Deaths up 14%. Births down 28%. Disability up 37%. Wake up, politicians!
By Guy Hatchard | TCW Defending Freedom | September 1, 2023
The official figures for births and deaths in New Zealand between July 1 2022 and June 30 2023 have been released. The short summary accompanying the release of the horrifying figures compares these with the previous 12 months, and reports increases in deaths and reductions in live births. The 2022/23 figures would have better been compared with the July 2018 to June 2019 totals, the first available pre-pandemic period. We report this comparison below.
There were 38,442 deaths among all ages for July 2022-June 2023 compared with 33,753 deaths in the 2018/19 period. This is an increase of 4,689 deaths (up 14 per cent) and equates to 90 excess deaths per week.
Deaths among 15-to-64-year-olds were up by 6 per cent. Figures released by the Household Labour Force Survey report the rate of disability sufficient to preclude joining the workforce among this age group has increased by 37.5 per cent over the same period and now stands at 14.3 per cent of the workforce. That is huge.
Alarmingly, live births fell from 26,500 in 2018/19 to 19,185 in 2022/23, a decrease of 7,400 or 28 per cent. This is an unprecedented drop.
Covid deaths during this period averaged around two to three per week and can be discounted as a causal factor for the increase in deaths. Nor is an ageing population sufficient explanation for the figures.
We have been aware of data like this for some time now, but there has been deafening silence from our politicians, who are currently running for re-election. We are heading into this election under unusual and coercive constraints which have no precedent in our history as a nation.
Due to the events of the last three years, the machinery of government has assumed more control over our medical and food choices. The birth and death figures must be regarded as a verdict on policies which have enjoyed cross-party support.
As a result of government policies, we have lost many of our rights as citizens. None of the parties currently elected to Parliament has any plans to revoke this government overreach. So what has gone wrong and how will this affect us if we re-elect the same group of political parties to power?
Pandemic policies have established a precedent allowing the government to enforce compliance with its medical rules. They coerced almost everyone to take injections with high rates of adverse effects. Restrictions on social movement and communication have been normalised. Agreements with social media providers and the mainstream press have censored the availability of independent information and hampered scientific dialogue. Access to official public health data has been limited.
The government has passed the Therapeutic Products Bill which has legitimised the substitution of thousands of natural ingredients with untested synthetic alternatives without requirements for clear labelling. The Bill also facilitates dose restrictions and banning of many traditional herbal products and supplements at the whim of a bureaucrat.
The government has authorised the addition of fluoride to public water supplies. It has mandated the addition of chemical supplements to staple foods including a synthetic form of folic acid to flour which is hard to metabolise and inhibits some metabolic pathways vital for health.
Re-electing sitting members of parliament from any party is a prescription for more of the same. Our current politicians are refusing to face up to some hard facts. We are in the midst of a medical emergency of unparalleled proportions. Our hospitals are overwhelmed, our politicians are silent.
Unbelievably, these politicians and medical tsars continue to ignore accumulating evidence being published in learned science journals pointing to adverse effects of mRNA vaccines. Despite this, the government is still funding advertising encouraging the population to receive further booster injections. They don’t work and they endanger health.
There are no plans to investigate what has gone wrong. It is time to say goodbye to MPs from across the political spectrum who have spectacularly failed our nation in its hour of need. If they are re-elected, our ability to manage our own health choices will be gone for good.
The judgment on their competence is there in black and white from their own statistics – deaths up 14 per cent and births down 28 per cent. It doesn’t take a genius to know where this is going. Mistakes were made and they cannot be hidden or denied any longer. Some hard questions must be asked and answered.
Our media are lazy and compliant in a cover-up. They have enjoyed government support.
None of this is in the character of our nation or in its history. It is time to wake up.
A Picture Is Worth A Thousand Words
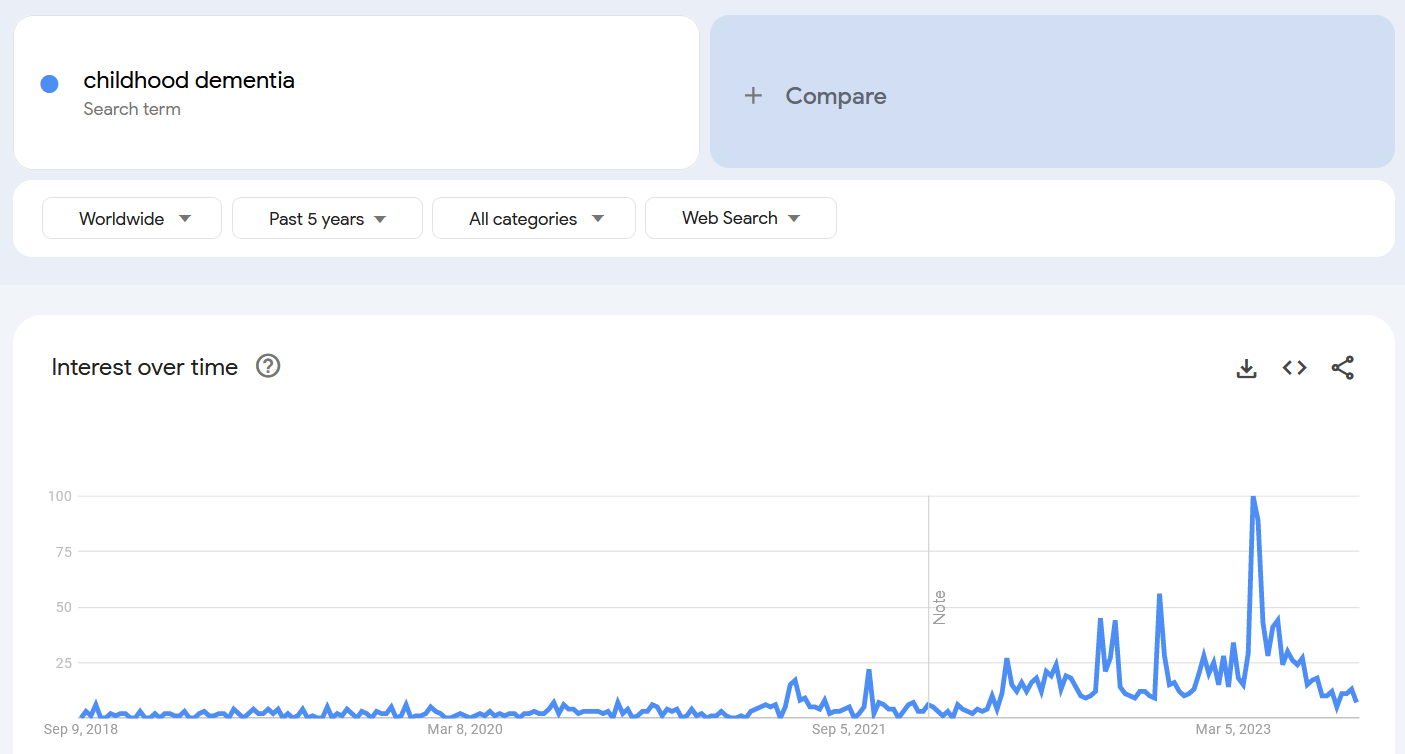
Childhood Dementia in 2022
The Naked Emperor’s Newsletter | September 3, 2023
What on Earth happened in early 2022 for searches for childhood dementia to have rocketed upwards so dramatically?
