This article found that at one year of age, babies born to mothers who had COVID (not vaccine), had a roughly twice-higher rate of neurodevelopmental disorders:
those born to the 222 mothers with a positive SARS-CoV-2 polymerase chain reaction test during pregnancy were more likely to receive a neurodevelopmental diagnosis in the first 12 months after delivery, even after accounting for preterm delivery.
Considering that COVID is a bad disease for a sizable minority of people, there is no surprise. Covid is bad and gives people all sorts of problems. Then I started thinking: a lot of adverse effects of Covid vaccines mimic the adverse effects of Covid. The younger is the vaccine recipient, the worse some effects of vaccination (such as myocarditis) are.
A great number of expectant mothers received up to three Covid vaccine shots during pregnancy. Did anyone bother testing one-year-old children of vaccinated and boosted (during pregnancy) women for neurodevelopmental disorders, before approving this vaccine for all pregnant women?
The question is, obviously, rhetorical, since “mRNA Babies” of triple-vaxed-during-pregnancy mothers are only beginning to get born right now and are at most a few months old. Not one such baby reached a year of age. So nobody tested them for developmental disorders at one year of age, before approving the three vaccine shots for expectant mothers.
The usual argument of vaccinators that “since Covid does it too, you should take the vaccine” does not hold water. To a woman who decided to take the vaccine, the probability of getting a vaccine is 100%. The probability of her getting Covid is much less. In the above study, out of 7,772 births, only 222 (2.8%) were exposed to Covid during pregnancy. So while vaccination is 100% guaranteed for those who elect to vaccinate, the chance of Covid is over 30 times less likely. And the “vaccine” does not prevent Covid anyway and does not even reduce the viral load.
There is literally zero data on one-year-old children of triple-vaccinated mothers because the oldest ones are 3-4 months old as of today.
However, there are disturbing developments regarding newborns. Vaccination does seem to have an effect on births and pregnancies.
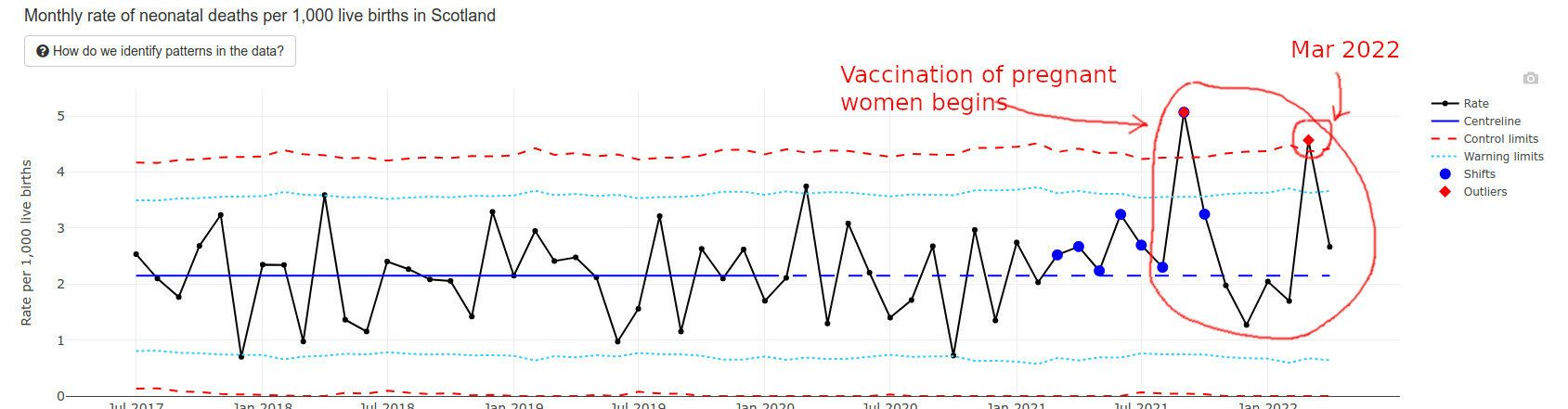
Infant Deaths in Scotland
The best data I found regarding recently born newborns happens to come from Scotland. They have an interesting “wider impacts” page that I am quoting below.
Infant deaths are way above average and exceeded “Alert Limits” twice.
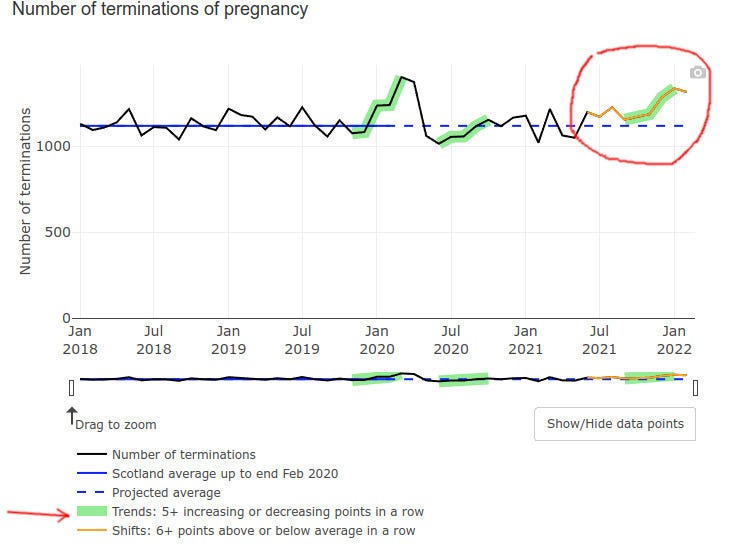
Even pregnancy terminations went up at the end of 2021, possibly but not certainly explained by prenatal vax problems:
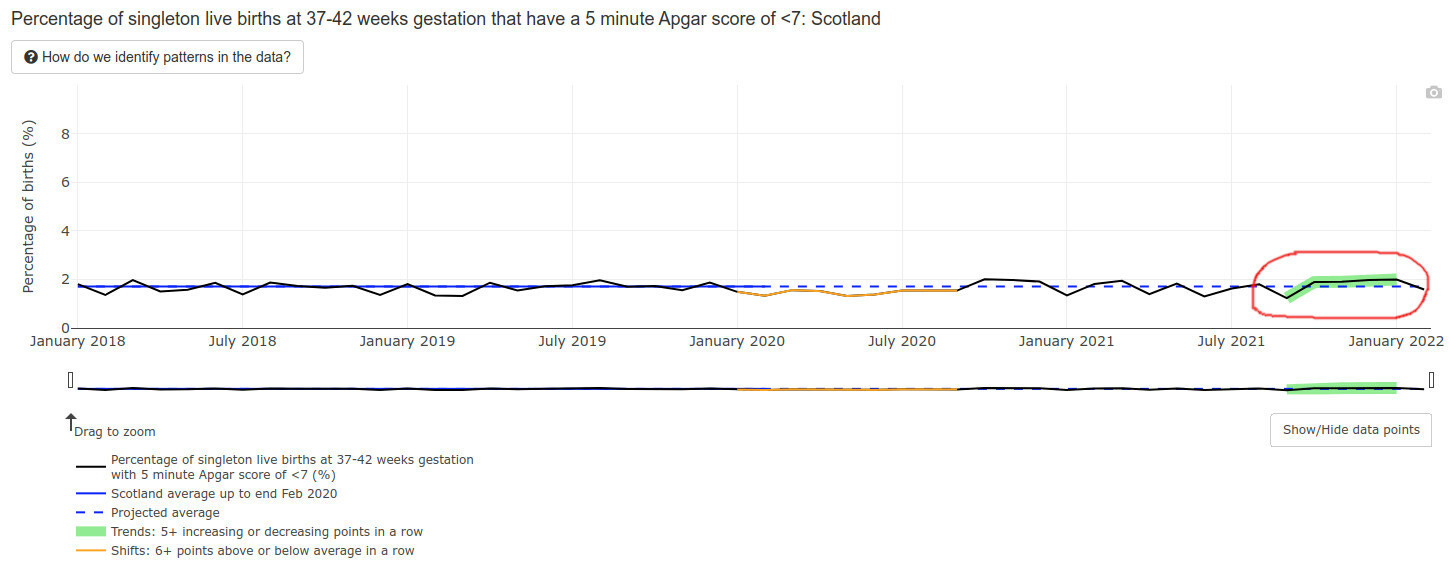
Low Apgar score births (for those readers who do not have kids, Apgar score is how healthy is the baby at birth, the best being a score of 10) triggered a green alarm signal:
Mind you, an Apgar score is also a developmental evaluation of sorts — at 5 minutes after birth. What will happen to the developmental milestones of those lucky babies of vaccinated mothers, who survived the pregnancies, did not die postnatally, and lived to one year of age? I literally have no idea and nobody else in the world does — the time has not passed yet.
The data we have is NOT encouraging.
CDC Solution: Remove and Lower Milestones
The CDC possibly caught a whiff of this, because in February of 2022 they literally removed half the developmental milestones, bumped some others to higher ages, and lowered standards for yet more of them. (Hat tip @CLesterwood)
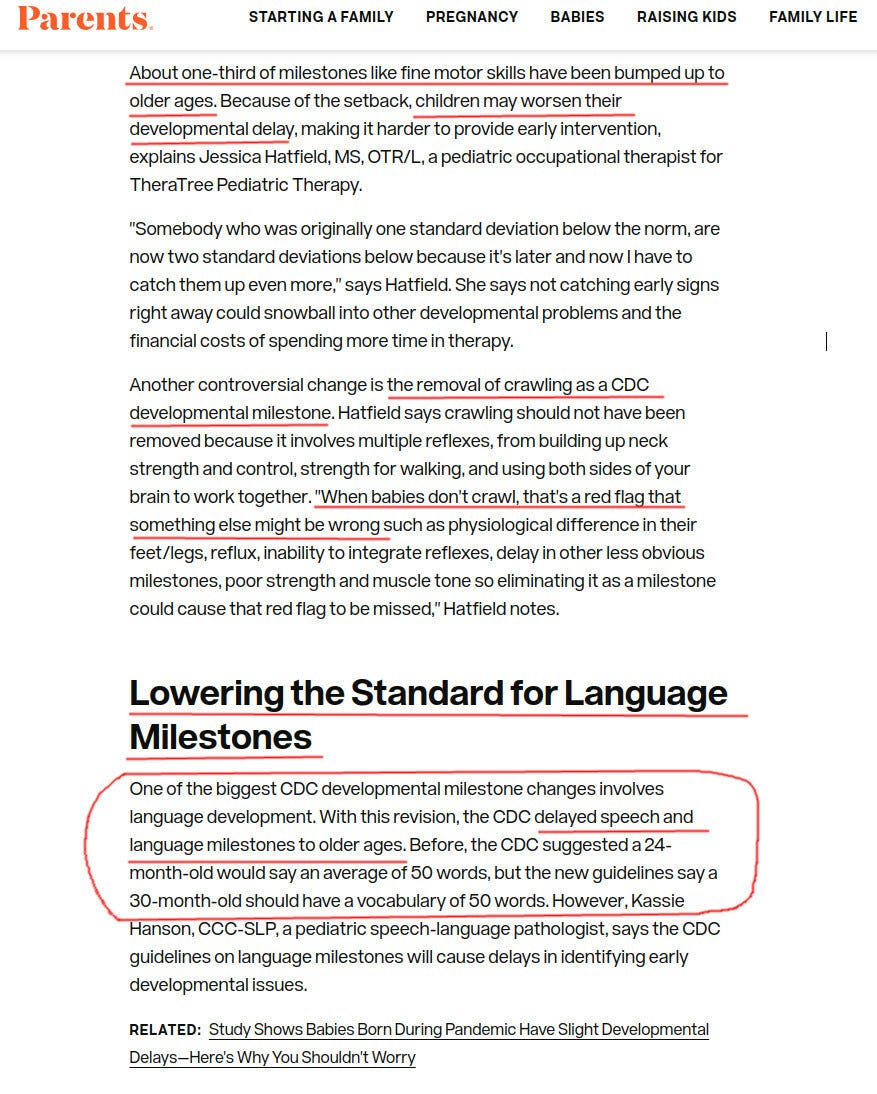
About one-third of milestones like fine motor skills have been bumped up to older ages. Because of the setback, children may worsen their developmental delay, making it harder to provide early intervention, explains Jessica Hatfield, MS, OTR/L, a pediatric occupational therapist for TheraTree Pediatric Therapy.
