CPSO Pronounces Judgment Over Dr Trozzi
But the shots are still toxic, Pfizer committed fraud, everyone has been assaulted, and we must act now to save lives.
Dr Mark Trozzi | November 6, 2023
Health Canada recognizes that Pfizer committed fraud. The shots turn out to be even worse than I thought. They contain large quantities of DNA, and multiple genetic sequences including a very dangerous SV40 promoter sequence which promotes permanent genetic modification, disease, and cancer. Sadly, innocent people are uninformed and lining up for injections that they would never agree to if they knew what was in them and what it can do to them.
Here is my ten minute video to update you, with a focus on current priorities and strategies. Crisis is a combination of danger and opportunity. The SV40 revelation marks severe danger, but it is also an opportunity to finally set things right. This video includes genuinely kind and honest advice for the CPSO administrators and staff; and a small request for you to please share your judgement of me as a doctor with the CPSO.
Please Share Your Judgment of Dr Trozzi with the CPSO here:
- CPSO Compliment a physician https://www.cpso.on.ca/en/Public/Public-Information/Compliment-a-physician
- or by email direct to feedback@cpso.on.ca

CPSO v. Trozzi – Case Update – November 1, 2023
COLLEGE DENIES DR. TROZZI’S RIGHT TO FREEDOM OF EXPRESSION
We are the Administrative State and You are Not
The Ontario Physicians and Surgeons Discipline Tribunal has ruled that Dr. Mark Trozzi is guilty of professional misconduct and dishonourable conduct and is incompetent in the practice of medicine for questioning the government’s Covid-19 narrative. He was also found guilty of professional misconduct and was deemed incompetent for writing medical exemptions for Covid-19 injections in support of a patient’s right to refuse coerced medical treatment under Ontario’s Health Care Consent Act and section 7 of the Canadian Charter of Rights and Freedoms.
In 2021, the College of Physicians and Surgeons of Ontario established three Covid-19 restrictions through website statements — doctors were forbidden from: (i) making any statements that discourage anyone from following Covid-19 public policies and recommendations; (ii) prescribing alternative Health Canada approved medications for the treatment of Covid-19; and (iii) writing medical exemptions for Covid-19 injections, unless a patient had suffered a severe allergic reaction or developed myocarditis after a first shot. Based on the restrictions relating to freedom of expression and medical exemptions, the College issued investigation orders against Dr. Trozzi in 2021.
This eventually led to a five-day hearing in July of 2023 during which the College Tribunal focused its prosecution on Dr. Trozzi’s daily newsletter at drtrozzi.org, where he had supposedly caused harm by spreading “misinformation” about Covid-19 science. The College was particularly concerned with Dr. Trozzi’s view that neither Big Pharma nor Health Canada had done the due diligence required to prove the Covid-19 injections were safe and effective. The Tribunal concluded that his views were inflammatory, unprofessional and worthy of censure. On November 10th, the Tribunal will hold a penalty hearing to determine whether to revoke the licence of the 25-year ER veteran and former university professor.
Trozzi’s lawyer, Michael Alexander, commented: “The Tribunal wrote up the prosecution’s position on almost every issue. The one saving grace was the College’s acknowledgement that the right to free expression includes the right to make statements that may be wrong or mistaken. However, that position is difficult to reconcile with the Tribunal’s view that Dr. Trozzi can be punished for spreading misinformation.“
He added: “The Tribunal did not address our argument that the College lacked the authority to investigate and prosecute Dr. Trozzi since its Covid-19 restrictions were merely recommendations rather than binding rules or regulations, even though we cited the Ontario Divisional Court and the Ontario Court of Appeal in support of our position.”
Further, he stated: “The Tribunal totally ignored our cross-examination of the College’s expert witnesses, which makes the entire decision a complete travesty. On cross, the College’s main expert witness on Covid science, Dr. Andrew Gardam, admitted that he had never responded to the 41-page expert report provided by Dr. Trozzi in which he rebutted Gardam’s own 8-page expert report with 29 scientific citations. As a result, in closing submissions, we argued that Dr. Trozzi was unrefuted on Covid science; yet, the Tribunal made no mention of this fact.”
Finally, he added: “The Tribunal also paid no attention to the fact that the Supreme Court recognized an expansive right to freedom of expression as an inherent feature of parliamentary government as early as 1939, which gives the right a higher status than it enjoys under the Charter. In matters of law, we will appeal the decision to the Divisional Court on the standard of correctness.”
For media inquiries, please contact Michael Alexander by cell at 416-318-4512 and by e-mail at malexanderjd@protonmail.com.
Please support the fight to restore ethical medicine and the rule of law in Ontario and Canada.
Please sign this petition to defend my license to practice medicine in Ontario and ultimately restore Canadians’ access to many honest doctors who have been persecuted for resisting the unethical and unscientific covid agenda.
Reports about Dr Trozzi and the CPSO from others:
- Life site News: Dr. Mark Trozzi may lose medical license for defying COVID narrative
- Epoch Times Tribunal Finds Ontario Doctor Critical of COVID Measures Committed Professional Misconduct
- Derek Sloan Funding the Fight: Dr. Trozzi Latest Update – May Lose Licence Next Week
- Denis Rancourt, “In Canada, Dr Mark Trozzi has opposed the toxic death-causing vaccine in every way he can, so the CPSO @cpso has decided that he is incompetent! ( And “disgraceful, dishonourable or unprofessional”)”
Here’s a history to be proud of, and “accused” of:
- To follow Dr Trozzi’s public covid truth mission beginning January 2021 and right up until the present start here
- Or to begin with the most recent and work your way back start here
DNA Contamination/ SV40 promoter sequence/ Pfizer’s Fraud/ Health Canada
- Dr Trozzi Alert | There’s DNA in the RNA Shots. Lots! April 2023
- World Council For Health Urgent Panel of Global Experts Confirm Dangerous Criminal Undeclared DNA In Pfizer And Moderna Covid-19 “Vaccines”
- Epoch Times regarding plasmid DNA contamination and Health Canada
Cancer:
Canadian doctor sounds alarm over ‘turbo cancers’ in young people due to COVID jabs. ‘I’ve never seen anything like this,’ said Dr. William Makis regarding ‘stage four’ cancers presenting in young people and uncharacteristically aggressive leukemias.
Insurance Industry Execs ‘Alarmed’ by Surge in Deaths Among Young People — But Stop Short of Blaming COVID Shots
By Mike Capuzzo | The Defender | November 6, 2023
Executives at the largest insurance companies in the United States are alarmed that teenagers, young and white-collar Americans in the prime of life are inexplicably dying at a record pace, causing a “monumental outflow” of death claims and drag on profits that is shaking the industry and causing some to take a fresh look at the problem.
According to an Oct. 26 report in InsuranceNewsNet, U.S. insurance companies expected higher-than-normal payouts from excess deaths during the COVID-19 pandemic.
Insurers saw death benefits rise 15.4% in 2020, the biggest one-year increase since the 1918 Spanish flu epidemic, followed by a record $100.28 billion — nearly double the historic norm — in total death benefits paid out by the industry in 2021.
“The numbers were naturally forecasted to climb during the pandemic, but some industry and health authorities are concerned the rates haven’t greatly diminished as COVID infection rates have declined,” InsuranceNewsNet reported.
According to InsuranceNewsNet, insurers are especially concerned by data from the Centers for Disease Control and Prevention (CDC) that show “mortality rates alarmingly rising for different categories,” including younger adult mortality rates that are up more than 20% above historic norms in 2023.
The CDC numbers reported in August show the death rate for Americans ages 15-45 rose 20-24% above normal in 2020, and soared in 2021, to a nearly 30% death increase for 15-year-olds and a more than 45% increase for 45-year-olds.
Surge in excess deaths ‘caught carriers off guard’
Most troubling to insurers, CDC data reported in August showed that Americans in the period January-May 2023 were still dying at abnormally high rates with the pandemic long over. Mortality rates were 25% higher than normal among 15- to 19-year-olds and 20% higher among 45-year-olds considered in the prime of life.
Even twenty-somethings were dying at a rate nearly 15% above normal and thirty-somethings at a pace 20% higher than usual, the CDC data show.
Samantha Chow, global leader for Life, Annuity and Benefits Sector at Capgemini, a large, multinational Paris-based consulting company, told InsuranceNewsNet, “The surge in excess deaths caught carriers off guard” and the issue demands urgent attention by the industry.
The issue is, “Can the industry handle a sudden spike in claims?” She added, “The real concern for life insurers lies in preparing for an unexpected wave of death claims and the impact on their assets under management.”
“Do they have enough reserves to weather these outflows, given the excess deaths? It’s not just about death or health,” Chow said. “It is about the industry’s ability and readiness to manage this monumental outflow.”
The excess deaths and the record drag on insurance company revenue and the predictive chaos in actuarial tables they represent, alarmed the Society of Actuaries (SOA), the world’s largest professional actuarial organization.
Excess mortality is defined as excess deaths in a given population and time period above the expected number.
The SOA has conducted ongoing research since 2021 to gather “a high-level view of U.S. Group Term Life Insurance mortality results during the COVID-19 pandemic” compared to prior baseline results.
The SOA Research Institute studied more than 2.7 million claims and over $120 billion in earned premiums reported by “20 of the top 21 U.S. group term life insurers” in the U.S., representing approximately 90% of the employer-based group term life insurance industry.
In an August 2022 poll among its more than 30,000 members worldwide, the SOA found that 85% of members thought excess mortality rates would continue to 2025. In August this year, the same poll found 79% believed excess mortality rates will continue through 2026.
Life insurance executives and actuaries told InsuranceNewsNet, “The numbers are alarming and could continue to drag earnings and surge death claims for years to come.”
Society of Actuaries: no connection between historic death rates and COVID shots
Yet in its latest report issued in May, the SOA Research Institute found no connection between the historic U.S. death rates and insurance payouts starting in 2021 and COVID-19 vaccine mandates that rolled out the same year.
Chow blamed the excess deaths and claims on “the ripples of COVID-19 and its varying impacts, leading to higher rates of depression, suicide, and increased substance abuse.”
Other insurance executives told The Wall Street Journal they blamed “delays in medical care as a result of lockdowns in 2020, and then, later, people’s fears of seeking out treatment and trouble lining up appointments” for a surprising surge in non-COVID-19 death claims, especially heart and circulatory issues and neurological disorders.
But Dr. Pierre Kory, president and chief medical officer of the Front Line COVID-19 Critical Care Alliance (FLCCC), who treats long COVID and vaccine-injured patients in his practice, called on insurance companies to work with media and governments and investigate the powerful evidence that countless deaths and disabilities are temporally linked to the COVID-19 mRNA vaccines and read the exploding science that pinpoints mRNA technology lethality.
In an interview with The Defender, Kory cited the more than 1 million COVID-19 vaccine-linked injuries, disabilities and more than 30,000 deaths reported by doctors, nurses and others to the Vaccine Adverse Event Reporting System (VAERS).
