Victoria government lied about who had access to Covid contact tracing data

By Didi Rankovic | Reclaim The Net | December 28, 2021
The government of the Australian state of Victoria not only decided to deliberately keep citizens in the dark about court rulings exposing the fact the privacy of their data collected by contact tracing apps can be compromised – but is now doubling down.
And the way the state’s Acting Premier Jacinta Allan, who has currently taken over while Premier Dan Andrews is being investigated for “concealing treason and fraud,” chose to defend the failure to inform people about matters pertaining to sensitive private information about them was to say the government was – shielding them from misinformation.
Australian media say the attempts to hide the truth have been made repeatedly, and Allan’s logic in defending the move is that if revealed, the Supreme Court’s secret ruling that said the data was not “absolutely protected” would have given rise to a “baseless scare campaign” as media reporting the facts would have caused “fear and misinformation.”
She did not clarify what type of “misinformation and fear” was expected to arise from the truth.
“The decision was taken in the balance of providing confidence in the Victorian community that this wasn’t a matter that needed to have that level of misinformation spread about it,” Allan said on Tuesday of the way the multiple levels of deceit had been handled.
This Supreme Court finding came to light after the Herald Sun reported that despite explicit promises of information safety, and its use only for health purposes, this was a lie – and one ongoing for two years.
Instead of making contact tracing data available only in order to fight the epidemic, it was also available to law enforcement, and authorities like the WorkCover agency.
It was precisely that agency’s demands to be given access to tracing app data that launched the legal case, when the Department of Health asked the court to order WorkCover to stop.
Another revelation is that the state’s Covid commander Jeroen Weimar petitioned the court to keep the case secret for five years. He tried to persuade the court that maintaining Victorians’ trust in the tracing system was what really matters – at the same time downplaying the importance of the citizens’ right to know their data can be shared, despite assurances from Covid tracers that this was not possible.
Asked if it was right to hide from the public the truth about the safety of their data – and the fact a court case was unfolding financed by their tax money, Allan said, “They don’t deserve a fear campaign, they don’t deserve misinformation,” and added that their data “will be protected.”
Shadow Attorney-General Matt Bach sees the scandal differently:
“People should be shocked and appalled. We should never become accustomed to this level of dishonesty.”
Big Brother Watch launches legal challenge to England’s vaccine passport
By Didi Rankovic | Reclaim The Net | December 27, 2021
London-based rights group Big Brother Watch, a vocal opponent of Covid passes being introduced in England, has launched a legal challenge to the scheme it considers an example of divisive and discriminatory dystopia.
After raising nearly a quarter of a million pounds online to fund its cause (and crowdfunding campaign continues) – which Big Brother Watch said would go entirely towards fighting against Covid passes, including via costly legal challenges – the group has decided to oppose the government’s Covid passes law in court.
Big Brother Watch is challenging the law on mandatory Covid passports in England claiming that it violates privacy, and is draconian and discriminatory in nature. They are also raising concerns that the Human Rights Act and equality law may fall victim to the new Covid pass rules.
Previously, the rights group urged its supporters to speak up against the scheme as unnecessary and counterproductive, as well as introducing a checkpoint society, surveillance state, along with mission creep and detrimental measures that will become irreversible.
In a pre-action letter to launch the legal battle against the law that is proving to be highly controversial even among the ruling majority in the UK parliament, the group notes that the government failed to provide any evidence about the Covid passes benefiting public health, while a damning parliamentary report said that there was no scientific or logical justification for their introduction.
In addition, Big Brother Watch stated, the Scientific Advisory Group for Emergencies (SAGE) failed to recommend Covid passports, and for all these reasons the scheme is seen as draconian, and pointless.
Nonetheless, PM Johnson’s government recently pushed the proposal through parliament despite nearly 100 MPs from his Conservative Party voting against – the biggest rebellion of the Johnson era.
Since mid-December, those entering nightclubs, sports and other large events must show the pass that proves they have been fully vaccinated or recently tested.
In announcing the bid to reverse this policy by legal means, Big Brother Watch Director Silkie Carlo said that Covid IDs “don’t tell you that a person doesn’t have Covid or can’t spread Covid, but do make society less free, less equal and less accessible for people.”
New York Democrat introduces new social media censorship bill
The bill aims to curb people’s speech by targeting platforms
By Didi Rankovic | Reclaim The Net | December 27, 2021
If a state senator got his way, the state of New York could soon get a new law aimed at regulating what content can appear on social media. The bill is designed to circumvent existing federal-level solutions in some instances and is reportedly inspired by internal documents leaked by former Facebook employee Frances Haugen.
But many legal experts believe that the bill, if passed, would eventually be overturned as unconstitutional for preventing dissemination of protected content.
The bill sponsored by state Senator Brad Hoylman wants to tackle what’s referred to as unlawful online content such as “misinformation” (particularly around Covid/vaccines), and posts that might allegedly lead users to develop eating disorders or engage in self-harm.
Envisaged in the bill is an amendment to New York’s penal code that lets citizens, the state attorney general and city corporation councils sue tech companies behind social media networks, or individuals, if they are suspected of “contributing” to spread of misinformation in a manner that’s “knowing or reckless.”
And while the bill is worded in a way that states content seen as endangering people’s safety or health should be clamped down on if it is “promoted” – including (but not exclusively) by means of algorithms and other methods of recommendation, experts say the distinction between that and any post created by users is not clear enough to stand up to legal scrutiny.
“The distinction between ‘hosting’ and ‘amplifying’ content is incoherent,” Santa Clara University School of Law professor Eric Goldman has told the New York Post, adding that Hoylman has taken that “incoherent” idea – “and embraced its most censorial option.”
According to Goldman, content that Hoylman’s bill takes aim at, such as, but not limited to, what’s considered false or harmful information that concerns Covid or political issues is in fact protected free speech under the First Amendment.
And for that reason, this expert believes, the draft legislation is unconstitutionally overbroad.
Commenting on the bill, David Greene of the Electronic Frontier Foundation concurred that the law would face First Amendment hurdles, and noted that because of the rapidly changing official guidance regarding the pandemic, it is very hard to even define what qualifies for Covid misinformation (when so much “expert” information has turned out to be false.)
“It’s really very difficult to impose liability in an environment where the truth can be hard to grasp at any point in time,” this attorney remarked.
Health agency spied on millions during Covid lockdowns
RT | December 26, 2021
Canada’s Public Health Agency has admitted to secretly tracking location data from at least 33 million mobile devices to analyze people’s movements during Covid-19 lockdowns.
The agency earlier this year collected data, including geolocation information from cell-towers, “due to the urgency of the pandemic,” a PHAC spokesperson told the National Post, essentially confirming a report by Blacklock’s Reporter. The tracking data was allegedly only used to evaluate the effectiveness of lockdown measures and identify possible links between the movement of people and the spread of Covid-19.
PHAC obtained the information, which was “de-identified and aggregated,” through an outside contractor, Canadian telecommunications giant Telus. The contract ran from last March to October, and PHAC said it no longer had access to the data after the deal expired.
However, the agency plans to similarly track the movements of citizens over the next five years toward such ends as preventing the spread of other infectious diseases and improving mental health. PHAC last week posted a notice to prospective contractors seeking anonymous mobile data dating as far back as January 2019 and running through at least May 2023.
Critics argued that government tracking of citizens is likely more extensive than has been revealed and may become more troublesome in the years ahead.
“I think that the Canadian public will find out about many other such unauthorized surveillance initiatives before the pandemic is over—and afterwards,” privacy advocate David Lyon told the Post. He noted, too, that “de-identified” data can easily be “re-identified.”
Author Julius Reuchel said the tracking initiative smacks of a surveillance state spying on citizens “for your safety.” Another author, Paul Alves, said that with its new contract, PHAC will have direct access to all mobile location data, and expressed fear that “contact tracing will no longer require permission or a warrant.”
Leaked files expose Syria psyops veteran astroturfing BreadTube star to counter Covid restriction critics
BY KIT KLARENBERG AND MAX BLUMENTHAL · THE GRAYZONE · DECEMBER 24, 2021
By covertly recruiting popular YouTube influencer Abigail Thorn to counter growing opposition to UK gov’t Covid restrictions, psy-ops pros are bringing home the tactics they honed in the Syrian dirty war.
Leaked documents have revealed a state-sponsored influence operation designed to undermine critics of the British government’s coronavirus policies by astroturfing a prominent founder of the BreadTube clique of “anti-fascist” YouTube influencers.
The project aims to conduct psychological profiling on British citizens dissenting against policies such as mandatory vaccination and lockdowns, then leverage the data to establish a YouTube channel that portrays these critics as dangerous “superspreaders” of “disinformation.”
Designed “to curb the influence of pseudoscience material online, with specific emphasis on Coronavirus-related ‘anti-vaxxing’ sentiment,” the operation is run by the UK’s Royal Institution, and dubbed “Challenging Pseudoscience.”
Its top patron is Charles, the Prince of Wales, next in line to the British throne, who recently hit out at supposed “conspiracy theories” surrounding COVID-19 vaccines. The organization received a substantial cash injection in 2020 from the UK government’s Culture Recovery Fund earmarked for video production.
Leaked files obtained by The Grayzone indicate that the Royal Institution has enlisted the services of Valent Projects, a “social change” communications firm founded by a public relations operative previously involved in the UK Foreign Office’s campaign for violent regime change in Syria. Valent has also been sponsored by the US Agency for International Development (USAID), a US intelligence cut-out, for a project aimed at “investigating disinformation.”
Valent’s central role in the operation highlights the trend of information warfare specialists bringing the techniques they honed against targets like the Syrian government back home to the West, where increasingly unpopular governments confront masses of citizens ever-bristling at coronavirus restrictions.
As in Syria, where communications firms like Valent created, trained and instrumentalized media organizations to further regime change objectives, they have covertly recruited a famed British YouTube influencer to lend their carefully calculated messaging campaign an authentic flavor.
According to internal documents, Valent plans to design a “mass appeal social media campaign fronted and owned by prominent social media figure Abigail Thorn,” the founder of Philosophy Tube. Valent’s research on British citizens who reject official policy on COVID-19 “will be used to devise a campaign that utilises YouTuber Abigail Thorn’s existing platform to achieve a measurable cognitive shift in the target audience,” the files state.

