In the U.K. we are facing threats once again of restrictions and vaccine passports being imposed over winter should the prospect of an ‘overwhelmed’ NHS be sounded by the Government’s medical advisers in the coming weeks.
But how realistic is this threat of health service ‘collapse’? South Korea is currently providing an object lesson in how the concept appears to be very much in the eye of the beholder.
The South East Asian country has been experiencing a spike in reported infections in recent weeks as the Delta variant has become dominant, hitting over 3,000 in one day for the first time on September 24th.
Three thousand ‘cases’ is very low, of course, compared to our 30,000 or so since early July, and the country is similar in size to the U.K., with a population of 52 million to our 67 million.
While the country does do less testing, deaths are also very low, with daily confirmed deaths currently between just five and 10 a day.
Excess mortality has also remained low throughout the pandemic, currently sitting at around 6% having been negative over the winter.
Despite these enviable Covid stats, though, the country is currently living under various Covid restrictions and the Government has said that while it plans to reopen, it will reverse course should ‘cases’ go above 4,000 per day. Why? According to the Government’s Minister of Health, Kwon Deok-cheol, the South Korean “healthcare system would not be able to cope with 4,000 or 10,000 new confirmed cases per day”.
At a Korea Broadcasting Journalists Club roundtable on Tuesday, Minister of Health and Welfare Kwon Deok-cheol said that South Korea’s medical response system would be “sufficiently capable” of handling a daily caseload of 3,000 or more confirmed cases and that the country would be able to proceed with a gradual return to everyday life, provided that the Government’s late-October targets of fully vaccinating 80% of adults and 90% of senior citizens are met.
He also said that the shift toward a “living with Covid” approach was not hasty, noting that while the U.K. began its gradual return to normal life while its full vaccination rate was just 1.6%, whereas South Korea had a full vaccination rate of 46.6% as of Tuesday.
But he also noted that observation of basic disease prevention guidelines such as wearing masks indoors and regularly ventilating indoor spaces would remain necessary, saying that “our healthcare system would not be able to cope with 4,000 or 10,000 new confirmed cases per day.”
“For that reason, we are considering a phased easing [of restrictions] – based on business types, for example – rather than a full-scale elimination [of said restrictions],” he added.
Vaccine passports are also being considered, apparently in order to protect the unvaccinated.
The South Korean government similarly explained that with the 976 critical care beds and 10,212 beds for patients with moderate symptoms that it had secured as of Tuesday, the South Korean healthcare system would be able to cope with as many as 3,500 new confirmed cases per day.
In addition to relaxing restrictions on private gatherings for fully vaccinated people and gradually removing restrictions on the use of multipurpose facilities, Kwon also said consideration was being given to the adoption of “vaccine passes,” where only fully vaccinated people or other restricted categories of people would be allowed to use certain establishments during the initial stages of the gradual return to everyday life.
He went on, saying that Germany grants permission for indoor events or use multipurpose facilities such as hospitals, long-term care facilities, nightlife establishments, and cinemas only to people who present a pass that certifies they have been either fully vaccinated, have tested negative for Covid, or have fully recovered from a previous Covid infection.
“With confirmed cases currently being observed among unvaccinated people – many of them leading to critical symptoms and even death – we are considering applying such an approach, if only to protect these people,” he said.
I have to say it is bizarre to read the same worries about ‘cases’ getting too high and putting unsustainable pressure on the health service in a country which is experiencing a fraction of our reported infections and an even smaller fraction of our deaths. How can we take this seriously when South Korea has more than three times the number of hospital beds that the U.K. has, 10 per 1,000 population compared to three per 1,000?
Nations whether in the East or West are now being held hostage by their health services and their supposed capacity to cope with coronavirus surges. But it’s clear from the very different scales of these supposed capacity threats in different countries that this spectre of an overwhelmed and collapsing health service is largely a figment of the political imagination.
No doubt a winter Covid wave can stretch a health service considerably. But if even England in January had thousands of empty hospital beds on January 18th, when the number of Covid hospital patients hit 39,254, and did not ‘collapse’ (and the Nightingale hospitals remained empty), then it’s difficult to see how the threat is in any way a realistic one. At that winter peak, Covid patients occupied less than a third of the total hospital beds (31%), while 8,696 beds remained unoccupied. Besides which, if winter hospital capacity is the crucial issue for lockdowns and other measures, would it not be a whole lot cheaper and more effective just to boost it more?
Lockdown proponents will claim that the U.K. winter wave was mitigated by restrictions. But the truth is the U.K. suffered one of the biggest winter surges in the world, regardless of what measures were in place in other countries. States in America with few or no restrictions such as Florida and South Dakota, and light-touch Sweden, did not suffer worse winters. There is thus nowhere that lockdown proponents can point to and say, look, that’s what would have happened here if we hadn’t locked down. There is no reason to think that without restrictions the U.K.’s winter surge would have ended up much worse.
While governments around the world continue to hold the threat of an overwhelmed health service over their populations as a kind of political blackmail (albeit often sincerely believed), the experience of South Korea shows that the threat is ill-defined, largely illusory, and not a sound basis for imposing illiberal measures and ruinous restrictions.
The UK Ministry of Defence has inadvertently revealed its plan to spy on social media platforms in order to detect “change(s) in population sentiment.”
Despite ostensibly being about “better use of existing silos,” the MoD’s Data Strategy for Defence document explains how the military should move towards “Automated scanning of social media platforms” to detect “change in population sentiment.”
“Nowhere does the document explain why a strategy paper has gone so far off the beaten track that it promotes collecting data the MoD doesn’t have and using it for decidedly non-military purposes,” reports the Register.
Since the beginning of the COVID pandemic, the military has increasingly turned its attention inward towards its own citizens rather than doing what it should do, which is fighting foreign adversaries.
As author Laura Dodsworth revealed, GCHQ has embroiled itself in anti-vaccine and anti-lockdown messaging by targeting people who challenge the official COVID narrative online.
“She says some people believe they have been targeted by the 77th Brigade, part of the 6th Division of the Army,” reported the Telegraph.
