Clinical Rationale for SARS-CoV-2 Base Spike Protein Detoxification in Post COVID-19 and Vaccine Injury Syndromes
Publication of Baseline Protocol for Those Suffering from Long-COVID and Post-Acute Sequelae after COVID-19 Vaccination
By Peter A. McCullough | Courageous Discourse | August 27, 2023
For several weeks I have been messaging the scientific community and the public about an approach addressing the burden of SARS-CoV-2 Spike protein in tissues and organs in the human body that is largely responsible for post-COVID and vaccine injury syndromes.
No therapeutic claims can be made since large, prospective, double-blind randomized, placebo-controlled trials have not been completed on any of the compounds mentioned in this paper. I checked clinicaltrials.gov and no such trials have been planned. The Biden HHS US Action Plan for Long-COVID Research has pumped a billion dollars into long-COVID research and no new therapies have emerged. HHS, NIH, CDC, FDA have not recognized the larger issue of vaccine damage to the body.
At three and one half years into the pandemic and two and a half years into the COVID-19 vaccine debacle, myself and my clinic partners formulated a baseline regimen upon which additional drugs or agents can be added. We believe the Spike protein and the inflammation caused by it and its proteolytic fragments are at the heart of the pathophysiology we are observing.
We searched the literature for all available sources of evidence for products that can aid the human body in breaking down and catabolizing the Spike protein. We found two compounds, nattokinase and bromelain. Both of which additionally have fibrinolytic properties which are advantageous in the prothrombotic milieu induced by the persistent Spike protein. Curcumin was added for its anti-inflammatory properties in the setting of post-COVID and vaccine patients. The main safety caveats are bleeding and allergic reactions, both of which are manageable. It is our experience that both nattokinase and bromelain can be used in addition to antiplatelet and anticoagulant drugs with physician monitoring.
The empiric regimen can be continued for 3-12 months or more and be guided by clinical observation:
-Nattokinase 2000 FU (100) mg orally twice a day without food
-Bromelain 500 mg orally once a day without food
-Curcumin 500 mg orally twice a day (nano, liposomal, or with piperine additive suggested)
![]()
McCullough PA, Wynn C, Procter BC. Clinical Rationale for SARS-CoV-2 Base Spike Protein Detoxification in Post COVID-19 and Vaccine Injury Syndromes. Journal of American Physicians and Surgeons Volume 28 Number 3 Fall 2023, 90-93.
The full manuscript is linked and serves as your reference. While we are seeing case examples of improvement, we aim to collaborate with others as we did with the McCullough Protocol, to demonstrate clinical effectiveness of Base Spike Detoxification as a fundamental strategy for a large number of individuals who have suffered long-term consequences from SARS-CoV-2 infection and COVID-19 vaccination.
Revisiting the Biden Legal Position on Masks
Brownstone Institute | August 26, 2023
Last year, it seemed that masks were gone for good. US District Judge Kathryn Kimball held that Biden’s national mask mandate on airplanes was “illegal.” Airlines and airports immediately revoked their mask requirements. Flight attendants sang in celebration, passengers cheered, and companies welcomed the change in policy.
While Americans rejoiced, the Biden Administration worked behind the scenes to ensure that it could reimplement mask mandates at any time, in any place, for any reason.
The humiliation exercise never had a scientific basis. Existing air filtration systems made the threat of viral transmission on aircraft negligible. Studies found that there was “no direct evidence” of Covid-19 being transmitted aboard aircraft.
Despite the data, President Biden issued nationwide mask mandates in his first hours in office. His administration appealed Judge Kimball’s decision last April. “Our focus here was seeing what power we had to preserve,” explained White House Press Secretary Jen Psaki.
The case was dismissed as moot because the court found, “there is not a grain of evidence that the CDC has any plans to promulgate an identical mandate.”
Recent news suggests that prediction may have been wrong. The Covid regime appears to be revamping for a resurgence of mandates and potential lockdowns. CNN ran a headline Wednesday urging readers to “break out the masks against Covid.” The federal government has entered into Covid-related contracts with consultants and medical equipment providers to enforce “safety protocols” beginning in the next two months.
The return of Covid hysteria begs the question: what “power” did Jen Psaki and the White House want to preserve? Their legal briefs appealing Judge Kimball’s decision offer clues.
In court, the Biden Administration argued that mask mandates should be permissible even if there is no evidence to support them. Further, government lawyers wrote that these mandates should be permissible to any extent that bureaucrats deem necessary, even if the risk of Covid is nonexistent.
That is not hyperbole. Opponents of the mandates argued that the government should have “controlled trials” to provide evidence of efficacy and potential negative side effects before implementing universal masking.
The Biden Administration responded that the government did not need to provide any evidence or rational basis for its orders. Instead, “the CDC’s determination that there was good cause” should be sufficient. Government edicts should not be subject to judicial scrutiny, according to the government’s brief.
Further, there should be no limit to that authority, according to the Biden Administration. “It was equally permissible for the CDC,” the brief argued, “to make the masking requirement applicable to all passengers… regardless of whether there is any indication that the plane is diseased or dirtied.”
It’s not difficult to discern what we might call the Biden Doctrine of administrative rule-making. It means that the agencies can order whatever they want, whether or not there is any plausible basis in law or whether or not there is any rational basis for it at all. It is a doctrine of bureaucratic supremacy.
Will Scientific Evidence Ever Silence the Pro-Mask Cult?
Facial equity mask
BY DR GARY SIDLEY | THE DAILY SCEPTIC | AUGUST 24, 2023
It is a long-established conclusion from the scientific world that face masks achieve no appreciable reduction in viral transmission. We knew this in 2015-16 with regard to surgeons and their patients (here and here). We knew this in 2020 from a gold-standard Cochrane review, an analysis of 14 studies on influenza and a healthcare investigation that concluded that masks “may paradoxically lead to more transmissions”. We knew this in 2021 based on the Danish mask study and two comprehensive evidence reviews (here and here). We knew this in 2022 in relation to primary schools and universities, and a debunking of premature pro-mask conclusions drawn from the Bangladesh study. And – as if more evidence was needed – at the start of 2023 we had the latest Cochrane review, yet again concluding that covering our faces with cloth and plastic does not significantly reduce the likelihood of contracting respiratory viral infections. Yet, despite this collective scream from the scientific community that the ‘MASKS DON’T WORK’, it seems that nothing will muzzle the strident protestations of the mask disciples, such as those at Independent SAGE.
A recent article in the Daily Mail led with the scary headline: ‘Scientists raise alarm over new Covid variant and call for return of face masks.’ Two of the scientists raising concerns were Professors Trish Greenhalgh and Stephen Griffin, the former announcing, “It’s, once again, time to mask up”, while the latter concurs – albeit more cryptically – with his recommendation of the re-imposition of a “mitigation-based approach”. Both Greenhalgh and Griffin are members of Independent SAGE.
When Independent SAGE was formed in May 2020, as an alternative to official SAGE, it claimed to be a group of multi-disciplinary experts whose mission was to offer the Government scientific advice on how to minimise deaths during the Covid crisis. In reality, it constituted a group of zero-Covid fanatics pushing extreme counter-pandemic measures: whatever non-evidenced, human-rights-infringing restrictions the Government proposed, Independent SAGE typically called for them to be longer and harsher.
A cursory inspection of the group’s membership explains a lot. The previously-mentioned Trish Greenhalgh is, undoubtedly, the most extreme spokesperson for the pro-mask cult, previously asserting that the search for rigorous scientific evidence was the “enemy of good policy“. The founding Chairman of the group, Professor David King, was the senior scientific advisor to the Government of Tony Blair, currently an influential advocate of globalist agendas promoting top-down control of the population. Another core participant is the lifelong member of the Communist party – Professor Susan ‘let’s-wear-a-mask-forever‘ Michie. Also, the current co-Chair of Independent SAGE is Anthony Costello, a Professor of Global Health and Sustainable Development at University College London and a former director at the World Health Organisation. Given the histories and affiliations of these group participants it was predictable that they would grasp the next available opportunity to call for the return of community masking.
Clearly, the use of the term ‘independent’ in relation to this group was a misnomer. In stark contrast, Dr. Ashley Croft – the independent expert commissioned by the Scottish Covid Inquiry – appears to be a much better fit for the role of supplier of impartial information, free from the shackles of groupthink and mainstream ideology. Dr. Croft is a Consultant Public Health Physician and Medical Epidemiologist. In his report he lists his conclusions about the physical measures taken against COVID-19 as follows (emphasis mine):
In 2020 there was scientific evidence to support the use of some of the physical measures (e.g. frequent handwashing, the use of PPE in hospital settings) adopted against COVID-19. For other measures (e.g. face mask mandates outside of healthcare settings, lockdowns, social distancing, test, trace and isolate measures) there was either insufficient evidence in 2020 to support their use – or alternatively, no evidence; the evidence base has not changed materially in the intervening three years.
It has been argued that the restrictive measures introduced during the COVID-19 pandemic resulted in individual, societal and economic harm that was avoidable and that should not have occurred.
This genuinely independent voice was not well-received in some quarters. Unused to the expression of viewpoints that deviate from the dominant Covid narrative, the mainstream media predictably squealed disapproval about Croft’s perspective and resorted to attempts to smear him for his “vaccine scepticism”. And no doubt those ideologues at Independent SAGE will – as I write – be doing likewise.
