, are on the long list of the American College of Physicians’ corporate sponsors, along with Big Food giants Tyson Foods and PepsiCo.
The American Geriatrics Society’s financial disclosure statement shows that it has various corporate sponsors, including Merck and Pfizer.
The American Osteopathic Association also has several corporate sponsors, including Pfizer, Astellas, Merck and Sanofi.
New ACIP committee member Retsef Levi, Ph.D., in a post on X, said that instead of these industry-sponsored organizations, the working groups plan to engage experts from a broader set of disciplines.
The working group participation will now “be based on merit & expertise,” he wrote, “not membership in organizations proven to have COIs [conflicts-of-interest] and radical & narrow view of public health!”
Related articles in The Defender
- Breaking: RFK Jr. Removes All Members of CDC Vaccine Advisory Committee
- RFK Jr. Taps 8 New ACIP Members, Offit Concedes Most ‘Seem Reasonable’
- RFK Jr. Hit With Lawsuit Over Changes to COVID Vaccine Policies for Kids, Pregnant Women
- Lawyer Leading Lawsuit Against RFK Jr. Over COVID Vaccines Used to Work for Moderna
- American Academy of Pediatrics Wants to Shut Down Religious Vaccine Exemptions
This article was originally published by The Defender — Children’s Health Defense’s News & Views Website under Creative Commons license CC BY-NC-ND 4.0. Please consider subscribing to The Defender or donating to Children’s Health Defense.
20 State AGs Put Top U.S. Pediatric Group On Notice for “Abusive” and “Experimental” Trans Therapy Guidance
By Jefferey Jaxen | September 26, 2024
“It is abusive to treat a child with biologically altering drugs that have an unknown physiological trajectory and end point. It is also inhumane to endorse such experimentation without a confident safety profile, especially if more times than not, it proves to be medically unnecessary.”
This statement unpins the tone of the legal notice signed by 20 state Attorneys General to the American Academy of Pediatrics (AAP) asking the group to answer to possible violations of state consumer protection statutes over its questionable standards on gender dysphoria care for minors.
“… the AAP continues to authoritatively declare that puberty blockers are ‘reversible,’” the letter continued. “That claim is scientifically unsupported and contradicts what is medically known. And because that claim raises questions under most state consumer protection laws, it has the undersigned alarmed,” the letter goes on to state.
Idaho AG and co-signer of the action letter Raúl Labrador stated, “It is shameful the most basic tenet of medicine – do no harm – has been abandoned by professional associations when politically pressured,” said Attorney General Labrador. “These organizations are sacrificing the health and well-being of children with medically unproven treatments that leave a wake of permanent damage.”
Why are these AGs acting now? The momentum has gained breakaway speed regarding the science of gender affirming care for minors.

