“Stunning!” Apollo Moon Photos Too Good to be True?
Photographer-filmmaker Massimo Mazzucco takes on the New York Times
By Kevin Barrett | November 1, 2025
Jason Farago, who appears to be a Deep State propagandist and pro-UkroNazi culture warrior, just published a New York Times interactive photo-video piece headlined “How Lunar Photography Brought the Heavens Down to Earth.” Farago celebrates the alleged artistic genius of the Apollo moon photos, viewing them as the climax of the overlapping artistic and scientific histories of moon explorations and representations.
Moon landing skeptic and professional photographer Massimo Mazzucco says that’s bullshit. Farago’s extravagant praise of the Apollo astronauts’ brilliant use of deep depth of field just means they knew how to crank the f-stop up to f16 or f32 (which I figured out about five seconds after buying the cheapest available Pentax when I was a journalism student back in 1976). His orgasmic effusions about the beautifully-rendered lunar surface texture sound like something an LSD tripper might say while staring hypnotically at the ground in some godforsaken stretch of barren desert. And his ranting about how many of the moon landing photos are so perfectly composed and executed that they look totally fake really takes the cake:
“The photographs were in fact so good—and the 70mm stock so detailed—that doubts set in on the blue sphere below. With their rich chiaroscuro and starless skies, Bean and Conrad’s photos looked uncannily like a Hollywood stage set.”
Uncannily indeed. Is Farago engaging in classic neocon doublespeak (surface layer for the ignorant rubes, esoteric layer for the cognoscenti)? Is he nudging and winking at the cognoscenti in a shared moment of dupers’ delight? Was this assignment handed out by the Deep State desk at the New York Times to blow smoke to cover for delays in the Artemis missions? Or is Mazzucco wrong in his claims that many moon landing photos are obviously fake, and that the most likely explanation of these and other anomalies is that the Apollo missions didn’t really put men on the moon circa 1969-1972?
Watch Mazzucco deconstruct bad New York Times propaganda, watch his film American Moon, and make up your own mind.
Excerpts from the Interview
Welcome to a special edition of False Flag Weekly News, the weekly news show that normally peels back the news headlines to reveal what’s crawling around underneath. Today we are going to be interrogating the perhaps most influential newspaper in the Western world, The New York Times, by way of a special art and science uh photo analysis that they did discussing the moon landing photos from the Apollo missions. And who better to talk back to the media on that subject than Massimo Mazzucco? He is the director of September 11th: The New Pearl Harbor, possibly the best and most comprehensive 9/11 documentary film, as well as American Moon, probably the best film about the moon landing. So, hey, congratulations on making the best conspiracy films in two genres.
Thank you. It’s not for me to say they’re the best. I can certainly say they’re the longest. Because September 11th: The New Pearl Harbor is five hours and the American Moon is three and a half.
Well, that’s what I meant by comprehensive. I was trying to be nice. (laughter)
Okay. Okay. Let me just clarify very quickly. There’s a reason for that. I don’t like to entertain people more than is needed, except that for both films, I use the technique where I first present the problems or the issues (with the official stories). Then I present the explanations or answers that the debunkers have for each of those issues. And then I present the debunking of the debunkers. So each argument, each issue, is presented from three times: The presentation (of holes in the official stories), what the debunkers say about it, and what I have to say about what they say.
There’s a term that David Ray Griffin coined first. It’s called debunking the debunkers. And that’s why I like to have it all in one film, all comprehensive, both questions and answers. And then people can make up their own mind, of course.
Yeah, it’s a great format. And honestly, I think they’re the best as well as the most comprehensive films, partly because of that format. And we’re going to follow that type of format here too, because we’re going to see what the New York Times says about these images. And then you get to say what you have to say about them. And unfortunately, we don’t have the New York Times here to answer you, so we’ll just have to leave it at that.
Let’s look at our slideshow. We’re going to do a close read on this New York Times photo exhibit. Here’s their opening shot. They’re really ecstatic about the artistic quality of the moon landing photos. And in a couple of places, they actually mention that it looks almost suspicious. These photos are almost too good to be true. What do you think, Max?
I don’t think they’re good at all. No, I have to tell you… maybe your audience doesn’t know. I have been a photographer for the first part of my life, let’s say between age 20 and 40.. And I was a professional, at the top level. I was working for magazines all over the world. I was using actually the same cameras and film and lighting that supposedly were used in the Apollo missions.
I’ll give you one quick anecdote so you understand the point of view of a professional. I learned my trade from a famous photographer, now deceased. He just passed away a few months ago. His name was Oliviero Toscani. He’s actually the guy who made the Benton campaign all over the world. He was very, very famous. I would put him in the top 10 in the world history of fashion photography. I was his assistant for about three years. Then we parted ways. I went on to have my own career.
Back in 2000, when I saw the lunar pictures for the first time—all of them, not just the few that were published before, but all of them that were put out by NASA on the internet—I looked at them and I could see all the defects that I would find myself when I tried to replicate sunlight in the studio. So I got very suspicious. I called Toscani and I said, “Oliviero, what did you think the first time you saw the Apollo moon pictures?” And his answer was, and I quote him:
“I always thought that had they given me the job, I would have done a much better job.”
Wow, better than Neil Armstrong! Because you’re going to see how the New York Times praises Neil Armstrong (as a photographer)…Okay, so they begin with this poetic passage: “The darkness we expected. What we had underestimated was the silence, the quiet of the vacuum, disturbed only by our breath and the radio in our ears.” So that’s supposedly these Air Force guys, these astronauts. You think that they hired a literary guy…
There’s a problem. These astronauts were wearing what is called the PLSS, the Portable Life Support System, which provides them with both a cooling system for the body—because you have over 100 degree Celsius temperature on the surface of the moon—and air for breathing.
So in the back of the PLSS, you have these pumps that are supposed to be both circulating water and pushing air through the system so that you can actually breathe. Except when you listen to their conversations, there’s absolutely no noise. There’s no noise whatsoever.
No wonder they underestimated the silence.
Yeah, exactly. Because you’re in a studio when nobody is making a sound. That’s why you hear all the silence. If you had those machines really on, you would hear probably a purring in the back of your ear. You would hear of these pumps working. Nothing of that is ever heard in their conversations.
In the opening picture, that light tells me that is a studio spotlight facing straight into the camera. It is not the sunlight. The sunlight acts differently. With the kind of lenses that they had, the kind of distortion that you would have inside the lens is much different than that. That, to me, tells me that that is a spotlight facing straight into the camera and making it look like the sun.
Another thing that you can tell is what is called the fall-off. You have a major amount of light coming through the center of the picture, straight in line with the sun. But off to the sides, if you look at the edge of the crater on the middle of the right of the picture, you can see that the more you go away to the right, the darker the ground gets. If this was the sun, you would have illumination that is equal all over the sand. In this case, you can tell that it is degrading towards darkness as you move to the right, and that is because that is the spotlight. It’s not the actual sun.
