Texas Medical Doctors Testify Before State Senate to Oppose Mandatory COVID Shots
By Brian Shilhavy | Health Impact News | May 8, 2021
This past week the Texas Senate Committee on State Affairs took testimony from Texas physicians regarding SB 1669: Stop Forced Vaccination and Vaccine Passports in Texas.
SB 1669 was sponsored by Senator Bob Hall.

You can learn more about this bill at the National Vaccine Information Center’s Advocacy Portal (registration required.)
Here is some of the text provided to the public regarding Senate Bill 1669:
Contact your Texas State Legislators and Demand No Forced Vaccination, No Vaccine Passports, No Exceptions – Support SB 1669
Mandated vaccination in Texas with COVID-19 vaccines will be the reality unless the legislature takes decisive action now. In fact, it has already started happening.
Houston Methodist Hospital has told its 26,000 employees to get vaccinated by June 7th or get fired. Atria Senior Living, which has 16 facilities in Texas, is requiring all employees to receive 2 COVID-19 vaccines by May 1, 2021 as a condition of employment or face termination.
The city of Farmer’s Branch, Texas is requiring COVID-19 vaccination to access the city run facility called The Branch Connection. Forget taking a cruise with Royal Caribbean from Texas unless you’ve been COVID-19 vaccinated. St. Edwards University in Austin became one of the first colleges to mandate COVID-19 vaccines.
This is just the beginning.
Governor Abbott’s Executive Order Prohibiting COVID-19 Vaccine Passports Falls Short at Protection
Texas Governor Greg Abbott has been quoted saying that in Texas, COVID-19 vaccines “are always voluntary and never forced.”
The truth is Executive Order GA 35 falls short at preserving the right of law-abiding Texas citizens to be able to function normally in society without having to show proof of a COVID-19 vaccination.
EO GA 35 only prohibits the government, or public or private entities funded by the government, from requiring documentation of an individual’s COVID-19 vaccination status. This does nothing to prohibit businesses not receiving government funding from banning customers who don’t have a COVID-19 vaccine. Also, this executive order fails to give any protection to employees whose employers are requiring COVID-19 vaccination as a condition of employment.
In addition, the limited protections offered in EO GA 35 will be short lived because the order only applies to “Emergency Use Authorization” (EUA) COVID-19 vaccines. Once a vaccine has received full FDA approval, the EUA designation no longer applies and therefore neither will any protection in this executive order including the ban on forced vaccination by the government. Full FDA approval will be soon. Moderna, the manufacture of one of the 3 available COVID-19 vaccines, is already seeking full FDA approval, and Pfizer, one of the other manufacturers, announced it would seek full approval in the first half of 2021.
Governor Abbott’s executive order also falls short when compared to Florida Governor Ron DeSantis’s executive order banning vaccines passports which additionally prohibits all business from requiring COVID-19 vaccination status or post infection recovery status to gain access to or service from the business, and it applies to all COVID-19 vaccines instead of expiring after full FDA approval is achieved. It also protects personal privacy rights by prohibiting the government from publishing or sharing a person’s COVID-19 vaccination status to third parties.
Texans Need a Law Passed to Protect them From Forced Vaccination and Vaccine Passports (If you want to immediately see what you can do to help pass SB 1669 into law in Texas scroll down to “Action Needed)”
We are grateful to announce that Texas history has been made with the filing of
SB 1669 in the Texas Legislature by Senator Bob Hall.SB 1669 prohibits discrimination or segregation based on vaccination or immune status and prohibits forced vaccination in all areas of your life.
We need your help getting SB 1669 moving as the bill is currently stalled awaiting a hearing in the Senate State Affairs Committee. Legislators need to be educated about the shortcomings in Governor Abbott’s executive order and the vulnerabilities for mandated vaccination in Texas based on current law so they can pass this bill or amend parts of it onto other bills.
This is by far the most comprehensive bill prohibiting mandated vaccination in all areas that could affect your life including government orders, employment, healthcare, education, access to businesses, access to events and venues like sports and concerts, long-term care, nursing homes, insurance, and childcare.
Read more at the National Vaccine Information Center’s Advocacy Portal.
Senator Bob Hall, in his opening statements at the Senate hearing this week stated:
The chief responsibility and Constitutional role of our government is to protect the rights of the individual. Employees can take off their helmets, masks, and uniforms at the end of the work day, but they cannot remove a vaccine.

Dr. Richard Bartlett was the first physician to testify in favor of SB 1669 to Stop Forced Vaccination and Vaccine Passports in Texas.
Dr. Bartlett has over 28 years of medical practice experience and is a veteran primary care and emergency room doctor in West Texas.
Dr. Bartlett is best known since the COVID crisis started as a doctor who has cured many patients using an older, already FDA approved drug, called budesonide, which is an inhaled corticosteroid. (Learn more here.)
During his testimony, Dr. Bartlett explained that there are existing treatments already available to treat COVID patients, making it unnecessary to mandate experimental new “vaccines.”
He pointed to a recent Oxford University study just published that showed 90% success rate in using inhaled budesonide with COVID patients in preventing long-term care or hospitalization.
From the Oxford study:
The STOIC study found that inhaled budesonide given to patients with COVID-19 within seven days of the onset of symptoms also reduced recovery time. Budesonide is a corticosteroid used in the long-term management of asthma and chronic obstructive pulmonary disease (COPD).
Findings from the phase 2 randomised study, which was supported by the NIHR Oxford Biomedical Research Centre (BRC), were published on the medRxiv pre-print server.
The findings from 146 people – of whom half took 800 micrograms of the medication twice a day and half were on usual care – suggests that inhaled budesonide reduced the relative risk of requiring urgent care or hospitalisation by 90% in the 28-day study period. Participants allocated the budesonide inhaler also had a quicker resolution of fever, symptoms and fewer persistent symptoms after 28 days. (Source.)
Dr. Bartlett works in the Emergency Room, and he stated that there are very few patients coming in now with COVID, but “I am now seeing more people come in (to the ER) who are having complications from the COVID shot.”
And Dr. Bartlett points out that these are mostly younger people who were in excellent health before the shot, since Dr. Bartlett works in Lubbock, Texas, which is a college town.

Dr. Ben Edwards of Veritas Medical in Lubbock, Texas, was the next physician to give testimony in favor of SB 1669 to Stop Forced Vaccination and Vaccine Passports in Texas.
Dr. Edwards received his degree from Baylor University, and later graduated from UT-Houston Medical School. He moved to Waco to complete his training at the Waco Family Practice Residency Program where he was Chief Resident. He now operates three clinics in West Texas.
Dr. Edwards stated his concern that “the forced and coerced COVID-19 vaccinations would, in my opinion, be a violation of the Nuremberg Code,” as well as several other international codes on bioethics and human rights.
He cited the fact that the CDC is now reporting 4,178 deaths reported to VAERS, while for the previous 20 years combined there were 4,182 deaths recorded from all vaccines.
He also pointed out that a Harvard Study has previously estimated that only about 1% of all adverse reactions to vaccines are ever reported to VAERS. Two other subsequent studies showed the same thing.
In his own practice, Dr. Edwards stated that he has received “numerous reports within hours of receiving the COVID vaccines that people have suffered strokes, heart attacks, pulmonary embolisms (blood clots), and sudden death.”
Dr. Edwards went on to cite research which shows that those with natural immunity to COVID (they already had it) will see a 2 to 3 fold increase risk of adverse reactions from the COVID shots.
Over half of Texans now have this natural immunity. He stated:
On a personal note, I believe that God gave us an amazingly robust immune system, and I don’t think you can improve on God.

The next physician to testify in favor of SB 1669 to Stop Forced Vaccination and Vaccine Passports in Texas was Dr. Amy Offutt from St. Marble Falls, TX.
Dr. Offutt is trained in Integrative Medicine. She was recently appointed by Governor Greg Abbott to the Pediatric Acute-Onset Neuropsychiatric Syndrome Advisory Council. In addition, she serves on the Board of Directors for ILADS (International Lyme and Associated Diseases Society).
Dr. Offutt is another physician who has been successfully treating COVID patients with existing early treatment protocols.
She testified:
As of last Friday, my practice has treated 579 acutely ill patients as old as 98 years of age, with only ten hospitalizations and one dead.
The man who died presented on the 12th day of illness was a transplant patient and had already been to the ER multiple times before seeking care from us. This was such an unnecessary tragedy.
Dr. Offutt believes that “informed consent is the core to shared decision making in medicine.”