Removing crawling as a milestone??? Are you kidding us? For those of my readers who are parents, do you think that crawling is unimportant as a milestone?
Vaccinated Infants Exposed to SIX Doses of Covid Vaxx in a Year!
Imagine a vaccine enthusiast mother, who gets three doses during her pregnancy. Say, two doses during month 4 and one during the last week of pregnancy. The unborn baby is, obviously, exposed to all that.
That’s a total of, drumroll, six spike protein, and nanoparticle exposures. For a tiny newborn, all during one first year of her life.
And what if the mom has several Covids while being pregnant and vaccinated?
They will ask the mom to vaccinate the baby regardless of those covid infections. This literally amounts to six doses within a year or close to, without even counting actual covids that the vaxed moms have. Pfizer will make $132 from these six shots. Not sure if the baby will eventually need much more expensive treatments.
Do you think that it is a little bit too much? Do you think Pfizer or the FDA care?
They want the COVID-19 vaccine approval for children so bad, Peter Marks himself and his cronies published the very study he has to use to evaluate for approval.
As promised, the FDA has ginned up a report that ostensibly will be used to try to justify “approval” (whatever they mean by that now) of COVID-19 vaccines for infants and toddlers (children < 5 years old). Here’s the report for your reference.
This report comes after a torrent of massive reports from Moderna and Pfizer that claim to review studies of the safety and efficacy of COVID-19 vaccines in children. It is not hard to see what shenanigans the FDA has been up to to try to bolster a vaccine that fewer and fewer adults want. It’s more of the same: exaggerate the apparent risk of the virus and minimizing the perception of risk. In other words, lies.
There is no evidence of clinical urgency. Infants and toddlers (and children in general) do not get COVID-19; they do not (yet) die from COVID-19. All that can change when antibody dependent enhancement kicks in for the vaccinated. FDA’s own reports cites 1,086 deaths “from COVID-19” and 10,700,000 “cases” of COVID-19 in children aged 0-17. There have been 832 days since April 1, 2020 when diagnoses started for COVID-19. For the entire population of children in the US (73,000,000), the risk of COVID-19 infection since the onset of COVID is 10,700,000/73,000,000 = 0.14657. The risk of a child dying if they have a diagnosis is 1,086/10,700,00 or 1086/10700000 = 0.00010149532. The risk of any child dying of COVID-19 over this time period is 1,086/73000000 = 0.00001487671. The per-day risk is on the order of 1.78806611e-8 (0.000000001788). There is no real unmet clinical need and the FDA needs to go back to college to understand how to use RT-PCR correctly. Children do not get COVID-19, and they do not die.
Inconsistent use of the idea “vaccinated”. This has been the pattern from the very first study. FDA, CDC, Moderna, Pfizer, and others pull out whatever definition of “vaccinated” they want. Examples: “Vaccinated” is defined in the original trials as people who received both doses and who did not develop COVID-19 before two weeks passed after the second exposure to the vaccine. In fact, that means that people who developed COVID-19 due to disease enhancement were dropped from the study calculations. First, this is the first time people were dropped from a vaccine trial for getting infected with the pathogen targeted by the vaccine up to 13 or 14 days after being vaccinated. Second, it’s actually five entire weeks – one month and one week – 44 days – after the first exposure. ALL of the vaccine efficacy being cited by FDA is suspect. Moderna’s and Pfizer’s vaccines never achieved >90% true vaccine efficacy; the best estimate is more like 75%.
Inconsistent use of the idea “vaccine efficacy”. Over the time period since the first COVID-19 vaccine trials, various definitions of “vaccine efficacy” have been used. Decreased transmission. Reduction in infection rates. Reduced hospitalization. Presence of neutralizing antibodies. Presence of antibodies. All are used and cited in FDA’s report whenever convenient, all in an ad-hoc manner. It’s more than irritating. It’s moving the goal post and represents reckless (and ineffective) attempts to manipulate public perception. This practice continues in the reports and studies that are cited by FDA. I do not trust the efficacy data FDA cites in their report (why would we given Point 1?).Further evidence of the futility of the evidence used to claim efficacy comes from Moderna’s Sponsor Briefing report to the FDA:“3.3 Regulatory Considerations for Clinical Development of COVID-19 Vaccines in Children
Effectiveness
Regulatory precedent with other preventive vaccines provides a basis for inference of vaccine effectiveness in pediatric populations based on immunobridging to a young adult population in which clinical disease endpoint vaccine efficacy has been demonstrated for the same prototype vaccine. The immune marker(s) used for immunobridging do not need to be scientifically established to predict protection but should be clinically relevant to the disease. Based on available data in humans and animal models, FDA considers neutralizing antibody titers (a functional measure of the vaccine immune response against SARS-CoV-2) to be clinically relevant for immunobridging to infer effectiveness of COVID-19 vaccines in pediatric age groups. Because no specific neutralizing antibody titer has been established to predict protection against COVID-19, two immunogenicity endpoints (GMT and SRR) are considered appropriate for comparing the range of neutralizing antibody responses elicited by the vaccine in pediatric versus young adult populations.
Also embedded in this piece of work is the fact that FDA does not need evidence of long-term immunity; they are settling for something called “immunobridging” – guessing at the efficacy of a vaccine in one clinical population from measurements made from other clinical populaton.
They also are making people dependent on vaccines… expecting patients to have antibodies from one vaccine to the next. This makes no sense immunologically. We don’t need continuously high antibody levels against any pathogen. We have memory B-cells and T-cells. In accepting this paradigm, FDA is completely off its rocker and will cause immune exhaustion with constant vaccinations every 3-4 months.
Incomplete consideration of the scientific data (Barnstable County, Israel, Ontario). We know that months after vaccination, those who are vaccinated are at higher risk of infection and now of hospitalizations. Data actually show negative vaccine efficacy in children (per Jeremy Hammond). See: “Evidence for Negative COVID-19 Vaccine Effectiveness in Children”. From that article:“vaccine effectiveness (VE) in children becomes(sic) negative within several months since receipt of the second dose.Researchers from the New York State Department of Health published a study on the preprint server medRxiv on February 28 noting that the evidence for vaccine effectiveness in children, particularly those aged five to eleven, was “limited”. So, they aimed to provide data to inform policymaking.“During Omicraon variant predominance,” the authors concluded, “VE against infection declined rapidly” for young children in the state of New York, “with low protection by one month following full-vaccination.”Comparing COVID-19 cases during January between unvaccinated and vaccinated children, they estimated initial vaccine effectiveness for children aged twelve to seventeen to be 76 percent, but this dropped to below 50 percent after just five weeks since receipt of the second dose.Moreover, for young children (aged five to eleven), they observed a drop from 65 percent to just 12 percent after only one month.Thereafter, their estimate indicated significantly negative effectiveness for this age group, as shown in Figure 2 of their paper: by 35 to 41 days, VE reached negative 10 percent, and by 42 to 48 days, it reached negative 41 percent.
Jeremy goes on to report (correctly) that the authors of the article misinterpreted their own data. History will remember Jeremy as a reporter with great integrity.
Moderna and Pfizer reports fail to study long-term risks. Like I said, more of the same shenanigans. In this report, for example, Moderna offers data on myocarditis only up to Day 28 after the vaccine. Why Day 28? Why not “since the vaccine has been administered” to more accurately reflect the real-world clinical situation? They also state that myocarditis in a large concern in people infected with SARS-CoV-2 – but the comparison is to the uninfected, not the vaccinated, and we know that the spike protein is the cause (syncytia among heart muscles caused by the spike protein). The spike protein, of course, is the basis of their mRNA vaccines.
Incestuous COIs/Unjustified Influence by Regulators. Peter Marks is charged with setting the decisions at FDA whether to consider vaccines for specific populations. Why the hell is he involved in a study conducted to bolster the vaccines he is going to have to decide upon? See “Benefit-risk assessment of COVID-19 vaccine, mRNA (Comirnaty) for age 16–29 years”. That “study” is also guilty of all of the same loose logic as above; it is noteworthy that the study assumes as “worst case scenario” of zero deaths from myocarditis following COVID-19 vaccination (Credit: Toby McDonald, who wrote this to me:“I’m reading the Moderna “Sponsor Briefing Document” and they built their benefit-risk assessment off of Funk et al. (2022). So I looked up Funk and it’s a recent paper by six staffers at the FDA including Peter Marks, Richard Forshee, and Hong Yang (who wrote the dreadful benefit-risk assessment for kids 5 to 11 back in October). Quite literally in their “worst-case scenario” they predict 0 deaths from myocarditis in the vaccine group. It’s a stunning work of fiction.”
I’m on an email thread with Steve Kirsch (he considers me part of his “debate team”. Last week, Steve challenged Peter Marks to a debate:“Hi Peter,You are right about the vaccine uptake problem. According to independent survey we just commissioned, only 33% of Americans opted to go further than the first 2 doses.You were quoted in that CNN article:“We do have a problem with vaccine uptake that is very serious in the United States and anything we can do to get people more comfortable to be able to accept these potentially life-saving medical products is something that we feel we are compelled to do,” said Dr. Peter Marks, director of the Center for Biologics Evaluation and Research.Isn’t it time for you to end the misinformation problem by debating us in a public forum?My colleagues and I look forward to hearing from you.
The only way to end the misinformation is to debate the top misinformation spreaders. You will never win by trying to censor us.
To my knowledge, Marks has not replied. I replied to Steve and the entire email thread, including Marks, though:
“Steve,
History is going to remember one person on this email thread in a manner in which I would not ever care to be seen associating with.
I would therefore decline to participate in such a debate.
Sincerely,
James Lyons-Weiler, PhD
I could continue and debate dozens more points in the report dump by the FDA. I don’t have to. Marks himself provides evidence of being way off-target immunologically and lying about the “need” for COVID-19 vaccines for children.
Here’s an old video of Prevaricating Peter lying about the need for “high antibody titres” for immunity, and that children’s immune response is “not enough for some of these variants” (no data on that, just words):
The comments in that video have not aged well. Call your Senator and Congressional Reps and demand that Peter Marks resign. Email them this article. Marks and the FDA are NOT basing their considerations on independent fact, science and logic. He and his cronies are either incompetent or working for the industry. Either way, he and his cronies have to go.
I recently posted a deeply referenced compilation of evidence detailing the historic humanitarian catastrophe that has slowly unfolded within most advanced health economies across the world. Caused by a global mass vaccination campaign led by the Pharma masters of BMGF/WHO/CDC that illogically (but profitably) targeted a rapidly mutating coronavirus. They did it with what turned out to be the most toxic protein used therapeutically in the history of medicine. In vials mixed with lipid nano-particles, polyethylene glycol and who knows what else.
As these events become more and more recognized by the average citizen (and occasional journalist), a new pathetic “Disinformation Campaign” was launched in response trying to blame all the young people dying as simply a need for increased awareness of the rare condition called Sudden Adult Death Syndrome (SADS), rather than examples of the legions dying from the vaccines. The fact checkers also came out in support of this narrative, branding anyone who thinks the vaccines are the cause of SADS as a conspiracy theorist. Like this self-appointed social media watchdog. Mentions of SADS are popping up from many countries… all in the last few weeks. Here, here, here, hereand.. oh whatever. This article even listed a dozen such publicized deaths in the past few weeks from all over the world… but blamed them all on SADS. You get it. What is nauseating is the tone of purported good intention within these articles, informing folks that if you are related to someone young who died suddenly you should go see a cardiologist to make sure you don’t have an abnormal EKG. After it turns out normal, they will assuredly tell you to get vaccinated, an absurdity atop a mountain of absurdities caused by our bio-medical-media industrial complex over the past 2+ years.
Ugh, lets move on. In this post, I will move away from numbers and data and studies to give a more qualitative view of how the vaccines’ impacts are manifesting in the “belly of the beast,” (i.e. on the inside of a major academic medical center).
The most profound reflection of this last week came from a patient who is a physician and therapist. She was hospitalized recently for non-COVID reasons and observed: “I think many of the physicians are exhibiting dissociation. It takes an enormous amount of energy to maintain their narrative and hold off the reality hitting them in the face every day.” I thought of this reading the recent piece you referenced from The Annals of Emergency Medicine.
Wikipedia:“The major characteristic of all dissociative phenomena involves a detachment from reality, rather than a loss of reality as in psychosis. Research has suggested that dissociation is inversely related to mindfulness, which is a potential treatment.“
TY PK for this dose of mindfulness.
