A 59-year-old man unfortunately died in Mexico in late April. Having been bed-bound for weeks and suffering from type-2 diabetes and chronic renal failure, he was at high risk from respiratory virus infection.
It became newsworthy, and the World Health Organization thousands of miles distant even released a media statement, because recent advances in genetic sequencing allowed the presence of Type A (H5N2) influenza virus – a type of bird flu – to be reported in a single clinical sample a month later. Refuting the WHO’s distant bureaucrats attributing mortality to the virus, Mexico’s health secretary is reported as noting that it was chronic illness that caused the death.
Irrespective of cause, deaths are a tragedy for family and friends. This one made global news purely because of advances in diagnostic technology. The WHO, the media, and a growing pandemic industry had been waiting for this inevitable event, testing and screening, as it is critical to perhaps the largest business scheme in human history. There are hundreds of billions on the table, and the will and means to take it. We all need to understand why, and what is supposed to happen next.
Covid and the Resetting of Public Health
Covid-19 has proven the business case for gain-of-function research. It looks increasingly likely that some genetic fiddling really did succeed in moving a bat coronavirus into humans, where it is more amenable to monetization (there is no profit in sick bats, or fear of them). Importantly, despite the broad economic and health catastrophe that followed, those behind the program are continuing much the same work, and not being held to account. There is vast profit with little or no real risk.
However, what the Covid episode really demonstrated is the financial and political gains that can be achieved irrespective of outbreak severity. As Klaus Schwab and Thierry Malleret pointed out in mid-2020 in their book Covid-19: The Great Reset, Covid-19 can be used to subvert post-World War II concepts of democracy and human rights and return society to a corporate authoritarian model (“Stakeholder Capitalism”), even though the illness is usually mild.
What is needed is a shared narrative among those who stand to benefit; media, governments, and the corporate world. While the term “Great Reset” seems to have been discarded as unpopular, the World Economic Forum’s (WEF’s) stated intent to penetrate governments and change society to the benefit of their members is clearly undiminished.
Devastating mortality is not needed to drive societal change; just the fear of it. You need a test, visuals such as masks and circles on the pavement, a dependent media, and a research and health establishment whose career opportunities are dependent on compliance. The ramping up of surveillance for the vast sea of viral variants that is nature has just been officially confirmed through the adoption of amendments to the 2005 International Health Regulations at the World Health Assembly (WHA) in Geneva. Irrespective of the reality of risk or the massively disproportionate public funding required, the world is going to find a lot more potential threats, and is building a whole industry that will ensure they translate into corporate profit.
The Opportunity of Influenza
Avian influenza, or bird flu, has been around perhaps as long as birds (so was likely a dinosaur malady in Cretaceous times). Humans must have lived alongside it for over 200,000 years, and our primate ancestors far longer. Bird flu viruses are part of a range of variants of the influenza virus family that undergo regular mutation and recombination (even mixing genome from viruses that normally infect different species) that makes them appear relatively new to our immune system. This makes them more harmful and results in a new influenza outbreak almost every year, as our immunity from the last one (or from a prior influenza vaccine) only partially addresses the next.
Sometimes, recombination allows an influenza virus that is mostly confined to other animals, such as birds, to undergo a wider shift that allows it to infect other species, such as humans. This is similar to what scientists sometimes try to simulate in the lab through ‘gain-of-function’ research, such as modifying bat coronaviruses to become pathogenic to humans.
Humans have always lived in very close proximity with, and eaten, animals that harbor influenza viruses. The last major ‘spillover’ of influenza from birds to humans was the Spanish flu pandemic in 1918-19. It killed perhaps 20 to 40 million people, most probably due to secondary bacterial pneumonia as there were no modern antibiotics. In the century since, an event of this nature has not recurred, and with modern antibiotics and medical care, the mortality of the Spanish flu should now be far lower.
So, why are we seeing the current hysteria regarding bird flu, and why is the media promoting narratives such as potential mortality massively greater than the Spanish flu or any influenza outbreak in human history? The answer, presumably, lies earlier in this article. A very wealthy corporate and financial sector that is influential over governments and media that knows, and has demonstrated, that wealth can be concentrated to the tune of hundreds of billions of dollars through fear of a virus.
There is now a rapidly expanding army of virologists, ‘virus hunters,’ public health bureaucrats, and modelers whose sole reason for receiving funding is to find and publicize new variants of viruses. We have international public-private partnerships devoted to developing and distributing vaccines for such events, supported by taxpayer funding. We also have a draft pandemic treaty that has just been deferred by the WHA, intended to further increase public funding for this private good. From an industry viewpoint, its rapid passage in the coming months would benefit from fear and urgency.
Making Bird Flu Work
Declaration of a bird flu pandemic therefore looks almost inevitable, whether facilitated by ongoing gain-of-function research and a lab leak, or through a natural passage to humans. This inevitability is not so much because it is a real and existential threat, but rather because the industry – the financial-Pharma-media-public health complex that has arisen before and through Covid, needs it. The virus is real. The threat can also be made to appear existential. It is likely to proceed with something like the scenario below.
Traces of genome and even whole viruses can be found in raw agricultural produce. Testing these, and human sewage (contaminated with virus from birds or humans), is already underway and will demonstrate this. Genome has already been found in milk, probably because we looked for it – this has probably also happened often, undetected, before.
Extensive testing of workers on chicken farms and on farms where other infected animals are housed (e.g. dairy herds) will find people who test positive for the virus. Biology is highly variable and some people will establish short-lived mild infections. A few will become severely ill and die due to some immune deficiency or factors such as a very high infective dose. Once listed as a rare pneumonia of unknown cause, such infections can now be definitively pinned as bird flu and used very effectively by media to increase viewership. Within the public health community, these occurrences promote salary and research funding and are extremely important.
Mass killing (culling) at chicken farms. This won’t halt spread, as spread mainly occurs through wild bird species. It could theoretically protect workers from the low (but not zero) risk they face. Importantly, it makes news and promotes a perception that something really bad is afoot. Those who order culls do not suffer from them, and industrial chicken producers are compensated by taxpayers, who will also pay more for eggs and chicken meat. Left unchecked, many chickens would have died in an outbreak, while some would have survived.
Mass killing of secondary hosts such as cattle. Again, a low risk to humans. It is also relatively easy to quarantine cattle herds until an outbreak has run its course. However, culling creates publicity and the impression of a dynamic, desperate response, important in creating a sense of a public health sector scrambling to save the public. It also supports a movement claiming that farming for meat should be replaced by highly processed factory-derived alternative foods, an alternative that is struggling for market share. The fake meat industry is supported by some of the same major investors as Pharma, who are very vocal in the pandemic agenda.
Modeling to demonstrate potential mass death within the population. The major modeling groups (e.g. Imperial College London, University of Washington, Gates Foundation) are funded by entities who are invested in Pharma and gained greatly from Covid-19. Modelers understand outcomes that benefit sponsors, which may have influenced the emphasis on worst-case and highly unrealistic outcomes during Covid-19.
Requirement for mass vaccination (or killing) of backyard chickens to keep the community safe. The concept of ‘greater good’ is the most popular of the concepts that underpin fascism, and can be used to ensure broad compliance, with vilification of non-compliers being the penalty. This was used widely by pro-corporate politicians such as Justin Trudeau to isolate and denigrate those who wanted to weigh harms against the benefits of Covid vaccines or supported the concept of bodily autonomy. The UK and Ireland recently introduced a requirement to register all backyard chickens, to facilitate this process.
Requirement for vaccination of chicken owners – owners of every farm or backyard hen. This will be sold as further protecting their neighbors and communities. Those refusing will be portrayed as ‘putting their entire communities at risk, especially ‘the most vulnerable.’ This message, however distanced from context and reality, is very powerful and the media demonstrated during Covid how willing they are to exploit such division and scapegoating.
Lockdowns, school closures, closure of smaller workplaces. As during Covid, this will involve mainly those lacking influence at WEF and similar forums. There will be some deaths in the community, and even busy ICUs from influenza or other causes. The busy ICUs will be highlighted as unusual (which, of course, they are not) to promote a need to ‘all pull together’ and overcome the threat. This is a difficult message to counter, as on a superficial level such fascistic greater good claims make support for individual choice, fundamental to free societies, difficult.
