More Important Ivermectin Study Results
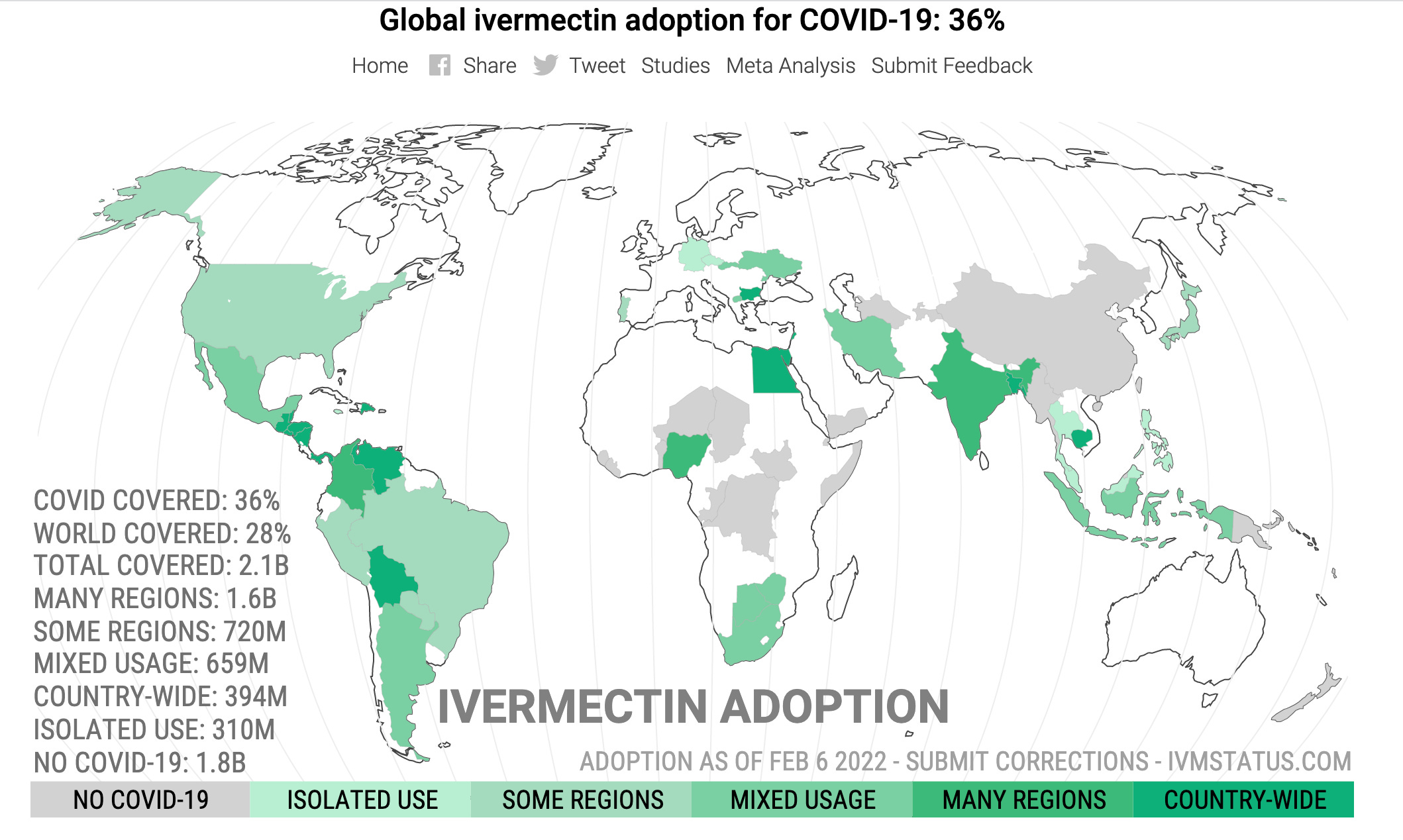
Click here for more details on the map above
By Robert W Malone MD, MS | February 6, 2022
Research Gate, February 2022 DOI:10.13140/RG.2.2.20069.68320
This important preprint needs to hit alternative and mainstream media now.
The Study:
Background: Previously, we demonstrated that ivermectin use as prophylaxis for COVID-19 was associated with reductions in COVID-19 infection, hospitalization, and mortality rates, and in the risk of dying from COVID-19, irrespective of regularity and accumulated use of ivermectin, in an observational, prospectively obtained data from a strictly controlled city-wide program in a city in Southern Brazil (Itajaí, SC, Brazil) of of medically-based, optional use of ivermectin as prophylaxis for COVID-19.
In this study, our objective was to explore the data obtained from the program to evaluate whether the level of regularity of ivermectin use impacted in the reductions in these outcomes, aiming to determine if ivermectin showed a progressive dose-, regularity-response in terms of protection from COVID-19 and COVID-19 related outcomes.
Materials and methods: This is a prospective observational study of the program mention above, that used ivermectin at a dose of 0.2mg/kg/day for two consecutive days, every 15 days. We obtained and analyzed the data regarding the accumulated dose of ivermectin use, in addition to age and co-morbidities, to analyze the patterns of reduction of COVID-19 infection, hospitalization, and mortality rates, and risk of dying from COVID-19, according to the regularity and amount of ivermectin used in a 5-month period.
Following definitions of regularity, we considered as strictly regular subjects that used at least 180mg of ivermectin (180mg = 30 tablets), and as sporadic users subjects that used 60mg (= 10 tablets) or less during the 5-month period.
Comparisons between subjects that did not use ivermectin and these two levels of regularity of ivermectin use were performed. Analysis of the intermediate levels of ivermectin use are present in the supplement appendix of this study. To analyze hospitalization and mortality rates, we utilized the database of COVID-19 infections of all participants, from Itajaí and outside. To analyze COVID-19 infection rate and risk of dying from COVID-19 we utilized the Itajaí city database.