Boasting over one million subscribers to her YouTube channel and more than 7000 Patreon supporters, Thorn has established a potent vehicle for any communications campaign. She is also a core member of BreadTube, an assortment of left-branded social media influencers that has attracted intense establishment interest for its purported ability “to pop YouTube’s political bubbles to create space for deradicalisation.”
While top BreadTubers are best known for employing memes and theatrical ploys to counter right-wing narratives, they have also dedicated intense energy to attacking the anti-imperialist left as “tankies” engaged in a secret “red-brown alliance” with right-wing extremists.
In his book, “BreadTube Serves Imperialism: Examining the New Brand of Internet Pseudo-Socialism,” socialist organizer Caleb Maupin likened BreadTube to the “counter-gangs” deployed by British and US intelligence to infiltrate and dismantle insurgent forces from Kenya to Southeast Asia.
BreadTube “speaks in the name of left-wing sounding ideals. In reality, it is likely serving one section of the American ruling elite and the intelligence agencies,” Maupin wrote.
The covert relationship between BreadTube’s Abigail Thorn, Valent Projects, and the Royal Institute appears to validate Maupin’s thesis.
“It does not surprise me at all to find out there is documented evidence that the British Royal Family and an intelligence contractor is bankrolling the work of Abigail Thorn,” Maupin told The Grayzone. “It lines up with everything I have observed about her and the BreadTube trend overall.”
Maupin continued, “BreadTube’s ‘socialism’ is not really socialism, it is mobilizing young liberals to keep dissident elements in line. It’s securing the rule of British and American corporations over the planet by trying to silence those who get in its way.”
The national security establishment’s favorite socialists
Since launching Philosophy Tube in 2013, Abigail Thorn’s YouTube channel boasts over 7000 paying Patreon fans and well over one million YouTube subscribers. By probing complex philosophical and political issues in a highly accessible, engaging manner and deploying elaborate, artisanal audio and visual effects, she has emerged as a social media celebrity. A lengthy profile video produced by the BBC refers to her as “one of the most high-profile transgender figures in the UK.”
Thorn is among the most prominent figures within the loosely knit collective of YouTube influencers known as BreadTube. Inspired by the title of anarchist Peter Kropotkin’s tract, The Conquest of Bread, BreadTube advances a hyper-identitarian, imperialism-friendly interpretation of socialist politics that has earned its creators enthusiastic promotion from establishment interests.
The New York Times, for example, published a lengthy 2019 profile of a young man named Caleb Cain who supposedly “fell down the alt-right rabbit hole” on YouTube. Cain claimed he was de-radicalized through exposure to videos by Thorn and other popular BreadTubers like Natalie Wynn of Contrapoints. During the Trump era, as the Google-owned YouTube implemented a raft of stringent speech codes, it began amplifying BreadTube influencers through its algorithm.
Other popular BreadTube figures include Vaush, a video gamer from Beverly Hills, California named Ian Koshinski. Known for his superficial understanding of Marxism, crude invective against Trump supporters (“they disappear, or we all do”), female high school athletes who complain about being forced to compete against biological males (“sorry you fucking suck, dumb bitch”), and imprisoned journalist Julian Assange (“I want Assange to die in a CIA black site just because it would trigger all the worst people on Twitter”), the self-described “libertarian socialist” has earned the moniker “Vaush Limbaugh” from his critics.
Then there is Shaun, a British BreadTuber whose recent attack on left-wing political comedian Jimmy Dore’s criticisms of government Covid restrictions contained echoes of the “Challenging Pseudoscience” project prepared for Thorn by intelligence-related outfits. Shaun’s arguments relied heavily on statements by official experts and US government bodies like the FDA and CDC. While Dore has been limited by YouTube’s sweeping speech codes, Shaun’s viral video appears to have benefited from an algorithmic boost.
“All the key signs of infiltration are there,” Caleb Maupin said of BreadTube. “Since when does US mainstream media highlight the work of Marxist revolutionaries? Why are people who seem so unfamiliar with basic elements of socialist ideology suddenly elevated to the position of respected experts by the algorithms? Why do their foreign policy views seem to line up so closely with the US State Department? I have had no doubt they were being covertly supported by powerful entities with goals other than overthrowing capitalism.”
Unlike some fellow BreadTubers, Thorn comes across as amiable and trustworthy, fostering a personal bond with her viewers and regularly publishing thank you notes to patrons, listing them each by name. These qualities have attracted support for Philosophy Tube by both public and private backers.
Thorn’s April 2021 dismantling of the politics of right-wing culture warrior Jordan Peterson has racked up almost two million views and was sponsored by Curiosity Stream, a US media streaming service. The video opens with a black screen disclosing the support provided by the company and claiming Thorn would donate her fee to the feminist campaign group, Sisters Uncut. The video is also emblazoned with YouTube’s “paid promotion” logo.
Yet no such disclaimer referring to support from the Royal Institution can be found on any of her other uploads. And that may be because the Covid campaign was intended to be covert.
Astroturf campaign seeks to achieve ‘measurable cognitive shift’
The “Challenging Pseudoscience” operation designed for Thorn was launched in February 2021 by liberal science journalist Angela Saini. The author of several popular titles and a forthcoming book on “the origins of patriarchy,” she is also part of The Lancet Covid-19 Commission’s Task Force on Global Health Diplomacy.
The commission’s chief, Peter Daszak, a zoologist who serves as president of the US-based NGO known as EcoHealth Alliance, was forced to resign in June over conflict of interest issues.
In the years leading up to the outbreak of Covid-19, Daszak worked extensively on bat coronaviruses and gain of function research at the Wuhan Institute of Virology. His organization received tens of millions in funding from the Pentagon’s Defense Threat Reduction Agency, a division “[countering] weapons of mass destruction and improvised threat networks.” In December 2019, Daszak warned that coronaviruses can “get into human cells,” one can “manipulate them in the lab pretty easily,” and “you can’t vaccinate against them.”
The host of Saini’s project, the Royal Institute, was founded in 1799 by British scientists of the day “with the aim of introducing new technologies and teaching science to the general public.” Landed gentry and royalty have always occupied the Institution’s highest levels. Queen Elizabeth II’s cousin, Field Marshal Prince Edward, the Duke of Kent, has served as president since 1976.
The files indicate that the Royal Institution enlisted the services of Valent Projects, a communications firm “[working] with clients in the UK and all over the world to counter disinformation and strengthen the bonds between people.”
Valent was founded by Amil Khan, a former Reuters and BBC reporter who officially left journalism “to help good causes navigate the new information landscape.”
From February, Valent Projects proposed a “two-phase” project to “develop an understanding of the psychological drivers behind the generation and spread of anti-vaxxer narratives.” It planned to exploit this data “to develop and test public messaging responses.”
The findings would “inform other programming by Challenging Pseudoscience… as well as other stakeholders including the science community and concerned governments and public health bodies.”
In the campaign’s first phase, extensive online interviews were to be conducted, along with “ethnographic research” to secure “comprehensive understanding of the key online audiences driving anti-vaxxing mis/disinformation around the Coronavirus pandemic.”

Valent Projects then planned to “draw together insights” from these findings, developing “comprehensive audience profiles” – including “demographic information” – to design a “mass appeal social media campaign fronted and owned by prominent social media figure Abigail Thorn,” who runs online channel Philosophy Tube.
Valent indicated its intent to exploit Philosophy Tube’s sizable platform to “achieve a measurable cognitive shift [emphasis added] in the target audience.”
Reaching the intended viewers was forecast to be a significant task in itself, however. Valent noted most Philosophy Tube viewers are within the 18 to 35 age range, but “existing research” suggested the “most prolific consumers of pseudoscience material” were over the age of 45.
The firm felt the “best topic to address this issue is probably along the lines of ‘the thing about expertise’ [sic].” Fittingly, in August 2020 Thorn uploaded a video, “Who’s afraid of the experts?” Featuring comedian Adam Conover of the popular show, “Adam Ruins Everything,” the 45 minute-long defense of the scientific consensus on the HIV/AIDS debate is the first result in any search for the term “vaccine” on Philosophy Tube’s channel.
The leaked documents thus expose what had long been suspected by critics of BreadTube: the popular social media collective has been instrumentalized by powerful interests with connections to Western intelligence agencies.
An astroturfed information warfare campaign hiding in plain sight
Multiple requests for comment from The Grayzone to Abigail Thorn’s agent and Angela Saini have gone unanswered.
When quizzed about the leaked files on Twitter, Valent Projects CEO Amil Khan flew into a rage, angrily asserting they were “obtained through hacking and then doctored,” in the manner of “classic doxing,” and threatened legal action against this journalist for publicizing them.
Khan later pumped out a series of tweets aimed at controlling the damage of his imminent exposure. In one, he falsely claimed that a co-author of this piece would publish their reporting in “Russian state affiliated media.”
Yet when challenged about his claim of doctoring, Khan did not respond.
Subsequent requests for clarity on which elements of the documents were maliciously altered and how that might have taken place have also gone unanswered. But evidence of the secret project’s existence was hiding in plain sight.
For example, Valent Projects lists the Royal Institution on its website as a client. An accompanying writeup notes it “developed and implemented a data-led behaviour change campaign [emphasis added] aimed at understanding and working with the psychological drivers behind anti-vaxer sentiment in the UK” for the organization.
Similarly, a post on the company’s official LinkedIn page refers to an “analysis of tens of thousands of UK-based social media users “posting/sharing anti-vax content online” it conducted for Countering Pseudoscience, which would “be used to inform ethnographic research designed to understand ‘why’ people hold these views.” In other words, a specific programming strand outlined in the documents.

From Valent Projects’ LinkedIn page
Moreover, none other than Abigail Thorn was guest-of-honor at Challenging Pseudoscience’s launch event in February, “Vaccines: Warriors and Worriers,” which featured a debate on “how vaccines work, why people are skeptical despite the evidence, and how disinformation about vaccines spreads online.”

Abigail Thorn of Philosophy Tube participating in the Royal Institution’s “Vaccines: Warriors and Worriers” event
Also on the event’s panel were an immunologist named Zania Stamataki and Marianna Spring, the BBC’s first “specialist disinformation reporter.” She has repeatedly perpetuated falsehoods about the size of anti-lockdown protests in 2020 and nature of their participants. In a bizarre experiment, she furthermore personally set up numerous “fake troll” accounts on assorted online platforms that “engaged” with “misogynistic” content, allegedly for academic purposes.
In May, Thorn published a characteristically ornate video, “Ignorance & Censorship,” which touched on the topic of “disinformation” and vaccines. The next month, Challenging Pseudoscience convened a similarly named panel discussion, “Misinformation or Censorship.”
Then, the newly-launched Challenging Pseudoscience podcast shared two prior Royal Institution debates – the aforementioned Vaccines: Warriors and worriers, and “Disinformation and how to counter it,” which featured none other than Amil Khan as a speaker. It would be entirely unsurprising if this deluge was a coordinated effort.
A wide-ranging, long-running, cross-platform propaganda campaign involving multiple actors requires substantial resources. Until 2020, however, the Royal Institution struggled financially despite its royal patronage and elite trustees.
The organization has been forced to rent out its grand central London headquarters for conferences, corporate bashes and weddings. To plug a multimillion pound budget deficit in late 2015, the Royal Institution auctioned off treasured first editions of works by Charles Darwin, Isaac Newton and other eminent scientists. The fire sale prompted the BBC to ask whether the organization was on the verge of collapse.
Miraculously though, in October 2020, the Institution received hundreds of thousands of pounds from the UK government’s £1.57 billion Culture Recovery Fund “to help face the challenges of the coronavirus pandemic and ensure it has a sustainable future.”
An accompanying press release noted the Royal Institution had over the course of the pandemic “[developed] a successful programme of weekly science talks online” broadcast via its “well-established” YouTube channel, which today boasts 1.11 million subscribers. The cash injection would “increase the number of livestreamed science talks” hosted by the organization, and help it develop “new digital content.”
Valent Projects staffer Hamish Falconer has disclosed that the “exciting” Challenging Pseudoscience campaign has also received “generous support” from the Open Society Foundations of CIA-adjacent billionaire George Soros.
As the Washington Post’s David Ignatius reported in 1991, Soros was at the heart of a network of “overt operators” helping US intelligence carry out “spyless coups” against former Soviet satellite states.
In July 2021, Soros teamed up with fellow billionaire Bill Gates to purchase a UK-based Covid-19 test developer for $41 million.
Three months later, as Alex Rubinstein documented for The Grayzone, Soros partnered with tech oligarch Reid Hoffmann to found Good Information Inc, a social media censorship operation marketed under the aegis of “countering disinformation.”
Hamish is the son of Charlie Falconer, a longtime friend and former roommate of former UK Prime Minister Tony Blair. Following Blair’s May 1997 election victory, Falconer senior was elevated to the unelected House of Lords, and served in a series of high-ranking government posts throughout his pal’s tenure.
Along the way, he applied “huge pressure” to Attorney General Lord Goldsmith to change his view that invading Iraq would be illegal. His intervention may have played a decisive role in greenlighting the war of aggression.

Valent founder “embedded into terrorist organizations,” ran Syria psy-ops for armed extremists
Hamish Falconer’s hiring at Valent Projects in March 2021 highlights the firm’s deep ties to the UK’s intelligence apparatus. At the time, he was ostensibly on leave from the UK Foreign Office.
Khan trumpeted Falconer’s hire on LinkedIn, declaring that “he brings the action end to our work – experimenting and innovating with digital influence for good.” Having met in Pakistan “over a decade ago,” the pair “have not stopped talking and comparing notes since.”
Falconer’s spartan online résumé sheds little light on his professional history, noting only a spell at the UK government’s Department for International Development, followed by a seven-month gap, before he joined the Foreign Office as a ‘Diplomat’ until August 2020.
No detail is offered either on where Falconer has been posted, or what his role entailed at any point. He is a graduate of Yale University’s Maurice R. Greenberg World Fellows Program, named for the AIG founder who nearly became CIA director. The Greenberg fellows program identifies and grooms prospective future influencers, including no shortage of US-backed would-be coup leaders. Among the most famous alumni of the program is jailed Russian opposition figure Alexey Navalny.
The Greenberg program’s profile of Falconer states, “he has led the Foreign Office’s Terrorism Response Team, UK efforts to start a peace process in Afghanistan and served in Pakistan and South Sudan,” and served a stint at the National Crime Agency – London’s equivalent of the FBI.
Counter-terror is not a stated Foreign Office purview, but just one of “three core areas of focus” for the UK foreign intelligence service MI6. It may just be a coincidence the agency’s spies typically pose as ‘diplomats’ overseas.
By contrast, Khan’s activities between December 2008, when he left his position as ‘hostile environments reporter’ for the BBC, and October 2017, when he joined elite UK national security think tank Chatham House as an ‘associate fellow’ – the next entry on his public CV – can be pieced together with much greater certitude, but still only approximately.