- Long term effects from Covid?
- Omicron?
- Long term effects from lockdowns?
- Vaccines?
I think I know what most people will say it is.
The worldwide rise in searches started early 2022 and peaked in April 2023. Fortunately, since then the trend has been firmly down. Let’s hope it stays that way!
Base Spike Protein Detoxification Explained on FlashPoint
By Peter A. McCullough, MD, MPH | Courageous Discourse | September 2, 2023
Gene Bailey is the steady and faithful host of Flashpoint, a popular faith based show on The Victory Channel that truly cares about its audience. The producers treat everyone like family.
Gene had Dr. McCullough slow it down and explain the rationale why patients with multiple rounds of SARS-CoV-2 infections and or COVID-19 vaccines should consider Base Spike Protein Detoxification (BSD). Its called “base” because it is the base of therapy in clinical practice to which other drugs or supplements can be added. With this core for 3-12 months or more, patients have the best chance of avoiding damage or illness in the cardiovascular, neurological, hematological, and immunological systems. See video
Because both nattokinase and bromelain are blood thinners known to influence the prothrombin time, partial thromboplastin time, and d-dimer concentrations, patients should be aware of minor or major bleeding complications. These have been used in addition to aspirin, clopidogrel, and anticoagulants such as apixaban, however, careful physician observation and potential dose adjustment may be required. Additionally, allergies to nattokinase, bromelain, or curcumin (turmeric) are contraindications.
Feedback has been tremendously positive from patients and physicians who finally have a peer-reviewed, published approach to long-COVID and vaccine injury syndromes. All of the products are available without a prescription. BSD is likely to be community standard of care until large, prospective randomized trials, and agency or society based clinical practice guidelines are developed.
Peter A. McCullough, MD, MPH
President, McCullough Foundation
First Principles and Self-Controlled Opposition
By Emanuel E. Garcia, M.D. | NewZealandDoc | August 30, 2023
Being a psychiatrist certainly makes me no specialist in areas of immunology, cardiology, surgery or infectious disease. But having earned a doctorate in medicine I was provided an education in reasoning within this extraordinarily complex discipline from first principles. Therefore as an inquisitive physician throughout the covid operation, I could not help but be baffled by the response of institutional authorities.
Forgive me for repeating myself, but a ‘first principles’ approach would never have led to lockdowns, distancing, masks or the nefarious Jab. It would never have led to mandates or apartheid. And it would never have led to the promulgation of mRNA agents and the relentless push not only to inject all of humanity but, alas, all of the animal kingdom upon which humanity relies for food.
I repeat myself because with the whiff of yet another novel ‘variant’ restrictive measures are again in the news in America, whose so-called president has promised a yet more effective jab.
Effective at what, one may ask? At creating even more disastrous adverse effects and excess death? At degrading one’s natural immune system so as to render one more susceptible to infections and cancers?
Leaving aside the fact that I never believed a vaccine of any kind was necessary to manage the covid threat, for reasons I have laid out in many essays already, the description of the emergency-use instrument was proof enough for me that it would be a disaster. Flooding a body with millions upon millions of coronavirus spike protein antigens manufactured by the body itself, thanks to the integration of messenger RNA into cell machinery, did not seem like a very good idea — unless one wished to wreak havoc.
Even a psychiatrist like me could see that the potential for spike protein/antibody complexes in tremendous numbers could create autoimmune catastrophe via myriad mechanisms, and even a psychiatrist would suspect that somehow those pesky things would cross the blood-brain barrier despite assurances to the contrary. In short, I figured that they would go everywhere.
And so they have.
The greater looming question, a question that continues to vex me to this day, is why or how so many medical specialists — some of whom have now come to have changed their tune — initially insisted that the Jab would be advisable for the elderly and medically compromised, if not for all. And indeed I wonder how some of these specialists, prominent in the current opposition to the Jab, came themselves to have received it.
You see, to argue from another set of first principles — principles of psychological rationality — it simply made no sense then, nor does it make sense now. Nor does it make any conceivable sense that the astonishingly predominant majority of physicians could have touted the Jab, forgotten about informed consent and early treatment, and cheered the imprisonment of healthy people against all hitherto formulated pandemic guidelines.
That we have been betrayed by our institutional medical authorities, trans-nationally and intra-nationally — and here I am thinking not only of the infamously corrupt World Health Organisation and Federation of State Medical Boards but of entities such as the Medical Council of New Zealand and the American Board of Internal Medicine and many others — is no longer a surprise. We can see them for what they are, for the despicable agenda they have imposed, and for the scientific and ethical foundation they, by their actions, have destroyed.
That we have been betrayed by our governments also is no surprise, given their dismissal and oppression of the very citizenry from whom these governments are supposed to derive their power.
The fight against these powers is not easy, as we know; and as we also know these powers delight in confusing and dividing any concerted opposition, which they accomplish in many ways, so as to weaken us.
During ‘conventional’ wartime it is commonplace for adversaries to send out spies, to infiltrate each other, to play the game of double and even triple agents, and to mislead each other in every possible way. In this war — in this war of the Globalist Few against the Populist Many — the massive communications agency masquerading as ‘news’ and ‘trusted media sources’ has hammered away without pause. It’s an irregular and really unfair war, and a thoroughly unique one given its scale, even though the techniques themselves of artful deception and purposeful division and the combination of soft and hard force have been around forever.
That our enemy — the enemy of real science and human autonomy, the proponent of censorship and the persecution of dissent — will seek to control us is obvious. However, the notion of ‘controlled opposition’ is in vogue and proceeds too trippingly from the tongue. Strictly speaking it is only one of the various means and devices used to disrupt our clamoring.
I’ve never liked this designation because it can become another of those irrefutable assertions whenever a disagreement arises and can be made to cover so many scenarios that it loses usefulness. Surely there can be spies and traitors and infiltrators and the like, and there always will. That’s life.
I worry more about ‘self-controlled opposition’ — about people who need no higher official to pull their strings but who have an uncanny knack for knowing how to curry favor and when to keep from going ‘too far’.
A realist is compelled to acknowledge that within any group of people, on whatever side, personalities will arise whose fealty is more to themselves than to the common mission. These are the folks with the kind of pull that can bend a movement astray.
