Why Can’t the Government be More Transparent About the Data Guiding its Decisions?

By Professor Anthony A. Fryer | Lockdown Sceptics | April 27, 2021
When I look back over the last year or so of the pandemic, I can forgive the first couple of months. We were all finding our feet with a largely unknown entity. However, as a clinical scientist with over 30 years in NHS laboratories and as an academic researcher with over 200 peer-reviewed clinical research articles in scientific and medical journals (including over 130 involving use of the polymerase chain reaction [PCR]), I found my views increasingly divergent from those of the Government and its advisors. Those who know me will know that it takes a lot to get me annoyed, but I could not sit by and do nothing when I could see the immense damage being done to countless lives and businesses in the name of supposedly protecting us from SARS-CoV-2.
But let me say at the start; I am not one to deny the damage that COVID-19 can do. (And I deliberately use that term, rather than SARS-CoV-2. It’s the disease that causes the problems – most people manage the virus without much difficulty.) COVID-19 can be very nasty and my heart goes out to all those affected. But the way in which the Government handled the pandemic has, in my view, been shocking. It’s felt like it has focused blindly on the virus (and not very well at that either – just think about PPE in care homes for a start) and ignored the massive implications on every other level.
So I wrote. I wrote letters to the local paper, emailed the Chief Medical Officer, submitted evidence to a Parliamentary Inquiry, signed the Great Barrington Declaration, published scientific papers on the ineffectiveness of face coverings and on the non-Covid harms to people with diabetes, and wrote to my MP. Several times. I also joined UsforThem and the Health Advisory and Recovery Team (HART).
Back in October 2020, I wrote one of my letters to my MP, Fiona Bruce, raising a number of concerns about the Government’s handling of the pandemic, and requesting that she raise these concerns with the powers that be on my behalf. While the letter was written as a member of the public, I felt that my expertise and experience put me in a position to comment in a way that perhaps others couldn’t.
In the letter, I highlighted three main concerns:
1. Evidence. That measures to reduce the spread of coronavirus SARS-CoV-2 were introduced without evidence to support them.
2. Context. That such measures were generating more harms than those caused by the virus itself, and this was not being reflected in a balanced way in the press briefings, including in the figures presented, thereby creating an atmosphere of fear.
3. Testing. That the way in which testing data has been presented had been misleading to the public and media. This area was of particular concern to me, given my clinical and research experience in the field.
In respect of the above three areas, I requested the following of my MP:
1. Please could you lobby that scientific evidence underpinning decisions is provided with all future communications.
2. I would ask that you raise this with the Prime Minister and Secretary of State for Health as a matter of urgency to ensure that contextual information is co-presented at press briefings for comparison.
3. I would be grateful if you could impress upon the Secretary of State for Health, the Chief Medical Officers and the Chief Scientific Officer to present adjusted data in a more balanced way to reflect the major difference in rates of cases now with those in April.
… and…
I would request that you (i) ask the Secretary of State for Health to ensure that all positive tests are repeated before labelling an individual as positive, and (ii) that the estimated one third of deaths attributed to COVID-19 because of a SARS-CoV-2 positive test, but where the cause of death was not COVID-19, be removed from the figures.
On April 13th 2021, some six months later, the reply arrived, along with a letter from Lord Bethell (Parliamentary Under Secretary of State at the Department of Health and Social Care), dated April 7th.
The response, which you can read here, was both enlightening and disheartening, if not unexpected.
Here is my commentary on the response from Lord Bethell, passed on by my MP:
Evidence
Lord Bethell referred to the release of papers and minutes from SAGE, presumably to exemplify the evidence underpinning the decisions to implement mitigation measures. The complete lack of credibility of anything coming from SAGE notwithstanding, this is hardly an independent assessment of the evidence underpinning the Government’s decisions.
To me, anyone with any scientific nous could present a fairly long list of actions that the Government has taken without first presenting clear evidence to indicate their effectiveness and an evidence-based risk-assessment of potential non-Covid harms. The “Rule of Six”, the 10pm curfew, face coverings (anywhere, let alone in schools), lockdowns (in any of its many guises, including Tiers), etc, etc, etc. Where is the assessment of non-Covid physical and mental health harms, economic impact, or the effect on our children’s education and wellbeing? Or even evidence on reducing transmission of the virus itself, for that matter?
All we have seem to have seen is exaggerated figures predicting doomsday scenarios, mostly based on modelling rather than actual data, none of which have come to pass. These seem only aimed at scaring the public into following their non-evidence-based guidelines (an approach which, to me, could itself have a potentially significant negative mental health impact).
Context
In terms of presenting COVID-19 data in a wider context, Lord Bethell’s response seemed silent on this one. I am still waiting to hear a press conference which presents the non-Covid harms that we are hearing about all the time in the scientific literature, from the mental health sector, from education, from the business world and from thousands of individual stories.
We are instead presented with advertising campaigns which tell us to “act like you have it”. Not only is that completely illogical – if we all took that literally, society would stop. All of it. No hospitals, no supermarkets, no police, nothing. We’d all be at home self-isolating. But it verging on emotional blackmail. Please give the public some respect and allow them to make responsible decisions.
Testing
The third area covered three distinct points:
- Comparing like with like. A request to not compare figures in October with those in April when testing levels were at a much lower level.
- False positives. A request to define positive ‘cases’ accurately by correctly addressing the issue of false positives.
- ‘With’, not ‘from’. A request to exclude deaths where COVID-19 was not the cause of death from the figures for COVID-associated deaths.
a. Comparing like with like. On the first of these, it’s hard to identify whether Lord Bethell had anything to say on this. He didn’t address it directly. My point focused on the unbalanced way figures were presented back in October which, in my view, presented to the public another doomsday, worst-case scenario to frighten them into compliance with Government wishes. Models presenting huge potential death tolls, all of which were subsequently shown to be out by orders of magnitude.
b. False positives. On the second point, Lord Bethell’s response went into some detail, the content of which itself seemed to either miss the point, or indeed add fuel to my initial concern.
On the positive side, there were some admissions about the PCR test. For example, his response stated: “We are also aware that when PCR test detects viral material it does not indicate that the virus is intact and infectious.” So a positive test doesn’t equate to infectiousness, or even having the virus at all. That’s obvious. It’s just a pity this isn’t mentioned in any of the press briefings along with an evidence-based assessment of its impact on the figures. “Positive tests”, “infections” and “cases” are used interchangeably.
Regarding the PCR test cycle threshold (Ct), he also acknowledged that “…values obtained in this way are semi-quantitative, meaning they do not measure the precise quantity of the virus…” He focuses on the small number of samples with a cycle threshold of over 37. I would be interested in what proportion are above 27, as there is increasing evidence that test samples above this level are significantly less likely to be infectious (and have a much higher false positive risk). Indeed, some data published by the Oxford Group based on the UK’s COVID-19 Infection Survey illustrated that the vast majority of ‘positive’ PCR tests have a Ct value of >27 (Pritchard et al. Impact of vaccination on SARS-CoV-2 cases in the community: a population-based study using the UK’s COVID-19 Infection Survey). So most of the positive tests contain low levels of virus (if any) and the risk of transmission is small.
But even taking Lord Bethell’s Ct cut-off, his comments on test specificity are particularly revealing. He acknowledges that, “Like any diagnostic test, there is a possibility of a false negative or false positive result”, but goes on to say, “but this is very small”. He states that: “Independent, confirmatory testing of positive samples indicates a test specificity that exceeds 99.3%, meaning the false positive rate is less than 1%.”
My HART colleague Dr Claire Craig did some sums on this. At a false positive rate of 0.7%, there would have been 8,700 false positives and 6,200 true positives for the week beginning April 12th on PCR. In other words, 58% of the positives would have been false. If we include the Lateral Flow Tests, then 70% of the cases would have been false positive that week.
My real question is, why are the ‘case’ figures not revised downwards accordingly, or at least the impact of false positives explained at the briefings?
c. “With”, not “from”. On the third point, Lord Bethell made some valid points, though their interpretation was a little off kilter. My concern related to the definition of the figures used to define Covid-associated deaths in official figures. In my mind there were three ways these could be derived; (i) those where the cause of death was primarily COVID-19 (“from” Covid), (ii) those where the person had a SARS-CoV-2, or even COVID-19, but where this was not the cause of death (“with” Covid), and (iii) those who had a false positive test for SARS-CoV-2 (i.e., did not actually have the virus or COVID-19 when they died).
My view was that these latter two would over-estimate the figures for Covid-associated deaths and should be excluded (though I acknowledge that separating the first two from each other can sometimes be difficult in clinical practice). Lord Bethell rightly pointed out three other possible scenarios that could theoretically cause an under-estimate of the figures. Firstly, those who “had COVID-19 but had not been tested”, secondly, those who had “tested positive only via a non-NHS or PHE laboratory” so their positive result was not recorded on their death certificate, and thirdly, those who “had tested negative and subsequently caught the virus and died”. He also acknowledged that it is possible that my options (ii) and (iii) above are plausible scenarios: “It is true that people who have tested positive for COVID 19 could, in a few cases, have died from something else.” (His phrasing is interesting here – I wonder if he realises that PCR is not a test for the disease, COVID-19, but for the virus, SARS-CoV-2?) It is saddening that he feels the need to qualify the option that overestimates death with the phrase “in a few cases”, but not his three scenarios that might lead to under-counting, despite the likelihood that these have much less impact on the figures.
Have we moved on since October?
My feeling is that we have moved on in some areas. Now we have the vast majority of susceptible individuals vaccinated (one of the few success stories), a huge number of people who are resistant or immune, herd immunity, and a whole range of effective treatments (and that’s excluding the two magic pills we are promised by autumn). This should mean that we are completely back to normal – no masks, no distancing, no sanitisers – and focusing on how we can help those in other countries to get to the same place, and recovering from the damage caused by the mitigation measures.
But sadly we still don’t get anything high profile (e.g. in Government briefings) on my areas of concern. Nothing on the evidence underpinning the Government’s decisions, nothing on non-Covid harms, nothing on the impact of false positives on “cases” and Covid-associated deaths. And still, millions of people in the UK suffer needlessly. An apology would be nice.