Valent Projects founder Amil Khan
A leaked document indicates that he first crossed paths with Falconer while managing a ‘countering violent extremism’ propaganda campaign for the UK government in Islamabad. The file relates to a Foreign Office funded effort to train “articulate Syrian armed and civilian grassroots opposition entities,” and promote them to “Syrian and international audiences” as a credible alternative to the government of Bashar al-Assad.
The project was delivered by ARK, a shadowy intelligence contractor founded by the likely MI6 operative, Alistair Harris, which has raked in innumerable lucrative contracts from waging covert information warfare operations on behalf of the UK government.
Khan was heavily involved in ARK’s Syrian efforts. Another leaked file, outlining some of the company’s work inside Syria shows that it oversaw a “rebranding” of the CIA-armed Free Syrian Army to portray it as a moderate, secular force unconnected to the hardcore jihadist factions that dominated the armed opposition. Khan is named as one of three operatives managing the media office of the parallel Syrian National Coalition government controlled by London through intelligence cutouts like ARK.

This work placed Khan in extremely close quarters with members of violent ‘rebel’ factions implicated in hideous crimes against humanity. That he “[provided] political and media support to opposition political and military groups” in Syria has been openly confirmed. A scathing internal Whitehall review of the Foreign Office’s information warfare operations in the country concluded they were “poorly planned, probably illegal, and cost lives.”
It wasn’t the first time Khan been in such murderous company. At some point after leaving ARK in August 2014, he joined InCoStrat, another contractor that conducted destabilizing psy-ops on the UK government’s behalf throughout the Syrian crisis. InCoStrat delivered “strategic communications support” to a variety of armed groups on-the-ground, including the notoriously brutal, Saudi-backed militia known as Jaysh al-Islam.
Khan also played a central role in this dubious initiative. In a document discussing its ability to “[develop] contacts in Arabic-speaking conflict affected states,” InCoStrat bragged how, “in his previous career as a journalist,” Khan “established relationships with, and embedded himself into terrorist organizations in the UK and the Middle East,” gaining “unique insight into their narratives, communication methods, recruitment processes and management of networks” as a result.

InCoStrat was founded by ex-Foreign Office political officer Emma Winberg and UK military intelligence journeyman Paul Tilley, a former director of Strategic Communications for the UK Ministry of Defence in the Middle East and North Africa. Winberg left to join Mayday Rescue, parent ‘charity’ of the fraudulent humanitarian group known as the White Helmets. She later married its founder, James Le Mesurier, who died in mysterious circumstances in 2019 after damaging revelations of financial corruption came to light.
A broad landscape of state-backed Covid propaganda ops
It’s probable the “Countering Pseudoscience” project is just one part of a wider landscape of online astroturf initiatives designed to restore cratering public trust in authorities around Covid policy.
Valent Projects has also conducted work for the Institute for Strategic Dialogue, a neoconservative think tank, researching “violent actors using the ‘dark web’ to mobilise recruits and threaten public figures in Europe.” This initiative was likely also aimed at countering lockdown opposition.
Back in April 2020, Khan appeared on a panel discussion convened by the organization, “Countering Disinformation in a Time of COVID19.”
At the start of December, the Institute released a brief report, “Between conspiracy and extremism: A long COVID threat?”, which attempted to frame the “radicalization” of anti-lockdown protesters as a terrorist threat. What input Khan may have had in this publication was unclear.
Valent Projects is just one of an array of companies that have brought psy-ops techniques honed in Syria and other theaters of Western information warfare back home with them, like soldiers returning from battlefields marketing their deadly skills to private security and intelligence firms. And Abigail Thorn is just one YouTuber, at a time when the British state is known to be maliciously recruiting digital personalities to further its interests across the globe.
For example, Foreign Office contractor Zinc Network maintains a clandestine nexus of Russian-speaking social media influencers throughout the former Soviet Union, to promote “media integrity, democratic values [and] complex social issues,” a campaign so intensive its relationship with these individuals necessitates “daily management.” This squadron of undercover psy-ops warriors are supported by an expert “in-house team of Russian speaking producers, researchers and digital growth strategists” in London, helping them create, edit and promote their output.
Coincidentally, Zinc has been engaged in efforts since the onset of the pandemic to concoct a link between extremist activities and anti-lockdown, vaccine hesitant views. It has also published research on how to best market a test-and-trace app to UK citizens, “as part of a broader research project on public understanding of and support for Artificial Intelligence.”
It is simply inconceivable that similar operations have not been enacted elsewhere in the world, or that this phenomenon is exclusive to the UK. Further, it is impossible to know if the next slick viral video countering grassroots dissent of an official narrative is state or quasi-state propaganda, cleverly crafted to induce a “cognitive shift” in viewers, in which the star of the online show is effectively an intelligence asset rattling off a script drawn up by full-time spooks.
The Beginning of the End? The virus part of the pandemic will probably soon be over.
eugyppius | December 26, 2021
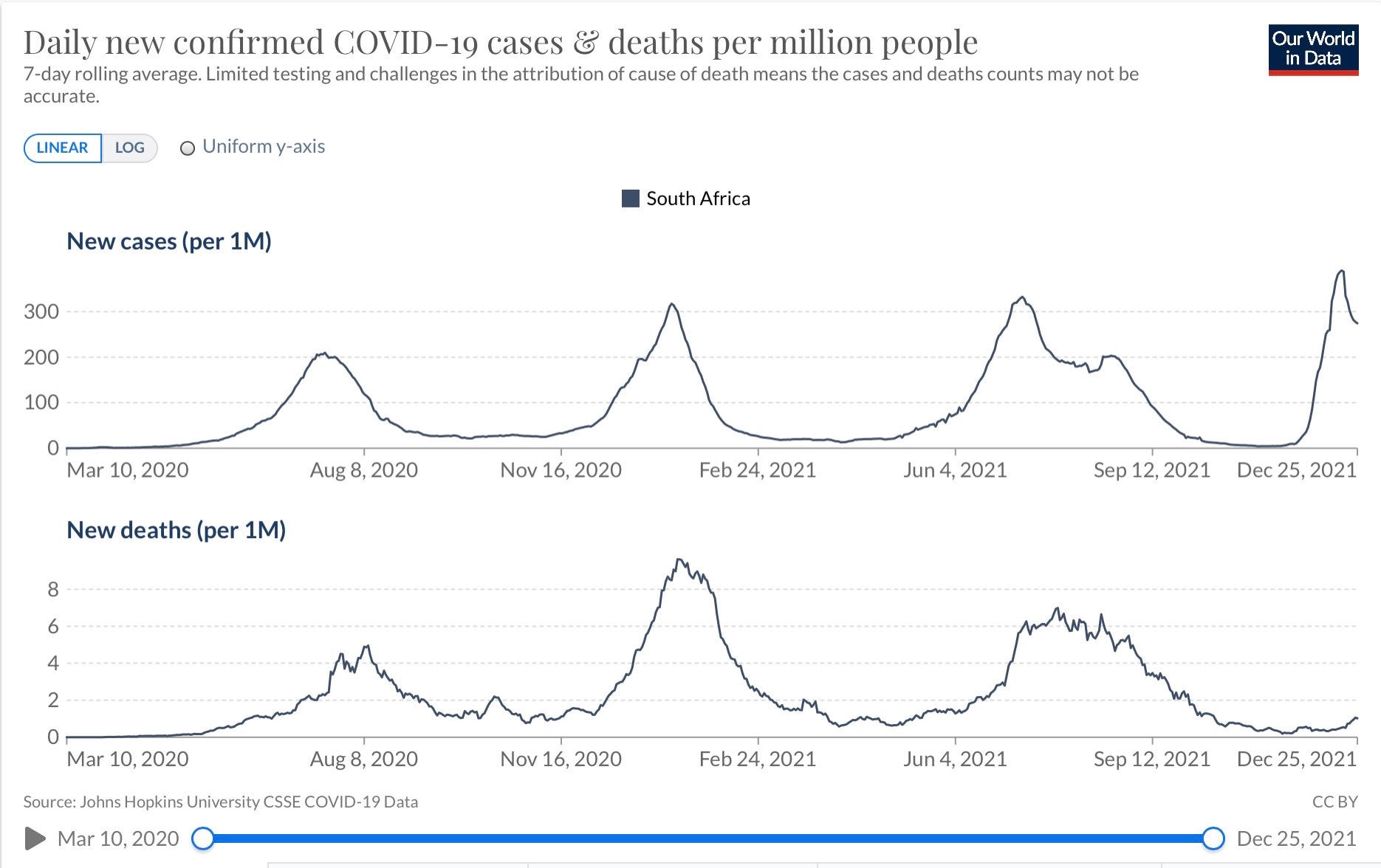
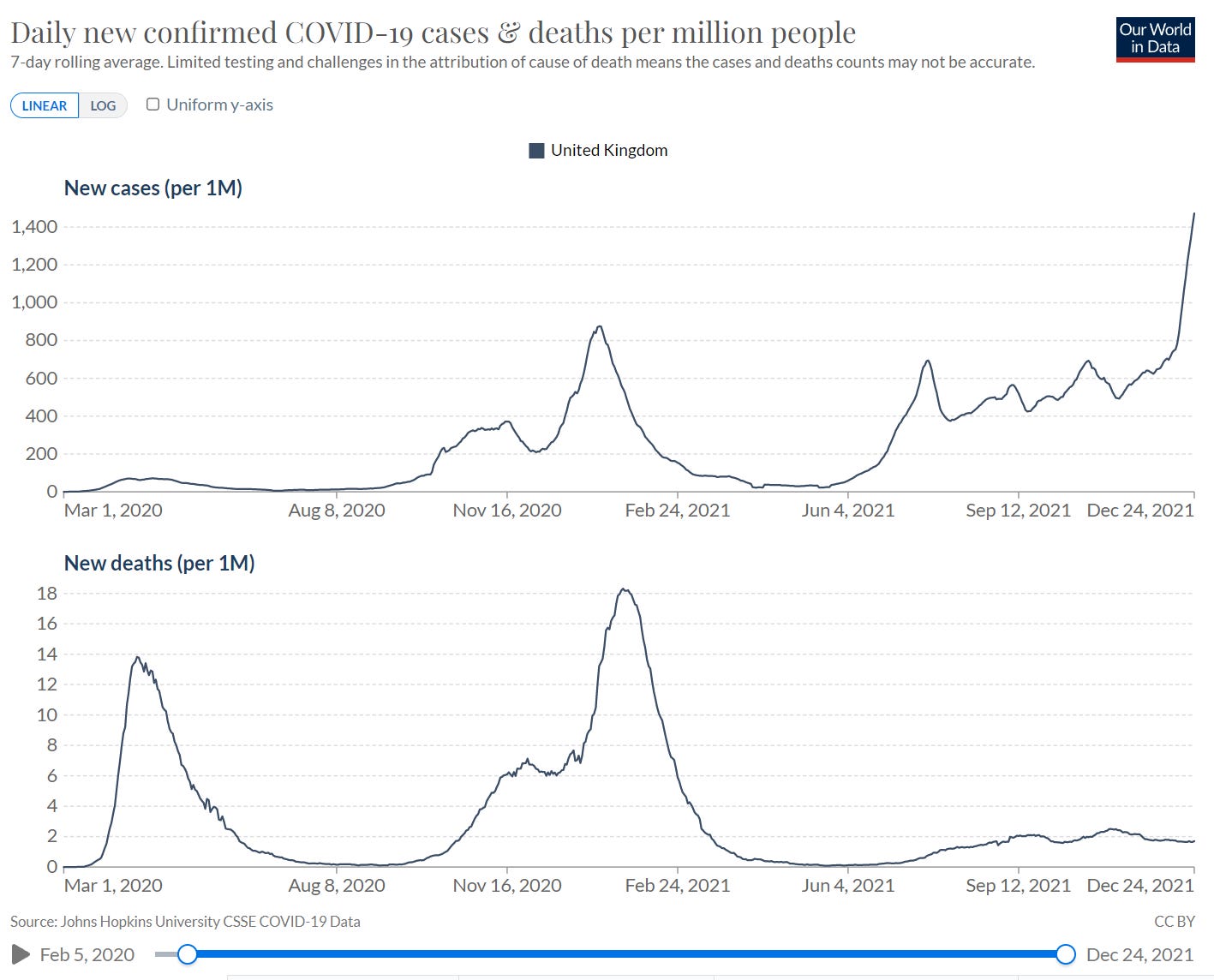
Early reports that Omicron is substantially milder than other SARS-2 strains are every day confirmed by new data. A month into the unprecedented South African case spike, driven entirely by Omicron, Corona deaths remain low. It’s earlier days in the United Kingdom, where Omicron is only just over half of cases. So far, though, it is the same story there:
In the coming months, Omicron will outcompete all other lineages everywhere in the world. At that point, Corona will have completed its transformation into a mild coronavirus that nobody should care about, in the same way that nobody cares about other common human-infecting coronaviruses like hCoV-OC43. Unforeseen developments are always possible; Omicron might in time acquire greater pathogenicity. Particularly if we insist on vaccinating widely, we might drive its evolution in new and potentially dangerous directions. Those are, however, mere possibilities. Right now, everything tells us that the virus part of the pandemic will soon be over.
The major question, is how the rest of the Corona Circus will respond. Some thoughts on that:
In the short term, rising cases will probably fuel demand for more vaccinations. This is the blunt, stupid way that our public health experts respond to infections now, but it is not a game that will go well for the vaccinators. The vaccines will fail even more profoundly in stopping Omicron transmission, and there will be far fewer severe outcomes for them to prevent. I don’t know how long the crackpot vaccination regime can survive overt absurdities like this.
Omicron will probably also unwind the broader containment regime. South Africa has already abandoned their most intrusive tracing, quarantine and isolation policies, declaring a shift towards mitigation (which is what they should have done in the first place). Trying to defeat a minimally symptomatic highly contagious virus with the comically inadequate tools of the contact tracer is simply too ridiculous.

