Strategic Group, a major rental housing provider in Alberta, Canada, announced that all new tenants need to show a vaccine passport to live in its properties. Critics claim the renter’s vaccine mandate sets a dangerous precedent.
“Vaccination of everyone in our community is the only way we are going to get through this pandemic and back to a sense of normalcy,” said Riaz Mamdani, founder and CEO of Strategic Group, in an October 28 press release.
“The safety of our team and our residents is a top priority, so ensuring full vaccination across the board is the least we can do.”
The press release said that “all employees, residents, and prospective residents” have to be vaccinated. Existing tenants will have to show proof of vaccination. Anyone “unable to be vaccinated (i.e., children under the age of 12) is exempt until able to receive the vaccine.”
“These rules apply to all of Strategic Group’s residential communities in Alberta.”
The renter owns more than 100 1 and 2-bedroom units in Edmonton and Calgary.
The Canadian Pressreported that the Strategic Group COO Tracey Steman said that the company was “very proud” of the mandatory vaccination policy.
“And we’d like to see other landlords implement the same policy… It will help to end this pandemic,” Steman continued. “We’ve had really good feedback from our tenants.”
According to the company’s CEO, residents inspired the new policy as they were saying that “they value knowing that all their neighbors are vaccinated – they feel even safer in their own homes.”
Eva Chipiuk of the Justice Center for Constitutional Freedoms (JCCF) told LifeSiteNews that Strategic Group’s vaccine mandate for tenants “sets a dangerous precedent in Alberta and in Canada.”
“According to this renter’s policy, you do not deserve a roof over your head unless you have taken an experimental injection,” said Chipiuk.
“Such a policy, utterly unthinkable two years ago, is now frighteningly announced with pride,” she added.
“Under what authority is this policy being made?”
Chipiuk noted that the laws banning smoking indoors were discussed in “government housing.”
“This is not the same. These rental companies are taking the law into their own hands. If we allow this to happen, what will be next and who will find themselves without a place to live?” the lawyer asked.
In an article on The Lawyers Daily, landlord-tenant lawyer Caryma Sa’d explained why it is illegal for landlords to enforce vaccine passport mandates for tenants. Sa’d noted that refusing a potential client because of their vaccination status is discrimination.
Also, “landlords cannot simply make unilateral changes to the terms of the agreement, which would include imposing proof of vaccination as a condition of the tenancy.”
“This would prevent a landlord from attempting to evict a tenant based on vaccination status, unless it can be established that the tenant is substantially interfering with the reasonable enjoyment of others within the unit or otherwise causing serious problems at the residential complex because of their vaccination status,” the lawyer continued.
The president of the Canadian Federation of Apartment Associations John Dickie told the Canadian Press that it was “possible” for some landlords to follow Strategic Group’s lead and implement a vaccine passport mandate, but that was not likely to be “very widespread.”
“We’re not the health police,” said Dickie.
“Rental housing providers realize people need housing. We’re not in the habit of inquiring into people’s political views.”
You’ve probably seen a handful of people on social media say that vaccine passport systems make them “feel safe.” You know and I know that these systems have nothing to do with health or safety.
Well, some authorities in Canada just admitted what you and I knew: the aim is to punish the unvaccinated.
The British Columbia Parks and Recreation department says: “Remember, the purpose of the PoV card is to incentivize residents to be vaccinated, not to control the spread of the virus.”
Then further: “This is an important shift to keep aware of for your decision-making; the province has shifted from actions that provide a COVID-safe environment to actions that provide discretionary services to the vaccinated.”
Patricia Daly, Chief Medical Health Officer for Vancouver Coastal Health, added:
“The vaccine passport requires people to be vaccinated to do certain discretionary activities such as go to restaurants, movies, gyms, not because these places are high risk. We are not actually seeing covid transmission in these settings.
It really is to create an incentive to improve our vaccination coverage…. The vaccine passport is for non-essential opportunities, and it’s really to create an incentive to get higher vaccination rates.”
So even though cities and countries with these systems in place are doing no better than countries that don’t, that isn’t the point.
The point, as I’ve said all along, is to punish those who decline the vaccines.
UNICEF Spokesperson James Elder has just returned from Yemen with some tragic news about children living in what the United Nations calls the worst humanitarian crisis in the world.
Speaking at a press briefing in Geneva, he said: “The Yemen conflict has just hit another shameful milestone: 10,000 children have been killed or maimed since Saudi Arabia’s bombing campaign started in March 2015. That’s the equivalent of four children every day.” Elder told reporters that the estimates provided by the international UN agency were likely an understatement of the actual number of children killed and injured, which is rarely recorded by anyone. “These are of course the cases the UN was able to verify. Many more child deaths and injuries go unrecorded, to all but those children’s families.”
International experts have identified four significant dangers that have brought the country to the brink of humanitarian collapse. First of all, it is a brutal and protracted military conflict, and the blame for unleashing it lies entirely with the US and Saudi Arabia. Secondly, the colossal economic devastation that struck all regions of the country resulted from the military conflict. Also, there is a lack of infrastructure and social services, i.e., health, nutrition, water and sanitation, social protection, and education. Finally, the UN is critically underfunded.