Propensity score matching (PSM) was employed, followed by multivariate adjusted analysis for residual differences (doubly adjusted analysis).
Results:
- Of the 7,345 cases of COVID-19, 3,034 occurred in non-users, 1,627 in sporadic users, and 289 in strict users, while the remaining cases occurred in the intermediate levels of ivermectin use. Strict users were older (p < 0.0001) and non-significant higher prevalence of type 2 diabetes and hypertension.
- COVID-19 infection rate was 39% lower among strict users [4.03% infection rate; ( p < 0.0001] than in non-users (6.64% infection rate), and non-significant 11% reduction compared to sporadic users (4.54% infection rate) (n = 1,627 in each group; RR, 0.89; 95%CI 0.76 – 1.03; p = 0.11).
- Hospitalization rate was reduced by 100% in strict users, compared to non-users and to sporadic users, both before and after Propensity score matching ( p < 0.0001).
- After Propensity score matching, hospitalization rate was 35% lower among sporadic users than non-users (RR, 0.65; 95%CI, 0.44 – 0.70; p = 0.03).
- In propensity score matched groups, multivariate-adjusted mortality rate was 90% lower in strict users compared to non-users (p = 0.003) and 79% lower than in sporadic users (p = 0.05), while sporadic users had a 37% reduction in mortality rate compared to non-users (p = 0.043).
- Risk of dying from COVID-19 was 86% lower among strict users than non-users (p = 0.006) and marginally significant, 72% lower than sporadic users (p = 0.083), while sporadic users had a 51% reduction compared to non-users (p = 0.001).
Conclusion: Non-use of ivermectin was associated with a 10-times increase in mortality risk and 7-times increased risk of dying from COVID-19, compared to strictly regular use of ivermectin in a prospectively collected, strictly controlled population.
A progressive dose-response pattern was observed between level of ivermectin use and level of protection from COVID-19 related outcomes and consistent across different levels of ivermectin use.
The results of this study clearly demonstrate that prophylactic use of ivermectin must be initiated immediately for people in high risk categories in the United States and worldwide. This includes individuals with one or more co-morbidities and the middle aged/elderly. Our “design-to-fail” government funded clinical trials for early treatment and governmental obstructionism regarding life saving treatments to patients must end now.
The CDC chart below for all deaths since the start of the outbreak clearly shows a jump in deaths after 50 years old.
However, as the data for deaths per million per age group is not disclosed, so the age for start of prophylaxis has yet to be determined.
As Omicron has less pathogenicity and slightly different disease profile this too could influence what age prophylaxis treatment should begin. But the data are in, prophylactic use of ivermectin saves lives.
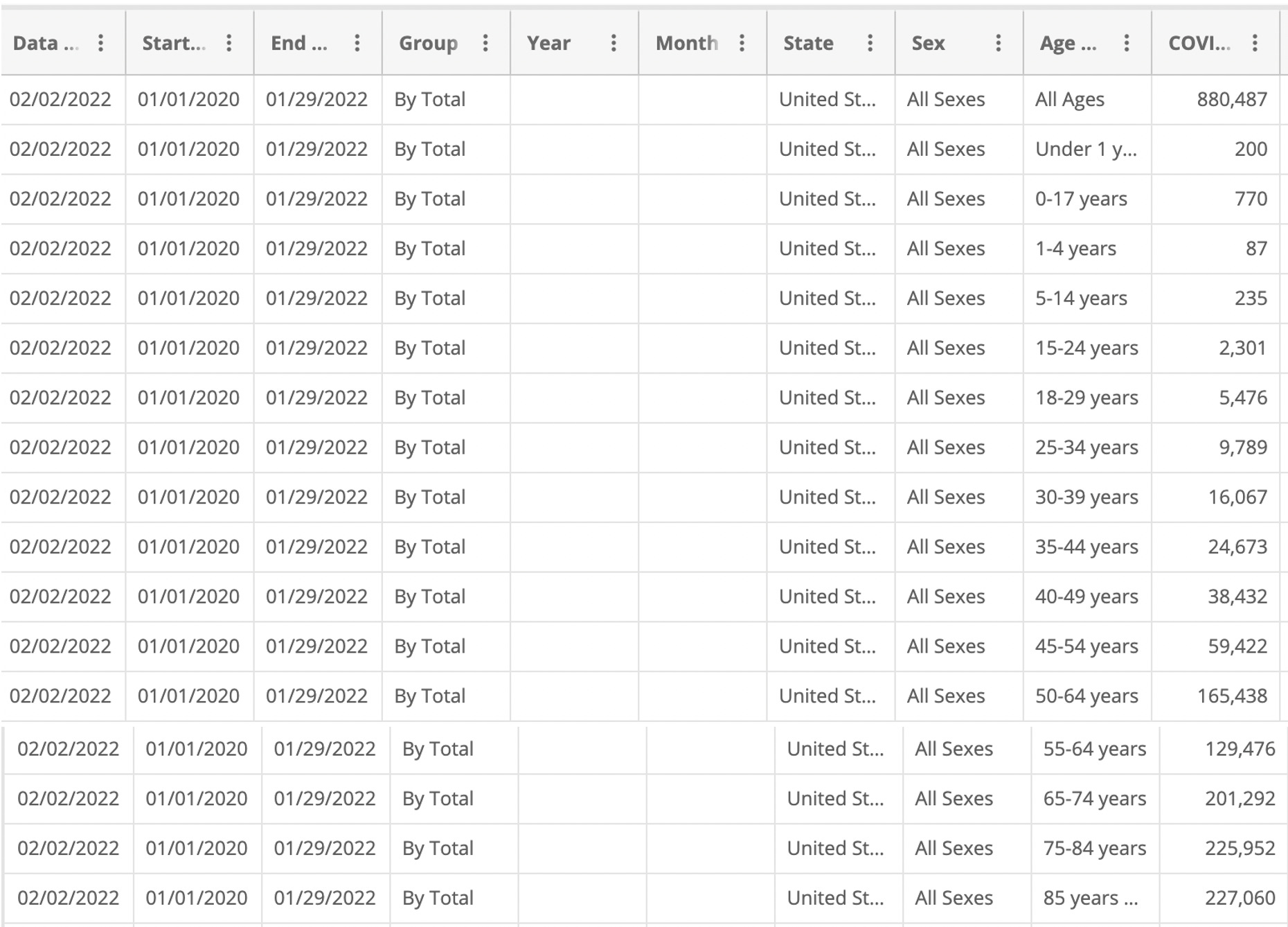
In regards to the table above, the age stratification of disease shows why a universal vaccination program for a vaccine with a high adverse event profile is not advised. It is time to stop all mandates at the Federal and State level. It is time to stop pushing this vaccine on children.