In the longer term, things look much more uncertain. It is hard to shake the feeling that Corona has swept away the last vestiges of liberal democracy in Europe, and perhaps in the whole world. I don’t think these political systems have been very good for the West, but our new theocratic regimes steered by the Corona astrologers have been vastly worse. As soon as the hysteria boils off, many of these villains will begin trying to get the panic machine up and running again. The alternative is a future where nobody much cares what they have to think, where they’re no longer able to interfere in millions of lives, and – perhaps most crucially – where a lot of politicians, journalists, and ordinary people begin to realise what utter failures they and their policies have been. There are failures that lose you your job, there are failures that make you a public disgrace, and then there are their failures, the kind that lead to arrest, indictment, imprisonment, and worse.
COVID Jabs: Ineffective, Oppressive and Dangerous
By Iain Davis | OffGuardian | December 23, 2021
There is no moral, legal or logical argument for mandatory vaccination. The only logical argument, from a public health perspective, would be either to reduce the spread of infection or reduce the impact on health services via some other mechanism.
We will explore the evidence which shows that the COVID-19 supposed “vaccines” are incapable of achieving either.
That didn’t stop the UK parliament voting to allow the government to mandate vaccination for NHS staff. In doing so, they laid the path clear for a wider, national mandate.
Prior to the vote, the British Medical Journal published the protestation of concerned medical professionals who highlighted that there is insufficient evidence to support a mandate.
UK MPs apparently decided that the doctors and nurses didn’t know what they were talking about and were not interested in the scientific evidence they cited. While this illustrates that decision making is not led by science, perhaps this is not the primary concern.
Whatever the political or popular opinion may be, to insist that an individual must submit to injection against their will is to deny them their inalienable right of bodily integrity.
This right was described by Professor David Feldman in Civil Liberties and Human Rights In England and Wales:
A right to be free from physical interference. [This] covers negative liberties: freedom from physical assaults, torture, medical or other experimentation, immunization and compelled eugenic or social sterilization, and cruel or degrading treatment or punishment. It also encompasses some positive duties on the state to protect people against inference by others.”
Both the European Convention on Human Rights (Article 3) and the Universal Declaration of Human Rights (Articles 1 & 3) allegedly guarantee the integrity of the person.
However, these are “Human Rights” written on pieces of paper by politicians and lawyers. As such, they can be overruled by governments and other politicians and lawyers. Human Rights are not rights, they are government permits and permits can be rescinded.
More importantly, in the UK, there is a clear legal precedent for the concept of bodily integrity. In Montgomery vs Lanarkshire Health Board the Supreme Court ruled:
An adult person of sound mind is entitled to decide which, if any, of the available forms of treatment to undergo, and her consent must be obtained before treatment interfering with her bodily integrity is undertaken.”
If society decrees that the population no longer has a right to bodily integrity then the people become the slaves of that society. A society that advocates mandatory vaccinations equally advocates slavery. Those who advocate mandatory vaccination support slavery in principle. None of the justifications they offer negate this fact.
The legal definition of ownership is the “exclusive legal right to possession.” A vaccination mandate decrees that the individual no longer has legal possession of their own body. It removes the individual’s legal right to ownership of their physical being and hands it over to the state. This constitutes slavery.
Slavery is defined as:
The condition of being legally owned by someone else and forced to work for or obey them”
There are those who suggest that the “common good” warrants slavery. They state, based upon assumption and ignorance, that when a person refuses COVID-19 vaccination they are putting others at risk and behaving in a way that jeopardises the common good.
They maintain that society should have the right to violate the bodily integrity of its slaves.
As pointed out by many, a mandate differs from law. However, a government mandate is something the state uses to claim the non-existent right to force people to obey. Individuals can be punished–fined or even imprisoned–for failing to abide with a state mandate. The right to bodily integrity is denied by mandate and all citizens are made slaves by virtue of it.
Some anti-rationalists have argued that a mandate does not constitute “force.” This is a ridiculous contention.
Threatening to fine people is coercion and warning of potential imprisonment is the threat of violence. This is the literal definition of the use of force:
Coercion or compulsion, especially with the use or threat of violence.”
Where violence is defined as:
Extremely forceful actions that are intended to hurt people or are likely to cause damage”
Those who believe in the concept of the common good, debating the point at which it overrides individual sovereignty, accept that some group they choose to empower has the right to force others to obey.
Regardless of whatever rationale they claim, by ultimately insisting that no citizen has the right to bodily integrity, they promote slavery, including their own.
Some people are a bit squeamish about admitting their support for slavery and prefer to pretend that forcing compliance through other means is not slavery.
The head of Ryan Air, Michael O’Leary, apparently thinks that denying people access to society, employment, food and medical treatment is not a “mandate” and therefore forcing them to take the vaccine through this mechanism doesn’t amount to slavery.
O’Leary’s suggestion is that those who decline the vaccine should be punished for their disobedience. He thinks that threatening people with poverty, starvation and a shorter life expectancy is perfectly acceptable in order to force them do as he wishes. He believes that, if this isn’t officially mandated, doing so will somehow protect their rights:
[A mandate] is an infringement of your civil liberties. But you simply make life so difficult. Or [make it that] there are lots of things that you can’t do unless you get vaccinated”
Proponents of the “common good,” who insist that getting vaccinated is the “right thing” and therefore not complying is wrong, cannot both proclaim society’s alleged authority to ignore the inalienable right of bodily integrity and simultaneously pretend they oppose slavery.
If, as a society, we allow the government to mandate or if, like O’Leary, we choose to enforce vaccination by other means, then we have collectively consented to live in a slave state where we are all slaves.
If we go down this path we condemn future generations to slavery. Yet somehow those who decline the offer of slavery, who oppose it in principle, are considered to be selfish by wider society.
The supporters of slavery justify this to themselves because they believe the extremely limited public health impact of a low mortality respiratory disease is more important than human freedom.
This opinion is informed by the flawed and irrelevant assumption that the jabs protect others. The efficacy and safety of the vaccines is immaterial. To deny an individual’s right to bodily integrity is slavery. It does not matter what the claimed justification is.
There are already many slaves being traded, exploited and abused in the UK. While the experience of those who suffer the daily hell of modern slavery is in no way comparable to merely being forcibly injected with a drug once or twice a year, the principle of slavery is the same. It seems odd that the suggested “common good” doesn’t demand freedom for those currently living as slaves. Perhaps society no longer cares.
Putting aside the lack of moral and legal legitimacy, there are other reasons why we should reject any notion of a vaccine mandate. Primarily that the so-called vaccines don’t work and are dangerous.
THE JAB BASICS
The word “infection” is defined as:
“The state produced by the establishment of one or more pathogenic agents (such as a bacteria, protozoans, or viruses).”
If you had looked at the medical definition of “vaccine” in 2019 you would have understood a vaccine to be:
A preparation of killed microorganisms, living attenuated organisms, or living fully virulent organisms that is administered to produce or artificially increase immunity to a particular disease”
Where immunity was defined as:
The quality or state of being immune; especially: a condition of being able to resist a particular disease especially through preventing development of a pathogenic microorganism or by counteracting the effects of its products.”
A vaccine was a drug that “especially” reduced infection. It could theoretically stop a pathogenic agent, such as a bacteria, protozoans, or virus from establishing itself in a biological system. Thus reducing the incidents of disease and subsequent transmission of the pathogen.
However, in the wake of the pseudopandemic, that is not what the changed definition of “vaccine” has come to mean today. The only thing an alleged, so-called vaccine is required to demonstrate is immunogenicity:
A preparation that is administered (as by injection) to stimulate the body’s immune response against a specific infectious agent or disease”
Purely by changing the definition, a “vaccine” is now a drug that stimulates an immune response. It says nothing about how effective or safe that immune response is. Inflammation is an immune response and it is potentially lethal.
Absent the ability to protect against infection, most people would consider a drug which only reduces the severity of disease to be a treatment, not a vaccine.
While it is true that language constantly evolves and definitions change all the time, where that change fundamentally redefines the commonly accepted meaning of a word, everyone needs to be aware of the new interpretation. If not, they could accept an implied meaning that no longer exists.
For example, people could easily be fooled into believing a COVID-19 “vaccine” stops infection. To draw a distinction between what most people imagine “vaccine” to mean and what it now means, we will refer to the alleged COVID-19 “vaccines” as jabs.
THE JABS HAVE NOT COMPLETED & DO NOT NEED TO COMPLETE ANY CLINICAL TRIALS
Unlike every vaccine that preceded them, the jabs have not completed clinical trials prior to being given to more people than any other vaccine in history.
At the time of writing there are no results posted for the NCT04614948 trial of the Pfizer-BioNTech mRNA jab; none for the NCT04516746 Astrazeneca jab; there are no results from Moderna’s NCT04470427 trial nor any from J&J’s NCT04368728 trial of their Jansen jab.
When the UK medicines regulators, the MHRA, said that they “carried out a rigorous scientific assessment of all the available evidence of quality, safety and effectiveness,” prior to allowing the jabs’ Emergency Use Authorisation (EUA,) they did not mean they had studied the results of any clinical trials. They couldn’t, because there aren’t any.
What they meant is that they had received interim reports from the manufacturers and their sponsors (UK Research and Innovation, National Institutes for Health Research (NIHR), Coalition for Epidemic Preparedness Innovations (CEPI), Bill & Melinda Gates Foundation, Lemann Foundation etc.) The MHRA, as other regulators around the world, based their decision to grant the EUAs on these interim reports, not upon the results of any clinical trials.
This enables the mainstream media to report news agency statements which mislead the public:
Massive coronavirus vaccine trials involving tens of thousands of participants have so far surfaced no signs of serious side effects.”
The continual impression given is that the jabs are clinically proven to be safe and effective. In reality, few adverse reactions have been reported in the trials because no trial results have been posted.

