NIH hit with lawsuit for blocking COVID Gain of Function research evidence
NIH Failed to Promptly Release Documents Concerning “Gain of Function/Gain of Threat” Research on Influenza, MERS, SARS, and COVID
Center for Food Safety | May 4, 2021
Last week, Center for Food Safety (CFS) filed a Freedom of Information Act (FOIA) lawsuit against the National Institutes of Health (NIH), an agency with the Department of Health and Human Services (HHS). CFS is suing the agency over its failure to release government documents related to the approval and issuance of NIH contracts and grants that fund research projects involving controversial gain of function/gain of threat studies with dangerous, so-called “enhanced potential pandemic pathogens.”
“The NIH’s refusal to make public the research it is funding to enhance the transmissibility, infectiousness, and lethality of potential pandemic viruses is grossly irresponsible,” said Andrew Kimbrell, executive director of Center for Food Safety. “We are litigating to get that information because transparency and public knowledge about these highly hazardous experiments could be an important step in avoiding the next pandemic.”
An enhanced, “laboratory-generated” potential pandemic pathogen results from the enhancement of a potential pandemic pathogen’s transmissibility or virulence in humans. Gain of function/gain of threat studies, or research that improves the ability of a pathogen to cause disease, is a subset of life sciences research that most commonly involves the creation or use of enhanced potential pandemic pathogens.
CFS’s lawsuit focuses on the agency’s withholding of records concerning NIH’s funding of proposed research that could create, transfer, or use enhanced potential pandemic pathogens for which additional review under HHS’ Framework for Guiding Funding Decisions about Proposed Research Involving Enhanced Potential Pandemic Pathogens (HHS P3CO Framework) is required.
“FOIA requires NIH to release records promptly. Unfortunately, the agency has failed to comply with FOIA’s statutory deadlines with respect to our request,” said Victoria Yundt, staff attorney at Center for Food Safety.”Consequently, NIH has unlawfully deprived the public of its statutory right to obtain records containing crucial information about government approval and funding of new and continued gain of function/gain of threat studies that consist of creating, transferring, or using enhanced potential pandemic pathogens in U.S. laboratories, which—if released from a laboratory accident—could result in catastrophic consequences to the human environment.”
Without the requested records, CFS cannot determine how many gain of function/gain of threat projects have been funded by the NIH, nor how many of these projects have undergone the proper review or comply with other federal laws and regulations.
NIH’s unlawful withholding of public records undermines FOIA’s basic purpose of government transparency. CFS has a history of suing the federal government to compel agencies to be compliant with FOIA. CFS’s FOIA program is committed to upholding the principles embodied in FOIA, such as maintaining an open and transparent government.
Why are we being lied to about Covid? There’s no good reason
By Dr Mike Yeadon | Conservative Woman | May 10, 2021
Be in no doubt, among the reasons that voices and opinions like mine are never heard in the main media is extreme censorship more suited to China than a liberal democracy. Please allow me to illustrate with an example close to my heart why it is high time for us to change our response.
Ivermectin is one of the WHO’s ‘essential drugs’ which all countries should have access to. It’s very cheap as its patent has long expired; it’s one of the most-used drugs in world history; it’s extraordinarily safe; it is often life-saving against parasitic infections. It is also one of the best-established pharmaceutical treatments for Covid-19, showing benefit in every stage of the disease, in multiple independent clinical trials of varying quality. On January 3, 2021, Dr Tess Lawrie attempted to alert the Prime Minister to the potential of ivermectin. Her video here was pulled from YouTube within hours of posting, though it survives on Vimeo. The paper by the FLCCC group of US intensivists (whose survival rates for severe Covid-19 are best in class) that was the inspiration for Dr Lawrie’s work was accepted after extensive open peer review (including two career employees of the FDA) and ‘provisionally accepted’ by the ‘open science’ journal Frontiers in Pharmacology. The screenshot of the abstract tweeted by Clare Craig shown here attracted more than 100,000 views. Then, mysteriously, it was rejected and pulled by the Frontiers editor in chief. It is still here in cached form though the Ministry of Truth has been at work and placed it in a memory hole, so no trace survives on Frontiers’ own website.
Intended for a Special Issue on ‘repurposed drugs’ for Covid-19, various guest editors were so incensed at this behaviour that they resigned in protest. You can read their letter here. They concluded that ‘these unfortunate events constitute gross editorial misconduct by Frontiers.’ Fortunately this major paper is now published by the American Journal of Therapeutics and can be read in its final form here.
This nevertheless successfully delayed by nearly six months its circulation to leading public health bodies starting mid-November. A copy was sent to Sir Jeremy Farrar (boss of the Wellcome Trust and member of Sage) who passed it on to Professor Peter Horby (also on Sage), amongst others, on November 18, 2020. So the efficacy of ivermectin must be well known to the Government’s advisers, but they have done nothing about it. Likewise, the formal and rigorous meta-analysis performed by Dr Tess Lawrie’s team at the Evidence-Based Medicine Consultancy Ltd has been communicated to Matt Hancock, but without reply.
I am telling you about this, because all that governments, their scientific advisers, big pharma (here’s Merck, who originally developed & marketed it) and regulatory agencies will tell you is that ivermectin doesn’t work in Covid-19. They are lying. I am inviting any of them to sue me, but they won’t, for I would win easily.
If ivermectin was more widely used, there’d be no need for vaccines.
To date, despite the brains, expertise and stature of those scientists questioning the official Covid-19 narrative, as a group they quite patently have been ineffective. And this is unlikely to change while, as polite professionals, they won’t say: ‘This is corruption and they’re lying deliberately to scare the people.’ Furthermore, unwittingly, they have been playing the parts intended by those, including our own Government and their advisers, who control the global Covid narrative.
They judged correctly that we polite Brits wouldn’t accuse them of outright lying, even though they often do exactly that. Boris Johnson’s recent piece to camera, telling us that it was lockdown and not vaccination which reduced cases and deaths, is a case in point.
Yet it’s certain this isn’t true, and also certain he and his advisers know it isn’t true.
The government’s advisers are not fools. Some may be, but the upper echelons are very smart. They believe polite people won’t say ‘not only are you lying but you’re doing it in concert with other, non-democratic actors’, because that’s conspiracy theory stuff, right? Powerful people never use their influence to benefit their interests, do they? Hmm. The only thing that’s different is scale and the power their public positions give them. Other than that, they’re just another a bunch of grubby criminals, ripping off unsuspecting people.
Truth is our most powerful tool. And that truth is that we’re being lied to.
The truth also, however hard it is to believe it, is that there is unequivocal and clear evidence of planning and co-ordination. Not to face this fact is to have your head in the sand. Where it’s leading is easy to discern, once people are willing to lift their internal censoring and look objectively at the evidence.
First, though, the lies. It’s abundantly clear now that pretty much everything that the public has been told and continues to be told is between untrue and downright lies.
I offer as a shortlist that:
-PCR mass testing reasonably reliably distinguishes infected and infectious people from others;
-that masks reduce transmission of respiratory viruses;
-that transmission of infection in the absence of symptoms is an important contribution to epidemic spreading;
-that lockdowns as executed reduce hospitalisation and deaths;
-that no matter how small the remaining susceptible population and no matter that virtually no people who, if infected, might die remain unvaccinated, the position is perilous;
-that no pharmaceutical treatments are available;
-that variants are different enough to warrant border closures and require new vaccines;
-that the gene-based vaccines are safe and effective;
-that ‘vaccine passports’ will increase safety while having no material impacts on freedom of choice in a liberal democracy.
It is impossible to believe that intelligent, well-connected and well-briefed senior advisers to governments don’t know that almost all, if not all, of the above are simply not true.
It is not a matter of opinion in almost all cases. These statements, which have been explicitly stated and used in justification for the extraordinary interferences in the lives of citizens in democratic countries, are mostly demonstrably wrong, as defined by there being multiple well-conducted, peer-reviewed studies showing the contrary.
To continue with the pretence that there’s scientific uncertainty, and it’s therefore understandable that an adviser might offer nuanced advice, is wrong and misleading. This perhaps is where the mainstream media has been most culpable.
It is not reasonable to expect typical viewers and readers of speeches, articles and editorials – whether by scientist sceptics or by critical commentators – to appreciate that, when we point out that what’s happening doesn’t make sense, we mean ‘the executive is knowingly and deliberately harming the country and its citizens’. We are mostly not saying this, leaving it to the audience to sum up for themselves. But in my view the audience are reluctant to do this. They want to believe in government and perhaps above all they want a quiet life. To disbelieve is so much harder than to believe.
So in recent weeks I’ve made a clear decision no longer merely to point out what it is that governments and their advisers and spokespersons around the world are doing is wrong, scientifically unjustified and harmful, but to join the dots in an attempt to provide potential explanations of why they’re doing these things.
It is time for all Doubting Thomases to take a lead and state unambiguously that ‘government and its advisers are telling us things that are manifestly untrue and maintaining restrictive, damaging measures for which there’s no justification’. By not doing so they are playing into the hands of those who I firmly believe are engaged in a determined series of crimes against humanity.
Why do I say this? Simply because there is no benign interpretation of the acts of commission and omission consistently imposed upon us and no explanation of the statements which are flatly wrong other than an intention to deceive the population.
Looking around us now, we see that the prevalence of the virus in the community is effectively zero. Note that the authorities have never conceded and determined the operational false positive rate of PCR mass testing. Subtracting any reasonable estimate of oFPR and we observe no cases at all. This was true for months as indicated by the positive rate in lateral flow tests.
No variant of the virus differs by more than 0.3 per cent from the original sequence, and numerous academic immunologists have stated strongly that there is no possibility that booster/top-up/variant vaccines are required. Yet we get daily ‘fear porn’ on this topic. The European Parliament just voted through the basic outlines of a vaccine passport system. It’s a racing certainty that the UK will soon follow.
Mask regulations continue in force and many psychologists believe some people are so traumatised that they will continue to wear them indefinitely, even though they are useless.
The economy and currency may already be damaged beyond repair. Yet there’s another six weeks minimum until the last restrictions are scheduled to be lifted.
Almost no one is dying ‘with’ Covid-19 now, and the attribution methodology overestimates this anyway. Yet hospitals and primary health care remain far less accessible than they should be, inevitably resulting in causing or storing up avoidable non-Covid-19 deaths, to say nothing of the suffering and misery of the millions awaiting treatments for painful and worrying illnesses.
Most terrifyingly, it appears we will soon be required to possess VaxPass apps if we wish to continue to access our lives.
This system can run effectively only if everyone is vaccinated. This is a monstrous concept, because it is known that all four vaccines in use in Europe contain a fatal design flaw: they cause the fusogenic, pro coagulation spike protein to be expressed wherever the vaccine is taken up. In some people, especially those so young that they’re at no measurable risk of death if infected by the virus, vaccination results in their deaths from thromboembolic events. Permitting the inexpert population to walk into this trap is unconscionable: there will be thousands of further vaccine-induced deaths of young people.
