HighWire Dispels Misinformation About Measles
The HighWire with Del Bigtree | February 28, 2025
Del does a deep dive into the science behind the measles virus, dispelling decades of misinformation from public health agencies, as well as what is actually driving the recent measles outbreaks in the U.S. See a shocking scientific equation comparing the number of individual deaths that would occur if the measles vaccine had never been introduced based on pre-vaccine stats to the number of deaths from MMR injury.
How Speaking Out Against Harmful COVID Policies Can Get You Banned by the NHS
The story of a bizarre punishment
By MJ Sutherland | Health Advisory & Recovery Team | December 27, 2024
It’s been an incredible journey.
At the end of July 2021, I walked out of a well-paid job with Dumfries & Galloway Council. I resigned in protest—against fraudulent COVID testing, child maltreatment through misuse of tests and enforcement of mask mandates, and the complete disregard for their lack of authority to do any of it. What they were doing to Other People’s Children in schools was indefensible, and I wasn’t going to stay silent. Later I forced them to admit, via the Scottish Information Commissioner, that they had no legal authority for any of it. I’d long since left the council by this time.
At first, the threats were thinly veiled: hints that speaking out could jeopardise my job, suggestions that I should “be careful” what I said, because “we don’t want to lose you…” But when I refused to back down, their tactics became more direct. I was accused of spreading misinformation—despite providing mountains of evidence—and warned that my activism could “damage my reputation.” It was clear they wanted me to stop asking questions. I didn’t, and after being warned about my “behaviour” once too often, I walked out – but not before sending a damning email to hundreds, if not thousands, of council workers, accusing the council’s top brass of fraud, misfeasance and child abuse.
By October 2021, I was working with Phil Hyland of PJH Law, and together we sent the council a formal letter warning them of the crimes they’d be complicit in if they continued. It still feels surreal that I got to be part of that. I’d already sent similar notices and detailed evidence to the local health board, but both the council and NHS ignored everything I submitted.
Then, in December 2021, things escalated when an NHS “Consultant in Public Health” closed a local primary school, forcing children into self-isolation until they could produce a negative PCR test before they could return. Knowing the truth about these tests—their inaccuracies, their misuse—I couldn’t stay quiet. This wasn’t just bad policy; it was child abuse. We issued a Notice to Cease and Desist to Dr Regina McDevitt. We attached the PJH Law letter we’d sent to the council, along with the evidence pack detailing the harm these policies were causing.
This time, there was a reaction. But instead of addressing the harm to children or engaging with the evidence, NHS Dumfries & Galloway’s CEO, Jeff Ace, decided instead to ban me from all NHS premises for six months.
This was a bizarre move, especially since I hadn’t set foot in an NHS building for years. I was still entitled to go for medical appointments (although I had none), but presumably not allowed to visit patients, although I didn’t know anyone in hospital at the time, so no difference there. I was still entitled to submit FOI requests as I had been doing, but presumably not allowed to protest by waving placards outside NHS buildings, which I wasn’t doing anyway. But, as pointless and absurd as it may be, banned I was.
I can only suspect Jeff’s motive was to to feel better about himself, like he’d actually achieved something, but here’s the irony: while they were busy “punishing” me, they quietly dropped the requirement for children to produce negative PCR tests before returning to school. So, in the end, something got through. But the message was clear: dissent would not be tolerated.
Since then, I’ve kept busy. I’ve been prodding, poking, and shining a light on the fraud and abuse that fuelled the covid tyranny. This wasn’t just about masks or tests; it was about the false claims of authority that let these institutions get away with it all.
Last year, I had the honour of being interviewed by Dr Ahmad Malik about my activism. We discussed the council’s capitulation on masks, the informed consent documents I created, and how this fight has unfolded. And now, HART have invited me to share my story as someone who chose the difficult path by communicating the truth about covid policies and their effects.
Looking back, I’m pleased to say that the threats didn’t stop me. Neither did losing my career. And while I’ve chosen that difficult path, I wouldn’t change a thing.
Like I said, it’s been an incredible journey.
MJ Sutherland
Founder of Declaration of Dumfries
Kafka-NHS
The witch hunts against dissident doctors continue
Health Advisory & Recovery Team | June 8, 2024
In June 2021, Dr. Sam White, a general practitioner, released a video calling out harmful covid policy. From a scientific perspective every word he said was entirely defensible. Moreover it is clear that he was speaking from an ethical position of wanting to protect his patients from harm. He pulled no punches in addressing the most prominent issues that were causing harm – lack of treatment for the frail, inappropriate gene therapies and masking. In interviews, in 2022, he called the situation a war between good and evil. In doing so he unleashed a torrent of anger among those in a position of power over him, which, three years on, continues to harm him.
He had already resigned from his GP partnership in protest at their vaccination policy in February 2021. His conscience had been keeping him awake at night because he did not want to be a part of the vaccine rollout. Consequently, after resigning he was signed off with stress rather than having to work his notice. NHS England still saw fit to suspend him with an emergency order in June. Dr White managed to record a conversation with an NHS senior clinical adviser who implied that he was mentally unwell. Dr White believes that possession of that recording led the NHS to revoke their suspension. However, by then the NHS had referred him for a GMC investigation and an automatic GMC suspension.
The GMC overturned the suspension in August 2021 but imposed restrictions on him including a ban on mentioning covid on social media and requiring the removal of his previous posts. The legal position is that doctors have a right to free speech but if the GMC could prove Dr White’s speech was a threat to the health of the public or undermined trust in the profession then he could be sanctioned.
Dr White looked to his indemnity provider for support to fund his legal case but they washed their hands of him saying it was a “conduct issue”. With the help of crowd funding support, Dr White took the case to the High Court in November 2021. The verdict was published in December 2021, overruling the GMC and saying they had not followed due process in their actions. The High Court documentation was removed from the judiciary’s website in September 2022 such that other doctors in a similar position will be unable to refer to it in their defence. It is available on the Wayback Machine.
Dr White has asked to be removed from the register, as he is no longer practising conventional medicine, but the GMC have refused and are continuing to persecute him. Every interview he has undertaken has been transcribed and put forward as evidence that he is undermining public health policy and causing the public to lose trust in the profession. The next tribunal hearing is scheduled to last three weeks in August and September 2024. This ongoing investigation, three years later, indicates a relentless effort to discredit and punish Dr. White for his dissenting views.
If that sounds bad, wait until you hear about the NHS’s role.
The same day as the High Court hearing, unbeknown to Dr White or his lawyers, NHSE had a meeting where they decided to refer Dr White for a health assessment, despite the fact he no longer worked in the NHS. This was an opportunity to reopen the investigation into him. They have repeatedly asked if he had returned to NHS work and said he must tell them if he did. What was their intent here? Were they planning to ask any future employer to suspend him all over again?