I thought his comment was the perfect introduction to this post, where I will share disturbing “insider info,” compiled largely from recent correspondences with a senior ICU and ER Nurse, both via email and phone. Although she is not working full-time in ICU’s or ER’s anymore, she still does shifts on occasion, particularly night shifts. Night shifts, although brutal, are WAY more fun and relaxed than day shifts. That is, most of the time, unless you get slammed due to less staff being around. Although the worst shifts of my career were night ones, thankfully they were rare.
What is great about night shifts is the camaraderie and closeness that develops among staff that choose to primarily work nights. The pool of such folks is small, and they choose night shifts for various but often similar reasons (preference, child care responsibilities, other jobs, hatred of day shifts etc). The general atmosphere is more “intimate,” as you end up having conversations, longer and deeper than you would or could in the middle of a hospital day. This is because at night there are no families around, no administrators, most patients are sleeping (sort of), no masses of swirling ancillary specialists like dietitians, physical therapists, occupational therapists, speech therapists, physician sub-specialists, transporters, social workers, food service workers, maintenance folks etc.
Anyway, this was the first email I received from her (editorial note: I wrote out or translated all her abbreviations but made no other edits to substance – I had to do it as her writing style clearly reflected someone who has been writing myriad nursing notes her whole career :).
On May 12, 2022, at 7:47 PM, L. <XXXX> wrote:
I wish I could have you as my doc. Nurse of 20 yrs + ICU – cardiac, neuroICU/ neurosurgical ICU mostly, and ED at Level 1. Vax injured from 2 Pfizer doses mandated by my major University hospital system. Clotting issues, open bleeding, spontaneous with no ability to stop, weeping down arms and legs. Severe leg clot post-surgery in March. Had to get D-Dimer ordered by force at little ED I was in, and use my own portable doppler I brought in from work, b/c they had no Ultrasound techs or equipment access – TPA (clot buster med) finally. Cervical lymph nodes enlarged since vax especially, for over 1.5 yrs. Cannot biopsy at least one as it sits on my Left carotid, now wrapped around it, . Got Covid originally while working ED in March 2020. “N antibody” still high as of Nov 2021. Hit neuro, never respiratory. Had same issues with H1N1 vaccine which was also mandated and then I got Guillain Barre Syndrome and neurological weakness – out of work 5 months. Will not get any boosters or vaccines this year, but have no exemption as all docs took to the “deer in headlight” look and said nothing. I will lose my career this winter if I refuse. Functional med/family practitioner – she has a long wait list and I have no idea how she sits with this data on vaccine injured. My VAERS report – it was deleted. Pharmacist never entered as required so I did. It has vanished. My batch numbers – significant for bad neurologic responses, clotting. I lost my Hematologist-Oncologist doctor to vaccine injury – he is out and never to practice again – in his early 40s. He was a “true believer” and in denial until it was him who was the injured patient. Our cancer hospital – know most of the case managers and many doctors since they were residents. They now have case loads in the 1000s rather than 250-400 over any given quarter. Not enough bed or infusion space for the cancer patients as outpatients. Radiation treatment backlog. All at a huge cancer hospital monstrosity itself. All kinds – brain, lymph, stomach, pancreas, blood, AND EYE CANCERS – orbital especially in younger people recently vaxxed. Microvascular ischemia on rise in vaxxed younger people. Strokes way up in no-risk, no co-morbidities, young to younger-ish. Ask me anything. I’ll tell you inside scoop from the floors and suites. This has to stop. They need to admit the fraud and crime and STOP. The liability must be lifted, mandates ended. They KNOW NOW and many KNEW THEN. Don’t know if you’ll even read this, but I follow all of you on substack and Twitter – those not banned yet! – and read ALL the data. I’ve been a lab rat myself from an issue from a car accident yrs back – I know the process. So much fraud. Keep going. Never give up. Never, never, never give up. Thank you for all you do, hope that you inspire and the confirmation of that little voice in me, that said NO way back, everything was off. I did not have an option or data then. I have data now, and it will keep coming. The option is NO.
Follow up:
Lost 4 practitioners to serious side effects of “strongly encouraged” boosters. 2 hospitalized, one in MICU. The irony is, for most staff, completely lost … All in early 30s to mid 40s. They had no need for boosters while BEING OUTSIDE ALL WEEKEND even if they truly believed in efficacy of them. All had Covid previous, N antibodies fully measurable. One female, one male, both inpatient. Female still nursing newborn.
On Fri, May 13, 2022 at 11:27 AM Pierre Kory <> wrote:
I am stunned by your email. Stunned. We know it’s bad, like real bad but this is the worst inside look I have heard yet. I am on the outside and don’t talk to most former colleagues so don’t have a feel. We should talk. Would you be interviewed on a VSRF (Kirsch’s organization) webinar? I assume not, but who knows, maybe anonymously like with altered voice and blurry screen? This needs to get out. Send me contact… and name? First name is fine… Thanks for this – Pierre
She wrote again before we talked, it was this email below that prompted me to ask her number so we could discuss in more depth:
It’s the inside folks who talk to each other, and you have to speak another language depending on who’s listening. That has been a skill set unto itself. It’s texting, the phone calls from area to area with back stories on patient issues. I was getting texts from my old stat team covering cardiac catheterization lab – the clots. The clots stunned everyone…it continues. My cardiac units – where I spent the bulk of my nursing years – lung and heart transplant included – have so many anomalies presented with patients that never existed before. Re-writing the script for each new problem never encountered. The constant codes (cardiac arrests). Can’t keep up.
Lost quite a few coworkers to either VAX injury itself – took them out of the work force, OR they resigned/accepted firing or retired once mandates were settled. It’s the phone calls I have with my cohorts in the other areas of the system. The real story is in those conversations. The doctors now admitting to injury is growing, but they can’t tell their patients why they are no longer practicing. Losing specialists is big problem not easily solved.
The signaling coming from management MD/PhD administrators has not been towards what winter will bring, but is focused on congratulating everyone on clinical excellence during the last 2 yrs. I think there is great trepidation in their approach because they see the data, they know the inside info on injury, disability/death of faculty and staff not from Covid itself, but the forced vax. We lost only a few to original Covid, with underlying co-morbidities that made outcomes a given in many cases.
I can’t come on a public show, but I can share info. My name is Linda (not her real name). In my current position, I read many charts and see in depth info – so much boosting and reboosting and not following other protocols – it’s a given now that the explosions in diagnosis of the cancers and cardiac issues especially come from these decisions. In some cases, the first thing you see on a chart is huge letters stating VAXXED alongside the pt’s diagnosis, treatments thus far, which is usually at odds with normal disease course, age and projected outcome, etc. They’re pushing the vax status, in bright letters, to the top of the list so it can be considered – not for every patient, but the “challenging cases” … That may be for research purposes.
I will explain the above – what Linda is saying is that practitioners are starting to call out the patient’s vaccination status more clearly on the first screen of the medical record in those cases where they know or suspect the vaccine is related to the patients’s new “mysterious” or “complex” problem. Let’s be clear though, the doctor’s don’t necessarily or explicitly include vaccines as a possible cause in their reasoning/impression/plan section of the patient note. But it seems the nurses and junior docs are now calling it out in some small/large way. Disassociation breaking, ever so slowly?
It makes me just stop, and by end of the week, take into account cases of say, ocular orbital cancer in 20-somethings. Have had 6 in last 2 weeks with no Family History or other indicators. Out of the blue, some with brain mets now. All vaxxed unwillingly, all had Covid and recovered fine prior to employer forced vax. The employers, the areas the patients reside in….nothing in common other than the previous. The actuaries are correct. Excess mortality, let along whatever-life-left disability. Stunning numbers.
I ended up talking to Linda.. about lots of things. She is clearly a fellow spirit, highly experienced in ICU and Emergency medicine, and she told me even more disturbing developments, like the fact that on some night shifts, nurse teams are seeing more cardiac arrests in a single shift than ever before and in unprecedented younger age patients. On some shifts, they have had so many that the “crash carts” are rolled straight from one arrest to another because Pharmacy, especially on night shifts, are not able to re-stock fast enough. This situation has happened maybe once in my whole career… when two arrests happened on the same floor or unit within a short time period.
She also told me that night nurses are more openly discussing the vaccine as the cause of what they are seeing (much more than during day shifts apparently). However, they do this largely in text, and they use “code”. Their code word for a vaccination injury or cause is “that issue,” i.e. in reference to a 22 year old who suddenly arrested on the hospital ward, “he is having that issue.” Note these are nurses.. not the docs.. but some of the docs are talking to her, like the one above who performed 6 enucleations (eyeball removals) this year already in young people (very rare to have to do this, especially in this age group). She also told me about how her interventional cardiologist nurse friends related that some patients are coming in with massive heart attacks, and during the angiogram the interventional cardiologists are seeing such extensive thrombi filling the entire artery (as documented by some embalmers), that they say “I can’t stent or remove this, this guy needs surgery, like now.”
In that conversation with Linda, I was also finally able to confirm a fraud that I had suspected was occurring within U.S hospitals regarding the accuracy (or willful inaccuracy) of the vaccination status listed in the medical record of a patient newly admitted to the hospital. It has long been my strong belief that this fraud drove the U.S data used to support some of the last remaining false narratives (i.e narratives #6 and $7 below) . Note these ever-shifting narratives were all directed at combatting vaccine hesitancy, which as some of you may know, was the primary military objective of the vaccinators.
BMGF/WHO/NIH et al. had clearly identified vaccine hesitancy as the main enemy in the battle plans they drew up and distributed after their viral pandemic simulation exercises over the past decade. In this prominent medical journal publication on addressing viral pandemics, they state “the World Health Organization has listed vaccine hesitancy among the greatest threats to global health, calling for research to identify the factors associated with this phenomenon.” Vaccine hesitancy is why the HHS gave $1 Billion to U.S media to support a relentlessly positive public relations campaign supporting the uptake of vaccines.
Now let’s get back to this fraud. First, note that during all of 2021, (well, up until late November when I was let go from my last pandemic ICU job on a completely fabricated accusation), I had only taken care of one ICU patient that was officially documented in their medical record as “fully vaccinated.” I knew that it could simply not be true that only one patient that I took care of the entire year was fully vaccinated. I knew this was false based on data from countries that more transparently (mistakenly?) reported vaccination status and hospital outcomes. In multiple reports starting in February 2021, the majority of hospitalizations and deaths (even when adjusted to rates per 100,000) had long been the vaccinated.
One of the more ridiculous attempts to cover this fraud up in the U.S was a media narrative launched in June/July of 2021, created from statements by Fauci and Wollensky, that 99% of patients in hospital and dying were the unvaccinated. They literally did this with a straight face, knowing that they were including in their numerator all the deaths that occurred prior to the start of the vaccination campaign. Yup, if you died in 2020, you were reported as dying in an unvaccinated status. Not subtle. But that was not the only lie. We must never forget the famous slip by the NY times.. when they suddenly and surprisingly called out the CDC for “withholding large amounts of COVID data” throughout the pandemic. Umm.. their actual job is to collect and disseminate data. Not subtle. Even crazier is that at the time of that narrative launch, during a lecture, a CDC slide deck mistakenly showed a slide which revealed that 26% of patients in U.S hospitals were vaccinated. But this number was falsely and fraudulently lower than the actual number. By a long shot.
Here is how I think they falsely suppressed the real rate of vaccinated patients entering U.S hospitals and dying:
In the most popular electronic medical record system in the U.S (EPIC), on the sidebar of every page in the chart are the name, demographics, room number, provider team, and COVID vaccination status of the patient. What I found weird from the outset was that, in EPIC, there were only two categories under the COVID-19 vaccine status section, “Vaccinated” or “Unknown.” There was no “Unvaccinated” status. Also realize that “Unknown” was interpreted by all providers and official data as akin to being “Unvaccinated”. Everyone I took care of in the ICU in 2021, except one, had an “Unknown” vaccination status. How could that be? How come only one ICU patient of mine in the entire year was reported as being “fully vaccinated?” Even if the vaccines worked really well (which I knew they didn’t), something was off, like really off.