As the year advances, the evidence against mass masking continues to accumulate. In April, researchers at London’s St. George’s Hospital reported that a mask mandate in 2020-21 in their healthcare settings “made no discernible difference to reducing hospital-acquired SARS-CoV-2 infections”. And – lest we forget – we purportedly live in a free and open society where coercive restrictions should only be imposed where there is unequivocal proof of a pronounced and widespread benefit from adoption of the behaviour targeted; we are a million miles away from that scenario, and that is even before we consider the harms of community masking.
But will this quieten the pro-mask cult? It seems these perpetual advocates of face coverings are driven by some supra cognitive construct that trumps the empirical evidence. Mass concealment of human faces appears to signify something sacred to groups like Independent SAGE: is it equality, egalitarianism, altruism? Or could their persistent pushing of masks be simply due to cognitive dissonance: they have stridently trumpeted the practice for so long that it would now be too psychologically painful, and damaging to their status and self-image, to admit their previous energies have been woefully misplaced? Whatever the underlying reason, we can expect escalating appeals from the muzzle mafia over the coming months.
Dr. Gary Sidley is a retired NHS Consultant Clinical Psychologist and co-founder of the Smile Free campaign.
NEW VARIANTS TRIGGER CALLS FOR RETURN TO LOCKDOWNS
The Highwire with Del Bigtree | August 24, 2023
Mass media is calling for the reinstitution of COVID restrictions due to new variants, with no conversation about the efficacy or the harm they’ve caused. Jefferey Jaxen connects all the dots, which appears to be pointing to a Pandemic 2.0.
The Royal Society Lockdown Report Authors Understand That by Ignoring the High Quality Evidence they Reach the Politically Acceptable Conclusion
BY DR CARL HENEGHAN AND DR TOM JEFFERSON | THE DAILY SCEPTIC | AUGUST 25, 2023
This week saw the publication of a suite of systematic reviews by the Royal Society (RS) on the effect of non-pharmaceutical interventions in the pandemic.
Politico headlined with ‘Top review says Covid lockdowns and masks worked, period’. The Guardian led with ‘Lockdowns and face masks “unequivocally” cut the spread of Covid, report finds’, and the i newspaper stated: ‘Masks and social distancing did reduce Covid infections, new report shows, proving lockdown sceptics wrong.’
So there you have it, a slam dunk, sceptics, you were all wrong. You should have masked up and stayed in lockdown.
Even more so when you listen to the Chair of the report’s group, Mark Walport, who said: “There is sufficient evidence to conclude that early, stringent implementation of packages of complementary NPIs was unequivocally effective in limiting SARS-CoV-2 infections.”
Four systematic reviews informed the effectiveness of non-pharmaceutical interventions in the Covid pandemic. However, here is some of what these reviews report.
A systematic review on environmental control measures:
Many of these studies were assessed to have critical risk of bias in at least one domain, largely due to confounding factors that could have affected the measured outcomes. As a result, there is low confidence in the findings.
One study, an RCT, showed that daily testing of contacts could be a viable strategy to replace lengthy quarantine of contacts. Based on the scarcity of robust empirical evidence, we were not able to draw any firm quantitative conclusions about the quantitative impact of TTI interventions in different epidemic contexts.
Effectiveness of face masks for reducing transmission of SARS-CoV-2:
We analysed 35 studies in community settings (three RCTs and 32 observational) and 40 in healthcare settings (one RCT and 39 observational). Ninety-one percent of observational studies were at ‘critical’ risk of bias (ROB) in at least one domain, often failing to separate the effects of masks from concurrent interventions.
Effectiveness of international border control measures during the COVID-19 pandemic:
There is little evidence that most travel restrictions, including border closure and those implemented to stop the introduction of new variants of concern, were particularly effective.
The report makes the same errors that the UKHSA and Public Health England did. They ignored the critical biases and the confounders when drawing conclusions. Some of the comments misunderstand the evidence required for making healthcare decisions.
Chris Dye, Professor of Epidemiology at the University of Oxford, who led the review on masks for the Royal Society, said if they had only looked at randomised controlled trials, they would have come to the same conclusion as the Cochrane review. However, the researchers behind the paper released Thursday chose to analyse a larger body of studies and found strong evidence that masks work.
So, if we ignore high-quality evidence, we arrive at the conclusion we want – they fully understand the politics. Low-quality evidence means the estimated effect will differ substantially from the actual effect – we’ve known this for quite some time, and it is fundamental to the delivery of evidence-based interventions. An approach that uses low-quality evidence shouldn’t inform healthcare, and it doesn’t. That’s why we have NICE, which uses the best available evidence to develop recommendations that guide health, public health and social care decisions.
Did the reviewers, for instance, ask if there was a protocol for any of these studies – something we have previously pointed out. There were none, despite protocols being essential for robust research.
There is something we do agree with in the report, that the “future assessments should also consider the costs as well as the benefits of NPIs, in terms of their impacts on livelihoods, economies, education, social cohesion, physical and mental wellbeing, and potentially other aspects”. However this report looked at none of that. The single focus on one outcome, ignoring harms, further hinders informed decision-making.
The RS report wants us to believe that RCTs are impossible during a pandemic: “While RCTs should not be discounted, it is highly likely that most information in a future pandemic will continue to be observational.”
Yet the pandemic has re-emphasised the importance of high-quality randomised clinical trials and highlighted the need for preparation, coordination and collaboration.
The Royal Society review shows that some academics are losing their ability to think critically. Instead of retrofitting evidence to preconceived conclusions, it would be much better to report the uncertainties and set out those questions that need addressing. Refusal to acknowledge uncertainties does a disservice to society and undermines public trust in research.
Staying at home decreases your risk of all sorts of hazards – in the short term, you won’t get run over and you’ll reduce the risk of an infection or an accident. But what matters is the costs of what happens when you reemerge.
Kaiser Family Foundation Finds Many Believe COVID-19 Mass Vaccination Responsible for Sudden Deaths
Poll Statistics Reveal America Waking Up to Immunization Debacle
By Peter A. McCullough, MD, MPH | Courageous Discourse | August 23, 2023
The Kaiser Family Foundation is a pro-vaccine organization that has an biased polling system aimed at showing satisfaction and benefit of mass vaccination among other family issues. The May 23 through June 12, 2023 poll reveals some shocking new data. A substantial minority of Americans believe the COVID-19 vaccines have caused great harm. Here are the results.
![]()
As you can see it is roughly a third of Americans are awake and understand the COVID-19 vaccines have failed, cause great harm, and pose a giant safety risk to Americans. It is also interesting to note a quarter of respondents have been awakened to the link between childhood hyper vaccination and autism spectrum disorder. I wonder what the actual sentiment is on vaccines if Kaiser had asked the questions in a more unbiased manner and did not load up their survey with charged words such as “false” and “misinformation”.
Those Doctors Calling for Spreaders of Covid Misinformation to be Punished Should be Careful What they Wish For
Many of their Claims – that the Vaccinated Couldn’t Infect Others, For Instance – Turned Out to be False
BY NIGEL WILSON | THE DAILY SCEPTIC | AUGUST 24, 2023
The Journal of the American Medical Association recently published a review of alleged ‘misinformation’ about COVID-19 that physicians were responsible for, either on social media and in other news sources.
In the paper, the corresponding author, Dr. Sarah L. Goff, MD PhD, defined misinformation. She surveyed social media platforms and news sources for anything written by other physicians that fits her selected examples of both. She then proposes that physicians guilty of writing what she judges to be misinformation should be “regulated and disciplined”.
Dr. Goff and her co-authors define misinformation as “false, inaccurate or misleading information according to the best evidence available at the time” and disinformation as “having an intentionally malicious purpose”.
Dr. Goff states: “We conservatively classified inaccurate information as misinformation rather than disinformation because the intent of the propagator cannot be objectively assessed.”
Dr. Goff identified four major themes of alleged misinformation. These included: (1) vaccines were unsafe and/or ineffective; (2) masks and/or social distancing did not decrease risk for contracting COVID-19; (3) other medications for prevention or treatment were effective despite not having completed clinical trials or having been FDA approved, and (4) other misinformation.
Dr. Goff includes a brief discussion of vaccine safety and effectiveness and mask effectiveness, but does not attempt to undertake a full review of the published evidence in these areas. Instead, she seems to assume that her readers will agree that any suggestion that vaccines or masks were ineffective or unsafe are self-evidently false.
Dr. Goff states that the American Medical Association has called for disciplinary action for physicians propagating COVID-19 misinformation. She laments the fact that “few physicians appear to have faced disciplinary action” for alleged sins against Covid orthodoxy.
I am not an expert in analysis of published medical research. I don’t work in a School of Public Health like Dr. Goff. I have worked as a licensed physician in England for over 40 years as a family doctor and an occupational physician and I have over 40 years’ experience reading the medical peer review literature. I retired from full time medical practice in 2017. I have a reasonable understanding of English, maths, logic and critical thinking. I don’t pretend to have read all the published research on masks or vaccinations. However, I continue to read leading medical journals on a regular basis.
I understand the concept of truth and how hard it is to establish an absolute truth in science. I understand the enlightenment principles that any ideas can be discussed, that nobody has a veto on ideas and that it is important to doubt and test all of our ideas continually. There is no indication from her writing that Dr. Goff understands how important it is to doubt, question and test the effectiveness and safety of interventions such as vaccines and masks.
From my reading of the peer review literature, for illustration purposes, I identified the following four publications as examples of publications which should raise concerns and questions about COVID-19 vaccines and masks.