NHS England has a list of “approved providers”. Any doctor not on their list cannot work for the primary employer of doctors in the country. In 2023, NHS England removed Dr White from their list, effectively barring him from practising within the NHS. He had already shifted his practice to private healthcare with a holistic focus, but this further punishment leaves him with no other options.
The GMC is far from perfect but at least it has due process and a system of appeal for where there might be an injustice. NHS England can unilaterally destroy a career, with no legal recourse.
In some ways, the most disturbing aspect of the whole affair was revealed in the communications between the GMC and NHS England. Firstly, the derogatory terms used about the doctor to justify their behaviour are shocking and reveal a lack of professionalism and intolerance for differing opinions within the medical establishment. Moreover, this language served as a means to rationalise their harsh and unjust actions towards him. Secondly, they appeared to be acting in cahoots. The GMC’s apparent open and fair processes have been bypassed by direct communication with NHS England, stripping Dr White of a right to employment.
Dr. Sam White’s case is a stark example of systemic injustice and the erosion of professional rights within the NHS and the GMC. His ongoing persecution for voicing dissenting views underscores a troubling intolerance for ethical and scientific debate, reminiscent of a Kafkaesque nightmare where rationality and justice are subordinated to bureaucratic oppression.
From Florida’s Surgeon General, a devastating indictment of the vaccine and its pushers
By Neville Hodgkinson | TCW Defending Freedom | June 22, 2023
When it comes to error correction, the USA’s 50 sovereign states offer more opportunity for an authoritative challenge to the misuse of power than we enjoy in the UK. Dr Joseph Ladapo, the Florida Surgeon General, has made public a letter excoriating federal health officials over their promotion of the mRNA Covid vaccines. The government, he said, ‘has relentlessly forced a premature vaccine into the arms of the American people with little or no concern for the adverse ramifications’.
The letter was to Drs Robert Califf, head of the Food and Drug Administration, and Rochelle Walensky, director of the Centers for Disease Control and Prevention. Lapado wrote: ‘Your ongoing decision to ignore many of the risks associated with mRNA Covid-19 vaccines, alongside your efforts to manipulate the public into thinking they are harmless, have resulted in deep distrust in the American health care system.’
As reported here earlier this year, senior American scientists have called for a ‘bipartisan, scientifically minded Covid-19 commission so the public health disaster of the past three years is not repeated’. They face an uphill struggle in achieving that aim, but Ladapo’s no-holds-barred letter means that at least some of Florida’s 22.6million citizens have a chance of knowing the jabs are not ‘safe and effective’, as the British public are constantly being told.
Ladapo would surely have been less forthright if Ron DeSantis, Florida’s Republican governor and a possible future US president, were not also on the warpath over the Biden administration’s handling of the pandemic. The Florida Supreme Court has approved DeSantis’s request to convene a grand jury to investigate ‘wrongdoings’ associated with the vaccines.
But DeSantis is not alone. The Texas Attorney General has launched an investigation into whether Pfizer, Moderna and Johnson & Johnson, the companies producing the jabs, misrepresented their safety and efficacy and manipulated trial data. The investigation could open the door to lawsuits by people injured by the mRNA products.
Meanwhile, what hope of redress do Britons have, not just for vaccine damage but for the lives shattered by cruel and unprecedented lockdowns?
The public inquiry led by Baroness Hallett looks likely to be worse than useless, as Laura Dodsworth, author of the best-selling A State of Fear: How the UK Government Weaponised Fear During the Covid-19 Pandemic, has described.
It is in ‘the wise and noble tradition of the great British public inquiry’, Rod Liddle commented in the Sunday Times last weekend. That is, keep the public away from it for as long as possible, and say nothing useful or meaningful unless ‘at least 20 years after whatever it is that they are inquiring about, at which point most of the relevant people are stiff as a stoat’.
The headline on Liddle’s article declared: ‘The data is clear: lockdowns are useless. But you won’t hear that from the inquiry.’
Sadly, neither the Sunday Times nor its daily stablemate, nor just about any of the mainstream media in the UK, have yet ventured into questioning the ‘safe and effective’ narrative about the vaccines. So let’s look at what Ladapo, who as state surgeon general can hardly be dismissed as a conspiracy theorist, has told the American public.
‘Data are unequivocal,’ Ladapo wrote. ‘After the Covid-19 vaccine rollout, the Vaccine Adverse Events Reporting System (VAERS) reporting increased by 1,700 per cent, including a 4,400 per cent increase in life-threatening conditions.
‘Dismissing this pronounced increase as being solely due to reporting trends is a callous denial of corroborating scientific evidence also pointing to increased risk and a poor safety profile. It also fails to explain the disproportionate increase in life-threatening adverse events for the mRNA vaccines compared to all adverse events.
‘Based on the CDC’s own data, rates of incapacitation after mRNA vaccination far surpass other vaccines.’
Ladapo cited a recent study which found an excess risk of serious adverse events ‘of special interest’ for 1 in 550 people after mRNA vaccination. He wrote: ‘As you are aware, this is extraordinarily high for a vaccine. In comparison, the risk of serious adverse events after influenza vaccination is much lower. For you to claim that serious adverse events such as these are “rare” when Pfizer and Moderna’s clinical trial data indicate they are not, is a startling exercise in disinformation.
‘I want to re-emphasise that these questions could have been answered if you had required vaccine manufacturers to perform and report adequate clinical trials . . . I anticipate with regret that you will repeat past mistakes and prematurely promote new therapies to Americans without accurately and truthfully weighing data on risks and benefits.’
Ladapo then asked Califf and Walensky to answer 12 questions relating to the safety data, and concluded: ‘Your organisations are the main entities promoting vaccine hesitancy – Florida promotes the truth. It is our duty to provide all information within our power to individuals so they can make their own informed health care decisions. A lack of transparency only harms Americans’ faith in science.’
Regular readers of TCW as well as The Daily Sceptic know that numerous scientists support Ladapo’s position, such as reported here, here, here, here, here, here and here.
At present, however, the FDA and CDC, like the NHS, continue to ignore such reports, asserting that ‘the known and potential benefits of these vaccines clearly outweigh their known and potential risks, and that ‘being up to date on vaccinations saves lives compared with individuals who did not get vaccinated’.
Broken Trust
Can the relationship with state healthcare ever be repaired?
Health Advisory & Recovery Team | April 21, 2023
For many people, the words ‘trust the experts’ now invoke a sort of pavlovian horror response. This trope serves as a visceral reminder of 3 years’ constant gaslighting for daring to question the narrative, the relentless stream of celebrity medics repeating the ‘safe and effective’ mantra and the bullying and coercion to take a ‘vaccine’ that millions of people didn’t feel they needed or wanted. It had all the hallmarks of an abusive relationship. Core medical ethical principles were destroyed, the weaknesses of protocolised top-down healthcare delivery were exposed and of course there was direct harm to individuals. Is it any wonder that a great many of the British public never want to hear the words ‘our NHS’ ever again, cringing as they remember the weekly clapping ritual.