According to the Ministry of Defence, the 77th Brigade uses “legitimate non-military levers as a means to adapt behaviours of the opposing forces and adversaries.”
The military’s main “adversaries” are now apparently British citizens who complain about lockdown while questioning the efficacy and safety of vaccines.
Dodsworth said she “hit a brick wall” when attempting to get answers about the unit’s activities, noting, “and I find that when someone puts up a brick wall, it’s because that’s where the real story lies.”
The unit played its role in the broader agenda, facilitated by government-affiliated behavioral psychologists, to terrify the public into mass obedience to lockdown rules by exaggerating the threat posed by COVID.
The plan, devised by the Canadian Joint Operations Command, relied on propaganda techniques like those used during the Afghan war. What on earth is going on in the upper echelons of Ottawa?
High-up elements of the Canadian Forces have been waging psychological operations on the public over Covid-19 to manipulate their emotions and thoughts, and to gauge their reactions. While this is not uncommon around the world, getting caught is.
A new article in Canada’s National Post states that the Canadian Joint Operations Command used “propaganda techniques similar to those employed during the Afghanistan war” on the Canadian public.
The Post cites a December 2020 investigation by retired Major-General Daniel Gosselin, who was asked to look into it by then-Chief of the Defence Staff General Jon Vance.
According to the article, the federal government was innocent and not aware of the plan – a claim I find unbelievable, considering the amount of gaslighting and knowingly pointless regulations the government has subjected Canadians to since the start of the pandemic scare.
The plan involved “shaping” and “exploiting” information, the Post noted, to “head off civil disobedience by Canadians” and “bolster government messages about the pandemic.”
Among the stranger aspects was scaring Canadians with stories of a wolf invasion.
This, according to the Post, involved Canadian Forces’ military information operations staff forging a letter from the Nova Scotia government warning about wolves on the loose, in September 2020.
The Post claims the letter’s release was inadvertent, and basically ran with the Canadian Forces’ claim that this was down to a few bad apples, reservists who “lacked formal training and policies governing the use of propaganda techniques.”
Canadian journalist Dan Dicks, who was among the first to report on and analyze the wolves story, noted at the time that it was a classic example of a psychological operation.
Dicks has also pointed out what the National Post omitted, highlighting:
“They created a fake letter from the government saying there are dangerous wolves, and they set up loudspeakers in the area, projecting out wolf noises. This isn’t just research, this isn’t just a training exercise, they’re actively engaging in this psychological operation to scare people using loudspeakers.
‘Psyops’, he noted, is a term used “to denote any action which is practiced mainly by psychological methods with the aim of evoking a planned psychological reaction in other people,” and they are “aimed at influencing a target audience’s value system, belief system, emotions, motives, reasoning, or behaviour.”
Canadian journalist James Corbett likewise commented on this at the time, pointing out how a rumour is floated to see how the public reacts:
“This entire coordinated campaign to convince an entire public of a threat that doesn’t exist, in order to test how they will react to that, what will the public respond to and how will they respond? That really speaks volumes to the world we are living in. And you really think they are going to do all of that, but they are never going to use that for any nefarious purposes?”
An article in the Ottawa Citizen noted at the time that Canada’s Department of National Defence claimed: “The fake letter wasn’t meant to be released to the public and an investigation is underway to determine how that happened. The letter was an aid for the propaganda training.”
The department also claimed to not know why the loudspeaker was set up to transmit wolf sounds.
I guess a member of the public who read the letter must have taken it upon themselves to set up the loudspeaker then, hey?
The same Ottawa Citizen article cites Bard College professor Emma Briant, who specializes in researching military propaganda, calling the stunt a “major violation of ethics.”
UK “anti-masker” razor-blade poster hoax
The “shaping” and “exploiting” of information on Covid-19 to gauge and shape the public mood is, of course, not unique to Canada. To give another example, in May 2020, the UK Column obtained a leaked internal document of the Scientific Advisory Group for Emergencies (SAGE) from March 26, 2020, which advised:
“Use the media to increase the sense of personal threat. Use the media to increase the sense of responsibility of others. Use the media to promote positive messaging around actions. Tailor the messaging and use and promote social approval for desired behaviours.”
I recently spoke to UK-based journalist Iain Davis on a variety of issues pertaining to fear porn and media hype around the issue of Covid-19.
In our interview, Davis spoke of another hoax that appeared on the BBC last July: a Cardiff woman who claimed she had been cut by a razor blade allegedly stuck on the back of an ‘anti-mask’ poster.
What the BBC did not bother investigating was that the poster in question was laminated, thus stiff, and the razor blade stuck flat to the back of it, making it virtually impossible that the woman had actually cut herself.
“When you took it off the wall, it would have been like a card, not a piece of paper you could scrunch up, it would have been a stiff card,” David said.
Nor did the BBC question why she threw away the ‘evidence’ instead of turning it over to the police she had contacted. They didn’t look into her apparent history of outlandish and improbable claims, like being disemboweled and walking to hospital holding her intestines in, nor her admitted history of self-harming, lending credence to the likelihood she staged the sliced-hand photo.
While this story seemingly originated from an unstable individual, it was pushed unquestioningly by British state-owned media.
Further, as Davis noted, the nonsensical razor poster story re-emerged two months later, this time with London transport warning of “anti-mask posters with razor blades.”
In this story, the Rail, Maritime and Transport (RMT) union cited by the BBC actually said it wasn’t aware of any razor-blade incidents. Yet the BBC ran with the claims nonetheless (using the previous unstable person’s photo to support the claims).
These were not the first razor-blade poster stories, though. In 2020, the BBC and other media ran stories claiming razor blades (and needles) had been put behind anti-5G posters, again not providing any actual evidence to back the claims.
Anti-mask, anti-5G… and ‘razor-blade posters’. Clearly, this looks like another psyop to indoctrinate the public into equating people who have legitimate and science-based concerns about particular issues as being not only bat-s**t crazy, but dangerous, a menace to society.
