Sometimes it pays to step back in history to understand exactly how something monumental was created. This is the story of how one Big Lie turned our world upside down and ruined the lives of millions of people.
Hard to believe that one Big Lie could have created all the pandemic controls, especially lockdowns, school closings and quarantines, that devastated our lives, our economy and our society. But it happened.
A very powerful, influential person told the world in early 2020 that the new China virus that leads to COVID-19 infection was especially lethal. It quickly pushed a fast, enormous response to protect public health. Was the truth was being told? It was not. There was an exaggeration of the new virus lethality for the entire population.
In truth, it was only severe for the oldest age category. Helped by corrupt data from CDC, overstatement of COVID lethality continues today to maintain public fear.
But first it is important to discuss the meaning of critically important terms. What the Big Lie was all about had to do with the fatality or death rate of what early in 2020 was seen as an invading new virus coming from China. How should we think about the fatality rate of a virus?
Terminology
One simple and correct way is how many people die from the infection caused by the virus: the Infection Fatality Rate (IFR). But another possible way would be to invoke the Case Fatality Rate (CFR); the fraction of documented cases of people with the virus that resulted in death.
How can you know how many people are infected? A lot of testing would be necessary. For our COVID pandemic there has been, surprisingly, very little wide blood testing across the whole population. Many people with infections have no symptoms or just mild ones and do not seek testing or medical attention. The CDC has done a terrible job of getting good data on infection numbers.
As to cases ascribed to COVID, there are reasons why that number surely underestimates how many people are really infected. Why? Because only some people, usually with symptoms, get tested and if found positive become a case. On the other side, the PCR test method most widely used has often been implemented in a way to get false positive results.
Mainly because the number of cycles the test is run is far too high (above 25) and picks up fragments of the virus (or any coronavirus) that does not document real COVID infection. Thus, the CFR is not a reliable or accurate measure of the real death rate despite widely published case numbers.
Key Moment In History
During a March 11, 2020 hearing of the House Oversight and Reform Committee on coronavirus preparedness, Dr. Anthony Fauci, director of the National Institute of Allergy and Infectious Disease, put it plainly: “The seasonal flu that we deal with every year has a mortality of 0.1 percent,” he told the congressional panel, whereas coronavirus is “10 times more lethal than the seasonal flu,” per STAT news. [0.1 percent also expressed as .001]
He also said: “The bottom line: It is going to get worse.” And this: “The stated mortality, overall, of [the coronavirus], when you look at all the data including China, is about 3 percent.”
That figure of 3 percent, far from reliable, is 30 times greater than the figure given for the seasonal flu. Fauci exaggerated to create a crisis. Simply by implying great lethality for everyone infected by the new COVID virus.
And it should be noted that CDC has found the flu IFR ranged from 0.1 percent (the figure cited by Fauci) to 0.17 percent [.0017] from 2014 to 2019, because seasonal deaths vary significantly.
What Fauci said put the country, with the help of big media, into convulsions. It created the foundation for authoritarian contagion controls driving a spike into the lives of Americans. Fauci intentionally created the pandemic by creating fear.
New York City Analysis
An interesting analysis was made for IFR for New York City at the height of the pandemic in May 2020. It illustrates how both death and infection data can be fine-tuned to get an IFR. As to deaths, blood testing found that 19.9 percent of people had antibodies indicating infection, yielding a number of 1,671,351 infected. As to deaths from COVID, there were three components: 13,156 confirmed, 5,126 probable, and 5,148 excess for a total of 23,430, that may have overstated deaths.
Probable meant likely COVID death but not confirmed through testing. Excess meant the number above expected seasonal baseline level. Using the total deaths divided by total infected produces an IFR of .014. Higher than the usual quoted flu value [.001] for the height of the pandemic in high density New York City.
And without consideration of variations among most vulnerable groups. A high rate of fatality for elderly people would cause a deceptive high value for IFR for the entire population.
Deaths certainly have declined significantly in the past year and more (even as high transmissivity delta variant has probably maintained high levels of infections). Why? Because of far better actions in hospitals and because infected people have surely learned a lot about home treatments to catch COVID infection early after initial symptoms and possibly a positive test. Cutting the deaths in half for the same number of infected people results in an IFR of .007, probably a more realistic figure for today.
World Health Organization
At an October 2020 meeting of the World Health organization, Dr Michael Ryan, the Head of Emergencies revealed that they believe roughly 10 percent of the world has been infected with Sars-Cov-2. This is their “best estimate.” This figure was based on the average results of all the broad seroprevalence (blood) studies done around the world. The message was that the virus is nothing as deadly as everyone predicted.
At the time the global population was roughly 7.8 billion people, if 10 percent have been infected that is 780 million infections. The global death toll then attributed to Sars-Cov-2 infections was seen as 1,061,539. That’s an infection fatality rate of roughly or 0.14 percent [.0014]. Consistent with seasonal flu and the predictions of many experts from around the world. And inconsistent with the dire picture given by Fauci.
Great Analysis
Now consider the detailed analysis “Public Health Lessons Learned From Biases in Coronavirus Mortality Overestimation” by Ronold B. Brown published in August 2020. He has doctoral degrees in public health and organizational behavior.
Here are highlights from this article that focused on what Fauci said.
“The validity of this estimation could benefit from vetting for biases and miscalculations. The main objective of this article is to critically appraise the coronavirus mortality estimation presented to Congress.”
[What Fauci said] “helped launch a campaign of social distancing, organizational and business lockdowns, and shelter-in-place orders.”
“Previous to the Congressional hearing, a less severe estimation of coronavirus mortality appeared in a February 28, 2020 editorial released by NIAID [Fauci’s department] and the Centers for Disease Control and Prevention (CDC). Published online in the New England Journal of Medicine (NEJM.org), the editorial stated: ‘…the overall clinical consequences of Covid-19 may ultimately be more akin to those of a severe seasonal influenza (which has a case fatality rate of approximately 0.1 percent).’
Almost as a parenthetical afterthought, the NEJM editorial inaccurately stated that 0.1 percent is the approximate case fatality rate of seasonal influenza. By contrast, the World Health Organization (WHO) reported that 0.1 percent or lower is the approximate influenza infection fatality rate, not the case fatality rate.“
Brown correctly hit the key semantic issue: CFR versus IFR.
“IFRs are estimated following an outbreak, often based on representative samples of blood tests of the immune system in individuals exposed to a virus. Estimation of the IFR in COVID-19 is urgently needed to assess the scale of the coronavirus pandemic.“ [Now, over a year later this has not happened.]
Brown correctly emphasized “it is imperative to not confuse fatality rates [CFR and IFR] with one another; else misleading calculations with significant consequences could result.” [That is exactly what Fauci engineered.]
Brown said the 1 percent figure in the testimony was consistent with the “coronavirus CFR of 1.8-3.4 percent (median, 2.6 percent) reported by the CDC.” [As I write this data in The Washington Post shows a CFR of 1.6 percent. This substantiates that the health care system has made progress in curbing COVID deaths. But this current CFR is still 16 times higher than the IFR figure for the seasonal flu. IFR remains the issue.]
Now Brown gets to the heart of the problem: “A comparison of coronavirus and seasonal influenza CFRs may have been intended during Congressional testimony, but due to misclassifying an IFR as a CFR, the comparison turned out to be between an adjusted coronavirus CFR of 1 percent and an influenza IFR of 0.1 percent.”
[Did Fauci, the widely lauded expert, not know what he was doing? Hard to believe this. If he knew, then we have the explanation for the Big Lie.]
By May 2020 “it was clear that the coronavirus mortality total for the season would be nowhere near 800,000 deaths inferred from the 10-fold mortality overestimation reported to Congress [emphasis added].
Even after adjusting for the effect of successful mitigation measures that may have slowed down the rate of coronavirus transmission, it seems unlikely that so many deaths were completely eliminated by a nonpharmaceutical intervention such as social distancing, which was only intended to contain infection transmission, not suppress infections and related fatalities.”
As to getting good data to determine IFR, Brown noted: “A revised version of a non–peer-reviewed study on COVID-19 antibody seroprevalence in Santa Clara County, California, found that infections were many times more prevalent than confirmed cases.
As more serosurveys are conducted throughout the country, a nationally coordinated COVID-19 serosurvey of a representative sample of the population is urgently needed, which can determine if the national IFR is low enough to expedite an across-the-board end to restrictive mitigating measures.”
[In other words, with systematic blood testing, if we have an IFR for COVID similar to the IFR for the seasonal flu, then the many disruptive and costly actions by the public health establishment are not justified. And they never were! ]
Another Analysis
The title of this September 2020 article by Len Cabrera is “Mistake or Manipulation.” An initial point made was: “A review of the early events mentioned in Dr. Brown’s paper and the lack of any corrections to the record suggest that the misstatement [by Fauci] before Congress was not a mistake.” If not a mistake, then it was intentional.
This point was dead on: “In his testimony, Dr. Fauci claimed the mortality of flu was 0.1 percent and that the case fatality rate of COVID was 3 percent but could be as low as 1 percent with asymptomatic cases. This is an apples-to-oranges comparison of the flu’s infection fatality rate (IFR) to COVID-19’s case fatality rate (CFR).”
And this critical point was made: “All cases are infections, but not all infections are confirmed cases, so the number of infections always exceeds the number of cases, making IFR less than CFR.” In other words, if the number of deaths is the same, then a lower denominator for calculating CFR compared to that for getting the IFR results in a higher number for CFR.
Are we to believe that the esteemed Fauci did not know this? Or is it reasonable to conclude that Fauci knew exactly what he was doing, namely using some simple data to create a pandemic crisis that required massive authoritarian government actions? Fauci set the stage for his wait-for-the-vaccine pandemic strategy that he sold to President Trump.
This required that the government establish blocks to wide use of the safe, cheap, effective and FDA approved generic medicines already found to cure COVID in early 2020, namely ivermectin and hydroxychloroquine. Details about these early treatment protocols are given in Pandemic Blunder.
Here is another point made: “A careful viewing of the testimony suggests the line [COVID being 10 times worse than flu] was not a mistake.
Dr. Fauci was specifically asked if COVID was less lethal than H1N1 or SARS. Rather than refer to his own NEJM article saying SARS had a case fatality rate of 9-10 percent (3 to 10 times worse than COVID), Dr. Fauci said, “Absolutely not… the 2009 pandemic of H1N1 was even less lethal than regular flu… this is a really serious problem that we have to take seriously.”
He repeated that COVID’s “mortality is 10 times that [of influenza]” and concluded with, “We have to stay ahead of the game in preventing this.”
This also was a prescient view: ”This was a perfect series of switches: IFR to CFR, voluntary isolation for the sick to mandatory isolation for everyone, two weeks to flatten the curve to indefinite lockdown until there’s a vaccine. (If you think it will be voluntary, you’re not paying attention.)”
Add this to the quest for truth: “A study in France looked at all-cause mortality data from 1946 to 2020 and concluded that ‘SARS-CoV-2 is not an unusually virulent viral respiratory disease pathogen” because there is no significant increase in mortality. Of the deaths in 2020, the study said, ‘unprecedented strict mass quarantine and isolation of both sick and healthy elderly people, together and separately, killed many of them.’”
Here is the article’s correct conclusion: “Sadly, many politicians were duped and went along with the recommendations for lockdowns and masks that followed from Dr. Fauci’s 10-times-deadlier testimony. Don’t expect them to admit their mistakes, either. Perhaps the only thing harder for a politician than telling the whole truth is admitting a mistake.”
What Is The Truth?