It may be recalled that the war with Yemen began in March 2015, when Saudi Arabia brazenly and cynically launched a bombing campaign to restore the former regime, which obeyed orders from Riyadh, essentially maintaining Yemen’s status as a parallel and subordinate state to the Saudis. This had been the case before the popular revolution in the country, which triggered powerful Saudi airstrikes. The United States sold hundreds of billions of dollars worth of arms to the Kingdom during this war, in addition to intelligence and logistical support for Saudi military aircraft. Evidence shows that the UK is the second-largest supplier of arms to Riyadh, which is being actively used in an undeclared war, mostly against civilians. Other Western countries, including “democratic” France and Canada, have also profited enormously from this war, supplying the Saudis with mountains of offensive weapons.
These are the words and deeds of the so-called democratic West. Calling for democracy and freedom in their words, Western countries in reality supply arms and military equipment at every opportunity, thus fomenting military conflicts in which hundreds of thousands of people die in Yemen, Iraq, Syria, Afghanistan, and Libya. It makes one wonder where are the so-called international organizations which allegedly aim to prevent conflict and prosecute those who incite and encourage these bloody wars?
The United States, the skilled cheaters of double standards in politics and human rights, has once again manifested itself concerning Yemen. US Secretary of State Anthony Blinken has loudly reiterated that resolving the conflict in Yemen remains an alleged top priority of US foreign policy. These comments were made during a telephone conversation with the newly appointed United Nations Special Envoy for Yemen Hans Grundberg. And this was said at a time when the Pentagon was sending a new shipment of aerial bombs to Saudi Arabia, which the Saudis are actively using in their war against, as Riyadh says, “the fraternal Yemeni people.”
So far, only human rights groups have accused these countries of complicity in Saudi Arabia’s war crimes in Yemen. One investigation found that the bomb dropped from a Saudi warplane in August 2018, which hit a school bus and killed more than 40 children, came from the United States. But it was just one bomb, while Yemeni officials say most Saudi airstrikes have targeted residential areas, and all Saudi bombs and missiles are purchased abroad from “democratic” countries.
The head of the UN Children’s Agency also presented journalists with these grim figures on the suffering of Yemeni children, from malnutrition to education and sanitation. For example, he said: “Let me share a few more numbers: Four out of every five children need humanitarian assistance; that’s more than 11 million children, and 400,000 children suffer from severe acute malnutrition More than two million children are out of school. Another four million are at risk of dropping out. Two-thirds of teachers, more than 170,000, have not received a regular salary for more than four years. 1.7 million children are currently internally displaced because of violence. As the violence has intensified, especially in the Marib area, more and more families have fled their homes. A staggering 15 million people (more than half of them, about 8.5 million, are children) do not have access to safe water, sanitation or hygiene. With the current level of funding and without an end to the fighting, UNICEF will not be able to help all these children.” And he went on to predict a grim prognosis: “There is no other way to help them without a lot of international support, which will result in a large number of Yemeni children dying.”
But does it matter to the gentlemen in western capitals who make huge profits from the blood of Yemeni children and the supply of arms, which allows them to eat sweet and sleep well? It’s none of their business. As they usually say in the United States, it’s just business, nothing personal.
Despite the efforts of UNICEF and other international organizations, the severity of the humanitarian situation in Yemen cannot be overemphasized. The economy is in a critical state. GDP has fallen 40% since 2015 when neighboring Arab Saudi Arabia decided to punish Yemenis for their “disobedience.” Vast numbers of people lost their jobs, causing family incomes to plummet. About a quarter of people, including many health workers, teachers, engineers, and sanitation workers, rely on civil servants’ salaries that are paid irregularly, if at all. And while the displacement and destruction of schools have resulted in classrooms that can hold up to 200 children, teachers are showing up. Yes, unpaid teachers come in and teach on their enthusiasm to educate the next generation.
In addition to the Saudi-imposed war, with the US behind it, many Yemenis are starving not because there is no food but because there is not enough money to buy it. “But such people have no choice, which means they are forced to sell everything from jewelry to pots just to feed their own children,” writes Egypt’s Al-Ahram. “But their children continue to starve, as families end up selling off all their possessions and cannot buy simple food for themselves or their children.”
Economists believe that UNICEF alone urgently needs more than $235 million to continue its life-saving work in Yemen until mid-2022. Failure to do so will force the agency to reduce or terminate life-saving assistance to vulnerable children. “Funding is critical,” notes Al-Ahram. “We can draw a clear line between donor support and lives saved,” it adds. And perhaps the newspaper’s most emotional comment was the following: “Yemen is the most brutal place in the world to be a child. And, incredibly, it’s getting worse.”
Last month, the United Nations warned that 16 million Yemenis, more than half the population, are facing starvation. Unless the international community steps up support, food aid could soon dry up. Doctors warn that a staggering 99% of Yemenis have not been vaccinated against Covid-19. The country is now battling a third deadly wave of infections in which large numbers of people, especially children and the elderly, will die due to a lack of vaccines. How the West treats the suffering of Yemenis, who are direct co-conspirators in Saudi Arabia’s shameful war, was directly commented on by Yemen’s Al-Sahwa : “We need the promised vaccines, but it is also shameful that by buying up all the vaccines for themselves, rich countries like the UK and Germany are blocking all decisions to get the medicine we need into our country.”