Population-wide mass vaccination. Mass vaccination can be promoted as inconvenient but necessary as an all-in community safety issue. Although people may be more resistant as harms from Covid vaccination become more widely acknowledged, bird flu is already being portrayed as potentially far worse. The vaccine will be pitched as a way to get freedoms back, a form of coercion once anathema in public health but now mainstream. With hundreds of billions in Pharma sales at stake, it is an extremely hard train to stop. Billions spent on advertising, political sponsorship, and propaganda are literally minor business expenses.
The order of the above steps, and the emphasis, may change. None of the steps will stop bird flu. It spreads through wild bird species and will continue to do so. Occasionally, it will spill over into humans. Very occasionally these will cause a significant outbreak. The Spanish flu was a bad example, but life rapidly went back to normal.
Managing Perceptions
In the century since the Spanish flu, influenza outbreaks have continued to resolve naturally with little change in human behavior, but steadily building alarm. The Hong Kong flu of 1968-69 had been shrugged off as an annoyance and didn’t even stop Woodstock. The SARS outbreak in 2003 (a coronavirus, not influenza) promoted widespread fear, yet killed in total the same as die every 8 hours from tuberculosis. The Swine flu outbreak of 2009, which killed less than normal seasonal influenza, precipitated an international crisis. Pandemics, though real, are mostly about perceptions. So is the response.
The pandemic industry has become far better, and more systematic, at managing perceptions. This is the whole basis on which the behavioral psychology of government ‘nudge units’ was based during Covid. The aim was not a calculated overall public good, but to promote a particular set of public behaviors to address a narrowly defined threat. This is now underway for bird flu. A large part of the populace will comply with increasingly strict measures, not because they have been presented accurate information in context upon which they can make rational choices, but because they are fooled, or coerced, into behaviors they would not normally follow. They will accept restrictions and interventions that they would normally resist.
Unless wider society regains control of the agenda, the Pharma industry and its investors are set to make a killing through bird flu. It will be at least as big as Covid. It will also serve an important role in further building the pandemic industry, justifying the finalization of the postponed WHO Pandemic Agreement (treaty). It is a vital cog in the Great Reset.
Outbreaks do occur and we should monitor and prepare for them. However, we have allowed the development of a system where outbreaks are almost all that matter. Perceptions of risk, and resultant funding, have become grossly disproportionate to reality. The perverse incentives driving this are obvious, as are the harms. The world will be increasingly unequal and impoverished, and sick, building on the outcomes of the Covid response. Fear promotes profit better than calmness and context. It is on us to remain calm and continually educate ourselves regarding context. No one will sell these to us.
David Bell, Senior Scholar at Brownstone Institute, is a public health physician and biotech consultant in global health. He is a former medical officer and scientist at the World Health Organization (WHO), Programme Head for malaria and febrile diseases at the Foundation for Innovative New Diagnostics (FIND) in Geneva, Switzerland, and Director of Global Health Technologies at Intellectual Ventures Global Good Fund in Bellevue, WA, USA.
June 10, 2024
Posted by aletho |
Corruption, Deception, Science and Pseudo-Science, Timeless or most popular | Covid-19, COVID-19 Vaccine |
Leave a comment
The World Health Organization (WHO) is expanding its “health promoting schools” initiative worldwide, citing flagging vaccination rates and the need to provide medical services to underprivileged children and combat alleged misinformation.
The COVID-19 pandemic is behind the latest push to expand its “Making Every School a Health Promoting School” program, the WHO said, citing “the largest disruption of education systems in history” and “the health effects of mass school closures” and other pandemic-related disruptions.
The agency said the initiative aims to “serve over 2.3 billion school-age children” worldwide.
But critics say that behind the WHO’s noble-sounding plan to expand health-promoting schools — also known as school-based health centers (SBHCs) — is an attempt to gain “a foothold in our schools,” to bypass parental consent and expand vaccination, data collection and surveillance.
Laura Sextro, CEO and chief operating officer of The Unity Project, a California-based health freedom and parental rights nonprofit, told The Defender that SBHCs are “very, very agenda-driven organizations within the school system.”
Sextro said SBHCs “will cover everything from sex education [to] radical gender ideology. They’ll be talking about driving vaccines … That is something that frankly parents should have the autonomy” over.
Valerie Borek, associate director and lead policy analyst for Stand For Health Freedom, said SBHCs will promote “vaccines, especially COVID, HPV, and influenza.”
“School-based health centers have no place in public schools,” said Sheila Matthews, co-founder of AbleChild: Parents for Label and Drug Free Education. Matthews alleged the centers allow “Big Pharma access to our children, who are a captive audience.”
Nigel Utton, a board member of the World Freedom Alliance and coordinator of its Education Charter, said the WHO can’t be trusted to support the health of young people. “If it did, no child in the world would live in unsanitary conditions, or be subjected to trafficking, poor nutrition or emotional intimidation within school systems,” he said.
“Instead, the WHO wastes enormous resources on forcing vaccination programs — injecting children with dangerous chemicals including animal proteins, heavy metals and other unspecified ingredients,” Utton added.
Critics also question the involvement of private interests in SBHCs, including the Bill & Melinda Gates Foundation — and Bill and Melinda Gates themselves — in promoting SBHCs and funding the WHO’s reports on the subject.
School-based health centers give ‘Big Pharma access to our children’
SBHCs aren’t new — the concept dates back to the 1970s. The WHO, UNESCO and UNICEF have actively promoted such programs since 1995.
SBHCs are intended to offer “primary care, mental health care, and other health services in schools,” particularly in underserved communities. This includes services such as immunizations and “well-child care.”
A 2020 paper in Health Promotion Perspectives, whose lead author, Manuela Pulimeno, Ph.D., is UNESCO’s chair on health education and sustainable development, said health-promoting schools help “integrate health educational goals in a holistic perspective at school” and have shown positive outcomes.
“To achieve this goal, health-related contents may be embedded in the school curricula as core discipline,” the paper states.
The American Academy of Pediatrics (AAP) has endorsed SBHCs, stating they “improve access to health care services for students by decreasing financial, geographic, age, and cultural barriers.”
In the U.S., the School-Based Health Alliance promotes SBHCs. According to the alliance, about 3,900 SBHCs operate nationally, up from around 1,900 in 2012. A September 2023 study in JAMA Network Open called for “additional SBHC expansion.”
In 2022, the Biden administration issued $75 million in grants to states to expand SBHCs, while the Centers for Disease Control and Prevention incorporated SBHCs into its “Whole School, Whole Community, Whole Child” model.
On a global level, “work is currently underway with early adopter countries such as Egypt, Kenya, North Macedonia and Paraguay to support governments in building a new generation of school health programmes,” the WHO said in a May 26 report.
WHO’s global standards for SBHCs include censorship and surveillance
In their report, the WHO developed eight “global standards” for SBHCs (page 3), in which school health services represent just one such standard. Other standards include school and government policies, school governance and leadership, school and community partnerships, schools social-emotional and physical environments and curriculum.
These are accompanied by 13 “implementation areas,” (page 17) calling for reinforcement of “intersectoral government and multi-stakeholder coordination,” strengthening “school and community partnerships,” curriculum development, “teacher training and professional learning” and monitoring and evaluation.
Critics say these proposals allow schools to implement vaccine programs. For instance, SBHCs have been linked to higher human papillomavirus (HPV) vaccination rates, according to a 2022 report.
Merck, the maker of the Gardasil HPV vaccine, is a funder of the School-Based Health Alliance, whose board includes several members with ties to Big Pharma and vaccine-promoting organizations.
The Gardasil HPV vaccine is often administered to teenagers as part of school vaccination programs. In October 2023, a 12-year-old boy in France died days after collapsing and injuring himself minutes after HPV vaccination at his school.
In the U.S., several state and city government websites include vaccinations among the list of services SBHCs provide.
“Increased vaccine uptake is a mark of success for school-based health programs,” Borek said. “They’re considered an optimal place to promote and administer vaccines. In fact, schools and vaccine policy go hand in hand historically — vaccines didn’t have a strong foothold until schools mandated them for admission.”
Utton pointed out that “schools have been used to coerce and manipulate children into taking vaccinations against the will of their parents. Teachers have been indoctrinated, and those who have questioned the manipulative agenda have been ostracized.”