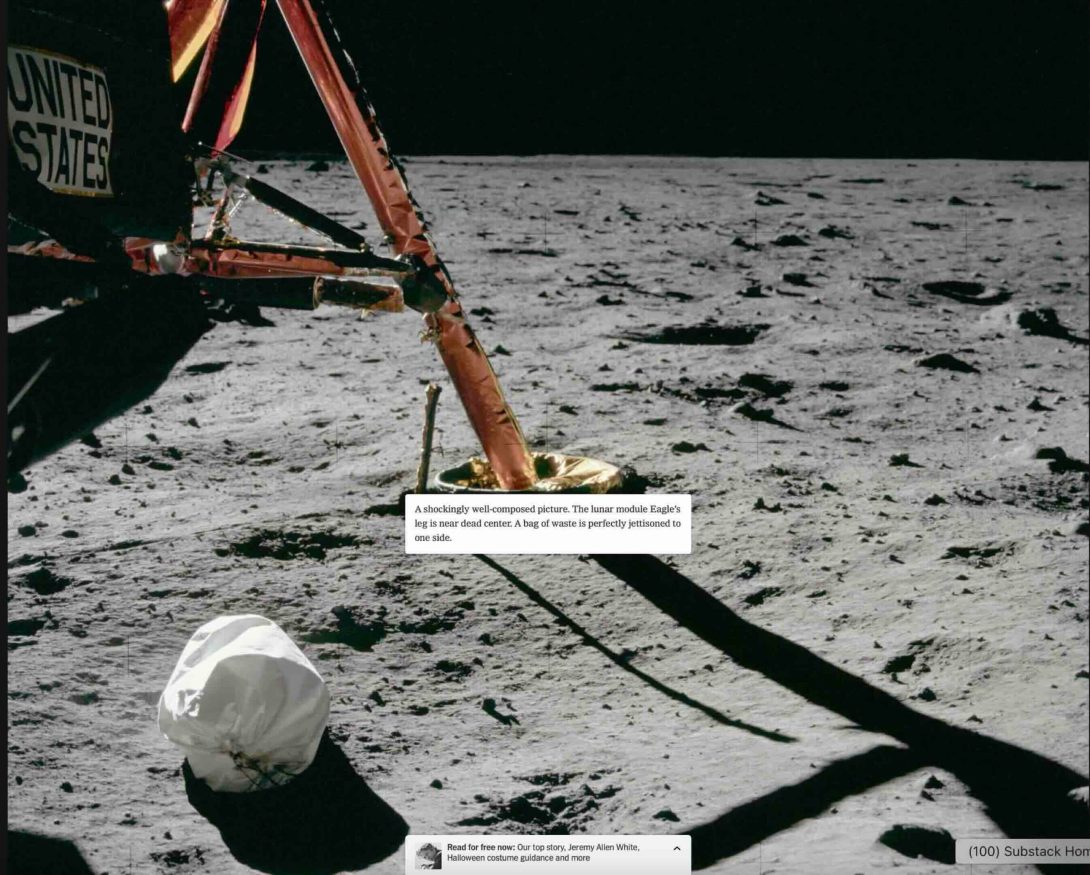
So here’s one where they say it’s a shockingly well-composed picture.
Yeah. I think they’re trying to influence the viewer by using all these words, shocking and beauty and all that. There’s absolutely nothing shocking in this picture.
“The lunar module’s eagle’s leg is near dead center. A bag of waste is perfectly jettisoned to one side.” So maybe they’re telling us it’s all a bag of waste. I don’t know.
How do you imperfectly jettison?
Ye ah I’ve jettisoned a lot of waste in my life but I can’t tell the perfect from the imperfect myself. But the New York Times, they’re critics. They know this stuff.
Yeah.
Do you see anything suspicious about this image?
I do but it would be a little too long to explain. Again there’s a fall off. But it’s very mild because they lowered the contrast. So I can tell that there is more light right below the LEM in the center left of the picture, it is brighter than on the far right. But it’s a very, very mild difference because the contrast is very low.So you can’t really tell here. Only a professional can tell.
The New York Times tells us: “During their camera training it became evident that Armstrong had a better eye than Buzz Aldrin…” Which meant he was the one taking most of the pictures for Apollo 11 in 1969…took more than 100 photographs. And the New York Times guy says: “I would happily claim, in fact, that Armstrong authored one of the last century’s signal works of American portraiture, his head-on view of Aldrin, legs contrapposto like a Greek statue in the southwest of the Sea of Tranquility.” Wow.
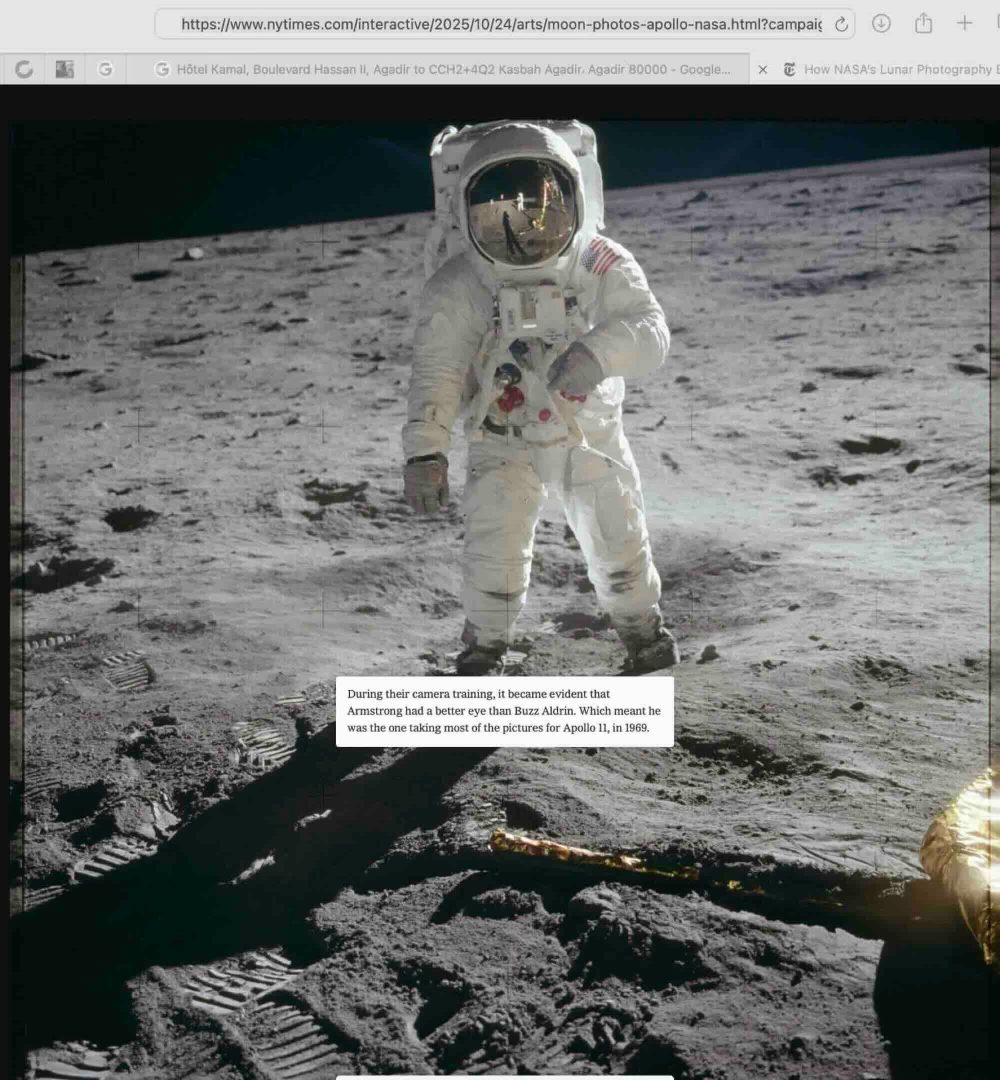
I would suggest we look at something else in this picture rather than read the caption. And the fact is that Aldrin, the person allegedly pictured in the photograph, is inside a little crater which is based maybe 10 centimeters lower than the average surface. And if you look at the way the photo is taken we can see the top of the helmet. Now remember the camera is allegedly sitting on Armstrong’s chest. So it should be at the same height, basically, as where the hand of Aldrin is, just a little higher. It would be impossible if I shot from my chest, even though the guy is in a little bit of a vacuum. It’s a small, it’s a little lower than the surface, but only like 10 centimeters. I cannot see the top of his head. So this picture is taken from a much higher viewing point than the actual chest of the photographer.