Research and clinical practice show that using re-purposed drugs for Covid-19 have huge benefits. These include multi-drug, multi-staged treatments for Covid-19 disease that prevent severe disease, decreases hospitalization rates and decreases death. It is time our government and state licensing board recognize this and let physicians practice medicine.
‘Off-label’ drug use: an FDA regulatory term, not a negative implication of its medical use. Int J Impot Res. 2008 Mar-Apr;20(2):135-44. doi: 10.1038/sj.ijir.3901619. Epub 2007 Nov 15. PMID: 18004389.
Highlights:
- A doctor’s decision to inform the patient of the ‘off-label’ status of the prescription is not relevant to the physician’s standard of care for an informed consent case.
- The FDA has specifically stated that its procedures and requirements have no effect on the practice of medicine and that the FDA does not prohibit doctors from prescribing drugs in an ‘off-label’ manner.
- The FDA’s approval of a drug is immaterial to the effectiveness in the drug’s ‘off-label’ use. In fact, prescribing medication in an ‘off-label’ manner can constitute the standard of care in many cases.
- A doctor’s duty is to practice medicine and treat his patient, not inform the patient of the FDA’s non-medically related labeling. Therefore, doctors should not be branded with the additional duty of disclosing non-pertinent information, such as the FDA’s medically irrelevant distinction, to their patients
*It is estimated that 21% of all prescription drugs are prescribed “off-label.”
For fun, I took the countries that reportedly use Ivermectin country-wide and compared them to the USA, Israel and Sweden. I chose a three month cut-off, although the results were extended further. I did this because I don’t know when some of the countries began ivermectin use.
Can you guess who now has the highest death rates per million? Yeh –
- USA
- Israel
- Sweden

Notes: I included – India, because although not all regions use Ivermectin – although the most populated due. Likewise Africa – which many nations treat with ivermectin prophylactically and these world maps do not break down Africa by Nations (weirdly imperialistic). I did not include Bulgaria, as although they use ivermectin – their death rate numbers are skewed for other reasons not worth delving into.
There are a lot of confounding variables here. Such as natural immunity, vaccination rates of the elderly and those with co-morbidities, as well as seasonality of the virus, vitamin D3/zinc levels and age of population.
But it is still an interesting snap shot as to where much of the world is right now.
China’s support is a game changer for Russia
BY M. K. BHADRAKUMAR | INDIAN PUNCHLINE | FEBRUARY 6, 2022
During the visit by President Vladimir Putin to Beijing on Friday, the world attention was focused on how far China would go in support of Russia in the latter’s standoff with the US and NATO. From the joint statement issued after the visit, China has given fulsome support to Russia, endorsing Moscow’s demand for security guarantee and its opposition to NATO expansion, the two core issues.
Russia never expected or sought any Chinese intervention in any military confrontation with the western alliance. Russia has the capability to safeguard its sovereignty.
The Chinese support to Russia at the present juncture can still manifest in a variety of ways. Aside China’s backing at the UN Security Council, what really matters most for Moscow would be the myriad ways in which Beijing can mitigate the effect of any harsh western sanctions against by way of transfer of technology, trade, investments, etc. Conceivably, Putin and Xi Jinping have reached an understanding.
Already, a significant step has been taken in this direction during Putin’s visit with the agreement on new Russian oil and gas deals with China worth an estimated $117.5 billion, and China promising to ramp up Russia’s Far East exports. A new 30-year contract to supply 10 billion cubic meters (bcm) per year to China from Russia’s Far East was signed.
Separately, Russian oil giant Rosneft signed a deal with China’s CNPC to supply 100 million tonnes of oil through Kazakhstan over 10 years, effectively extending an existing deal, which is worth an estimated $80bn. The construction of the Power of Siberia 2 gas pipeline to China with a massive capacity of 50 bcm annually is also under discussion.
No doubt, Russia is seriously diversifying its markets for oil and gas exports. This will create space for Moscow to negotiate with its European partners. The new deal with Beijing will not necessitate diversion of Russia’s gas exports to Europe, as they are linked to the gas reserves from the Pacific island of Sakhalin, whereas Russia’s European pipeline network sources gas from the Siberian fields.
The ball is in now entirely in the European court — whether to continue to source assured energy supplies from Russia at such incredibly low prices or punish itself by forgoing that option.
While sanctions may inflict some dislocation initially necessitating readjustments, Moscow will cope with it, as past experience shows. With around $640 billion in foreign exchange reserves, Moscow could persevere longer than the Europeans in the energy market.
The big question is about Putin’s decisions regarding the dangerous situation on Russia’s western borders. The short answer is that Putin will not be browbeaten by the Biden Administration’s threat of sanctions.