Many countries worldwide are well aware of the plight of the Yemeni people, especially the children and elderly, and deplore the fact that Saudi Arabia still seeks a military solution to the Yemeni crisis, stating that this approach will lead to nothing but death and destruction. They have repeatedly called on Riyadh to abandon a military solution and instead seek political ways to end the devastating war in Yemen. Speaking at a briefing for journalists, Iranian Foreign Ministry spokesman Saeed Khatibzadeh said: “Unfortunately, the Saudi government is still looking for a military solution for Yemen, even though it knows and has understood after a long time that war has no other result than killing innocents and civilians, damaging the peoples of the region and security.” The sooner the Government of Saudi Arabia shows its commitment to political solutions and ends this destructive war, the better for the country and the region, as well as for the peace and security in the entire region.
A Canadian doctor pushing COVID-19 vaccine shots for children ages 5 years and up who’s been featured in numerous media reports received nearly $2 million in Pfizer funding for vaccine research.
Whether it was intentional or if the media kinda-sorta forgot to mention the conflict, or if they simply didn’t bother doing their own research before using Dr. Jim Kellner as a lead adviser on the COVID shot isn’t clear. But what is clear is that Pfizer has given the University of Calgary professor and pediatrician $1.9 million, with $787,004 of it still being allocated until 2022.
Kellner didn’t attempt to hide his conflict of interest; it’s easily found in his publicly posted curriculum vitae, with the current funding explicitly stated.
Yet, according to True North news, “Kellner’s name turns up over 41 times and appears in numerous videos and articles on the topic of vaccination without any indication of how much money he has received from the vaccine manufacturer Pfizer.”
“Liberal” MPs in Canada have expressed support for the government’s proposed internet censorship legislation. They went further to propose the appointment of a “Digital Safety Commissioner” who would be responsible for investigating complaints about “hurtful” content to be reported by users anonymously.
According to a report on Blacklock’s Reporter, Federal Liberal MPs have endorsed Trudeau’s internet censorship plans, on condition that there will be “proper due process” for those accused of posting “hurtful content.”
Liberal MP Nathaniel Erskine-Smith insisted that the government should “ensure that there is public process or due process.”He added: “Fundamentally we need a public due process system to manage takedown by large companies.”
Internet censorship and online harassment are some of the top things the Trudeau administration is focusing on. The government started with Bill C-10, which focused on policing “user-generated content” on social media platforms such as YouTube and TikTok. The bill did not pass before the end of the last parliamentary session because of opposition from conservatives.
Now Trudeau’s former Minister for Heritage Steven Guilbeault has proposed a new internet censorship bill. He said the new bill “is going to be controversial.”
“People think that C-10 was controversial. Wait until we table this legislation,” he added.
The new bill proposes social media companies to be held liable for “hurtful content” on their platforms. It also seeks to enable Canadians to anonymously complain about hurtful content to have it taken down.
However, the government is yet to define the term “hurtful.”
Under current laws, so-called “hate speech” is illegal.
Attacking the new bill, Conservative MP Michael Chong said: “I can say clearly that we don’t support censorship. We don’t support restrictions on freedom of the press.”
The Canadian Trucking Alliance (CTA) has warned of substantial “supply chain disruptions” if the US enforces vaccine passports at the border.
A few weeks ago, the US Department of Homeland Security announced a vaccine mandate for all international travel including truck drivers that will take effect in January. The announcement has been heavily criticized by cross-border truckers. According to Transportation Network, one executive in the Canadian trucking industry warned that the mandate would lead to a “disaster.”
This week, the CTA warned that the mandate would increase supply chain disruptions. Trucks facilitate about 70% of the $650 billion trade between Canada and the US. About 40,000 US drivers and 120,000 Canadian drivers operate in the cross-border trade between the two countries.
The CTA said that about 20% of drivers will stop cross-border operations once the vaccine mandate is enforced.
“CTA conservatively estimates that 20 percent of Canadian truck drivers crossing the border (22,000), and 40 percent of U.S. truck drivers (16,000), would almost immediately exit the Canada-US trade system should the vaccination mandate take effect in January 2022,” the organization said.
It called on both the US and Canadian governments to “reexamine appropriate mandate timelines for cross-border truck drivers.”
The group also argued that more time is needed to create a “seamless mutual system of identification for drivers” to avoid delays when drivers are showing proof of vaccination.
However, the Biden administration appears to be disregarding the warnings of “dire consequences” from leading truck organizations by proceeding with the vaccine passport plans.
Here come jabs in schools without parental consent.
“Bonnie J. Fraser Henry OBC FRCPC is a Canadian physician who is the Provincial Health Officer for British Columbia, the first woman in this position. Henry is also a clinical associate professor at the University of British Columbia. She was a family doctor and is a specialist in public health and preventive medicine.”
In fact, the politicians have worked on this for years, and enshrined it in legislation, she says.
