Son Alleges Texas Hospital’s COVID Treatment Plan Killed Unvaccinated Father
By Michael Nevradakis, Ph.D. | The Defender | August 21, 2023
For decades, Constantine “Gus” Kotsanis was a respected otolaryngologist in Grapevine, Texas. Having emigrated from Greece at age 15, Constantine became a University of Texas-Southwestern medical professor, a cancer and autism researcher and founder of the Kotsanis Institute of Functional Medicine.
In an interview with The Defender, Constantine’s son, Andy Kotsanis, said that in the 1980s, his father helped transform what was previously the Grapevine Medical Center into the Baylor Scott & White Medical Center — Grapevine, affiliated with Baylor University. It is now the largest not-for-profit health system in Texas.
It was in that same hospital, that on March 14, 2021, Constantine “violently lost his life,” his son said — days after being admitted with respiratory problems and a subsequent COVID-19 diagnosis.
Andy said he believes his father’s death resulted from the treatment he received, including remdesivir, fentanyl and other drugs Constantine and his family had not authorized.
Andy also alleges he was “threatened and assaulted by the police and the hospital administrator” as his father was dying, and barred from the room as his father passed away.
Today, Andy is raising awareness about his father’s death — and the stories of others who endured similar treatment — through his own activism and as a social media outreach coordinator for the FormerFedsGroup Freedom Foundation.
Andy discussed his family’s experience around his father’s hospitalization and subsequent death at Baylor Scott & White, and the activism he is now involved in as a result. He shared extensive documentation and photos with The Defender to corroborate his story.
Hospital president to victim’s family: ‘I’m not letting you see him’
Andy told The Defender that he was the very first baby born at Baylor Scott & White’s then-new outpatient operating room. Just days earlier, his father “was the first physician to do a procedure in that operating room,” he said. “So, there’s a very long history with my father and Baylor.”
“This is a story of tragedy, but also betrayal, because he helped build that place,” Andy said.
According to Andy, his father was not vaccinated for COVID-19. “He was not a fan of it,” he said. He said he now believes his father’s vaccination status may have played a crucial role in the treatment he received in the hospital.
After hearing about Gail Seiler’s story, Andy said, “Maybe they played that same game with him and did not tell the truth completely to us,” he said.
Andy said his father spent “a little over six days” in the hospital. He was admitted when “he had a hard time breathing. … He was really struggling, [in] a great state of hypoxia, almost to the point where he was exhausted with breathing.”
At the hospital, his father tested positive for COVID-19 and was admitted. According to Andy, the pulmonologist assigned to his father, Dr. Jagadeshwar Gummi Reddy, administered four rounds of remdesivir daily.
“At first, my father was calling me, saying ‘I feel a little bit better, everything’s fine,’” Andy said. “Then things started to go downhill very quickly. … I didn’t understand at the time what remdesivir was, how powerful it was and what it did to people or how deadly it was.”
A few days later, another phone call came from the hospital, this time from nurse Sarah Grice, who told Andy’s mother, “I had to put your husband in restraints, because he was confused about why he had tubes in his lungs.”
After his father’s death, Andy discovered that hospital medical records claimed no restraints were used.
“At the time, I didn’t know that there’s a formula that they follow: They sedate you and they’ll put you in restraints if they have to put remdesivir in you,” Andy said. “We requested to speak to the hospital administrator, Chris York, president of Baylor Grapevine at the time.”
According to Andy, York “arrogantly” told them, “‘I don’t care who your dad was or who your husband was, I’m not letting you see him.’ I said, ‘I think this is criminal. You’re not letting me see my dad. I don’t know what’s going on. Please let me see my father.’”
But York told them, “If you think it’s a crime, call the police,” according to Andy, who said, “I’ll never forget that sentence for the rest of my life.”
Nurse ‘started performing the most violent chest compressions I’ve ever seen’
Grice called the family again, telling Andy’s mother, “Your husband said he wants to die and be put on a ventilator.” This sounded nothing like my dad, Andy said, “because all over his chart, it says he didn’t want to be intubated. No ventilator, no remdesivir.”
“So how do you go from ‘No, I don’t want to be on a ventilator’ to ‘I want to die, put me on the ventilator’ in a matter of less than six days?” Andy asked.
On what turned out to be the day before his father’s death, Andy, his mother and their attorney “barged in the front door … demanding to see my father,” Andy said. “We were ready to press charges if they didn’t let us in.”
Subsequently, York “made the decision to only let my mother in,” Andy said, while Reddy spoke to him in person. According to Andy, this discussion was peculiar.
“He came downstairs with his mask off, with his hands shaking like he was scared, like someone was after him,” Andy said. “He introduced himself [and said] ‘My hands are tied. There’s nothing I can do.’ I said, ‘That’s not a good answer, sir,’ and he just walked away. It was almost like he was being bullied.”
Reluctantly, Andy’s mother approved the use of the ventilator that day, Andy said. But at 5 a.m. the next morning, the hospital called to say his dad was coding.
Again, only one family member was allowed into Andy’s father’s hospital room, so the family decided to let Katerina, his sister, be that person.
Expecting “some humane treatment,” Andy said they were instead met at the front door by Donna, an older nurse, and Demorrius Jones, a policeman, who “arrogantly greeted us in a very rude way.”
According to Andy, they got York on the phone, who said, “No one can go into the room. You have to watch him die through the glass.”
Andy told The Defender that, through the glass, they saw nurse practitioner Rommel Villas Lantajo handing a syringe to Grice, who then injected Constantine.
“Before she injected him, I saw the heart monitor,” Andy said. “He had a pulse of 122. So, I’m thinking to myself ‘Why is he coding? He has a heartbeat.’”
After the injection, “his pulse started to drop rapidly, and she [the nurse] started to do the most violent chest compressions I’ve ever seen,” Andy said.
“His body was bouncing 10 inches off the table. It was like watching someone get chainsawed in half. It was very violent and brutal, and looked more like she was trying to kill him, not save his life,” Andy said.
Andy said his father’s health was “already compromised with all those drugs they gave him” in the preceding day, which included fentanyl, adding that “he was still on the ventilator when she [Grice] was doing what she was doing.”
Grice subsequently stopped administering chest compressions and, according to Andy’s mother, “turned off all the machines.” Immediately following this, “My dad lifted his chest off the table, and then he had a seizure and died in front of my mother” while she was screaming “Stop, stop, stop!”
Andy was not present as his father died, though, because the police officer had “forced me out of the ICU. He threatened to arrest me if I didn’t leave the hospital immediately.”
Father’s death ‘malicious and arbitrary’
“They did this to a very kind, gentle soul,” Andy said, adding that his father’s death was “malicious and arbitrary, on behalf of Chris York, the administrator.”
“I’m still in shock,” Andy said, telling The Defender :
“The aftermath was so bad. I’m still in therapy over it. I’m very sad. I can’t put into words what a panic attack is like. I didn’t have irritable bowel syndrome until my dad died. You only get that when you experience something traumatic. Some people consider that a form of PTSD [post-traumatic stress disorder].”
“I’ve had several panic attacks,” Andy added. “I’ve lost count.” He said he’s “almost had to institutionalize” his mom. “I put my whole life on hold and I’m still, to this day, at her aid, trying to help her. She’s still not the same,” he said.
Andy also noted the anomaly of an extraordinary number of pages — many of them duplicates — in his father’s medical charts. “You’re in the hospital for six days but the chart is 948 pages long?” he asked. Another anomalous document dealt with “permission to be filmed,” he said, calling it “a very suspicious document.”
‘This is a huge cover-up’
His father’s experience led Andy to become an activist, he said.
“I’m trying to promote my story on my website and to inform everyone, the whole planet, that we’re witnessing the collapse of the healthcare system. … They’re using drugs in hospitals that are clearly not working,” he said. “I’m trying to show people that this is what they did to me. This is what they probably plan to do to you if you’re in there.”
“If that’s how you want to say goodbye to a loved one, go to Baylor Scott & White,” Andy said. “They’ll be more than happy to accommodate you if that’s your desire. That’s how I feel about this organization.”
“Hopefully, in the future, this can be a reference point for people to go, ‘We don’t want to be like Baylor, don’t pull a Baylor, don’t be like Baylor.’ That’s where I’m going with this,” Andy said. “This was so vicious and atrocious. I’ll never forget it.”
Aside from his website, Andy’s activism has included “putting road signs out, [placing] cards on doors,” he said, adding that such acts are “perfectly legal in the state of Texas” due to the Texas Citizens’ Participation Act.
However, just weeks after Andy began these activities, he was warned by local police and a local detective to “be careful” where he placed his signs and cards because his “First Amendment rights are limited.”
Andy said he experienced more difficulty with police when he attempted to press manslaughter charges against Baylor Scott & White. Local police referred him to Baylor Police and the Texas Rangers. When Andy contacted the Rangers, they advised him to “start a paper trail” by calling Baylor Police.
Yet, Baylor Police refused to take a report, telling him to “call our legal department.”
“So, this is a huge cover-up,” Andy told The Defender. “The police are covering up, in my opinion, what I would consider a homicide.”
Andy said his efforts, though, have managed to secure a degree of professional difficulty for York. According to Andy, “He orchestrated this, and now he’s no longer in the state of Texas. For a small while, he was an administrator in Arkansas, but thanks to my efforts informing his new employer, he’s no longer [there].”
In addition to his individual activism, Andy joined the FormerFedsGroup Freedom Foundation, which advocates on behalf of victims of COVID-19 hospital protocols and others with similar experiences. He described them as “the best group you can find if you’re a victim.”
“We’re on a mission,” Andy said. “We’re here to help as many people get as many stories out there and turn the narrative around.”
Many people have reached out to him through the FormerFeds Group but also through his own website, said Andy, describing similar treatment that they or loved ones experienced at hospitals, including at Baylor Scott & White.
Referring to the COVID-19-related hospital protocol prescribed by the Centers for Disease Control and Prevention, Andy said he is not certain if it was followed by Baylor Scott & White in his father’s case. But he noted that his and other victims’ experience make it sound like “there’s a formula they’re following.”
Andy said these efforts are important to everyone, even if they haven’t been victims of COVID-19 hospital protocols or similar treatment.
“We all get old and will need a little extra attention,” he said. “The question is, what kind of attention is that going to be? I’m hoping it’s going to be a real standard of care.”
Andy shared some words of advice for individuals who have had similar experiences or who may end up in the hospital for similar reasons.
“If you can get the chart, get the chart, print the chart. Read it before you do any reporting. Do your own homework,” he said.
He also recommends seeking professional help to grieve. “It’s okay to ask for help.”
“Also, understand that there are people like me out there, a lot of us that are going to, for as long as we’re alive, try to turn this thing around,” he added. “Don’t give up because you feel like you’re going nowhere. I have felt that way many times. … Believe in yourself. Don’t give up. Be persistent.”
Michael Nevradakis, Ph.D., based in Athens, Greece, is a senior reporter for The Defender and part of the rotation of hosts for CHD.TV’s “Good Morning CHD.”
This article was originally published by The Defender — Children’s Health Defense’s News & Views Website under Creative Commons license CC BY-NC-ND 4.0. Please consider subscribing to The Defender or donating to Children’s Health Defense.
Hurricane Katrina and the “Angels of Mercy”
Ethical boundaries in medical decision-making
By Jonathan Engler and Jessica Hockett | HART | August 21, 2023
The debate as to how much “pandemic” harm was caused not by a virus, but rather by the dystopian response to the perceived threat of a virus, has been raging for some time now.
Jonathan tweeted about this last year in relation to Lombardy and that thread was turned into this Panda article.
An analysis of the spatial characteristics of deaths during the spring 2020 wave in Northern Italy was carried out by him along with a Panda colleague; this suggested that it looked nothing like a spreading virus, and more like the sudden imposition of a policy response.
More recently, Jessica has essentially come to the same conclusions about New York: that something terrifyingly unnatural appears to have happened, which cannot be explained by the sudden spread of a deadly virus.
It surely does not require any scientific understanding whatsoever to glance at the below graph of total mortality rate in NYC going back to 2015 and see that what happened in a few weeks during spring 2020 suggests an abrupt episode of ferocious lethality which was at odds not only with anything observed anywhere at the time or thereafter, but also with even the highest estimates of the infection fatality rate alleged to have caused “the pandemic”.
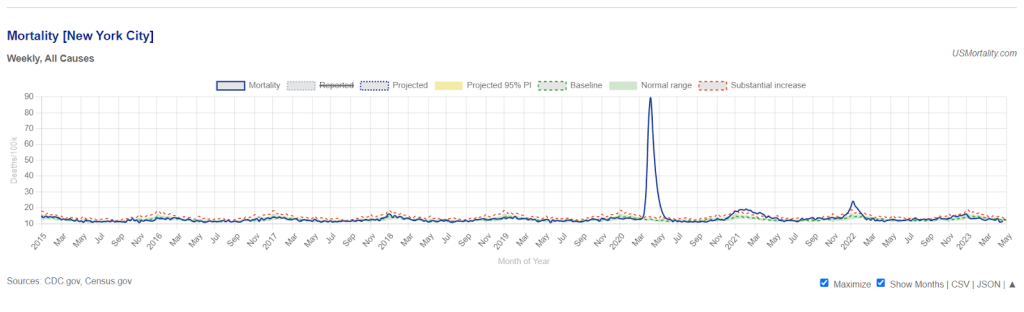
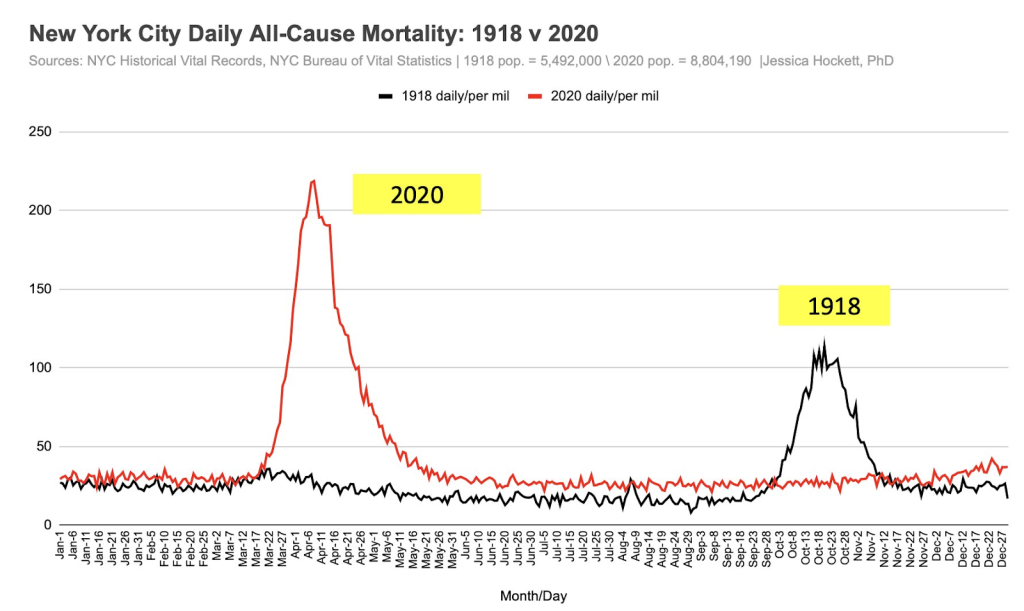
If we look back even further, it can be seen that the reported spring 2020 mortality spike in New York is actually around double that observed in the autumn of the 1918 pandemic. But other places in 2020 did not see waves of deaths anywhere near those observed during the 1918 pandemic.