Vaccines have become a kind of black hole, sucking so much of our discursive energy into endless debate. I have learned over these past three and a half years that no vaccine can be trusted — just as no medication can be. It is sound and rational to demand to know about the ingredients and adjuvants of every vaccine, just as it is sound and rational to want to know how fluoxetine is supposed to work and how it might go wrong. But we are left with the choice to partake and receive, or not. A choice that is non-negotiable, no matter what our governments may say while brandishing their scepter of fear.
Which brings me back to first principles. When the rebellious crew of fifty-six Americans signed the Declaration of Independence, they made preeminently clear the principles of human autonomy, rights that were inborn rather then conferred. They were, naturally, creatures of their time, molded by its social and cultural and racial constraints. The first principles, however, that they espoused and enshrined, held with them the key to overcoming these constraints. It took a while for their reasoning to be extended to its logical end to include all men and women, regardless of color — but it got there thanks to the enunciation of these foundational principles.
Same for psychoanalysis. Whatever one thinks or knows or thinks he or she knows about Freud and analysis and the mores of fin de siècle Vienna, the principle of free association as a portal to the unconscious mind transcends the societal and cultural milieu of the age in which it was discovered.
As we fight this fight of our lives the surest sign of corruption within our midst is whether our leaders adhere to or stray from principle.
So, going forward, if I start hearing about a better mRNA vaccine or an improved method of masking or a friendlier way to limit our freedom to assemble; if I start to read about how the harsh measures imposed and the rationale for a lightning-quick jab had some merit, all in the name of the greater good of course, I’ll know whom I’m up against.
New research shows mRNA jabs could weaken immune responses
Experts say mRNA vaccine can make cells of the immune system “lazy” when it comes to fighting off viral and bacterial infections
Maryanne Demasi, reports | August 31, 2023
Last week, a new peer-reviewed paper published in Frontiers in Immunology has sparked concern over whether mRNA shots could be weakening a person’s immune response.
The small study involved 29 children aged 5-11 years. Blood samples were taken from the children before and 28 days after a second dose of Pfizer’s mRNA vaccine. Samples from eight children were also analysed at six months.
Researchers found that vaccination resulted in reduced levels of cytokines – molecules that play a crucial role in mobilising an immune response against viruses and bacteria.
“Our study showed that, in children, SARS-CoV-2 mRNA vaccination decreases inflammatory cytokine responses,” wrote the authors.
This study builds on a previous pre-print in adult volunteers, that showed Pfizer’s mRNA vaccine could modulate the response of immune cells to non-specific viral fungal and bacterial infections.
The two studies are small, and the clinical outcomes were not assessed, so researchers cannot prove that mRNA vaccines increase a person’s susceptibility to “non-specific” infections in the real world.
However, this phenomenon has been shown to occur with other vaccines that are currently on the market.
In low-income countries with a high infectious disease pressure, so-called “non-live” vaccines such as the diphtheria, tetanus and pertussis (DTP) vaccine have been associated with increases in all-cause mortality and morbidity.
Christine Stabell Benn, epidemiologist, and professor at the University of Southern Denmark, is at the forefront of studying the phenomenon of “non-specific” effects of vaccines.

Christine Stabell Benn, epidemiologist and professor at University of Southern Denmark
“We found in our work that three months after subjects received the DTP vaccine, they showed lower immune responses in vitro to other infectious stimuli,” said Stabell Benn.
“Essentially, the immune cells become lazy, and they simply don’t respond as vigorously when they are challenged with an infectious agent,” she added.
The opposite was true when “live” vaccines were administered to people, such as the BCG (tuberculosis) vaccine.
“After BCG vaccination, immune cells would react more actively in response to other bacterial stimuli by reprogramming cells in the bone marrow to spit out more active innate immune cells,” said Stabell Benn.
The covid-19 vaccines are non-live vaccines, and Stabell Benn says the recent studies looking at reduced cytokine levels may be the “wakeup call” needed to do further studies.
“We now have two immunological studies that suggest the mRNA vaccines could suppress your ability to respond to other viruses, at least for a period of time, and it warrants urgent investigation,” said Stabell Benn. “Especially in children, because we are talking about a population at very low risk of severe covid-19 disease.”
Denmark stopped recommending vaccinating young children against covid-19, but in the US, it’s now part of the childhood immunisation schedule for individuals 6 months or older.
Stabell Benn said, “In the US where they are still vaccinating young children, they should immediately do a randomised study with mRNA vaccines, and investigate whether the reduced effect on cytokines translates into poorer clinical outcomes.”
Stabell Benn says it cannot be excluded that widespread use of the mRNA vaccines could be linked to recent unusual global outbreaks of bacterial infections, as well as viral infections.
This year for example, cases of respiratory syncytial virus (RSV) have skyrocketed across Australia, with some states reporting close to 10 times the number of cases compared to the same time last year.
Stabell Benn said, “A major factor for increased infections is the lockdowns that weakened immune systems because they are meant to be continuously stimulated, but we cannot exclude that the vaccines have also played a significant role.”
Currently, her team is conducting a study comparing vaccinated to unvaccinated children aged 5-11 years in Denmark.
“We will assess the clinical outcomes of these children, and most importantly, answer the question of whether there are any clinical differences in terms of the risk of other infections, other diseases in the children who were vaccinated or not,” she said.
Stabell Benn recently called for a new framework for testing and approving vaccines, in a paper published in the journal, Drug Safety (see key points below).
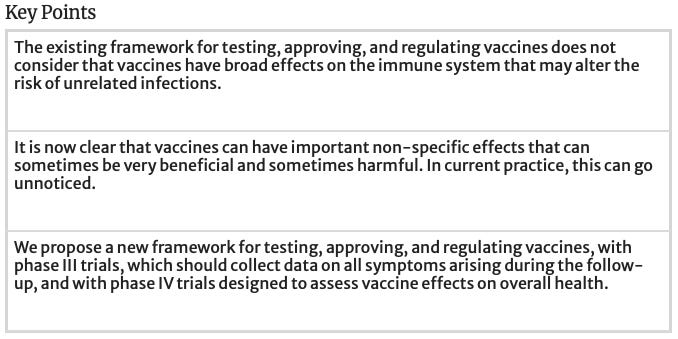
Stabell Benn said this framework should have been applied to the covid-19 trials. A major flaw in testing was that they did not assess whether the mRNA vaccines affected the risk of contracting other infections.
“While they reported covid-19 cases, they overlooked the possibility that people might’ve developed other infections like pneumonia down the track due to a weakened immune response after mRNA vaccination,” said Stabell Benn.
Problem-Reaction-Solution
Big Pharma excels in creating customers for life
Health Advisory & Recovery Team | August 31, 2023
For those of us who started pulling uncomfortable threads of ‘hang on a minute, that doesn’t seem quite right’ and kept going, the world is now a strange landscape. When it comes to our health, many of us have had life-long assumptions smashed to smithereens.