An inclination to throw the baby out with the bathwater is now a strong instinct for many who feel completely let down. If the relationship with state healthcare stands any chance of being repaired, harms enacted in recent years need to be properly acknowledged and people’s concerns carefully listened to. The uncomfortable question as to whether the NHS can function in its current incarnation should be aired. For a lot of people a ‘great reset’ of the medical profession would be a necessary condition of return. Indeed, many medics wonder if they can remain in a system that is clearly failing those it is supposed to serve.
As one doctor with decades of experience laments:
“If I continue to practise conveyor belt and recipe book medicine under the current system, the benefit is only to the Medical Business Model; hospitals, laboratories, diagnostic centres and the pharmaceutical industry all benefit in a model designed to keep the patient sick.”
Another consultant doctor reflecting on the past few years, had the following comments:
“The most odious revelation to me was when early on the directive came forth forbidding doctors, on pain of GMC punishment, to use their own initiative to treat a Covid patient with any other substance, drug, or agent whatsoever than that which was approved officially (of course at this point there was nothing in that category), save only for using it in an officially approved Clinical Trial. I felt utterly betrayed as a doctor. The whole essence of the doctor-patient relationship was abruptly abolished. We were now in the CMO-patient relationship. My role was merely to be a minor minion box-ticking algorithm slave. No clinical discretion. No discussion along the principles of best interest of the patient with informed consent. Oh no, that’s old hat! I saw the moral authority and overshadowing support of the entire medical establishment wither up like Jonah’s gourd.”
Multiple articles are now appearing reporting that morale for those working within the NHS is at an all-time low.1,2,3 One can only imagine that bearing witness to some of the most inhumane policies in NHS history for 3 years straight has not helped. Add to this the long hours on low pay, with increasingly limited time to spend with patients due to unmanageable waiting lists, and you have a perfect recipe for abysmal job satisfaction. Do we really want those in charge of our healthcare decisions to be forced to work under these conditions?
So now to the question of trusting medical advice that has been co-opted, protocolised and politicised, not to mention censored and distorted by financial interests. The UKHSA is supposed to be the government gatekeeper that is ‘responsible for protecting every member of every community from the impact of infectious diseases’. Just yesterday the agency was still urging people on Twitter to go and get their first and second covid vaccine. This is now so ludicrously at odds with the available evidence that any sane member of the public should conclude that the regulatory system in the UK is officially broken. It is worth taking the time to read the comments under the tweet to see that the public’s natural survival instincts seem to have well and truly kicked in. This random selection suggests the UKHSA may need to read the room:
If you tuned in to the Twitter Space on Sunday ‘Are mRNA injections causing cancers?’ hosted by Dr Kat Lindley and Neil Oliver, you would have heard a heated exchange between consultant orthopaedic surgeon Dr Ahmad Malik and London-based oncology professor, Angus Dalgleish. Dr Malik wanted to get to the bottom of why Professor Dalgleish felt moved to write an article advocating for young people to take the covid vaccine in July 2021 entitled:
What every young person who fears the jab MUST be told: Vaccine expert ANGUS DALGLEISH dismantles beliefs that have seen rates stall among the 18-30s
Well that seems like a pretty clear message. Get the damned vaccine.
Given his background in vaccine research, Prof Dalgleish would have been very clear that long-term safety data is not an optional extra when injecting young people or pregnant women. When questioned, Prof Dalgleish revealed that he did not actually write the article himself. There was a phone interview with a Daily Mail journalist, which he described as ‘bullying’ and the article was an entirely perverted representation of that call. Nonetheless, his name appears alongside the article with the effect that the message therein appears to come from a distinguished professor of medicine.
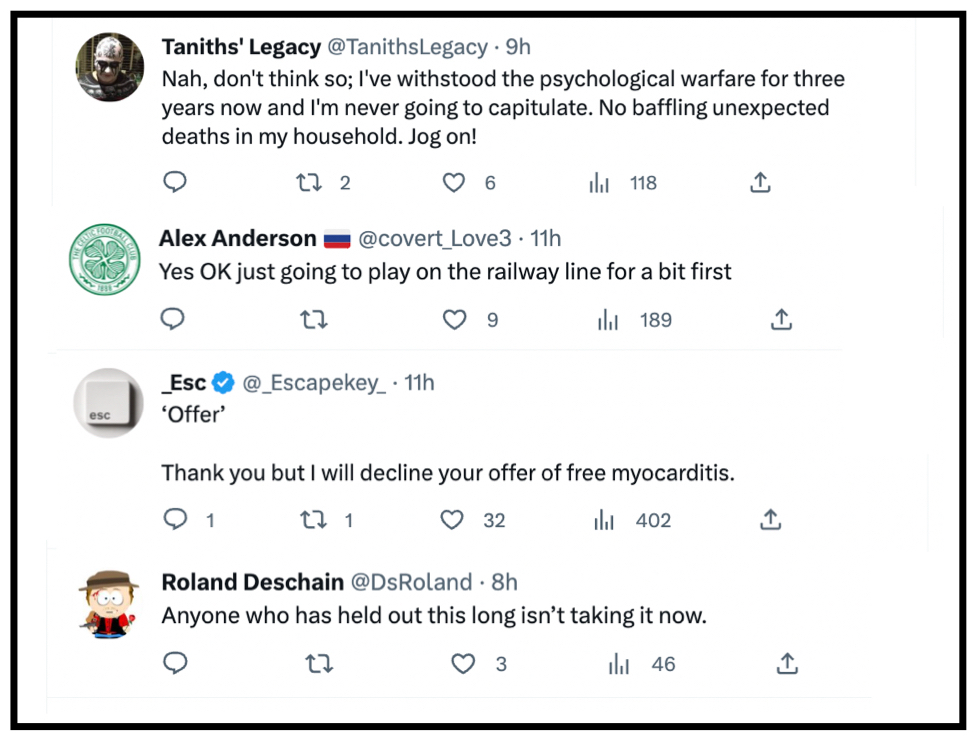
Professor Dalgleish dramatically revised his position on covid injections after his son suffered acute myocarditis following the shots. Whilst it is obviously a good thing that he was courageous and open-minded enough to change his stance, it is very worrying that he is still an outlier. One can count on one hand the working medics willing to speak out on this issue. And it begs the question, what if Professor Dalgleish’s son hadn’t been injured? Would there have been more advertorials in the Daily Mail with his name alongside? Why are journalists ‘bullying’ through a particular narrative on medical matters? This rather suggests they have a particular agenda. As one Dr Roger Hodkinson, an eminent Cambridge educated pathologist says, “when politics plays medicine, that’s a very dangerous game.” Notably Dr Hodkinson is now only available to view on Bitchute, having been deplatformed from the more mainstream channels such as YouTube. More media censorship of highly qualified counter-narrative voices.