I invite thoughtful people to ask that difficult question: ‘Why are they doing this?’
It is my deduction and conclusion that the only motivation that fits all the observations is the intention to ‘herd’ every citizen into a VaxPass system. This is a completely novel system. Never before have all individuals been represented in a single, interoperable database as a unique digital ID, accompanied by an editable health-related field. Whoever controls that database, and the algorithms which govern what it permits and denies, has literally totalitarian control of the entire population. There is no personal threshold crossing or transaction which doesn’t fall to those operating that system.
At the very least, the public deserves to be warned that this is coming. I do not expect conventional judicial processes to protect us in any way. Every institution has already failed the people of the UK.
Given that numerous government decisions (as instructed by Sage) have arguably already led to many avoidable deaths, I think it’s only reasonable to consider what the prize is that leads intelligent people to do the things they’ve done and continue to peddle.
The possible answers to this question are all bad. I cannot conceive of a situation where we will shortly be permitted to resume our normal lives. There is not the slightest hint of that in any case.
I have found it impossible to come up with a benign interpretation of the events. No one works as carefully and for so long as evidently has been done, across the world, only suddenly to stop. Why? I’ve asked hundreds of people and not a single one has (a) pointed out where my logic fails or (b) come up with a benign interpretation.
My own conviction is that the purpose is, at minimum, to establish a system of totalitarian control which will mean the extinguishing of liberal democracy.
It almost doesn’t matter what the next steps might be, but they could, for example, have been sold to numerous people as the only solution to ‘anthropogenic global warming’: the amount of resources we’ll be permitted to produce and consume will be set by some unseen controllers. It is possible they could go a step further than this, and see reducing population or depopulation as another route to solving the perceived problem of AGW.
Consider the elimination of the class of the inquiring journalist, the censorship of all mass media. The relentless smearing and exclusion of those who ask too many awkward questions. The astonishing waste of public money, which apparently the foreign exchange markets are unperturbed about. The destruction of SMEs which provide a third of all jobs and a substantial proportion of tax revenues. The relentless lying. The misinformation. The use of psychological operations to frighten and subdue. The utter disregard for those vaccinated with ‘vaccines’ that are way too unsafe for their role. The bending past illegality of the use of incorrect information to persuade pregnant women to get vaccinated. The numerous breaches of the Nuremberg Code, since no one is being explicitly told that these vaccines are experimental and so recipients are being unwittingly enrolled in an unprecedentedly large and unmonitored Phase 3 clinical trial. The announcement that, soon, our minor children are to be vaccinated.
Add in the ‘top-up vaccines’. They’re not vaccines. Whoever has been vaccinated has no need of further vaccination. Immunology is perhaps my strongest suit, so I am certain of this. Is it impossible that in those one billion vials which pharma has already told us its manufacturing, there is some gene sequence which will instigate one of a few dozen pathologies, with onset times ranging from near-immediate to a short number of years? I assure you, biotechnology has awesome power, and it can be used for good or ill.
I think I’ve made a decent case that what governments and their advisers have done easily amounts to conspiracy. The same ‘mistakes’ have been made everywhere. The same tricks and manipulation. Those who claim this is all coincidence are coincidence theorists.
I argue that unless this is pointed out to the public before any possible ‘vaccine passports’ system is established, we’ve all collectively failed to discharge our duties to be courageous, to take chances, to risk looking foolish: I am absolutely committed to continuing to speak out for as long as I have breath in my body.
Second Stage Terror Wars

By Edward Curtin | May 11, 2021
“We’ll know our disinformation program is complete when everything the American public believes is false.” – William Casey, CIA Director, Feb. 1981
It is well known that the endless U.S. war on terror was overtly launched following the mass murders of September 11, 2001 and the linked anthrax attacks. The invasion of Afghanistan and the Patriot Act were immediately justified by those insider murders, and subsequently the wars against Iraq, Libya, Syria, etc. So too the terrorizing of the American people with constant fear-mongering about imminent Islamic terrorist attacks from abroad that never came.
It is less well known that the executive director of the U.S. cover story – the fictional 9/11 Commission Report – was Philip Zelikow, who controlled and shaped the report from start to finish.
It is even less well known that Zelikow, a professor at the University of Virginia, was closely associated with Condoleezza Rice, George W. Bush, Dickey Cheney, Paul Wolfowitz, Brent Scowcroft, et al. and had served in various key intelligence positions in both the George H. W. Bush and George W. Bush administrations. In 2011 President Obama named him to his President’s Intelligence Advisory Board as befits bi-partisan elite rule and coverup compensation across political parties.
Perhaps it’s unknown or just forgotten that The Family Steering Committee for the 9/11 Commission repeatedly called for Zelikow’s removal, claiming that his appointment made a farce of the claim that the Commission was independent.
Zelikow said that for the Commission to consider alternative theories to the government’s claims about Osama bin Laden was akin to whacking moles. This is the man, who at the request of his colleague Condoleezza Rice, became the primary author of (NSS 2002) The National Security Strategy of the United States of America, that declared that the U.S. would no longer abide by international law but was adopting a policy of preemptive war, as declared by George W. Bush at West Point in June 2002. This was used as justification for the attack on Iraq in 2003 and was a rejection of the charter of the United Nations.
So, based on Zelikow’s work creating a magic mountain of deception while disregarding so-called molehills, we have had twenty years of American terror wars around the world in which U.S. forces have murdered millions of innocent people. Wars that will be continuing for years to come despite rhetoric to the contrary. The rhetoric is simply propaganda to cover up the increasingly technological and space-based nature of these wars and the use of mercenaries and special forces.
Simultaneously, in a quasi-volte-face, the Biden administration has directed its resources inward toward domestic “terrorists”: that is, anyone who disagrees with its policies. This is especially aimed at those who question the COVID-19 story.
Now Zelikow has been named to head a COVID Commission Planning Group based at the University of Virginia that is said to prepare the way for a National COVID Commission. The group is funded by the Schmidt Futures, the Skoll Foundation, the Rockefeller Foundation and Stand Together, with more expected to join in. Zelikow, a member of the Bill & Melinda Gates Foundation’s Global Development Program Advisory Panel, will lead the group that will work in conjunction with the Johns Hopkins Center for Health Security at the Bloomberg School of Public Health. Stand together indeed: Charles Koch, Bill Gates, Eric Schmidt, the Rockefellers, et al. funders of disinterested truth.
So once again the fox is in the hen house.
If you wistfully think the corona crisis will soon come to an end, I suggest you alter your perspective. Zelikow’s involvement, among other things, suggests we are in the second phase of a long war of terror waged with two weapons – military and medical – whose propaganda messaging is carried out by the corporate mainstream media in the pursuit of the World Economic Forum’s Great Reset. Part one has so far lasted twenty years; part two may last longer. You can be certain it won’t end soon and that the new terrorists are domestic dissidents.
Did anyone think the freedoms lost with The Patriot Act were coming back some day? Does anyone think the freedoms lost with the corona virus propaganda are coming back? Many people probably have no idea what freedoms they lost with the Patriot Act, and many don’t even care.
And today? Lockdowns, mandatory mask wearing, travel restrictions, requirements to be guinea pigs for vaccines that are not vaccines, etc.?
Who remembers the Nuremberg Codes?
And they thought they were free, as Milton Mayer wrote about the Germans under Hitler. Like frogs in a pot of cold water, we need to feel the temperature rising before it’s too late. The dial is turned to high heat now.
But that was so long ago and far away, right? Don’t exaggerate, you say. Hitler and all that crap.
Are you thankful now that government spokespeople are blatantly saying that they will so kindly give us back some freedoms if we only do what they’re told and get “vaccinated” with an experimental biological agent, wear our masks, etc.? Hoi polloi are supposed to be grateful to their masters, who will grant some summer fun until they slam the door shut again.
Pfizer raked in $3.5 billion from vaccine sales in the first quarter of 2021, the first three months of the vaccine rollouts, and the company projects $26 billion for the year. That’s one vaccine manufacturer. Chump change? Only a chump would not realize that Pfizer is the company that paid $2.3 billion in Federal criminal fines in 2009 – the largest ever paid by a drug company – for being a repeat offender in the marketing of 13 different drugs.
Meanwhile, the commission justifying the government’s claims about COVID-19 and injections (aka “vaccines”) will be hard at work writing their fictive report that will justify ex post facto the terrible damage that has occurred and that will continue to occur for many years. Censorship and threats against dissidents will increase. The disinformation that dominates the corporate mainstream media will of course continue, but this will be supplemented by alternative media that are already buckling under the pressure to conform.
The fact that there has been massive censorship of dissenting voices by Google/ YouTube, Facebook, Twitter, Wikipedia, etc., and equally massive disinformation by commission and omission across media platforms, should make everyone ask why. Why repress dissent? The answer should be obvious but is not.
The fact that so many refuse to see the significance of this censorship clearly shows the hypnotic effects of a massive mind control operation.
Name calling and censorship are sufficient. Perfectly healthy people have now become a danger to others. So mask up, get your experimental shot, and shut up!
Your body is no longer inviolable. You must submit to medical procedures on your body whether you want them or not. Do not object or question. If you do, you will be punished and will become a pariah. The authorities will call you crazy, deviant, selfish. They will take away your rights to travel and engage in normal activities, such as attend college, etc.
Please do not recall The Nuremberg Code. Especially number 7: “Proper preparations should be made and adequate facilities provided to protect the experimental subject against even remote possibilities of injury, disability or death.” (my emphasis)
“Now is the time to just do what you are told,” as Anthony Fauci so benevolently declared.
I am not making a prediction. The authorities have told us what’s coming. Pay attention. Don’t be fooled. It’s a game they have devised. Keep people guessing. On edge. Relieved. Tense. Relaxed. Shocked. Confused. That’s the game. One day this, the next that. You’re on, you’re off. You’re in, you’re out. We are allowing you this freedom, but be good children or we will have to retract it. If you misbehave, you will get a time out. Time to contemplate your sins.
If you once thought that COVID-19 would be a thing of the past by now, or ever, think again. On May 3, 2021 The New York Times reported that the virus is here to stay. This was again reported on May 10. Hopes Fade for Global Herd Immunity. You may recall that we were told such immunity would be achieved once enough people got the “vaccine” or enough people contracted the virus and developed antibodies.
On May 9, on ABC News, Dr. Fauci, when asked about indoor mask requirements being relaxed, said, “I think so, and I think you’re going to probably be seeing that as we go along, and as more people get vaccinated.” Then he added: “We do need to start being more liberal, as we get more people vaccinated.”