The last few years have been a brutal introduction to the harsh realities of the medical industrial complex. Its recent behaviour has completely shattered public trust. Overnight, medical ethics including bodily autonomy and informed consent were tossed out. The dying were unable to see loved ones, blanket DNRs were applied and people were subjected to forced procedures (e.g. PCR testing) or were discriminated against based on their covid vaccination status. Most went along with these inhumane diktats that came from ‘on high’. Is it any wonder that many people would now be reluctant to enter a hospital even where there was a genuine need? There has to be a balance where people regain the confidence to seek care if genuinely needed. Throwing the baby out with the bath water will not lead to fewer excess deaths. Patients rightly want the best available care but in the current system of protocolised medicine, that pathway is far from guaranteed.
What is striking, when spending time amongst those still firmly planted behind the Overton window, is the notion that for any ailment – particularly with advancing age – the answer is always pharmaceutical or surgical interventions rather than lifestyle changes. This is clearly superb for Big Pharma. Less certain, is the benefit for the end user. Blanket approvals of the novel, mRNA injections across all age groups – in spite of total lack of long-term safety data – showed us clearly, in real-time, how money and politics corrupts health regulators. This renders the current system totally defunct. This article in The Epoch Times reports how 65% of drug recommendations by the FDA are approved based on a single study. In the meantime doctors who want to promote lifestyle changes as first line treatment ahead of more dangerous interventions, find themselves increasingly working in a system opposed to them.
Trying to make an informed assessment of risks and benefits becomes almost impossible, once you realise how untrustworthy scientific literature has become. Or perhaps always was. ‘But it says so in the Lancet…’ Hopefully, many have now realised how empty this sentence sounds. Research outcomes are heavily influenced by the desires of those funding them, who just happen to be the ones manufacturing the drugs. This meme, whilst humorous, is worryingly accurate:
From statins to HRT, to proven-to-be-ineffective surgeries, to antidepressants, there is almost zero discussion in modern ‘medicine’ of preventative measures that do not benefit Big Pharma. Diet, exercise, breathing techniques, stress management, ensuring proper balance of micronutrients, enquiring about emotional and relationship causes of ill health. These should be the basic lines of enquiry for any competent physician, long before offering various magic bullets following the luxurious seven minute consultation via Zoom. GPs offering this paltry level of service are complicit in ensuring their own redundancy within a few short years. AI would serve just as well, the human factor having been almost entirely scrubbed out.
Most people with elderly parents know that they often need special plastic containers to house the numerous medications that they take on a daily basis. Often many of these drugs were added in sequence to deal with side effects (or more correctly, ‘effects’) of the medications that were introduced first. This close-to-the-bone satire that has been circulating online really sums it up:
“I took ASPIRIN for the headache caused by the ZYRTEC™ for the hay fever I got from the RELENZA™ for the upset stomach and flu-like symptoms caused by the VIAGRA™ for the erectile dysfunction from the PROPECIA™ for the hair loss caused by the RITALIN™ for my short attention span caused by the SCOPODERM TTS™ for the motion sickness that I got from the LOMOTIL™ for the diarrhoea caused by the XENICAL™ for the weight gain caused by the PAXIL™ for the anxiety that I got from the ZOCOR™ that I’m taking for my high cholesterol, because a good diet and exercise is just too much trouble.”
There seems to be the prevailing belief that human beings can only stay alive with constant interference from the medical profession. But what if the entire system keeps you sick, in order to retain you as a loyal customer to The Firm? What if much of the so-called ‘safety’ data are in fact just as flawed as those used to push the covid ‘vaccines’ in 2020? For those of us who became curious (suspicious?), we felt it might be worth having a retrospective look at other trends in medical diagnostics and treatments.
As it turns out, the more you look, the more you find…
Doing more harm than good?
A deep dive into questionable drugs and surgical practices that are built into standard protocols here in the UK would fill a book. Maybe several books. That is beyond the scope of this article, however here are a few ‘top picks’ to get started:
- Statins: This has been allowed on occasion to seep into mainstream consciousness, but it is still worth reading the book written by Dr Malcolm Kendrick, entitled The Great Cholesterol Con. There is simply no good evidence for the widespread use of statins. The notion that they don’t have harmful effects is also nonsense. A 17-year study on the elderly showed that low serum cholesterol was associated with increased frailty, accelerated mental decline, and early death. This should get any sensible clinician asking questions about what effects deliberately lowering it might have on long-term health. During ward rounds one senior consultant says to his juniors, ‘let’s stop this wonder drug’, scoring it off the prescription list. The juniors ask why he calls it that, to which he replies ‘I wonder what use it is!’
- SSRIs: a growing number of studies show they are less effective than thought. Has this resulted in a decline in prescriptions? Of course not. In fact psychiatry in general is an area that many medics describe as barbaric. The links between gut and brain health are now widely accepted and yet almost no money goes into mainstream R&D in this area. Cures are simply not as profitable as life-long customers.
- HRT: There is evidence for an increased risk of blood clots and stroke as well as an increased risk of breast and ovarian cancer in women using HRT. In researching this article and questioning women who had recently started on these drugs, most had not been adequately informed as to any associated risks. Many had no idea what kind of HRT they were even taking. This shows the level of blind faith people still have in a system that, judging by the history of criminal fines paid out, does not have a very good track record, to say the least.
- Angioplasty: For decades, we were led to believe that angioplasties are an effective treatment for not only angina (chest pain) but also served as protection from a heart attack. Now, the evidence seems to point to the procedure being ‘useless’ or even worse than useless. Lifestyle and diet changes are more effective and have the capacity to reverse the progression of coronary heart disease. This hardly seems like rocket science but somehow has taken decades to ‘realise’.
- Childhood Vaccinations: or as we like to call them, The Sacred Cows. Daring to even utter the words that these interventions may carry risks as well as benefits, or pointing out that there are no long-term safety studies using a genuine placebo, seems to create an allergic reaction in even the most sceptical of folks. However, at HART the adage ‘everything is back on the table’ is one we hold dear. Many people who now have the appetite to question The Science™ are quietly murmuring the name of the book Turtles All the Way Down. Perhaps it is worth reading, just to know what the alternative view point is. We do not need protection from theories. We need them to be aired and debated, so we can reach full and informed decisions. No topic should be out of bounds, including this one. Perhaps especially this one.
This list could go on ad infinitum, but instead we will end with a list of suggestions given by various practising medics when asked about drugs or interventions that they question. Once again, we point out that people are individuals. Protocols are not good for individuals. Do your research, take responsibility and remember that The Experts may have their hands tied firmly behind their back by The Money.