VAERS, run by the CDC and U.S. Food and Drug Administration, is the government’s “early warning system” to detect vaccine harms.
Dr. Peter McCullough, one of the most highly published cardiologists in the world, pointed to a study of deaths after vaccination with detailed autopsies in Heidelberg, Germany. “Of 35 fatalities within 20 days of injection, 10 were ruled out as clearly not due to the vaccine (eg drug overdose). The remaining 25 (71%) had final diagnoses consistent with a vaccine injury syndrome including myocardial infarction, worsening heart failure, vascular aneurysm, pulmonary embolism, fatal stroke, and vaccine-induced thrombotic thrombocytopenia,” McCullough wrote.
He also cited his own systematic review of “all autopsy studies that include COVID-19 vaccine-induced myocarditis as a possible cause of death” that found that “all 28 deaths were causally linked to COVID-19 vaccination by independent adjudication.”
Kory said a large and expanding volume of scientific literature has described the pathogenicity of the artificial spike protein, unleashed by the mRNA injection into the body.
“We know from research on autopsy series that among those who died from the vaccine, spike protein was disseminated to all organs and vessels of the body,” he told The Defender.
“Spike-induced damage occurs by numerous mechanisms, including necrosis of vessel walls leading to things like aortic dissection, inflammation of important organs, including the heart and brain causing myocarditis and cognitive deficits respectively,” Kory said.
He also also cited “fibrinoid aggregates circulating in the blood causing poor perfusion in the microcirculation as well as hypercoagulability in the blood causing strokes and heart attacks, immunosuppression causing increased risk of infectious illnesses, and/or reactivation of latent viruses.”
Edward Dowd, the former BlackRock fund manager who oversaw $14 billion in assets on Wall Street for the largest asset manager in the world, exposed the excess-death crisis in insurance-industry data in his December 2022 book, “‘Cause Unknown’: The Epidemic of Sudden Deaths in 2021 and 2022.”
Dowd told The Defender that according to insiders at one of the biggest insurance companies in the U.S., “People in the industry know what’s going on but nobody at the top” is yet prepared to recognize it. “The CEOs and CFOs don’t believe it’s the vaccine. It’s not that these people are evil. They’re not separating facts from emotion.”
Dowd added:
“It’s not just that there’s a vast conspiracy. There was this fear that generated a destruction of critical thinking. My ethics professor at Indiana University said you can’t rationalize facts with someone whose position is based on emotion and ego.”
‘We don’t have proof’ yet — but data are ‘persuasive’
In his book, Dowd reported on insurance industry research in 2016, which found that group life policyholders, whose health insurance is covered by Fortune 500 companies and tend to be younger and well-educated, were the healthiest Americans, dying at one-third the rate of the general U.S. population. The trend of greater white-collar health continued through 2020.
But in 2021, after the COVID-19 jabs were mandated across the Fortune 500, the trend flipped. Ages 25-64 of the group life policyholders suddenly experienced 40% excess mortality, compared to 32% in the general population.
Disabilities also soared after the COVID-19 shots, from an annual U.S. baseline of 29-30 million disabled to 33.2 million.
Dowd, who continues to research excess deaths and disabilities for his Humanity Projects, told The Defender his new research, drawn from U.K. government statistics, shows deaths of schoolchildren went down in the U.K. in 2020 during the pandemic because the leading cause of death for children ages 1-14 is accidents.
With lockdowns and school closures, “Deaths went down. But then they started to go up again in 2021, and they’ve reached a new high in 2023 of 20%” above normal, he said.
Dowd told Russel Brand that such a huge jump in childhood deaths is “a six-standard deviation from the norm. A standard deviation is basically a probability from normal. It’s very unlikely.”
A five-standard statistical deviation is so remarkably far outside the norm it “would be the equivalent of a 7-foot giant being born, or many of them,” he said. “This is a six-standard deviation.”
Down said he believes the COVID-19 vaccines are causing widespread, otherwise inexplicable, excess deaths. “We don’t have proof. It’s our thesis,” he said. But “if you have a brain in your head,” the data are persuasive, he said. “Obviously I think it’s the vaccines.”
Mathew Crawford, a Texas-based statistician and finance specialist who spent years analyzing COVID-19 data for his Substack newsletter, told The Defender the insurance industry has been in denial over growing evidence for vaccine-induced excess deaths for more than a year.
In March 2022, he said, the CEO of German health insurance giant BKK ProVita presented evidence that the vaccines had already killed tens of thousands of Germans. He was fired the next day, as the story vanished from the news.
In June 2022, Lincoln National reported a 163% increase in death benefits paid out under its group life insurance policies in 2021.
In August 2022, Reinsurance Group of America’s (RGA’s) financial reports showed massive 2021 losses downplayed by the report authors, “plus plans for new accounting methods that we should all be worried are designed to sweep iatrogenocide under the rug,” Crawford said.
The SOA Research Institute report that claims to exonerate the COVID-19 vaccines in excess deaths actually does the opposite, Crawford said. Among other evidence, he said, it “shows group life insureds — particularly of working age — are seeing even more excess mortality than the larger U.S. population,” and “the sharp numbers during Q3 2021 coincide with vaccine mandates for working age individuals.”
The ‘worm is turning’
But Dowd said he believes “the worm is turning” on denial of vaccine harms.
He said he was optimistic that the work of Josh Stirling, founder of the Insurance Collaboration to Save Lives, a nonprofit that aims to reduce mortality by providing life insurers with tests to screen policyholders for health problems, shows a “big tent” is forming in the industry to tackle the problem.
“I think the truth is coming out,” Dowd said. “The stocks of Pfizer and Moderna continue to go lower. More and more people are getting disabled and injured over time.”
He cited the Rasmussen poll released Nov. 2 that found 24% of Americans “believe someone they know died from COVID-19 vaccine side effects, and even more say they might be willing to become plaintiffs in a class-action lawsuit against vaccine makers.”
The poll also found “There are almost no political differences on these questions,” said Dr. Robert Malone. “For example, 25% of Republicans say they know someone personally who died from side effects of COVID-19 vaccine, as do 24% of Democrats and those not affiliated with either major party. This is important – because this shows it is not a ‘tribal’ response. People from all walks of life are waking up.”
Kory said insurance executives need to ask themselves, What explains “the sudden, unprecedented rise in life insurance claims in the 3rd quarter of 2021 among the healthiest sector of society?”
Why were “working age, white collar Americans with group life insurance policies (i.e. largely Fortune 500 corporate employees)” suddenly dying at rates significantly higher than before?
“What happened in the white-collar workplace at that time?” he asked.
Kory said the answer is clear:
“I will give you the only possibilities that could explain such a sudden rise: a series of terrorist attacks, wartime mobilization, or the proliferation of corporate vaccine mandates. As far as I can remember, only one of those events actually took place.”
Kory and investigative reporter Mary Beth Pfeiffer in October published an op-ed in The Washington Examiner, “What’s behind the spike in deaths among younger, working people?” and another, in August, in USA Today titled, “More young Americans are dying — and it’s not COVID. Why aren’t we searching for answers?”
“Deaths among young Americans documented in employee life insurance claims should alone set off alarms,” they wrote in USA Today. “Week in, week out, this unnatural loss of life is on the scale of a war or terrorist event.”
“Life insurance data show a massive spike in excess deaths among younger, working-age people that began in 2021, even as COVID-19 deaths decreased, and continues today,” they wrote in The Examiner. “So far, good explanations are elusive. A concerted, bipartisan investigation should explore this threat to America’s economic future and recommend a course of action.
5 takeaways from mortality report
If the worm is turning, it’s not evident in major media or government policy.
Associated Press fact-checkers rated as “false” Kory’s claim that “an increase in death benefits paid out by life insurance providers in the third quarter of 2021 in the U.S. provides evidence that the COVID-19 vaccines, which became widely available in 2021, led to a spike in deaths.”
The AP said the vaccines are proven safe and effective and “insurance industry leaders say the delta variant of the coronavirus and deferred medical care during the pandemic likely contributed to the increase in deaths.”
The CDC says there is no evidence that excess deaths are linked to vaccines. “These vaccines are safe and effective and have undergone the most extensive safety monitoring in U.S. history,” a CDC public affairs specialist said.
The AP reported that death after vaccination remains extremely rare, dismissing as not causally linked to the vaccines the unprecedented toll of deaths and injuries reported to VAERS.
Kory cited five takeaways that challenge that assumption from the mortality report on excess U.S. deaths by the SOA Research Institute:
- Among working people 35-44 years old, “a stunning 34% more died than expected in the last quarter of 2022, with above-average rates in other working-age groups, too,” Kory said, quoting data from the SOA Research Institute report. “COVID-19 claims do not fully explain the increase,” the SOA report noted.
- From 2020 through 2022, there were more excess deaths proportionally among white-collar than blue-collar workers: 19% versus 14% above normal. The disparity nearly doubled in the fourth quarter of 2022, U.S. actuaries reported.
- The executive of a large Indiana life insurance company was clearly troubled by what he said was a 40% increase in the third quarter of 2021 in those ages 18-64. “We are seeing, right now, the highest death rates we have seen in the history of this business — not just at OneAmerica,” CEO Scott Davison said during an online news conference in January 2022. “The data is consistent across every player in that business.”
- Excess deaths are a global phenomenon. The U.K. also saw “more excess deaths in the second half of 2022 than in the second half of any year since 2010,” according to the Institute and Faculty of Actuaries. In the first quarter of 2023, deaths among people 20-44 years old were akin to “the same period in 2021, the worst pandemic year for that age group, U.K. actuaries reported. In Australia, 12% more people died than expected in 2022, according to that nation’s Actuaries Institute. A third of the excess was non-COVID deaths, a figure the institute called “extraordinarily high.”
- Death rates are lower than in 2020 and 2021, but they are far from normal. In the year ending April 30, 2023 — 14 months after the last of several pandemic waves in the U.S. — at least 104,000 more Americans died than expected, according to Our World in Data. In that period, 52,427 excess deaths were reported in the U.K., 81,028 in Germany, 17,731 in France, 10,418 in the Netherlands, and 2,640 in Ireland.
Kory said the major media silence on the issue and the SOA’s “strong desire to not be drawn into any debates regarding” COVID vaccine lethality,” despite evidence unearthed by the society’s research, is why he and Pfeiffer wrote the USA Today op-ed in the first place.
“Unsurprisingly,” Kory said, “the SOA does not attempt to interpret or even specifically mention the timing, suddenness, and magnitude of the rises in death claims of young, white-collar workers.”
“I would agree that it is not their job to do this, so the rest of us will,” he said. The way forward is “simply to ask if there were any other events preceding and during those massive spikes that could explain the rises. I can find no other rational explanation than the roll-out of vaccine mandates as the cause.”
Mike Capuzzo is the managing editor of The Defender. He is a former prize-winning reporter for The Philadelphia Inquirer and The Miami Herald, a science writer, and a regional magazine founding editor and publisher who has won more than 200 journalism awards as a writer, editor and publisher.