Working for a monopoly such as the NHS, with a mortgage and a family to feed, one might well find medical ethics end up somewhere below personal financial obligations. This is regrettable but understandable. Medics are human beings. Perhaps it is the fault of an increasingly secular society that somehow medics have been elevated to demi-gods and as a result their word is often deemed infallible. However, many more people now realise that this is simply not the case. If this disordered power dynamic is to be realigned, certain conditions need to be met:
- A genuine admission that mistakes were made. Not that ‘The Science™’ changed. It did not change and millions of people who resisted the military grade psy-op are fully aware of this;
- An overhaul of medical training so that clinicians do not feel afraid to speak out when they see something is wrong, and in fact should be encouraged to do so;
- The gaslighting must stop altogether. Those who have suffered injury or trauma need to be given proper air time and have their concerns addressed. They also need to be properly and fairly compensated.
- Open and unfettered discussions need to take place, allowing medics to speak freely about what has happened during the past 3 years, identifying with honesty and integrity what must not be repeated.
Taxpayers spend in excess of £220 billion per annum on the NHS. Weekly excess deaths are presently consistently way above average, whereas after a period of high mortality in the frail and elderly it should be well below normal levels. The public (and indeed the staff) deserve better. If this is impossible, perhaps the entire system needs to be completely reimagined.
Footnotes
Insider reveals truth about Covid-19 pandemic from within the National Health Service
How the misdiagnosis of deaths occurred and was due to changes from 2016
The Naked Emperor’s Newsletter | January 15, 2023
An ex-director at one of the largest hospital trusts in the UK decided they wanted to reveal what really happened during the pandemic. They have kindly allow me to reproduce their thoughts. The catalyst for this revelation, according to the insider, was Dr. Malhotra speaking out about cardiac problems post vaccination.
This is an interesting take on what happened inside the National Health Service (NHS) and confirms, with more details, what we already knew and suspected.
Introduction (Long but important to understand the rest)
In 2016, the British Government proposed & piloted a change to the process of how deaths were certified across all hospitals in the UK. I have attached a link to this Department of Health (DoH) document.
The DoH document proposed a switch to the “Medical Examiner” (ME) System and was sent to a number of different audiences for feedback and consultation. The ME system was already being piloted at two hospitals up north. The results of the consultation are here.
Prior to the Covid-19 Pandemic, the death certification process involved treating doctors of a patient to attend Bereavement Services/Patient Affairs to discuss the death and either:
a) refer the death to the Coroner or
b) write a Medical Certificate of Cause of Death (MCCD).
The MCCD states the cause of death. Whereby a direct cause (1a) or contributing causes (1b) (1c) (1d) are stated along with co-morbidities (not directly causing the death) being written in (2) on the MCCD. The MCCD is only ever a probable cause of death, it is not definitive.
The only definitive way of determining an accurate and plausible cause of death is to refer the deceased patient to HM Coroner (if certain criteria is met), for HM Coroner to accept and take on the case, resulting in a Post Mortem (PM) being conducted by a Histopathologist. When a death is seen as natural and there is nothing untoward, the MCCD is written by the treating doctor of a deceased patient. Usually this is an F1, F2, SHO or Registrar that attends. It is rare for a treating Consultant to attend, but they will finalise the cause of death.
A strict hospital hierarchy exists within the NHS for doctors. It is as follows – from lowest to highest rank: Foundation Year 1 (FY1), Foundation Year 2 (FY2), Senior House Officer (SHO), Registrar (Reg), Consultant, Clinical Lead, Medical Director. Junior doctors will very rarely speak up or challenge their seniors. A senior decision is seen as final and it will be carried out and executed without any hesitance or questioning. In my 5.5 years of experience in End of Life Care, I have only ever seen one junior doctor disagree with a proposed cause of death and challenge their consultant.
With the number of deaths that occur in a hospital, as you can imagine, there is a great deal of variation with regards to causes of death, as we have numerous different doctors writing an MCCD and coming up with various different potential diseases in different orders.
The proposed ME system would change this, as the government would now hire and pay one Medical Examiner, to sit in every hospital and write all MCCD’s for all deceased patients. This would effectively eliminate any variation in causes of death.
In 2016, when I heard of this proposal, I worked as a Bereavement Officer at a hospital in Central London. My mentor/line manager at the time was a former Chief Nurse who managed Bereavement Services and all hospital deaths would be controlled by her and the department.
We essentially carried a huge amount of power with regards to decision making, as we would go through all patient notes following the death of a patient, and essentially guide and advise doctors on what would need to be written with regards to an MCCD or Coroners Referral.
In my personal opinion, our role was to sit on the fence and act in the best interests of a deceased patient (and their families), but also protect the hospital and our doctors from any potential negligence. As you can imagine many battles were fought over decisions about a cause of death of a patient or a referral to the coroner with a vast amount of doctors over the years.
F2’s and SHO’s were particularly the worst with regards to carrying an arrogance of knowing what should be written on an MCCD or stating that a patient didn’t need to be referred to the Coroner (often stating that their Consultant had given them instructions). It is worth noting that Consultants are also only human and can be incorrect at times too. We have to remember that they are succeeded in hierarchy by a Clinical Lead and beyond that a Medical Director. Who have far more experience and knowledge.
When I asked my mentor in 2016, how the ME system would change things, I was told that Bereavement Services/Patient Affairs would become purely administrative and that the clinical judgement would fall to the Medical Examiner.
The power and decision making with regards to MCCD/Coroners Referrals was being taken away not only from treating doctors but also from Bereavement Services/Patient Affairs/Bereavement Officers/Bereavement Service Managers/Directors of End of Life Care.
This decision making power was being handed solely to the Medical Examiner, who has not been involved in the treatment of a patient during an admission. I took all this information in at the time and acquired as much knowledge as I could from my mentor/line manager.
In 2016, I also happened to make a move and take up an opportunity to manage my own Bereavement Services at one of the largest hospital trusts in the whole of the UK. On average, I would oversee MCCD/Coroner Referrals for approx 1750 deaths on an annual basis. I developed a very close working relationship and friendship with one of the Medical Directors (a doctor with the highest ranking in a hospital). This was especially helpful when having to challenge doctors with regards to MCCDs/Coroners Referrals.
Progressing to Director of End of Life Care, I became involved with the reporting of mortality rates, conducting mortality reviews and writing hospital policies. I had also developed an excellent working relationship with the HM Coroner who oversaw our Trust. HM Coroner holds the power to investigate any hospital or trust with regards to a death or a number of deaths. A slight problem may arise, in that HM Coroner has an allegiance to the Crown and the Government.
When a death is reported to the Coroner. This was previously reported via telephone call by the treating doctor. A discussion was had with the Coroners Office and a direct outcome and instruction would come from the Coroner’s Office, by way of HM Coroner (via a phone call).
