It can be difficult to keep up with the CDC’s ever-changing COVID-19 booster recommendations, but what is consistent is that the number and frequency of boosters are continually increasing and data supporting these recommendations keeps decreasing. At one point, even mainstream media called out the CDC for the lack of data for these recommendations.
To pin down the CDC on one of its recommendations, in April 2022, ICAN asked the CDC to produce its data that support the efficacy of COVID-19 boosters for 12-49 year olds. The response? Shocking.
The CDC admitted that “A search of our records failed to reveal any documents pertaining to your request.” None. Not one record. Not one study. This means the CDC did not have any data to back up its claims or recommendations for boosters in this age group.
For anyone that has looked at the data regarding boosters, the CDC’s response is unsurprising because study after study shows that repeated boosters increase the chances of contracting COVID-19 disease. For example, as a recent Cleveland Clinic study showed (see Figure 2 in the study), the chances of contracting COVID-19 increase with each additional dose of COVID-19 vaccine.
The above is another piece of evidence in ICAN’s snowballing work to hold our “health” agencies accountable for every unsupported recommendation and false claim made to the public.
See below for more instances where ICAN uncovered “health” agencies making unsupported claims to the public:
Substack All-Star Igor Chudov just published another important article. This article asks if the CDC was lying all along about “vaccine effectiveness?”
My question (and it’s a serious one) is this: Can someone name ONE pronouncement of CDC officials that either wasn’t a lie or of highly-dubious veracity?
Partial List of Lies …
Per my assessment, the CDC and other national public health agencies and their key experts …
Lied about there being no evidence of early cases in America.
Lied when they said there was no possibility this virus leaked from a lab.
Lied about the effectiveness of masks.
Lied when they said the virus could be spread on physical surfaces.
Lied when they said it would take only two weeks to “flatten the curve.”
Lied when they said that virus transmission could easily happen outside.
Lied about the stats of “cases” and “deaths.”
Lied about the mortality risk to children and healthy young adults.
Lied about ivermectin and HCQ being worthless drugs for treatment.
Lied about remdesivir being a safe drug.
Lied about the vaccines being “safe and effective.”
Lied when they labeled these shots as “vaccines.”
Lied about the “vaccines” and boosters preventing “severe” cases and deaths.
Lied about the necessity or importance of testing people (including the asymptomatic) over and over.
Lied when they attacked and sought to censor people who were telling the truth.
Lied when they “adjusted” estimates of ILI in the Flu Season of 2019-2020 … to make it seem this flu season did not produce “widespread” and “severe” ILI (Covid?) outbreaks.
Before Covid, lied about the effectiveness of the flu vaccines.
A few other questions …
Do liars continue to lie? Will liars lie again?
Do liars often try to cover-up their lies?
Do liars in positions of great power often attack people who try to expose their lies?
Is it smart to continue to trust proven or known liars?
How many lies does some person or agency have to tell before people start to realize they are listening to a liar?
Eight leading critics of the United States’s COVID-19 response have called for an investigation of the many failures of policy architects and key decision makers — at institutions ranging from the Centers for Disease Control and Prevention and Food and Drug Administration to universities and hospitals — over their repeated mishandling of the pandemic.
Given the immense harm inflicted on our society by the follies of a ruling class and their expert advisers who never failed to make a wrong decision when presented with the opportunity, as well as the fact that lives are still being destroyed by their lingering policies, we can only hope this blueprint does not go ignored.
Dubbing themselves the “Norfolk Group,” the association of scholars includes such prominent names as Stanford epidemiologist Jay Bhattacharya, Harvard epidemiologist Martin Kulldorff, UCSF physician Tracy Beth Høeg, Johns Hopkins University surgeon Marty Makary, and Indiana University School of Medicine immunologist Steven Templeton.
According to the Norfolk Group’s website, although initially organized by the Brownstone Institute in May 2022, the eight members of the group have since worked free from outside influence to draft the 80-page document they published earlier this year, “Questions for a COVID-19 Commission.”
Presented as a series of summaries and questions pertaining to key elements of U.S. COVID policy, the document, in effect, lays out a thorough indictment of the consistent incompetence of our ruling class while also raising concerns over the possible influence on policy by special interests such as teachers unions and drug companies.
Regarding natural immunity, the authors ask, “Why did the CDC downplay infection-acquired immunity, despite robust evidence for it?”
In respect to school closures, they ask, “Why were schools and universities closed despite early evidence about the enormous age-gradient in COVID-19 mortality … and early evidence that school closures would cause enormous collateral damage to the education and mental health of children and young adults?”
On that matter, they also wonder, “Why did the CDC incorporate policy language proposed by leaders of teachers unions on the scientific and public health aspects of school reopening without soliciting expertise of outside scientists in public health, infectious diseases, or other related fields?”
When discussing lockdowns, they inquire, “Why was so much influence on public health policy accorded to Drs. [Francis] Collins and [Anthony] Fauci? They control the largest source of infectious disease research funding in the world. How many infectious disease scientists, who should have been strong voices during the pandemic, kept quiet for fear of losing the research funding on which their livelihood depends?”
In their section on epidemiologic modeling, they demand, “Why did world leaders overly rely on models that made unverified assumptions about the pandemic’s trajectory rather than trying to verify these assumptions and their implications?”
When addressing COVID-19 vaccines, they raise questions such as, “Why did many organizations continue with mandates through summer and fall of 2021, despite data demonstrating both waning efficacy of symptomatic infection and reduced long term ability to curb viral spread?”
Regarding masks, they state, “Prior to the COVID-19 pandemic, the evidence that masks did little if anything to stop the spread of respiratory viruses was uncontroversial,” before summarizing a few studies demonstrating this and asking the obvious: “[W]hy did public health officials and agencies promote the idea that masks would be effective against SARS-CoV2?”
In its entirety, the Norfolk Group’s “Questions for a COVID-19 Commission” serves as a blueprint for the kind of investigation our country needs. Just don’t expect the Biden administration to do anything about it.
Daniel Nuccio holds master’s degrees in both psychology and biology. Currently, he is pursuing a PhD in biology at Northern Illinois University studying host-microbe relationships. He is also a regular contributor to The College Fix where he writes about COVID, mental health, and other topics.
Pfizer missed a deadline to turn over internal studies on myocarditis, per an FDA order. The deadline came and went. Now, they quietly have a new date in June. Why the delay on such important data? And, why does the FDA set arbitrary deadlines which aren’t enforced?
As Biden announces the coming end of the Covid Public Health Emergency in the US, the new majority in Congress appear to not be letting agencies off the hook. The past three years of remarkably poor public health policy have placed the CDC, WHO, and Social Media companies in the sights of numerous committee investigations, and new legislation seeking answers and medical freedom.
Airline pilot and co-founder of US Freedom Flyers, Josh Yoder, and Clinical Cardiologist, Dr. Thomas Levy, join Del to discuss the recent FAA change to the heart test limits and the coincidental timing of the change coming amid increasing concerns over myocarditis from the COVID-19 vaccine.
The CDC’s information page on Covid-19 vaccines contains the following bullet points on “How mRNA COVID-19 vaccines work:”
First, mRNA COVID-19 vaccines are given in the upper arm muscle or upper thigh, depending on the age of who is getting vaccinated.
After vaccination, the mRNA will enter the muscle cells. Once inside, they use the cells’ machinery to produce a harmless piece of what is called the spike protein…. After the protein piece is made, our cells break down the mRNA and remove it, leaving the body as waste.
Or, in other words, as we have long been told, “it” – the mRNA – “stays in the arm.” And then, after having instructed the muscle cells to produce the spike, is disposed of.
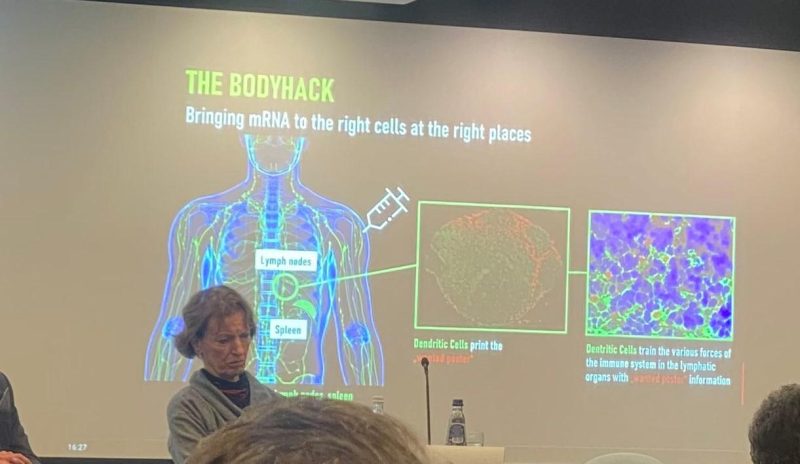
But look at the below picture from a recent presentation on mRNA vaccination at the European Parliament. The picture was posted on Twitter by Virginie Joron, a French member of the parliament. The speaker is no less an authority than Özlem Türeci, the Chief Medical Officer of BioNTech: the German biotech company that developed what has come to be known to most of the world as the “Pfizer” Covid-19 vaccine.