This article was originally published by The Defender — Children’s Health Defense’s News & Views Website under Creative Commons license CC BY-NC-ND 4.0. Please consider subscribing to The Defender or donating to Children’s Health Defense.
An explosive discussion with ex-CDC scientist Norman Pieniazek
BY MARTIN NEIL, JONATHAN ENGLER, AND JESSICA HOCKETT | OCTOBER 30, 2023
Dr Norman Pieniazek is a molecular biologist, geneticist, epidemiologist with 147 publications in virology and parasitology. Before he retired, he spent 24 years working at the Center for Disease Control (CDC) in the USA. He has also spent time abroad including time working in Spain and Poland.
We met up with Norman for what was planned to be a short meeting to introduce ourselves and informally discuss common interests around covid. However, this turned into a two-hour long, wide-ranging and fascinating discussion that touched on a huge number of topics.
Early on in the meeting Norman made the wise suggestion that we record and share the discussion. So, he hit the record button on Skype and we started again. The video, accessible below, is approximately two hours long. Be aware that, given it wasn’t planned as an ‘interview’ or for broadcast, it is largely unstructured. However, for those short of time here is a synopsis of the discussion with a focus on what Norman said1:
- The bacterial pneumonia hypothesis suggests that early treatment – hydroxychloroquine, ivermectin and antibiotics address bacterial infection. Norman confirmed bacteria are everywhere in our bodies including in the lungs, creating an ever-present potentially hazardous predisposition that, given the right circumstances, might cause a deadly bacterial pneumonia infection.
- Well-understood remedies such as the stockpile of antibiotics, as recommended by Fauci, were cast aside in 2020. Bacterial infection can cause sepsis hence we need antibiotics. A Cytokine storm is caused by bacterial infection in the lungs, filling them with fluid; this lowers the oxygen level in the blood because of poor lung function.
- In-person diagnosis by a physician based on physical symptoms was largely replaced by the PCR test, and with the rise in tele-health visits, social distancing etc physicians stopped using stethoscopes to listen to a patient’s chest. This is an essential diagnostic tool to enable a doctor to audibly tell whether a patient has crossed the line into a bacterial infection which will then require antibiotics.
- Norman knew Donald Henderson who co-authored a classic work on how to best respond to a flu epidemic. Henderson and colleagues did not recommend any of the NPIs that were followed during covid because of the obvious severe health, social and economic costs. (As an aside this work was co-authored by Prof. Thomas Inglesby at John Hopkins who attended Event 201 and, oddly, recommended NPIs be used for covid – the very same ones he had rejected previously).
- Orthodox immunology was ignored – herd immunity is a fiction given there is a ‘soup’ of constantly mutating coronaviruses.
- Why didn’t scientists at the CDC question things early in 2020? Work from home restrictions meant that people at CDC couldn’t communicate and coordinate to overturn the madness being imposed from the ‘sixth floor’ top brass. You could not isolate CDC from the HHS (Health and Human Services) and it was HHS that were calling the shots.
- The Wuhan scientists were on a routine ‘fishing expedition’ for coronaviruses and unusual pneumonias. Why was this work being done in Wuhan? It is easier to do in China because it is legal and because there are lots of hospitals, in a concentrated area, where the population is in relatively poor health. Also, it is easier to get permission to perform a painful bronchial lavage procedure on patients to obtain pathogens in China; this is much harder to do in the USA. This procedure is done in the lower respiratory tract and guarantees higher quality samples than can be obtained using swabs, which really just measure the quality of the air that has entered your upper respiratory tract.
- To determine what pathogen is causing lower respiratory tract symptoms you should not use swabs and PCR. Why not? CDC acknowledges the inability of swabs to collect causative agents as reported by the EPIC study in these 2015 NEJM articles (one done on adults and one on children). Hence a positive result gained from a sample taken from the upper throat or the nose does not mean an infection is caused by the detected pathogen.


- In 2002-2004 SARS-COV was not subject to mass PCR testing, yet SARS-COV-2 was. PCR was used for SARS-COV but only on samples taken using bronchial lavage, but NOT from swab samples taken from the nose or upper throat.2
- Wu et al discovered WH-Human-1 using samples collected by bronchial lavage, and next generation sequencing of the collected genetic samples, and ultimately reported it in GenBank.
- Before reporting on GenBank they published a preprint identifying the genetic sequences3, which was appropriated and found its way into the hands of Corman and Drosten, who then decided to exploit it for personal gain (via commercial PCR testing), fabricating a story about validating it against SARS-1. It was subsequently renamed SARS-COV-2. (For a proposed timeline of events see here).
- Norman thinks SARS-COV-2 is simply a beta coronavirus (a cold), one of the many thousands of cold viruses that had remained undiscovered until 2020, but which have always been ever present in nature.
- SARS-COV-2 cannot be a novel virus created in a lab or by natural zoonotic mutation. It is simply novel to detection4. As soon as the EUA approved PCR tests started to be used the virus was simultaneously discovered in a number of disparate geographical regions. There was no evidence of sudden spread.
- In effect the results of any test are as much determined by the choice of test to apply as by the presence/absence of viruses. Norman says, “you will find whatever you want to find”. Hence people will be symptomless yet will have a lot of, whatever viruses happen to be around in their nose or throat.
- The established taxonomy of viruses is unusable simply because there are so many unknown viruses circulating in the wild.
- The mRNA vaccine technology ended in a ‘garbage heap’, because it is extremely toxic, and was rendered obsolete by protein subunit vaccines by 2019. So, the mRNA vaccines were doomed from the start. Subunit (protein-based) vaccines have been known since the late 1970s, but Moderna, Pfizer and BioNTech needed a way to realise a return on their vast investments in mRNA. Hence the pandemic.
- Novavax is a protein subunit vaccine, based on the spike protein, which was available in August 2020 but did not get approval from the FDA. Although it is protein based it will stay in the deltoid muscle injection site. It was however approved in Canada. It may not be very good for you (and ineffective against coronaviruses), but it is less dangerous than the mRNA vaccines.
- mRNA vaccines were found to be too dangerous for animals. Also, arguments that they are a safe basis for cancer drugs are based on lies. There is a competing technology called humanised monoclonal antibodies that cured President Carter from a melanoma that had migrated to his brain and there are now 500 versions of these drugs currently available.
- Norman was told that the patent on the flu vaccines, grown in eggs, expired in 2020. Hence there was little ROI in continuing with this technology.
- Viruses are in your respiratory tract and antibodies, responding to vaccines, are in your blood. These two things do not match well because the antibodies in the blood do not get into the lungs. The immune system ‘stays away’ from the complex respiratory system that deals with the thousands of pathogens we breathe in with every breath.
- Are serology studies a pointless exercise? Because of wide variation between individual’s antibody measurement only makes sense by studying change in any single individual over time.
- Testing for antibodies means nothing because antibodies in the blood cannot travel to the lungs to react.
- Testing for antigens is a cheaper and less sensitive version of the PCR test with the same limitation.
- Norman is very sceptical of a number of covid virus theories including those by Walter Chesnut and JJCoey’s infectious clone theory, though they weren’t discussed in any great detail and were probably not characterised fully (or maybe even fairly).
- The issue with ‘infectious clones’ is that ‘you do not know what to create’ because there are millions of sequences of coronavirus so there is no ‘clonality’ and each one has 30 thousand nucleotides and there are combinatorically infinite changes you could potentially need to consider when creating a coronavirus5. It therefore isn’t possible to know what to change, via Gain of Function (GoF), to make the virus behave in more dangerous ways.
- As part of the ‘partnership for peace’ programme in 1994 Norman hired two ex-Soviet bioweapons scientists and asked them ‘how come you worked for 20 years and didn’t create any new deadly viruses?’
- They can create thousands of virus combinations, but the problem is how to test these creations. There is no way to test the billions and billions of possible changes to a virus and identify which changes to the sequence are ‘bad’. You need the phenotype, and you cannot deduce the phenotype from the genotype. So how would GoF researchers – E.g., EcoHealth alliance – know exactly what to create?
- The claim that Saddam Hussian had biological weapons was groundless and this was confirmed to Norman by Donald Henderson who was involved at the time and who said it was not possible.
- Thus, GoF claims that changes to spike protein and furin cleavage sites make a virus more deadly are fiction. It isn’t possible and there is no proof they can produce deadly bioweapons. Those advocating this position and making these claims – EcoHealth alliance (Fauci, Baric and Duszak) should get fired by their bosses for producing “not a tiger but a kitty”.
- We discussed Gulf War syndrome. Norman said people imagine anthrax is dangerous, but the ex-Soviet bioweapons researchers said to attack New York with anthrax would need 20,000 Boeing 747s flying over the city, dropping millions of tons of anthrax spores from a low height then people spreading it with shovels. The only way to infect people with anthrax is by direct means via an oxygen line or a direct injection.
- Norman said the Tokyo gas attack was successful in Japan because the terrorist used sarin, a nerve agent. The biological agents used, botulinum and anthrax, fortunately failed.
- Within the CDC Fauci was called the ‘mean midget’ and during the AIDS epidemic he sunk Robert Gallo by inventing the story that Gallo had stolen the HIV virus from Luc Montagnier, thus destroying Gallo’s chances of being awarded the Nobel prize (he was also denied a patent).
- Fauci is “not stupid, he is mean”. Fauci wanted to get a Nobel prize, but he didn’t get a Nobel prize for AIDS, so he wanted it for the Wuhan virus. In January 2023 knowing that he wasn’t going to get the Nobel prize he “pulled the plug” and published this paper saying new types of vaccines are needed for respiratory infections, as an act of spite.
We learned a lot from Norman and are very grateful to him for giving us his valuable time. You will notice that we briefly discussed the vaccines, but you will be very pleased to hear that Norman has agreed to follow up with another meeting in early December to share his thoughts on this important topic (see here for a sneak peek)
You can access Norman’s other material on YouTube and Facebook (much of his material is in Polish and Norman speaks six languages!) His twitter handle is @normanpie.
1 Note that this synopsis is not a verbatim and true transcription of the conversation.
2 This document presents evidence PCR was used to collect samples, but no mass testing was undertaken.
3 Submitted (05-JAN-2020) Department of Zoonoses, National Institute of Communicable Disease Control and Prevention, Chinese Center for Disease Control and Prevention. The first submission to GenBank had two subsequent revisions.
4 The supposed ‘novel and deadly’ attributes of the virus are discussed extensively here.
5 See this paper. “Mammals are the reservoir hosts of the majority of emerging zoonoses (2, 3, 18). If we assume that all 5,486 described mammalian species (19) harbor an average of 58 viruses in the nine families of interest (as estimated here in P. giganteus) and that these viruses exhibit 100% host specificity, the total richness of mammalian viruses awaiting discovery exceeds ~320,000.”