The trials were designed to be blind Randomised Control Trials (RCTs.) As they were trialling the first proposed vaccines for a novel disease, the standard RCT approach to determine the safety and efficacy of the jabs was to compare the long term health outcomes of jab recipients to those of a placebo group. These would be “blinded,” meaning that the trial participants were not told if they had been jabbed or received a placebo.
The secondary outcomes for the trials were designed to assess the effects of the vaccines. This including assessment of any adverse drug reactions (ADRs) for up to 2 or more years after the final dose. So far, none of the secondary outcomes have been measured because we are more than a year away from the end of the minimum trial periods.
There is now no chance that these clinical trials will ever reveal any meaningful results. As reported in the British Medical Journal both J&J and Moderna have “unblinded” their trials by giving their jab to their placebo groups. They have abandoned the secondary outcomes, years before the trials are complete. When asked, neither Astrazeneca nor Pfizer-BioNTech denied doing the same.
In any event, it appears their trials were poorly designed and lacked scientific credibility. It is strongly alleged that Pfizer-BioNTech, at least, falsified data, unblinded their study, failed to adequately train staff and were reluctant to follow up on reported adverse events.
When independent researchers used a Freedom of Information request (FoIR) to ask UK regulator, The Medicines and Healthcare products Regulatory Agency (MHRA), why the Pfizer-BioNTech NCT04614948 clinical trial hadn’t assessed the vaccine’s impact upon pregnant women, the MHRA stated:
The above trial was not conducted in the UK, the MHRA did not assess its content and are therefore not in a position to answer specific questions relating to it.”
Not bothering to consider the primary clinical trial doesn’t appear to be a very “rigorous scientific assessment.” Rather, it seems the MHRA are among a group of regulators who unquestioningly accepted whatever the manufacturers claim without genuinely scrutinising anything.
The MHRA have now formally adopted this laissez-faire approach to future jab regulation. Having aligned themselves with the Access Consortium of regulators (Australia, Canada, Singapore and Switzerland), the MHRA are among those who see no reason for any further regulatory scrutiny prior to the approval of new jabs.
The Consortium believe new iterations, responding to allegedly new variants of COVID-19, can effectively be waved through automatically. This is based upon the impossible.
The MHRA assert that their initial EUA reflected their appraisal of the “pivotal clinical trials,” for which there are no posted results. Having authorised the jab roll-outs without any substantiating evidence, the MHRA now claim that, for all tweaked future versions:
Clinical efficacy studies prior to approval are not required. Regulatory Authorities request bridging data on immunogenicity from a sufficient number of individuals”
This speeds up the process of getting jabs straight out of the corporate labs and into the arms of a broadly misinformed public. Whatever tweaks the manufacturers choose to make will just be rubber stamped by the Consortium as long as the pharmaceutical corporations submit the appropriate immunogenicity claims.
The issuance of an EUA is not the same as regulatory approval of a medicine. As explained by the U.S. regulator, the Food and Drug Administration (FDA,) an EUA is a temporary authorisation of an investigational medication:
An EUA for a COVID-19 vaccine may allow for rapid and widespread deployment for administration of the investigational vaccine to millions of individuals”
The FDA also state that an investigational drug, still in trials, is an experimental drug:
An investigational drug can also be called an experimental drug.”
The current COVID-19 jabs are still in trials and are “experimental drugs.” So-called fact checkers have been dispatched to mislead the public into believing this is not the case.
For example Full Fact, the UK based political activists who work with policy makers to market their own business, claimed:
The three Covid vaccines currently approved for use in the UK have already been shown to be safe and effective in clinical trials.”
This was a factually inaccurate statement. In terms of issuing EUAs, all that was known from the phase 3 trials was the interim results.
These reported what little data was available from the first two months of phase 1. This was merely a claim that the jabs were relatively safe for a small cohort of fit and healthy, predominantly younger people. We will shortly discuss why even this assertion is false.
All we can say at this juncture is that there is no perceptible regulation of the jabs. They are effectively unregulated.
The trials have yet to demonstrate that the jabs are either safe or effective. The exclusion criteria for all the trials ruled out trialling the jabs on those most vulnerable to COVID-19. The interim reports from phase 1 only claim efficacy and safety among those least susceptible to apparent COVID-19 risks. Now those trials will never be completed.
The interim trial reports claimed efficacy in terms or relative instead of absolute risk reduction. This enabled the manufacturers to claim a 95%+ reduction in mortality (efficacy.) This was then reported to the public who were swayed by this reporting bias.
The claimed absolute risk reduction (efficacy) was typically less than 1%. Had this been reported to the public the people would have been less enthusiastic and perhaps more sceptical about the jabs, which is why it wasn’t.
The EUAs, on both sides of the Atlantic, also came with immunity from prosecution for the manufacturers. In the UK, the Human Medicines (Coronavirus and Influenza) (Amendment) Regulations 2020 extended the liability protection offered to administering medical practitioners to the pharmaceutical corporations.
Immunity from prosecution is an apparent deal breaker for the drug companies. In early 2021 the managing director of the World Bank, David Malpass, reported that some jab manufacturers would not distribute their jabs to countries that did not fully indemnify them against prosecution:
The immediate problem is indemnification. Pfizer has been hesitant to go into some of the countries because of the liability problems, they don’t have a liability shield. So we work with the countries to try to do that.”
There is no doubt that the jabs are experimental drugs that have not completed any clinical trials. As such the population who have received them are part of a global medical experiment. In partnership with government, that experiment is being conducted by global pharmaceutical corporations which have no liability for any harm they may cause.
This fact is then covered up by the global media corporations and appointed fact checkers, who also work in partnership with government.
Statements from the NHS such as “The COVID-19 vaccines are the best way to protect yourself and others” or “any side effects are usually mild and should not last longer than a week” are not based upon any clinical trial evidence. They are speculative, misleading and potentially dangerous proclamations.
Unless, before being jabbed, recipients were explicitly made aware of these facts they cannot possibly have given informed consent.
In each and every instance, despite the fact free denials of the comically misnamed fact checkers, this constitutes a breech of the Nuremberg Code.
BLAMING THE UNJABBED
Following the comments of the health secretary, Sajid Javid, the MSM dutifully reported that there are around 5M “unvaccinated” people in the UK. This figure appears to be only partially accurate.
According to figures released by the UK Health Security Agency (UKHSA), by mid December 2021, with the booster roll-out well underway, of the approximate 44.6M adults in England, around 38.6M had received at least two doses and were therefore temporarily deemed to be “fully vaccinated.”
This means that currently about 6M adults in England alone are officially “unvaccinated.” England represents approximately 84% of the UK population. Assuming similar vaccine distribution figures for the whole of the UK, this suggests that at least 6.9M adults are officially unvaccinated. This represents nearly than 13% of the adult UK population.
The size of the unvaccinated population is set to grow. The UK government have already said that a booster will be needed for the NHS COVID Pass (certificate) for international travel.
Initially the UK government said that they didn’t intend to extend this to the domestic vaccine passport but they also repeatedly denied that they would introduce vaccine passports.
Subsequent comments from the Health Secretary clarified the government’s intention to continually shift their definition of “fully vaccinated.” To be fully vaccinated the slave must always agree to the next jab.
With the jab sales force insisting that boosters will be needed for years to come, it seems “fully vaccinated” status will last for about 6 month.
The MSM, on behalf of the government who fund them, have propagandised the nation into believing that it is the unvaccinated who are “overwhelming” health services. With headlines like ICU is Full Of The Unvaccinated – My Patience With Them Is Wearing Thin, it is no wonder that the jabbed majority are turning their hate towards the people who don’t want the jabs. It is extremely common to read social media comments such as:
Unvaccinated people are taking beds from other sick people, some of whom become sicker as a result. Not being vaccinated during a pandemic is an act of selfishness hiding behind the facade of individual liberty.”
The “ICU is Full” Guardian article was from an anonymous source. No one was willing to put their name to it. It was primarily an appeal to emotion and offered no evidence to back up any of its claims. This is because the evidence does not support any aspect of the published story. The only apparent reason for the article was to incite hatred.
Real journalists, like Kit Knightly from the OffGuardian, which is censored by the social media platforms, have been willing to put their name to the reporting of the facts.
As he shows, ICUs are not overwhelmed at all. They are quite busy, as usual, but they are certainly not overrun with COVID-19 “cases,” as the Guardian and others have deceptively claimed.
Currently there are 4330 critical care beds in England. On December 14th 2021, 925 were occupied by so-called COVID-19 patients, a COVID-19 ICU bed occupancy rate of 21.4%. There were 775 (17.9%) unoccupied ICU beds with 2657 beds (61.4%) taken by patients who had not tested positive for the selected COVID-19 nucleotide sequences.
In their Week 50 Vaccine Surveillance Report UKHSA state that, for the preceding 4 week period, 2965 alleged COVID-19 adult hospital patients had not received a jab and 4557 had received at least one. Therefore UKHSA claim that the un-jabbed represent 39.4% of total COVID-19 hospital admissions.
For the same 4 week period, UKHSA also reported that 715 of the 3083 total adult deaths, within 28 days of a positive test, were people who were not jabbed. This represents 23.2% of alleged COVID-19 deaths. With 28 deaths attributed to those with an unknown jab status, the remaining 2340 were jabbed. The jabbed represent 76% of all alleged COVID-19 deaths.
Similar data for Wales also belies the false claim that it is the unjabbed who are “overwhelming” health services. In November 2021 12.8% of hospital inpatients were “unvaccinated.” The “vaccinated” accounted for 84.5% of hospital inpatients with 2.7% of unknown jab status.
The anonymous claims reported in the Guardian weren’t even remotely accurate. The tale was a propagandist disinformation. It was “fake news.”
Yet the politicians are desperate to peddle the same lie, with the assistance of their compliant MSM. Once again, the Guardian reported the comments of the Health Secretary as if they were realistic. Speaking about the people who have considered the evidence and have decided not to take the jab, Javid said:
They must really think about the damage they are doing to society. They take up hospital beds that could have been used for someone with maybe a heart problem, or maybe someone who is waiting for elective surgery.”
At no point did the fearless journalists at the Guardian inform the public that what he was saying was total nonsense. Instead, they doubled-down on the lies with added disinformation of their own, claiming that “nine out of 10 of those needing the most care in hospital are unvaccinated.” Yet another example of absolute fake news, intended to deceive the public.
As we will discuss shortly, it is the seeming clamour to “get boosted,” incessantly pushed by the MSM and the politicians, effectively shutting down primary healthcare, that presents a far greater risk to public health. The mendacity of Javid’s disinformation was breathtaking.
The people who are queuing for their jabs aren’t selfish, just misinformed. However, the 13% of adult the population who don’t want one aren’t selfish either.
The MSM and the politicians persistently try to drive a wedge between the jabbed and the unjabbed. They seek to cause divisions based upon disinformation, lies and propaganda.
The reason for this is clear. Just like all tyrannical regimes throughout history, the current UK dictatorship wish to scapegoat a minority in order to avoid wider public attention turning on them. They do this to reduce the chance of the people questioning the tyrants who are enslaving them. It is nothing more complex than divide and rule.
THE JABS DON’T WORK
Speaking in October, the current UK Prime Minister, Boris Johnson, effectively admitted that the jabs are not “vaccines.” They do not function like any vaccines we are familiar with. Apparently, they are much more like a treatment:
Double vaccination provides a lot of protection against serious illness and death but it doesn’t protect you against catching the disease, and it doesn’t protect you against passing it on.”
Johnson’s observation was partially accurate. Recent research from the US found that there was no difference in viral load between the vaccinated and the unvaccinated. These findings appear to be corroborated by a study from Singapore, which strongly advocated the jabs for their claimed ability to reduce mortality, but also noted:
PCR cycle threshold (Ct) values were similar between both vaccinated and unvaccinated groups at diagnosis, but viral loads decreased faster in vaccinated individuals […] viral load indicated by PCR Ct values was similar between vaccinated and unvaccinated patients.”
For the jabs to function as a vaccine, in the traditional sense, the higher the jab rate the lower disease prevalence should be. This is an obvious point, but seemingly one that needs to be stressed as the wider public appear to be largely unaware of this.
There is no statistical correlation between population jab rates, infection rates and disease prevalence. A joint U.S. and Canadian study, which assessed statistical reports from 68 countries and 2947 US counties found:
At the country-level, there appears to be no discernable relationship between percentage of population fully vaccinated and new COVID-19 cases in the last 7 days. In fact, the trend line suggests a marginally positive association such that countries with higher percentage of population fully vaccinated have higher COVID-19 cases per 1 million people.”
Yet, somewhat contrary to their own findings, the researchers still promoted the jabs as part of broader approach to disease mitigation using non pharmaceutical interventions, including wearing face-masks, lockdowns and social distancing. As we will discuss shortly, promoting the official narrative is now a prerequisite for peer review and publication.
Presumably, to stay within the permitted boundaries of the official scientific consensus, the researchers maintained the new definition of “vaccine,” describing a drug incapable of reducing infection rates that acts like a treatment:
Vaccinations offers protection to individuals against severe hospitalization and death.”
The peninsula of Gibraltar, with a population of around 34,000, was delighted to declare that it had achieved a 100% jab rate. Thereafter it suffered a surge in reported cases.
In the Republic of Ireland, the city of Waterford has a 99.7% jab rate and the highest case rate in Ireland.
In Israel, where the definition of “fully vaccinated” means someone received two initial jabs and a booster (3 jabs,) there have been 67 recorded cases of the Omicron variant. Of these 54 (nearly 81%) were fully jabbed. Of the remaining 13 cases we don’t know if any of them were genuinely unjabbed. They could have received one or two jabs and still be categorised as not “fully vaccinated.”
If we look at a recent map of vaccine coverage provided by CNN we can identify some interesting comparisons.
Brazil, with jab coverage of 150 jabs per 100 people, has more than 103,000 COVID cases per million people (CPM). Neighbouring Bolivia, with 77 jabs per 100, has a case rate of just under 47,000 CPM. Paraguay has a slightly higher jab rate of 88 and a slightly higher case rate of 64,000 CPM. Argentina, with the highest jab rate of all, at 220 per 100, also has the highest CPM of all, at just over 117,000.