List of drugs with questionable efficacy/safety from currently prescribing doctors:
- Dementia drugs: noted poor efficacy, serious side-effects;
- Anticoagulants: should be used more judiciously due to risks of bleeds after falls;
- Bisphosphonates: this drug for osteoporosis has notoriously bad side effects, and shows questionable efficacy;
- Benzodiazepines and other so-called ‘Z’ drugs (zopiclone, eszopiclone, zaleplon and zolpidem): habit forming with evidence of severe side effects such as dementia, infections, respiratory disease exacerbation, pancreatitis, and cancer. They cause severe withdrawal symptoms;
- Gliflozins: the new ‘wonder drugs’ used in diabetes and heart failure. Concerns about kidney damage and they come with no long-term safety profile;
- GLP-1 agonist injectables: originally marketed for diabetes, now being sold as weight loss drugs. Concerns over risks of thyroid and pancreatic cancer and can cause pancreatitis;
- Psychiatric drugs in general. Recommended reading: Toxic Psychiatry by Peter Breggin;
- Antivirals: For example Tamiflu, which is now labelled a ‘fiasco’. The drug caused severe side effects such as hallucinations, self-injury, abnormal behaviour and renal impairment;
- Proton Pump Inhibitors (PPIs): evidence of major side effects with long-term use, including dementia, chronic kidney disease and increased cancer risk;
- Beta Blockers: evidence that long-term use is not associated with improved cardiovascular outcomes, with considerable side effects, such as depression and fatigue;
- Anti-arthritis drugs: Overuse of NSAIDs in particular can cause bleeding, heart attack, stroke, and renal damage.
To quote Aldous Huxley: ‘Medical science is making such remarkable progress that soon none of us will be well’.
A New Covid ‘Variant’… Just in Time for Election Season!
By Ron Paul | August 28, 2023
Just four and a half months since President Biden declared an end to the Covid “emergency,” the media is suddenly full of stories about the return of Covid. This time a new “variant” is being rolled out and the media, in collusion with big Pharma and the fear-industrial complex, are churning out stories about how forced masking is making a comeback.
Also, the “unvaccinated” are again to be denied basic human rights in the name of fighting a virus that the vaccine demonstrably does not protect against.
In short, they are desperately trying to revive the tyranny, insanity, and utter irrationality of the two-year Covid scare. And they are pretending none of us remembers how they destroyed society with their lockdowns, mask mandates, and vaccine mandates. They are hoping that none of us will remember the suicides, lost jobs, broken marriages, increased alcoholism and drug abuse, and the rest of what went along with the world’s experiment with global lockdown.
Even Fauci himself is back – like a moth drawn to the light of publicity. Despite all the scientific evidence that the lockdowns were a disaster, that they did far more harm than good, Fauci has re-emerged with his trademark arrogance and claimed that they were the right thing to do and should be done again if that’s what it takes to force people to take the vaccine. A vaccine that does not work.
They won’t even allow us to mention the spike in all-around mortality or the millions who may have been vaccine-injured the first time around. They want us to think that 20-year-old world-class athletes have always just dropped dead of heart attacks out of the blue. It’s all normal! Don’t question it! What are you, some kind of conspiracy theorist? Are you a science-denier?
Yes, look for a renewal of all those old hollow phrases used to attack those of us who can see with our own eyes and hear with our own ears. Their slogans are meant to silence any debate. The same “experts” like Fauci who claimed “I am the science” are back and they shamelessly demand to silence us again.
The big question is… why? Why are they doing this and how do they think they can get away with it a second time? One reason they believe they can get away with it again is that no one has ever been punished for what they did the first time. The Federal Government made sure that the pharmaceutical companies would not be liable for vaccine damages.
The public figures who openly became monsters, demanding the unvaccinated be drummed out of society and maybe even off the face of the earth have not been shamed or shunned. Politicians who displayed cowardice and worse have not been voted out of office for their treachery.
Why are they coming back around for another round of Covid tyranny? Fear is a weapon to gain control. Last time around they generated fear to radically change how America voted. Suddenly everyone was mailed ballots. How closely were they checked? No one knew and no one dared ask. The people who did ask about the election are now facing jail terms.
They want us to shut up while they do it again. Will we?
Copyright © 2023 by RonPaul Institute
Pfizer drip feeds data from its pregnancy trial of covid-19 vaccine
Analysis of the data so far shows the trial was underpowered, poorly designed and incomplete
BY MARYANNE DEMASI, PHD | AUGUST 24, 2023
In January 2021, in the absence of any human data in pregnancy, the CDC stated on its website that mRNA vaccines were “unlikely to pose a specific risk for people who are pregnant.”
Former CDC director Rochelle Walensky backed it up with a full-throated endorsement of covid-19 vaccination in pregnancy.
“There is no bad time to get vaccinated,” said Walensky.
“Get vaccinated while you’re thinking about having a baby, while you’re pregnant with your baby or after you’ve delivered your baby,” she added.
Behind the scenes however, Pfizer was scrambling to conduct a clinical trial of its vaccine in pregnant women.
By February 2022, Pfizer revealed it still did “not yet have a complete data set.” Its statement read:
“The environment changed during 2021 and by September 2021, COVID-19 vaccines were recommended by applicable recommending bodies (e.g., ACIP in the U.S.) for pregnant women in all participating/planned countries, and as a result the enrollment rate declined significantly.”
This month, Pfizer finally posted some trial results on clinicaltrials.gov.
The data do not appear in a peer-reviewed journal or a pre-print, nor has it been submitted to the FDA for evaluation.
I spoke with experts who have analysed the data with a fine-tooth comb and made some alarming observations.
Pfizer originally planned to recruit 4000 healthy women aged 18 or older who were 24 to 34 weeks pregnant. Half would be randomised to the vaccine and the other half to a saline placebo.
The efficacy and safety of the vaccine would be determined by assessing covid-19 cases, antibody responses, and adverse events.
Peculiarly, Pfizer planned to vaccinate all the mothers in the placebo group, one month after giving birth to their babies.
Retsef Levi, a professor at the Massachusetts Institute of Technology Sloan School of Management said that vaccinating mothers in the placebo group during the assessment period would introduce a new variable into the experiment and “corrupt” the data.
“We now know that mRNA from the vaccine is detected in the breast milk, so those babies born from mothers who were all vaccinated after giving birth, are also potentially exposed to mRNA through breastfeeding,” explained Levi.
“This corrupts the comparison of the two groups of babies because you don’t have a true control group anymore,” he added.
Less than 10% of the originally planned 4000 study participants ended up in the trial.
“Only 348 women were recruited – 174 in each arm – meaning that the trial was never going to have the statistical power, particularly when analysing potential harms,” said Levi.
Notably, study protocols indicate that Pfizer was given the green light as early as May 2021 by drug regulators to scale back the trial and reduce the sample size.
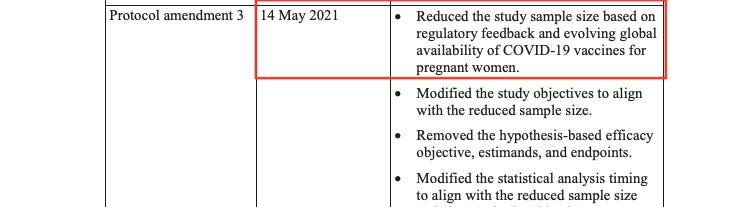
“To me, the wording in the protocol suggests that the FDA or another regulator basically gave Pfizer permission to do less,” remarked Levi.