The next physician to testify in favor of SB 1669 to Stop Forced Vaccination and Vaccine Passports in Texas was Dr. Angelina Farella from Webster, TX.
Dr. Farella is a pediatrician with over 25 years experience. She started out her testimony to the Senate Committee by stating:
I am here today to protect our children in Texas. This is a very scary situation that we are in right now.
Dr. Farella stated that as a pediatrician she has given out tens of thousands of vaccines, and that she is not “anti-vaccine,” but:
I am against this COVID vaccine, if we can even call it that (a vaccine.)
What we are doing to our children with this vaccine is actually criminal.
All of these physicians are “frontline physicians” who actually treat patients, but their clinical experiences in treating COVID patients is being censored by the corporate media, and ignored by the government and Big Pharma, in favor mass vaccination instead.
Here is their testimony. This is from our Rumble Channel, and it is also on our Bitchute Channel.
Facebook Has Deleted The Richie Allen Show Page

By Richie Allen | May 8, 2021
Facebook deleted The Richie Allen Show page overnight. There was no warning. The page had been managed by a friend of mine as I haven’t had a personal Facebook account for a few years.
I had my pals login details, so I could go in and post the recording of each day’s radio show. Rodge (my mate) rarely posted. When he did, it was to remind you that the show was about to start, or when I was on holiday, to remind you why I was away.
I’ve only ever posted the show on there and recently, articles from this website. Three months ago, Facebook emailed Rodge to say that the visibility of the page would be severely restricted, because the page was posting fake news. This was nonsense, but I didn’t care.
In the radio show, I interview academics and journalists who have been effectively banned from the media. In the articles, I report what these people are saying. The fake news claim is pathetic. I am a journalist and I hold myself to the highest standard.
I make it crystal clear when I am offering an opinion. “That’s conjecture,” I say. When stating a fact, I offer empirical evidence to support the claim.
I couldn’t care less that Facebook has banned the page. I was going to close the page several years ago when I deleted my personal page. I despise Facebook, but Rodge compelled me to keep it open. He’s a good lad so I said go ahead.
You know me. I despise megalomaniacal truthers and attention seekers who use information and people as their props. The indy media is filled to the brim with celebrity wannabes. For me, the information has always been the star and a proper presenter should put the guest and the info ahead of him or her. I’m not important. I am a conduit.
So you’ll believe me when I tell you this. They’re coming for The Richie Allen Show and they’re coming fast. Every other week, the show is criticised in a national newspaper, either here or back home, not because of anything I have said or done, but because of some of the people I have hosted. I’m never offered right of reply.
Some weeks ago, Talk Radio presenter James Whale allowed some goon from an organisation called Hope Not Hate, free rein to smear me and my radio show. It went on for ten minutes. Whale, the gormless stooge, never challenged him.
When I politely Tweeted Whale to inquire as to when I’d be given right of reply, he blocked me. Astonishing stuff. I’d have been fired for doing that, in my time on commercial radio.
Three times last week, academics declined to come on the show. This has become more common over the last two years.
They’d all heard of me and two of them said they really appreciated the show, but still they declined. “Richie, I’ll get destroyed if I come on with you,” is a standard reply now.
Why is this happening? It’s all about the numbers. That makes me smile. Ian Collins, on his Talk Radio show, in reply to a listener who told him that he loved the Richie Allen Show, said that “it’s all about the numbers.”
You’re damn right it is Ian. My live show averages 150,000 listeners a night. Read that line again. Ok, so they’re not all in the UK. In the last 30 days, the show has had 248,864 unique listeners in 98 countries.
The Podcast is downloaded or streamed more than two million times a month.
There has never been a show like it. You know me. I ain’t boasting. I’m making a point.
They’re not going to stand for it. I’ve known this for some time, as has my friend and colleague Hayden Hewitt and FAB Radio’s Paul Ripley. We’ve discussed it. They won’t stand for a show with that kind of reach, featuring content that challenges the covid narrative or anything else for that matter.
I’ll keep doing it though. I have a state of the art radio studio and an independent stream. I have my website. I have friends like Paul Ripley, Hayden Hewitt, and you. They’re going to try and make it harder and harder for you to find me. But I’ll always be here.
Have a great weekend. Join me for the most chilled music show in radio tomorrow at 10am.
Over a dozen U.S. cities and counties are now pro-freedom ‘sanctuaries’ against COVID measures
LifeSiteNews – May 5, 2021
More than a dozen cities and counties in the United States are fighting COVID-19 restrictions by designating themselves pro-freedom “sanctuaries” or by simply refusing to enforce emergency orders.
The counties are primarily located in highly regulated states – like Michigan and California – that have suffered catastrophic economic and mental health impacts amid months of business closures and mask mandates.
Late last year, county commissioners in Campbell County, Virginia passed a “First Amendment Sanctuary” resolution, declaring that “(n)o Campbell County funds will be used to restrict the First Amendment.” No funding “shall be expended to aid federal or state agencies in the restriction of said rights,” it added.
“We’re not going to utilize county resources to enforce the governor’s orders,” a district representative from the county told local news. “We’re not going to aid the Virginia Department of Health in shutting our businesses down.”
At least nine other cities and counties have passed similar “sanctuary” designations, including Burrillville, Rhode Island, Delta County, Michigan, Kosciusko County, Carroll County and the city of Mooresville in Indiana, and multiple jurisdictions in California and Texas.
In Michigan’s Baraga County earlier this year, the county sheriff and other officials approved the “Baraga Manifesto,” slamming Gov. Gretchen Whitmer’s “clearly unconstitutional measures that treat human beings like herd animals.”
“Since March 10, 2020, the People of the State of Michigan have endured restrictions on their freedom which have not been seen in North America since the days of King George III and the American Revolution,” the officials wrote. “Enough is enough.”
“Accordingly, we hereby put the State of Michigan on NOTICE that we have no intention of participating in the unconstitutional destruction of our citizens’ economic security and Liberty,” they continued. “We further declare our intention to take no action whatsoever in furtherance of this terribly misguided agenda.” The manifesto echoes defiant local resolutions approved in Nebraska and Colorado.
At least one conservative county also has signaled its resistance to coronavirus vaccine mandates.
Assemblymen in Kenai Peninsula Borough, Alaska, passed a resolution in December stressing that the county supports vaccination on an “optional basis.” The statement, which passed 8-1, says that “the best interests of the state” are not served by mandating a vaccine that “many people are concerned… could potentially have serious harmful effects on themselves.”
State legislatures have pushed back against COVID-19 rules as well, with more than nine states enacting new restrictions of executives’ emergency powers or advancing vaccine passport bans since the start of the crisis.
Government Documents reveal how Brits have been manipulated into complying with Medical Tyranny
THE DAILY EXPOSE • MAY 6, 2021
The ordinary hard working people of the United Kingdom have been played. They have been manipulated and coerced into complying with medical fascism, thanks to the psychological warfare unleashed by the UK Government and its Scientific advisors every waking hour since March 2020.
The authority’s weapons have included the television, the radio, the newspapers. But their most important weapon in ensuring the general public have complied with dictatorial tyranny and offered themselves up as lab rats in the largest experiment to ever be conducted in human history, is a weapon that everyone reading this will know personally. Because that weapon has been you.
To understand just how the authorities have managed to manipulate and coerce the British people into complying with medical fascism we must go back to March 2020. It was at this point that Boris Johnson had one simple instruction for the British people, that instruction being that “you must stay at home”. Stay at home in order to protect the NHS and save lives. This was sold to the British people by informing them that the authorities needed just “three weeks to flatten the curve”. But those three weeks turned into six weeks. Then those six weeks turned into twelve weeks. Then those twelve weeks turned into twelve months, and still to this day the freedoms that were taken for granted prior to March 2020 do not seem within reach.
But how on earth have they managed to get away with it? Well we only need to delve into government documents which are readily available to the public, if they know how to find them. The first document we discovered is titled ‘Options for increasing adherence to social distancing measures’ and was published on the 22nd March 2020, one day prior to the announcement that the British people “must stay at home”.
This is one of the problems they felt they has in persuading people to social distance –
A substantial number of people still do not feel sufficiently personally threatened; it could be that they are reassured by the low death rate.
They were quite right, and are still quite right to be reassured by the low death rate, as statistics show that just 0.2% of those who develop the alleged Covid-19 disease tragically die. And even then the vast majority who do die are over the age of 85 and also have underlying conditions.
But that wouldn’t help to create the illusion of a problem if they couldn’t get people to social distance so here’s what the behavioural insight team advised the UK Government to do in response to this problem –
The perceived level of personal threat needs to be increased among those who are complacent, using hard-hitting emotional messaging. To be effective this must also empower people by making clear the actions they can take to reduce the threat.

‘Perceived’ is probably the most key word within that advice given to the UK Government on how to manipulate the British people. As this entire charade has been entirely about perception. If there was any level of personal threat then there would be no need to use hard hitting emotional messaging as people would already genuinely feel threatened. If there was truly something for the British people to be wary of then it would not need a mass media advertising campaign to make them aware of it.
But here’s an example of some of the ‘hard hitting emotional messaging’ used to manipulate the British people into complying with medical fascism –

“Don’t kill granny with the virus” warns Matt Hancock who blames spike in Covid cases on middle-class youth. This is just one example of many that have been used to increase the perceived level of personal threat.
But propaganda messages via the media weren’t enough on their own so that’s where the most vital weapon up the authorities sleeve came in – you. The ‘Options for increasing adherence to social distancing measures’ document has within it a section titled ‘Coercion’. No we’re not making it up, and this was one of the points made within that section –
Social disapproval from one’s community can play an important role in preventing anti-social behaviour or discouraging failure to enact pro-social behaviour, (therefore) consideration should be given to the use of social disapproval.

Those who fell for the propaganda and lies broadcast on every mainstream TV channel and radio station, and published in every mainstream newspaper have been the glue that has kept the destruction of life as we knew it together. Because they have policed the introduction of medical fascism for the authorities, and they don’t even realise that they have and are being used.
The document lists every single tactic used to ensure the British people complied with the loss of their rights and freedoms and these have included –
- Using media to increase the sense of personal threat
- Using media to increase the sense of responsibility to others
- Using and promoting social approval for desired behaviors
- Using social disapproval for those who do not comply


The document explains in full how they have managed to manipulate and coerce the British public into complying with medical fascism using psychological warfare. But how exactly are authorities going to keep up this charade now that the “miraculous” experimental vaccines are being rolled out across the country? How are they going to ensure the British people continue to comply with medical fascism now that the most vulnerable to this alleged disease have been vaccinated?
Well another document found on the Government website helps us to find the answer to that. The document is titled ‘Behavioural and social considerations when reducing restrictions’ and was released on the 10th February 2021. A document which essentially confirms the writing is on the wall for a return to normality and that the introduction of vaccine passports (freedom passes) is inevitable.
One of the points made in the document describes the issues that may arise as some interventions are lifted. With complications on messaging due to “differences across tiers” and “immunity or vaccination certificates providing exemptions” for those who are vaccinated to carry out or take part in certain activities.