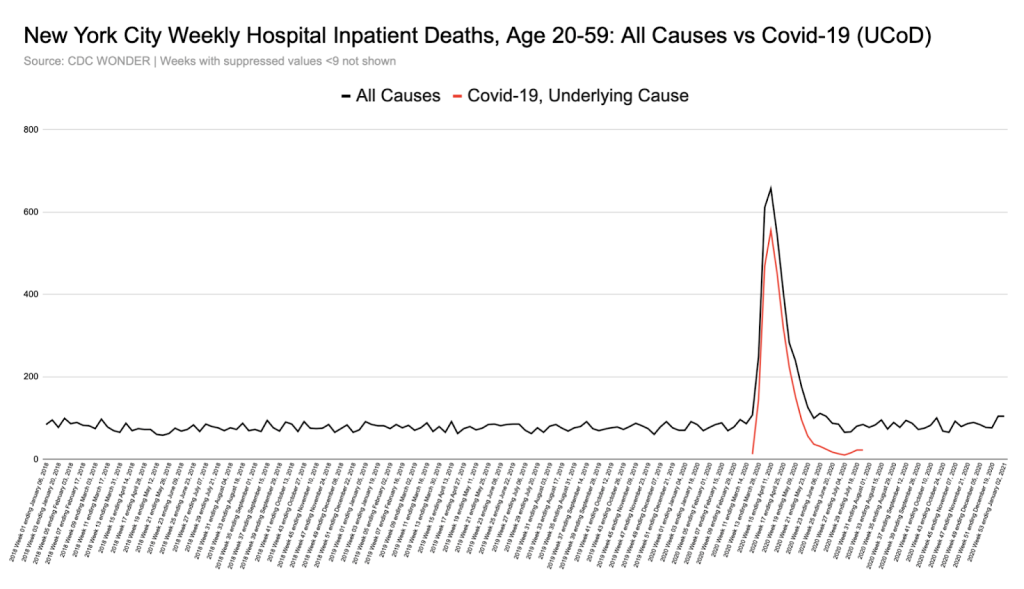
Moreover, unlike elsewhere, the increase in deaths was seen across a younger demographic, not exclusively in the elderly.
As shown in the graph below, all-cause hospital inpatient weekly death counts in the 20-59 age group were dramatically elevated for a short period, by a shocking 6-fold at their peak, with nearly all these deaths being coded as ‘covid’.
In fact, in New York, the % increase in all-cause deaths during the spring “1st wave” period was the same in the 20-69 year old age group as in the 70s and over:
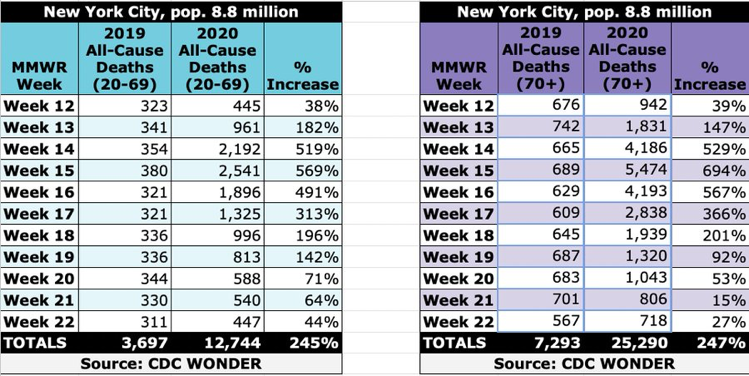
In other places, however, what we were told was the same disease caused by the same virus left the younger age groups largely untouched, with nearly all deaths being in the elderly.
This discrepancy remains completely unexplained. It seems unarguable that certain difficult questions certainly need asking about what happened in New York in 2020 if we are to unravel the truth about what happened there.
Of course, the narratives emerging from Northern Italy and New York in 2020 were instrumental in driving fear and hysteria worldwide. Moreover, the number of deaths in both places informed early estimates of the IFR. These inciting incidents directly sparked much of the worldwide exaggerated, fear-driven response to what we now know was (if anything) a virus mainly affecting the frail and elderly, to which most people already had sufficient immunity to prevent severe illness.
For these reasons, it is essential that particular attention is paid to try to ascertain precisely what happened in these specific places.
It’s worth detailing – as evidence for the deeply dystopian mindset operating at the time – just some of the many deviations from normality that adversely affected human health and immunity, or which constituted sudden changes to healthcare practice.
These included (but were not limited to):
- Stress and anxiety from confinement (being told to stay home) and fear propaganda
- Discouragement to attend hospitals if ill
- Reduced community prescribing of broad-spectrum antibiotics
- Low staff levels in healthcare settings due to self-isolation of those “testing positive,” even with no symptoms
- Isolating the elderly
- Barring loved ones from hospital and care homes
- Fear (on the part of HCWs) of tending to covid positive patients, compromising basic medical and care needs.
- Early and inappropriate invasive ventilation
- Overuse of midazolam and opiates
Inevitably, and rightly, some researchers have started to perform post-pandemic autopsies analysing the motives and reasoning used to justify policies and other changes in behaviour and to examine their real world consequences.
Some medical practitioners have taken umbrage at any suggestion that the stressful environment and sudden expectations and pressures laid upon them may have resulted in well-meaning medical staff crossing ethical lines, or violating the Hippocratic Oath.
Those who wish to point out that there is historical precedent for medical staff behaving diabolically while thinking they are doing good often invoke atrocities during the 1930s and 1940s (and receive opprobrium as a result).
However, there is a much more recent example, and one which we were oblivious to until recently, despite this incident being totally “out in the open”, the subject of a lengthy investigative article, book, and a TV mini-series: the post Hurricane Katrina incident at Memorial Hospital Center in New Orleans in 2006.
Wikipedia provides the basic facts:
In the hurricane aftermath, the basement of Memorial Hospital Center flooded, power failed, and battery power for essential equipment started to run out. Most, but not all, patients were successfully evacuated.
The hurricane occurred on 29th August. A shocking finding was made in the aftermath, as described in the Wikipedia article:
On September 11, mortuary workers recovered 45 bodies from the hospital. Toxicology tests were performed on 41 bodies, and 23 tested positive for one or both of morphine and the fast-acting sedative midazolam [branded as Versed in the US], although few of these patients had been prescribed morphine for pain.
In the following weeks, it was reported that staff had discussed euthanizing patients. Some reports went further; Bryant King, an internist at Memorial, told CNN that he believed “the discussion of euthanasia was more than talk.”
LifeCare told the state Attorney General’s office that nine of their patients might “have been given lethal doses of medicines by a Memorial doctor and nurses.”
King publicly charged that one or more healthcare workers had killed patients, based on conversations with other health care workers. King told CNN that when he believed a doctor was about to kill patients, he boarded a boat and left the hospital. King explained his actions in terms of his opposition to Pou’s alleged actions, arguing “I’d rather be considered a person who abandoned patients than someone who aided in eliminating patients.”
Following an investigation into the deaths described above, the local DA (“District Attorney”) decided there was sufficient evidence to charge three medical staff with four counts of second-degree murder. Charges against two were later dropped in exchange for testimony.
The prosecution was deeply unpopular. Despite substantial evidence of deliberate actions taken to terminate lives – indeed, enough to satisfy the legal definition for homicide – many members of the public felt medical staff were simply “doing their best” under very trying circumstances. According to a local reporter the incident “ignited a furious debate in New Orleans and elsewhere about whether sharp ethical boundaries can be drawn around decisions on patient comfort made in a crisis.”
The DA failed to win re-election, and when the new DA convened a Grand Jury* at an undisclosed location, much of the previously amassed evidence was not presented and some of the key witnesses not called. The Grand Jury decided that charges should be dropped.
Unsurprisingly, several commentators (e.g., Loyola University Law Professor Dane Ciolono) opined that the Grand Jury was convened and run in such a way as to ensure charges would be dropped while providing “cover” for such an outcome.
Whatever actually occurred at Memorial Hospital, or whatever the staff’s motives, the incident speaks to an unsettling, yet undeniable truth: during a crisis, “ethical red lines” – however deeply held and valued – may be easily crossed. Society may judge those decisions acceptable or understandable, as appears to have happened with the Memorial Hospital case.
In summary, it would appear that the legal process was manipulated to assure an outcome which accorded with public opinion – that is to say to extinguish the possibility of prosecution while maintaining the pretence of due legal process. In this way, facing up to the stark reality – that as a society we mete out justice arbitrarily when we wish to – was avoided. Perhaps the well-ordered rules-based system suggested by statutory definitions of what actions constitute crimes, is to some extent just “for show”.
The Memorial Hospital case obliterates – with a relatively recent example – the notion that doctors and nurses all have the same ethical boundaries which they simply will not cross under any circumstances.
Could such boundaries have been crossed during the recent covid event?
A number of commentators are considering the possibility that changes in the policies and practices around the use of certain drugs (midazolam and opiates), and procedures (invasive ventilation) – sometimes in combination – may have contributed to the high mortality reported, at least in some specific places.
In relation to drugs, in an article published on his Substack last year, the blogger known as Bartram’s Folly explored the possibility that (in the UK) sheer fear and panic may well have driven medical staff to use midazolam and opiates more liberally in patients with covid, which may have encompassed anyone with a positive covid test.
In the UK one such mechanism which may have encouraged this measure is the NICE Guideline NG163 (no longer on their website but available here or as PDF download here), about which others have also written in detail. This guideline effectively transposed the advice for treating end-stage cancer patients with midazolam and opiates into that for covid patients. More detail on this here.
Of the guideline, Bartram said,
“… the NICE guidelines appear to have introduced a pathway for doctors which allowed for (perhaps even encouraged) more than a gentle nudge for those who were ill with Covid towards death, some of whom might well have survived given the chance. This iatrogenesis hypothesis would mean that at least some of the deaths recorded as with Covid might well have been a direct result of the care guidelines as set out by NICE.“
Later, Bartram makes the point that the pretext of a crisis situation or emergency may establish the grounds for ethical boundaries to be crossed or disregarded, at least temporarily, under the auspices of ignorance or ‘doing one’s best’ with the information said to be known or available at the time:
It is important to note that in the iatrogenesis hypothesis it isn’t necessary for some people to have had an evil intent – it is entirely possible that individuals promoted and exercised a policy that resulted in needless deaths while believing that they were ‘doing the right thing’ (e.g., see Hannah Arendt’s concept of the banality of evil).
In particular, ‘petty bureaucrats’ appear to be readily able to think up policies without seeing the need to consider the full consequences, and when these consequences are eventually revealed will usually point to the minutes from endless meetings with other petty bureaucrats to show that they weren’t personally responsible for the policy and they were simply following process.
Of course, once a framework had been decided front-line staff might have been grateful for the guidance offered given the challenging times, at least until the negative consequences of the guidance became painfully clear.
It should also be remembered that – in the US at least – certain extraordinary policy measures may have been important factors. For example, during the emergency NYC Governor Cuomo issued executive orders and suspended laws which gave doctors and nurses immunity and absolved hospitals of the responsibility to keep close patient records. (The order itself can be found here, and some legal commentary on it here.) Articles in JAMA can be interpreted as giving ethical permission for physicians to issue unilateral DNR orders, avoid CPR, and ration ventilators and critical care beds.
Moreover there are numerous examples of doctors, nurses and others in the US who later said they were following guidance, learning as they went. (See this interesting essay by Dr Kory, for example.) Under these circumstances it is easy to see how they could assume that something which ordinarily might have been questionable would become acceptable as “everyone else was doing it”.
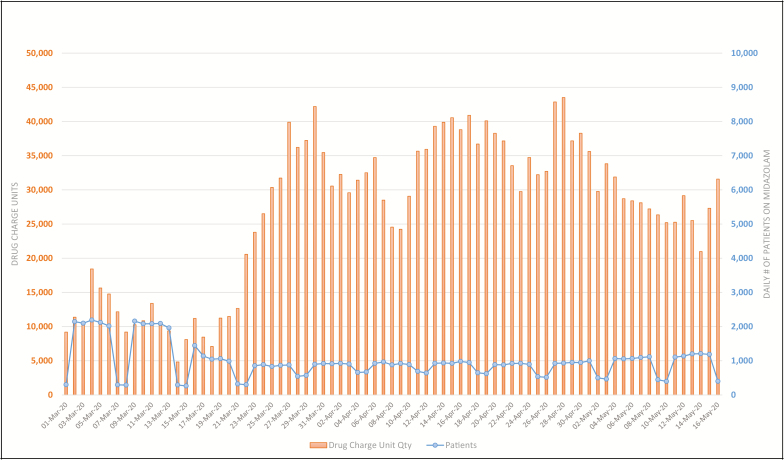
Evidence of increased midazolam use can be seen in the US as well as in the UK. This graph from a study describing the use of 7 specific drugs in 47 hospitals in NY shows the daily count of patients (blue) who received midazolam and the disproportionate quantities used (orange) between March 1 and May 16, 2020.
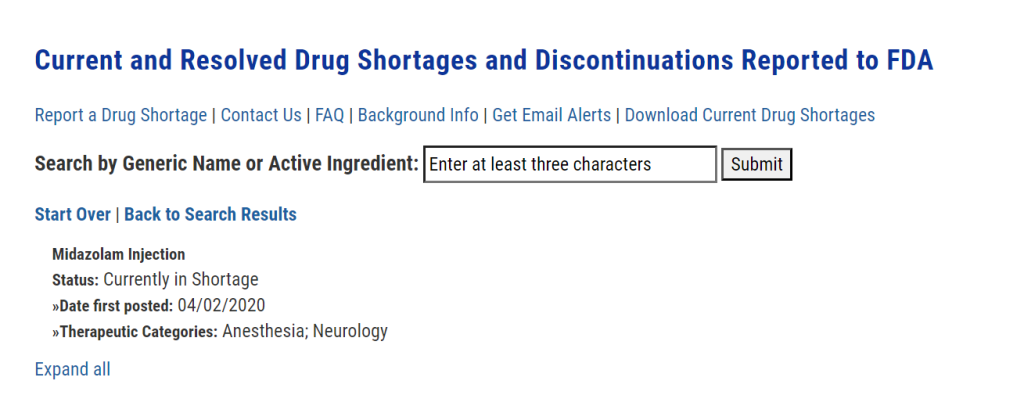
Moreover, midazolam is currently listed by the FDA to have been in short supply since 2 April 2020:
This Guardian article from 13 April 2020 reports on a letter sent by “a group of prominent medical practitioners and experts” to capital punishment states imploring them to:
“release their stocks of essential sedatives and paralytics that they hoard for executions” so that they can be “used for intubations and mechanical ventilation of the most severely ill coronavirus patients who cannot breathe for themselves”.
The tone of this letter can be taken to illustrate the sense of sheer panic prevailing at the time – certainly not conducive to rational decision-making – combined with the assumption that invasive ventilation was going to be extensively required and used.
This takes us to the question of invasive ventilation, whether it might have been used too often, inappropriately, and why.
As well as panic, the role of fear on the part of healthcare workers cannot be underestimated. Here is Dr Vinay Prasad stating that:
“It is a unique situation in medicine. In our whole medical career, doctors have never been personally afraid the way they were [with covid].”
Official guidance (see for example this from a British anaesthetists’ professional association) certainly reinforced the idea that one of the benefits of early intubation was to reduce the aerosolization of virus, such that it would be safer for those caring for the patients, compared to when non-invasive forms of ventilation were used.