“It’s not surprising though. The vaccine had already been recommended for pregnant women and many have taken it, so there is no upside to completing a trial that may detect signals of potential harms. It can only create problems for them, right?” he added.
Given that pregnant women were being vaccinated with a product that had not undergone rigorous safety testing in pregnancy, the FDA was asked if and why it allowed Pfizer to scale back the trial.
The FDA replied, “As a general matter, FDA does not comment on interactions it may or may not be having with sponsors about their clinical trials.”
Angela Spelsberg, an epidemiologist and medical director at the Comprehensive Cancer Center Aachen in Germany agreed that the integrity of the study had been compromised.
“There are just not enough babies in this trial to detect rare or very rare adverse events. We learned from studies in animals that lipid nanoparticles in the vaccine can deposit in many organs including the ovaries, so we must be extremely cautious about the potential negative impacts of the vaccine on reproductive health,” said Spelsberg.
“The scientific community urgently needs access to the pregnancy study data on the patient level for transparency and independent scrutiny of vaccine safety and efficacy because regulatory oversight is failing,” she added.
The small sample size may have been the result of the strict selection process.
Pfizer recruited participants with an impeccable pregnancy history, and most were in their third trimester (27-34 weeks gestation), a stage when the baby’s major development has already occurred.
“It appears that they cherry picked the mothers to get the best results,” said Levi. “We have no idea what impact this vaccine has on the early stages of development of an embryo or foetus, because all the women had advanced pregnancies when they were recruited.”
Spelsberg agreed.
“The first trimester is particularly vulnerable to adverse reproductive health outcomes,” she said.
“Based on only weak observational evidence, regulators have reassured the public that the vaccines are safe throughout pregnancy. However, we don’t have reliable evidence on the vaccine’s impact on miscarriages, malformation, foetal deaths, and maternal health risks because they excluded pregnant women from pivotal trials,” added Spelsberg.
Levi also noticed that “only partial data” were published.
“It doesn’t include any important metrics such as covid infections or antibody levels and its says we must wait until July 2024 for those results. It’s disturbing to say the least,” said Levi.
Also missing from the dataset was a full account of birth outcomes. Of the 348 women in the trial, Pfizer only reported on the birth of 335 live babies.
Of the 13 pregnancies unaccounted for, Pfizer reported one foetal death (stillbirth) in the vaccine group and the outcome of the other 12 pregnancies remains unknown.
“This is unacceptable,” said Levi. “Failing to report the outcome of 12 pregnancies could mask a potentially concerning signal of the vaccine in pregnancy. What happened to the babies, did they all die? Were their mothers vaccinated or unvaccinated?”
Finally, there were quite a few babies that were lost to follow-up in the trial.
“Twenty-nine babies in the placebo arm didn’t get to the end of the 6-month surveillance period, versus 15 babies in the vaccine arm. That’s almost double. Again, this is concerning and requires a detailed and transparent explanation,” said Levi.
Overall, both Levi and Spelsberg say the delays and failure to disclose vital data are unacceptable.
“Pfizer took a year to publish the data. When they finally did, it is incomplete. And we are expected to wait until July 2024 for the next batch of results, while authorities continue to recommend the vaccine in pregnant women,” said Levi.
“We still don’t have solid scientific evidence whether this vaccine is safe for pregnant women and their babies,” said Spelsberg. “It’s a tragedy and a scandal that vaccine use has been recommended, even mandated to women before, during and after pregnancy.”
Questions were put to Pfizer, but the company did not respond by the deadline.
Moderna is also conducting a clinical trial of its mRNA vaccine in pregnancy, but no data are available.
Clinical Rationale for SARS-CoV-2 Base Spike Protein Detoxification in Post COVID-19 and Vaccine Injury Syndromes
Publication of Baseline Protocol for Those Suffering from Long-COVID and Post-Acute Sequelae after COVID-19 Vaccination
By Peter A. McCullough | Courageous Discourse | August 27, 2023
For several weeks I have been messaging the scientific community and the public about an approach addressing the burden of SARS-CoV-2 Spike protein in tissues and organs in the human body that is largely responsible for post-COVID and vaccine injury syndromes.
No therapeutic claims can be made since large, prospective, double-blind randomized, placebo-controlled trials have not been completed on any of the compounds mentioned in this paper. I checked clinicaltrials.gov and no such trials have been planned. The Biden HHS US Action Plan for Long-COVID Research has pumped a billion dollars into long-COVID research and no new therapies have emerged. HHS, NIH, CDC, FDA have not recognized the larger issue of vaccine damage to the body.
At three and one half years into the pandemic and two and a half years into the COVID-19 vaccine debacle, myself and my clinic partners formulated a baseline regimen upon which additional drugs or agents can be added. We believe the Spike protein and the inflammation caused by it and its proteolytic fragments are at the heart of the pathophysiology we are observing.
We searched the literature for all available sources of evidence for products that can aid the human body in breaking down and catabolizing the Spike protein. We found two compounds, nattokinase and bromelain. Both of which additionally have fibrinolytic properties which are advantageous in the prothrombotic milieu induced by the persistent Spike protein. Curcumin was added for its anti-inflammatory properties in the setting of post-COVID and vaccine patients. The main safety caveats are bleeding and allergic reactions, both of which are manageable. It is our experience that both nattokinase and bromelain can be used in addition to antiplatelet and anticoagulant drugs with physician monitoring.