China does not consider that a full scale invasion of Ukraine is in the Russian calculus but it neatly sidesteps the issue, nonetheless. Putin acts very cautiously, and almost always is reactive. Be it in Chechnya, Georgia, Syria or Ukraine itself, that has been the pattern. Of course, it is a different matter that in all these instances, Putin acted decisively to make sure his objectives were realised.
In the situation surrounding Ukraine, the Biden Administration is forcing Putin’s hands. The latest US and NATO troop reinforcements to Russia’s neighbours—particularly to the Baltic states, in close proximity to St. Petersburg — were completely unwarranted and can only be seen as a calculated act of provocation when there has so far been no evidence of an adequate justification for a major Russian military operation.
Yet, there could be a method in this madness, given the real possibility of risky military operations in Donbass by an emboldened Ukrainian military or even worse, by the nationalist battalions in that region (to whom NATO has secretly provided a large influx of arms in recent weeks.)
In the event of any attack on Donbass, make no mistake, Russian intervention is guaranteed. The legislation under consideration with the Duma in Moscow currently factors in precisely such a contingency. It calls upon the Russian government to recognise the independence of Donetsk and Luhansk and, secondly, authorises the government to provide with new weapons to these two “people’s republics.”
A plausible scenario could be that Russia will patiently wait for the Ukrainian provocation. That is, it all boils down to a question of resolve. For Russia, the stakes are exceedingly high and its staying power is far greater than that of its Western adversaries.
There is a big element of brinkmanship here. What is happening in Europe at the moment has turned out to be a huge distraction for the US and as time passes, the Biden Administration would rue that its Indo-Pacific strategy is faltering and it is bogged down. The likelihood of Russia backing off is zero.
Evidently, the North Korean missile testing is already putting enormous strain on the US’ alliance system in the Far East. Unlike Ukraine, the US’ security interests are directly affected. Yet, on Friday, a US-drafted statement condemning Pyongyang crash-landed.
Ironically, China called on the US to be more flexible in its dealings with North Korea and joined six other member countries (including Russia and India) in refusing to sign the joint statement.
China’s ambassador to the UN, Zhang Jun later told reporters, “If they do want to see some new breakthrough, they should show more sincerity and flexibility. They should come up with more attractive and more practical, more flexible approaches, policies and actions and accommodating the concerns of the DPRK.”
This is where the US is facing the new reality that its Cold War mentality to isolate China in the Asia-Pacific region and Russia in Europe will not work.
The solidarity between China and Russia reflected in Friday’s joint statement goes far beyond the immediate crisis in Ukraine or the tensions over Taiwan and has an epochal significance heralding a new era in international relations based on a pluralistic world order where the role of the US will no longer be exclusive or defining.
Russia and China have a broad consensus today on almost all core issues related to global strategic stability, which is unprecedented in modern history.
The joint statement mentions the US not less than five times while highlighting the common stance of China and Russia on several key regional and global issues, including the expansion of NATO, the US-led ideological clique in the name of democracy, the US’ Indo-Pacific strategy, AUKUS, etc.
Xi told Putin he is willing to work with him to plan a blueprint and guide the direction of China-Russia ties under the new historical conditions. China has lent support to the fundamental principle of the indivisibility of security that Russia is upholding. In these circumstances, if the US with its zero-sum mindset thinks it can defeat Russia through sanctions, it is being delusional.
Stonewalling the Russian demands is not going to be feasible, either. The challenge facing the Biden Administration will be how to preserve its credibility, especially in the European eyes. For, if Russia is compelled to act militarily to defend its non-negotiable core interests, as it will be at some point, a dangerous escalation may happen.
Is the US ready for an open-ended conflict with Russia? Are its allies game for it? Can they afford it? Will their domestic opinion allow it — war with a thermonuclear nuclear power in Europe to defend ill-defined notions?
A far more judicious course would be to seek a diplomatic formula that takes into account all of these self-evident realities and negotiate some kind of a document that guarantees Russia’s legitimate security needs.
Increased energy prices could “cause heart attacks and strokes”
In the middle of the cost of living crisis, the press has found yet another reason people might keel over… and it’s still not the vaccine.
By Kit Knightly | OffGuardian | February 5, 2022
Our UK readers will be familiar with the press coverage of the cost of living crisis in this country, as wages continue to fall further and further behind inflation, and the economy reels from the deliberately devastating lockdown, the cost of everything from food to fuel is ever increasing.
People are understandably troubled and anxious, whether or not the energy cost crisis is genuine or manufactured for the sake of profits, the reality is that many people will face the choice of heating their homes or eating enough food over the last two months of winter and into the spring.
This could easily result in people – especially the elderly or disabled – suffering health problems or even death due to the cold or malnutrition. Many of these people will likely become “covid cases” or “covid deaths” once they’re subjected to the totally unreliable tests.
It’s all a perfect little circuit. And it serves the Covid agenda in more ways than one, because it’s just handed the press yet another explanation for heart attacks that haven’t happened yet.
It seems like only a few days ago we ran an article pointing out all the numerous different reasons the press are predicting people will have heart attacks this year… and that’s because it was.
Stress, anxiety, the weather, “long covid” and a plague of undiagnosed aortic stenosis are all predicted to cause thousands upon thousands of heart attacks and strokes in the near future.
And now so is the increased cost of living.
Appearing on Lorraine on ITV yesterday morning, Dr Amir Khan claimed:
… if you can’t afford to heat your home, it actually causes an increased risk of developing heart attacks and strokes because your blood vessels contract to conserve heat, which pushes your blood pressure up, and over time that has an impact on your heart attack risk.”