In 2019, the World Health Organisation (WHO) published a report entitled ‘Non-pharmaceutical public health measures for mitigating the risk and impact of epidemic and pandemic influenza’. The WHO concluded: “There are a number of high-quality randomised controlled trials demonstrating that personal measures (e.g. hand hygiene and face masks) have at best a small effect on transmission.”
In February 2023 a Cochrane review into the effectiveness of masks concluded: “Compared with wearing no mask in the community studies only, wearing a mask may make little to no difference in how many people caught a flu-like illness/Covid-like illness.”
A study from the Department of Infectious Diseases in Cleveland, Ohio, in December 2022 found that “the bivalent COVID-19 vaccine only offered modest effectiveness”.
A study from the University of Queensland in September 2022 concluded: “Never in vaccine history have 57 leading scientists and policy experts released a report questioning the safety and efficacy of a vaccine. They not only questioned the safety of the current COVID-19 injections but were calling for an immediate end to all vaccination. Many doctors and scientists around the world have voiced similar misgivings and warned of consequences due to long-term side effects.”
These four publications are examples which give us a legitimate reason to question the use of masks and the Covid vaccines and to look further for evidence. Are we not allowed to raise questions about these issues without being threatened with disciplinary procedures? Not to ask any questions would be lacking in curiosity in the extreme, especially for practising physicians concerned about the safety of their patients and the integrity of their advice. These publications do not prove anything conclusively, but they should not be ignored. Expressing doubt and asking questions about the safety and effectiveness of vaccines and masks is not false, inaccurate or misleading, to use the definition adopted by Dr. Goff. If questions arise in my mind, why don’t similar questions arise in the minds of Dr. Goff and her co-authors? How did Dr. Goff reach such a degree of certainty about the effectiveness of masks and vaccines against COVID-19 that she can classify any statement to the contrary as misinformation worthy of disciplining a colleague? Why does she conclude that a colleague who disagrees with her does not have the right to be heard? Why would she seek to silence those who disagree with her?
Inaccurate information which is not deliberately intended to deceive is simply inaccurate. In science and medicine there are many inaccurate statements made in good faith by researchers who are presenting their data or their theories as accurately and honestly as possible. It is important that all theories and all research data can be published, even when the data or the theory are wrong. Disciplinary action for any statement which turns out to be inaccurate or false would surely suppress a large proportion of all scientific and medical discourse. Is this what Dr. Goff wants?
It could be argued that the examples of misinformation used by Dr. Goff are themselves misinformation. To suggest that anyone who states that the Covid vaccines were unsafe and/or ineffective is guilty of misinformation is to ignore significant evidence which raises questions about the vaccines. To suggest that anyone who states that masks did not decrease risk for contracting COVID-19 is guilty of misinformation is also to ignore evidence to support this view. It could be argued that Dr. Goff is using false, inaccurate or misleading examples of misinformation in her study in order to suppress dissenting views.
Dr. Goff appears to have very little humility. She does not appear to be in any doubt that she and her co-authors are infallible in relation to masks and vaccines. She seems to think she is the ultimate arbiter of truth, and that she is immune from being regulated or disciplined for her views in the way she promotes for others. I would not propose disciplining or applying regulatory sanctions to Dr. Goff or her colleagues if her publication includes false, inaccurate or misleading statements. Instead, I would propose respectful dialogue with her to debate her proposal, offering arguments to the contrary with a view to educating her and myself.
In England, medical doctors are obliged to respect colleagues’ skills and contributions, and to treat colleagues fairly. We must create a working environment in which it is safe to ask questions and raise concerns. I believe in these principles. Failure to adhere to these standards can lead to disciplinary action against medical doctors. I understand that similar professional obligations apply to medical doctors in the United States. Dr. Goff does not appear to respect the skills and contributions of colleagues who disagree with her. She seems to be promoting a working environment in which it is not safe for those who disagree with whatever the orthodoxy within the medical profession is at any one time to ask questions and raise concerns. Does she not realise that this may make it unsafe for her to raise concerns and ask questions in due course?
Dr. Goff acknowledges in her final sentence that “a coordinated response by federal and state governments and the profession that takes free speech carefully into account is needed”. This tiny nod towards free speech is somewhat undermined by her attempts to censor her colleagues’ right to disagree with her. Free speech is nothing if it is not accorded to those with whom we disagree.
Frederick Douglass, the American social reformer said: “To suppress free speech is a double wrong. It violates the rights of the hearer as well as those of the speaker.” If Dr. Goff persuades those in power to regulate or discipline those who disagree with her, then their right to free speech is violated and our right to hear them is violated. Does Dr. Goff not have a glimmer of doubt about her omniscience? Does she not think there is even a faint possibility that physicians who disagree with her might have something useful to say?
Why do some physicians think that the best response when another physician disagrees with them is to censor their colleague? How could any physicians achieve such unshakeable certainty in their own omniscience? When did they forget the fundamental principles of the enlightenment, that all ideas can be discussed and that nobody has a veto on any ideas? How did the principles of treating colleagues with respect and upholding the free speech of those with whom we disagree become so degraded?
Dr. Goff and her co-authors should be careful what they wish for. They seek to discipline colleagues for daring to disagree with their orthodoxy. If they succeed, the cancel police may be coming for them next.
Dr. Nigel Wilson MRCGP FFOM is a retired consultant occupational physician.
German Judge Gets Probation Sentence For Allowing Kids to go Maskless
After his house was raided in 2021

NAKED EMPEROR | AUGUST 23, 2023
Christiaan Dettmar, a family judge from the Weimar District Court in Germany recently faced the Erfurt Regional Court for his stance against the unnecessary imposition of mask mandates on children. In April 2021, going against the grain, he ruled that children at two Weimar schools should not be burdened with wearing Covid masks in class, defying the restrictive guidelines set by the Thuringian Ministry of Education.
However, in a move reflective of the bureaucratic stranglehold on such decisions, higher courts dismissed his ruling, claiming it unauthorised. The Thuringian Higher Regional Court stated that the family judge did not possess the jurisdiction on this matter, a viewpoint also echoed by the Federal Court of Justice. They insisted that only administrative courts should handle state orders regarding corona protection measures.
At the time (in April 2021), Dettmar had his office, private residence and car searched after he ruled that children should not be wearing masks. He also had his phone confiscated after his decision which embarrassed the government.
His decision to end mask mandates was made after hearing evidence from Professor Kappstein on the lack of benefit of wearing masks and observing distance rules for the children and third parties. Kappstein said that after evaluating all the international data on the subject of masks, the effectiveness of masks for healthy people in public is not supported by scientific evidence.
Dettmar concluded that not only are masks useless but they are also dangerous.
The compulsion imposed on school children to wear masks and to keep their distance from each other and from third persons harms the children physically, psychologically, educationally and in their psychosocial development, without being counterbalanced by more than at best marginal benefit to the children themselves or to third persons. Schools do not play a significant role in the “pandemic”.
The PCR tests and rapid tests used are in principle not suitable on their own to detect an “infection” with the SARS-CoV-2 virus. This is already clear from the Robert Koch Institute’s own calculations, as explained in the expert reports. According to RKI calculations, as expert Prof. Dr. Kuhbandner explains, the probability of actually being infected when receiving a positive result in mass testing with rapid tests, regardless of symptoms, is only two per cent at an incidence of 50 (test specificity 80%, test sensitivity 98%). This would mean that for every two true-positive rapid test results, there would be 98 false-positive rapid test results, all of which would then have to be retested with a PCR test.
A (regular) compulsion to mass-test asymptomatic people, i.e. healthy people, for which there is no medical indication, cannot be imposed because it is disproportionate to the effect that can be achieved. At the same time, the regular compulsion to take the test puts the children under psychological pressure, because in this way their ability to attend school is constantly put to the test.
In the recent trial against Judge Dettmar, although the prosecution demanded a hefty three-year prison term, the defence, representing the concerns and wishes of countless parents and citizens, argued for acquittal. The presiding judge at the Erfurt Regional Court noted that the Weimar judge’s decision emanated from his personal views.
After originally being sentenced to two years in prison, the court has now suspended the sentence on probation.
However, it is still possible that Dettmar may lose his office and pension as a result of the conviction.
Throughout the proceedings, the courtroom was electric with tension and support. Spectators broke into spontaneous applause in favour of Dettmar. This would have continued except the judge threatened to throw them out. The prosecution’s attempt to paint the judge’s intentions as malicious was met with scepticism. They claimed that he intentionally set up a child protection procedure against the mask mandate, misrepresenting it as a statement against government measures. Their evidence, mainly based on emails and chat messages, was tenuous at best.
The defence, however, passionately highlighted the judge’s genuine concern for the well-being of children. They asserted that the case was merely an attempt to suppress and penalise differing opinions in a society where free thought should be celebrated.
Reiterating his unwavering stand, Dettmar confirmed he would make the same decision again. The subsequent lifting of school mask mandates by German states in April 2022 only reinforces the argument that such restrictions should never have been in force in the first place.
The American Board of Internal Medicine’s Longstanding War On Doctors Is Escalating
The ABIM’s history proves their present actions are political/financial and not scientific. They are making examples of us “dissenters” to scare the rest of the country’s docs to keep quiet.
BY PIERRE KORY, MD, MPA | AUGUST 23, 2023
The unholy alliance of industry captured high-impact medical journals, federal public health agencies, professional societies (ABIM, AMA, APHa etc), and most importantly, the state medical licensing boards directed by the Federation of State Medical Boards (FSMB) are still going hard after us “dissenting” doctors. You know, those of us that very publicly called out the unscientific policies implemented by corrupted policymakers in a directed pursuit of profits and power. Their actions trying to silence us (and to scare other doctors from speaking out) are escalating.
