This particular note spoke loudly to me and this lovely person gave me permission to share her words
“Dear Jessica,
I have been following your work for some time now. I thank God for you and your truth telling during this dark day of medical experimentation.
I’m sending this email to you to add colour to your work analyzing data. I know the trends and the data are vitally important but so are anecdotes and stories.
I have a 3 year old daughter and gave birth to my son in November. He’s almost 8 months now and, thank God, very healthy. I live in Fort Warrior.
[JUST FOR CONTEXT] I am unvaccinated (or un-injected is maybe what we should say). I knew I wanted to get pregnant in early 2021 and decided in advance that I wouldn’t take the jab based on the precautionary principle. I tend to be more skeptical of doctors and pharma than most — I favour nutrition and lifestyle interventions first but I know a lot of people feel “safe” going to their doctor for a pill/pharmaceutical that ails them. I kept a lot of my opinions to myself.
Fast forward to my first OB appointment in June of 2021. They were all over me about getting the COVID-19 jab at my appointment. I never brought it up, they did. The nurse practitioner fielding intake questions advised me of the following:
– the vaccine was highly recommended by the College of Obstetrics and Gynecology;
– the vaccine stays in the arm, and generates an immune response through antibodies that will also protect the baby (and do cross the placenta);
– pregnant women are at an especially high ICU risk and there have been bad outcomes;
– I’m at higher risk of infection because I have a child in daycare;
– they don’t have “long-term” safety data but they have no reason to believe that the vaccine is unsafe;
– pregnant women have priority on the vaccine.
I am a rule-follower so even though I had made the decision in advance to not take this death jab, it was a rattling appointment. It honestly caused me so much stress throughout the pregnancy because I felt they made it seem like you were doing something wrong if you didn’t get this death jab. Every doctors’ appointment had me so stressed and worried. You have this guilt about not doing “as the doctor told” and then worrying that if you got COVID and something did happen, they’d all be rolling your eyes and treating you like shit. I gave birth in a mask, but thank God everything went well and my son is healthy.
Since these jabs rolled out, I know of one woman who had a stillbirth a month before her due date. Devastating. I also have a good friend whose baby is having many health problems. Her first baby was born the same time as my first and didn’t have any of these problems. I notice too that doctors are not connecting the dots. One of the issues my friend’s baby has is a heart murmur. I’m no expert on this but she said to me that the cardiologist told her that up to 1/3rd of babies have murmurs and they just go away on their own. That didn’t sound right to me but I don’t know. She also said the baby had to go to physio and had a virus (and got COVID). It just seemed like there were so many issues and she never even raised the possibility that it might be related to taking the vax during pregnancy. Another colleague of mine who got the jab and booster while she was breastfeeding said her daughter had green poop for a week after the booster and that she lost her supply. She actually took her baby to Sick Kids and they told her she was basically crazy.
My cousin also didn’t get the jab and gave birth around the same time as me. Her baby is doing good. Got Covid at 2 months old and recovered faster than my cousin’s whole family who got it at the same time. Seems to fit the trend in the data.
I have so much rage and anger over this because I was so close to putting my baby at risk because of intense pressure from the OB office and from the mandates they rolled out at my work. I was able to get an “accommodation” because I started the job in March and had been working entirely from home and was about to take a leave. But it was gross listening to the head of HR at my job talking about the news related to “pregnant people” (ugh) and how vulnerable they were as she condescendingly implied that I was a moron for not doing more to protect my son.
Babies are being maimed; harmed. Women are being gaslighted. Breastmilk, which is literally medicine for a growing baby, is contaminated and causing harm because of these disastrous injections. This is evil. My heart is breaking every day. Every time I breastfeed my son with my milk I am so emotional. I want more kids but I’m terrified of the medical system. They doctors are in on this crime and are deliberately ignoring obvious data. I don’t even want to take my son back to the doctors for anything. It feels like going to a crime scene. I think of all the women I know who got this shot but want kids one day. They don’t even know what they’re in for and for their sake I hope I’m wrong, but damn.
I still don’t get the feeling people are waking up in Fort Warrior. I have a few friends who are aware, but they oppose all vaccines (and the more I read, so do I) so they were already for sure never going to get this experimental one. It feels really repressive here. People want to forget the medical tyranny and apartheid rolled out in the fall and pretend like we can just move on from the darkness.
I don’t know where things will go from here, but I’m so very grateful for your courage. I also appreciate the way you explain scientific findings in interviews. It’s really helpful.
Sending you so much love, mental, physical and spiritual health as you do this work. I am sure it’s so taxing to comb through these tragedies, but you are performing a vital human service.”
In gratitude, I stand. With mighty power.
July 18, 2022
Posted by aletho |
Civil Liberties, Deception, Science and Pseudo-Science, Timeless or most popular | Covid-19, COVID-19 Vaccine, Human rights |
Leave a comment
The BBC is either the worst media organisation on Earth or the best, depending upon your perspective. On the one hand it is a truly world-class propaganda machine. On the other it is completely incapable of challenging government narratives or power because it is effectively a branch of the UK government and is itself beholden to power.
As an agency of the state, the BBC has actively sought to destabilise overseas governments around the world. It is a master of propaganda and frequently lies to the public, either overtly or by omission, with the goal of convincing the people to accept whatever falsehood or agenda it has been tasked to sell.
From top to bottom, the BBC’s commitment to journalistic integrity is missing. It is simply a mouthpiece for the ruling cartel. It comprehensively fails to deliver the most crucial social function of journalism: holding power to account.
According to the corporation’s published values, “trust is the foundation of the BBC.” The Oxford English Dictionary offers a pejorative meaning of the word “trust”: “acceptance of the truth of a statement without evidence or investigation.”
This definition of “trust” seems appropriate for the BBC. While it declares itself to be “independent, impartial and truthful,” it routinely trots out claimed “facts” that lack supporting evidence and produces investigative reports absent any real investigation. Indeed, the BBC broadcasts appalling lies as a matter of course.
And so it is with a certain degree of mirth that we now learn from the BBC that it intends to air a “documentary” about a phenomenon it has already opted to call “vaccine hesitancy.” (Bear in mind: A “documentary” is “a film or television or radio programme that gives facts and information about a subject.”)
The producer of the upcoming programme, due to air on the 20th of July, Craig Hunter, explains:
Moving beyond the often misrepresented debate, this programme reveals why some people remain vaccine hesitant.
The deprecatory word “hesitant” means “tentative, unsure, or slow in acting.” There is no room in the programme-maker’s minds for the possibility that people who chose to remain “unvaccinated” have considered the risk-benefit of these shots, have looked at the available evidence and have decisively concluded that they don’t want a COVID-19 jab.
Hunter’s statement absolutely “misrepresents” the debate. As Craig is the producer of the forthcoming BBC documentary, it seems the chance of the programme delivering a balanced exploration of the issue is remote to non-existent. There is little reason to expect the BBC to provide anything that is “independent, impartial and truthful.”
Indeed, objectively discussing any facet of the alleged pandemic is way beyond the reach of the BBC. As a state propaganda operation, all it can do is parrot the official narrative spouted by the government and its partners, who are, in this instance, the pharmaceutical corporations.
In its press release announcing the documentary, the BBC claims that the programme will focus on:
. . . confronting the latest science and statistics to emerge in the field and dissecting how misinformation spreads on social media.
The BBC cannot succeed in this task because the science and the statistics rarely support the disinformation it has been commissioned to spread. Consequently, it must deceive and misdirect its audience to make sure they believe its propagandist tripe. More to the point, the BBC is itself one of the most prolific distributors of online misinformation.
For example, in its press release the BBC says:
After multiple lockdowns and more than 197,000 deaths, experts are warning we’re now entering a fifth wave of the pandemic. So why are five million adults in the UK still yet to receive a single dose of the vaccine?
Putting aside for the moment that there are actually more than eleven million UK adults yet to receive a single dose of the vaccine and the fact that the BBC itself reported that there were just three million less than a week later, the rest of this claim assumes, without good reason, that there was a “pandemic” in the first place. We now know there is very little evidence that a genuine pandemic ever occurred, yet the BBC keeps up its charade by omitting key facts.
Here is one such key fact: In 2009 the World Health Organisation (WHO) suddenly and radically changed its long-time definition of the word “pandemic.” It removed the defining phrase “several, simultaneous epidemics worldwide with enormous numbers of deaths and illness,” replacing it with reference to a disease for which “most people do not have immunity.” Under this definition, practically any new disease can be declared a pandemic. But the BBC won’t inform its audience of the WHO’s changed definition nor the fact that under the original, and more valid, definition, COVID-19 disease could never have been described as a pandemic.
The BBC has left its audience in the dark about a number of other important facts: (1) as of the 19th of March 2020, UK public health authorities did not consider COVID-19 to be “a high-consequence infectious disease” due to its low mortality; (2) all-cause mortality (the overall death rate) in 2020, the year of the so-called “outbreak,” ranked as only the 9th highest death rate in the first two decades of the 21st century; (3) people with injured limbs and stomach pain were being admitted to hospital as registered COVID-19 patients, thus giving an entirely false impression of a severe pandemic disease; (4) there is no statistical evidence of any beneficial effect from any supposed COVID-19 vaccine; and (5) many deaths have been caused, not by any single disease, but by the policy response to an alleged pandemic.
In the press release for its upcoming “documentary,” the BBC refers to the figure of 197,000 UK deaths from COVID-19 as if that figure is scientifically or statistically indisputable. Not only can it be questioned, it has been! So why doesn’t the BBC mention this?
By deliberately using the largest possible figure, the BBC is attempting to elicit an emotional reaction to the highly questionable number of supposed COVID deaths. The BBC is playing on people’s emotions in order to avoid any objective analysis of the data. Its intention is to manipulate its audience into unquestioning acceptance of a story about a severe pandemic which does not stand up to scrutiny.
Let’s pause to make an important point: The collection, analysis and reporting of COVID-19 mortality data has been deliberately altered and manipulated by governments around the world, all of which worked and continue to work in partnership with the WHO. Nowhere has this manipulation been more pronounced than in the UK, where the engineering of COVID-19 mortality statistics has been quite remarkable.
Mainstream media outlets, especially the BBC, have perpetuated baseless fearmongering. For example, for the first time in the history of reporting deaths from a respiratory disease, propagandists like the BBC are reporting cumulative deaths instead of the annual mortality rates or the more common seasonal variation in these figures. If the same were done for, say, influenza, total flu deaths would be measured in millions, depending on the chosen start date for the accumulation of the mortality data.
Another example: The BBC has chosen to report what the government claims to be “deaths with COVID-19 on the death certificate.” While some of these likely were genuine COVID-19 deaths, the expansive, all-encompassing methodology that the government and the WHO created to attribute as many deaths as possible to COVID-19 renders the bulk of these statistics virtually meaningless. In truth, we don’t know how many people in the UK have died as a direct consequence of COVID-19, though estimates in the region of 20,000 – 25,000 seem reasonable.