Puberty blockers are not fully reversible and come with serious long-term consequences. According to the Cass Report commissioned by NHS England, using puberty blockers are used to suppress hormones during or before puberty can interfere with neurocognitive development, compromise bone density and may negatively affect metabolic health and weight.
And when puberty blocker use is followed directly by cross-sex hormone use, which is often the case, infertility and sterility is a known consequence.
The controversial world of gender care isn’t the only space that the AAP has dove into without an abundance of caution. The group made headlines in 2023 by radically altering their front line weight loss recommendations children ages 12 and up to include a new class of risky drugs and weight-loss surgery.

The AAP’s murky ‘science’ recommendations reached an early level of appalling shame in 2019 when, during a public hearing in 2019 to discuss an act before it was signed into law, pediatrician Dr. Helene Felman, representing Washington D.C.’s chapter of the American Academy of Pediatrics (AAP), stated:
“As a pediatrician, I like the legislation as it stands because it offers the opportunity to capture those young adults who can make informed decisions at technically any age.”
11 was ultimately decided upon until a federal court for the District of Columbia granted a preliminary injunction in a case funded by The Informed Consent Action Network.
The American Medical Association (AMA) had also thrown its full weight behind attempting to remove the parents from medical decisions involving their children.
Looking at where their energy has gone in key moments, one thing appears clear, the AAP wants children isolated from their parents and given over to the medical system for pharmaceutical interventions with known risk profiles. Why?
The AMA Said Trust Your Doctor on Smoking
By Kevin Homer | Brownstone Institute | February 10, 2023
The American Medical Association (AMA) urges physicians to promote COVID-19 vaccines and bivalent boosters. The AMA even supplies members with social media talking points and strategies to deal with vaccine detractors. It is not the first time that my profession has endorsed a product that may be hazardous to your health.
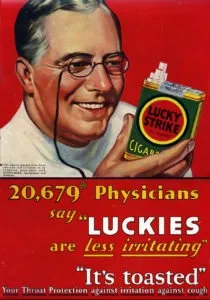
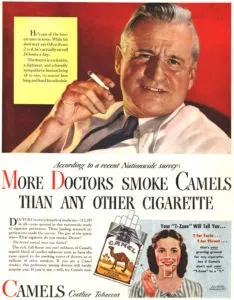
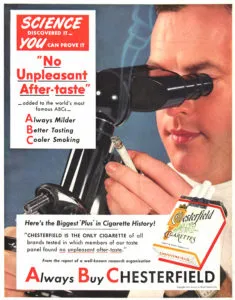
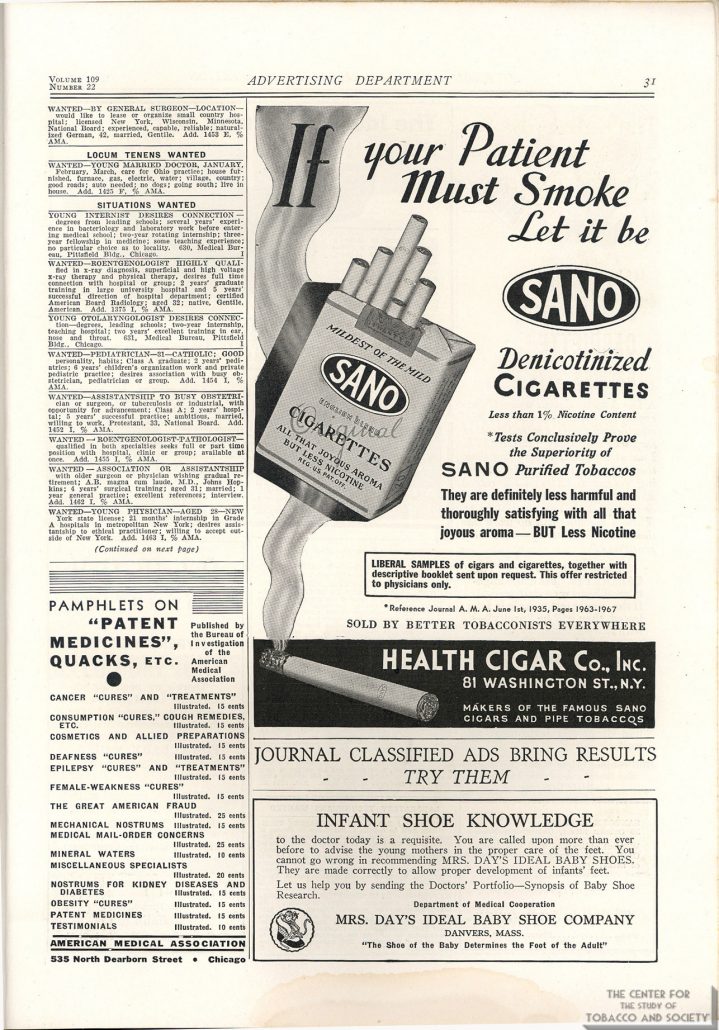
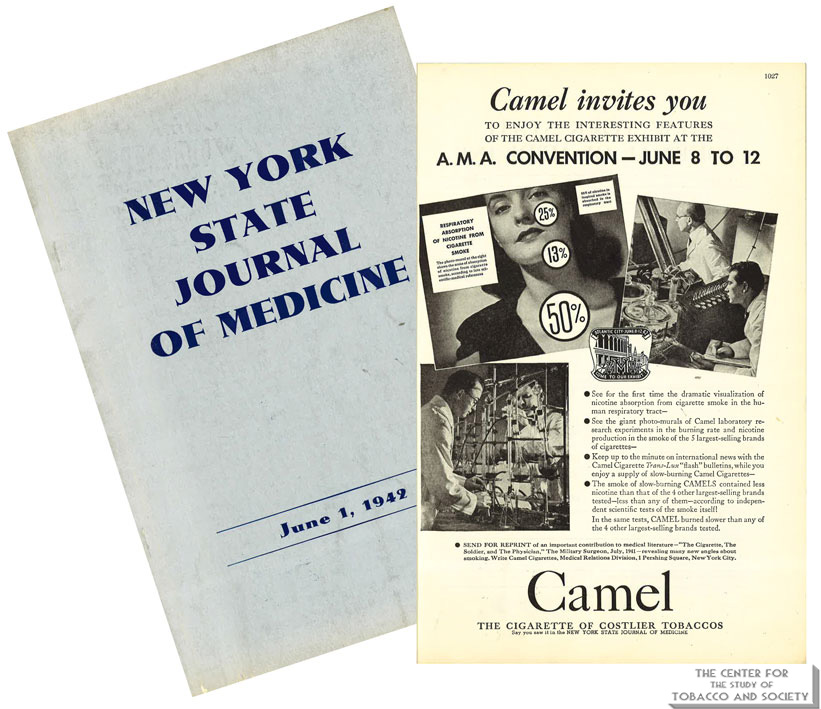
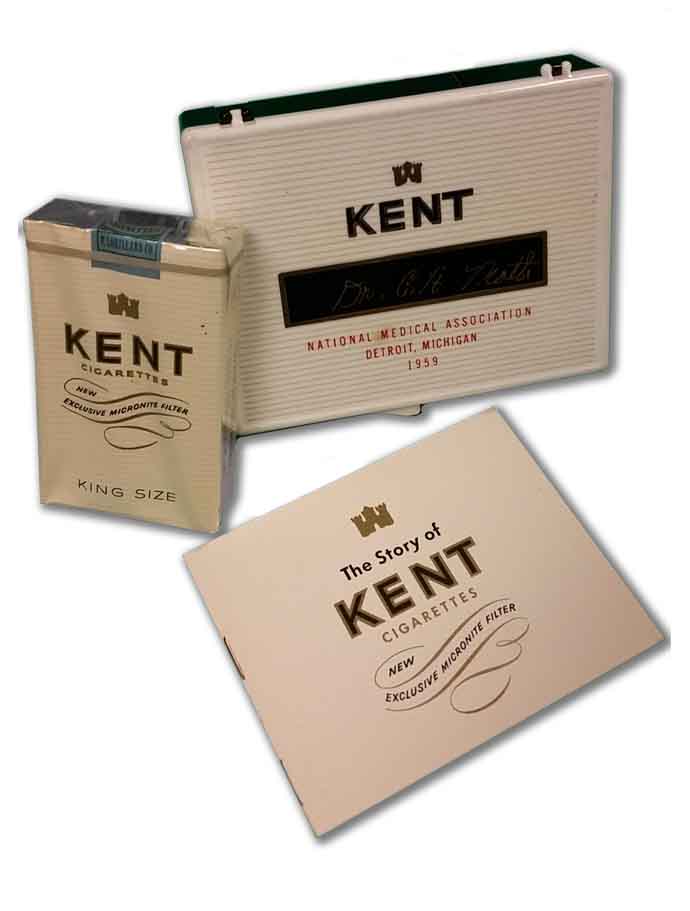
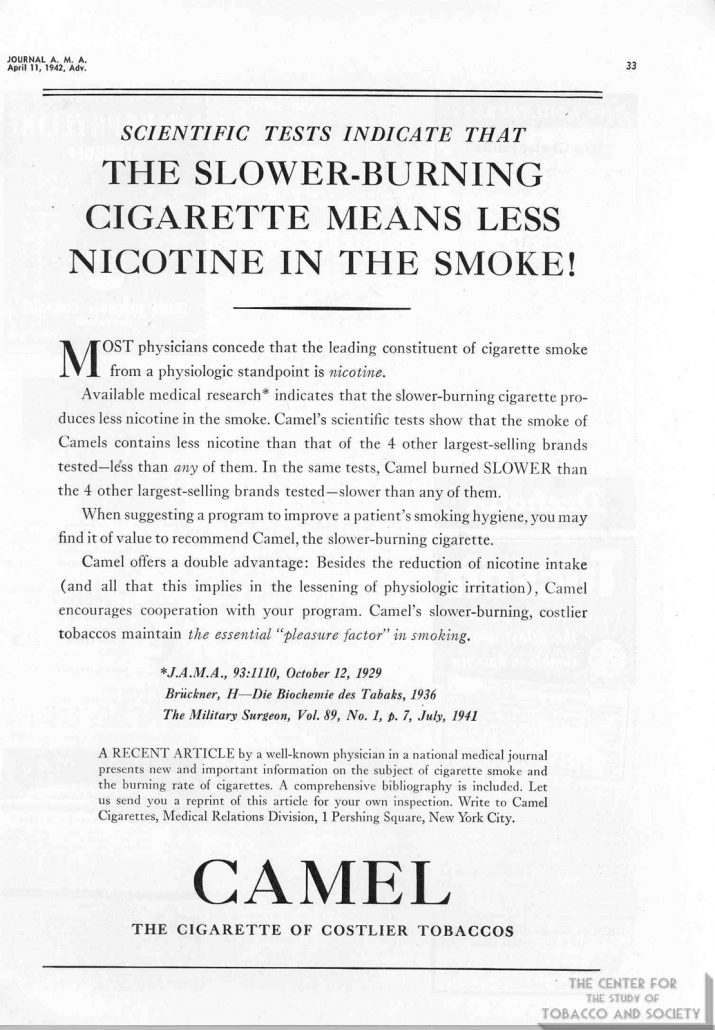
For most of the 20th century, the AMA turned a blind eye toward the dangers of tobacco use. During the 1930s, 40s and 50s, tobacco companies paid handsomely to advertise cigarettes in AMA’s journal, JAMA. In a 1948 editorial minimizing the ill effects of smoking and justifying tobacco advertising in its publications, JAMA noted that “cigarette business is a tremendous business,” as if the size of the bottom line can mitigate a conflict for an organization founded for the “betterment of public health.”