Borek said the “psychological pressure” a child experiences when a school authority figure recommends any kind of medical care creates a “fertile ground for pushing policy.”
SBHCs ‘will certainly be a tool to collect data’
Included among the WHO’s global standards for SBHCs are interventions in school curriculums and proposals to “embed school health content” in training for educators.
The 2020 Health Promotion Perspectives paper said the WHO calls for the incorporation of “health literacy” in “the core curriculum as children enter school.”
Critics told The Defender that changes like these could lead to the inclusion of non-health-related topics in school curricula under the guise of health education.
Virginie de Araujo-Recchia, a French lawyer and member of ONEST, France’s National Organization of Ethics, Health and Transparency, told The Defender that SBHCs may be “favored by the political powers in an attempt to achieve a fusion between education, citizenship and environmental causes.”
The WHO’s global standards for SBHCs also target “misinformation.” According to UNESCO, SBHCs “can … teach young people develop the critical thinking skills they need to reject harmful health-related myths and misconceptions,” noting that “This is a key in responding to pandemics like Covid-19 and HIV.”
The global standards call on schools to develop “versatile physical spaces that can be adapted to changing restrictions, as in managing the COVID-19 pandemic.”
The WHO’s global standards also contain provisions for increased data collection and surveillance in schools, with the 13th “implementation area” calling on schools to “Design, develop and share practices for collecting, storing and analysing data.”
This is linked to calls to provide “capacity-building in evaluation (e.g. data collection and analysis)” and investments “in feasible … interoperable systems for collecting and storing data from monitoring at all levels of the education and/or health system.”
According to Stand for Health Freedom, SBHCs are “completely unregulated” in the U.S.
For instance, it is unclear how HIPAA (the Health Insurance Portability and Accountability Act of 1996) andthe Family Educational Rights and Privacy Act will be applied to SBHCs and students’ health information.
SBHCs “will certainly be a tool to collect data on anything from vaccine status to sexual preference,” Sextro said.
Children can become ‘health trainers of their parents’
The WHO claims SBHCs involve “all stakeholders, and particularly students, parents and caregivers.” The agency’s global standards call for “opportunities for parents … to participate meaningfully in the governance, design, implementation and evaluation” of SBHCs and their inclusion on “design teams” and governance boards.
But the WHO appears to contradict itself, excluding parents from the “system of global standards for health-promoting schools” and noting that the “target readership” of its SBHC-related documents is “mainly people in government.”
According to Nemours KidsHealth, the centers “only provide care to children with parents’ written permission.” However, the organization notes that this “permission” usually consists of “the option to sign a permission form at the beginning of each school year.”
A consent form for an Atlanta SBHC shared with The Defender says nothing about parents being notified before, during or after treatment. Last year, a Connecticut school board was sued for rejecting a government-funded school-based mental health clinic that aimed to treat teens without parental consent.
“The reason they’re doing this is because they don’t want parents to be able to exercise their rights, which is to … make medically informed decisions on behalf of their children. And so, they’re usurping the parents,” Sextro said.
“Parents need to be front and center in their child’s medical care,” Borek said. “These centers are cleaving that relationship by promoting medical assessments and treatment without the presence of a parent.”
A proposed bill in New Hampshire (SB 343) would require parents to be present when services are provided at an SBHC.
“Schools are clearly not the place to introduce school health centers,” de Araujo-Recchia said. “Our children are neither guinea pigs for mass medical experimentation nor beings to be sacrificed.”
Notably, UNESCO suggests SBHCs can help children “educate” their parents on health matters. According to the 2020 Health Promotion Perspectives paper, SBHCs can help children “become health trainers of their parents, relatives and friends, impacting positively the entire society.”
Gates ‘has a direct financial benefit’ from SBHCs
Earlier this year, Melinda French Gates announced a $23 million investment in the School-Based Health Alliance, alongside fellow billionaire MacKenzie Scott, ex-wife of Amazon CEO Jeff Bezos.
The Gates Foundation has also provided financial support for the publication of at least two WHO reports on SBHCs.
“The Gates Foundation and Gavi, The Vaccine Alliance [founded and funded by Gates] fiercely promote childhood vaccination, and make a lot of money from it,” de Araujo-Recchia said. “This is not philanthropy at all, but a stranglehold and ideology,” citing the WHO’s partnership with the Rockefeller Foundation as another example.
Sextro said Gates “has a direct financial benefit and interest in promoting these school-based health centers, because they will directly promote everything from the pharmaceutical to the vaccine interest that he and the Gates Foundation have.”
The WHO’s global standards for SBHCs include calls for the delivery of “comprehensive school health services based on a formal agreement between schools (or local education departments) and health service providers.”
According to the School-Based Health Alliance, 21% of funding for SBHCs in the U.S. came from private foundations in 2022, while according to the AAP, “local hospitals [may] provide … financial support for SBHCs.”
The WHO “is mainly financed by private funds from companies or foundations owning pharmaceutical labs,” de Araujo-Recchia said. “The capital links between the mainstream media, digital giants, American financial giants and the WHO demonstrate real collusion.”
Michael Nevradakis, Ph.D., based in Athens, Greece, is a senior reporter for The Defender and part of the rotation of hosts for CHD.TV’s “Good Morning CHD.”
This article was originally published by The Defender — Children’s Health Defense’s News & Views Website under Creative Commons license CC BY-NC-ND 4.0. Please consider subscribing to The Defender or donating to Children’s Health Defense.
June 9, 2024
Posted by aletho |
Civil Liberties, Full Spectrum Dominance | COVID-19 Vaccine, Human rights, WHO |
Leave a comment
The witch hunts against dissident doctors continue
In June 2021, Dr. Sam White, a general practitioner, released a video calling out harmful covid policy. From a scientific perspective every word he said was entirely defensible. Moreover it is clear that he was speaking from an ethical position of wanting to protect his patients from harm. He pulled no punches in addressing the most prominent issues that were causing harm – lack of treatment for the frail, inappropriate gene therapies and masking. In interviews, in 2022, he called the situation a war between good and evil. In doing so he unleashed a torrent of anger among those in a position of power over him, which, three years on, continues to harm him.
He had already resigned from his GP partnership in protest at their vaccination policy in February 2021. His conscience had been keeping him awake at night because he did not want to be a part of the vaccine rollout. Consequently, after resigning he was signed off with stress rather than having to work his notice. NHS England still saw fit to suspend him with an emergency order in June. Dr White managed to record a conversation with an NHS senior clinical adviser who implied that he was mentally unwell. Dr White believes that possession of that recording led the NHS to revoke their suspension. However, by then the NHS had referred him for a GMC investigation and an automatic GMC suspension.
The GMC overturned the suspension in August 2021 but imposed restrictions on him including a ban on mentioning covid on social media and requiring the removal of his previous posts. The legal position is that doctors have a right to free speech but if the GMC could prove Dr White’s speech was a threat to the health of the public or undermined trust in the profession then he could be sanctioned.
Dr White looked to his indemnity provider for support to fund his legal case but they washed their hands of him saying it was a “conduct issue”. With the help of crowd funding support, Dr White took the case to the High Court in November 2021. The verdict was published in December 2021, overruling the GMC and saying they had not followed due process in their actions. The High Court documentation was removed from the judiciary’s website in September 2022 such that other doctors in a similar position will be unable to refer to it in their defence. It is available on the Wayback Machine.
Dr White has asked to be removed from the register, as he is no longer practising conventional medicine, but the GMC have refused and are continuing to persecute him. Every interview he has undertaken has been transcribed and put forward as evidence that he is undermining public health policy and causing the public to lose trust in the profession. The next tribunal hearing is scheduled to last three weeks in August and September 2024. This ongoing investigation, three years later, indicates a relentless effort to discredit and punish Dr. White for his dissenting views.
If that sounds bad, wait until you hear about the NHS’s role.
The same day as the High Court hearing, unbeknown to Dr White or his lawyers, NHSE had a meeting where they decided to refer Dr White for a health assessment, despite the fact he no longer worked in the NHS. This was an opportunity to reopen the investigation into him. They have repeatedly asked if he had returned to NHS work and said he must tell them if he did. What was their intent here? Were they planning to ask any future employer to suspend him all over again?