There was only one hypothesis I could come up with to reconcile these observations. I suspected that during the admission process to the hospital, there must have been some sort of barrier to deeming someone “vaccinated.” I hypothesized that in order to be documented as vaccinated on admission, you had to have received the vaccine from a primary care physician’s clinic who worked for that same hospital system in a system office, and that they had already documented in the electronic medical record. If you got a vaccine from anywhere else outside that hospital system’s clinic, you were assigned an “Unknown”, i.e. “Unvaccinated” status in the electronic medical record.
And lo and behold, Linda confirmed this was the case in one major health system she worked at. What I found most striking is that she worked in two different hospital systems, in one (the smaller one) it was very easy to document a patient in the record as vaccinated. The admitting nurse could accept any documentation, from a Walgreen’s card to even a verbal report from the patient or family and they could put it in the record on admission and the patient would show up as “vaccinated” on the main screen sidebar.
In the other, larger, major (and I mean major) health system she worked in, if the patient received the vaccine from anywhere but an employed provider’s clinic within the health system (even if the patient had a vaccine card on them), she was forced to put it in an “open field” buried on page 2 of the initial nursing assessment not where nobody, and certainly no physician looked for it. All these patients were automatically documented on the main screen as “Unknown”, i.e “Unvaccinated”, even if the dates of each shot were entered into that nursing note field.
This process is what led the vast majority of U.S doctors to become convinced that the only people dying in hospitals were the unvaccinated. Which made perfect sense, I mean, the vaccinators did not want anyone to know the vaccines were not preventing hospital or death, so it would be helpful to their mission if they could make everyone think that all hospital patients were unvaccinated. This way, all the health care workers would get vaccinated out of fear of dying and would also aggressively insist that all their patients and family members get vaccinated. Which is what happened. It is also why a large percentage of the population (at least the ones I meet at lectures, conferences, and symposia) no longer want to see a “system doctor” or go to a “system hospital,” no matter how grand their brand/reputation once was. Fun fact: a long-time donor of large annual gifts to the Mayo clinic.. decided to direct their donation to the FLCCC this year because they felt the Mayo Clinic had departed from their founding principles and mission. Go FLCCC.
The system docs behaved this way because they saw with their own eyes, “the (false) reality” of what would happen if you were unvaccinated. This, combined with the medical journal propaganda publishing only favorable and selective analyses of vaccine efficacy and safety drove nearly all the nation’s doctors to go completely mad.
Their fervor to vaccinate everyone and everything, even in patients who just recovered from COVID, was something to behold. I saw overt hectoring, harassment and even rage. Twitter was one of the most terrifying places to watch doctors arrogantly propagate the need to be vaccinated.. even for folks who had (often hard-earned) natural immunity. I almost feel bad for some of those docs as history will not judge them kindly. Forgive them for they know not what they do. They were literally screaming across Social Media, Media, and Medical Journal editorials, that you will be OK if you just get vaccinated. The high profile docs were the worst, except I have little sympathy for them as some/many/most were likely complicit in the deception rather than just fooled like the rest. Folks like Eric Topol, Peter Hotez, Alastair McAlpine, Tom Friedan (who I used to deeply admire as NYC Health Department Commissioner), Eric Feigl-Ding-(bat), Jeremy Faust (probably the biggest ignoramus on Twitter, having taken an early lead in that competition since the pandemic broke in 2020), and Monica Gandhi. Leana Wen deserves particular ire as she is the most active prostitute for the Pharma-captured federal health agencies on mass media. A media darling as it were.
Then you started to see doctor walk-outs protesting the unvaccinated, increasing numbers of doctors publicly stating they would start refusing to see unvaccinated patients, heck, the Pharma controlled outlet called Medscape even got an ethicist to argue that it was OK to refuse to treat the unvaccinated. Yup. Crazy town. Clown World. One of my patients who is a hospital pharmacist even told me that at her hospital, the hospitalists were vaccinating patients admitted for COVID..as they were being discharged from the hospital. That’s right, as the patients were being discharged after having recovered from COVID, they were recommending and administering vaccines for the same illness. I even heard of one case where a team of clinicians decided to vaccinate a severely ill COVID patient in the ICU.
I also witnessed aggressive attacks in one of the nation’s largest medical-centers staff physician email forum. Doctors “screaming” that everything would be fine if everyone just got the damn vaccine. Deriding anyone bringing forth arguments about untested safety, suspicious efficacy data, and concerns about mandates violating patient autonomy and medical ethics. Anyone who brought forth “adverse data” towards the vaccines were treated with dismissal and a retaliatory posting of selectively favorable data with the imprimatur of the Pharma captured agencies and Pharma captured journals. I will never forget this time in the history of medicine. Ever.
Some other “insights” into the medical system I haver come across, from another ER nurse:
I have no research to offer but first hand experience from working as an RN
in an ER.
Ringing in ears and hallucinations have followed vaccinations in 3 of my
patients. Family members at a loss. I mention the vaccine but most don’t
even hear it…
The gentleman with the ringing in the ears (just had his 4th booster the day
before) I suggested he didn’t get any more boosters as ringing in the ears
is an adverse reaction to the vaccine. His wife looked at me and yelled
“his doctor told him he won’t survive the anti-virals for COViD” I was
speechless. The patient continued on and told me about his experience with
the vaccines 1st shot-he had a seizure, doctor recommended 2nd shot. After
2nd shot he was very sick, doctor recommended 3rd shot and he was
hospitalized 4th shot ringing in ears, abdominal bloating and months away
from dialysis. Wife added that she also had seizure after first vaccine and
she had that attitude that it was no big deal.
I have said this before, it’s criminal what is happening. I have cried on
my way home from shifts, I tell whoever will listen. The information I have
collected over the last 7 months (time of vaccine/booster in relation to
chief complaint) is jaw dropping.
I took a break from working for the summer but continue to keep in touch
with the nurses…
My friend told me about an 80yr old man, 4 strokes in the last year and
they all line up with his 4 shots but the doctors response is “he’s 80,
he’s going to have strokes”
Has anyone come across research in regards to GI bleeds and low hgb? I have
a lot of this patients, GI bleeds out of the blue… and they are young!
I had 28yr old black obese young woman… new diagnosis of enlarged heart
and CHF. Vaccine was roughly 1 month prior to ER admit and I suggested no
more vaccines for COViD and her response was “my doctor told me this
happened because I got the vaccine and a tattoo on the same day”
60ish lady…….just got over COViD (after have 3 COViD vaccines) and she told
me she was going in for second booster next week!!!!!!
Kids are having random seizures and are put on anti-seizure medication for
2 years…when I ask parents what caused the seizure, the neurologist has no
idea. All these children vaccinated for COViD-100%. NO ONE CONNECTS THE
DOTS.
The screenshot below is of 3 days I worked and I’m in the ER for 12 hours
and don’t see all admits. I’m also super busy so it’s hard to check status
of all admit patients… of course this is very limited information but a lot
of the patients have some issue 2-3 months post vaccine/booster.
I’m still shocked we don’t have a “vaccine team” monitoring all the
patients as they come into the ER but no one cares. Not the ER medical
director, not the doctors, not the COViD response team…..no one. Nurses see
it and they are talking but many are fearful of getting fired.
Thank you for all that you are doing! Although I can’t read all the emails,
I am just happy to know that there are others out there that are in the
same boat as I am.
I’m disgusted with the AMA and AAP. I don’t trust a thing they say. I don’t
trust them with my four children as they have not protected our children
over the past 2 years.
Thank you!
And another:
May 26 05:28PM -0400
Katie (not her real name),
Thank you for sharing your story! This is what I live every day and I tell my husband how hard it is to see so much damage. I have had more patients diagnosed with aggressive cancers than I have seen in the last two decades.
… I’ve been so especially concerned about the clotting effects with Total joints treated with Tranexamic Acid. I’ve been keeping track of my patients (that I would consider) have had mild/moderate vax injury. i.e. – reactivation of latent viruses, (oral herpes (not just one or two lesions, but their whole mouth broke out – something that had never happened before) shingles – affecting their eyes, that took more treatment than normal) – Histoplasmosis; *blood clots/Cardiac problems – Stroke from new onset Atrial fib in a patient on blood thinners within 12 hr post injection, Atrial fibrillation in a healthy, athletic 34 yr old male, new onset hypertension without prior history; * Persistent cough, months of diarrhea, migraine, neuropathy of upper extremity to the extent she could not write/type – all extensively checked out without cause. But, all within a few days/weeks/couple months of injection. All my practitioners are still advocating the Vax!!! What do you think we should do??? I’ve got to get the guts to gently visit with our Chief of Staff. CRNA, Colorado
Last one, from a colleague:
Just had dinner with my friend, a colleague friend of his here, Dr XXX renowned YY Physician . PRO Vaccine. Was adamant all physicians should get the vaccine and should not be able to practice without it. Was a trailblazer for the vaccine here. He got boosted around Christmas time, had a stroke less than a week after, lost his eyesight in one eye, lost his practice, cannot be a doctor any longer, and said undoubtedly it was from the Pfizer vaccine and encouraged all of his doctor friends to max out their disability insurance to protect themselves. I know not surprising to you, but this guy was so pro vaccine and clearly admits his stroke and his loss of eyesight from the vaccine!!
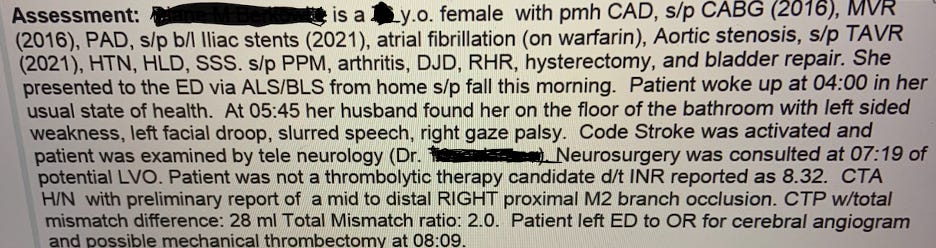
And then there is this doozy – another nurse sent me a case history below of an elderly woman whose blood thinner was highly “supra-therapeutic” (i.e. very thin blood at risk of major bleeding), yet she had a massive stroke caused by a blood clot. This simply does not happen.
On Friday, the FDA released its risk benefit assessment of Moderna’s Emergency Use Authorization (EUA) application to inject mRNA into kids 0 to 17 years old. I’ve been reading it for the past two days and here are the things that stood out to me.
I. Introduction, a shell game to hide the bad data
The risk benefit document for Moderna is 190 pages single-spaced. It was released two business days before the June 14-15 VRBPAC meeting. A similar risk benefit assessment for Pfizer’s EUA application for kids under 5 will be released tomorrow (just 24 hours before the meeting). This guarantees that NONE of the members of the VRBPAC will have read either of these documents prior to the meeting — which is exactly what the cartel wants.
One of the ways that Moderna and the FDA rig the game is by adding endless layers of complexity to hide how bad the data really is. This should have been four separate documents — Moderna in adolescents 12 to 17, Moderna in kids 6 to 11, Moderna in kids 2 to 5, and Moderna in kids 6 months to 23 months. Looked at individually, the shot fails in each of these four age groups. But by lumping them together it creates noise that makes it difficult to understand what’s going on.
Another really pernicious thing that Moderna does is to further subdivide these populations into eight different subpopulations (Randomization Set, Full Analysis Set, Immunogenicity Subset, Per-protocol Immunogenicity Subset, Per-protocol Set for Efficacy, Modified Intent-to-treat Set, MITT1 Set, Safety Set, Solicited Safety Set).
See what they did there? The public just wants to know — does the product work and what are the side effects? By dividing the data into eight subcategories involving four different age groups now you have to wade through 32 different tables to try to make sense of what happened in the clinical trial.
They do something similar with the adverse events by dividing it across five tables x four age groups = 20 adverse event tables in all.
Subdividing the data in this way also allows Moderna to eliminate or hide data that it does not like. This is what people call “massaging the data” and it is unethical and a violation of scientific norms. We’ll return to this topic below.
II. No actual health benefits so Moderna/FDA use the immunobridging trick
The risks of Covid-19 are so low in the childhood population that there were ZERO severe cases of Covid-19 in either the treatment or the control group.
Therefore, the number needed to vaccinate, to prevent a single severe case of Covid-19 in the childhood population is infinity. (Technically it’s undefined because you cannot divide by zero, but you take my point). The FDA and CDC guidance documents for how to write a risk benefit assessment state that one must provide a number needed to treat, the absolute risk reduction, and the relative risk reduction. Moderna just skipped all that because the cartel makes its own rules.