If you listen to many experts, you hear this truth based on CDC data: 99.8 or 99.9 percent of people across all ages who get infected by COVID do not die. That means that the IFR overall is .001 or .002. In other words, not so terribly worse than the flu IFR, but it does vary with age.
In September 2020 these CDC age related data were reported:
Updated survival rates and IFR by age group:
0-19: 99.997 percent, IFR .003 percent
20-49: 99.98 percent, IFR .02 percent
50-69: 99.5 percent, IFR .5 percent
70+: 94.6 percent, IFR 5.4 percent
Note that through age 49 the IFR is less than the average for flu of 0.1 percent, but higher for older people. And only for the 70+ group is the IFR more than 10 times greater. In other words, only for the oldest group is what Fauci said in his congressional testimony accurate. What if Fauci had said something in tune with that reality? The vaccine program he pushed should have focused on the elderly, not the entire population.
From the important recent report “COVD-19: Restoring Public Trust During A Global Health Crisis” are age data and COVID CFR [through Feb. 16, 2021]. Note these are Case Facility Rate data, meaning that the figures are very exaggerated because the number of infected are very much higher than the number of cases: probably 100 million more infections than cases. Thus, the total across all age groups of 1.701 percent, [.01701] should be corrected to .289 percent [.00289]; this is about three times higher than the cited flu IFR, not the 10 times higher given by Fauci. And it would be much lower for the less than 70 population.
A very recent article said this: “While estimates of COVID-19’s infection fatality rate (IFR) range from study to study, the expert consensus does indeed place the death rate at below 1 percent for most age groups.” Fauci did indeed overhype COVID for all but the very elderly. This supports the view of the eminent Dr. Peter McCollough that a wise COVID vaccine strategy would have been to target the elderly, not the entire population.
The widely acclaimed medical researcher John P. Ioannidis of Stanford University has examined IFR for COVID in considerable detail,
In October 2020 he said this: “The infection fatality rate of COVID-19 can vary substantially across different locations and this may reflect differences in population age structure and case-mix of infected and deceased patients and other factors. The inferred infection fatality rates tended to be much lower than estimates made earlier in the pandemic.”
At that time, he said:” Across 51 locations, the median COVID-19 infection fatality rate was 0.27 percent (corrected 0.23 percent).” Higher than the Fauci quoted value for the flu (0.1 percent), but not 10 times greater.
A new report from the defense department gives data on 5.6 million fully vaccinated Medicare participants age 65 and older. There were 161,000 recent breakthrough COVID infections and the IFR was 0.021. It noted an IFR for this group of0 .12 (about five times greater) during the March to December 2020 period when there was far less effective hospital care and no mass vaccination.
Both IFRs for elderly Americans are greater than the quoted typical flu value, but far from a very lethal viral infection.
Recently, it was reported that according to CDC work “More than 39 million Americans have been diagnosed with coronavirus infection since the pandemic started in 2020.” Using that figure, that may be too low because only 1.4 million blood samples were tested, together with the current CDC value of about 700,000 COVID fatalities results in an average IFR of 0.018.
Why is 39 million infected people low? Because many medical experts have said that there are probably some 100 million Americans with natural immunity resulting from COVID infection.
The key word to question in what CDC did is “diagnosed.” In other words, people who were tested and found positive. But clearly a large fraction of asymptomatic and mildly symptomatic people did not get tested. So, what if you add 100 million to the 39 million figure and then use that as the denominator, with 700,000 deaths in the numerator, and calculate the IFR?
You get an IFR of 0.005. Not ten times higher than the flu value cited by Fauci in his congressional testimony [actually 3 times higher than the high end of flu IFR values].
Podcaster Jack Murphy, who founded Liminal Order, deduced that because the CDC said there were twice as many people who were infected with COVID, then it automatically meant that the lethality rate must be cut in half, commenting that the virus that had killed 646,000 Americans in the last 19 months is “far less lethal than already known.”
Murder Motivation
To accept the entire argument for a Big Lie it is necessary to explain the motivation for Fauci to intentionally tell the public that the new China virus was extremely lethal. So much worse than seasonal flu. So awful that extreme government action was needed.
It is relevant to note that in January 2017 Fauci warned the Trump administration, in a public talk, that no doubt there would be a “surprise outbreak” of a new infectious disease pandemic. “The thing we’re extraordinarily confident about is that we’re going to see this in the next few years,” he said. He got what he wanted.
Maybe all the talk about a “plandemic” was spot on. And maybe Fauci had insights because he was funding the work at the Wuhan Laboratory to develop extremely toxic viruses.
What Fauci said about high lethality set in motion an onerous set of government actions justified on the basis of protecting public health. Why would anyone want to overstate the lethality of the new COVID-19 virus? It was the only way to use onerous pandemic control and management methods that Fauci favored. It was necessary to set in motion a COVID vaccine program. Most of all, his strategy was used to create very high levels of FEAR in the public so that they would accept his favored government actions.
Understand this. Fauci is not a trained public health expert, nor a trained epidemiologist or virologist. He was a plain physician who over many decades as a top NIH bureaucrat accumulated enormous power. He never did what true public health experts have an ethical obligation to do. That is to tell the public both the positives and negatives of public health policies and actions.
The point is this: By pushing the need for pandemic actions to address a very lethal virus a host of government actions produced so much economic, social and personal hardships and dislocations. And many analyses have concluded that more Americans died from the government actions than from the COVID virus.
Perversely, pandemic public health actions actually harmed public health. But with widespread mainstream media support Fauci got away with everything.
Hundreds of thousands of Americans died unnecessarily. Fauci is guilty of criminally negligent homicide stemming from his initial and very public overstatement of the lethality of the COVID virus. Those who have screamed for his prosecution have a valid case.
With his power he created policies that created data to support this lethality claim. One big action was to create a testing protocol using the PCR technology in ways that created very high case levels. The inventor of that technology said it was inappropriate for diagnosing the viral infection. Millions of COVID cases resulted from running PCR equipment at very high cycle rates [high than 25]. Meanwhile the government never did widespread blood testing to get data for knowing the IFR.
The other major way to keep up public support for pandemic controls was to ensure high numbers of COVID deaths. This was done through directives on how death certificates should be filled out and through financial incentives for hospitals to certify deaths as COVID ones.
Recent analysis that in March 2020 CDC changed guidelines on how death certificates were to be filled out. Different than the procedure used for 17 years prior to this change.
This study found a COVID fatality figure of 161,392 with the new reporting versus 9,684 for the older procedure. There is little doubt that COVID death data, even accounting for some overcounting because of people dying not from any COVID influence, have been too high. This means that IFR data have been too high.
The combination of false high levels of cases and deaths helped maintain public fear of a very lethal virus. That is not correct for nearly all people younger than 70 years old.
Conclusions
To sum up: COVID was intentionally over hyped by Fauci as a very deadly disease to justify the most extreme public health actions. This was the Big Lie. Most valid data now show COVID lethality is similar to that for seasonal flu for the vast majority of people. But accepting that truth would not have justified the array of excessive government actions used for the false pandemic.
Yes, many people have died from COVID, but deaths have been overreported and infections underreported. And most deaths – at least 85% – could have been prevented by using generic medicines, such as ivermectin. There is no doubt that a great many people die with COVID but not FROM COVID, also arguing for a low IFR. At one point CDC said that only 6% of deaths resulted only from COVID, making the IFR much lower than the flu IFR.
Finally, recognizing the true lower IFR for COVID the whole rationale for mass vaccination collapses, especially in view of very high levels of adverse effects and deaths from the vaccines themselves.
Which makes perfect sense if you appreciate that the COVID IFR is now similar to the flu IFR for most people. Especially if you recognize that CDC has found the flu IFR ranged from 0.1 percent (the figure cited by Fauci) to 0.17 percent from 2014 to 2019.
Understanding that the lethality of COVID is far from the terrible picture painted by Fauci at the very beginning of the pandemic is key to weighing the risk/benefit ratio when deciding to get vaccinated. For most people the risk from the vaccine is greater than the benefit. Only the elderly have a good reason to get the shot.
Some 81 percent of COVID deaths are for people over 65. As has been pointed out by many people, the average age of most COVID deaths for elderly victims have been consistently higher than average life expectancy ages.
A new article has made important observations. The main one is that countries with low vaccination levels have been doing better than those with mass vaccination programs, like the US. The results are consistent with a widely accepted understanding that the vaccines do not effectively stem virus infection or transmission. More vaccination equated to more viral spreading.
The new study ended with advice to learn “to live with COVID-19 in the same manner we continue to live a 100 years later with various seasonal alterations of the 1918 Influenza virus.”
Dr. Joel S. Hirschhorn is the author of Pandemic Blunder and many articles on the pandemic, worked on health issues for decades. As a full professor at the University of Wisconsin, Madison, he directed a medical research program between the colleges of engineering and medicine. As a senior official at the Congressional Office of Technology Assessment and the National Governors Association, he directed major studies on health-related subjects; he testified at over 50 US Senate and House hearings and authored hundreds of articles and op-ed articles in major newspapers. He has served as an executive volunteer at a major hospital for more than 10 years. He is a member of the Association of American Physicians and Surgeons, and America’s Frontline Doctors.
October 21, 2021
Posted by aletho |
Deception, Science and Pseudo-Science, Timeless or most popular, War Crimes | Covid-19, NIH, United States |
Leave a comment
In the wake of WMD-liar Curveball’s videotaped confession, Colin Powell was demanding to know why nobody warned him about Curveball’s unreliability. The trouble is, they did.
Can you imagine having an opportunity to address the United Nations Security Council about a matter of great global importance, with all the world’s media watching, and using it to… well, to make shit up – to lie with a straight face, and with a CIA director propped up behind you, I mean to spew one world-class, for-the-record-books stream of bull, to utter nary a breath without a couple of whoppers in it, and to look like you really mean it all? What gall. What an insult to the entire world that would be.
Colin Powell doesn’t have to imagine such a thing. He has to live with it. He did it on February 5, 2003. It’s on videotape.
I tried to ask him about it in the summer of 2004. He was speaking to the Unity Journalists of Color convention in Washington, D.C. The event had been advertised as including questions from the floor, but for some reason that plan was revised. Speakers from the floor were permitted to ask questions of four safe and vetted journalists of color before Powell showed up, and then those four individuals could choose to ask him something related – which of course they did not, in any instance, do.
Bush and Kerry spoke as well. The panel of journalists who asked Bush questions when he showed up had not been properly vetted. Roland Martin of the Chicago Defender had slipped onto it somehow (which won’t happen again!). Martin asked Bush whether he was opposed to preferential college admissions for the kids of alumni and whether he cared more about voting rights in Afghanistan than in Florida. Bush looked like a deer in the headlights, only without the intelligence. He stumbled so badly that the room openly laughed at him.
But the panel that had been assembled to lob softballs at Powell served its purpose well. It was moderated by Gwen Ifill. I asked Ifill (and Powell could watch it later on C-Span if he wanted to) whether Powell had any explanation for the way in which he had relied on the testimony of Saddam Hussein’s son-in-law. He had recited the claims about weapons of mass destruction but carefully left out the part where that same gentleman had testified that all of Iraq’s WMDs had been destroyed. Ifill thanked me, and said nothing. Hillary Clinton was not present and nobody beat me up.
I wonder what Powell would say if someone were to actually ask him that question, even today, or next year, or ten years from now. Someone tells you about a bunch of old weapons and at the same time tells you they’ve been destroyed, and you choose to repeat the part about the weapons and censor the part about their destruction. How would you explain that?