Looks like you can garner lots of awards when your heart is a stone, Bonnie.
And, like Presidential wannabe Governor Cuomo, she even had time to write a book about her leadership in the pandemic, titled Be Kind, Be Calm, Be Safe. Do these people know what they are, or are they high on their own supply?
Here someone collected her telling the truth about masks last year and flip-flopping later:
Dr. Paul Alexander advocates for a complete change over of pandemic responders; to fire those who have failed us, stop shifting the blame to the public who have done their part, and elect qualified experts.
Rebel News: Telling the other side of the story. https://www.RebelNews.com for more great Rebel content.
YouTube is censoring conservative and independent voices. We don’t know how long we have left on YouTube. But you’ll always be able to find us at https://www.RebelNews.com
Unlike almost all of our mainstream media competitors, Rebel News doesn’t receive any government funding. We rely on our generous audience to help keep us reporting.
Please consider supporting Rebel News by making a donation, purchasing a RebelNews+ subscription, shopping in our online store, or any of the other methods below:
The Davos World Economic Forum (WEF) is a premier forum for governments, global corporations and international entrepreneurs. Founded in 1971 by engineer and economist Klaus Schwab, the WEF describes its mission as “shaping global, regional and industry agendas” and “improving the state of the world”. According to its website, “moral and intellectual integrity is at the heart of everything it does.”
The WEF has been involved in the coronavirus pandemic in several ways.
First, the WEF was, together with the Gates Foundation, a sponsor of the prescient “Event 201” coronavirus pandemic simulation exercise, held in New York City on October 18, 2019 – the same day as the opening of the Wuhan Military World Games, seen by some as “ground zero” of the global pandemic. China itself has argued that US military athletes may have brought the virus to Wuhan.
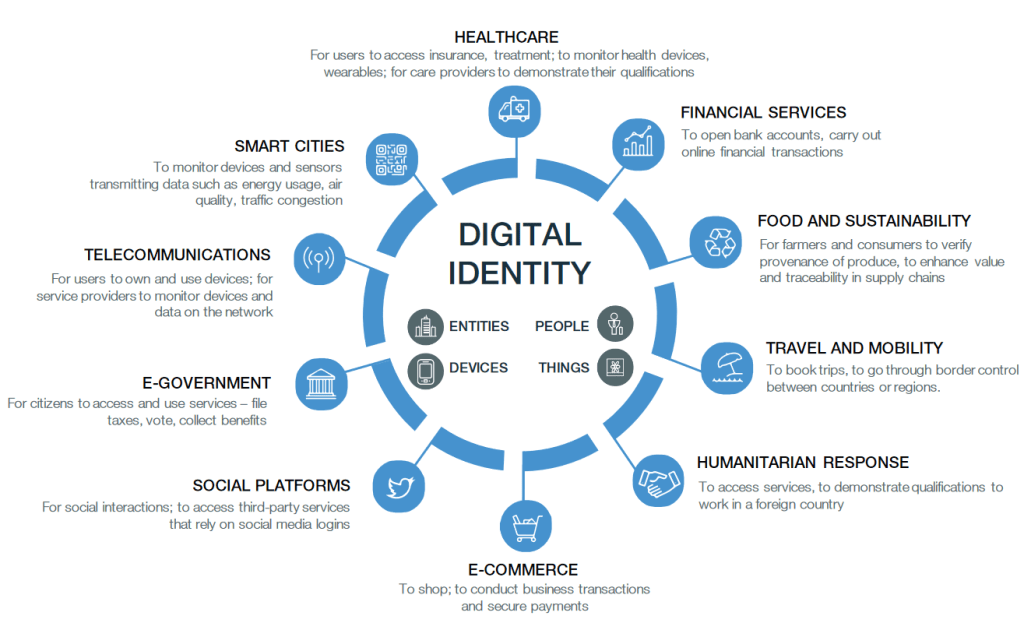
Second, the WEF has been a leading proponent of digital biometric identity systems, arguing that they will make societies and industries more efficient, more productive and more secure. In July 2019, the WEF started a project to “shape the future of travel with biometric-enabled digital traveler identity management”. In addition, the WEF collaborates with the ID2020 alliance, which is funded by the Gates and Rockefeller foundations and runs a program to “provide digital ID with vaccines”. In particular, ID2020 sees the vaccination of children as “an entry point for digital identity.”
Third, WEF founder Klaus Schwab is the author of the book COVID-19: The Great Reset, published in July 2020, which argues that the coronavirus pandemic can and should be used for an “economic, societal, geopolitical, environmental and technological reset”, including, in particular, advancing global governance, accelerating digital transformation, and tackling climate change.
Finally, the WEF has been running, since 1993, a program called “Global Leaders for Tomorrow”, rebranded, in 2004, as “Young Global Leaders”. This program aims at identifying, selecting and promoting future global leaders in both business and politics. Indeed, quite a few “Young Global Leaders” have later managed to become Presidents, Prime Ministers, or CEOs (see below).