The BBC never questions the mortality statistics. It simply takes the figures from the government and reports them without any investigation or analysis. This is essentially the BBC’s purpose: to report whatever it is told to report.
In announcing its faux documentary, the BBC says:
In this timely, eye-opening investigation [. . .] Professor Hannah Fry seeks to understand why eight percent of the population remain unvaccinated against Covid-19.
In reality, more than twenty percent of adults in the UK are “unvaccinated.” The BBC can’t even write a press release for its forthcoming documentary without publishing deceptive statistics. So it is safe to say the “documentary” itself will be little more than a marketing promotion for the jabs.
Statistics from the UK Health Security Agency (UKHSA) on vaccine coverage in England show that the actual percentage of the “unvaccinated” population is very close to thirty percent, not the eight percent the BBC alleges. The English figures are broadly representative of the UK as a whole and can be extrapolated.
Jab uptake increases with age. Thus, if we exclude children under 18, then more than twenty percent of the UK adult population are unvaccinated.
The subsequent uptake of booster jabs has declined markedly from the one-and-two dose uptake. Millions of Brits decided, for whatever reason, that two shots was their limit. Only fifty-two percent have elected to have the first booster (the third jab).
Speaking in December 2021, then-Health Secretary Sajid Javid said that, in order to be considered fully vaccinated for the proposed “covid pass,” one would need to have three jabs. If three becomes the definition of “fully vaccinated,” which seems unlikely given the lack of interest, then currently forty-eight percent of the total UK population, and more than thirty-five percent of the adult population, are not “fully vaccinated.”
The BBC launched its “documentary” by trying to deceive its audience into believing that there is only a tiny fringe minority of indecisive folk who don’t want the COVID jabs. In point of fact, it is nearly half of the UK population.
Not only has the BBC lied about the statistics in its press release, it has even misrepresented the debate it proposed to examine by calling the millions of people who made an informed decision not to have the jabs “hesitant.” But that’s because the BBC is all about propaganda, not journalism.
When some diligent independent researchers did what real journalists are supposed to do and picked up on the BBC’s deception, the BBC simply changed its press release. Since citing real statistics was a bit too tricky for the BBC—after all, it only has an annual budget of around £5 billion—the revised web page now reads:
In this timely, eye-opening investigation [. . .] Professor Hannah Fry seeks to understand why a portion of the population remain unvaccinated against Covid-19.
Despite there being no reason to trust anything the BBC ever says, the broadcaster implores its viewers to “trust” it simply by pronouncing its own trustworthiness. For the BBC, your “trust” demonstrates your “faith,” allowing it to tell you stories without the need for investigative journalism or even supporting evidence. By contrast, the evidence invariably reveals that the BBC is completely untrustworthy.
According to BBC, its so-called “documentary” is going to be based on bombarding seven hapless unvaccinated lay people with a barrage of pro-vaccine “experts.” Once browbeaten into submission by these authoritative opinions, the victims will then be subject to the BBC’s logical fallacy tactic of appeal to authority. In other words, these high priests of “the science” will explain how the BBC’s seven victims have been misled by “anti-vaxxer” propaganda.
It is highly likely that even if the seven subjects cogently explain why they have decided not to be injected with experimental concoctions, the BBC will edit out any and all valid points they make—and/or deny whatever evidence they cite. We can make these predictions with relative ease, simply by noting the extraordinary level of deceit already present in the BBC’s press release announcing its “programme.”
We can make still further forecasts about the BBC’s alleged “investigation.” For one thing, it won’t honestly report on the current status of the vaccine trials.
Namely, it will neglect to inform its audience that the NCT04368728 trial of the Pfizer-BioNTech jab isn’t finished. And it will not reveal that neither the NCT04470427 trial of Moderna’s mRNA jab nor Johnson & Johnson’s NCT04614948 Jansen trials have posted any results, because these trials, too, are incomplete. Moreover, the BBC will strenuously avoid pointing out the implication of these facts—probably by not reporting them.
Unless the recipients of these drugs were told that the jabs they were about to receive were experimental, they couldn’t possibly have given their informed consent. Consequently, whenever they weren’t informed, administration of the jab contravened nearly every known medical ethic, including those outlined in the Nuremberg Code. But the BBC won’t mention this, either.
It is also safe to say that the BBC will not tell its audience that AstraZeneca concluded the NCT04516746 trial of its AZD1222 adenovirus jab more than a year before schedule by not bothering to conduct a quality control review, rendering its so-called vaccine trial results practically meaningless.
The BBC will not tell anyone that the British Medical Journal (BMJ) disclosed that both Moderna and Jansen (J&J) confirmed that they had given the jabs to their placebo control groups, ending any prospect of their trials ever meeting the basic standards for randomised controlled studies. When the BMJ asked Pfizer if it had done the same, Pfizer declined comment.
Instead, the BBC will almost certainly claim that the jabs have been through extensive clinical trials. It will just omit the part about them having failed to properly complete any.
The BBC will not acknowledge the freedom of information requests and subsequent court ruling in the US that overturned the Food and Drug Administration’s (FDA) decision to delay release of Pfizer’s primary safety monitoring data for 75 years. The Federal Court forced the FDA to release the damning results of Pfizer’s own early monitoring of adverse reactions following the jab rollout in the US and Europe.
In the space of just a couple of months, there were approximately 42,000 adverse reactions to the Pfizer mRNA jab alone, with just over 25,000 of those confirmed by medical exam and the other 16,000+ unconfirmed. Of these, more than 1,200 injuries resulted in death. More than 11,000 of the injured had not recovered from their serious adverse event at the time of reporting.
The BBC certainly won’t report the Israeli study, the results of which indicate that the Pfizer jab prompts a marked decline in male fertility.
Nor will the BBC mention that Pfizer’s own research shows that, contrary to all of Pfizer’s marketing claims, the corporation knew during the trial phase that the lipid nanoparticles used in its jabs found their way into the liver, adrenal glands and spleen and, in particular, accumulated in female recipients’ ovaries.
The BBC may well have to acknowledge the more-than-38,000 possible vaccine deaths reported to the US VAERS system, the 2,200 deaths reported in the UK and the 46,000 deaths recorded by the European Medicines Agency. Its “experts” will point out that there is no evidence that these deaths are caused by the vaccines and will say that the risk of the disease COVID-19 is far higher than any known risks from the COVID-19 jabs.
The BBC will almost certainly make extraordinary and extremely silly claims about how many lives the jabs have allegedly saved. Again these claims will be based upon nothing but baseless assumptions about what could have happened according to some spurious “predictive model.” Rather like claiming your anti-unicorn spray has stopped a million unicorns from grazing your lawn because you don’t have any unicorns in your garden.
As we have just discussed, the risks of harm from COVID-19 claimed by the government and its propaganda outlets—the BBC foremost—are so implausible they verge on absurd. Yet the BBC will not inform its audience that, to date, not one of the regulators has produced a comprehensive risk-benefit analysis for any of the jabs. So the inevitable BBC claims that the jab benefits outweigh the risks will literally be based upon nothing at all.
Something else that the BBC won’t mention is that none of the respective regulatory agencies have done anything to investigate any reported vaccine deaths.
The BBC will not go anywhere near reporting the findings of a team of eminent German pathologists who performed autopsies on 40 corpses of people who died within two weeks of vaccination—and who identified the vaccine as the likely cause of death in one-third of the cases.
Nor will the BBC report statements like those from the UK regulator, the MHRA, that adverse reactions, including deaths, are significantly undereported, with just ten percent of serious reactions and between two percent and four percent of non-serious reactions recorded.
What the BBC will do instead is rely upon carefully cherry-picked scientific papers, a narrow band of selected “expert opinion,” speculative statistics and emotionally charged anecdotes to convince its audience that the seven victims of its hit piece, though well meaning, are all hopelessly deluded due to the scourge of online disinformation. It may well try to squeeze in reference to the proposed Online Safety Act and suggest that this government policy is essential to tackle the disinformation problem fabricated in its documentary.
Of course, if the BBC were serious about its professed wish to “fully explore this complex and deeply divisive debate,” it wouldn’t simply subject a group of ordinary men and women to a tirade of unchallenged claims from its hand-picked group of “experts.” If it really wanted to tackle the debate with any objectivity or journalistic integrity, it would also report the views of some of the many eminently qualified scientists and physicians who do question the COVID-19 narrative and the alleged safety and efficacy of the vaccines.
It would be genuinely interesting to see people like Professor Sucharit Bhakdi, Dr. Mike Yeadon, Professor Carl Heneghan and Professor Arne Burkhardt explain some of their reservations. Perhaps other scientists, physicians and experts who have questioned the vaccines and the COVID-19 pandemic could be heard.
Maybe the statistician and Nobel Laureate Professor Michael Levitt; epidemiologists like Professor John Ioannidis or Professor Knut Wittkowski; experts in clinical drug development such as Alexandra (Sasha) Latypova; or physicians such as Dr. Peter McCullough or Dr. Roger Hodkinson could be invited to challenge the BBC’s preferred experts.
The audience and the seven subjects of the BBC’s attack could then hear both sides of the argument. But that won’t happen.
Alas, many won’t get to see the BBC’s vaccine marketing programme because they have already decided that they will no longer pay for its propaganda to be beamed into their heads. These numbers are swelling all the time, hence the deceptive plan to allegedly end the BBC license fee while a desperate workaround is conjured up to make sure the BBC’s coffers remain stuffed with gargantuan amounts of public money.
Still, we might get to watch “Unvaccinated, with Professor Hannah Fry” when it finds its way on to Odysee, BitChute, Rumble or some other worthy video-sharing platform. If so, it will perhaps be interesting for some to see how accurate or inaccurate this article is.
In the meantime, let’s give the Beeb the benefit of the doubt and hope this post is way off the mark. Instead of the awful propagandist drivel we might expect, let’s hope the BBC proves that these suspicions are born of nothing but unfounded, anti-BBC bias.
Bet they aren’t.
July 18, 2022
Posted by aletho |
Deception, Fake News, Full Spectrum Dominance, Mainstream Media, Warmongering | BBC, Covid-19, COVID-19 Vaccine |
Leave a comment
Accidental Pregnancies are an Independent Indicator of Fertility
Three weeks ago, I wrote an article about Germany, highlighting a very large and consistent drop in births starting January this year, 9 months after vaccination of young people began, until March.
Dramatic Decline in Births in Germany
Since then, I found more data regarding Germany:
- Arkmedic pointed out that April births are available (read his article!)