But these stories are being cooked up in underhand ways by some powerful forces that shouldn’t be engaged in these matters, while the masses actually concerned about these issues are raising their concerns in peaceful manners: petitions, peaceful demonstrations, scientific papers… All that is easily obscured by a few tabloid stories with screaming headlines.
According to Davis, the point is “to seed the idea into the public imagination to associate people that question vaccines with extremism, ultimately with terrorism. There is a lineage going back quite a few years where you can see this narrative being seeded into the public consciousness. It has really ramped up in the last couple of months.”
Indeed, in November 2020, the Ottawa Citizenrevealed the Canadian Forces’ desire to “establish a new organization that will use propaganda and other techniques to try to influence the attitudes, beliefs and behaviours of Canadians,” noting they’ve already spent over $1 million to “train public affairs officers on behaviour modification techniques of the same sort used by the parent firm of Cambridge Analytica.”
While noting nominal opposition and concern by the defence minister, the Citizen reported that “work is already underway on some aspects of the plan and some techniques have been already tested on the Canadian public,” as well as that “a series of town halls were already conducted last week for a number of military personnel on the strategies contained in the draft plan.”
Dan Dicks, in his commentary on the wolves scare story, aptly opined, “It frustrates me so much that the government is actively trying to silence me as being ‘fake news’ or putting out ‘false information’, when they are actively engaged in propaganda campaigns to distribute false information designed to scare Canadians.”
Indeed, we who speak out on uncomfortable issues are censored, ostracized, and labeled as ‘conspiracy theorists’, while governments are actively spewing misinformation and manipulating the masses.
First year students at the University of Bath have been given armbands by authorities to signal whether they’ve been double-vaccinated, with unvaxxed students having to wear a different colour.
“Freshers have been given wristbands to signal whether they are vaccinated against coronavirus amid anger at emerging “two-tier” university campuses,” reports the Telegraph.
“Students arriving this week at the University of Bath have been given a different coloured wristband on club nights if they can prove in advance they are double jabbed, or have Covid-19 immunity.”
Those who cannot prove they’ve been vaccinated are forced to enter a different queue in a clear example of segregation.
Bath is a notoriously left-wing city, as is its main university.
Vaccine passports are being enforced on campuses despite the government’s inability to impose them on the country after studies found they would be discriminatory and ethically unsound.
Students at Sheffield University must also present a COVID pass to gain access to enter freshers events or union nights out, meaning those who fail to comply will miss out on a social life altogether, with one student revealing how he felt “excluded” and feared being “shamed in front of friends.”
Students at Oxford and Cambridge are also being asked to disclose their vaccination status.
“We are worried that some universities appear to have implemented what amounts to a vaccine passport via stealth,” said Arabella Skinner, the director of parents group UsForThem.
“The idea of making students display their private medical information in such a public way is unacceptable. This echoes examples of discrimination we have seen in schools through the pandemic and raises concerns of a two-tier system for students to access education.”
Vaccine passports have largely proven to be ineffective everywhere they’ve been adopted, including in France where in many cases they are not even enforced.
After Israel set up one of the world’s first vaccine passport schemes, it experienced a record new wave of COVID infections.
Before 2020, evidence for the efficacy of community masking – that is, asking ordinary members of the public to wear cloth or surgical masks when going about their business – was shaky at best.
This evidence was reviewed in detail by Jeffrey Anderson, a former director of the Bureau of Justice Statistics. He notes that:
of the 14 RCTs that have tested the effectiveness of masks in preventing the transmission of respiratory viruses, three suggest, but do not provide any statistically significant evidence in intention-to-treat analysis, that masks might be useful. The other eleven suggest that masks are either useless—whether compared with no masks or because they appear not to add to good hand hygiene alone—or actually counterproductive.
In another piece that’s well worth reading, Professor Steve Templeton provides a list of quotations from what he calls “the BP era” (Before Things Got Political). Each quotation, taken from one or other expert, testifies to the lack of evidence that community masking works against respiratory pathogens.
For example, in a systematic review published early last year, Jingyi Xiao and colleagues “did not find evidence that surgical-type face masks are effective in reducing laboratory-confirmed influenza transmission, either when worn by infected persons… or by persons in the general community to reduce their susceptibility”.
This is presumably why, at the start of the COVID-19 pandemic, health authorities in both the U.K. and the U.S. advised against community masking.
For example, on 4th March 2020, Chris Whitty told Sky News that “wearing a mask if you don’t have an infection reduces the risk almost not at all”. And as late as 3rd April, Jonathan Van Tam said “there is no evidence that general wearing of face masks… affects the spread of the disease”.
Likewise, in a tweet sent on 27th February, the CDC said that it “does not currently recommend the use of facemasks”. And two days later, the U.S. Surgeon General urged people to “STOP BUYING MASKS” because they are “NOT effective” at preventing the general public from catching coronavirus.
In a video interview from May of 2019, Anthony Fauci actually laughed at the notion of wearing a face mask. The interviewer asks him, “The best way for me to prevent getting an infectious disease… is what? Wearing a mask?” To which Fauci replies, “No, no no… you avoid all the paranoid aspects.”
Yet by the summer of 2020, the health authorities in both countries had done an about-face, and were now recommending face masks to the public. These recommendations subsequently became mandates.
‘The Science,’ in other words, had changed. But what prompted this change? The charitable answer is that new evidence emerged suggesting that community masking does work against SARS-CoV-2. However, this new evidence looks just as shaky – if not shakier – than the pre-Covid evidence.
