The UK Joins the Pirates
By Craig Murray | June 15, 2026
I was genuinely surprised by the Starmer regime’s refusal to state that the Israeli boarding of the Global Sumud flotilla on the High Seas was illegal. I did not realise it was because the UK was planning to undertake similar illegal seizure itself.
The Gaza Flotilla seizure was illegal: while for obvious reasons freedom of navigation had been the undisputed basis of UK maritime policy for centuries. The UK is a set of islands whose population is dependent on food imports to stay alive. Freedom of navigation is a core strategic interest of the UK. The relevant provisions of the UN Convention on the Law of the Sea were very heavily UK driven, including on passage through straits.
Abandoning the primacy of freedom of navigation is absolutely a radical policy departure for the UK, driven like so many other changes to traditional British legal positions by the Starmer regime’s extreme support for Israel.
It is not generally understood how profound a change this is. Even the Tory government of David Cameron, with William Hague as Foreign Secretary, had opposed the Israeli naval blockade of Gaza and particularly Israeli seizure of vessels on the High Seas. William Hague stated in 2010 to the House of Commons of the boarding of the Mavi Marmara:
We are seriously concerned about the seizure of British nationals in international waters,
This is a long term British legal position now directly repudiated by Starmer, Lammy and Cooper.
I had not realised that not only was the UK now supporting the campaigns of illegal blockade and seizure of vessels being openly pursued by Israel and by Trump, but Starmer was actually intending to abandon freedom of navigation and join the Trump/Netanyahu doctrine.
That is what the UK has now done by its seizure of the Smyrtos as it had passed through the Straits of Dover en route to Sikka in India.
The Dover Strait is a strait. The clue is in the name. The UK has absolutely no right to close it to Russian shipping. This is in Article 39 of the UN Convention of the Law of the Sea:
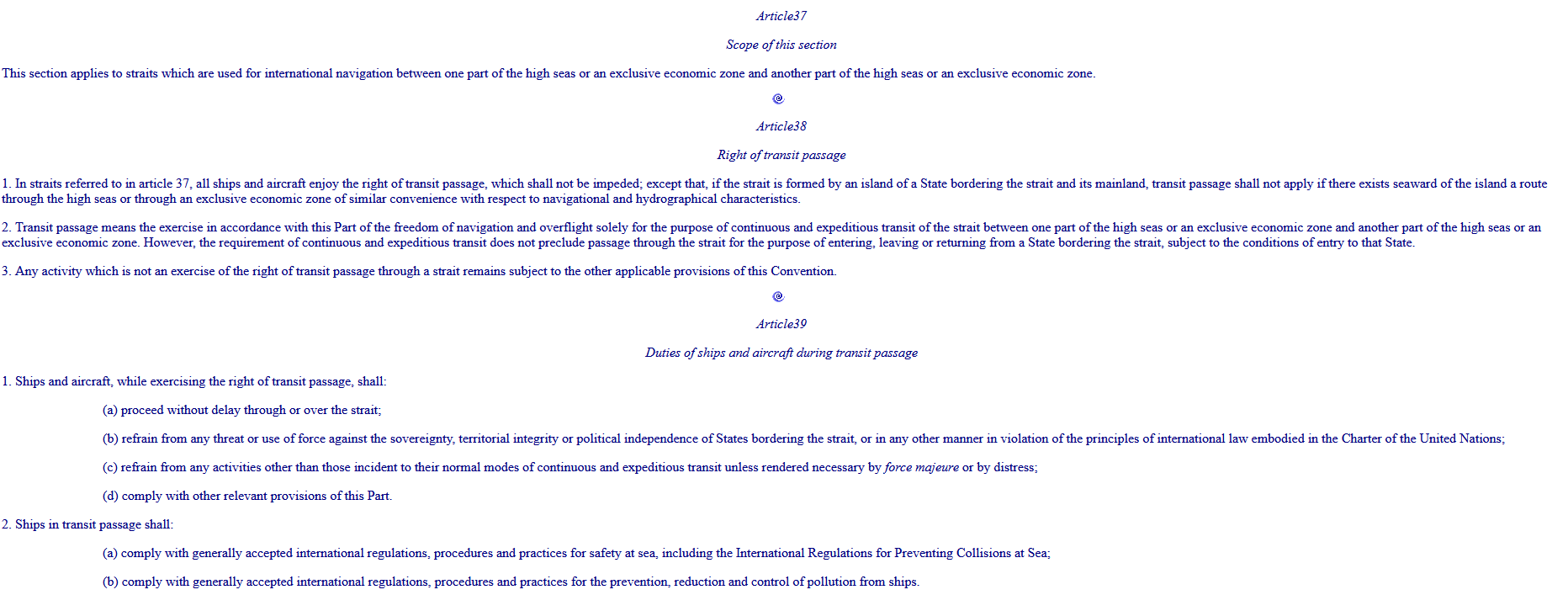
Transit of international straits “shall not be impeded” is pretty plain. This is the applicable legal regime for both the Strait of Dover and the Strait of Hormuz. Obviously in time of war different considerations apply, and commercial shipping of belligerent states – and to and from belligerent states – becomes a legitimate target. Iran is fully justified in also treating states permitting attacks launched from their territory as belligerent states.
If hostilities end this Article 39 regime that should apply again in the Strait of Hormuz.
It is worth a footnote to say that Iran had, until the recent illegal aggression by Israel and the United States, always strictly observed the international law on straits even though Iran did not sign the Convention and actually had entered a formal reservation on passage through straits. Even during the war, Iran had attempted, in extremely difficult circumstances, to establish a system for passage of genuinely neutral vessels.
It is astonishing that at this moment, when navigation of the Strait of Hormuz is arguably the single most live question in all of international politics, the UK has decided to abandon the principle of free transit through straits.
It takes hypocrisy to an entire new level, it truly beggars belief, that the day after closing the Dover Strait to Russian shipping, Starmer issued a joint statement with Germany, France and Italy insisting on “Freedom of Navigation” in the strait of Hormuz.