Recently, what I call the “misinformation committee” of the American Board of Internal Medicine (ABIM) voted to strip Professor Paul Marik and myself of our Board certifications. To best understand why they would do this, I think it is important to review what the ABIM is, how it operates, and then detail their absurd attempt to paint us as misinformationists by using disinformation.
Let’s trace my current relationship with the ABIM to today:
At the end of my training, I became Board Certified by the ABIM in three specialties (Internal Medicine, Pulmonary Diseases, and Critical Care Medicine).
What is the ABIM? Well, from this devastating article by Kurt Eichenwald, an accomplished corporate investigative journalist who did a devastating takedown of the ABIM and its officers in a Newsweek piece in 2015:
The ABIM is a purported nonprofit that certifies new physicians as meeting standards of practice. Beginning in the early 1990s, the ABIM ordered certified doctors to be recertified, again and again. Without the ABIM seal of approval, lots of internists and subspecialists can’t get jobs and can’t admit patients to hospitals. So by taking advantage of that monopolistic power, the ABIM has forced hundreds of thousands of physicians to follow recertification processes that doctors complain cost them tons of money (paid to the ABIM), require tons of time (taken from families and medical practices) and accomplish nothing.
In many doctor’s opinion, this cash grab of the ABIM by selling “certifications” is a corrupt farce. There is no evidence that certifying doctors in this highly costly way does anything to improve the quality of care delivered. The ABIM has not only refused to produce data showing the program improves patient care but also hasn’t conducted any studies on that matter. In fact, the ABIM and its related organizations are:
harming American medicine and diminishing the quality of scientific research, pushing physicians to close practices rather than wasting time on expensive and frustrating busywork, and forcing specialists to play a game of medical trivial pursuit. (Even Baron has admitted that he was tested for recertification on topics he never used in his practice.)
But it sure does generate cash for ABIM executives. Note that Board Certification used to simply be a sort of “honor” denoting that the member passed a more rigorous examination in their specialty. That “honor” comes at a price though:
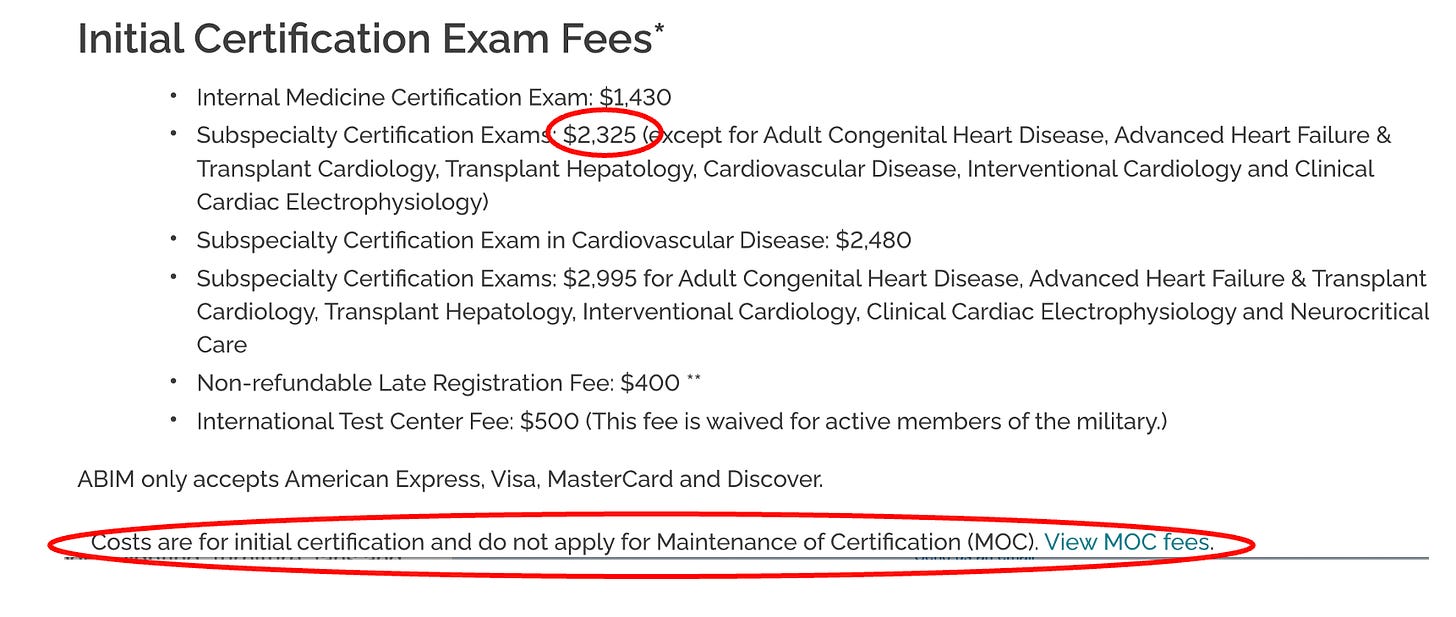
Since I am (was?) Board certified in 3 specialties, lets do some math as this is what it costs me to re-certify every ten years:
$1,430 for Internal Medicine
$2,325 for Pulmonary Diseases
$2,325 for Critical Care Medicine
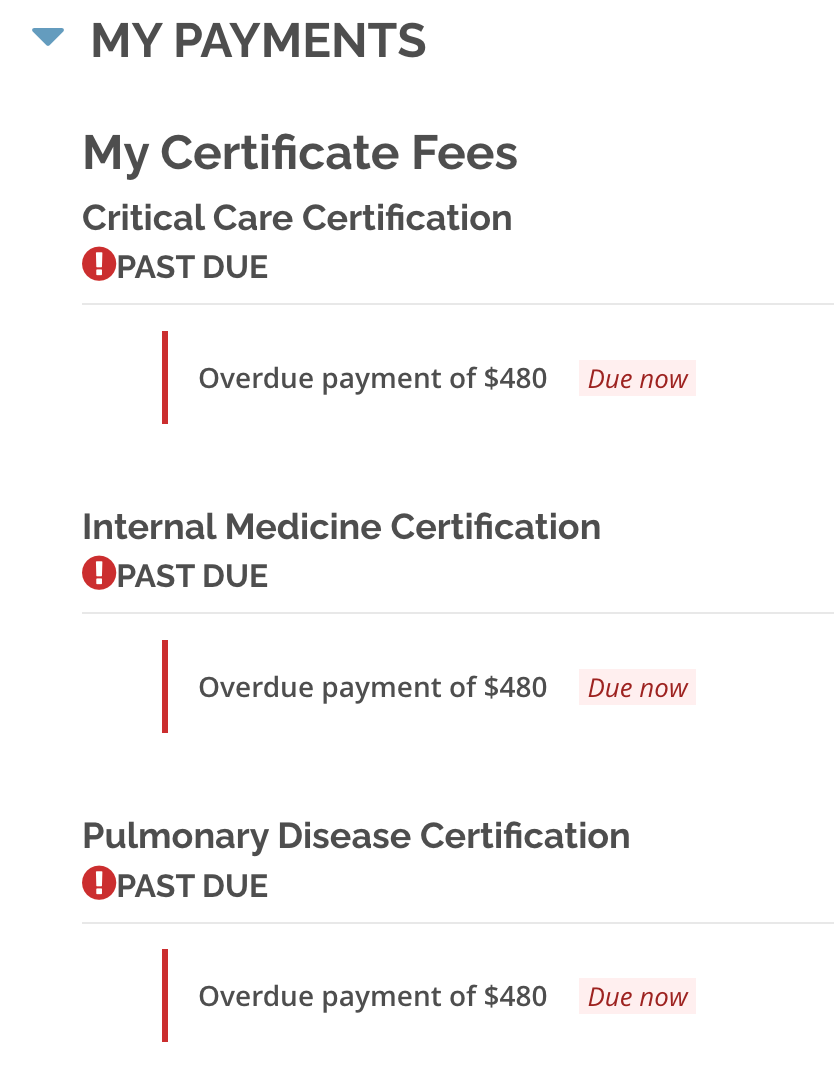
But wait, we are not done yet. These bastards were not making enough money with once-every-ten-year recertification exam fees, so they invented a new program of annual busywork education requirements which they called Maintenance of Certification (MOC) which costs you $220 every year for every certification (plus late fees if you forget). To wit, I went into my patient portal and discovered. I owe them $480 for each of my certifications!
And get this – that money essentially goes to ABIM executive salaries and pensions and other dubious private investments as described by Eichenwald where he details the insane lengths the ABIM goes to “hide” the compensation and pension data on its executives. What is worse is that ABIM certification has now been made a requirement of employment as a faculty member of academic medical centers and hospitals and is also a requirement to be on many insurance company panels (these actions further strengthen the control of doctor behavior).
Doctors have started publicly slamming the group in industry publications. “ABIM is imposing on us an onerous and ill-conceived tool, one that most physicians agree is irrelevant,” Dr. Karmela Chan wrote in Internal Medicine News. “I am glad this conversation is happening, because, frankly, the process was enough to make me want to quit being a doctor.” Further, in a recent poll of 2,211 physicians conducted on a doctors-only website called Sermo, 97 percent of the respondents criticized recertification.
Richard J. Baron, the ABIM CEO that sent letters threatening decertification to me and Paul, makes close to a million dollars a year, however that data is almost impossible to find due to the ABIM’s multiple attempts to obscure it as well as its spokespeople avoiding answering any inquiries on the topic. Here is a summary of Eichenwalds findings on the ABIM:
- In 2015, they were 5 months late in filing their publicly available financial report with the IRS (that several journalists were very interested in).