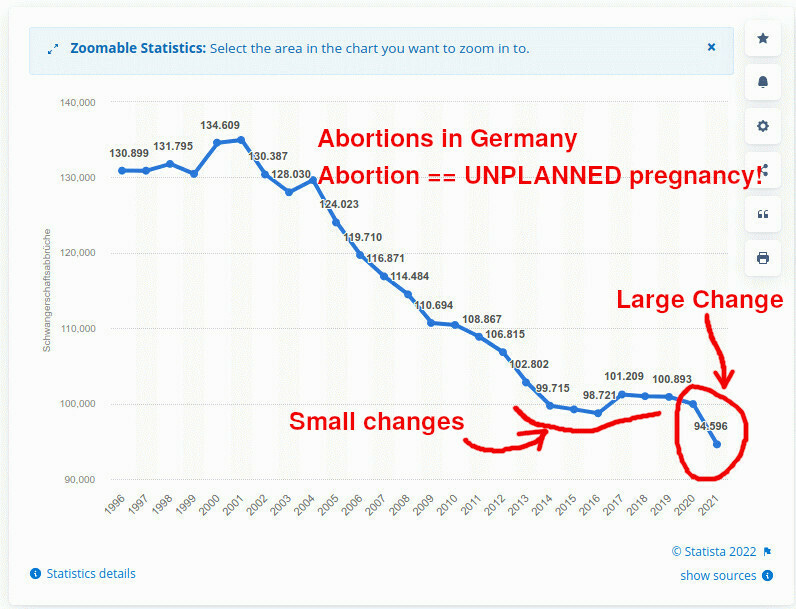
- I found data on 2021 ABORTIONS in Germany, also showing an uncharacteristically large decline in abortions (accidental pregnancies). The abortion data is a completely independent confirmation of the declining fertility of Germans.
Births
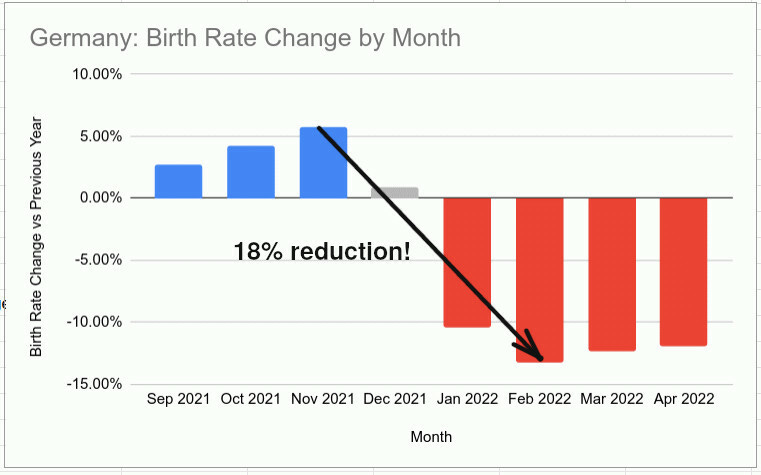
We have new data for April — births dropped by 12% in 2022, compared to April of 2021.
Before I go further, I have to remind my readers: birth rates are always seasonal! Most parents prefer to make a “spring baby”, which often ends up with them making a “summer baby” because conception takes more time than expected. So, never compare adjacent months as they are guaranteed to have dramatic changes that are simply seasonality-driven, with differences very repeatable over the years. Only compare months of one year with the same months of another year, please.
The data comes from the German Bureau of Statistics. (if this link does not bring you to the exact page, select “population” and drill down to “births”). I summarized it for you:

You can see that births suddenly started dropping in Dec 2021, (going from +5% yoy in November to 1% in December, down to -10% in January and -13.28% in February. The suddenness and extent of this drop are unprecedented.
The data for April confirmed that the reduction in birth rate over the first three months is not a fluke and is continuing for the fourth month.
Many people feel strongly about abortions. I understand. I am asking you to suspend your feelings for a moment and look at abortions like a demographer would.
Remember: abortions result from unplanned pregnancies! Aside from a relatively small amount of abortions happening due to fetal abnormalities, most abortions happen because the pregnancy was unexpected, unwanted, and accidental.
What this means is, absent large changes in the laws of the land, sudden increases or decreases in abortions happen only because of changes in fertility.
Live births may see increases or decreases because of changed desire to have children due to social factors. In the case of abortions, however, the pregnancy is ALMOST ALWAYS unplanned to begin with, so social factors like economic expectations have little to do with most abortions. Those abortions are only indications of fertility and desire to have unprotected sex.
So… abortions in 2021 fell by 5.3%!

How large is this effect? Between 1996 and 2021, abortions fell by an average of 1,452 abortions per year. In the year 2021, abortions fell by 5,352! The recent years prior to 2021 saw little change in abortions. Thus, the decline of 5,352 abortions in the year 2021 likely is due to the changed fertility of young people in Germany and shows a great decline in unplanned, accidental pregnancies. Abortions are never planned, remember!
Please recall that younger Germans in 2021 did not start vaccinations until about May or so. Thus, if vaccinations are the cause of lower fertility, their effect on pregnancies would not be seen until the second half of 2021.
Furthermore, since abortion is done after about a month into the pregnancy, you can add about a month and deal with about 5 months out of 12 in 2021, most affected by vaccinations. Thus, a 5% drop in abortions could roughly mean a 12% decline in fertility starting about July.
This is a rough, back-of-the-envelope calculation that indicates that abortion data largely agrees with the hypothesis that declines in birth rates are caused by vaccination, and not by social conditions.
The abortion story is not, as such, a proof of causation: it is a piece of evidence that agrees with my vaccination hypothesis, and strongly disagrees with the possibility that change in fertility is caused by social factors.
So we see that both abortions, as well as April birth data in Germany, coincide and suggest that vaccinations caused a large drop in fertility among the people of Germany.
See Also
July 17, 2022
Posted by aletho |
Timeless or most popular, War Crimes | COVID-19 Vaccine, Germany |
Leave a comment
Transcription:
Dear colleagues at the WHO, I think the time has come to admit that the mass vaccination program that you have been proposing in an attempt to put an end to the COVID-19 pandemic has been a complete failure. At the beginning of this year, I’ve been urging you to open a scientific debate on the potential risks of mass vaccination with these vaccines – in the midst of a pandemic. I’ve never received a response to that request. But shortly thereafter one of the most renowned vaccinologists on this planet wrote me an email saying; ‘vaccinating with these vaccines would only breed new variants. But that it wouldn’t make sense for me to go against the mainstream because nobody would listen to me anyway, and hopefully that second-generation vaccines would solve the problem.’
So, I wanted to let you know that it is not because you are the WHO, that you can afford to ignore the opinion of people who have long-standing expertise – in all of the different disciplines involved in this pandemic: virology, immunology, vaccinology, evolutionary biology, epidemiology, zoonoses, etc. Whereas, some of us have been predicting that mass vaccination with these vaccines in the midst of a pandemic would inevitably lead to the expansion of more infectious variants, your leading scientists have been preaching the simplistic mantra that the more we vaccinate the less the virus will replicate, and the lower the likelihood that new variants will emerge. Now, the consequences of these simplistic and erroneous viewpoints is that today we are dealing with dominant circulation of Omicron, the most infectious SARS-CoV-2 variant that we have seen so far, and probably the most infectious virus that we have seen so far.
So, given the fact that we are now dealing with a number of variants that are circulating and a multitude, of course, of sub-variants, and that infection rates are going through the roof, and that also we are already most likely having a number of animal populations that are serving as a reservoir for the virus, the likelihood that viral variants are now recombining and building reassortments within one and the same host is becoming increasingly likely. So, what that means is that it will become increasingly difficult to trace the origin of new variants, and that it will be even more challenging to predict the characteristics of those new variants in terms of infectiousness, in terms of virulence, pathogenicity, and also in terms of resistance to vaccinal antibodies or to vaccines in general.
But what is very clear is that if those new variants are to survive on a background of high population-level immune pressure, then those variants will need to be more infectious – like, for example, the Omicron variant. The Omicron variant, however, is offering a very nice opportunity, because Omicron has acquired a substantial level of resistance to the vaccinal antibodies, and that means that the vaccinal antibodies are less likely to outcompete the innate antibodies, which is very good news, because we know that innate antibodies can protect against SARS-CoV-2. This has been repeatedly reported in the literature. We also know that innate antibodies can be trained, and therefore they can even improve their recognition and protection against the virus. Innate antibodies can be trained just like other innate immune effectors can be trained, by repeated exposure to what we call pathogen-associated molecular patterns. This is, in fact, nicely shown by the data published by the UK Health Security Agency, previously Public Health England – where they have shown that basically with aging and also with more exposure to the pathogen, the number of cases in the unvaccinated people was dramatically reduced, and even to an extent such that vaccine efficacy, or we should say, in the population, vaccine effectiveness, would become negative. There is also increased evidence, or increasing evidence, that training of innate antibodies as a result of natural infection can enhance the abrogation of the infection, and that training of adaptive immunity – particularly the induction of T-cell memory, also as a result of natural infection – can enhance the abrogation of disease.
Thanks to the increased resistance of Omicron to vaccinal antibodies, the innate antibodies are set free and can now enable the vaccinees to eliminate the virus, to control viral transmission, and to lead to a dramatic decrease in the viral infection rate, just like healthy unvaccinated people are doing. So, in other words, the resistance to Omicron means, in fact, that we are freeing up a huge capacity of sterilizing immunity in vaccinees because the vaccinees are, in fact, regaining full functionality of their innate immune antibodies. That, of course, will lead to herd immunity because herd immunity requires that you induce a type of immunity that can sterilize the virus, that can dramatically diminish transmission. This would also mean: by freeing up this huge capacity of sterilizing immunity in the vaccinees – after certainly a very important incline of infectious cases – we would have a rapid decline of this wave. And we would also have a rapid decline of disease cases, and even more importantly and more dramatically, of severe disease. Now we know with (moderate) disease, when you recover from disease, you develop acquired immunity, which is long-lived and will protect you. And the few cases of severe disease, we have, of course, to treat – that is what we’ve always said.
It is important to realize that, in fact, Omicron is more or less serving, indeed, as a live attenuated vaccine, and that this is a unique opportunity. The fact that we free up the sterilizing capacity in the vaccinees, thanks to the increased level of resistance of Omicron to the vaccinal antibodies – those are no longer capable of outcompeting the innate antibodies – we may have a unique opportunity to achieve herd immunity, or to start building herd immunity. And so, it is very, very important that we leave people alone, and that we leave the children alone, and that we let the virus spread. And so, we shouldn’t have any vaccination against this Omicron variant, and we shouldn’t have lockdowns.
If we are now going to vaccinate against Omicron, we are going to take away this window of opportunity for the population to generate herd immunity, thanks to freeing up our innate antibodies. And what we are going to do is in fact we would build against antibodies, against the spike protein of Omicron, and particularly against the receptor-binding domain of this Omicron spike protein.