In the first paragraph of his response, Lord Bethell states that “we are committed to open sharing of the scientific advice that guides our response to COVID-19 where possible”. I am yet to be convinced.
Dr Anthony Fryer is Professor of Clinical Biochemistry at the Institute for Science and Technology in Medicine at Keele University and member of HART and is writing in a personal capacity.
“The UK Currently Operates a System of Informed Consent for Vaccinations.” Currently, Minister?

By Will Jones • Lockdown Sceptics • April 27,2021
Dr Helen Westwood, a GP whose previous letters and comments have appeared on Lockdown Sceptics, wrote to her MP Sir Graham Brady in March with some concerns about the vaccines and the potential for coercion. She has now received a reply from Vaccines Minister Nadhim Zahawi that is far from reassuring.
Here’s what she wrote.
Dear Sir Graham,
Firstly I wish to thank you again for your ongoing hard work in arguing for a more proportionate response to dealing with COVID-19. The concerns I wish to raise with you today relate to the vaccination program and the proposition of vaccination certificates.
As you know I am a GP. I am horrified by the talk of ‘No Jab, No Job’ policies and vaccination certificates.
The GMC are very clear that “all patients have the right to be involved in decisions about their treatment and care” and that “doctors must be satisfied that they have a patient’s consent… before providing treatment or care”. They also state “doctors must… share relevant information about the benefits and harms of proposed options and reasonable alternatives, including the option to take no action”.
Following interim analysis of the ongoing clinical trials, emergency use authorisation has been granted by the MHRA for both the Pfizer BioNTech and the AstraZeneca vaccines. They are as yet unlicensed. The clinical trials are due to continue until 2023. I find it alarming that much attention is paid to the headline figures of relative risk reduction (RRR) with no mention of the absolute risk reduction (ARR). The RRR of the Pfizer BioNTech vaccine is 95.1% (CI 90.0%-97.6%, p=0.016). Dig a little deeper into the data and you learn that the ARR is only 0.7% (CI 0.59%-0.83%, p<0.001) and the number needed to vaccinate in order to prevent one infection is 142 (CI 122-170).
The WHO published a bulletin written by John Ioannidis, Professor of Medicine at Stanford University, in October 2020. He quotes an infection fatality rate (IFR) for Covid of 0.00-0.57% and in those under the age of 70 it stands at 0.05%.
Given the minimal risk healthy people under the age of 70 face, and the very small absolute risk reductions noted in the clinical trials, I have to ask why are we so desperate to vaccinate the whole population? For healthy, working age people Covid poses less of a risk than seasonal flu. It has never been proposed that we vaccinate the entire adult population against flu; we target the populations most at risk.
The speed at which these vaccines have been developed is truly remarkable. However, I have grave concerns that they are being rolled out on such a scale and at such pace. I am not sure whether you are familiar with the work of Joel Smalley MBA (a member of HART) but he has done some very interesting analysis of mortality data. Whilst correlation (between vaccination administration and rises in mortality) absolutely does not mean causation, the striking patterns he has highlighted suggest to me that now is the time to pause and reflect on the data we have so far. We know from the clinical trials that the Pfizer BioNTech vaccine causes a drop in lymphocytes around seven days post administration; theoretically at least this could pose a risk of intercurrent infection, especially in frail patients.
Both vaccines in current use in England employ novel technology, namely mRNA (Pfizer BioNTech) and Adenovirus vector (AZ). Human challenge studies have only recently begun. We do not currently know anything about the medium and long term safety of these vaccines. There are concerns about Antibody Dependent Enhancement (ADE) reactions whereby vaccinated individuals may develop more severe disease upon exposure to the wild virus. Theoretical concerns have also been raised about potential cross reactivity with Syncytin-1 which could have effects on placental development and therefore fertility. Until these areas have been studied we cannot advise patients fully. This has significant implications for the informed consent process.
There seems to be some enthusiasm for “vaccination passports” among the population, whether for domestic use or international travel. These have been compared to Yellow Fever certificates that are required for individuals travelling to certain destinations. In reality there is no comparison. The mortality rate for Yellow Fever is in the region of 30%, transmission of Yellow Fever is confined to a relatively small number of countries and there are long term safety data available regarding the licensed vaccine.
Uptake of the Covid vaccine has been notably lower amongst certain ethnic minorities. The reasons for this are as yet unclear, but any policy requiring proof of vaccination has the potential to lead to indirect discrimination.
Professor Chris Whitty has said that doctors and care workers have a “professional responsibility” to get vaccinated. Given that reduction of transmission is not an outcome that is being measured in the clinical trials that are still ongoing, I do not agree with him. Article 6 of the Universal Declaration on Bioethics and Human Rights states: “Any preventive, diagnostic and therapeutic medical intervention is only to be carried out with the prior, free and informed consent of the person concerned, based on adequate information. The consent should, where appropriate, be express and may be withdrawn by the person concerned at any time and for any reason without disadvantage or prejudice.”
On November 4th 2020 Theresa May MP made a speech in the House of Commons. She was referring to the closure of places of worship when she said, “My concern is that the Government today making it illegal to conduct an act of public worship, for the best of intentions, sets a precedent that could be misused by a Government in future with the worst of intentions, and that has unintended consequences.” I fear the same could be said for the introduction of vaccination passports.
Personally I have declined this vaccine because of the concerns outlined above. I hope this decision does not mean I am unable to work, visit a restaurant or travel.
Yours sincerely,
Dr Helen Westwood
Here is Nadhim Zahawi’s response, passed on to Dr Westood by Sir Graham Brady.
This is how Dr Westwood replied this week.
Dear Sir Graham,
Thank you for sending me the letter you received from Nadhim Zahawi MP, Minister for Business and Industry & Minister for COVID Vaccine Deployment in response to the representations you made to him on my behalf. I have attached his letter and my original email.
I must say I find his responses entirely unsatisfactory. He has failed to address any of my concerns. I know he is an intelligent man, so I can only assume that he has been deliberately disingenuous rather than not understanding the questions posed.
I am already aware of the processes involved in the development and testing of new drugs. I understand that Phases 2 and 3 are usually run sequentially but, given the urgency of this situation, a pragmatic decision was taken to run them in parallel. For elderly patients at increased risk from COVID-19 infection I can understand this approach. However, when the program is being rolled out to younger, healthy individuals whose risk-benefit ratio is entirely different, an alternative approach is required. It is imperative that individuals are not exposed to a greater risk of harm undergoing a medical intervention than the risk of not doing anything. Primum non nocere. Since my original email, significant concerns have been raised in a number of European countries about the risk of rare cerebral venous sinus thromboses associated with thrombocytopenia. Young, fit, healthy people who were at negligible risk of COVID-19 have tragically died.
Mr Zahawi has elected not to make any comment on the concerns I raised regarding rises in mortality in the immediate post-vaccination period. This is a pattern that has been repeated in multiple locations, currently most notably in India. I would like to know what research is being done by the UK Government to investigate this.
I note that Mr Zahawi referred to the fact that the UK “currently operates a system of informed consent for vaccinations”. I have two concerns regarding this statement. Firstly, how is the consent fully informed if we do not know the answers to the questions I have raised? I know from first hand experience that individuals attending for Covid vaccinations are not routinely being informed that the clinical trials are ongoing until 2023. Nor is the potential issue of antibody dependent enhancement being discussed. The advice for vaccinating pregnant women changes virtually day by day. Secondly, why does he need to use the word “currently”? Are there plans for mandatory vaccination in future? Already there are discussions about making vaccination compulsory for care home workers. In September 2019 the Guardian reported that Secretary of State for Health Matt Hancock was seriously considering making vaccinations compulsory for state school pupils. I defy anyone not to find this proposal chilling.
With regard to black, Asian and minority ethnic populations, again Mr Zahawi seems to have entirely missed my point. I was not arguing for the prioritisation of these groups; I was pointing out that uptake in these groups has been lower and therefore any certification system has the potential to lead to indirect discrimination.
I agree with Mr Zahawi that an effective vaccine is an excellent way to protect those that need protection, but it also needs to be safe. Given his failure to address the concerns I raised I can only assume he does not have answers to my questions.
Yours sincerely,
Dr Helen Westwood
Search & Seizure at Home of Judge Who Rendered the Sensational Weimar Mask-Judgment
2020News | April 26, 2021
As 2020News has just learned, the judge at the Weimar District Court, Christian Dettmar, had his house searched today. His office, private premises and car were searched. The judge’s cell phone was confiscated by the police. The judge had made a sensational decision on April 8, 2021, which was very inconvenient for the government’s anti Coronavirus measures policy.
At the suggestion of a mother, the judge had ruled in a child welfare proceeding pursuant to Section 1666 of the German Civil Code (BGB), Ref.: 9 F 148/21, that two Weimar schools were prohibited with immediate effect from requiring students to wear mouth-nose coverings of any kind (especially qualified masks such as FFP2 masks), to comply with AHA minimum distances, and/or to participate in SARS-CoV-2 rapid tests. At the same time, it had determined that classroom instruction should be maintained (full text of the ruling in German including three expert opinions – English translation will be available soon).
This was the first time that evidence was presented before a German court regarding the scientific reasonableness and necessity of the prescribed anti-Corona measures. The expert witnesses were the hygienist Prof. Dr. med Ines Kappstein, the psychologist Prof. Dr. Christof Kuhbandner and the biologist Prof. Dr. rer. biol. hum. Ulrike Kämmerer.
After examining the factual and legal situation and evaluating the expert opinions, the judge came to the conclusion that the measures he had forbidden posed a present danger to the mental, physical or psychological well-being of the child to such an extent that significant harm could be foreseen with a high degree of certainty in the event of further development without intervention.