The connection between smoking and lung cancer was recognized early in the century. At the same time, the AMA became increasingly dependent on money generated by tobacco sales. Tobacco companies sponsored meetings of medical societies, setting up their booths alongside exhibitions of the latest medical treatments. Free cartons were distributed at physician meetings. Cigarette makers even paid for publication of pseudoscientific reports claiming the health benefits of their products.
Doctors who opposed smoking faced ridicule from their colleagues. Dr. Alton Ochsner, a renowned surgeon and sentinel voice warning of the dangers of tobacco, began publishing on the connection between smoking and lung cancer in the early 1940s. His 1954 book Smoking and Cancer: A Doctor’s Report was negatively reviewed in prominent medical journals, characterized as a medieval model of logic that belongs in the nonscience section of a library. Prior to his appearance on Meet the Press, Dr. Ochsner was told he could not discuss the relationship between smoking and lung cancer on air.
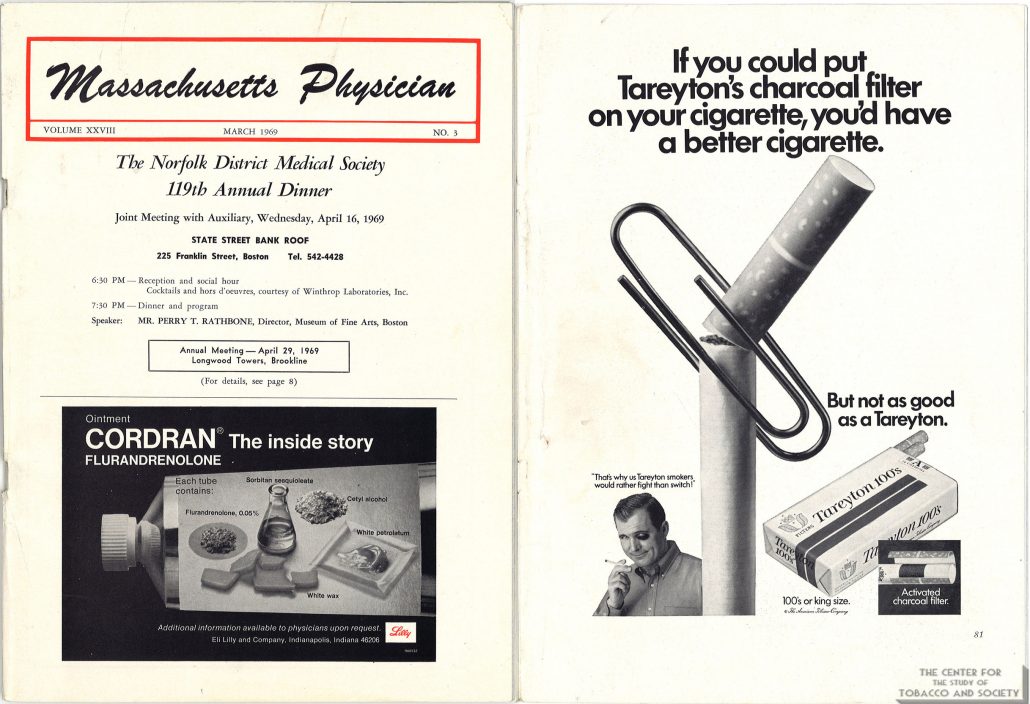
Yet the mounting evidence was hard to ignore. In 1954, JAMA stopped accepting cigarette advertisements and published an editorial rebuking tobacco company advertising practices. But five years later, a JAMA editorial was still skeptical of the evidence linking smoking to cancer, and a 1961 Nebraska State Medical Journal editorial dismissed the evidence as merely “statistical.” Tobacco companies continued to sponsor state medical meetings as late as 1969. By then most people were aware of the dangers of smoking.
In 1964, the Surgeon General concluded that cigarette smoking causes lung cancer and other life-limiting health conditions. The next year, a warning label was required on packages of cigarettes. By 1971, the government banned cigarette advertisements on television and radio. Instead of taking the lead against an obvious threat to public health, the AMA asked for time and money to study the effects of tobacco.
Between 1964 and 1976, the AMA received more than $20 million from the tobacco industry to fund research. Instead of using the money for smoking cessation programs, many of the funded studies focused on ways to make a safer cigarette. To keep money flowing into its Education and Research Foundation the AMA delayed, stating in a confidential 1971 report that, “AMA is not prepared to make any statement regarding termination of the smoking-health research program.” The report went on to complain that tobacco companies are “in arrears on 1970 contributions.” The dependency on tobacco money created a political alliance between doctors and cigarette makers as their lobbyists joined forces in Washington.
The delay benefitted tobacco sales and maintained the AMA’s “research” payments, but it angered Dr. Ochsner, who accused the AMA of being derelict. The AMA called Dr. Ochsner’s position “extreme.” But name-calling could not stall the inevitable conclusion any longer. In 1978 the AMA finally agreed with what most people had already realized: smoking causes lung cancer, and many other health problems. The romance with big tobacco was over.
Or was it?