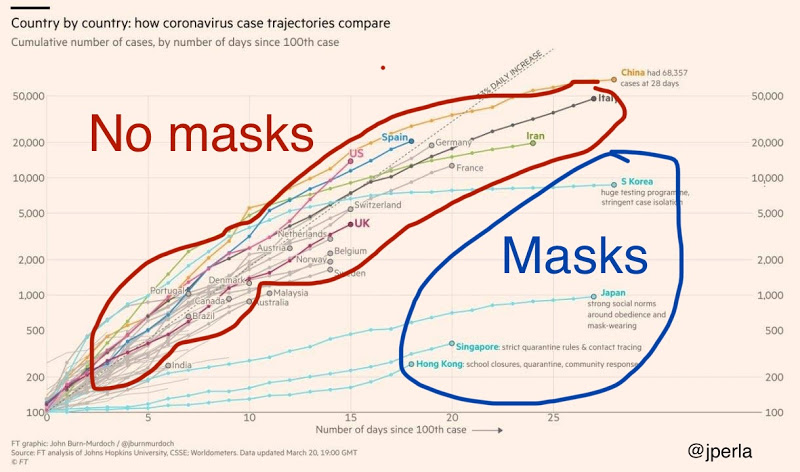
I suspect that something else happened. Back in the spring of 2020, all Western countries were on the same upward trajectory, with cases doubling every few days. Meanwhile, Japan, Korea, Hong Kong and Singapore had all manged to ‘flatten the curve’, despite eschewing draconian lockdowns.
Commentators were searching around for an explanation, and ‘masks’ seemed like a good one. After all, Western health authorities had advised against masks. Yet many East Asians had been wearing them for years.
If you were on social media at that time, you probably remember seeing a version of this chart, which went viral numerous times:
Putting ‘correlation doesn’t equal causation’ aside, it appears to suggest that masks are the crucial factor for bringing COVID under control. Of course, the subsequent imposition of mask mandates in Western countries didn’t forestall large winter outbreaks, which rather undermines the mask theory.
Nonetheless, it seemed plausible enough at the time. And articlesbeganappearinginmajornewsoutlets that questioned the West’s reluctance to wear face masks. On social media, commentators asked why we shouldn’t follow the East Asian countries, given their far greater success in handling the pandemic.
I suspect this pressure had more to do with the health authorities’ about-face than any fundamental change in the quality of evidence. It was another case of ‘politician’s logic’. ‘Something must be done; mask-wearing is something; therefore we must do it.’
In a matter of weeks, ‘The science’ went from ‘don’t do X’ to ‘do X’. And yet it took another whole year for the first RCT of community masking to be published. The theory I’ve outlined is speculative, of course. But I don’t see what else can account for such a sudden shift in public health advice.
This week, the Australian Federal Health Minister announced a commitment to COVID-19 vaccines for kids aged 5 to 11 years pending TGA-approval, after Pfizer claimed, in a press release, that it had obtained “favourable” results.
Pfizer’s ongoing Phase 2/3 trial apparently showed the vaccine “was safe, well tolerated and showed robust neutralising antibody responses”. However, the results were not submitted to the drug regulator, nor were they published in a medical journal, so for now, we must take their word for it.
Pfizer registered the trial plan, showing that it tested a lower dose (10µg) as well as two higher doses (20µg and 30µg) in 5- to 11-year-olds. Whether the vaccine can provide protection against symptomatic disease or severe COVID-19 remains to be seen.
The manufacturer also claimed that the vaccine had a “favourable safety profile”, however, it is important to note that the trial has not enrolled enough children (2,268) to detect any rare but serious harms that might arise from the vaccine
Only healthy kids were recruited in the trial – children with known or suspected immunodeficiency, a history of autoimmune disease, any condition associated with prolonged bleeding, anyone receiving treatment with immunosuppressive therapy or corticosteroids were excluded from the trial.
Notably, these are the same cohort of children who have been prioritised for the vaccine.
Despite little to no data available for its safety and efficacy, the Israeli Ministry of Health gave the green light to start vaccinating high risk 5- to 11-year olds with the lower-dose (10µg) of the vaccine.
Pfizer senior vice-president Dr Bill Gruber said he felt “a great sense of urgency” in the process, and Pfizer’s CEO Albert Bourla said trial data would be submitted to the various international drug regulators for “immediate authorisation.”
The language of Pfizer executives, the frenzied press coverage, and the political will of Governments, is all designed to pressure drug agencies to fast-track authorisations.
Younger than 5 years old?
Pfizer announced that trial data involving children under 5 are expected later this year.
Last week, Cuba began vaccinating toddlers as young as 2, using its homegrown vaccine, the Soberana 02, from the Finlay Vaccine Institute administered at adult doses. To my knowledge, there has been no data from Phase III trials published in the peer-reviewed literature in children as young as 2 with this vaccine.
China’s drug agency has cleared three COVID-19 vaccines produced by Sinopharm and Sinovac and is vaccinating children aged 3 years and older, under emergency use authorisation.
12- to 15-year-olds
Most major western nations have authorised COVID-19 vaccines for those aged 12 years and older.
In Australia for example, children aged 12 to 15 years began receiving the mRNA vaccines last week. According to the NSW Premier, 20% of children in the state of NSW have already had their first jab.
They require a two-dose regimen, the same dose given to adults, which aligns with the US FDA and Health Canada advisories on vaccines for this age group. (See my previous analysis for 12-15yr olds)
This does not align with the UK’s more cautious approach. After significant political and media pressure, UK chief medical officers recommended a single dose of the Pfizer vaccine, because of concerns about rare side effects such as heart inflammation.
Brazil appears to be an outlier at the moment. It was reported that the Minister for Health called for the suspension of the COVID-19 immunisation of people aged 12 to 17 after the death of a 16-year old girl named Isabelli Borges Valentim, eight days after she received the Pfizer shot. Authorities are still investigating the incident but the drug regulator denies any link to the vaccine.
Myocarditis/Pericarditis
This issue has stirred up some heated debate.
Now that real world data is becoming widely available, myocarditis (inflammation of the heart muscle) and pericarditis (inflammation of the membrane surrounding the heart) are being reported as rare harms related to the Pfizer & Moderna mRNA vaccines.
Israel, because of its fast vaccine roll-out, was first to raise the alarm – 148 cases of myocarditis were reported within 30 days of immunisation, more commonly after the second jab. It prompted the Israeli Ministry of Health to launch an investigation into any possible link between these cases of myocarditis and vaccination.
Since then, other countries such as the UK, the US and Canada have corroborating data.