Well, it’s a sin of omission, so ultimately Powell could claim he forgot. “Oh yeah, I meant to say that, but it slipped my mind.”
But how would he explain this:
During his presentation at the United Nations, Powell provided this translation of an intercepted conversation between Iraqi army officers:
“They’re inspecting the ammunition you have, yes.
“Yes.
“For the possibility there are forbidden ammo.
“For the possibility there is by chance forbidden ammo?
“Yes.
“And we sent you a message yesterday to clean out all of the areas, the scrap areas, the abandoned areas. Make sure there is nothing there.”
The incriminating phrases “clean all of the areas” and “Make sure there is nothing there” do not appear in the official State Department translation of the exchange:
“Lt. Colonel: They are inspecting the ammunition you have.
“Colonel: Yes.
“Lt. Col: For the possibility there are forbidden ammo.
“Colonel: Yes?
“Lt. Colonel: For the possibility there is by chance, forbidden ammo.
“Colonel: Yes.
“Lt. Colonel: And we sent you a message to inspect the scrap areas and the abandoned areas.
“Colonel: Yes.”
Powell was writing fictional dialogue. He put those extra lines in there and pretended somebody had said them. Here’s what Bob Woodward said about this in his book “Plan of Attack.”
“[Powell] had decided to add his personal interpretation of the intercepts to rehearsed script, taking them substantially further and casting them in the most negative light. Concerning the intercept about inspecting for the possibility of ‘forbidden ammo,’ Powell took the interpretation further: ‘Clean out all of the areas. . . . Make sure there is nothing there.’ None of this was in the intercept.”
For most of his presentation, Powell wasn’t inventing dialogue, but he was presenting as facts numerous claims that his own staff had warned him were weak and indefensible.
Powell told the UN and the world: “We know that Saddam’s son, Qusay, ordered the removal of all prohibited weapons from Saddam’s numerous palace complexes.” The January 31, 2003, evaluation of Powell’s draft remarks prepared for him by the State Department’s Bureau of Intelligence and Research (“INR”) flagged this claim as “WEAK”.
Regarding alleged Iraqi concealment of key files, Powell said: “key files from military and scientific establishments have been placed in cars that are being driven around the countryside by Iraqi intelligence agents to avoid detection.” The January 31, 2003 INR evaluation flagged this claim as “WEAK” and added “Plausibility open to question.” A Feb. 3, 2003, INR evaluation of a subsequent draft of Powell’s remarks noted:
“Page 4, last bullet, re key files being driven around in cars to avoid inspectors. This claim is highly questionable and promises to be targeted by critics and possibly UN inspection officials as well.” That didn’t stop Colin from stating it as fact and apparently hoping that, even if UN inspectors thought he was a brazen liar, US media outlets wouldn’t tell anyone.
On the issue of biological weapons and dispersal equipment, Powell said: “we know from sources that a missile brigade outside Baghdad was disbursing rocket launchers and warheads containing biological warfare agents to various locations, distributing them to various locations in western Iraq.”
The January 31, 2003, INR evaluation flagged this claim as “WEAK”:
“WEAK. Missiles with biological warheads reportedly dispersed. This would be somewhat true in terms of short-range missiles with conventional warheads, but is questionable in terms of longer-range missiles or biological warheads.”
This claim was again flagged in the February 3, 2003, evaluation of a subsequent draft of Powell’s presentation: “Page 5. first para, claim re missile brigade dispersing rocket launchers and BW warheads. This claim too is highly questionable and might be subjected to criticism by UN inspection officials.”
That didn’t stop Colin. In fact, he brought out visual aids to help with his lying
Powell showed a slide of a satellite photograph of an Iraqi munitions bunker, and lied:
“The two arrows indicate the presence of sure signs that the bunkers are storing chemical munitions . . . [t]he truck you […] see is a signature item. It’s a decontamination vehicle in case something goes wrong.”
The January 31, 2003, INR evaluation flagged this claim as “WEAK” and added: “We support much of this discussion, but we note that decontamination vehicles – cited several times in the text – are water trucks that can have legitimate uses… Iraq has given UNMOVIC what may be a plausible account for this activity – that this was an exercise involving the movement of conventional explosives; presence of a fire safety truck (water truck, which could also be used as a decontamination vehicle) is common in such an event.”
Powell’s own staff had told him the thing was a water truck, but he told the U.N. it was “a signature item…a decontamination vehicle.” The UN was going to need a decontamination vehicle itself by the time Powell finished spewing his lies and disgracing his country.
He just kept piling it on: “UAVs outfitted with spray tanks constitute an ideal method for launching a terrorist attack using biological weapons,” he said.
The January 31, 2003, INR evaluation flagged this statement as “WEAK” and added: “the claim that experts agree UAVs fitted with spray tanks are ‘an ideal method for launching a terrorist attack using biological weapons’ is WEAK.”
In other words, experts did NOT agree with that claim.
Powell kept going, announcing “in mid-December weapons experts at one facility were replaced by Iraqi intelligence agents who were to deceive inspectors about the work that was being done there.”
The January 31, 2003, INR evaluation flagged this claim as “WEAK” and “not credible” and “open to criticism, particularly by the UN inspectorates.”
His staff was warning him that what he planned to say would not be believed by his audience, which would include the people with actual knowledge of the matter.
To Powell that was no matter.
Powell, no doubt figuring he was in deep already, so what did he have to lose, went on to tell the UN: “On orders from Saddam Hussein, Iraqi officials issued a false death certificate for one scientist, and he was sent into hiding.”
The January 31, 2003, INR evaluation flagged this claim as “WEAK” and called it “Not implausible, but UN inspectors might question it. (Note: Draft states it as fact.)”
And Powell stated it as fact. Notice that his staff was not able to say there was any evidence for the claim, but rather that it was “not implausible.” That was the best they could come up with. In other words: “They might buy this one, Sir, but don’t count on it.”
Powell, however, wasn’t satisfied lying about one scientist. He had to have a dozen. He told the United Nations: “A dozen [WMD] experts have been placed under house arrest, not in their own houses, but as a group at one of Saddam Hussein’s guest houses.”
The January 31, 2003, INR evaluation flagged this claim as “WEAK” and “Highly questionable.” This one didn’t even merit a “Not implausible.”
Powell also said: “In the middle of January, experts at one facility that was related to weapons of mass destruction, those experts had been ordered to stay home from work to avoid the inspectors. Workers from other Iraqi military facilities not engaged in elicit weapons projects were to replace the workers who’d been sent home.”
Powell’s staff called this “WEAK,” with “Plausibility open to question.”
All of this stuff sounded plausible enough to viewers of Fox, CNN, and MSNBC. And that, we can see now, was what interested Colin. But it must have sounded highly implausible to the U.N. inspectors. Here was a guy who had not been with them on any of their inspections coming in to tell them what had happened.
We know from Scott Ritter, who led many UNSCOM inspections in Iraq, that U.S. inspectors had used the access that the inspection process afforded them to spy for, and to set up means of data collection for, the CIA. So there was some plausibility to the idea that an American could come back to the UN and inform the UN what had really happened on its inspections.
Yet, repeatedly, Powell’s staff warned him that the specific claims he wanted to make were not going to even sound plausible. They will be recorded by history more simply as blatant lies.
The examples of Powell’s lying listed above are taken from an extensive report released by Congressman John Conyers: “The Constitution in Crisis; The Downing Street Minutes and Deception, Manipulation, Torture, Retribution, and Coverups in the Iraq War.”
October 20, 2021
Posted by aletho |
Deception, Fake News, Mainstream Media, Warmongering, Timeless or most popular | Iraq, United States |
Leave a comment
Two bombings in as many weeks causing hundreds of casualties at Shia mosques in Afghanistan raises fears of a sectarian war erupting in the Central Asian country.
The surge in atrocities comes at a challenging time for the new Taliban government which is trying to establish international recognition as the legitimate authorities of Afghanistan. Much of the Taliban claim to rule relies on assurances that it would bring stability and security following the historic withdrawal of all US troops on August 31.
The Taliban – like the majority of Afghanistan’s 38 million population – is mainly of Sunni muslim faith. It has every incentive, however, to protect the lives of the minority Shia community. The bomb massacres at the two mosques in the northern city of Kunduz on October 8 and Kandahar, in southern Afghanistan, on October 15 were claimed by the ISIS affiliate group, Islamic State-Khorasan Province (ISIS-K).
This same group carried out the attack at Kabul airport on August 28 killing 13 US troops and over 160 Afghan civilians. It is officially designated as an enemy by Washington as well as by the Taliban. But is there a case of “my enemy’s enemy might be useful”?
The Taliban have vowed to root out ISIS-K and other Al-Qaeda-affiliated extremists. They all share an ultra-conservative profession of Sunni Islam, but it is not in the interests of the Taliban to see Afghanistan descend into a sectarian war when it is trying to mobilize national reconstruction after 20 years of war against the United States and other occupying NATO forces.
ISIS-K and other Al-Qaeda affiliates are also known by other terms, including Daesh, Takfiri or Wahhabi. They view Shia as heretics and liable to be put to death. Their cult-like theology put them in a different category from the Taliban who are rational players committed to national development.
But the surge in sectarian killings in Afghanistan has bigger geopolitical connotations.
A conference in Moscow planned for October 20 will bring together regional countries to chart a way forward for Afghanistan’s reconstruction. Attending the summit will be senior Chinese government officials and Taliban representatives. While the group is listed as a terrorist organization in Russia and banned, its delegation has been invited to Moscow to discuss the situation in the region.
Beijing has offered investment of billions of dollars to help Afghanistan recover from years of war devastation. The Taliban, for their part, have welcomed the “fraternal” contribution from China.
All regional countries have much to gain if Afghanistan can harness stability and economic development. The country’s prodigious mineral wealth and its strategic geographical location for transport and energy links make Afghanistan a potential linchpin in China’s Belt and Road Initiative and more generally Eurasian economic integration.
Russian President Vladimir Putin has expressed deep concern about the growing presence of terrorists in Afghanistan and a potential spread of extremism to the neighboring former Soviet republics.
China has also legitimate security concerts over threats posed by thousands of Uighur Islamists who have been engaged in terrorist violence in Afghanistan and Syria. Beijing has been assured by the Taliban that Kabul will not provide a safe haven for Uighur terrorists to launch attacks into its neighboring western province of Xinjiang.
In the first Shia mosque bombing on October 8, ISIS-K reportedly named one of its suicide bombers as a Uighur member.
The geopolitical significance seems clear. The surge in violence in Afghanistan is aimed at preventing the country from creating a stable government and to stifle a postwar reconstruction from cooperation with regional partners, in particular China.
In contrast to the overtures from Beijing, Moscow, Iran, Pakistan and others, the United States has sought to throw obstacles in the way of Afghanistan’s new Taliban government. Of course, revenge over Washington’s shameful retreat from the country is to be expected.
But Washington’s freezing of Afghanistan’s foreign reserves estimated at $10 billion as well as cutting off international finance from the World Bank and International Monetary Fund at a time when the country is facing an acute humanitarian crisis goes beyond vengeance. There seems to be a calculated agenda to consign Afghanistan to a fate of permanent failed state and to ensure that it won’t become a thriving part of the Eurasian model. In short, vindictive sabotage.
This then begs the question of whether the US has some clandestine role in supporting ISIS-K and its sectarian war agenda?
Speaking about the Shia mosque bombings, Iran’s President Ebrahim Raesi has openly accused the United States of sponsoring the growth of Daesh terror groups in Afghanistan with the purpose of inciting sectarian conflict.