In future, maybe they should simply run press releases saying “Covid vaccine only thing in world which doesn’t cause a heart attack”
As Neil Oliver pointed out on Twitter…
How the Biomedical State Maintains the ‘All the Experts Agree’ False Consensus

The Daily Bell | February 4, 2022
We’ve previously explored the mind-numbing “experts say” mantra that the corporate media parrots non-stop. Talking heads incessantly implore the peasant class to “respect the science.”
The purpose is to create a mirage of consensus in order to discourage real journalists or normal people from looking into matters themselves. This tactic is pervasive, but nowhere has it been more widely employed than in the COVID era.
Because, if three key facts were permitted to infect the public consciousness, they would inevitably result in mass upheaval of the ruling class that perches on top of society, feeding on it like vultures:
- A.) the original virus almost certainly escaped from a Wuhan lab (if it wasn’t purposely released; let’s not underestimate the hubris of the biomedical state). Worse, that leaky Chinese lab relied on funding from the United States National Institutes of Health (funneled through a “non-profit” called EcoHealth Alliance) to perform dangerous gain-of-function research on bat coronaviruses.
- B.) The vaccines (which are actually mRNA gene therapies) do not work to prevent infection as promised and cause extensive side effects that were covered up in the original trials.
- C.) The “social distancing” lockdown measures – which plunged untold billions worldwide into poverty, death, and despair – were totally ineffective at preventing the spread of the virus: “Shelter-in-place orders had no detectable health benefits.” Imagine the criminality of all the suffering for no good reason.
At every turn, the “experts” got it wrong.
So how does the biomedical establishment maintain the façade of legitimacy?
The biomedical state uses multiple mechanisms to discourage scientists from dissenting from the approved narrative
You’ve heard the talking point ad nauseam: “99% of scientists agree the vaccines are safe and effective.”
First of all, that figure is not vindicated by any actual polling; it’s just an offhand catchphrase.
Second, what happens to scientists who deviate from the “safe and effective” slogan?
- Their message will get censored or distorted (or both)
- Might lose their professional license
- Ostracized by their peers
- If they’re a researcher, they’ll risk wrecking their career and losing critical funding from NIH and pharma corps.
JFK Jr. explains:
“As director of the National Institute of Allergy and Infectious Diseases (NIAID), Dr. Anthony Fauci dispenses $6.1 billion in annual taxpayer-provided funding for scientific research, allowing him to dictate the subject, content, and outcome of scientific health research across the globe. Fauci uses the financial clout at his disposal to wield extraordinary influence over hospitals, universities, journals, and thousands of influential doctors and scientists—whose careers and institutions he has the power to ruin, advance, or reward.”
- You’ll get smeared in the corporate media
Exhibit A:
Epidemiologists at Harvard, Stanford, and Oxford – three of the most highly-regarded mainstream institutes of higher learning in the world – authored the Great Barrington Declaration in October 2020.
The gist of the document (which you can read here) is that a COVID Zero policy (the elimination of the SARS-CoV-2) virus in the population is a pipe dream. The social distancing and lockdown orders had devastating effects on public physical and mental health. Those at risk of severe illness or death from infectious disease should be protected while the non-vulnerable (the vast majority of the population) should resume normal life.
Those rational, science-based propositions should have been aired publicly in a healthy national debate.
But, predictably, open debate is not how Anthony Fauci and Francis Collins, NIH Director, do things. Instead of debating the merits of the Barrington Declaration, Collins sent an email to Fauci on Oct 8 (later leaked) that read:
“This proposal from three fringe epidemiologists… seems to be getting a lot of attention – and even a co-signature from Nobel Prize winner Mike Leavitt and Stanford. There needs to be a quick and devastating published takedown of its premises. I don’t think like that on line yet – is it underway?”
Does that sound like the language of a public health servant doing God’s work to protect the people from a deadly virus – or that of a cynical political operative?
Is coordinating a media hitjob on ideological opponents part of the NIH Director’s job description?
More importantly, though, if they can orchestrate a smear campaign against three “fringe” epidemiologists from Harvard, Stanford, and Oxford, what signal does that send to a run-of-the-mill MD in Wisconsin who might be inclined to ask critical questions?
The message is obvious: “shut your mouth or we’ll come for you.”

They don’t even have to go after everyone. All they need is to bag a few high-profile scalps to set the example.
MSNBC Misinfo: Zeke Emanuel Peddles Fear, Says Unvaxxed Children ‘Likely To Get Serious Case Of Covid’

By Tyler Durden | Zero Hedge | February 5, 2022
Dr Ezekiel Emanuel – former Biden Covid-19 adviser and brother of former Chicago Mayor Rahm Emanuel (and the real ‘Ari Gold’ from Entourage) appeared on MSNBC Wednesday, where he proceeded to peddle the lie that unvaccinated children are ‘likely’ to get a ‘serious’ case of Covid.
“This repeats what we’ve seen in older kids, five and above, where we know the vaccine does protect very well. And there we still have under 50%, I believe, of the children vaccinated, and that’s a serious problem for the country,” Emanuel told host Kristen Welker after she asked about parents’ willingness to vaccinate their children. “Parents have to be more willing – I think they hear some of these rare side effects and think they’re very common.”
“With the omicron variant, kids are either going to get the vaccine or they’re likely to get a serious condition of omicron. Having omicron with the vaccine is almost invariably going to be better and safer for children,” Emanuel added. “I am confused about parents’ attitudes. Five and above seems like a no-brainer. Two to five, I understand some hesitancy. Two and under with the small dose, I think probably a very good idea.”
It’s been widely established that Omicron is a relatively mild strain of Covid – from which children face an extremely low risk.
Another recent study cited by economist Emily Oster also reiterated the extremely low risk young children face of severe COVID-19 outcomes. “What we can say is that based on everything we know, the risks to small children from COVID-19 are extremely small,” she wrote. –Fox News
MSNBC faced harsh criticism over Emanuel’s statement.