CHD Sues Philadelphia Over Law Allowing 11-Year-Olds to Consent to Vaccines Without Parents’ Consent
By Brenda Baletti, Ph.D. | The Defender | November 1, 2023
Children’s Health Defense (CHD) and several parents today filed a lawsuit in federal court challenging a Philadelphia law that allows minors to consent to vaccination without their parents’ knowledge, saying the legislation violates the constitutionally protected doctrine of informed consent and fundamental parental rights.
The lawsuit alleges the City of Philadelphia engaged in a “wink and a nod” practice of vaccinating children behind parents backs without informed consent for the past 15 years, under the cover of the 2007 General Minor Consent Regulation.
That rule allows children 11 and older to consent to vaccination without parental knowledge as long as they receive a “vaccine information statement” (VIS) for the administered shot.
It also absolves the vaccine administrator of liability if the minor gives consent.
On May 14, 2021, the city’s Department of Public Health also enacted an additional COVID-19 Minor Consent Regulation, allowing children ages 11 and up to consent to the COVID-19 vaccine available under Emergency Use Authorization.
Under that regulation, children could give consent if they received the U.S. Food and Drug Administration fact sheet because a COVID-19 VIS did not exist at the time.
Tricia Lindsay, attorney for the plaintiffs, told The Defender the fundamental rights of parents to direct the upbringing of their children are at stake in the case:
“The only time that a parent loses rights to their children is by a strict showing that they are not capable of taking care of their child.
“But here the government of Philadelphia is issuing a blanket statement and taking away parental rights without due process, and that is one of the greatest violations ever.
“They are using emergency powers and the excuse of concerns over ‘health and safety’ to justify it. But it’s camouflage. It’s a Trojan horse. They are using these buzzwords to justify their tyranny … which is what you call it when you remove a person’s fundamental rights without due process.”
Seven Pennsylvania parents joined CHD in suing the City of Philadelphia, its Department of Public Health and City Health Commissioner Cheryl Bettigole, M.D., MPH, alleging the regulations violate their rights.
The lawsuit, filed in the U.S. District Court for the Eastern District of Pennsylvania, said those regulations also “raise troubling issues of informed consent, freedom of religion, parental rights, and due process, implicating both the United States Constitution and the Constitution of the Commonwealth of Pennsylvania and other federal and Commonwealth laws.”
The plaintiffs are asking the court to declare Philadelphia’s 2007 and 2021 Minor Consent Regulations illegal and to stop them from being enforced.
CHD President Mary Holland told The Defender :
“It’s absurd to imagine that it is safe or desirable for 11-year-olds to make potentially life-altering medical decisions on their own without parental guidance, knowledge or consent. Philadelphia’s so-called consent policies violate state, federal and constitutional laws. I am happy that CHD is able to help put an end to these policies that actually endanger children’s health.”
National Childhood Vaccine Injury Act and VISs
Plaintiffs allege that Philadelphia’s regulations conflict with the consent requirements of the National Childhood Vaccine Injury Act of 1986 (NCVIA), the federal law that has primacy over conflicting local laws on such matters, according to the U.S. Constitution.
They also argue that the complicated requirements for seeking compensation — if someone is injured by a vaccine protected by the NCVIA — would be incomprehensible to most, if not all, children.
Under the NCVIA, vaccine manufacturers are protected from liability for a vaccine’s adverse effects if the vaccines are listed on its “Vaccine Injury Table.” The table lists covered vaccines, their recognized injuries and the timeframes within which those injuries must occur to be considered compensable.
Liability for injuries caused by vaccines listed on the table cannot be pursued in a regular court of law, but are instead compensated through the National Vaccine Injury Compensation Program (VICP).
The VICP also can provide compensation for an injury by a covered vaccine, even if the injury isn’t listed as compensable on the Vaccine Injury Table. However, the legal and administrative process is more complicated.
Even for listed injuries, it can be difficult to obtain compensation from the VICP. The backlog of cases is substantial and the proceedings are often drawn out by contentious expert battles.
The NCVIA mandates that the secretary of the U.S. Department of Health and Human Services create and publish VISs that detail the risks and potential adverse events associated with covered vaccines. Those sheets must be presented to children’s parents or legal guardians prior to vaccine administration.
The VIS is important, the complaint says, so that parents can recognize adverse events if and when they happen, and seek necessary medical treatment and also document such events in a timely manner, which is essential for seeking compensation through the VICP.
“If a parent is not aware of what their child has done,” Lindsay said, “then they don’t know what to look out for and they don’t know if the problem they are seeing is related to a vaccine.”
The NCVIA specifically mandated that VISs must be presented in a jargon-free and straightforward way that parents can understand.
The NCVIA doesn’t mention making them comprehensible to children, because the drafters of the NCVIA never imagined children would have to understand them on their own, the complaint alleges.
“The NCVIA simply does not contemplate that a child may be vaccinated without parental consent,” the complaint states. “Quite the opposite — the language of the NCVIA is clear that the VIS is provided to the parent who is able to offer informed consent on behalf of his or her child.”
But this law, the lawsuit alleges, removes parents from the equation altogether.
What about COVID vaccine injuries?
The COVID-19 vaccines are not covered by the NCVIA or the VICP.
Instead, under the Public Readiness and Emergency Preparedness (PREP) Act, people injured by a COVID-19 vaccine or “countermeasure” can seek compensation only under the Countermeasures Injury Compensation Program (CICP).
Since 2010, when the CICP approved its first claim, the program has compensated a total of 36 claims for vaccine injuries — six of those awards were for COVID-19 vaccine-related injuries.
The complaint also noted that COVID-19 vaccines available for 11-year-olds are still investigational. “Children are not capable of understanding the risks associated with a novel vaccine and cannot appreciate that there are no long-term studies of the safety or effectiveness of these vaccines,” the complaint states.
Lindsay said it was particularly concerning that Philadelphia specifically included the COVID-19 vaccines in the regulations and that the regulations continue to stand even though the Biden administration ended the COVID-19 public health emergency in May.
She said:
“Why would we extend this risk further to a novel vaccine, which we now know has many more problems? Why would we be signing up children to a mass experiment and taking away their guardian, the person that stands on the frontline, that’s there to protect them, to cover them, to guide them?
“It has nothing to do with the benefits of children because if it did, you would approach the guardian of that child, the person that is given the authority and has the responsibility of that child to see that that child is safe and allow them to make an informed decision as to what they deem best for their child.”
Can 11-year-old children give informed consent for medical interventions?
The complaint cites a long list of activities that are typically restricted for minors or restricted without parental consent in Pennsylvania.
For example, minors under the age of 21 cannot purchase alcohol or tobacco or enter a casino. A person must be 18 to enter into a contract or to register for the selective services without parental consent. One must be 16 to donate blood and 14 to consent to mental health treatment.
It is also illegal, the complaint notes, for pharmacists to administer vaccines to children 5 and older without parental consent.
According to the complaint:
“Philadelphia’s Minor Consent Regulations turn these requirements on their head. Rather than protecting children, Philadelphia’s Minor Consent Regulations let any child walk into a temporary vaccine ‘pop-up clinic’ or elsewhere on a whim, roll up her sleeve and receive a vaccine without her parents’ knowledge and even more importantly, her parents’ protective veil of consent. …
“The Minor Consent Regulations are a house of cards built on the unsupported, unsupportable and preposterous presumption that every Philadelphia child aged eleven and up is capable of true informed consent, that every child knows her own medical history, her family’s medical history, and can truly ascertain the potential serious risks and alleged benefits of a treatment, and can read and understand any written information — written for adults — presented to her without further explanation.”
The lawsuit alleges children likely cannot fully comprehend the VISs, let alone consent to the vaccines. Philadelphia children, it notes, have very low reading proficiency scores — only 34% of elementary students and 43% of high school students tested at or above the proficient level for reading.
It also raises concerns that no concrete proof a child-provided consent is even required.
This, the plaintiffs say, is in conflict with both the federal NCVIA and Pennsylvania law. The latter requires the written informed consent of a parent before a physician is allowed to perform medical or surgical procedures on a child.
The complaint cited the Troxel v. Granville Supreme Court case and a series of other cases that found “the interest of parents in the care, custody, and control of their children” is a constitutionally protected right.
Other minor consent lawsuits and struggles
When the pandemic began, most states had existing laws mandating parental consent for vaccination, with a few limited exceptions. But once the vaccines became available, some states and localities attempted to lower the age at which children could consent to vaccination on their own.
During Tennessee’s COVID-19 vaccination campaign, the state’s Department of Health invoked the “mature minor’ doctrine” to allow minors 14 and older to be vaccinated without a parent’s consent.
But in response to grassroots mobilization and testimony by CHD, Tennessee lawmakers in April passed a law requiring healthcare providers to obtain consent from a parent or legal guardian before vaccinating a minor.
In March 2022, CHD prevailed in a lawsuit against Washington, D.C., Mayor Muriel Bowser, the D.C. Department of Health (D.C. Health) and D.C. public schools after the U.S. District Court for the District of Columbia issued an order granting a preliminary injunction prohibiting the schools from enforcing the D.C. Minor Consent for Vaccinations Amendment Act of 2020 — a law that would have allowed children as young as 11 to be vaccinated without the knowledge or consent of their parents.
In that lawsuit, the D.C. District Court ruled in favor of CHD’s argument that the NCVIA pre-empted D.C.’s law that attempted to lower the age of consent for vaccinations to 11, and prevented the mayor of the District of Columbia, the D.C. Department of Health and D.C. public schools from enforcing the law.
The court, in that case, commented specifically on the intended function of the VIS:
“If Congress did not mean for the legal representative of a child to receive a VIS when his child receives a vaccine, then the phrase ‘the legal representatives of any child’ would be superfluous. All Congress would have needed to say is that a healthcare provider should give a VIS ‘to any individual to whom such provider intends to administer such vaccine.’ But it did not do that.”
In June, New York legislators also attempted to pass Senate Bill S762A, which would have allowed minors to be vaccinated without parental knowledge or consent. But grassroots efforts, including those undertaken by CHD, prevented that from becoming codified into New York state law.
Brenda Baletti Ph.D. is a reporter for The Defender. She wrote and taught about capitalism and politics for 10 years in the writing program at Duke University. She holds a Ph.D. in human geography from the University of North Carolina at Chapel Hill and a master’s from the University of Texas at Austin.
This article was originally published by The Defender — Children’s Health Defense’s News & Views Website under Creative Commons license CC BY-NC-ND 4.0. Please consider subscribing to The Defender or donating to Children’s Health Defense.
“Shedding” of Covid mRNA Vaccine Components and Products From The Vaccinated to the Unvaccinated – Part 1
It’s happening. The manufacturers and regulators knew it was a risk, yet, like numerous aspects of the Covid vaccine mRNA technology, did not test for excretion potential of spike proteins or LNP’s.
Pierre Kory’s Medical Musings | November 1, 2023
Awareness of the Federal Regulators and Vaccine Manufacturers
The data showing the toxicity and lethality of the vaccines started within weeks of the roll-out with hundreds of thousands of adverse events and hundreds of deaths reported to VAERS in January of 2021, far exceeding previous stopping points of any new medical product or vaccine.