Have a closer look at Türeci’s slide, which tells a very different story than that which the CDC has been telling Americans for the last two years.
Far from “staying in the arm” and entering the muscle cells at the injection site, the injection site is only the point of departure for a journey that is supposed to take the mRNA rather to the lymph nodes. The subtitle of the slide is “Bringing mRNA to the right cells at the right places.” The deltoid is not the right place; the lymph nodes are.
Once in the lymph nodes, a specific sort of cell, the dendritic cells, is supposed to manufacture the spike protein: here colorfully described as the “wanted poster” that will help the immune system to identify the SARS-CoV-2 virus in case of subsequent exposure.
A passage from The Vaccine, the book that Türeci and her husband, BioNTech CEO Ugur Sahin, wrote which journalist Joe Miller, explains why BioNTech’s platform specifically targets the lymph nodes:
What Ugur learnt was that the location to which a vaccine delivers its ‘wanted poster’ really mattered. The reason for this, the couple’s team in Mainz later realised, was that not all dendritic cells … were created equal. The ones that resided in lymph nodes – of which the spleen is the largest – were particularly adept at capturing mRNA and making sure the instructions it carried were acted upon. These kidney-bean shaped organs, found under our armpits, in our groins, and at several other outposts in the body, are the information hubs of the immune system. (p. 98)
Indeed, Sahin and Türeci were so determined to get their mRNA into the lymph nodes that they had an earlier mRNA construct injected directly into the patient’s lymph nodesin the groin (p. 104).
Needless to say, such an approach was not likely to obtain wide acceptance as a vaccine! This is why the couple, as explained in their book, needed to package the mRNA in lipid nanoparticles, in order to ensure that mRNA administered by way of an intramuscular injection would, nonetheless, be widely distributed around the body and thus reach the lymph nodes.
This is to say that the wide biodistribution of the mRNA that came to light after rollout was never a bug. It is a feature of BioNTech’s mRNA technology. Having elicited an immune response by way of injection into the groin, Sahin is even said to have wondered, “How substantial could the immune response be if a vaccine got into all lymphatic tissues around the body, and recruited all the resident DCs [dendritic cells] into action?” (p. 105)
So, why has the CDC been lying about this for the last two years and insisting that the mRNA “stays in the arm?” Well, the obvious answer is that the idea of the mRNA staying at the injection site is reassuring, since otherwise we could fear systemic adverse effects of precisely the sort that have emerged since rollout.
It is worth noting, moreover, that in developing its vaccine, as discussed in my earlier article here, BioNTech simply skipped the so-called safety pharmacology studies whose purpose is precisely to test a candidate vaccine for potential systemic adverse effects – and regulators, including the FDA, let the company do it.
Robert Kogon is a pen name for a widely-published financial journalist, a translator, and researcher working in Europe.Follow him at Twitter here. He writes at edv1694.substack.com.
The Centers for Disease Control and Prevention (CDC) on Thursday added COVID-19 vaccination to its routine immunization schedule for children and adults.
Although the CDC does not have the authority to set requirements itself, the agency’s immunization schedule provides formal guidance for state and local public health officials who set the rules for which vaccines are required to attend school.
The schedule also is the basis for vaccine recommendations made by most physicians.
“Given all that we have learned about the dangers and ineffectiveness of COVID-19 shots over the last two years, it is horrifying to see the CDC now recommend this as a routine shot to children,” Mary Holland, Children’s Health Defense (CHD) president and general counsel told The Defender.
“Although it is unsurprising given the agency capture, it is nonetheless tragic,” she added.
Under the new guidelines, the CDC recommends healthy children 6 months to 11 years old receive a primary series of two doses of the mRNA Moderna or Pfizer-BioNTech monovalent COVID-19 vaccine, followed by a booster of the bivalent shot.
It recommends that healthy people age 12 and older receive two doses of either the Moderna, Pfizer or Novavax vaccine followed by a bivalent booster.
All COVID-19 vaccines being administered in the U.S. to people under 18 are Emergency Use Authorized (EUA) products. The U.S. Food and Drug Administration (FDA) did grant full approval to Pfizer’s Comirnaty COVID-19 vaccine for ages 12 and older, however, the Comirnaty vaccine is not available in the U.S. — which means all children who get the Pfizer vaccine are getting an EUA product.
In Wednesday’s congressional hearing on the Biden administration’s response to COVID-19, Rep. Dan Crenshaw (R-Texas) asked CDC Director Dr. Rochelle Walensky, why the CDC broke with its own norms and put an EUA vaccine on the childhood immunization schedule for a disease that poses very little risk to children and for which the vaccine poses many potential side effects without preventing transmission.
Walensky responded:
“The reason that the ACIP [Advisory Committee on Immunization Practices] recommended the CDC put the COVID-19 vaccine on the pediatric schedule was only because it was the only way it could be covered in our ‘Vaccines for Children’ program.
“It was the only way that our under-uninsured children would be able to have access to the vaccines … That was the reason to put it there.”
Data collected by the CDC through its Vaccine Adverse Event Reporting System (VAERS) and a growing number of other sources indicate serious health risks associated with COVID-19 vaccination for children.
“The COVID vaccines have not been shown to be either effective or safe for children,” CHD argued in an amicus brief filed in Louisiana last year. “The benefits to children are minuscule, while the risks — including the risk of potentially fatal heart damage — are ‘known’ and ‘serious,’ as the FDA itself has acknowledged.”
Other changes to the childhood schedule include adding the PVC15 shot, a pneumococcal conjugate vaccine used to help protect against pneumococcal bacteria and only recently approved for children; updated guidance for the flu and hepatitis B vaccines; and new recommendations for the measles, mumps and rubella (MMR) and polio vaccines.
The CDC now recommends an additional dose of the MMR vaccine in places where there is a mumps outbreak. It also recommends an additional poliovirus vaccine for children and adults if new polio cases emerge.
This would mean the childhood vaccination schedule would increase the number of recommended injections from 54 to 72 over the course of a person’s childhood, between the ages of 6 months and 18 years, The Defender reported last year.
CDC schedule protects pharmaceutical companies from liability for vaccine injuries
Vaccine makers are not liable for injuries or deaths associated with EUA vaccines but can be held liable for injuries caused by a fully licensed vaccine — unless that vaccine is added to the CDC’s childhood vaccination schedule.
Parents of children injured by vaccines listed on the childhood schedule can seek compensation through the taxpayer-funded National Vaccine Injury Compensation Program (NVICP), a no-fault alternative to the traditional legal system for resolving vaccine injury claims.
However, the revisions voted on by the ACIP committee last year explicitly state (slide 24) that the pneumococcal polysaccharide vaccine (PPSV23) and COVID-19 vaccines are not covered under the NVICP.
Instead, the COVID-19 vaccines added to the childhood schedule will remain covered by the Countermeasures Injury Compensation Program (CICP). To date, only 19 claims related to COVID-19 filed with the CICP have been found eligible for compensation, though no compensation has yet been paid.
Since it was established in 2010, the CICP only compensated 30 of the nearly 12,000 claims filed.
Are we seeing ‘the beginning of the end of Big Pharma’s reign’?
The addition of the COVID-19 vaccine to the immunization schedule “helps ‘normalize’ this vaccine and sends a powerful message to both healthcare providers and the general public that everyone ages 6 months and older should stay up to date with recommended COVID-19 vaccines (including a booster, when eligible), just as they would with any other routinely recommended vaccine,” Dr. Neil Murthy and Dr. A. Patricia Wodi said in a statement reported by CNN.
This “normalization” comes at a time when over 85% of the U.S. population hasn’t been boosted, despite the massive government-sponsored media push.
Nationally, only 12% of children ages 6 months to 4 years have received one dose of the vaccine. Only 58% of children ages 12 to 17 and 32% of children ages 5 to 11 have received two doses of the vaccine. Numbers vary widely across states.
Holland commented on the implications of adding this shot to the schedule:
“The childhood schedule is already unscientific and unjustifiable. Adding this shot may well be the straw that breaks the camel’s back. Parents are likely to resist, finally calling the entire childhood vaccine schedule into question.
“That day has been long in coming, but it is now here. I believe we are now watching the beginning of the end of Big Pharma’s reign over the nation’s children.”
At Wednesday’s congressional hearing, lawmakers repeatedly raised concerns about how regulatory agencies’ flawed recommendations led to a lack of confidence in public institutions.
Rep. Cathy McMorris Rodgers (R-Wash.) said, “There’s serious distrust today with our public health agencies. [Polling indicates] 40% of the public does not trust our public health agencies to handle the next public health emergency.”
Walensky indicated that vaccination rates for all vaccines on the childhood schedule among kindergarten children declined last year, dropping from 95% to 93% over the last two years, amounting to hundreds of thousands of parents opting not to comply with the childhood vaccination schedule.