Even if you don’t care about international law and believe that Trumpian realpolitik is better, to act against freedom of navigation now would seem an unwise decision. The UK is now copying actions like the United States naval blockades of Cuba and Venezuela, and the Israeli genocidal blockade of Gaza. These are gross violations of the Law of the Sea.
UK Government minister Lisa Nandy was on television news last night as the government pumped out militaristic propaganda. The Royal Navy’s action in boarding and capturing an entirely unarmed and peaceful merchant vessel was portrayed as an act of Nelsonian brilliance. Nandy justified the seizure on the grounds that Russia’s oil sales pay for its war with Ukraine, and that the UK was enforcing sanctions against Russia.
Neither provides an atom of legal justification for seizing the vessel. The UK is not at war with Russia. Ukraine is, and the Ukrainian navy would have been entitled to seize the vessel. For reasons of cheap popularity and to increase the massive amounts of public money swirling around the corruption honeypot of military spending, UK ministers seem determined to move us to the brink of war with Russia. But we are still not at war, and the UK accordingly has no right to seize peaceful and innocent Russian bound, owned or flagged commercial vessels.
The UK is legally entitled to put whatever sanctions it wishes on Russia. But it can only enforce those within its legitimate jurisdiction. A foreign vessel, even when engaged in innocent passage or transit passage through a UK strait or other territorial waters, is not under UK jurisdiction. The Smyrtos was in fact in international waters south of the UK when seized.
In fact this attempt to enforce western sanctions in areas where western powers have no jurisdiction is a classical example of the current aggressive resurgence of imperialism, where the “rules based order”, meaning rules imposed by the imperialists, replaces international law.
Nandy also stated that the Smyrtos was a member of the “Russian shadow fleet”. This is a term that the Starmer regime and their client mainstream and corporate media have relied upon repeatedly to demonise the Russian owned or directed merchant fleet.
Russia sells oil to countries like India and China perfectly lawfully. That this oil is carried in ships bearing flags other than Russian is perfectly normal.
Nil or close to nil of those ships carrying hydrocarbons to and from the UK are UK registered and flagged.
It has been a sad truth of international shipping for many decades that commercial vessels bear flags of convenience, and that jurisdictions compete to offer the very lowest standards of crew salary and welfare regulations, officer and crew training, vehicle condition and maritime safety and inspection regimes.
Most of the registries of well-known international flag of convenience states such as Panama, Liberia and the Marshall Islands, do not really exist in the sense of being government departments of those countries, as they should be. They are private companies with almost no real world footprint, which pay a fee to the government to operate the registry, and collect the fees from the shipowners registering. The register is just names in a laptop – and very often that laptop is in London.
UK colonies often have substantial such fake registries. The UK is a strong opponent of the International Transport Workers Federation, which has struggled against this system to improve mariners’ rights.
The system evolved for wealthy shipowners to avoid all maritime safety, environmental and welfare regulation, and the UK and other western countries which pander to the needs of the ultra wealthy have always been complicit. The incredible hypocrisy of western states pointing fingers at Russia for running “Flags of convenience” is breathtaking.
The West has spent decades building and profiting from the global flags of convenience system. Russia is simply using the same system that Western companies created and still dominate.
Incidentally the MOD’s own propaganda footage, shown by all UK mainstream media yesterday, proves that the Smyrtos is a modern, clean, well-equipped and comfortable vessel and all the propaganda about ancient rustbucket is completely untrue.
I have finally managed to pin down the alleged legal basis of the seizure of the Smyrtos, and it is that the vessel was stateless and thus subject to boarding under Article 110 of the UN Convention of the Law of the Sea.
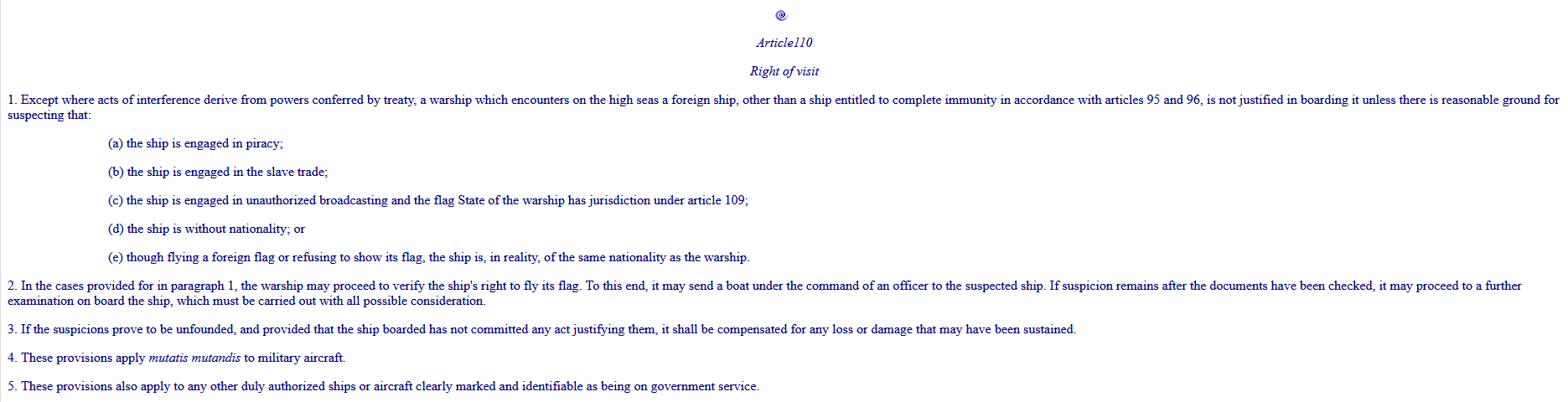
The UK is claiming that the Smyrtos fell foul of Article 110.1 (d) that it was “without nationality”.