But then, in what CNN reported as a Mother’s Day prediction, he pushed the date for “normality” out another year, saying, “I hope that [by] next Mother’s Day, we’re going to see a dramatic difference than what we’re seeing right now. I believe that we will be about as close to back to normal as we can. We’ve got to make sure that we get the overwhelming proportion of the population vaccinated. When that happens, the virus doesn’t really have any place to go. You’re not going to see a surge. You’re not going to see the kinds of numbers we see now.”
He said this with a straight face even though the experimental “vaccines,” by their makers own admissions, do not prevent the vaccinated from getting the virus or passing it on. They allege it only mitigates the severity of the virus if you contract it.
Notice the language and the vaccination meme repeated three times: “We get more people vaccinated.” (my emphasis) Not that more people choose to get vaccinated, but “we get” them vaccinated. Thank you, Big Daddy. And now we have another year to go until “we will be about as close to back to normal as we can.” Interesting phrase: as we can. It other words: we will never return to normality but will have to settle for the new normal that will involve fewer freedoms. Life will be reset, a great reset. Great for the few and terrible for the many.
Once two vaccines were enough; then, no, maybe one is sufficient; no, you will need annual or semi-annual booster shots to counteract the new strains that they say are coming. It’s a never-ending story with never-ending new strains in a massive never-ending medical experiment. The virus is changing so quickly and herd immunity is now a mystical idea, we are told, that it will never be achieved. We will have to be eternally vigilant.
But wait. Don’t despair. It looks like restrictions are easing up for the coming summer in the northern hemisphere. Lockdowns will be loosened. If you felt like a prisoner for the past year plus, now you will be paroled for a while. But don’t dispose of those masks just yet. Fauci says that wearing masks could become seasonal following the pandemic because people have become accustomed to wearing them and that’s why the flu has disappeared. The masks didn’t prevent COVID-19 but eliminated the flu. Are you laughing yet?
Censorship and lockdowns and masks and mandatory injections are like padded cells in a madhouse and hospital world where free-association doesn’t lead to repressed truths because free association isn’t allowed, neither in word nor deed. Speaking freely and associating with others are too democratic. Yes, we thought we were free. False consciousness is pandemic. Exploitation is seen as benevolence. Silence reigns. And the veiled glances signify the ongoing terror that has spread like a virus.
We are now in a long war with two faces. As with the one justified by the mass murders of September 11, 2001, this viral one isn’t going away.
The question is: Do we have to wait twenty years to grasp the obvious and fight for our freedoms?
We can be assured that Zelikow and his many associates at Covid Collaborative, including General Stanley McChrystal, Robert Gates, Arnie Duncan, Deval Patrick, Tom Ridge, et al. – a whole host of Republicans and Democrats backed by great wealth and institutional support, will not be “whacking moles” in their search for truth. Their agenda is quite different.
But then again, you may recall where they stood on the mass murders of September 11, 2001 and the endless wars that have followed.
DECLARATION OF CANADIAN PHYSICIANS FOR SCIENCE AND TRUTH
The Declaration
We are a broad and diverse group of Canadian physicians from across Canada who are sending out this urgent declaration to the Colleges of Physicians and Surgeons of our various Provinces and Territories and to the Public at large, whom we serve.
On April 30, 2021, Ontario’s physician licensing body, the College of Physicians and Surgeons of Ontario (CPSO), issued a statement forbidding physicians from questioning or debating any or all of the official measures imposed in response to COVID-19. 1
The CPSO then went on to threaten physicians with punishment – investigations and disciplinary action.
We regard this recent statement of the CPSO to be unethical, anti-science and deeply disturbing.
As physicians, our primary duty of care is not to the CPSO or any other authority, but to our patients.
When we became physicians, we pledged to put our patients first and that our ethical and professional duty is always first toward our patients. The CPSO statement orders us to violate our duty and pledge to our patients in the following ways:
1. Denial of the Scientific Method itself: The CPSO is ordering physicians to put aside the scientific method and to not debate the processes and conclusions of science.
We physicians know and continue to believe that throughout history, opposing views, vigorous debate and openness to new ideas have been the bedrock of scientific progress. Any major advance in science has been arrived at by practitioners vigorously questioning “official” narratives and following a different path in the pursuit of truth.
2. Violation of our Pledge to use Evidence-Based Medicine for our patients: By ordering us not to debate and not to question, the CPSO is also asking us to violate our pledge to our patients that we will always seek the best, evidence-based scientific methods for them and advocate vigorously on their behalf.
The CPSO statement orders physicians for example, not to discuss or communicate with the public about “lockdown” measures. Lockdown measures are the subject of lively debate by world-renown and widely respected experts and there are widely divergent views on this subject. The explicitly anti-lockdown Great Barrington Declaration – https://gbdeclaration.org – was written by experts from Harvard, Stanford and Oxford Universities and more than 40,000 physicians from all over the world have signed this declaration. Several international experts including Martin Kuldorf (Harvard), David Katz (Yale), Jay Bhattacharya (Stanford) and Sunetra Gupta (Oxford) continue to strongly oppose lockdowns.
The CPSO is ordering physicians to express only pro-lockdown views, or else face investigation and discipline. This tyrannical, anti-science CPSO directive is regarded by thousands of Canadian physicians and scientists as unsupported by science and as violating the first duty of care to our patients.
3. Violation of Duty of Informed Consent: The CPSO is also ordering physicians to violate the sacred duty of informed consent – which is the process by which the patient/public is fully informed of the risks, benefits and any alternatives to the treatment or intervention, before consent is given.
The Nuremberg Code, drafted in the aftermath of the atrocities perpetrated within the Nazi concentration camps – where horrific medical experiments were performed on inmates without consent – expressly forbids the imposition of any kind of intervention without informed consent.
In the case of the lockdown intervention for example, physicians have a fiduciary duty to point out to the public that lockdowns impose their own costs on society, including in greatly increased depression and suicide rates, delayed investigation and treatment of cancer (including delayed surgery, chemotherapy and radiation therapy), ballooning surgical waiting lists (with attendant greatly increased patient suffering) and increased rates of child and domestic abuse.
We physicians believe that with the CPSO statement of 30 April 2021, a watershed moment in the assault on free speech and scientific inquiry has been reached.
By ordering physicians to be silent and follow only one narrative, or else face discipline and censure, the CPSO is asking us to violate our conscience, our professional ethics, the Nuremberg code and the scientific pursuit of truth.
We will never comply and will always put our patients first.
The CPSO must immediately withdraw and rescind its statement of 30 April 2021.
We also give notice to other Canadian and international licensing authorities for physicians and allied professions that the stifling of scientific inquiry and any order to violate our conscience and professional pledge to our patients, itself may constitute a crime against humanity.
1 College of Physicians and Surgeons of Ontario Statement on Public Health Misinformation (4/30/21). https://twitter.com/cpso_ca/status/1388211577770348544
The College is aware and concerned about the increase of misinformation circulating on social media and other platforms regarding physicians who are publicly contradicting public health orders and recommendations. Physicians hold a unique position of trust with the public and have a professional responsibility to not communicate anti-vaccine, anti-masking, anti-distancing and anti-lockdown statements and/or promoting unsupported, unproven treatments for COVID-19. Physicians must not make comments or provide advice that encourages the public to act contrary to public health orders and recommendations. Physicians who put the public at risk may face an investigation by the CPSO and disciplinary action, when warranted. When offering opinions, physicians must be guided by the law, regulatory standards, and the code of ethics and professional conduct. The information shared must not be misleading or deceptive and must be supported by available evidence and science.
Signatures
- Anne Shannon
- Andrea Roy
- Adam Salt
- Alexandre Guay
- Andrea Zaretsky
- Andrew Mahon
- annkwist@rogers.com Kwist
- Antonio Coffa
- Deno Gettas
- Beata G
- Bernard de Souza
- Beth Lindhorst
- Karen Mackey
- Bruce McKay
- Ron Bublitz
- Carla Dancey
- Deb Mair
- ROBERT PAQUETTE
- Christine Pohanka
- Cindy Create
- Claire Gosselin
- Corinne Mackenzie
- Barbara & David Schmidt
- Judith Robinson
- Donna Cuomo
- Deborah Kay
- Julia McLaren
- Dwayne Vann
- Emma Sattar
- Dave Thompson
- Elizabeth Romanowska-Konsik
- Darlene Elias
- Elizabeth Balcar
- Erin Beckman
- Richard Caviedes
- Chris Filby
- Pat Brown
- Rachel Vlietstra
- Greg Schmalz
- Gerard Lamontagne
- Freya Godard
- Ken Roberson
- Blaine Goodine
- Grazyna Sanchez
- Mary Hale
- Anja Reich
- Silvia engels
- Helke Ferrie
- Vicki Samson
- Laura Peterson
- Michelle Greenwell
- Jackie Beninato
- Jake Hoheisel
- Jan Fiss
- Jeff Graham
- Jennifer LONERGAN
- Judy Symington
- Janine Jalbert
- Jordyn Kaye
- Jeremy McKee
- Julie Montpetit
- Kathleen Perry
- Kathy Braun
- Katia Rodrigues
- Keith Baxter
- Cheryl Leite
- Larissa Flanagan
- Laurie Fetherstonhaugh
- Lauren Annez
- Sharon Leonard
- Lorraine Struyk
- larry hachey
- Linda Winger
- Luciano Perna
- Madeleine Menard
- Marissa Secord
- Marlena Murray
- Marnee Stern
- Lori McKay
- Michael Germain
- Michele Mihalik
- Michelle Losier
- Marlee Moore
- Nancy Chown
- Nikki Pulla
- Norma Ford
- Nicoline Lentze
- Nigel Bell
- Melodie VanderWal
- Colleen Roberts
- Pamela Velos
- Rick Hayter
- Rochagné Kilian
- Dale & Roeli Lutz
- ronald beaulieu
- Sarah MacInnis
- Sarah Pollard
- Sara Pahlevan
- Sabina SARGEANT
- Stephanie Cheung
- Sebastian Rozdzynski
- Sherry Lee
- Jacinthe Phillips
- Sophie Hawkins
- Steve Foget
- Sue Timmermans
- sydney felker
- Taron Puri
- Christine Simpson
- Tibor Finesz
- Lara Doucette
- Thomas J Tassé
- Thomas Russell
- Erica Tratch
- Summer Hanes
- Uwe Grunert
- Valerie Debicki
- Vladikir Gagachev
- Verna Hutchinson
- Roger Baird
Laurence Fox Threatens Met Police & Calls Them “Thugs”
By Richie Allen | May 10, 2021
In a series of extraordinary tweets, the actor turned politician Laurence Fox called the Metropolitan Police thugs and said that there would be trouble if they kept returning to his house for no reason.