We know that this receptor-binding domain has already undergone a number, or several, important mutations. So, if we put again full pressure on this domain, there is a high likelihood that we are now going to promote variants that will be able to use a receptor that is different from ACE-2 to enter into the cell. And we know that SARS-CoV-2 can do that because it has already been described that SARS-CoV-2 can use receptors other than ACE-2 to enter into the cell. But so far this way of entering – this alternative way of entry into the cell – has not been the preferred way for the virus for entering the cells. But it would only take probably one or two mutations for the virus to make these alternative receptors the preferred receptors for viral entry.
By doing mass vaccination against Omicron, we may be putting enough immune pressure on viral infectiousness to give variants that are capable of entering into the cell through an alternative receptor – to give them a competitive advantage, and so, to provide them with a fitness advantage so that they can now become dominant in the population. What this means is pretty catastrophic, because this would mean that basically we end up with a situation where we have antibodies that still strongly bind to the virus, to the receptor binding domain, but that can no longer neutralize the virus because the virus is now using another domain to enter into the cell, a domain which is different from the domain that is blocked by the antibodies.
Such a situation is in fact, a textbook example, for how you provoke antibody-dependent enhancement of the disease. So, this would mean that such a situation, the virus covered with strongly binding antibodies but not being able to neutralize the virus, would basically lead, or would be similar, to a situation where the virus has acquired a higher level of virulence. This would be – this situation would really, really, really be at risk of provoking the kind of disastrous consequences that I have been warning against at the beginning of this year. And we know that industry is already gearing up for mass vaccination against Omicron. And, as this, according to my humble opinion, could potentially be – with a high likelihood – a real disaster. We must prevent such a thing from happening.
So in order to – or I would say unless – unless immediate action is taken to prevent this, it is clear that decision-makers in your organization, the WHO, will be held responsible, accountable, and liable for the dramatic consequences that this biological experiment on human beings could possibly entail. So I hope that this time you will take my warning very seriously into consideration.
Thank you.
July 16, 2022
Posted by aletho |
Science and Pseudo-Science, Timeless or most popular, Video, War Crimes | COVID-19 Vaccine, WHO |
Leave a comment
I have reported time and again about the insanity behind the vaccine’s approval for children, now from 6 month’s to 5 years. Every time the evildoers need to slash off another slab of meat from the body of humanity they raise the overall pain and suffering a few notches.
This is their final slash—you can’t get much younger than 6 months (unless they will want to vaccinate foetuses, but soon there won’t be any of those around to vaccinate.)
Rather than focus on the heinous act of approving an experimental injection to children who have no say in the matter, and if they did, wouldn’t even begin to comprehend the implications, I am going to focus instead on the efforts of “the agenda” to convince children and their parents it is a good idea to let the hairy monster into their beds so they can be raped by the tentacles of corporate greed and the unconscionable ugliness of human evil.
Sorry for the harshness of such a description. In my opinion it isn’t harsh enough.
I don’t think there is anything more abhorrent in the human playbook of evil than the effort to convince a child to hurt itself in order for the perpetrator of such a crime to benefit. What could be worse? Using the innocence of a child to cause harm for anyone’s benefit is at the top of Satan’s list (or whatever other name you want to give a human’s propensity to sink deeply into the shadowy muck of the dark side).
Come on people, pay attention!
(This demand is not for my readers as I am sure you all are in agreement with this presentation—unless you accidentally stumbled on this article, if so, pay attention.)
There is nothing any of you can say that will justify this tactic of coercing children to “be a superhero” or “be like Elmo” and take this jab “for humanity’s sake.” Nothing. No matter how you twist it all up to support your argument, you simply are wrong. This is evil; this is hateful, hurtful, repugnant, disgusting, and unconscionable. Try me with your argument; give me your best shot.
You can’t do it. There is nothing you can say that will get you out of this.
Again, dear shrew, it is not you this is aimed at. We are warriors for the cause; I am speaking with you here, not to you. If you have any friends or family who might benefit from this lecture, please share. I doubt if it will do much good, but we must keep trying.
Here is what I am talking about.
I will certainly not cover the dozens of examples of using a child’s innocence as a weapon to coerce them to put pressure on their parents and caregivers to be vaccinated. I will only site a few situations I have come across to make my point. If you want further details, or wish to see these examples in the broader context of their situations, of course Google search them or otherwise find the information. The details don’t really change anything, nor does the specific context. These tactics are evil at their core, regardless.
Let me start with the effort to push kids into vaccination through superhero coercion, “be a superhero” is the basic theme of this style of coercion. Bus banner ads, ads in schools, on social media, everywhere you might find a kid. “You aren’t good enough as you are, here is your chance to be better, be a superhero!” So kids, who have it hard enough in today’s cultural climate desperately trying to establish their own personal identity, have to be bludgeoned (by the authority figure “bully”) to go “this path—our path” to be “ok.” Granted, I have not seen any slogans that blatantly say “you aren’t good enough as you are” but clearly any effort in showing kids they can be “better” by identifying with a bigger than life fantasy “superhero” doesn’t need to spell it out.
Let’s just jump over the legal ramifications of all of this. Believe it or not there are laws forbidding such blatantly unethical coercion targeting young people incapable of even understanding a lick of informed consent. No one seems to think any of that ethical and legal stuff to be relevant. That’s right. Laws and ethics don’t matter much when you are about to be gobbled up by some unseen virus monster. “Quick! Get some kids on the altar so we can slash their hearts out as a sacrifice to the Boogeyman Dark Virus Monster, he is going to kill us all!!” If you want to read a bit more about this check it out here.
And how about Elmo? Elmo is the Sesame Street children’s icon, which is supposed to be an eternal 3 1/2 year old. He recently succumbed, supposedly voluntarily, to the jab. If Elmo can do it, we all can do it, yea Elmo! —The most selfless red puppet in the world… oops, I mean Muppet™. Get it?
A quote from the paediatrician that Elmo visits in the PSA:
“I learned that Elmo getting vaccinated is the best way to keep himself, our friends, neighbours and everyone else healthy and enjoying the things they love.”
Oh, please. Sorry, as we all know, that is unadulterated BS, not to mention unscientific, and also untrue. What else? Propaganda? Sure, throw that in for good measure.
Probably the most egregious example of this child coercion was the “Make a Wish” foundation’s effort to force kids into compliance by announcing their effort to ease the pain of terminally ill children was only available to those who are vaccinated.
Granted, due to pressure, they have rescinded this “rule” but come on, really? Terminally ill children need to vaccinate? Sure they do, “to save others” not so unfortunate as to be facing death… well, maybe not.
“Make-A-Wish Foundation is requiring Wish kids, their siblings (and other family members), and “any minors participating in the Wish” to be fully vaccinated before having their wishes granted.”
Nice.
You folks that don’t agree with what I am saying here have your argument put together yet? Like, vaccination is good for the little ones because it prevents Covid, which is raging? Where did you get that one? Your own eyes? Your own experience? I don’t think so.
There is nothing like that going on out there (maybe later when vaccinated people, due to destroyed immune systems, are dropping like flies and unvaccinated people are burying their vaccinated loved ones or visiting them in hospitals).
You heard it because the same people telling you all this other garbage wants you to hear it. And believe it.
Are you going to say we need herd immunity? Or that vaccinating babies is “just the right thing to do to help the community,” really? Since when has sacrificing children been the right thing to do for the community? Oh right, they used to do that to keep the bogeyman away back in cave-man days.
Well, I guess that makes sense then. The mainstream media certainly has told us about a whole bunch of invisible boogeymen. Sure, just like in the old days, we can correlate certain bad things with Covid… people HAVE died and gotten sick… but has that really been because of this new Covid Boogeyman? Could be, but really as bad as they have said? Think.
Going back to the point of this article, to condone these techniques to get kids to take this thing is unconscionable. I don’t care if people are dying on the street from this virus (they aren’t) a civil, and moral, human being does not use shame, fear, and “wanting to belong” as a tactic to get children to comply—to anything medical without clear informed consent. Ever.
Although in my opinion it is immoral and unethical to lie, manipulate and coerce parents to vaccinate their children, it is a special kind of evil to target little children as the focus of your efforts for compliance using their innocence as a tool. This is what pedophiles do, and it is wrong in every way imaginable.
I will conclude with this ubiquitous statement: There is no reason to give this vaccine to anyone, and certainly no reason to give it to children.
I could go on with all the scientific reasons, but everyone has their own brand of science so what I say will not matter. And to be honest, the REAL reasons not to vaccinate your children are not based on science, they are based on those other things that seem to be in shorter and shorter supply these days—compassion, soul, love, and simply being human.
It is just wrong to sacrifice children for any reason. Even if the world was indeed going down in flames due to some out of control virus (it isn’t) parents shouldn’t risk their children and offer them to the boogeyman as some sort of compensation.
Maybe people don’t believe they are “sacrificing” them, but they are certainly putting them at risk. It is clear the vaccines do not work as they say they do, and it is clear they are not 100% safe (if parents don’t know this they have been living under a rock and shouldn’t even have children in the first place).
Children do not need this and they do not need to take the risk. Regardless of what Elmo says.
Todd Hayen is a registered psychotherapist practicing in Toronto, Ontario, Canada. He holds a PhD in depth psychotherapy and an MA in Consciousness Studies. He specializes in Jungian, archetypal, psychology. Todd also writes for his own substack, which you can read here
July 16, 2022
Posted by aletho |
Deception, Timeless or most popular, War Crimes | COVID-19 Vaccine |
Leave a comment
This month’s release of Pfizer-BioNTech COVID-19 vaccine documents by the U.S. Food and Drug Administration (FDA) reveals three more reports of deaths among vaccine trial participants and further instances of Pfizer downplaying serious adverse events sustained by participants and listing the injuries as “not related” to the vaccine.
Of the approximately 80,000 pages released this month, the most revelatory is a 3,611-page “confidential” document with no title — only the file name “fa_interim_narrative_sensitive.”
The document contains information about vaccine trial participants who died, who sustained adverse events during the trial or who contracted COVID-19 during the trial.
All participants listed in the document received the 30 μg dose of the BNT162b2 candidate vaccine, which the FDA in August 2021 granted Emergency Use Authorization.
The FDA on July 1 released the documents as part of a court-ordered disclosure schedule stemming from an expedited Freedom of Information Act (FOIA) request filed in August 2021.
Public Health and Medical Professionals for Transparency, a group of doctors and public health professionals, initially submitted the FOIA request.
Document details deaths of three trial participants
The “interim narrative” document contains reports of three clinical trial participants who died — and in all cases, the investigator ruled out the possibility the deaths were related to Pfizer’s vaccines.
One instance pertains to a 56-year-old white female in the U.S. (unique Subject ID C4591001 1007 10071101), who suffered cardiac arrest on Oct. 18, 2021, and died three days later. She was vaccinated on July 30, 2020, and Aug. 20, 2020.