We will inspect that claim more closely in a moment. But, assuming it for a moment to be true, note that you only have a right to visit and inspect on the High Seas a ship that is without nationality. Article 110 absolutely does not confer any right to seize a ship on the High Seas not found on inspection to be in unlawful activity. The UK has seized the Smyrtos, brought it into UK territorial waters and then claimed it is under UK jurisdiction.
Nowhere is that allowed in the Convention.
Now let us look at the claim that the Smyrtos is without nationality. This is an astonishing story which the media will not tell you.
When the Smyrtos set sail from Russia it was flying the Cameroonian flag, and on the Cameroonian register. That is not in doubt.
While the ship was on its voyage, on 10 June Cameroon withdrew its registration. It did so because the EU and UK threatened to halt development aid to Cameroon unless they removed Russian vessels from their shipping register.
So the UK blackmailed Cameroon into deregistering the ship. Then, before the ship could reach a friendly port, the UK boarded it because it had been deregistered.
Now doubtless there are chortling people in the UK security and military industries self-congratulating themselves over how clever they are. But while this may be a clever ruse de guerre, it is hardly a ruse de paix. It is not going to survive scrutiny by an international court. An unexpected change of registration, forced upon the owners, is very difficult to complete instantly, but doubtless one was in train and perhaps finished. The UK actions are patently – and deliberately – unreasonable.
Politicians seek to drum up cheap popularity by stupid jingoism. Starmer has won a cheap headline. The world inches closer to the next world war. The UK loses yet more legitimacy in the eyes of the wider world.
Meantime Trump claims as a great victory a possible return of the Strait of Hormuz to the open status it enjoyed before he started an illegal war in the interests of Israel.
Freedom of navigation was a principle worth defending. It has been abandoned in favour of a return to the rule of the seas by those with the strongest navies. Fortunately Putin is neither as war hungry nor as politically desperate as Starmer. However Russia will now be obliged to send at least a frigate to keep the Strait of Dover open. The drums of war beat ever closer.
Craig Murray is a former Head of Maritime Section of the UK Foreign and Commonwealth Office. He is a former Alternate Head of the UK Delegation at the UN Preparatory Commission for the UN Convention on the Law of the Sea.
Israeli government plans to fund extremist occupier group in occupied West Bank with $1.89M: Report

MEMO | June 15, 2026
The Israeli government of Prime Minister Benjamin Netanyahu plans to allocate 5.5 million shekels ($1.89 million) in state funding to the extremist occupier group known as the “Hilltop Youth,” the Yedioth Ahronoth daily said Monday.
The newspaper said the budget was outlined in a document issued by the Settlement and National Missions Ministry, headed by Minister Orit Strock, which will oversee the transfer of funds through regional settlement councils in the occupied West Bank.
The funding plan is scheduled to run from June through the end of the year and totals 5.5 million shekels, it added.
According to the newspaper, each member of the Hilltop Youth movement would receive the equivalent of approximately $550 per month to help cover food, clothing and living expenses for more than 650 youths living in hilltop outposts and pastoral settlement sites across the occupied West Bank.
The Hilltop Youth is an occupier movement whose members primarily live in unauthorized settlement outposts in the West Bank and are known for opposing efforts to evacuate them.
The group has frequently been linked to attacks against Palestinians and is considered the ideological nucleus of the extremist “Price Tag” movement, which has carried out retaliatory attacks against Palestinians and their property.
Founded in 1998, the movement is largely composed of Israeli occupiers aged between 16 and 26, who left their homes and schools to live in illegal settlement outposts built on hilltops overlooking Palestinian communities.
The group is considered an offshoot of the extremist movement Gush Emunim, which advocates expanded Jewish settlement in the occupied Palestinian territories.
According to Israeli and Palestinian rights groups, violence by Israeli occupiers in the occupied West Bank has increased significantly in recent years, including attacks on Palestinian communities, farmland and property.
Since Oct. 8, 2023, at least 1,169 Palestinians have been killed, 12,666 injured, around 23,000 arrested and approximately 33,000 displaced in the occupied West Bank amid intensified Israeli military operations and occupier attacks, according to Palestinian figures.
Press TV reporter wounded in Israeli drone strike on southern Lebanon

Hadi Hoteit, Press TV correspondent in southern Lebanon
Press TV – June 15, 2026
A Press TV correspondent has been struck by an Israeli drone while reporting in southern Lebanon, despite wearing a clearly marked press vest.
Israeli forces deliberately targeted Hadi Hoteit in the southern Lebanese town of Kfar Tebnit on Monday, according to Lebanon’s National News Agency (NNA), despite the journalist wearing clearly marked press gear.
Hoteit sustained a shrapnel wound to his foot and was transported to Al-Najda Al-Shaabia Hospital in Nabatieh, where he underwent surgery and is receiving medical treatment.
The NNA reported that the Israeli military fired a shell that landed near the journalist.
The strike comes just one day after Iran and the United States finalized a memorandum of understanding to end the war on all fronts, including in Lebanon.
Despite the announcement, Israeli forces continue to attack areas in southern Lebanon.
Shortly before the attack, Hoteit posted on X, “We are back to South Lebanon, and hopefully the ceasefire this time will be different. This is my understanding of the situation and possible scenarios.”
Also on Monday, an Israeli drone struck another car at a roundabout in Kfar Tebnit, killing one person.
Time for Trump to Tell Benjamin Netanyahu to Go Away!
Netanyahu always says “What you own belongs to me”
By Philip Giraldi • Unz Review • June 14, 2026
In addition to the regular lethal American and Israeli attacks on Iran, last week alone the Israeli military killed 13 Gazans and 13 Lebanese. Gaza is now 70% Israeli occupied, contrary to what was agreed upon in the ceasefire arrangement, as is much of south Lebanon. More than 1,000 Gazans have been murdered by Israel since the temporary ceasefire was declared in October 2025. And one might add to the toll the constant aggression in south Syria, where Israel is creating an army base presence to be followed by settlers that creeps ever closer to the capital Damascus. It is an encroachment that Prime Minister Benjamin Netanyahu and his band of war criminals intend to turn into a component of “Greater Israel” together with Gaza and Lebanon.