VAERS is the primary government-funded system for reporting adverse vaccine reactions in the U.S. While reports submitted to VAERS require further investigation before a causal relationship can be confirmed, VAERS historically has been shown to report only 1% of actual vaccine adverse events.
According to Retsef Levi, Ph.D., with the Massachusetts Institute of Technology, the vaccines “cause unprecedented levels of harm, including the death of young people and children.”
Multiple studies have determined that the vaccines increase the risk of myocarditis and pericarditis, particularly in young men.
An October 2022 study revealed the CDC was aware of the safety signal for these side effects months before it informed the public.
At the recent FDA vaccine advisory committee meeting, several committee members also raised concerns about recommending annual bivalent boosters for children given the lack of data.
Dr. Archana Chatterjee, Ph.D., committee member and dean of the Chicago Medical School and vice president for medical affairs at Rosalind Franklin University said:
“As we look at this question [simplifying the vaccination schedule] for young children, the data is just too few for us to really make scientifically sound decisions regarding this question. The trial data need to be much more robust than we have seen in the past.”
In light of data like this, vaccination for COVID-19 for children and healthy people is losing public and even governmental support in some places.
Under public pressure and facing a series of lawsuits, last week California dropped its plan to mandate COVID-19 vaccination for school children.
As of Feb. 6, 21 states have legislation or executive orders banning student vaccine mandates, according to the National Academy for State Health Policy, a nonpartisan organization of state health policymakers.
Only the District of Columbia currently has a vaccine mandate for school children, although it is not set to go into effect until the 2023-2024 school year.
Denmark ended its universal COVID-19 vaccination campaign for healthy individuals in February 2022.
Brenda Baletti Ph.D. is a reporter for The Defender. She wrote and taught about capitalism and politics for 10 years in the writing program at Duke University. She holds a Ph.D. in human geography from the University of North Carolina at Chapel Hill and a master’s from the University of Texas at Austin.
The CDC recently codified International Classification of Disease (ICD) codes for Covid-19 vaccine status. ICD codes are extensively used in medical records, medical insurance data and health research to classify precisely disease states as well as injuries from exogenous agents such as accidents, medication and medical device injuries, toxic chemicals, etc. Vaccination status is not a disease or an injury state, yet CDC has rationalized creating ICD codes for it. The coding is set to become effective on April 1, 2023.
As described by Dr. Robert Malone, “The ICD classification system is run by the World Health Organization, not the US government.” The vaccine status ICD codes were developed by the US Centers for Medicare and Medicaid Services (CMS) some nine months ago, and CDC is implementing them.
The coding scheme, Z28.xxx, includes both vaccination status and possible reasons for the status. However, there does not appear to be a code for “fully vaccinated,” only for various states of “not fully vaccinated.”
The code Z28.0 means “immunization not carried out because of contraindication.” Z28.1 means “immunization not carried out because of patient decision for reasons of belief or group pressure.”
Z28.2 means “immunization not carried out because of patient decision for other and unspecified reason.”
Z28.8 means “immunization not carried out for other reason” which because of code Z28.2 must refer to reasons not attributable to patient decisions.
Finally, Z28.39 means “other underimmunization status,” including “Delinquent immunization status” and “Lapsed immunization schedule status.”
However, a potential contradiction arises because code Z28.310 means “unvaccinated for COVID-19.”
In order to reconcile this, the Z28 codes in the previous paragraph must refer to vaccines other than for Covid-19. The only other Covid-19 code is Z28.311 which means “partially vaccinated for COVID-19,” where “partial” refers to the CDC definition for “fully vaccinated” at the time when the patient visits the health-care provider who records the vaccination status in the medical chart.
It is apparent that the details of reasons for patient choices for vaccine status are not specified in codes for Covid-19 vaccines, but the CDC has some two months to fix this. There are no specific codes yet for “refused to divulge COVID-19 vaccination status” or “unknown COVID-19 vaccination status,” but these codes are likely to be added at some point.
What is the usage for which this information is planned? There is certainly a public health rationale for agencies to be able to monitor population vaccination status. Personal health information is routinely analyzed by public health agencies, insurance companies and health researchers, but in anonymized and grouped formats. The identifiable information is recorded in the databases, however HIPAA and other laws strictly protect identifiable health information and regulate how such information may be used for analyses.
In theory, vaccination status could be no different. Medical records already know your age, gender and race, where you reside, about your obesity, diabetes, your smoking and alcohol usage and your HIV status. Some of this information could be stigmatizing if released publicly, but at present there are no politicized or other circumstances to force unwanted choices on members of the public based on this compiled personal information.
Imagine, however, that one day, government agents are pounding on your door at 6am, telling you that you are required to take smoking cessation medications, under penalty of forced residence in a “smoking-cessation hotel” until you submit to the government’s requirement.
The medications have built-in transmitters that are activated when exposed to stomach acid, so taking them is recorded. After all, 500,000 Americans die every year from smoking-related diseases and their end-of-life medical care is an expense for which the government no longer wants to pay. Your smoking is economically hurting the medical care that grandma needs. Or something.
But Covid-19 and its vaccination are different. The Covid vaccines and their boosters were created under emergency-use authorization (EUA) protocols and are not fully licensed. The Biologics License Application (BLA) versions, e.g., Comirnaty, are not generally available in the US. This licensing chicanery has not gone unnoticed by the American public and a substantial fraction of people find the vaccines controversial.
Many people have seen their multiple-vaccinated friends and relatives get Covid, some multiple times. Many have also seen friends and relatives harmed by the vaccines, and most people know of the incessant daily deaths of healthy athletes, deaths discussed as caused by “coincidence.” People have seen the vaccines touted as solutions to the pandemic, yet utterly fail across the population to suppress transmission of the infection.
And, people have been bombarded with daily narratives for two solid years that the vaccines are “safe and effective” and that they must be taken, and that unvaccinated people are “bad,” “selfish,” demonized as doing damage to society, and should be shunned.
That is, personal vaccination status today is the most stigmatizing personal data of modern times, surpassing having AIDS. As such, any government compilation must be “bulletproof” against hacking and misuse. As well, the government must be trusted to maintain the data for use only as other personal medical data have been used.
Given the two-plus years of massive government propaganda about the vaccines, about their adverse effects, about Covid, about early Covid treatment, and the government collusion with social media companies in suppression of valid dissenting medical and scientific opinions and data, there is no empirical reason to support trusting the government with such sensitive, stigmatizing data.
There is no reason to believe that the government will not release the status information to insurance companies or other companies doing large business with the American public. Further, there is no recourse should the government actually release such confidential data. Thus, nothing may stop such companies from restricting activities based on the stigmatized data. For example, public travel could be blocked; bank accounts could be blocked; purchasing could be blocked.
The free pursuit of happiness is enshrined in our Declaration of Independence. The government cannot lawfully interfere with normal transactions of everyday life. But private companies working at the government’s behest, with government-supplied personal status information, could very well do it.
As has been seen from the FOIA documents, hundreds of government employees have spent the pandemic years doing exactly this unconstitutional behavior in getting social media companies to suppress Americans’ freedom of speech.
Furthermore, there is now no rational government interest in compiling vaccination status at all. At a time when vaccination was generally thought (incorrectly) to reduce Covid-19 transmission across the population, there might have been a rationale for doing so.
However, on August 11, 2022, the CDC stated publicly that the Covid-19 vaccines do not work as a public health measure to control virus transmission. They said, “Receipt of a primary series alone, in the absence of being up to date with vaccination* through receipt of all recommended booster doses, provides minimal protection against infection and transmission (3,6).” “Being up to date with vaccination provides a transient period of increased protection against infection and transmission after the most recent dose, although protection can wane over time.”
The fact that such benefit is “transient” and wanes implies that after some short period, boosters fail to reduce risk of transmission and thus that vaccine mandates are invalid.
The only government interest in mandating Covid vaccines, and thus in compiling personal information about vaccination status, is that the vaccines reduce transmission. They don’t.
Secondly, the CDC’s August 11th policy guidance does not distinguish between vaccinated and unvaccinated people in any way for any policy. There is thus no compelling government purpose in defining people as vaccinated or unvaccinated. It would be like the government compiling personal information on hair color, except that hair color is not stigmatizing and vaccination status is extremely stigmatizing.
The government itself—through the CDC—has determined that vaccination status is not of policy importance. There can thus be no compelling interest for the government to forcibly collect this information against the wishes of the population, even were it not stigmatizing. So much more so after the government has spent the last two years publicly demonizing unvaccinated people for their rational and legitimate personal health choices.
Harvey Risch, Senior Scholar at Brownstone Institute, is a physician and a Professor Emeritus of Epidemiology at Yale School of Public Health and Yale School of Medicine. His main research interests are in cancer etiology, prevention and early diagnosis, and in epidemiologic methods.
The mask is slipping (pun fully intended), all over the place – regarding the Big Tech/Big Government collusion. Now it’s time to pay close attention to the role played by the Centers for Disease Control and Prevention (CDC).
We’ve already been awed – just by the magnitude of the whole thing – if not exactly “shocked” by the Twitter Files.