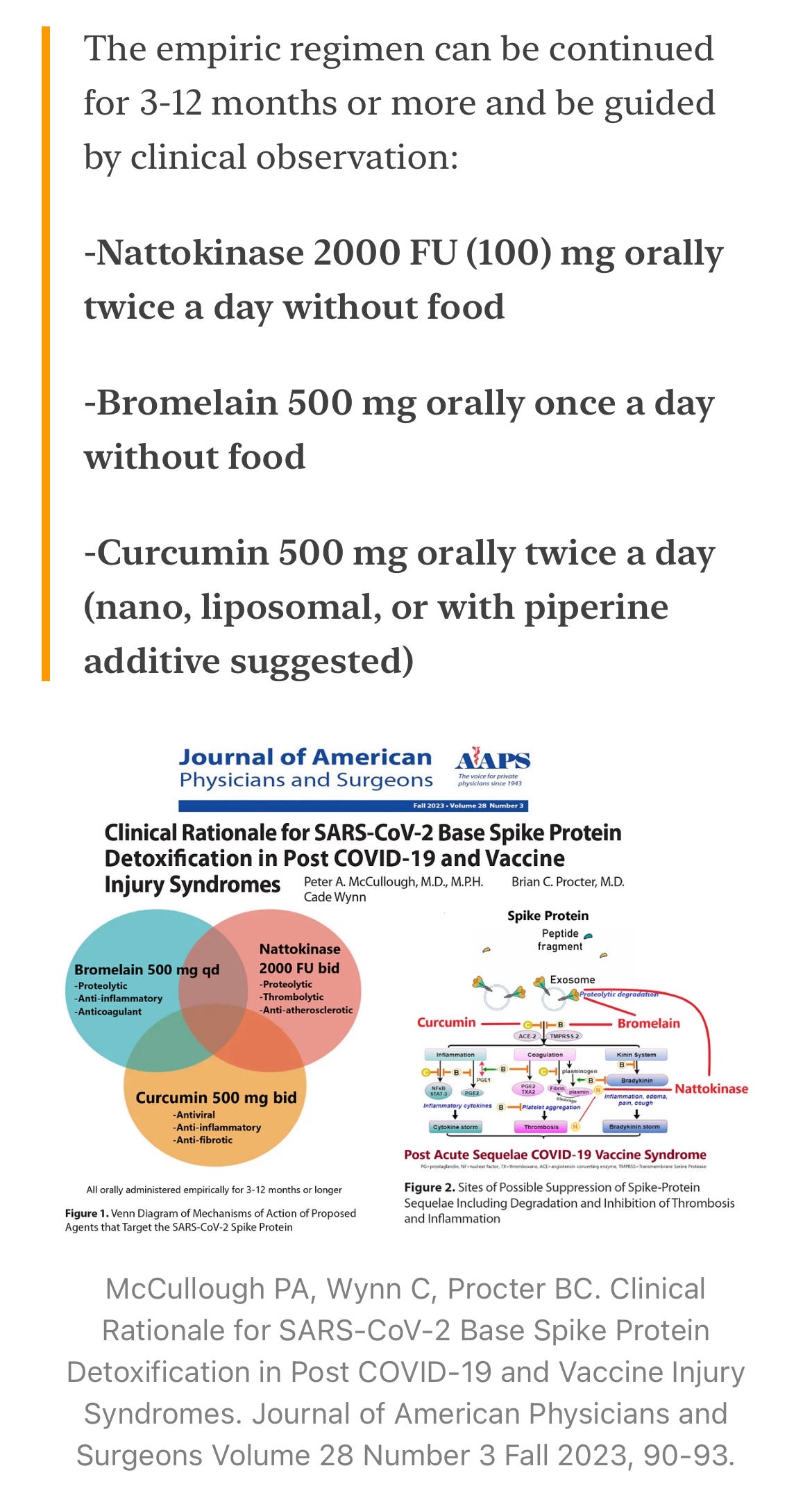
The empiric regimen can be continued for 3-12 months or more and be guided by clinical observation:
-Nattokinase 2000 FU (100) mg orally twice a day without food
-Bromelain 500 mg orally once a day without food
-Curcumin 500 mg orally twice a day (nano, liposomal, or with piperine additive suggested)
![]()
McCullough PA, Wynn C, Procter BC. Clinical Rationale for SARS-CoV-2 Base Spike Protein Detoxification in Post COVID-19 and Vaccine Injury Syndromes. Journal of American Physicians and Surgeons Volume 28 Number 3 Fall 2023, 90-93.
The full manuscript is linked and serves as your reference. While we are seeing case examples of improvement, we aim to collaborate with others as we did with the McCullough Protocol, to demonstrate clinical effectiveness of Base Spike Detoxification as a fundamental strategy for a large number of individuals who have suffered long-term consequences from SARS-CoV-2 infection and COVID-19 vaccination.
Deaths by Vaccination Status
Safe and Effective?
NAKED EMPEROR | AUGUST 25, 2023
The Office for National Statistics (ONS) have finally published their ‘Deaths by vaccination status, England’ dataset. This is for deaths occurring between 1 April 2021 and 31 May 2023.
I know many people consider these data unreliable but I always have a look at it nevertheless.
To assess whether the vaccine is safe I decided to look at all cause deaths separated by vaccine status (Table 5). This shows the number of all cause deaths for the unvaccinated and ‘ever vaccinated’ by month. It is also separated by age group (18-39; 40-49; 50-59; 60-69; 70-79; 80-89 & 90+).
For each month I looked at the total number of deaths and calculated what percentage of those deaths were in the ‘ever vaccinated’ category. So if there were 30 unvaccinated deaths and 70 vaccinated deaths, the percentage of ‘ever vaccinated’ deaths would be 70%.
This doesn’t really tell us anything, however. The headline might be shocking, e.g. ‘90% of deaths occurring in the vaccinated’ but if 90% of the population are vaccinated then that is to be expected.
However, if a higher percentage of deaths are occurring in the vaccinated (than the percentage of people vaccinated), then perhaps the vaccines are causing some harm. There are many confounders which confuse things but it is at least a signal that something is up and should be looked at. For example if 90% of the country is vaccinated but 95% of deaths are in the vaccinated then perhaps the vaccine is causing the additional 5% of deaths.
So, I took the data showing the percentage of people vaccinated with at least one dose from the UK government website, cleaned it up so that it matched the ONS formatting and created a few graphs.