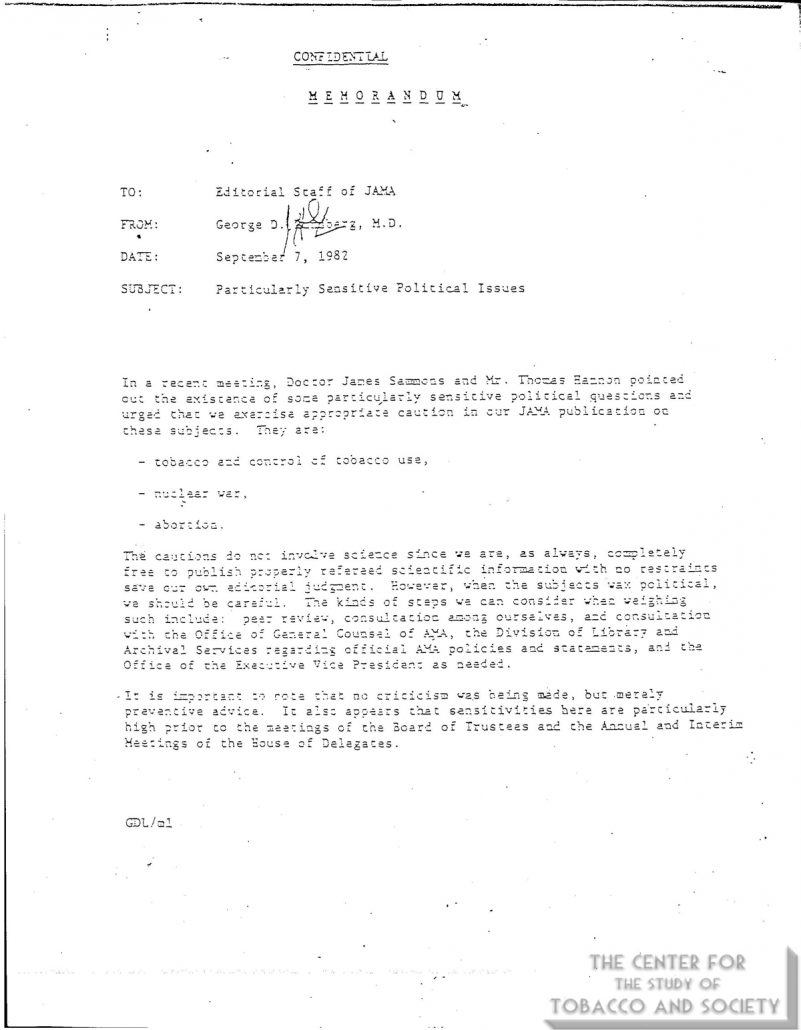
As late as 1982, JAMA publications were warned to steer clear of “politically sensitive” topics like tobacco use. After most of a century of being on the tobacco dole, the AMA could not make a clean break. The AMA portfolio contained investments in tobacco companies until the late 1990s.
In 1998, the tobacco industry settled lawsuits filed by state governments with a massive Master Settlement Agreement. In exchange for perpetual annual payments and tight regulatory control, the tobacco industry could continue to sell its products protected from future lawsuits brought by participating states and jurisdictions.
But who really benefitted from the Tobacco Settlement? Only 2.6 percent of the money has been used for smoking prevention and cessation programs. Some states have used the tobacco money to fill budget gaps. South Carolina gave money to tobacco farmers affected by a drop in prices. Altria Group, a global tobacco company, is on the US News & World Report 10 best-performing stocks list. Altria, Phillip Morris, and British American Tobacco have all grown annual dividends consecutively since the settlement. According to Dr. Ed Anselm, “The most addictive thing about tobacco is money.”
Tobacco use remains the number one preventable cause of death in the United States. In the first fifty years after the Surgeon General’s 1964 report, more than 20 million Americans died of smoking. How many of these deaths would have been prevented if doctors had not been conflicted by financial entanglements with the tobacco industry?
Money blinds objectivity. When money drives decisions, controverting evidence is ignored, dissenting voices are ridiculed, open debate is suppressed, talking points are distributed, conclusions are delayed, and people die from a product with liability protection.
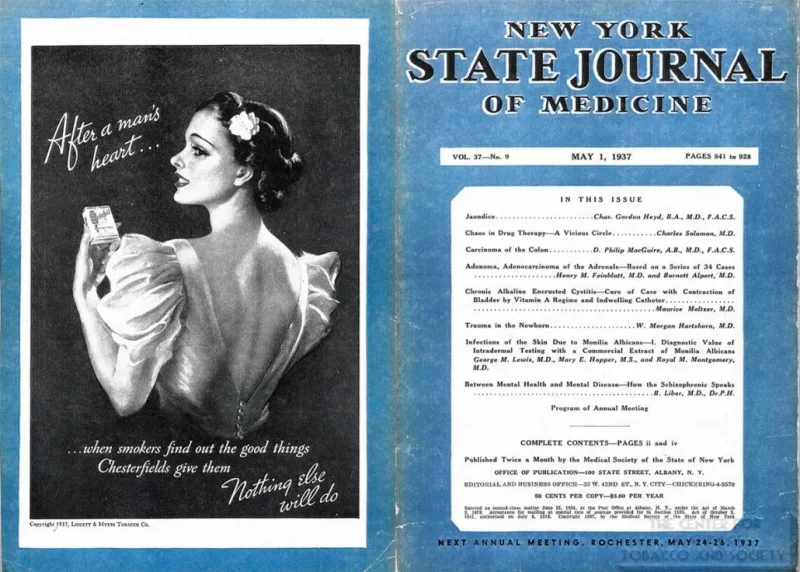
The New York State Journal of Medicine published a retrospective of tobacco’s relationship to medicine in its December 1983 issue. Flipping through the pages is enlightening. Surrounding the articles describing the greed and politics of Big Tobacco are advertisements from medicine’s new love—Big Pharma. Doctors have exchanged one bedfellow for another.
By endorsing irrelevant COVID-19 vaccines and poorly tested bivalent boosters, the AMA is pushing a product without concern for its potential negative health effects. Like before, the medical profession lags behind public opinion. According to recent Rasmussen Reports, 7 percent of vaccinated individuals report a major side effect, and nearly half of Americans believe that COVID-19 vaccines have caused unexplained deaths, about the same proportion who believed that smoking caused cancer in the 1960s while the AMA was studying the issue.
A conflicted profession cannot honestly evaluate data. Nowadays, the pharmaceutical business is a tremendous business. An organization benefitting from product sales cannot be trusted to evaluate that product.
If doctors could not recognize the health dangers of tobacco for most of the last century, why should we trust them when they say novel vaccines are safe and effective?
Kevin Homer, MD has practiced anatomic and clinical pathology at a community hospital in Texas since 1994.
Why Doctors Push COVID-19 Vaccination so Hard
By Peter A. McCullough, MD, MPH | Courageous Discourse | December 7, 2022
Patients commonly ask me why their other doctors push COVID-19 vaccination so hard still to this day with alarming safety statistics, loss of efficacy, and now a complete lack of human trial data with the bivalent boosters?
The answer may come by following a money trail from HHS and CDC called “COVID-19 Community Corps” that early in 2021 made undisclosed individual payments to hundreds of organizations to promote mass vaccination. There were notable medical groups including the American Medical Association, American Association of Family Physicians, American Association of Nurse Practitioners, American College of Obstetrics and Gynecology, American Academy of Pediatrics, American Association of Pediatrics, and the American Medical Student Association.
![]()
More investigation is likely to reveal that federal money received was temporally linked to e-mail blasts, town hall meetings, and many other activities pushing mass vaccination.
Could COVID-19 Community Corps money to the AMA have been the reason why the AMA launched its campaign to “abolish” the use of ivermectin in 2021 so the public would be panicked into taking more shots?
How could the pediatric associations take federal money before the clinical trials for their patients were completed or the vaccines approved via EUA?
Did they promote the vaccines to pediatricians before clinical trial results were known?