Yesterday, police visited his home for the second time in two months. The officers said they had received reports of a party at the actor’s address. He says he was having dinner with his father.
Fox tweeted that the police presence had made his daughters cry and that officers should go and solve knife crime. The Reclaim Party leader was previously visited by Met Police officers in March ahead of the City Hall elections.
The officers warned him then, that his campaigning could be in breach of lockdown restrictions. Fox filmed the encounter and shared it online.
We really are here now. The police really are knocking on doors to count the number of people in your home, in your private residence. Maybe the Met police should rename themselves the stasi.
Even more worrying for me, is that there’s no outrage. Look at Twitter. Rather than pile-on the police for behaving like Nazi’s, users prefer to mock Fox and his family and call him a racist.
COVID-19: Just the Facts

By Will Jones | Lockdown Sceptics | May 9, 2021
Twelve key questions about COVID-19 and lockdowns answered. All answers fully referenced from peer-reviewed research and leading authorities.
How deadly is COVID-19?
Stanford Professor of Medicine and Epidemiology John P. A. Ioannidis in the European Journal of Clinical Investigation has reviewed data from studies globally and estimated that the infection fatality rate (IFR) of COVID-19 is around 0.15%. It varies considerably by region (for reasons such as demographics and prior susceptibility) and between countries within regions. In Europe and the Americas it is around 0.3%-0.4%. In Africa and Asia it is around 0.05%.
It also varies considerably between ages and depending on the presence of underlying conditions. Cambridge Professor of Statistics David Spiegelhalter has used the mortality data from the spring 2020 epidemic in England and Wales to show that the risk of dying from a COVID-19 infection roughly increases by 12-13% for each year older, doubles every 5-6 years and is around 10,000 times higher for the oldest compared to the youngest. It is also roughly equivalent to the normal risk of dying in a given year (though is mostly in addition to that normal risk). Men have around double the risk of death of women of the same age.

The average age of death from Covid in England and Wales in the spring epidemic was 80.4 according to the ONS, splitting 78.7 for men and 82.5 for women. The average age of death in the UK is 79.3 for men and 82.9 for women (though note these are modelled estimates of life expectancy at birth based on life tables, not the actual average age of those who die each year). Public Health England has estimated that life expectancy was reduced by 1.3 years for men and 0.9 years for women in 2020 due to the Covid and lockdown death tolls, though these figures are also modelled.
Economist John Appleby writing in the BMJ has shown that every year prior to 2009 was more deadly than 2020 in England and Wales once the size and age of the population is taken into account. The same analysis also shows that previous pandemics have not resulted in continued elevated death rates for more than a year or two despite not having vaccines for the diseases, indicating how the human immune system and the diseases adapt into a less deadly relationship.

A Swedish review of Covid deaths outside hospitals (i.e., in care homes and private homes) in one county found 85% were from a different underlying cause. In Northern Ireland, 38% of Covid deaths in spring 2020 were determined to be not primarily due to COVID-19. However, the same figure in England and Wales was 8%, suggesting significant differences in how Covid deaths are registered between jurisdictions.
How is COVID-19 spread?
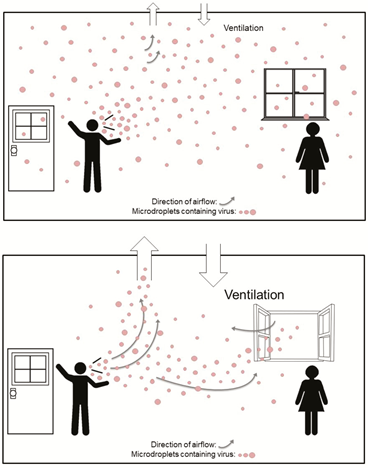
According to the most up-to-date data, COVID-19 primarily spreads via aerosols that build-up in the air of a room rather than via larger droplets or through contact with surfaces (fomites). This is why many of the measures taken to combat the spread of COVID-19, such as distancing, barriers, face masks (see below) and cleaning surfaces are ineffective. Outdoor transmission is very rare.
Public Health England has used data from the Government testing programme to show that the secondary attack rate (proportion of contacts who catch the virus from an infected person) in private homes is around 10.1%. An American study in JAMA found it was 16.6%.
The low secondary attack rate in the high-exposure context of private homes is indicative of high levels of pre-existing immunity to the disease, as discussed in the BMJ by Peter Doshi. Note that immunity is not binary – a person can be resistant on one occasion and not resistant on another, for a variety of reasons. Cross-reactive T-cells that provide a measure of immunity have been found in a number of studies in 20-50% of unexposed people. Exposure without detectable infection (detectable by a PCR test) has also been found to induce a degree of T-cell immunity.
Infection with COVID-19 has been shown in a number of studies, including one on U.S Marines published in the Lancet, to confer natural immunity that gives around 80% protection from re-infection and 90% protection from symptomatic re-infection, with ten times lower viral load (corresponding to infectiousness).
What about asymptomatic and pre-symptomatic transmission?
Asymptomatic infection is typically characterised by a much lower viral load and consequently much lower infectiousness. The study in JAMA on household secondary attack rate (SAR) cited above found that asymptomatic infections had a SAR of just 0.7% versus a SAR of 18% for symptomatic infection. The proportion of infections that are asymptomatic increases among those with immunity from previous infection or vaccination, showing that it is a characteristic of immunity.
People become infectious around two days prior to onset of symptoms as viral load peaks. This pre-symptomatic transmission is estimated to account for around 6.4% of spread, according to a study of actual transmission events from Singapore. Modelled estimates of the contribution of pre-symptomatic spread appear to go too high.
This means that people without symptoms, whether asymptomatic or pre-symptomatic, are not major drivers of the epidemic.
Do lockdowns work?
Restrictions on social contact, such as stay-at-home orders, business closures and gathering limits, have consistently been shown in peer-reviewed studies to have had no significant impact on outcomes such as Covid infections and deaths. Here is a sample, with a key quote from each.
- “Full lockdowns and wide-spread COVID-19 testing were not associated with reductions in the number of critical cases or overall mortality.” “A country level analysis measuring the impact of government actions, country preparedness and socioeconomic factors on COVID-19 mortality and related health outcomes” by Rabail Chaudhry, George Dranitsaris, Talha Mubashir, Justyna Bartoszko, Sheila Riazi. EClinicalMedicine (Lancet) 25 (2020) 100464, July 21st, 2020.
- “We find that shelter-in-place orders had no detectable health benefits, only modest effects on behaviour, and small but adverse effects on the economy.” “Evaluating the effects of shelter-in-place policies during the COVID-19 pandemic” by Christopher R. Berry, Anthony Fowler, Tamara Glazer, Samantha Handel-Meyer, and Alec MacMillen, Proceedings of the National Academy of Science of the USA, April 13th, 2021.
- “Stringency of the measures settled to fight pandemia, including lockdown, did not appear to be linked with death rate.” “Covid-19 Mortality: A Matter of Vulnerability Among Nations Facing Limited Margins of Adaptation” by Quentin De Larochelambert, Andy Marc, Juliana Antero, Eric Le Bourg, and Jean-François Toussaint. Frontiers in Public Health, November 19th, 2020.
- “Comparing weekly mortality in 24 European countries, the findings in this paper suggest that more severe lockdown policies have not been associated with lower mortality. In other words, the lockdowns have not worked as intended.” “Did Lockdown Work? An Economist’s Cross-Country Comparison” by Christian Bjørnskov. CESifo Economic Studies March 29th, 2021.
- “While small benefits cannot be excluded, we do not find significant benefits on case growth of more restrictive NPIs.” “Assessing Mandatory Stay‐at‐Home and Business Closure Effects on the Spread of COVID‐19” by Eran Bendavid, Christopher Oh, Jay Bhattacharya, John P.A. Ioannidis. European Journal of Clinical Investigation, January 5th, 2021.
Studies which conclude otherwise are invariably based on models rather than data.
Professor Simon Woods, a mathematician, has shown that infections were in decline prior to the start of all three lockdowns in England.

You can find a useful round-up of the studies showing lockdowns don’t work at AIER.
Does social distancing work?
Many studies (including some of those above) which conclude that lockdowns don’t work nonetheless add that voluntary social distancing practices do reduce infections or deaths by suppressing spread. However, this is typically stated without supporting evidence. In fact, the evidence on this is also quite weak.
An international comparison study in Nature by R.F. Savaris and colleagues found that actually staying at home (measured by mobile phone mobility data) made no significant difference to outcomes either. “We were not able to explain the variation of deaths per million in different regions in the world by social isolation, herein analysed as differences in staying at home, compared to baseline,” they wrote. “In the restrictive and global comparisons, only 3% and 1.6% of the comparisons were significantly different, respectively.”
The fact that transmission is mainly via aerosols that build-up in the air of a room means that keeping a physical distance from people makes little difference to risk. A study from MIT used a model of viral dynamics to show that physical distancing makes no significant difference to transmission risk in indoor spaces.
Social distancing doesn’t have a significant impact on infections or deaths for a number of reasons.
Firstly, much of the spread, especially which leads to serious infection and death, is nosocomial, i.e., it occurs in care homes and hospitals. According to data from the ONS, 39% of Covid deaths in England and Wales in spring 2020 were care home residents. According to Public Health Scotland, between half and two thirds of serious Covid infections during the winter were picked up in hospital.
Second, not everyone is staying at home, even when they’re unwell. ONS figures show that nearly half of people in the U.K. travelled to work during the January lockdown. A major survey from King’s College London found that less than half of those with symptomatic Covid fully self-isolated during their infectious period.
Because social distancing does not significantly suppress viral spread, there is no reason to expect a large new wave of infections when social distancing practices are eased or ended. This aligns with the experience of states in the U.S. such as Florida, Texas and South Dakota which ended restrictions or never imposed them and did not experience noticeably worse outcomes than states which maintained them.

Are lockdowns harmful?
Lockdowns are extremely harmful to human health and well-being, leading to large reductions in access to healthcare, education and sources of social support, and considerable reductions in economic activity resulting in large-scale losses of earnings and livelihoods.
A U.K. Government report estimated that the first lockdown would kill at least 63,000 people through missed medical care and worsened economic conditions. It argued this loss of life was justified because COVID-19 was predicted to kill directly up to 1.5 million people or around 2.2% of the population. However, this figure is many times higher than the death toll in any country on earth no matter how lax its response. The worst affected country as of May 8th 2021, Hungary, has lost less than 0.3% of its population with COVID-19 according to official data. Sweden, with looser restrictions, has lost less than 0.14%.