During the coronavirus pandemic, several WEF Global Leaders and Global Shapers (a junior program of the Global Leaders) have played prominent roles, typically promoting zero-covid strategies, lockdowns, mask mandates, and ‘vaccine passports’. This may have been a (largely failed) attempt to protect public health and the economy, or it may have been an attempt to advance the global transformation agenda outlined above, or perhaps both.
In this regard, some notable Young Leaders include Jeffrey Zients (US White House Coronavirus Response Coordinator), Stéphane Bancel (CEO of Moderna), Jeremy Howard (founder of influential lobby group “Masks for All”), Leana Wen (zero-covid CNN medical analyst), Eric Feigl-Ding (zero-covid Twitter personality), Gavin Newsom (Governor of California, selected in 2005), Devi Sridhar (British zero-covid professor), Jacinda Ardern (Prime Minister of New Zealand), French President Emanuel Macron (selected one year prior to his election in 2017), Austrian Chancellor Sebastian Kurz, German Chancellor Angela Merkel (selected back in 1993), German Health Minister Jens Spahn, and former British Prime Minister Tony Blair (a leading proponent of ‘global vaccine passports’).
To get a full overview of their members, see Global Leaders for Tomorrow and Young Global Leaders on WikiSpooks (a Wiki focusing on covert power structures) as well as the official Young Global Leaders website. For an overview of some notable members in politics and the media, see below.
In conclusion, the Davos World Economic Forum has indeed been involved in the strategic management of the coronavirus pandemic, with a major emphasis on using the pandemic as a catalyst for digital transformation and the global introduction of digital identity systems.
Digital Identity: The vision of the World Economic Forum (WEF, 2018)
WEF “Young Global Leaders”
An overview of some WEF Young Global Leaders (2005-2021) and Global Leaders for Tomorrow (1993-2003) in politics and the media. The list is not exhaustive.
Jeffrey Zients (White House Coronavirus Response Coordinator since 2021, selected in 2003), Jeremy Howard (co-founder of lobby group “masks for all”, selected in 2013), California Governor Gavin Newsom (selected in 2005), Pete Buttigieg (selected in 2019, candidate for US President in 2020, US secretary of transportation since 2021), Chelsea Clinton (Clinton Foundation board member), Huma Abedin (Hillary Clinton aide, selected in 2012), Nikki Haley (US ambassador to the UN, 2017-2018), Samantha Power (US ambassador to the UN, 2013-2017, USAID Administrator since 2021), Ian Bremmer (founder of Eurasia Group), Bill Browder (initiator of the Magnitsky Act), Jonathan Soros (son of George Soros), Kenneth Roth (director of “Human Rights Watch” since 1993), Paul Krugman (economist, selected in 1995), Lawrence Summers (former World Bank Chief Economist, former US Treasury Secretary, former Harvard University President, selected in 1993), Alicia Garza (co-founder of Black Lives Matter, selected in 2020), Stéphane Bancel (Moderna CEO).
Media
CNN medical analyst Leana Wen (selected in 2018), CNN chief medical correspondent Sanjay Gupta, Covid Twitter personality Eric Feigl-Ding (a ‘WEF Global Shaper‘ since 2013), Andrew Ross Sorkin (New York Times financial columnist), Thomas Friedman (New York Times columnist, selected in 1995), George Stephanopoulos (ABC News, 1993), Lachlan Murdoch (CEO of Fox Corporation).
Technology and Social Media
Microsoft founder Bill Gates (1993), former Microsoft CEO Steven Ballmer (2000-2014, selected in 1995), Amazon founder Jeff Bezos (1998), Google co-founders Sergey Brin and Larry Page (2002/2005), former Google CEO Eric Schmidt (2001-2017, selected in 1997), Wikipedia co-founder Jimmy Wales (2007), PayPal co-founder Peter Thiel (2007), eBay co-founder Pierre Omidyar (1999), Facebook founder and CEO Mark Zuckerberg (2009), Facebook COO Sheryl Sandberg (2007).
Great Britain, Canada, New Zealand
Professor Devi Sridhar (a leading ‘zero covid’ proponent, selected in 2020/21), former British Prime Ministers Tony Blair and Gordon Brown (both selected in 1993), BBC World Service journalist Dawood Azami, Lynn Forester de Rothschild (co-owner of The Economist), Nathaniel Rothschild (son of Lord Rothschild), historian Niall Ferguson (selected in 2005), William Hague (Foreign Secretary, 2010-2014), Charles Allen (CEO of ITV, 2004-2007; Chairman of EMI, 2008-2010).
New Zealand Prime Minister Jacinda Ardern (since 2017, selected in 2014), Canadian Deputy Prime Minister Chrystia Freeland (selected in 2001; former managing director of Reuters). Canadian Prime Minister Justin Trudeau is a WEF participant, but is not a confirmed Young Global Leader.
Germany
Chancellor Angela Merkel (selected in 1993, 12 years before becoming Chancellor), current Health Minister Jens Spahn and former Health Ministers Philipp Roesler and Daniel Bahr, current co-chair of the Green Party and failed Chancellor candidate Annalena Baerbock (selected in 2020), former co-chair of the Green Party Cem Özdemir (selected in 2002), media mogul and Axel Springer CEO Mathias Doepfner (selected in 2001), talk show host Sandra Maischberger, late Foreign Minister and Vice Chancellor Guido Westerwelle (1997), former German President Christian Wulff (selected in 1995, 15 years before becoming President), Reto Francioni (former CEO of Deutsche Boerse).