Armed Jewish settlers are meanwhile devastating what remains of the Palestinian West Bank, destroying farms and livelihoods as well as entire villages. Taybeh, the last Christian village, was made uninhabitable last week after weeks of raids killing livestock, poisoning water and cutting down olive trees. If a Palestinian tried to intervene he was beaten and in some cases killed. Churches and Mosques on the West Bank are routinely desecrated and non-Jews in religious attire or trying to enter a holy site are frequently spat upon particularly in Jerusalem. The Israel Defense Force (IDF), meanwhile, regularly stands by and watches the displays of wanton brutality and does nothing. Lest there be any confusion regarding what is coming, the Knesset has now authorized $51 million to build more than 60 new completely illegal settlements on Palestinian land in the occupied West Bank.
What all these places have in common apart from the cruel Israeli hand is that the United States, often in the form of Trump personally, has been a guarantor of the ceasefires as well as the source of the so-called but utterly dysfunctional Board of Peace, has done nothing to stop the slaughter. Rather, it is continuing to provide Israel with weapons, money and political cover. It is therefore complicit in the war crimes. Here at home, Trump is promoting the Israeli program by supporting the criminalization of anyone who speaks up against the crimes against humanity being committed by his “best friend” Bibi, choosing to destroy freedom of speech rather than allowing any exposure of Israel’s crimes. This is reminiscent of June 8th 1967, when Israel attacked the USS Liberty, killing 34 American crewmen and injuring 172 more. A cover-up followed to protect Israel, coordinated by President Lyndon B Johnson, a hideous excuse for a human being who would likely have found it pleasant to have a chat about “values” with Trump.
If there is one thing that is most definitely true it is that the United States gains absolutely nothing in either the national interest nor in the well being of the average American from the bondage to Israel and Netanyahu. If opinion polls mean anything, the public in the US has figured that out and has turned sharply against the Jewish state and now favors both the Palestinian cause and the drive to end the totally meaningless war against Iran. That means that it is past time for the United States to cut the tie that binds with Israel and look to its own interests. That is necessary even if Congress and President Donald Trump continue to push in the opposite direction to complete their subjugation by the Israelis, which now includes a planned fusion of the US and Israeli defense and intel bureaucracies.
If we have learned anything from all of the above and more, there is one thing true about the President Donald Trump administration and that is its particular incompetence at foreign relations, i.e. how it deals with other nations, and, by extension, how it mismanages national security. Part of the blame surely belongs to Trump himself as he has little or no empathy for other human beings unless they are either capable of doing him harm or profiting him personally, as do Netanyahu and the Jewish billionaires. And he also has a tendency to change direction spontaneously and without much concern for the actual issues that might be important to his audience. All that matters is whatever he happens to think will make him look good at any given moment, which recently has manifested itself as plastering his own name on public buildings. Responding to a recent journalist’s question about the rising inflation rate, he answered that he “Loved the inflation!” It was like saying “Goodbye midterms!”
Witness for example how on Thursday last week Trump announced in the morning that he would be attacking Iran that night to seize its major oil export facility on Kharg Island as part of a plan to cripple the country’s ability to sustain energy shipments. By 2 o’clock in the afternoon, however, he had called off the planned attack due to his perception that the US and Iran are now on the verge of an agreement to end the fighting and settle the various issues that have created the conflict in the first place. The mediating Pakistani Prime Minister did, for what it’s worth, confirm a possible peace agreement on Friday even though knowledgeable observers immediately commented that the claim was unsustainable as no negotiations were actually going on between parties and Iran has denied any such progress over key issues. As of Saturday, nothing was confirmed but Trump again asserted that there would be a “signing” of a “memorandum of understanding” as a first step to a peace agreement on Sunday, presumably to coincide with his birthday. Most observers however continue to argue that a weak-kneed and vulnerable Trump, though desperate to disengage from a disastrous Iran war, is only staying with it due to intense pressure from Israel and its domestic US lobby which may be prepared to employ “Epstein” blackmail on the president to maintain American participation in the conflict. If Trump were even to consider withdrawing from his ring of fire around Iran Israel would immediately take whatever steps are necessary to blow-up the agreement and resume fighting, be it by way of a false flag to drag the US back in or possibly exploiting the “Iran has a nuke” lie.
So it would be wise to accept that Donald Trump is a ship without a rudder and interactions with most of the Middle East will continue to be driven by Israel while bilateral talks elsewhere with major players like Russia and China appear to have dried up completely. Appointing real estate billionaires Steve Witkoff and son-in-law Jared Kushner as personal presidential representatives, both of whom are inexperienced and ardent Zionists, certainly did not improve prospects for what passed for negotiations with anyone. No one can trust Trump.
Israel’s reach far exceeds the country’s size and real power. A recent “friend” of Trump is Argentine Prime Minister Javier Milei, who, surprise-surprise, is also a great friend of Israel, having made the usual obeisance trip to the Wailing Wall in Jerusalem during a State Visit to Israel shortly after being elected. Raised a Catholic, Milei reportedly wanted to convert to Judaism but decided not to as its “no work on Saturday” rule would have interfered with serving as prime minister. Not content with taking all the Middle East, Israel’s Jews are also looking farther afield. Patagonia in Argentina has reportedly been particularly targeted by Israeli buyers with the assistance of the Milei regime which helped get around environmental restrictions. Israelis are also buying up numerous properties in Cyprus as well as in Greece, nearby states which would be convenient as refuges if Israel finally provokes one too many of its neighbors and it finds itself on the receiving end of a nuke. Benjamin Netanyahu’s resident American spy Jonathan Pollard reportedly has mentioned both Turkey and Egypt as “next” to feel the wrath of Zion after Iran is finished off. Either army could easily defeat the chickenshits in the Israeli army who are better at raping and torturing than they are at fighting.