NHS England has a list of “approved providers”. Any doctor not on their list cannot work for the primary employer of doctors in the country. In 2023, NHS England removed Dr White from their list, effectively barring him from practising within the NHS. He had already shifted his practice to private healthcare with a holistic focus, but this further punishment leaves him with no other options.
The GMC is far from perfect but at least it has due process and a system of appeal for where there might be an injustice. NHS England can unilaterally destroy a career, with no legal recourse.
In some ways, the most disturbing aspect of the whole affair was revealed in the communications between the GMC and NHS England. Firstly, the derogatory terms used about the doctor to justify their behaviour are shocking and reveal a lack of professionalism and intolerance for differing opinions within the medical establishment. Moreover, this language served as a means to rationalise their harsh and unjust actions towards him. Secondly, they appeared to be acting in cahoots. The GMC’s apparent open and fair processes have been bypassed by direct communication with NHS England, stripping Dr White of a right to employment.
Dr. Sam White’s case is a stark example of systemic injustice and the erosion of professional rights within the NHS and the GMC. His ongoing persecution for voicing dissenting views underscores a troubling intolerance for ethical and scientific debate, reminiscent of a Kafkaesque nightmare where rationality and justice are subordinated to bureaucratic oppression.
June 8, 2024
Posted by aletho |
Civil Liberties, Corruption, Full Spectrum Dominance, Science and Pseudo-Science | COVID-19 Vaccine, Human rights, NHS, UK |
Leave a comment
Appellate Decision Sides with Physicians Rights to Free Speech
Several medical credentialing boards instituted COVID-19 Misinformation Policies in September of 2021 and have used them to censor and retaliate against academics and practicing physicians who performed research, clinical care, and presented their findings on the early treatment of acute COVID-19 and vaccine safety. The boards’ position is that they and the government agencies they agree with, hold agency over the truth. By establishing that power dynamic, members who disagree with them are spreading misinformation and can be convicted in closed panel meetings without the member being allowed to present their views based upon the data and evidence at hand.
The Association of American Physicians and Surgeons sued three medical specialty boards for their threatened actions against the board certifications of physicians because of speaking out on medical controversies. Physicians earned and need these board certifications in order to hold professorships, practice medicine in most hospitals, and remain in most insurance networks.
Defendants are the American Board of Internal Medicine (“ABIM”), the American Board of Family Medicine (“ABFM”), and the American Board of Obstetrics & Gynecology (“ABOG”). In addition, Alejandro Mayorkas, Biden’s Homeland Security Secretary, is a defendant due to alleged government interference with freedom of speech.
The Fifth Circuit also invalidated Galveston Local Rule 6, by which that federal district court has infringed on plaintiffs’ right to amend their lawsuits. The Fifth Circuit agreed with AAPS that this district court rule is contrary to the Federal Rules of Civil Procedure, and thus must be voided.
“AAPS can now pursue its claim against censorship by the Biden Administration,” AAPS Executive Director Jane Orient, M.D., stated.
Fifth Circuit Judge James Ho agreed with the panel majority on the key issues and wrote separately to decry attempts by some today to impose censorship on others. “In America, we don’t fear disagreement—we embrace it. We persuade—we don’t punish. We engage in conversation—not cancellation,” Judge Ho wrote.
“We know how to disagree with one another without destroying one another. Or at least that’s how it’s supposed to work,” Judge Ho added as he sided fully with this lawsuit against censorship.
The precedent-setting ruling in favor of the First Amendment was issued by the U.S. Court of Appeals for the Fifth Circuit. This influential Court established the right to object in court to censorship of physicians’ speech on topics ranging from government Covid policies to abortion. AAPS General Counsel Andrew Schlafly should be congratulated for this stalwart effort in defense of our civil liberties.
June 8, 2024
Posted by aletho |
Civil Liberties, Full Spectrum Dominance, Science and Pseudo-Science | Covid-19, COVID-19 Vaccine, United States |
Leave a comment
The Highwire with Del Bigtree | June 6, 2024
The WHO’s Pandemic Treaty missed its deadline, but their amendments to the International Health Regulations have passed enshrining new pandemic rules for the legally binding contract for 196 countries.
June 8, 2024
Posted by aletho |
Deception, Video | COVID-19 Vaccine, United States |
Leave a comment
Excess death data from 47 countries in the Western world show that excess mortality has remained high for the last three consecutive years — despite COVID-19 lockdown measures and COVID-19 vaccines, concluded the authors of a peer-reviewed study published Monday in BMJ Public Health.
“This is unprecedented and raises serious concerns,” said the team of Dutch researchers, who analyzed all-cause mortality reported in the “Our World in Data” database.
The open-access database included reports from the Human Mortality Database — known as “the world’s leading scientific data resource on mortality in developed countries” — and the World Mortality Dataset, which researchers used to track excess mortality during the COVID-19 pandemic.
In addition to presenting excess death figures, the Dutch authors cited research showing negative health outcomes related to COVID-19 vaccination programs and lockdown measures.
The researchers called on government leaders and policymakers to “thoroughly investigate underlying causes of persistent excess mortality.”
The Telegraph — a prominent mainstream U.K. newspaper — today ran a front-page article on the study with the headline, “Covid vaccines may have helped fuel rise in excess deaths.”
Dr. Meryl Nass posted a photo of the article on Substack, writing, “The dam has broken.”
Earlier this year, Norwegian researchers published a peer-reviewed study in BMC Public Health, showing an increase in excess non-COVID-19 mortality — or deaths attributed to causes other than a COVID-19 infection — in Norway in 2021 and 2022. TrialSite News reported on the Norway study last week.
The study authors noted a “temporal concordance” between Norway’s increase in non-COVID-19 excess mortality and the country’s increase in mRNA COVID-19 vaccination.
Dr. Pierre Kory told The Defender, “This is unsurprising and totally in line with what we have argued is the effect of the mRNA vaccines.”
Kory — who has written numerous op-eds calling for an investigation into what’s causing excess deaths — said there are “numerous mechanisms of the spike protein used in the shots [that] cause endothelial damage and hypercoagulability [excessive blood clotting] leading to heart attacks, strokes, aortic aneurysms.”
“Other mechanisms increase the risk of cancer,” he said, “in particular the ubiquitous findings of DNA contamination of the vials with cancer-promoting sequences such as SV40.”
‘Every death needs to be acknowledged’
The Dutch team’s study on excess deaths in 47 countries showed that excess mortality in 2020 was documented in 41 of the 47 countries.
Over the next two years, that number increased to 42 and 43 countries in 2021 and 2022, respectively.
Overall, there were 3,098,456 excess deaths from Jan. 1, 2020, to Dec. 31, 2022, with just over 1 million of those occurring in 2020.
“In 2021,” they wrote, “the year in which both containment [i.e., lockdown] measures and COVID-19 vaccines were used to address virus spread and infection, the highest number of excess deaths was reported: 1,256,942 excess deaths.”
They reported that in 2022 — “when most containment measures were lifted and COVID-19 vaccines were continued” — there were 808,392 excess deaths.
The authors pointed out that during the pandemic, politicians and the media emphasized “on a daily basis that every COVID-19 death mattered and every life deserved protection through containment measures and COVID-19 vaccines.”
“In the aftermath of the pandemic, the same morale should apply,” they said. “Every death needs to be acknowledged and accounted for, irrespective of its origin.”
The authors of the Dutch study called for government transparency in cause-of-death data so researchers can do “direct and robust analyses to determine the underlying contributors.”
This also means that autopsies need to be done to determine the exact reason for death, they added.
The Dutch authors noted that the data they analyzed may not have recorded all actual deaths because “countries may lack the infrastructure and capacity to document and account for all deaths.”
Record-keeping mishaps or delays may also cause deaths to go unrecorded.
Cardiovascular deaths driving non-COVID excess mortality in Norway
The Dutch authors’ findings were corroborated by the earlier Norwegian study on non-COVID-19 excess mortality in Norway from 2020 to 2022.
Researchers at the Norwegian Institute of Public Health analyzed death records in which a COVID-19 infection was not listed as the cause of death to discover the causes of non-COVID-19 excess deaths.
They used data from the Norwegian Cause of Death Registry, known for high data quality and reliability.
The Norwegian authors found “significant” excess mortality in 2021 and 2022 for all causes (3.7% and 14.5%), for cardiovascular diseases (14.3% and 22.0%), and for malignant tumors in 2022 (3.5%).