Finally, how could federal dollars flow to gynecologists/obstetricians when pregnant women and those of childbearing potential where excluded from randomized trials reported just a few months before the HHS initiative?
These broad acts of public bribery, corruption, and vaccine racketeering worked to put millions of lives danger as we learned about the risks of COVID-19 vaccination in 2021.
As we sit here today, the CDC VAERS system through November 25, 2022, is reporting 15,508 US deaths after COVID-19 vaccination, 22% occurred within 96 hours of the shot. There have been 15,505 Americans disabled, 9266 with heart damage, and 356,269 office visits, urgent care encounters, or hospitalizations attributed to vaccine side effects.
Never again can we allow our public health agencies use unchecked financial power to promote any medication or vaccine to healthcare providers. Corruption and indoctrination are deadly.
Doctors File First Lawsuit Challenging California Law That Seeks to Punish Physicians for COVID ‘Misinformation’
By Suzanne Burdick, Ph.D. | The Defender | October 6, 2022
Two doctors on Tuesday became the first to file a federal lawsuit to stop a new California law that subjects the state’s doctors to discipline, including the suspension of their medical licenses, for sharing “misinformation” or “disinformation” about COVID-19 with their patients.
Dr. Mark McDonald, a Los Angeles psychiatrist, and Dr. Jeff Barke, an Orange County primary care physician and founding member of America’s Frontline Doctors, filed the complaint in the U.S. District Court for the Central District of California.
The lawsuit names 12 members of the Medical Board of California and California Attorney General Robert Bonta.
The plaintiffs also filed papers seeking a preliminary injunction to protect their free speech rights as the case unfolds.
Barke told The Defender :
“[This new law] puts patients at risk. Requiring physicians to consider the state’s narrative when making a medical decision, is bad medicine and dangerous. Consensus in science only occurs when dissenting opinions are censored.”
Commenting on the lawsuit, Mary Holland, president and general counsel for Children’s Health Defense, said, “California’s new law is a clear violation of the First Amendment. It’s startling that the legislature and the governor would even attempt to pass such legislation.”
Holland added:
“Censoring information about health never leads to health, but it certainly can and has led to medical catastrophes. I look forward to courts striking this law down.”
The Los Angeles Times today reported that some doctors fear California’s new law “could do more harm than good.”
“What was misinformation one day is the current scientific thinking another day,” Dr. Eric Widera, a professor of medicine at the University of California San Francisco, told LA Times.
Liberty Justice Center, a national nonprofit law firm dedicated to protecting Americans’ constitutional rights, is representing McDonald and Barke.
Daniel Suhr, managing attorney at the center, said, “We rely on our doctors to give us their best medical advice, yet the State of California is stopping doctors from doing just that. That’s not just wrong, it’s unconstitutional.”
He added, “Doctors enjoy the same free speech rights as other Americans. The State of California cannot define a so-called scientific consensus on an issue and then punish anyone who dares challenge it.”
Law is ‘at odds with the scientific method itself’
California Assembly Bill 2098 (AB 2098), signed into law Sept. 30 by Gov. Gavin Newsom, defines “misinformation” as “false information that is contradicted by contemporary scientific consensus contrary to the standard of care” and “disinformation” as “misinformation that the licensee deliberately disseminated with malicious intent or an intent to mislead.”
Newsom said the law applies only to physicians’ speech with patients during discussions directly related to COVID-19 treatment.
But Drs. McDonald and Barke allege AB 2098 violates the First Amendment, imposes “government-approved orthodoxy” and “is at odds with the scientific method itself.”
The lawsuit states:
“Disagreement is integral to the progress of medical science, a value that cannot be served by using the power of the state to punish those who dissent from the official line.
“This is particularly objectionable in the context of a new disease like COVID-19, about which consensus opinions and official guidance have regularly adjusted as new information is learned.
“At the beginning of the pandemic, public health authorities insisted that the public not wear masks, arguing they would provide little benefit and should be reserved for front-line medical professionals — that was soon replaced with broadly mandated mask wearing for much of the population.
“Schools were closed in the face of the fear that the disease would spread among children too young to adhere to quarantine procedures — but it turned out that the young were at the least risk, and that such closures may well have been harmful to their development.
“Reasonable minds disagreed then, and continue to disagree now, about any number of such topics, but the search for truth cannot be furthered by a government edict imposing orthodoxy from above, punishing those who disagree with the loss of their profession and their livelihood.”
The lawsuit also alleges that AB 2098 “intrudes into the privacy of the doctor-patient relationship” by “replacing the medical judgment of the government for that of the licensed professional and chilling the speech of those who dissent from the official view.”
The plaintiffs asked that the court “enjoin enforcement of AB 2098 and leave these important matters to the marketplace of ideas.”
AB 2098 was introduced in mid-February by California Assemblymember Evan Low — one of seven Democratic lawmakers who in January formed the Vaccine Work Group to develop legislation promoting the use of COVID-19 vaccines while “battling misinformation.”
The American Medical Association (AMA), which strongly supports the bill, hopes other states will follow suit in “ensuring that licensing boards have the authority to take disciplinary action against health professionals for spreading health-related disinformation,” according to a new policy adopted at its mid-June annual meeting aimed at addressing public health “disinformation.”
The AMA’s adopted policy expanded on prior efforts and called for the organization to work with “health professional societies and other relevant organizations to implement a comprehensive strategy to address health-related disinformation disseminated by health professionals.”
Language in the bill points out that the Federation of State Medical Boards (FSMB) has warned that physicians who spread misinformation or disinformation “risk losing their medical license, and … have a duty to provide their patients with accurate, science-based information.”
The FSMB, as previously reported by The Defender, takes money from Big Pharma and has a history of challenging and attacking non-pharmaceutical medical approaches used by integrative doctors as falling outside the “standard of care” as they define it.
“If this period has taught us anything,” McDonald said, “it is that the scientific and medical environments are constantly evolving, as new information and studies confirm or reject prior policies.
He added:
“Doctors need the freedom to explore alternatives and share opinions that challenge the scientific consensus — that is inherent in the nature of the scientific enterprise.
“California cannot insert itself into the physician-patient relationship to impose its views on doctors and end all debate on these important questions.”
Suzanne Burdick, Ph.D., is a reporter and researcher for The Defender based in Fairfield, Iowa. She holds a Ph.D. in Communication Studies from the University of Texas at Austin (2021), and a master’s degree in communication and leadership from Gonzaga University (2015). Her scholarship has been published in Health Communication. She has taught at various academic institutions in the United States and is fluent in Spanish.
This article was originally published by The Defender — Children’s Health Defense’s News & Views Website under Creative Commons license CC BY-NC-ND 4.0. Please consider subscribing to The Defender or donating to Children’s Health Defense.
Biden Regime War on Humanity with Mass Destruction in Mind

By Stephen Lendman | November 14, 2021
If only what’s ongoing would end on awakening from a bad dream.
Horrors unleashed by Biden regime and complicit dark forces are horrifyingly real.