Hezbollah leader Sayyed Hassan Nasrallah said the atrocities demonstrated that the objective of ISIS-K was to embroil Afghanistan in religious civil war and he also accused the American CIA as being responsible for the bloodshed. He claimed that the US has transported Daesh militants from Syria and Iraq to Afghanistan for a new phase of dirty war.
The collusion between US military intelligence and Islamist extremists has been spotlighted elsewhere. Former Afghan President Hamid Karzai claimed in 2017 that the Pentagon had assisted the infiltration of his country with ISIS brigades.
In 2018, the Russian government said it recorded transport of ISIS militants across Afghanistan with the use of “unidentified helicopters”.
We also know that massive supplies of weaponry and finances were funneled by the Pentagon to jihadi terror groups in Syria under the guise of arming “moderate rebels”.
During its occupation of Iraq, the US is documented to have used a counterinsurgency policy known as the Salvador Option in which pseudo-gangs led by American special forces deliberately incited sectarian violence as a way to manage political interests. The British authorities deployed similar dirty war tactics during the conflict in Northern Ireland and in other colonial-era campaigns.
With all of these things in view, it bears asking the question: is sectarian war in Afghanistan being fomented by powers who do not want to see the country prospering in a peaceful and stable Eurasian region led by China and Russia?
Finian Cunningham is an award-winning journalist. For over 25 years, he worked as a sub-editor and writer for The Mirror, Irish Times, Irish Independent and Britain’s Independent, among others.
October 20, 2021
Posted by aletho |
Deception, False Flag Terrorism, War Crimes | Afghanistan, United States |
Leave a comment
Former MI6 man Christipher Steele is the subject of an obscenely vapid ABC documentary, with a contemptible interview by George Stephanopoulos that’s so deferential it’s like watching a first date that should be an interrogation.
Just as MI6 super spy James Bond is back in theatres with No Time to Die, former MI6 agent Christopher Steele is back in the spotlight with the story that refuses to die, in an ABC ‘documentary’ titled Out of the Shadows: The Man Behind the Steele Dossier, now streaming on Hulu.
Steele came to fame as the shadowy force behind the Steele Dossier, the document which was the spark that lit the Trump-Russia collusion fire that was doused in gasoline by obsessive partisan media coverage and numerous, spurious government investigations for the last five years. The dossier claimed that then-candidate Trump was “colluding with Moscow” and that those devious Russians had “kompromat” on Trump in the golden form of a “pee tape.”
Steele’s “coming out of the shadows” consists of him sitting down with George Stephanopoulos and having a cuddle session on fancy sofas in a posh apartment.
Stephanopoulos is the perfect choice for the softball interview since he and Steele have a lot in common – they’ve both worked for the Clintons. Stephanopoulos as adviser to President Bill Clinton and Steele as de facto dirt-finder for Hillary Clinton’s presidential campaign.
ABC tried to stretch the excruciatingly thin gruel of this supposed ‘interview’ into an hour-long documentary by adding talking heads from their own newsroom. They failed, as the end result is a one-hour show that is hilariously shallow and vapid, even by ABC News standards.
Out of the Shadows spends considerably more time rehashing the “history” of Russia, Vladimir Putin and Trump than it does actually talking to Steele. Russia is deemed “a rogue state virus spreading westward with its villainy,” Putin a “KGB killer,” and Trump a “threat to American democracy.” In other words, it’s standard establishment media talking points.
Steele’s background is somewhat explored, but being the ever-diligent super spy that he is, Steele never explicitly states that he worked for MI6. I guess he doesn’t want to blow his cover.
What Steele actually says in this interview is of strikingly minimal impact. Thanks to Stephanopoulos’ anti-journalistic, anti-adversarial, deferential approach, no new ground is broken.
It’s well-known that Steele didn’t just compile the dossier, he actively pushed it to media outlets, in effect working to try and scupper Trump’s election campaign. The fact that he was ostensibly working for Democrats at the time certainly makes it appear as if he was a part of a wider disinformation/interference operation, but of course that’s a topic Stephanopoulos whistles past in this patty-cake chat.
Steele admits to no wrongdoing or error, despite the U.S. intelligence agencies “eviscerating” his findings after thorough investigation, and the FBI labelling him “untrustworthy.”
The issue of the “sources” Steele uses doesn’t get the attention it deserves either, as it’s reported that he only used one “key collector,” but Steele is quick to make clear it was “one collector” but not “one source.” That seems like a distinction without a difference.
As the documentary reports, that one collector was not a person in Moscow, but actually someone in Washington DC whose name is not revealed. The Justice Department Inspector General Michael Horowitz reported this person claimed that the information being given to Steele was “word of mouth and hearsay.” In other words, Steele was acting less as an intelligence expert seeking truth with his dossier than he was being a gossip columnist spreading rumor and innuendo.
Steele’s declaration, “I stand by the work we did, the sources we had, and the professionalism we applied to it,” is as devoid of substance as the rest of the interview.
The most damning aspect comes toward the end, and even that is soft pedaled, when Stephanopoulos asks Steele about both the dossier’s allegation that Trump counsel Michael Cohen went to Prague to meet with Russian intelligence and about the pee tape.
Cohen denies a Prague meeting ever took place, and since he has now flipped against Trump, one would assume he’s telling the truth. But Steele’s resolve remains, as he conjures up a wild scenario where Cohen is still lying because he wants to avoid being charged with treason.
Stephanopoulos, of course, lets this utter lunacy pass almost without notice. He could’ve asked Steele how exactly Cohen got to Prague, since his passport shows no travel to the Czech Republic. Or pressed Steele to provide details or at least a passable explanation for how that meeting could possibly have taken place? But he didn’t, he just smiled and continued playing footsie with Steele.
The ‘pee tape’ is the most salacious accusation in the dossier, and despite it never surfacing and no evidence it exists, Steele still stands by the claim…sort of. He says that the tape “probably does” exist but that he wouldn’t “put 100% certainty on it.”
When Stephanopoulos asks why the tape hasn’t come out, Steele replies that “it hasn’t needed to be released…because I think the Russians felt they’d got pretty good value out of Donald Trump when he was president.”
Look, I loathe Trump, always have and always will, but this sounds like the ravings of someone deeply infected with a ferocious case of Trump Derangement Syndrome, which is maybe why he is still taken seriously by the equally afflicted establishment media.
The more you know about Steele, the more readily apparent it becomes that he’s an absolute charlatan and bullshit artist masquerading as a serious intelligence expert. He’s no James Bond, he’s not even George Smiley. He’s more like a cross between Mr. Bean and Inspector Clouseau, who should, like this vacant and vacuous interview/documentary, be relentlessly ridiculed and righteously disrespected.
October 20, 2021
Posted by aletho |
Deception, Film Review | Hillary Clinton, MI6, UK, United States |
Leave a comment
You may have noticed the media cycle has subtly begun for next week’s House Oversight Committee climate change show-trial, as energy crises unfold worldwide and President Biden prepares to take 13 Cabinet members and no grants of legislative authority from Congress supporting his “climate” agenda to the annual “Conference of the Parties” in Glasgow (where, like President Obama before him, he will claim that while legislative authority would be nice, in its absence he will do what he wants anyway — not, in fact, how these things are supposed to work).
With that backdrop, see the attached opening trial brief and declarations of Lindzen, Happer, Horner and Walter which were filed on Friday in open records litigation in Los Angeles. The subject of the records at issue is the role of academia (specifically, plaintiffs’ tort bar consultants among UCLA Law faculty) in the climate litigation industry, and what they boast of to at least one major donor behind these efforts. You may recall one such email by UCLA Law faculty describing the AGs, activists, “prospective funders” and faculty gathering at the “secret meeting at Harvard” was “about going after climate denialism—along with a bunch of state and local prosecutors nationwide”.
As context to the Regents’ behavior in this matter, the trial brief and declarations detail the climate industry’s Enron origins, and the role of academics supporting the plaintiffs’ effort (also noted is the spate of briefings of federal judges by the plaintiffs’ side, initiated after Judge Alsup dismissed litigation against oil companies in the Northern District of California, which briefings also trace back to UCLA faculty).
In another footnote, early in the attached Horner Declaration, you’ll find timely reference to a 1999 email warning of the consequences of seeking to rig the economics of the energy industry in the name of “global warming” (later, climate change). Cue the past few weeks’ headlines from around the world manifesting just those consequences:
Maybe Enron can dodge the macro problem and have our micro benefits, but then again I have to think that a politicized international energy market for any reason will create as much or more downside than upside. (April 1, 1999 memo to Lay)
It is difficult to escape the conclusion that, as cynical as they were about it, Enron Knew.… a couple very important things*. Despite being the company that had bet the most on greenhouse warming and most wanted the alarmism to take root, Enron also knew the systemic economic risks from pushing the climate agenda. But, in the pursuit to “make [itself] rich,” plowed ahead. Others followed in Enron’s footsteps, with far too much success, and we all are now facing the consequences.
* PS See here for the other key point Enron knew, something that puts the lie to the very foundation underpinning the ongoing climate litigation tsunami — Enron knew and bitterly debated the uncertainties of the theory underpinning the climate agenda.
The excerpts from and links to emails and memos debunk the claims that, as one piece put it, “The Utilities Knew, Exxon Knew, Shell Knew, They All Knew” of catastrophic man-made global warming in the 1970s, or 1980s… showing there was instead intense and often bitter internal fighting over the risks of designing business plans around the theory when it was so laden with uncertainty. That was in the late 1990s.
10-15-21-Opening-Trial-Brief-PetitionerDownload
Jt-Evidentiary RecordDownload
October 19, 2021
Posted by aletho |
Corruption, Deception, Economics, Science and Pseudo-Science, Timeless or most popular | United States |
Leave a comment
Joining me today is Ben Swann, here to discuss how he has been fighting back against the COVID-19 tyranny, and the actions he is taking to create a space where the truth can be heard. And no discussion with Ben would be complete without a back and forth about the many different ways in which COVID-19 itself is a deception.
Podcast: Play in new window | Download | Embed
Subscribe: Apple Podcasts | Email |
(https://www.rokfin.com/TLAVagabond)
(https://odysee.com/@TLAVagabond:5)
(https://www.bitchute.com/channel/24yVcta8zEjY/)
October 19, 2021
Posted by aletho |
Civil Liberties, Deception, Mainstream Media, Warmongering, Science and Pseudo-Science, Timeless or most popular, Video | Covid-19, COVID-19 Vaccine, Human rights |
Leave a comment
At long last, thanks to the testimony of a Palestinian held at Guantanamo Bay, someone might finally be held accountable for the gross human rights violations the agency inflicted on so many with such impunity for years.
In a landmark move, the Biden administration has advised the US Supreme Court that Abu Zubaydah, a Palestinian man who has been in US custody for nearly 20 years, can provide limited testimony for use in a Polish criminal investigation into his torture at a CIA “black site” in that country.
Acting Solicitor General Brian Fletcher has stated that Zubaydah’s testimony will be subject to US national security review, and while he would be permitted to describe his treatment while in CIA custody, “information that could prejudice the security interests” of Washington could be redacted.
Nonetheless, even such truncated scope for disclosure is a seismic development, for Zubaydah has been held incommunicado since his March 2002 capture in Pakistan. Indeed, his CIA torturers specifically sought “reasonable assurances that [Zubaydah] will remain in isolation and incommunicado for the remainder of his life,” in order that their criminal maltreatment remained secret, and they were insulated from prosecution. Such assurances were eagerly granted by Washington.