The “narrative comments” accompanying the report on the woman’s death stated her death could not have been related to the vaccine, due to the amount of time that had elapsed following her second dose:
“In the opinion of the investigator, there was no reasonable possibility that the cardiac arrest was related to the study intervention or clinical trial procedures, as the death occurred 2 months after receiving Dose 2.”
The woman’s medical history did not indicate any cardiovascular problems, although ongoing obesity, gastroesophageal reflux disease and sleep apnea syndrome were listed.
The second report of a death was that of a 60-year-old white male in the U.S. (unique Subject ID C4591001 1162 11621327), who received one dose of the vaccine (on Sept. 10, 2020) and died sometime in the following three days of atherosclerotic disease.
According to the document:
“The study site received a police report indicating that the police visited the subject’s home to perform a welfare check on 13 Sep 2020 (Day 4) and found him dead.”
The participant’s medical history indicated ongoing autoimmune thyroiditis, obesity and depression, and a prior craniocerebral injury and prior hip arthroplasty.
According to the report:
“It was reported that the subject’s body was cold and had visible lividity. According to the medical examiner, the probable cause of death was progression of atherosclerotic disease. Relevant tests were unknown. Autopsy results were not available at the time of this report.
“In the opinion of the investigator, there was no reasonable possibility that the arteriosclerosis was related to the study intervention, concomitant medications, or clinical trial procedures, but rather it was related to suspected [emphasis added] underlying disease. Pfizer concurred with the investigator’s causality assessment.”
In other words, the participant’s death was attributed to a “suspected” cause, while the possibility that it was vaccine-related in any way, was dismissed.
The third death listed in the “fa_interim_narrative_sensitive” documents was listed under the section in the document listing reports from trial participants who withdrew, not those who died.
The report pertained to a 72-year-old Hispanic/Latino male in the U.S. (unique Subject ID: C4591001 1152 11521497) who received one dose of the vaccine, on Oct. 7, 2020.
The subject sustained vasovagal syncope (a fainting incident) on Oct. 26, 2020, and was admitted to the hospital, causing him to miss his scheduled follow-up vaccination appointment on Oct. 28, 2020.
According to the document:
“The subject was transferred to the intensive care unit. Family medical history relevant to the syncope was unknown.
“On an unspecified date, the syncope resolved and the subject was discharged from the hospital.”
He was withdrawn from the study on Nov. 6, 2020. However, according to the subject’s sister, he died of “unknown” causes on Nov. 11, 2020.
As stated by the document (dated Nov. 22, 2020):
“The cause of death was reported as unknown. It was not reported if an autopsy was performed. A death certificate might be available at a later date.”
Nevertheless, this lack of information did not prevent the study investigator or Pfizer from dismissing the possibility that the participant’s death was vaccine-related. The document states:
“In the opinion of the investigator, there was no reasonable possibility that the syncope was related to the study intervention, concomitant medications, or clinical trial procedures.
“Pfizer concurred with the investigator’s causality assessment. Per Pfizer, the syncope was most likely coincidental and associated with underlying clinical conditions.”
The document contained no reports of deaths among trial participants who received the placebo.
Investigators attribute 4 serious adverse events to vaccine, Pfizer disagrees
According to the latest document release, investigators attributed the vaccine to serious adverse events in four cases, however, Pfizer disagreed with the investigators’ conclusions in three out of the four cases.
The incidents are:
• A 53-year-old white female in the U.S. (unique Subject ID: C4591001 1018 10181159), who developed “lower back pain and bilateral lower extremity pain with radicular paresthesia” on Oct. 20, 2020, which was ongoing as of the date of the document (Nov. 22, 2020).
She was vaccinated on Aug. 14 and Sept. 4, 2020.
The woman’s medical history did not indicate lower back or lower extremity pain, just ongoing migraines and a prior history including a right shoulder dislocation, fibrocystic breast disease and Vitamin D deficiency.
The study investigator and Pfizer disagreed on whether the serious adverse event she experienced was related to the vaccination. As stated in the document:
“In the opinion of the investigator, there was a reasonable possibility that the lower back pain and bilateral lower extremity pain with radicular paresthesia were related to the study intervention, but not related to concomitant medications or clinical trial procedures.
“Pfizer did not concur with the investigator’s causality assessment and considered that there is not enough evidence to establish a causal relationship with the study vaccine apart from a chronological association at this time of the report.
“Based on the information currently available, it was more likely that the lower back pain and bilateral lower extremity pain with radicular paresthesia was associated with the subject’s underlying known neurological condition.”
• A 71-year-old white female in the U.S. (unique Subject ID: C4591001 1142 11421247) sustained ventricular arrhythmias on Oct. 14, 2020 — the same day she received the second dose of the vaccine — and which continued until Oct. 21, 2020.
The woman received her first dose on Sept. 21, 2020. Her medical history indicated she was wearing a cardiac pacemaker and was experiencing ongoing atrioventricular block (complete), atrial fibrillation and supraventricular tachycardia.
Again, the study investigator and Pfizer could not agree as to whether this adverse event was related to the vaccination. The document states:
“In the opinion of the investigator, there was a reasonable possibility that the ventricular arrhythmia was related to the study intervention based on the temporal relationship since the arrhythmias began within 24 hours of Dose 2, but not related to concomitant medications or clinical trial procedures.
“Pfizer did not concur with the investigator’s causality assessment. Additionally, Pfizer commented that there was not enough evidence to establish a causal relationship with the study intervention apart from a chronological association at this time of the report.
“In absence of evidence for an inflammatory response to study intervention, it was more likely that the ventricular arrhythmia was associated with the subject’s underlying known cardiac conditions.”
Pfizer dismissed the possibility that the vaccine may have exacerbated the subject’s existing cardiac conditions.
• A 48-year-old white female in the U.S. (unique Subject ID: C4591001 1178 11781107), who received one dose of the vaccine on Sept. 4, 2020, and withdrew from the study on Sept. 25, 2020.
In the interim, the participant sustained right axilla lymphadenopathy, with “at least four enlarged lymph nodes” — a condition that was still ongoing as of the document date of Nov. 22, 2020.
Her medical history indicated ongoing positional vertigo, osteoarthritis, eczema, sinus headaches, seasonal allergies and a Pitocin allergy, as well as prior menorrhagia, uterine fibroids and a past hysterectomy. In addition, her body mass index (BMI) was listed as being 36.9.
Pfizer also in this case did not agree with the study investigator’s assessment:
“In the opinion of the investigator, there was a reasonable possibility that the lymphadenopathy was related to the study intervention. Pfizer did not concur with the investigator’s causality assessment.”
• A 30-year-old Asian female in the U.S. sustained a shoulder injury related to vaccine administration (SIRVA).
The documents did not list any severe adverse events occurring in anyone outside the U.S., even though the documents contain reports from trials in Argentina, Brazil and South Africa.
‘Unrelated’ adverse event reports habitually dismiss possibility injuries were vaccine-related
The documents reveal a large discrepancy between the number of adverse events deemed to be related to the vaccination (four) compared to those reported to be “not related” (113 non-placebo participants).
The reports associated with each incident reveal an ongoing tendency to dismiss any possibility injuries were vaccine-related — even in instances where no alternative cause was identified or where patients had no relevant prior medical history.
In still other instances, the cause of the adverse event was attributed to itself, while in several other cases, pre-existing conditions worsened following vaccination.
A significant number of accidents and falls — and subsequent injuries — also were reported.
Instances where severe adverse events were brushed over as being “not related” to the vaccination, despite no relevant medical history, include:
• A 75-year-old white male in the U.S. (unique Subject ID: C4591001 1013 10131176), who was vaccinated on Aug. 13 and Oct. 7, 2020, sustained 13 adverse events between Aug. 29 and Sept. 16, 2020, many of which were ongoing as of the document date of Nov. 22, 2020.
These adverse events included congestive heart failure, acute hypoxic respiratory failure, acute renal failure, aspiration pneumonia, anemia, hypokalemia, hyponatremia, leukopenia, sepsis, small bowel obstruction and mild concentric left ventricular hypertrophy.
The participant had ongoing gastroesophageal reflux disease, hiatus hernia, hypercholesterolemia, hypertension and constipation, in addition to prior small intestinal and knee surgery.
The report attributed the patient’s adverse events to his prior surgical history. The document stated:
“In the opinion of the investigator, there was no reasonable possibility that the abdominal adhesions, small intestinal obstruction, pneumonia aspiration, and acute respiratory failure were related to the study intervention, concomitant medications, or clinical trial procedures, but were rather likely related to subject’s previous surgery.
“Pfizer concurred with the investigator’s causality assessment.”
• A 73-year-old white female in the U.S. (unique Subject ID: C4591001 1079 10791246) sustained a “cerebrovascular accident” (stroke), as well as expressive aphasia, on Oct. 22, 2020. She was vaccinated on Sept. 4 and Sept. 25, 2020.
Her medical history listed osteoarthritis, seasonal allergies and being postmenopausal. Nevertheless, her stroke and aphasia were deemed to be “not related” to the vaccine, although no cause was listed. Instead, the document stated, “pending medical records” with regard to the cause of her adverse events.
• A 66-year-old white female in the U.S. (unique subject ID: C4591001 1021 10211190) suffered a stroke on Nov. 2, 2020, with ongoing symptoms as of the document date on Nov. 22, 2020. She was vaccinated on Sept. 10 and Oct. 1, 2020.
Her medical history indicated ongoing gastroesophageal reflux disease, seasonal allergies and postmenopause, as well as a BMI of 28.5.
Her stroke was dismissed as being “not related” to the vaccine, although no alternative cause was listed.
• A 68-year-old white male in the U.S. (unique Subject ID: C4591001 1092 10921015) sustained arrhythmia atrial fibrillation and elevated troponin on Aug. 26, 2020. He received his first dose on Aug. 19, 2020, and his second dose on Oct. 6, 2020, as it required “clearance from his cardiologist.”
His medical history did not specifically indicate heart conditions. Instead, it indicated ongoing basal cell carcinoma on his nose, as well as hypersensitivity, seasonal allergies, myopia, dyslipidemia, hypertension, actinic keratosis and gastroesophageal reflux disease.
Although the study investigator wrote, in reference to the cause of his injuries, that “medical records [are] being reviewed not able to answer at this time,” the report dismissed possibility that his adverse events were related to the vaccine.
• A 45-year-old Black male in the U.S. (unique Subject ID: C4591001 1156 11561006) with ongoing Type 1 diabetes sustained deep vein thrombosis and a pulmonary embolism on Aug. 31, 2020. He received one dose of the vaccine, on Aug. 20, 2020, and was discontinued from the study on Sept. 8, 2020, “because he no longer met the eligibility criteria.”
Both adverse events were deemed as being “not related” to his vaccination, and were instead indicated as being “related to medical history of Type 1 diabetes mellitus.”