- The report is full of obfuscations and anomalies of reporting of not only the actual money earned by the executives, and particularly Baron, but his financial conflicts of interest are even better hidden.
- A big percentage of the ABIM’s millions was in the form of cash to one former employee.
- The ABIM in 2013 had 57 million against liabilities of 105 million – while Baron was going around saying that its assets are three times its liabilities (this was a 100% lie. When I get to the ABIM’s response to our defense letter, remember that what liars do is.. lie).
- It lost $4.8 million on $55.5 million in revenues, no small feat and almost entirely due to a bloated payroll.
- It also claims it spends no money on lobbying while it spent between 100K to 160K annually to lobby Congress on Medicare and Medicaid (another lie).
- The data on top officers compensation is so obscured and fragmented, Eichenwald reported that he had found it much easier to discover executive compensation at Enron, Worldcom and Adelphia – all famous for lying on tax filings. Again no small feat (to be one of the top corporate liars in the U.S).
- Officers “double dip” – former CEO Christine Cassel got $741K from ABIM and $247K from the ABIM “Foundation” (slush fund for ABIM officials) and also got $219K in “other compensation” – totaling $1.2 million for one year. (Nice gig if you can get it).
- But wait, we are not done. Cassel also got $504K in “deferred compensation” for a total of $1.71 million more that year (six times the median compensation for similar sized non-profits). Six times.
Then there is this doozy of an article which came out this week in The Defender by Children’s Health Defense, detailing the ABIM CEO Richard Baron’s conflicts of interest:
Some of the most disturbing reveals:
“The head of a national medical organization who publicly called for doctors to lose their licenses unless they supported government narratives on COVID-19 treatments and vaccines concealed his relationship with a public relations firm whose client list also included Pfizer, Moderna and the Centers for Disease Control and Prevention (CDC).
Dr. Richard Baron, president and CEO of the American Board of Internal Medicine (ABIM) is a client of Weber Shandwick, investigative journalist Paul D. Thacker reported on Wednesday.
Note that I went after Weber Shandwick in my book, “The War on Ivermectin” where I argue (without proof, although I believe that is coming because I know of a subpoena coming their way) that they created and launched the “Horse Dewormer PR campaign,” highlights of which was the famous FDA tweet and absurd Rolling Stone article:

In late 2021, Baron publicly pushed for doctors who spread “misinformation” about COVID-19 and the vaccines to lose their license and certification.
Last year, Baron partnered with Weber Shandwick to propose a South by Southwest (SXSW) panel titled “When Doctors Prescribe Misinformation.” The proposal was subsequently accepted and the panel took place at SXSW in Austin, Texas, on March 13.
According to Thacker, “Weber Shandwick’s panel featuring Dr. Baron has been widely promoted by the PR firm’s employees,” including Sarah Mahoney, executive vice president, Healthcare Communications, Strategy & Planning for Weber Shandwick, who in a LinkedIn post, wrote she “can’t think of a more important topic right now.”
Although to the unawake the following may seem normal public health practice, but to those of us fighting agency capture by Big Pharma, it is absurd:
The CDC’s National Center for Immunization and Respiratory Diseases (NCIRD) in September 2020 awarded Weber a $50 million contract “to promote the vaccination of children, pregnant women and those at risk for flu and increase the general acceptance and use of vaccines,” according to the PR firm’s website.
Thacker said he believes much of what is labeled “misinformation” in medicine and academic research “is really just corporate PR,” and that “Congress needs to take a harder look at funding for ‘misinformation research.’“
Speaking of taking a harder look at where the funding is coming from for “misinformation research” and the ABIM, it turns out that.. we can’t. Why? Check out this tweet showing a clause inserted into the ABIM’s by-laws in 1998:
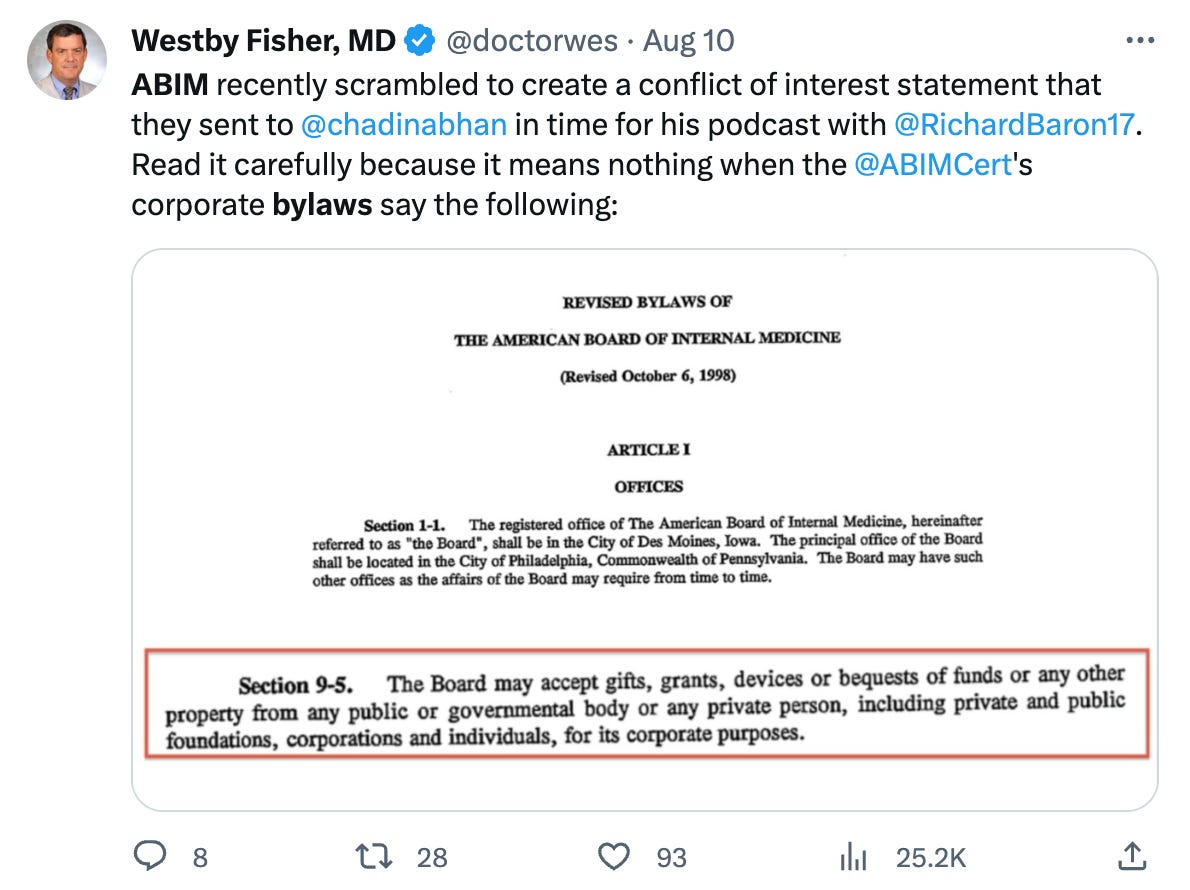
But wait, it gets better, like way better. Also in their by-laws:
Information that is disclosed will be kept confidential except to the:
-
- President and Chair of the Board;
- The chairs of the relevant Subspecialty Boards, Test-Writing Committees, and other Committees of the Board, members who serve on the relevant Boards and Committees, and staff working with the respective committees;
- The Conflict of Interest Committee members and Conflict of Interest Committee staff,
except as required for the purposes of continuing medical education.
So, basically, they can take money from any corporate entity and do not have to disclose it to anyone. Again, nice gig if you can get it.
Back to the ABIM’s history: One of Eichenwalds more disturbing observations about the behavior of the ABIM:
I can attest to the ABIM’s pomposity. Starting with my first story about the ABIM, the organization usually has refused to acknowledge I even asked a question. The only other group to do that in my 30-year journalism career was a company that processed payments for child pornography websites. Plus, when I reported on the uprising by doctors, the ABIM ignored the facts and instead investigated me.
Now lets fast forward to Covid. On July 29, 2021, the FSMB (this entity controls the state medical licensing boards, not the ABIM – at least on paper) issued a policy statement that “Physicians who generate and spread COVID-19 vaccine misinformation or disinformation are risking disciplinary action by state medical boards, including the suspension or revocation of their medical license.”
What is interesting is how fast and how rigidly the ABIM followed the FSMB’s lead and enacted their own misinformation policy despite the fact that, as my colleague Meryl Nass has pointed out:
“suddenly claiming that using licensed drugs for COVID, criticizing federal policies for COVID or criticizing the value of COVID vaccines is unprofessional” gives the specialty board the right to revoke a certification—well, that was never part of its contract with me. So pulling my certification for issues that were never specified in the original contract is breach of contract.
I think it would only be a breach if contracts, like our Constitution and the practice of medical ethics, were still “a thing.”
The ABIM apparently liked the FSMB’s “misinformation policy” idea to attack dissenting doctors so much (or were told to like it) that 2 months later, they, along with their colleagues at the American Board of Pediatrics and the American Board of Family Medicine, issued a statement supporting the FSMB’s position, saying, “We all look to board certified physicians to provide outstanding care and guidance; providing misinformation about a lethal disease is unethical, unprofessional and dangerous.” (note that they seem particularly focused on Covid misinformation and not any other disease model or therapeutics. Do you think it could be because Covid vaccines and therapeutics opened immensely profitable markets to Pharma overnight?).