But – what in the world was happening at Facebook, around the same time? After all, Facebook is an almost orders of magnitude bigger and more influential social network than Twitter.
For the time being, we don’t have the same “direct line” to internal documents as is the case with Twitter, which was made possible by the dedication to transparency by the new owner himself.
However, what could be dubbed as the “Facebook Files” are based on credible sources, too – Reason is coming out with a story based on confidential emails that emerged thanks to a court case – the state of Missouri suing the Biden administration.
The emails show that Facebook (and by extension Instagram) representatives and the CDC not only kept in touch at all times, but that the tech giant also “routinely asked government health officials to vet claims relating to the virus, mitigation efforts such as masks, and vaccines.”
In turn, the CDC kept a watchful eye on what speech was allowed on Facebook, what policies toward censorship of “inconvenient” Covid topics applied, and this government agency had no problem instructing the social network behemoth how to behave in these instances.
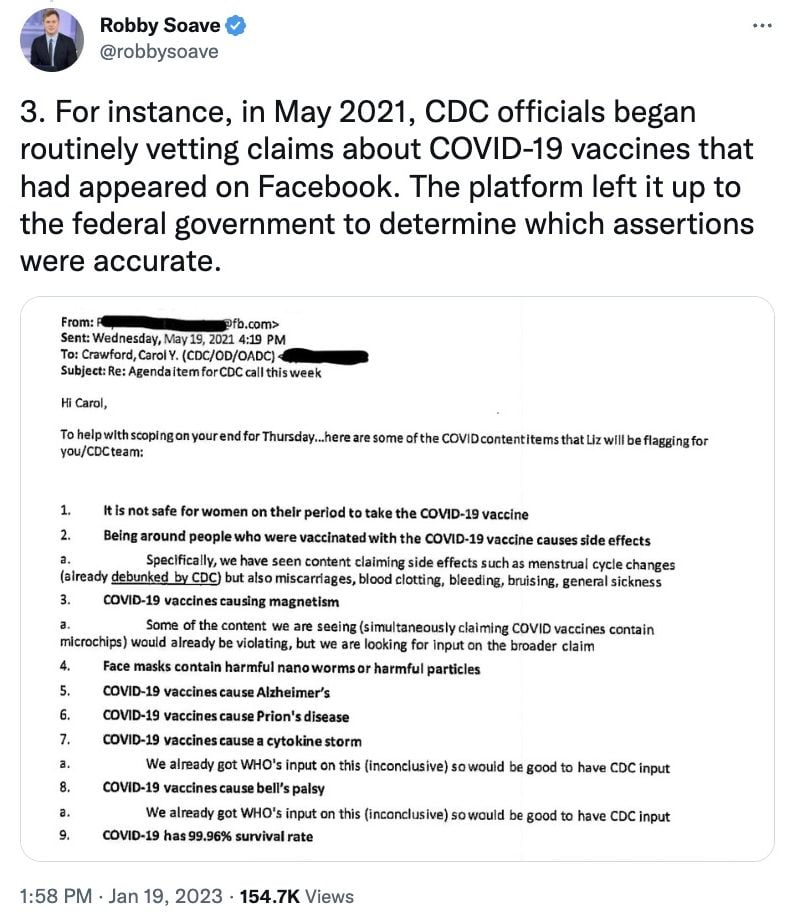
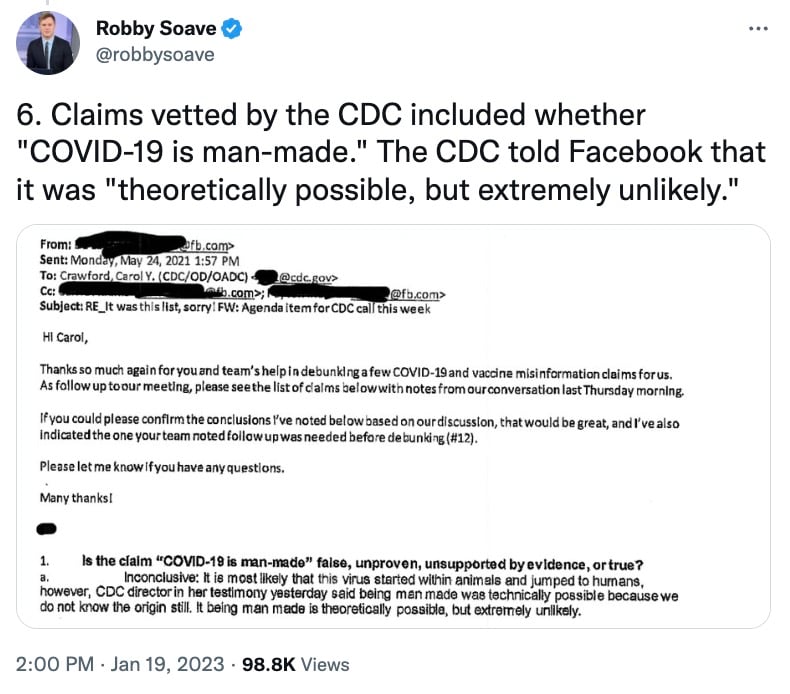
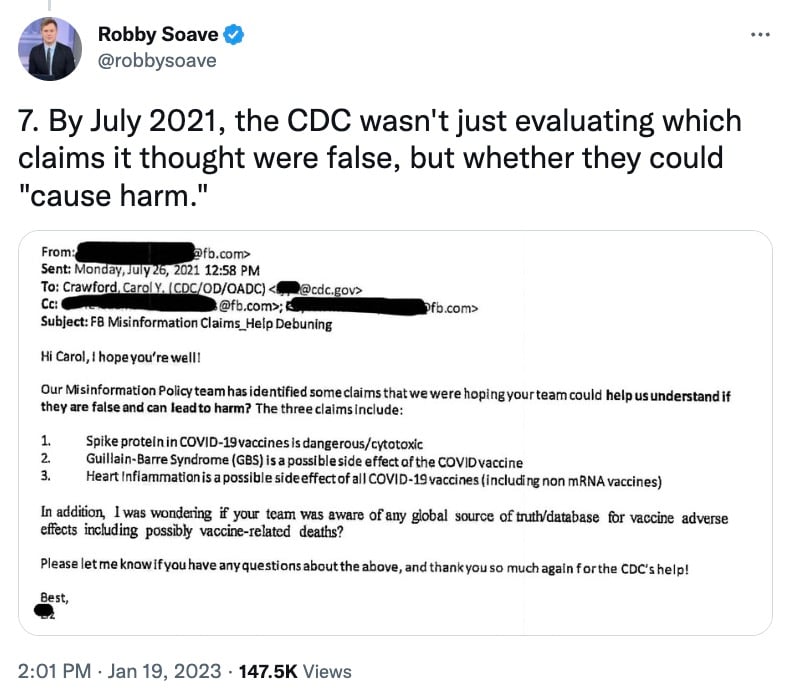
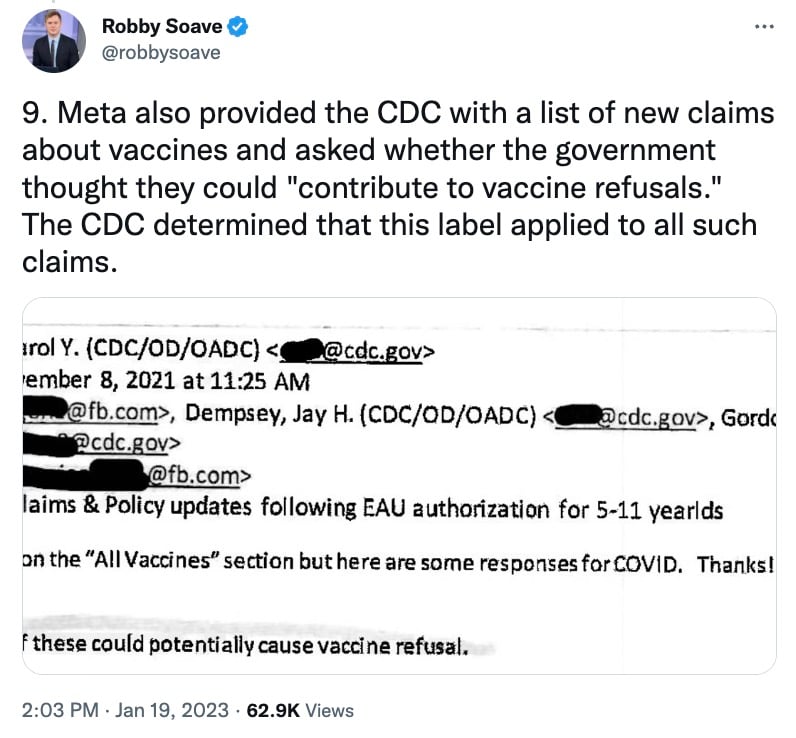
Robbie Soave, a senior editor for Reason, revealed some examples of what was happening in a series of tweets citing the emails and providing screenshots. One shows that in May 2021, CDC started to get involved in “vetting” content on Facebook that concerns Covid vaccines. And CDC had the last word on what was allowed to remain online as “accurate.”