Could he have been on a little hill or something?
He could have except there was none. It’s all flat. They’re all basically on the same surface. If you look at other pictures of the situation it’s really all pretty much flat. And it’s one curious thing. You cannot prove that the pictures are fake. But again I can see now that the New York Times has used…a corrected set of pictures not the original ones. In the original ones, the original scans that were made from the original negatives, the contrast is much higher, and you can tell very, very easily that the guy allegedly being Aldrin is sitting in a spotlight. All around him, if you turn back the contrast to the way it was originally, before it was manipulated, you could tell that Aldrin is inside of a circle of more light, and that’s where the spotlight hits, as opposed to the background. The background, as soon as you lower… the contrast gets much darker than the ground he is standing on. And that should not be happening, if the source light were the sun.
I can’t believe the New York Times would be manipulating these pictures.
They’re not manipulating them themselves. They’re using a set of manipulated pictures that have been circulated by NASA, which are not original, but of course where the problems are less evident.
And here it says that’s our photographer reflected in Aldrin’s gold visor and one of the only still images of Armstrong on the moon. And so they zoom in and show the photographer reflected in the visor.
Yes. Well I mean that could be anybody of course. One wonders why would Armstrong, the first man on the moon, not have any pictures of himself? I mean you organize such a precise, such an accurate trip to the moon, where every detail is scheduled and laid down. They have papers with: “1005 turn around. 10010 breathe again.” I mean, everything is scheduled. And then they forget to take pictures of the first man on the moon. And we only have pictures of Aldrin. Could it possibly be that Armstrong, who did not want to be manipulated more than necessary, did deny them the right to say that that was him? Just remember, of the first man of the moon we have no pictures except one shot where you can actually see his face a little bit through the visor. And all the others it’s Aldrin. It’s very strange…they forget that you should schedule an actual photo up for the first man on the moon.It’s shocking. It goes together with the fact that they lost the original tape of the first moonwalk.
And of course their claim is that Armstrong was such a good photographer that he got to take all the pictures.
It doesn’t take a good photographer to take those pictures. They have the camera strapped on the chest.All they have to do is set the F-stop to focus the diaphragm, the lens opening the iris. And press click. They’re not even aiming, because they have the camera strapped to the chest. So all these shots that are well composed are actually a stroke of luck. Because you cannot see inside. You don’t have a viewer. You don’t have the viewfinder in that situation. So they’re really aiming by moving their shoulders. And guess what? All the pictures are so perfectly centered. Which is a little suspicious.
And here we see that Alan Bean and Pete Conrad of Apollo 12 are apparently even better photographers from the chest than Neil Armstrong is. These are even more “extraordinary.” And there were a total of 583 photos allegedly taken by Alan Bean and Pete Conrad of Apollo 12.
There’s absolutely nothing (extraordinary). What’s so incredible about this, is it is a set. All you need to do is sit there, focus and click. I mean there’s no artistry. The very idea that you’re looking for artistry…
Well, the horizon is horizontal.
The horizon is horizontal. And there are no hills in the distance, by the way. If you take what’s called the 360 panoramic of the whole, you turn around, you just stand there and turn around, click click click. And then they join them all together and you have a 360.
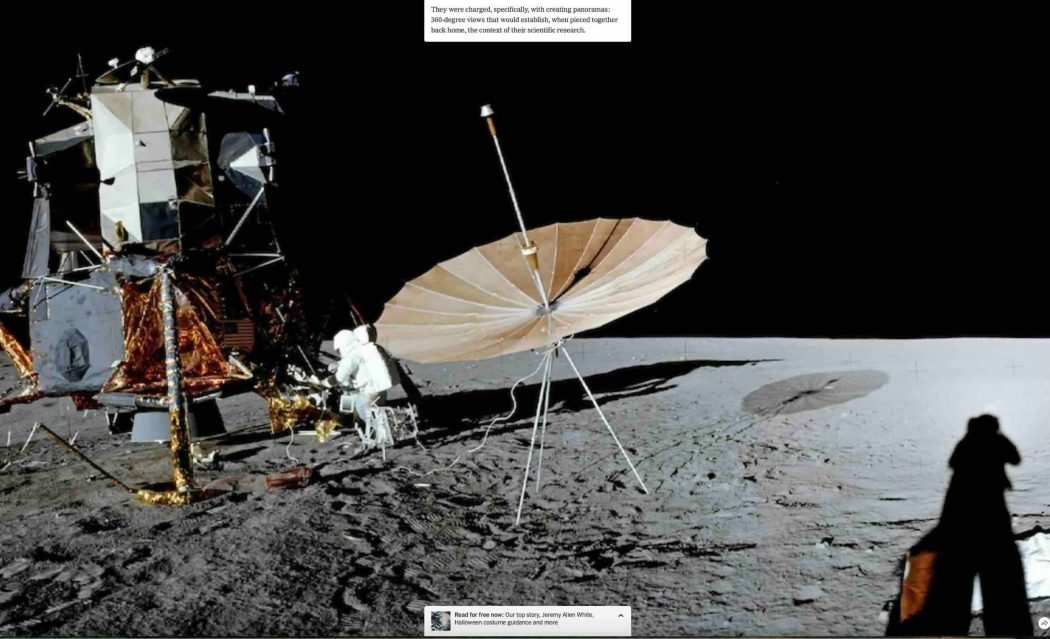
This landscape is like 200 yards not even in every direction. There’s no hills anywhere in the distance. Only after Apollo 15 did they realize that their sets were so skimpy that they had to add mountains in the distance. Apollos 11, 12 and 14 had a very very short horizon like this. I mean very short. And if you think that that object on the left was put there by a man, it means that the distance from here to there is maybe 20 yards. So you have another 20 yards and then what’s the end of the moon? There’s nothing else.