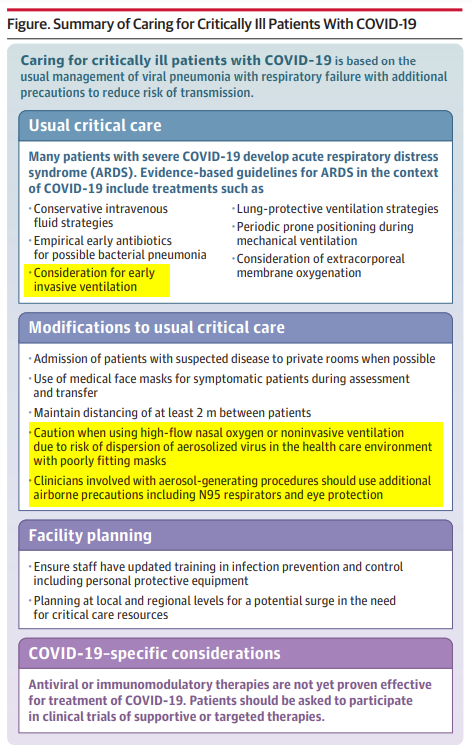
This JAMA Clinical Update “Care for Critically Ill Patients With COVID-19” published on 11 March 2020 strongly supports the idea that the thinking was very much that non-invasive oxygen augmentation could be dangerous for healthcare workers:
The journalist Alex Berenson was early to point out that ventilator shortage may have more to do with overuse “to protect staff” than to being overwhelmed by patients in respiratory failure.
It seems like fear may well have been augmented by official guidance to result in significant overuse of this measure.
It is important to understand the differences between the Memorial Hospital incident and what may have happened in the early stages of the covid crisis. In New Orleans, it may indeed have been reasonable to assume that it was going to be impossible to evacuate the patients (who were given midazolam and opiates to ease suffering) in time, and that they were indeed unsaveable due to the extraordinary circumstances. (Whether or not this was actually the case will probably never be known, because of the legal shenanigans described above.)
However, whether that applies to all, some, or just a few of those who died in spring 2020 after being administered the same or other drugs (or placed on mechanical ventilators or issued a unilateral DNR, etc.) is still a matter of debate whereas for sure, Hurricane Katrina was self-evidently an extreme weather event that created devastation and emergency conditions in its fury and wake.
Certainly, it seems clear that personal fear and a belief in the lethality of this infection drove much medical decision-making in the early days. It is not hard to imagine actions being taken which were then rationalised by imagining the suffering that had been prevented, limited resources preserved, and many lives saved. The deaths witnessed could easily have acted as positive reinforcement in the minds of healthcare workers as to how serious the illness was. These protocols could lead to the deaths of patients who were not particularly old and frail and thus reinforce the message that the virus was potentially fatal even in such people
The decisions that healthcare workers made, and the influences on and factors involved in those decisions, will be discussed and dissected for decades to come. When humanity is ready to confront what occurred – and admit that ethical inversions in hospitals and care homes contributed to unintentional iatrogenic death, we can move toward keeping it from happening again.
* (A Grand Jury in the US is a specific type of court empowered by law to determine whether probable cause exists to support criminal charges for a suspect in a crime. Louisiana – in which New Orleans is situated – is one of 23 US states that use grand juries for indictments in serious crimes.)
Eris vaccine marketing hits Germany, complete with panic about a nonexistent August “Covid wave”
eugyppius: a plague chronicle | August 20, 2023
We will not be free of the virus until we are free of the vaccinators.
The leftist taz newspaper on 17 August: New German Wave: The new Covid variant Eris has arrived in Germany. Concerns about a new wave are growing – but the country is not well prepared.
The pandemic is over, but the virus is still dangerous: Reports of the new variant EG.5.1. seem to confirm this analysis. EG.5.1. (Eris) has been considered a “variant of interest” since 9 August. According to the WHO, the phenotype does not differ fundamentally from other Omicron lineages and does not require special public health measures …
With the announced end of the pandemic, virtually all mandated protective measures have been lifted in Germany. The most important instrument in the fight against Covid-19 is thus the immunisation of the population through infection or vaccination.
Das Erste, state media, on 19 August: Covid Variant “Eris”: How Dangerous is the New Mutation EG.5?
The World Health Organisation WHO has upgraded the new Covid mutationEG.5. This variant, called “Eris,” now belongs to the “variants of interest.” …
As WHO Covid expert Maria Van Kerkhove explained in Geneva on Wednesday, more severe outcomes have not been observed with Eris, but vaccination confers less protection than with other virus variants. …
Even though the new variant is unlikely to cause severe disease, the [German vaccine regulatory authority] STIKO still recommends getting vaccinated – above all to avoid possible long-term consequences of SARS-CoV-2 infection and to protect employees in medical and nursing care.
n-tv, a subsidiary broadcaster of RTL, on 18 August: The Number of Coivd-19-Cases Continues to Rise.
The pharmaceutical company Moderna has announced that its updated Covid vaccine according to an initial study is effective against the Eris sub-variant. The company now expects to launch the new vaccine in time for the autumn vaccination season. Approval from vaccine regulators however is still pending.
Moderna, like vaccine manufacturers Novavax and Pfizer, has developed versions of its vaccines with Biontech SE that target Eris subvariants. Shortly before, the pharmaceutical company Pfizer had reported that its revised vaccine had been effective against Eris in a study with mice. …
Most recently, it was suspected that the cinema hype surrounding the feel-good film “Barbie” and the gloomy biopic “Oppenheimer” may have caused many infections. At the same time, the Robert Koch Institute (RKI) recorded an increase in the number of reported Covid infections. Experts, however, see no reason for concern so far.
Frankfurter Rundschau, a regional Frankfurt paper, on 17 August: Covid comeback with “Eris”: First experts demand return to masking.
Is Covid on the attack again? There are indications that the virus is once on the rise once more. …
British doctors are already calling for a return to masking. [Relentless virus charlatan and deranged hypermasker] Trisha Greenhalgh suggests that, “in view of the spread of new variants,” masking in high-risk situations should be considered.
The [virus surveillance] of the Federal Ministry of Health shows that the numbers are also on the rise in Germany. … “Eris” is already responsible for every fourth corona infection, according to new figures from the RKI. “The number of Covid-19 cases reported to the RKI .. seems to be related to the increasing circulation of this ‘variant of interest’,” the Robert Koch Institute says.
The increase in the case numbers – at least in Great Britain – coincides with the opening of the blockbusters “Barbie” and “Oppenheimer” in British cinemas, which has given rise to talk of the “Barbenheimer” phenomenon. It is well known that larger crowds in enclosed indoor spaces are associated with an increased risk of corona infection. So is it time for a mask renaissance?
In the USA, more and more voices calling for one. [Relentless virus pest] Eric Feigl-Ding … used the hashtag #MaskUp on Twitter to call once again for protecting oneself from Covid infections with masks. Health Minister Karl Lauterbach shared the post, warning that the latest Covid data from New York is “worrying.” …
“There is still a risk that a more dangerous variant will emerge, which could lead to a sudden increase in cases and deaths,” emphasises WHO Director-General Tedros Adhanom Ghebreyesus. Not only adapted vaccines that take the new variants into account, but also wearing a mask would then help to protect oneself and others, Frankfurt virologist Martin Stürmer told Spiegel.
tagesschau, state media, on 17 August: Covid Case Numbers are Rising Again.
The number of laboratory-confirmed Corona cases in Germany is rising again – but at a relatively low level. This development has been ongoing for around a month, reports the Influenza Working Group at the Robert Koch Institute (RKI) … According to the report, about 2,400 confirmed cases of Covid-19 were reported nationwide last week. This is more than double the number reported in the week ending 9 July, when there were about 1,000. …
According to the RKI report, the activity of acute respiratory diseases in general in the population was “at a low summer level.” … “Anyone with symptoms of an acute respiratory infection should stay at home for three to five days and until the symptoms have clearly improved,” advises the RKI. …
Despite all of this obnoxious verbiage, absolutely nothing of virological note is happening in Germany. Official Covid testing has been all but abolished here, forcing our journaloids to unearth statistics from RKI influenza surveillance – something they refused to do during the pandemic itself, because the flu people routinely posted data that undermined their panic narrative. Here, I’ve circled in red the scary rise in infections from the latest RKI report that we’re meant to be worried about:
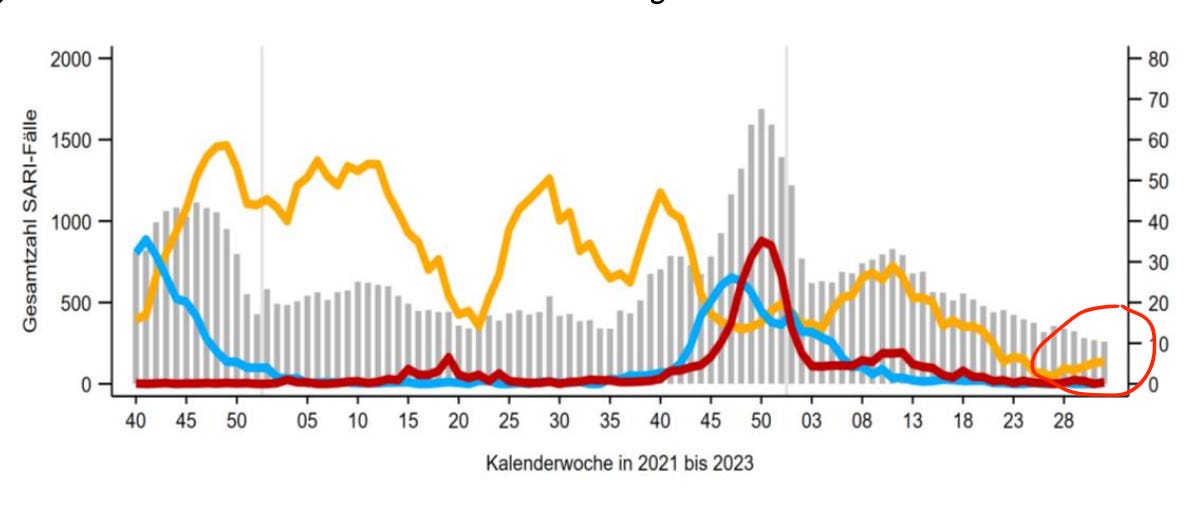
This microscopic uptick is dwarfed by the February/March wave that peaked between weeks 8 and 13. Our media luminaries took next to no notice of this frightening late-winter surge, and as I type this, Covid diagnoses have not even re-achieved their June levels. The difference between the state of things now and the state of things in February is not the unremarkable Eris variant. XBB was also debuting across Europe early this year, driving the post-February case peak, and nobody cared. The only thing that is different now, is the proximity of the autumnal vaccination liturgy and the prospect of new, updated vaccines from Pfizer/BioNTech, Moderna and Novavax. That is why we are hearing about variants and masks and Long Covid all over again. It is also why many of these articles contain buried within them somewhere the advice to line up for the shiny new anti-Covid juice this Fall. This whole thing is, very plainly, a psy-op, if a very low-effort one.
There are several patterns in the German reporting that are worth noting. First of all, the latest hysteria was unleashed on 17 August, prompted by a report on Eris from the German news agency Deutsche Presse-Agentur. Particularly in the realm of routine reporting, the news agencies are a powerful coordinating force, and their influence here means that the full media panic machine is not engaged. We’re looking instead at pieces thrown together by low-level staff desperate to fill column inches. Second, all the German stories are firmly downstream from Anglophone sources, going so far as to recycle from British tabloids the improbable theory of a “Barbenheimer” wave (it is painful even to type this stupid word). Third, at least German health authorities – Karl Lauterbach excepted – resolutely refuse to provide virus doom quotes. Thus the Frankfurter Rundschau had to appropriate the tweets of Anglosphere mask hysterics like Greenhalgh and Feigl-Ding to make Eris sound scary.
I know there are rumours that American authorities are planning to bring back mask mandates and other restrictions in the coming months, and I’ll be honest: We should be so lucky. If the pandemicists try to kick up another round of non-pharmaceutical interventions this fall, they’ll be flirting with self destruction. There are important prerequisites for virus panic: You need a plausibly novel pathogen, the risk of which can be exaggerated. You need a prevailing sense of stability, with nothing else much going on, because the public health interventions themselves have to seem new. Risk, excitement and the prospect of a break from routine are important enticements. That’s all gone now. Covid is not a new scary virus anymore; nearly everyone has had personal experience with it. Solid majorities everywhere have learned to hate lockdowns, despise masking and avoid the mRNA vaccines. The pandemicists need a plausibly new virus to reopen the circus, and they need a lot of people to forget about what a misery the last pandemic response was. They’ll have another chance in ten or fifteen years, I’d guess. Then, it’ll be time to worry.
Critics Slam JAMA Study Claiming 52 U.S. Doctors Spread COVID ‘Misinformation’
By Monica Dutcher | The Defender | August 18, 2023
Critics of a study published this week in JAMA concluding 52 doctors from across the U.S., propagated “COVID-19 misinformation about vaccines, treatments, and masks on large social media and other online platforms” called the study nothing more than “propaganda.”
“Ultimately, misinformation is just a weaponized term meaning nothing,” said Vinay Prasad, M.D., MPH. “People who use it are often completely ignorant of science and truth.
Prasad and others pointed to several flaws in the study, including the researchers’ definition of “misinformation,” the reported percentage of those with post-COVID-19 condition, or “long COVID” and the false claim that the Johnson & Johnson vaccine alone led to deaths — as deaths also have been linked to the Pfizer and Moderna mRNA vaccines.
The CDC as the arbiter of COVID truths
The University of Massachusetts researchers who produced the study defined misinformation as “assertions unsupported by or contradicting U.S. Centers for Disease Control and Prevention [CDC] guidance on COVID-19 prevention and treatment during the period assessed or contradicting the existing state of scientific evidence for any topics not covered by the CDC.”
But in an Aug. 16 Substack article, Prasad — a hematologist-oncologist and professor in the Department of Epidemiology and Biostatistics at the University of California, San Francisco — challenged the notion of using the CDC as the litmus test for pandemic-related information.
CDC “made many errors,” Prasad wrote, citing a paper he published in March, documenting 25 statistical or numerical errors made by the CDC that he said raised questions about the agency’s “real or perceived systematic bias.”
It’s also well documented that the agency constantly changed its mask guidance and published conflicting information about vaccine effectiveness.
Dominique Brossard, professor and chair of Life Sciences Communication at the University of Wisconsin-Madison, who studies medical misinformation, told USA Today, “The guidance kept on changing … Communication around the vaccine was horrible.”
Dr. Jeff Barke, an Orange County, California, primary care physician and founding member of America’s Frontline Doctors, called the CDC “a captured agency,” saying “it makes no sense whatsoever to recommend this toxic product [COVID-19 vaccines] to children.”
The CDC never came out with early treatment guidelines, Barke said. It was always about vaccines and masks. Barke recalled prescribing ivermectin to his patients and the pharmacists not filling it, asking him for the “diagnostic code” in order to proceed.
Barke told The Defender :
“The pharmacy never asks for a diagnostic code if you prescribe OxyContin for a patient. So it’s OK for a doctor to prescribe a Schedule II narcotic — no questions asked — but I can’t prescribe a product that has a proven safety record of 50 or 60 years.”
Barke is a co-plaintiff in a lawsuit to stop a California law that subjects the state’s doctors to discipline, including the suspension of their medical licenses, for sharing “misinformation” or “disinformation” about COVID-19 with their patients.
What exactly is ‘misinformation’?
The study’s authors identified four categories of “misinformation”:
- Claiming vaccines were unsafe and/or ineffective.
- Promoting unapproved medications for prevention or treatment.
- Disputing mask-wearing effectiveness.
- “Other misinformation,” to include conspiracy theories and the virus’s origins.
The authors reviewed COVID-19-related posts from doctors on the social media platforms Twitter (now X), Facebook, Instagram, Parler and YouTube between January 2021 and December 2022.
The researchers initially focused their Twitter review on America’s Frontline Doctors’ profile because of the organization’s “volume of COVID-19 misinformation in its tweets” and “large following.”
Physicians who followed America’s Frontline Doctors’ Twitter page were targeted on Twitter and other platforms.
Using the search terms “COVID,” “vaccine,” “doctor,” “physician,” “ineffective,” “pharmaceutical,” “ivermectin,” “hydroxychloroquine” and others, the authors of the study identified 52 doctors — 50 licensed and two unlicensed — who used social media to spread COVID-19 “misinformation.”