Other emails show that Facebook (Meta) made sure the CDC was given de facto power to police Covid “misinformation,” while at the same time flagging content for the CDC, consulting with it on claims that could “contribute to vaccine refusals.”
At the same time, Reason is acknowledging that this was by no means the only federal agency to engage in similar activities, all aimed at pressuring some of the world’s biggest social platforms to allow only a certain narrative, and discredit any skepticism, even that coming from medical professionals and scientists.
Even President Biden made sure to “contribute” to this effort, when he in June 2021 bizarrely accused Facebook of “killing people.”
This was really meant to say that the giant had better not dare allow any Covid content the White House failed to “vet” behind the scenes – one way or another.
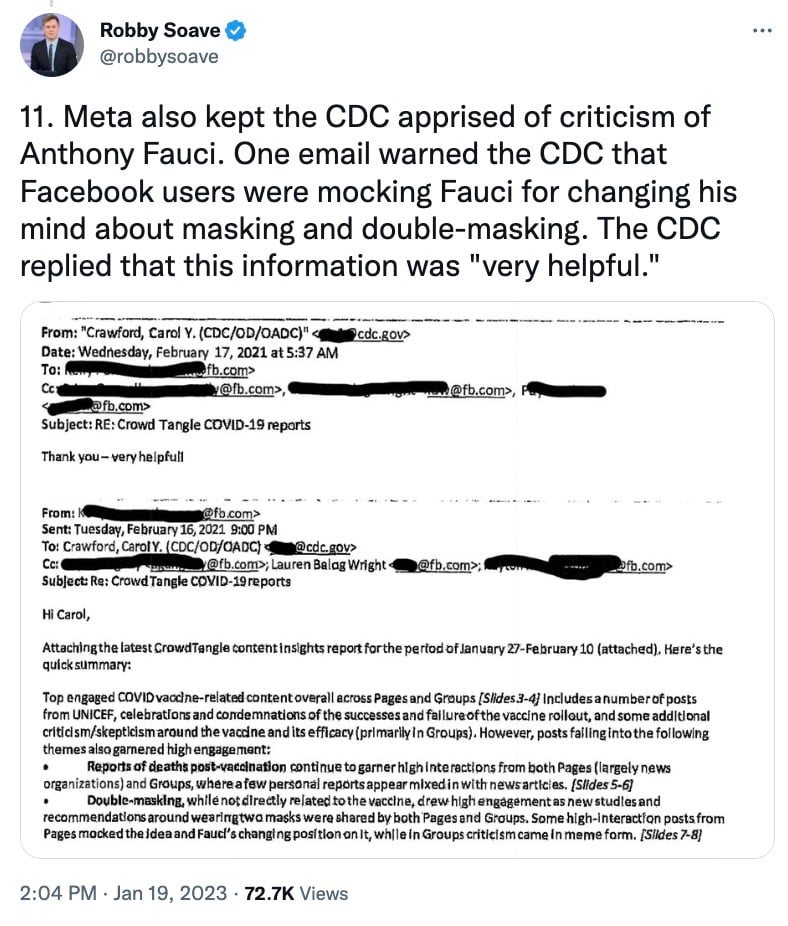
And the giant obliged, sometimes probably even exceeding the level of compliance expected from the administration. An internal email now reveals that Facebook went as far as to “snitch” on its own users making fun of Anthony Fauci, apparently in a bid to defend his reputation – again, at the expense of free speech.
“One email warned the CDC that Facebook users were mocking Fauci for changing his mind about masking and double-masking. The CDC replied that this information was ‘very helpful’,” Soave, the magazine’s senior editor and host on The Hill TV channel, tweeted.
The upcoming, March issue of Reason delves into how the CDC turned into the speech police when it came to pressuring social media to block content that the government agency decided was Covid “misinformation.”
And this was online speech that this, and other government agencies, have no constitutional way of directly suppressing without breaking the law.
“There is a word for government officials using the threat of punishment to extort desired behaviors from private actors. That word is: jawboning,” Soave remarked in one of the tweets.
And one can imagine – and the emails now show – just how gun-shy and ready to please those in power Facebook had become, after years of public vilification, and who knows what kind of pressure behind the scenes in the wake of the 2016 US election.
Newly released emails reveal that leadership within the US Centers for Disease Control and Prevention and National Institute of Health acted to prevent the release of a long-delayed review of fluoride’s toxicity by the National Toxicology Program. The emails specifically claim that Assistant Secretary for Health Rachel Levine intervened to stop the release of the NTP review, also known internally as a monograph.
An email dated June 3rd, 2022, shows Nicole Johnson, Associate Director for Policy, Partnerships and Strategic Communication in CDC’s Oral Health Division contacting Jennifer Greaser, a Senior Public Health Policy Analyst in CDC’s Washington office. Johnson states:
“The latest we heard (yesterday) is that ASH Levine has put the report on hold until further notice.”
ASH Levine refers to the U.S. Assistant Secretary of Health, Rachel Levine.
The emails were released as part of the ongoing legal dispute between the U.S. Environmental Protection Agency (EPA) and plaintiffs Food and Water Watch, the Fluoride Action Network (FAN), and others who are seeking an end to water fluoridation Throughout the historic lawsuit the plaintiffs have argued that the practice violates the EPA’s Toxic Substances Abuse Act.
Hearings for the lawsuit began in June 2020, but were delayed for more than two years after U.S. District Court Judge Edward Chen put the proceedings on hold pending the release of the NTP’s review of all of the available research on fluoride. The NTP had previously claimed the review would be available in May 2022. However, the review has not been made public and hearings have been delayed and rescheduled as the judge awaited the NTP’s conclusions.
In late October 2022, Judge Chen ended the two year stay on the lawsuit when he ruled that the NTP review could be viewed in its unpublished form to better inform his final decision. However, due to concerns from the EPA, Judge Chen ruled that the report could not be made public unless the NTP releases it.
On December 14, 2022, the plaintiff’s filed several exhibits with Judge Chen, including a redacted version of the NTP’s assessment of fluoride’s neurotoxicity and internal emails between the CDC and the NTP which were obtained via Freedom of Information Act requests.
What do the #FluorideEmails reveal?
Michael Connett, attorney for the plaintiffs, outlined the findings of the emails in several exhibits submitted to Judge Chen. “These emails confirm that the NTP considered the May 2022 monograph to be the NTP’s final report,”Connett writes. “They also confirm that the CDC was opposed to the NTP releasing the report, and that leadership at the top levels of the Department of Health Human Services intervened to stop the report from being released.”
As Connett notes, on April 28, 2022, Dr. Mary Wolfe, the Director of NTP’s Office of Policy, Review and Outreach, emailed Casey Hannan, the Director of CDC’s Division of Oral Health, and stated that the NTP’s “analysis and conclusions are set”. Dr. Wolfe also let Hannan know that the NTP had reviewed the CDC’s submitted comments, but still planned to release the review “mid/late May” 2022.
In a May 11, 2022 email, Wolfe again notifies Hannan and the CDC that the NTP has “set May 18, 2022 for publication of the monograph. The monograph will be posted to the NTP website, and we will email a notice of the posting to NTP listserv subscribers.”
However, later that day and the following day, Dr. Karen Hacker, the Director of CDC’s National Center for Chronic Disease Prevention and Health Promotion (NCCDPHP), tells Dr. Wolfe that there is concern within the CDC about publishing the NTP review without an additional review by “NIH leadership”. Hacker also asked about the potential of a “interagency review” by the Department of Health and Human Services (HHS).
Dr. Wolfe subsequently told the CDC that “we (the NTP) believe the current findings, as stated in the monograph, reflect the scope of our evaluation and the available scientific literature and no revision is needed”.
Meanwhile, while Dr. Wolfe was defending the work of the NTP, internal emails among officials at the CDC’s Division of Oral Health reveal that the CDC was already preparing to prevent the release. A May 12, 2022 email from Hannan states:
“The May 18th release date for [the monograph] is almost certainly not going to happen. OASH and NIH OD are pretty clearly going to get more involved.”
OASH is a reference to the Office of the Assistant Secretary of Health, the second highest office in the Department of Health and Human Services, while NIH OD refers to the NIH’s Office of the Director, the highest office within the NIH. The current Director of the NIH is Lawrence A. Tabak.
Jay Sanders, Education & Outreach Director with the Fluoride Action Network, told The Last American Vagabond he believes the emails “reveal a concerted effort at the highest level of the U.S. public health bureaucracy to squash a key report on fluoride neurotoxicity”. Sanders also stated the emails “show the lengths these agencies are willing to go to to protect their pet project, fluoridation, from any scientific scrutiny.”
Together with the June 3rd, 2022 email, these communications point to direct intervention from the head of the NIH and the Assistant Secretary for Health at the Department of Health and Human Services.
The emails confirm what has long been suspected. Namely, that government officials at some level were preventing the release of this important review on the toxicity of fluoride. The CDC interference comes on top of an already unusual process employed by the NTP to evaluate the data on the safety of water fluoridation.