In June, the US FDA decided that the link between the mRNA vaccines and myocarditis, particularly in young males, was sufficiently clear that it revised its vaccine fact sheets to include a warning.
The CDC released data showing the incidence of “expected” versus “observed” incidences of myocarditis and pericarditis and found a significant increase in the observed rates. The graph shows the higher rates in red (see table numbers circled in red).
Another study, published in JAMA which looked at data from 40 hospitals in the US showed a similar pattern to the CDC, although at higher incidences, suggesting that the vaccine’s adverse events were being underreported.
Researchers then took a more granular look at the database for reported adverse events (VAERS database) between 1 January and 18 June, and found boys aged 12-15 years vaccinated with their second shot of the mRNA vaccine, with no underlying medical conditions were 4 to 6 times more likely to develop a cardiac adverse event, than ending up in hospital with COVID-19.
The study was published as a pre-print online but it ignited a twitter storm, with critics claiming the study ‘over-estimated’ the risk and it was biased because one of the authors belonged to a group that did not support making vaccines compulsory.
Sceptics say that most of the myocarditis cases are mild, and that children recover quickly from hospitalisation. Others are not so quick to dismiss the potential risk of ‘sub-clinical disease’ (myocarditis without symptoms) in children.
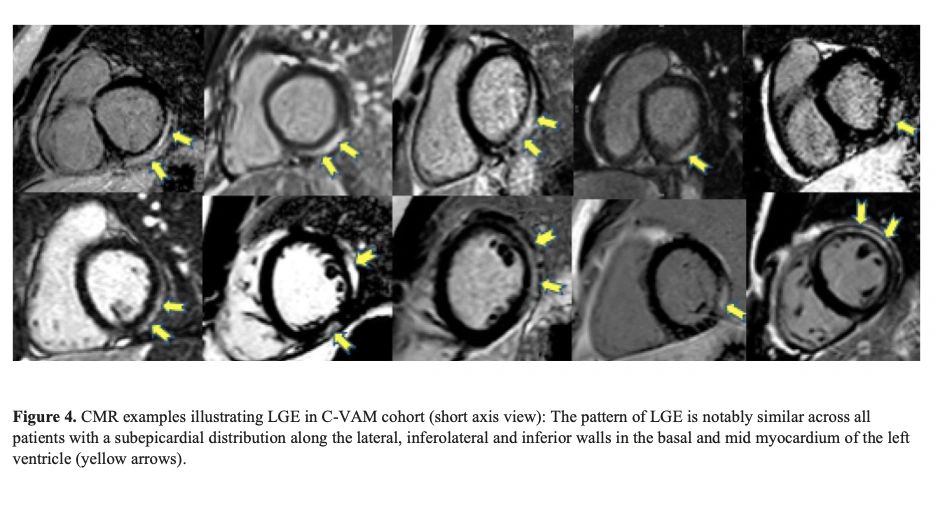
Notably, a retrospective multi-centre study across 16 US hospitals including patients <21 years of age with a diagnosis of myocarditis following COVID-19 vaccination, found concerning abnormalities in heart tissue (the left ventricle) (See image with yellow arrows).
Jain SS, et al doi: 10.1542/peds.2021-053427.
Careful monitoring is required to see if these abnormalities lead to fibrosis, which can have long-term implications for young patients.
Early findings suggest that post-vaccination myocarditis could be mediated by the toxicity of ‘spike protein’ on heart muscle cells or from circulating spike proteins in plasma after vaccination.
The risk of myocarditis associated with contracting COVID-19 infection may be higher than that after vaccination, but more research is needed to weigh harms against benefit.
If we don’t vaccinate kids, what about long COVID?
The fear of long-COVID has been a major impetus behind vaccinating kids.
A recent review by Monash University, analysing 14 international studies on long COVID in children and adolescents, found no difference in the symptoms reported by those who had experienced COVID-19 and those who had not.
Lead researcher on the study, Professor Nigel Curtis told newsGP the review’s findings should be reassuring for parents and carers.
Similarly, a webinar hosted by The BMJ revealed the results of the largest citizen-scientist participation study to date in young children. It used a smartphone app to monitor the illness and symptoms of children after testing positive to COVID-19.
The researchers found that the median duration of illness was 6 days. Only 4.4% of children had illness duration >28 days and 1.8% had symptoms >56 days. Encouragingly, their symptom ‘burden’ was greatly reduced by this time (none became worse) with the most common symptoms being headache and fatigue.
The researchers looked at neurological symptoms such as epileptic seizures, convulsions, impaired attention and concentration, but none were reported.
Lead investigator on the study, Prof Emma Duncan from Kings College in London concluded “Long illness duration of COVID-19 in children is uncommon.”
Vaccine Mandates for kids
Despite COVID-19 vaccine mandates for teachers in places such as New York and Australia (Victoria and New South Wales), no Federal government has announced plans to make the vaccines compulsory for children (yet).
Canadian and English professors have argued that making COVID-19 vaccines mandatory for children, will “encourage uptake”.
U.S. Surgeon General Vivek Murthy has also suggested that COVID-19 vaccine mandates for students could happen at the state and local level in the US, once they have been approved for paediatric use by the US FDA.
In a surprise announcement this week, the Los Angeles public school system said students aged 12 and older will now have to be double-vaccinated by the end of the year, to attend classes on campus or take part in sports and other extracurricular activities. It remains to be seen whether other school districts will follow.
Consent from kids
Before the age of 14, minors are generally thought to lack the cognitive capacity and maturity to make rational judgments about their health.
In fact, most US state laws presume that minors lack medical decision-making capacity and therefore require parental consent for most health care decisions, including vaccination, with some exceptions.
However, in the case of COVID-19, under what is termed ‘Gillick competency’, those under 16 years can make independent decisions about a medical treatment if they can demonstrate they have the capacity to consent, even if their parent withholds consent.
This applies to every Australian state and territory as part of the ‘common law’ and in the UK.
The Victorian government has produced ‘communication packs’ for teachers and educators on how to ‘promote’ COVID-19 vaccines to minors.