Although ignored (to this day), anyone paying unbiased attention could see a further mountain of evidence develop, including a skyrocketing number of newspaper and television reports of healthy athletes and young people arresting and dying while doing normal everyday activities or sports (countered by corporate/government controlled media with a plethora of fact checking articles using cherry picked data to inform the world that what they are seeing is not factually true).
Then life insurance industry data emerged showing historically unprecedented rises in death claims being paid out amongst the healthiest sectors of society temporally associated with the proliferation of Covid mRNA vaccine mandates within schools, corporations, universities, health care institutions, federal contractors etc. Most telling of the deathly impact of mandates was the fact that the largest increases among the sudden, rapid rises in excess deaths occurred among employed white collar workers.
The reality is that these data are still ignored by media and public health agencies across the world. Even more worrying are the more recent reports finding universal contamination of every studied vaccine vial with large magnitude, excess levels of DNA fragments and DNA plasmids. Then the discovery that the DNA plasmids used in the manufacturing process contained genetic sequences that both promote DNA integration into the human genome as well as promote the development of cancer.
It truly is unimaginable that we now must consider the risks (and reality) of “shedding” of the vaccine products from the vaccinated to the unvaccinated. This now has implications for nearly every human being walking the earth, vaccinated or unvaccinated (including me).
This series will explore the regulatory, scientific, epidemiological, and clinical data indicating that shedding is occurring. The health of who knows how many is now being threatened, with the extent of the risks likely both highly variable and difficult to predict, both in the short term and long term. That is unless we start to seriously study the phenomenon further. So, let’s review what is known.
Within 3 months of the rollout of the global Covid mRNA vaccination campaign, I was consulted by two different unvaccinated women in their late 30’s and early 40’s respectively, who reported that they were suffering acute menstrual abnormalities in the days following close exposure to a recently vaccinated practitioner (one visited a massage therapist and another an acupuncturist). Both had a history of highly regular, uncomplicated menstrual cycles over decades.
Since that time, at least twenty other unvaccinated and vaccinated people, both men and women, have reported to me compelling histories of typical post-mRNA vaccine adverse effects subsequent to close exposure to vaccinated family members, contacts, or friends.
Further, my partner Scott Marsland at our Leading Edge Clinic, who also specializes in treating Long Covid/Long Vax syndromes, has a growing series of detailed case histories of similar “shedding” events occurring. I will revisit this in a later post in this series, but I will briefly say here that our clinical observations conclude that symptomatic shedding events do occur. However, we have little idea of exactly how common it is occurring among the general population.
This is further complicated by the fact that even if it were occurring frequently, the vast majority of people suddenly developing typical vaccine side effects symptoms after exposure to a vaccinated person would never think to relate it to exposure to shed vaccine products. It is my belief that very few people in the general public are aware of the possibility it could occur. You know, because the regulators have assured the country that mRNA technology is “safe and effective.”
However, my general sense is that it occurs largely in people who have increased physiologic sensitivity to environmental exposures, toxins, or pharmaceuticals and that it is generally transmitted by someone recently vaccinated or someone who is producing a lot of spike protein. Note that is my “general sense.” More studies are required to fully understand both the frequency of and physiologic impacts from such events.
My ignorance as to the frequency of symptomatic shedding events is due to the fact that the concept of transmitting spike proteins (or lipid nanoparticles) from a Covid mRNA vaccinated person to another is one of the least studied and published-on aspect of the mRNA vaccine technology.
What is so shocking about that lack of research (actually nothing is shocking anymore) is that shedding has major global implications. Apparently it is not just me who thinks this because, as an expert on several aspects of Covid, I have been lecturing across the U.S, Europe, and South America in conferences, Parliamentary hearings, or invited lectures. Questions about shedding appear everywhere (in the dozens of Q & A’s that I have participated in, it is nearly always the first question. It is also a very common topic in the chat of our FLCCC weekly webinar.
Know that in this tonight’s FLCCC webinar, I will present a 15-20 minute overview of this series along with my private practice partner Scott Marsland. We expect to be deluged with questions after.
Anyway, I believe that by the end of this series on the science, epidemiology, and clinical observations of shedding, you will be convinced that it can and does occur.
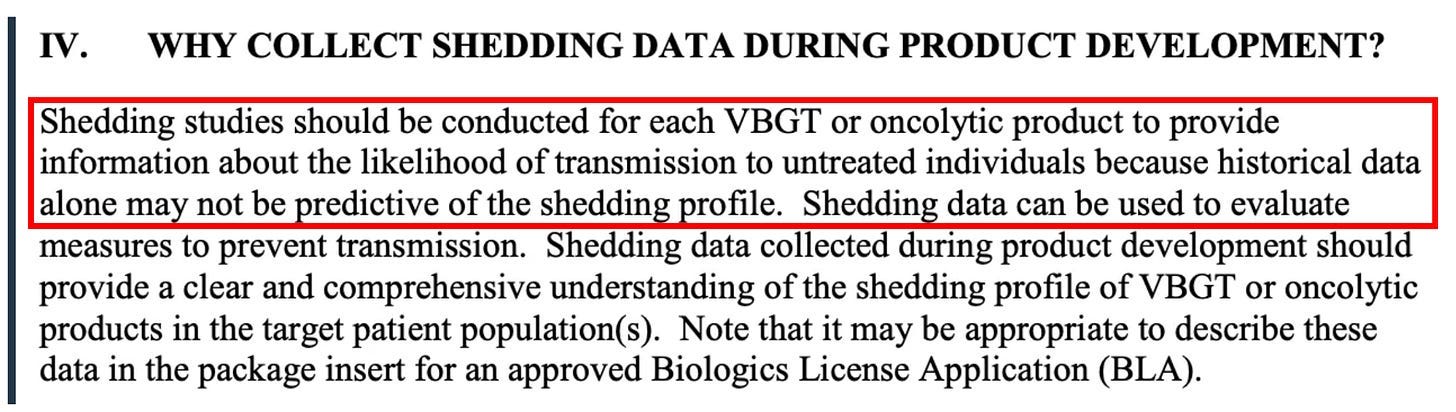
From our Federal government, in this FDA document, the term “shedding” is defined as:
“The release of viral or bacterial gene therapy products from the patient by any or all of the following routes: feces (feces); secretions (urine, saliva, nasopharyngeal fluids, etc.); or through the skin (pustules, lesions, sores).”
They forgot to mention “exhaled breath.” More on that later. The “products” they refer to that can be transmitted from a Covid vaccinated person to another include not only the genetically programmed spike protein product, but also the lipid nanoparticle (LNP) containing the mRNA that is in the injections as well as naked mRNA that can be released from the LNP. Even more worrying is the recent shocking discovery that every single Moderna and Pfizer vaccine vial is contaminated with high levels of DNA plasmids potentially capable of integrating into the human genome. Contemplating that last one is disturbing, the implications of which we will not know for some time.
First off, let’s be clear that the Covid mRNA and DNA vaccines are gene therapy medicinal products (GMTPs or GTP’s) as stated in the FDA’s 2015 document on Gene Product Shedding Studies.
“Gene therapy products are all products that mediate their effects by transcription and/or translation of transferred genetic material and/or by integrating into the host genome and that are administered as nucleic acids, viruses, or genetically engineered microorganisms.
Also note that in this European Medicines Agency (EMA) document, the mRNA vaccines also meet their definition of gene therapy medicinal products (GMTP’s).
Ok, now that we know what a gene therapy product is and that the Covid mRNA injection is actually a form of gene therapy (marketed to the public as a “vaccine”), what does that have to do with “shedding?” Again from the FDA document regarding the evaluation of the safety of gene therapy products, they emphasize the importance of studying shedding:
Shedding is distinct from biodistribution because the latter describes how a product is spread within the patient’s body from the site of administration while the former describes how it is excreted or released from the patient’s body. Shedding raises the possibility of transmission of virus or bacteria based gene therapy products (VBGT) from treated to untreated individuals (e.g., close contacts and health care professionals).
This guidance represents FDA’s current thinking on how and when shedding data should be collected for VBGT and oncolytic products during preclinical and clinical development and how shedding data can be used to assess the potential for transmission to untreated individuals.
So, with these findings in mind, it may be no wonder why the FDA insists on shedding studies:
Further on in the document, the FDA again emphasizes the importance of shedding studies:
Note that the FDA emphasizes the importance of doing human shedding studies and not just relying on animal studies:
To inform the design of human shedding studies, shedding data may be collected in animals following administration of the VBGT or oncolytic product. These data can help estimate the likelihood and potential shedding profile in humans, particularly when there is concern about transmission to untreated individuals. However, such data cannot substitute for human shedding studies for several reasons.
But again, no studies testing whether excretion of mRNA-containing LNPs, modified spike-encoding mRNA, or spike produced by vaccinated people have been done. Well, I shouldn’t say none, because in this paper the author cites a Pfizer document obtained by FOIA which apparently revealed that shedding was studied in the urine and feces of intra-muscular injected rats. Unfortunately, that document is no longer at the website referenced.
To summarize from the above, the FDA’s position is that:
- the mRNA vaccines are gene therapy products
- Gene therapy products require shedding studies in both animals and humans
- Gene therapy product shedding raises the possibility of transmission from treated to untreated individuals
Note that much of the rest of this series of posts on shedding is guided by a masterful comprehensive review of the topic of gene therapy product shedding by independent researcher (by definition) Helene Banoun in Infectious Diseases Research. Hers is one of the only papers I could find that attempted to meticulously explore what is known about shedding of the mRNA gene therapy vaccines.
As already stated, an important point Banoun makes is:
There was no regulation of mRNA clinical trials prior to RNA vaccines, yet there is strict regulation of gene therapy products. It is difficult to justify that mRNA vaccines are not considered in the same way as gene therapies regarding this regulation; indeed the only difference is that they are (historically) supposed to protect against a disease and not cure it. Gene therapies are intended for a small number of people in poor health, whereas vaccines are used on a large scale on healthy people: it would therefore be wise to apply stricter rules to them.
She further points out another omission of the regulatory process:
Any experiment involving the deliberate transfer of a nucleic acid to a human must be preceded by Institutional Biosafety Committee approval (document on the regulatory standards is here), but approval was not given because of the emergency clearance given to mRNA vaccines.
Therefore, according to both the American and European agencies, mRNA vaccines are gene therapy products and should have been subjected to excretion studies of all secreted fluids (urine, exhaled droplets, saliva, sputum, nasopharyngeal fluids, semen, breast milk, feces, and sweat). Again, these studies were not done for mRNA vaccines nor for the DNA adenovirus vaccine (J&J).
So, where are the clinical human shedding studies? Well, I just learned of one that is about to be published (next ten days?) where the research team exposed a population of unvaccinated women to vaccinated individuals and their assessment outcome was the development of menstrual abnormalities. I know the results but want to respect the research teams right to present their original work. They have promised to share their manuscript with me and Paul Marik as soon as the peer-review and acceptance process is complete. I have no idea what journal they submitted to but I can be highly confident it is not the New England Journal of Medicine.