There is a fundamental flaw to this system, as there is no documentation of the decision and instruction from the Coroner’s. It comes via word of mouth. There is always room for error without any electronic documentation. Every Hospital/Trust & HM Coroner will have a different system of reporting deaths. I personally made a decision to safeguard my hospital and the trust, by developing an electronic coroners referral form, which I proposed to our Coroner and developed after their agreement. We now had documentation of every death being reported and every outcome.
When reporting a death, the Coroner will look at a proposed cause of death and accept it, or reject the cause of death and take on the case (death of the patient), leading to an Inquest or a PM.
In 2019, our Medical Director, came into my office one morning and stated that the Board of Directors at the Hospital had made a decision to switch to the Medical Examiner System. Hearing the words ME system was a massive case of Déjà vu (conversation with my mentor in 2016). I knew exactly what the ME system was, but I chose instead, to play the fool and enquire what exactly the ME system was and what it meant for our service, my staff and our roles. Everything the Medical Director mentioned to me that day was a carbon copy of what I already knew
I knew that my time in End of Life Care had come to an end. I’d reached the top and there was no more progress for me. Losing all power and decision making to any ME coming into the hospital did not appeal to me. I’d already made up my mind that I needed to leave. Seeking a new challenge and experience, I made a move in 2019 to another major hospital in Central London, this time side tracking into operational management. I was in charge of the operational management of Nephrology, Rheumatology, Dermatology and Diabetes & Endocrinology.
2020 – Covid Arrives
In Jan 2020, I remember hearing about the first case of Covid-19 at our hospital, with a patient arriving from China and walking into our A&E. A&E was shutdown and steam cleaned that day, I recollect the moment I heard about this. In my mind, I saw the reporting of Covid-19 in the media as nothing more than Bird Flu or Ebola, which had caused panic but yet passed. I wasn’t worried in the slightest bit.
Things began to escalate around in Feb 2020, around the time I was going on holiday. Due to the reporting by the media, I bought N95 masks as a precaution for my trip and to give to my parents and younger sister. I was blessed to have had an opportunity to spend a few days in Sri Lanka for a wedding and then nearly a whole month in Australia (March 2020). I watched as the narrative of a deadly infectious disease continued to grow with every day that passed. I made a decision to cut my holiday short by a couple of days so that I could make sure I got back to my family and not end up being stranded in Australia.
Upon returning to the UK in late March 2020. One of the immediate things that struck me was the lack of any temperature monitoring or questioning at Heathrow Airport. This seemed odd for a potentially deadly infectious disease that was spreading around the world. This was especially odd, as Sri Lanka & Australia had questioned me/checked temperatures upon arrival, with even Singapore monitoring temperatures during transit.
My mother had just recovered from Cancer, my father was over 70 and my younger sister was born with Down’s Syndrome alongside having multiple other conditions. I had three high risk individuals to Covid-19 in my family and I was scared/fearful of giving them Covid-19. I asked my hospital to allow me to work from home. They refused. I wasn’t deemed high risk, although I lived with my parents at the time. I needed to help my mum and my sister. The hospital held no regard for the safety of it’s employees. They forced me to come into work. I spent two months isolating in my bedroom, I barely came out of my room, for fear of spreading an infectious disease. Never once did I think about the situation or my prior experience or knowledge, I was just reacting to the media frenzy. I was full of panic and stress.
The first irregularity I noticed, was the government and media stating that Covid-19 was an infectious disease. However just before the first lockdown was implemented, I noted that the government had downgraded the status of Covid-19 stating it was no longer infectious. This made no sense to me. Why would we need to isolate if they downgraded the status? My circle of friends contained many medics and dentists. They were all panicking at the time, saying they had inadequate surgical masks and that they needed N95 masks.
N95 masks were seen as the only way to prevent medical professionals from becoming infected with Covid-19. The public being asked to wear surgical masks made no sense to me. The virus would be able to go straight through. Something didn’t seem right.
I ended up meeting and dating an FY1 doctor (my ex gf) around October 2020. We clicked because she was different from every other doctor, I had previously spoken to about Covid-19. She also had her suspicions and believed it wasn’t as infectious as it was made out to be. We both started to slowly realise that Covid-19 was a real disease (as it was showing up on X-rays in patients) but that it wasn’t infectious at all [NE – I have since confirmed with them that they mean not as infectious as was being made out], despite all the reporting in the media.
I needed to experience working in a Covid-19 hotspot and see all the action for myself. In March 2021, I quit my job at the hospital in Central London and took up an opportunity to manage A&E and AMU (Acute Medical Unit) at a hospital in South London. The 6 months that I spent working in A&E/AMU confirmed all my suspicions and culminated in my decision to end my career in the NHS.
The entire 6 months, I was not tested once with a PCR Test, despite walking into wards full of Covid-19 Positive patients on a daily basis. Yet we were required to test multiple times when visiting another country.
The PCR Test that the NHS was using to test patients, is known to have false-positive results. This is shown in numerous studies which can be found online, an example of which is:
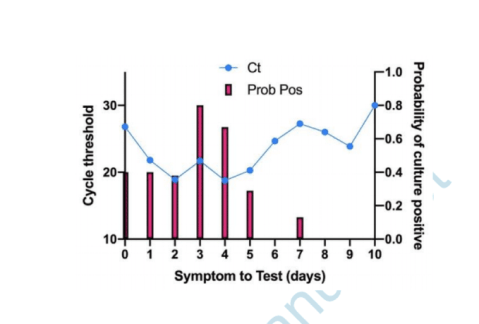
Are you infectious if you have a positive PCR test result for COVID-19? – The Centre for Evidence-Based Medicine.
If a patient tests positive for Covid-19 with a PCR Test, this doesn’t mean they are infected. If tested again, they may well turn out with a negative test. However in the NHS, patients are only tested once and this stays on their record throughout their admission. Hospital policies were changed alongside the implementation of the Medical Examiner System, to ensure that any patient who died within 30 days of positive test, would have to have Covid-19 as their primary cause of death. This was regulated by the Medical Examiner.
The highest cause of death at every hospital per annum pre Covid-19 is Pneumonia. Pneumonia is a Respiratory Disease like Covid-19. Pneumonia can be broken down into 4 different causes of death: Bronchopneumonia, Aspiration Pneumonia, Community Acquired Pneumonia & Hospital Acquired Pneumonia.
These four causes when added together kill the largest number of people on an annual basis prior to the pandemic.
The Medical Examiner (one individual in each hospital), was certifying all these Pneumonia deaths as Covid-19 deaths. When 4 different diseases being grouped and now being called Covid-19, you will inevitably see Covid-19 with a huge death rate.