The most striking feature of the CNN map is the very low vaccinations rates in Africa. Nigeria, Tanzania and Zambia, for example, have less than 10 jabs per 100. They are among the countries with the lowest case rates in the world. Zambia has just over 11,000 CPM and Nigeria and Tanzania much less. By contrast Botswana, with a relatively high African vaccination rate of 62 per 100 people, has a CPM of nearly 82,000.
Some scientists are apparently mystified by the low rates of COVID-19 in Africa as a whole. They offer a range of possible explanations. They point towards a younger population or early border closures, some suggest lower urban density or perhaps more outdoor activity to account for the obvious anomaly.
Calling it a “mystery” Prof. Wafaa El-Sadr, global health lead at Columbia University, said:
Africa doesn’t have the vaccines and the resources to fight COVID-19 that they have in Europe and the US, but somehow they seem to be doing better.”
African nations are certainly doing better than the U.S. With approximately 4% of the World’s population and a vaccine rate of 147 per 100 people, the U.S. account for more than 36% of the current 27,586,743 active global cases.
In fact, the list of the top 20 nations with the highest case rates around the world is predominantly composed of the countries with the highest vaccination rates.
Scientists are looking at all the variables to try and figure out what could possibly explain the African mystery. The only factor they aren’t considering is the most obvious one.
Despite most African nations having no first wave, the global scientific and medical authorities are hell-bent on preventing the second with the jabs. Prof. Salim Abdool Karim from the South Africa’s University of KwaZulu-Natal said:
We need to be vaccinating all out to prepare for the next wave.”
Professor Karim was invited to join the World Health Organisation’s (WHO) science council in April 2020. The WHO have made jabbing African populations its next priority.
There are multiple studies which demonstrate that natural immunity derived from infection is considerably better than any imparted by the jabs. A recent Israeli investigation suggests that natural immunity, following infection, is up to 27 times more robust than any conferred by the jabs.
Regardless of scientific debates about antigens, T-cells and immunogenicity etc., which all relate to how the jabs supposedly function, very basic statistical analysis is sufficient to clearly demonstrate that they do not work as vaccines.
The only remaining claim for the jabs efficacy is that they reduce hospitalisation and death. Unfortunately, there is a lot of evidence which casts doubt upon this claim too.

Anthony Fauci (left) & Salim Abdool Karim (right)
If the jabs are incapable of stopping infection and transmission and serve only to reduce natural immunity, there is no possible public health rationale for a jab mandate. An uninfected individual is no more likely to catch COVID-19 from an unjabbed person than they are from a jabbed citizen. According to the official definition of a COVID-19 case, the statistics show that the jabs don’t make any difference whatsoever to the spread of disease.
In his more recent address to the nation, pushing the unregulated booster jabs, Boris Johnson said:
Over the past year we have shown that vaccination is the key to beating Covid and that it works […] It is now clear that two doses of vaccine are simply not enough to give the level of protection we all need […] we must urgently reinforce our wall of vaccine protection to keep our friends and loved ones safe […] As we focus on boosters […] it will mean some other appointments will need to be postponed until the New Year […] If we don’t do this now, the wave of Omicron could be so big that cancellations and disruptions, like the loss of cancer appointments, would be even greater next year”
Johnson’s speech was utterly incoherent. On the one hand the vaccines work but on the other they don’t and a booster is required. To fend off a wave of cases, defined by a test that can’t identify cases, apparently trivial health interventions, like cancer screening appointments, need to be cancelled for the benefit of the nation’s health and the common good.
Shortly following Johnson’s plea to “get boosted now” the UK government clarified that GP surgeries across the land would focus upon jabs and emergency appointments only.
By declaring a “national mission” to jab as many people as possible, primary care has practically been suspended in the UK. This has been done in the winter, in the middle of an alleged respiratory disease pandemic. The Health impact from this will be disastrous.
The British Medical Association has already warned that the reconfiguration of the NHS, first into a COVID-19 only service and now a jab only service, has terrible public health consequences.
Just in the 3 month period following the first lockdown there were up to 1.5M fewer elective admissions to hospital; first time patient attendance, for all conditions, dropped by 2.6M; urgent cancer referrals were down by an alarming 280,000, with up to 26,000 fewer patients starting treatment, of which 15,000 would normally have first come to light via a GP referral.
Yet, knowing all this, the government would have you believe that their intention is to save life. This claim is not credible.
THE JABS ARE DANGEROUS
Further evidence from Israel suggests that the the period between the first and second jab, and shortly thereafter, increases the COVID-19 mortality risk. Vulnerability to disease is significantly greater during this 3 to 5 week period.
Prof. Dr. Seligmann (Ph.D) and his research partner calculated the base rate likelihood of COVID-19 mortality for different age groups prior to being jabbed. For example, for those over 60, it was 0.00022631% per day. He then contrasted this with the official Israeli data for mortality immediately post jab.
During the 13 day period after the first dose of the Pfizer jab, the COVID-19 daily mortality risk for the over 60’s was 14.5 times higher at 0.003303% per day. After 13 days this risk increased to 0.005484% per day, more than 24.2 times greater. This rose further, up to 6 days after the second dose, to 0.006076% per day, representing a 26.85-fold increased risk of COVID-19 mortality for the jabbed.
Prof. Seligmann found similarly huge increases in the COVID-19 mortality risk for all the jabs during what he called the “period of vaccination.” Once the recipients were “fully vaccinated” Seligmann found some benefit for the jabbed, as they afforded a marginal reduction in COVID-19 mortality risks when compared to those of the unjabbed.
He calculated that, for this benefit to outweigh the massive increase in risk during the “period of vaccination,” the jabs would have to provide near 100% protection for more than two years just to offset the initial health cost of being jabbed. This benefit is not seen in the data.
A recent Swedish study is one among many to show that any possible COVID-19 benefit, once fully jabbed, wanes quickly. Unable to protect those most vulnerable to COVID-19 after 6 months, Dr Seligmann’s research indicates that there is no COVID-19 health benefit associated with the jabs.
Official risk/benefit analysis suggests that being fully jabbed provides some marginal protection against hospitalisation. There is also a barely discernible statistical signal suggesting that they also reduce mortality, to a very limited degree.
Prof. Seligmann found the same. However, this only related to the COVID-19 statistics and they are based upon non-diagnostic RT-PCR test results. Official claims take no account for the additional “period of vaccination” risk identified by Seligmann.
Prof. Selligman and Dr. Spiro P. Pantazatos, assistant Professor of Clinical Neurobiology at Columbia University, subsequently undertook further evaluation of the all cause mortality risk following the jabs.
Their research showed an estimated U.S. Vaccine Fatality Rate (VFR) of 0.04%, suggesting that the CDC declared VFR of 0.002% underestimates mortality caused by the jabs by a factor of 20. The scientists found that the data indicated U.S. jab related deaths of between 146,000 and 187,000 for the period between February to August 2021.
Pantazatos and Seligmann also identified a significant increase in the all-cause mortality risk in the first 5-6 weeks following the first jab. Again, demonstrating that the initial risk of being jabbed is not offset by the short-lived benefit once “fully vaccinated.”
There is little reason to accept the officially reported statistics.
The attribution of COVID-19 to mortality is spurious. Death within 28 or 60 days of a positive RT-PCR test is used, depending on whose statistics you look at. This is not “proof” that COVID-19 was the cause of death.
Attribution of COVID-19 to hospital admissions is equally weak. Research by independent auditors shows that people with a range of non-COVID related presentations, such as limb or head injuries, are often admitted to hospital as supposed COVID-19 patents.
The researchers found that, in more than 90% of alleged COVID-19 admissions, there was no clinical reason to describe them as such.
All alleged benefits of the jabs are based upon these woolly definitions and questionable statistical assertions. Consequently, if we truly want to understand the possible benefits of the jabs, we need to look at all cause mortality.
This can be considered more reliable because it is simply an anaylisis of all registered deaths, irrespective of the cause.
If the jabs work and are safe, then a difference in all cause mortality between the the jabbed and the unjabbed should be observed. While the jabbed aren’t protected against other causes of death, they are supposedly protected against COVID-19 and this should be detectable in the data.
A team of statisticians from Queen Mary University London conducted a study of all cause mortality data in England. They examined the vaccine surveillance monitoring reports issued by the Office of National Statistics (ONS).
They noted that initially, as we’ve discussed, these official reports seem to show a benefit from the jabs. However, they identified a series of anomalies in the data.
They found that non-COVID-19 mortality patterns, for the supposedly unjabbed, had peaks that correlated with the jab rollouts. After the “period of vaccination” the Non COVID-19 mortality for both the jabbed and allegedly unjabbed cohorts remained similar and relatively stable. Further, in general, the unjabbed appeared to have unusually high non-COVID-19 mortality while the jabbed seemingly had unusually low non-COVID-19 mortality.
They also looked at the different categories of jabbed people. These were “within 21 days of first dose,” “at least 21 days after first dose,” and “second dose.”
They found a consistent but large variation in the mortality figures between these groups. “Second dose” non-COVID-19 mortality was persistently below baseline mortality, while “within 21 days” mortality was always far above baseline.
Most striking was the different patterns in mortality between the three studied age groups. Historical data shows that for those in the 60-69, 70-79 and 80+ age groups, while all cause mortality increases with age, the three groups always shared the same mortality distribution pattern, typically with a peak in the winter months. This is often referred to as “excess winter mortality.”
Yet in 2021, not only did the three groups have separate periods of peak mortality, dispersed unseasonably throughout the year, for the unjabbed that mortality corresponded directly with the jab rollouts in each age group. Nor did these peaks in unjabbed mortality corrolate to supposed waves of COVID-19. They followed the jab rollouts.