Yeah, that’s a pretty flat moon.
Look! The shadow of the LEM reaches almost the end of the moon. There’s no distance. I mean, think! You’re in a desert. You have to picture yourself in a desert with a LEM and imagine there’s nothing behind that little hill. There’s nothing. You can see nothing. It’s a joke. This is clearly a set. And besides, because of the use of the wide angle, this actually looks larger than it was in reality. In reality this set is no more than 10 meters by 10 meters, 30 feet by 30 maybe. That’s about it.
We’re told that they were “tasked with creating panoramas, 360-degree views that would establish when pieced together back home the context of their scientific research.” Then in the New York Times presentation it shows you the 360-degree panorama. Here’s the theme of the whole piece: “In one-sixth gravity, art and science did not seem so far apart.” They’re trying to tell us that the amazing artistry of these photos is some hybrid of art and science.
I really fail to see any artistry at all in these pictures. I’m sorry. I mean I know enough about good photography. Not only have I been a professional photographer for 25 years but I have enjoyed photography. I loved it. I know the great photographers, from Ansel Adams to Karsh. There’s a lot of history of photography that I can recognize. And I tell you what is an artistic picture. I see absolutely nothing artistic about these at all.
You’re not going to add Neil Armstrong to the list of great photographers…
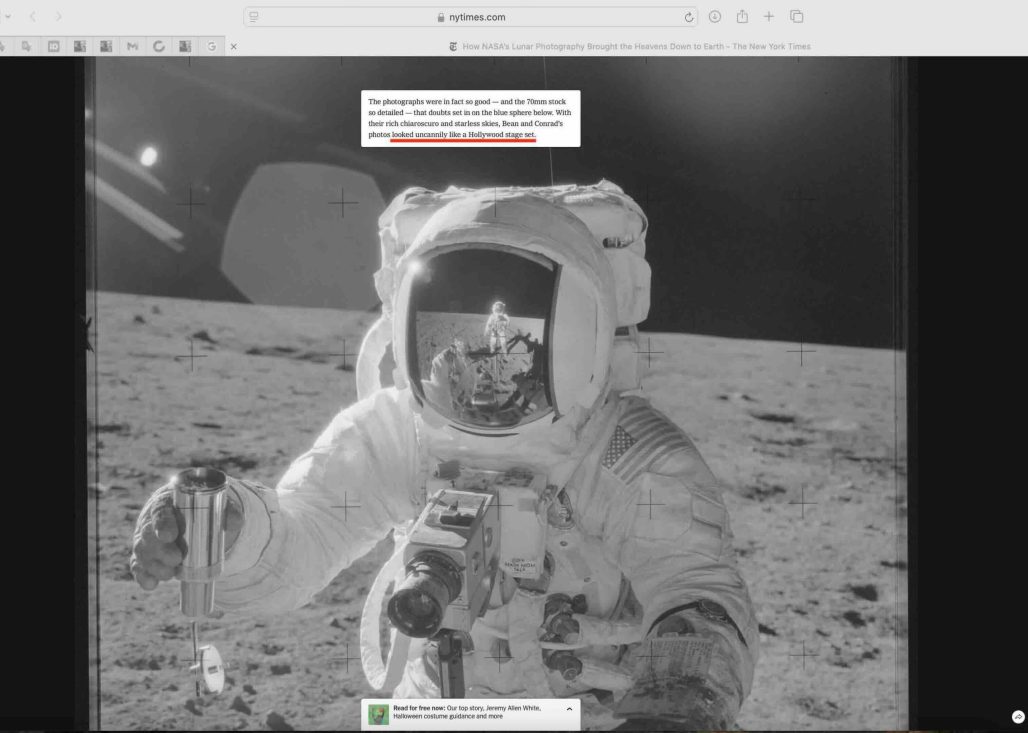
Okay, here again the astronaut reflected in the visor, the little guy in the middle of the picture: On his right, our left, the terrain is much darker than on his left, our right. The sun is on the side. It should be equally illuminating both sides of his background. It is not. That means that is a spotlight that centers on him and it’s illuminating more the right-hand side from the way we see it than the left. That’s called an oopsie.
Interestingly, they chose this picture to tell us that it’s so good that it looks like a Hollywood stage set. This reminds me of Douglas Rushkoff’s Coercion, which describes mind control techniques that are common to operators from CIA interrogators to used car salesmen. And he describes how the key to mind control is to basically break down the subject’s sense of reality. And the way they do that is: the used car salesman takes you for a test drive. And at just the right point in the test drive he kind of turns to you while you’re driving the car and he says: “Is this the kind of car that you can see yourself driving?”And you try to see yourself driving the car that you actually are driving, and you have a sort of a brain fart. You have this space-out moment and lose contact with reality. And the car salesman then just takes over your world and orders you to drive back to the dealership. And he doesn’t ask you, do you want coffee? He just forces you to drink coffee, brings out the contract, and you walk out with the new car. And the CIA does a similar thing when they interrogate you. And so anyway, in this example, they’re inoculating you against the idea that this is a stage set by telling us it looks so good that it almost looks like it could be a stage set.
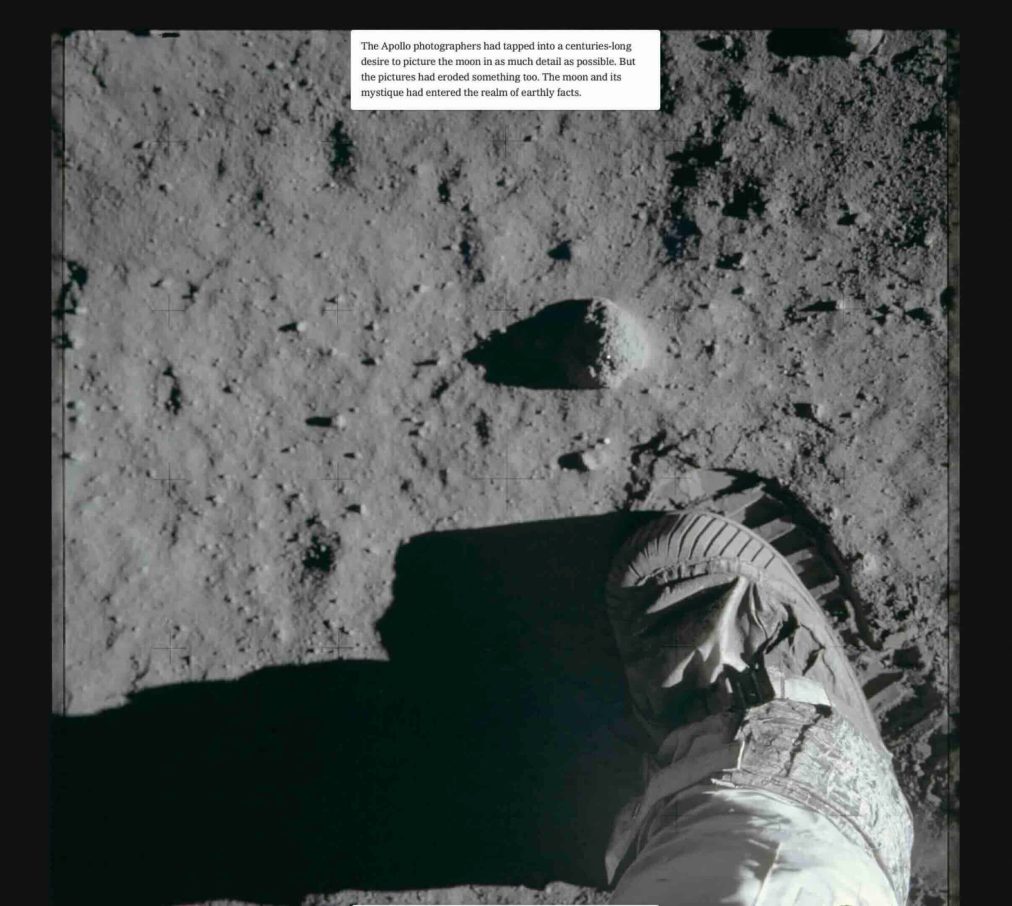
This is not the best picture of a footprint. But you can tell even from this picture—look how sharp and how… how sturdy, how solid are the little (rectangles of “moon sand”) that look like chocolate bars imprinted in the sand. Remember, there’s no atmosphere. Therefore there’s no humidity. Therefore that sand should be falling apart as soon as you remove your foot. How can you make it stick in such precise shapes without the humidity on earth?