Again from Meryl Nass (please subscribe to her Substack):
Furthermore, the processes the ABIM is using, as described by CEO Richard Baron, MD in his podcast with the New England Journal of Medicine are procedurally unfair. Dr. Baron earns $1 million/year to threaten doctors for a crime that does not exist. Baron, notably, refused to specify where the line was between misinformation and genuine disagreement in that podcast, though he seems to have no difficulty at all drawing the line when it comes to licensees who speak publicly about how to manage COVID. In a truly Orwellian effort, the ABIM and the ABIM Foundation have dedicated the year to ‘building trust’ in medicine.”
In what I suspect was the ABIM’s first enforcement of their shiny new policy, they go after Peter McCullough, Paul Marik, and myself on the same day (May 26, 2022) with a letter quoting numerous public statements we made, implying that we needed to defend the substance of such statements with supporting data or risk losing our certifications.
“Game on” I thought, looking forward to the exercise of “debating” scientific data with the ABIM. However, our FLCCC lawyer, Alan Dumoff pointed out that the ABIM’s policy and procedures state that the process of accusing a member of misinformation requires that they first provide evidence to us that what we said was inaccurate. So, we wrote back, pointing out to the ABIM their brazen “error” (yeah right) in not complying with their own policy and procedures.
“Nonsense” they wrote back (in short). Their logic was truly shocking – they say that the fact they provided the substance and references to my public statements means they did their duty (rather than their providing references that would refute my statements which is what their policy states they need to do).
You can read their brazen, illegitimate, dismissive response here:

This letter above demonstrates the unchecked power they have – they alone determine whether they are following their own policy which they so clearly were not. What did I say about liars before?
Anyway, rebut them we did. We wrote a 76 page treatise with 175 references, 11 exhibits, and 22,000 words, marshaling and weaving numerous data sources to support all our public statements that they had a problem with. May it enter the historical record here (I think you Covid vaccine and ivermectin data geeks will find the letter impressive).
We sent that letter over 6 months ago… and finally got an answer a few weeks ago. To understand the misinformation committee’s response, note this statement from an editorial written by Baron where he tries to give examples of misinformation:
A whole range of statements with which many — or even most —physicians might disagree would therefore not trigger our disciplinary process. On the other hand, when someone certified by the ABIM says something like “the origin of all coronary heart disease is a clearly reversible arterial scurvy” or “children can’t spread Covid” or “vaccines don’t prevent Covid deaths or hospitalizations,” we are not dealing with valid professional disagreement; we are dealing with wrong answers.
That last sentence is critical as Baron literally is saying that the ABIM gets to determine what is a valid professional disagreement versus a “wrong answer.” Good to know, especially in regards to the fact that the narrative that “vaccines prevent Covid deaths or hospitalizations” was strongly refuted in our initial response letter.
This issue about drawing a line between misinformation and genuine disagreement is a critical one. From our letter of appeal written by our lawyer Alan Dumoff:
Threshold Issue: What Standard Distinguishes Legitimate Differences of Professional Opinion and Misinformation
We disagree with the Committee’ s interpretation of the data, which we address below, but the initial question is by what standard the American Board of Internal Medicine (“ABIM” or “Board”) evaluates evidence to determine that disagreement with consensus generally, and regarding controversial matters around COVID-19 policy specifically, rise to the level of actionable misinformation. The Board’s policy recognizes the right to legitimate debate, which requires it not merely show evidence supporting a consensus view but that it demonstrate that these professional disagreements are not legitimate but outright misinformation.
If not grounded in an articulated standard, at the very least, the Board must demonstrate that the views at issue are false by citing the fallacies in the actual substance of the evidence provided, not simply by critiquing a few isolated studies divorced from the totality of evidence. Resting solely upon citations to mainstream publications while substantially avoiding the evidence in our Submission, and our detailed critiques of these publications does not provide a basis for the Board to take action against my clients.
A diplomate’s medical positions must be plainly erroneous to merit sanction. Departure from consensus is hardly unusual and by itself insufficient. While the Sanctions Notice gives the appearance of having done so, the Committee did not directly engage the numerous imperfections in the mainstream approach Drs. Kory and Marik’s have pointed to in substantial detail. The Committee has not engaged the evidence submitted and demonstrated it is illegitimate, only that it departs from the consensus, that is insufficient to support a sanction.
The point is that the ABIM appears absurdly obsessed with getting doctors to spout only consensus opinions. This is literally unprecedented in science. From Michael Chrichton the author:
I want to pause here and talk about this notion of consensus, and the rise of what has been called consensus science. I regard consensus science as an extremely pernicious development that ought to be stopped cold in its tracks. Historically, the claim of consensus has been the first refuge of scoundrels; it is a way to avoid debate by claiming that the matter is already settled. Whenever you hear the consensus of scientists agrees on something or other, reach for your wallet, because you’re being had. Let’s be clear: the work of science has nothing whatever to do with consensus. Consensus is the business of politics. Science, on the contrary, requires only one investigator who happens to be right, which means that he or she has results that are verifiable by reference to the real world. In science consensus is irrelevant. What is relevant is reproducible results. The greatest scientists in history are great precisely because they broke with the consensus. There is no such thing as consensus science. If it’s consensus, it isn’t science. If it’s science, it isn’t consensus. Period.
I love that last line so much it bears repeating, “If it’s consensus, it isn’t science. If it’s science, it isn’t consensus. Period.”
Now, let’s look at their response to our 76 page letter teeming with supportive data for our statements. Can read their letter in its entirety here but I thought I would just pull the most illustrative sections:
… the CCC (i.e. misinformation committee) concluded that your statements about the purported dangers of, or lack of justification for, COVID-19 vaccines are false and inaccurate because they, too, are not supported by factual, scientifically grounded, and consensus driven scientific evidence. In fact, the overwhelming body of factual, scientifically grounded, and consensus-driven evidence – at and since the time you made those statements – shows that the COVID-19 vaccines are safe and effective for children and for adults
I have heard of the term “evidence-based medicine (EBM)” which is what I practice, but not “consensus driven science” (completely new invention – pernicious indeed. I Actually adhere to the original definition and conceptual framework envisioned by the founders of evidence based medicine which was incredibly well detailed in a by my friend “A Midwestern Doctor” in his brilliant recent post “What Happens To Doctors Who Innovate”.
Anyway, they then listed a few published, peer-reviewed papers supporting their point, blissfully un-acknowledging of the fact that the high-impact journals have been systematically censoring pretty much all negative analyses of the vaccine campaign’s impacts while publishing nothing but positive reports with cherry-picked and/or fraudulent data – so there is no way for the truth about vaccines to win in scientific debates my friends.
The high-impact journal censoring of adverse vaccine data is identical to their censoring of dozens of positive trials of ivermectin, something I extensively detail in the chapter called “The Journal Rejections of Positive Ivermectin Studies” in my book.
It gets even better – they next argue against my claims of lack of safety of the vaccines by, get this, referencing proclamations by the WHO and CDC. They ignore all the immense data to the contrary that I submitted while of course being willfully oblivious to the fact that the CDC and WHO are fully Pharma captured agencies:
Moreover, the vaccine safety data overwhelmingly (overwhelmingly?) contradicts your statements about vaccine risks. See, e.g., Centers for Disease Control and Prevention, “Safety of COVID-19 Vaccines,” https://www.cdc.gov/coronavirus/2019-ncov/vaccines/safety/safety-of-vaccines.html (updated March 7, 2023) (reporting that “Adverse Events (Serious Safety Problems) Are Rare,” and that “[t]he benefits of COVID-19 vaccination outweigh the known and potential risks”); World Health Organization, “Safety of COVID-19 Vaccines,” https://www.who.int/news-room/feature-stories/detail/safety-of-covid-19-vaccines (March 31, 2021) (stating that “[b]illions of people have been safely vaccinated against COVID-19,” that “mRNA vaccines [for COVID-19] have been rigorously assessed for safety, and clinical trials have shown that they provide a long-lasting immune response”).
The paragraph above should enter the historical record… somewhere. That will NOT age well. The only thing more absurd to contemplate is whether they know they are lying in their letter or if they are simply referencing propaganda that they themselves swallowed whole? In a way, the former might be more acceptable to me at this point.
Their opinion on how I got ivermectin wrong was similarly brazen – they ignored all the meta-analyses (historically considered the strongest form of data, a fact they seem to have willfully avoided) in favor of listing a handful of trials where ivermectin was supposedly found ineffective, relying mostly on citing “the Big 6” (what I named the chapter describing the fraud behind the 6 largest, Pharma-conflicted and most publicized trials on ivermectin). This was 100% unsurprising.
Check it out:
First, the CCC concluded that your statements about the safety and efficacy of ivermectin and hydroxychloroquine as treatments for COVID-19 are false and inaccurate because they are not supported by factual, scientifically grounded, and consensus driven scientific evidence (there it is again).
Susanna Naggie, M.D., M.H.S., et al., “Effect of Ivermectin vs Placebo on Time to Sustained Recovery in Outpatients With Mild to Moderate COVID-19,” 328 JAMA 1721 (2022), https://www.nejm.org/doi/full/10.1056/nejmoa2115869 (finding in a double-blind, randomized, placebo-controlled study with 1,800 participants that “[a]mong outpatients with mild to moderate COVID-19, treatment with ivermectin, compared with placebo, did not significantly improve time to recovery,” and that “[t]hese findings do not support the use of ivermectin in patients with mild to moderate COVID-19”);
I laughed out loud when they led their argument with the Naggie trial funded by the NIH as it contained the most brazen fraud of the Big 6 Pharma Ivermectin trials. All you need to know about the trial is that they moved the primary comparison endpoint of the trial.. in the middle of the trial. They moved the main comparison from symptoms at Day 14 to Day 28. Note that changing endpoints in the middle of a trial is a supposed never event. Except the same trick was pulled in the Remdesivir trial.