Results showed most of the 52 physicians (76.9%) who posted “misinformation” did so in more than one of the four categories identified. The majority posted vaccine “misinformation.”
Dr. Meryl Nass — who on Thursday sued the Maine Board of Licensure in Medicine and its individual members, alleging the board violated her First Amendment rights and her rights under the Maine Constitution — called the JAMA study “a piece of propaganda.”
Nass said:
“There is no science. They [the authors] are trying to make it look like they’re doing something quantitative when they’re not. There was a lot known about the ineffectiveness of the vaccines at the time they were working on this paper.”
Unpacking the misinformation in the misinformation study
The University of Massachusetts researchers said doctors’ claims that myocarditis was common in children who received the vaccine and that the risks of myocarditis outweighed the risk of vaccination were “unfounded.”
But myocarditis “does outweigh the benefits of vaccinations for some ages — in men — and some doses,” said Prasad, citing an article published in the Journal of Medical Ethics.
The paper, which focused on booster mandates at American universities, concluded the mandates were unethical because they could result in greater health risks, like booster-associated myocarditis, than benefits to healthy young adults.
Several other studies have shown either myocarditis deaths across all age groups, or elevated myocardial injury after vaccination.
The researchers also flagged any posts discussing pre-pandemic studies that definitively concluded masks do not prevent the spread of respiratory viral infections. And they deemed as misinformation any post that undermined the role of masks in slowing the spread of the infection and that pointed to rising cases in areas with mask mandates.
But a plethora of studies on mask ineffectiveness emerged during the time the Massachusetts team was conducting its research on physicians and “misinformation.”
There were also reports on “The Foegen effect” — the idea that deep re-inhalation of droplets and virions caught on facemasks might make COVID-19 infection more likely or more severe. German physician Dr. Zacharias Fögen introduced the concept in a study that concluded: “mask use might pose a yet unknown threat to the user instead of protecting them, making mask mandates a debatable epidemiologic intervention.”
“The totality of the evidence to date shows no benefit from community mask wearing,” said Prasad, who pointed to Cochrane’s multiple analyses.
According to the JAMA study, doctors who said the COVID-19 vaccines were ineffective at preventing COVID-19 spread or that the virus originated in a lab in China were propagators of misinformation.
Yet plenty of data show the vaccines did not prevent transmission, and scientists even testified to evidence that COVID-19 could have resulted from controversial gain-of-function research at the Wuhan Institute of Virology.
In the wake of the pandemic, multiple organizations have published guidelines on “medical misinformation” — including YouTube and the American Medical Association (AMA).
Last June, the AMA adopted a new policy to limit medical disinformation, including ensuring that medical licensing boards can take disciplinary action against health professionals who spread health-related disinformation.
In California, however, a judge ruled in January that the state does not have the power to penalize doctors who spread “misinformation” or “disinformation.”
“COVID-19 is a quickly evolving area of science that in many aspects eludes consensus,” the judge decided.
Monica Dutcher is a Maryland-based senior reporter for The Defender.
This article was originally published by The Defender — Children’s Health Defense’s News & Views Website under Creative Commons license CC BY-NC-ND 4.0. Please consider subscribing to The Defender or donating to Children’s Health Defense.
Can You Overdose on Ivermectin? Dr. Pierre Kory’s Answer Will Shock You
The Vigilant Fox | Vigilant News | August 17, 2023
“Of all the harmful misinformation spread over the past couple of years, one of the most disturbing false narratives was targeted at the Nobel-Prize-winning, human medicine ivermectin,” expressed filmmaker Mikki Willis in his ground-breaking documentary titled, Ivermectin: The Truth.
Ivermectin is “one of the safest and most effective medicines of this era. A medicine that, according to the numerous top scientists I’ve interviewed … could have ended the pandemic before it began.”
But Ivermectin is “horse dewormer,” the media said. “It could put you in a coma.” “It can kill you,” pundits warned.
But is this actually true?
Popular podcaster Greg Hunter, AKA USA Watchdog, asked Dr. Pierre Kory, one of the world’s leading experts on Ivermectin, straight-up, “Can I OD (overdose) on Ivermectin if I get two or three times the [standard] dose. Can I kill myself?”
“Let me answer scientifically. So there is a world-famous toxicologist named Jacques Descotes, and he’s French. And two years ago, he was commissioned to do a scoping review of the entire data on the safety of Ivermectin in its history. And his conclusion after doing this comprehensive review is that he does not believe that there has been one single case of anyone dying from an Ivermectin overdose.”

Prof. Jacques Descotes: Image – Academica.edu
“Oh, Lord,” reacted Greg Hunter. “How many pills have been given worldwide? I heard 4 billion, but it must be more than that.”
“Over 4 billion,” Dr. Kory confirmed. “Now, people have died where the deaths were reported as caused by Ivermectin. But when he [Prof. Jacques Descotes] reviewed those cases, he didn’t think those arguments [were] credible.”
Let’s dive deeper into Prof. Descotes’ analysis.
But first, a quick look at his impressive credentials. “Pr. Jacques Descotes, MD, PharmD, PhD, Professor Emeritus, Claude Bernard University of Lyon (France), [is] a world-known toxicologist with a 40-year track [record] as an independent consultant for the pharmaceutical industry as well as an advisor to regulatory bodies worldwide,” BusinessWire wrote.
In March 2021, he conducted a review of Ivermectin’s safety profile based on over 350 articles – plus accessible web sources. Here are his conclusions:
“Ivermectin has been administered orally to hundreds of millions of people throughout the world in the past three decades. The assessment of reported adverse events temporally associated with Ivermectin exposure shows that Ivermectin-induced adverse effects have so far been infrequent and usually mild to moderate.
“It is noteworthy that no deaths have seemingly ever been reported after an accidental or suicidal overdose of Ivermectin. No greater toxicity of Ivermectin has been substantiated in elderly people despite repeated assertions that an ageing blood-brain barrier might lead to increased Ivermectin toxicity level. The positive clinical experience accumulated with Ivermectin administration led many medical experts to break away from early adamant contra-indications in pregnant women. Finally, several national pharmacovigilance networks around the world released information and opinions to ascertain Ivermectin safety in human subjects. So far, there are no critical safety limitations to Ivermectin prescription in current indications.
I also want to point out that no severe adverse event has been reported in dozens of completed or ongoing studies involving thousands of participants worldwide to evaluate the efficacy of Ivermectin against COVID-19.”
“In order to overdose from Ivermectin, you have to take either a hundred or a thousand times the standard dose,” declared Dr. Kory.
“And there have been accidental poisonings where people have taken large amounts. But you know what happens every time? When they take these massive amounts of Ivermectin, it tends to affect them neurologically. They’ll get confused. They might be stumbling — uncoordinated. They go to the hospital, and there’s no treatment required. But within days, the patients return to normal. So, there’s been no life-ending injuries. No deaths reported with Ivermectin. So, that shows you why it’s one of the safest drugs in history, even at massive overdoses.
Greg Hunter’s full interview with Dr. Pierre Kory is available to watch.
Medical Board Chief who wanted Doctors delicensed for ‘misinformation’ in bed with PR firm tied to CDC, Pfizer, Moderna
By Michael Nevradakis, Ph.D. | The Defender | August 18, 2023
The head of a national medical organization who publicly called for doctors to lose their licenses unless they supported government narratives on COVID-19 treatments and vaccines concealed his relationship with a public relations firm whose client list also included Pfizer, Moderna and the Centers for Disease Control and Prevention (CDC).
Dr. Richard Baron, president and CEO of the American Board of Internal Medicine (ABIM) is a client of Weber Shandwick, investigative journalist Paul D. Thacker reported on Wednesday.
In late 2021, Baron publicly pushed for doctors who spread “misinformation” about COVID-19 and the vaccines to lose their license and certification. Baron said then that “putting out flagrant misinformation is unethical and dangerous during a pandemic.”
Weber, the world’s second-largest PR firm, has branded its team as “misinformation and disinformation” experts and says it provides clients with services to help manage any perceived threats posed by spreaders of such information.
The firm has organized conference panels on “medical misinformation” in which Baron participated.
Last year, Baron partnered with Weber Shandwick to propose a South by Southwest (SXSW) panel titled “When Doctors Prescribe Misinformation.” The proposal was subsequently accepted and the panel took place at SXSW in Austin, Texas, on March 13.
According to Thacker, “Weber Shandwick’s panel featuring Dr. Baron has been widely promoted by the PR firm’s employees,” including Sarah Mahoney, executive vice president, Healthcare Communications, Strategy & Planning for Weber Shandwick, who in a LinkedIn post, wrote she “can’t think of a more important topic right now.”
The CDC’s National Center for Immunization and Respiratory Diseases (NCIRD) in September 2020 awarded Weber a $50 million contract “to promote the vaccination of children, pregnant women and those at risk for flu and increase the general acceptance and use of vaccines,” according to the PR firm’s website.
Under the contract, Weber employees were embedded in the NCIRD to “communicate the risks and recommended actions for outbreaks and convey vaccine recommendations to healthcare providers,” according to Thacker.
Medicine has always been ‘in bed with Big Pharma’
Several doctors have faced disciplinary action by state medical boards for allegedly spreading “misinformation.” One of them is internist and biological warfare epidemiologist Dr. Meryl Nass, a member of Children Health Defense’s scientific advisory committee.
Nass on Thursday sued the Maine Board of Licensure, which suspended her license in January 2022.
The board’s suspension arose from its adoption of a position statement promulgated by the Federation of State Medical Boards (FSMB) threatening physicians “who generate and spread COVID-19 vaccine misinformation” with suspension or revocation of their medical license.
In 2021, ABIM and FSMB collaborated to create the statement used to discipline Nass.
Nass told The Defender that in order to get certified by organizations like ABIM, there are several requirements, primarily related to demonstrating competence in one’s field of specialization, including completing a residency, being certified by the residency director, and paying for and passing the board examinations.
Nass told The Defender that in order to get certified by organizations like ABIM, there are several requirements. She explained:
“You complete a medical residency in your field of specialization. Your residency director certifies your competence and moral character, and you must pay for and pass your board examination to demonstrate your command of your specialty.
“When you’ve paid them for board certification and successfully completed all the requirements, how can they change the rules 20 or 50 years later and say, ‘we’re going to decertify you now because we don’t like your viewpoint?’
“There was nothing in any documentation from the Board of Internal Medicine about misinformation, or any other standards that the board can impose apart from competency to practice when it issued certifications.”
Dr. Richard Eggleston, a retired ophthalmologist in Clarkston, Washington, also faces disciplinary action — by the Washington Medical Commission — arising from articles he published in a local newspaper in 2021, questioning the official narrative and medical advice related to COVID-19.
Doctors aren’t being targeted exclusively for spreading “misinformation” — some, like Dr. Mary Kelly Sutton, an integrative physician, were targeted for their less-than-100% support for COVID-19 vaccines.
Last month, the Massachusetts medical board revoked Sutton’s medical license, claiming she improperly exempted eight children from required school vaccinations. This came a year after California also revoked Sutton’s medical license.
Sutton told The Defender, “The voice of medicine today is determined by the marketing wisdom of Madison Avenue, not by what is sound information from scientific research.”
Sutton said the whole practice of medicine rests on sharing and providing information necessary for informed decisions and consent. When specialty boards issue vague accusations, they engage in “harassment,” and an “egregious overreach of power” and are obstructing the practice of medicine.
A California law aimed at punishing doctors for providing “misinformation” to their patients is now in “legal limbo” following conflicting rulings in state courts earlier this year, which could affect Sutton’s and other California doctors’ cases going through the courts.
This trail of evidence demonstrates medical boards are not simply acting on their own authority but in collusion with state governments, federal agencies and private companies.
“There’s no one who is a ‘misinformation’ or ‘disinformation’ expert whose opinion does not align with the government and with the corporations,” Thacker told The Defender. “That’s what makes them an ‘expert.’”
“What’s always been true is that medicine has been in bed with Big Pharma,” he added. “It’s now becoming a lot more transparent. These relationships are much more transparent.”
‘A very political attempt to shut down people from having alternative viewpoints’
According to Thacker, Baron began his “crusade for the biopharmaceutical industry” in September 2021. In a post for ABIM’s blog, Baron said, “I want to state unequivocally that ABIM can and does take action, independent of state licensing boards, to remove certification from physicians for unprofessional and unethical behavior.”
For Thacker, Baron’s concern about “misinformation” was first triggered when physicians spoke out against COVID-19 vaccine safety, efficacy and side effects. “These are the same concerns held by Weber Shandwick, who Pfizer and Moderna are paying big buck[s] to promote their vaccines,” he said.
“Baron’s relationship with Weber Shandwick was not disclosed” by JAMA, Thacker said, “nor in an accompanying viewpoint Baron wrote for JAMA.”
After an inquiry by Thacker, JAMA’s editor-in-chief, Kirsten Bibbins-Domingo, said, “We initiated our internal investigation earlier this week, in accordance with our standard processes for allegations of non-disclosure of conflicts.”
“It is notable that Baron has done his best to mislead the public and other physicians about what he is doing,” Nass said. “He claims the ABIM is trying to ‘protect the legitimacy of medical expertise’ rather than censoring viewpoints it does not like.”
Nass said Baron “conjures up examples of what the board might censure.” She pointed to a Feb. 23, 2023, New England Journal of Medicine (NEJM) article Baron co-authored with attorney Carl J. Coleman, which stated:
“When a licensed physician insists that viruses don’t cause disease or that COVID-19 vaccines magnetize people or connect them to cell towers, professional bodies must be able to take action in support of fact and evidence based practice.”
“Yet this is a fabrication,” Nass said, adding:
“Instead, Dr. Baron, who earns about $1.2 million yearly from the ABIM and the ABIM Foundation, has decertified Drs. Peter McCullough, Paul Marik and Pierre Kory — all highly celebrated, published and esteemed doctors in their fields.
“None of them have uttered any mumbo-jumbo about cell towers, magnetism or a non-viral etiology for COVID-19. All have had their board certifications revoked for the viewpoints they expressed — viewpoints that are supported by a preponderance of the medical literature.”
In a January 2022 article for Health Affairs, Coleman wrote, “Licensing boards are state agencies subject to the First Amendment, and as such they are limited in their ability to penalize physicians based on the content of their speech.”
Yet, a 2022 NEJM article co-authored by Baron argued that while “Differences of opinion in medicine are necessary for progress … there are some opinions that have been so thoroughly repudiated by existing evidence as to be considered definitively wrong.”
‘All this money is sloshing around now for misinformation research’
According to Thacker, “PR firms are now moving into the ‘disinformation’ space after decades of deceit on behalf of multiple industries,” with Weber Shandwick having “expanded into the disinformation space in late 2021,” promoting tactics that help “brands combat misinformation and disinformation that may implicate them.”
Speaking to Thacker, Dr. Aaron Kheriaty, director of bioethics at the Ethics and Public Policy Center, said, “The ABIM is clearly part of this ‘medical misinformation’ push, which is orchestrated by pharmaceutical companies and their PR allies” and which serves “the interests of Big Pharma.”
Remarking on the presence of a “medical misinformation” panel at SXSW, long known as a music, film and technology festival, Thacker told The Defender, “Anyone and everyone is getting involved in ‘misinformation’ and ‘disinformation.’”
“Baron has given a TED Talk, for instance. Why is TED Talks involved in this?” he asked.
In 2019 Baron delivered a talk at TEDx Chicago titled, “Please Don’t Confuse Your Google Search with My Medical Degree.”
For Thacker, the answer relates to financial interests. “All this money is sloshing around now for ‘misinformation’ research. Anyone can hop up and down saying ‘I’m an expert on misinformation and disinformation, get me a grant, get me on a panel,’” he said.