Moderna is in a race against natural immunity. But natural immunity has already won because 74.2% of kids had natural immunity by February — so by now the number is probably closer to 100%. The God-given immune system in kids has already done its part to stop the pandemic and now the FDA wants to mess that up to enrich the cartel and keep the pandemic going forever.
So how does Moderna/FDA claim that this shot was “effective”? They use an unethical statistical trick called “immunobridging.”
It makes me mad that I even have to explain it because it’s such junk science. But we all need to know exactly how the FDA rigged the process so that we can explain to the jury at Nuremberg 2 why these monsters should be convicted so here goes:
Remember, the Moderna shots produced NO reductions in severe outcomes because the risk of Covid-19 in this age group is infinitesimally small (see studies: here, here, here, and here). So Moderna ignored the actual health outcomes and switched to looking at antibodies in the blood. In the process, they engaged in two egregious sleights of hand:
First, Moderna claims that the sample size for each of the four subgroups of children is about 3,000. But when it came to looking at antibodies in the blood, Moderna threw out about 90% of the sample and only looked at the bloodwork of about 300 kids in each age group. No explanation was given for the criteria they used to exclude 90% of the sample from their analysis. We know that up to 30% of kids have no antibody response at all to Covid-19 shots so perhaps they actually started with a much larger sample and then threw out the data that showed no effect from the shot?
The second sleight of hand is that “no placebo recipients were included in the Immunogenicity Subset” (p. 26). Do you realize how huge this is? This is no longer an RCT at all — they did not include the bloodwork from anyone in the placebo group. So the study cannot rule out the possibility that the increase in antibody levels was not from the vaccine at all but could have been from natural immunity. Just astonishing.
After these sleights of hand, Moderna then compares the antibody levels in the blood of about 10% of the children against the antibody levels in a sample of about 300 adults ages 18 to 25 enrolled in a previous clinical trial. If the antibody levels are similar (which they are), Moderna claims, ‘And therefore it will prevent disease in the future in kids!’
A few problems with that claim:
The Moderna study only measured antibody levels two months after the second dose — the time period when the antibody levels are at their peak (what Berenson calls “the happy valley”). But real world experience with these vaccines shows that any efficacy quickly wanes to zero by six months and then goes NEGATIVE after that.
The second problem, and this is unresolvable and instantly disqualifying for Moderna, is that at the April 6, 2022, meeting of the FDA’s “expert advisory committee” one member after another acknowledged that there are no “correlates of protection” for these vaccines. What that means in plain English is that you cannot use antibodies (or B-cells, T-cells, or any other proxy) to predict whether someone is immune or not.
Eric Rubin, who serves on that committee and is also the editor of the NEJM stated it bluntly, “We know what kind of antibody response can be generated, we just don’t know if it works.” You can watch it yourself on video:
The third problem is that the Moderna study was completed back in mid-2021 — when the original Wuhan and Alpha strains were prevalent. Since then, the Omicron variant has entirely replaced the original strains and real world data show that both Moderna and Pfizer shots are not effective against the Omicron variant. So in spite of all of the chicanery (discarding 90% of the sample, immunobridging, claiming correlates of protection that are not valid) Moderna cannot show any evidence that this shot will be effective against SARS-CoV-2 as it exists now.
III. It’s all harms
Let’s talk about harms from this shot (and remember, it’s all harms in this population because the shot made no difference on real world health outcomes). And there, things get really weird really fast.
The median study follow-up duration was just 53 days after dose 2. After that they wiped out the control group. Here’s how they justified it:
Following authorization of an alternative COVID-19 vaccine for this age group on May 10, 2021, participants in the study were permitted to unblind to study treatment. Crossover vaccination with mRNA-1273 of participants initially randomized to placebo began in October 2021. (p. 26)
For each age category, Moderna spreads the adverse events across 5 different tables to increase the noise to hide the signal. But the bottom line is that the adverse events are off the charts.
In the adolescent population 99.2% of vaccine recipients reported at least one adverse reaction after any injection with 25.3% reporting a reaction that was Grade 3 or higher. (p. 54).
Holy sh*t those numbers are high. Grade 3 means: unable to return to work or school the next day because the person is so sick.
A different FDA staffer must have written the summary statements for the other three age groups because they don’t say it this plainly but the adverse event rates are similar across all of the children.
This adverse event data is so high it’s disqualifying.
But then things get even weirder — the adverse event rates in the placebo group were also very high in many, but not all, categories. Moderna used this to say, ‘well yes, the adverse event rate in the treatment group was higher than anything anyone has ever seen before but the rates were also somewhat high in the placebo group and so therefore nothing-to-see-here(TM).’
My strong suspicion in that Moderna rigged the placebo. Why wouldn’t they — the FDA has no regulations concerning the contents of placebos (see Golomb 1995 and Golomb et al. 2010). The dirty little secret of the vaccine program is that manufacturers almost always use rigged placebos to create an artificially high “background rate” to hide adverse events. The brilliant quant Jessica Rose made a similar observation yesterday in her analysis of the FDA risk benefit document:
I still have a very strong suspicion that these ‘placebos’ are not saline and rather empty LNPs. [Lipid nanoparticles — the delivery vehicle that Moderna uses to get mRNA into the cell. An “empty LNP” would be the nanoparticles without the mRNA antigen.]
I’m almost certain this is what Moderna did. In the 2- through 5-year-old age group 37.5% of placebo recipients reported unsolicited adverse events as compared with 40% of vaccine recipients (see p. 139). A number that high in the placebo group would have been impossible if Moderna had used an inert saline placebo.
IV. The way that the FDA rigged the myocarditis data is absolutely sinister
I know that this article is already long but I need to flag one more essential point.
FDA review of the Moderna mRNA shot in adolescents has been held up for a year because the Moderna shot causes myocarditis in this age group — particularly in boys.
So I was curious to see how the FDA would attempt to get around this. And it’s all right there on pages 19 and 20. It’s one of the most chilling things I’ve ever read. The FDA’s argument goes like this:
‘Yes, by spring and summer of 2021 there were already seven high quality studies from around the world showing that mRNA shots increase myocarditis risk. By fall of 2021, the reports continued to come in from the U.K., Europe, Canada, and Nordic countries showing a 2x to 7x increased risk of myocarditis from mRNA shots. Yes, the CDC’s own study of the Vaccine Safety Datalink showed a 2x higher risk of myocarditis from Moderna shots. By May of 2022, we have additional studies from the U.K., Denmark, several Nordic countries, Italy, and France showing a 3x to 7x increased risk of myocarditis from the Moderna shot.’
In all, the FDA cited TWENTY-SIX STUDIES showing that mRNA shots in general, and Moderna in particular, increase the risk of myocarditis.
‘But not to worry!’ the FDA announces in the 4th paragraph in this section. The FDA, CDC, and Kaiser Permanente put their fixers on the case in February and March of this year and made the safety signal shrink down to a more manageable 7% to 50% increased risk of myocarditis and even those results were massaged to make sure that they were not statistically significant, so, nothing-to-see-here(TM). It was the same fixers who they always use — Tom Shimabukuro and John Su — whose entire job is making vaccine safety signals disappear. Those guys are absolutely going to hell.
‘So that’s that,’ the FDA announces. ‘Just ignore those 26 high quality studies from around the world showing an increased risk of myocarditis. Our fixers laundered the data for Moderna so we’re all good.’
V. What is to be done
Children’s Health Defense just launched an excellent 1-click call to action that I highly encourage you to do (and please share it with all of your friends).
Up until Monday night (June 13) at 11:59 p.m. eastern time you can officially register your profound displeasure with the FDA by submitting a formal comment (here) — look for the blue Comment button in the upper left corner of the website. 129,397 comments have already been received — let’s see if we can get that number above 140,000.
If you want to write to public health political appointees, FDA staff, and VRBPAC members, all of their email addresses are here:
Please be polite but let them know that they absolutely must vote NO on the EUA applications from Moderna and Pfizer.
VI. Conclusion
The FDA risk benefit document in connection with the Moderna mRNA shot in kids is dishonest. The public health establishment has abandoned science, logic, reason, rationality, empathy, health, and medicine. The FDA is more than happy to sacrificechildren in order to ingratiate themselves further with the cartel. The proposal to expand the Moderna EUA to kids 0 to 17 is a crime against humanity.
We are absolutely going to win this fight, either in the short term or in the long term. These shots will eventually be withdrawn from the market because they do not work and they cause catastrophic harms. The members of the Vaccines and Related Biological Products Advisory Committee can save themselves a lot of misery (and additional criminal charges at Nuremberg 2.0) by rejecting these applications from Moderna and Pfizer this week.
A growing number of young healthy adults are mysteriously dying. Watch Jefferey Jaxen and Del try to make sense of, what is now being called, “Sudden Adult Death Syndrome” (SADS).
The Vaccine Injury Compensation Program (VICP) is overwhelmed and understaffed with the amount of injury claims being filed from the Covid-19 Vaccines. The program is now on life support and is on the verge of collapse.
The CDC has walked back it’s initial recommendation to mask for Monkeypox, which triggered a firestorm of criticism from the medical and scientific communities.
Pfizer and Moderna have a problem — their Covid-19 shots do NOT work. Everyone knows this. The shots do not stop infection, transmission, hospitalization, nor death. Over half a billion doses of this product have been injected into Americans in the past 17 months and these shots have made NO discernible impact on the course of the pandemic. Far more Americans have died of coronavirus since the introduction of the shots than before they were introduced.
Pfizer and Moderna are making $50 billion a year on these shots and they want that to continue. So they need to reformulate the shots. Maybe target a new variant, maybe change some of the ingredients — who knows, these shots don’t work so it’s not clear what it will take to get them to work. This is a problem because reformulated shots mean new clinical trials and new regulatory review by the FDA. There is a decent chance that any reformulated shot might fail a new clinical trial and the public is deeply skeptical of these shots so the scrutiny would be intense.
So Pfizer and Moderna have figured out a way to use regulatory capture to get their reformulated Covid-19 shots approved WITHOUT further clinical trials. Their scheme is called the “Future Framework” and it will be voted on by the FDA’s Vaccines and Related Biological Products Advisory Committee (VRBPAC) on June 28.
II. Doubling down on a failed strategy
Viruses vary by region. At any given time, the influenza strain circulating in England is different than it is in South Africa which is different than in southeast Asia. However, pharmaceutical companies prefer to create one-size-fits-all vaccines in order to decrease manufacturing costs and thereby increase profits. So the W.H.O. and public health agencies around the world (including FDA and CDC) have created a vast “influenza surveillance network” that identifies the different influenza strains in circulation. Then they engage in an elaborate theatrical performance called the “flu strain selection process” where they select four influenza strains that will go into the one-size-fits-all flu vaccine used throughout the world that year.
This carefully choreographed process is a complete and total failure. This is not a surprise — using a one-vaccine-fits-all approach to prevent a rapidly evolving virus that varies by region is never going to work. Lisa Grohskopf from the CDC’s Influenza Division reports that last year the flu shot was somewhere between 8% and 14% effective (based on data from seven sites that participate in the U.S. Flu Vaccine Effectiveness Network).
But a case study of a flu outbreak at the University of Michigan between October and November 2021 found that the effectiveness of the flu vaccine was literally zero.
Over the last thirty years, the federal government has paid out more compensation for adverse events in connection with the flu shot than any other vaccine — so we know that the shot comes with a high rate of harms. Given that the flu shot does not stop the flu, the harms thus outweigh the benefits.
In a sane world, the WHO, FDA, and CDC would admit that they made a strategic mistake and then change course to find better ways to support the human immune system. But we don’t live in a sane world. Instead, the FDA is proposing to take the failed flu strain selection process and apply it to future Covid-19 shots.
III. The FDA knew that Covid-19 shots would fail but they proceeded anyway
There are a quadrillion x quadrillion viruses in the world (literally more viruses on earth than stars in the known universe). Only a couple hundred of those seem to have the potential to impact human health. But some viruses make better candidates for a vaccine than others. Viruses that have been around a long time, that are very stable and evolve slowly are the best candidates for a vaccine.
Viruses that evolve rapidly are bad candidates for a vaccine. There is no vaccine for the common cold nor HIV because these viruses evolve too quickly. The SARS-CoV-2 virus is a bad candidate for a vaccine which is why all previous attempts to develop a vaccine against coronaviruses have failed (they never made it out of animal trials because all of the animals died during challenge trials or were injured by the vaccine).