“There is a fairly unanimous sentiment within [headquarters] that [Zubaydah] will never be placed in a situation where [he] has any significant contact with others and/or has the opportunity to be released,” a classified memo declared. “While it is difficult to discuss specifics at this point, all major players are in concurrence that [Zubaydah] should remain incommunicado for the remainder of his life.”
So it was that Zubaydah was moved around an assortment of CIA black sites for four years, and was viciously tortured every step of the way. Among other gruesome acts, he was repeatedly waterboarded, locked in a tiny coffin-like box for hundreds of hours, hung from hooks, denied sleep, and forced to remain in ‘stress positions’ for extended periods – resulting in permanent brain damage and the loss of his left eye – in an attempt to extract information that he didn’t actually possess.
Zubaydah’s arrest was hailed as a major coup at the time, with US officials branding him a major Al-Qaeda financier, a key link between the group’s leader Osama bin Laden and its overseas operational cells, the manager of the camp in Afghanistan where the 9/11 hijackers were purportedly trained, a central figure in every major Al-Qaeda terrorist operation, and “engaged in ongoing terrorism planning against US interests.”
None of this was true. The basis for these lurid, false claims was a CIA psychological assessment of Zubaydah, which was primarily concerned with justifying his vicious abuse – it falsely stated, for example, that he had written Al-Qaeda’s manual on resisting interrogation, arguing that, due to his “incredibly strong resolve, expertise in civilian warfare [and] resistance to interrogation techniques,” torture was the only means by which information could be extracted from him.
Before this abuse commenced, Zubaydah was interviewed by FBI operative Ali Soufan. While he was recovering from life-threatening injuries incurred during his capture by Pakistani intelligence – he had been shot in the thigh, testicles, and stomach with an assault rifle – Soufan treated him well, building rapport and trust. This light-handed approach prompted Zubaydah to open up – he named Khalid Sheikh Mohammed as the “mastermind” of the 9/11 attacks, and described rumors of a “dirty bomb” plot being planned by a US citizen.
This information may not even have been accurate, however. The FBI’s top Al-Qaeda analyst, Dan Coleman, describes Zubaydah as a mere “safehouse keeper” with severe mental problems, who “claimed to know more about Al-Qaeda and its inner workings than he really did.” The torture he suffered no doubt played a pivotal role in prompting him to make such claims.Khalid Sheikh Mohammed was subsequently waterboarded 183 times, and admitted to all manner of grave crimes – including planning to blow up a building that didn’t even exist at the time of his capture.
In any event, Soufan was confident Zubaydah had no more secrets to tell, but the CIA claimed to be unconvinced – after all, Langley paid its Pakistani counterparts $10 million for him, and needed a greater return on that investment. When the torture finally stopped, with no further intelligence gathered, the agency was forced to conclude Soufan had been right all along.
As the Senate Select Committee report later found, the CIA still considered its tactics a success, to be “used as a template for future interrogation of high-value captives,” on the basis that such hideous treatment had “confirmed Zubaydah did not possess the intelligence” it erroneously assessed him to have.
That report is classified today, although Zabuydah’s name appears a total of 1,343 times in a publicly released executive summary and accompanying documents. It notes that the CIA frequently had trouble distinguishing “detainees who had information but were successfully resisting interrogation from those who did not actually have the information,” and at least 26 individuals had been wrongfully held by the agency.
This included an “intellectually challenged” man whose detention was used as leverage to force a family member to provide information, two former CIA sources, and two individuals whom the CIA had assessed to be connected to Al-Qaeda based solely on information fabricated by another detainee who’d been subjected to ‘enhanced interrogation’ techniques. Detainees often remained in custody at black sites for months after the agency determined there was no reason to keep them.
Other shocking excerpts reveal that a number of CIA personnel attached to the detention and interrogation program had on their personal files “notable derogatory information” that called into question “their eligibility for employment, their access to classified information, and their participation in CIA interrogation activities.” Among them were officers who, “among other issues, had engaged in inappropriate detainee interrogations, had workplace anger management issues, and had reportedly admitted to sexual assault.”
The agency seemed assured of its immunity from prosecution for its crimes, with several detainees having been informed they would never get out of CIA custody alive. One was told they’d be leaving only “in a coffin-shaped box,” while another was warned “we can never let the world know what I have done to you.” CIA officers also threatened several detainees with harm to their families should any details of their maltreatment be made public – this included telling one that their children’s lives would be at risk, a second that his mother would be sexually abused, and a third that his mother’s throat would be cut.
Since September 2006, Zubaydah has been held at Guantanamo Bay, despite the CIA having acknowledged that he wasn’t even a member of Al-Qaeda, let alone a significant figure within the group. The scars from his time in “black site” detention remain writ large today, with virtually perpetual headaches, an “excruciating sensitivity to sounds,” frequent seizures, and an inability to recall his own father’s name.
Still, the Supreme Court permitting him to make limited disclosures about his experiences is an encouraging sign that the invocation of “state secrecy privilege” to block disclosure of key evidence related to the CIA’s global post-9/11 torture program may no longer be a viable get-out for officials. This, in turn, raises the prospect that, at long last, someone might finally be held accountable for the gross human rights violations the agency and its assorted contractors inflicted on so many with such impunity for so long.
Kit Klarenberg is an investigative journalist exploring the role of intelligence services in shaping politics and perceptions.
October 18, 2021
Posted by aletho |
Deception, False Flag Terrorism, Subjugation - Torture | CIA, Human rights, United States |
Leave a comment
FBI’s involvement in 6 January riots could be bigger than the mainstream media have recently acknowledged, according to US political commentator Julie Kelly. She wonders whether the DC incident was part of the agency’s Operation Cold Snap against Whitmer kidnapping case plotters, unveiled by BuzzFeed in July 2021.
The US Department of Justice announced on 8 October 2020 that six men had been arrested and charged federally with conspiring to kidnap the Michigan Governor Gretchen Whitmer. The DoJ’s press release said that “through confidential sources, undercover agents, and clandestine recordings, law enforcement learned particular individuals were planning to kidnap the Governor and acting in furtherance of that plan”.
However, on 12 July 2021, BuzzFeed revealed that the FBI allegedly used at least 12 informants in the Whitmer kidnapping case, who not only kept the agency in the loop, but were allegedly used by the FBI to “induce or persuade” the defendants to go along with the violent scheme. The agency’s operation was called Cold Snap.
According to BuzzFeed, the FBI assets “had a hand in nearly every aspect of the alleged plot, starting with its inception”.
One of those infiltrators, Stephen Robeson, 57, helped organise a series of meetings around the country “enthusiastically pushing people he knew to attend” and even “paid for some hotel rooms and food as an incentive to get people to come”. At these meetings many of the alleged plotters first met one another.
Another informant, an Iraq War veteran, known as “Big Dan”, rose to the second-in-command of the group, encouraged members to work with other potential suspects and paid for their transportation to meetings. He allegedly urged the supposed mastermind of the Whitmer kidnapping plot to carry his plan out, and then laid the trap that eventually led to the arrest.
The defendants in the kidnapping case later accused the FBI of “entrapment”, saying the infiltrators encouraged the group and even led military-style trainings for the plot.
All these meetings and training were captured on film by FBI agents “to produce major headlines as early voting was underway in the crucial swing state of Michigan”, argued Julie Kelly in her op-ed for American Greatness (AG).
She noted that the blame for the plot was pinned on then-President Donald Trump. “There is a through line from President Trump’s dog whistles and tolerance of hate, vengeance, and lawlessness to plots such as this one”, then-presidential candidate Joe Biden claimed on 8 October 2020.
“It also appears that the Whitmer operation was only part of the FBI’s overall plan to infiltrate and perhaps direct the conduct of unsuspecting ‘militia’ men in 2020”, Kelly continued, stressing that the agency’s operation was not limited to Michigan but was a “multi-state” probe.
Citing a testimony by one of the lead FBI special agents in the Whitmer case, the political commentator highlighted that there had been other FBI “domestic terrorism” investigations in Baltimore and Milwaukee and Cincinnati and Indiana involving other militia members.
According to Kelly, “Big Dan” was also ordered by the FBI to convince a man in Virginia to participate in a plan against Virginia Governor Ralph Northam. “Just like in the Whitmer plot, ‘Big Dan’ advised his target how to build an explosive device and urged him to attend a training camp in Wisconsin”, she noted.
The AG senior contributor insists that “it’s hard to imagine Operation Cold Snap ended with the arrest of Whitmer’s would-be abductors”. According to her, the 6 January riot, attended by several groups of right-wing militia, could have been a continuation of the same FBI op, this time in Washington, DC.
She suggested that it was hardly a coincidence that FBI chief Christopher Wray promoted Steven M. D’Antuono, special agent in charge of the Detroit Field Office, Michigan, to head of the DC FBI Field office on 13 October 2020 – just five days after the arrest of kidnap plotters and ahead of the November 2020 elections. Apparently, D’Antuono was seen as a man for the job, according to the political commentator.
Citing a New York Times article unveiling FBI infiltrators’ role in 6 January riots, Kelly presumed that the NYT report could only be seen as the start of a slow drip of information about the extent” of the agency’s role in the Capitol breach.
“It’s only a matter of time before we learn how many “Big Dans” or Stephen Robesons were part of January 6,” Kelly believes.
October 18, 2021
Posted by aletho |
Civil Liberties, Deception | FBI, United States |
Leave a comment
“It is now apparent that these products in the blood stream are toxic to humans. An immediate halt to the vaccination programme is required while an independent safety analysis is undertaken to investigate the full extent of the harms, which the UK Yellow Card data suggest includes thromboembolism, multi-system inflammatory disease, immune suppression, autoimmunity and anaphylaxis, as well as Antibody Dependent Enhancement (ADE).” Tess Lawrie, Evidence-Based Medicine Consultancy
“For we wrestle not against flesh and blood, but against the rulers of the darkness of this world, against spiritual wickedness in high places.” Ephesians 6:12
Question – Have the mRNA vaccines been tested on animals?
Answer – Yes, they have.
Question – Were the animal trials successful?
Answer – Yes and no.
Yes, the experiments on mice showed that a low dose of the vaccine induces a robust antibody response to the infection.
But, no, the antibodies were not able to attack the spike protein from a different strain of the virus.
Question – I’m not sure what that means? Do you mean that the vaccine DOES provide some limited protection from the original (Wuhan) virus, but does not necessarily provide protection from the variants?
Answer – That’s right, but it’s a bit more complicated than that because– as the virus changes — the antibodies that helped to fight the original virus can actually enhance the “infectivity” of the variant. In other words, vaccine-generated antibodies can switch-sides and increase the severity of the illness. Simply put, they can make you sicker or kill you. Scientists have known this for a long time. Check out this clip from a 2005 research paper:
“A jab against one strain might worsen infection with others….
In the.. study, Gary Nabel of the National Institute of Allergy and Infectious Diseases.. injected mice with spike protein from a SARS virus taken from a human patient infected in early 2003. They then collected the antibodies the animals produced.
In lab experiments, they showed that these antibodies were unable to attack spike protein from a different strain of SARS, isolated from a patient infected in late 2003…. The team next tested whether the antibodies would attack spike proteins from two SARS strains isolated from civets, from which the virus is thought to have originally jumped into humans. In this case, they found hints that the antibodies actually boosted the ability of the virus to infect cells. …
The results show that the virus changes over time, so that a strain that crops up in one outbreak might be quite different from that in a later outbreak. “This virus is not standing still and we need to take this into account,” Nabel says.