Weber embedded staffers within the CDC while representing Pfizer, Moderna
Thacker wrote that prior to discovering Baron’s ties to Weber Shandwick, he had confirmed the PR firm’s ties to COVID-19 vaccine manufacturers Pfizer and Moderna.
These ties did not prevent the CDC from awarding the $50 million contract to Weber Shandwick in September 2020 to push vaccines. The Daily Mail subsequently reported Thacker’s findings.
Medical Marketing and Media reported “Weber’s duties include providing 10 on-site health communications staffers, seven health comms specialists, two health research specialists and one social media specialist” to NCIRD, as well as “generating story ideas, distributing articles and conducting outreach to news, media and entertainment organizations.”
In October 2020, a blog post by Stacy Montejo, senior vice president at Weber Shandwick, disclosed that Pfizer is one of the firm’s clients. A month later, with Moderna’s COVID-19 vaccine awaiting Emergency Use Authorization, the company hired Weber Shandwick to handle the vaccine’s publicity, according to PR Week.
Such relationships have continued to the present. In June, Moderna announced a new communications strategy “to further educate the world about Moderna’s mRNA technology and its promise to transform the future of human health.”
The effort is led by Laura Schoen, “who is sometimes titled president of global healthcare at Weber Shandwick, and other times chief healthcare officer at IPG DXTRA, Weber Shandwick’s parent company,” Thacker wrote.
Lucy Rieck, a Weber Shandwick employee, previously publicly tweeted support for a panel Moderna proposed for this year’s SXSW, titled “COVID, Monkeypox, Disease X, What’s Next?” That proposal does not appear to have been accepted for presentation.
Conflicts of interest between Weber Shandwick, the CDC and NCIRD, and Pfizer and Moderna do not appear to have been disclosed.
In October 2022, Sen. Rand Paul (R-Ky.) sent a letter to the CDC inquiring about its relationship with Weber Shandwick and requesting “information regarding the nature of Weber’s work for the NCIRD.” It’s unclear whether the CDC complied with the request.
Todd S. Richardson, one of the attorneys representing Eggleston, told The Defender “While it is certainly understandable that governmental agencies will hire PR firms to help them get their message out … it becomes of real concern to me when those agencies, or people working within the agencies, try to silence those who disagree.”
According to Thacker, the web of relationships between Weber Shandwick doesn’t just extend to Big Pharma companies, the CDC and its agencies, or to doctors such as Baron. Academics such as Brown University’s Claire Wardle, Ph.D., a key figure in the “misinformation research” space, have participated in some of the firm’s events.
Wardle, a professor of the practice of Health Services, Policy and Practice at Brown University who has no scientific or medical credentials, participated in an online meeting organized by Weber Shandwick in October 2020 to discuss “election misinformation.”
Subsequently, Wardle played a key advisory role in the Biden administration, federal agencies, social media platforms and Ivy League institutions as they sought to censor content that ran counter to the government’s COVID-19 narrative.
According to Thacker, she “helped organize many of today’s campus disinformation groups … with funding from Google” and later sent Twitter a report aimed at countering the “growing threat of disinformation to trust in COVID-19 vaccines.”
Thacker said the biopharmaceutical industry is “the smartest at putting out disinformation. What other industry has bought off the medical community and the science community?” he asked. “They bought off the researchers, the government, the academic journals.”
Thacker said he believes much of what is labeled “misinformation” in medicine and academic research “is really just corporate PR,” and that “Congress needs to take a harder look at funding for ‘misinformation research.’“
Michael Nevradakis, Ph.D., based in Athens, Greece, is a senior reporter for The Defender and part of the rotation of hosts for CHD.TV’s “Good Morning CHD.”
This article was originally published by The Defender — Children’s Health Defense’s News & Views Website under Creative Commons license CC BY-NC-ND 4.0. Please consider subscribing to The Defender or donating to Children’s Health Defense.
Dr. Meryl Nass sues Maine Medical Board over suspension, alleges Board violated her first amendment rights
By Brenda Baletti, Ph.D. | The Defender | August 17, 2023
Dr. Meryl Nass today filed suit against the Maine Board of Licensure in Medicine and its individual members, alleging the board violated her First Amendment rights and her rights under the Maine Constitution.
The complaint alleges the board engaged in retaliatory conduct against Nass, a practicing internal medicine physician and member of the Children’s Health Defense (CHD) scientific advisory board, when the board suspended her medical license for publicly expressing her dissenting views on official COVID-19 policies, the COVID-19 vaccine and alternative treatments.
“Because she was outspoken, the board targeted Dr. Nass as someone to silence,” her attorney, Gene Libby told The Defender.
In fall 2021, the board issued a position statement, quoted in the complaint, stating that licensees could face disciplinary action if they “generate and spread COVID-19 vaccine misinformation or disinformation.”
In October 2021, soon after the statement was issued, the board received a complaint alleging Nass was spreading misinformation online and soon after launched an investigation.
The board suspended Nass’ medical license on Jan. 12, 2022, without a hearing, accusing her of engaging in “unprofessional conduct” by spreading “misinformation about COVID-19.”
It also accused her of improperly prescribing hydroxychloroquine and ivermectin for three patients for off-label uses of those drugs.
The board suspended Nass’ license and ordered a neuropsychological evaluation, implying she was mentally impaired or a substance abuser and incompetent to practice medicine.
“There were no grounds to order a mental health examination,” Libby said. “That was simply a means to communicate to the public that there was something wrong with Dr. Nass, to discredit her and tarnish her reputation.”
After Nass moved to have the board dismiss its complaint against her, alleging First Amendment violations, the board on Sept. 26, 2022, withdrew its accusations of “misinformation”, just prior to her first hearing date, Oct. 11, 2022.
The board’s case now rests on Nass’ alleged non-adherence to the medical “standard of care” as it pertained to ivermectin and hydroxychloroquine for treating COVID-19 and on the alleged “record-keeping” issues.
Nass told The Defender :
“The two primary complaints against me were that my statements were misleading and that I was prescribing drugs off-label. My speech — which I should note, was not simply opinion, it was an educated opinion developed after consulting the medical literature — is protected by the First Amendment.
“And prescribing drugs off-label is a perfectly legal thing to do, as explicitly stated on the FDA [U.S. Food and Drug Administration] website. Somewhere between 20-50% of drugs are prescribed off-label. The lawyers on the board staff know all of this. It’s their job to know the law with respect to medicine.
“They didn’t do this because they thought I had committed some kind of violation. They did it because they thought I’m older and I wouldn’t have the money to challenge them and so they could get away with it — they thought they could turn me into a poster child to scare all the doctors in the country.
“It is part of this broader attempt by the U.S. government and governments across the world to criminalize dissent by criminalizing so-called ‘misinformation.’”
Libby said the remaining allegations against Dr. Nass “are simply a pretext to discipline her. Because now, from an institutional standpoint, the board has to do something. She’s been under suspension for 19 months, which is the longest suspension that I’m aware of for any physician in the state.”
The board refused to schedule hearings on Nass’ suspension on consecutive days. Instead, it has held one day of hearings every other month. There have been six days of hearings so far over 10 months — and Nass’ license has been suspended the entire time.
“This is fundamentally unfair to Dr. Nass, but she’s within the grip of an institution that doesn’t want her speaking out,” Libby said.
In her lawsuit, Nass alleges the board and its members used their power to “crush dissenting views and chill disfavored speech.”
Nass is asking the court for declaratory relief, for an injunction to stop the board from continuing to retaliate against her and for monetary damages and legal fees.
CHD is providing financial and legal resources to Nass’ Maine-based legal team.
CHD President Mary Holland told The Defender :
“CHD is proud to support Dr. Nass’ lawsuit against the Maine medical board and its individual members.
“The board and its members have deprived Dr. Nass of her license and livelihood for over a year with no basis whatsoever. This kind of censorship, intimidation and punishment of doctors of conscience must stop.
“People need independent, thoughtful, caring physicians like Dr. Nass to be honored, not hounded as the board has done.
“I am pleased to see this case move forward in the courts in the interests of justice, for Dr. Nass, her patients and the broader society.”
Board provided resources to ‘combat spread of vaccine misinformation’
The Maine board’s Fall 2021 position statement expressed its support for a statement by the Federation of State Medical Boards (FSMB) — a private organization with no regulatory authority — which threatened physicians “who generate and spread COVID-19 vaccine misinformation” with suspension or revocation of their medical license.
According to the statement, physicians have a high degree of public trust and therefore a responsibility to “share information that is factual, scientifically grounded and consensus-driven for the betterment of public health.”
The Maine board’s statement endorsed the FSMB statement, encouraged physicians to address misinformation when encountered, directed physicians to use circulated materials from the American Medical Association (AMA) and said that questioning the COVID-19 vaccine qualifies as “misinformation,” according to the complaint.
The AMA materials provide scripts, talking points and strategies for “combating the spread of vaccine misinformation.”
The Maine board’s chair, Dr. Maroulla Gleaton, is also an FSMB director.
Nass is a widely recognized expert on the anthrax vaccine and biological warfare. She testified before Congress six times and was quoted in major media outlets including The New York Times, The Washington Post, the Los Angeles Times and the Chicago Tribune.
She has also been a prominent critic of governmental handling of the COVID-19 pandemic, the suppression of effective treatments such as ivermectin and hydroxychloroquine and the safety and risks of the vaccine — all topics she has discussed in her Substack, on the radio, in interviews and elsewhere.
But, the complaint notes, her positions have been in conflict with those asserted in the position statement and the resources it highlights as “supporting the fight against COVID-19 misinformation.”
This was merely an attempt by the board to justify its decision to immediately suspend Nass and to intimidate her, the complaint alleges.
Board’s only concern was ‘silencing’ Nass and ‘branding her as crazy’
When Nass questioned the board’s authority to investigate a complaint unrelated to the practice of medicine and instead “focused entirely on a statement made in her private life,” the board responded, on Oct. 14, 2021, that she was engaged in “alleged unprofessional conduct” by provisioning “misleading and/or inaccurate” information.
In the January board meeting where the board decided to suspend her license, the conversation focused on Nass’ “unprofessional conduct due to the spreading of misinformation about COVID-19.”
The board also cited three matters related to treating patients, alleging Nass improperly diagnosed a patient “over the phone,” that she had provided misinformation to a pharmacist about why she was prescribing ivermectin for a patient, and that she had improperly issued another prescription.
On Sept. 7, 2022, Nass moved to dismiss the complaint, alleging the board was violating her First Amendment rights.
The board responded by withdrawing all charges based on her speech, retaining only the charges related to the treatment of three patients.
Libby told The Defender that through the entire investigation and hearings, the board never even spoke to the three patients. It did not inform them their medical records had been subpoenaed, or ask them about their treatment by Dr. Nass.
“Yet the remaining disciplinary charges are all predicated on Dr. Nass’ consultation with and advice to these patients.”
Libby called the patients to testify in Nass’ hearings. They all made “glowing comments” about her availability, her medical advice and her handling of their cases and expressed anger that Nass was being targeted by the board for their cases.
Libby said he interpreted this to indicate the board’s singular focus was not to ensure patient well-being, but rather “silencing Dr. Nass and attempting to brand her as crazy.”
According to the complaint, the board’s animus against Nass is also demonstrated by the fact that it is flouting its own rules for selecting and paying expert witnesses.
Board guidelines stipulate that witnesses can be paid a maximum of $125/hour for preparation and $175/hour for testimony and that the witnesses should have the same specialty as the practitioner in question and be licensed to practice in Maine.
But the board is paying Dr. Jeremy Faust, an emergency room physician from Brigham & Women’s Hospital in Boston, $500/hour to testify.
And board member Gleaton, who has conflicts of interest because of her position as FSMB director and has acted in openly mocking ways, has refused to recuse herself.
The next medical board hearing is set for mid-September.
But in the meantime, Libby said “The actions of the board are so outrageous, they need to be acted on legally.”
Brenda Baletti Ph.D. is a reporter for The Defender. She wrote and taught about capitalism and politics for 10 years in the writing program at Duke University. She holds a Ph.D. in human geography from the University of North Carolina at Chapel Hill and a master’s from the University of Texas at Austin.
This article was originally published by The Defender — Children’s Health Defense’s News & Views Website under Creative Commons license CC BY-NC-ND 4.0. Please consider subscribing to The Defender or donating to Children’s Health Defense.
The WHO’s Proposed Amendments Will Increase Man-Made Pandemics
By Meryl Nass | Brownstone Institute | August 17, 2023
This report is designed to help readers think about some big topics: how to really prevent pandemics and biological warfare, how to assess proposals by the WHO and its members for preventing and responding to pandemics, and whether we can rely on our health officials to navigate these areas in ways that make sense and will help their populations. We start with a history of biological arms control and rapidly move to the COVID pandemic, eventually arriving at plans to protect the future.
Weapons of Mass Destruction: Chem/Bio
Traditionally, the Weapons of Mass Destruction (WMD) have been labelled Chemical, Biological, Radiologic, and Nuclear (CBRN).
The people of the world don’t want them used on us—for they are cheap ways to kill and maim large numbers of people quickly. And so international treaties were created to try to prevent their development (only in the later treaties) and use (in all the biological arms control treaties). First was the Geneva Protocol of 1925, following the use of poison gases and limited biological weapons in World War I, banning the use of biological and chemical weapons in war. The US and many nations signed it, but it took 50 years for the US to ratify it, and during those 50 years the US asserted it was not bound by the treaty.
The US used both biological and chemical weapons during those 50 years. The US almost certainly used biological weapons in the Korean War (see this, this, this and this) and perhaps used both in Vietnam, which experienced an odd outbreak of plague during the war. The use of napalm, white phosphorus, agent orange (with its dioxin excipient causing massive numbers of birth defects and other tragedies) and probably other chemical weapons like BZ (a hallucinogen/incapacitant) led to much pushback, especially since we had signed the Geneva Protocol and we were supposed to be a civilized nation.
In 1968 and 1969, two important books were published that had a great influence on the American psyche regarding our massive stockpiling and use of these agents. The first book, written by a young Seymour Hersh about the US chemical and biological warfare program, was titled Chemical and Biological Warfare; America’s Hidden Arsenal. In 1969 Congressman Richard D. McCarthy, a former newspaperman from Buffalo, NY wrote the book The Ultimate Folly: War by Pestilence, Asphyxiation and Defoliation about the US production and use of chemical and biological weapons. Prof. Matthew Meselson’s review of the book noted,
Our operation, “Flying Ranch Hand,” has sprayed anti-plant chemicals over an area almost the size of the state of Massachusetts, over 10 per cent of its cropland. “Ranch Hand” no longer has much to do with the official justification of preventing ambush. Rather, it has become a kind of environmental warfare, devastating vast tracts of forest in order to facilitate our aerial reconnaissance. Our use of “super tear gas” (it is also a powerful lung irritant) has escalated from the originally announced purpose of saving lives in “riot control-like situations” to the full-scale combat use of gas artillery shells, gas rockets and gas bombs to enhance the killing power of conventional high explosive and flame weapons. Fourteen million pounds have been used thus far, enough to cover all of Vietnam with a field effective concentration. Many nations, including some of our own allies have expressed the opinion that this kind of gas warfare violates the Geneva Protocol, a view shared by McCarthy.
A Biological Weapons Convention
Amid great pushback over US conduct in Vietnam, and seeking to burnish his presidency, President Nixon announced to the world in November 1969 that the US was going to end its biowarfare program (but not the chemical program). Following pointed reminders that Nixon had not eschewed the use of toxins, in February 1970 Nixon announced we would also get rid of our toxin weapons, which included snake, snail, frog, fish, bacterial, and fungal toxins that could be used for assassinations and other purposes.
It has been claimed that these declarations resulted from careful calculations that the US was far ahead technically of most other nations in its chemical and nuclear weapons. But biological weapons were considered the “poor man’s atomic bomb” and required much less sophistication to produce. Therefore, the US was not far ahead in the biological weapons arena. By banning this class of weapon, the US would gain strategically.