There’s no end of them in prospect without a second US revolution to accomplish what the first one failed to address when everything changed but stayed the same under new management.
If genocidist Bill Gates had dictatorial powers he likely craves, refuseniks unwilling to self-inflict harm through kill shots — and oppose masks that don’t protect and risk respiratory harm — would be criminalized.
Calling for punishing them, he wants truth and full disclosure about all things flu/covid banned by digital censorship, along with medical surveillance, simulated bioterrorism attacks he likely wants rehearsed ahead of launching the real things for greater mass-extermination than already.
Separately, the American Medical Association (AMA) promoter of medical tyranny in support of mandatory kill shots filed an amicus brief on Thursday with the 5th Circuit Court of Appeals in support of the draconian Biden regime mandate from hell.
The brief falsely called seasonal flu — deceptively called covid — a major public health threat, a bald-faced Big Lie.
It backs mandatory kill shots for everyone.
It lied claiming they’ll contain infections and transmission of the viral illness.
It lied saying kill shots will protect the jabbed and unjabbed alike.
It lied claiming they’re essential to protect US workers.
It lied saying they’re safe and effective.
It lied claiming that the vast majority of individuals with flu/covid are unjabbed.
The amicus brief was infested with beginning to end bald-faced Big Lies by an agency hostile to its stated mission of protecting health.
Along with US/Western dark forces, their anti-public health handmaidens, Pharma profiteer-pushers of toxic kill shots and MSM co-conspirators, the AMA is a mortal enemy of protecting and preserving what’s too precious to lose.
It supports policies intended to destroy health with unparalleled genocide in mind.
Flu/covid is easily treated and cured.
Yet the AMA opposes known safe and effective protocols for protection against contraction of flu/covid, along with obliterating outbreaks when occur in a few days.
When taken as directed, jabs irreversibly harm health.
The AMA supports kill shots with that objective in mind.
The pandemic it cited doesn’t exist — except for jabbed individuals.
It wants the health of young kids destroyed by mandatory kill shots.
It also wants US public health wrecked by mandating them for all doctors, nurses and other healthcare staff.
Numerous young/highly conditioned professional athletes in the US/West and elsewhere either collapsed and died from kill shots or became seriously ill and disabled.
Despite numbers continuing to rise, US/Western MSM suppressed what should be headline news.
Most athletes who perished or became seriously ill were diagnosed with heart-related issues.
What’s been unheard of in athletes and other young people pre-2020 is now at epidemic levels worldwide.
Numbers of young kids likely to die or fall seriously ill when mass-jabbing is fully underway should chill parents and others to denounce the practice.
Kill shots are designed to cause maximum destruction of public health.
Shunning them is crucial to protecting it.
American Medical Association Instructs Doctors to Deceive
By Dr. Joseph Mercola | September 23, 2021
The Winter 2021 “AMA COVID-19 Guide: Background/Messaging on Vaccines, Vaccine Clinical Trials & Combatting Vaccine Misinformation,”1 issued by the American Medical Association (AMA) raises serious questions about the AMA’s adherence to transparency, honesty, ethics and the moral standards to which it will hold its members.
The AMA was founded in 1847 and is the largest professional association and lobbying group of physicians and medical students in the U.S. According to the AMA itself, its mission is to promote the art and science of medicine and the betterment of public health.
How then do they explain this “COVID-19 messaging guide,” which explicitly teaches doctors how to deceive their patients and the media when asked tough questions about COVID-19, treatment options and COVID shots?
AMA Teaches Doctors How to Deceive
“It is critical that physicians and patients have confidence in the safety and efficacy of COVID-19 vaccines as they become available for public use,” the “AMA COVID-19 Guide” states, adding:2
“To overcome vaccine hesitancy and ensure widespread vaccine acceptance among all demographic groups, physicians and the broader public health community must continue working to build trust in vaccine safety and efficacy, especially in marginalized and minoritized communities with historically well-founded mistrust in medical institutions.”
Indeed, the entire guide is aimed at teaching doctors how to foster confidence in the medical profession in general, as it pertains to treatment of COVID-19, but in particular as it pertains to the experimental COVID shots.
The guide provides “suggested narratives” for various engagements, such as when communicating on social media, as well as “talking points to guide external communications,” such as when being interviewed. It lists nine specific “key messages” that they want doctors to focus on when communicating about COVID-19. These key messages can be summarized as follows:
Express confidence in vaccine development
-
- Stress the importance of vaccines
- Highlight the need to combat the spread of vaccine misinformation
- Adhere to updated ethical guidance for physicians and medical personnel, which says they have a moral obligation to get vaccinated themselves
- Give general vaccine recommendations, such as the recommendation for everyone over the age of 6 months, including pregnant women, to get an annual flu shot
- Stress the importance of eliminating nonmedical vaccine exemptions
- Highlight the increased availability of flu vaccines, and the importance of getting a flu shot even if you’ve gotten a COVID injection
- Highlight the importance of including minorities, both in vaccine trials and as trusted messengers who can “promote social pressure” to get minorities vaccinated and dispel historical distrust in medical institutions
- Denounce scientific analyses “predicated on personal opinions, anecdote and political ideologies”
AMA Concerned About Disinformation
On page 7 of the guide, under the science narrative heading, the AMA declares it is “deeply concerned that rampant disinformation and the politicization of health issues are eroding public confidence in science and undermining trust in physicians and medical institutions,” adding that “Science should be grounded in a common understanding of facts and evidence and able to empower people to make informed decisions about their health.”3
To that end, the AMA is calling upon “all elected officials to affirm science and fact in their words and actions,” and for media to “be vigilant in communicating factual information” and to “challenge those who chose to trade in misinformation.”
AMA Then Instructs Doctors on How to Disinform
It’s a disappointment, then, to find the AMA instructing doctors on how to misinform the public using a variety of psychological and linguistic tools. Perhaps one of the most egregious examples of this is the recommended “COVID-19 language swaps” detailed on page 9.
As you can see below, the AMA explicitly instructs doctors to swap out certain words and terms for other, more narrative-affirming choices. Shockingly, this includes swapping “hospitalization rates” to “deaths” — two terms that are not even remotely interchangeable!
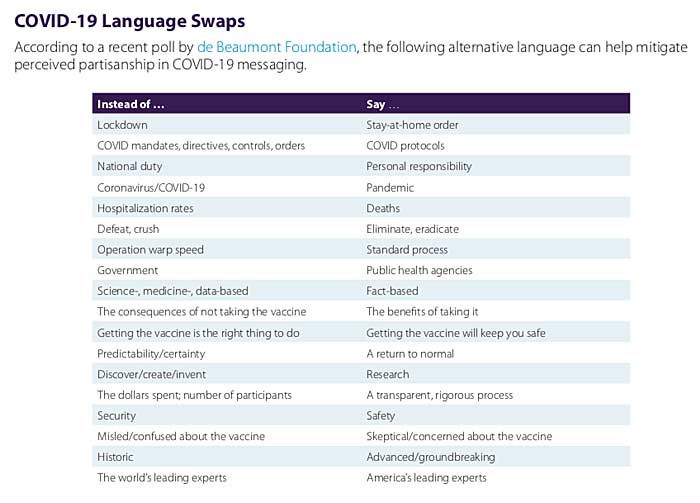
Another highly questionable word swap is to not address the nitty, gritty details of vaccine trials, such as the number of participants, and instead simply refer to these trials as having gone through “a transparent, rigorous process.”