The researchers concluded:
Whatever the explanations for the observed data, it is clear that it is both unreliable and misleading […] we believe the most likely explanations are systematic miscategorisation of deaths between the different groups of unvaccinated and vaccinated; delayed or non-reporting of vaccinations; systematic underestimation of the proportion of unvaccinated [and] incorrect population selection for Covid deaths. With these considerations in mind we applied adjustments to the ONS data and showed that they lead to the conclusion that the vaccines do not reduce all-cause mortality, but rather produce genuine spikes in all-cause mortality shortly after vaccination.”
The head of the research team, Prof. Dr. Norman Fenton, gave a radio interview where he explained why his paper had not been peer reviewed or submitted to a journal for publication:
The unvaccinated seem to be dying after not getting the first dose and the single dose are dying after not getting the second dose […] the vaccinated are dying within 14 days of vaccination and are simply being categorised as unvaccinated […] There is no evidence for their efficacy when it is measured by the only sensible way to measure it, which is all cause mortality […] When we first started doing research on this we had no problem getting our work into peer reviewed papers, because we weren’t challenging the narrative […] As soon as it became clear, you know, with the sort of mass testing of asymptomatic people, that the potential for false positives for asymptomatics was inflating case numbers and COVID so-called hospitalisations and deaths, as soon as we started raising those concerns in our work, as soon as we submitted it for publication, it was being rejected without review. Something I have never had before.”
Rejecting science, because it doesn’t abide by the official narrative, is not a new problem but it is “anti-science” and suggests a coordinated effort to deceive. The work of Prof. Seligmann and others, looking at both COVID-19 and all cause mortality, appears to independently corroborate the finding of Queen Mary team.
There is no doubt that the jabs can kill. There have been a number of inquests that have found that death was caused by complications following the jabs.
Causes of death have included venous infarction thrombosis, intracerebral haemorrhage, anaphylaxis, vaccine-induced thrombosis & thrombocytopenia and “unrecognised consequences of elective COVID-19 vaccines,” to name a few. The only question is the scale of the mortality caused by the jabs.
US researchers found a 19 fold increase in myocarditis (heart inflammation) among the 12 – 15 year olds which directly correlated with the jab roll-out. The study was peer reviewed and then published, before being withdrawn by journal editors without explanation.
Myocarditis is extremely serious for young people and often requires a heart transplant in later life, significantly reducing their life expectancy.
Just as some in the scientific community are mystified by the almost perfect correlation between jab and COVID-19 “case” rates, so the medical profession are similarly bewildered by the marked rise in cardiac emergencies in Scotland. These too followed the jab rollout for the impacted age groups.
Apparently doctors haven’t got the faintest idea what the cause could possibly be. They are not investigating if it could be the jabs.
Why they aren’t could be seen as yet another mystery, because the statistical evidence indicates that the jabs are lethal. If we look at statistics from the ONS it is evident that, between January and October 2021, the jabbed under 60’s in England were dying at approximatly double the rate of the unjabbed.
This is not an insignificant fact but comes with important caveats. Prof. Fenton and his team did not analyse this age group because it is too broad. Depending on the progress with the jab rollouts, with older people jabbed first, the jabbed cohort is likely have a higher baseline mortality risk than the jabbed.
Taken in isolation this statistic doesn’t reveal much. It is more telling in context with a German study which also found a clear correlation between the jabs and mortality.
Together these add further corroboration the other statistical findings we’ve discussed. The German scientists, Prof. Dr. Rolf Steyer and Dr. Gregor Kappler, concluded:
The higher the vaccination rate, the higher the excess mortality. In view of the forthcoming policy measures aimed at reducing the virus, this figure is worrying and needs to be explained if further policy measures are to be taken with the aim of increasing the vaccination rate.”
The only rationale that can explain how the ONS, MHRA, EMA, FDA and other official bodies around the world are maintaining the lie that the jabs save lives is that they have chosen, or have been ordered, to release disinformation that knowingly endangers public health. There is yet more evidence from the clinical trials that this is the case.
The FDA, MHRA, EMA and other supposed regulators granted EUA’s for the Pfizer/BioNTech jab based upon 2 months of extremely limited, interim trial data. Research by the Canadian COVID Care Alliance has exposed this wholly untrustworthy process. There was no mention in the original, interim trial data, submitted by Pfizer, of the scale of the ADRs caused by their product.
Using relative risk they claimed their jabs were amazing and nearly everyone, including the regulators, simply took their word for it. Those who didn’t were vilified as “covid deniers” or “anti-vaxxers.”
Six months into the jab rollout Pfizer released more data with another interim study. They made more claims about the efficacy and safety of their BNT162b2 jabs:
BNT162b2 continued to be safe and have an acceptable adverse-event profile. Few participants had adverse events leading to withdrawal from the trial.”
However, this wasn’t true at all. In their released report, published by “respected journals” like the Lancet, they forgot to analyse the supplementary evidence concerning ADRs, also contained within their findings.
This revealed a consistent elevated risk of Adverse Events (AEs) for the jabbed. For example, “related events” are adverse health events that are deemed to be caused by the jab. For the jabbed the related risk ratio was 23.9, for the unjabbed it was 6. This is nearly a 300% increase in the risk of health harm if you take the Pfizer jab.
Serious adverse events are likely to put you in hospital. For the jabbed the risk was 0.6, for the unjabbed it was 0.5. In other words the jab increases your risk of being hospitalised by 10%.
A drug that increases illness in the population is not an “effective vaccine.” Reducing “case numbers” for one ailment is an utterly pointless exercise if population levels of illness and hospitalisation increase as a result. It gets worse.
Prior to unblinding their own trials, thereby ending the supposed RCTs years before completion, jabbed and unjabbed cohorts were equal in size. 15 people died in the jabbed cohort and 14 died in the unjabbed cohort. Following unblinding a further 5 jabbed people died, including 2 who were previously unjabbed.
The jab increases the mortality risk. This is precisely as observed by Seligmann, Fenton, Steyer, Kappler, Pantazatos and many other scientists and statisticians.
Pfizer were eager to report the 100% reduction in COVID-19 mortality in the main body of their study. Of the 21,926 people in the jabbed cohort only 1 died with a positive RT-PCR confirmed COVID-19 “case.” Whereas 2 of the 21,921 placebo group died. Hence Pfizer’s 100% improvement claim of efficacy.
They failed to mention that their product doubled the chance of you suffering a cardiovascular event and they definitely shied away from the most unpallatable reality of all. There were 4 heart attack deaths among the jabbed compared to 1 in the placebo group. A 300% increased risk of fatal heart failure following the jab.
If the objective of the jabs is to “save life” then it is impossible to understand how they ever received EUAs.
Fully indemnified against prosecution and with carte blanche from the regulators to do whatever they like, the pharmaceutical corporations are fully committed to jabbing all our children, including infants.
This is something our governments and the majority of the population wholeheartedly approve of. If you question it you are selfish.
THE REGULATORS SEEMING EFFORTS TO HIDE THE TRUTH ABOUT THE JABS
It is common to read claims from the regulators, and everyone else who advocates the jabs, that the benefits of the vaccines outweigh the risks.
This is based on the alleged risk of COVID-19, which is practically impossible to assess due to the massive corruption of the data, and an apparent blank refusal to consider any risks from the vaccines.
At first glance, the safety profiles for the jabs look appalling. So far, in the UK alone, there are 1,822 possible jab related deaths recorded via the MHRA yellow card scheme.
In response to a Freedom of Information Request (FOIR,) the MHRA revealed that they had received:
“[…] a total of 404 UK spontaneous suspected ADR reports for any vaccine between 01/01/2001 – 25/08/2021 associated with a fatal outcome.”
With more than 1,800 suspected fatalities reported for the COVID jabs already, currently they potentially account for three and half times more fatalities than all other vaccines combined over the last two decades. This is a statistical pattern repeated in every nation that has rolled them out.
We also know that the vast majority of possible ADRs remain unreported. A 2018 survey study of paediatric healthcare professionals found that 64% had not reported known ADRs. Of the total surveyed 16% didn’t even know the Yellow Card system existed and 26% didn’t know how to use it, with only 18% having undertaken any relevant training.
So it is not at all surprising that the MHRA state:
“It is estimated that only 10% of serious reactions and between 2 and 4% of non-serious reactions are reported.”
There is no evidence that the MHRA have done anything to improve yellow card reporting. Apparently they have promoted the Yellow Card Scheme, it is just that no one noticed. With nearly 400,000 COVID jab ADR reports on the system already, it is likely that the true figure is in excess of 10 million and possible UK deaths caused by the jabs could certainly exceed 18,000.
This is necessarily speculative to a degree, because the MHRA have not investigated any of the recorded ADRs. They have no idea how many people have been killed by the jabs and have shown no interest in finding out.
While they claim their role is to investigate potential ADRs, to provide an “early warning system” for possible vaccine harm, they also say:
The suspected ADRs described in this report are not interpreted as being proven side effects of COVID-19 vaccines.”
This is reasonable if those reports are then investigated. That is not what the MHRA do. Their position and their statements are wholly unreasonable.
To date, they have provided nothing that proves these reports are not evidence of ADRs. Their given interpretation, that these reports provide no proof, is meaningless. Nothing can ever be proven if you don’t bother to examine the evidence.
There is no commitment from the MHRA that they will ever investigate any Yellow Card reports for the jabs. All they will do is highlight possible safety issues, note the reports, and maybe discuss these with other national regulators. There is no expressed intention to question the manufacturer’s claims for the jabs at all.
The UK’s MHRA claim that a dedicated team look for “signals” in the data and where a signal is found they will discuss this with some selected experts.
Given that they acknowledge both the under-reporting and that current monitoring suggests the jabs have a mortality rate orders of magnitude worse than any vaccine, you would imagine that the MHRA would have identified a very concerning “signal.” Indeed they admit:
Yellow Cards in isolation are sufficient to allow signal detection.”
Yet they choose not to use the Yellow Cards as an “early warning.” There is no record of them following up on any Yellow Card reports. Instead they first apply a number of relative risk calculations to see if the signal is worthy of further discussion.
In particular, they use the MaxSPRT (Sequential Probability Ratio Test). This compares reported ADRs to the general population, or background, risk of the same adverse event. If the likelihood ratio test (LRT) indicates that the risk is higher following a jab, then a signal has been identified. However, dishonesty lurks within this approach.
MaxSPRT is based upon a series of assumptions about the data. Specifically that it is constantly monitored in real time and that there is a matched exposure between the jabbed and the unjabbed to contrast incident rates.
When we are talking about 40M jabbed compared to 7M injabbed adults, the disparity between and the size of the jabbed and the unjabbed cohorts invalidates this methodology.
Many biostatiticians have pointed out the limitations of using MaxSPRT for large volume database analysis:
This particular LRT, which conditions on the total number of events, is designed for the rare event case in which only one event is expected to be observed per exposure […] However, when events are not extremely rare, or when the probability within a stratum of more than one event occurring is not small, the assumptions of this LRT are violated.”
In other words the MHRA appraisal is highly sensitive to extremely rare ADRs but is likely to hide, rather than reveal, the more common side effects that are killing people. The MHRA are using a system that will obscure serious problems with the jabs. The only signals their dedicated team might discuss with experts will be “extremely rare.”
They won’t see any signals for more common adverse events and can therefore overlook the obvious and ignore the danger.

MHRA – Dedicated Team
Presumably this is why the MHRA have chosen not to use the “Yellow Cards in isolation.” The raw data clearly indicates huge reason for concern. It has to be reworked and remodelled in order to ignore the glaringly evident. Again, this is a common feature of all jab safety monitoring (pharmacovigilance) systems, which scientists have described as “utterly inadequate.”
Correlation does not prove causation, yet where correlation is persistent and pronounced the chance of it not demonstrating causation diminishes rapidly. Wherever we look, the jabs appear to be causing severe ADRs on an alarming scale.
COVID JABS: INEFFECTIVE, OPPRESSIVE AND DANGEROUS
There is no evidence to substantiate any official or MSM claims about COVID-19 jab efficacy or safety. They are experimental drugs with unknown risk profiles that are being forced upon people without offering them any opportunity to give their informed consent. The jab roll-outs breech numerous international conventions including the Nuremberg Code.
What data does exist is alarming, to say the least, and all the indications are that the jabs are extremely dangerous. There is no doubt that they can kill. Those who support a jab mandate are advocating that people should be forced to take a potentially lethal injection. Those who are aware of this, understandably, do not wish to take them.
For this they are being demonised by government, the MSM and a large percentage of those who have elected to be jabbed. If they try to raise any concerns they are dismissed by the same as anti-vaxxers, conspiracy theorists, covid-deniers or dangerous refuseniks and are accused of being selfish. Despite that fact that it is the jab obsession that is destroying public health and medical services.
There is clear evidence of obfuscation and denial to hide the dangers of the jabs from the public. This seems to cross the threshold of criminality in nearly every nation state where the jabs are deployed. National populations are clearly under attack by their own governments and their partners.
However, perhaps the most insidious aspect of the jabs is their central role within a new system of governmental authority that is enslaving humanity. Our jab status is the required license to participate in a technocratic, behavioural control and surveillance grid. Not only will our vaccine passport (app) monitor and report where we go, who we meet and what we are allowed to do, it will also determine what services we can access.
Those who think the jabs are essential to protect themselves and others, against a low mortality respiratory virus, have either not been given, or choose to ignore, the information required to make this judgement. They believe that they are free because they can now register to use the services that hitherto were freely available to all. They have accepted that they need permission from the government simply to conduct normal, everyday activities.
They are committed to take whatever drugs are given to them for the rest of their lives. If they wish to retain their societal permits, this is not negotiable. Their imaginary freedom is conditional upon their continued compliance.
They do not own their own body and are no longer, in any sense, free. They are elective slaves and are seemingly content to condemn future generations, including their own children, to the same fate.
You can read more of Iain’s work at his blog In This Together or on UK Column. His new book Pseudopandemic, is now available, in both in kindle and paperback, from Amazon and other sellers. Or you can claim a free copy by subscribing to his newsletter.
Vaccinating 5 to 11 yo: the UK does not advise healthy kids to get it, while USA starts mandating it for school
Our policy is not sensible
By Vinay Prasad MD MPH | December 23, 2021
It is always instructive to highlight differences in the vaccination policies between nations. After all, the clinical trials that guide these decisions are the same across nations.
Yet, different experts can view the same risk-benefit decisions differently, or view uncertainty differently. In my mind, there is clearly a problem if one nation advises AGAINST doing something while another location MANDATES it. I think we should all agree that this makes no sense. One should not deploy the brute force power of the mandate if a decision is sufficiently debatable that another nation literally advises against it.
This already happened with LA County’s mandate for 2 doses for teens 12-15. I detailed how LA’s school mandate was in tension with UK and Norway’s guidance with respect to number of doses and timing of doses in the US News and World Report.
Now, we see it again. The UK’s expert body JCVI (Joint Committee on Vaccination and Immunisation) is moving forward with vaccinating 5 to 11 year olds with underlying health conditions, who are at risk, but not all healthy 5 to 11 year olds.
When it comes to healthy 5 to 11 year olds this is what JCVI is waiting for:
All quite reasonable, if you ask me!
Now, contrast the UK with the US.
New Orleans has already moved ahead and mandated vaccination in 5 to 11 year olds. And the AFT president has said she stands behind such mandates. New Orleans policy goes into effect February 1.
The penalty for non-compliance with these mandates will likely be exclusion from in person schooling. That penalty is far harsher than the risk of sars-cov-2 in a healthy unvaccinated child, which is very low. The best data for that is the new Germany paper.
Can we at least acknowledge how crazy it is that one nation DOES NOT RECOMMEND something while another nation MANDATES IT to attend something as basic and necessary as grade school?
In 2019, in the wake of poor uptake of MMR (a vaccine with far less disagreement & uncertainty) UNICEF wrote:

It is a shame we cannot live up to that standard now. Our fear has overtaken our compassion and sense.
Vinay Prasad MD MPH is a hematologist-oncologist and Associate Professor in the Department of Epidemiology and Biostatistics at the University of California San Francisco. He runs the VKPrasad lab at UCSF, which studies cancer drugs, health policy, clinical trials and better decision making. He is author of over 300 academic articles, and the books Ending Medical Reversal (2015), and Malignant (2020).
Covidian migration patterns
el gato malo – bad cattitude – december 24, 2021
these graphics are from longtime gatopal™ kbirb who has done so much excellent analysis lo these 21 months.
these are especially great.
let’s look:
(note this is only thru july 2021 and seems to be ongoing and is likely larger by now)

well, that’s not terribly ambiguous, is it? (though based on everything i’ve seen in the mountain west, net migration there looks strongly positive)
we can see that if we get more granular:

big winners: the free states of florida, texas, arizona
big losers: the karentopias of california, new york, illinois
this really speaks volumes.
red v blue gets extreme:
and it sure looks like “access to education” is a major driver.

though this graphic (from NYT ) has interesting overlay too.
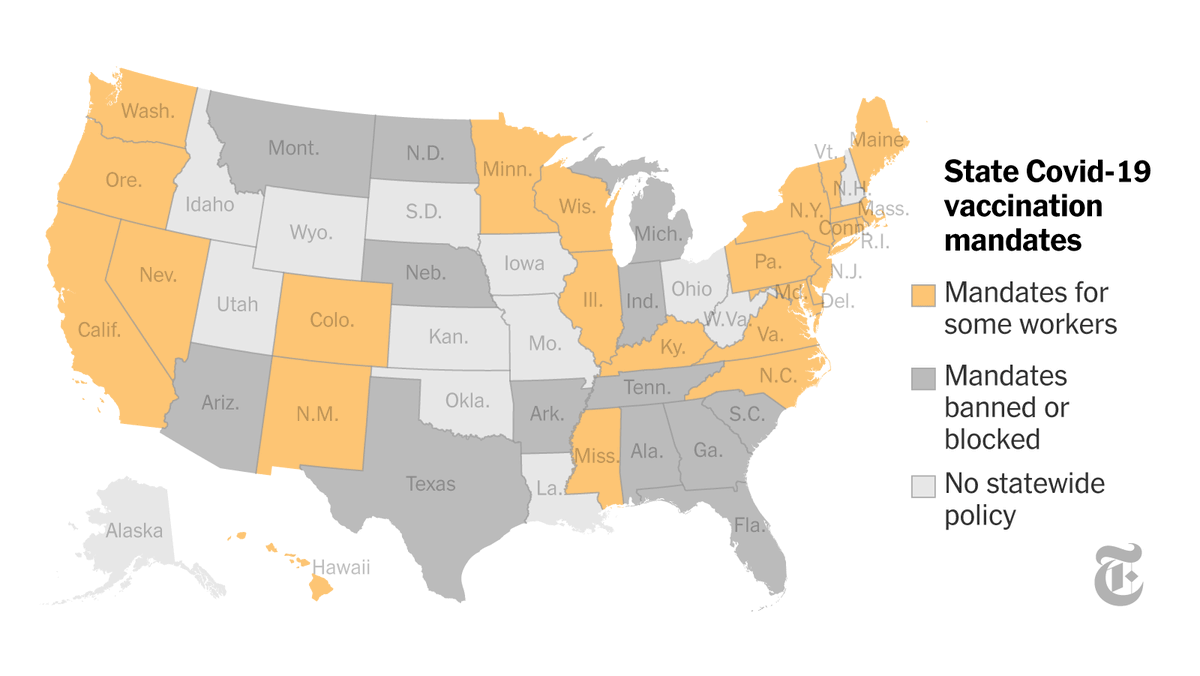
speaking as one who spent the summer in a free state only to return to the assault and dingbattery of a masked up, restricted, and vaxxpassed puerto rico, it is JARRING.
once you see that this is not really a thing, that life is normal in half the country, and that continuing to play this game or even care about it is utterly optional, there is no closing your eyes again.
you cannot go back to a mask mandate grocery store and not see all these people as having mental health issues (or at the very least some sort of societal spinal atrophy that renders them unable to support a republic.)
half the people i know are talking about leaving PR. it’s become intolerable, especially once you have seen the options firsthand. hearing the same about new york, SF, LA, etc.
it’s just endless and capricious and increasingly aimed at deliberately making life miserable for any who refuse to comply. this round feels personal. “all you have to do to make the persecution end is comply!” it’s an oppressively ubiquitous mantra and the “jim covid” laws are entering every phase of life.
but one trip to florida and the spell breaks.
you realize you’re being conned because you see it first hand and remember.
maybe you moved there because you wanted your kids to see the inside of a classroom at some point before 2024.
this derangement is going to seriously redraw some american maps.
the damage is not the pandemic, it’s the policy. that’s why this is divided so starkly by donkey vs elephant. covid has been a political, not an epidemiological crisis and remains one.
and the more we can support state’s rights and thereby create more and more varied choice for people to pursue their happiness, the more this flow will become a torrent.
hopefully the last people out of the karen-capitals will remember to turn off the lights when they leave…
Delicensing Doctors for ‘Harmful Misinformation’
By Jane M. Orient, M.D. | Assosiation of American Physicians and Surgeons | December 17, 2021
In addition to being subjected to various forms of censorship, for the first time in living memory American doctors are getting threat letters from licensure boards warning them against distributing “harmful misinformation.” Medical boards in 12 states have disciplined doctors because of this allegation. While it is claimed that there’s an epidemic of misinformation during the COVID-19 pandemic, the warnings don’t spell out what that means.
We don’t have an epidemic of patients dying because doctors told them to refuse treatment or to drink Clorox or aquarium cleaner.
In fact, no patients need to have suffered any harm at all for the medical board to investigate a doctor’s no-longer-free speech. All it takes is an anonymous complaint.
Pharmacists who were converted into the overseers of physicians’ prescribing practices will complain that a doctor had prescribed ivermectin for COVID-19.
Or an employer might complain that a doctor supported a worker’s request for a medical exemption that wasn’t on the CDC’s list of acceptable reasons.
Or the doctor might have spoken at a political meeting at which mask mandates were being challenged.
Or a patient might complain that a doctor wasn’t wearing a mask in his private consulting room, even when no COVID-19 patients were anywhere near and the doctor had demonstrated immunity.
Or a pathologist might have stated publicly that his busy lab was seeing a higher percentage of cancers in vaccinated patients.
“Harmful misinformation” appears to mean anything that contradicts or asks questions or raises doubt about the dogma that “vaccines are safe and effective,” or suggests a treatment not endorsed by the Food and Drug Administration (FDA), Centers for Disease Control and Prevention (CDC), National Institutes of Health (NIH), and their corporate sponsors.
One source of the allegedly “harmful misinformation” is a database created and maintained by the CDC, the Vaccine Adverse Event Reporting System (VAERS). Anybody can enter a suspected vaccine adverse reaction, and the public can access it. So, “it can be abused by people trying to sow fear,” write Shayla Love and Anna Merlan in VICE News. One person filed a fraudulent report, promptly removed, claiming that an influenza vaccination had turned him into the “Incredible Hulk.”
Flawed as it is, VAERS is the best CDC has to offer for looking for “danger signals.” Of course, correlation doesn’t prove causality. As Lindy McGee from Texas Children’s Hospital correctly pointed out, “I can report if I get hit by a truck after I’ve gotten a vaccine and that would be reported as associated with a vaccine. It does not make any implication of causality.” However, there is a double standard. If you get hit by a truck, but test positive for COVID-19, the hospital will get paid for counting you as a COVID death.
Adverse reports to VAERS are many times higher for COVID-19 vaccines than for all other vaccines combined since the database was established in 1988. The website vaers.hhs.gov clearly states: “Knowingly filing a false VAERS report is a violation of Federal law (18 U.S. Code § 1001) punishable by fine and imprisonment.” So, presumably most of the approximately 20,000 reports of death concern people who really did die soon after getting the jab, most within a few days. It could be 20,000 coincidences, but the count is not “misinformation.”
Love and Merlan call the compilers of VAERS information at openvaers.com/covid-data “dumpster divers.” Matt Motta of Oklahoma State University and Dominik Stecuła of Colorado State University refer to that January article favorably in their Aug 25 essay that says VAERS is only good for researching “vaccine hesitancy.” They don’t mention that the featured VAERS death count of 329 from Jan 22, 2021, has steadily increased.
Also viewed as “misinformation” is the opinion of physicians and researchers that hydroxychloroquine, ivermectin, and other “repurposed” drugs are beneficial in COVID-19, as shown in more than 1,000 studies. Reports of dying patients who recovered when hospitals were legally forced to step aside and allow off-protocol treatment are ignored.
The safe option for doctors is to promote the jab or keep silent, and not to suggest anything different from what Anthony Fauci approves. By silencing doctors who are ethical professionals, one opens the gates for the reckless charlatans.
Recall that in Orwell’s Newspeak, the meaning of words is inverted. The Ministry of Love is in charge of torture; the Ministry of Plenty, of starvation; and the Ministry of Truth, of propaganda.
Is the Minitrue defining “misinformation” today?
Featured Video

Larry Johnson: U.S. Desperation Grows as Iran Is Winning
or go to
Aletho News Archives – Video-Images
From the Archives
Alarmist climate science as a textbook example of groupthink
By Paul MacRae | May 1, 2012
A while ago, I received an email from a friend who asked:
How can many, many respected, competitive, independent science folks be so wrong about [global warming] (if your [skeptical] premise is correct). I don’t think it could be a conspiracy, or incompetence. … Has there ever been another case when so many ‘leading’ scientific minds got it so wrong?
The answer to the second part of my friend’s question—“Has there ever been another case where so many ‘leading’ scientific minds got it so wrong?”—is easy. Yes, there are many such cases, both within and outside climate science. In fact, the graveyard of science is littered with the bones of theories that were once thought “certain” (e.g., that the continents can’t “drift,” that Newton’s laws were immutable, and hundreds if not thousands of others).
Science progresses by the overturning of theories once thought “certain.” … continue
Blog Roll
 Aletho News
Aletho News- Larry Johnson: U.S. Desperation Grows as Iran Is Winning
- Why don’t UK media mention the Israel lobby?
- New US shipment of 6,500 tons of military aid arrives in Israel
- Military aid to Ukraine vital for ‘US hegemony’ – Republican senator
- Zelensky’s favorite drone company at center of Ukrainian corruption alert
- The Broken Contract
- US CENTCOM’s Request for Dark Eagle Missiles Shows Shortage of Weapons and Limited Options
- Iran consolidates Strait of Hormuz control in post-war power shift, leaving US in dark
- A pause, not a ceasefire: Washington stalls, Tehran recalibrates
- US blockade crumbles as Iran turns to overland routes
- If Americans Knew
- US ships 6,500 tons of munitions, equipment to Israel in 24 hours
- A New Library in Gaza Rises From the Ashes of Destruction
- Israel’s top Jewish religious body ‘refuses to condemn’ smashing of Jesus statue
- Nun assaulted in Jerusalem amid ‘pattern’ of anti-Christian attacks by Israelis
- Former Tik Tok official describes massive pressure from Israel lobby
- Amid ceasefire violations and genocide, Israel commits piracy – Daily Update
- Five Laws and Standards That Require the US Cut Off Weapons to Israel
- Israel’s diabolical killing machine and how it targets journalists.
- The Global Sumud Flotilla to Gaza — A cry at sea to the world’s dormant conscience
- Politico’s powerful parent company tells Politico they must support Israeli narrative
- No Tricks Zone
- Oversupply Of Volatile Solar Energy Leads To Record NEGATIVE Prices!
- New Study: Extreme Heat Records, Heatwaves, Extreme Cold Records Declining Across US Since 1899
- It’s The Cold, Stupid! Cold 20 Times More Lethal Than Heat, Multiple Studies Show
- European Institute For Climate And Energy: “Climate Debate is Seldom About Science”
- New Study: The Climate May Be 5 Times More Sensitive To Solar Forcing Than Commonly Assumed
- EV Industry Reached $70 Billion In Losses In 2024 Due To Delusional Green Ideologies
- Reality Check: Maldives Have Actually Grown In Size Or Remained Stable Over Recent Decades
- Abrupt Climate Change Also Occurred NATURALLY In The Past …25 Times During Last Ice Age
- Cave Discovery Reveals Today’s Desert Climates Were Recently Far Warmer, Wetter, Teeming With Life
- German Expert: Heat Dome Led To Record Temps In Western USA…Warmer In 1934, 1936