The mainstream media was reporting on this huge increase in Covid-19 deaths due to the Medical Examiner system being in place. Patients being admitted and dying with very common conditions such as Old Age, Myocardial Infarctions, End Stage Kidney Failure, Haemorrhages, Strokes, COPD & Cancer etc were all now being certified as Covid-19 via the Medical Examiner System.
Hospitals were switching to and from the Medical Examiner system and the Pre Pandemic System as when they pleased. When Covid-19 deaths needed to be increased, the hospital would switch to the Medical Examiner System. Doctors were one week being told they needed to complete an MCCD, to then be told the following week that they weren’t required to fill out an MCCD, as the Medical Examiner was handling this.
Hospitals were incentivised to report Covid-19 deaths over normal deaths, as the government was paying hospitals additional money for every Covid-19 death that was being reported. The Medical Examiner system ensured that Covid-19 was being put down as the cause of death. The government sends out the annual NHS budget to Primary Care Trusts. This is split to fund Hospitals and GP Surgeries. A clinical coding team at each hospital will assign codes to each treatment or death, so that money is paid out to the hospitals.
Any doctor who argued against Covid-19 as a cause of death was bullied and vilified. The General Medical Council maintains a register of all doctors within the UK. This ensures that there is a fear of being struck off for speaking out against an agenda. The GMC effectively controls all doctors in the UK. Even if a doctor realises what is going on and wants to speak out. They will think twice about talking, as they would be risking their entire career and everything that they’ve worked so hard for.
Doctors essentially have their hands tied, many have families, kids, mortgages and mouths to feed. If I was in their situation, I would think twice about speaking out, for fear of being struck off by the GMC and losing everything.
The NHS Track & Trace App, which was introduced to try and control the spread of the virus, did not apply to medical professionals. We were all asked to turn this off, as Doctors and staff isolating for 14 days disrupted patient flow, beds and the discharge of patients.
Any doctor that I spoke to regarding taking the Covid-19 vaccine, were insistent that they were going to wait for a period of time, before taking it themselves, to ensure that it was safe. How is it ethical to give a vaccine to your patients, but not want to take it yourself? In my 12 years of NHS service, never has a doctor pushed or influenced the public to take a vaccine. Yet on social media, I was seeing close friends who were doctors, starting to post on social media that they have taken the vaccine and that the public should. I wouldn’t be surprised if doctors were being forced to promote the vaccine by their superiors or if they were receiving monetary gain in doing so.
I have no doubt in my mind, that the Government has planned the entire pandemic since 2016, when they first proposed the change to medical death certification. Stress leads to disease and illness. Panic leads to people following whatever orders and instructions that are given to them by authority, such as prolonged mask use, which leads to an increase in admissions in to the NHS system due to hypoxia and bacterial pneumonia.
The NHS treatment pathway involved patients being placed onto ventilators. There is a 50% chance of death from this clinical decision alone. How many innocent people have died from the clinical decision to place them onto a ventilator.
During boardrounds (where every admitted patient is discussed), we were seeing patients on a daily basis being admitted due to suffering from adverse affects of taking the vaccine. Patients were blacking out after taking the vaccine or suffering from clots or strokes.
The NHS is all about money and making money. The safety of a patient didn’t seem like the most important thing. It was more about how do we make more beds available so that another patient can be treated. Patients with no next of kin are discharged to nursing homes with care packages. I can’t comment on what happened to these patients in nursing homes, during the pandemic, as I have no experience of their inner workings.
Patients are seen as money, even upon death, hospitals receive money for each death. Is there an actual concern for patient health and safety? I know numerous doctors who are driven primarily by money and monetary gain.
THE REASON WHY I LEFT THE NHS in 2021
56 yr old male, admitted into A&E with end stage kidney failure, has a previous history of regular dialysis treatment for this. No respiratory symptoms on admission and no temperature. However when tested with a PCR Test he unfortunately tests positive. This stays on his record throughout his admission. Our hospital is relatively small in comparison to others I have worked at, we have no dialysis machine as a result. We urgently need to transfer this patient to another hospital otherwise this patient will die. Our treating doctor calls up larger hospitals with a dialysis machine to organise his transfer. All doctors pick up the phone and request the Covid-19 status of the patient. A transfer is declined due to a Covid-19 infection protocol. Our doctors again reiterate the point that this patient will die without dialysis. We are told there is nothing that can be done and that the patient cannot be accepted for transfer.
This gentleman ended up dying without dialysis. Now please tell me what goes on the MCCD….
1a) Covid-19
2) End Stage Kidney Failure
Not written by the treating doctor who disagreed with this cause of death, but by a medical examiner, put in place by the government and the hospital.
When innocent people are being killed by a corrupt organisation and system, for pure monetary gain, I can’t stand by and be part of this anymore. My conscience was clear and I no longer wanted to be a part of this anymore. I am very blessed and lucky that I was in a position to walk away. I’ve been able to speak out, because my hands are not tied and I am not regulated by any organisation or governing body. I believe in speaking the truth and in doing so, I am only just an instrument for God.
I joined the NHS, 12 years ago because I had a desire to help those in need, but the moment I realised that I was not doing this anymore was the time for me to walk away. I apologise to you all if the above thread is confusing with regards to terminology or you cannot understand it’s contents. I’m hoping that at the very least, it can be understood by my fellow medical professionals or by journalists who would like to report the truth.
Open Letter to Therese Coffey Urging Her to Apologise to the Care Workers Forced Out by Vaccine Mandate
BY TOBY YOUNG | THE DAILY SCEPTIC | OCTOBER 10, 2022
Campaign group Together’s latest campaign, an Open Letter to Health Secretary Therese Coffey urging her to “Apologise, Reinstate, Compensate the 40,000 Care Workers Forced Out by Covid Jab Mandate” has attracted over 10,000 signatures within a few hours of going live. Here is an extract:
Forcing out approximately 40,000 social care workers for declining the Covid jab was not just unethical, but disastrous for the care sector and those it supports. The sector now has 165,000 vacancies, with 500,000 members of the public waiting for assessments, care or reviews. The situation is grave and urgent, not least as without a functioning care sector the NHS will collapse.
Failure to respect bodily autonomy was wrong in principle. ‘No jab, no job’ amounted to blackmail. But even on a practical level, the ‘mandate’ policy was always illogical and ill-advised.
For starters, natural immunity was totally ignored as a factor – for reasons that remain unclear. Throughout most of 2021 it was clear that Covid jabs did not prevent transmission and by October, the Guardian was explicitly reporting that ‘research reveals fully vaccinated people are just as likely to pass (the) virus on… whether an infected individual is themselves fully vaccinated or unvaccinated makes little or no difference to how infectious they are to their household contacts’. This alone should have been enough to kill off this divisive policy. Yet, seemingly oblivious to the actual scientific data, your predecessor Sajid Javid took to television the same month, belligerently ‘warning’ care workers ‘if you cannot be bothered to go and get vaccinated then get out… go and get another job.’