He wrote: “… the children are not only endangered in their mental, physical and spiritual well-being by the obligation to wear face masks during school hours and to keep their distance from each other and from other persons, but, in addition, they are already being harmed. At the same time, this violates numerous rights of the children and their parents under the law, the constitution and international conventions. This applies in particular to the right to free development of the personality and to physical integrity from Article 2 of the Basic Law as well as to the right from Article 6 of the Basic Law to upbringing and care by the parents (also with regard to measures for preventive health care and ‘objects’ to be carried by children)…”
The judge agreed with the experts’ assessment that the masks were not useful for viral protection, that the PCR test could not detect a disease-causing infection with the necessary certainty, and that asymptomatic transmission played no detectable role epidemiologically with respect to SARS-CoV-2. On the contrary, the masks would have a negative impact on children’s health due to handling-related contamination. Testing in school classes would be unnecessary, harmful and also extremely problematic in terms of data protection.
The judge’s ruling confirms the mother’s assessment: “The children are harmed physically, psychologically and pedagogically and their rights are violated, without this being offset by any benefit for the children themselves or third parties.”
In conclusion, the judge stated, “100,000 elementary school students would have to put up with all the side effects of wearing masks for a week in order to prevent just one infection per week. To call this result merely disproportionate would be a wholly inadequate description. Rather, it shows that the state legislature regulating this area has fallen into a factual disconnect that has reached historic proportions.”
The decision, which 2020News analyzed – in English – in more detail here, had caused quite a stir. It had been downloaded about two million times from the 2020News website alone.
In a side note on the sidelines of proceedings with other parties, the decision in question had been described as unlawful by the Weimar Administrative Court without any comprehensible justification.
UK Hiring COVID Marshals to Patrol Streets Until 2023 Despite Lockdown Restrictions Supposedly Ending in June
By Paul Joseph Watson | Summit News | April 27, 2021
Government councils in the UK are hiring COVID Marshals to patrol streets from July until the end of 2023, despite the fact that all lockdown restrictions are supposed to end in June.
“A new army of Covid Marshals is being recruited for roles that could last until 2023 despite Government plans to lift all remaining restrictions on June 21,” reports the Telegraph.
“Councils around the country are advertising jobs that do not begin until July – several days after the supposed freedom day.”
One example is Hertfordshire County Council, which is “offering a contract of up to £3 million to firms that can supply 60 marshals from July 1 until January 31 next year.”
“The contract comes with a possible one-year extension, meaning marshals would still be patrolling until 2023,” states the report.
The Marshals will be tasked with ensuring “compliance” and helping the public understand “regulations and guidance,” despite the fact that all regulations are supposed to be terminated in 8 weeks time.
“We know that the virus is still circulating and will be for some time. We know from last year that numbers of infections can change rapidly, and Government are very clear that we should plan in case a third wave arises. It would be a dereliction of duty not to prepare for a third wave,” said Jim McManus, director of public health for Hertfordshire County Council.
Critics have accused the government of wasting taxpayer money by allowing councils to use government grants to fund the program.
“To start hiring people based on the situation we faced last year, before we had rolled out the vaccines, does seem to be a waste of public money,” said Mark Harper MP, Tory chairman of the Covid Recovery Group.
The fact that COVID Marshals will be patrolling the streets beyond June once again illustrates how the timetable to lift restrictions is completely phony.
Just like the UK government promised for months that it wouldn’t introduce vaccine passports while secretly funding their creation, the state has been caught lying yet again.
In all likelihood, fearmongering over a “third wave” of the virus, despite the UK vaccinating virtually all of its vulnerable population, will be used to reintroduce lockdown at the beginning of Autumn.
Are Covid Fatalities Comparable with the 1918 Spanish Flu?
By Ethan Yang | AIER | April 27, 2021
On April 23, 2021 The New York Times published an article titled “How Covid Upended a Century of Patterns in U.S. Deaths.” The article lays out some data regarding the unprecedented uptick in the US death rate that occured in 2020.

As shown in the graph provided by the New York Times, US death rates have been steadily declining over the past century, likely due to advances in technology and living standards. Last year certainly signaled a noticeable break from this trend with a sizable increase in deaths, but not nearly the same as the 1918 Flu which is a universal benchmark for a killer influenza virus.
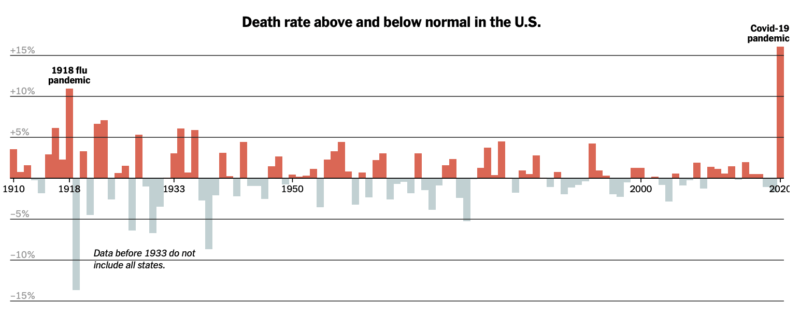
This graph provided by the New York Times indicates the spike in excess deaths in 2020, which is the number of deaths that have occured exceeding the predictions of standard death trends. This is of course all important information. Last year was certainly a horrific year with the outbreak of Covid-19, the lockdowns, and all the chaos that followed. It was a year of death and despair which should not be taken lightly.
Important Discussion: Deaths and Victims
It is common to invoke comparisons with the 1918 Flu Pandemic, as that was an extremely devastating virus that rocked the world. The article makes multiple references to the 1918 pandemic but there are a couple that raise interesting questions for further investigation. The first point is as follows,
“Combined with deaths in the first few months of this year, Covid-19 has now claimed more than half a million lives in the United States. The total number of Covid-19 deaths so far is on track to surpass the toll of the 1918 pandemic, which killed an estimated 675,000 nationwide.”
Comparing the death counts between the 1918 Flu and Covid-19 without adjusting for population growth is extremely misleading. In 1918 the population of the United States was roughly 103 million, while near the end of 2020 it stood at roughly 330 million. According to CDC statistics compiled by a study in JAMA Covid-19 killed 345,000 people in 2020 and now stands at around half a million as stated by the New York Times. Adjusted for the population growth of over 200 million people and holding the death rates constant, the 1918 Flu would have killed over 2 million people if it occured today, which is more than four times greater than Covid-19.
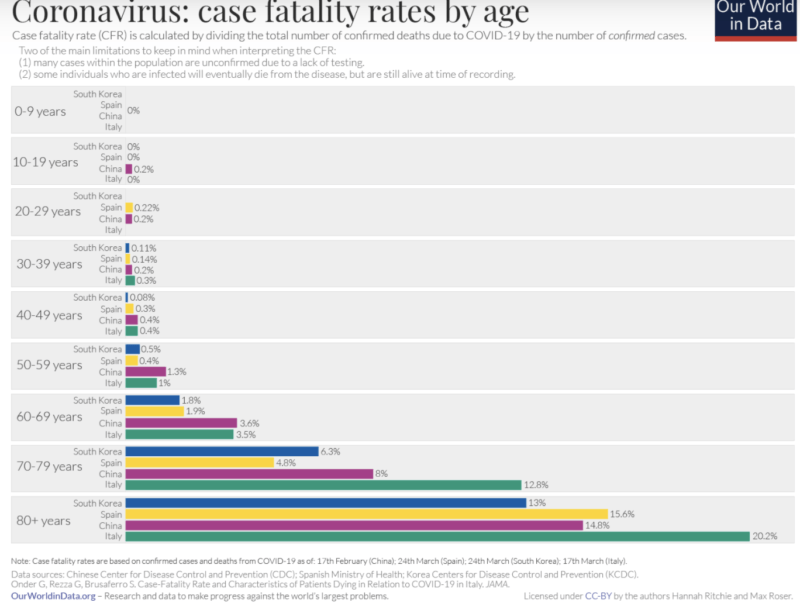
Furthermore, the two diseases are vastly different in terms of who is vulnerable. Covid-19’s severe outcomes almost exclusively affect the elderly and the immunocompromised, particularly those over the age of 65, which is also approaching the life expectancy of a human. Furthermore 94 percent of Covid deaths occurred with preexisting conditions. It poses virtually no risk to children, minimal risk to young adults, and only seems to kill more than 1 percent of victims with those over the age of 65.
On the other hand the Spanish Flu was devastating to virtually all age groups and did not discriminate between the healthy and the unwell. The CDC writes the following about the 1918 Flu:
“Mortality was high in people younger than 5 years old, 20-40 years old, and 65 years and older. The high mortality in healthy people, including those in the 20-40 year age group, was a unique feature of this pandemic.”
It is clear that the comparison is flawed between the 1918 Flu and Covid-19, as the former was a devastating killer virus whereas the latter only poses a threat to vulnerable populations.
Too Much Statistical Noise
It is certainly worth investigating the noted increase in excess deaths in 2020 as that is obviously a problem. However, the article seems to suggest that Covid-19 was the main causal factor driving increases in death. Although that is certainly a reasonable intuition given that it is a novel virus, clearly there is far more at play.
The main issue to point out is that there were two health crises, not one. Covid-19 is certainly one but we cannot simply ignore the absolutely devastating and unprecedented use of lockdown policies that drastically upended all of society in a way that a virus could never accomplish.
The effects of lockdowns have been thoroughly studied by AIER and in a series of articles I noted just some of the damage to the economy, young people, and the normal functioning of society. All these disruptions led to adverse outcomes whether it be mental health issues, decline in living standards, or even disrupted healthcare procedures. In a press release the CDC noted that in May 2020, it recorded the highest number of drug overdoses ever recorded in a 12-month period.
A study in JAMA notes that although there was a substantial increase in overall deaths in 2020, Covid-19 was only one part of the problem, assuming all Covid deaths are directly attributable to Covid and not a comorbidity.

Some statistics of note are an increase in deaths due to heart disease, unintentional injuries, stroke, and diabetes. Although more investigation would be needed to understand how all of this comes together, it wouldn’t be absurd to believe that lockdown policies led to an increase in deaths due to their many disruptions to normal societal functions.
To cite one example of many, the Mackinac Center Legal Foundation recounts on one of its clients by writing,
“One of the affected medical practices, Grand Health Partners, operates in the Grand Rapids area. It performs endoscopies and other elective surgeries, many of which were deemed nonessential by executive order. Due to the shutdown, many of their patients were not able to receive treatment and have suffered because of it.”