Tiers? But Boris Johnson said we were going back to normal on the 21st June, why on earth would we need tiers? Because he’s a liar.
Another line in the document explains that another problem for the authorities in getting the British public to continue to comply with medical fascism is that “as perceptions of immunity grow, messaging may need to explain why continued adherence to specific protective measures is important”.

Why exactly will the British people need to continue to adhere to restrictions if they now have a miraculous experimental vaccine that will “save” them from Covid-19? After all the Health Secretary, Matt Hancock is constantly reminding us that “vaccination is our route back to normal”.
Well maybe the next part of the document can explain why, and it’s a card they have kept up their sleeve and are yet to really play, but we all know it is coming.
he document states that “17% of adults expect life to return to normal in six months or less. Modelling from SPI-M suggests this is optimistic. Additionally, the challenge of new variants may call for sudden, strict reimposition of measures”.

If you thought life was going back to normal on the 21st June then think again, it’s not in the script, quite the opposite is going to happen and we’ve just shown you the evidence in black and white.
A Third of All Recent ‘Covid Deaths’ in England and Wales Not Caused by Coronavirus
21st Century Wire | May 6, 2021

After a year of incessant fearmongering, fraudulent PCR testing and generally inflating its Covid numbers, new data analysis reveals how the government’s rampant statistical fraud still continues unabated, as increasing numbers of people whose underlying cause of death was not due coronavirus – are still being included in the government’s hallowed ‘death count.’
Despite this exposure, the mainstream media and government officials seem unwilling to acknowledge how this fundamental deception has been used as the underlying basis for nearly every single ‘public health’ measure – coming at an incalculable cost for those countries and societies placed under the yoke of so-called ‘virus mitigation’ policies.
The inflated Covid death numbers are then used by the government and media as a ‘moral trigger’ to impose rolling lockdowns, as well as other repressive and needless policies such as mask mandates, business and school closures, deregulated emergency vaccine roll-outs, and arbitrary non-science-based “social distancing” rules.
The UK Telegraph reports…
Nearly one third of recently registered Covid deaths in England and Wales are people who died primarily from other causes, the latest figures show.
Weekly death data from the Office for National Statistics (ONS) shows that, for nearly 33 per cent of people included in the overall coronavirus death figures, Covid was not an underlying cause of death but was merely mentioned on the death certificate.
The number of people who are not principally dying from Covid but are still being included in the official figures has been creeping up steadily as the pandemic has declined.
It had been running at around 10 per cent for most of the crisis but had risen to nearly a quarter by mid-April and is continuing to increase.
In the latest data, published on Wednesday, which records death registrations in the week ending April 23, some 260 deaths from Covid were recorded in England and Wales, but only 67.7 per cent (176) of those had the virus as an underlying cause.
COVID Vaccines: Necessity, Efficacy and Safety
Doctors for Covid Ethics | OffGuardian | May 5, 2021
This paper was originally hosted on the Doctors for Covid Ethics Medium account, but the platform censored the expert group and removed the paper, claiming the post was “under investigation”:

An archived version is still available here.
*
Abstract: COVID-19 vaccine manufacturers have been exempted from legal liability for vaccine-induced harm. It is therefore in the interests of all those authorising, enforcing and administering COVID-19 vaccinations to understand the evidence regarding the risks and benefits of these vaccines, since liability for harm will fall on them.
In short, the available evidence and science indicate that COVID-19 vaccines are unnecessary, ineffective and unsafe.
- Necessity: Immunocompetent individuals are protected against SARS-CoV-2 by cellular immunity. Vaccinating low-risk groups is therefore unnecessary. For immunocompromised individuals who do fall ill with COVID-19 there is a range of medical treatments that have been proven safe and effective. Vaccinating the vulnerable is therefore equally unnecessary. Both immunocompetent and vulnerable groups are better protected against variants of SARS-CoV-2 by naturally acquired immunity and by medication than by vaccination.
- Efficacy: Covid-19 vaccines lack a viable mechanism of action against SARS-CoV-2 infection of the airways. Induction of antibodies cannot prevent infection by an agent such as SARS-CoV-2 that invades through the respiratory tract. Moreover, none of the vaccine trials have provided any evidence that vaccination prevents transmission of the infection by vaccinated individuals; urging vaccination to “protect others” therefore has no basis in fact.
- Safety: The vaccines are dangerous to both healthy individuals and those with pre-existing chronic disease, for reasons such as the following: risk of lethal and non-lethal disruptions of blood clotting including bleeding disorders, thrombosis in the brain, stroke and heart attack; autoimmune and allergic reactions; antibody-dependent enhancement of disease; and vaccine impurities due to rushed manufacturing and unregulated production standards.
The risk-benefit calculus is therefore clear: the experimental vaccines are needless, ineffective and dangerous. Actors authorising, coercing or administering experimental COVID-19 vaccination are exposing populations and patients to serious, unnecessary, and unjustified medical risks.
1. THE VACCINES ARE UNNECESSARY
1. Multiple lines of research indicate that immunocompetent people display “robust” and lasting cellular (T cell) immunity to SARS-CoV viruses [1], including SARS-CoV-2 and its variants [2]. T cell protection stems not only from exposure to SARS-CoV-2 itself, but from cross-reactive immunity following previous exposure to common cold and SARS coronaviruses [1,3-10]. Such immunity was detectable after infections up to 17 years prior [1,3]. Therefore, immunocompetent people do not need vaccination against SARS-Cov-2.
2. Natural T-Cell immunity provides stronger and more comprehensive protection against all SARS-CoV-2 strains than vaccines, because naturally primed immunity recognises multiple virus epitopes and costimulatory signals, not merely a single (spike) protein. Thus, immunocompetent people are better protected against SARS-CoV-2 and any variants that may arise by their own immunity than by the current crop of vaccines.
3.The vaccines have been touted as a means to prevent asymptomatic infection [11], and by extension “asymptomatic transmission.” However, “asymptomatic transmission” is an artefact of invalid and unreliable PCR test procedures and interpretations, leading to high false-positive rates[12-15]. Evidence indicates that PCR-positive, asymptomatic people are healthy false-positives, not carriers. A comprehensive study of 9,899,828 people in China found that asymptomatic individuals testing positive for COVID-19 never infected others[16].
In contrast, the papers cited by the Centre for Disease Control[17,18] to justify claims of asymptomatic transmission are based on hypothetical models, not empirical studies; they present assumptions and estimates rather than evidence. Preventing asymptomatic infection is not a viable rationale for promoting vaccination of the general population.
4. In most countries, most people now have immunity to SARS-CoV-2[19]. Depending on their degree of previously acquired cross-immunity, they will have had no symptoms, mild and uncharacteristic symptoms, or more severe symptoms, possibly including anosmia (loss of sense of smell) or other somewhat characteristic signs of the COVID-19 disease. Regardless of disease severity, they will now have sufficient immunity to be protected from severe disease in the event of renewed exposure. This majority of the population will not benefit at all from being vaccinated.
5. Population survival of COVID-19 exceeds 99.8% globally[20-22]. In countries that have been intensely infected over several months, less than 0.2% of the population have died and had their deaths classified as ‘with covid19’. COVID-19 is also typically a mild to moderately severe illness. Therefore, the overwhelming majority of people are not at risk from COVID-19 and do not require vaccination for their own protection.
6. In those susceptible to severe infection, Covid-19 is a treatable illness. A convergence of evidence indicates that early treatment with existing drugs reduces hospitalisation and mortality by ~85% and 75%, respectively[23-27]. These drugs include many tried and true anti-inflammatory, antiviral, and anticoagulant medications, as well as monoclonal antibodies, zinc, and vitamins C and D.
Industry and government decisions to sideline such proven treatments through selective research support[24], regulatory bias, and even outright sanctions against doctors daring to use such treatments on their own initiative, have been out of step with existing laws, standard medical practice, and research; the legal requirement to consider real world evidence has fallen by the wayside[28].
The systematic denial and denigration of these effective therapies has underpinned the spurious justification for the emergency use authorisation of the vaccines, which requires that “no standard acceptable treatment is available”[29]. Plainly stated, vaccines are not necessary to prevent severe disease.
2. THE VACCINES LACK EFFICACY
1. At a mechanistic level, the concept of immunity to COVID-19 via antibody induction, as per COVID-19 vaccination, is medical nonsense. Airborne viruses such as SARS-CoV-2 enter the body via the airways and lungs, where antibody concentrations are too low to prevent infection. Vaccine-induced antibodies primarily circulate in the bloodstream, while concentrations on the mucous membranes of lungs and airways is low.
Given that COVID-19 primarily spreads and causes disease by infecting these mucous membranes, vaccines miss the immunological mark. The documents submitted by the vaccine manufacturers to the various regulatory bodies contain no evidence that vaccination prevents airway infection, which would be crucial for breaking the chain of transmission. Thus, vaccines are immunologically inappropriate for COVID-19.
2. Medium to long-term vaccine efficacy is unknown. Phase 3, medium-term, 24-month trials will not be complete until 2023: There is no medium-term or long term longitudinal data regarding COVID-19 vaccine efficacy.
3. Short term data has not established prevention of severe disease. The European Medicines Agency has noted of the Comirnaty (Pfizer mRNA) vaccine that severe COVID-19 cases “were rare in the study, and statistically certain conclusion cannot be drawn” from it[30]. Similarly, the Pfizer document submitted to the FDA[31] concludes that efficacy against mortality could not be demonstrated. Thus, the vaccines have not been shown to prevent death or severe disease even in the short term.
4. The correlates of protection against COVID-19 are unknown. Researchers have not yet established how to measure protection against COVID-19. As a result, efficacy studies are stabbing around in the dark. After completion of Phase 1 and 2 studies, for instance, a paper in the journal Vaccine noted that “without understanding the correlates of protection, it is impossible to currently address questions regarding vaccine-associated protection, risk of COVID-19 reinfection, herd immunity, and the possibility of elimination of SARS-CoV-2 from the human population”[32]. Thus, Vaccine efficacy cannot be evaluated because we have not yet established how to measure it.
3. THE VACCINES ARE DANGEROUS
1. Just as smoking could be and was predicted to cause lung cancer based on first principles, all gene-based vaccines can be expected to cause blood clotting and bleeding disorders [33], based on their molecular mechanisms of action. Consistent with this, diseases of this kind have been observed across age groups, leading to temporary vaccine suspensions around the world: The vaccines are not safe.
2. Contrary to claims that blood disorders post-vaccination are “rare”, many common vaccine side effects (headaches, nausea, vomiting and haematoma-like “rashes” over the body) may indicate thrombosis and other severe abnormalities. Moreover, vaccine-induced diffuse micro-thromboses in the lungs can mimic pneumonia and may be misdiagnosed as COVID-19. Clotting events currently receiving media attention are likely just the “tip of a huge iceberg”[34]: The vaccines are not safe.
3. Due to immunological priming, risks of clotting, bleeding and other adverse events can be expected to increase with each re-vaccination and each intervening coronavirus exposure. Over time, whether months or years[35], this renders both vaccination and coronaviruses dangerous to young and healthy age groups, for whom without vaccination COVID-19 poses no substantive risk. Since vaccine roll-out, COVID-19 incidence has risen in numerous areas with high vaccination rates[36-38].
Furthermore, multiple series of COVID-19 fatalities have occurred shortly after the onset vaccinations in senior homes[39,40]. These cases may have been due not only to antibody-dependent enhancement but also to a general immunosuppressive effect of the vaccines, which is suggested by the increased occurrence of Herpes zoster in certain patients[41].
Immunosuppression may have caused a previously asymptomatic infection to become clinically manifest. Regardless of the exact mechanism responsible for these reported deaths, we must expect that the vaccines will increase rather than decrease lethality of COVID-19 — the vaccines are not safe.
4. The vaccines are experimental by definition. They will remain in Phase 3 trials until 2023. Recipients are human subjects entitled to free informed consent under Nuremberg and other protections, including the Parliamentary Assembly of the Council of Europe’s resolution 2361[43] and the FDA’s terms of emergency use authorisation[29]. With respect to safety data from Phase 1 and 2 trials, in spite of initially large sample sizes the journal Vaccine reports that, “the vaccination strategy chosen for further development may have only been given to as few as 12 participants”[32].
With such extremely small sample sizes, the journal notes that, “larger Phase 3 studies conducted over longer periods of time will be necessary” to establish safety. The risks that remain to be evaluated in Phase 3 trials into 2023, with entire populations as subjects, include not only thrombosis and bleeding abnormalities, but other autoimmune responses, allergic reactions, unknown tropisms (tissue destinations) of lipid nanoparticles[35], antibody-dependent enhancement [43-46] and the impact of rushed, questionably executed, poorly regulated[47] and reportedly inconsistent manufacturing methods, conferring risks of potentially harmful impurities such as uncontrolled DNA residues[48]. The vaccines are not safe, either for recipients or for those who administer them or authorise their use.
5. Initial experience might suggest that the adenovirus-derived vaccines (AstraZeneca/Johnson & Johnson) cause graver adverse effects than the mRNA (Pfizer/Moderna) vaccines. However, upon repeated injection, the former will soon induce antibodies against the proteins of the adenovirus vector. These antibodies will then neutralize most of the vaccine virus particles and cause their disposal before they can infect any cells, thereby limiting the intensity of tissue damage.