European Union
EU Commission Presidents Jose Manuel Barroso (2004-2014, selected in 1993) and Jean-Claude Juncker (2014-2019, selected in 1995), French President Emanuel Macron (since 2017, selected in 2016), former French President Nicolas Sakozy (2007-2012, selected in 1993), Austrian Chancellor Sebastian Kurz, former Italian Prime Minister Matteo Renzi (2014-2016, selected in 2012), former Spanish Prime Minister Jose Maria Aznar (1996-2004, selected in 1993), Klaus Regling (CEO of the European Financial Stability Mechanism since 2012), Guy Verhofstadt (former Belgian Prime Minister, Chair of the Brexit Steering Group), Danish Minister for the Environment Lea Wermelin, Finnish Prime Minister Sanna Marin, former Finnish Prime Minister Alexander Stubb, and Mark Leonard (founding director of the Soros-funded European Council on Foreign Relations).
Switzerland
Natalie Rickli (Director of Health of the Canton of Zurich, selected in 2012), former Presidents of the Swiss National Council Christa Markwalder (selected in 2011) and Pascale Bruderer-Wyss (selected in 2009), Geneva politician Pierre Maudet (selected in 2013), NZZ media group CEO Felix R. Graf (selected in 2007), former Swiss Justice Minister Ruth Metzler (selected in 2002), former Swiss television CEO Roger de Weck (2011-2017, selected in 1994), former UBS CEOs Peter Wuffli (selected in 1994) and Marcel Rohner (selected in 2003), former Credit Suisse CEO Tidjane Tiam (1998).
Video Annex
1) Bill Gates demanding “digital immunity proof” in March 2020
2) Edward Snowden warning of the “destruction of rights” (March 2020)
CALGARY: The Justice Centre today responded to the federal government announcement that unvaccinated Canadians will lose their right to move and travel freely within Canada, their right to leave Canada, and their right to earn a living and participate in society without discrimination.
“The government is seeking to have 100% of Canadians injected with the experimental mRNA vaccine, which has not been subjected to any long-term testing on humans,” states lawyer John Carpay, President of the Justice Centre.
With the Canada-U.S. land border closed to non-essential travel, this Covid-19 vaccine travel mandate will effectively prevent unvaccinated people from leaving Canada in any way. In addition to denying unvaccinated Canadians the right to travel by plane or train, the federal government has also announced that federal employees and contractors will lose their jobs unless they participate in the world-wide experiment with new mRNA vaccines.
“We were recently promised, this past summer, that life would go back to normal once 70% of Canadians were injected with mRNA. This high vaccination rate has been achieved but has not stopped the spread of the virus. The new mRNA vaccine also provides no guarantee against the Delta variant,” continues Mr. Carpay.
According to media reports, Prime Minister Trudeau declared that these discriminatory measures against unvaccinated Canadians are needed to keep people “safe,” including children.
“Government data and statistics from every Canadian province, and from countries around the world, tell us that children, teenagers and young adults face no serious threat from Covid, which makes the Prime Minister’s rhetoric about saving children highly misleading,” continues Mr. Carpay.
“Medical reports and scientific studies make it clear that both vaccinated and unvaccinated people spread Covid-19. There is no scientific basis for turning unvaccinated Canadians into second-class citizens,” stated Allison Pejovic, Justice Centre Staff Lawyer.
Currently, Canada’s provincial and federal governments accept two injections as enough to qualify for “full” vaccination. But this may soon change to requiring three, four and more injections to maintain one’s legal status as “fully” vaccinated, as has been demonstrated in Israel and the Netherlands.
“Governments throughout history have used the notion of ‘science’ to support their policies, along with various appeals to public health, safety, security, morality, and so on. No government will violate human rights without putting forward a good-sounding justification, such as the war on terrorism, communism, online hate, drugs, or a nasty virus,” continues Mr. Carpay.
The government’s own data and statistics tell us that Covid is much closer to the annual flu than to the Spanish Flu of 1918. This matters because the entire world was put into a state of panic by the dire predictions of Dr. Neil Ferguson of Imperial College, who claimed in March of 2020 that Covid would be like the Spanish Flu of 1918, killing tens of millions of people.
“Canada’s vaccine passports, and the creation of first-class and second-class citizenship, are founded on Neil Ferguson’s demonstrably false claim that Covid is an unusually deadly killer,” states Mr. Carpay.
“Covid is real. Fear of Covid is wildly exaggerated. Over the past 18 months, government-funded media have been very successful in persuading the majority that vaccine passports (and lockdown policies preceding them) are based on science. When people hear a message thousands of times, they believe it to be true,” continues Mr. Carpay.
“The Justice Centre is profoundly disturbed that these federal mandates will prevent unvaccinated Canadians from leaving the country. Such a mandate is an egregious and unacceptable infringement of Canadians’ constitutionally protected mobility rights. There is no scientific justification for this,” concludes Ms. Pejovic.