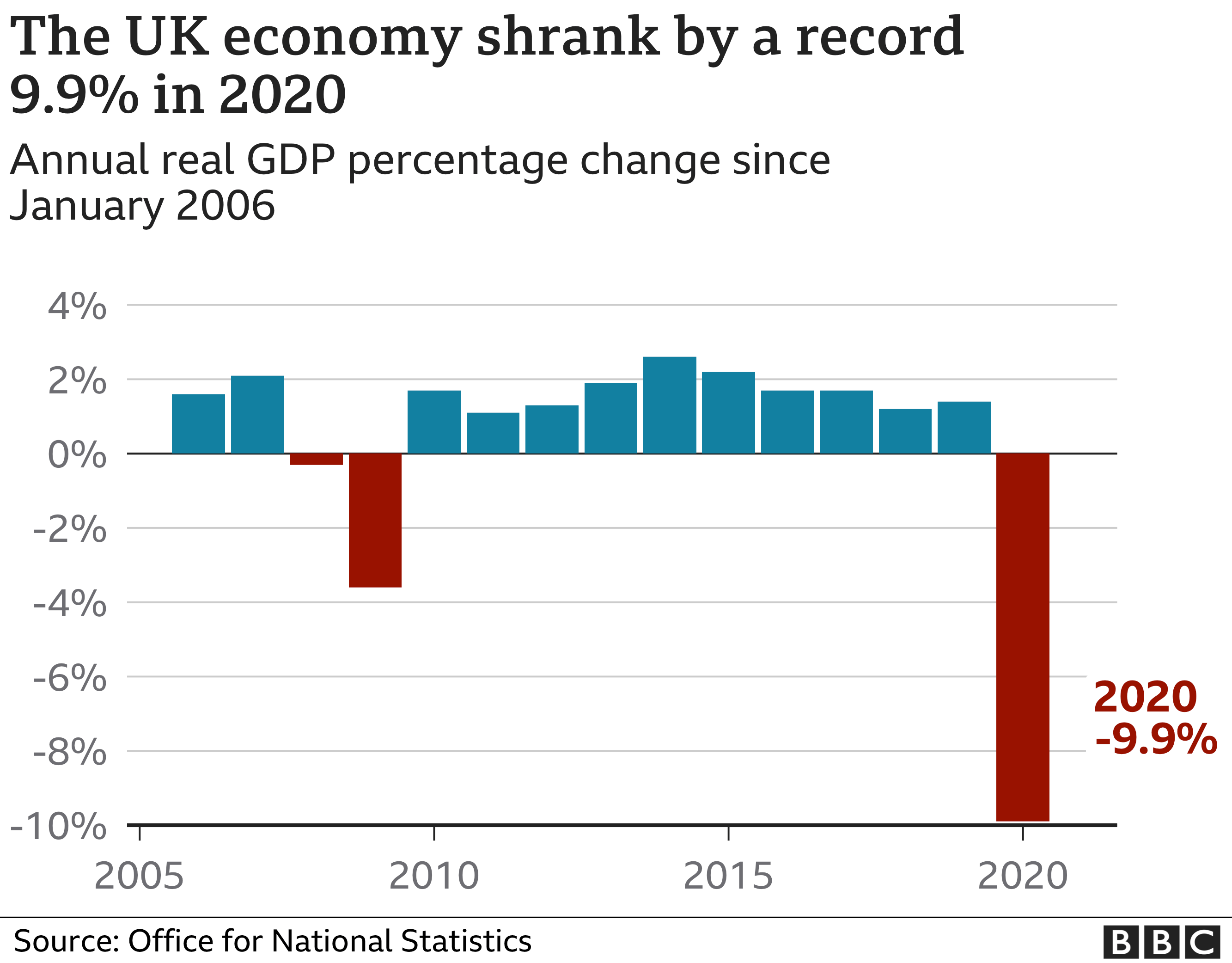
The UK economy shrank by almost 10% in 2020, the largest annual fall on record.
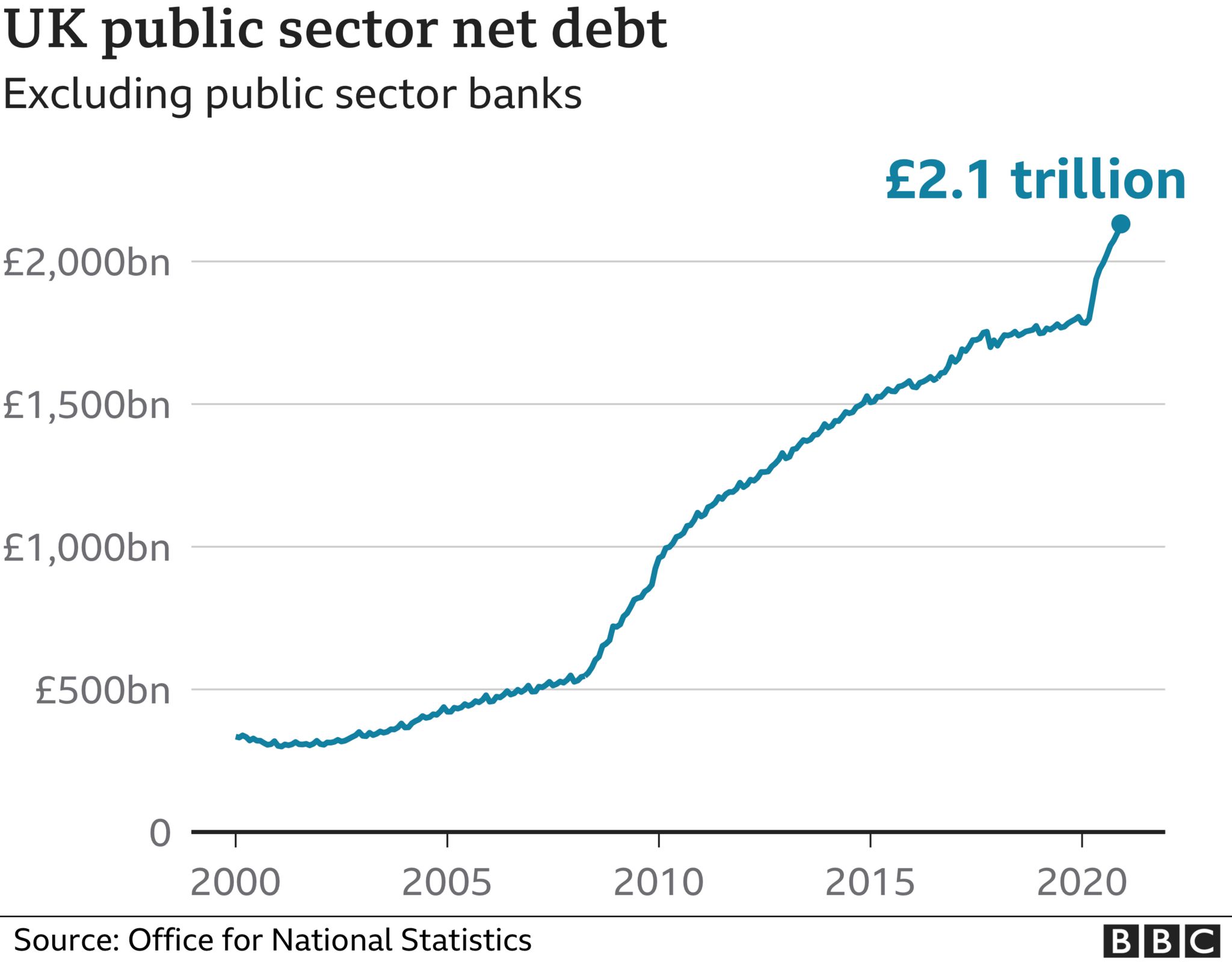
UK national debt has also jumped considerably during the pandemic to £2.1 trillion.
Lockdowns take a toll on mental health. The ONS estimates that the proportion of UK adults experiencing some form of depression is “more than double” what it was before the pandemic, increasing from 10% in 2019 to 21% in 2020.
The United Nations has estimated that disruption in healthcare services caused by government responses to COVID-19 in Afghanistan, Nepal, Bangladesh, India, Pakistan and Sri Lanka (home to some 1.8 billion people) may have led to 239,000 maternal and child deaths. Of these, an estimated 228,000 were children under five, who are at very low risk from the virus.
The United Nations has also estimated that an additional 207 million people could be pushed into extreme poverty over the next decade due to the long term impact of lockdowns.
A website has been created by the signatories of the Great Barrington Declaration to document some of the harms of lockdowns called Collateral Global.
Are the vaccines effective?
The vaccines, particularly the mRNA vaccines such as Pfizer’s, appear to be effective at preventing COVID-19 infection. They succeed in producing antibodies to SARS-CoV-2. They appear to give a level of protection comparable to that provided by infection (80-90%). A Public Health England study suggested they cut transmission rates in half after one dose.
However, among those groups who are most vulnerable to the virus they appear to be significantly less effective. A Danish study in nursing homes found that the Pfizer vaccine (often the best performing vaccine) was reduced to 64% effectiveness at preventing COVID-19 among fully vaccinated care home residents. A German study found a third of those over 80 fully vaccinated with the Pfizer jab did not generate antibodies.
Some coronavirus variants are showing signs of partial escape from vaccine-induced immunity. The AstraZeneca vaccine, for example, was found to be only 21.9% effective against the South African variant. The need for regular boosters tailored to new variants has been suggested.
Are the vaccines safe?
A number of safety concerns have been raised about the vaccines, some of which have led to some of the vaccines being restricted or removed in some countries.
The U.S. vaccine adverse effects reporting system (VAERS) has generated reports of deaths linked with Covid vaccinations at a rate 30 times greater than with flu vaccinations (although the number of deaths associated with flu vaccines is very low). Hundreds of serious adverse reactions have been reported in the UK.
A major study in the UK reported “an abundance of patients admitted to hospital within seven days of vaccination”.
The vaccines involve using genetic instructions to induce the body to produce the virus’s spike protein. However, there are concerns that the spike protein is itself pathogenic. One study reported that: ”The SARS-CoV-2 spike protein (without the rest of the viral components) triggers cell signalling events that may promote pulmonary vascular remodelling and pulmonary arterial hypertension as well as possibly other cardiovascular complications.” The spike protein by itself was shown to harm the lungs of mice.
There is also evidence that a Covid vaccination programme can cause a spike in infections. The association of vaccination programmes and Covid surges in a number of countries has been discussed in the pages of the BMJ. Dr. Clare Craig has argued against it being behaviour based (people letting their guard down) and pointed to the results from the vaccine trials which showed a reduction in white blood cells in the days following the jab that may indicate temporary immune suppression.

The risk-benefit calculation for Covid vaccination has been acknowledged by leading figures including Chief Medical Officer Chris Whitty to be different for those who are at lower risk from the disease, particularly the young. In the U.K., the AstraZeneca vaccine is no longer recommended for those under 40.
Do masks work?