Alongside exploring and cutting through the statistical noise posed by increases in death plausibly related to lockdowns, there still needs to be a discussion on quantifying the Covid-19 death count. Genevieve Briand, an economist at John Hopkins University, was subject to a massive degree of controversy for putting out a flawed but important lecture – later expanded into a research paper – that pointed out among other things that Covid-19 deaths may be inappropriately reclassified as deaths from other leading causes.
This is especially worthy of discussion given that the overwhelming majority of Covid deaths occur with comorbidities amongst eldery populations often nearing or exceeding life expectancy.
Key Takeaway
The data is clear; 2020 was a horrific year full of death and despair. The New York Times’ article certainly does a great job at starting a conversation about this topic. However, its comparisons of Covid-19 and the 1918 Flu raises more questions than answers. Furthermore its presentation of data regarding increases in deaths requires more context.
Upon further investigation, it is clear that Covid-19 claimed many lives. However, it is also clear that there is a substantial presence of statistical noise from comorbidities and increases in death from other causes. This raises many questions not just about the collateral damage of our policy response, but also about whether we are even operating with the appropriate information to be making such decisions with people’s lives in the first place.
Lockdowns Devastating For Child Development & Language Skills
By Richie Allen | April 27, 2021
A major survey has concluded that lockdowns are having a devastatingly negative impact on child development. Data from 50,000 pupils and a survey of schools across England, has revealed that an increased number of four- and five-year-olds need urgent help with their language skills.
The Education Endowment Foundation (EEF) research suggests that the lockdowns have deprived the youngest children of social contact and experiences essential for developing their vocabulary. According to the BBC:
Less or no contact with grandparents, social distancing, no play dates, and the wearing of face coverings in public have left children less exposed to conversations and everyday experiences.
Of 58 primary schools surveyed across England:
- 76% said pupils starting school in September 2020 needed more support with communication than in previous years
96% they were concerned about pupils’ speech-and-language development. - And 56% of parents were concerned about their child starting at school following the lockdown in the spring and summer.
Sally Miner, head teacher at Ryder Hayes school in Walsall told the BBC that problems with communication were “really limiting” for young children, particularly if they were unable to express themselves, interact with peers and make themselves understood.
“It’s absolutely key,” she said. “It’s all about a child’s self-esteem and confidence. She went on to say:
“All the research shows that if a child does have issues with language at that age, by adulthood they’re four times more likely to struggle with reading, three time more likely to have mental health issues, twice as likely to be unemployed and have social-mobility issues, so getting this right at such an early age is literally the key to children’s futures.”
Lockdowns are a crime against humanity. Lockdowns are a form of child abuse. If lockdowns are child abuse, the witch doctors and lying politicians responsible for them are child abusers, plain and simple. There must be a day of reckoning for them.
Canadian government seeks to police videos posted on social media in ‘assault’ on free speech
RT | April 27, 2021
Critics of Canada’s Liberal government are accusing it of mounting an ‘assault’ on free speech after it proposed modifications to a broadcasting law that would enable it to regulate user-generated video content on social media.
At the heart of the controversy is ‘Bill C-10’, an amendment to the Canadian Broadcasting Act (1991) that purports to give the Canadian Radio-television and Telecommunications Commission (CRTC) oversight abilities over online streaming services such as Netflix and Amazon.
When the Trudeau government introduced the bill, it contained language exempting content created by individuals. But that clause was removed by a parliamentary committee during the bill’s final review stages on Friday, creating an avenue for the CRTC to treat YouTube videos and TikTok posts uploaded by Canadian users as ‘programs’ – the same way it does broadcast networks.
The move “doesn’t just infringe on free expression, it constitutes a full-blown assault upon it and, through it, the foundations of democracy,” according to former CRTC commissioner Peter Menzies.
“It’s difficult to contemplate the levels of moral hubris, incompetence or both that would lead people to believe such an infringement of rights is justifiable,” Menzies told the National Post newspaper.
The bill’s critics said the changes – made by the Liberal-dominated House of Commons Heritage committee – were especially alarming in light of recent proposals by Heritage Minister Steven Guilbeault to give Ottawa the power to order platforms to take down content deemed objectionable.
At present, online services like Netflix and Amazon Prime are not subject to Canadian content rules.
A spokesperson for Guilbeault told the Toronto Star that the bill would still “exempt individual users from being considered broadcasters” and the clause was simply removed to allow for better regulation of things like music playlists.
“Where content uploaded by individual users is curated by a platform, and is deemed of significant impact, that platform, not the users, could be subject to the Broadcasting Act,” she told the paper.
But critics aren’t buying it. Cara Zweibel, fundamental freedoms programs director at the Canadian Civil Liberties Association, contends that the legislation “opens up a regulatory door” for Ottawa to implement future regulations on user content.
The same concerns were echoed on social media. University of Ottawa law professor Michael Geist asked Guilbeault how “removing your own legislative safeguards and regulating user generated content for millions of Canadians” could be considered as “standing up to web giants”?
Meanwhile, privacy lawyer David Fraser branded the minister’s approach to policymaking an “incoherent word salad of buzzwords.”
“Regulating what I post on YouTube or forcing Facebook or Twitter to pay for news links that I share on their platforms is simply idiotic,” he wrote.
Others said the Liberals took an “already bad law” and made it worse, warning of an “exodus” from platforms if it came into force.
Not everyone was against the proposals, however. Daniel Bernhard, executive director of advocacy group Friends of Canadian Broadcasting, said the bill was not the “assault on liberty some were making it out to be.”
In a series of tweets that denounced “hypothetical concerns” about a “tyrannical CRTC”, Bernhard said options to regulate social media monopolies are “far less intense than broadcast licensing” and that “even in that hyper regulated system, CRTC has never been found to have censored or intervened in programming.”
CNN’s New “Reporter,” Natasha Bertrand, is a Deranged Conspiracy Theorist and Scandal-Plagued CIA Propagandist

CNN’s new national security reporter Natasha Bertrand, then of Politico and NBC News, with MSNBC’s Rachel Maddow, Sept. 19, 2019
By Glenn Greenwald | April 27, 2021
The most important axiom for understanding how the U.S. corporate media functions is that there is never accountability for those who serve as propagandists for the U.S. security state. The opposite is true: the more aggressively and recklessly you spread CIA narratives or pro-war manipulation, the more rewarded you will be in that world.
The classic case is Jeffrey Goldberg, who wrote one of the most deceitful and destructive articles of his generation: a lengthy New Yorker article in May, 2002 — right as the propagandistic groundwork for the invasion of Iraq was being laid — that claimed Saddam Hussein had formed an alliance with Al Qaeda and Osama bin Laden. In February, 2003, on the eve of the invasion of Iraq, NPR host Robert Siegel devoted a long segment to this claim. When he asked Goldberg about “a man named Abu Musab al-Zarqawi,” Goldberg replied: “He is one of several men who might personify a link between Iraq and al-Qaeda.”
Needless to say, nothing could generate hatred for someone among the American population — just nine months away from the 9/11 attack — more than associating them with bin Laden. Five months after Goldberg’s New Yorker article, the U.S. Congress authorized the use of military force to impose regime change on Iraq; ten months later, the U.S. invaded Iraq; and by September, 2003, close to 70% of Americans believed the lie that Saddam had personally participated in the 9/11 attack.

Goldberg’s fabrication-driven article generated ample celebratory media attention and even prestigious journalism awards. It also led to great financial reward and career advancement. In 2007, The Atlantic‘s publisher David Bradley lured Goldberg away from The New Yorker by lavishing him with a huge signing bonus and even sent exotic horses to entertain Goldberg’s children. Goldberg is now the editor-in-chief of that magazine and thus one of the most influential figures in media. In other words, the person who wrote what is arguably the most disastrous article of that decade was one most rewarded by the industry — all because he served the aims of the U.S. security state and its war aims. That is how U.S. corporate journalism functions.
Another illustrative mascot for this lucrative career path is NBC’s national security correspondent Ken Dilanian. In 2014, his own former paper, The Los Angeles Times, acknowledged his “collaborative” relationship with the CIA. During his stint there, he mimicked false claims from John Brennan’s CIA that no innocent people were killed from a 2012 Obama drone strike, only for human rights groups and leaked documents to prove many were.
A FOIA request produced documents published by The Intercept in 2015 that showed Dilanian submitting his “reporting” to the CIA for approval in violation of The LA Times’ own ethical guidelines and then repeating what he was told to say. But again, serving the CIA even with false “reporting” and unethical behavior is a career benefit in corporate media, not an impediment, and Dilanian rapidly fell upward after these embarrassing revelations. He first went to Associated Press and then to NBC News, where he broadcast numerous false Russiagate scams including purporting to “independently confirm” CNN’s ultimately retracted bombshell that Donald Trump, Jr. obtained advance access to the 2016 WikiLeaks archive.
On Monday, CNN made clear that this dynamic still drives the corporate media world. The network proudly announced that it had hired Natasha Bertrand away from Politico. In doing so, they added to their stable of former CIA operatives, NSA spies, Pentagon Generals and FBI agents a reporter who has done as much as anyone, if not more so, to advance the scripts of those agencies.
Bertrand’s career began taking off when, while at Business Insider, she abandoned her obsession with Russia’s role in Syria in 2016 in order to monomaniacally fixate on every last conspiracy theory and gossip item that drove the Russiagate fraud during the 2016 campaign and then into the Trump presidency. Each month, Bertrand produced dozens of Russiagate articles for the site that were so unhinged that they made Rachel Maddow look sober, cautious and reliable.
In 2018, it was Jeffrey Goldberg himself — knowing a star CIA propagandist when he sees one — who gave Bertrand her first big break by hiring her away from Business Insider to cover Russiagate for The Atlantic. Shortly after, she joined the Queen of Russiagate conspiracies herself by becoming a national security analyst for MSNBC and NBC News. From there, it was onto Politico and now CNN : the ideal, rapid career climb that is the dream of every liberal security state servant calling themselves a journalist. Her final conspiratorial article for The Atlantic before moving to Politico is the perfect illustration of who and what she is:

CNN’s new national security star was no ordinary Russiagate fanatic. There was no conspiracy theory too unhinged or evidence-free for her to promote. As The Washington Post‘s media reporter Erik Wemple documented once the Steele Dossier was debunked, there was arguably nobody in media other than Rachel Maddow who promoted and ratified that hoax as aggressively, uncritically and persistently as Bertrand. She defended it even after the Mueller Report corroborated virtually none of its key claims.