The network even tweeted (and then deleted) the easily debunked misinformation, receiving a serious ratio of comments to ‘likes.’
Intentional? Or…
Following the backlash, Emanuel issued a Saturday tweet in which he says he “misspoke.”
Steve’s fact-based COVID-19 hub

By Steve Kirsch | February 2, 2022
Spotify made a press release about their new platform policies which prohibits any information which in their sole opinion may cause offline harm or poses a direct threat to public health. They refer people to their “fact-based” COVID-19 hub for accurate information.
I think their “fact-based” hub is filled with misinformation, so I decided to write my own simplified version that takes just a couple of minutes to read.
Here it is:
- Early treatments using repurposed drugs in a proven protocol are the best way to treat COVID. Treating as soon as symptoms appear is key. Fareed and Tyson have now treated over 10,000 people infected with COVID without any deaths as long as the people arrived early in the disease. The NIH and CDC ignore these treatments. I recommend you choose an early treatment protocol where there have been at least 10,000 COVID patients treated early without a single death (such as the Fareed-Tyson protocol), and start it as soon as you have symptoms.
- The evidence is clear that all of the current COVID vaccines available in the US today are both unsafe and ineffective. They are not suitable for anyone because they are more likely to kill you than to save you. If they don’t kill you, they may permanently damage your immune system or leave you permanently disabled. Avoid these at all costs. After 90 days, it appears that the vaccines have negative efficacy against Omicron, making you up to twice as likely to be infected. This is likely why case rates are so high in highly vaccinated countries. See Incriminating Evidence for details.
- Cloth and surgical masks do not work. There have been just two randomized trials with masks and COVID (Denmark and Bangladesh) and they proved that surgical and cloth masks have no effect. Similarly, N95 masks do not work in practice either. The FAA rules basically require you to wear these masks on planes, mandating a medical intervention that is much more likely to make you sick and has no chance to protect you. See Incriminating Evidence for details.
- If you require PPE that might protect you from COVID, consider a 3M respirator with a P100 filter. Even better is to use a PAPR with your respirator (with a P100 or P3 filter). See this article on masks and respirators for details. These products that protect you do not protect others. The FAA will not allow these devices on a plane.
- Social distancing is not the right way to think about risk reduction. Think instead the 4 D’s: draft, distance, density, duration. Putting yourself in an unventilated small room at close distance to a source for a long duration will maximize your exposure. The 6 foot rule for standing in line is nonsensical since as soon as you enter the airspace of the person in front of you, you will be breathing the virus from people who were standing in that spot hours (to days) ago (depending on the ventilation in the area). There is absolutely nothing magical about 6 feet.
- Mitigation strategies such as testing, masking, isolation, and vaccination are largely ineffective. See this article for a convincing example.
- The best way to treat COVID is to do the opposite of what the CDC and FDA advises. So when they tell you to mask up, get boosted, avoid all repurposed drugs and supplements (including ivermectin, HCQ, fluvoxamine, vitamin D, zinc, aspirin, budesonide, etc), take paxlovid, molnupiravir, and remdesivir, you know what to do.
- There is only significant spread if you have symptoms. For example, in a study in China, they looked at 1,174 close contacts of these asymptomatic individuals and could not find ONE CASE of a person getting COVID from the asymptomatic people. Therefore, testing asymptomatic people is unnecessary because it is a lot of effort for near 0 gain.
- Omicron is very mild compared to Delta. After you recover from an Omicron infection, data shows you will be protected from Delta as well.
- As of December 3, 2021, Omicron had spread to 38 countries, but the WHO couldn’t find anyone who died from Omicron. How is this a national emergency?
- People who get the virus and recover are always better off than a vaccinated patient. Unlike vaccinated people, if a naturally infected patient is ever re-infected, they cannot transmit the virus to others (as far as we know so far).
- Censorship of COVID advice by social media (in particular the hazards of the vaccines and the effectiveness of early treatment protocols) has cost hundreds of thousands of lives.
- None of the health authorities issuing mandates and directives are willing to participate in a recorded scientific discussion with the so-called “misinformation spreaders” such as Robert Malone, Peter McCullough, Robert Kennedy, … Our authorities are afraid of the truth.
- The CDC, FDA, and NIH are all corrupt agencies that have looked the other way at safety signals. There are over 1M adverse events in VAERS and these represent over 40M adverse events in the real world. This is unprecedented, yet the CDC isn’t able to find a safety signal other than a “slightly elevated” risk of myocarditis. Attempts to bring the VAERS data to their attention is futile. They won’t even do a proper calculation of the underreporting factor which is required to do a proper risk-benefit analysis. They ignore the DMED data entirely.
Compare my fact-based COVID-19 hub to Spotify’s and let me know which one you like better.
EU Wants To Keep Vaccine Passports In Place For Another ENTIRE YEAR
By Steve Watson | Summit News | February 4, 2022
The unelected bureaucrat governors of the EU in the European Commission have proposed keeping the bloc’s COVID vaccine passport system in place for another entire year, despite the fact that many member countries are ramping down restrictions.
In a notice on its website, the Commission states “Today the European Commission is proposing to extend the EU Digital COVID Certificate by a year, until 30 June 2023.”
It continues, “The COVID-19 virus continues to be prevalent in Europe and at this stage it is not possible to determine the impact of a possible increase in infections in the second half of 2022 or of the emergence of new variants.”
“Extending the Regulation will ensure that travellers can continue using their EU Digital COVID Certificate when travelling in the EU where Member States maintain certain public health measures,” the statements adds.
It continues, “The Commission is adopting the proposal today to make sure the European Parliament and the Council can conclude the legislative procedure in time before the current Regulation expires.”
The move comes even as several countries, including Denmark, Norway, Italy, Sweden, France, in addition to non-EU countries such as Switzerland and England move to scrap restrictions including the vaccine passes.