In contrast, in the mRNA vaccines, there is no protein antigen for the antibodies to recognize. Thus, regardless of the existing degree of immunity, the vaccine mRNA is going to reach its target — the body cells. These will then express the spike protein and subsequently suffer the full onslaught of the immune system.
With the mRNA vaccines, the risk of severe adverse events is virtually guaranteed to increase with every successive injection. In the long term, they are therefore even more dangerous than the vector vaccines. Their apparent preferment over the latter is concerning in the highest degree; these vaccines are not safe.
4. ETHICS AND LEGAL POINTS TO CONSIDER
Conflicts of interest abound in the scientific literature and within organisations that recommend and promote vaccines, while demonising alternate strategies (reliance on natural immunity and early treatment). Authorities, doctors and medical personnel need to protect themselves by evaluating the sources of their information for conflicts of interest extremely closely.
Authorities, doctors and medical personnel need to be similarly careful not to ignore the credible and independent literature on vaccine necessity, safety and efficacy, given the foreseeable mass deaths and harms that must be expected unless the vaccination campaign is stopped.
Vaccine manufacturers have exempted themselves from legal liability for adverse events for a reason. When vaccine deaths and harms occur, liability will fall to those responsible for the vaccines’ authorisation, administration and/or coercion via vaccine passports, none of which can be justified on a sober, evidence-based risk-benefit analysis.
All political, regulatory and medical actors involved in COVID-19 vaccination should familiarise themselves with the Nuremberg code and other legal provisions in order to protect themselves.
References:
[1] Le Bert, N.; Tan, A.T.; Kunasegaran, K.; Tham, C.Y.L.; Hafezi, M.; Chia, A.; Chng, M.H.Y.; Lin, M.; Tan, N.; Linster, M.; Chia, W.N.; Chen, M.I.; Wang, L.; Ooi, E.E.; Kalimuddin, S.; Tambyah, P.A.; Low, J.G.; Tan, Y. and Bertoletti, A. (2020) SARS-CoV-2-specific T cell immunity in cases of COVID-19 and SARS, and uninfected controls. Nature 584:457–462. [back]
[2] Tarke, A.; Sidney, J.; Methot, N.; Zhang, Y.; Dan, J.M.; Goodwin, B.; Rubiro, P.; Sutherland, A.; da Silva Antunes, R.; Frazier, A. and al., e. (2021) Negligible impact of SARS-CoV-2 variants on CD4+ and CD8+ T cell reactivity in COVID-19 exposed donors and vaccinees. bioRxiv -:x-x.[back]
[3] Anonymous, (2020) Scientists uncover SARS-CoV-2-specific T cell immunity in recovered COVID-19 and SARS patients. [back]
[4] Beasley, D. (2020) Scientists focus on how immune system T cells fight coronavirus in absence of antibodies. Reuters, 10/07/2020. [back]
[5] Bozkus, C.C. (2020) SARS-CoV-2-specific T cells without antibodies. Nat. Rev. Immunol. 20:463. [back]
[6] Grifoni, A.; Weiskopf, D.; Ramirez, S.I.; Mateus, J.; Dan, J.M.; Moderbacher, C.R.; Rawlings, S.A.; Sutherland, A.; Premkumar, L.; Jadi, R.S. and al., e. (2020) Targets of T Cell Responses to SARS-CoV-2 Coronavirus in Humans with COVID-19 Disease and Unexposed Individuals. Cell 181:1489–1501.e15. [back]
[7] Mateus, J.; Grifoni, A.; Tarke, A.; Sidney, J.; Ramirez, S.I.; Dan, J.M.; Burger, Z.C.; Rawlings, S.A.; Smith, D.M.; Phillips, E. and al., e. (2020) Selective and cross-reactive SARS-CoV-2 T cell epitopes in unexposed humans. [back]Science 370:89–94. [back]
[8] McCurry-Schmidt, M. (2020) Exposure to common cold coronaviruses can teach the immune system to recognize SARS-CoV-2. La Jolla Institute for Immunology. [back]
[9] Palmer, S.; Cunniffe, N. and Donnelly, R. (2021) COVID-19 hospitalization rates rise exponentially with age, inversely proportional to thymic T-cell production. J. R. Soc. Interface 18:20200982. [back]
[10] Sekine, T.; Perez-Potti, A.; Rivera-Ballesteros, O.; Strålin, K.; Gorin, J.; Olsson, A.; Llewellyn-Lacey, S.; Kamal, H.; Bogdanovic, G.; Muschiol, S. and al., e. (2020) Robust T Cell Immunity in Convalescent Individuals with Asymptomatic or Mild COVID-19. Cell 183:158–168.e14. [back]
[11] Drake, J. (2021) Now We Know: Covid-19 Vaccines Prevent Asymptomatic Infection, Too.[back]
[12] Bossuyt, P.M. (2020) Testing COVID-19 tests faces methodological challenges. Journal of clinical epidemiology 126:172–176. [back]
[13] Jefferson, T.; Spencer, E.; Brassey, J. and Heneghan, C. (2020) Viral cultures for COVID-19 infectivity assessment. Systematic review. Clin. Infect. Dis. ciaa1764:x-x. [back]
[14] Borger, P.; Malhotra, R.K.; Yeadon, M.; Craig, C.; McKernan, K.; Steger, K.; McSheehy, P.; Angelova, L.; Franchi, F.; Binder, T.; Ullrich, H.; Ohashi, M.; Scoglio, S.; Doesburg-van Kleffens, M.; Gilbert, D.; Klement, R.J.; Schrüfer, R.; Pieksma, B.W.; Bonte, J.; Dalle Carbonare, B.H.; Corbett, K.P. and Kämmer, U. (2020) External peer review of the RTPCR test to detect SARS-CoV-2 reveals 10 major scientific flaws at the molecular and methodological level: consequences for false-positive results. [back]
[15] Mandavilli, A. (2020) Your Coronavirus Test Is Positive. Maybe It Shouldn’t Be.[back]
[16] Cao, S.; Gan, Y.; Wang, C.; Bachmann, M.; Wei, S.; Gong, J.; Huang, Y.; Wang, T.; Li, L.; Lu, K.; Jiang, H.; Gong, Y.; Xu, H.; Shen, X.; Tian, Q.; Lv, C.; Song, F.; Yin, X. and Lu, Z. (2020) Post-lockdown SARS-CoV-2 nucleic acid screening in nearly ten million residents of Wuhan, China. Nat. Commun. 11:5917.[back]
[17] Moghadas, S.M.; Fitzpatrick, M.C.; Sah, P.; Pandey, A.; Shoukat, A.; Singer, B.H. and Galvani, A.P. (2020) The implications of silent transmission for the control of COVID-19 outbreaks. Proc. Natl. Acad. Sci. U. S. A. 117:17513–17515.[back]
[18] Johansson, M.A.; Quandelacy, T.M.; Kada, S.; Prasad, P.V.; Steele, M.; Brooks, J.T.; Slayton, R.B.; Biggerstaff, M. and Butler, J.C. (2021) SARS-CoV-2 Transmission From People Without COVID-19 Symptoms. JAMA network open 4:e2035057.[back]
[19] Yeadon, M. (2020). What SAGE got wrong. Lockdown Skeptics.[back]
[20] Ioannidis, J.P.A. (2020) Global perspective of COVID‐19 epidemiology for a full‐cycle pandemic. Eur. J. Clin. Invest. 50:x-x. [back]
[21] Ioannidis, J.P.A. (2021) Reconciling estimates of global spread and infection fatality rates of COVID‐19: An overview of systematic evaluations. Eur. J. Clin. Invest. -:x-x. [back]
[22] CDC, (2020) Science Brief: Community Use of Cloth Masks to Control the Spread of SARS-CoV-2. [back]
[23] Orient, J.; McCullough, P. and Vliet, E. (2020) A Guide to Home-Based COVID Treatment. [back]
[24] McCullough, P.A.; Alexander, P.E.; Armstrong, R.; Arvinte, C.; Bain, A.F.; Bartlett, R.P.; Berkowitz, R.L.; Berry, A.C.; Borody, T.J.; Brewer, J.H.; Brufsky, A.M.; Clarke, T.; Derwand, R.; Eck, A.; Eck, J.; Eisner, R.A.; Fareed, G.C.; Farella, A.; Fonseca, S.N.S.; Geyer, C.E.; Gonnering, R.S.; Graves, K.E.; Gross, K.B.V.; Hazan, S.; Held, K.S.; Hight, H.T.; Immanuel, S.; Jacobs, M.M.; Ladapo, J.A.; Lee, L.H.; Littell, J.; Lozano, I.; Mangat, H.S.; Marble, B.; McKinnon, J.E.; Merritt, L.D.; Orient, J.M.; Oskoui, R.; Pompan, D.C.; Procter, B.C.; Prodromos, C.; Rajter, J.C.; Rajter, J.; Ram, C.V.S.; Rios, S.S.; Risch, H.A.; Robb, M.J.A.; Rutherford, M.; Scholz, M.; Singleton, M.M.; Tumlin, J.A.; Tyson, B.M.; Urso, R.G.; Victory, K.; Vliet, E.L.; Wax, C.M.; Wolkoff, A.G.; Wooll, V. and Zelenko, V. (2020) Multifaceted highly targeted sequential multidrug treatment of early ambulatory high-risk SARS-CoV-2 infection (COVID-19). Reviews in cardiovascular medicine 21:517–530. [back][back]
[25] Procter, {.B.C.; {APRN}, {.C.R.{.; {PA}-C, {.V.P.; {PA}-C, {.E.S.; {PA}-C, {.C.H. and McCullough, {.{.P.A. (2021) Early Ambulatory Multidrug Therapy Reduces Hospitalization and Death in High-Risk Patients with SARS-CoV-2 (COVID-19). International journal of innovative research in medical science 6:219–221. [back]
[26] McCullough, P.A.; Kelly, R.J.; Ruocco, G.; Lerma, E.; Tumlin, J.; Wheelan, K.R.; Katz, N.; Lepor, N.E.; Vijay, K.; Carter, H.; Singh, B.; McCullough, S.P.; Bhambi, B.K.; Palazzuoli, A.; De Ferrari, G.M.; Milligan, G.P.; Safder, T.; Tecson, K.M.; Wang, D.D.; McKinnon, J.E.; O’Neill, W.W.; Zervos, M. and Risch, H.A. (2021) Pathophysiological Basis and Rationale for Early Outpatient Treatment of SARS-CoV-2 (COVID-19) Infection. Am. J. Med. 134:16–22. [back]
[27] Anonymous, (2020) Real-time database and meta analysis of 588 COVID-19 studies. [back]
[28] Hirschhorn, J.S. (2021) COVID scandal: Feds ignored 2016 law requiring use of real world evidence.[back]
[29] Anonymous, (1998) Emergency Use of an Investigational Drug or Biologic: Guidance for Institutional Review Boards and Clinical Investigators. [back] [back]
[30] Anonymous, (2021) EMA assessment report: Comirnaty. [back]
[31] Anonymous, (2020) FDA briefing document: Pfizer-BioNTech COVID-19 Vaccine. [back]
[32] Giurgea, L.T. and Memoli, M.J. (2020) Navigating the Quagmire: Comparison and Interpretation of COVID-19 Vaccine Phase 1/2 Clinical Trials. Vaccines 8:746. [back][back]
[33] Bhakdi, S.; Chiesa, M.; Frost, S.; Griesz-Brisson, M.; Haditsch, M.; Hockertz, S.; Johnson, L.; Kämmerer, U.; Palmer, M.; Reiss, K.; Sönnichsen, A.; Wodarg, W. and Yeadon, M. (2021) Urgent Open Letter from Doctors and Scientists to the European Medicines Agency regarding COVID-19 Vaccine Safety Concerns. [back]
[34] Bhakdi, S. (2021) Rebuttal letter to European Medicines Agency from Doctors for Covid Ethics, April 1, 2021. [back]
[35] Ulm, J.W. (2020) Rapid response to: Will covid-19 vaccines save lives? Current trials aren’t designed to tell us. [back][back]
[36] Reimann, N. (2021) Covid Spiking In Over A Dozen States — Most With High Vaccination Rates.[back]
[37] Meredith, S. (2021) Chile has one of the world’s best vaccination rates. Covid is surging there anyway.[back]
[38] Bhuyan, A. (2021) Covid-19: India sees new spike in cases despite vaccine rollout. BMJ 372:n854. [back]
[39] Morrissey, K. (2021) Open letter to Dr. Karina Butler. [back]
[40] Anonymous, (2021) Open Letter from the UK Medical Freedom Alliance: Urgent warning re Covid-19 vaccine-related deaths in the elderly and Care Homes. [back]
[41] Furer, V.; Zisman, D.; Kibari, A.; Rimar, D.; Paran, Y. and Elkayam, O. (2021) Herpes zoster following BNT162b2 mRNA Covid-19 vaccination in patients with autoimmune inflammatory rheumatic diseases: a case series. Rheumatology -:x-x. [back]
[42] Anonymous, (2021) Covid-19 vaccines: ethical, legal and practical considerations. [back]
[43] Tseng, C.; Sbrana, E.; Iwata-Yoshikawa, N.; Newman, P.C.; Garron, T.; Atmar, R.L.; Peters, C.J. and Couch, R.B. (2012) Immunization with SARS coronavirus vaccines leads to pulmonary immunopathology on challenge with the SARS virus. PLoS One 7:e35421. [back]
[44] Bolles, M.; Deming, D.; Long, K.; Agnihothram, S.; Whitmore, A.; Ferris, M.; Funkhouser, W.; Gralinski, L.; Totura, A.; Heise, M. and Baric, R.S. (2011) A double-inactivated severe acute respiratory syndrome coronavirus vaccine provides incomplete protection in mice and induces increased eosinophilic proinflammatory pulmonary response upon challenge. J. Virol. 85:12201–15. [back]
[45] Weingartl, H.; Czub, M.; Czub, S.; Neufeld, J.; Marszal, P.; Gren, J.; Smith, G.; Jones, S.; Proulx, R.; Deschambault, Y.; Grudeski, E.; Andonov, A.; He, R.; Li, Y.; Copps, J.; Grolla, A.; Dick, D.; Berry, J.; Ganske, S.; Manning, L. and Cao, J. (2004) Immunization with modified vaccinia virus Ankara-based recombinant vaccine against severe acute respiratory syndrome is associated with enhanced hepatitis in ferrets. J. Virol. 78:12672–6. [back]
[46]Czub, M.; Weingartl, H.; Czub, S.; He, R. and Cao, J. (2005) Evaluation of modified vaccinia virus Ankara based recombinant SARS vaccine in ferrets. Vaccine 23:2273–9 [back]
[47]Tinari, S. (2021) The EMA covid-19 data leak, and what it tells us about mRNA instability. BMJ 372:n627 [back]
[48] Anonymous, (2021) Interview with Dr. Vanessa Schmidt-Krüger, Hearing #37 of German Corona Extra-Parliamentary Inquiry Committee 30 January, 2021. [back]
Why I’m Removing All Articles Related to Vitamins D, C, Zinc and COVID-19