What are some of the bad things that can happen when you vaccinate against a rapidly evolving virus? Original antigenic sin, antibody dependent enhancement, and the possibility of accelerating the evolution of the virus in ways that make it more virulent (and even more resistant to vaccination).
Trevor Bedford has his own lab at the Fred Hutchinson Cancer Center where he researches the evolution of Covid-19. He gave a fascinating presentation at the April 6 meeting of the FDA’s Vaccines and Related Biological Products Advisory Committee meeting where he explained that SARS-CoV-2 is evolving rapidly. He explained that SARS-CoV-2 evolves twice to ten times as fast as the flu virus and these mutations “substantially” reduce vaccine effectiveness. Following the introduction of Covid-19 vaccines, the evolution of the virus has accelerated.
Dr. Bedford’s presentation rattled some of the smarter members of the VRBPAC because his data scream — “SARS-CoV-2 is a bad candidate for a vaccine!” But FDA officials just mumbled some platitudes and then continued on with the meeting.
The only way out of the pandemic is to withdraw these vaccines from the market and pivot to therapeutics. Instead, the FDA is proposing to just hide the data from the American people.
IV. The “Future Framework” = no more clinical trials for Covid-19 shots ever again
The purpose of the “Future Framework” is to rig the Covid-19 vaccine regulatory process in perpetuity in favor of the pharmaceutical industry. If this “Future Framework” is approved all future Covid-19 shots, regardless of the formulation, will automatically be deemed “safe and effective” without additional clinical trials because they are considered “biologically similar” to existing shots.
This is literally the worst idea in the history of public health.
If you change a single molecule of mRNA in these shots it will change health outcomes in ways that no one can anticipate. That necessarily requires new clinical trials — which is what the FDA is proposing to skip.
The FDA’s “expert advisory committee” (VRBPAC) met on April 6, 2022 to discuss the “Future Framework” for the first time. All of the committee members agreed that Covid-19 shots are not working, that boosting multiple times a year was not feasible, and that the shots need to be reformulated. They also unanimously agreed that there are no “correlates of protection” that one can use to predict what antibody levels would be sufficient to prevent SARS-CoV-2 infection.
On June 28 the VRBPAC will meet once again to discuss the “Future Framework” and it will be presented as a done deal because manufacturers want a decision on vaccine strain selection by June in order to deliver shots for autumn vaccination appointments.
So if the FDA authorizes Covid-19 shots for kids on June 14 and 15 and then approves the “Future Framework” on June 28th, the shots that will be given to kids in the fall will be the reformulated shots that skipped clinical trials.
V. Monovalent Covid-19 shots failed, so maybe throwing two, three, or four variants into a single shot will make it better?
When it comes to the flu shot, the FDA tries to hedge their bets by putting four strains of the virus into a single shot (so called “quadrivalent” vaccines). As I explained above, this strategy does not work. But these people are not very clever so that’s exactly what they are planning to do with future Covid-19 shots.
Moderna is already signaling that they intend to manufacture a Covid-19 shot with the Alpha variant and then, to make it “new and improved (TM)”, they will add genetically modified mRNA targeting the Beta variant. Here’s the best part — Moderna claims that this formulation (Alpha + Beta) will somehow protect against Omicron variants — even though by the time these reformulated shots get to market, none of these variants will likely still be in widespread circulation.
There are reasons to believe that this approach will make future Covid-19 shots even less effective and more dangerous than the current failed Covid-19 shots.
Think about it. The more mRNA you put into a shot, the higher the adverse event rate (as the genetically modified mRNA hijacks the cell and starts cranking out spike proteins). So if Pfizer and Moderna put more mRNA into these shots (in order to cover multiple variants) adverse event rates will skyrocket.
But if Pfizer and Moderna put less mRNA per variant into a shot (in order to keep the total amount of mRNA at 100 mcg for Moderna and 30 mcg for Pfizer) then the effectiveness against any one particular variant will be reduced.
The Future Framework is 100% guaranteed to fail. If the “Future Framework” is approved, effectiveness of these shots will decrease, adverse events will increase, these shots will fuel the evolution of variants that evade the vaccines, and there will be no clinical trial data before these reformulated Covid-19 shots are unleashed on the unsuspecting public.
VI. Summary
The FDA’s Vaccines and Related Biological Products Advisory Committee will meet on June 28 to vote on a “Future Framework” for evaluating so-called “next generation” Covid-19 shots. The “Future Framework” is a plan to rig the Covid-19 vaccine regulatory process in perpetuity.
The “Future Framework” would take the “flu strain selection process” that fails every year and apply it to future (reformulated) Covid-19 shots. Federal bureaucrats, many of whom have financial conflicts of interests, would choose which SARS-CoV-2 variants to include in a yearly (or twice yearly) Covid-19 shot. In the process, all future Covid-19 shots will be deemed automatically “safe and effective” without further clinical trials because they are considered “biologically similar” to existing Covid-19 shots.
The “Future Framework” is the most reckless idea in the history of public health. It shows that the FDA has completely abandoned science and its statutory duty to protect the public. If the Republic is to survive, we must stop the “Future Framework” before June 28.
VII. Call to action
We have very little time and an enormous challenge in knocking this proposal down before the VRBPAC meets on June 28. So I am asking to you to contact your elected officials to tell them to reject this dangerous proposal.
Below are talking points that you can paste into an email, a script that you can use on the phone, and a tool for looking up your elected officials. I am only asking you to contact 8 officials — the President and Vice President; your two Senators and U.S. Representative; and your Governor, state House/Assembly member, and state Senator. Please be respectful but make it clear that this plan must be stopped.
Talking points (to paste into an email, letter, or fax)
Subject line: NO “flu framework” for future Covid-19 shots
The FDA and CDC are developing a “Future Framework” to authorize future Covid-19 shots without requiring additional clinical trials. This would be a public health disaster. I am asking you to contact the FDA to tell them to stop all work on this “Future Framework” immediately. If the FDA proceeds with this “Future Framework” I am asking you to eliminate all funding for the FDA in this year’s budget.
Phone script
Hi, my name is ____________. I live at __________________[address]. I’m calling because the FDA is proposing a “Future Framework” to authorize future Covid-19 shots without requiring additional clinical trials. This would be a public health disaster. I am asking you to contact the FDA to tell them to stop all work on this “Future Framework”. If the FDA proceeds with this “Future Framework”, I am asking you to eliminate all funding for the FDA in this year’s budget.
Whom to contact: 8 phones calls, letters, emails, or faxes:
President Joseph R. Biden
The White House
1600 Pennsylvania Ave NW
Washington, DC 20500
(202) 456-1111 (The White House comment line is open between the hours of 11 to 3 p.m. EST Tues.-Thurs.) https://www.whitehouse.gov/contact/ https://twitter.com/POTUS
The message for State elected officials is slightly different:
Hi, my name is ____________. I live at __________________[address]. I’m calling because the FDA is proposing a “Future Framework” to authorize future Covid-19 shots without requiring additional clinical trials. This would be a public health disaster. If the FDA proceeds with this “Future Framework” I are asking you to nullify the actions of the FDA and reject any Covid-19 shots that have not gone through proper clinical trials.
This is a great tool to look up contact info for your Governor, state Senator, and state House/Assembly member:
That’s it, just 8 people. We want to let them know that we are watching, that we understand what they are up to, and that this wretched plan must be stopped.
Extra credit:
Here are the email addresses for all of the public health political appointees, FDA staff, and VRBPAC members who have a say in connection with the “Future Framework”. Let’s contact them as well (proposed subject line and email text below).
Subject line: The “Future Framework” is the WORST idea in the history of public health. Please vote NO.
1. The FDA must revoke the authorizations for Moderna, Pfizer, and J&J Covid-19 shots and withdraw them from the market immediately. SARS-CoV-2 was never a good candidate for a vaccine. These shots do not stop infection, transmission, hospitalization, nor death. They appear to have negative efficacy and are driving the evolution of variants that evade vaccines. The pandemic will never stop as long as the FDA and CDC are promoting shots that lack sterilizing immunity.
2. The FDA and CDC must pivot to therapeutics. This was always the answer. About twenty off-the-shelf treatments are more effective than vaccines (if used for prophylaxis or early intervention). Get these safe and effective medicines to people who need them and let doctors be doctors again and treat patients based on their own best clinical judgment.
3. Any reformulated Covid-19 shots MUST go through proper clinical trials and FDA review. That means:
• Large (50,000+ person) double-blind randomized controlled trials with inert saline placebos conducted by an independent third party;
• Safety and efficacy studies for two years prior to any application; the treatment and control groups must be followed for 20 years to monitor adverse events and all-cause mortality (no more wiping out the control group after 6 months to hide bad outcomes);
• Greater than 90% efficacy with less than 1% Grade 3 Adverse Events; and
• Proper monitoring for carcinogenesis, mutagenesis, and impairment of fertility.
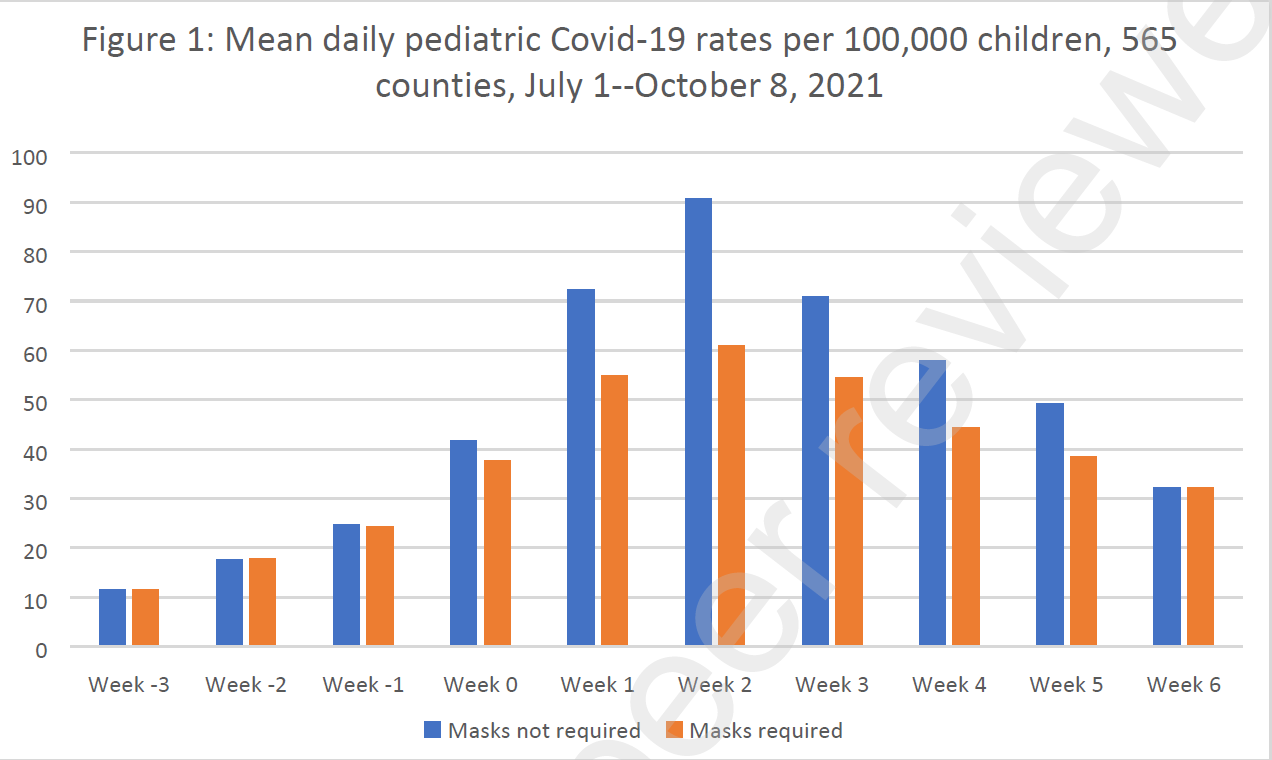
Last year, the CDC published a paper comparing Pediatric COVID-19 Cases in Counties With and Without School Mask Requirements. The authors looked at data from 520 United States counties, concluding that “Counties without school mask requirements experienced larger increases in … case rates … compared with counties that had school mask requirements.” Corona astrologers and face diaper fetishists everywhere have used the findings to argue for forcing healthy children who are at no risk to wear fasks masks for multiple hours each school day.