• A 67-year-old white male in the U.S. (unique Subject ID: C4591001 1178 11781015) sustained several adverse events on Oct. 10-11, 2020, including ascending aorta ectasia, diastolic dysfunction of the left ventricle and transient global amnesia. These conditions were ongoing as of the document date of Dec. 4, 2020. He was vaccinated on Aug. 25 and Sept. 15, 2020.
The patient’s medical record indicated ongoing depression, attention deficit hyperactivity disorder, hypertension, insomnia and neck pain.
While the cause of his adverse events was deemed as being “not related” to the vaccination, the study did state a cause, listing it as “possibly” having been hypertension.
• A 58-year-old Hispanic/Latino female from Argentina (unique Subject ID: C4591001 1231 12313674) sustained adverse events including panlobular emphysema, pneumonitis, and left submaxillary sialadenitis beginning on Sept. 29, 2020. The first two conditions were indicated as continuing as of the document date of Dec. 4, 2020.
She was vaccinated on Aug. 24 and Sept. 13, 2020. Her medical record indicated ongoing Sjogren’s syndrome and insomnia.
The cause of these adverse events was deemed as being “not related” to the vaccines, although for the first two adverse events, the stated cause was listed as “unknown,” while for the third, the cause was listed as Sjogren’s syndrome.
• A 56-year-old Hispanic/Latino female from Argentina (unique Subject ID: C4591001 1231 12314001) was diagnosed with acute coronary syndrome on Nov. 8, 2020, which was still ongoing as of the document date of Dec. 4, 2020. She was vaccinated on Aug. 25 and Sept. 15, 2020.
Her medical history consisted of ongoing hypothyroidism, allergic rhinitis and asthma — but no coronary troubles.
Nevertheless, according to the study investigator, her condition was determined to be “not related” to the vaccination, although the cause was listed as “unknown.”
‘Cause unknown’ but no chance the vaccine was to blame
In other examples, adverse events were assigned no specific cause or only a “probable” cause, but investigators dismissed the possibility the vaccines may have caused the injuries.
For example:
• A 34-year-old Hispanic/Latino male from Brazil (unique subject ID: C4591001 1226 12261745) developed a Leydig cell tumor in his left testicle on Sept. 23, 2020. He received the first dose of the vaccine on Sept. 16, 2020, and second dose on Oct. 7, 2020.
His medical history listed only ongoing allergic rhinitis.
While the study investigator claimed that the adverse event was “not related” to the vaccination, the cause was listed as “unknown.”
• A 19-year-old Hispanic/Latino female from Brazil (unique Subject ID: C4591001 1231 12311281) with no indicated medical history was diagnosed with acute appendicitis and QT interval prolongation — a heart condition — on Sept. 18, 2020. She was vaccinated on Aug. 15 and Sept. 4, 2020.
These conditions were deemed to be “not related” to the vaccination, although the causes were indicated as “unknown.”
• A 41-year-old Hispanic/Latino female from Argentina (unique Subject ID: C4591001 1231 12311315) was diagnosed with anemia and malignant melanoma on Sept. 25, 2020, with symptoms continuing as of the document date of Dec. 4, 2020.
She was vaccinated on Aug. 15 and Sept. 3, 2020.
The adverse events were indicated as being “not related” to the vaccination, but instead due to a “probable relationship with [a] vaginal tumor under study.”
• A 44-year-old Hispanic/Latino male from Argentina (unique Subject ID: C4591001 1231 12312854) was diagnosed with supraventricular arrhythmia on Sept. 17, 2020. He received the two vaccine doses on Aug. 21 and Sept. 11, 2020.
His medical history listed only ongoing sleep apnea syndrome and a BMI of 50.4.
According to the study investigator, the arrhythmia was “not related” to the vaccines, but instead “probably” corresponded “to an accessory intraventricular line.”
• A 56-year-old mixed-race male from Brazil (unique subject ID: C4591001 1241 12411825) was diagnosed with acute pyelonephritis on Nov. 2, 2020, and hypochromic anemia two days later. Both conditions were still listed as ongoing as of the document date of Dec. 4, 2020.
The participant was vaccinated on Sept. 17 and Oct. 8, 2020. His medical history listed ongoing hypertension.
According to the study investigator, these adverse events were “not related” to the vaccination. Instead, his acute pyelonephritis was due to a “possible” bacterial urinary tract infection, while the hypochromic anemia cause was “to be clarified.”
Worsening of pre-existing conditions ‘not related’ to vaccine
In other instances, participants experienced a worsening of pre-existing conditions. However, in all instances, no relation to the COVID-19 vaccine was determined.
For instance:
• A 72-year-old white male in the U.S. (unique Subject ID: C4591001 1092 10921187) sustained congestive heart failure on Oct. 1, 2020. He received his first dose of the vaccine on Sept. 15, 2020, and his second dose on Oct. 6, 2020.
The participant’s medical history included ongoing coronary artery disease, atrial fibrillation, type 2 diabetes, asthma, obesity, dyslipidemia, hypertension, insomnia and seasonal allergies. Moreover, he had previously had a defibrillator installed.
The cause of his adverse event was simply indicated as “progression of cardiovascular disease” unrelated to the vaccine. The possibility that the vaccine may potentially have precipitated the worsening of his heart condition was not considered.
• A 73-year-old white female in the U.S. (unique Subject ID: C4591001 1111 11111095) was reported as having sustained an “undiagnosed mental disorder” on Sept. 25, 2020, which was still ongoing as of the document date of Dec. 4, 2020. She was vaccinated on Aug.11 and Sept. 1, 2020.
The participant’s medical history did not indicate any prior mental disorders or conditions. Nevertheless, the cause of the adverse event was indicated by the study indicator as being “not related” to the vaccination and instead simply due to “mental instability.”
• A 58-year-old white male from the U.S. (unique Subject ID: C4591001 1109 11091387), who sustained worsening osteoarthritis of the right knee on Oct. 14, 2020, and later also experienced deep vein thrombosis on Oct. 20, 2020, which was still ongoing as of the document date of Dec. 4, 2020.
The participant’s medical history indicated ongoing osteoarthritis, ongoing hypercholesterolemia, hypothyroidism, sleep apnea syndrome, rosacea and an enlarged prostate. A prior knee surgery was also listed.
Both adverse events were deemed to be “not related” to the vaccination and instead attributed to the patient’s prior knee surgery and “previous medical history.”
• A 70-year-old white female from the U.S. (unique subject ID: C4591001 1127 11271023) experienced a worsening of her asthma on Oct.1, 2020. She later also developed malignant invasive ductal carcinoma in her left breast, on Nov. 5, 2020. Both cases were still ongoing as of the document date of Dec. 4, 2020.
She received her two doses of the vaccine on July 30 and Aug. 18, 2020. Her medical history, aside from ongoing asthma, also indicated a recurrent urinary tract infection and ongoing bronchitis, seasonal allergies, myopia, migraines, hypothyroidism, hypertension, insomnia, hyperlipidemia, osteoarthritis, bilateral deafness and postmenopause.
According to the document, both adverse events were “not related” to the vaccination, and instead were attributed to an “allergy” and to a “malignancy,” respectively.
Reports of multiple adverse events ignored
Other examples include cases where patients sustained multiple adverse events, many of which were entirely ignored by the study investigators’ assessments.
These include:
• A 61-year-old white male from the U.S. (unique Subject ID: C4591001 1114 1114108), who sustained 10 vaccine injuries beginning on Sept. 12, 2020, after he received the first dose of the vaccine on Aug. 24, 2020, and his second dose on Sept. 30, 2020.
The adverse events he experienced included acute kidney injury, atrial fibrillation, chest pain, left ventricular hypertrophy, mitral valve regurgitation, bilateral hand pain, pulmonary hypertension, skin avulsion on his left finger, a Staphylococcal infection and tricuspid regurgitation. Several of these conditions were still ongoing as of the document date of Dec. 4, 2020.
The patient’s medical history indicated ongoing peripheral neuropathy, type 2 diabetes, anxiety, depression, asthma, Staphylococcal infection, hypertension, hyperlipidemia and a prior leg amputation.
According to the study investigator, “the staphylococcal infection” was “not related” to the vaccine, but instead was connected to the patient’s hypertension, musculoskeletal causes and an “infection.” No mention was made in this assessment as to the probable causes of the other adverse events.
Some adverse events ‘caused’ by … the adverse event
In still other cases, the “cause” of participants’ adverse events was indicated as being the same as the adverse event itself.
Examples include:
• A 68-year-old white male from the U.S. (unique Subject ID: C4591001 1095 10951204), who was diagnosed with bladder cancer on Nov. 2, 2020. He was vaccinated on Sept. 2 and Sept. 21, 2020.
According to the document, the participant’s ongoing medical history included hypertension, benign prostatic hyperplasia, hypercholesterolemia, angina pectoris, coronary arterial stent insertion, coronary artery disease, erectile dysfunction and osteoarthritis.
However, the cause of his bladder cancer was attributed as “cancer” and deemed to be “not related” to the vaccination and “most likely coincidental and associated with the underlying clinical conditions.”
• A 48-year-old white male from the U.S. (unique Subject ID: C4591001 1124 11241106) sustained an acute myocardial infarction on Sept. 27, 2020. He previously received two doses of the vaccine, on Aug. 26 and Sept. 16, 2020.
His medical history indicated ongoing high cholesterol, gastroesophageal reflux disease and back pain.
According to the study investigator, the adverse event sustained by the participant was “not related” to the vaccination, but instead “related to cardiovascular risk,” with no further elaboration provided.
• A 73-year-old white female in the U.S. (unique Subject ID: C4591001 1223 12231159) was found to have a pancreatic mass on Nov. 5, 2020. She was vaccinated on Sept. 10 and Oct. 1, 2020.
Her medical records indicated ongoing osteoarthritis, menopause, gastroesophageal reflux disease, hypertension, dyslipidemia, hypothyroidism, Eustachian tube dysfunction, prophylaxis, irritable bowel syndrome, osteoporosis and benign monoclonal hypergammaglobulinemia.
The cause of her adverse event, which was indicated to be “not related” to the vaccination, was listed as “new development of pancreatic mass” without any elaboration as to the factors that may have caused it to appear.
‘Cause unknown’ but no chance the vaccine was to blame
In other examples, adverse events were assigned no specific cause or only a “probable” cause, even as the possibility that they were related to the vaccination was dismissed.
For example:
• A 34-year-old Hispanic/Latino male from Brazil (unique Subject ID: C4591001 1226 12261745) developed a Leydig cell tumor in his left testicle on Sept. 23, 2020. He received the first dose of the vaccine on Sept. 16, 2020, and second dose on Oct. 7, 2020.
His medical history listed only ongoing allergic rhinitis.
While the study investigator claimed that the adverse event was “not related” to the vaccination, the cause was listed as “unknown.”