In a February, 2020 article headlined “How Politico’s Natasha Bertrand bootstrapped dossier credulity into MSNBC gig,” Wemple described how she was rewarded over and over for “journalism” that would be regarded in any healthy profession with nothing but scorn:
Where there’s a report on Russian meddling, there’s an MSNBC segment waiting to be taped. Last Thursday night, MSNBC host Joy Reid — subbing for “All In” host Chris Hayes — turned to Politico national security reporter Natasha Bertrand with a question about whether Trump “wants” Russian meddling or whether he can’t accept that “foreign help is there.“ Bertrand responded: “We don’t have the reporting that suggests that the president has told aides, for example, that he really wants Russia to interfere because he thinks that it’s going to help him, right?”
No, we don’t have that reporting — though there’s no prohibition against fantasizing about it on national television. Such is the theme of Bertrand’s commentary during previous coverage of Russian interference, specifically the dossier of memos drawn up by former British intelligence officer Christopher Steele. With winks and nods from MSNBC hosts, Bertrand heaped credibility on the dossier — which was published in full by BuzzFeed News in January 2017 — in repeated television appearances.
Wemple systematically reviewed the mountain of speculation, unproven conspiracies and outright falsehoods Bertrand shoveled to the public as she was repeatedly promoted. But it was the document that gave us deranged delusions about pee-pee tape blackmail and Michael Cohen’s trip to Prague that was her crown jewel: “The Bertrand highlight reel features a great deal of thumb-on-scale speculation regarding the dossier,” Wemple wrote.
And when information started being declassified that proved much of Bertrand’s claims about collusion to be a fraud, she complained that there was too much transparency, implying that the Trump administration was harming national security by allowing the public to know too much — namely, allowing the public to see that her reporting was a fraud. A journalist who complains about too much transparency is like a cardiologist who complains that a patient has stopped smoking cigarettes, or like a journalist who voluntarily rats out her own source to the FBI or who agitates for censorship of political speech: a walking negation of the professional values they are supposed to uphold. But that is Natasha Bertrand, and, to the extent that there are some people who still believe that working at CNN is desirable, she was just rewarded for it again yesterday — just as journalists who rat out their own sources to the FBI and advocate for internet censorship are now celebrated in today’s rotted media climate.
Bertrand’s trail of journalistic scandals and recklessness extend well beyond her Russiagate conspiracies. Last October, she published an article in Politico strongly implying that Director of National Intelligence John Ratcliffe was speaking without authorization or any evidence when he said Iran was attempting to undermine President Trump’s 2020 presidential campaign. But last month, the Biden administration declassified an intelligence report which said they had “high confidence” that Iran had done exactly what Ratcliffe alleged: namely, run an influence campaign to hurt Trump’s candidacy. A former national security official, Cliff Sims, said upon hearing of CNN’s hiring that he explicitly warned Bertrand’s editors that the story was false but they chose to publish it anyway.
It was also Bertrand who most effectively laundered the extremely significant CIA lie in October, 2020 that the documents obtained by The New York Post about the Biden family’s business dealings in China and Ukraine were “Russian disinformation.” Even though the John-Brennan-led former intelligence officials admitted from the start that they had no evidence for this claim, Bertrand not only amplified it but vouched for its credibility by writing that the Post‘s reporting “has drawn comparisons to 2016, when Russian hackers dumped troves of emails from Democrats onto the internet — producing few damaging revelations but fueling accusations of corruption by Trump” (that those 2016 DNC and Podesta documents produced “few damaging revelations” would come as a big surprise to the five DNC operatives, led by Chairwoman Debbie Wasserman-Schultz, who were forced to resign when their pro-Hillary cheating was revealed).
It was this Politico article by Bertrand that was then used by Facebook and Twitter to justify their joint censorship of the Post‘s reporting in the weeks before the 2020 election, and numerous media outlets — including The Intercept — gullibly told their readers to ignore the revelations on the ground that these authentic documents were “Russian disinformation.” Yet once it did its job of helping defeat Trump, that claim was debunked when even the intelligence community acknowledged it had no evidence of Russian involvement in the appearance of these materials, and Hunter Biden himself admitted he was the subject of a federal investigation for the transactions revealed by those documents.

Politico, Oct. 19, 2020
But even when her fantasies and conspiracies are debunked, Bertrand — like a good intelligence soldier — never cedes any ground in her propaganda campaigns. She was, needless to say, one of the journalists who most vocally promoted the CIA’s story — published as Trump was announcing his plans to withdraw from Afghanistan — that Russia had paid bounties to the Taliban for the death of U.S. soldiers. Yet even when the U.S. intelligence community under Joe Biden admitted last week that it has only “low to moderate” confidence that this even happened — with the NSA and other surveillance agencies saying it could find no evidence to corroborate the CIA’s story — she continued to insist that nothing had changed with the story, denying last week on a Mediaite podcast that anything had happened to cast doubt on the original story: “I think it’s much more nuanced than it being a walk-back. I don’t think that’s right actually.”
Even a cursory review of Bertrand’s prolific output reveals an endless array of gossip, conspiracy and speculative assertions masquerading as journalism. The commentator Luke Thomas detailed many of these transgressions on Monday and correctly observed that “arguably no single reporter has contributed more to the deranged and paranoid national security fantasies of the center-left than Natasha Bertrand. She’s an embarrassment to her profession and will, therefore, fit right in at CNN.”
As Thomas noted, beyond all of Bertrand’s well-documented and consequential propaganda, “she sees conspiracies and perfidiousness around every corner,” pointing to this demented yet highly viral tweet that deciphered comments from former Sen. Orrin Hatch (R-UT) as inadvertently revealing some secret scheme to expand Trump’s pardon powers. That scheme, like most of her speculative predictions, never materialized.
Then there is her garden-variety ethical scandal. In January, freelancer Dean Sterling Jones accused Bertrand of stealing his work without credit or payment. In a post he published, Jones documented how he emailed Bertrand a draft with reporting he had been working on, and in response she agreed to report it jointly with him on a co-byline. Yet two weeks later, the article appeared in The Atlantic with Bertrand as the only named reporter. Only after Jones complained did they insert a sentence into the story begrudgingly citing him as a source. “By my count,” Jones wrote, “Bertrand’s article contains at least six unequivocal examples of direct copying and revisions of my work.” When he published his post detailing his accusations, Bertrand arrogantly refused even to provide comment to the freelancer whose work she pilfered.
Natasha Bertrand has spent the last five years working as a spokesperson for the alliance composed of the CIA and the Democratic Party, spreading every unvetted and unproven conspiracy theory about Russiagate that they fed her. The more loyally she performed that propagandistic function, the more rapidly she was promoted and rewarded. Now she arrives at her latest destination: CNN, not only Russiagate Central along with MSNBC but also the home to countless ex-operatives of the security state agencies on whose behalf Bertrand speaks.
Once again we see the two key truths of modern corporate journalism in the U.S. First, we have the Jeffrey Goldberg Principle: you can never go wrong, but only right, by disseminating lies and propaganda from the CIA. Second, the organs that spread the most disinformation and crave disinformation agents as their employees are the very same ones who demand censorship of the internet in the name of stopping disinformation.
I’ve long said that if you want to understand how to thrive in this part of the media world, you should study the career advancement of Jeffrey Goldberg, propelled by one reckless act after the next. But now the sequel to the Goldberg Rise is the thriving career of this new CNN reporter whose value as a CIA propagandist Goldberg, notably, was the first to spot and reward.
The Truth About the Covid ‘Crisis’ in India
By Will Jones • Lockdown Sceptics • April 27, 2021
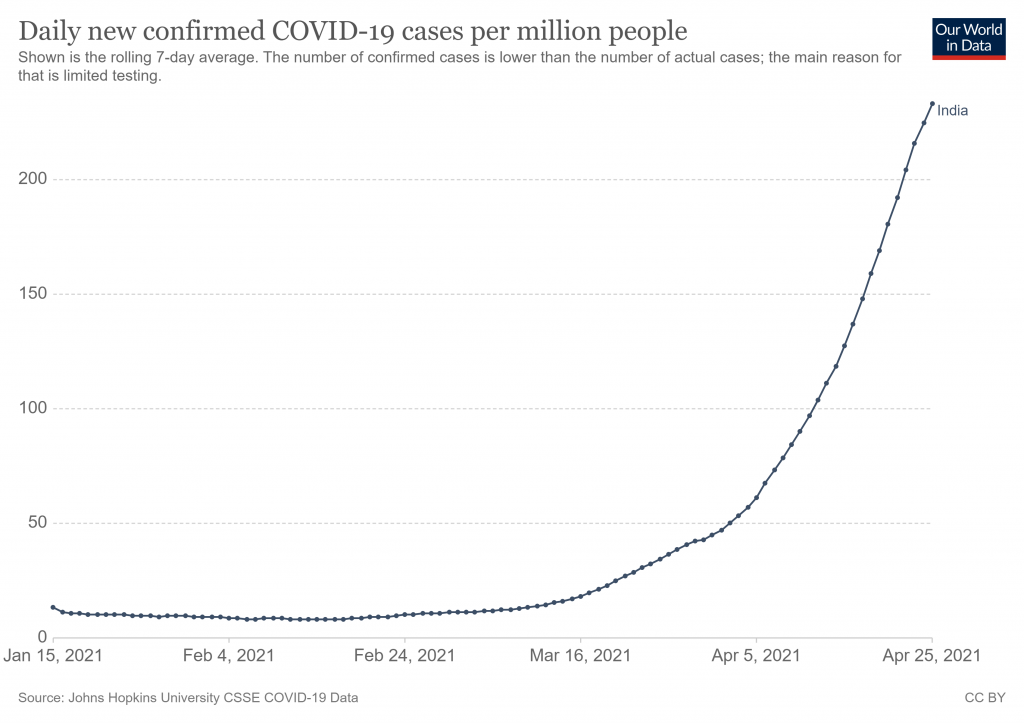
Now that Chile is settling down a bit, the latest Covid cautionary tale is India, which never seems to be out of the news at the moment as its positive cases and deaths have rocketed in the past few weeks.