Maybe they brought a little aerosol spray can and some gluey substance.
Exactly. You need humidity to get sand to stick like that. And there’s no humidity on the moon.
Why Lebanon doesn’t trust Israeli-American intentions — and why it shouldn’t
By Hussein Mousavi | Press TV | November 1, 2025
As Lebanon’s government, led by Prime Minister Nawaf Salam, inches closer to implementing its multi-phase plan to disarm Hezbollah, one question continues to divide the country:
What if Hezbollah lays down its arms… and the Israeli regime still doesn’t change its behavior?
The plan – drafted under the supervision of the Lebanese Armed Forces (LAF) and backed by the US, France, and several Arab states, including Saudi Arabia, Qatar, and the UAE – seeks to reassert the state’s monopoly on the use of force.
On paper, it sounds like a long-delayed step toward full “sovereignty.” That’s how the Lebanese premier and his allies – both inside and outside the country – try to present the issue.
Yet for many ordinary Lebanese, the proposal feels less like progress and more like exposure. And so, it raises a deeper fear.
Disarming the Hezbollah resistance movement, they fear, could strip Lebanon of its last line of deterrence, without changing anything about Israeli long-standing hostility.
Syrian precedent: Disarmament without security
Elsewhere in the region, Syria’s experience stands as a grim reminder. Even after the Jolani regime made public gestures toward normalization with the Israeli regime, the airstrikes on Syrian territory have never stopped. They continued unabated.
These attacks – justified by Israel as “preemptive” measures against so-called Iranian entrenchment (despite any evidence suggesting the same) have convinced many in Lebanon that military restraint does not necessarily guarantee security.
To many Lebanese, that says it all: even a weakened and cooperative neighbor hasn’t been spared unprovoked Israeli assault.
So, for the majority of Lebanese, the question resonates: If a disarmed, diplomatically compliant Syria was still bombed, why would a disarmed Lebanon be treated any differently?
That logic has sunk deep… even among communities once skeptical of the resistance. This isn’t about ideology anymore. It’s about survival, sovereignty and dignity.
People genuinely fear that weakness, not resistance, invites aggression.
Social undercurrents: A shift in perception
Hezbollah’s argument for keeping its weapons has always been rooted in resistance to Israeli military occupation and the defense of Lebanese sovereignty and territorial integrity.
For years, that claim was losing traction—chipped away by the US, Israeli regime (Hasbara), and Persian Gulf-funded campaigns that painted the resistance movement as a destabilizing force.
But the chaos next door changed the mood.
The violence in Syria, especially the relentless massacres committed by Al-Qaeda-linked groups in Suweida, jolted many Lebanese back to a hard truth: in a region defined by uncertainty and terrorism, some form of deterrence is still necessary.
Even among Christians and Druze, there’s a quiet shift. What was once a divisive argument is slowly becoming a reluctant consensus:
“Lebanon without a deterrent is Lebanon exposed. And now, no one in Beirut really believes the skies will stay quiet after disarmament. Not anymore.”
Washington’s back-out: The missing guarantees
Lebanese skepticism was further reinforced by Washington itself. If anyone still hoped for international reassurance, Washington’s recent message was clear.
During his visit to Beirut, US envoy Tom Barrack openly admitted that Washington could not provide any binding guarantees that the Israeli occupation forces would refrain from future military action, even if Hezbollah were to be fully disarmed.
It was a rare moment of honesty, and a devastating one. For many Lebanese, it confirmed what Hezbollah has been saying for years: Without credible security guarantees, disarmament amounts to a strategic suicide.
Barrack’s inflammatory statement spread quickly across social media platforms and prime-time talk shows. It fueled the perception that Western powers are happy to demand disarmament but will not lift a finger to protect Lebanon afterward.
So, for now, Hezbollah’s deterrent remains the only shield people trust in a region where promises evaporate, and treaties rarely hold.
A state caught between principle and survival
That leaves the Lebanese government trapped in a painful paradox and facing an impossible balance.
Internationally, disarmament is pitched as a prerequisite for reconstruction after the 2024 Israeli aggression. Domestically, it looks more like a setup, an attempt to squeeze out concessions that Washington and Tel Aviv couldn’t win through war.
PM Salam insists the Lebanese Army can fill the security gap once Hezbollah disarms. But everyone knows the LAF is overstretched, underfunded, and struggling to retain personnel amid an economic meltdown.
Even LAF Commander “Rodolph Haykal” has quietly admitted the limits.
And with UNIFIL’s mandate due to expire in 2026, the southern buffer zone that once helped keep the peace is fading fast.
Given these realities, Hezbollah’s arsenal (long portrayed by Israeli, American, and certain Arab media as “the problem”) is tied to something deeper: the complete absence of trust in Israel’s intentions, and the lack of any reliable security guarantees from its allies.
Trust, deterrence, and the price of “peace”
Trust can’t be declared in a press release. It’s earned through behavior, consistency, and respect. For Lebanon, disarmament cannot be separated from reciprocity.
Unless the Israeli regime demonstrates, through verifiable actions, that it will respect Lebanese sovereignty – and unless those commitments are backed by enforceable international guarantees – any talk of disarmament will remain politically impossible and socially toxic.
A peace built on parity
Lebanon’s real dilemma isn’t whether disarmament is good in theory. It’s whether peace can exist without parity, and whether Western powers are willing to enforce that parity with real guarantees, not vague assurances.
Until that happens, every call for disarmament will collide with the realities of regional mistrust… and also with the same hard truth: You can’t convince its citizens to give up their shield when the sky above them still burns.
And that’s why, for many in Lebanon today, neither the government nor the resistance has any reason to trust the Israeli regime.