This raises the prospect that a vaccine against one strain of SARS virus could prove ineffective against others. Worse, a jab against one strain might even aggravate an infection with SARS virus from civets or another species. “It’s obviously a concern,” Nabel says..
This would not be the first case where exposure to one strain of a virus can worsen infection with another.” (“Caution raised over SARS vaccine”, Nature )
Question – I’m still confused. Can you summarize what they’re saying?
Answer – Sure. They’re saying that scientists have known for nearly two decades that vaccines narrowly aimed at just one protein are bound to fail. They’re saying that the spike protein is highly-adaptable and capable of changing its shape to survive. They’re saying that vaccines aimed at the spike protein will inevitably produce variants that evade vaccine-generated antibodies. They’re saying that by narrowing the vaccine’s focus to the spike protein alone, the drug companies have ensured that previously helpful antibodies will do an about-face, allow the virus to enter healthy cells, replicate at will, and cause sickness or death. They are saying that the current crop of vaccines is in fact perpetuating the pandemic. And–since the science has been clear for the last 16 years– we can add one more observation to the list, that is, that the current approach to mass vaccination is neither haphazard, slapdash or random. It is intentional. The vaccination campaign managers are deliberately ignoring the science in order to sustain a permanent state of crisis. Science is being manipulated to achieve a political objective.
Question – I think you’re exaggerating, but I’d like to get back to the animal trials instead of arguing politics. As you probably know, the reports in the media do not square with your analysis, in fact, all of the articles in the MSM say the animal trials were a rousing success. Here’s a short blurb that I found today that confirms what I’ve been saying:
“… vaccination of nonhuman primates with the mRNA vaccine induced robust SARS-CoV-2 neutralizing activity and notably, rapid protection in the upper and lower airways….” (Covid-19, NIH.gov)
Question – Are you suggesting the authors are lying?
Answer – No, they are not lying. They’re just not telling you the whole truth, and you need to know the whole truth so you can make an informed decision. The vaccines DO provide some (temporary) protection. We don’t dispute that. They also trigger a strong immune response. We don’t dispute that either. But what difference does it make? Let me explain: Let’s say, you have a really bad head cold so you take a new medication that you think will relieve the pain. And–sure enough– an hour after taking the pills– Presto — your congestion and headache are completely gone. That’s fantastic, right? Wrong, because what you fail to realize is that the medication is laced with slow-acting strychnine that kills you three days later. Do you still think it was a good idea to take the medication?
Of course, not. And the same rule applies to these vaccines which do, in fact, boost your antibodies and provide some fleeting “immunity”. But they can also kill you. Don’t you think that should be factored in to your decision? Keep in mind, people have died 3, 4, 5 weeks after inoculation without any prior warning. Many of them might have even been bursting with antibodies, but they’re still dead. Can you see the problem?
Question – Okay, but there’s still this matter about the animal trials. The media says that the drug companies performed the animal trials and they were successful. Do you disagree with that?
Answer – They were not successful and the “fact checkers” that were hired to discredit vaccine critics like me, have deliberately mischaracterized what happened in the trials. For example, here’s a typical “fact checker” article titled “COVID-19 vaccines did not skip animal trials because of animal deaths” by Reuters. Here’s an excerpt:
“Posts claiming that COVID-19 vaccine producers skipped animal trials due to the animals in those trials dying are false. Pfizer-BioNTech, Moderna and Johnson & Johnson, which have been granted emergency authorization use by the Food and Drug Administration (FDA) in the United States, all conducted animal trials and had no significant safety concerns to report.”
Sounds reassuring, right? But then they say:
“Due to time constraints and the urgency to find a vaccine for COVID-19, Moderna and Pfizer did receive approval to run animal testing and early trials on humans at the same time, as opposed to fully completing animal trials before moving on to human trials. This, however, does not mean animal trials were skipped or that the safety of the vaccines were compromised.”
Let me see if I got this straight: The drug companies were in such a hurry that they conducted their minimalist animal trials at the same time as their human trials (which is unprecedented) and then rushed the results to the FDA so they could be rubber stamped and waved through under the Emergency Use Authority?
Is that how it went down?
Yes, it is.
But if they were rushed through in a couple months, then the “fact checkers” are tacitly admitting that there is no long-term safety data. And there IS no long-term safety data, nor is there any attempt to disprove the research from the earlier trials where the ferrets, mice and other animals died following injection of mRNA vaccines. They don’t deny it, they just ignore it as if sweeping it under the rug will make it all go away. Here’s a clip from the research paper that Reuters refers to in its article:
“We demonstrate that the candidate vaccines… respectively—induce strong antigen-specific immune responses in mice and macaques….Both (vaccines) protected 2–4-year-old macaques from challenge with infectious SARS-CoV-2, and there was reduced detection of viral RNA in immunized macaques as compared to those that received saline.” (Note–We’ve already acknowledged that the vaccines do produce a strong immune response. Here’s more:)
“Neutralizing GMTs declined by day 56 (35 days after dose 2), consistent with the contraction phase; however, they remained well above the GMT of the human sera panel. The duration of the study was not long enough to assess the rate of decline during the plateau phase of the antibody response.” (“BNT162b vaccines protect rhesus macaques from SARS-CoV-2”, Nature )
Can you see what’s going on? The trial was only 56 days-long, in fact, none of the animal trials exceeded 56 days. Think about that for a minute. The reason the animals died in prior trials is because they were exposed to a mutated version of the (wild) virus that eventually killed them. That’s how ADE (antibody-dependent enhancement) works. It doesn’t happen overnight and it doesn’t happen in 56 days. It takes much longer than that for a mutated version of the virus to emerge and reinfect the host. The drug companies know that. They’re not stupid. So the fact that the animals mounted a strong immune response is completely irrelevant. We KNOW they mounted a strong immune response. We also know they died some months later when a different strain of the virus emerged. Bottom line: The production of antibodies does not mean a drug is safe.
The obvious purpose of the trials was to get the vaccines over the finish-line before anyone figured out what was going on. It’s the same reason why the drug companies “unblinded” their human trials after the vaccines got the green light from the FDA. Shortly after the trials were concluded, the people in the placebo arm were allowed to get vaccinated.
Why would they do that? Why would they vaccinate the people who willingly allowed themselves to be guinea pigs for the sake of public health, only to vaccinate them shortly after, thus, eliminating any chance of finding out what the long-term safety issues might be? It makes no sense, does it?
Take a look at this short clip from the British Medical Journal whose scientists are equally bewildered:
“The (drug) companies say they have an ethical obligation to unblind volunteers so they can receive the vaccine. But some experts are concerned about a “disastrous” loss of critical information if volunteers on a trial’s placebo arm are unblinded…
Although the FDA has granted the vaccines emergency use authorization, to get full license approval two years of follow-up data are needed. The data are now likely to be scanty and less reliable given that the trials are effectively being unblinded.
Consumer representative Sheldon Toubman, a lawyer and FDA advisory panel member, said that Pfizer and BioNTech had not proved that their vaccine prevents severe covid-19. “The FDA says all we can do is suggest protection from severe covid disease; we need to know that it does that,” he said.
He countered claims, based on experience with other vaccines, six weeks of follow-up was long enough to detect safety signals. Six weeks may not be long enough for this entirely new type of “untested” [mRNA] vaccine, Toubman said.
Goodman wants all companies to be held to the same standard and says they should not be allowed to make up their own rules about unblinding. He told The BMJ that, while he was “very optimistic” about the vaccines, “blowing up the trials” by allowing unblinding “will set a de facto standard for all vaccine trials to come.” And that, he said, “is dangerous.”
(“Covid-19: Should vaccine trials be unblinded?” The British Medical Journal )
Do you like his choice of words: “blowing up the trials”? Do you think it is a fair description of what the drug companies did?
Yes, it is.
And what possible motive would the drug companies have to blow up the trials? I can see only two possibilities:
- They think their vaccine is so terrific, it will save the lives of many of the people in the placebo group.
- They expect a high percentage of the people in the vaccine group to get either severely sick or die, so they want to hide the evidence of vaccine-linked injury.
Which is it?
You know the answer. Everyone watching this farce knows the answer.
Question – Okay, so let’s cut to the chase: Are the vaccines are safe or not?
No, they are not safe. The way we decide whether a drug is safe or not is by putting it through a rigorous process of testing and clinical trials. After the testing, the data is passed on to physicians, statisticians, chemists, pharmacologists, and other scientists who review the data and make their recommendations or criticisms. That didn’t happen with the Covid vaccines, in fact, all the normal standards and protocols were suspended in the name of “urgency”. But many believe that the “urgency” was manufactured to push through vaccines that would never have been approved on their own merits. All you have to do is look through the vaccine injury data (VAERS) and you’ll see this is the most lethal medical intervention of all time and, yet, the public health experts, the media and the government keep crowing that they’re “safe and effective”. It’s nonsense and the drug companies know it’s nonsense which is why they reject all liability for the people that are going to be killed by these “poison-death shots.”
Do you know what goes on inside your body after you are injected with one of these “gene based” vaccines?
Once the vaccine enters the bloodstream it penetrates the cells that line the blood vessels forcing them to produce spike proteins that protrude into the bloodstream like millions of microscopic thorns. These thorns activate blood platelets which trigger blood clotting followed shortly after by an immune response that destroys the infected cells thus weakening the vascular system while draining the supply of killer lymphocytes. In this way, the vaccine launches a dual attack on the body’s critical infrastructure causing widespread tissue damage throughout the circulatory system while leaving the immune system less able to fend off future infection.
Now if you think you can have a long-and-happy without a functioning circulatory system, then none of this matters. But if you’re bright enough to realize that wreaking havoc on your vascular system is the fast-track to the graveyard, then you’ll probably understand that injecting these “poison-death shots” is a particularly bad idea.
By the way, it’s a real stretch to call these hybrid injections, “vaccines”. They have about as much in common with a traditional vaccine as a python does with a coffee table. Nothing. The “vaccine” moniker was chosen in order to shore-up public confidence, that’s all. It’s part of a marketing strategy. There is no real similarity. The majority of people trust vaccines and see them as a shining example of medical achievement. The drug companies wanted to tap into that trust and use it for their own purposes. That’s why they called it a “vaccine” instead of “gene therapy” which more accurately describes ‘what it does.’ But–like we said– it’s just a marketing strategy.
Have you ever wondered how the drug companies were able to roll out their own-individual vaccines just weeks apart from each other? That’s a pretty good trick, don’t you think; especially since vaccine development typically takes from 10 to 15 years. How do you think they managed that? Here’s an excerpt from an article which provides a little background on the topic:
“The virus behind the outbreak that began in Wuhan, China, was identified on Jan. 7. Less than a week later — on Jan. 13 — researchers at Moderna and the NIH had a proposed sequence for an mRNA vaccine against it, and, as the company wrote in government documents, “we mobilized toward clinical manufacture.” By Feb. 24, the team was shipping vials from a plant in Norwood, Mass., to the National Institute of Allergy and Infectious Diseases, in Bethesda, Md., for a planned clinical trial to test its safety.” (“Researchers rush to test coronavirus vaccine in people without knowing how well it works in animals”, Stat )
Got that? “The virus broke out in Wuhan… on Jan. 7, and less than a week later Moderna had a proposed sequence for an mRNA vaccine against it???
Really? Is that the same Moderna that had been playing-around with mRNA for over a decade but was never able to successfully bring a vaccine to market?
Yep, the very same company. Here’s more:
“And by Feb. 24, the team was shipping vials from a plant in Norwood, Mass??”