• A 19-year-old Hispanic/Latino female from Brazil (unique Subject ID: C4591001 1231 12311281) with no indicated medical history was diagnosed with acute appendicitis and QT interval prolongation — a heart condition — on Sept. 18, 2020. She was vaccinated on Aug. 15 and Sept. 4, 2020.
These conditions were deemed to be “not related” to the vaccination, although the causes were indicated as “unknown.”
• A 41-year-old Hispanic/Latino female from Argentina (unique Subject ID: C4591001 1231 12311315) was diagnosed with anemia and malignant melanoma on Sept. 25, 2020, with symptoms continuing as of the document date of Dec. 4, 2020.
She was vaccinated on Aug. 15 and Sept. 3, 2020.
The adverse events were indicated as being “not related” to the vaccination, but instead due to a “probable relationship with [a] vaginal tumor under study.”
• A 44-year-old Hispanic/Latino male from Argentina (unique Subject ID: C4591001 1231 12312854) was diagnosed with supraventricular arrhythmia on Sept. 17, 2020. He received the two vaccine doses on Aug. 21 and Sept. 11, 2020.
His medical history listed only ongoing sleep apnea syndrome and a BMI of 50.4.
According to the study investigator, the arrhythmia was “not related” to the vaccines, but instead “probably” corresponded “to an accessory intraventricular line.”
• A 56-year-old mixed-race male from Brazil (unique Subject ID: C4591001 1241 12411825) was diagnosed with acute pyelonephritis on Nov. 2, 2020, and hypochromic anemia two days later. Both conditions were still listed as ongoing as of the document date of Dec. 4, 2020.
The participant was vaccinated on Sept. 17 and Oct. 8, 2020. His medical history listed ongoing hypertension.
According to the study investigator, these adverse events were “not related” to the vaccination. Instead, his acute pyelonephritis was due to a “possible” bacterial urinary tract infection, while the hypochromic anemia cause was “to be clarified.”
Other explanations for participants’ vaccine injuries include:
• A 78-year-old white male from the U.S. (unique Subject ID: C4591001 1097 10971011), who suffered from pneumonia between Sept. 20 and Oct. 5, 2020. He had previously received two doses of the vaccine, on Aug. 20 and Sept. 9, 2020.
According to the document, the cause of his pneumonia was “not related” to the vaccines. Instead, the listed cause was “pt [patient] contracted pneumonia from somewhere.”
• An 84-year-old white male from the U.S. (unique Subject ID: C4591001 1097 10971084) contracted pneumonia on Oct. 7, 2020, symptoms of which were still ongoing as of the document date of Dec. 4, 2020. He had previously been vaccinated on Sept. 1 and Sept. 23, 2020.
Similar to the patient above, the cause of the participant’s pneumonia was indicated as being “not related” to the vaccination. The narrative comment instead stated that “Pt [patient] contracted pneumonia from unknown source.”
Very few severe adverse events — and no deaths — were reported in other countries, although Argentina, for instance, was home to the largest of the Pfizer vaccine trials in 2020.
The next 80,000-page cache of FDA documents pertaining to the FDA’s authorization of the vaccine is set to be released on Aug. 1.
Michael Nevradakis, Ph.D., is an independent journalist and researcher based in Athens, Greece.
© 2022 Children’s Health Defense, Inc. This work is reproduced and distributed with the permission of Children’s Health Defense, Inc. Want to learn more from Children’s Health Defense? Sign up for free news and updates from Robert F. Kennedy, Jr. and the Children’s Health Defense. Your donation will help to support us in our efforts.
July 16, 2022
Posted by aletho |
Deception, Science and Pseudo-Science | COVID-19 Vaccine, FDA |
Leave a comment
Two-and-a-half years ago, the Grand Poobahs of global vaccinology admitted — in behind-closed-door confessions caught on camera at the World Health Organization (WHO) — that public and professional confidence in vaccines was “wobbly,” and deservedly so.
As the gathered experts conceded, the glaring inadequacies of vaccine safety science and the dysfunctional safety monitoring systems that permit routine “obfuscation” of serious adverse events were understandable reasons for public distrust.
At the time, it seemed as though such momentous disclosures would presage a death knell for vaccine “business as usual” — but then along came COVID-19, and with it, the instant memory-holing of the WHO’s stunning admissions.
Rather than finally address the self-confessed vaccine disaster, public health officials and global leaders — ranging from presidents to private-sector employers to top military brass to central bankers — used COVID-19 as an opportunity to double down in the opposite direction, forcibly stuffing the “vaccine hesitancy” genie back in the bottle with ethically untenable vaccine mandates.
After 18 months of force-feeding the COVID-19 jabs, however, manufacturers are now discarding tens of millions of doses “amid sagging demand.”
In some respects, this could be construed as evidence of policy failure, but the fact is that the COVID-19 shots accomplished a significant goal for the parties that pushed them, launching a renewed vaccine gold rush that — with growing emphasis on voguish, biotech-reliant biopharmaceuticals — seems likely to extend well beyond the COVID-19 era.
As the head of Bayer’s pharmaceuticals division observed in late 2021, mRNA vaccine technology and other forms of cell and gene therapy — for all of their by now well-documented and even species-threatening dangers — have crossed over both the regulatory and public palatability threshold.
Pfizer, Johnson & Johnson (J&J), AstraZeneca, Sanofi and Eli Lilly — some of major players in the biopharma space — are actively prioritizing “strategic alliances” and “collaborations to expand their [biopharmaceutical] product portfolios.”
Meanwhile, the U.S. Food and Drug Administration (FDA) and Centers for Disease Control and Prevention (CDC) are poised to roll out, at breakneck speed, approvals and recommendations for whatever new childhood and adult vaccines are sent their way.
In short, using technologies both “conventional” and new, a multipronged effort is afoot to jump-start and ensure a frenzied vaccine-palooza.
The mRNA pipeline
Having succeeded in foisting COVID-19 mRNA injections on an initially unsuspecting public, manufacturers and government agencies like the National Institutes of Health (NIH) are now salivating at the prospect of an endless series of mRNA vaccines.
It is no coincidence that the mRNA jabs in the works target some of the very conditions being reported as COVID-19 vaccine adverse events, a neat “create-a-problem, develop-a-drug-to-manage-the problem” trick that accounts for many other drugs already on the market.
In the pipeline are mRNA vaccines for the following:
- Cancer: Researchers are conducting dozens of clinical trials to test “mRNA treatment vaccines in people with various types of cancers.” Dr. Ryan Cole, a pathologist, described the dramatic surge in endometrial and other cancers following the rollout of COVID-19 shots.
- Shingles: Cole and others also noted the uptick of shingles in COVID-19 vaccine recipients. Moderna in March announced its development of an mRNA shingles vaccine, as well as mRNA vaccines for herpes and cancer.
- Other forms of immune suppression: With numerous indications that COVID-19 shots are reprogramming the immune response, officials and manufacturers are dusting off HIV as the supposed bogeyman. Moderna and NIH are partnering in mRNA vaccine clinical trials for HIV. This would represent a particular coup for Dr. Anthony Fauci, who over four decades has found development of an HIV vaccine to be “a daunting scientific challenge.”
- Heart attacks: Cardiac problems are among the few COVID-19-vaccine-related adverse events grudgingly acknowledged by manufacturers and the FDA. In the U.K., researchers are investigating the use of “exactly the same technology as the Pfizer and Moderna vaccines to inject micro RNAs to the heart,” claiming they can get whatever heart cells survive after a heart attack to proliferate.
- COVID and influenza: Manufacturers also are gearing up for a new generation of mRNA-based flu shots and mRNA combination vaccines which, they promise, will “protect against several different infections at the same time, such as influenza, COVID-19 and other respiratory infections.”In the meantime, CDC just recommended that seniors (aged 65 years or older) receive “enhanced” flu shots — either high-dose, adjuvanted or recombinant — in lieu of “standard-dose unadjuvanted, inactivated vaccines.” Adjuvanted influenza vaccines feature a new generation of “smart” vaccine adjuvants designed to ensure even the most mediocre vaccine sends recipients’ immune systems into overdrive.
For babies — something old, something new
In June, the FDA reaffirmed its long-standing allegiance to an agenda of guaranteed harm when it authorized emergency use COVID-19 shots for infants as young as 6 months old.
After the conflict-of-interest-riddled FDA advisors’ 21-0 vote, Rep. Louie Gohmert (R-Texas) commented, “[I]n balancing the risk to rewards here, all the risks are to the innocent children and all of the billion-dollar rewards go to the government-protected pharmaceuticals.”
Seizures and psychosis are already being reported as adverse events in the under-5 age group.
In decrying FDA’s decision to give COVID-19 shots to tots, some dissenters waxed nostalgic about the perceived “rigor” of the pre-COVID-19 vaccine approval process, seemingly amnesiac about the FDA’s lengthy history of regulatory capture and business-friendly shortcuts.
As a reminder, at least two-thirds of the vaccines approved by the FDA from 2006 through late 2020 benefited from “flexibility in the evidence required for approval,” resulting in accelerated approvals.
This “turn-a-blind-eye” pattern also held sway in the FDA’s and CDC’s recent decisions to pile on two more options to the childhood schedule, options that will do nothing to improve the safety of measles-mumps-rubella (MMR) and pneumococcal conjugate vaccines (PCV) that have been injuring children for decades.
First, on June 3, the FDA approved GlaxoSmithKline’s (GSK’s) Priorix, an MMR vaccine initially launched in Europe in the late 1990s.
GSK developed Priorix using the MRC-5 cell line (derived from the lung tissue of a male fetus aborted at 14 weeks).
A 2020 analysis by the Italian association CORVELVA of a version of Priorix that also contains a varicella component found that the amount of DNA in the vaccine was “well above the allowed threshold,” and that continuous use of the cell line over time resulted in “vaccines containing progressively more and more modified human genetic material, that is dangerous for the health of the vaccinees themselves.”
The FDA’s go-ahead for Priorix shatters Merck’s position as the sole U.S. purveyor of MMR vaccines. Previously, FDA showed no sign of being troubled by Merck’s monopoly, despite the pharmaceutical behemoth being dogged by “a slew of controversies” that included whistleblower allegations of MMR-related fraud and undeniable evidence of a link with autism.
Moreover, as Children’s Health Defense Chairman Robert F. Kennedy, Jr. pointed out in late 2019, when the FDA belatedly began to “tee up” Priorix as a replacement for Merck’s scandal-ridden MMR-II, rather than use an inert placebo to test Priorix, the FDA allowed GSK to use MMR-II as the comparator!
Even these sham clinical trials, Kennedy noted, had “horrifying” results. Within 42 days, nearly 50% of recipients of both manufacturers’ formulations experienced adverse events, with over 10% ending up in the emergency room. By six months, almost 4% of recipients had been diagnosed with a “new onset chronic disease.”