The entire reason why I did a “deep dive” into shedding science is because shedding was not studied when it absolutely should have been and I believe with near certainty that it occurs. Note my use of “near certain” is only to seem objective but it really is too late for that – both my partner Scott and I have diagnosed and successfully treated a number of shedding “victims.”
The lack of shedding studies prior to the mRNA rollout was, in my opinion, an insanely reckless and irresponsible omission (or willfully criminal, take your pick). As an evolving expert in the evaluation and treatment of Covid mRNA vaccine injury syndromes, I and others have identified the spike protein as the main component responsible for not only the pathogenicity of Covid but also of the vaccines, with this review paper proposing a new field named “spikeopathy” (study of the disease processes triggered by the spike protein).
If vaccine transcribed spike protein can be transmitted in sufficient quantity from vaccinated folks to unvaccinated ones, it stands to reason that adverse effects of the vaccine can develop in some unvaccinated people who came into contact (or close proximity) with vaccinated people. How did they get away with not studying this possibility?
An easy answer is they were doing science at “warp speed.” The more uncomfortable answer is that the “vaccines”, although meeting the definition of a gene therapy product, were actually not even legally considered a medical product at all and thus did not require a diverse range of safety studies (like on genotoxicity, reproductive risks, excretion potential etc). What? Why? How?
The reality is that the Covid vaccines, as a result of successive federal legislative actions which evolved over decades, was legally categorized as a “countermeasure” under a “public health emergency.” Such “countermeasures” require no specific regulatory approval process prior to dissemination. All a countermeasure needs is the recommendation of the Secretary of Health and Human Services that “it may be effective.”
This is the conclusion derived from the legal investigatory work of various independent and legal experts and researchers like Catherine Watts, Todd Callender, and Sasha Latypova. If interested in learning more, I would watch this lecture by Sasha Latypova (scroll down the page to find her lecture). As they have uncovered, “countermeasures” (even gene therapy ones) do not legally require studies of excretion potential, bio-distribution, pharmacokinetics, genotoxicity, insertional mutagenesis etc.
They don’t even require FDA regulated clinical trials of efficacy or safety.
So why did Pfizer and Moderna even do the efficacy trials? Latypova maintains that they did this not only to satisfy the public’s confidence to increase vaccine uptake, but also to “fool” the public into thinking these vaccines were medical products subject to standard (albeit accelerated) pharmaceutical product regulatory processes.
This obscured the reality that they were instead classified as military “countermeasures” against a perceived (if not actual) bioweapon. To wit, the COO of Operation Warp Speed was a General from the Department of Defense (DOD) and the vaccine manufacturers were under contract with the DOD to produce the countermeasure, sometimes referred to as a “demonstration (demo)” and/or a “prototype” in numerous legal documents they uncovered.
Anyway, as a result of this lack of a legal requirement to fully study these products in a public health emergency, the list and types of studies that should have been conducted (but were not) is long. Researchers and clinicians have been screaming about this since they were rolled out. These cries were met with a deafening silence by governmental health agencies across the world.
I know, it is a lot to take in.
But the latest “word on the street” is that the finance and insurance industries may finally be waking up to this fraud and its devastating impacts on U.S disability and death rates. Knowledge of these society-wide impacts largely results from the work of two different research teams led by former Blackrock portfolio manager Ed Dowd and insurance industry consultant Josh Stirling).
This article describes the reasons why Pfizer and Moderna stock are crashing of late. Put more succinctly, from what I hear it is due to the hedge fund guys shorting their stock. I believe Pfizer is in even deeper trouble now that this “forensic” paper just got published finding that they hid vaccine trial deaths which obscured a 3.7 fold increased risk of cardiac death in the vaccinated arm of their trial.
“Shedding” Part 1– Shedding of Covid mRNA Vaccine Components and Products From The Vaccinated to the Unvaccinated – Part 1
“Shedding” Part 2 – The Bio-Distribution and Excretion Potential of Covid mRNA Vaccine Products
“Shedding” Part 3 – Can You Absorb Lipid Nanoparticles From Being Exposed To a Vaccinated Person?
“Shedding” Part 4 – Evidence of Placental and Breast Milk Transmission of Covid mRNA Vaccine Components
“Shedding” Part 5 – Evidence of Shedding Causing Illness In Others
“Shedding Part 6– Clinical Case Notes Describing Shedding Phenomena Among Leading Edge Clinic Patients
“Shedding” Part 7 – Shedding Via Sexual Intercourse – Clinical Reports
As the German Health Ministry drowns in millions of unwanted vaccine doses, Karl Lauterbach begs Germans to please, please line up for their fifth jab

eugyppius: a plague chronicle | November 1, 2023
From the erstwhile vaccine propagandists at Der Spiegel, who I think are also tiring of the insipid autumnal vaccination liturgy and its noxious political enablers:
Federal Health Minister Karl Lauterbach has again called on people to get a booster vaccination. “Despite the pandemic and awareness campaigns, the importance of the Covid booster is apparently greatly underestimated,” he tells Spiegel. “So far, unfortunately, only a fraction of those for whom it is recommended have had a booster vaccination.” He calls on all at-risk groups and older people to catch up and ideally combine it with a flu vaccination.
According to the vaccine uptake statistics of the Robert Koch Institute, only about 2.5 million people have received three or more boosters. This means that only a fraction of those over 60 are likely to have sufficient protection against Covid …
They let Lauterbach flap his gums a little more about population immunity, Long Covid, secondary infections and how the vaccines can make all this better because reasons, before sticking the knife in him:
Lauterbach urgently needs to boost vaccine uptake. The pharmaceutical contracts concluded under his predecessor Jens Spahn have secured much larger quantities of vaccine than are currently being used. Between September and November, about 14.1 million vaccine doses of monovalent vaccine targeted at XBB 1.5. will be delivered. An additional 10.6 million vaccine doses of Novavax XBB 1.5. vaccines will also become available, as soon as they are approved by the European Commission.
Our dissolute snake oil salesmen – who is either so stupid or so desperate that he actually tweeted a link to this not-so-subtle takedown – is currently sitting on 11.5 million Pfizer/BioNTech doses, trembling at the prospect of Novavax dropping another 10 million on his head, with no hope at all that more than 5 million Germans will ever line up for these worthless products. This is despite the best efforts of the regional press, who have been trying to gaslight their elderly readers into getting yet another jab since September. Today the Main Post published a typical piece, claiming that vaccine demand is starting to creep up now, really it is; while yesterday it was the turn of Münchner Merkur to claim that everyone is talking about the shiny new vaccines and to drag in some pulmonologist to talk about the “predominantly positive reception” they’ve enjoyed.
Dear idiot reporters: The official vaccine dashboards may be down, but the RKI still publish day-by-day uptake statistics. Stop lying.
Fired Unvaccinated New York City Teachers Still Fighting for Reinstatement and Back Pay After Supreme Court Win
By Brenda Baletti, Ph.D. | The Defender | October 31, 2023
In a precedent-setting victory last month, a New York State Supreme Court judge ruled that 10 New York City school teachers fired for refusing the COVID-19 vaccine on religious grounds must be reinstated with back pay, benefits, seniority and attorney fees.
But the city immediately appealed the decision, so none of those teachers have returned to their jobs or received any payments.
“These workers absolutely did win reinstatement and back-pay,” Sujata Gibson, the teachers’ attorney told The Defender. “Unfortunately, in New York State courts, the government is entitled to an ‘automatic stay’ of any such relief pending resolution of the appeal.”
Gibson also said:
“CHD [Children’s Health Defense] is supporting us in our fight to defend these wins on appeal, and we are pursuing additional options to try to speed this process up and secure relief for additional plaintiffs. But the fight is not over yet.”
Nearly 7,000 New York City Department of Education (DOE) workers who sought religious accommodation from the COVID-19 vaccine mandate in 2021 were denied based on standards that a federal court later ruled unconstitutional.
Some of the workers, along with Teachers For Choice, sued the city in February, in a lawsuit sponsored in part by CHD and CHD New York.
The suit also sought class-action certification for all DOE workers who were denied religious exemptions. Judge Ralph Porzio denied the motion to grant class status, a ruling the plaintiffs are appealing.
Regardless, Gibson said the decision was “a precedent-setting victory, and a watershed moment in the teachers’ fight.”
Thousands of workers were subjected to the very same processes the judge ruled were “arbitrary and capricious,” and they could sue individually based on that precedent, if it is upheld by the appeals court, Gibson said.
Michael Kane, one of the plaintiffs and a member of Teachers For Choice, told The Defender that after filing the appeal, the city has six months to take the next step in the case — so even though they won with the last ruling, the fired teachers will have to continue to fight for their rights and the relief they are entitled to.
The struggle continues, despite confusion on social media
Last week, a Fox News story from Oct. 25, 2022, “New York Supreme Court reinstates all employees fired for being unvaccinated, orders backpay” was picked up and celebrated on social media by influential figures and their followers. It circulated on X, formerly Twitter, and Instagram, where hundreds of thousands of social media users “liked” the posts, Kane said.
The story itself was vague — it did not cite the actual case that had been ruled on and it gave the impression that all New York City workers fired for refusing vaccination would be returning to work with back pay.
In fact, the story was posted after the state’s Supreme Court ruled in favor of plaintiffs George Garvey and 15 other New York City Department of Sanitation employees who were fired by the city for non-compliance with the mandate.
That historic ruling was applicable not only to the 16 workers who sued but also to all public employees in New York City, including the police and fire department.
But in that case, the city also appealed the ruling and the appeals process is ongoing.
New York City workers, with substantial public support, continue to fight, Kane said.
He added:
“This isn’t just for us, it’s for our kids and our grandkids. This is laying the groundwork. It took over 50 years for Plessy v. Ferguson to be overturned by Brown v. Board of Education. Civil rights battles are long, protracted struggles, and that’s what we’re in. It’s not fun, but that’s what we’re in.”
Brenda Baletti Ph.D. is a reporter for The Defender. She wrote and taught about capitalism and politics for 10 years in the writing program at Duke University. She holds a Ph.D. in human geography from the University of North Carolina at Chapel Hill and a master’s from the University of Texas at Austin.
This article was originally published by The Defender — Children’s Health Defense’s News & Views Website under Creative Commons license CC BY-NC-ND 4.0. Please consider subscribing to The Defender or donating to Children’s Health Defense.
Potential Health Risks of mRNA-Based Vaccine Platforms
Despite 30 Years of Development, Thousands of Patents, Basic Questions are Unanswered
By Peter A. McCullough, MD, MPH | Courageous Discourse | November 1, 2023
My clinical practice is loaded with patients who took one or two vaccines early in 2021 and realized like most of us that the the mRNA products were not safe. A common question is: “doctor when does this shot get out of my body?”