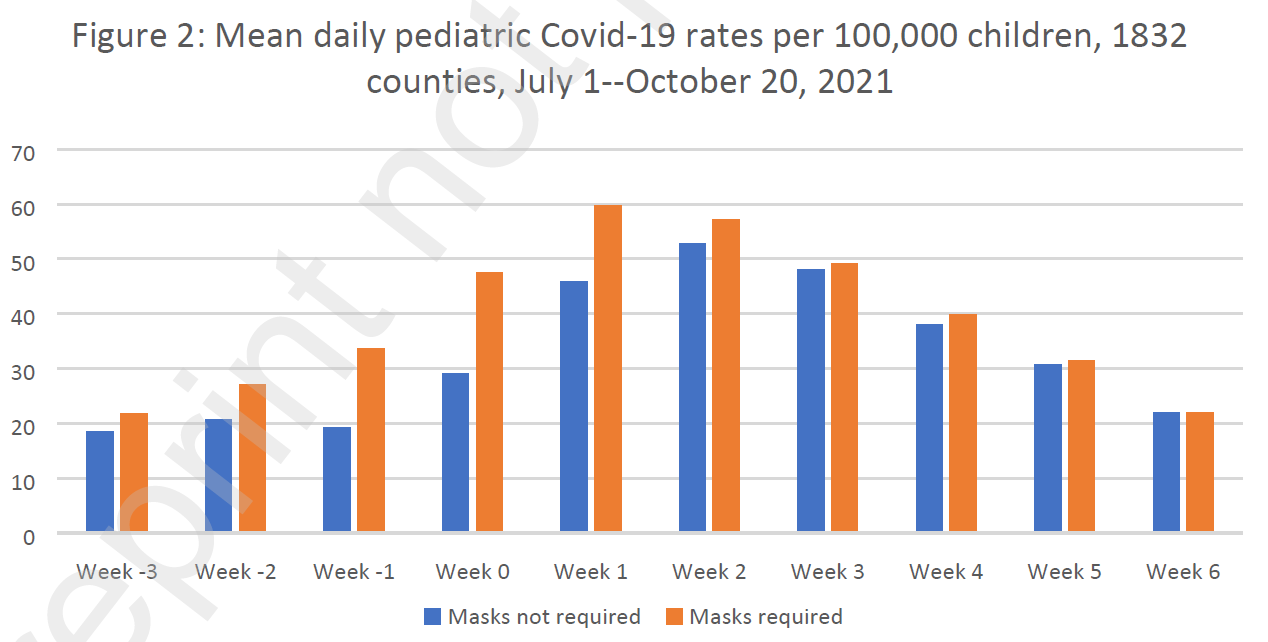
More county-level data on American infection rates and mask mandates has since become available, and two Toronto scientists have taken the opportunity to replicate the study, looking now at 1,832 counties. In a turn of events that will surprise nobody, they find that the larger dataset shows that mask mandates actually do zero, and that prior findings were almost surely an illusion.
Here are masked vs. unmasked case rates, using a smaller data pool similar to that from the CDC study:
Week 0 is the week of school reopening after the summer holidays.
Yes, the maskless counties seem to do worse! Yet the Toronto authors point out that the original CDC study only considered infection rates through the second week after schools reopened, which turned out to be “exactly the peak of school case numbers for [their] sample of counties.” This obscured the fact “that cases quickly declined in later weeks and did so faster in counties without mask mandates.” Even the smaller sample used by the CDC study, in other words, showed no difference in masked vs. unmasked counties by the six-week mark.
The replication, with a much bigger dataset, meanwhile, showed that maskless counties never led infections at all:
Note that, in the larger sample, the maskless start out with lower rates of infections and catch up; in the smaller sample, they started out with higher rates which collapsed more quickly.
The authors note that the CDC study, by ending their analysis on 4 September 2021, effectively excluded counties with a school-start date after 14 August, which entailed an oversampling of southern states. I’ll fill in the blanks here: Counties in the American south tend to have fewer school mask requirements, and also to experience late summer infection spikes related to high temperatures and extensive reliance on climatisation.
Although masks have become the most clearly discredited measure deployed against SARS-2 (which is saying something), they just won’t go away. Even in places that have lifted all Corona restrictions, a great many people continue to mask in public, and it seems likely that many countries – Germany among them – will retain vestigial mask requirements indefinitely, probably for years. Masking is a totally unsupported superstitious practice that does nothing against viral infection, and yet for precisely this reason, no amount of evidence will ever convince the maskers to stop.
Over the past two decades, my company – M·CAM – has been monitoring possible violations of the 1925 Protocol for the Prohibition of the Use in War of Asphyxiating, Poisonous, or other Gases, and of Bacteriological Methods of Warfare (the Geneva Protocol) 1972 Convention on the Prohibition of the Development, Production, and Stockpiling of Bacteriological and Toxin Weapons and Their Destruction (the BTWC).
In our 2003-2004 Global Technology Assessment: Vector Weaponization M·CAM highlighted China’s growing involvement in Polymerase Chain Reaction (PCR) technology with respect to joining the world stage in chimeric construction of viral vectors. Since that time, on a weekly basis, we have monitored the development of research and commercial efforts in this field, including, but not limited to, the research synergies forming between the United States Centers for Disease Control and Prevention (CDC), the National Institutes for Allergies and Infectious Diseases (NIAID), the University of North Carolina at Chapel Hill (UNC), Harvard University, Emory University, Vanderbilt University, Tsinghua University, University of Pennsylvania, many other research institutions, and their commercial affiliations.
***
The National Institute of Health’s grant AI23946-08 issued to Dr. Ralph Baric at the University of North Carolina at Chapel Hill (officially classified as affiliated with Dr. Anthony Fauci’s NIAID by at least 2003) began the work on synthetically altering the Coronaviridae (the coronavirus family) for the express purpose of general research, pathogenic enhancement, detection, manipulation, and potential therapeutic interventions targeting the same. As early as May 21, 2000, Dr. Baric and UNC sought to patent critical sections of the coronavirus family for their commercial benefit.1 In one of the several papers derived from work sponsored by this grant, Dr. Baric published what he reported to be the full length cDNA of SARS CoV in which it was clearly stated that SAR CoV was based on a composite of DNA segments.
“Using a panel of contiguous cDNAs that span the entire genome, we have assembled a full-length cDNA of the SARS-CoV Urbani strain, and have rescued molecularly cloned SARS viruses (infectious clone SARS-CoV) that contained the expected marker mutations inserted into the component clones.”2
On April 19, 2002 – the Spring before the first SARS outbreak in Asia – Christopher M. Curtis, Boyd Yount, and Ralph Baric filed an application for U.S. Patent 7,279,372 for a method of producing recombinant coronavirus. In the first public record of the claims, they sought to patent a means of producing, “an infectious, replication defective, coronavirus.” This work was supported by the NIH grant referenced above and GM63228. In short, the U.S. Department of Health and Human Services was involved in the funding of amplifying the infectious nature of coronavirus between 1999 and 2002 before SARS was ever detected in humans.
Against this backdrop, we noted the unusual patent prosecution efforts of the CDC, when on April 25, 2003 they sought to patent the SARS coronavirus isolated from humans that had reportedly transferred to humans during the 2002-2003 SARS outbreak in Asia. 35 U.S.C. §101 prohibits patenting nature.
This legality did not deter CDC in their efforts. Their application, updated in 2007, ultimately issued as U.S. Patent 7,220,852 and constrained anyone not licensed by their patent from manipulating SARS CoV, developing tests or kits to measure SARS coronavirus in humans or working with their patented virus for therapeutic use. Work associated with this virus by their select collaborators included considerable amounts of chimeric engineering, gain-of-function studies, viral characterization, detection, treatment (both vaccine and therapeutic intervention), and weaponization inquiries.
In short, with Baric’s U.S. Patent 6,593,111 (Claims 1 and 5) and CDC’s ‘852 patent (Claim 1), no research in the United States could be conducted without permission or infringement.
We noted that gain-of-function specialist, Dr. Ralph Baric, was both the recipient of millions of dollars of U.S. research grants from several federal agencies but also sat on the World Health Organization’s International Committee on Taxonomy of Viruses (ICTV) and the Coronaviridae Study Group (CSG). In this capacity, he was both responsible for determining “novelty” of clades of virus species but directly benefitted from determining declarations of novelty in the form of new research funding authorizations and associated patenting and commercial collaboration. Together with CDC, NIAID, WHO, academic and commercial parties (including Johnson & Johnson; Sanofi and their several coronavirus patent holding biotech companies; Moderna; Ridgeback; Gilead; Sherlock Biosciences; and, others), a powerful group of interests constituted what we would suggest are “interlocking directorates” under U.S. anti-trust laws.
These entities also were affiliated with the WHO’s Global Preparedness Monitoring Board (GPMB) whose members were instrumental in the Open Philanthropy-funded global coronavirus pandemic “desk-top” exercise EVENT 201 in October 2019. This event, funded by the principal investor in Sherlock Biosciences and linking interlocking funding partner, the Bill and Melinda Gates Foundation into the GPMB mandate for a respiratory disease global preparedness exercise to be completed by September 2020 alerted us to anticipate an “epidemic” scenario.
We expected to see such a scenario emerge from Wuhan or Guangdong Province, China, northern Italy, Seattle, New York or a combination thereof, as Dr. Zhengli Shi and Dr. Baric’s work on zoonotic transmission of coronavirus identified overlapping mutations in coronavirus in bat populations located in these areas.
This dossier is by no means exhaustive. It is, however, indicative of the numerous criminal violations that may be associated with the COVID-19 terrorism. All source materials are referenced herein. An additional detailed breakdown of all the of individuals, research institutions, foundations, funding sources, and commercial enterprises can be accessed upon request.
Note
This work was supported, in part, by a fund-raising effort in which approximately 330 persons contributed funds in support of the New Earth technology team and Urban Global Health Alliance.
It is released under a Creative Commons license CC- BY-NC-SA. Any derivative use of this dossier must be made public for the benefit of others. All documents, references and disclosures contained herein are subject to an AS-IS representation. The author does not bear responsibility for errors in the public record or references therein. Throughout this document, uses of terms commonly accepted in medical and scientific literature do not imply acceptance or rejection of the dogma that they represent.
This is the fourth instalment of Paula Jardine’s six-part investigation into the planning behind ensuring vaccine acceptance and countering vaccine ‘hesitancy’. You can read Part 1, published on Wednesday, here, Part 2, published on Thursday, here, and Part 3, published yesterday, here.
WHEN Unicef launched the Child Survival Revolution in 1983, it openly acknowledged that infectious childhood diseases in industrialised countries had ceased to be a serious threat before vaccines were introduced, thanks primarily to improvements in sanitation and nutrition.
Later, something resembling a bait and switch took place in traditionally accepted scientific thinking on this empirical observation. The US Centers for Disease Control (CDC) now brands the central role played by improved sanitation and nutrition an anti-vaccination myth, and largely credits vaccines for the reduction in disease burden instead. This amounts to a misrepresentation, an untrue statement of a material fact that is being used to inflate the past performance of vaccines. It would count as unlawful mis-selling in other commercial contexts.
The World Health Organisation (WHO) says: ‘Immunisation is a global health and development success story, saving millions of lives every year.’ It puts the number of lives saved annually at between 3.5million and 5million.
Yet, perversely, universal vaccination may be masking health and mortality problems that arise from the vaccines as, by definition, there’s no control group for comparison. Igor Chudov analysed the 2021 statistics from Florida: ‘What I found is that in 2021, parents of newborns in Florida were much more “vaccine hesitant”, for reasons obvious to my readers, and therefore childhood vaccinations decreased from 93.4 per cent previously to only 79.3 per cent in 2021. During the same time, “all cause” infant mortality under one year of age in Florida also DECREASED by 8.93 per cent.’ (his emphasis)
Chudov’s findings chime with those of Australian physician Dr Archie Kalokerinos who investigated a doubling of the infant mortality rate in Aborigine communities in the 1970s on behalf of the Northern Territories government. He discovered the death rate rose after they began vaccinating malnourished Aborigine children. In some communities, every second child was injured or died.