Hopefully, the conversations about COVID-19 vaccines, between health professionals and minors, are conducted without coercion, pressure or judgment.
Not surprisingly, this has raised the age-old question about who is better placed to determine the best medical treatment for a child – a parent or a Government minister?
The debate will continue and experts will need to wade through muddy waters to find a balance between protecting children’s health and the uncertainty over the long-term harms of the vaccine.
The Met Office’s website describes the work they do, rambling on about forecasting the weather and world leading science. Nowhere can I find any reference to publishing fake news or disseminating misleading propaganda.
According to the Cambridge Dictionary:
Decline = change to a lower amount
Continues = keeps happening
So the meaning of that headline is crystal clear:
Arctic sea ice keeps getting less.
One look at their graph shows this is patently not true, despite grossly misleading linear fit, intended to fool people.
It is very easy to show that Arctic sea ice has stabilised. As their graph itself shows, there have only been three years since 2007 with lower ice extent than that year, and eleven have had higher extents.
Also the average of the last ten years is higher than 2007’s extent.
In itself, this is too short a period to make any meaningful judgements. But that is no excuse for the Met Office to publish such a manifest falsehood.
I have left a comment on their blog, but as is usual it is blocked. Maybe Richard Betts would care to comment!
The British government is expected start adding fluoride to the drinking water all over the country according to a story in the Guardian.
The story focuses on a joint statement the Chief Medical Officers (CMOs) of England, Scotland, Wales and Northern Ireland published on Thursday, which recommends everyone, everywhere should have fluoride added to their water supply.
The report was already praised in a tweet from UK Health Secretary Sajid Javid:
Good to see UK CMOs examining how water fluoridation can improve oral health & prevent tooth decay which disproportionately affects more deprived groups.
Reinforces why our Health and Care Bill will make it simpler to expand water fluoridation schemes.https://t.co/jKCqGtFmMr
While fluoridation is already in place in some parts of the UK, it has always been considered a matter for local government and currently affects less than 10% of the country.
Proposed changes to the regulations in sections 128-129 of the new Health and Care Bill would centralise this power, taking the decision out of the hands of local councils and handing it to the Health Secretary.
The authors of the report, including England’s CMO Chris Whitty (who we are more than familiar with, thanks to Covid) are not subtle in their attempts to cloak the proposed policy in “progressive” camouflage.
Statistics on tooth decay in children and the working class are trotted out so fluoridation could be sold as both “protecting children” and tackling “entrenched inequality”.
But what is the real risk-reward situation for fluoridated tap water?
Well, the only potential benefit of fluoride is preventing tooth decay. That’s it. (And even then, over-exposure to fluoride can actually damage your teeth through dental fluorosis).
The potential side effects of fluoride toxicity are far more dangerous than needing a root canal.
There is some evidence fluoride could increase the risk of cancer – a 2006 study found an increased risk of osteosarcoma in young boys – but the most serious problem associated with fluoride is developmental neurotoxicity.
In 2012 a study from the Harvard School of Public Health found fluoride exposure is detrimental to the intellectual development of children, with an author of the study saying [emphasis added]:
Fluoride seems to fit in with lead, mercury, and other poisons that cause chemical brain drain. The effect of each toxicant may seem small, but the combined damage on a population scale can be serious, especially because the brain power of the next generation is crucial to all of us.”
The results found that children raised in areas with widespread water fluoridation had markedly lower average IQs than children from areas with no fluoride in the water:
This pilot study in a community with stable lifetime fluoride exposures supports the notion that fluoride in drinking water may produce developmental neurotoxicity
To sum up: Fluoride in the water could potentially make future generations of people compliant, gullible and stupid.
Or, in other words, it’s the perfect thing to start pumping into the water when you’ve just tried to launch a global coup, and not enough people are falling for it.
It’s official: I am spouting misinformation about the Covid vaccines. Full Fact – the Google, Facebook and George Soros-funded outfit that Ofcom has said it relies on to tell it what to censor regarding COVID-19 – has ‘fact checked‘ my recent piece on PHE data showing negative vaccine effectiveness in August and branded it “incorrect”.
Writer Leo Benedictus – henceforth to be known as the Oracle – takes particular issue with the headline, which he says “falsely claims that a report from Public Health England (PHE) shows the COVID-19 vaccines having ‘negative effectiveness’ in the over-40s”.
“This is not true about the COVID-19 vaccines – nor is it true that the PHE report shows this,” the Oracle declares. Except it is. The data contained in the report is completely clear, and the calculation of unadjusted vaccine effectiveness from that data is straightforward.
According to the Oracle, however, this is not a valid way of estimating vaccine effectiveness. Benedictus quotes the PHE report stating as much – “The vaccination status of cases, inpatients and deaths is not the most appropriate method to assess vaccine effectiveness and there is a high risk of misinterpretation” – and notes that I too quote this. What he fails to acknowledge, though, is that I also examine the reason PHE gives for this claim and counter it.
The only substantive reason PHE gives that vaccine effectiveness might be underestimated in its data is that “vaccination has been prioritised in individuals who are more susceptible or more at risk of severe disease”. In other words, the high-risk are over-represented in the vaccinated and this skews the sample. I countered that the large majority of the older age groups are now vaccinated so this bias should be very much reduced. Of course, we also need to ask why, if this is supposedly the key confounder of the data presented, we are not also provided with the necessary data on risk categories so that it can be duly quantified and accounted for.
Benedictus reiterates PHE’s claim that vaccine effectiveness should only be estimated via the published studies. However, as I noted in my article, these studies are riddled with serious problems and inconsistencies that bring their findings into question. They are also out of date since they don’t cover the Delta surge, which is the first time the vaccines have really been stress-tested in the U.K.
Benedictus spends half the ‘fact check’ in a bizarre attempt to argue that my vaccine effectiveness calculation is wrong because I used the data PHE itself used for the size of the unvaccinated population. He points out it is different to the ONS figures on this. Er, take that one up with PHE, Leo.