When discussing their findings, the authors noted that some people opposed COVID-19 mass vaccination campaigns “due to concerns about potential harmful effects of allegedly insufficiently tested vaccines.”
They noted that the uptick in non-COVID-19 excess deaths happened at the same time that most Norwegians had received an mRNA COVID-19 vaccine — but they were careful to avoid outright stating a causal link between COVID-19 vaccines and excess deaths.
“From data available to us, it was not possible to compare excess mortality in vaccinated and unvaccinated individuals,” they said.
They said preliminary analyses from the National Preparedness Register for COVID-19 in Norway did not show signs of increased mortality among vaccinated older people.
TrialSite News speculated that the study’s authors avoided suggesting that the surge in excess cardiovascular deaths could be tied to Norway’s mass vaccination program because they may have faced difficulty getting their work published.
The Norwegian authors said lockdowns may also have contributed to the increase in non-COVID-19 excess deaths.
“There has been concern that lockdowns have resulted in less use of health care, leading to diseases that otherwise would have been discovered remaining undiagnosed, possibly with increased mortality,” they wrote.
Studies need to be done to assess this possibility, they said.
“Researchers,” they added, “should also investigate whether the [lockdown] restrictions have resulted in deterioration of lifestyle factors, such as less physical activity, a less healthy diet and even social and mental health issues that influence mortality.”
This article was originally published by The Defender — Children’s Health Defense’s News & Views Website under Creative Commons license CC BY-NC-ND 4.0. Please consider subscribing to The Defender or donating to Children’s Health Defense.
June 5, 2024
Posted by aletho |
Science and Pseudo-Science | COVID-19 Vaccine |
Leave a comment
Today, the largest protest against the World Health Organization (WHO) began, with an opening speech by Kazuhiro Haraguchi, a former Minister for Internal Affairs and Communications in Japan and a current member of the House of Representatives. The massive gathering aimed to highlight several critical issues, as Haraguchi delivered a powerful and heartfelt address that resonated with many.
Haraguchi began by addressing the grief and loss felt by countless individuals and families due to the pandemic. With a deep sense of sincerity, he extended his condolences and took responsibility for the failings of those in power. “I apologize to all of you. So many have died, and they shouldn’t have,” he said. His words reflected a deep empathy and regret for the preventable tragedies that have occurred, setting a somber yet resolute tone for the event.
One of the key points in Haraguchi’s speech was his criticism of the ban on Ivermectin, a drug developed by Dr. Satoshi Omura, which he believed could have played a significant role in combating the pandemic. Haraguchi questioned the motives behind the ban, suggesting that economic interests were prioritized over public health. “Why? Because they are cheap. They don’t want it because it will interfere with the sales of the vaccines,” he argued. This statement drew loud applause from the crowd, many of whom felt that corporate profits had taken precedence over human lives.
Haraguchi then shared a deeply personal story about his own health struggles. After receiving vaccines, he developed a severe illness, specifically a rapidly progressing form of cancer. “This time last year, I had neither eyebrows nor hair. Two out of the three supposed vaccines I received were lethal batches,” he revealed. This candid account of his battle with cancer, which included significant physical changes like hair loss, struck a chord with the audience. He recounted an incident where his appearance became a point of distraction in the Diet, with an opponent focusing more on his wig than the issues at hand.
Adding to the conversation, Haraguchi disclosed that he was not the only member of Japan’s National Diet to suffer adverse effects from vaccines. He mentioned that three of his colleagues had been severely affected, with some even hospitalized. “They are falling to pieces, some hospitalized. But they don’t speak up,” he explained. This revelation underscored a broader issue: the reluctance or inability of public figures to discuss their personal health challenges openly.
Haraguchi was particularly passionate about the attempts to silence those who question current policies and government actions. He recounted a recent incident where he was banned from speaking on Channel 3 after an interview with its president. “The other day, I spoke with the President of Channel 3, and I was banned. They are trying to silence our voices,” he stated. This attempt to censor dissenting voices highlighted a critical concern about freedom of speech and expression. Haraguchi urged the audience to remain steadfast in their resolve, saying, “They are trying to block our freedom, our resistance, our power. But we will never lose.”
In the conclusion of his speech, Haraguchi issued a rallying call for action. He urged the people to stand united in challenging the government and its questionable decisions. “Let’s overthrow this government,” he proclaimed, emphasizing the need for change and accountability. He called on legislators to continue fighting for the people’s lives and freedoms, “Let’s make it happen,” he concluded.
The protest that is happening right now (31st May 2024), which aims to draw tens of thousands of participants, marked a significant moment in the global discourse about pandemic management and health policies. Haraguchi’s speech, filled with personal anecdotes and strong criticisms, resonated deeply with the attendees.
June 3, 2024
Posted by aletho |
Corruption, Science and Pseudo-Science, Timeless or most popular, War Crimes | COVID-19 Vaccine, Japan |
Leave a comment
Spoiler: they don’t care about your health and they never have, not really
In 2019 the World Health Organization listed “vaccine hesitancy” as one of the top ten threats to global health.
“The reluctance or refusal to vaccinate despite the availability of vaccines,” this multi-billion-dollar agency explained, “threatens to reverse progress made in tackling vaccine-preventable diseases.”
According to the WHO: “Vaccination is one of the most cost-effective ways of avoiding disease—it currently prevents 2-3 million deaths a year, and a further 1.5 million could be avoided if global coverage of vaccinations improved.”
In 2019 a lot of people believed this to be true, shaking their heads in dismay at “those crazy antivaxxers.”
Five years later there’s a shift happening.
More people than ever before—especially those in healthcare professions—are starting to do their own research, use their own human brains to think about things that they always took at face value, and change their minds about vaccines.
According to a peer-reviewed article published last week in Nature’s Scientific Reports, there has been a “global rise in vaccine hesitancy.”
One of my readers, Beth, would likely agree.
An M.D. colleague of mine, who has been squarely pro-vaccine his entire career, has started to change his mind about vaccines.
The reason?
He’s spending most of every day in his clinical practice treating mainstream patients who are suffering from severe adverse reactions to the vaccines they’d been so eager to get.
After seeing the reactions for himself, he did something he did not used to do as a busy clinician in private practice: he started looking beyond the CDC’s recommendations and reading scientific studies for himself.
Several studies he read, and alternative news articles about them, left him with so much cognitive dissonance that he almost decided to quit medicine for good.
Three of these peer-reviewed scientific studies about COVID-19 vaccine safety caught his attention:
1) A 2022 study by Italian scientists that showed that 94 percent of vaccinated patients who went to the doctor with subsequent health problems presented with abnormal blood. The three Italian scientists who examined freshly drawn blood of more than a thousand patients noted that though they had no clear explanation for their findings, they were so unusual that they felt the need to alert the medical community.
2) A 2022 study published in the journal Food and Chemical Toxicology by an international team of researchers that included an MIT senior scientist and one of the world’s foremost and most respected cardiologists, presented evidence that the mRNA vaccines impaired type 1 interferon signaling, which has diverse—and sometimes devastating—consequences to human health, including a “causal link” to neurodegenerative disease, myocarditis, immune thrombocytopenia, and cancer.
3) An extended analysis conducted by a team of nine experts from Harvard, Johns Hopkins, and several other elite universities that found that COVID-19 booster shots for young people actually caused many more serious adverse events for every one (1) theoretical COVID-19 infection-related hospitalization they prevented. Among the team of scientists that published this paper was Dr. Salmaan Keshavjee, M.D./Ph.D., the director of the Harvard Medical School Center for Global Health Delivery. The paper concluded that, given efficacy and safety concerns, mandating COVID-19 vaccines for college students was unethical.
This doctor had previously testified in favor of allowing state officials to bar unvaccinated or partially vaccinated children from attending public school, private school, and daycare. The bill he supported, thankfully, was not passed into law.
Why would he have supported taking medical freedom and vaccine choice away from parents?
I choose to believe that nearly all doctors have human health and their patients’ wellbeing at the forefront of their minds.
Yes, doctors like the respect they get from being medical doctors.
Sure, they love the money and the houses they can buy with it, the vacations they can take, and the elite colleges they can afford to send their children to.
But most doctors also care, deeply, about the people who come to them for help.