But one story that has caught some attention illustrates clearly the Israeli manic desire to steal other peoples’ property, most particularly land, no matter what it takes to carry out the theft. As is always the case, they are not held accountable for their criminality by Donald Trump who has his own soft spot for stealing the property of others and chooses to cut corners, witness the grandiose plans for a Trump Riviera luxury development on the beachfront of Gaza. And then there are the current shenanigans on an island off Albania which is being multi-billion dollar “developed” by daughter Ivanka and son-in-law Jared Kushner using United Arab Emirates (UAE) cash to become a major resort for the rich and famous. Kushner got the money as a benefit derived from his family connection and fortunately a lot of Albanians are mad as hell about the deal that was struck and are demonstrating!
But the story out of the United States and Canada as well as over the weekend in London tops many of the Trump/Israeli tricks due to its sheer audacity and criminality. Amnesty International UK is demanding the British government stop a real estate event scheduled to take place in London that includes companies openly advertising the sale of land in Israeli settlements in the illegally occupied West Bank.
The ‘Great Israeli Real Estate Event’ is a traveling roadshow that has held events in Canada and the United States and has now been planning for the sale in London on Sunday. The events are organized by Israeli real estate firm called My Home in Israel. It sells land to prospective buyers through a team of US-based real estate agents with the sales normally taking place in synagogues or other Jewish-owned and operated buildings. There have inevitably been protests against the sales in cities like Los Angeles and New York, where the “lots” have been promoted to the local Jewish communities. The lots being sold include considerable sections located in illegal settlements on the Palestinian West Bank, land that has been stolen from its owners. The Amnesty International report published last week in opposition to the London show exposed Israel’s state-led ethnic cleansing campaign in the West Bank – “documenting the displacement of at least 5,910 Palestinian Bedouin and herding community members since 2023, the demolition of over 3,400 homes and structures in [Palestinian West Bank] Area C, and an unprecedented surge in state-backed settler violence and land grabs.”
So there you have it, whatever Israel wants Israel takes without any concern for those who die or lose their homes in the process. And the United States government sits by and watches as Netanyahu spins lie after lie. Well, enough is enough. America is hated almost as much as Israel for its behavior and if it continues there will be severe consequences. Time to show Netanyahu the door and tell him and his supporting cast of AIPAC and Jewish billionaire buddies to get the hell out.
Philip M. Giraldi, Ph.D., is Executive Director of the Council for the National Interest, a 501(c)3 tax deductible educational foundation (Federal ID Number #52-1739023) that seeks a more interests-based U.S. foreign policy in the Middle East. Website is https://councilforthenationalinterest.org address is P.O. Box 2157, Purcellville VA 20134 and its email is inform@cnionline.org.
Israeli officials: ‘Security zones’ to remain in Lebanon, Syria, Gaza

Al Mayadeen | June 15, 2026
Israeli War Minister Israel Katz said the Israeli army will continue to hold so-called “security zones” in Lebanon, Syria, and Gaza indefinitely, asserting that what he described as border security requirements take precedence over any political or diplomatic arrangements.
He stated that the policy is being pursued in coordination with Israeli Prime Minister Benjamin Netanyahu, adding that the IOF would remain deployed in these areas without a defined timeline.
According to Katz, the stated objective of maintaining these zones is to prevent what he described as threats from armed groups operating near the borders.
He said Israeli forces would remain in the “security zones” in Lebanon, Syria, and Gaza in order to protect Israeli settlements and border areas, framing the deployments as a defensive necessity to mask its colonial nature.
“We will not compromise on the vital interests of Israel’s security and the protection of our citizens, and we will not leave the security zones,” Katz said.
He also stated that this position had been communicated to US President Donald Trump, US War Secretary Pete Hegseth, and other senior officials.
Netanyahu signals rejection of withdrawal from Lebanon
Separately, Israeli media cited officials close to Prime Minister Benjamin Netanyahu as saying that he informed Trump that “Israel” does not intend to withdraw from Lebanon under any emerging understandings linked to regional negotiations.
According to these reports, Israeli forces will remain in their current positions in southern Lebanon and continue what Tel Aviv describes as operations aimed at preventing threats from Hezbollah.
Netanyahu also reportedly rejected any linkage between developments on the Lebanese front and broader US-Iran diplomatic arrangements, insisting that “Israel” would not be bound by agreements affecting its military posture.
Internal political backing for hardline stance
Israeli political figures across the governing coalition expressed support for maintaining occupation deployments in Lebanon and other theaters.
“Israel’s” Finance Minister Bezalel Smotrich was quoted in Israeli media as arguing that any attempt to connect the Lebanese and Iranian fronts should be resisted, while also emphasizing the importance of preserving military deterrence without direct confrontation with Washington.
Other ministers, including Itamar Ben-Gvir, reportedly stated that any US-brokered agreement with Iran would not be binding on “Israel”, asserting that Tel Aviv would continue to determine its own security policy independently.
Energy Minister Eli Cohen and Transport Minister Miri Regev also stressed the need to maintain what they described as clear deterrence while avoiding unnecessary escalation with the US administration.
Israel Fails to Sabotage Islamabad Accord… At Least for Now
By Larry C. Johnson | SONAR21 | June 14, 2026
Well, when news broke that Israel had bombed the southern suburb of Beirut on Sunday afternoon, the Iranians started gearing up for promised retaliation only to be dissuaded by a Donald Trump bribe. Iran and the US reportedly were closing in on an agreement based on Iran’s 14-point plan when the Israeli strike in Lebanon threw everything into chaos. Iran quickly started ramping up for a renewed missile strike on Israel, but Donald Trump rump reportedly offered Iran financial incentives to not attack Israel.
Iranian media outlet Mehr reported that a 14-point memorandum of understanding between the US and Iran calls for the release of $24 billion in frozen Iranian assets during a 60-day negotiation period, with half of that — $12 billion — required to be made available to Iran before negotiations even begin. The MOU also reportedly includes immediate and permanent cessation of war on all fronts including Lebanon, a US commitment not to interfere in Iran’s internal affairs, lifting of the naval blockade within 30 days, and reopening of the Strait of Hormuz under Iranian arrangements.