Nixon told the world that the US would initiate an international treaty to prevent the use of these weapons ever again. And we did so: the 1972 Convention on the Prohibition of the Development, Production and Stockpiling of Bacteriological (Biological) and Toxin Weapons and on their Destruction, or Biological Weapons Convention (BWC) for short, which entered into force in 1975.
But in 1973 genetic engineering (recombinant DNA) was discovered by Americans Herbert Boyer and Stanley Cohen, which changed the biological warfare calculus. Now the US had regained a technological advantage for this type of endeavor.
The Biological Weapons Convention established conferences to be held every 5 years to strengthen the treaty. The expectation was that these would add a method to call for ‘challenge inspections’ to prevent nations from cheating and would add sanctions (punishments) if nations failed to comply with the treaty. However, since 1991 the US has consistently blocked the addition of protocols that would have an impact on cheating. By now, everyone accepts that cheating occurs and is likely widespread.
A leak in an anthrax production facility in Sverdlovsk, USSR in 1979 caused the deaths of about 60 people. While the USSR tried a sloppy cover-up, blaming contaminated black market meat, this was a clear BWC violation to all those knowledgeable about anthrax.
US experiments with anthrax production during the Clinton administration, detailed by Judith Miller et al. in the 2001 book Germs, were also thought by experts to have transgressed the BWC.
It has taken over 40 years, but in 2022 all declared stocks of chemical weapons had been destroyed by the USA, by Russia, and the other 193 member nation signatories. The chemical weapons convention does include provisions for surprise inspections and sanctions.
Pandemics and Biological Warfare Receive Funding from Same Stream
It is now 2023, and during the 48 years the Biological Weapons Convention has been in force the wall it was supposed to build against the development, production, and use of biological weapons has been steadily eroded. Meanwhile, especially since the 2001 anthrax letters, nations (with the US at the forefront) have been building up their “biodefense” and “pandemic preparedness” capacities.
Under the guise of preparing their defenses against biowarfare and pandemics, nations have conducted “dual-use” (both offensive and defensive) research and development, which has led to the creation of more deadly and more transmissible microorganisms. And employing new verbiage to shield this effort from scrutiny, biological warfare research was renamed as “gain-of-function” research.
Gain-of-function is a euphemism for biological warfare research aka germ warfare research. It is so risky that funding it was banned by the US government (but only for SARS coronaviruses and avian flu viruses) in 2014 after a public outcry from hundreds of scientists. Then in 2017 Drs. Tony Fauci and Francis Collins lifted the moratorium, with no real safeguards in place. Fauci and Collins even had the temerity to publish their opinion that the risk from this gain-of-function research was ‘worth it.’
What does gain-of-function actually mean? It means that scientists are able to use a variety of techniques to turn ordinary or pathogenic viruses and bacteria into biological weapons. The research is justified by the claim that scientists can get out ahead of nature and predict what might be a future pandemic threat, or what another nation might use as a bioweapon. The functions gained by the viruses or other microorganisms to turn them into biological warfare agents consist of two categories: enhanced transmission or enhanced pathogenicity (illness severity).
1) improved transmissibility may result from:
a) needing fewer viral or bacterial copies to cause infection,
b) causing the generation of higher viral or bacterial titers,
c) a new mode of spread, such as adding airborne transmission to a virus that previously only spread through bodily fluids,
d) expanded range of susceptible organs (aka tissue tropism); for example, not only respiratory secretions but also urine or stool might transmit the virus, which was found in SARS-CoV-2,
e) expanded host range; for example, instead of infecting bats, the virus is passaged through humanized mice and thus acclimated to the human ACE-2 receptor, which was found in SARS-CoV-2,
f) improved cellular entry; for example, by adding a furin cleavage site, which was found in SARS-CoV-2,
2) increased pathogenicity, so instead of causing a milder illness, the pathogen would be made to cause severe illness or death, using various methods. SARS-CoV-2 had unusual homologies (identical short segments) to human tissues and the HIV virus, which may have caused or contributed to the late autoimmune stage of illness, impaired immune response and ‘long COVID.’
Funding for (Natural) Pandemics, Including Yearly Influenza, was Lumped Together with Biological Defense Funding
Perhaps the comingling of funding was designed to make it harder for Congress and the public to understand what was being funded, and how much taxpayer funding was going to gain-of-function work, which might lead them to question why it was being done at all, given its prohibition in the Biological Weapons Convention, and additional questions about its value. Former CDC Director Robert Redfield, a physician and virologist, told Congress in March of 2023 that gain-of-function research had not resulted in a single beneficial drug, vaccine, or therapeutic to his knowledge.
Nonprofits and universities like EcoHealth Alliance and its affiliated University of California, Davis veterinary school were used as intermediaries to obscure the fact that US taxpayers were supporting scientists in dozens of foreign countries, including China, for research that included gain-of-function work on coronaviruses.
Perhaps to keep the lucrative funding going, fears about pandemics have been deliberately amplified over the past several decades. The federal government has been spending huge sums on pandemic preparedness over the past 20 years, routing it through many federal and state agencies. President Biden’s proposed 2024 budget requested “$20 billion in mandatory funding across DHHS for pandemic preparedness” while the DHS, DOD, and the State Department have additional budgets for pandemic preparedness for both domestic and international spending.
Although the 20th century experienced only 3 significant pandemics (the Spanish flu of 1918-19 and 2 influenza pandemics in 1957 and 1968) the mass media have presented us with almost non-stop pandemics during the 21st century: SARS-1 (2002-3), avian flu (2004-on), swine flu (2009-10), Ebola (2014, 2018-19), Zika (2016), COVID (2020-2023), and monkeypox (2022-23). And we are incessantly told that more are coming, and that they are likely to be worse.
We have been assaulted with warnings and threats for over 2 decades to induce a deep fear of infectious diseases. It seems to have worked.
The genomes of both SARS-CoV-2 and the 2022 monkeypox (MPOX) virus lead to suspicion that both were bioengineered pathogens originating in laboratories. The group of virologists assembled by Drs. Fauci and Farrar identified 6 unusual (probably lab-derived) parts of the SARS-CoV-2 genome as early as February 1, 2020 and more have been suggested subsequently.
I do not know if these viruses leaked accidentally or were deliberately released, but I am leaning toward the conclusion that both were deliberately released, based on the locations where they first appeared, the well-orchestrated but faked videos rolled out by the mass media for COVID, and the illogical and harmful official responses to each. In neither case was the public given accurate information about the infections’ severity or treatments, and the responses by Western governments never made scientific sense. Why wouldn’t you treat cases early, the way doctors treat everything else? It seemed that our governments were trading on the fact that few people knew enough about viruses and therapeutics to make independent assessments about the information they were being fed.
Yet by August 2021, there was no corresponding course correction. Instead, the federal government doubled down, imposing vaccine mandates on 100 million Americans in September 2021 in spite of ‘the science.’ There has been no accurate statement yet from any federal agency about the lack of utility of masking for an airborne virus (which is probably why the US government and WHO delayed acknowledging airborne spread by COVID for 18 months), the lack of efficacy of social distancing for an airborne virus, and the risks and poor efficacy of 2 dangerous oral drugs (paxlovid and molnupiravir) purchased by the US government for COVID treatment, even without a doctor’s prescription.
Never have any federal agencies acknowledged the truth about the COVID vaccines’ safety and efficacy. Instead, the CDC turns definitional and statistical cartwheels so it can continue to claim they are “safe and effective.” Even worse, with all that we know, a third generation COVID vaccine is to be rolled out for this fall and the FDA has announced that yearly boosters are planned.
All this goes on, even a year after we learned (with continuing corroborations) that children and working age adults are dying at rates 25 percent or more above the expected averages, and the vascular side effects of vaccination are the only reasonable explanation.
Maiming with Myocarditis
Both of the two US monkeypox/smallpox vaccines (Jynneos and ACAM2000) are known to cause myocarditis, as do all 3 COVID vaccines currently available in the US: the Pfizer and Moderna COVID-19 mRNA vaccines and the Novavax vaccine. The Novavax vaccine was first associated with myocarditis during its clinical trial, but this was downplayed and it was authorized and rolled out anyway, intended for those who refused the mRNA vaccines due to the use of fetal tissue in their manufacture.
Here is what the FDA’s reviewers wrote about the cardiac side effects noted in the Jynneos clinical trials:
Up to 18.4% of subjects in 2 studies developed post-vaccination elevation of troponin [a cardiac muscle enzyme signifying cardiac damage]. However, all of these troponin elevations were asymptomatic and without a clinically associated event or other sign of myopericarditis. p. 198
The applicant has committed to conduct an observational, post-marketing study as part of their routine PVP. The sponsor will collect data on cardiac events that occur and are assessed as a routine part of medical care. p. 200
In other words, while the only way to cause an elevated troponin level is to break down cardiac muscle cells, the FDA did not require a specific study to evaluate the extent of cardiac damage that might be caused by Jynneos when it issued its 2019 license. How frequently does myocarditis occur after these vaccines? If you use elevated cardiac enzymes as your marker, ACAM2000 caused this in one in thirty people receiving it for the first time. If you use other measures like abnormal cardiac MRI or echo, according to the CDC it occurs in one in 175 vaccinees. I have not seen a study with rates of myocarditis for Jynneos, but there was an unspecified elevation of cardiac enzymes in 10 percent and 18 percent of Jynneos recipients in two unpublished prelicensure studies available on the FDA website. My guess for the mRNA COVID vaccines is that they cause myocarditis in this general range, the vast majority of which remain undiagnosed and probably asymptomatic.
Why would our governments push 5 separate vaccines all known to cause myocarditis on young males who have been at extremely low risk from COVID, and who simply get a few pimples for 1-4 weeks from monkeypox unless they are immunocompromised? It’s an important question. It does not make medical sense. Especially when the vaccine probably does not work—Jynneos didn’t prevent infection in the monkeys in whom it was tested nor did it do well in people. And the CDC has failed to publish its trial of Jynneos vaccine in the ~1,600 Congolese healthcare workers on whom the CDC tested it for efficacy and safety in 2017. The CDC made the mistake of announcing the trial, and posting it to clinicaltrials.gov as required, but has not informed its advisory committee that reviewed the vaccine, nor the public, of the trial’s results.
There can be no question about it: our health agencies are guilty of malfeasance, misrepresentation, and deliberate infliction of harm on their own populations. The health agencies first incited terror with apocalyptic predictions, then demanded patients be medically neglected, and finally enforced vaccinations and treatments that were tantamount to malpractice.
COVID Vaccines: The Chicken or the Egg?
The health authorities could have just been ignorant — that could possibly explain the first few months of the COVID vaccines’ rollout. But once they figured out, and even announced in August 2021 that the vaccines did not prevent catching COVID or transmitting it, why did our health authorities still push COVID vaccines on low-risk populations who were clearly at greater risk from a vaccine side effect than from COVID? Particularly as time went on and newer variants were less and less virulent?
Once you acknowledge these basic facts, you realize that maybe the vaccines were not made for the pandemic, and instead the pandemic was made to roll out the vaccines. While we cannot be certain, we should at least be suspicious. And the fact that the US contracted for 10 doses per person (review purchases here, here, here, here and here) and so did the European Union (here and here) and Canada should make us even more suspicious – there is no justification for agreeing to purchase so many doses for vaccines at a time when the vaccines’ ability to prevent infection and transmission was questionable, and its safety suspect or worrying.
Why would governments want ten doses per person? Three maybe. But ten? Even if yearly boosters were expected, there was no reason to sign contracts for enough vaccine for the next nine years for a rapidly mutating virus. Australia bought 8 doses per person. By December 20, 2020 New Zealand had secured triple the vaccines it needed, and offered to share some with nearby nations. No one has come forward to explain the reason for these excessive purchases.
Furthermore, you don’t need a vaccine passport (aka digital ID, aka a phone app that in Europe included a mechanism for an electronic payments system) unless you are giving out regular boosters. Were the vaccines conceived of as the means for putting our vaccinations, health records, official documents–and most importantly, shifting our financial transactions online, all managed on a phone app? This would be an attack on privacy as well as the enabling step to a social credit system in the West. Interestingly, vaccine passports were already being planned for the European Union by 2018.
A Pandemic Treaty and Amendments: Brought to You by the Same People who Mismanaged the Past 3 Years, to Save us from Themselves?
The same US and other governments and the WHO that imposed draconian measures on citizens to force us to be vaccinated and take dangerous, expensive, experimental drugs, withheld effective treatments, and refused to tell us that most people who required ICU care for COVID were vitamin D-deficient and that taking vitamin D would lessen COVID’s severity–decided in 2021 we suddenly needed an international pandemic treaty. Why? To prevent and ameliorate future pandemics or biological warfare events… so we would not suffer again as we did with the COVID pandemic, they insisted. The WHO would manage it.
To paraphrase Ronald Reagan, the words, “I’m from the WHO, and I’m here to help” should be the most terrifying words in the English language after the COVID fiasco.
What the WHO and our governments conveniently failed to mention is that we suffered so badly because of their medical mismanagement and our governments’ merciless economic shutdowns and mismanagement. According to the World Bank, an additional 70 million people were forced into extreme poverty in 2020 alone. This was due to policies issued by our nations’ rulers, their elite advisers and the World Health Organization, which came out with guidance to shut down economic activity that most nations adopted without question. The WHO is acutely aware of the consequences of economic lockdowns, having published the following:
Malnutrition persisted in all its forms, with children paying a high price: in 2020, over 149 million under-fives are estimated to have been stunted, or too short for their age; more than 45 million – wasted, or too thin for their height…
Starvation may have killed more people than COVID, and they were disproportionately the youngest, rather than the oldest. Yet the WHO prattles on about equity, diversity, and solidarity—having itself caused the worst food crisis in our lifetime, which was not due to nature but was man-made.
How can anyone take seriously claims by the same officials who mishandled COVID that they want to spare us from another medical and economic disaster–by using the same strategies they applied to COVID, after they masterminded the last disaster? And the fact that no governments or health officials have admitted their errors should convince us never to let them manage anything ever again. Why would we let them draw up an international treaty and new amendments to the existing International Health Regulations (IHR) that will bind our governments to obey the WHO’s dictates forever?
Those dictates, by the way, include vaccine development at breakneck speed, the power to enforce which drugs we will be directed to use, and which drugs will be prohibited, and the requirement to monitor media for “misinformation” and impose censorship so that only the WHO’s public health narrative will be conveyed to the public.
The WHO’s Pandemic Treaty Draft Requires the Sharing of Potential Pandemic Pathogens. This is a Euphemism for Bioweapons Proliferation.
Obviously, the best way to spare us from another pandemic is to immediately stop funding gain-of-function (GOF) research and get rid of all existing GOF organisms. Let all nations build huge bonfires and burn up their evil creations at the same time, while allowing other nations to inspect their biological facilities and records.
But the WHO in its June 2023 Bureau Text of the Draft Pandemic Treaty has a plan that is the exact opposite of this. In the WHO’s draft treaty, which most nations’ rulers appear to have bought into, all governments will share all viruses and bacteria they come up with that are determined to have “pandemic potential” — share them with the WHO and other governments, putting their genomic sequences online. No, I am not making this up. (See screenshots from the draft treaty below.) Then the WHO and all the Fauci’s of the world would gain access to all the newly identified dangerous viruses. Would hackers also gain access to the sequences? This pandemic plan should make you feel anything but secure.
Fauci, Tedros, and their ilk at the WHO, and those managing biodefense and biomedical research for nation states are on one side, the side that gains access to ever more potential biological weapons, and the rest of us are on the other, at their mercy.