Anyway, in a presentation by Naggie, in this secondary endpoint, you can see that ivermectin was superior at Day 14 to a high degree of Bayesian “statistical significance” but the “statistical significance” was not reached at Day 28 (I use quotes around statistical significance because it is an erroneous concept when doing Bayesian statistics but that is what they did anyway when they pre-specified a threshold of above 0.95 as “significant”). Can anyone tell me why they moved the endpoint to Day 28 in the middle of the trial:
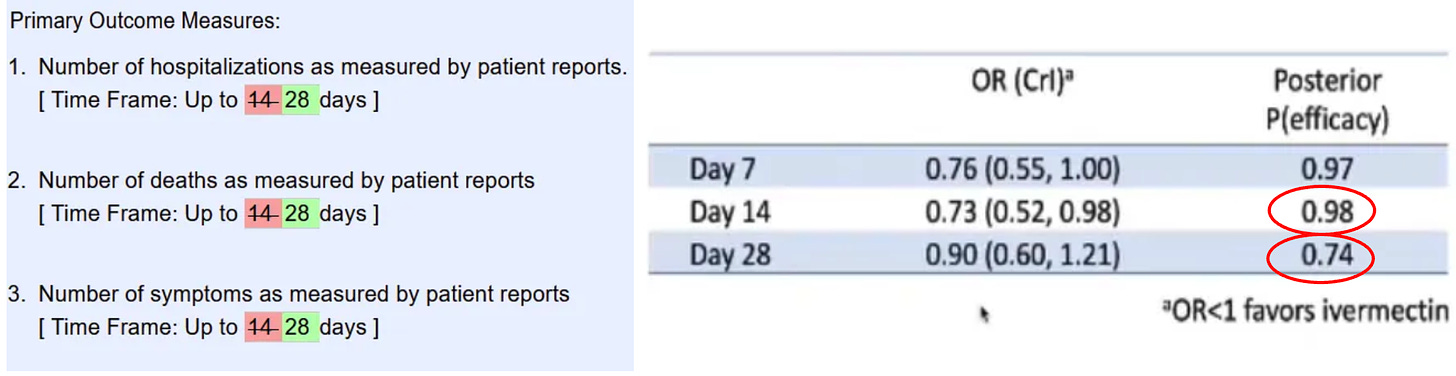
With this brazen maneuver (and many others) it allowed Naggie et al to publish this conclusion: “these findings do not support the use of ivermectin in patients with mild to moderate COVID-19.” Not-so-fun fact: Naggie also sat on the NIH covid treatment guidelines committee where she voted to not recommend ivermectin right before she and her University received tens of millions.. to study ivermectin in Covid. You want more? She also owns stock in a competitor to ivermectin (monoclonal antibodies for Omicron) and has received money from numerous other Big Pharma companies including Gilead. Lets get back to the letter…
Rather, the CCC seeks to accomplish precisely what you assert ABIM should be doing: seeking to “further the professional integrity of medicine by encouraging evidence-based debate” (emphasis added).
Indeed, as set forth in ABIM’s False or Inaccurate Medical Information policy, physicians have an ethical and professional responsibility to provide factual, scientifically grounded, and consensus driven scientific evidence (there it is again). As discussed above, by touting the effectiveness of ivermectin and hydroxychloroquine as COVID-19 treatments and casting doubt on the efficacy and safety of COVID-19 vaccines with such seemingly authoritative statements, you have made statements that are inimical to ABIM’s ethics and professionalism standards for board certification.
In light of all the evidence and circumstances, the CCC determined to recommend that your board certification be revoked.
There is only one silver lining here. One – the impending loss of my certifications does not affect me materially because I have a private fee-based practice due to my need for complete autonomy and lack of restrictions in empirically treating the vaccine injured with various repurposed and alternative therapeutics. I thus cannot and will not accept insurance, and secondly, my academic career is over – no longer will I ever enter back into the system of medicine.
About the only opportunity this whole attack has created is one where I get to defend myself on appeal in a debate with three academic white coats of their choosing. Bring. It. On.
Although the outcome of the debate is assuredly pre-determined, I know it will satisfy a deep yearning many of us dissidents have had for going on 3 years now – to debate someone, anyone, anywhere. Crush them with data. Make ‘em look silly although I will be the only one who knows it happened. It will let me vent my disgust at how they have widely disseminated corrupted scientific evidence and policies while simultaneously ignoring the clinical observations and expertise of frontline doctors who have treated thousands of actual Covid patients.
I will then toss in a little lecture about how RCT’s have long ceased to be a credible means of proving anything in science given that in modern medicine only “Big RCT’s” count and that all “Big RCT’s” require such massive funding that the bias of the funders outweighs any objectivity such trials can profess to attain. I will also remind them that throughout modern medical history, the findings of RCT’s and retrospective observational trials are identical, yet academia has been taught to systematically ignore observational trials. Reason: only massively funded entities can conduct a “Big RCT” while any committed clinician willing to give up nights and weekends can conduct an observational trial. Pharma cannot allow research to be conducted that they have no control over – so they took over the journals and medical school curriculums which now literally teach that observational controlled trials can only be considered “hypothesis generating” and thus their results should not be acted on. Nonsense.
I will also remind them that they are violating international law and human, civil, and political rights as argued by Meryl Nass in another of her excellent posts regarding her own persecution by her state licensing Board:
International law is on our side. A total of 172 countries are parties to the International Covenant on Civil and Political Rights:
According to the 1948 Universal Declaration of Human Rights, Article 19,
“Everyone has the right to freedom of opinion and expression; this right includes freedom to hold opinions without interference and to seek, receive and impart information and ideas through any media and regardless of frontiers.”
According to the 1966 International Covenant on Civil and Political Rights,
“Everyone shall have the right to freedom of expression; this right shall include freedom to seek, receive and impart information and ideas of all kinds, regardless of frontiers, either orally, in writing or in print, in the form of art, or through any other media of his choice.”
And the Nebraska Attorney General protected doctors and pharmacists in Nebraska from their Boards, explicitly allowing them to prescribe HCQ and IVM. His opinion is a tour de force, which goes into detail about why the CDC, FDA and NIH guidelines are contradictory, unscientific and should not be followed. It should be cited in every case.
I also plan on reminding them that the FDA got its ass handed to them in court last week during a hearing of Paul Marik, Mary Tally Bowden and Robert Apter’s suit against the FDA. From an Epoch Times article on the hearing:
“FDA explicitly recognizes that doctors do have the authority to prescribe ivermectin to treat COVID,” Ashley Cheung Honold, a Department of Justice lawyer representing the FDA, said during oral arguments on Aug. 8 in the U.S. Court of Appeals for the 5th Circuit.
The statements “don’t prohibit doctors from prescribing ivermectin to treat COVID or for any other purpose” Ms. Honold said.
“FDA is clearly acknowledging that doctors have the authority to prescribe human ivermectin to treat COVID. So they are not interfering with the authority of doctors to prescribe drugs or to practice medicine,” she said.
So, if the FDA recognizes we have the authority to prescribe ivermectin, then assuredly we are allowed to have the opinion that it is a valid therapy. However, the ABIM will not allow an ABIM certified physician to publicly express this opinion or recommend this practice. Maybe the ABIM should have a little chat with the FDA?