Because transmission of COVID-19 is primarily via aerosols building up in the air of indoor spaces, face masks have little to no impact on risk of infection or transmission. This is because even surgical masks do not filter out enough infected aerosols to be considered respiratory protection devices. In addition, aerosols routinely escape with breath around the sides of the mask.
Accordingly, studies consistently find no significant benefit from wearing masks. The Danmask-19 randomised controlled trial (RCT) found that surgical masks provide no significant protection for the wearer from COVID-19 infection. This is in line with other RCTs for other similar viruses. One, published in autumn 2020, concluded face masks “did not seem to be effective against laboratory-confirmed viral respiratory infections nor against clinical respiratory infection”.
The Government’s scientific advisers admit masks are little use to the wearer, saying they “may provide a small amount of protection to an uninfected wearer; however, this is not their primary intended purpose”. Rather they are “predominantly a source control” (preventing transmission). The advisers cite the findings of a study by Brainard et al, which reviews a number of RCTs and concludes surgical masks provide the wearer with protection from just 6% of infections. The same study’s review of RCTs for masks as source control finds no evidence above low quality.
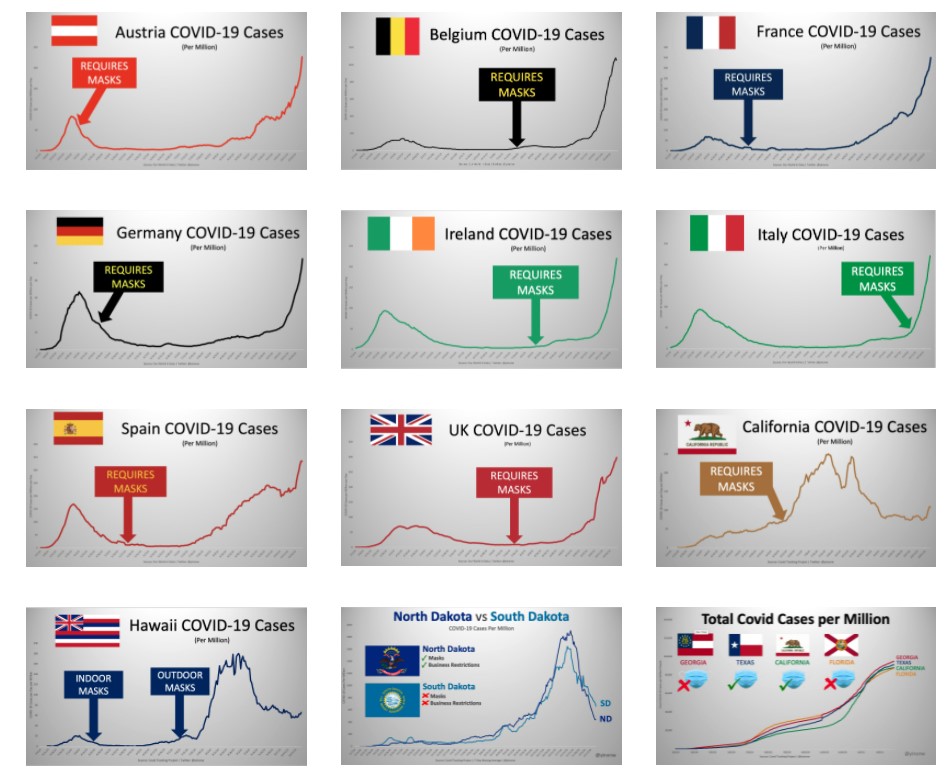
Yinon Weiss has plotted real-world data to show there is no sign of mask mandates altering the course or size of Covid epidemics in countries and states around the world.
Are masks safe?
A number of studies raise concerns about the safety of face masks used daily and for long periods.
A study in Water Research has called for a “full investigation” into the safety of face masks, after detecting easily detached particles of microplastics and heavy metals. “The toxicity of some of the chemicals found and the postulated risks of the rest of the present particles and molecules, raises the question of whether DPFs [disposable plastic face masks] are safe to be used on a daily basis.”

Professor Michael Braungart, head of the Hamburg Environmental Institute, has warned: “Many of them are made of polyester, so you have a microplastic problem. If I have the mask in front of my face, then of course I inhale the microplastic directly and these substances are much more toxic than if you swallow them, as they get directly into the nervous system,”
The World Health Organisation highlights a number of potential harms and risks of prolonged mask use in its guidance, including contamination, skin lesions and headaches.
A study in Clinical Research in Cardiology, “Effects of surgical and FFP2/N95 face masks on cardiopulmonary exercise capacity“, finds significant impact on lung function from wearing a mask during exercise: “The pulmonary function parameters were significantly lower with mask… the ventilation was significantly reduced with both face masks… Peak blood lactate response was reduced with mask. … Participants reported consistent and marked discomfort wearing the masks.”
Face masks have been found to be a transmission risk, with infectious virus remaining on the mask for several days.
There are also important psychological consequences from frequent and widespread mask wearing.
Are effective treatments available?
A number of treatments have been used by clinicians around the world that appear to have some beneficial impact on treating COVID-19. Among the most promising are Ivermectin, as detailed in the American Journal of Therapeutics, and Budesonide, as detailed in the Lancet. The safety profile of these well-established drugs is well-known and not controversial.
What should governments have done?
The UK Government has a Pandemic Preparedness Strategy, drafted in 2011 in line with international ethical norms and scientific evidence. It is primarily for an influenza pandemic, but also envisages a SARS-like pandemic and anticipates up to 315,000 deaths, most in the space of a few weeks. It primarily recommends hand hygiene and self-isolation of the infected. It does not recommend school closures, border closures, business closures, face masks in the community or bans on large gatherings. It aims to encourage “business as usual”, stating:
During a pandemic, the Government will encourage those who are well to carry on with their normal daily lives for as long and as far as that is possible, whilst taking basic precautions to protect themselves from infection and lessen the risk of spreading influenza to others. The UK Government does not plan to close borders, stop mass gatherings or impose controls on public transport during any pandemic. …
Large public gatherings or crowded events where people may be in close proximity are an important indicator of ‘normality’ and may help maintain public morale during a pandemic. The social and economic consequences of advising cancellation or postponement of large gatherings are likely to be considerable for event organisers, contributors and participants.
The Government should have followed this strategy, as it was doing until around March 16th 2020, and not been pressured into deviating from it. It should have recognised that no pandemic has caused elevated mortality for more than a year or two and maintained a sense of proportion.
That said, the strategy is notably silent on the role of hospitals and care homes in spreading the virus (nosocomial spread). It includes no special provisions for protecting care home residents, hospital patients, or any other vulnerable category. It could therefore be improved by considering how focused protection, as advocated in the Great Barrington Declaration, could reduce deaths among the vulnerable. It could also give more consideration to how infected patients could be more effectively isolated from uninfected patients in hospitals.
It should also place more emphasis on quickly finding effective treatments besides vaccines, especially repurposed drugs which are readily available and whose safety profile is known.
Dr Mike Yeadon – “Please warn everyone not to go near top-up vaccines”
THE DAILY EXPOSE • MAY 9, 2021
We spoke to Dr Mike Yeadon about his views on the experimental Covid-19 vaccines, the medicine regulators approving them and his fears for the future.
From the outset, Dr. Yeadon said “I’m well aware of the global crimes against humanity being perpetrated against a large proportion of the worlds population.
“I feel great fear, but I’m not deterred from giving expert testimony to multiple groups of able lawyers like Rocco Galati in Canada and Reiner Fuellmich in Germany.
“I have absolutely no doubt that we are in the presence of evil (not a determination I’ve ever made before in a 40-year research career) and dangerous products.
“In the U.K., it’s abundantly clear that the authorities are bent on a course which will result in administering ‘vaccines’ to as many of the population as they can. This is madness, because even if these agents were legitimate, protection is needed only by those at notably elevated risk of death from the virus. In those people, there might even be an argument that the risks are worth bearing. And there definitely are risks which are what I call ‘mechanistic’: inbuilt in the way they work.
“But all the other people, those in good health and younger than 60 years, perhaps a little older, they don’t perish from the virus. In this large group, it’s wholly unethical to administer something novel and for which the potential for unwanted effects after a few months is completely uncharacterized.
“In no other era would it be wise to do what is stated as the intention.
“Since I know this with certainty, and I know those driving it know this too, we have to enquire: What is their motive?
“While I don’t know, I have strong theoretical answers, only one of which relates to money and that motive doesn’t work, because the same quantum can be arrived at by doubling the unit cost and giving the agent to half as many people. Dilemma solved. So it’s something else. Appreciating that, by entire population, it is also intended that minor children and eventually babies are to be included in the net, and that’s what I interpret to be an evil act.
“There is no medical rationale for it. Knowing as I do that the design of these ‘vaccines’ results, in the expression in the bodies of recipients, expression of the spike protein, which has adverse biological effects of its own which, in some people, are harmful (initiating blood coagulation and activating the immune ‘complement system’), I’m determined to point out that those not at risk from this virus should not be exposed to the risk of unwanted effects from these agents.”
The Israel Supreme Court decision last week cancelling COVID flight restrictions said: “In the future, any new restrictions on travel into or out of Israel need, in legal terms, a comprehensive, factual, data-based foundation.”
In a talk you gave four months ago, you said –
“The most likely duration of immunity to a respiratory virus like SARS CoV-2 is multiple years. Why do I say that? We actually have the data for a virus that swept through parts of the world seventeen years ago called SARS, and remember SARS CoV-2 is 80% similar to SARS, so I think that’s the best comparison that anyone can provide.
“The evidence is clear: These very clever cellular immunologists studied all the people they could get hold of who had survived SARS 17 years ago. They took a blood sample, and they tested whether they responded or not to the original SARS and they all did; they all had perfectly normal, robust T cell memory. They were actually also protected against SARS CoV-2, because they’re so similar; it’s cross immunity.
“So, I would say the best data that exists is that immunity should be robust for at least 17 years. I think it’s entirely possible that it is lifelong. The style of the responses of these people’s T cells were the same as if you’ve been vaccinated and then you come back years later to see if that immunity has been retained. So I think the evidence is really strong that the duration of immunity will be multiple years, and possibly lifelong.”
In other words, previous exposure to SARS – that is, a variant similar to SARS CoV-2 – bestowed SARS CoV-2 immunity.
The Israel government cites new variants to justify lockdowns, flight closures, restrictions, and Green Passport issuance. Given the Supreme Court verdict, do you think it may be possible to preempt future government measures with accurate information about variants, immunity, herd immunity, etc. that could be provided to the lawyers who will be challenging those future measures?
Yeadon: “What I outlined in relation to immunity to SARS is precisely what we’re seeing with SARS-CoV-2.The study is from one of the best labs in their field.” So, theoretically, people could test their T-cell immunity by measuring the responses of cells in a small sample of their blood. There are such tests, they are not “high throughput” and they are likely to cost a few hundred USD each on scale. But not thousands. The test I’m aware of is not yet commercially available, but research only in U.K.