These new government restrictions on civil liberties are still announcements at this stage, and no law has been passed by Parliament or by way of cabinet regulation (Order-in-Council). So, no legal challenge is possible at this time. If the government intends to implement these vaccine travel mandates and give them the force of law, these policies can then be challenged in court.
In Oakville, Ontario in Canada, engaged couples will have to show a vaccine passport to attend a meeting for a marriage license. The only way around the requirement is to get married in a different town.
“Appointments for marriage licenses and ceremonies that have already been booked prior to September 22 will not require proof of full vaccination,” the city website says. “…however, any new appointments for marriage licences and ceremonies will be required. Ceremonies will be held inside town hall as of November 4, 2021.”
A marriage license is a requirement to be recognized as legally married in Canada. In Oakville, a marriage license cannot be obtained online.
“You must schedule an appointment to receive your marriage licence,” the city’s website says. “To be eligible for an appointment, please ensure that the intended date of your marriage is finalized and you have an officiant that has agreed to perform the marriage.”
Additionally, a couple might not get married if they do not pass a screening at the city’s building.
“When you arrive at Town Hall for your scheduled appointment, you will be required to complete a COVID-19 self-assessment,” the city said. “If you do not successfully meet the screening criteria, you will not be allowed to enter the building and your appointment will be canceled.”
The city’s requirement for proof of vaccination for marriages is in line with the vaccination mandate implemented in Ontario last month.
Three US medical certifying boards have warned doctors that they risk losing their certification and licence if they spread covid vaccine misinformation.
Internists, family doctors, and paediatricians received an email on 9 September that quoted a warning from the Federation of State Medical Boards in July1 which read: “Providing misinformation about the covid-19 vaccine contradicts physicians’ ethical and professional responsibilities, and therefore may subject a physician to disciplinary actions, including suspension or revocation of their medical licence.”2
Richard Baron, president and chief executive of the American Board of Internal Medicine (ABIM), told The BMJ that the move was an attempt to establish a standard of care. “As standard setting organisations, we thought it was important to be on record, in a public way, to make clear that putting out flagrant misinformation is unethical and dangerous during a pandemic.” Baron said that the statement has been well received—“4 to 1 positive.” But community physicians contacted by The BMJ thought differently.
“When I got that email I thought I’d better not put anything on social media about vaccines,” said Shveta Raju, a community physician in the Atlanta, Georgia, area, who has treated covid patients and led the vaccination effort at her outpatient clinic.
“The email was sent more as a veiled threat to keep doctors on the official, established narrative, and that’s what I find chilling,” said a paediatrician who pseudonymously blogs under the name Elizabeth Bennett. “Pandemic or no, there is a problem with having an ill defined concept of misinformation that’s tied to public health messaging that hasn’t been consistent. How are physicians supposed to figure out what is misinformation when public health messaging swings so wildly?” Bennett asked.
Undefined offence
Baron said that the statement was also intended to signal the certifying boards’ support for physicians “trying to do the right thing.”
“We wanted to support that group and say ‘hey, we do have a standard of care here and you are doing the right thing when you uphold it,’” he said.
Raju responded, “If that was their intent, they should have defined misinformation. By leaving it undefined, the message was that we can’t talk about this at all.” She said that physicians are, by and large, a conservative group. “If they’re not sure what can be deemed misinformation, physicians would rather be quiet.”
Bennett concurred: “The thing I find most alarming is that they don’t define misinformation, but if they strip you of your board certification, you would lose your means of earning a living.”
Doctors spreading misinformation?
Official and social media company efforts to target “vaccine misinformation” predate the pandemic.3 But the new statement from ABIM, the American Board of Family Medicine, and the American Board of Paediatrics is one of several recent statements putting doctors in the spotlight for the first time.
In Canada, warnings about physician information began earlier, when in April the College of Physicians and Surgeons of Ontario declared that physicians “have a professional responsibility not to communicate anti-vaccine, anti-masking, anti-distancing, and anti-lockdown statements or promote unsupported, unproven treatments for covid-19.”4
The Canadian statement triggered an outcry, leading to a clarification that the statement was “not intended to stifle a healthy public debate about how best to address aspects of the pandemic.” But concerns continued. In June, a Canadian member of parliament held a press conference on censorship of Canadian clinicians and scientists. YouTube removed the video of the meeting.56
The BMJ asked ABIM about the size of the problem of board certified physicians spreading misinformation.
“We don’t have a sense of numbers of physicians spreading misinformation,” Baron said. “We’re at the beginning.” He believed it was only a “small number of doctors.” The medical boards opted to send the statement to all doctors, he said, because focusing on just the offending individuals would “miss the impact they’re having because of how much their voices are being amplified.”
As an example of “unprofessional or unethical behaviour,” Baron cited the case of a Florida doctor offering medical exemptions from mask wearing for $50 (£37; €43).7
Personalised medicine—or one-size-fits-all?