By Dr. Joseph Mercola | May 4, 2021
Over the past year, I’ve been researching and writing as much as I can to help you take control of your health, as fearmongering media and corrupt politicians have destroyed lives and livelihoods to establish global control of the world’s population, using the COVID-19 pandemic as their justification.
I’ve also kept you informed about billionaire-backed front groups like the Center for Science in the Public Interest (CSPI), a partner of Bill Gates’ Alliance for Science, both of whom have led campaigns aimed at destroying my reputation and censoring the information I share.
Other attackers include HealthGuard, which ranks health sites based on a certain set of “credibility criteria.” It has sought to discredit my website by ensuring warnings appear whenever you search for my articles or enter my website in an internet browser.
Well-Organized Attack Partnerships Have Formed
HealthGuard, a niche service of NewsGuard, is funded by the pharma-funded public relations company Publicis Groupe. Publicis, in turn, is a partner of the World Economic Forum, which is leading the call for a “Great Reset” of the global economy and a complete overhaul of our way of life.
HealthGuard is also partnered with Gates’ Microsoft company, and drug advertising websites like WebMD and Medscape, as well as the Center for Countering Digital Hate (CCDH) — the progressive cancel-culture leader with extensive ties to government and global think tanks that recently labeled people questioning the COVID-19 vaccine as a national security threat.
The CCDH has published a hit list naming me as one of the top 12 individuals responsible for 65% of vaccine “disinformation” on social media, and who therefore must be deplatformed and silenced for the public good. In a March 24, 2021, letter1 to the CEO’s of Twitter and Facebook, 12 state attorneys general called for the removal of our accounts from these platforms, based on the CCDH’s report.
Two of those state attorneys general also published an April 8, 2021, op-ed2 in The Washington Post, calling on Facebook and Twitter to ban the “anti-vaxxers” identified by the CCDH. The lack of acceptance of novel gene therapy technology, they claim, is all because a small group of individuals with a social media presence — myself included — are successfully misleading the public with lies about nonexistent vaccine risks.
“The solution is not complicated. It’s time for Facebook CEO Mark Zuckerberg and Twitter CEO Jack Dorsey to turn off this toxic tap and completely remove the small handful of individuals spreading this fraudulent misinformation,” they wrote.3
Pharma-funded politicians and pharma-captured health agencies have also relentlessly attacked me and pressured tech monopolies to censor and deplatform me, removing my ability to express my opinions and speak freely over the past year.
The CCDH also somehow has been allowed to publish4 in the journal Nature Medicine, calling for the “dismantling” of the “anti-vaccine” industry. In the article, CCDH founder Imran Ahmed repeats the lie that he “attended and recorded a private, three-day meeting of the world’s most prominent anti-vaxxers,” when, in fact, what he’s referring to was a public online conference open to an international audience, all of whom had access to the recordings as part of their attendance fee.
The CCDH is also partnered with another obscure group called Anti-Vax Watch. The picture below is from an Anti-Vax Watch demonstration outside the halls of Congress. Ironically, while the CCDH claims to be anti-extremism, you’d be hard-pressed to find a clearer example of actual extremism than this bizarre duo.5
Gates-Funded Doctor Demands Terrorist Experts to Attack Me
Most recently, Dr. Peter Hotez, president of the Sabin Vaccine Institute,6 which has received tens of millions of dollars from the Bill & Melinda Gates Foundation,7,8,9 — with funds from the foundation most recently being used to create a report called “Meeting the Challenge of Vaccine Hesitancy,”10,11 — also cited the CCDH in a Nature article in which he calls for cyberwarfare experts to be enlisted in the war against vaccine safety advocates and people who are “vaccine hesitant.” He writes:12
“Accurate, targeted counter-messaging from the global health community is important but insufficient, as is public pressure on social-media companies. The United Nations and the highest levels of government must take direct, even confrontational, approaches with Russia, and move to dismantle anti-vaccine groups in the United States.
Efforts must expand into the realm of cyber security, law enforcement, public education and international relations. A high-level inter-agency task force reporting to the UN secretary-general could assess the full impact of anti-vaccine aggression, and propose tough, balanced measures.
The task force should include experts who have tackled complex global threats such as terrorism, cyber attacks and nuclear armament, because anti-science is now approaching similar levels of peril. It is becoming increasingly clear that advancing immunization requires a counteroffensive.”
Why is Hotez calling for the use of warfare tactics on American citizens that have done nothing illegal? In my case, could it be because I’ve written about the theory that SARS-CoV-2 is an engineered virus, created through gain-of-function research, and that its release was anticipated by global elites, as evidenced in Event 201?
It may be. At least those are some of my alleged “sins,” detailed on page 10 of the CCDH report, “Disinformation Dozen: The Sequel.”13 Coincidentally enough, the Nature journal has helped cover up gain-of-function research conducted at the Wuhan Institute of Virology, publishing a shoddy zoonotic origins study relied upon by mainstream media and others, which was riddled with problems.14,15
So, it’s not misinformation they are afraid of. They’re afraid of the truth getting out. They’re all trying to cover for the Chinese military and the dangerous mad scientists conducting gain-of-function work.
You may have noticed our website was recently unavailable; this was due to direct cyber-attacks launched against us. We have several layers of protective mechanisms to secure the website as we’ve anticipated such attacks from malevolent organizations.
What This Means for You
Through these progressively increasing stringent measures, I have refused to succumb to these governmental and pharmaceutical thugs and their relentless attacks. I have been confident and willing to defend myself in the court of law, as I’ve had everything reviewed by some of the best attorneys in the country.
Unfortunately, threats have now become very personal and have intensified to the point I can no longer preserve much of the information and research I’ve provided to you thus far. These threats are not legal in nature, and I have limited ability to defend myself against them. If you can imagine what billionaires and their front groups are capable of, I can assure you they have been creative in deploying their assets to have this content removed.
Sadly, I must also remove my peer reviewed published study16 on the “Evidence Regarding Vitamin D and Risk of COVID-19 and Its Severity.” It will, however, remain in the highly-respected journal Nutrients’ website, where you can still access it for free.
The MATH+ hospital treatment protocol for COVID-19 and the iMASK+ prevention and early outpatient COVID-19 protocol — both of which are based on the use of vitamins C, D, quercetin, zinc and melatonin — are available on the Front Line COVID-19 Critical Care Alliance’s website. I suggest you bookmark these resources for future reference.
It is with a heavy heart that I purge my website of valuable information. As noted by Dr. Peter McCullough during a recent Texas state Senate Health and Human Services Committee hearing, data shows early treatment could have prevented up to 85% (425,000) of COVID-19 deaths.17 Yet early treatments were all heavily censored and suppressed.
McCullough, in addition to being a cardiologist and professor of medicine at the Texas A&M University Health Sciences Center, also has the distinction of having published the most papers of any person in the history of his field, and being an editor of two major medical journals. Despite that, his video, in which he went through a paper he’d published detailing effective early treatments, was summarily banned by YouTube in 2020.
“No wonder we have had 45,000 deaths in Texas. The average person in Texas thinks there’s no treatment!” McCullough told the senate panel.18 Indeed, people are in dire need of more information detailing how they can protect their health, not less. But there’s only so much I can do to protect myself against current attack strategies.
They’ve moved past censorship. Just what do you call people who advocate counteroffensive attacks by terrorism and cyberwarfare experts? You’d think we could have a debate and be protected under free speech but, no, we’re not allowed. These lunatics are dangerously unhinged.
The U.S. federal government is going along with the global Great Reset plan (promoted as “building back better”), but this plan won’t build anything but a technological prison. What we need is a massive campaign to preserve civil rights, and vote out the pawns who are destroying our freedom while concentrating wealth and power.
Sources and References
- 1 AG Letter to Tech CEOs March 24, 2021 (PDF)
- 2, 3 Washington Post April 8, 2021
- 4 Nature March 15, 2021
- 5 Twitter Mercola March 25, 2021
- 6 WHO Peter Hotez
- 7 PND July 1, 2011
- 8 Bill & Melinda Gates Foundation
- 9 Sabin Vaccine Institute February 11, 2019
- 10 Sabin Vaccine Institute June 2, 2020
- 11 Sabin Vaccine Institute May 28, 2020
- 12 Nature April 27, 2021
- 13 CCHD Disinformation Dozen: The Sequel
- 14 Monali Rahalkar Criticism for the Addendum: A pneumonia outbreak associated with a novel coronavirus of probable bat origin (Zhou et al 2020)
- 15 Monali Rahalkar Critique to the Addendum (Zhou et al 2020) and other contradictions in reporting the facts about RaTG13 and its history
- 16 Nutrients October 31, 2020;12, 3361; doi:10.3390/nu12113361
- 17, 18 Lifesitenews.com April 8, 2021
Why Is There No Correlation Between Masks, Lockdowns, and Covid Suppression?
In the past couple of months, our esteemed public health experts have had a rough go of defending the supposedly settled science behind lockdowns and mask mandates.
White House covid-19 advisor Andy Slavitt was first on the chopping block back in mid-February, when he was reduced to parroting empty platitudes about social distancing after failing to explain why a completely open Florida had numbers no worse than a strictly locked-down California. Then comes media darling Dr. Anthony Fauci, who has had a particularly embarrassing series of public appearances of late. During a recent MSNBC interview Fauci expressed confusion and wasn’t “quite sure” as to why Texas was experiencing falling cases and deaths an entire month after lifting its mask mandates and capacity restrictions. Moreover, during a hearing with Representative Jim Jordan, Fauci completely dodged Jordan’s question of why Texas has lower case rates than some of the most notable lockdown states. Fauci, refusing to answer the question, simply responded that having a lockdown is not the same thing as obeying lockdowns. Fauci was correct here, but he indirectly claimed that citizens of New York and New Jersey, two notorious lockdown states, were complying less with mitigation measures than a state that had, and still has, practically none. A quick check of Google’s covid-19 mobility reports lays this counterintuitive claim to rest.
The American Media’s Agenda
When governments and media outlets around the world have successfully captured audiences by stoking fear of covid-19, the data that should so easily assuage this fear become irrelevant, and interviews like those mentioned above are simply brushed aside in favor of a fear-born allegiance to the “morally superior” government-mandated lockdowns, curfews, mask mandates, and more. This “scared straight” approach, as Bill Maher correctly described it, is the state’s bludgeon of compliance.
As far as scaring citizens straight, Project Veritas has released footage showing CNN employees explaining how the network plays up the covid-19 death toll to drive numbers. Especially disgraceful was CNN technical director Charlie Chester’s admission that the network doesn’t like to report recovery rates because “[t]hat’s not scary…. If it bleeds it leads.”
CNN isn’t alone in the fearmongering business. Thanks to the surplus of United States media outlets willing to churn up a disproportionate amount of negative covid-19 headlines—roughly 90 percent of covid-19 news in the United States is negative compared to 51 percent internationally—is it any surprise that nearly 70 percent of Democrats, 51 percent of Republicans, and almost 50 percent of independents think the chances of being hospitalized with covid-19 range anywhere from 20 percent to over 50 percent?
Where’s the Correlation?
Government- and media-induced panic have blinded us to the data, which for the past thirteen months have consistently shown zero correlation between the timing, strength, and duration of mitigation measures and covid-19 incidence. Nowhere could this lack of correlation be more prevalent than among lockdowns and mask usage.
Leaving aside the disastrous and deadly consequences of government lockdowns—see here, here, and here—the evidence for lockdowns’ ability to mitigate covid-19 mortality remains scant.
Looking at the United States, we can address the widely believed notion that states with more intense lockdowns will see fewer covid-19 deaths by plotting each state’s average restriction ranking over the past thirteen months against the total number of covid-19 deaths for each state. To get the average ranking, the author averaged data from Oxford University’s Blavatnik School of Government—this source ranked each state by the average time spent at a stringency index measure greater than sixty up until mid-December 2020—and WalletHub, which also ranked each state by stringency using a weighted average of various measures from January 2021 onward. Now, if the past year’s worth of sanctimonious lectures from public health experts have any scientific weight behind them, we should see a very strong negative correlation between the intensity of states’ restrictions and total covid-19 deaths.
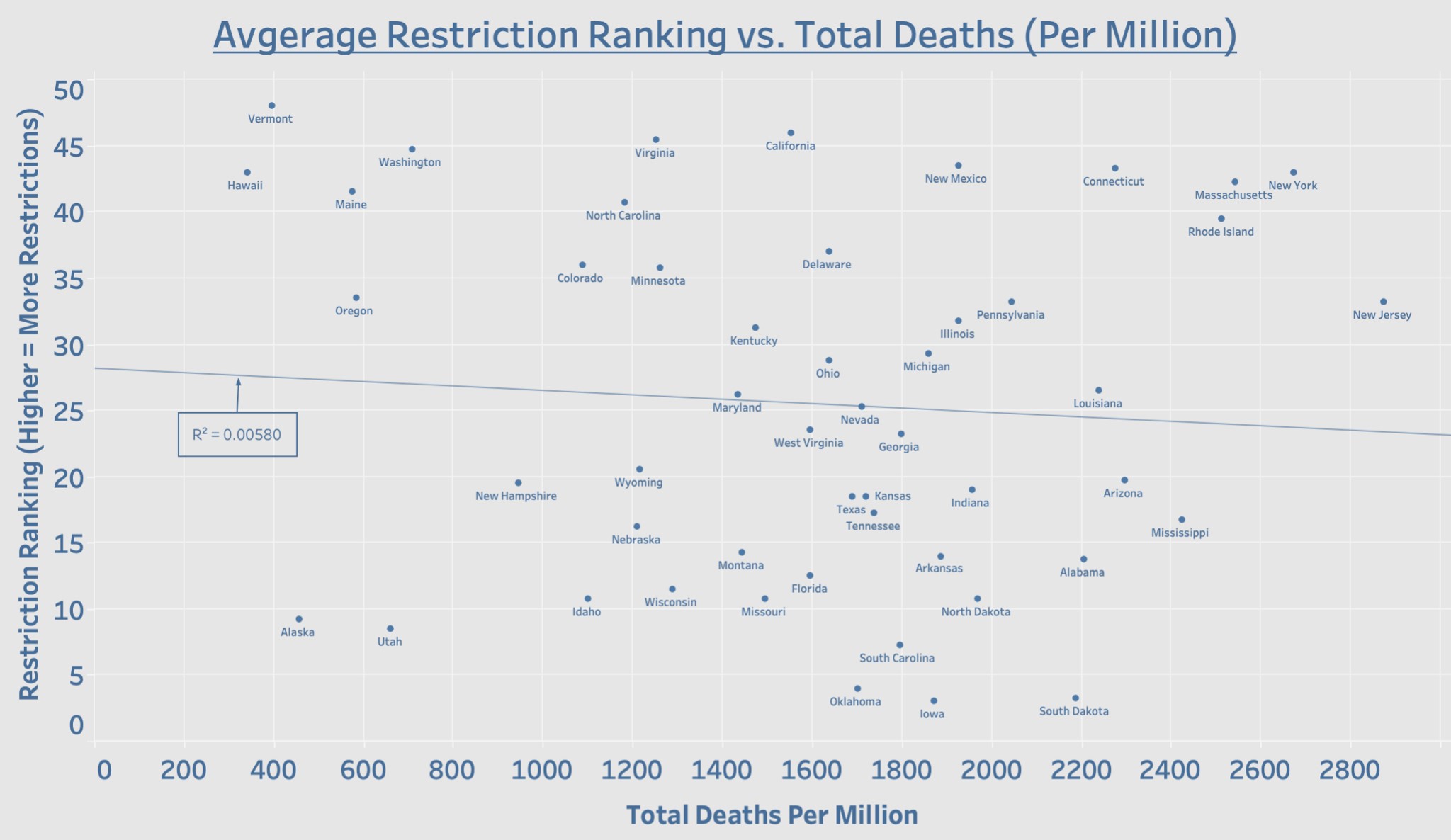
Source: Data on deaths (as of Apr. 28, 2021) from the NYTimes Covid-19 Data Bot. Data on restriction rankings from the NYTimes Covid-19 Data Bot (through December 2020); Adam McCann, “States with the Fewest Coronavirus Restrictions,” WalletHub, Apr. 6, 2021 (since January 2021); and Laura Hallas, Ariq Hatibie, Saptarshi Majumdar, Monika Pyarali, and Thomas Hale, “Variation in US States’ Responses to COVID-19” (Blavatnik School of Government Working Paper No. BSG-WP-2020/034, December 2020).
Contrary to what the public health experts have been telling us for more than a year, there is no correlation between the strength of a state’s lockdown measures and total covid-19 deaths. In fact, notorious lockdown states such as New York and New Jersey have some of the worst mortality numbers to date. To blame noncompliance for these poor numbers is ridiculous on its face considering that states with no restrictions, such as Texas and Florida, have far fewer deaths than New York and New Jersey. In fact, you’ll find that every state that has either removed its mask mandate or all covid-19 restrictions entirely is outperforming New York and New Jersey in terms of deaths.
The same lack of correlation can be seen when comparing average lockdown stringency with the total number of patients hospitalized who have suspected or confirmed covid-19. As a point of clarification, the author summed the current number of patients hospitalized each day to arrive at the total number of patients hospitalized. This will result in slightly inflated total numbers, since patients may spend more than one day in the hospital, but having applied the same aggregation method across all states, the total hospitalization metric still provides an accurate assessment of covid-19 hospitalizations in each state.