On November 9th 2021, the Department of Health and Social Care warned Javid that his ‘mandate’ policy would result in upwards of 40,000 care staff leaving the sector. He persisted with it anyway, and on 11 November workers who had not already been forced out were sacked in droves. Many lost not only their jobs, but also their pensions.
Already a range of well-known people including Prof Carl Heneghan, journalists Allison Pearson and Julia Hartley-Brewer, author and broadcaster Laura Dodsworth, Richard Tice of Reform UK and Laurence Fox of the Reclaim party, medics Dr Tony Hinton, Dr Renee Hoenderkamp, Dr Clare Craig and Dr Teck Khong, and sportsman Matt Le Tissier, have all signed.
You can read the Open Letter in full and sign it here.
The NHS just edited their Monkeypox page… to make it scarier
OffGuardian | May 24, 2022
Afew days ago the UK’s National Health Service (NHS) edited their Monkeypox page to alter the narrative in a few key ways.
Firstly, they removed a paragraph from the “How do you get Monkeypox?” section.
Up until a few days ago, according to archived links, the Monkeypox page said this, regarding person-to-person tranmission [emphasis added]:
It’s very uncommon to get monkeypox from a person with the infection because it does not spread easily between people.
… this has now been totally removed.
Secondly, they’ve removed this paragraph, which was present up until at least November of 2021 (and maybe much more recently, there are no archives between November and May) [emphasis added]:
[Monkeypox] is usually a mild illness that will get better on its own without treatment. Some people can develop more serious symptoms, so patients with monkeypox in the UK are cared for in specialist hospitals.
The new “treatment” paragraph reads [again, emphasis added]…
Treatment for monkeypox aims to relieve symptoms. The illness is usually mild and most people recover in 2 to 4 weeks […] You may need to stay in a specialist hospital, so your symptoms can be treated and to prevent the infection spreading to other people.
So, they remove that it will “get better on its own”, and again reinforce the idea of spreading the disease despite this being described as “very uncommon” as recently as last week.
They even add a line about self-isolating, which was never mentioned before:
as monkeypox can spread if there is close contact, you will need to be isolated if you’re diagnosed with it.
Finally, they now include a warning you can get Monkeypox by eating undercooked meat, which will doubtless feed into the anti-meat narrative too (oh, wait, it already is).
To sum up, history is being re-written a little here.
Before, monkeypox “did not spread easily between people”. Now it does.
Before, monkeypox would “get better on its own without treatment”. Now it won’t.
It’s early days to say that Monkeypox is going to be the “new Covid”, and maybe this rollout will stall and be forgotten in a couple of weeks, but there’s no doubt they are taking some tips from the Covid playbook so far.
If Hospitals Are Currently Under Pressure, They Only Have Themselves to Blame
By In-house doctor | The Daily Sceptic | April 10, 2022
There follows a guest post by our in-house doctor, a former senior NHS medic, who says the latest ‘perfect storm’ causing pressure on the health service in parts of the country is more a self-induced squall.
In the middle of last week, several NHS Trusts issued warnings about the acute strain their services were under. The South Central Ambulance Service went so far as to declare a critical incident – normally reserved for a situation in which demands on the service exceed the capacity to manage those demands. I was surprised that so many NHS bodies spread over a wide geographical area issued public warnings about their failure to cope at the same time. Statements referred to high demand on services (hardly news) and lacked any specific detail about critical capacity constraints. Accordingly, the Daily Sceptic asked me to interrogate the available data to work out the extent to which a Covid resurgence might be responsible for the latest ‘perfect storm’ to hit the NHS.
Graph 1 shows daily admissions of Covid positive patients from the community. Admissions have risen in the last few weeks, but seem to be tailing off. Data from Graph 1 have been the subject of hysterical articles in the mainstream press implying the latest Omicron BA.2 subvariant may be triggering a new wave of acute Covid infections. It’s not sensible to interpret Graph 1 as a stand-alone figure without considering contextual information from other datasets.

Graph 1
Graph 2 for example shows information from the Primary Diagnosis dataset. Regular readers will recall this set shows the numbers of patients admitted suffering from acute Covid compared to the patients testing positive for Covid but admitted for another condition. The grey line shows the ratio is gradually falling – in other words the headline figures in Graph 1 are misleading, because nearly 60% of those patients are not actually ill with Covid but admitted for other reasons.

Graph 2
Graph 3 shows the numbers of patients testing positive for Covid in intensive care departments. The rise in cases seen in Graph 1 since the beginning of March 2022 is absent – so although there are more hospital inpatients testing positive for Covid than at the end of February, they are not ending up in critical care. Further, the data from the most recent ICNARC report reveal that the latest tranche of Covid ICU patients have lower oxygen requirements and better respiratory ratios than the cohort from this time last year – in other words, they are not as acutely ill.

Graph 3
Graph 4 is very instructive. It shows the average length of stays of Covid patients up to the end of December 2021. This data was released in March and unfortunately is only complete up to the end of 2021, but it is reasonable to infer that current length of stay is unlikely to be worse now than in December of 2021, due to increased availability of new monoclonal antibody drugs which reduce disease severity for the highest risk patients. Graph 4 expresses average length of stay as the mean average (blue bars) and the median average (orange bars). Both these averages are steadily reducing with the median length of stay being down to four days by the end of December 2021. For the information of statistically curious readers, the median average in this case is probably more representative of the situation as the mean average can easily be skewed to the upside by a small number of very long-stay patients.

Graph 4
Overall, from the available Covid-specific patient data, we see a rise in total positive Covid tests on admission from the community, but fewer than half of these patients are symptomatic for Covid. Very few patients are ill enough to need ICU care and the length of stay for acutely ill Covid patients continues to fall. The vast majority require a few days of supplementary oxygen, intravenous steroids and monoclonal antibody infusion (or other adjunctive therapies) before being fit to discharge. So where is the problem?
Last week Saffron Cordery, deputy CEO of NHS providers, commented that staff absences played a part in the current crisis. Graph 5 shows the data for Covid related staff absences up to March 2nd (the latest figures released) – they don’t seem to have changed much lately and were on a downward trend since the turn of the year. It’s possible they may have started to increase again, but the figures are not yet released for public scrutiny.

Graph 5
My personal suspicion is that Graph 6 shows the main issue causing trouble in hospitals. Graph 6 shows the number of patients in hospitals deemed medically fit for discharge. It is shown as a stacked bar chart, so the blue bar represents the patients who actually were discharged and the orange bar shows patients who were fit for discharge but had to remain in hospital for administrative reasons (often referred to as ‘bed blocking’). Readers will readily notice the ‘weekend effect’ in the figures, and that about 11,000 patients per day are in hospital when they are fit to be discharged – about 10% of the total NHS bed stock.