The European Commission admits in its statement that it is up to the individual countries whether they carry on using the EU COVID vaccine passport scheme.
“The domestic use of EU Digital COVID Certificates remains a matter for Member States to decide, the statement notes, adding “The EU legislation on the EU Digital COVID Certificate neither prescribes nor prohibits the domestic use of EU Digital COVID Certificate (such as for access to events or restaurants).”
It also notes that “At the same time, where a Member State establishes a system of COVID-19 certificate for domestic purposes, it should continue to ensure that the EU Digital COVID Certificate is also fully accepted for those purposes. Beyond that, the Commission also encourages Member States to align their domestic validity periods with the validity period set at EU level for the purpose of travel.”
As we reported in November, despite vaccine passport schemes and high vaccination rates in many of the countries affected, COVID cases across Europe continued to surge as winter kicked in.
In addition, a recent investigation by experts in Spain concluded that vaccine passports have no significant impact on reducing COVID-19 infection rates.
The findings are similar to evidence found by the UK government that vaccine passports could actually increase Covid rates in the country.
The Spanish study noted that the only positives of such a scheme are that it “warns people that there is still danger from the pandemic and encourages vaccination uptake among the reticent.”
In other words, although vaccine passports have no discernible impact on their stated goal – reducing the spread of COVID-19 – they do succeed in keeping people fearful and compliant.
That conclusion dovetails with a recent admission by French Minister of Health Olivier Véran that the vaccine passports are “a disguised form of vaccination obligation,” but are “more effective.”
Eli Yale Surveillance State
By Stephen Lendman | February 5, 2022
Since seasonal flu was renamed covid over two years ago, medical tyranny became the new abnormal on thousands of US college and university campuses nationwide.
Rights guaranteed by international and US constitutional law no longer apply.
Health and freedom-destroying mandates replaced them.
The higher education experience I enjoyed long ago is gone since medical tyranny took over.
Yalies are enduring some of the worst of what no one should tolerate under virtual surveillance state standards.
A university hotline was established to make “confidential (snitching) reports.”
It largely relates to assuring “compliance with (draconian flu/covid) health and safety standards” that harm and don’t protect.
According to your.yale.edu, it’s to enforce compliance with all things flu/covid to include:
Destruction of normal campus interactions by mandated social distancing.
The same goes for masking.
What Yale calls “personal protective equipment (sic)” risks potentially serious respiratory harm while providing nothing beneficial.
So-called “cleaning and disinfecting standards” are best achieved by old-fashioned soap, water and other good personal hygiene practices.
Yale’s hotline for snitching on non-compliers to any of the above and whatever else relates to flu/covid operates “24 hours a day, seven days a week, every day of the year.”
The Washington Free Beacon (WFB) discussed one example of how Yale’s surveillance state operates.
On a Saturday night at 9:30 PM, a student in what appeared to be a deserted campus library went maskless to relax.
Alone with no one around, there was no reason to wear what’s required by university rules when others are nearby.
Somebody spotted, filmed and reported him.
In response, he got the following Office of the Dean notice, saying:
“The Compact Review Committee (CRC) is reviewing a report that your conduct failed to meet the commitments you agreed to in the Yale Community Compact.”
“The CRC has received the enclosed report from Melanie Boyd, Dean of Student Affairs, Yale College (flu/covid) Health and Safety Leader…”
“You have until (24 hours from this notice to) provide the CRC with any relevant information you would like the Committee to consider in its evaluation.”
“(F)ailure to do so could lead to disciplinary action with the Yale College Executive Committee.”
“The CRC will review the matter and decide whether your conduct poses a risk to the health and safety of yourself or other community members.”
Days after receiving the above notice, he received the following reply:
The so-called CRC “determined that your conduct posed a risk to the health and safety of yourself or other community members (sic).”
“Should you continue to engage in behavior that violates the Yale Community Compact, you will be placed on Public Health Warning and may face more serious outcomes, including the removal of permission to be on campus.”
On the same evening that the reprimanded student went maskless with no one around him in a near-deserted campus library, “1,000 maskless students gathered for Yale’s annual holiday dinner,” the WFB reported.
A video of the event showed the maskless attendees.
Apparently unsnitched on or for whatever other reason(s), no disciplinary actions were reported.
According to what students told the WFB, “rules increasingly feel like overkill.”
Enforcing them is “spotty.”
So far, there’s been no “organized opposition.”
Mass surveillance state Yale discourages it.
What one unnamed student called “a silenced majority (reflects fear of) administrative consequences” for openly addressing what harms health and denies students the full academic experience they deserve.
Other colleges and universities instituted their own surveillance state practices.
Northwestern University with campuses in Evanston, IL and Chicago is one.
Harvard is another. “Speak up,” it urged!
“Simple. Anonymous. 24/7.”
“Keep Harvard a safe place to live, learn and work (sic)” — by making it unsafe and unfit for students, faculty and staff.
By imposing draconian health and freedom-destroying mandates.
At Yale, no official guidelines were published to explain what alleged offenses merit what punitive actions.
The same is likely true on other campuses with draconian rules in place.
Most important is that kill shots and all else flu/covid have nothing to do with protecting and preserving health.
They aim to destroy public health and what remains of fundamental freedoms.
We’ve been lied to and mass deceived for over two years.
For students, academic life as it should be is gone.
For working-age individuals required to be jabbed and masked et al, destroying health and freedom is a condition of employment where these draconian standards were implemented.
The same applies to where free access to other public places are restricted or otherwise impeded.
I mentioned the following once before in an earlier article:
What’s going on reminds me of a comic routine performed on television long ago by famed entertainer/tightwad-impersonating Jack Benny (1894 – 1974).
Approached by a thug impersonator and told “Your money or your life,” Benny responded:
“I’m thinking it over.”