Hussein Mousavi is a Lebanese journalist and commentator
Burevestnik and Poseidon: Russia’s New Double Deterrent Against First Strike Aggression
Sputnik – 01.11.2025
President Putin has announced the back-to-back successful testing of the Burevestnik nuclear-powered, nuclear-capable unlimited range cruise missile, and the Poseidon nuclear-powered, nuclear-capable unmanned underwater vehicle. Sputnik asked a seasoned US Army vet and military analyst to comment on Russia’s new twin deterrence potential.
“The Burevestnik and the Poseidon are very interesting weapons… pretty much designed as defensive in nature,” retired US Army Lt. Col. Earl Rasmussen told Sputnik, characterizing the pair of nuclear doomsday scenario strategic systems as an effective new “counter strike type of capability.”
Touting the twin systems’ miniaturized nuclear engines as their key standout capability, Rasmussen noted that nuclear power essentially means unlimited range and loitering.
The weapons fundamentally enhance Russia’s nuclear deterrence, according to the observer. “There are some crazy generals out there that think they can win, do a preemptive strike and win a nuclear war, which is insane, essentially,” Rasmussen recalled, alluding to ideas like the Prompt Global Strike (PGS). Burevestnik and Poseidon are designed to nullify them.
With a system like the Poseidon, “you don’t have to strike anything. You could detonate it, probably flood and wipe out the entire British Isles or the entire east coast of the United States. So the impact could be quite devastating,” and far beyond the ‘acceptable loss’ calculations of any PGS-style planners.
“Like I said, I don’t look at Russia using them as a pure offensive-type weapon. I look at them as more of a defensive weapon and as a counterstrike type of capability. But it really, really enhances that capability to counter an adversary’s offensive actions against Russia,” Rasmussen summed up.
Kupyansk and Krasnoarmeysk Encirclements Make Ukraine’s Defeat ‘Too Big to Hide’
By Ekaterina Blinova – Sputnik – 01.11.2025
Volodymyr Zelensky and his Commander-in-Chief Oleksandr Syrsky are infamous for sacrificing Ukrainian lives to prolong fighting, Mikael Valtersson, former officer of the Swedish Armed Forces and Air Defense, tells Sputnik, commenting on the Krasnoarmeysk (Pokrovsk) and Kupyansk encirclements.
“[Their] policy has left up to 20,000 Ukrainian soldiers in a very precarious position. They are left with two bad alternatives, either being eliminated defending hopeless positions or taking heavy losses during a very hard withdrawal. In both cases Ukraine will lose invaluable military units,” Valtersson notes.
There is a little, if any, chance that Zelensky could order a surrender, as “the worst thing that could happen from Kiev’s point of view would be thousands of retreating or surrendering Ukrainian soldiers,” according to the pundit.
Zelensky’s team has put on a brave face, insisting there are no encirclements, while barring foreign journalists from the area.
“Such journalists would only expose Kiev’s lies about the situation and crush Ukrainian credibility,” Valtersson says.
Meanwhile, Ukraine’s defeat is a thing too big to hide, the military expert notes, projecting that Russia’s advance in November and December would lead to Ukraine losing several cities.
“Large cities like the Slavyansk, Kramatorsk, Konstantynivka urban area, Zaporozhye, Dnepropetrovsk and Kharkov might be up for grabs,” the pundit suggests. “The worst is yet to come for Ukraine in 2025. We are now witnessing the final fall of Krasnoarmeysk and Kupyansk.”
The Evolving Lens on SIDS: From Mystery to Focus on CDC’s Schedule
By Jefferey Jaxen | November 1, 2025
In America, infants are dying at a rate of around 1,300 to 4,500 per year depending on the reporting source. Lives ended suddenly, unexplained with the greater medical system appearing to be okay with it as evidenced by their lack of deeper investigation into the ‘syndrome.’
Sudden Infant Death Syndrome (SIDS) has long-haunted parents and pediatricians alike. Defined traditionally as the sudden death of an apparently healthy infant under one year old for unknown reasons – scientific and legal momentum may be moving towards public understanding.
For decades, it was viewed as an enigmatic “diagnosis of exclusion,” often chalked up to environmental factors like prone sleeping, overheating and in extreme cases blaming the parents for abuse.
Yet, as of 2025, this static portrait is fracturing. Emerging research, landmark court rulings, and legislative reforms reveal SIDS not as a singular black box, but a tapestry of metabolic, genetic, and iatrogenic vulnerabilities—chiefly, immature detoxification pathways and post-vaccination inflammatory cascades.
Florida’s House Bill 188, filed for the 2026 legislative session, exemplifies this paradigm shift legislatively. The bill amends state statutes to mandate comprehensive autopsies for Sudden Unexpected Infant Deaths (SUID) and Sudden Death in the Young (SDY), explicitly requiring microscopic toxicology, full immunization records from the past 90 days, and reporting to the CDC’s national SUID/SDY Case Registry.
No longer optional, these protocols aim to unmask hidden contributors, such as vaccine excipients or genetic polymorphisms, that prior “undetermined” classifications obscured.
And the best part, the bill comes with penalties for noncompliance—fines up to $5,000 and potential license revocation—underscore a growing impatience with incomplete probes. By integrating immunization data with federal surveillance, HB 188 positions SIDS investigations as proactive risk-factor hunts, potentially reclassifying dozens of annual cases from “unexplained” to preventably-framed within the context of the largely untested infant CDC vaccine schedule.
This rigor finds stark validation in the 2023 U.S. Court of Federal Claims ruling on Sims v. Secretary of Health and Human Services (No. 15-1526V), a rare vaccine court triumph that dismantled SIDS as a default for post-vaccination fatalities.
An eleven-week-old infant succumbed just eight hours after receiving five routine shots after a well baby visit. Autopsy revealed cerebral edema [brain swelling] and pulmonary congestion.
The Special Master Christian Moran ruled the vaccines triggered a “Table” encephalopathy via cytokine storms breaching the blood-brain barrier, leading to herniation and arrest. Expert witnesses retained by the Sims family skillfully displayed and achieved the “preponderant evidence” standard under the National Vaccine Injury Compensation Program (NVICP) against all odds that the Department of Justice attornies and their expert witnesses fought to deny justice.
HHS Secretary Kennedy said during a 2025 interivew with Tucker Carlson:
“The lawyers in the Department of Justice, the leaders of it were corrupt. They saw their job as protecting the trust fund rather than taking care of people who made this national sacrifice.”
The Sims family vaccine court award of $300,000 has ignited momentum and advocacy. As detailed in Wayne Rohde’s June 2025 Substack analysis, the case—amid fewer than 5% NVICP death-claim successes—challenges the “coincidental” narrative, urging deeper scrutiny of ~100 pending infant petitions. With the appeal deadline passing without action, we may be witnessing a precedent-proof vaccine link in such cases, eroding SIDS’s explanatory monopoly.
Scientifically, the puzzle pieces align with revelations on cytochrome P450 (CYP450) enzymes, the liver’s metabolic gatekeepers. A 2025 paper by Dr. Gary Goldman has highlighted infants’ CYP450 immaturity: at birth, activity hovers at 30-60% adult levels, with preterm babies hit hardest by “poor metabolizer” genetics (15-40% prevalence).