Even the usually level-headed Kate Andrews in the Spectator has been painting the situation in lurid colours.
As it happened, the UK’s worst nightmares were never realised. The Nightingale hospitals built to increase capacity were barely used. But what the British Government feared most is now taking place elsewhere. India is suffering an exponential growth in infections, with more than 349,000 cases reported yesterday, as well as nearly 3,000 deaths. Hospitals are running out of oxygen for patients and wards are overflowing. There are reports of long queues as the sick wait to be seen by medical professionals. It’s expected the situation will deteriorate further before it gets better.
Jo Nash, who lived in India until recently and still has many contacts out there, has written a very good piece for Left Lockdown Sceptics putting the current figures in context – something no mainstream outlet seems to have any interest in doing.
Jo makes the crucial point that we need to keep in mind the massive difference in scale between India and the UK. At 1.4 billion people, India is more than 20 times larger than the UK, so to compare Covid figures fairly we must divide India’s by 20. So 2,000 deaths a day is equivalent to a UK toll of 100. India’s current official total Covid deaths of approaching 200,000 is equivalent to just 10,000 in the UK.
In a country the size of India and with the huge number of health challenges faced by the population, the number of Covid deaths needs to be kept in perspective. As Sanjeev Sabhlock observes in the Times of India, 27,000 people die everyday in India. This includes 2,000 from diarrhoea and 1,200 from TB (vaccinations for which have been disrupted by the pandemic). The lack of adequate hospital provision for Covid patients may be more a reflection of the state of the health service than the severity of the disease.

Jo Nash also points out that poor air quality plays a role.
Delhi, the focus of the media’s messaging, and the source of many of the media’s horrifying scenes of suffering, has the most toxic air in the world which often leads to the city having to close down due to the widespread effects on respiratory health…
Respiratory diseases including COPD, TB, and respiratory tract infections like bronchitis leading to pneumonia are always among the top ten killers in India. These conditions are severely aggravated by air pollution and often require oxygen which can be in short supply during air pollution crises…
According to my contacts on the ground, people in Delhi are suffering from untreated respiratory and lung conditions that are now becoming serious. I’ve also had breathing problems there when perfectly healthy and started to mask up to keep the particulate matter out of my lungs. I used to suffer from serious chest infections twice yearly during the big changes in weather in India, usually November/December and April/May. When I reluctantly masked up that stopped. My contacts have reported that the usual seasonal bronchial infections have not been properly treated by doctors afraid of getting Covid, and people’s avoidance of government hospitals due to fear of getting Covid. Undoubtedly, these fears will have been fuelled by the media’s alarmist coverage of the situation. Consequently, the lack of early intervention means many respiratory conditions have developed life-threatening complications. Also, people from surrounding rural areas often travel to Delhi for treatment as it has the best healthcare facilities and people can go there for a few rupees by train. This puts pressure on Delhi’s healthcare system during respiratory virus seasons.
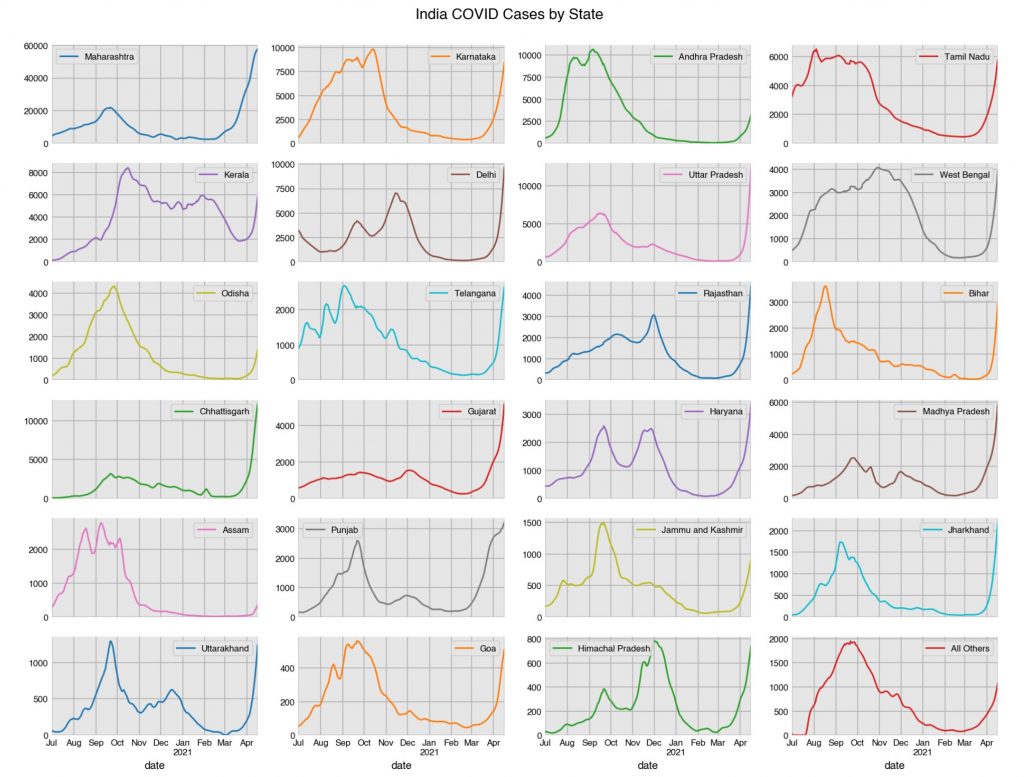
Positive cases look like they may be peaking in many regions now.
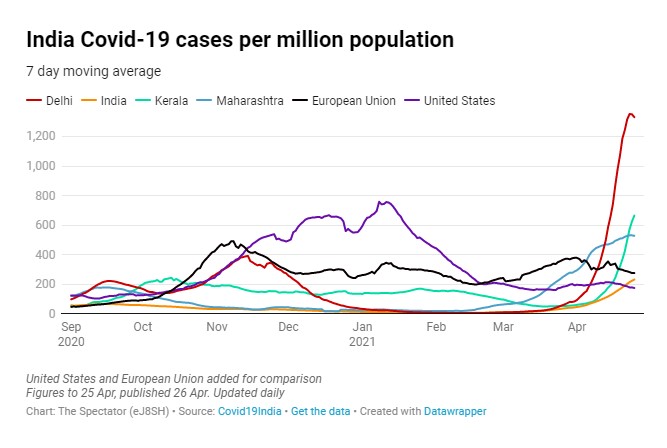
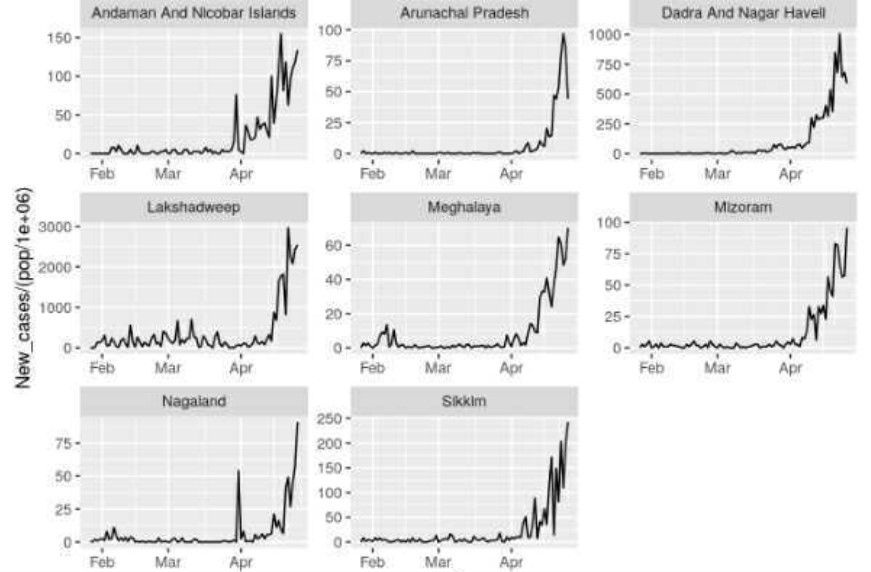
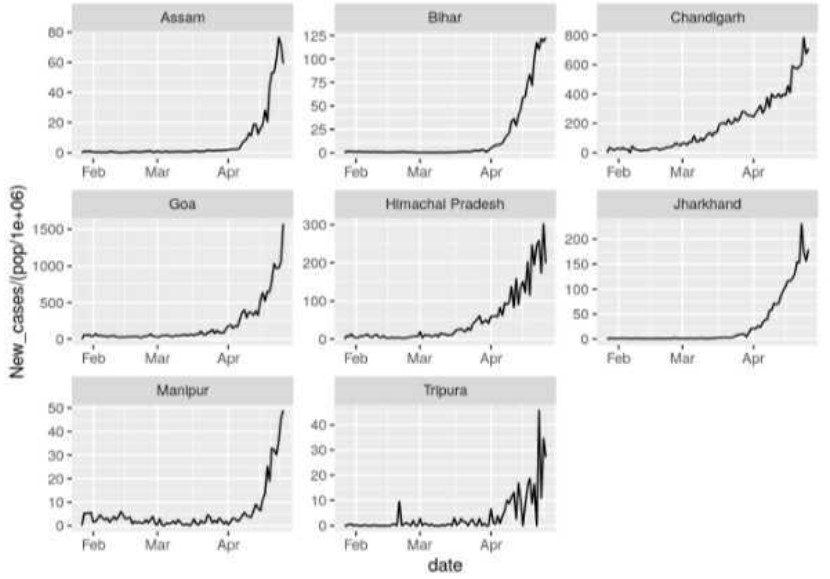
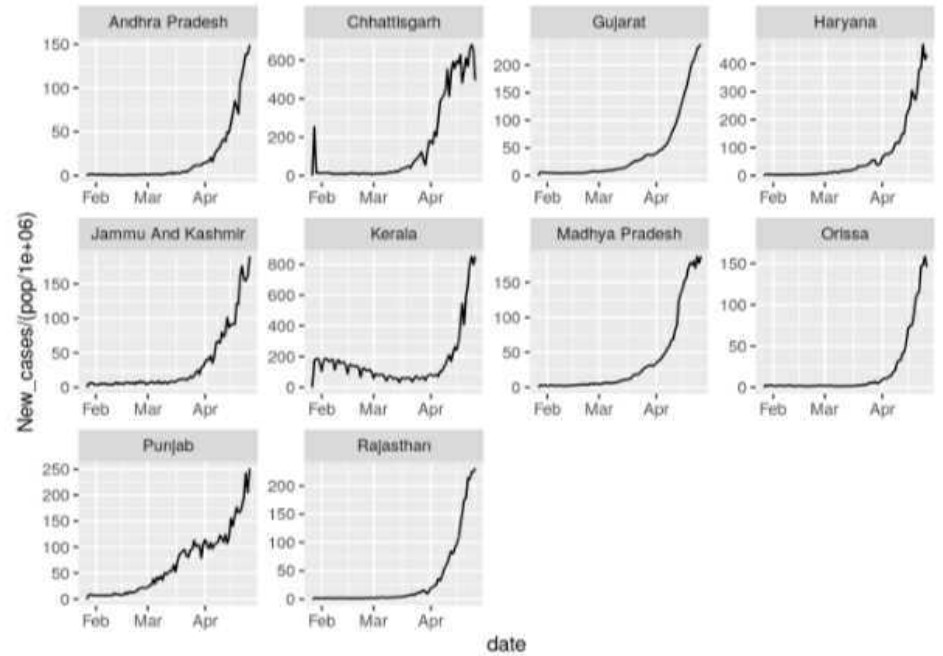
One mystery, as yet unexplained, is why India, which has not experienced a strong surge like this so far, suddenly did in March and April. Adding to the mystery is that the simultaneity of the surge across the regions is unexpected in a country as large as India and contrary to earlier outbreaks last year. Nick Hudson from Panda suggests it means there must be something artificial about it as it is not a natural pattern, since viruses naturally spread across the country with some delay and variation evident between regions.