This poorly conceptualized plan used to be called proliferation of weapons of mass destruction—and it is almost certainly illegal. (For example, see Security Council resolution 1540 adopted in 2004.) But this is the plan of the WHO and of many of our leaders. Governments will all share the weapons.
The Genomic Sequencing Conundrum
And governments are to commit to building biolabs that must include genomic sequencing. No explanation has been forthcoming about why each nation needs to install its own genome sequencing laboratories. Of course, they would sequence the many viruses that will be detected as a result of the pathogen surveillance activities nations must perform, according to the WHO treaty draft. But the same techniques can be used to sequence human genomes. The fact that the EU, UK, and US are currently engaged in projects to sequence about 2 million of their citizens’ genomes provides a hint they may want to collect additional genomes of Africans, Asians, and others.
This might fly as simply sharing state-of-the-art science with our less-developed neighbors. But it is curious that there is so much emphasis on genomics, compared to an absence of discussion about developing repurposed drugs for pandemics in the draft treaty or IHR amendments.
But we can’t forget that virtually all developed nations, in lockstep, restricted the use of safe generic hydroxychloroquine, ivermectin, and related drugs during the pandemic. In retrospect, the only logical explanation for this unprecedented action was to preserve the market for expensive patentable drugs and vaccines, and possibly to prolong the pandemic.
Genomes offer great potential profits, as well as providing the substrate for transhumanist experiments that could include designer babies.
The latest version (aka the WHO Bureau draft) of the pandemic treaty can be accessed here. I provide screenshots to illustrate additional points.
Draft pages 10 and 11:




The WHO Treaty Draft Incentivizes Gain-of-Function Research
What else is in the Treaty? Gain-of-Function research (designed to make microorganisms more transmissible or more pathogenic) is explicitly incentivized by the treaty. The treaty demands that administrative hurdles to such research must be minimized, while unintended consequences (aka pandemics) should be prevented. But of course, when you perform this type of research, leaks and losses of agents can’t always be prevented. The joint CDC-USDA Federal Select Agent Program (FSAP) which keeps track of research on potential pandemic pathogens collects reports of about 200 accidents or escapes yearly from labs situated in the US. The FSAP annual report for 2021 notes:
“In 2021, FSAP received 8 reports of losses, 177 reports of releases, and no reports of thefts.”
Research on deadly pathogens cannot be performed without risks both to the researchers and the outside world.
Draft page 14:

Vaccines Will be Rolled Out Speedily Under Abbreviated Future Testing Protocols
Vaccines normally take 10-15 years to be developed. In case you thought the COVID vaccines took too long to be rolled out (326 days from availability of the viral sequence to authorization of the first US COVID vaccine) the WHO treaty draft has plans to shorten testing. There will be new clinical trial platforms. Nations must increase clinical trial capacity. (Might that mean mandating people to be human subjects in out-of-the-way places like Africa, for example?) And there will be new “mechanisms to facilitate the rapid interpretation of data from clinical trials” as well as “strategies for managing liability risks.”
Draft page 14:
Manufacturer and Government Liability for Vaccine Injuries Must be “Managed”
Nations are supposed to use “existing relevant models” as a reference for compensation of injuries due to pandemic vaccines. Of course, most countries do not have vaccine injury compensation schemes, and when they do the benefits are usually minimal.
Is the US government’s program to be a model of what gets implemented internationally?
The US government scheme for injuries due to COVID pandemic products (the Countermeasures Injury Compensation Program or CICP) has compensated exactly 4 (yes, four) of the 12,000 claimants for COVID product-related injuries as of August 1, 2023. All pandemic EUA drugs and vaccines convey a liability shield to the government and manufacturers (this includes monoclonal antibodies, pre-licensure remdesivir, paxlovid, molnupiravir, some ventilators and all COVID vaccines) and the only avenue for injury compensation is through this program.
Slightly over 1,000 of the 12,000 claims have been adjudicated while 10,887 are pending review. Twenty claims were deemed eligible and await a benefits review. Benefits are only paid for uncovered medical expenses or lost income. A total of 983 people, or 98 percent of those whose claims have been adjudicated had their claims denied, many because they missed the brief one-year statute of limitations. Below are the latest data from this program:
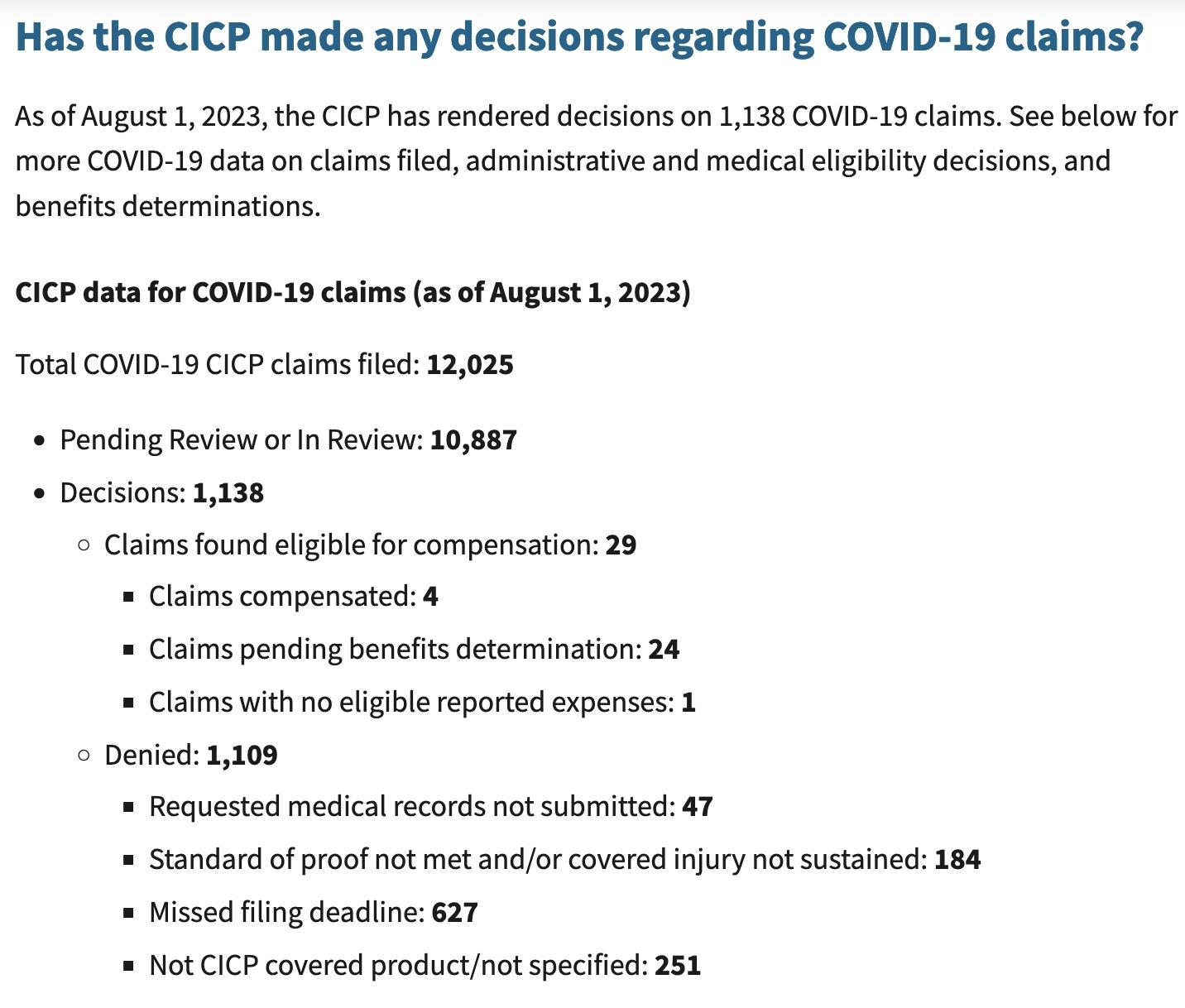
The treaty draft also demands weakening the strict regulation of medical drugs and vaccines during emergencies, under the rubric of “Regulatory Strengthening.” As announced in the UK last week, where ‘trusted partner’ approvals will be used to speed licensure, this is moving toward a single regulatory agency approval or authorization, to be immediately adopted by other nations (p 25).
Next Up: Vaccines Developed in 100 Days
A plan to develop vaccines in 100 days and have them manufactured in 30 additional days has been widely publicized by the vaccine nonprofit CEPI, founded in 2017 by Sir Dr. Jeremy Farrar, who is now the WHO’s Chief Scientist. The plan has been echoed by the US and UK governments and received some buy-in from the G7 in 2021. This timeframe would only allow for very brief testing in humans, or would, more likely, limit testing to animals. Why would any country sign up for this? Is this what we the people want?
The plan furthermore depends on the vaccines only being tested for their ability to induce antibodies, which is termed immunogenicity, rather than being shown to actually prevent disease, at least for the initial rollout. My understanding of FDA regulation was that antibody levels were not an acceptable surrogate for immunity unless they had been demonstrated to actually correlate with protection. However, the FDA’s recent vaccine decisions have scrapped all that and vaccines are now being approved based on antibody titers alone. The FDA’s vaccine advisory committee has asked it for better indicators of efficacy than this, but the advisers have also voted to approve or authorize vaccines in the absence of any real measures showing that they work. I learned this because I watch the FDA vaccine advisory meetings and provide a live blog of them.
We all know how long it took for the public to become aware that the COVID vaccines failed to prevent transmission and only prevented cases for a period of weeks to months. The US government has still not officially admitted this, even though CDC Director Rochelle Walensky told CNN’s Wolf Blitzer the truth about transmission on August 6, 2021.
It is critical for the public to understand that safety testing can only be accomplished in human beings, as animals react differently to drugs and vaccines than humans do. Therefore, limited testing in animals would mean there was no actual safety testing. But testing vaccines in humans for only short periods is also unacceptable.
Testing vaccines during brief trials in humans (the Pfizer trials only followed a “safety subset” of trial subjects for a median of two months for safety) allowed COVID vaccines to be rolled out without the public being aware they could cause myocarditis and sudden deaths, most commonly in athletic young males in their teens and twenties, or a myriad of other conditions.
Finally, following this rapid manufacturing plan, thorough testing for potential failures in the manufacturing process could not be performed. With the current plan for far-flung, decentralized manufacturing facilities that are said to be necessary to achieve vaccine equity for all, there are nowhere near enough regulators who could inspect and approve them.
Will the WHO Respect Human Rights?
The need to respect “human rights, dignity, and freedom of persons” is embedded in the current International Health Regulations (IHR), as well as other UN treaties. However, the language guaranteeing human rights, dignity, and freedom of persons was peremptorily removed from the proposed IHR Amendments, without explanation. The removal of human rights protections did not go unnoticed, and the WHO has been widely criticized for it.
The WHO apparently is responding to these criticisms, and so the language guaranteeing human rights that was removed from the drafts of the International Health Regulations has been inserted into the newest version of the pandemic treaty.
Conclusions
As long predicted by science fiction, our bio- and cyber-scientific achievements have finally gotten away from us. We can produce vaccines in 100 days and manufacture them in 130 days–but there will be no guarantees that the products will be safe, effective, or adequately manufactured. And we can expect large profits but no consequences for the manufacturers.
Our genes can be decoded, and the fruits of personalized medicine made available to us. Or perhaps our genes will be patented and sold to the highest bidder. We might be able to select for special characteristics in our children, but at the same time, a human underclass could be created.
Our electronic communications can be completely monitored and censored, and uniform messaging can be imposed on everyone. But for whom would this be good?
New biological weapons can be engineered. They can be shared. Maybe that will speed up the development of vaccines and therapeutics. But who really benefits from this scheme? Who pays the price of accidents or deliberate use? Wouldn’t it be better to end so-called gain-of-function research entirely through restrictions on funding and other regulations, rather than encouraging its proliferation?
These are important issues for humanity, and I encourage everyone to become part of the conversation.
Dr. Meryl Nass, MD is an internal medicine specialist in Ellsworth, ME, and has over 42 years of experience in the medical field. She graduated from University of Mississippi School of Medicine in 1980.
‘A Fauci Clone’: New NIAID Director Oversaw Remdesivir Trials, Has Ties to Biosafety Lab Research

By Michael Nevradakis, Ph.D. | The Defender | August 15, 2023
When he retired in December 2022, Dr. Anthony Fauci, then-director of the National Institute of Allergy and Infectious Diseases (NIAID) was the highest-paid federal employee and the recipient of the largest federal retirement package in history.
Fauci’s successor, Dr. Jeanne M. Marrazzo, will soon take over leadership of the agency — and its $6.3 billion budget.
Fauci praised Marrazzo, telling CNN, “She’s very well-liked. She’s a really good person. I think she’s going to do a really good job.”
But some of her critics, including medical and public health experts interviewed by The Defender, questioned Marrazzo’s suitability for leading NIAID, citing her limited experience as a medical practitioner and her role in supervising clinical trials of remdesivir, a controversial drug used to treat hospitalized COVID-19 patients.
Critics also called out her steadfast support for strict restrictions and countermeasures during the pandemic, and her receipt, since 1997, of more than $20 million in grants from the National Institutes of Health (NIH) and payments from Big Pharma — including from Gilead, the manufacturer of remdesivir.
And lastly, some pointed to Marrazzo’s key administrative role in a University of Alabama (UAB) institution which houses a BSL3 (biosafety level 3) laboratory that conducts gain-of-function research.
Before being named director of the NIAID, Marrazzo was director of the Division of Infectious Diseases at the UAB at Birmingham. She will replace Dr. Hugh Auchincloss, who has served as NIAID’s acting director following Fauci’s departure.
Commenting on the appointment, Brian Hooker, Ph.D., senior director of science and research for Children’s Health Defense (CHD), said:
“It looks like Dr. Marrazzo will give us more of the same, unfortunately. Her flip-flopping, penchant for Big Pharma, and support of draconian public health (control) measures mean that she’ll take a reactionary posture to any ‘pandemic threat’ and may be as gleeful as Fauci at the prospect of new pandemics.
“I have dim hopes that she may learn some lessons while the investigations into Fauci lying to Congress play out. However, these bureaucrats don’t really believe that the law applies to them.”
The NIAID is the second largest center at the NIH. According to CNN, it “supports research to advance the understanding, diagnosis and treatment of infectious, immunologic and allergic diseases,” as well as “research at universities and research organizations around the United States and across NIAID’s 21 laboratories.”
“Marrazzo fits the mold of every public health leader so far that has led the charge during the pandemic,” Dr. Kat Lindley, president of the Global Health Project and director of the Global COVID Summit, told The Defender.
Lindley added:
“My concern with Marrazzo is actually her Big Pharma ties, her lack of clinical experience with COVID-19 in particular, and her blatant ignorance on early treatment and support for unproven, scientifically debunked measures, in particular masking.
“Any scientist or physician should understand that masking has never proven to be effective and, in the case of children, even detrimental.”
Touted remdesivir as ‘silver bullet’ for treating COVID
During her tenure at UAB, the university served as one of the clinical trial sites for remdesivir, an antiviral originally developed by Gilead Sciences as a treatment for Hepatitis C and respiratory syncytial virus (RSV).
According to the NIH, the trial was intended “to evaluate the safety and efficacy of the investigational antiviral remdesivir in hospitalized adults diagnosed with coronavirus disease 2019.” Marrazzo supervised the UAB trial site.
UAB has long served as a research site for remdesivir. A February 2021 UAB report states, “Gilead entered into collaboration with the UAB-led Antiviral Drug Development and Discovery Center … to study remdesivir against coronaviruses” in 2014.
“These earlier studies enabled remdesivir to more quickly be tested and approved for human use as a treatment for COVID-19 when the 2020 pandemic struck,” UAB stated.