Swapping the factual term “Operation Warp Speed” for “standard process” is another outrageous misdirection. The two simply aren’t interchangeable. In fact, they’re actually diametrically opposed to one another. Standard process for vaccine development includes a long process of over a decade and a large number of steps that were either omitted or drastically shortened for the COVID shots.
Following standard process is what makes vaccine development take, on average, 10 years and often longer. Operation Warp Speed allowed vaccine makers to slap together these COVID shots in about nine months from start to finish. You cannot possibly say that the two terms describe an identical process.
The Power of Language
Other language swaps are less incredible but still highlight the fact that the AMA wants its members to help push a very specific and one-sided narrative that makes power-grabbing overreaches and totalitarian tactics sound less bad than they actually are, and make questionable processes sound A-OK.
Language is a powerful tool with which we shape reality,4 because it shapes how we think about things. As noted by storyteller and filmmaker Jason Silva:5
“The use of language, the words you use to describe reality, can in fact engender reality, can disclose reality. Words are generative… We create and perceive our reality through language. We think reality into existence through linguistic construction in real-time.”
For example, “lockdown” sounds like involuntary imprisonment imposed by a totalitarian regime, which is what it is, whereas “stay-at-home order” sounds far less draconian. After all, “home” is typically associated with comfort and safety.
The same goes for using “COVID protocols” in lieu of “COVID mandates, directives, controls and orders.” “Protocols” sounds like something that is standard procedure, as if the COVID measures are nothing new, whereas “mandates, controls and orders” imply that, indeed, we’re in medical fascism territory, which we are.
How to Steer, Block, Deflect and Stall Inconvenient Questions
The AMA could have instructed its members to simply stick to the facts and be honest — and in some sections, it does do that — but it doesn’t end there. Rather, the AMA provides a full page of instructions on how to steer the conversation, and how to block, deflect and stall when faced with tough questions where an honest answer might actually break the official narrative.
Here’s a sampling of these instructions. I encourage you to read through page 8 of the guide, and pay attention to these psychological tricks when listening to interviews or reading the news.
Interviewing techniques
-
- Steer the conversation back to the narrative by saying: “Before we leave that matter, let me add …”
- Block a tough question by saying: “That’s [proprietary, confidential etc], but what I can tell you is …”
- Deflect an unwanted question by saying: “That’s a common misperception but the reality is …”
- Redirect away from an unwanted question, back to the official narrative by saying: “I don’t have the details on that, but what I know is …”
- Stall by saying: Repeat the question asked, or acknowledge the question by saying, “I’m glad you asked …”
It’s worth noting that the AMA also stresses that: 1) Doctors are to speak for the AMA, and 2) doctors are NOT to offer their personal views. Speaking for the AMA is listed under “Your Responsibilities” when being interviewed, while not discussing personal views is listed under “Interview Don’ts.”
AMA Is Rapidly Eroding All Credibility
The AMA’s guidance isn’t all bad. Some of its advice makes perfect sense. But the inclusion of language swaps that result in false statements being made, and tools for steering, blocking, deflecting, redirecting and stalling in order to avoid direct answers do nothing but erode credibility and thus trust in the medical community.
Its direct instruction to not share personal views is another trust-eroding strategy. When people talk to their doctor, they want to hear what that doctor actually thinks, based on their own knowledge and experience.
They don’t expect their doctor — or a doctor appearing in an interview — to simply rehash a narrative dictated by the AMA. If we cannot trust our medical professionals to give their honest opinions and give direct answers, there’s little reason to even discuss our concerns with them, and that’s the opposite of what the AMA claims it seeks to achieve.
The AMA is concerned about the proliferation of misinformation and eroding trust, yet it’s telling its members to keep their professional views to themselves and lie about COVID deaths. With this guidance document, the AMA is essentially implicating itself as a source and instigator of medical misinformation that ultimately might injure patients.
In a Stew Peters Show interview (see bitchute), Dr. Bryan Ardis criticized the AMA guidance document, pointing out that while the AMA claims it put out the guidance to prevent political ideologies from dictating medicine, it is actually proving that the AMA itself is deferring to political ideology rather than medical facts.
The AMA wants its members to act as propagandists for a particular narrative — using “politically correct language” — rather than sharing information and acting in accordance with their own conscience and professional insight. As noted by Peters:
“If a doctor’s just going to repeat what the AMA tells them, why have doctors at all? You can get plenty of starving propagandists at any liberal college, but instead we want to turn our medical professionals into ideological zombies with stethoscopes.”
Sources and References
AMA issues mix of mindless propaganda & “Trust the SCIENCE” jargon to teach doctors to lie about Covid jabs
By Meryl Nass, MD | September 14, 2021
I am looking over the “AMA Covid -19 Guide. Winter 2021. It is not a guide. It only deals with Covid vaccines, not treatment. It’s raison d’etre is:
“To overcome vaccine hesitancy and ensure widespread vaccine acceptance among all demographic groups, physicians and the broader public health community must continue working to build trust in vaccine safety and efficacy, especially in marginalized and minoritized (this is not my misspelling–Nass) communities with historically well-founded mistrust in medical institutions. As COVID-19 vaccines become more widely available, it is critical that physicians continue to ensure they practice and encourage their patients to wear masks, physical distance and wash hands until a critical mass of the population is vaccinated.”
It is an extraordinary document. I wonder how much the AMA got paid to put their name on it. Probably a lot.
It is extraordinary because it would repel most doctors. It was obviously written by a non-doctor. I have an idea of one person who may have had a hand in creating it–John Grabenstein, a pharmacist and propagandist extraordinaire, who helped craft the fake science on the anthrax vaccine. He works for the Immunization Action Coalition now. He is a one man band who knows how to pull all the levers to push terrible vaccine policies.
It turns out that the current AMA President, Gerald Harmon, was instrumental in pushing the experimental and dangerous anthrax vaccine, and punishing refusers and truth tellers. This got him rapid promotions, and he retired as a Major General. No doubt he worked with Grabenstein back then, and probably now.
Whoever wrote the “Guide” did not know that whooping cough and pertussis were the same thing, or that the DTP vaccine includes tetanus. It is of interest that there is no name on it, no clue about how it came into existence.
All this business about “equity.” If the federal government cared about equity, why are they always bombing and droning people of color? What equity means to them is that a 25% acceptance of the Covid vaccine by Black people cannot be allowed to stand. And the refusal by blacks to participate in clinical trials is especially egregious.