To date, the European Medicines Agency (EMA) has received more than 37,000 adverse event reports for Priorix and another 11,000-plus for the varicella-containing version — with 58% and 79% of adverse events, respectively, occurring in the under-two age group that will now receive the jabs in the U.S.
Following the nominal slap on the wrist for Merck’s MMR-II, the FDA and CDC also offered Merck some good news, approving on June 17 and then recommending — for routine use in infants and children 6 weeks to 2 years of age — the company’s 15-valent PCV15 (brand name “Vaxneuvance”) as an interchangeable alternative to Pfizer’s Prevnar 13 (PCV13).
The CDC stopped short of issuing a “preferential recommendation” for PCV15, however. Admitting to “certain uncertainties, including concerns related to potentially higher reactogenicity” — with “reactogenicity” defined as the “state of being able to produce adverse reactions” — the CDC leaves it up to the hapless infants who receive Vaxneuvance to discover the shots’ “higher reactogenicity” for themselves.
Even without the addition of Vaxneuvance to the schedule, pneumococcal conjugate vaccines — with ingredients like aluminum and polysorbate 80 — have shown themselves plenty capable of wreaking havoc on the health of the infants expected to get four doses by the time they are 12 to 15 months old.
Eager to add even more injections to the childhood vaccine schedule, the industry is also eyeing as a potential cash cow a pediatric (and adult) mRNA vaccine against respiratory syncytial virus (RSV).
In 2019, 30 candidate RSV vaccines were in the pipeline, and in 2021, the FDA fast-tracked an mRNA-based RSV vaccine developed by Moderna.
HPV downsizing — getting HPV shots into young people by any means necessary
The competition between Merck and GSK is also fierce where human papillomavirus (HPV) vaccines are concerned.
In the U.S., Merck’s Gardasil (and later, Gardasil 9) handily beat out GSK’s Cervarix, which is no longer available to American youth — but with 100 or more countries having added HPV jabs to their national vaccination schedules, much more than the U.S. market is in play.
Data suggest HPV vaccine coverage in the U.S. starts out relatively high, with an estimated 66% of 13- to 17-year-olds getting a first dose, but the percentage completing the series (an additional one to two doses) drops off to 49%.
Worldwide, acceptance of HPV vaccines is even lower — for girls, global coverage is estimated at about 15% of those in the target age range.
Undoubtedly, one of the reasons for the global public’s lukewarm stance on HPV vaccination is the occurrence of serious adverse autoimmune reactions that have left many recipients, both female and male, disabled for life.
Merck is mired in lawsuits (with attorneys, including Kennedy) alleging it knowingly concealed Gardasil-associated adverse events.
Rather than re-evaluate — as some researchers have strongly urged — the adverse event profile that, until COVID-19 shots, made HPV vaccines some of the most dangerous on the market, agencies like the National Cancer Institute (NCI) are instead beginning to argue in favor of single-dose HPV vaccination (either Cervarix or Gardasil 9).
Punting to a one-dose regimen would, NCI officials disingenuously say, “simplify the logistics of vaccination, which could allow more girls [and boys] worldwide to be vaccinated.”
Monkeypox profiteering
As Rob Verkerk, Ph.D., reported last month, the suspected case definition of monkeypox is broad enough to include anyone with a common cold — or with post-COVID-19-vaccine immune suppression — who has a shingles rash.
Verkerk’s counsel is to worry about “what the WHO and collaborating institutions, governments and corporations are up to,” rather than succumb to fear-mongering about monkeypox itself.
In the U.S., what the government is “up to” is ordering more than 4 million doses of monkeypox vaccine — a whitewashed smallpox vaccine linked to heart inflammation — and formulating a “national monkeypox vaccine strategy,” including a protocol aimed at the vaccine’s use in children.
In other words, with a “COVID-19 corporatocracy playbook” that, in Verkerk’s words, “is now well and truly oiled,” corporate and government leaders of ill intent appear to believe they can continue to play the vaccine game indefinitely, using “fear and manipulated science to engender support for the global control of health.”
It is up to us to prove them wrong.
© 2022 Children’s Health Defense, Inc. This work is reproduced and distributed with the permission of Children’s Health Defense, Inc. Want to learn more from Children’s Health Defense? Sign up for free news and updates from Robert F. Kennedy, Jr. and the Children’s Health Defense. Your donation will help to support us in our efforts.
July 15, 2022
Posted by aletho |
Science and Pseudo-Science, Timeless or most popular | CDC, COVID-19 Vaccine, FDA, United States |
Leave a comment
‘People are getting bad advice and we can’t say anything.’
By Marty Makary M.D., M.P.H. and Tracy Beth Høeg M.D., Ph.D. | Common Sense | July 14, 2022
The calls and text messages are relentless. On the other end are doctors and scientists at the top levels of the NIH, FDA and CDC. They are variously frustrated, exasperated and alarmed about the direction of the agencies to which they have devoted their careers.
“It’s like a horror movie I’m being forced to watch and I can’t close my eyes,” one senior FDA official lamented. “People are getting bad advice and we can’t say anything.”
That particular FDA doctor was referring to two recent developments inside the agency. First, how, with no solid clinical data, the agency authorized Covid vaccines for infants and toddlers, including those who already had Covid. And second, the fact that just months before, the FDA bypassed their external experts to authorize booster shots for young children.
That doctor is hardly alone.
At the NIH, doctors and scientists complain to us about low morale and lower staffing: The NIH’s Vaccine Research Center has had many of its senior scientists leave over the last year, including the director, deputy director and chief medical officer. “They have no leadership right now. Suddenly there’s an enormous number of jobs opening up at the highest level positions,” one NIH scientist told us. (The people who spoke to us would only agree to be quoted anonymously, citing fear of professional repercussions.)
The CDC has experienced a similar exodus. “There’s been a large amount of turnover. Morale is low,” one high level official at the CDC told us. “Things have become so political, so what are we there for?” Another CDC scientist told us: “I used to be proud to tell people I work at the CDC. Now I’m embarrassed.”
Why are they embarrassed? In short, bad science.
The longer answer: that the heads of their agencies are using weak or flawed data to make critically important public health decisions. That such decisions are being driven by what’s politically palatable to people in Washington or to the Biden administration. And that they have a myopic focus on one virus instead of overall health.
Nowhere has this problem been clearer—or the stakes higher—than on official public health policy regarding children and Covid.
First, they demanded that young children be masked in schools. On this score, the agencies were wrong. Compelling studies later found schools that masked children had no different rates of transmission. And for social and linguistic development, children need to see the faces of others.
Next came school closures. The agencies were wrong—and catastrophically so. Poor and minority children suffered learning loss with an 11-point drop in math scores alone and a 20% drop in math pass rates. There are dozens of statistics of this kind.
Then they ignored natural immunity. Wrong again. The vast majority of children have already had Covid, but this has made no difference in the blanket mandates for childhood vaccines. And now, by mandating vaccines and boosters for young healthy people, with no strong supporting data, these agencies are only further eroding public trust. … Full article
July 14, 2022
Posted by aletho |
Video | COVID-19 Vaccine, United States |
Leave a comment
Justice Paul Belzil just decided that it was legally okay for doctors to remove Canadians from organ transplant waitlists if they’re unvaccinated.
As reported by the Westphalian Times’s Marie Oakes, Belzil filed his decision on Tuesday in a case concerning Annette Lewis, who was essentially given the choice of ‘comply or die’ after doctors changed the rules surrounding organ transplant waitlists to require being fully vaccinated.
According to Lewis, a doctor “told me if I did not take the COVID-19 vaccine, I would not get the transplant, and if I did not get the transplant, I would die.”
She added, “I ought to have the choice about what goes into my body, and a life-saving treatment cannot be denied to me because I chose not to take an experimental treatment for a condition — COVID-19 — which I do not have and which I may never have.”
But judge Belzil disagreed, arguing that “her beliefs and desire to protect her bodily integrity [do not] entitle her to impact the rights of other patients or the integrity of the [transplant program] generally.”
He ultimately ruled that the charter doesn’t apply to clinical treatment decisions and that Lewis’s rights, therefore, had not been violated.
Lewis isn’t alone in her struggle either. As previously reported by The Counter Signal, hospitals and health networks across the country have chosen to deny the unvaccinated organ transplants even when prospective patients are healthy and have found a donor.
In October 2021, Toronto’s University Health Network (UHN) (the largest health research organization in Canada and Canada’s largest transplant centre) adopted a policy requiring all organ transplant patients to be fully vaccinated against COVID-19 before doctors operate on them.
The decision immediately affected roughly 4,300 Canadians awaiting life-saving care, some of whom have likely passed away by now.
July 13, 2022
Posted by aletho |
Civil Liberties, Science and Pseudo-Science | Canada, COVID-19 Vaccine, Human rights |
Leave a comment
Samizdat | July 13, 2022
Hong Kong is set to introduce electronic tracking bracelets for citizens who decide to quarantine at home after testing positive for Covid-19, the health chief has announced. Violators of the isolation rules face hefty fines and possibly even jail time.
The territory’s secretary for health, Lo Chung-mau, announced the move during a Monday press briefing, saying the bracelets are meant to stop infected people from spreading the illness further and will operate on the ‘Leave Home Safe’ app rolled out last year.
“We have to make sure that home isolation is more precise while being humane,” Lo said, adding that the trackers will be introduced on Friday.
Breaching Hong Kong’s quarantine order could result in fines up to $3,200 and a maximum of six months behind bars. Individuals who are able to isolate at home must do so for two weeks, though will be allowed to leave if they test negative for two days in a row and have their first pair of vaccine doses.
While the territory previously required overseas arrivals to use bracelets with unique QR codes to check in and account for their movements, the gadgets were later replaced with genuine tracking tech. The system is set to be expanded, though the government has not said what type of bracelet it will use for the latest initiative.
The health secretary also noted that Hong Kong will implement a color-coded system similar to the one in place in mainland China, which labels different levels of infection risk as yellow or red. Those with the red designation will face heavy restrictions on their movement, including outright bans on entering public venues, while yellow entails lesser limits.
However, the city’s recently inaugurated chief executive, John Lee, has since stressed that the traffic light system would only apply to “a specific and small number of people,” but nonetheless argued that Hong Kong needs “some identification method” to distinguish citizens with active infections from those quarantining as a precaution.
Local officials continue to warn that Hong Kong’s Covid-19 outbreak remains “very serious,” urging residents to minimize travel and observe social distancing rules, which were just extended for another two weeks on Tuesday.
The Department of Health said it recorded 2,558 new local coronavirus cases on Tuesday, as well as another 211 infections among travelers from abroad. It did not offer a daily update for fatalities, but noted the territory had tallied 9,420 deaths in total throughout the pandemic, most of them occurring this year.
July 13, 2022
Posted by aletho |
Civil Liberties, Science and Pseudo-Science | China, Covid-19, COVID-19 Vaccine, Human rights |
Leave a comment