A 2021 vaccination impact study led by Professor Neil Ferguson of Imperial College London made the great claim that vaccine campaigns in low and middle income countries had saved a total of 23million children’s lives over the past two decades, and projected that this figure will increase to 37million by 2030. But as with any honest cost-benefit analysis, Ferguson’s estimates need to be offset against another statistic. GAVI itself acknowledges that vaccination campaigns had, until a decade ago, negligently added to the chronic infectious disease burden in the developing world: ‘In 2000, roughly 39 per cent of all healthcare-related injections administered globally were delivered with reused disposable or inadequately sterilised syringes, which resulted in an estimated 23 million people infected annually with hepatitis B, hepatitis C and human immunodeficiency virus (HIV).’
It took a decade to reduce these incidental infections to near zero by using disposable syringes.
The example that is used to generate sufficient anxiety or fear is measles, a highly transmissible virus which remains a leading cause of death in parts of Africa and Asia. The CDC insists that getting the vaccine is safer than getting the disease yet provides no statistics to illustrate the relative risk.
According to the UK-based Vaccine Knowledge Project, ‘in high income regions of the world such as Western Europe, measles causes death in about 1 in 5,000 cases, but as many as 1 in 100 will die in the poorest regions of the world. Worldwide, measles is still a major cause of death, especially among children in resource-poor countries.’ One US-based website aimed at public health students and practitioners ignores the nuance, putting the risk of death from measles at 1 in 500 while selectively setting it against a one in a million chance of an allergic reaction to the MMR and ignoring the risk of all the other potential adverse reactions on the US government’s official table of measles vaccine injuries.
Internal documents at the Centers for Disease Control (CDC) show that Rep. Thomas Massie (R-Kentucky) ignited quite the firestorm when he contacted the agency to point out serious Covid vaccine disinformation that their top officials and vaccine scientists had signed off on.
I reported on the story last year after Massie produced audio recordings of CDC officials and scientists admitting the error to him, yet continued to publicly make the false claim: that original studies proved Covid vaccines helped people who’d already had Covid. They didn’t.
Watch the story and listen to the CDC audio recordings here.
Recently, emails obtained through a Freedom of Information request show more than a thousand pages of emails mentioning Massie and his concerns swirled around at CDC.
What did they say? Well, much of the time we don’t know because that’s hidden behind big, blue redactions.
Public info redacted by CDC regarding the agency’s Covid vaccine disinformation
We do see that before admitting the claim was wrong, CDC scientists tried to defend their false information.
CDC scientists and officials first attempt to defend the false info they were publicizing about Covid-19 vaccines
CDC scientists and officials try to defend the false info they were publicizing about Covid-19 vaccines
CDC also apparently tracks and logs CDC-related tweets by members of Congress, broken down by party affiliation.
CDC tracking tweets by members of Congress
CDC tracking tweets by members of Congress
It’s unclear why conversations between CDC officials and scientists on matters of great public health importance would be kept hidden from public view.
Nobody was held publicly accountable for the serious and potentially dangerous false information the CDC officials and scientists signed off on and publicized.
STAT News has a new article titled, “The ‘five pandemics’ driving 1 million U.S. Covid deaths.” Like almost everything they publish, the article is clever, well-written, and almost entirely wrong. The author, J. Emory Parker, claims that the pandemic is primarily a story of older, unvaccinated, rural, poor people with a deadly initial wave that has faded into a lower infection fatality rate today. I’m not going to refute it point-by-point other than to say that he is missing the forest for the trees.
Democrats now interpret all data through the lens of The Narrative(TM) that makes Dems look like heroes, Pharma look like Gods, and Republicans look like unwashed barbarians who deserve death for their failure to obey their betters. It’s not so much science as bougie-supremacy. Self-reflection, paradox, and admitting mistakes are of course banned from the bougie lexicon.
In this short article, I’ve stolen his title (in hopes of messing with the search engines) and I set the record straight. Any honest assessment of the last two years leads to the inexorable conclusion that every facet of the pandemic is a direct result of the intellectual and moral failures of the “expert class” itself.
1. Tony Fauci created the pandemic by funding risky gain-of-function research at a bioweapons lab in Wuhan China. Somehow a chimera virus, engineered to be more lethal to humans, escaped. No Tony Fauci, no pandemic. All else flows from this.
2. Fauci, the FDA, and CDC blocked access to prophylaxis and early treatment. The CDC’s own research showed that chloroquine is safe and effective for prophylaxis and early treatment of SARS coronaviruses (hydroxychloroquine is even safer than chloroquine). The U.S. had a massive stockpile for this very purpose that was never used. About 90% of Covid-19 fatalities in the U.S. could have been prevented if public health officials had followed proper protocols and used about twenty off-the-shelf treatments that are safe and effective. Instead the FDA and CDC ridiculed the best treatments, stopped doctors from prescribing them, and prohibited pharmacies from filling these prescriptions.
3. Hospitals used the wrong protocols and continue to use the wrong protocols. Failing to provide early treatment (turning people away from hospitals to preserve capacity), ventilators, and Remdesivir are all death sentences. Large hospitals have such abysmal outcomes because they used the wrong protocols and they seem to have no ability to course-correct based on actual data.
4. Blue states that followed the CDC’s advice to return Covid+ patients to nursing homes committed senicide — the systematic murder of the elderly. The death toll in the elderly was and is so high because they were never provided prophylaxis, immune support, nor any early treatment and their residences were intentionally seeded with the sick — once again in the misguided attempt to preserve hospital capacity(TM).
5. Promoting mass injections with negative efficacy, keeps the pandemic going indefinitely. These useless shots also seem to be driving the evolution of variants. The pandemic will never end as long as the government continues to promote these mRNA shots that lack sterilizing immunity.
The entire pandemic, from the origins, through the early days, until now, is a self-inflicted, man-made crisis. This is iatrogenic pandemicide — created, spread, and made more deadly by the people who claim that they are “experts”. Everything that public health has done for two years has made things significantly worse. As long as the people who are wrong about everything remain in power, the crisis will continue.
It has been two weeks since a United States district court struck down President Joe Biden’s mandate, imposed through the Centers for Disease Control and Prevention (CDC), that people wear masks when traveling via public transportation, or by taxi or ride-share service, as well as when at related locations, such as airports. After the court decision, most transportation companies and locations have been quick to make clear that people are free to leave their faces uncovered. Many people have been very happy to do just that.
The CDC, however, has not given up on hectoring people to “wear your mask.” On Tuesday, the CDC released a “media statement” titled “CDC Recommendation for Masks and Travel.” Starting off, the media statement declares that the CDC “recommends that everyone aged 2 and older – including passengers and workers – properly wear a well-fitting mask or respirator over the nose and mouth in indoor areas of public transportation (such as airplanes, trains, etc.) and transportation hubs (such as airports, stations, etc.).” Further, the CDC states that it encourages “operators of public transportation and transportation hubs to support mask wearing by all people, including employees.”
Fortunately, the response of many individuals and businesses to this advice ranges from “whatever” to “leave me alone.” More and more people have gotten over inflated fear of coronavirus that never posed a threat of major sickness or death to most people. People have also progressively become aware of the absurdity and destructiveness of forced business closures, “social distancing,” ubiquitous coronavirus testing, experimental coronavirus “vaccines,” mask mandates, and other pseudoscience actions the CDC has pushed since 2020.
America is largely back to the good old days of most people ignoring for the most part when government “public health officials” and people in the media relate CDC guidance that people do this or that. Plus, given the horrid track record of the CDC through the coronavirus scare, more people are now aware of the charade of CDC guidance than ever before. Instead of just ignoring CDC recommendations, many more people than before will feel the urge to research the recommendations and publicly challenge the recommendations when they are found wanting. There should now hopefully also be much more steadfast resistance from the start to any new effort to morph recommendations from the CDC or other so-called health experts into mandates.
Still, the CDC’s media statement this week and the US government hanging on to other coronavirus crackdown measures, including coronavirus shots and testing mandates, to the extent the measures have not been struck down by courts, show that the threat of grand scale tyranny in the name of countering a new purported health crisis remains. In addition, some state and local governments are both holding on to the remnants of coronavirus tyranny and remaining ready to jump back into much more expansive action suppressing freedom in the name of public health.
People must remain vigilant. People must spread the message that the lesson from the coronavirus crackdown is that government violations of individual rights in the name of advancing public health objectives or countering the new disease of the day must be resisted resolutely and vociferously.
People should also keep in mind that, in a variety of circumstances, doctors and other people working the medical field may provide advice that is grounded in the CDC’s priorities and runs counter to the best medical course.
The lure of evil remains strong. To ensure that respect for freedom regained from the coronavirus crackdown tyrants does not fade away, people must remain on guard against and adamantly refuse to accept new encroachment efforts. To keep what has been regained of the good old days, and even expand upon it, people must take action, starting with saying “no” to the health authoritarians at the CDC and elsewhere.
By Dr. Elias Akleh | Global Research | July 3, 2018
The Zionist Israeli state calls on the Old Testament/Torah as a historical document to prove its legality to “re-claim” Palestine; their god’s promised land. To assert this legality and the myth of the promised land Zionist Organization, since its establishment, had recruited the science of archaeology, employing western Christian biblical archaeologists, to provide the required “historic” proof of the right of the Jews; alleged modern Israelites, to Palestine. This became very critical after Julius Wellhausen; the biblical scholar and Professor Ordinarius of Theology and head of the German School of Biblical Criticism, published his 1883 book “Geschichte Israels”, later titled as “Prolegomena zur Geschichte Israels” claiming that the Old Testament/Torah stories were invented during the Babylonian exile to serve certain theological and political purposes.
American biblical scholars and archaeologists, such as William Fox Albright, were recruited to refute Wellhausen’s claims. Albright was endorsed by covertly Zionist financed Biblical Colloquium; a scholarly society devoted to the analysis and discussions of biblical matters, and the preparations, publication, and distribution of biblical literature to brainwash readers and students with a specific theological ideology. Albright, as well as other biblical archaeologists like him, was also honored (bribed) by the American Friends of the Israel Exploration Society. His writings; such as “Why the Near East Needs the Jews”, are flagrant racist Zionist propaganda ignoring the vast archaeological history of the indigenous Palestinians while emphasizing the fake unproven Israelites’ narrative in Palestine. … continue
This site is provided as a research and reference tool. Although we make every reasonable effort to ensure that the information and data provided at this site are useful, accurate, and current, we cannot guarantee that the information and data provided here will be error-free. By using this site, you assume all responsibility for and risk arising from your use of and reliance upon the contents of this site.
This site and the information available through it do not, and are not intended to constitute legal advice. Should you require legal advice, you should consult your own attorney.
Nothing within this site or linked to by this site constitutes investment advice or medical advice.
Materials accessible from or added to this site by third parties, such as comments posted, are strictly the responsibility of the third party who added such materials or made them accessible and we neither endorse nor undertake to control, monitor, edit or assume responsibility for any such third-party material.
The posting of stories, commentaries, reports, documents and links (embedded or otherwise) on this site does not in any way, shape or form, implied or otherwise, necessarily express or suggest endorsement or support of any of such posted material or parts therein.
The word “alleged” is deemed to occur before the word “fraud.” Since the rule of law still applies. To peasants, at least.
Fair Use
This site contains copyrighted material the use of which has not always been specifically authorized by the copyright owner. We are making such material available in our efforts to advance understanding of environmental, political, human rights, economic, democracy, scientific, and social justice issues, etc. We believe this constitutes a ‘fair use’ of any such copyrighted material as provided for in section 107 of the US Copyright Law. In accordance with Title 17 U.S.C. Section 107, the material on this site is distributed without profit to those who have expressed a prior interest in receiving the included information for research and educational purposes. For more info go to: http://www.law.cornell.edu/uscode/17/107.shtml. If you wish to use copyrighted material from this site for purposes of your own that go beyond ‘fair use’, you must obtain permission from the copyright owner.
DMCA Contact
This is information for anyone that wishes to challenge our “fair use” of copyrighted material.
If you are a legal copyright holder or a designated agent for such and you believe that content residing on or accessible through our website infringes a copyright and falls outside the boundaries of “Fair Use”, please send a notice of infringement by contacting atheonews@gmail.com.
We will respond and take necessary action immediately.
If notice is given of an alleged copyright violation we will act expeditiously to remove or disable access to the material(s) in question.
All 3rd party material posted on this website is copyright the respective owners / authors. Aletho News makes no claim of copyright on such material.