This doctor once believed that by protesting against allowing unvaccinated and partially vaccinated children to attend school he was helping make America a healthier, happier place.
In his mind—programmed by four years of medical training, a residency, continuing education courses, most if not all of his colleagues, the billboards he passed on the highway on his commute to the office every day, the advertising he saw on TV, and the news channels he tuned into several times a day—vaccines were synonymous with health.
And the more vaccinated a child, the healthier.
You don’t know what you don’t know.

Screenshot of educational material about over-vaccination produced by the National Vaccine Information Center, a non-profit based in Washington, D.C., that was founded by a parent whose child was severely and irreversibly vaccine-injured based
He didn’t know that, due to federal law, vaccine manufacturers in America are not liable for vaccine-related adverse events caused by the products they manufacture.
And he admitted, in a confessional tone of voice, that before COVID he probably wouldn’t have cared anyway.
He didn’t believe in vaccine adverse events, had never filed a VAERS report, and had always dismissed patients’ concerns that the problem their child experienced right after being vaccinated as an “unfortunate coincidence.” In his mind, bad vaccine reactions simply didn’t exist.
He’d never bothered to peruse a single peer-reviewed article about vaccine safety, read a vaccine critical book, or attend a holistic health conference.
Why would he?
Reading a book about safety, efficacy, and necessity issues related to vaccines would have been like reading a book about the safety of broccoli or the efficacy of drinking water to hydrate the body.
But now this doctor has changed his mind.
He’s caring for hundreds of patients trying to heal from adverse reactions to the COVID vaccines. He’s been in practice for over twenty years but is currently seeing turbo cancers, heart problems, neurological problems, blood clots, and immune dysfunction that he has never seen before.
Most of these patients have had both COVID infections and at least two—sometimes as many as five or six—COVID vaccines.
It’s hard to pinpoint the exact cause of these problems and the mechanisms by which they are happening.
Could it be due to the COVID infections? The vaccines? The boosters? The conventional treatments, including Paxlovid? Or some combination of all of these?
Though he does not know, he has now filed over a dozen VAERS reports to alert the CDC. To date, no one at the CDC has responded to any of his reports.
This doctor has over a thousand families in his practice. He employs another medical doctor, a nurse practitioner, and front-end staff.
For the past three plus years he’s chosen to work quietly from behind the scenes, trying to gently educate his mainstream allopathic-minded patients about his new vaccine safety concerns without alienating them.
While the world needs more medical doctors to speak publicly about the vaccine safety concerns and the adverse events they’re seeing firsthand, this doctor is afraid to come out of the closet. He accepts insurance, has a diverse patient population, and doesn’t want to lose his license.
He’s also trying very hard to avoid being witch-hunted as so many COVID critical doctors, including my co-author Dr. Paul Thomas, M.D.; my colleague Dr. Steven LaTulippe, M.D.; and my friend and colleague Dr. Meryl Nass, M.D.; already have.
Medicine is big business.
These mRNA vaccines have proven their worth as money makers, allowing pharmaceutical executives to buy luxury real estate and put their newly minted billions into off-shore bank accounts.
The more people get vaccinated, the more money everyone in the industry makes.
There’s nothing wrong with making money.
But becoming rich at the expense of our children’s health and continuing to promote a toxic so-called preventative despite clear evidence that the harms outweigh the benefits is antithetical to the practice of medicine.
Still, as Beth so eloquently pointed out, the good news about this COVID nonsense is that more Americans than ever before are becoming aware of medical malfeasance. We may be on the cusp of a collective shift: a new national awareness about the importance of avoiding toxins, individualizing medicine, and thinking for ourselves.
June 2, 2024
Posted by aletho |
Science and Pseudo-Science, Timeless or most popular | COVID-19 Vaccine |
Leave a comment
In a new lawsuit, Webseed and Brighteon Media have accused multiple US government agencies and prominent tech companies of orchestrating a vast censorship operation aimed at suppressing dissenting viewpoints, particularly concerning COVID-19. The plaintiffs, Webseed and Brighteon Media, manage websites like NaturalNews.com and Brighteon.com, which have been at the center of controversy for their alternative health information and criticism of government policies.
We obtained a copy of the lawsuit for you here.
The defendants include the Department of State, the Global Engagement Center (GEC), the Department of Defense (DOD), the Department of Homeland Security (DHS), and tech giants such as Meta Platforms (formerly Facebook), Google, and X. Additionally, organizations like NewsGuard Technologies, the Institute for Strategic Dialogue (ISD), and the Global Disinformation Index (GDI) are implicated for their roles in creating and using tools to label and suppress what they consider misinformation.
Allegations of Censorship and Anti-Competitive Practices:
The lawsuit claims that these government entities and tech companies conspired to develop and promote censorship tools to suppress the speech of Webseed and Brighteon Media, among others. “The Government was the primary source of misinformation during the pandemic, and the Government censored dissidents and critics to hide that fact,” states Stanford University Professor J. Bhattacharya in support of the plaintiffs’ claims.
The plaintiffs argue that the government’s efforts were part of a broader strategy to silence voices that did not align with official narratives on COVID-19 and other issues. They assert that these actions were driven by an “anti-competitive animus” aimed at eliminating alternative viewpoints from the digital public square.
According to the complaint, the plaintiffs have suffered substantial economic harm, estimating losses between $25 million and $50 million due to reduced visibility and ad revenue from their platforms. They also claim significant reputational damage as a result of being labeled as purveyors of misinformation.
The complaint details how the GEC and other agencies allegedly funded and promoted tools developed by NewsGuard, ISD, and GDI to blacklist and demonetize websites like NaturalNews.com. These tools, which include blacklists and so-called “nutrition labels,” were then utilized by tech companies to censor content on their platforms. The plaintiffs argue that this collaboration between government agencies and private tech companies constitutes an unconstitutional suppression of free speech.
A Broader Pattern of Censorship:
The lawsuit references other high-profile cases, such as Missouri v. Biden, to illustrate a pattern of government overreach into the digital information space. It highlights how these efforts have extended beyond foreign disinformation to target domestic voices that challenge prevailing government narratives.
Webseed and Brighteon Media are seeking both monetary damages and injunctive relief to prevent further censorship. They contend that the government’s actions violate the First Amendment and call for an end to the use of these censorship tools.
As the case progresses, it promises to shine a light on the complex interplay between government agencies, tech companies, and the tools used to control the flow of information in the digital age. The outcome could have significant implications for the future of free speech and the regulation of online content.
May 30, 2024
Posted by aletho |
Civil Liberties, Full Spectrum Dominance, Science and Pseudo-Science | Covid-19, COVID-19 Vaccine, Human rights, United States |
Leave a comment
The North Carolina Supreme Court on May 23 agreed to hear the case of a Guilford County teenager who was given a COVID-19 vaccine against his will and without parental consent in August 2021, according to Carolina Journal.
The court’s decision to take up the case comes after a North Carolina appeals court ruled against the teen and his mother in March, upholding a lower court’s dismissal of their lawsuit.
Tanner Smith, then 14 years old, was instructed to get tested for COVID-19 at a Guilford County Schools vaccination site in order to continue playing football.
Despite Smith’s objections and the lack of parental consent, clinic workers administered a dose of the Pfizer COVID-19 vaccine, which at the time was available only under emergency use authorization (EUA).
In its unanimous ruling against Smith and his mother, Emily Happel, the appeals court found that the federal Public Readiness and Emergency Preparedness (PREP) Act shielded the defendants — Guilford County Board of Education and Old North State Medical Society — from liability in the lawsuit.
Commenting on the case, attorney Ray Flores, senior outside counsel for Children’s Health Defense, emphasized its significance for parental rights and the scope of the PREP Act’s liability shield.
“The North Carolina Supreme Court is the highest court so far to review parental rights vis-à-vis the PREP Act,” he told The Defender.
Flores argued that while the PREP Act is a “turbo-charged product liability immunity statute,” it should not shield “willful misconduct, fraud, breach of contract, undisclosed ingredients, false advertising — and certainly must not continue to abolish parental rights.”
Court recognized ‘egregious’ conduct but was ‘constrained’ by PREP Act
On August 19, 2021, Guilford County Schools sent a letter to Smith’s mother and stepfather about a “recent COVID-19 cluster” involving his football teammates. The letter recommended Smith report for a COVID-19 test to continue participating on the team.