Wow! Another Covid miracle! You almost get whiplash watching these companies crank out their “wonder drugs” at record-breaking speed.
Keep in mind, there’s a very high probability that the virus was man-made, (In other words, it’s a bioweapon.) and the people who have been implicated in the funding and creation of that bioweapon are also closely aligned with the big drug companies that have produced the antidote in record time that has already netted tens of billions of dollars in profits for a drug for which there was no reliable animal testing, no long-term safety data, and no formal regulatory approval.
So I’ll ask you again: Doesn’t that all sound a bit suspicious?
Is it really that hard to see the outline of a political agenda here? After all, aren’t the drug companies working with the regulatory agencies that are working with the public health officials that are working with the media that are working with the corrupted politicians that are working with the Intel agencies that are working with the meddling globalist billionaires that are working with the giant private equity firms that oversee the entire operation pulling the appropriate strings whenever needed?
It sure looks like it.
And, don’t the tectonic social changes we’ve seen in the last year have more to do with a broader scorched-earth campaign launched by the “parasite class” against the rest of humanity than they do with a fairly-mild virus that kills mainly old and frail people with multiple underlying health conditions?
Right, again. In fact, many have noticed the cracks in the pandemic artifice from the very beginning, just as many have pointed out that the virus-meme is just the mask behind which parasites continue to conduct their global restructuring project. In short, it’s all about politics; bare-knuckle, take-no-prisoners NWO politics.
Answer – You’ve asked a number of questions about the animal trials, but none about the biodistribution and the pharmacokinetics studies that were done at the same time. Why is that? (Note--Pharmacokinetics; “the branch of pharmacology concerned with the movement of drugs within the body.”)
Question– I didn’t know there were any. Did the media report on them?
Answer – No, they didn’t. They completely ignored them, even though they were produced by Pfizer and provide essential information about where the substance in the vaccine goes in the body, in what amounts, and for how long. By knowing how the drug is distributed, it is possible to make educated assumptions about its effect on the organs and other tissue. In other words, these studies are invaluable. The Doctors for Covid Ethics have done extensive research on the studies and written a report titled “The Pfizer mRNA vaccine: pharmacokinetics and toxicity”. Here’s a few excerpts that help to illustrate the dangers of the vaccines:
“As with any drug, a key consideration for the toxicity of the COVID mRNA vaccines is where exactly in the body they end up, and for how long they will stay there. Such questions, which are the subject of pharmacokinetics, are usually thoroughly investigated during drug development. Initial studies on pharmacokinetics and also on toxicity are carried out in animals… this document has rather far-reaching implications: it shows that Pfizer—as well as the authorities that were apprised of these data— must have recognized the grave risks of adverse events after vaccination even before the onset of clinical trials. Nevertheless, Pfizer’s own clinical trials failed to monitor any of the clinical risks that were clearly evident from these data, and the regulatory authorities failed to enforce proper standards of oversight. This dual failure has caused the most grievous harm to the public….
What do Pfizer’s animal data presage for biological effects in humans?
- Rapid appearance of spike protein in the circulation.
- Toxicity to organs with expected high rates of uptake, in particular placenta and
lactating breast glands
- Penetration of some organs might be higher with the real vaccine than with this
luciferase model… The rapid entry of the model vaccine into the circulation means that we must expect the spike protein to be expressed within the circulation, particularly by endothelial cells. ( Endothelial – The thin layer of cells lining the blood vessels) We have seen before that this will lead to activation of blood clotting through direct activation of platelets and also, probably more importantly, through immune attack on the endothelial cells…
Summary
Pfizer’s animal data clearly presaged the following risks and dangers:
- blood clotting shortly after vaccination, potentially leading to heart attacks, stroke, and venous thrombosis
- grave harm to female fertility
- grave harm to breastfed infants
- cumulative toxicity after multiple injections
With the exception of female fertility, which can simply not be evaluated within the short period of time for which the vaccines have been in use, all of the above risks have been substantiated since the vaccines have been rolled out—all are manifest in the reports to the various adverse event registries. Those registries also contain a very considerable number of reports on abortions and stillbirths shortly after vaccination, which should have prompted urgent investigation. […]
Of particularly grave concern is the very slow elimination of the toxic cationic lipids. In persons repeatedly injected with mRNA vaccines containing these lipids… this would result in cumulative toxicity. There is a real possibility that cationic lipids will accumulate in the ovaries. The implied grave risk to female fertility demands the most urgent attention of the public and of the health authorities.
Since the so-called clinical trials were carried out with such negligence, the real trials are occurring only now—on a massive scale, and with devastating results. … Calling off this failed experiment is long overdue. Continuing or even mandating the use of this poisonous vaccine, and the apparently imminent issuance of full approval for it are crimes against humanity.” (“The Pfizer mRNA vaccine: pharmacokinetics and toxicity”, Doctors for Covid Ethics )
Don’t you think people are entitled to know what the government wants to inject into their bodies? Don’t you think they have a right to know how it will effect their immune systems, their vital organs and their overall health? Don’t you think they have the right to decide for themselves which drugs they will take and which they will refuse to take?
Forcing someone to take a drug he does not want, is not just wrong. It’s un-American. Which is why people should reject vaccine mandates as a matter of principle. They are an attack on personal liberty, the foundation of our constitutional system. It’s a principle worth dying for.
As for the mass vaccination campaign, it is the most maniacally-genocidal project ever concocted by man. There’s simply no way to calculate the amount of suffering and death we are about to face for trusting people whose policies were obviously shaped by their undiluted hatred of humanity. As German microbiologist Dr. Sucharit Bhakdi said:
“In the end, we’re going to see mass illness and deaths among people who normally would have had wonderful lives ahead of them.”
It is a great tragedy.
October 18, 2021
Posted by aletho |
Civil Liberties, Deception, Science and Pseudo-Science, Timeless or most popular, War Crimes | COVID-19 Vaccine, Human rights, Moderna |
Leave a comment
All over the world, populations have been locked up, have become fearful, and none of it can be justified. Looking at the UK, the overall death rate for 2020 is not unprecedented, and some of the increase in the death rate is likely the result of an incomprehensibly bad covid policy.
Sometimes, a dam breaks, and reality intrudes on media and political narratives. Just such a break is the publication of the mortality rate for England and Wales by the UK’s Office for National Statistics (ONS). The report can be found here. The content that is of greatest interest is the total mortality and mortality rates over time. Below is figure 1 from the report. A red line has been added to give a sense of where mortality was in 2020 compared with the past. The figure shows mortality rates with no adjustments.
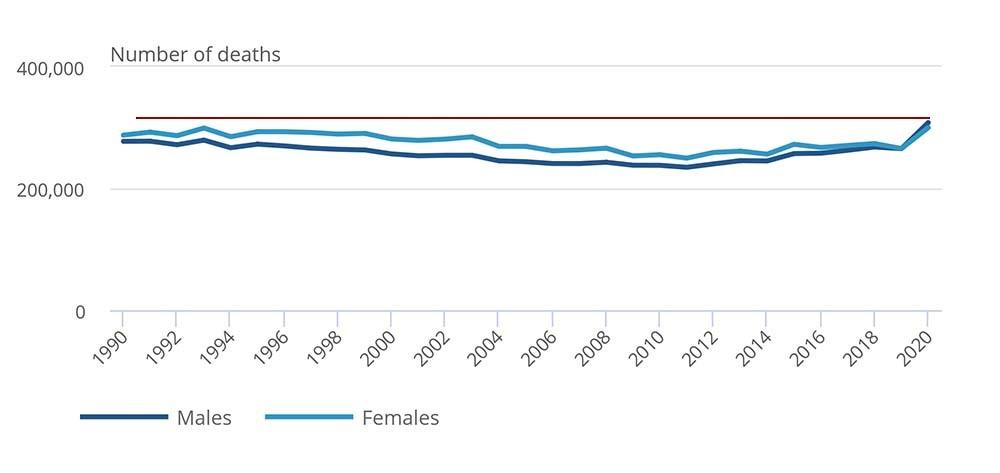
What is readily apparent is that there is, indeed, a jump in the mortality rate. However, if comparing the mortality rate with that of 1992, for example, we can see that it is not that high. In addition, the ONS provides a far more useful chart that shows age-standardized mortality rates. The report includes this discussion of the age-standardized statistics: “Age-standardised mortality rates (ASMRs) are a better measure of mortality than the number of deaths, as they account for the population size and age structure.” This is figure 3 from the report:

The exact figures for 2020 are 1,236.7 males and 894.2 females.
For comparison, the mortality rates for 2009 are the closest: 1,229.7 males and 886.6 females.
As can be seen from the ONS statistics above, the mortality rate is very slightly higher than in 2009 and is lower than in 2008.
No reference or academic study is needed to point out that there was no health crisis in the UK in either 2008 nor 2009. Indeed, these were considered perfectly normal years. This is very worrying data if considered in relation to the pandemic response. There have been many criticisms of the most extreme measures such as lockdowns, but even these critiques have been predicated on the belief that the pandemic was going to result in massive increases in mortality. According to the ONS data, no such massive increase took place. Instead, there was an uptick leading to 2008–09 mortality rates.
Unfortunately, this is not the whole story. At the start of the UK’s response to the pandemic, the government ordered the UK’s National Health Service (NHS) to make room in hospitals by removing anyone from a hospital that could be removed. The policy was called COVID-19 Hospital Discharge Service Requirements (C19HDSR) and the policy document can be found here. The subtitle of the report is ‘Why Not Home, Why Not Today?’ and this captures the spirit of the policy. It details the conditions under which patients should be discharged and the roles of the various actors in the policy.
The first point of note in the C19HDSR is that it does not refer to testing requirements for covid before discharge. Annex A provides the conditions under which patients should not be discharged and being covid positive is not included in the criteria. The policy document states that care homes should be filled with discharged patients. There is even an additional document for patients to read when going into aged care (see here). There is no reference to requirements for testing before release into aged care homes.
Although the NHS bureaucracy denied that significant numbers of covid-positive patients were being discharged under C19HDSR without covid testing, this was later shown to be untrue in a later study by Healthwatch and the British Red Cross (see here). The study researchers surveyed and interviewed 590 patients discharged under C19HDSR, and included whether the patients were tested for covid before discharge and whether they received their results before discharge. The two figures below show the figures from their research (from pp. 28–29):


Although the figures are from a sample of only 590 patients, they indicate that, at the very least, large numbers of patients were being forcibly discharged from hospitals without anyone knowing their covid status. The UK hospital ward system would be an ideal environment for the transmission of covid, with large numbers of people living close together in communal wards. At present, there is no further data on how many patients were discharged into aged care homes who were covid positive. However, given the data from Healthwatch and the British Red Cross, it would be reasonable to say that there must have been very many. In consideration that aged care homes are filled with the most covid-vulnerable populations, and involve considerable degrees of communal living, the policy likely very significantly contributed to the overall mortality rate in 2020.
When considering the ONS age-adjusted mortality statistics in conjunction with the policy of C19HDSR, it should be apparent that there is a big problem with the way that covid has been characterized, at the very least in the UK. It is not possible to say how much of the uptick in mortality was government policy related, but this adds a further significant question mark about the narrative surrounding the lethality of covid.
As stated, this is just the case of the UK in 2020. Nevertheless, this is a modern Western country that is supposed to have been hard-hit by covid in 2020. There is no reason to believe that it is some special outlier.