“However, I expect the company could be induced to provide test kits “for research” on scale, subject to an agreement. If you were to arrange to test a few thousand non vaccinated Israelis, it may be a double edged sword. Based on other countries experiences, 30-50% of people had prior immunity & additionally around 25% have been infected & are now immune.
“Personally, I wouldn’t want to deal with the authorities on their own terms: that you’re suspected as a source of infection until proven otherwise. You shouldn’t need to be proving you’re not a health risk to others. Those without symptoms are never a health threat to others. And in any case, once those who are concerned about the virus are vaccinated, there is just no argument for anyone else needing to be vaccinated.”
My understanding of a “leaky vaccine” is that it only lessens symptoms in the vaccinated, but does not stop transmission; it therefore allows the spread of what then becomes a more deadly virus.
For example, in China they deliberately use leaky Avian Flu vaccines to quickly cull flocks of chicken, because the unvaccinated die within three days. In Marek’s Disease, from which they needed to save all the chickens, the only solution was to vaccinate 100% of the flock, because all unvaccinated were at high risk of death. So how a leaky vax is utilized is intention-driven, that is, it is possible that the intent can be to cause great harm to the unvaccinated.
Stronger strains usually would not propagate through a population because they kill the host too rapidly, but if the vaccinated experience only less-serious disease, then they spread these strains to the unvaccinated who contract serious disease and die.
Do you agree with this assessment? Furthermore, do you agree that if the unvaccinated become the susceptible ones, the only way forward is HCQ prophylaxis for those who haven’t already had COVID-19?
Would the Zelenko Protocol work against these stronger strains if this is the case? And if many already have the aforementioned previous “17-year SARS immunity”, would that then not protect from any super-variant?
“I think the Gerrt Vanden Bossche story is highly suspect. There is no evidence at all that vaccination is leading or will lead to ‘dangerous variants’. I am worried that it’s some kind of trick.
“As a general rule, variants form very often, routinely, and tend to become less dangerous & more infectious over time, as it comes into equilibrium with its human host. Variants generally don’t become more dangerous.
“No variant differs from the original sequence by more than 0.3%. In other words, all variants are at least 99.7% identical to the Wuhan sequence.
“It’s a fiction, and an evil one at that, that variants are likely to “escape immunity.”
“Not only is it intrinsically unlikely – because this degree of similarity of variants means zero chance that an immune person (whether from natural infection or from vaccination) will be made ill by a variant – but it’s empirically supported by high-quality research.
“The research I refer to shows that people recovering from infection or who have been vaccinated ALL have a wide range of immune cells which recognize ALL the variants.
“This paper shows WHY the extensive molecular recognition by the immune system makes the tiny changes in variants irrelevant.
“I cannot say strongly enough: The stories around variants and need for top up vaccines are FALSE. I am concerned there is a very malign reason behind all this. It is certainly not backed by the best ways to look at immunity. The claims always lack substance when examined, and utilize various tricks, like manipulating conditions for testing the effectiveness of antibodies. Antibodies are probably rather unimportant in host protection against this virus. There have been a few ‘natural experiments’, people who unfortunately cannot make antibodies, yet are able quite successfully to repel this virus. They definitely are better off with antibodies than without. I mention these rare patients because they show that antibodies are not essential to host immunity, so some contrived test in a lab of antibodies and engineered variant viruses do NOT justify need for top up vaccines.
“The only people who might remain vulnerable and need prophylaxis or treatment are those who are elderly and/or ill and do not wish to receive a vaccine (as is their right).
“The good news is that there are multiple choices available: hydroxychloroquine, ivermectin, budesonide (inhaled steroid used in asthmatics), and of course oral Vitamin D, zinc, azithromycin etc. These reduce the severity to such an extent that this virus did not need to become a public health crisis.”
Do you feel the MHRA does a good job regulating ‘big pharma’? In what ways does ‘big pharma’ get around the regulator? Do you feel they did so for the mRNA jab?
“Until recently, I had high regard for global medicines regulators. When I was in Pfizer, and later CEO of a biotech I founded (Ziarco, later acquired by Novartis), we interacted respectfully with FDA, EMA, and the MHRA.
Always good quality interactions.
“Recently, I noticed that the Bill & Melinda Gates Foundation (BMGF) had made a grant to the Medicines and Healthcare products Regulatory Agency (MHRA)! Can that ever be appropriate? They’re funded by public money. They should never accept money from a private body.
“So here is an example where the U.K. regulator has a conflict of interest.” The European Medicines Agency failed to require certain things as disclosed in the ‘hack’ of their files while reviewing the Pfizer vaccine.
“You can find examples on Reiner Fuellmich’s “Corona Committee” online.
“So I no longer believe the regulators are capable of protecting us. ‘Approval’ is therefore meaningless.
“Dr. Wolfgang Wodarg and I petitioned the EMA Dec 1, 2020 on the genetic vaccines. They ignored us.
“Recently, we wrote privately to them, warning of blood clots, they ignored us. When we went public with our letter, we were completely censored. Days later, more than ten countries paused use of a vaccine citing blood clots.
“I think the big money of pharma plus cash from BMGF creates the environment where saying no just isn’t an option for the regulator.
“I must return to the issue of ‘top up vaccines’ (booster shots) and it is this whole narrative which I fear will he exploited and used to gain unparalleled power over us.
“PLEASE warn every person not to go near top up vaccines. There is absolutely no need to them. As there’s no need for them, yet they’re being made in pharma, and regulators have stood aside (no safety testing), I can only deduce they will be used for nefarious purposes.
“For example, if someone wished to harm or kill a significant proportion of the worlds population over the next few years, the systems being put in place right now will enable it.
“It’s my considered view that it is entirely possible that this will be used for massive-scale depopulation.”
Update on ivermectin for covid-19
By Sebastian Rushworth, M.D. | May 9, 2021
Back in January I wrote an article about four randomized controlled trials of ivermectin as a treatment for covid-19 that had at that time released their results to the public. Each of those four trials had promising results, but each was also too small individually to show any meaningful impact on the hard outcomes we really care about, like death. When I meta-analyzed them together however, the results suddenly appeared very impressive. Here’s what that meta-analysis looked like:

It showed a massive 78% reduction in mortality in patients treated with covid-19. Mortality is the hardest of hard end points, which means it’s the hardest for researchers to manipulate and therefore the least open to bias. Either someone’s dead, or they’re alive. End of story.
You would have thought that this strong overall signal of benefit in the midst of a pandemic would have mobilized the powers that be to arrange multiple large randomized trials to confirm these results as quickly as possible, and that the major medical journals would be falling over each other to be the first to publish these studies.
That hasn’t happened.
Rather the opposite, in fact. South Africa has even gone so far as to ban doctors from using ivermectin on covid-19 patients. And as far as I can tell, most of the discussion about ivermectin in mainstream media (and in the medical press) has centred not around its relative merits, but more around how its proponents are clearly deluded tin foil hat wearing crazies who are using social media to manipulate the masses.
In spite of this, trial results have continued to appear. That means we should now be able to conclude with even greater certainty whether or not ivermectin is effective against covid-19. Since there are so many of these trials popping up now, I’ve decided to limit the discussion here only to the ones I’ve been able to find that had at least 150 participants, and that compared ivermectin to placebo (although I’ll add even the smaller trials I’ve found in to the updated meta-analysis at the end).
As before, it appears that rich western countries have very little interest in studying ivermectin as a treatment for covid. The three new trials that had at least 150 participants and compared ivermectin with placebo were conducted in Colombia, Iran, and Argentina. We’ll go through each in turn.
The Colombian trial (Lopez-Medina et al.) was published in JAMA (the Journal of the American Medical Association) in March. There is one thing that is rather odd with this study, and that is that the study authors were receiving payments from Sanofi-Pasteur, Glaxo-Smith-Kline, Janssen, Merck, and Gilead while conducting the study. Gilead makes remdesivir. Merck is developing two expensive new drugs to treat covid-19. Janssen, Glaxo-Smith-Kline, and Sanofi-Pasteur are all developers of covid vaccines. In other words, the authors of the study were receiving funding from companies that own drugs that are direct competitors to ivermectin. One might call this a conflict of interest, and wonder whether the goal of the study was to show a lack of benefit. It’s definitely a little bit suspicious.
Anyway, let’s get to what the researchers actually did. This was a double-blind randomized controlled trial that recruited patients with mildly symptomatic covid-19 who had experienced symptom onset less than 7 days earlier. Potential participants were identified through a statewide database of people with positive PCR-tests. By “mildly symptomatic” the researchers meant people who had at least one symptom but who did not require high-flow oxygen at the time of recruitment in to the trial.
Participants in the treatment group received 300 ug/kg body weight of ivermectin every day for five days, while participants in the placebo group received an identical placebo. 300 ug/kg works out to 21 mg for an average 70 kg adult, which is quite high, especially when you consider that the dose was given daily for five days. For an average person, this would work out to a total dose of 105 mg. The other ivermectin trials have mostly given around 12 mg per day for one or two days, for a total dose of 12 to 24 mg (which has been considered enough because ivermectin has a long half-life in the body). Why this study gave such a high dose is unclear. However, it shouldn’t be a problem. Ivermectin is a very safe drug, and studies have been done where people have been given ten times the recommended dose without any noticeable increase in adverse events.
The stated goal of the study was to see if ivermectin resulted in more rapid symptom resolution than placebo. So participants were contacted by telephone every three days after inclusion in the study, up to day 21, and asked about what symptoms they were experiencing.
398 patients were included in the study. The median age of the participants was 37 years, and they were overall very healthy. 79% had no known co-morbidities. This is a shame. It means that this study is yet another one of those many studies that will not be able to show a meaningful effect on hard end points like hospitalization and death. It is a bit strange that studies keep being done on young healthy people who are at virtually zero risk from covid-19, rather than on the multi-morbid elderly, who are the ones we actually need an effective treatment for.
Anyway, let’s get to the results.
In the group treated with ivermectin, the average time from inclusion in the study to becoming completely symptom free was 10 days. In the placebo group that number was 12 days. So, the ivermectin treated patients recovered on average two days faster. However, the difference was not statistically significant, so the result could easily be due to chance. At 21 days after inclusion in the study, 82% had recovered fully in the ivermectin group, as compared to 79% in the placebo group. Again, the small difference was not statistically significant.
In terms of the hard end points that matter more, there were zero deaths in the ivermectin group and there was one death in the placebo group. 2% of participants in the ivermectin group required “escalation of care” (hospitalization if they were outside the hospital at the start of the study, or oxygen therapy if they were in hospital at the start of the study) as compared with 5% in the placebo group. None of these differences was statistically significant. But that doesn’t mean they weren’t real. Like I wrote earlier, the fact that this was a study of healthy young people meant that, even if a meaningful difference does exist in risk of dying of covid, or of ending up in hospital, this study was never going to find it.