The document is really kind of a hoot, it is so out of 1984. It shows you what the propagandists are really worried about, for example, the fact that too many people have learned the FDA “review” and the Pfizer preclinical tests were bogus:
On combating the spread of vaccine misinformation:
• With misinformation about the COVID-19 vaccine development process circulating widely, new AMA policy seeks to educate physicians on speaking with their patients about the vaccine and provide culturally appropriate education materials for all patients.
On vaccine development:
• To help physicians promote vaccine confidence among patients and the general public, we must continue to instill confidence in the information, education, and transparency around the FDA’s process for authorization or licensure, as well as the standards by which FDA will review future vaccine candidates and the clinical endpoints the FDA hopes to achieve.
• Physicians must be continuously updated about the review process for future COVID-19 vaccines. Any available safety and efficacy data must be in place as soon as possible so that any questions or concerns about the vaccine candidates can be addressed.
• The AMA has been talking to FDA officials about the role the agency needs to continue to play in alleviating vaccine concerns by ensuring the process is transparent and based on science.
• The widespread availability and adoption of a safe and efficacious vaccine will play an essential role in slowing transmission of COVID-19 and allow us to move safely and confidently toward the full re-opening of our businesses and schools, helping ease Americans back toward pre-pandemic life.
• Research shows growing levels of confidence in the safety and effectiveness of the COVID-19 vaccines, but there continues to be vacancy hesitancy among some individuals and in some communities, which we are striving to overcome.
• What’s clear is that the benefits of getting the vaccine to protect you from COVID-19 exceed the risks, which is why medical experts strongly recommend getting the vaccine.
• To improve the dialogue and provide opportunities for physicians to learn more about vaccine development, approval, and ongoing distribution plans and challenges, AMA has initiated a series of “town hall” type webinars with physicians and career staff at both the FDA and CDC. All events are archived on AMA’s website.
• To develop the most effective COVID-19 vaccine, U.S. clinical trials must include representation of all Americans to ensure treatments are studied in every population that may use it.
The AMA is pleased that efforts have been made by institutions to acknowledge the exclusion of Black and Latinx people from clinical trials historically.
Now there are many efforts underway to ensure Black and Latinx people, who have been disproportionately affected by the virus, are prioritized in clinical trials.
This not only provides better safety and efficacy data but is a more equitable strategy that will hopefully contribute to trust in the vaccine once available.
Featured Video

No Threat Can Force Iran’s Surrender /Trita Parsi & Lt Cl Daniel Davis
or go to
Aletho News Archives – Video-Images
From the Archives
An Expert Military Analysis of War with China
Actually, None is Necessary
By Fred Reed • Unz Review • December 13, 2020
The Correlation of Armed Forces: U.S. goods and services trade with China totaled an estimated $634.8 billion in 2019. Exports were $163.0 billion; imports were $471.8 billion. The U.S. goods and services trade deficit with China was $308.8 billion in 2019. Trade in services with China (exports and imports) totaled an estimated $76.7 billion in 2019. Services exports were $56.5 billion; services imports were $20.1 billion. The U.S. services trade surplus with China was $36.4 billion in 2019.
There is talk within the Washingtoniat of a possible war with China. Steve Bannon, who apparently was dropped on his head as a child, actually favors such a war. We hear the usual shoo-the-boobs alarm about how the Chinese are doing something terrible and we must gird our loins and American values and show them what for, bow wow, woof. The danger is that the current game of who-blinks-first in Asian waters might actually provoke a shooting war. You know the kind of thing: One warship refuses to get out of the way of another, a collision ensues, some retard lieutenant who signed up on waivers opens fire, and we’re off and running. It is not a good idea to let children play with matches.
The said war is discussed either in emotional terms by idiots or in purely naval terms by those familiar with such things, so we hear of the First Island Chain and the Second Island Chain and whose missiles against the other’s missiles and so on. This would be appropriate if we were fighting World War Two again. Which we aren’t. Let’s take a quick-and-dirty look at how such a war might go.
To begin the war, America would overestimate itself and underestimate China. This is doctrine in the Pentagon. … continue
Blog Roll
 Aletho News
Aletho News- Iran To Target Military Industrial-Tech Complex That Facilitated Gaza Genocide
- Collapsing Empire: The Resistance Disarms ‘Israel’
- Suicide Should Not Be a Government Service
- Rethinking America’s greatest threat: Iran vs. Israel-Firsters
- Iran accuses adversaries of false flags to strain Turkey ties
- Poland rules out sending Patriot missiles to US/Israel amid war on Iran
- Tehran approves new Hormuz plan with major restrictions
- No Threat Can Force Iran’s Surrender /Trita Parsi & Lt Cl Daniel Davis
- UK’s New Pandemic Plan Would Turn Big Tech Into a Mass Location Tracking Network
- Growing insecurity, soaring prices fuel protests in north as regime bans evacuation: Sources
- If Americans Knew
- Ann Coulter Rips Into Fox News for Iran War Coverage, Compares to False Rigged 2020 Election Reporting
- Joe Kent Urges Americans To Call White House and Congress To Object To Sending Troops Into Iran
- DNC Resolution to Reject AIPAC Funding Puts Democratic Leaders in the Hot Seat
- Swedish foundation to build 400 schools as over 650,000 Gaza children remain without education for 2 years
- Israeli army admits photshopping image of slain Lebanese journalist
- This is how Israel is systematically killing health workers under the cover of war in Lebanon
- Carrying life under fire: Israeli invasion of Lebanon leaves pregnant women facing deadly risks
- Champagne all around for the new death penalty (for Palestinians) law – Not a ceasefire Day 172
- Why are Palestinian books struggling to be seen on Amazon?
- The Line Between Affinity and Conspiracy
- No Tricks Zone
- New Study Finds Warming Saves Lives…Cold Temperatures 12 Times More Deadly Than Excess Heat
- German Science Blog Accuses PIK Climate Institute Of Hallucinating Climate Tipping Points
- Devastating Assessment Of Comirnaty Vaccine By Former Senior Pfizer Europe Toxicologist
- New Study: CO2 Is ‘Effectively Negligible’ As An Explanatory Climate Change Factor Since 2000
- Former Pfizer Toxicologist Dr. Helmut Sterz Tells Bundestag Hearing Pfizer Vaccine Should Have Never Been Approved
- Energy Expert: Germany’s Nuclear Phaseout Was A “500 Billion Euro Mistake”
- New Research: South Australia’s Mid-Holocene Sea Surface Temperatures Were 4°C Warmer Than Today
- Storing Green Energy To Last Germany 10 Days Would Require A 60-Million Tonne Battery
- New Studies: UK Sea Levels Were 4 Meters Higher Than Today During The Mid-Holocene
- Destructive Green New Deal: German Energy And Metal Group Warns Of Drastic Crisis

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}