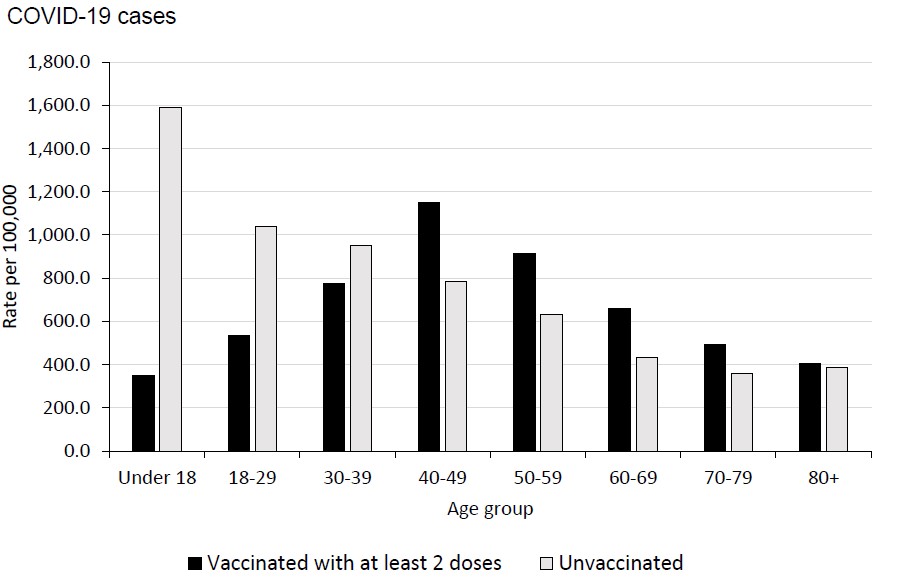
It does seem at times that Benedictus is fact-checking the PHE report rather than my article. At one point he takes the report to task because one of its charts sowed confusion as it “seemed to show for the month in question (August 9th to September 5th) that people in their 40s, 50s, 60s and 70s were more likely to test positive for Covid if they had been vaccinated than if they hadn’t”.
Except the chart didn’t ‘seem’ to show that; it did show that. Again though we are told that this data does “not give a reliable estimate of vaccine effectiveness” because of biases in the samples.
But who defines what makes an estimate of vaccine effectiveness ‘reliable’ enough to be permitted without being labelled false? All vaccine efficacy estimates have limitations arising from the limitations of the data, including those produced by PHE. I was careful to acknowledge the limitations of the estimates I was making, saying they were unadjusted for risk factors – though argued that this shouldn’t matter so much anymore given high coverage. There’s also the point that being high-risk may affect the risk of serious disease and death but there’s no reason to think it will have an impact on infection rates (save for the small number of immuno-compromised).
The unmistakable impression here is of a gatekeeping exercise by the Government and its outriders to ensure it controls the concept of vaccine effectiveness and no one unauthorised is allowed to make an estimate of it. Thus the availability of the data is carefully controlled and we only get a month at a time and without the additional data that would allow us to control for the supposed biases that the report tells us the data includes and which ‘invalidate’ any attempt to make an unauthorised calculation of vaccine effectiveness.
None of this concept-policing does anything to alter the facts, however. In recent weeks reported infection rates have been higher in the double vaccinated than in the unvaccinated for the over-40s. That means that, for this period, (unadjusted) vaccine effectiveness is negative in those age groups.
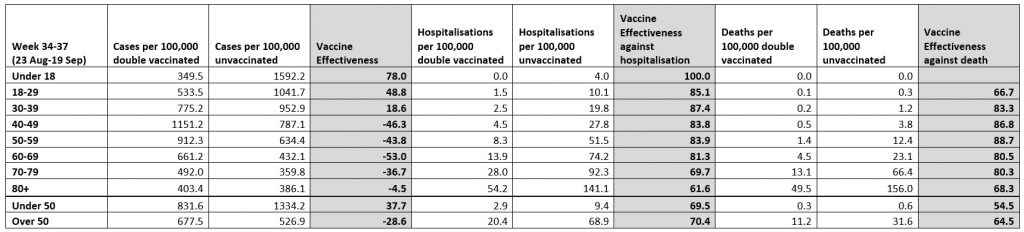
PHE has published two new reports since my article and in each the unadjusted vaccine efficacy has declined further. Here is the table using data from the latest report, covering August 23rd to September 19th (the related chart from the report itself is above).
It shows that in the two weeks since my article the vaccine effectiveness has dropped further, with unadjusted vaccine effectiveness in the over-40s now hitting as low as minus-53% among people in their 60s. This means that, on this data for this age group, the double vaccinated experienced a 53% higher reported infection rate than the unvaccinated in the past month. And that’s a fact.
Stop Press: Professor Norman Fenton and Professor Martin Neil on the Probability and Risk site have used age-adjusted all-cause mortality to estimate vaccine effectiveness and found that mortality rates are currently higher in the vaccinated than the unvaccinated.
Stop Press 2: Professor David Paton has produced a good Twitter thread responding to one of the more well-informed critics of this (and other) pieces citing the PHE data.
The scene: a British nuclear submarine. A detective has been sent to investigate the death of a sailor. When she asks the Naval Commander why there needs to be so much secrecy, as Britain is not at war, he responds ‘That is an illusion. We have always been at war’.
The series, entitled ‘Vigil’ is the BBC’s most watched drama of the year, and has been well publicised, attracting an audience of 10.2 million over its first week. It depicts a fight with an illusive, ruthless adversary that successfully manages to infiltrate a UK submarine to ‘knock out Britain’s nuclear deterrent’, killing British citizens in the process. The murder weapon of choice is a nerve agent; can you guess who the enemy is yet?
Of course it’s Russia. Nuclear submarines, nerve agent, a treacherous opponent; from the opening sequence with video footage of Vladimir Putin and Dmitry Medvedev projected onto a submarine, the audience is under no illusion as to who this adversary is. Nowadays, the British public almost expects it to be Russia.
For years now the UK population has been schooled on ‘evil Russia’ across all media platforms – from the news to TV dramas to films – with the line between fiction and reality becoming increasingly blurred. One of the most Googled questions about the ‘Vigil’ drama series is ‘is it real?’ This is hardly surprising given the sheer volume of anti-Russian content, with cinema often dramatising real life events and vice versa.