The BMJ asked whether physicians expressing doubt about the need for booster doses or vaccination of patients with natural immunity—two matters that have been the subject of debate and changing official guidance—would qualify as misinformation.8 “I don’t think we have concerns with doctors wrestling with areas where the science is unclear,” Baron said, “but there is no debate about whether people should get a primary vaccination series.”
Raju worries about the impact on personalised care. “The job of physicians is to take guidelines and apply them to the patient in front of them.” But now “physicians are basically being told that when it comes to covid vaccines it’s one-size-fits-all.”
Baron said, “We’re not trying to stifle conversations between doctors and patients. We understand that different people may look at evidence in different ways, but when you have an overwhelming preponderance of medical consensus in a certain area, you need at least to tell patients that there is an overwhelming professional consensus here.”
Cautious approach
Jeffrey Flier, former dean of Harvard Medical School, said that in the context of the pandemic, he was “not opposed to certain levels of misinformation triggering a decision to question somebody’s licence.” He said, “I can see this being an appropriate remedy at a time of public health emergency.
“But this is not how the system for licensure and certification has traditionally worked, and creates many opportunities for mistaken judgment about what is and is not misinformation, and those decisions would have to be rendered with extreme caution.”
Flier added, “We have to remember that there are legitimate areas of debate, and such matters should not fall within the scope of disciplinary actions.”
“There are reasons to be concerned that state boards might be unprepared for these kinds of decisions at a time when so many aspects of covid policy have been enmeshed with political views.”
Footnotes
This article was updated on 4 October to make clear that it was medical certifying boards, rather than licensing boards, that emailed physicians. The email quoted an earlier warning from the Federation of State Medical Boards.
Competing interests: PD gave a public statement at a 17 September 2021 FDA advisory committee to discuss covid-19 vaccines, where he highlighted the joint statement. The views and opinions expressed here are those of the author and do not necessarily reflect official policy or position of the University of Maryland.
Provenance: commissioned; not externally peer reviewed.
This article is made freely available for use in accordance with BMJ’s website terms and conditions for the duration of the covid-19 pandemic or until otherwise determined by BMJ. You may use, download and print the article for any lawful, non-commercial purpose (including text and data mining) provided that all copyright notices and trade marks are retained.
By Maryanne DemasiMaryanne Demasi | Brownstone Institute | June 15, 2026
For decades, vaccines have been treated as the sacred cow of modern medicine. I was taught that they were the holy grail. To question them was heresy. To raise concerns about safety was to risk professional exile.
“No child should be sacrificed on the altar of the religion of vaccines,” Siri writes, as he turns his focus to America’s overcrowded childhood immunisation schedule.
I assumed little in this book would surprise me. I’ve spent years reporting on drug safety, regulatory capture, and the corruption of science. But Siri showed me how wrong I was.
Siri is not a doctor or a scientist. He is an attorney, and this, he says, is his advantage. In court, rhetoric won’t save you. Evidence does. As he puts it, he doesn’t get to say “trust me” the way many doctors do. “I need to prove claims with real data.”
This site is provided as a research and reference tool. Although we make every reasonable effort to ensure that the information and data provided at this site are useful, accurate, and current, we cannot guarantee that the information and data provided here will be error-free. By using this site, you assume all responsibility for and risk arising from your use of and reliance upon the contents of this site.
This site and the information available through it do not, and are not intended to constitute legal advice. Should you require legal advice, you should consult your own attorney.
Nothing within this site or linked to by this site constitutes investment advice or medical advice.
Materials accessible from or added to this site by third parties, such as comments posted, are strictly the responsibility of the third party who added such materials or made them accessible and we neither endorse nor undertake to control, monitor, edit or assume responsibility for any such third-party material.
The posting of stories, commentaries, reports, documents and links (embedded or otherwise) on this site does not in any way, shape or form, implied or otherwise, necessarily express or suggest endorsement or support of any of such posted material or parts therein.
The word “alleged” is deemed to occur before the word “fraud.” Since the rule of law still applies. To peasants, at least.
Fair Use
This site contains copyrighted material the use of which has not always been specifically authorized by the copyright owner. We are making such material available in our efforts to advance understanding of environmental, political, human rights, economic, democracy, scientific, and social justice issues, etc. We believe this constitutes a ‘fair use’ of any such copyrighted material as provided for in section 107 of the US Copyright Law. In accordance with Title 17 U.S.C. Section 107, the material on this site is distributed without profit to those who have expressed a prior interest in receiving the included information for research and educational purposes. For more info go to: http://www.law.cornell.edu/uscode/17/107.shtml. If you wish to use copyrighted material from this site for purposes of your own that go beyond ‘fair use’, you must obtain permission from the copyright owner.
DMCA Contact
This is information for anyone that wishes to challenge our “fair use” of copyrighted material.
If you are a legal copyright holder or a designated agent for such and you believe that content residing on or accessible through our website infringes a copyright and falls outside the boundaries of “Fair Use”, please send a notice of infringement by contacting atheonews@gmail.com.
We will respond and take necessary action immediately.
If notice is given of an alleged copyright violation we will act expeditiously to remove or disable access to the material(s) in question.
All 3rd party material posted on this website is copyright the respective owners / authors. Aletho News makes no claim of copyright on such material.