Acevedo-Whitehouse and Bruno raise this point in a recent peer reviewed publication concerning the entire mRNA vaccine product pipeline.
Therapeutic applications of synthetic mRNA were proposed more than 30 years ago, and are currently the basis of one of the vaccine platforms used at a massive scale as part of the public health strategy to get COVID-19 under control. To date, there are no published studies on the biodistribution, cellular uptake, endosomal escape, translation rates, functional half-life and inactivation kinetics of synthetic mRNA, rates and duration of vaccine-induced antigen expression in different cell types. Furthermore, despite the assumption that there is no possibility of genomic integration of therapeutic synthetic mRNA, only one recent study has examined interactions between vaccine mRNA and the genome of transfected cells, and reported that an endogenous retrotransposon, LINE-1 is unsilenced following mRNA entry to the cell, leading to reverse transcription of full length vaccine mRNA sequences, and nuclear entry. This finding should be a major safety concern, given the possibility of synthetic mRNA-driven epigenetic and genomic modifications arising.
These are stunning revelations. I have called for a halt on mRNA research development until these fundamental questions can be answered. If synthetic mRNA cannot be broken down by the human body, there were be no way to shut off potentially dangerous antigens such as the Spike protein of SARS-CoV-2, Influenza virus hemagglutinin (HA), or any other toxin produced from the genetic code. To make matters worse, it appears that all of these proteins will be expressed on the cell surface and cause auto-immunity with any new mRNA vaccine. This alone is a show stopper for me in my practice. I am advising NO mRNA vaccines for my patients.
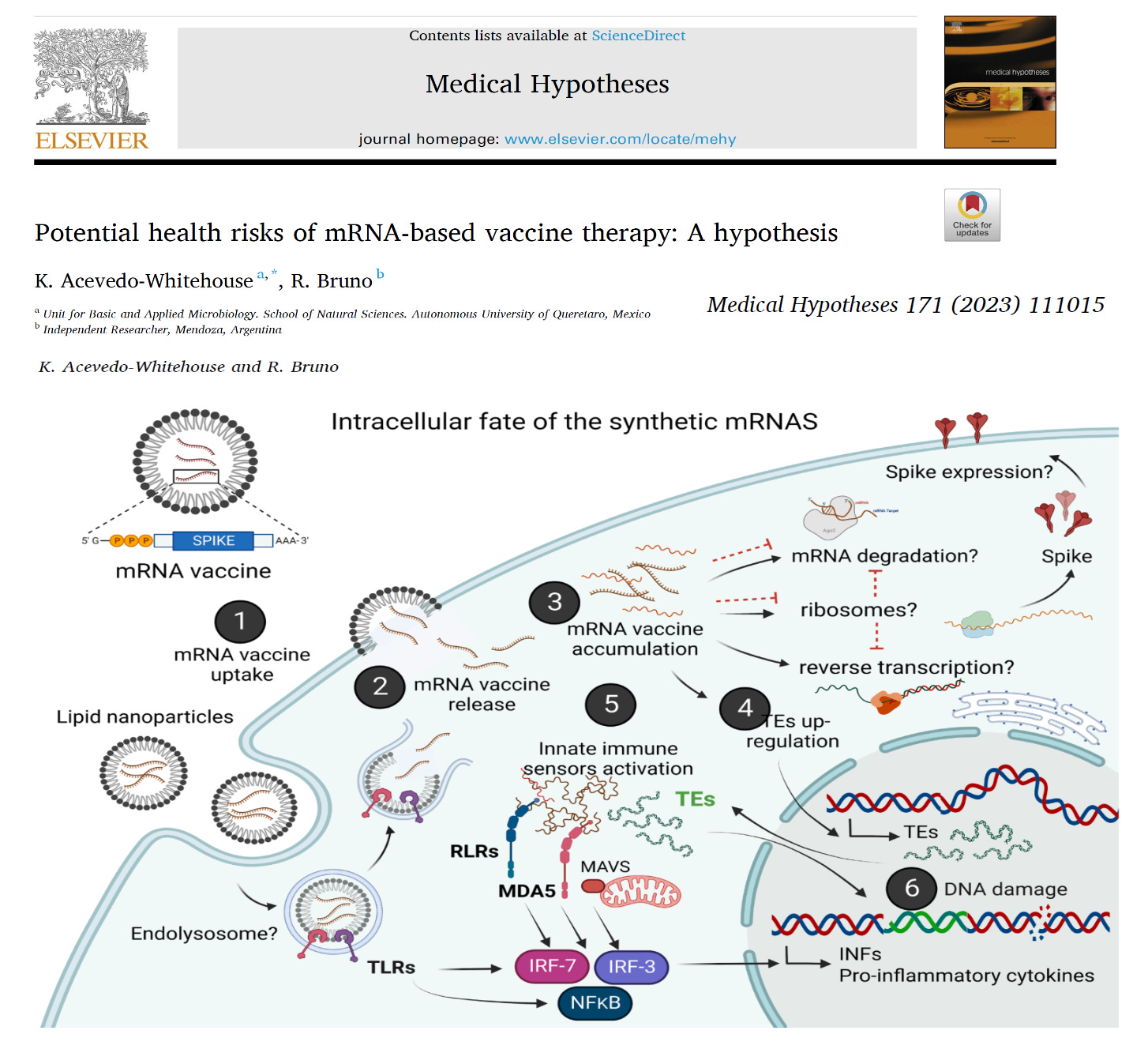
Acevedo-Whitehouse K, Bruno R. Potential health risks of mRNA-based vaccine therapy: A hypothesis. Med Hypotheses. 2023 Feb;171:111015. doi: 10.1016/j.mehy.2023.111015. Epub 2023 Jan 25. PMID: 36718314; PMCID: PMC9876036.
The Depopulation Bomb: A Halloween Sci-Fi Tale

By Clayton J. Baker, MD | Brownstone Institute | October 31, 2023
The following fictional story may or may not bear resemblance to events in real life.
Imagine, if you will, that you are a first-generation high tech gazillionaire. In fact, at one time you were said to be the richest man on earth, although that is no longer the case. Nevertheless, you remain unimaginably wealthy, with all the responsibilities and burdens that such wealth brings. (Given the extremely unusual circumstances of this tale, to make it more relatable, we will assign you a fictional name.) Your birth certificate reads Gilbert Harvey Bates III, but the world knows you as Gil Bates.
Gil Bates’s erstwhile net-worth preeminence (stolen as it was by an upstart online retailer named Biff Jezos) is not the only important loss he has suffered. Also in the rearview mirror is his youth, his marriage, and his position as CEO of the behemoth tech company he created, MacroHardTM.
After Gil Bates stepped down as CEO of MacroHardTM, he focused on his philanthropic work. The centerpiece of this work is the immensely well-funded (and therefore immensely influential) Bates Foundation. The Foundation’s scope may be mind-bogglingly broad, but one problem especially consumed Bates: there are far too many people on the planet.
In his youth, Gil Bates read a controversial book called The Overpopulation Bomb, written by a visionary scientist named Saul Derelicht. That alarming book, a huge bestseller in its day, described a neo-Malthusian hell on earth resulting from human overpopulation, and proposed mass sterilization and other aggressive population reduction techniques as the solution.
Gil Bates became convinced, and remains convinced – especially as the worldwide human population has soared beyond 8 billion units – that Homo sapiens have obscenely overpopulated the planet. Once Bates had sold software packages to the great majority of them, he vowed that this existential threat to the planet must be addressed.
But what was to be done? How could this great affront to Gaia be reconciled? When it comes to a responsibility so great, a task so immense, no single man – not even Gil Bates – could hope to accomplish it alone.
Fortunately for the future of Earth, Bates knew a host of like-minded, enlightened elites, pre-eminent individuals of great wealth, power, and worldwide influence. Among the most important:
- A dour Teutonic economist named Kraut Schlob. The son of an ambitious industrialist who built flamethrowers for the Third Reich, Schlob is the founder and chairman of the World Enslavement Forum. The Forum has become the premier worldwide gathering of hyper-elites who wish to discuss globalist policies, and enjoy the company of high-end prostitutes, free from the prying eyes of commoners.
- An immensely powerful – if embarrassingly vertically challenged – American health bureaucrat named Dr. Fantoni Auci. For decades, Dr. Auci controlled the overwhelming majority of US Government medical research funding. As such, no one in the vast American network of hospitals, research institutes, or universities dares to cross Dr. Auci, and he wields similar influence internationally. In fact, he oversees funding for multiple secret virology research laboratories, as far away as China.
- A mysterious veterinarian named Adalbert Ghoula. Ghoula is the CEO of Kaiser, Inc., the world’s largest and most rapacious pharmaceutical company, which Ghoula has grown into a veritable modern day IG Farben. In his earlier days, Ghoula oversaw the development of a vaccine that successfully induces the chemical castration and sterilization of swine.
The consensus, reached after lengthy consultations with these men and other luminaries, was that the worldwide human population must be reduced from 8 billion to 500 million units.
But how? Several possible avenues were proposed.
- War has been used for millennia to reduce populations, and while highly effective locally or regionally, it would be entirely ineffective at removing the necessary fifteen-sixteenths of people on Earth. After all, the deadliest war in history, World War II, resulted in a mere 80 million deaths, just 3 percent of the world’s population at the time.
- The use of a bomb was considered a special kind of bomb, reminiscent of the “neutron bomb” of yore, which would supposedly reduce populations while sparing infrastructure. This seemed closer to the mark than all-out war, but ultimately it was determined that setting off bombs would be both impractical and far too obvious. After all, even herd animals will not consent to being openly and massively slaughtered, no matter how necessary the culling may be. The herd must be kept forever in the dark.
- A plague, a pestilence, a pandemic seemed more promising. Past naturally occurring pandemics had reduced human populations much more successfully than wars. The Black Death of 1346-53 may have reduced the world population by as much as 25 percent, a much more encouraging number than the measly 3 percent from World War II. As an added economic bonus, the Black Death served as a very effective concentrator of wealth for the survivors, as it caused minimal collateral property loss.
However, a more detailed review of historical worldwide population estimates demonstrated that a pandemic alone could only serve as a temporizing measure at best. Most estimates show that by 1400, the worldwide population had unfortunately returned to its pre-plague total.
Clearly, the necessary 94 percent reduction in population could not be achieved by culling the herd alone. Sterilization would be needed as well. But how to achieve such mass sterilization? Many H. sapiens possess an intense desire to procreate – that’s the source of the problem, after all. Unfortunately, prior historical initiatives for mandatory sterilization – even those of limited scale and scope, such as those targeting the mentally deficient – have met great opposition, at least in the so-called “free” nations.
- However, a vaccine could be used for mass sterilization. Ghoula’s earlier work at Kaiser was proof of this. But a fundamental problem remained: how to get the unsuspecting population – specifically, its children and young adults – to take the stealth-sterilizing inoculation?
The solution, when it came, was a thing of beauty, sublimely subtle and symmetrical. The answer was a two-step process: a pandemic and a vaccine. One population reduction device would be released, presented as a worldwide plague. It would be followed by a second population reduction device, presented as the cure.