“This report, which has now been reviewed 4 times, is now going to be reviewed a 5th time by the NTP,” Fluoride Action Network attorney Michael Connett stated during the October 2022 hearing. “There will be at least 5 separate peer review processes extending over 4 years. This is, to put it mildly, exceptionally unusual.”
The next hearing in the #FluorideLawsuit takes place on January 12, 2023 at 2:30 PM US Eastern.
Many of us are familiar with the following conundrum: on one hand, highly credentialed scientists and doctors have written numerous research papers explaining the dangerous mechanisms of action underlying mRNA/DNA “platform” technologies. The papers are meticulously researched and depict, correctly in my opinion, many terrifying consequences of the technology that breaches the innate protective mechanisms of human cells. Furthermore, these theoretical papers are validated by the observed outcomes, such as for example, increases in all-cause mortality in high correlation with increases in rates of vaccination in a given territory, unprecedented increases in the adverse events and deaths recorded by various passive reporting (https://openvaers.com/), astonishingly high reports of the adverse events and deaths from the pharmas’ own pharmacovigilance systems, and autopsy findings in vaccinated post-mortem showing the mechanisms of mRNA technology damage in histopathologic evaluations. On the other hand, many who have received the injections report no adverse effects and deem the data points above a “crazy conspiracy”. The question from the uninjured seems to be – why don’t we see MORE deaths if what you say about mRNA products is true? Setting aside ethical limitations of this question, here is a possible answer why:
The mRNA shots do not conform to their label specifications. In practice both “blank” and “lethal” vials and anything in between is produced. Without full compliance, nobody, not even the manufacturers or regulators, know exactly what ends up being produced.
Vials of mRNA injections are not routinely tested by the manufacturers for conformity to the label. The only vial-level tests specified by Pfizer in leaked Chemistry Manufacturing and Controls (CMC) documents are the vial weight at filling, manual inspection for large visible particles, and some tests related to integrity such as vial capping. However, no vial or dose, i.e., “unit-level as dispensed” tests verifying the ingredients are described as routine. How is the public assured that each Pfizer dose contains 30 mcg of mRNA as stated on the label? What level of variability of this key ingredient and other ingredients is acceptable? The ingredient conformity tests described in Pfizer CMC package are based on the bulk product batch testing – an upstream manufacturing process step. It is a regulatory requirement to retain samples of each batch produced, and these samples of vials should exist and be available for examination. Per contracts with the US Government, the product is shipped to the DOD who retains the ownership of the vials until the product is injected into people. These contracts are very detailed and specify manufacturing data to be delivered to the DOD, however, I did not find any descriptions of sampling of the vials for purposes of verification of their contents vs the label. Furthermore, it is expressly forbidden by the international vaccine supply contracts to perform the vial tests for label conformity.
Despite the disturbing prohibition of the independent vial testing, covert random testing of the mRNA vials has been ongoing worldwide. Reported thousands of vials have been obtained and tested by dozens of research groups working independently of each other. The quality of these studies varies and depends on the conditions of the samples acquired, access to the lab equipment and the experience of the investigators. However, the consistent finding among all is that there is yet a single vial to be found in full conformance to the manufacturer’s label. A review of these independent testing efforts has been published recently. Another high-quality report summarizes experiences testing vials from various manufacturers in Germany. These studies use different techniques ranging from optical to electron microscopy, spectroscopy, as well as isolation of genetic and protein components and in some cases sequencing of the RNA.
Some vials contain RNA as well as high concentrations of DNA and protein impurities in quantities far exceeding allowed limits specified by the manufacturer. When RNA was sequenced, the sequences did not fully match the specified BNT162b2 sequence, and a large quantity of RNA fragments was found. In other instances, vials are found apparently without RNA or DNA in them (evidently absent nitrogen and phosphorus).
These results could depend on the methods used and more thorough testing may be needed. Nevertheless, I was able to confirm that the apparent “blank” vials from at least one researcher came from batches of Pfizer and Moderna that had almost no adverse events reports in VAERS: two batch numbers had 1 report each and one batch number had no reports. This should be contrasted with some batch numbers of Pfizer and Moderna associated with 5000+ adverse event reports in VAERS, and an average of ~1500 adverse event reports including ~700 serious reports and deaths across all CDC verified batch numbers.
Almost all vials examined contain high contamination levels of various metals that are toxic to human body. This finding is consistent across all groups and methodologies, and therefore should be deemed more conclusive. There is no explanation of the origin or purpose of these materials according to the known manufacturing processes. Additional findings include various forms of carbon, including, potentially graphene oxide which is a known toxin. Finally, almost all vials examined contain a variety nano- and micro-particulate contaminants – another conclusive finding with plenty of photo and video documentation. These appear under microscope examinations as shapes and structures of various sizes and include characteristic ribbons, fibers, and crystals. Several published reports by qualified and credentialed microscopy experts have excluded the possibility of environmental dirt on the microscope slides. Sometimes a process of movement and what can be described as “self-assembly” is visible and has been documented in a single take video. The researchers also take steps to maintain the chain of custody, examine unexpired product and keep the vials frozen per manufacturer’s instructions.
Below are some representative images from various manufacturers’ injection vials from many studies:
Dr. David Nixon – Australia, Pfizer
Another Dr. from Australia, Pfizer:
The images above are startling and remain unexplained to date. Some scientists insist these are all “salt and cholesterol”, and nothing to see here folks! I disagree. Images of salt and cholesterol under microscope may match some of these structures, but by far do not explain all of them, and seem especially poor explanations for assembly-disassembly processes that have been observed and video recorded. Sizes of these structures alone are problematic. Dismissing them as “manufacturing junk” is not a great way to instill confidence in anyone.
These contaminants and bizarre objects are not rare, in fact as the last image shows, at least some of the vials are teeming with them. While many speculations can be made, one overwhelming conclusion from all the vial tests by independent investigations is that the products are extremely “dirty”, do not conform to their labels and should thus be deemed adulterated. This is a clear indicator that the manufacture of these products is not compliant with the current Good Manufacturing Practices (cGMP).
Sloppy manufacturing process may result from numerous factors, including lack of accountability, negligence, incompetence and possibly fraud. Review of the contracts with the manufacturers made by the U.S. Department of Defense, BARDA and HHS shows that the main driver were the gigantic sums of money made available with no real accountability for quality or safety – all resulting from the forced extreme speed (“warp speed”) of the scale up of manufacturing. The U.S. DOD contracted Pfizer in May of 2020 for production of at least 100 million doses by October 31, 2020, and up to 500 million doses later. Pfizer’s initial contract award was for $10 billion, with many additional incentives for delivering more doses faster. Similar contracts were made with numerous other “vaccine” manufacturers, and hundreds of other suppliers, all under the guise of panic buying for covid countermeasures. No real accountability for product quality or consistency or safety was built into those contracts, in fact the manufacturers were explicitly exempt from all possible liability under the PREP Act, which is specified in a separate contract clause. The purchaser is the DOD, the distributor is the DOD (and not the licensed and accountable pharmaceutical distributors), and furthermore, the product is not serialized and hence open to both adulteration and falsification or mislabeling.
To meet the contract obligations, Pfizer’s manufacturing batch size has increased from microgram scale for lab and animal study volumes to commercial batches of ~140 liters at the end of 2020 and ~300 liters by late 2021. In my experience commercializing biotechnologies from academia, failure to scale is one of the leading causes of failures of all new technology ventures. Showering this problem with money rarely accelerates the solution, and very often accelerates the demise of the whole venture. This is common sense. For example, placing an order today for 1,000,000 of a new type of vehicles with Ford Motor Company to be delivered in 6 months will likely fail no matter the dollars spent, since even obtaining the raw materials in time will be problematic. Complex manufacturing requires materials, systems, capacity, experienced staff, established processes, suppliers, and most importantly control systems at the correct scale to be successful and produce high quality consistent product. Now imagine simultaneously asking several direct competitors – Ford, GM and Toyota to produce 1,000,000 new cars each in the next 6 months.
Based on review of available literature on mRNA manufacturing and my discussions with experts who have made mRNA in the lab, it is not clear that mRNA can be manufactured at the scale that is estimated for these injections from known shipment numbers and disclosed manufacturing documentation: 200-300 liters of drug product per average batch, 700+ batches a year in the US alone. This is particularly unlikely if strict cGMP rules are applied to the manufacturing requirements, and we know that cGMP is not followed for production of these injections. Recently FDA found Catalent non-cGMP compliant. Catalent handles large volumes of fill-finish for Moderna, therefore batches processed through Catalent are non-cGMP compliant.