Take the Skripal case, for instance. The apparent poisoning with ‘Novichok’ of the former spy Sergei Skripal and his daughter took place just a few months after a British/American TV series ‘Strike Back’ was released, in which a ‘rogue Russian biochemist‘ was working on a substance of the very same name. That was probably the first time that western audiences had ever heard the word ‘Novichok’, and yet, by extraordinary coincidence, it was to appear on our TV screens just a few months later, in the news. The finger of blame was immediately pointed at Moscow, just as preparations were being made for Russia to host the 2018 world cup. The timing could not have been worse for the Kremlin, and yet it helped Britain considerably in its bid to discredit Russia in its hosting of the sporting event.
TV and cinema being used by governments as instruments to sway and foster public opinion is nothing new. In the book ‘Propaganda and empire: the manipulation of British public opinion, 1880-1960’ John M MacKenzie explores the plethora of ways the British government promoted imperialism throughout the empire’s existence, not only through cinema, but using everything from cigarette cards to school textbooks. During the war, the British Ministry of Information also pumped out films with instructive government messaging under the direction of Humphrey Jennings. These documentaries were more about what to do and what not to do, promoting slogans such as ‘grow your own’ and ‘make do and mend’ to aid the war effort on the home front.
The ‘Vigil’ drama obviously had a considerable budget. And its political function is twofold; it highlights the ‘threat’ from Russia, and the question of the Trident’s future in an independent Scotland. By playing up the idea of a real, imminent danger from Russia, it persuades the viewer of the importance of retaining Britain’s nuclear deterrent. As tensions grow between East and West, and Boris Johnson pursues his ‘Global Britain’ strategy, we will no doubt see more programmes emphasising Britain’s military strength countering Russia and let’s not forget, China. Sadly, such manipulation of the population doesn’t encourage understanding between peoples and instead, fosters division and discrimination. At best it is Britain using Russia as a scapegoat to bolster its sense of national pride; at worse, it is laying the groundwork for a future conflict with Russia.
Johanna Ross is a journalist based in Edinburgh, Scotland.
Did you see the recent hype on the latest cholesterol-lowering confection from Pharma? No data whatsoever to suggest it will improve heart disease outcomes, but UK NICE body has pronounced that billions will be spent on it regardless? Well here Dr. Aseem Malhotra and Dr. Malcolm Kendrick lay bare the latest lipid scam on GB news!
With all medical eyes on COVID19, a cardiovascular drug with no proven benefit – at all – has been approved by NICE (The UK National Institute for Health and Care Excellence). Once a drug is approved by NICE it can, and will, be prescribed by doctors in England and Wales and Northern Ireland.
… approving drugs, or launching drugs before you have any evidence that they do anything – other than having a favourable effect on an established lipid biomarker – is ridiculous. But never mind, longer term studies on Inclisiran will be completed by 2023, and 2026. When will they actually be published?
Who cares, by the time they are published, Inclisiran will have made billions, and no-one will care if the results are positive, or negative, as it will have become established as ‘standard’ treatment.
A number of us found the NICE approval of Inclisiran so ridiculous that we wrote them a letter. … Read full article
For quite some time the British have accepted that British Jewish organizations have hijacked the political discourse. As has happened in other Western countries, the British political establishment has engaged is a relentless rant against antisemitsm. Sometime the focus drifts for a day or two. An alleged ‘Russian nerve gas attack’ provided a 48 hour pause. Occasionally we bomb Arabs in the name of ‘human intervention’ only to realize a day or two later that we have, once again, followed a premeditated foreign agenda. But, somehow, we always return to the antisemitism debate, as if our media and politicians are a herd of flies gravitating to a pile of poop. … continue
This site is provided as a research and reference tool. Although we make every reasonable effort to ensure that the information and data provided at this site are useful, accurate, and current, we cannot guarantee that the information and data provided here will be error-free. By using this site, you assume all responsibility for and risk arising from your use of and reliance upon the contents of this site.
This site and the information available through it do not, and are not intended to constitute legal advice. Should you require legal advice, you should consult your own attorney.
Nothing within this site or linked to by this site constitutes investment advice or medical advice.
Materials accessible from or added to this site by third parties, such as comments posted, are strictly the responsibility of the third party who added such materials or made them accessible and we neither endorse nor undertake to control, monitor, edit or assume responsibility for any such third-party material.
The posting of stories, commentaries, reports, documents and links (embedded or otherwise) on this site does not in any way, shape or form, implied or otherwise, necessarily express or suggest endorsement or support of any of such posted material or parts therein.
The word “alleged” is deemed to occur before the word “fraud.” Since the rule of law still applies. To peasants, at least.
Fair Use
This site contains copyrighted material the use of which has not always been specifically authorized by the copyright owner. We are making such material available in our efforts to advance understanding of environmental, political, human rights, economic, democracy, scientific, and social justice issues, etc. We believe this constitutes a ‘fair use’ of any such copyrighted material as provided for in section 107 of the US Copyright Law. In accordance with Title 17 U.S.C. Section 107, the material on this site is distributed without profit to those who have expressed a prior interest in receiving the included information for research and educational purposes. For more info go to: http://www.law.cornell.edu/uscode/17/107.shtml. If you wish to use copyrighted material from this site for purposes of your own that go beyond ‘fair use’, you must obtain permission from the copyright owner.
DMCA Contact
This is information for anyone that wishes to challenge our “fair use” of copyrighted material.
If you are a legal copyright holder or a designated agent for such and you believe that content residing on or accessible through our website infringes a copyright and falls outside the boundaries of “Fair Use”, please send a notice of infringement by contacting atheonews@gmail.com.
We will respond and take necessary action immediately.
If notice is given of an alleged copyright violation we will act expeditiously to remove or disable access to the material(s) in question.
All 3rd party material posted on this website is copyright the respective owners / authors. Aletho News makes no claim of copyright on such material.