The trial results, published in the New England Journal of Medicine (NEJM) in November 2020, found remdesivir shortened “the time to recovery in adults who were hospitalized with COVID-19 and had evidence of lower respiratory tract infection.”
Fauci later praised remdesivir as the “standard of care” for treating COVID-19.
However, according to investigative journalist Jordan Schachtel, studies “show that there are zero clinical benefits to injecting patients with remdesivir. Many studies show that remdesivir can severely injure vital organs such as the heart and kidneys.”
Yet, Marrazzo never disclosed a conflict of interest when publicly commenting on remdesivir, Schachtel said. She described it as a “silver bullet” in remarks shared with The Washington Post in July 2020, and in tweets praising the drug.
“Given the UAB-Gilead partnership, one would think that Dr. Marrazzo would refrain from commenting on issues through which she maintained a clear conflict of interest,” Schachtel wrote. “She did no such thing.”
According to the U.S. government’s Open Payments database, Marrazzo received seven payments from Gilead, totaling $2,474.93.
But as Marrazzo repeatedly praised remdesivir — and, according to Schachtel, has “never shown remorse” for this despite mounting evidence of the harm it has caused — she has repeatedly spoken out against hydroxychloroquine for treating COVID-19.
In June 2020, in reference to a study published in the NEJM claiming hydroxychloroquine is ineffective in protecting people from COVID-19, Marrazzo said these findings “should provide a very big nail in the coffin” for the use of this treatment.
The following month, Marrazzo called a video that went viral on social media describing hydroxychloroquine as a cure for COVID-19 “very irresponsible and despicable,” adding that she was “glad that video is hopefully not being shared very much.”
In October 2021, she said hydroxychloroquine and ivermectin hold “special appeal” to the unvaccinated.
Yet, in April 2020, prior to the conclusion of the remdesivir clinical trial, Marrazzo said, “We are using it [hydroxychloroquine] in our hospital … for a range of patients including when patients are beginning to deteriorate,” adding:
“And lots of media folks are asking what we think about hydroxychloroquine. And the reality is that we live and die by the evidence. And one issue is the argument about whether it’s even ethical to use these treatments when we don’t have the evidence.
“But I would get back to the compassionate use argument. When you have a patient who’s dying, you have to use what you can, what’s available.”
Cheerleader for COVID vaccines and Merck’s molnupiravir
Marrazzo has also praised COVID-19 vaccines and therapeutics. In May 2020, she was “hopeful” about the Moderna COVID-19 vaccine clinical trial — despite its enrollment of only eight volunteers, saying “We don’t have the luxury of time here in this case.”
In August 2021, she called the U.S. Food and Drug Administration’s approval of the Pfizer Comirnaty COVID-19 vaccine “great news,” saying, “Vaccines are our best weapon against this disease” and are “working incredibly well to prevent severe disease” and reduce hospitalizations.
In January 2022, Marrazzo said “Vaccination makes the biggest difference” in fighting COVID-19, adding that “boosters, of course, are going to augment that protection.”
And in October 2021, Marrazzo praised molnupiravir, Merck’s antiviral pill for COVID-19, stating it had “extraordinary potential.” Results of a preprint study later showed the drug may fuel the development of new and potentially deadly variants of COVID-19.
Marrazzo has received five payments from Merck, totaling $8,820.
Cardiologist Dr. Peter McCullough told The Defender Marrazzo “has been willfully blind to the failure of COVID-19 vaccines” and “appears incapable of mastering the four pillars of pandemic response to lead America through the next pandemic: 1) contagion control, 2) early treatment, 3) late treatment and 4) vaccination.”
A ‘slap in the face’ to vaccine, hospital protocol victims
During the COVID-19 pandemic, Marrazzo made frequent television appearances in which, according to a UAB statement, she “helped inform the world … sharing critical information and perspectives.” UAB touted Marrazzo as a COVID-19 expert during this period.
According to AL.com, Marrazzo was on Alabama Gov. Kay Ivey’s COVID-19 task force, supporting “emergency public health measures that closed business and mandated mask wearing.”
In March 2020, Marrazzo supported “flattening the curve,” calling on the public “to make personal sacrifices for the greater good.” In similar statements made on May 8, 2020, Marrazzo warned of a “backslide” if measures like social distancing were loosened.
In June 2020, she said masks can “change the trajectory of this epidemic.”
In a June 2020 YouTube video, “Why you should wear a mask,” Marrazzo said, “Masks have contributed to the control of this pandemic in other communities.” She called for masks for schoolchildren over age 6 and included mask-wearing in a list of “Three basic rules” along with hand washing and social distancing.
In an article she co-authored and in which she highlighted “the intersection of the COVID-19, HIV, and STI pandemics,” Marrazzo drew parallels between wearing masks and wearing condoms, writing:
“Condoms reduce transmission of HIV and bacterial STIs effectively, if used adequately and consistently, but lack of access to condoms or perhaps even personal preference limits their utility.
“As a correlate to barrier protection, masking has proven effective to reduce the expulsion of SARS-CoV-2 and other respiratory virus droplets.”
The paper also repeated claims regarding the “lack of benefit” of hydroxychloroquine, zinc and vitamins C and D in treating COVID-19. Conversely, referring to the COVID-19 vaccines, the authors stated, “There were few serious adverse events in either arm, and there were no deaths related to the vaccine.”
Blaming the unvaccinated
In May 2021, she criticized loosened Centers for Disease Control and Prevention (CDC) recommendations that the vaccinated do not need to wear masks, stating that because less than 50% were vaccinated in her community, she would still wear a mask indoors despite being fully vaccinated herself.
In July 2021 she warned of a “summer surge” that would be fueled by the unvaccinated.
In December 2021 Marrazzo again scolded the unvaccinated. “Your decision to get infected is unfortunately not just going to be affecting you,” she said. “It’s going to be serving a source of incredible infectiousness going forward.”
Dr. Scott Atlas, a member of the White House Coronavirus Task Force during the Trump administration, told KUSI News San Diego that Marrazzo “was completely wrong about COVID … Pushing pseudoscience, pushing … her belief that vaccines stopped the spread of the infection, that children have high risk, and that masks were efficacious.”
“Marrazzo represents everything that was done wrong in the handling of COVID,” said Gail Seiler, Texas chairperson, Projects and Content, for the FormerFedsGroup Freedom Foundation and a survivor of the CDC’s COVID-19 hospital protocols, including administration of remdesivir.
Seiler told The Defender that Marrazzo advocated for no early treatment until the patient “worsened to the point of hospitalization,” and at that point to give remdesivir, “a drug that she profits from.”
Seiler added:
“Because of people like Marrazzo, patients in the hospital were given no hope of survival. Because of her ignoring the evidence, over a million people died who shouldn’t have.
“Her selection to the NIAID is a slap in the face to every family whose loved ones were killed by the protocols she profited from. And it exemplifies why the general public has lost trust in agencies such as the NIAID.”
Financial ties to Big Pharma
Marrazzo received a total of $20,405,337 in NIH grants for 67 studies between 1997 and 2023, according to NIH data. These grants ranged between $6,000 and $2.82 million and averaged over $304,000 per grant.
Open Payments data show Marrazzo has received $28,761,36 across 37 “general payments” and $152,208.42 across seven payments for “associated research funding,” including $18,636.59 in consulting fees, $4,500 in honorariums, and payments from companies such as Merck, GlaxoSmithKline, Gilead, Janssen and Abbott Laboratories.
In December 2018, Marrazzo participated in a panel titled “Role of the Genital Tract Microbiome in Sexual and Reproductive Health,” during the Keystone Symposia Conference in South Africa, which was “made possible with funding from the Bill & Melinda Gates Foundation.”
Her employer, UAB, received at least two Gates Foundation grants pertaining to health-related research in recent years. This includes a June 2021 grant, “Modeling Impact of Service Delivery Redesign” totaling over $1.5 million, and a $124,921 grant in April 2020 for a project titled “COVID-19 CTA: HTS Core for screening compounds.”
UAB’s Division of Infectious Diseases boasts “an active research portfolio with approximately $39 million in external research funding.” Research specialties include “Pathogenesis of viral infections,” “Antiviral therapy,” “Travel medicine and international health” and “Host defenses and infectious diseases in immunocompromised patients.”
Big supporter of gain-of-function research
UAB also houses a BSL3 research laboratory, the Southeastern Biosafety Laboratory Alabama Birmingham (SEBLAB), funded in part by NIH. According to UAB, it is “one of a limited number of institutions,” adding that the university ranks “among the top 25 in funding from the National Institutes of Health.”
The university states that SEBLAB researchers are “able to bring their skills to bear on the SARS-CoV-2 pandemic, and other issues directly relevant to biodefense and emerging infectious disease,” with a focus on NIAID “priority pathogens” and discovery of “new treatments to prevent or combat” diseases caused by infectious agents.
These projects have also included “Testing drugs on SARS-CoV-2,” a process involving growing the virus in SEBLAB. According to UAB researcher Kevin Harrod, Ph.D.,“We grow the viruses, measure them and provide them to the BARDA [the U.S. government’s Biomedical Advanced Research and Development Authority] contractor.”
BSL3 and BSL4 laboratories across the U.S. and the world have been associated with controversial gain-of-function research, which some have said is responsible for the development and subsequent alleged leak from one such facility, the Wuhan Institute of Virology in China, leading to prominent calls to end such research.
According to Independent Institute, “Marrazzo’s views on the origin of COVID-19 are hard to find,” as are her views on gain-of-function research.
Francis Boyle, J.D., Ph.D., a professor of international law at the University of Illinois who drafted the Biological Weapons Anti-Terrorism Act of 1989, told The Defender that Marrazzo’s selection signals that the NIH and NIAID have no intention of stopping gain-of-function research at BSL3 and BSL4 facilities.
Boyle said:
“They will have her in place to deal with the next pandemic that they know is coming out of their own BSL3 and BSL4 labs, just as Fauci dealt with the COVID-19 pandemic that came out of the Wuhan BSL4 and the University of North Carolina BSL3 and that Fauci and [former NIH Director] Francis Collins funded.
“Under her auspices NIAID will continue to research, develop, manufacture and stockpile every hideous type of Nazi biological warfare weapon known to humanity … There will be no end to it and to these death scientists like her … unless and until we stop them by criminal prosecutions.”
Boyle called Marrazzo a “Fauci clone, not an original and independent thinker,” adding, “The Bidenites and the globalists and Big Pharma behind them picked her to continue the Fauci/NIAID policies and programs across the board.”
Michael Nevradakis, Ph.D., based in Athens, Greece, is a senior reporter for The Defender and part of the rotation of hosts for CHD.TV’s “Good Morning CHD.”
This article was originally published by The Defender — Children’s Health Defense’s News & Views Website under Creative Commons license CC BY-NC-ND 4.0. Please consider subscribing to The Defender or donating to Children’s Health Defense.
YouTube Greatly Expands Its Medical “Misinformation” Policies
New rules, largely determined by the WHO
By Christina Maas | Reclaim The Net | August 16, 2023
YouTube, the titan of online video content, has expanded its Covid misinformation policy to cover what it calls all forms of medical misinformation.
YouTube has also declared its plan to delist videos promoting “cancer treatments proven to be harmful or ineffective,” effectively disallowing content creators from encouraging natural cures.
The platform pledges to implement its medical misinformation policies when a topic exhibits high public health risks, is supposedly prone to misinformation, and when official guidance from health authorities is accessible to the public.
The changes also see YouTube recommitting to groups such as the WHO and other health bodies on what information is deemed to be acceptable for people to talk about on the platform – despite these institutions having recently received major blows to their credibility.
According to the policy update, YouTube will no longer host content that:
- Misinforms about prevention techniques or contradicts current health authority guidelines, including inaccuracies regarding the safety or efficacy of approved vaccines.
- Promotes treatments that local health bodies or the WHO have neither approved nor recognized as safe and effective. Moreover, it bans content that advocates for harmful substances or practices that have been scientifically proven to be detrimental.
- Denies the existence of specific health conditions.
As stated in its blog post, YouTube intends to punish content promoting not only what it believes to be overtly harmful treatments but also unproven ones that are audaciously offered as replacements for recognized alternatives.
For instance, influencers suggesting vitamin C supplements or garlic for cancer may have their content removed, the post states.
This marks a substantial escalation in the Google-owned platform’s ongoing crusade against what it believes to be the dissemination of medical misinformation, heavily catalyzed by the controversial experience of battling narratives about themes such as COVID-19 and vaccines, something YouTube was heavily criticized for as truthful content ended up being censored on the platform.
YouTube had targeted vaccine “misinformation,” such as demonetizing and deleting vaccine skepticism, thereby refining their approach in response to the global pandemic situation.
Featured Video

US Middle East Policy: The Growing Propensity for Genocide
or go to
Aletho News Archives – Video-Images
From the Archives
The New Baghdad Pact
By Dr Bouthaina Shaaban | February 23, 2017
A recently declassified CIA document prepared in 1983, and released on 20 January 2017, shows that the United States had at the time encouraged Saddam Hussein to attack Syria, which would have led to a vicious conflict between the two countries, thus draining their resources.
The report, which was then prepared by CIA officer Graham Fuller, indicates that the US tried adamantly to convince Saddam to attack Syria under any pretense available, in order to get the two most powerful countries in the Arab East to destroy each other, turning their attention away from the Arab-Israeli conflict. … continue
Blog Roll
 Aletho News
Aletho News- Iran defends limits on Strait of Hormuz passage
- ‘We warned you’: Hormuz Strait back to pervious state amid US blockade
- Iran rejects uranium transfer, warns of response to naval blockade
- US Middle East Policy: The Growing Propensity for Genocide
- Daniel Davis: Iran Reopens the Strait of Hormuz
- Trump taps military-grade flu pandemic architect to lead CDC amid simultaneous gain-of-function and vax development
- Israeli General: War with Iran does not serve Israel as global standing erodes over Gaza
- The collapse is real – Lebanon ceasefire marks a historic strategic defeat
- Trump keeps Hormuz blockade despite Iran reopening passage
- ‘New order’ in Strait of Hormuz: IRGC Navy mandates authorization for all vessels
- If Americans Knew
- Israel relegates another population to life in tents – Daily Update
- Senate again fails to block weapons to Israel
- Think the Iran war is a disaster? Blame these DC think tanks first.
- Number of Palestinian Prisoners Rises By 83% Since October 2023
- With multiple “ceasefires” in place, Israel keeps on killing in Gaza and Lebanon – Daily Update
- Mearsheimer: Israel Owns Trump
- Mark Levin and Jonathan Pollard Push for Nuking Iran
- TCN: America Enables Israel’s Crimes
- Israel’s Next Leader Will Be Just Like Bibi – but Without the Corruption
- Born into war, raised across borders: The story of Gaza’s premature babies separated from their parents amid Israel’s genocide
- No Tricks Zone
- Reality Check: Maldives Have Actually Grown In Size Or Remained Stable Over Recent Decades
- Abrupt Climate Change Also Occurred NATURALLY In The Past …25 Times During Last Ice Age
- Cave Discovery Reveals Today’s Desert Climates Were Recently Far Warmer, Wetter, Teeming With Life
- German Expert: Heat Dome Led To Record Temps In Western USA…Warmer In 1934, 1936
- New Study: No Linear Warming Or Glacier Retreat Along Northern Antarctic Peninsula Since 1980s
- An Inconvenient Tree: Uncovered In Alps… Europe Much Warmer Than Today 6000 Years Ago
- New Study Reports A 60% Slowdown In Greenland’s Ice Loss Rate In The Last Decade
- Low Intensity Tornado Wrecks Major Solar Farm, Creating A Potential Toxic Dump
- New Study Finds Warming Saves Lives…Cold Temperatures 12 Times More Deadly Than Excess Heat
- German Science Blog Accuses PIK Climate Institute Of Hallucinating Climate Tipping Points

{kind=link}
{kind=link}
{kind=link}