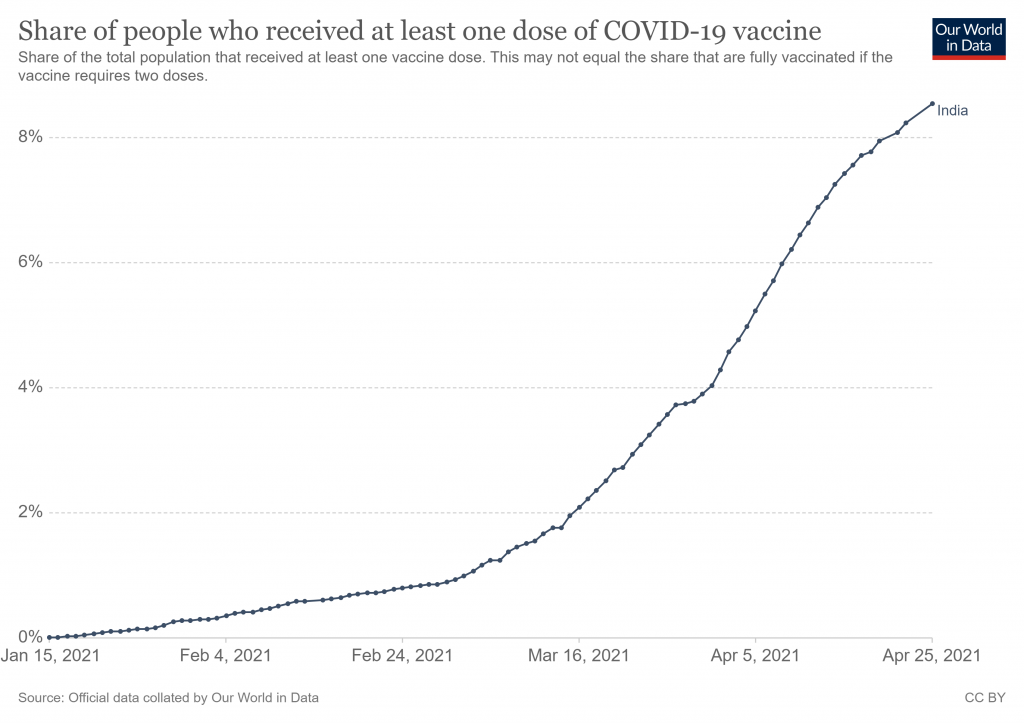
It hasn’t escaped people’s attention that one novel factor is the nationwide vaccine programme rollout, beginning in January and accelerating during March. Is this a further example of the post-vaccine infection spike seen in the various trials and population studies, possibly caused by temporary suppression of the immune system?
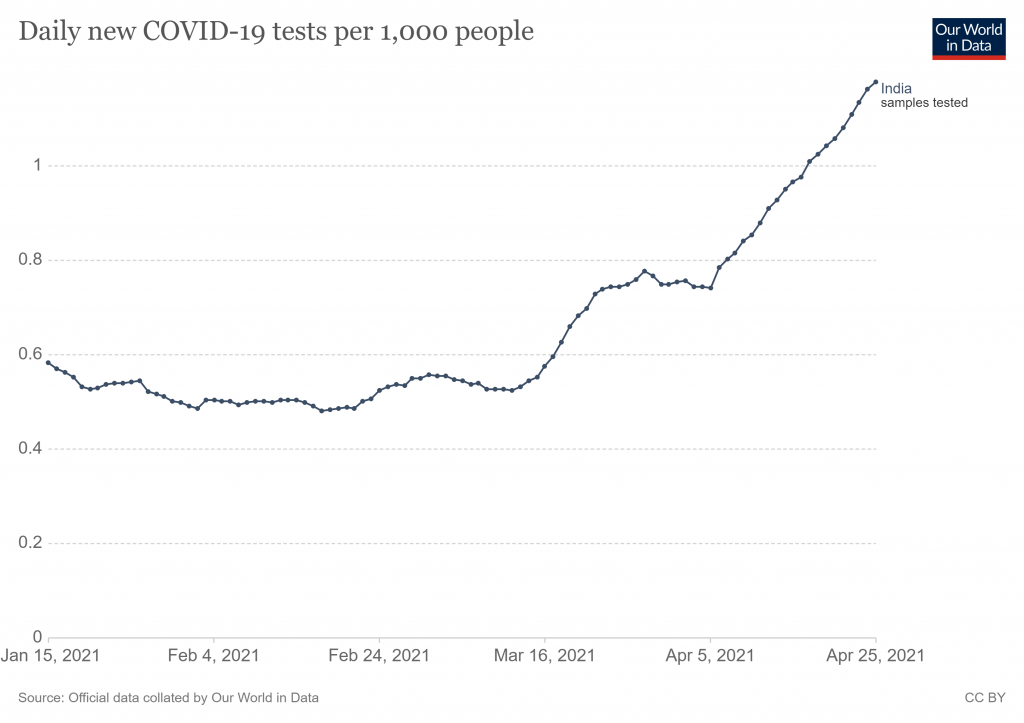
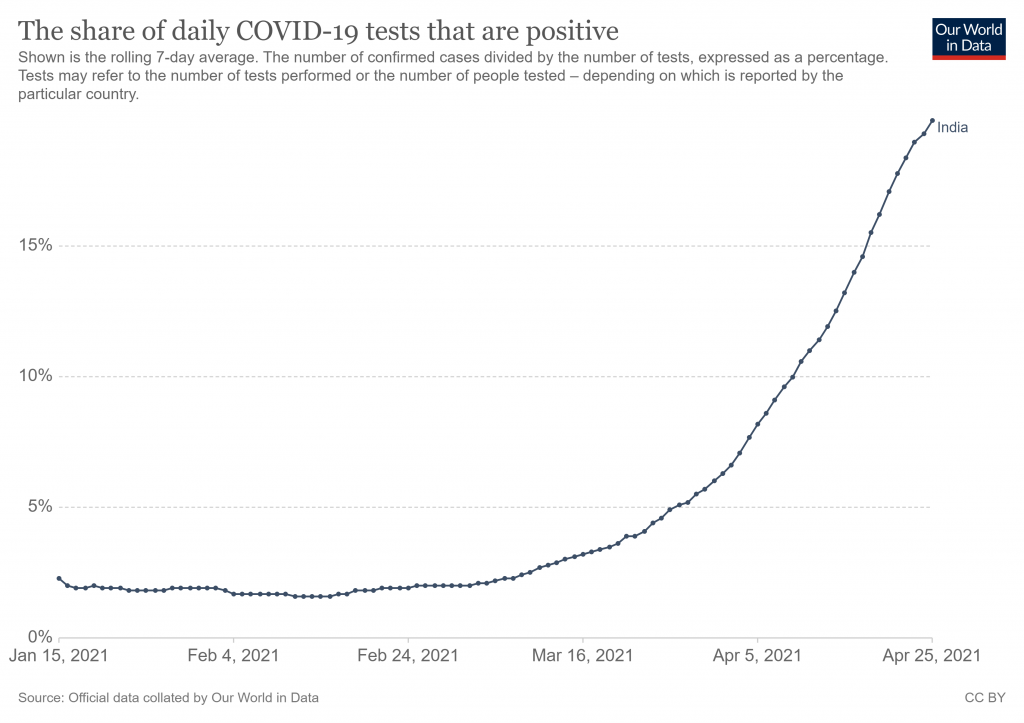
Testing is another possible factor, as the number of tests being carried out surged in March and April – though so did the positive rate, suggesting this can’t be the only explanation.
Whatever is going on, it’s a pity there is not more curiosity among our scientists and journalists. Instead, it’s just the usual scaremongering driven by the misrepresentation of data.
Stop Press: Former Assistant Secretary-General of the United Nations Professor Ramesh Thakur has been in touch with a comment he left on a story in the Australian.
Some context and perspective. India’s Covid deaths yesterday were 2,163 (seven-day rolling average). India’s average daily death toll is 25,000 from all causes.