The generation of mRNA by in-vitro transcription (IVT) at large scale and under current good manufacturing practice conditions is challenging. For example, the specialized components of the in-vitro transcription IVT reaction must be acquired from certified suppliers that guarantee that all the material is animal component-free and GMP-grade. Furthermore, the availability of large amounts of these materials is limited and purchasing costs are high. This is true, for example, in the case of the enzymes used for translation and capping. Even the glass vials themselves were reported as a shortage. Additionally, the low yields and batch failure are a known problem. Conceptual process flow of making mRNA drug substance contains several steps:
The process is composed of a 2-step enzymatic reaction in continuous form, followed by enzyme recycling using tangential flow filtration strategies and two multimodal chromatography steps, one in bind-elute mode for the intermediate purification, and a second in flowthrough mode for polishing. Formulation is achieved using a third tangential flow filtration module. This means the mRNA needs to be made by chemical reaction, and then purified, and then capped and purified again. There are many variations of this process, and no standards exist. At the “formulation” step (last box in the picture), there are further multiple steps to create lipid nanoparticles, and get the mRNA encapsulated. Further, there are fill and finish steps that likewise are not problem free and decrease the yield. Finally, transportation and manual dose preparation add an extra variability layer.
Here is a simple heuristic to understand any manufacturing process flow and not get confused by the jargon: each arrow in the flowchart points to places where errors accumulate Each output-input point in a complex manufacturing flow is where the errors can be checked for and rectified or, if unsolved, will amplify and destroy the product quality and consistency. This is especially dangerous at the extreme speed and scale.
In science papers mRNA manufacturing is described with problem-free cartoons, it all works beautifully regardless of whether it is microgram or kilogram output, and not a single paper on this topic dwells much on low yields or process failures. This is because the academia never has to confront reality. However, the pesky reality of manufacturing mRNA (or anything else) at large scale is highly error prone. Each step has a yield of anywhere between 50% and 80%, and sometimes the whole batch fails, and that is especially true at the large scale of production. mRNA reaction fidelity is less than 100%, the caps and tails fall off, mRNA breaks into fragments, lipid nanoparticles do not form perfectly and PEGylation can be inhomogeneous leading to their breakage and subsequent escape and breakage of mRNA. Large mRNA breaks into smaller fragments, and these remain in the substance. At large scale of reaction, the enzymatic process for making mRNA was reported seizing at 37.5 liters of mRNA substance (before encapsulation into LNP and making drug product) according to the European Medicines Agency (EMA) documents. It is not clear how this was resolved and transitioned to 100’s of liters scale in a matter of few months, and for all suppliers. mRNA fragments were deemed process related impurities by the EMA who raised a significant concern, but they were dismissed by the FDA as a “theoretical problem” – as leaked emails from EMA have shown. mRNA “fragments” may or may not code for proteins, however micro-RNAs (miRNA) can interfere with endogenous cellular processes to detrimental health effects which is described in many scientific papers and even in a textbook on biological weapons published by the NIH in 2018. Chapter 6 of the book describes gene therapy as a class of biological weapons. Coincidentally, the DOD-pharma contracts for covid-19 shots also explicitly state that the product is being developed for both civilian and military applications.
Returning to mRNA manufacturing, multiplying even an optimistic 80% yield by, for example, 7 process steps results in 20% final yield, and if the in-process failures are larger, final yield is single digit percentage or a failure has occurred. Each step generates large amounts of impurities, which are never fully removed as aggressive purification will break the fragile product. Furthermore, the mRNA substance is never equally distributed in the batch volume as thorough mixing of the product is not possible due to its fragility, and lipids tend to float to the top of the vat as well as stick and congregate together. Dangerous possibly cytotoxic aggregates of broken LNPs and mRNA (mRNA adducts) can result and were reported by Moderna a full year after large scale deployment of their product. As a result, the larger the volume of the batch, the more inhomogeneity at the vial level. These conditions can create over-concentrated, toxic vials and the ones that could be “blanks”, or anything in between. The larger the batch volume the more duds it will produce, which in case of this product is largely good news for the injectees. Avoidance of specifying any product conformity tests at the vial level by the manufacturers seems to be intentional in this context.
Data from Pfizer’s own CMC documentation submitted to EMA at the end of November 2020 shows “failure to scale” beginning at approximately 25% of the current commercial scale of the batch (current scale = 600,000 vials = 3-4 million doses per batch). The graphs below were generated using exact sizes in vials and doses for each Pfizer batch manufactured between August and November 2020 (Figure 1) and all Pfizer shipped doses in the US up to end of April 2022 (Figure 2). I used reported deaths and adverse events in VAERS database associated with those batches as a measure of batch variability. This does not address vial variability but provides directional information especially for the scale of manufacturing. The batches in Figure 1 were the first ones to ship commercially and were likely all used close to 100% since at that time the demand for these injections was insatiable. As the “scale-up” of manufacturing proceeded in 2020, the batches were manufactured in a variety of sizes from 50,000 and up to 300,000 vials (~140 liters of drug product). During this time, several major changes were made to the manufacturing, for example, transition from the pilot facility at Polymun Scientific to Pfizer’s own plants and changing major manufacturing steps to new processes.
Figure 1.
First, the overall data indicate a statistical trend toward increased number of reported deaths with the increase in the batch size – the more this product is used, the more deaths are reported. This is not news for anyone who has been paying attention to the injection related adverse events and deaths. However, the variability batch-to-batch demonstrated by the vertical dispersion of the death reports associated with batches of the same size is already apparent at approximately 150,000 vial batch size (25% of the full commercial scale). Batches of the same size are 4-5 times different from each other in the number of reported deaths.
The “failure to scale” story gets larger at scale, no pun. Recently, the exact sizes of Pfizer lots shipped in the United States became known via a FOIA data release, including all doses with associated lot numbers shipped as of end of April 2022 to various vaccination centers. Figure 2 is the plot of all batches from Pfizer, by their reported size in doses on the x-axis and serious adverse events including deaths reported for those lot numbers on the y-axis. Data from VAERS was downloaded on September 24, 2022.
Figure 2.
This graph includes the “early” scale up batches from Figure 1, as well as what appears smaller shipments possibly for batches that were largely distributed overseas. What is immediately apparent from the data – the staggering inconsistency of the product batch-to-batch and the rapid decline of apparent toxicity measured by the adverse events with increase in batch size. The latter trend is the opposite of what was observed with the early batches. The product is causing fewer adverse events per dose when there are more doses available. This does not make sense, except if these doses are simply sitting on the shelves. Of note is batch FM0173 (only 26,700 doses shipped in the US) that generated the highest rate of serious adverse events (3.3/1000 doses), upper left dot.
The scale of manufacturing strains the credulity. A batch of 12 million doses translates to approximately 900+ liters of mRNA! Given the manufacturing steps involved, impurities generates and the amount of raw materials, and the scale of manufacturing equipment and disposables needed, it should be questioned whether this truly was a single production run.
Figure 3 is the same data as in Figure 2, with outlier batches removed for clarity (includes batch sizes from 100K to 4M doses):
Figure 3:
It is evident that the variability batch-to-batch is highly significant and remains unexplained. It is also strangely declining as the size of the batch is becoming larger. The only reasonable explanation to this is that the usage of this product per batch has plummeted. Most of what is produced later in the time period is sitting on the shelves. At the end of the time period in this graph (end of April 2022), an estimated 100M doses were manufactured but not administered in the United States. At the beginning of this graph, nearly all manufactured doses were administered. That is the only reasonable explanation – and it proves that these injections cause the injuries and deaths reported to VAERS!
Table below lists all batches >4 million doses, including their date of manufacture and the number of serious adverse events and deaths reported for them in VAERS:
Table 1:
The “mega” batches are not entirely benign. They are simply a larger lottery pool. The single death reported for batch FL0007 is for an 8-year-old girl who died in Texas from a multi-system organ failure (VAERS ID 2327226-1) – see Figure 4. While the first batch listed in her report RL0007 appears to be a typo (RL series do not exist for Pfizer), it is evident that she received both doses from the same FL0007 batch and passed away 3 months later.
Figure 4:
Here is my educated guess on what is going on with the batch variability: Pfizer’s (and other manufacturers’) contracts were for delivery of DOSES. Millions of them and fast. Contract scope is simply a “demonstration of large-scale manufacturing” and billion-dollar bonuses attached for shipping millions of doses by certain dates. No accountability, no checks, no liability, just ship the doses on time! The batches of 5 million+ doses should be questioned in this context. These appear largely benign from the adverse event perspective but, since the demand for these shots has plummeted coinciding with production of mega-batches, it is hard to say what the real driver of “safety” is – over-dilution of the product or refusal of the customers to be injected. I hope it is the latter.
Here is as close as I can get to answering the question “why aren’t MORE people dying?”: Too many people have died and have been injured by these injections, and plenty more will ultimately have their lives cut short. The manufacturers are making both – lethal shots and highly diluted “blanks” in a sloppy, uncontrolled, unaccountable, and ultimately fraudulent manner.
To know the truth, these products must be tested at the vial and dose levels, in a random sampling by independent 3rd party laboratories. In the meantime, the products must be recalled, and a proper investigation initiated.
A growing number of parents oppose vaccine mandates as a precondition for public school attendance, and interest among adults in receiving COVID-19 booster shots is waning, according to a national poll by the Kaiser Family Foundation (KFF).