So, what can we conclude?
Ivermectin does not meaningfully shorten duration of symptoms in healthy young people. That’s about all we can say from this study. Considering the conflicts of interest of the authors, my guess is that this was the goal of the study all along: Gather together a number of young healthy people that is too small for there to be any chance of a statistically significant benefit, and then get the result you want. The media will sell the result as “study shows ivermectin doesn’t work” (which they dutifully did).
It is interesting that there were signals of benefit for all the parameters the researchers looked at (resolution of symptoms, escalation of care, death), but that the relatively small number and good health status of the participants meant that there was little chance of any of the results reaching statistical significance.
Let’s move on to the next study, which is currently available as a pre-print on Research Square (Niaee et al.). It was randomized, double-blind, and placebo-controlled, and carried out at five different hospitals in Iran. It was funded by an Iranian university.
In order to be included in the trial, participants had to be over the age of 18 and admitted to hospital because of a covid-19 infection (which was defined as symptoms suggestive of covid plus either a CT scan typical of covid infection or a positive PCR test).
150 participants were randomized to either placebo (30 people) or varying doses of ivermectin (120 people). The fact that they chose to make the placebo group so small is a problem, because it makes it very hard to detect any differences even if they do exist, by making the statistical certainty of the results in the placebo group very low.
The participants were on average 56 years old and the average oxygen saturation before initiation of treatment was 89% (normal is more than 95%), so this was a pretty sick group. Unfortunately no information is provided on how far along people were in the disease course when they started receiving ivermectin. It stands to reason that the drug is more likely to work if given ten days after symptom onset than when given twenty days after symptom onset, since death usually happens around day 21. If you, for example, wanted to design a trial to fail, you could start treating people at a time point when there is no time for the drug you’re testing to have a chance work, so it would have been nice to know at what time point treatment started in this trial.
So, what were the results?
20% of the participants in the placebo group died (6 out of 30 people). 3% of the participants in the various ivermectin groups died (4 out of 120 people). That is an 85% reduction in the relative risk of death, which is huge.
So, in spite of the fact that the placebo group was so small, it was still possible to see a big difference in mortality. Admittedly, this is a pre-print (i.e. it hasn’t been peer-reviewed yet), and the absolute numbers of deaths are small, so there is some scope for random chance to have created these results (maybe people in the placebo group were just very unlucky!). However, the study appears to have followed all the steps expected for a high quality trial. It was carried out at multiple different hospitals, it used randomization and a control group that received a placebo, and it was double-blinded. And death is a very hard end point that is not particularly open to bias. So unless the researchers have falsified their data, then this study constitutes reasonably good evidence that ivermectin is highly effective when given to patients hospitalized with covid-19. That’s great, because it would mean that the drug can be given quite late in the disease course and still show benefit.
Let’s move on to the third trial (Chahla et al.), which is currently available as a pre-print on MedRxiv. It was carried out in Argentina, and funded by the Argentinean government. Like the first trial we discussed, this was a study of people with mild disease. It literally boggles my mind that so many researchers choose to study people with mild disease instead of studying those with more severe disease. Especially when you consider that these studies are all so small. A study of people with mild disease needs to be very large to find a statistically significant effect, since most people with covid do well regardless. The risk of false negative results is thus enormous. If you’re going to do a small-ish study, and you want to have a reasonable chance of producing results that reach statistical significance, it would make much more sense to do it on sick hospitalized patients.
The study was randomized, but it wasn’t blinded, and there was no placebo. In other words, the intervention group received ivermectin (24 mg per day), while the control group didn’t receive anything. This is a bad bad thing. It means that any non-hard outcomes produced by the study are really quite worthless, since there is so much scope for the placebo effect and other confounding factors to mess up the results. For hard outcomes, in particular death, it should be less of a problem (although we wouldn’t expect any deaths in such a small study of mostly healthy people with mild disease anyway).
The study included people over the age of 18 with symptoms suggestive of covid-19 and a positive PCR test. The average age of the participants was 40 years, and most had no underlying health issues. A total of 172 people were recruited in to the study.
The researchers chose to look at how quickly people became free of symptoms as their primary endpoint. This is enormously problematic, since the study, as already mentioned, wasn’t blinded and there was no placebo. Any difference between the groups could easily be explained by the placebo effect and by biases towards treatment benefit among the researchers.
Anyway, the study found that 49% in the treatment group were free of symptoms at five to nine days after the beginning of treatment, compared with 81% in the control group. However, the lack of blinding means that this result is worthless. The methodology is just too flawed.
No data is provided on the number of people who died in each group. Since it isn’t reported, I think it’s safe to assume that there were no deaths in either group. Nor is any data provided on the number of hospitalizations in each group.
So, what does this study tell us?
Absolutely nothing at all. What a waste of time and money.
Let’s move on and update our meta-analysis. The reason we need to do a meta-analysis here is that none of the trials of ivermectin is large enough on its own to provide a definitive answer as to whether it is a useful treatment for covid-19 or not. For those who haven’t heard of meta-analyses before, basically what you do is just take the results from all different studies in existence that fulfill your pre-selected criteria, and then put them together, so as a to create a single large “meta”-study. This allows you to produce results that have a much higher level of statistical significance. It is particularly useful in a situation where all the individual trials you have to work with are statistically underpowered (have too few participants), as is the case here.
In this new meta-analysis, I’ve included every double-blind randomized placebo-controlled trial I could find of ivermectin as a treatment for covid. Using only double-blind placebo-controlled trials means that only the highest quality studies are included in this meta-analysis, which minimizes the risk of biases messing up the results as far as possible. In order to be included, a study also had to provide mortality data, since the goal of the meta-analysis is to see if there is any difference in mortality.
I was able to identify seven trials that fulfilled these criteria, with a total of 1,327 participants. Here’s what the meta-analysis shows:

What we see is a 62% reduction in the relative risk of dying among covid patients treated with ivermectin. That would mean that ivermectin prevents roughly three out of five covid deaths. The reduction is statistically significant (p-value 0,004). In other words, the weight of evidence supporting ivermectin continues to pile up. It is now far stronger than the evidence that led to widespred use of remdesivir earlier in the pandemic, and the effect is much larger and more important (remdesivir was only ever shown to marginally decrease length of hospital stay, it was never shown to have any effect on risk of dying).
I understand why pharmaceutical companies don’t like ivermectin. It’s a cheap generic drug. Even Merck, the company that invented ivermectin, is doing it’s best to destroy the drug’s reputation at the moment. This can only be explained by the fact that Merck is currently developing two expensive new covid drugs, and doesn’t want an off-patent drug, which it can no longer make any profit from, competing with them.
The only reason I can think to understand why the broader medical establishment, however, is still so anti-ivermectin is that these studies have all been done outside the rich west. Apparently doctors and scientists outside North America and Western Europe can’t be trusted, unless they’re saying things that are in line with our pre-conceived notions.
Researchers at McMaster university are currently organizing a large trial of ivermectin as a treatment for covid-19, funded by the Bill and Melinda Gates foundation. That trial is expected to enroll over 3,000 people, so it should be definitive. It’s going to be very interesting to see what it shows when the results finally get published.
Featured Video

Larry Johnson: U.S. Desperation Grows as Iran Is Winning
or go to
Aletho News Archives – Video-Images
From the Archives
Alarmist climate science as a textbook example of groupthink
By Paul MacRae | May 1, 2012
A while ago, I received an email from a friend who asked:
How can many, many respected, competitive, independent science folks be so wrong about [global warming] (if your [skeptical] premise is correct). I don’t think it could be a conspiracy, or incompetence. … Has there ever been another case when so many ‘leading’ scientific minds got it so wrong?
The answer to the second part of my friend’s question—“Has there ever been another case where so many ‘leading’ scientific minds got it so wrong?”—is easy. Yes, there are many such cases, both within and outside climate science. In fact, the graveyard of science is littered with the bones of theories that were once thought “certain” (e.g., that the continents can’t “drift,” that Newton’s laws were immutable, and hundreds if not thousands of others).
Science progresses by the overturning of theories once thought “certain.” … continue
Blog Roll
 Aletho News
Aletho News- Larry Johnson: U.S. Desperation Grows as Iran Is Winning
- Why don’t UK media mention the Israel lobby?
- New US shipment of 6,500 tons of military aid arrives in Israel
- Military aid to Ukraine vital for ‘US hegemony’ – Republican senator
- Zelensky’s favorite drone company at center of Ukrainian corruption alert
- The Broken Contract
- US CENTCOM’s Request for Dark Eagle Missiles Shows Shortage of Weapons and Limited Options
- Iran consolidates Strait of Hormuz control in post-war power shift, leaving US in dark
- A pause, not a ceasefire: Washington stalls, Tehran recalibrates
- US blockade crumbles as Iran turns to overland routes
- If Americans Knew
- US ships 6,500 tons of munitions, equipment to Israel in 24 hours
- A New Library in Gaza Rises From the Ashes of Destruction
- Israel’s top Jewish religious body ‘refuses to condemn’ smashing of Jesus statue
- Nun assaulted in Jerusalem amid ‘pattern’ of anti-Christian attacks by Israelis
- Former Tik Tok official describes massive pressure from Israel lobby
- Amid ceasefire violations and genocide, Israel commits piracy – Daily Update
- Five Laws and Standards That Require the US Cut Off Weapons to Israel
- Israel’s diabolical killing machine and how it targets journalists.
- The Global Sumud Flotilla to Gaza — A cry at sea to the world’s dormant conscience
- Politico’s powerful parent company tells Politico they must support Israeli narrative
- No Tricks Zone
- Oversupply Of Volatile Solar Energy Leads To Record NEGATIVE Prices!
- New Study: Extreme Heat Records, Heatwaves, Extreme Cold Records Declining Across US Since 1899
- It’s The Cold, Stupid! Cold 20 Times More Lethal Than Heat, Multiple Studies Show
- European Institute For Climate And Energy: “Climate Debate is Seldom About Science”
- New Study: The Climate May Be 5 Times More Sensitive To Solar Forcing Than Commonly Assumed
- EV Industry Reached $70 Billion In Losses In 2024 Due To Delusional Green Ideologies
- Reality Check: Maldives Have Actually Grown In Size Or Remained Stable Over Recent Decades
- Abrupt Climate Change Also Occurred NATURALLY In The Past …25 Times During Last Ice Age
- Cave Discovery Reveals Today’s Desert Climates Were Recently Far Warmer, Wetter, Teeming With Life
- German Expert: Heat Dome Led To Record Temps In Western USA…Warmer In 1934, 1936