Graph 6
Over two years into the pandemic, the NHS does not yet seem to have solved fundamental administrative problems in relation to patient flow through the system. I am also aware from personal communication with colleagues that most NHS trusts are still imposing unnecessary Covid protocols which add to the time taken to complete basic episodes of care such as routine operations. This reduces efficiency still further in a healthcare system not renowned for operational efficiency in the first place.
Speaking about the latest crisis, Mark Ainsworth, Director of Operations at the South Central Ambulance Service, said declaring a critical incident meant it could focus its resources on the neediest patients.
Discharging medically fit patients from hospital and exercising a modicum of common sense when compiling Standard Operating procedures might achieve the same effect.
The UK wants to criminalize “misinformation” online as its own health service gets caught posting falsehoods
By Dan Frieth | Reclaim The Net | February 11, 2022
Less than a week after the UK proposed criminalizing the posting of some types of “knowingly false” information online, England’s National Health Service has taken down a social media video over inaccurate information.
Last week, NHS England posted a video on its Twitter account with more than half-a-million followers to promote vaccination in kids.
The video claimed that 1% of children will be hospitalized because of Covid, 136 kids in the UK had died because of Covid, and 117,000 children have “long Covid.”
The video went viral attracting comments and retweets from some of the most popular influencers in the health category.
But some, including Dr. Robert Hughes, a clinical research fellow at the London School of Hygiene & Tropical Medicine, questioned the accuracy of the data.
“As both a parent and scientist who has been involved in research on symptom duration and severity of covid in children, the cited statistics didn’t make sense to me,” Hughes wrote in an article in UnHerd. “The idea that 1% of children with Covid are hospitalized for it didn’t pass the ‘sniff test.’”
The video also shared the story of a kid aged 11 that was suffering from long Covid. According to Hughes, the story contradicted the vaccination guidance in the UK, as it does not even recommend vaccination for that age group.
Additionally, there is not yet any substantial evidence to support that the vaccine prevents long Covid.
Hughes also notes that NHS England was silent when he and others questioned the accuracy of the data.
“Several people agreed with me, sharing their working for why these numbers are at best long outdated, may be orders of magnitude out, and risk undermining confidence in vaccine communications and uptake.
“But others seemed to dig in, praising both the content and tone of the messaging when challenged, and directing the discussion into an important, but different, one about the merits of extending Covid vaccination to children rather than the need for accurate and honest communication about vaccination,” Dr. Hughes wrote for UnHerd.
Hughes contacted the Office of the Statistics Regulator about the numbers. The Statistics Regulator agreed that it was important that the NHS provides accurate figures.
“It is important that figures provided by NHSE&I are accurate and reliable,” the Office of the Statistics Regulator said. “In this case the claim made in the video fell short of these expectations – we contacted NHSE&I and it acknowledged that the data were historic and had methodological shortcomings. We are therefore glad that the content has now been removed from Twitter.”
Before its removal, the video had already been widely shared.
Featured Video
America Racing to Strategic Defeat in Iran
or go to
Aletho News Archives – Video-Images
From the Archives
Should Europeans ‘Thank’ the Americans for Destroying Nord Stream?
By Robert Bridge | Strategic Culture Foundation | September 29, 2022
With an investigation continuing into the destruction of the Nord Stream gas pipeline that provided energy supplies to Europe from Russia, there appears to be just one prime suspect, and that should surprise nobody.
Following the sabotage of the Nord Stream 1 and 2 gas pipelines, former Polish Foreign Minister Radoslaw Sikorski already seemed to know the identity of the perpetrator when he tweeted out: “Thank you, USA.”
At first glance, it seemed that Sikorski was speaking sarcastically, berating Washington for carrying out an attack that will have severe repercussions for the people of Europe. After all, how could anyone see any good coming from the termination of Europe’s primary source of gas reserves with winter just around the corner? It was Sikorski’s homeland of Poland, after all, that urged its citizens to collect firewood in the face of dwindling gas reserves.
In fact, the Polish diplomat was speaking one-hundred percent literally… continue
Blog Roll
 Aletho News
Aletho News- Growing insecurity, soaring prices fuel protests in north as regime bans evacuation: Sources
- Iran denies responsibility for ‘depraved’ attack on Kuwait desalination plant
- Bring The Troops Back. End This War Now!
- Can we please stop calling Israel the ‘only democracy in the Middle East’ now?
- US should start removing its troops from Germany, proposes AfD co-leader Chrupalla
- Iran Red Crescent: 600 educational centers attacked in US-Israeli ‘war crimes’
- Russian Oil Tanker Arrives in Cuba Amid U.S. Blockade
- America Racing to Strategic Defeat in Iran: Lt Col Daniel Davis
- FTC Warns Visa, Mastercard, PayPal, Stripe Over Political Debanking
- Russian tanker approaches Cuba despite US oil blockade
- If Americans Knew
- Israeli police block Catholic cardinal from entering Church of the Holy Sepulchre on Palm Sunday
- Israel is assassinating journalists again, more than any other nation, anywhere, ever – Not a ceasefire Day 170
- Over 300 US service members wounded, majority have brain injuries – Not a ceasefire Day 169
- Researchers at Human Rights Watch Resign Over Blocked Report on Palestinian Refugee Return
- Jewish Groups Are Backing a War Americans Don’t Want
- Eric Fingerhut Thinks He’s the President of the Jews
- Top Jewish Philanthropists, Rabbis Urge Israeli President to Take Action Against ‘Jewish Extremists’
- Don’t Be Fooled. Zionist Leaders Have Always Wanted to Control Southern Lebanon
- Israel’s widespread use of torture is a core element of its genocide against the Palestinian people
- In Israel’s War on Iran, Many Middle East US Bases Rendered “All But Uninhabitable”
- No Tricks Zone
- New Study Finds Warming Saves Lives…Cold Temperatures 12 Times More Deadly Than Excess Heat
- German Science Blog Accuses PIK Climate Institute Of Hallucinating Climate Tipping Points
- Devastating Assessment Of Comirnaty Vaccine By Former Senior Pfizer Europe Toxicologist
- New Study: CO2 Is ‘Effectively Negligible’ As An Explanatory Climate Change Factor Since 2000
- Former Pfizer Toxicologist Dr. Helmut Sterz Tells Bundestag Hearing Pfizer Vaccine Should Have Never Been Approved
- Energy Expert: Germany’s Nuclear Phaseout Was A “500 Billion Euro Mistake”
- New Research: South Australia’s Mid-Holocene Sea Surface Temperatures Were 4°C Warmer Than Today
- Storing Green Energy To Last Germany 10 Days Would Require A 60-Million Tonne Battery
- New Studies: UK Sea Levels Were 4 Meters Higher Than Today During The Mid-Holocene
- Destructive Green New Deal: German Energy And Metal Group Warns Of Drastic Crisis