The results of the latest KFF COVID-19 Vaccine Monitor survey, released today, show more than one-third (35%) of parents now believe they should be the ones to decide whether their children receive a slate of childhood vaccines.
The poll encompassed a nationally representative sample of 1,259 adults who were interviewed between Nov. 29 and Dec. 8. According to The New York Times, the KFF is a “nonpartisan health care research organization.”
“It’s unfortunate that it took a wave of injuries and deaths from vaccines that never should have been released into the market — much less mandated — to draw long-overdue attention to the issue of vaccine safety,” said Robert F. Kennedy, Jr., chairman and chief litigation counsel for Children’s Health Defense.
Kennedy told The Defender :
“This latest poll is encouraging for those parents, physicians and scientists who for decades have been calling for an investigation into the relentless promotion by FDA, CDC and Big Pharma of inferior medical products without rigorous safety testing.
“As more parents begin to question the forced, routine administration of vaccines on healthy children, perhaps we will move closer to protecting children and holding vaccine makers and government agencies accountable for the harm these products cause.”
26% of parents today: ‘Risks of childhood vaccines for measles, mumps, and rubella outweigh the benefits’
According to the KFF poll, 65% of parents of children under age 18 “think healthy children should be required to be vaccinated to attend public schools.”
More than one-third of parents surveyed (35%) “now believe parents should be able to decide not to vaccinate their children, up from 23% in 2019.”
The poll also revealed declines in support for specific vaccines. For instance, 71% of respondents said “healthy children should be required to get vaccinated for MMR in order to attend public schools” compared with 82% who supported the MMR vaccine mandate for healthy children in 2019.
Nearly 3 in 10 parents (28%) said parents should be able to choose whether their children receive the MMR vaccine, compared with 16% in the 2019 poll.
A similar percentage (26%) responded that the “risks of childhood vaccines for measles, mumps, and rubella outweigh the benefits.”
A smaller decline was noted in the percentage of adults (85%) who felt the benefits of childhood MMR vaccination outweigh the risk. This represented a three-percentage-point decline from the 2019 Pew Research Center poll (88%).
These declines were driven by increased vaccine “skepticism” and a growing movement toward parental choice, on the part of Republicans and Republican-leaning independents — 44% of whom responded that parents should have a choice about whether or not their children receive the MMR vaccine, up from 20% in 2019.
Only 11% of Democrats provided the same response.
Moreover, only 56% of Republicans and Republican-leaning independents said “healthy children should be required to be vaccinated to attend public schools,” a decline of 23 percentage points compared to 2019.
A similar divide was apparent among respondents in reference to their COVID-19 vaccination status. While 83% of vaccinated respondents said healthy children should be required to be vaccinated in order to attend public schools, 63% of unvaccinated parents said parents should instead decide.
‘Tepid’ interest in COVID ‘boosters’ and flu vaccine
Interest in the updated COVID-19 booster is “tepid,” according to the KFF poll, which showed only 1 in 5 adults (22%) surveyed said they have received the updated bivalent booster and an additional 16% said they plan to receive it “as soon as possible.”
However, 12% of respondents said they would “wait and see” before deciding whether to get the new booster, 13% said they would get it only if required and 9% said they would “definitely not” get it.
An additional 27% were unvaccinated or only “partially” vaccinated, which means they are not eligible to get the booster.
Interest in the bivalent booster was highest among adults 65 and older (39%) and Democrat voters (38%), though both figures fall significantly short of a majority. Conversely, only 12% of Republicans and 11% of young adults under 30 said they had received a dose of the updated booster.
Also, 36% of “fully vaccinated” adults 65 and older said they don’t think they need the updated booster, while a “similar percentage,” according to KFF, said they did not think the benefit of the updated booster was worth it.
Overall, fewer than half of parents of children under 18 said their child has received the updated booster or is likely to do so.
Combined with children who have not been vaccinated and who are therefore ineligible for the booster, 58% of parents of 12- to 17-year-olds and 70% of parents of 5- to 11-year-olds responded in this manner.
Republicans and Republican-leaning independents, even if vaccinated, expressed skepticism toward the updated booster, with 64% stating they do not think they need it, and 61% saying they did not believe the benefit was worth it.
Even among Democrats, a majority (51%) said they were too busy or hadn’t had the time to get the updated booster, indicating it was not a high priority for them.
Even in the face of a so-called “tripledemic” of COVID-19, flu and RSV (respiratory syncytial virus) this fall and winter, and despite the majority of parents saying they are worried their children will get sick from RSV (56%, and 73% of parents of children under the age of 5), only 34% of parents said their child has gotten a flu shot this season.
Parents’ rights movement growing in prominence
According to The Times, “The shift in positions appears to be less about rejecting the shots than a growing endorsement of the so-called parents’ rights movement.”
Dr. Sean O’Leary, chairman of the American Academy of Pediatrics’ Committee on Infectious Diseases told The Times :
“The talking point that has been circulated is the concept of taking away parents’ rights. And when you frame it that simply, it’s very appealing to a certain segment of the population.”
O’Leary said he worried that the parental rights movement might slow down compliance with state-mandated childhood immunization schedules, telling The Times “We do have a global dip in vaccine coverage. So this is not a time to be considering a rollback of these laws.”
Michael Nevradakis, Ph.D., based in Athens, Greece, is a senior reporter for The Defender and part of the rotation of hosts for CHD.TV’s “Good Morning CHD.”
In 1967, Haley obtained an M.S. degree from the University of Idaho. He then entered a doctoral program at Washington State University, where he worked to make chemical modifications on ATP to try to identify how and exactly where ATP binds to cause muscle movement. In 1971, WSU granted him his Ph.D. degree in chemistry-biochemistry. https://emeramed.com/about/
Previously I argued whether Saudi Arabia’s repeated involvements in U.S. interventions and wars stem from free national will or in response to a specific condition. For starters, in Saudi Arabia there is no national will. In Saudi Arabia, the national will is the will of the Al Saud clan. Still, when a major Arab state allies itself with a superpower that committed unspeakable crimes against humanity in almost every Arab country, then something is wrong. This fact alone should compel us to examine the U.S.-Saudi relation for one exceptional reason. As a result of the U.S.-Saudi wars, hundreds of thousands of people in Afghanistan, Iraq, Iran, Libya, Syria, Yemen, and Somalia have lost their lives. Millions became displaced in their own homelands. And millions more rendered refugees.
Attributing the Saudi policies to the bonds of “partnership” with the U.S. is frivolous. There are no bonds between these two thugs except those of business, military deals, secret plots, and wars. Proving this point, bonds such as these have no space for the American and Saudi peoples to share significant cultural or societal exchanges. If partnership is not the reason for the Saudi contribution to the U.S. strategy of empire and imperialism, then another reason must exist.
This site is provided as a research and reference tool. Although we make every reasonable effort to ensure that the information and data provided at this site are useful, accurate, and current, we cannot guarantee that the information and data provided here will be error-free. By using this site, you assume all responsibility for and risk arising from your use of and reliance upon the contents of this site.
This site and the information available through it do not, and are not intended to constitute legal advice. Should you require legal advice, you should consult your own attorney.
Nothing within this site or linked to by this site constitutes investment advice or medical advice.
Materials accessible from or added to this site by third parties, such as comments posted, are strictly the responsibility of the third party who added such materials or made them accessible and we neither endorse nor undertake to control, monitor, edit or assume responsibility for any such third-party material.
The posting of stories, commentaries, reports, documents and links (embedded or otherwise) on this site does not in any way, shape or form, implied or otherwise, necessarily express or suggest endorsement or support of any of such posted material or parts therein.
The word “alleged” is deemed to occur before the word “fraud.” Since the rule of law still applies. To peasants, at least.
Fair Use
This site contains copyrighted material the use of which has not always been specifically authorized by the copyright owner. We are making such material available in our efforts to advance understanding of environmental, political, human rights, economic, democracy, scientific, and social justice issues, etc. We believe this constitutes a ‘fair use’ of any such copyrighted material as provided for in section 107 of the US Copyright Law. In accordance with Title 17 U.S.C. Section 107, the material on this site is distributed without profit to those who have expressed a prior interest in receiving the included information for research and educational purposes. For more info go to: http://www.law.cornell.edu/uscode/17/107.shtml. If you wish to use copyrighted material from this site for purposes of your own that go beyond ‘fair use’, you must obtain permission from the copyright owner.
DMCA Contact
This is information for anyone that wishes to challenge our “fair use” of copyrighted material.
If you are a legal copyright holder or a designated agent for such and you believe that content residing on or accessible through our website infringes a copyright and falls outside the boundaries of “Fair Use”, please send a notice of infringement by contacting atheonews@gmail.com.
We will respond and take necessary action immediately.
If notice is given of an alleged copyright violation we will act expeditiously to remove or disable access to the material(s) in question.
All 3rd party material posted on this website is copyright the respective owners / authors. Aletho News makes no claim of copyright on such material.















{kind=link}