These enzymes process vaccine adjuvants like aluminum (up to 3,350 mcg in year one) and polysorbate 80. A vicious circle appears as inflammation from shots further suppresses the detoxification ability prolonging toxin exposure.
VAERS data clusters 75% of SIDS-like reports within a week post-vaccination, peaking at day two—echoing the Sims timeline. In serotonin-deficient brains (flagged in 70% SIDS autopsies). In a node to Florida’s SB 188, Dr. Goldman’s study warns current toxicology protocols ignore these developmental gaps, fostering misclassifications.
Together, these threads weave a bolder SIDS narrative: less “syndrome,” more sentinel for systemic oversights. HB 188’s mandates, the Sims precedent, and CYP450 insights demand holistic federal and state-level probes—genetic screening, excipient dosing tiers, and inflammation biomarkers. As Rohde posits, transparency could halve misattributions, saving lives while honoring the unexplained’s gravity. In 2025, SIDS evolves from fatalism to fixable, urging science and policy to catch up before another crib goes silent.
Blanket Informed Consent for Biologics Could Be Deadly
What You Need to Know and Need to Do
By Dr. Sherri Tenpenny | November 1, 2025
There’s a linguistic shift happening inside the walls of hospitals, surgical centers, and outpatient clinics — one that most people won’t notice until it’s too late. The word “vaccine” is vanishing from medical consent forms. In its place is a far broader, far murkier term being used: biologics. Let’s clarify some definitions:
- Biologics refers specifically to a class of therapeutic drugs and medical products that are produced from living organisms or their components (e.g., made from proteins, organ cells, tissues, blood, tallow, gelatin, glycerol, etc.). Biologics are specifically regulated medical products that are made from or contain components of living organisms.
- Biogenics is a broader, more general term meaning produced by living organisms or biological processes. It could be anything made by a living organism — plants, animals, bacteria, fungi, etc.
Examples:- Tree resin (produced by plants)
- Coral or seashells (made by marine animals)
- Methane (from decaying organic matter)
- Alcohol (from yeast fermentation)
Therefore, all biological products are biogenic, but not all biogenic materials are biological products. That means many new, modern medicines labeled “cutting-edge” — from mRNA injections to bioengineered cells — fall into the category of medically regulated biogenic products.
The Redefinition of Medicine
At first glance, it may sound harmless. Buried in the word salad of admission paperwork is a seismic change you might be agreeing to without realizing it. As a patient in a hospital, you could be injected, infused, or implanted with a biologic product you never specifically discussed with your treating physician, simply because the consent form used a broad term like “biologics” or “biogenics” and you didn’t fully understand the scope of that word.
It’s not that the hospital is secretly adding products; rather, the way the consent forms are worded gives them legal permission to use FDA-approved biologics or biologic materials when they are deemed medically necessary, without first discussing the pros and cons of the product.
You can view the full list of biologics on the FDA’s website. Vaccines are listed among the “approved biologics.” If you blindly sign a consent to receive a biologic, you’ve opened the door to a sweeping range of interventions that go far beyond what most would knowingly authorize.
Informed Consent: A Myth in Modern Medicine
The purpose of requiring informed consent is to promote the autonomy of the individual in medical decision-making. It is a legal doctrine that supports many of our cherished American ideals about our rights as individuals.
For decades, medical care has been governed by the principle that patients must be fully informed, fully aware, and provide informed consent for every healthcare procedure. It was more than a legal requirement; it has long been an ethical cornerstone. But as PubMed’s 1996 article, Legal and Ethical Myths About Informed Consent reminds us, even the foundation of informed consent came from a murky beginning.
In attempting to ascertain the origins of the phrase “informed consent,” it was first in a 1957 California case; no antecedent cases could be unearthed. The entire informed consent paragraph (in the first informed consent case) was adopted verbatim, and without attribution, from the amicus curiae brief submitted by the American College of Surgeons. It is an ironic twist of history that informed consent was dreamed up by lawyers employed by physicians.
Over time, the standard for truly informed consent has quietly been eroded. In many hospitals and clinics, informed consent forms have become little more than a formality: a few checks in digital checkboxes and a scribbled signature on an iPad. These consent forms are often buried within pages of fine print drafted by attorneys, intentionally dense and difficult to read. Even patients who try to understand the language find it nearly impossible to decipher.
The forms no longer use plain language. Instead of saying “Do you consent to receive the influenza vaccine or a COVID jab?”, the consent form may now ask if you consent to the use of biologic agents. The assumption is that you, the patient, understand that vaccines are biological agents. This raises the question: Is the confusing change in language intentional?
“Medically Necessary Biologics” — The Next Frontier
There is a push to categorize biologics as medically necessary. Once that phrase becomes standard, it reframes these products as non-optional. That’s a linguistic shift that carries enormous implications. If something is medically necessary, then refusing it becomes extremely difficult.
Now imagine being prepped for surgery. You’re told you must sign standard consent for “biologic products as necessary during the procedure.” You sign, thinking it refers to anesthesia, sutures, IV fluids, perhaps antibiotics. Your body then becomes an open field for whatever the institution – or your doctor – regards as necessary: a flu shot, a pneumonia shot, a pertussis shot, a monoclonal antibody infusion, or plasma/blood (perhaps from a COVID-vaccinated donor). You may never know what went into your body unless you ask for the record.
The Problem with Blanket Consent
Let’s look closer at what biologics encompass, according to the FDA and Congressional Research Service documents: Vaccines, monoclonal antibodies, gene therapy, whole blood and plasma, stem cells and T-cells, recombinant proteins, and growth factors.
The side effects of biologics vary depending on the specific product and how it is administered. Because these therapies are derived from living systems and often target the immune system, they can produce a wide range of reactions — from mild and localized to serious or life-threatening.
Most biologic drugs carry a risk of allergic or hypersensitivity reactions, since the body often recognizes the biologic as foreign. Those used to treat autoimmune conditions such as rheumatoid arthritis or psoriasis work by suppressing immune activity, which can increase the risk of infections. When given by injection, biologics often cause redness, swelling, or pain at the injection site; those administered intravenously can trigger infusion reactions, such as flushing, shortness of breath, or a sudden drop in blood pressure.
Common side effects include allergic reactions, injection-site irritation, chills, weakness, diarrhea, nausea, vomiting, rash, itching, high blood sugar, cough, and constipation. Other frequently reported effects are shortness of breath, leg swelling (peripheral edema), headache, fever, muscle or joint pain, decreased appetite, elevated triglycerides, insomnia, abdominal or back pain, dizziness, and various infusion reactions.
More serious side effects have included low blood pressure, anaphylaxis, serious or opportunistic infections, cancer, serum sickness, autoimmune thyroiditis, blood clots, heart failure, bleeding disorders, interstitial lung disease, hepatitis, enterocolitis, gastrointestinal perforation, stomatitis, anemia, and low white blood cell counts.