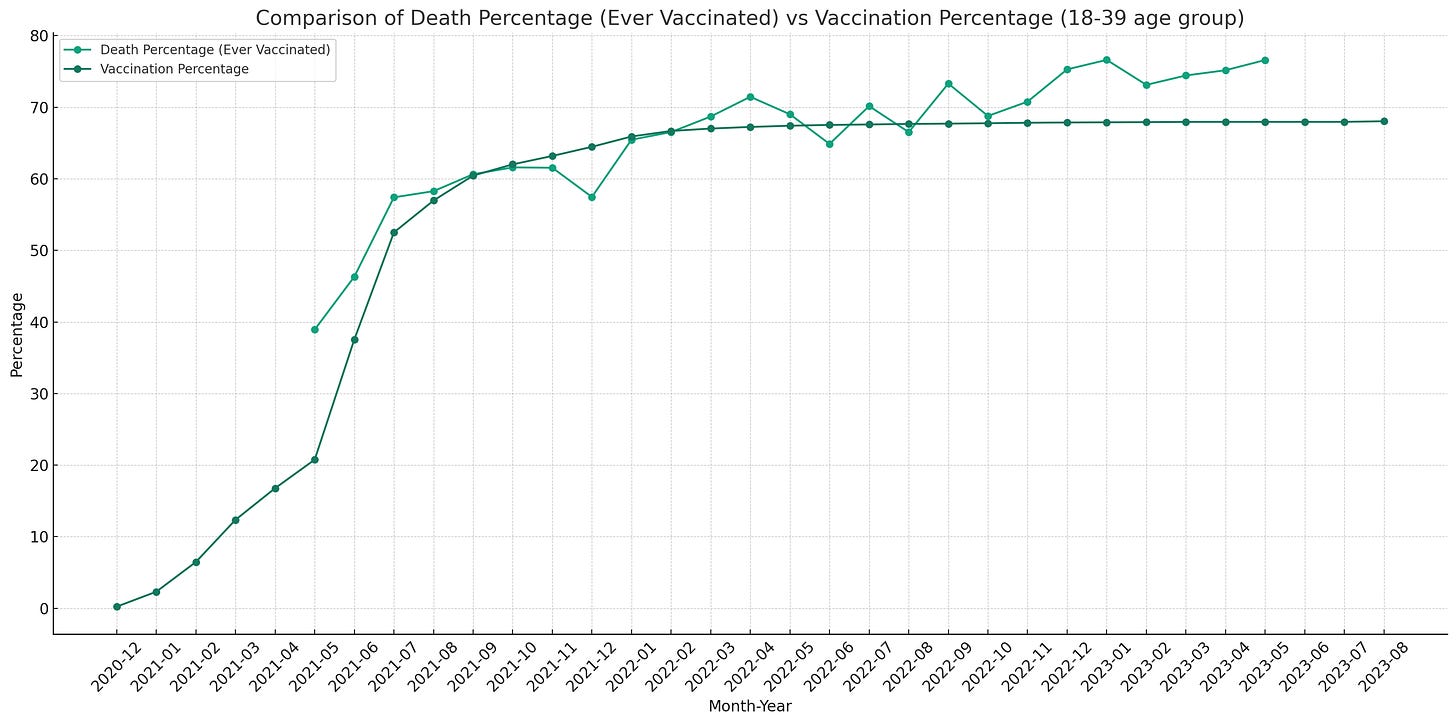
You can see that in the 18-39 age group, as the vaccine rollout started, there was a higher percentage of deaths in the vaccinated versus the number of people vaccinated. This may have been because sick or immunocompromised people were vaccinated first. The two percentages then quickly merged before beginning to separate again in mid 2022.
This is also the exact time when excess deaths began to skyrocket. Ever since that point, the percentage of deaths in the ‘ever vaccinated’ group has been higher than the percentage of people vaccinated.
Here are the graphs for the other age groups.

You can see that in all the age groups, except for the 50-59 year olds, the percentage of all cause deaths in the ‘ever vaccinated’ group is higher than the percentage of that group that is vaccinated. The data for the 80-89 and 90+ groups are particularly shocking.
Worthy of an investigation? Of course not. Instead the NHS is launching a £50,000 probe to uncover why NHS staff aren’t getting Covid and flu jabs. Probably because they can see the data presented above with their own eyes.
NEW VARIANTS TRIGGER CALLS FOR RETURN TO LOCKDOWNS
The Highwire with Del Bigtree | August 24, 2023
Mass media is calling for the reinstitution of COVID restrictions due to new variants, with no conversation about the efficacy or the harm they’ve caused. Jefferey Jaxen connects all the dots, which appears to be pointing to a Pandemic 2.0.
Featured Video
Chinese jet fuel and the myth of energy independence
or go to
Aletho News Archives – Video-Images
From the Archives
The Dirty Little Secret behind the “Global Terrorism Index”
The Omission of Israeli Terrorism in the Occupied Palestinian Territories
By Karin Brothers | Global Research | December 6, 2014
… The Israeli settlements — all of which are illegal – have been identified as a major impediment to peace. The refusal of a major “global” terrorism report to name the Israeli settlers as one of the groups most responsible for terrorism not only misrepresents a major source of regional violence but exposes the Global Terrorism Index as a propaganda tool that supports a U.S. agenda.
In recent years, governments have been attempting to thwart terrorism by blocking supportive fund-raising. When it comes to Israeli settlements, however, the US and Canada actually encourage fund-raising by giving organizations (such as Christian Friends of Israeli Communities (CFOIC) and the Jewish National Fund) financial support in the form of donor tax-deductions.
Charities which provide funds for the Israeli settlements should be regarded as terror-financing organizations. They should not only lose their tax-deductible status, but they should be banned because they support the violation of international humanitarian law. The terror-financing laws that are being strictly enforced for Muslim charities should be applied to Christian and Jewish charities as well. … Read full article
Blog Roll
 Aletho News
Aletho News- Chinese jet fuel and the myth of energy independence
- Ukraine Sea Drone Fired From Libya Hit Russian Tanker in Mediterranean
- IRGC: Iranian forces launched no attacks during ceasefire hours
- Trump Administration Moves To Automate U.S. Military Draft Registration
- Spain orders reopening of Tehran embassy, condemns Israel’s carpet bombing of Lebanon
- Israel faces ‘unsustainable’ strategic crisis following 40-day war against Iran: Analyst
- Iran restricts Hormuz access to 15 vessels per day under ceasefire terms: Report
- The ‘Opposition Party’ Has Done Nothing to Stop the Iran War and Much to Goad Trump Into Continuing It
- Moscow backs Tehran on status of Lebanon in US-Iran deal
- How UK Regulator Ofcom Quietly Bypassed International Law to Police American Speech
- If Americans Knew
- Amnesty: Urgent – Protect Lebanese civilians from brutal escalation in Israeli attacks
- Is The War Against Iran Over?
- Inside the Israeli army’s propaganda wing
- Hundreds of Gaza Amputees Stranded in Legal Limbo
- The gallows law: Israel moves toward executing Palestinian children
- Tucker Carlson: The Path to Peace requires ending ‘special alliance’ with Israel
- This is ceasefire? Israel’s biggest massacre yet in Lebanon, another journalist killed in Gaza – Daily Update
- Tucker Carlson on Israel: This Is the Behavior of an Ally? Really?
- Gazans face a triple crisis: severe shortages of water and bread, healthcare in tatters
- NY Times reports how Netanyahu took the US into Iran War
- No Tricks Zone
- An Inconvenient Tree: Uncovered In Alps… Europe Much Warmer Than Today 6000 Years Ago
- New Study Reports A 60% Slowdown In Greenland’s Ice Loss Rate In The Last Decade
- Low Intensity Tornado Wrecks Major Solar Farm, Creating A Potential Toxic Dump
- New Study Finds Warming Saves Lives…Cold Temperatures 12 Times More Deadly Than Excess Heat
- German Science Blog Accuses PIK Climate Institute Of Hallucinating Climate Tipping Points
- Devastating Assessment Of Comirnaty Vaccine By Former Senior Pfizer Europe Toxicologist
- New Study: CO2 Is ‘Effectively Negligible’ As An Explanatory Climate Change Factor Since 2000
- Former Pfizer Toxicologist Dr. Helmut Sterz Tells Bundestag Hearing Pfizer Vaccine Should Have Never Been Approved
- Energy Expert: Germany’s Nuclear Phaseout Was A “500 Billion Euro Mistake”
- New Research: South Australia’s Mid-Holocene Sea Surface Temperatures Were 4°C Warmer Than Today