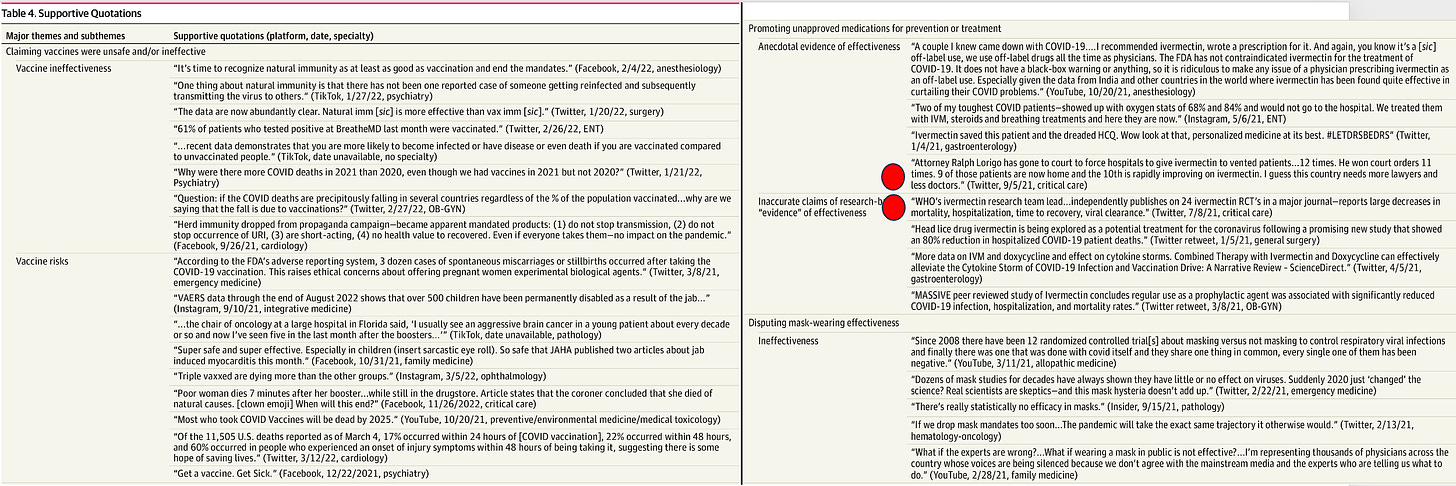
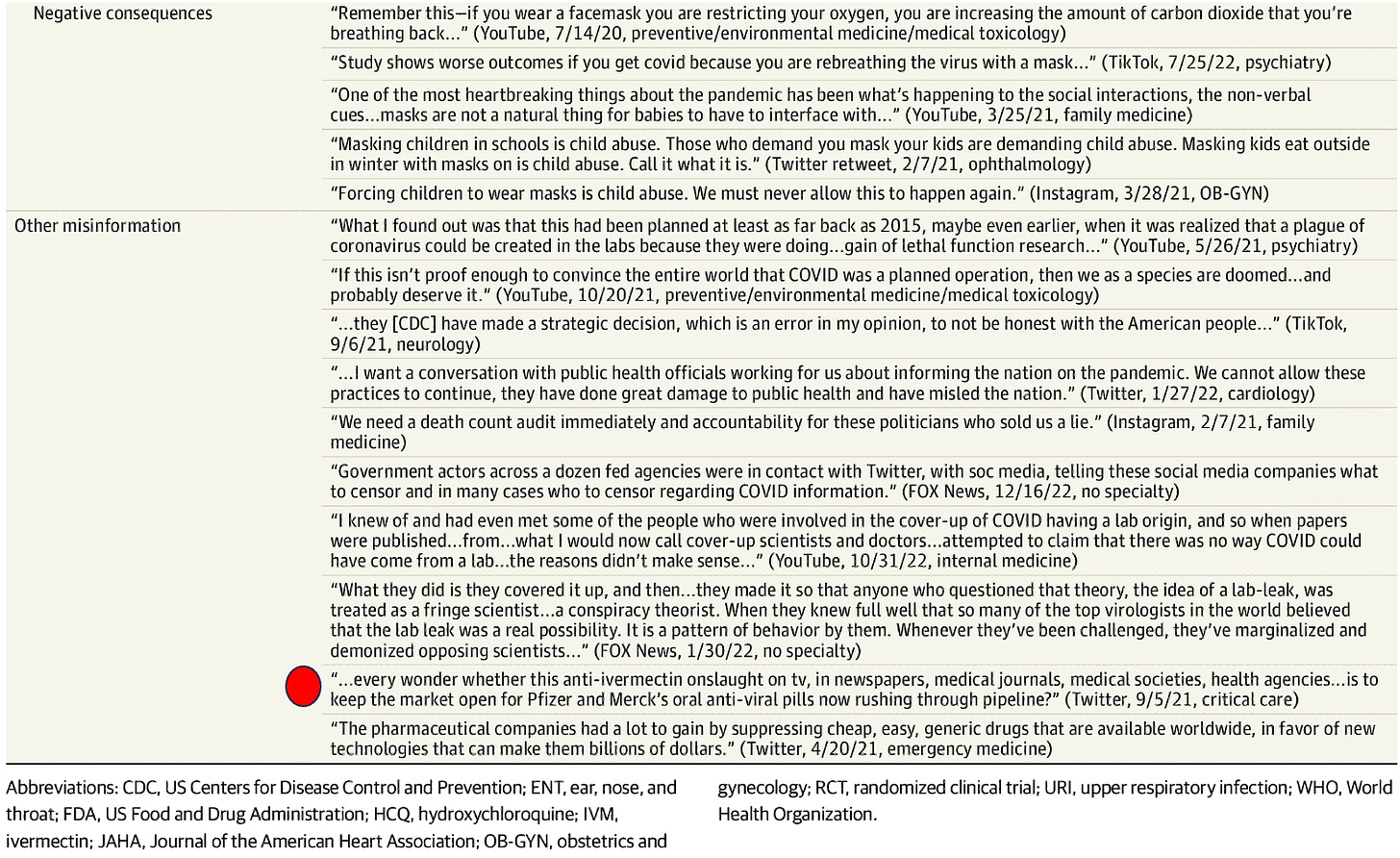
The nonsense doesn’t end with the ABIM, as they are only one prong of this campaign. How is this for some comic relief, published last week in one of the top journals in the world where they found that almost all the Covid misinformation in the U.S on social media can be traced to 52 doctors.

I was honored to discover that yours truly made the list! In their quoted examples of misinformation in Table 4, I have taken the liberty of owning up to the posts attributed to me, all of which I stand by to this day:
I think I will finish with this excerpt from a recent Wall Street Journal op-ed touching on the Missouri vs. Biden case where the administration is being sued for its systematic censoring of U.S citizens on social media by every intelligence and health agency in our Federal government :
This is where the decision of U.S. District Judge Terry Doughty sheds light. His detailed recounting shows a Washington energetic in protecting Americans from Covid opinions, expertise and claims that conflicted with its own, at a time when it served politicians to show they were trying to save Americans from encountering a virus that couldn’t be avoided. When government has a message to deliver, especially when the political stakes are high, it won’t be content just to push its own message, it will try to silence others. Fighting back will always be necessary. The only surprise in our age is how thoroughly the “liberal” position has become the pro-censorship position (that last line is a doozy).
Featured Video
US Military: Who’s Pulling the Strings? /Lt Col Daniel Davis
or go to
Aletho News Archives – Video-Images
From the Archives
From glorious millennia to death and destruction: Zionists rewrite Palestine’s story

By Miko Peled | MintPress News | September 20, 2021
One of the great tragedies of Palestine is that almost every day there is a commemoration of one massacre or another, the death of a child or destruction of a home or village, leading one to think that the Palestinian narrative is one of death and destruction, which is what Israel wants people to think. But the truth is that this is not the case. The Palestinian narrative is one of a glorious history with periods of great sadness and tragedy. It is the Zionist story that is full of killing, stealing and destruction and not, as they try to sell it, one of creation and growth.
September 16, 2021, marked 39 years since the massacres at Sabra and Shatila refugee camps in Lebanon. As people remember and mourn the thousands of unarmed civilians who were butchered and the countless who survived suffering terrible injuries and emotional scars, we must also remember the man that stood behind this bloodbath.
This was a man whose complicity even the Israeli authorities could not ignore, the former general and renowned war criminal Ariel Sharon. And although he was momentarily penalized and banished from politics, he very quickly returned, and for a quarter of a century, he was the most powerful and influential man in Israeli politics. … continue
Blog Roll
 Aletho News
Aletho News- University of Vienna Student Assembly votes for academic boycott of Israeli universities
- Pro-Israel voices win out, kill bill to stop US-Israel military integration
- Khamenei: US-Israeli System of Domination Has Been Defeated
- Iran to deepen ties with ‘principal strategic partner’ China: Ghalibaf
- House Votes to Terminate Iran War, While Preparing to Vote to Ramp Up the Ukraine War
- IRGC: No peace without Israel’s withdrawal from occupied Lebanese territories
- Israeli war chief vows continued strikes on Lebanon as part of ‘conditional’ truce
- UNIFIL peacekeeper killed after shells strike position near Marjayoun
- Hours after reiterating ‘ceasefire’, ‘Israel’ targets car in S.Lebanon
- US says Lebanon, Israel reach new ceasefire deal, Hezbollah vows resistance, rejects disarmament
- If Americans Knew
- The battle for Al-Aqsa: How Israel is reshaping the status quo
- Israeli study finds starvation in Gaza was result of deliberate policy
- US-Israel integration in NDAA is far from ‘America First’ – Joe Kent
- Now will the world believe? Israeli study finds starvation in Gaza was deliberate policy – Daily Update
- The Faustian Bargain of Journalists Embedding with the Israeli Military in Gaza
- AIPAC: Defending the Indefensible
- “You Either Leave Right Now or You Die”—Israel’s Ethnic Cleansing of a Village in Lebanon
- Selling American dead bodies to the US Navy for Israeli military training?
- AIPAC affiliate has funded lavish trips to Israel for dozens of Congress members since 7 October, filings reveal
- Trump called Netanyahu crazy, stopped Israel attack on Beirut: three articles
- No Tricks Zone
- New Study: Solar Photovoltaic, Wind Power Fail To Meet Annual Energy Demands 62% Of The Time
- Germany’s Die Welt: “Too Much Is Too Much” … Green Energies Are Cannabalizing Each Other!
- Germany’s Ecological Holocaust… Once Fairy Tale Forests Getting Cleared For Wind Turbines
- A Grand Solar Minimum Has Arrived…Global Cooling Of At Least 1°C Is Expected By The 2030s, 2040s
- European “Expert Commission” Urges COVID-19-Like Global Climate State Of Energency!
- Real-World Observations Do Not Support The Position That Climate Change Is Human-Caused
- Germany’s AfD Party Calls Debunked Climate Scenarios “Greatest Fraud In Human History”
- Researchers Find Rapid Global Warming Phase At End Of Last Ice Age (Ca.18,000 Years Ago)
- Even The DNA Of Single-Celled Plankton Can Upend Alarmist Arctic Sea Ice Melt Claims
- Scandal: Although Climate Panic Is Canceled By IPCC, Europe’s Policymakers Continue With Their Crushing Policies