Trump essentially offered Iran a bribe to not attack Israel. Hedeclared on Truth Social that the US deal with Iran was “now complete,” authorizing the toll-free reopening of the Strait of Hormuz and the immediate removal of the US.naval blockade, instead of waiting 30 days. He also agreed that Iran could receive the $12 billion as soon as the ceasefire agreement was signed on Friday.
With that change, the Supreme National Security Council of Iran confirmed the achievement of an agreement between the United States and Iran:
“The Islamic Republic of Iran, under the leadership of its martyred leader, has completed its success over the American-Zionist enemy and, under the guidance of the Supreme Leader of the system (may God protect him), with the support of the entire nation and the diligent efforts of Islam’s warriors, after a difficult and intensive several months of negotiations and based on the resolution of the Supreme National Security Council, finalized the text of the Memorandum of Understanding regarding negotiations to end the war (negotiations in Islamabad) between Iran and the United States on the evening of June 14.
According to the agreements reached, the war and military operations on all fronts, including Lebanon, will end immediately and forever from tonight, and the naval blockade against Iran will be immediately and fully lifted. The signing of this Memorandum of Understanding will be officially carried out on Friday, June 19. Negotiations for the final agreement will be postponed until the other party fulfills its obligations in accordance with the Memorandum of Understanding. The Islamic Republic of Iran highly values the efforts of the Islamic Republic of Pakistan and the government of Qatar.”
But before you start popping champagne corks you must understand that Trump administration officials — mostly unnamed — are painting a different picture of the agreement. For example, asenior U.S. official rejected Iran’s claim that it would receive $12 billion in frozen assets unconditionally before the start of the 60-day negotiations, describing the assertion as “a spin,” Axios reports:
This is completely not true. This is a pay-for-performance deal, and no frozen funds will be released without the Iranians implementing their commitments,” the official said.
The point is simple… Major differences remain between the US and Iran regarding the details of the proposed MOU. Even if those details are eventually ironed out and a letter signed on Friday with both sides confirming their mutual agreement to the 14 prinicipals spelled out in the final MOU, this will mark the start of a negotiations process that will last at least two months, if not longer. And, at any time in the succeeding days, a US or Israeli violation of the MOU will likely lead Iran to renew its attacks on Israeli and/or US military targets.
Araghchi: US Responsible for Implementing MoU with Iran
Al-Manar | June 15, 2026
Iran’s Foreign Minister Abbas Araghchi has stressed the US’ responsibility regarding the implementation of the MoU with Iran as well as a complete halt to the Israeli regime’s attacks against Lebanon.
Araghchi made the remarks in his separate phone calls with Turkish, Iraq, and Egyptian counterparts Hakan Fidan, Fuad Hussein, and Badr Abdelatty.
He reviewed the process and provisions of the Islamabad understanding and lauded the positions and role of Turkey, Iraq, and Egypt in supporting the establishment of a ceasefire, reducing tensions, and diplomatic efforts to achieve stability and security in the region.
All sides emphasized the continuation of close consultations on regional developments and strengthening diplomatic efforts to maintain peace and stability.
Iran and the United States, after announcing a ceasefire on April 8, 2026, began negotiations with the mediation of Pakistan to definitively end the war.
The text of the memorandum of understanding that was signed, the foundation of which was Iran’s 14-point proposals at the very beginning of the ceasefire, was reviewed multiple times over the past 60 days in the capitals of the two countries.
Despite all the pressures, the violation of the ceasefire, and the repeated changes of position by the United States, Iran persisted in its stances.
After signing the MoU text, the two countries will put a series of intensive negotiations on their agenda over the next 60 days in order to reach a comprehensive agreement on the disputed issues.
US must cut military, intelligence assistance to Israel to protect Iran deal: Ex-Trump official
Press TV – June 15, 2026
A former official in US President Donald Trump’s administration says cutting US assistance to Israel could help strengthen the agreement between Tehran and Washington, amid the Tel Aviv regime’s continuous attempts to sabotage regional peace.
Joe Kent, who left the administration after disagreements over the United States’ joint unprovoked aggression against Iran alongside the regime, made the remarks in a post on X on Monday.
He welcomed the prospect of the conclusion of a memorandum of understanding between Tehran and Washington that could be followed by an agreement.
Kent said the durability of any agreement with Iran could be improved if the United States reconsidered its military and intelligence support for the regime, saying that Israeli officials have opposed efforts to achieve a diplomatic settlement.
The former Trump administration official said Washington should seek to eliminate factors that could prompt the US to resume the aggression “on Israel’s terms.”
A day earlier, Iran’s Foreign Ministry had announced that the MoU had been finalized and would be officially signed in Switzerland on Friday.
On April 7, Trump announced a ceasefire in the aggression, which had begun targeting the Islamic Republic on February 28 amid widely-reported Israeli instigation.
The announcement came amid decisive and successful Iranian retaliation and after the Islamic Republic announced closure of the Strait of Hormuz to enemies and their allies.
Following the announcement, though, the Israeli regime would keep violating another ceasefire in Lebanon, despite Tehran’s insistence that cessation of aggression should encompass all fronts.
Kent also advocated reducing the US military footprint at bases in the Persian Gulf’s littoral states.
“We should also quietly get our troops out of the bases in the [Persian] Gulf that can be reached by Iran,” he wrote.
Iran’s retaliation featured strikes on American outposts in the Persian Gulf’s coastal states that had allowed their territories to be used as launchpads for attacks on the Islamic Republic.
Iran deputy FM says MoU with US finalized, to be signed in Geneva on Friday

Press TV – June 14,2026
Iran’s Deputy Foreign Minister for Legal and International Affairs has announced that the memorandum of understanding (MoU) between Iran and the United States has been finalized and will be officially signed on Friday in Switzerland, while also declaring the immediate end of the US naval blockade and the permanent cessation of war on all fronts.
In remarks carried by Iranian media on Sunday, Kazem Gharibabadi confirmed that the text of the Islamabad MoU has been finalized.