The letter stated that testing would occur at Northwest Guilford High School on August 20, 2021, and that Old North State Medical Society would conduct the testing.
When Smith arrived at the testing site, workers gave him a form to fill out, which he believed to be related to the COVID-19 test.
Unbeknownst to Smith and his family, the site also operated as a COVID-19 vaccination clinic. Clinic workers attempted to contact Smith’s mother to obtain consent for administering the vaccine but were unsuccessful.
Despite the lack of parental consent and Tanner’s own objections, one of the clinic workers instructed another to “give it to him anyway,” and Tanner was injected with a dose of the Pfizer COVID-19 vaccine.
In August 2022, Emily Happel and Tanner Smith sued the Guilford County Board of Education and Old North State Medical Society, alleging battery and violations of their constitutional rights.
The plaintiffs argued that administering the COVID-19 vaccine without consent violated Tanner’s bodily autonomy rights and Emily’s parental rights under the North Carolina Constitution.
However, in February 2023, a lower court dismissed the case, citing the immunity provided by the federal PREP Act. The defendants argued that the PREP Act shielded them from liability for claims related to the administration of covered countermeasures, such as the COVID-19 vaccine, during a declared public health emergency.
The North Carolina Court of Appeals’ March decision affirmed the trial court’s dismissal of the lawsuit.
In its opinion, the court acknowledged the “egregious” nature of the conduct alleged in the case but found itself “constrained” by the broad immunity provided by the PREP Act.
The court held that both the Guilford County Board of Education and Old North State Medical Society were covered persons under the PREP Act and that the immunity applied to claims related to the administration of the COVID-19 vaccine.
The court noted that the PREP Act preempted state laws, including North Carolina’s statute requiring parental consent for EUA vaccines to minors.
‘We will win in the end’
Following the Court of Appeals decision, Emily Happel and Tanner Smith petitioned the North Carolina Supreme Court to hear their case.
The plaintiffs contended that the lower courts’ decisions have rendered North Carolina’s parental consent statute “totally useless” and “a law of aspiration, with no consequence for its blatant violation.”
David “Steven” Walker, attorney for the plaintiffs, wrote that the case:
“… involves legal principles of major significance to the jurisprudence of the State — the interplay between duty of the courts of North Carolina to remedy constitutional and other legal violations and a federal law that defendants purport forecloses that opportunity. …
“The trial court and the Court of Appeals interpreted the PREP Act so broadly as to shield nearly every act, no matter how egregious, from any legal consequence.”
On May 23, 2024, the North Carolina Supreme Court agreed to take up the case, focusing solely on the specific issue from Happel and Smith’s appeal concerning “Whether the trial court and the Court of Appeals erred when they determined that the PREP Act provided immunity to the defendants for constitutional violations and pre-empted all state law claims.”
The court’s decision to hear the case sets the stage for a potential landmark ruling on the scope of the PREP Act and its impact on state laws protecting parental rights.
Eight Republican members of the North Carolina House of Representatives filed an amicus brief in support of the plaintiffs, urging the Supreme Court to hear the case.
The legislators, represented by attorney B. Tyler Brooks of the Thomas More Society, argued that they have a “special interest in protecting the fundamental rights of the parents they represent and for whom the General Assembly has recently enacted legislation on the very subject embraced by this appeal.”
The law in question, N.C. Gen. Stat. § 90-21.5(a1), specifically prohibits the conduct of the clinic workers in this case. It states:
“Notwithstanding any other provision of law to the contrary, a health care provider shall obtain written consent from a parent or legal guardian prior to administering any vaccine that has been granted emergency use authorization and is not yet fully approved by the United States Food and Drug Administration to an individual under 18 years of age.”
Flores said the legislators’ “expertly drafted” brief “dismantles the lower courts’ finding that PREP extinguishes applicable state law” and that its “mere filing … reaffirms my conviction that we will win in the end.”
Flores is no stranger to challenging the PREP Act’s liability shield. In May 2023, he sued the U.S. Department of Defense (DOD) on behalf of George Watts, Jr., a 24-year-old who died from myocarditis complications after receiving the Pfizer-BioNTech COVID-19 vaccine.
Flores argued the DOD engaged in willful misconduct by continuing to distribute the EUA version of the vaccine after the FDA granted full approval to Pfizer’s Comirnaty vaccine.
EUA vaccines have a lower bar for safety and effectiveness. Watts delayed taking the vaccine until after FDA approval of Comirnaty, but the DOD did not make the approved vaccine available.
This article was originally published by The Defender — Children’s Health Defense’s News & Views Website under Creative Commons license CC BY-NC-ND 4.0. Please consider subscribing to The Defender or donating to Children’s Health Defense.
May 30, 2024
Posted by aletho |
Civil Liberties | COVID-19 Vaccine, United States |
Leave a comment
Cyprus saw a “substantial, statistically significant,” increase in mortality from all causes in late 2021 and early 2022 following the rollout of the COVID-19 vaccines, TrialSite News reported last week.
Researchers from Cyprus, the University of Liverpool and Harvard University found that during the third and fourth quarters of 2021, total deaths in the island nation increased 34.1% and 11.8% respectively. During the first quarter of 2022, total deaths increased 30.7%.
Cyprus began its COVID-19 vaccine rollout in December 2020, but the peaks in monthly vaccination rates occurred in May 2021 and December 2021 and were followed by jumps in the mortality rates.
“We concluded that excess mortality occurs in unprecedented levels in Cyprus,” the researchers wrote. “Our findings raise serious concerns regarding the potential impact of the vaccination campaign and other causes on mortality.”
The authors published their findings in the Journal of Community Medicine and Public Health. Based on the association they identified, they said, “a detailed cause-specific investigation of such a significant excess number of deaths is warranted to explore the potential factors leading to this concerning and unexplained increase in population mortality.”
The researchers analyzed mortality data from 2016-2022, as reported by the Cyprus Ministry of Health to the European Statistical Office, or Eurostat. They also analyzed weekly data on COVID-19 vaccinations and related deaths collected during the pandemic by the European Center for Disease Prevention and Control.
Using that data, they determined average all-cause mortality rates and excess deaths over time, deaths reported from COVID-19 and total COVID-19 vaccines administered for Cyprus by age group.
They compared excess deaths before and during the COVID-19 pandemic and examined how those numbers related to the vaccine rollout.
Denis Rancourt, Ph.D., all-cause mortality researcher and former physics professor at the University of Ottawa in Canada who was not involved in the study, told The Defender :
“There’s clearly a temporal association here between vaccines and excess all-cause mortality. This association is robust, it’s unambiguous, it’s clear, it’s in the data itself.”
Rancourt’s team of scientists at the Canada-based Correlation Research in the Public Interest has also conducted several studies that found strong associations between vaccine rollouts and excess mortality.
He said the mortality rates and the association with the vaccine reported in the Cyprus study are similar to what his team found in their own analysis of Cyprus, which is part of a larger study not yet published.
However, to confirm what caused the deaths, Rancourt said, “You have to dig deeper as the authors correctly point out to find out what is really going on here,” Rancourt added.
Data on excess deaths in Cyprus
Epidemiologists use all-cause mortality — a measure of the total number of deaths from all causes in a given time frame for a given population — as the most reliable data for detecting and characterizing events causing death and evaluating the population-level effect of deaths from any cause.
Excess death, or excess mortality, refers to the number of deaths from all causes during a crisis above and beyond what would be expected under ‘normal’ conditions.
Excess mortality is a “more comprehensive measure” of the impact of the COVID-19 pandemic on mortality than the confirmed COVID-19 deaths because it captures deaths from other causes, like vaccines, treatment protocols or other factors that are attributable to the “overall COVID-19 crisis,” the authors wrote.
“COVID-19 death data is notoriously not reliable,” Rancourt agreed.
Research also shows that the trends identified in Cyprus are consistent with broader regional and global trends, the authors said. Across the EU, the authors wrote, excess deaths increased in 2020 and continued through 2023, albeit at variable rates.
Cyprus, they noted, was one of the EU member states with the highest excess mortality — in 2022 it had the highest excess mortality rate in Europe, reaching 26.4%.