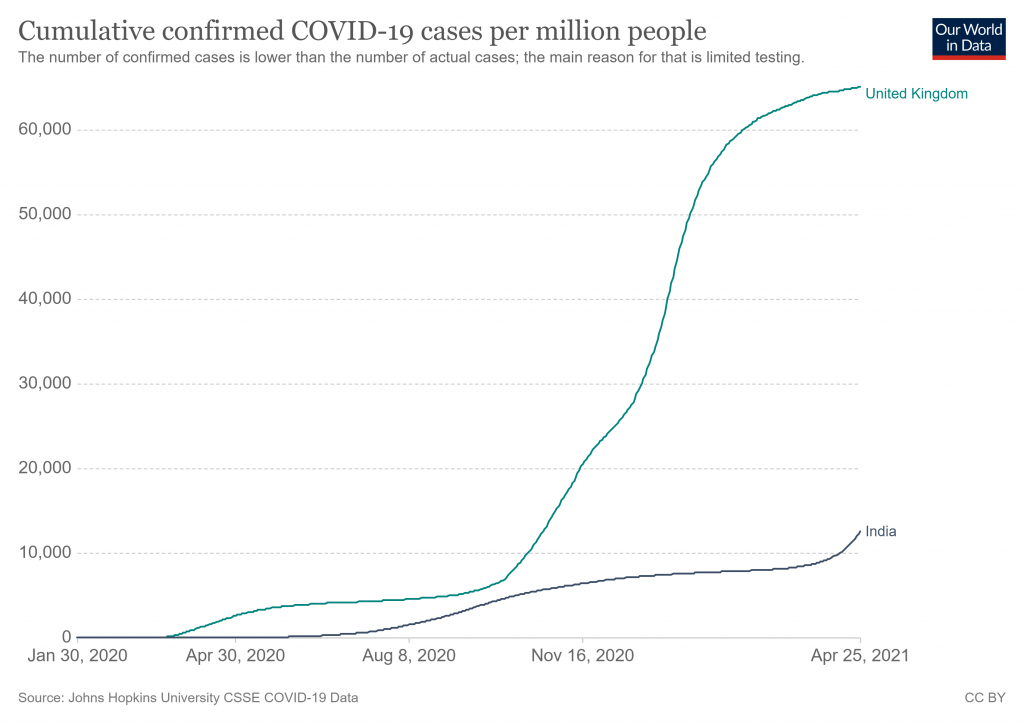
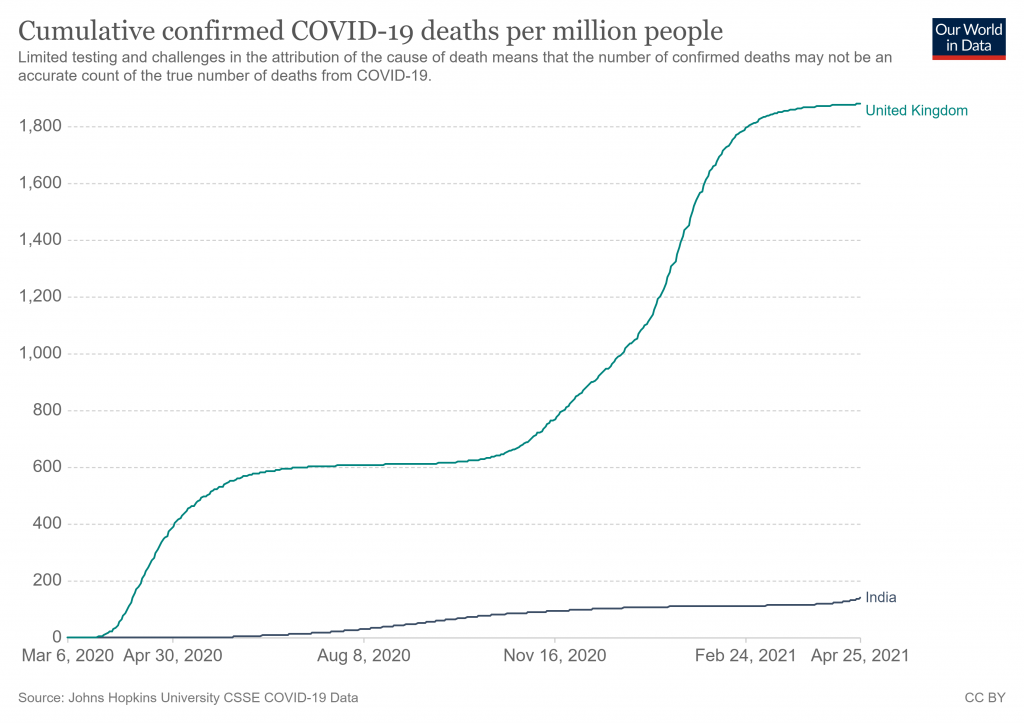
Second, despite this surge, as of now India’s Covid mortality rate is 140 dead per million people. This compares to 401 for the world average, 1,762 for the US, and 1,869 for the UK. It puts India 119th in the world on this, the single most important statistic for comparison purposes.
Third, the crux of the problem in India is not the proportion of cases and deaths from Covid. Rather, it is the lack of a fit-for-purpose public health infrastructure and medical supplies of equipment and drugs.
Fourth, although Government neglect of public health while prioritising vanity projects like a new Parliament building during the pandemic, building temples and statues etc. is a contributory factor, the real cause of a poor public health system is poverty. Put bluntly, poverty is the world’s biggest killer.
Fifth and finally, this is why a strong economy is not an optional luxury but an essential requirement for good health.
Featured Video

Pentagon insider says high US official Douglas Feith reported to Netanyahu
or go to
Aletho News Archives – Video-Images
Frlom the Archives
The Fiction of the Jewish History in Palestine
By Hasan Afif El-Hasan | The Palestine Chronicle | April 8, 2011
Prime Minister Benjamin Netanyahu told NNC Pierce Morgan on March 18, 2011 that he might agree to a Palestinian state through negotiations. And he added, “We will make territorial concessions although it is very painful to do that in our ancestral land.” Netanyahu was not talking about Poland where his ancestors lived. He was talking about Palestine where generations of its indigenous population ancestors lived, cultivated the land and are buried.
By the end of the nineteenth century, Zionism created a new Jewish identity of blood and soil. To mobilize their followers and supporters and appeal to their emotions, the Zionists created myths. Zionism started as a tribal religion without god, but in order to fulfill its function as a unifying force, Zionism required external religious and race symbols, not inner content. Its leaders regarded metaphysical religious belief and purity of race as having value in itself. They created a divine paradisiacal state of merger with the gods. Despite his non-religious ideology, Herzl’s writings were replete with religious references. The Jews should settle in Palestine because, in his words, “the Temple will be visible from long distance, for it is only our ancient faith that has kept us together”.
The Zionists and their supporters have invested tremendous financial and scholarly resources to work within the Hebrew Bible historical narratives to affirm the links between the intrusive Zionist population and the ancient Israelite past, and by doing so assert the right of that population to the land. The political end-game shaped the investigation and the outcome. Tracing the roots of Israel’s ethnic state in biblical antiquity is effectively to silence the indigenous Palestinian claim to the past and therefore to the land. The Biblical scholarship employs a bewildering array of terms for the region: “the Holy Land”, “the Land of the Bible”, “Eretz Israel”, “the Land of Israel”, or “Judah and Samaria.” To the casual reader these names appear interchangeable, but they all imply connection to ancient Israel.
Biblical narratives or poems that cannot be supported by archeology and common sense are treated by the Zionists and their supporters as historical language. … continue
Blog Roll
 Aletho News
Aletho News- Pentagon insider says high US official Douglas Feith reported to Netanyahu
- The Sludging of Rural America
- Lawyers’ groups demand end to British military bases in Cyprus
- CIA Assessment: The Resistance Cannot Be Crushed
- Hezbollah Returns: It Didn’t Start a War, It Is Ending One
- EU states seek ‘talks’ with Iran for access to Strait of Hormuz: Report
- Trump on Hormuz: “Others must take care of it” after US falters
- Who Is closer to collapse?
- A War that Backfired: Why the US-Israeli Campaign Is Strengthening Iran
- How Zionist Control Is Hurting US Interests
- If Americans Knew
- As US-Israel war on Iran rages, Gaza faces massive dust storm – Not a ceasefire Day 156
- No let-up in attacks on Gaza as Israel takes on Iran, Lebanon – Not a ceasefire Day 155
- ‘Of Course’: IDF Drops Case Against Soldiers Accused of Raping Palestinian Prisoner
- Don’t Fall for the Regime Change Talk. Israel Is ‘Mowing the Lawn’ in Iran
- Will Israel and the US wreck the Gulf States along with Iran?
- US so far burned through ‘years’ of munitions in Iran war: Report
- How the Israeli Tail Wags the American Dog
- Outdated intel likely led to deadly U.S. strike on Iranian elementary school, sources say
- Pentagon insider says high U.S official Douglas Feith reported to Netanyahu
- In fond memory of Walid Khalidi, the historian of Palestine
- No Tricks Zone
- Storing Green Energy To Last Germany 10 Days Would Require A 60-Million Tonne Battery
- New Studies: UK Sea Levels Were 4 Meters Higher Than Today During The Mid-Holocene
- Destructive Green New Deal: German Energy And Metal Group Warns Of Drastic Crisis
- New Study Documents A 20-Year Pause In Arctic Sea Ice Decline – Driven By Internal Variability
- Wake-up Call: Survey Shows Majority Of Germans Now Favor Postponing Climate Targets!
- Televised! Leading German Political Candidate Tells Schoolchildren CO2 Makes Sun Hotter!
- New Study: A Century Warming Of 1.1°C Is ‘Commonplace’ And ‘Not Unusual’ During This Interglacial
- New Study: ‘Internal Noise’ And Volcanic Forcing Can Trigger 10-15°C Warming Within Decades
- Glaciers Worldwide Are Suddendly Surging, Experts Blame Warming!
- Surprising Discovery: Sahara Is Greening…Billions Of Trees Where Once Thought To Be Barren