There’s nothing to think over about draconian flu/covid mandates.
It’s crucial to shun what’s designed to destroy health and freedom — on the phony pretext of providing protection not gotten.
Canadian trucker Freedom Convoy embraces GiveSendGo after GoFundMe censorship
By Tom Parker | Reclaim The Net | February 4, 2022
After having their fundraising efforts shut down by GoFundMe, the leaders of the Canadian trucker Freedom Convoy have switched to alternative platforms to fundraise and communicate with their supporters.
The Freedom Convoy, which has been traveling across Canada to protest vaccine mandates, has gained huge traction online and had raised over $10 million on GoFundMe. However, GoFundMe withheld the convoy’s funds twice and said that it’s “collaborating with local law enforcement” before permanently shutting down the campaign and refusing to pass on the millions of dollars that had been raised.
The shutdown of the campaign came days after a Canadian city council member had requested a lawsuit to seize GoFundMe funds raised by the Freedom Convoy.
Following these issues with GoFundMe, the Freedom Convoy launched a campaign on the alternative crowdfunding site GiveSendGo and has already raised tens of thousands of dollars. We have confirmed that this is the official campaign created by Tamara Lich who created the original campaign on GoFundMe.
While GoFundMe has removed multiple fundraisers from its platform, GiveSendGo has championed freedom of speech and platformed many fundraising campaigns that have been restricted by GoFundMe including those raising money for Kyle Rittenhouse and election investigations.
In addition to embracing GoFundMe, the organizers of the Freedom Convoy have also partnered with CloutHub to create a group for communicating with their supporters and set up a campaign page that contains quick links to the group and fundraising page.
“There is no more important movement for freedom across the American continent right now than the Freedom Convoy 2022,” CloutHub CEO Jeff Brain said. “We are proud to support the Canadian truckers and will help support the other trucker movements popping up around the world to fight against unlawful mandates. CloutHub is where the world connects and organizes to take on the issues they care about, including defending liberty and freedom.”
CloutHub, which had direct experience of Big Tech censorship when it was deplatformed by IBM in 2020, offers users an alternative platform that focuses on bringing people together and empowering them to connect and solve issues that they care about. It has also encouraged lawmakers to pursue laws that limit the power of Big Tech.
The GiveSendGo campaign can be found here. The page may be slow as it deals with heavy demand.
Featured Video
Chinese jet fuel and the myth of energy independence
or go to
Aletho News Archives – Video-Images
Book Review
Former Insiders Criticize Iran Policy as U.S. Hegemony
By GARETH PORTER | CounterPunch | February 27, 2013
“Going to Tehran” arguably represents the most important work on the subject of U.S.-Iran relations to be published thus far.
Flynt Leverett and Hillary Mann Leverett tackle not only U.S. policy toward Iran but the broader context of Middle East policy with a systematic analytical perspective informed by personal experience, as well as very extensive documentation.
More importantly, however, their exposé required a degree of courage that may be unparalleled in the writing of former U.S. national security officials about issues on which they worked. They have chosen not just to criticise U.S. policy toward Iran but to analyse that policy as a problem of U.S. hegemony. … continue
Blog Roll
 Aletho News
Aletho News- What is fueling unrest across the EU?
- Why no power can undermine Iran’s eternal dominance over the Strait of Hormuz
- Is The War Against Iran Over?
- Iran war will leave long-term ‘scar’ on Wall Street, investors warn
- How Iran decimated US power projection in West Asia: Military lessons of 40-day war
- Iran’s report details US-Israeli war crimes in targeting schools, hospitals, livelihoods
- NATO’s Slow Fracture: How Trump’s Iran War Exposed the Instrument of Hegemony
- Chinese jet fuel and the myth of energy independence
- Ukraine Sea Drone Fired From Libya Hit Russian Tanker in Mediterranean
- IRGC: Iranian forces launched no attacks during ceasefire hours
- If Americans Knew
- DNC Shoots Down Resolutions Calling Out AIPAC and Limiting Arms to Israel
- TCN: Is Israel Blackmailing President Trump?
- Israel killed at least 303 Lebanese yesterday – who were they? Daily Update
- Amnesty: Urgent – Protect Lebanese civilians from brutal escalation in Israeli attacks
- Is The War Against Iran Over?
- Inside the Israeli army’s propaganda wing
- Hundreds of Gaza Amputees Stranded in Legal Limbo
- The gallows law: Israel moves toward executing Palestinian children
- Tucker Carlson: The Path to Peace requires ending ‘special alliance’ with Israel
- This is ceasefire? Israel’s biggest massacre yet in Lebanon, another journalist killed in Gaza – Daily Update
- No Tricks Zone
- An Inconvenient Tree: Uncovered In Alps… Europe Much Warmer Than Today 6000 Years Ago
- New Study Reports A 60% Slowdown In Greenland’s Ice Loss Rate In The Last Decade
- Low Intensity Tornado Wrecks Major Solar Farm, Creating A Potential Toxic Dump
- New Study Finds Warming Saves Lives…Cold Temperatures 12 Times More Deadly Than Excess Heat
- German Science Blog Accuses PIK Climate Institute Of Hallucinating Climate Tipping Points
- Devastating Assessment Of Comirnaty Vaccine By Former Senior Pfizer Europe Toxicologist
- New Study: CO2 Is ‘Effectively Negligible’ As An Explanatory Climate Change Factor Since 2000
- Former Pfizer Toxicologist Dr. Helmut Sterz Tells Bundestag Hearing Pfizer Vaccine Should Have Never Been Approved
- Energy Expert: Germany’s Nuclear Phaseout Was A “500 Billion Euro Mistake”
- New Research: South Australia’s Mid-Holocene Sea Surface Temperatures Were 4°C Warmer Than Today