This was consistent with findings worldwide. For example, a study found the U.S. experienced substantial excess mortality during the pandemic. And the authors’ previously published research showed a substantial increase in mortality in Cyprus in 2021 compared to 2020, even when excluding deaths reported to be caused by COVID-19.
For their current study, the authors calculated the average all-cause mortality using pre-pandemic data from 2016-2019 and assessed how mortality deviated from that level. Before 2020, they found very little excess mortality.
They presented their findings in a series of tables and graphs.
They found two peaks in vaccination across Cyprus’s population of 904,705 people. In May 2021, when the first peak happened, 42% of the population was vaccinated. In December 2021 at the second peak, 71% of the population was vaccinated. They found that after each vaccination peak, there was a higher rate of excess deaths, which was more severe after the second peak.
They also noted that excess deaths remained low during the period between the start of the COVID-19 pandemic in Cyprus and the start of the vaccination campaign, only beginning to climb substantially after the vaccine was introduced.
Overall there were approximately 3,000 excess deaths in 2021-2022.
High mortality rate in summer ‘unheard of’
Rancourt said there were a few interesting things in the data that the authors didn’t highlight. Cyprus typically has higher mortality in the winter and low in the summer, he said.
“It’s unheard of to have a high mortality in the summer. But in 2021, just after the main first wave of vaccination rollout, after a large number of vaccine doses had been given, there was a very large summer peak in excess mortality.”
Then, there was another peak in the spring and summer following the winter 2022 vaccine push.
In their study, the researchers again found that when they excluded the reported number of deaths from COVID-19, the increase in all-cause mortality persisted. This finding is also consistent with other studies, the authors reported.
The authors said their study was limited by their inability to explore what caused the documented excess mortality. They blamed a lack of access to detailed death certificates, which haven’t been made available to researchers.
“We call for official authorities to share information on diagnoses and causes of death from corresponding death certificates in order to further explore the underlying causes of these troublesome increased mortality findings,” they wrote.
They did note several issues identified in the existing literature that provide hypotheses about the causes of the rise in all-cause mortality and highlight “the concerns that the vaccination campaign may have contributed to this worldwide observed excess mortality.”
Many researchers have identified links between the toxicity of vaccine batches and adverse events, they noted. Rancourt and his team have linked the vaccine rollouts to unprecedented peaks in all-cause mortality in a study of 17 countries.
Rancourt said they are currently completing a study of 125 countries, including Cyprus, and their analysis of that country produced similar results to the current study.
The study authors also noted that during the pandemic, pressures on the healthcare system undermined access to and quality of care, increasing mortality. They also noted that lockdowns had documented serious health effects including increased mortality.
Rancourt said his work demonstrated that there may be multiple causes of all-cause mortality from different pandemic-response-related practices, including vaccination and the application of different COVID-19 treatment protocols or the psychological stress of lockdowns and isolation.
However, frail, elderly and otherwise sick people were consistently most vulnerable to death.
This article was originally published by The Defender — Children’s Health Defense’s News & Views Website under Creative Commons license CC BY-NC-ND 4.0. Please consider subscribing to The Defender or donating to Children’s Health Defense.
May 29, 2024
Posted by aletho |
Science and Pseudo-Science, Timeless or most popular | COVID-19 Vaccine, Cyprus |
Leave a comment
During Intense Vaccine Campaign Population Declined but Cardiac Arrests Skyrocketed
We previously brought you news from King County, Seattle Washington about cardiac arrests from the elite MEDIC ONE EMS system which has the most accurate data in the country. It also happens to be one of the most heavily vaccinated metro areas in America.
Hulscher et al from the McCullough Foundation led a team of investigators that relied on the annual data reports and integrated them with COVID-19 vaccination and population statistics. This is an ecological analysis without individual case record data, so only broad population level inferences can be made.
“Approximately 98% of the King County population received at least one dose of a COVID-19 vaccine by 2023. Our analysis revealed a 25.7% increase in total cardiopulmonary arrests and a 25.4% increase in cardiopulmonary arrest mortality from 2020 to 2023 in King County, WA. Excess cardiopulmonary arrest deaths were estimated to have increased by 1,236% from 2020 to 2023, rising from 11 excess deaths (95% CI: -12, 34) in 2020 to 147 excess deaths (95% CI: 123, 170) in 2023. A quadratic increase in excess cardiopulmonary arrest mortality was observed with higher COVID-19 vaccination rates. The general population of King County sharply declined by 0.94% (21,300) in 2021, deviating from the expected population size. Applying our model from these data to the entire United States yielded 49,240 excess fatal cardiopulmonary arrests from 2021-2023.”
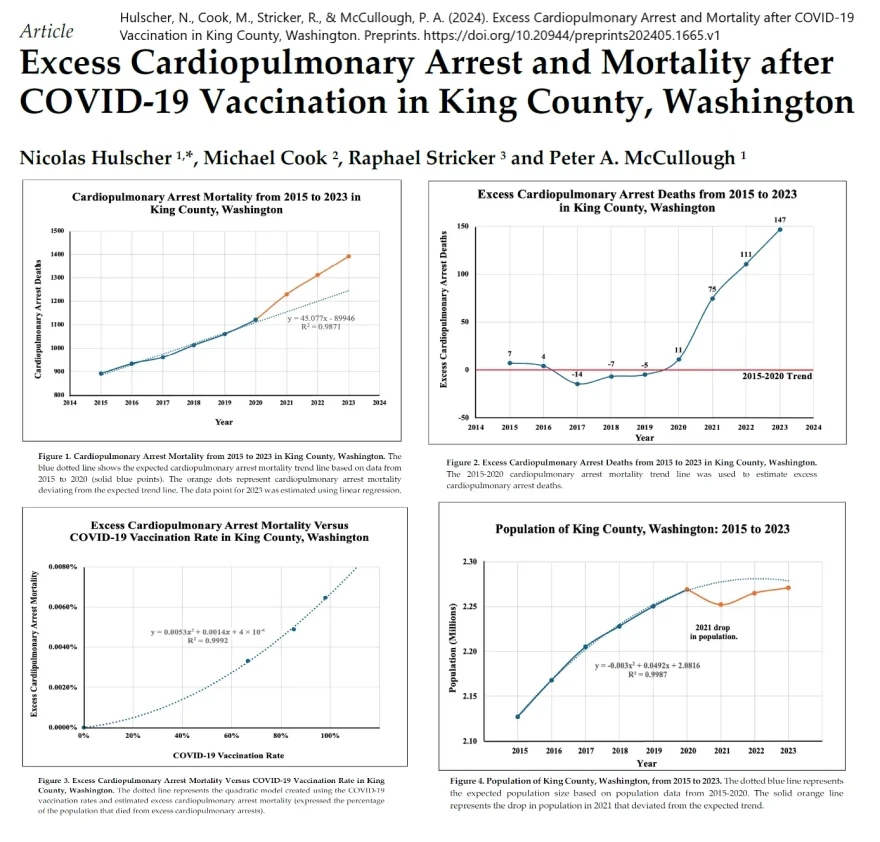
Hulscher, N., Cook, M., Stricker, R., & McCullough, P. A. (2024). Excess Cardiopulmonary Arrest and Mortality after COVID-19 Vaccination in King County, Washington. Preprints. https://doi.org/10.20944/preprints202405.1665.v1
These data are extremely worrisome given the rise in all-cause mortality observed in the United States that has been thoroughly investigated and reported by analyst Edward Dowd in his book “Cause Unknown”: The Epidemic of Sudden Deaths in 2021 & 2022 & 2023. Hulscher and colleagues found despite a pandemic decline in county population, both cardiac arrest events and fatal outcomes increased with vaccination. These findings among many others strongly support removal of all COVID-19 vaccines from public use and immediate clinical and research programs to stem the tide of vaccine cardiac arrests as they occur over the years after injection.
Peter A. McCullough, MD, MPH
President, McCullough Foundation
www.mcculloughfnd.org
Hulscher, N., Cook, M., Stricker, R., & McCullough, P. A. (2024). Excess Cardiopulmonary Arrest and Mortality after COVID-19 Vaccination in King County, Washington. Preprints. https://doi.org/10.20944/preprints202405.1665.v1
May 29, 2024
Posted by aletho |
Science and Pseudo-Science | COVID-19 Vaccine, United States |
Leave a comment