And the technology was already in place to make it happen. It merely had to be perfected, then enacted.
Employing the Black Magic of gain-of-function virology research, an animal respiratory virus, previously never infecting humans, was genetically engineered to readily infect and spread amongst humans. At a key moment in political history, when a particularly bothersome populist American President named T. Ronald Dump was running for reelection, the virus was released from a Chinese laboratory into the human population.
As the new virus spread, reports of the death and devastation it wrought were spread as well. In actuality, the virus had been engineered so that it was deadly only to the frail, chronically ill, and very old. It was cleverly propagandized, however, as a threat to persons of all ages, a modern day Black Death of sorts.
The US deep state, desperate to disrupt the Dump presidency and remove him from office, were willing partners to manage the control and manipulation of the population through propaganda, and to enforce unprecedented, prolonged lockdowns of society. Remarkably, they even convinced President Dump to sanction the lockdowns, and to fund the development of the vaccine. Most other countries followed suit.
The new virus rapidly killed off many of the oldest and sickest members of society, as would be expected of a novel respiratory virus. However, the locked-down and isolated populations were barraged with media messages that stirred up mass terror of the virus. Businesses were closed, save for those deemed “essential.” Schools were closed, though children were already known to be at statistically zero risk of death. Dissenters were harassed, scapegoated, and punished.
Then, a solution to the pandemic was presented: the vaccine. The vaccine was the savior, the only way out of this crisis.
A few irritating, contrarian dissenters fought back. They protested for civil rights. They stressed the near impossibility of producing an effective vaccine against a rapidly mutating respiratory virus. They identified numerous “safety signals” found in the vaccine trials, and tried to expose these as best they could. But the mainstream media drowned them out, the social media companies (controlled by the deep state) censored them ruthlessly, and after all, once the vaccines were mandated, most people took at least a couple of doses.
And the joke was on the dissenters in another, more important respect. These meddlesome do-gooders were indeed intelligent enough to identify the toxicities inherent in the vaccines. But they decried them as “safety signals.” The fatal toxicities they identified still seemed to them to be flaws, mistakes, and the unfortunate results of a hasty and mad rush to make money off of the pandemic.
Imagine the naïvete.
Early in the vaccine “rollout,” young women reported abnormal vaginal bleeding and other menstrual problems after receiving the vaccines, raising concerns about potential unintended consequences to female reproduction. Pathologists found ovaries infiltrated with multiple toxins from the vaccines, both the dreaded “spoke” protein of the virus and “lucid nanoparticles” from the vaccine’s delivery system. Even occluded Fallopian tubes were identified.
Soon thereafter, reports appeared in the alternative media of dramatically increased numbers of sudden deaths, primarily in young men, after receiving the vaccine. It often visibly occurred in athletes while on the playing field. This caused considerable alarm, impossible as it was to hide.
In a masterful demonstration of the “limited hangout,” officials acknowledged the sudden death phenomenon, but would not even allow mention of the vaccine as a possible cause within the mainstream medical community. Instead, protocols and clinics for this sudden epidemic of heart disease in the young were established, but strangely without any official curiosity as to the cause. All they knew for sure was that it couldn’t be the vaccine.
Of course, the infamous “spoke” protein, the same viral antigen chosen by the vaccine’s designers to induce the vaccinated patient’s body to produce in quantity, just happens to be the most toxic part of the virus. The “spoke” protein deposits itself in tissues throughout the body, wreaking havoc wherever it goes. It has a particular affinity for the heart muscle, causing the inflammatory process known as myocarditis that leads to cardiac arrests.
“Spoke” doesn’t stop with the heart, however. It is a remarkably versatile toxin, a sort of Swiss Army monkey wrench in the human body. It causes gigantic, gruesome, rubbery blood clots in the vasculature, seizures in the central nervous system, the aforementioned deposits in ovaries and Fallopian tubes (and testes, for that matter), etcetera, etcetera. What a stroke of genius to choose “spoke” as the antigen the vaccines induce replication of!
The vaccines held another nasty little secret, which even the pathetic, naïve resistance only recognized much later. The vaccines were “contaminated” with plasmids containing MV-40 and MV-40-like DNA sequences. Yes, that MV-40, the monkey virus known to cause cancer in multiple animal species.
Could the appearance of so-called “turbo cancers” in vaccinated persons somehow be related to this “contamination?” Well, another limited hangout, this time courtesy of Healthcare Canada, took care of that.
Excess death rates rose dramatically after the vaccine rollout. Birth rates plummeted. To the do-gooders, refuseniks, and dissidents, this was a scandal.
But what did they know? To use a phrase all-too-familiar to the seasoned software developer, these toxicities were not bugs, but features. The vaccines were working exactly as they were supposed to work.
Silly plebes! The “vaccines” were actually a deliberate, multi-pronged, population reduction device. They were designed to kill a percentage of young people – mostly male – outright, to poison and disable the female reproductive system at multiple points, and to insert teratogenic plasmids into recipients’ cells, to pick off others at undisclosed, later dates. They were merely packaged and marketed as a vaccine against a (lab-manufactured) flu-like illness.
As successful as they have been, there remains so much more work yet to be done.
A definite lull occurred in the population’s acceptance of repeated injections of the vaccine. The dissidents may be naïve, but they are persistent, and sometimes effective to a degree. But ultimately they will fail.
The general population is lazy, uneducated, and easily terrified. (Some say they are being done a favor by being culled.) They are accustomed to the precedents set by other vaccines. Their reluctance will be worn down with time. Of course respiratory viruses are imperfect targets for vaccines. Once again, that’s not a bug, it’s a feature! It only means that a new booster of the vaccine will be needed every year – at least.
With each new round of boosters, a new population of girls and young women will be rendered infertile. A new group of boys and young men will suffer cardiac arrest – a very quick and painless way to die, really.
Countless others will contract cancers – turbo cancer, to use the current term for these rapidly progressing and deadly malignancies, often of unusual types – bone cancers, muscle cancers, and other former rarities. Not an easy way to die, admittedly. But these tumors mercifully progress to end stage very swiftly, and their value as a population reduction device is undeniable.
Have no fear. It is only a matter of time; only a matter of lather, rinse, repeat. As long as the herd allows itself to be sent through the sheep dip whenever and however often the shepherds proclaim is necessary, H. sapiens will get to 500 million. All courtesy of a type of bomb after all, but in this case a microscopic bomb that is released in each person via a tiny little injection: The Depopulation Bomb.
Happy Halloween!
C.J. Baker, M.D. is an internal medicine physician with a quarter century in clinical practice. He has held numerous academic medical appointments, and his work has appeared in many journals, including the Journal of the American Medical Association and the New England Journal of Medicine. From 2012 to 2018 he was Clinical Associate Professor of Medical Humanities and Bioethics at the University of Rochester.
Featured Video

Trita Parsi: Iran War Ends Today? Threats of Deporting Trita Parsi
or go to
Aletho News Archives – Video-Images
From the Archives
Iran UN ambassador calls for destruction of all nuclear weapons

Iran’s ambassador to the UN Gholamali Khoshroo
Press TV – March 29, 2017
Iran’s ambassador to the UN Gholamali Khoshroo has called for the total eradication of nuclear weapons.
Khoshroo reiterated Iran’s call during a UN conference aimed at creating a nuclear weapons ban treaty in New York on Tuesday.
“Iran, as a victim of chemical weapons, strongly feels the danger posed by the existence of weapons of mass destruction and is determined to engage actively in international diplomatic efforts to save humanity from the menace of nuclear weapons,” he said.
Khoshroo stressed that Iran is committed to its Non-Proliferation Treaty (NPT) obligations, which include negotiations based on effective nuclear disarmament measures.
He added that several countries continue to ignore international calls and treaties for nuclear disarmament and even continue to increase their nuclear stockpiles. “They do not have political determination to abandon doctrines of nuclear deterrence and nuclear terror,” he went on to say.
Iran’s UN ambassador noted that boycotting the talks by many countries, including the US, shows that the world’s nuclear powers are by no means committed to the eradication of nuclear arms. Britain and France were also among the some 40 countries that did not join the talks.
“We note that prohibition of nuclear weapons must be accompanied by the elimination of such weapons. There can be no doubt that without complete abolition of nuclear weapons, there will be no absolute guarantee against the danger of nuclear war and the use of such weapons,” Khoshroo added.
Blog Roll
 Aletho News
Aletho News- Trita Parsi: Iran War Ends Today? Threats of Deporting Trita Parsi
- What Is SIDS?
- DHS docs: Govt bracing for nationwide anti-AI riots, preparing to crack down on dissent
- India signals rethink over West Asia
- Israeli Ex-Navy Chief admits massive damage from Iran missiles
- The strategic arsenal US lost in war against Iran – and why replenishment will take years
- Documents Suggest Fauci Knew COVID Was Created in Wuhan Lab, and mRNA Vaccines Wouldn’t Work
- No return to pre-war status for Strait of Hormuz – Iran’s top diplomat
- Ex-South Korean President sentenced for trying to provoke conflict with Pyongyang
- US publishes docs on ‘dangerous’ Ukrainian biolabs
- If Americans Knew
- Israeli Firm Accused of Launching Smear Campaigns During US, European Elections
- As World Cup kicks off, Gaza amputee girls chase football dreams
- Oxfam: More Palestinians killed by Israel across West Bank in last 3 years than previous 17 years combined
- US-Iran ceasefire may be imminent, but will Israel blow it up? – Daily Update
- The Issue of Israel Is Ending Democracy In Michigan
- Israel is stealing homes, livelihoods, and lives in West Bank
- Gaza is not an aberration – Israel planned this genocide decades ago
- Israel is changing the face of Lebanon, mainstream media is normalizing it – 3 articles
- Genocide lobby benefits from EU anti-racist fund
- Watching the World Cup from Gaza
- No Tricks Zone
- New Study: Significant CO2 Fluxes From Non-Volcanic Sources Are Largely Neglected In Carbon Budgets
- Women Climate Scientists Being Harassed, Insulted By Skeptics, Claims Berkeley Earth Researcher
- Germany’s Longterm Spring Climate Data Show “No Climate Trend”
- New Study: Solar Photovoltaic, Wind Power Fail To Meet Annual Energy Demands 62% Of The Time
- Germany’s Die Welt: “Too Much Is Too Much” … Green Energies Are Cannabalizing Each Other!
- Germany’s Ecological Holocaust… Once Fairy Tale Forests Getting Cleared For Wind Turbines
- A Grand Solar Minimum Has Arrived…Global Cooling Of At Least 1°C Is Expected By The 2030s, 2040s
- European “Expert Commission” Urges COVID-19-Like Global Climate State Of Energency!
- Real-World Observations Do Not Support The Position That Climate Change Is Human-Caused
- Germany’s AfD Party Calls Debunked Climate Scenarios “Greatest Fraud In Human History”