“The official signing of the Islamabad memorandum of understanding will take place on Friday in Switzerland,” he said.
“Starting tonight, the US naval blockade against Iran will be terminated,” Gharibabadi added, declaring “the immediate and permanent end of the war and military operations on various fronts, including Lebanon.”
The announcement follows weeks of intensive negotiations mediated by Pakistan, with support from Qatar, Saudi Arabia and Turkey.
The finalization of the MoU brings an end to the US-Israeli war of aggression against Iran, which began on February 28.
With one strike, Netanyahu tries to kill two peace deals
Netanyahu knew exactly what he was doing when he defied Trump’s red line and struck Beirut this morning
By Trita Parsi | June 14, 2026
It’s important to understand that, contrary to Donald Trump’s quip to Barak Ravid that Netanyahu has “no f***ing judgment,” the Israeli Prime Minister knows exactly what he is doing: With a set of strikes at the Dahiyeh neighborhood in Beirut, he is trying to kill both the pending US-Iran peace deal and the fragile peace between Israel and Lebanon that would come with it.
There is a further strategic dividend. Netanyahu is also seeking to preempt Iran’s attempt to establish a new regional deterrence equation—one in which attacks on Beirut, and potentially on Lebanon more broadly, would trigger a direct Iranian response against Israel. By striking now, he is not merely targeting an adversary; he is challenging the emergence of a regional order that would constrain Israel’s freedom of military action.
Netanyahu even posted a video on his Twitter bragging about the attack.
The exchange of fire between Israel and Iran last week was about far more than retaliation. After Israel defied President Trump and struck Beirut’s Dahiyeh neighborhood, Iran responded by attacking Israel directly—the first time Tehran had launched strikes on Israel in response to an Israeli attack on Lebanon. Israel defied Trump once more and retaliated against Iran, prompting another Iranian response, after which Israel confined its next strike to southern Lebanon rather than Beirut.
The cycle reflected Iran’s attempt to establish a new regional equation: that attacks on Lebanon would no longer be cost-free for Israel, but would carry the risk of direct Iranian retaliation. For the first time in decades, a major regional power was seeking to place hard-power constraints on Israel’s freedom of military action beyond its borders.
Having reestablished its own deterrence, Tehran was now attempting to establish extended deterrence to its partners as part of a broader effort to rebuild its forward-defense posture. Israel, unsurprisingly, viewed this as a direct challenge to its long-standing freedom of maneuver and moved quickly to prevent the new doctrine from taking hold.
Of course, extended deterrence can not be established through a single exchange of fire. At a minimum, it would require several rounds of action and reaction before either side accepted it as a new reality. And even then, it would never be foolproof. Tehran understands that its purpose cannot simply be to eliminate Israeli strikes on Lebanon, but to force Israeli leaders to think twice before authorizing them by attaching a new and significant cost: the likelihood of direct Iranian retaliation.
It was therefore clear that Netanyahu had not abandoned the fight. Yet for several days, even as Hezbollah and Israel continued to exchange fire, he refrained from striking Beirut’s southern suburbs and testing Iran’s new red line.
But today, just hours before President Trump was expecting Iran to sign a memorandum that would end the U.S.-Iran war and reopen the Strait of Hormuz, Netanyahu crossed both Tehran’s and Trump’s red line: keeping Beirut out of the conflict.
Netanyahu clearly timed this for maximum impact. With a single set of strikes, Netanyahu may have advanced two goals at once—torpedoing Trump’s peace deal and preventing the emergence of a new deterrence equation that would impose meaningful constraints on Israel’s military operations in Lebanon.
A diplomat involved in the talks told Fox News that: “This is a clear attempt by Israel to sabotage the President’s deal and drag the United States back into war.”
Trump, meanwhile, is once again reportedly “pissed off” at Netanyahu. In a Truth Social post, the president declared that the strike on Beirut “should not have happened,” while pointedly questioning whether it was a proportionate response to Hezbollah’s latest attack on Israel.
“Israel has the right to defend itself against threats,” Trump wrote, “but the attack it was responding to was very small and meaningless. Nobody was hurt, injured, or killed, and it should not disrupt this important process.”
The statement was notable not merely for its criticism of Netanyahu, but for what it implied: that Israel’s strike was neither militarily necessary nor diplomatically prudent at a moment when a potential breakthrough with Iran appeared within reach.
Washington is frustrated by Tehran’s insistence that Trump rein in Israel, even as American officials believe Iran has failed to similarly restrain Hezbollah. It is equally frustrated that a deal it urgently wants with Iran is now being held hostage by Israel, ironically at the request of the Iranians, since it is Tehran that insists that any ceasefire must be region-wide and prevent Israel from having the ability to restart the war.
That frustration is understandable. But Washington must also recognize a basic reality: the only way to delink a U.S.-Iran agreement from the Israel-Lebanon conflict is to delink the United States itself from Israel’s recurring resort to military escalation.
As long as Israel retains the capacity to drag the United States back into conflict, Tehran will see little reason to separate diplomacy with Washington from the wars Israel chooses to start and pull the US into.
Indeed, the principal reason Tehran insists on a region-wide ceasefire is to deny Israel the ability to draw the United States into yet another war with Iran itself.
If Trump were to clearly establish that the United States would neither participate in nor defend an unjustified Israeli military escalation, Tehran might no longer see the need to link a U.S.-Iran accord to the Israel-Lebanon front.
Such a calculated distancing from Israel would serve American interests in any case. But the need for it has rarely been more apparent than it is today.
Iran warns ‘no point’ in deal with US if Israel remains unrestrained
The Cradle | June 14, 2026
Iran’s Parliament Speaker Mohammad Bagher Ghalibaf warned in a statement on 14 June that there is “no point” in continuing efforts to reach a deal with Washington if Tel Aviv remains unrestrained, a few hours after a new Israeli attack on Lebanon’s capital.
“The Zionists’ aggression against the southern suburb [of Beirut] once again demonstrated that the US either lacks the will to uphold its commitments or lacks the ability to do so,” Ghalibaf said.