Each biologic drug has its own safety profile, and not all patients will experience these reactions. But because biologics act deeply within the body’s immune and cellular systems, their side effects can be complex, unpredictable, and sometimes severe. These products are not something you should be given without knowing the risks!
The Anesthesia Loophole
Anesthetized patients cannot give or withdraw consent in real time. Hospitals know this — and legal teams have prepared for it. That’s why pre-operative consent forms now carry generalized clauses authorizing “treatment using biologic materials.”
The rationale sounds protective: “We need flexibility in case of complications.”
The reality is exploitative: “We can administer what we deem appropriate.”
Under this loophole, you could receive a biologic without your explicit approval. Once it’s in your body, it cannot be undone. While this remains only a theoretical concern at this time, as AI increasingly takes over healthcare and personal options continue to be reduced, it is distinctly possible.
I found court cases where a patient received a biologic without specific consent. (here) (here). I didn’t find a published U.S. case that squarely says: “Because of the single word biologics in a blanket consent, a sedated patient got a biologic they would have refused.” But these two cases demonstrate the core risk is real.
What You Must Do
We are living in a time when words have become deceptive, from politics to healthcare. To protect yourself, you must re-establish your authority over your own body. Here’s a place to start. Print this and keep it with your health insurance card:
- Read every word. Never sign a consent form that contains vague terms like “biologics,” “biogenics,” or “cell-based therapies” without a full explanation from your doctor(s).
- Ask direct questions. Ask out loud: “Does this include vaccines, gene therapies, or blood products?” Write their answers and whether you agree or disagree.
- Refuse in writing. On both digital and paper copies, clearly state: “I do not consent to the administration of vaccines, biologics, or other synthetic materials.”
- Get a copy. Always request a printed copy or photo of your signed form, especially if it was done on an iPad.
- Have an advocate. Assign a trusted person to reiterate your refusal verbally and in writing if you are incapacitated. If you don’t have a close friend or family member who can navigate this with you, hire someone from GraithCare.com. They are knowledgeable and worth every penny.
- Document everything. After discharge, review your medical record and confirm what was administered. Side effects or complications may not materialize for weeks or months.
This is not paranoia; this is precautionary and wise self-care. The same level of attention you’d give to a financial contract should apply even more importantly to your medical care.
Bodily Autonomy Is a Spiritual Battle
At its heart, this is about sovereignty. The right to decide what enters your body — what merges with your cells — is not just a medical decision, it’s a moral and spiritual obligation.
Scripture says our bodies are temples of the Holy Spirit, not laboratories for untested technologies. To surrender consent to vague, corporate-crafted terms like “biologics” is to give the keys away to your own temple. I believe every human being deserves the dignity of true informed consent, not coerced compliance through deceptive wording.
Closing Thoughts
We are a litigious society, and physicians are always concerned and on the defensive about avoiding lawsuits. The timeless advice from that 1996 article on how you can best be perceived and help your patient’s decision-making process:
The best advice we can give is to treat patients like people, act sensitively and compassionately, and most of all, talk to patients. Have a conversation, have several; remember that this is a process. In this process, you will gradually come to know your patient’s decision-making style. Furthermore, do not press patients to decide quickly. Do not make them think that you do not have time for them. Because if you do, regardless of how much information they are given, they are going to be angry, and another name for an angry patient is plaintiff.
So please, before you sign anything: stop. Read. Ask. Refuse if you must. Line out what you don’t agree with, initial it, and date it. Your signature implies permission.
Featured Video
America Racing to Strategic Defeat in Iran
or go to
Aletho News Archives – Video-Images
From the Archives
Should Europeans ‘Thank’ the Americans for Destroying Nord Stream?
By Robert Bridge | Strategic Culture Foundation | September 29, 2022
With an investigation continuing into the destruction of the Nord Stream gas pipeline that provided energy supplies to Europe from Russia, there appears to be just one prime suspect, and that should surprise nobody.
Following the sabotage of the Nord Stream 1 and 2 gas pipelines, former Polish Foreign Minister Radoslaw Sikorski already seemed to know the identity of the perpetrator when he tweeted out: “Thank you, USA.”
At first glance, it seemed that Sikorski was speaking sarcastically, berating Washington for carrying out an attack that will have severe repercussions for the people of Europe. After all, how could anyone see any good coming from the termination of Europe’s primary source of gas reserves with winter just around the corner? It was Sikorski’s homeland of Poland, after all, that urged its citizens to collect firewood in the face of dwindling gas reserves.
In fact, the Polish diplomat was speaking one-hundred percent literally… continue
Blog Roll
 Aletho News
Aletho News- Growing insecurity, soaring prices fuel protests in north as regime bans evacuation: Sources
- Iran denies responsibility for ‘depraved’ attack on Kuwait desalination plant
- Bring The Troops Back. End This War Now!
- Can we please stop calling Israel the ‘only democracy in the Middle East’ now?
- US should start removing its troops from Germany, proposes AfD co-leader Chrupalla
- Iran Red Crescent: 600 educational centers attacked in US-Israeli ‘war crimes’
- Russian Oil Tanker Arrives in Cuba Amid U.S. Blockade
- America Racing to Strategic Defeat in Iran: Lt Col Daniel Davis
- FTC Warns Visa, Mastercard, PayPal, Stripe Over Political Debanking
- Russian tanker approaches Cuba despite US oil blockade
- If Americans Knew
- As Iran targets US military bases, will they be relocated to Israel? Not a ceasefire Day 171
- Will Trump Go Kamikaze?
- Is the University of Florida Shutting Down College Republicans over Israel Criticism?
- Jewish extremist arrested over alleged plot to firebomb Palestinian activist Nerdeen Kiswani’s home
- More than half of Palestinian child detainees have no charges
- The More Murderous Israel Gets, The More We Hear About “Antisemitism”
- Land Day and the Palestinian struggle after 30 months of genocide
- The Iran War Is About Palestine
- Israeli soldiers echo settler ideology, talk of revenge after targeting Palestinians and detaining CNN crew in the West Bank
- Israeli Policies Threaten Future of Christian Schools in Jerusalem
- No Tricks Zone
- New Study Finds Warming Saves Lives…Cold Temperatures 12 Times More Deadly Than Excess Heat
- German Science Blog Accuses PIK Climate Institute Of Hallucinating Climate Tipping Points
- Devastating Assessment Of Comirnaty Vaccine By Former Senior Pfizer Europe Toxicologist
- New Study: CO2 Is ‘Effectively Negligible’ As An Explanatory Climate Change Factor Since 2000
- Former Pfizer Toxicologist Dr. Helmut Sterz Tells Bundestag Hearing Pfizer Vaccine Should Have Never Been Approved
- Energy Expert: Germany’s Nuclear Phaseout Was A “500 Billion Euro Mistake”
- New Research: South Australia’s Mid-Holocene Sea Surface Temperatures Were 4°C Warmer Than Today
- Storing Green Energy To Last Germany 10 Days Would Require A 60-Million Tonne Battery
- New Studies: UK Sea Levels Were 4 Meters Higher Than Today During The Mid-Holocene
- Destructive Green New Deal: German Energy And Metal Group Warns Of Drastic Crisis