Source: Data on hospitalizations (as of Apr. 24, 2021) from the US Department of Health and Human Services. Data on restriction rankings from the NYTimes Covid-19 Data Bot (through December 2020); Adam McCann, “States with the Fewest Coronavirus Restrictions,” WalletHub, Apr. 6, 2021 (since January 2021); and Laura Hallas, Ariq Hatibie, Saptarshi Majumdar, Monika Pyarali, and Thomas Hale, “Variation in US States’ Responses to COVID-19” (Blavatnik School of Government Working Paper No. BSG-WP-2020/034, December 2020).
Internationally speaking, the data continue to expose lockdowns as the single greatest public health failure in human history. Plotting lockdown stringency against total covid-19 death toll reveals, yet again, zero correlation between the two variables.

Source: Data on deaths (as of Apr. 28, 2021) and lockdown stringency (as of Apr. 28, 2021) from Our World in Data.
In light of a year’s worth of data showing wildly different mortality and hospitalization outcomes for fifty states with fifty very different lockdown stringencies, as well as drastically different mortality outcomes for 166 countries with 166 different lockdown stringencies, one can only marvel that such a deadly and ineffective policy can be recommended by public health experts.
If the lockdowns failed to mitigate the spread of covid-19 in the United States just as in dozens of countries around the world—remember, the lockdowns fail without even taking their costs into account—it’s possible that mask usage is the missing piece of the mitigation puzzle.
It wouldn’t be fair to the reader to post quite literally hundreds of charts that show the exact opposite outcomes the media would have one expect after regions remove or institute mask mandates—Ian Miller has done more work in this area than anybody else. It also wouldn’t be fair to claim that mask mandates and mask usage are synonymous. However, based on reactions to states lifting their mask mandates, I don’t think any proponent of mask wearing would seriously expect the same level of mask usage should mandates be lifted. Nevertheless, the claim that mask usage negatively correlates with cases and deaths is easily refuted with a quick look at the data. Given the data available, we’ll again only be looking at the fifty states.