“You cannot gain concessions by giving the [Israeli] regime a green light. The ‘good cop, bad cop’ game has grown old. If you lack the will and the ability to fulfill your commitments, then there is no point in speaking about continuing down this path,” the parliament speaker added.
Meanwhile, Brigadier General Mohammad Jafar Asadi, deputy commander and deputy inspector of the Iranian military’s Khatam al-Anbiya Central Headquarters, said Israel’s attack on Beirut’s southern suburb will not go unanswered.
“If you seek an agreement or understanding, you must discipline the Zionist regime. If this rabid dog is not controlled, it will bite your leg before the ink is dry on the agreement,” said Ebrahim Rezaei, spokesperson for the Iranian parliament’s Foreign Policy and National Security Committee.
The latest Israeli airstrike on the Lebanese capital took place earlier on Sunday afternoon. The attack hit a building in the southern suburb’s Ghobeiry area.
According to the Lebanese Civil Defense, three people were killed and six others injured.
The Israeli army claimed it bombed a “command center belonging to the Hezbollah terrorist organization in Beirut.”
“The targeted command center was being used by Hezbollah operatives to advance terrorist plans against the citizens of the State of Israel,” the Israeli military added, calling its deadly attack on Beirut a “precise strike.”
The new attack on Beirut coincides with intensive Pakistani mediation to secure a Memorandum of Understanding (MoU) between the US and Iran.
Among Tehran’s terms is a full ceasefire in Lebanon and an end to Israel’s wars, attacks, and occupation across the region.
Following an Israeli attack on Beirut earlier this month, Iran carried out a ballistic missile attack on an Israeli air base and vowed harsher retaliation in response to any new attacks on the Lebanese capital.
Featured Video

Iran Walks Out On Peace Deal Due To Trump’s Threats
or go to
Aletho News Archives – Video-Images
From the Archives
Neocons confess: “We did 9/11-anthrax”
By Kevin Barrett | Press TV | September 6, 2014
As the 13th anniversary of the crimes of September, 2001 approaches, the neoconservatives are shrieking from the rooftops – and effectively confessing that they were the real perpetrators of the 9/11-Anthrax false flag operation. (The neocons, you may recall, openly called for a “new Pearl Harbor” in September, 2000 – and got one exactly one year later.)
Every year at this time, the neocons orchestrate and hype a series of public relations stunts designed to magnify fears of “radical Islam” and reinforce their crumbling 9/11-Anthrax cover story. But this year’s propaganda campaign is so extreme that it represents a tacit confession: The neocons know that the truth about the 9/11-Anthrax operation is slowly closing in on them; so they are over-reacting by desperately trying to stoke the dying embers of the so-called War on Terror, in order to maintain the myth that Muslims (rather than neoconservative Zionists) attacked America in the autumn of 2001.
When a hysterical person exhibits guilty demeanor by trying too hard to blame a crime on someone else, that person is almost certainly the real perpetrator. As the neocons try much too hard to blame Islam for 9/11 and “terrorism” in general, their hysteria inadvertently reveals their own culpability. Like Shakespeare’s Lady MacBeth, the neoconservative movement has blood on its hands and “doth protest too much.” … continue
Blog Roll
 Aletho News
Aletho News- The Swiss summit of imperial humiliation
- Iran to continue IAEA cooperation under existing framework, SNSC decision: Baghaei
- Report highlights US munitions crisis: Missiles cannot be replenished quickly even with al the money in the world
- Iran’s Oil Spigot Could Open Soon But Hurdles Remain
- Trump’s Attempt to End the Iran War Infuriates the Uniparty
- First round of Swiss-hosted Iran-US talks ends with 5 key agreements
- What Is Hay Fever?
- IRAN WALKS OUT ON PEACE DEAL DUE TO TRUMP’S THREATS – w/ Prof. Seyed Mohammad Marandi
- Moderna’s mRNA Flu Vaccine Gets Unanimous Thumbs-Up Despite Risks, Low Efficacy
- UK Speech Regulator’s Telegram Questions Point Toward Private Chats
- If Americans Knew
- The Republican & Democratic Politicians Trying to Scuttle Iran Agreement
- Israel’s continued targeting of civilians in Lebanon renders ceasefire meaningless
- U.S. intelligence warns Israel is likely to undermine Iran peace deal, officials say
- In Gaza, Fathers Can’t Promise Their Children Food, Safety, or Even Survival
- This baby joins thousands of Gazans in need of medical evacuation
- Israel Kills Al Jazeera Journalist & Beloved Ecologist: 2 Articles
- Promoters of Israel: Leo Terrell, Ghana, Floyd Mayweather, Van Jones
- Gaza Soccer Player Who Dreamed of Competing in World Cup Can Now Barely Watch It
- Gaza baby loses mom and a leg; Palestinian prisoner tortured to death – Daily Update
- JNS Policy Summit to kick off in Israel
- No Tricks Zone
- 3 New Studies Find Increasing Trends In Solar Radiation Since The 1980s – Easily Explaining Warming
- THE TRANSCEIVER PARADOX: Why Organoid Intelligence (OI) Could Become Our Ultimate Alien Predator
- German Wind Turbines Face Regulatory Shutdown Due To Excessive Noise
- New Study: Chile’s Relative Sea Level Was 3.2 Meters Higher Than Today During The Mid-Holocene
- Beyond The Pitch: Why FIFA’s World Cup Is One Of Humanity’s Best Investments
- Climate Alarmists Now Using Natural Phenomena To Support Their Claims
- New Study: Significant CO2 Fluxes From Non-Volcanic Sources Are Largely Neglected In Carbon Budgets
- Women Climate Scientists Being Harassed, Insulted By Skeptics, Claims Berkeley Earth Researcher
- Germany’s Longterm Spring Climate Data Show “No Climate Trend”
- New Study: Solar Photovoltaic, Wind Power Fail To Meet Annual Energy Demands 62% Of The Time