Source: Data for cases and deaths (as of Apr. 28, 2021) from the NYTimes Covid-19 Data Bot. Mask usage data from the Delphi Group’s COVIDcast.
Even though the trend lines travel in the exact opposite direction of what our public health experts would have us expect, the correlations are statistically meaningless. Note that the above chart only covers the 2.5-month period starting February 9, 2021, which is when COVIDcast began reporting mask usage numbers for each state. Therefore, the author included only the cases and deaths that occurred during this 2.5-month period. Despite this truncated time period, 2.5 months should have been more than enough to have exposed any sort of meaningful correlation between mask usage and both cases and deaths.
It is worth noting that Rhode Island and New York, each with some of the highest mask usage rates and lockdown stringencies in the country, are leading the pack with some of the largest case increases since early February. What is more, in the 2.5 months since early February the ten states with the highest rate of mask usage have been doing worse in both cases and deaths than the ten states with the lowest rate of mask usage.
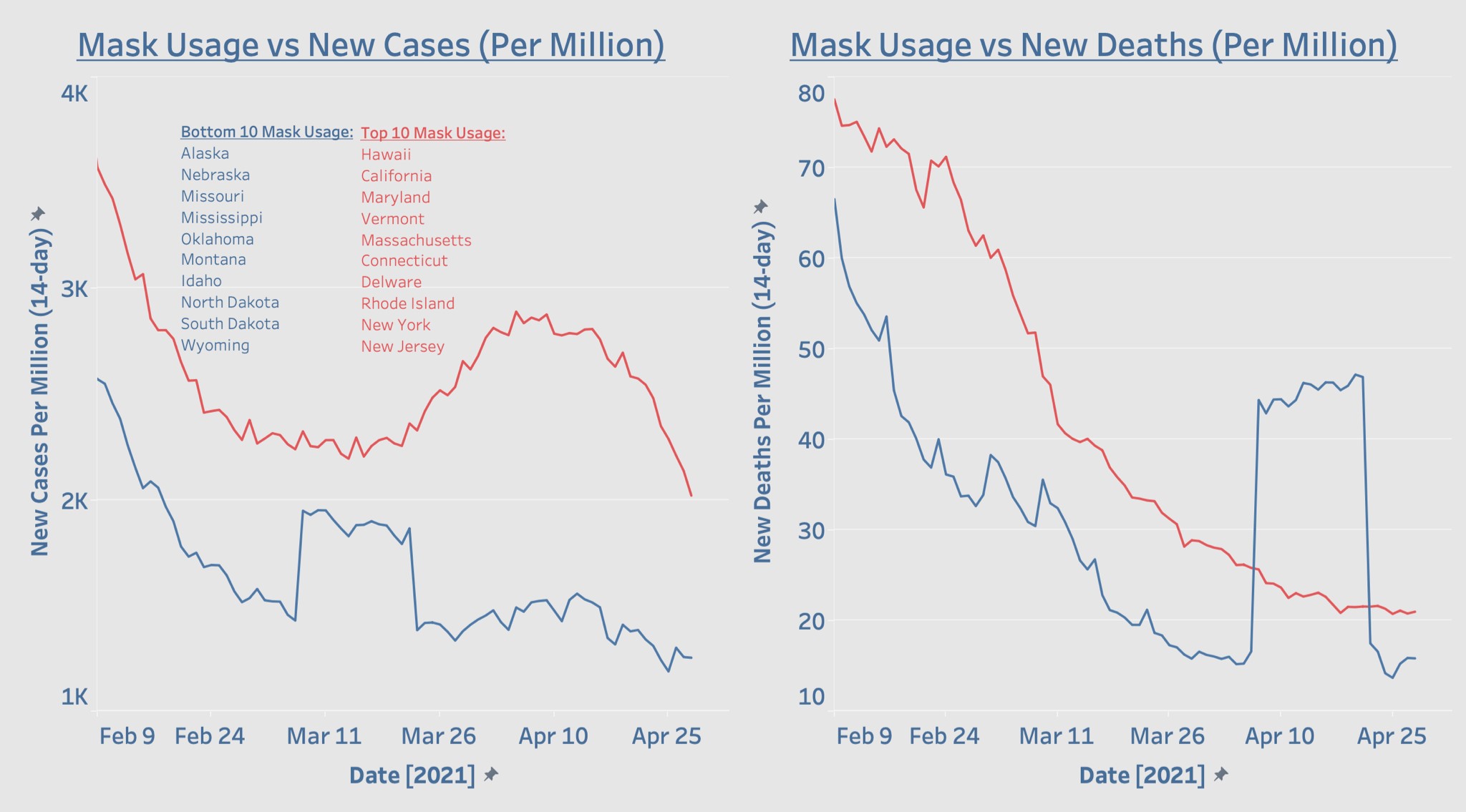
Source: Data for cases and deaths (as of Apr. 28, 2021) from the NYTimes Covid-19 Data Bot. Mask usage data from the Delphi Group’s COVIDcast.
Remember, we aren’t measuring the amount of rules that simply say you have to wear a mask. What’s being measured is the percentage of people actually wearing masks in public in each state. It’s quite difficult to look at the trends depicted above and make the case not only for continuing mask mandates, but wearing masks at all.
Some may have an issue with the fact that the trends above only cover the couple of months since February. Let’s assume, for the sake of a more complete picture, that mask usage trends were consistent for each state since the start of the pandemic. We can also expand our filter to the top and bottom fifteen states to account for some states’ movement in and out of the top and bottom ten states.

Source: Data for cases and deaths (as of Apr. 28, 2021) from the NYTimes Covid-19 Data Bot. Mask usage data from the Delphi Group’s COVIDcast.
In terms of cases, from April to around mid-June, states with the lowest rates of mask usage were outperforming states with the highest rates of mask usage. This trend reversed from mid-June through mid-January and then reversed again in favor of states with the lowest rate of mask usage.
In terms of deaths, states with the lowest rates of mask usage outperformed states with the highest rates of mask usage from April until mid-July. From mid-July to mid-February, death trends were more favorable to states with the highest rates of mask usage, but after mid-February death trends again became more favorable to states with the lowest rates of mask usage. Again, if we are assuming fairly consistent rates of mask usage across the entire duration of the pandemic while also assuming that the science behind masks is truly settled, it’s quite difficult to explain away any period of time in which states with the lowest rates of mask usage were outperforming states with the highest rates.
The supposedly settled science behind both lockdowns and mask mandates has always been in serious trouble but is even more so now. Completely leaving aside the incredible death toll of the lockdowns, their numerous social and psychological costs, the totalitarian denial of our most basic liberties, and the decimation of tens of thousands of small businesses, they would still be a miserable failure by nearly every covid-19 metric we have available. Though, to be fair, the lockdowns did make our cities quieter. But aside from that, the data continue to deny that either lockdowns or mask mandates are effective tools for mitigating the spread of covid-19.
Featured Video

Larry Johnson: U.S. Desperation Grows as Iran Is Winning
or go to
Aletho News Archives – Video-Images
From the Archives
Alarmist climate science as a textbook example of groupthink
By Paul MacRae | May 1, 2012
A while ago, I received an email from a friend who asked:
How can many, many respected, competitive, independent science folks be so wrong about [global warming] (if your [skeptical] premise is correct). I don’t think it could be a conspiracy, or incompetence. … Has there ever been another case when so many ‘leading’ scientific minds got it so wrong?
The answer to the second part of my friend’s question—“Has there ever been another case where so many ‘leading’ scientific minds got it so wrong?”—is easy. Yes, there are many such cases, both within and outside climate science. In fact, the graveyard of science is littered with the bones of theories that were once thought “certain” (e.g., that the continents can’t “drift,” that Newton’s laws were immutable, and hundreds if not thousands of others).
Science progresses by the overturning of theories once thought “certain.” … continue
Blog Roll
 Aletho News
Aletho News- Larry Johnson: U.S. Desperation Grows as Iran Is Winning
- Why don’t UK media mention the Israel lobby?
- New US shipment of 6,500 tons of military aid arrives in Israel
- Military aid to Ukraine vital for ‘US hegemony’ – Republican senator
- Zelensky’s favorite drone company at center of Ukrainian corruption alert
- The Broken Contract
- US CENTCOM’s Request for Dark Eagle Missiles Shows Shortage of Weapons and Limited Options
- Iran consolidates Strait of Hormuz control in post-war power shift, leaving US in dark
- A pause, not a ceasefire: Washington stalls, Tehran recalibrates
- US blockade crumbles as Iran turns to overland routes
- If Americans Knew
- US ships 6,500 tons of munitions, equipment to Israel in 24 hours
- A New Library in Gaza Rises From the Ashes of Destruction
- Israel’s top Jewish religious body ‘refuses to condemn’ smashing of Jesus statue
- Nun assaulted in Jerusalem amid ‘pattern’ of anti-Christian attacks by Israelis
- Former Tik Tok official describes massive pressure from Israel lobby
- Amid ceasefire violations and genocide, Israel commits piracy – Daily Update
- Five Laws and Standards That Require the US Cut Off Weapons to Israel
- Israel’s diabolical killing machine and how it targets journalists.
- The Global Sumud Flotilla to Gaza — A cry at sea to the world’s dormant conscience
- Politico’s powerful parent company tells Politico they must support Israeli narrative
- No Tricks Zone
- Oversupply Of Volatile Solar Energy Leads To Record NEGATIVE Prices!
- New Study: Extreme Heat Records, Heatwaves, Extreme Cold Records Declining Across US Since 1899
- It’s The Cold, Stupid! Cold 20 Times More Lethal Than Heat, Multiple Studies Show
- European Institute For Climate And Energy: “Climate Debate is Seldom About Science”
- New Study: The Climate May Be 5 Times More Sensitive To Solar Forcing Than Commonly Assumed
- EV Industry Reached $70 Billion In Losses In 2024 Due To Delusional Green Ideologies
- Reality Check: Maldives Have Actually Grown In Size Or Remained Stable Over Recent Decades
- Abrupt Climate Change Also Occurred NATURALLY In The Past …25 Times During Last Ice Age
- Cave Discovery Reveals Today’s Desert Climates Were Recently Far Warmer, Wetter, Teeming With Life
- German Expert: Heat Dome Led To Record Temps In Western USA…Warmer In 1934, 1936