The implications of this data are very difficult. Even for individuals that may be very cynical about government, the data suggests that governments have acted in the most extraordinary ways based on what can only be called a hysteria. This hysteria has, across much of the Western world, seen unprecedented losses of basic rights, convulsions in healthcare systems with potentially terrible long-term results, disruption of education, and misery, loneliness, and mental health problems. As for the negative economic consequences, they will be with everyone for years to come. The effects are macro and micro, for example, the massive extension of government borrowing, printing money, and the decimation of small businesses.
If the data from the UK is broadly representative, the only way to sum up what has taken place, and is still taking place, is that the world is experiencing the first-ever global hysteria. After all, 2008 was a perfectly normal year.
Mark Avis is an academic in a New Zealand university and writes on the culture wars, politics, geopolitics, and economics at his website markavis.org.
October 18, 2021
Posted by aletho |
Deception, War Crimes | Covid-19, UK, United States |
Leave a comment
PREGNANT women who have not been dragooned into having a Covid jab must have been terrified by the headlines in many newspapers last Monday. A typical one read: ‘Pregnant women who have not had vaccine make up a FIFTH of the most ill Covid patients in intensive care, figures show’.
It makes it sound like one in five unvaccinated pregnant women are in intensive care – but it’s not true. It’s a cynical misrepresentation of the figures, presumably to scare women into taking the experimental vaccines.
Pregnant women are the minority of patients on ICU. The number of non-pregnant patients dying with a Covid diagnosis on ICU is ten times higher, and more of that cohort are likely to have been vaccinated. And what none of the news stories discussed was the risk to pregnant women who take the vaccine. The Medicines and Healthcare products Regulatory Agency (MHRA), the government drugs watchdog, list 28 deaths in their pregnancy section which include miscarriages, foetal deaths and stillbirths post vaccination between August 26 and October 14, but do not make it clear whether the mother died alongside her baby. Currently, at least 480,000 women are pregnant and on October 8, there were only 14 pregnant women on ICU from a total of 890 male and female patients. That has now dropped to 13 (p 43). ICNARC_COVID-19_Report_2021-10-15.pdf.pdf Pregnant women in the 16 to 49 age range account for just 1.6 per cent of all patients in intensive care.
Respiratory problems and failure have always been the most common cause for pregnant women to need admission to ICU and pre-Covid more than 1 in 5 pregnant women on ICU were there for pneumonia. Historically, many pneumonias will have been due to influenza but more recently have been caused by Covid.
The data released by the NHS last week relate to pregnant women who have tested positive for Covid and are being supported by a machine bypassing their lungs which are too damaged by the disease to breathe. The extracorporeal membrane oxygenation (ECMO) machine makes sure their blood is oxygenated and enables the body’s cells and organs to function properly.
The truth is that since July there have been 118 patients who needed an ECMO but only 20 were pregnant, less than a fifth. Of the 20 who were pregnant, 19 were recorded as unvaccinated. There have been no Covid patients supported by ECMO machines for the last two weeks (p 60).
There are more explanations for the figures. According to Dr Clare Craig, a member of HART Group (Health Advisory & Recovery Team), a group of highly qualified UK doctors, scientists and academics: ‘There are very few of these machines in the country. [Last reported figure was 15.] Prioritising pregnant women for such therapy would be a reasonable approach so the proportion receiving this care would not necessarily reflect the proportion of pregnant women who were sick on intensive care.’
The number of pregnant women who have died, according to official figures (Table 9, p 42) from the Intensive Care Audit National Research Centre (ICNARC), is minuscule compared to the total of 16- to 49-year-old deaths. From May 1 to October 8 this year, three pregnant women died (1.4 per cent), five recently pregnant women had died (2.9 per cent) compared with 127 women who were not pregnant (13.9 per cent). Since September 2020 only six pregnant women on ICU have died and 16 if you include recently pregnant women.
These figures clearly show that a minority of pregnant women end up on ICU.
Dr Craig said: ‘The mortality rate among pregnant women is one tenth of that of non-pregnant women aged 16-49 years.
‘Pregnancy comes with a small amount of risk which is illustrated by the pre-Covid figures. Around 300 pregnant women a year were admitted to ICU from about 640,000 births. This is about 1 in 2,000. A further 1,400 women who had recently been pregnant were also admitted per year. Together, these made up 14 per cent of intensive care admissions for all women aged 16-49 years of age. The admission rate since Covid had increased to 1 in 1,500 pregnant women compared with 1 in 4,000 non-pregnant women of childbearing age.
‘Last year, 1 in 3 of those who tested positive were asymptomatic and the number of positive PCR results are disproportionately high for women of childbearing age who are much more likely to be tested routinely as part of their antenatal care.
‘Other conditions have similar symptoms to Covid. There are 200 viruses that can cause a common cold which can also present with a cough. Pre-eclampsia symptoms include a severe headache and pain under the ribs. Testing on admission and repeated testing on ICU, in an environment where SARS-CoV-2 is likely to be present, can result in overdiagnosis.’
No one has escaped the effects of Covid completely, not even pregnant women. Dr Craig said: ‘Overall, deaths in women of childbearing age rose in spring and winter 2020 but have been at expected levels since.
‘So, to stress again, the risk of dying on ICU with a Covid diagnosis is ten times higher in the non-pregnant population, more of whom are likely to have been vaccinated.’
No Covid drug manufacturer has released details of studies into pregnant women receiving the vaccine, which means all information relating to expectant mothers is speculation. Pfizer do not complete theirs until December 2021.
The NHS say that the data comes from over 100,000 Covid vaccinations in pregnancy in England and Scotland, and a further 160,000 in the US – culled from the American V-Safe app, a self-reporting system for women who found themselves pregnant after taking the jab. None of the data are available to be scrutinised and neither set constitute a scientific study. However, Dr Edward Morris, president of the Royal College of Obstetricians and Gynaecologists (RCOG), said: ‘We do understand women’s concerns about having the vaccine in pregnancy, and we want to reassure women that there is no link between having the vaccine and an increased risk of miscarriage, premature birth or stillbirth.’
An obstetrics and gynaecology doctor, who advises the UK Medical Freedom Alliance, a team of medical professionals, academics, scientists, and lawyers; said: ‘These numbers are so far from good science that we could be put on notice of liability if something goes wrong with a mother’s pregnancy because of the vaccine.’
Data from Public Health England showed that more than 81,000 pregnant women have received the first dose of the Covid jab, and around 65,000 have had their second.
Pregnant women were first offered the vaccine in December 2020, if they were health or care workers or in an at-risk group. Since April 2021, pregnant women have been offered the vaccine as part of the standard age-based rollout of the vaccination programme. No births in pregnant women from the April cohort who received the vaccine will have been completed until January 2022. So there is no way to know how vaccinated pregnant women, who had the vaccine in their first trimester, will fare until then, and we only have limited data from women vaccinated in the second and third trimester.
October 17, 2021
Posted by aletho |
Deception, Mainstream Media, Warmongering, Science and Pseudo-Science | Covid-19, COVID-19 Vaccine |
Leave a comment
It likely means years of languishing until some client state takes them on board under Washington’s strict conditions
The announcement that the Biden Administration has cleared two more Guantanamo Bay detainees for transfer is a hopeful sign in as much that two men have surpassed one hurdle on the way to freedom. But don’t be fooled, they may not see the light of day outside the barbed wire and concrete of the Cuban island for years. And if they do, it will most likely be in a foreign country not of their own choosing, with government monitors awaiting them. And if they are sent to the United Arab Emirates, it could be the next stop to an even greater hell.
Simple question: What kind of constitutional republic are we that supports federal measures that detain other human beings without charge for 20 years and then, when they are “cleared” to go, insist they must be released to a foreign government that agrees to treat them as criminals furthermore?
According to the New York Times, Sanad Yislam al-Kazimi and Assadullah Haroon Gul, of Yemen and Afghanistan respectively, cannot go back to their native countries because of obvious security concerns. Al-Kazimi is likely to go to neighboring Oman, which has taken some 30 repatriations over the years, and Gul’s fate is up in the air.
The Biden Administration has released but one Guantanamo Bay prisoner since he took office. But even then, the process for Abdul Latif Nasser’s release began during the Obama administration. Nasser, 56, who was never charged with a crime, actually got to return to his home country of Morocco, though he was subsequently put under investigation there, too.
So who is left? According to the Times, there are 39 detainees at the prison (which Obama had pledged to close during his time) today. Al-Kazimi and Assadullah now join 10 others of that number who are cleared to go but awaiting repatriation. Another 15 are not charged but are considered “law of war” prisoners and not cleared (news flash: supposedly we are not “at war” anymore — or are we? Apparently it is fungible). That includes Abu Zubaydah, who was waterboarded 83 times upon his capture nearly 20 years ago and still hasn’t been charged (and is still awaiting a ruling as to whether his detention is lawful). There are 10 who are awaiting trial (including the so-called 9/11 mastermind Khalid Sheikh Mohammed and four cohorts), and two already convicted. No one has any confidence that those trials will go anywhere soon, given the issues over torture evidence and the convoluted nature of the system. Meanwhile, as of 2019, each prisoner at GTMO has cost the U.S. taxpayers $13 million a year.
The military tribunal system is broken and many argue that it should have never been stood up after 9/11. It was illegal from the beginning, and efforts to “legalize” it only managed to keep it open. As we know, access to due process means one thing in America and another at Guantanamo Bay.
But yes, let’s talk about the “rules based order” some more. Biden may say his hands are tied by Congress, which won’t let him release prisoners anywhere near U.S. territory, or be tried in U.S. courts. But the fact is the interagency Periodic Review Board that clears the prisoners is under Executive Branch purview and the president should have some authority to expedite the processes and or/loosen the restrictions and conditions placed on potential host countries. Unfortunately, aside from the dense legal and administrative thicket, the stigma built up around these men has rendered them radioactive — who knows who will take them if given the right opportunity. They have been stripped of their humanity and their native lands, and to the American government they are nothing but a cost and legal burden. How long will it be before we forget why they are even there?
October 17, 2021
Posted by aletho |
Deception, Subjugation - Torture, Timeless or most popular | Human rights, United States |
Leave a comment
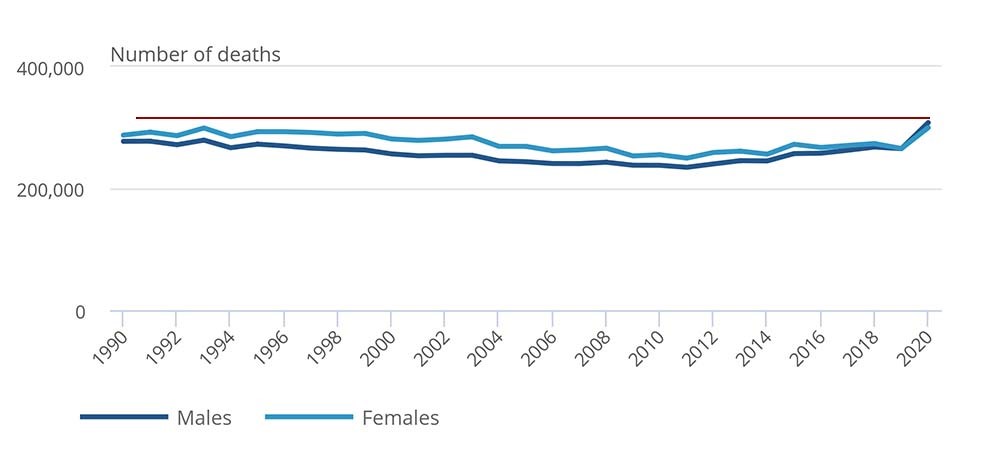
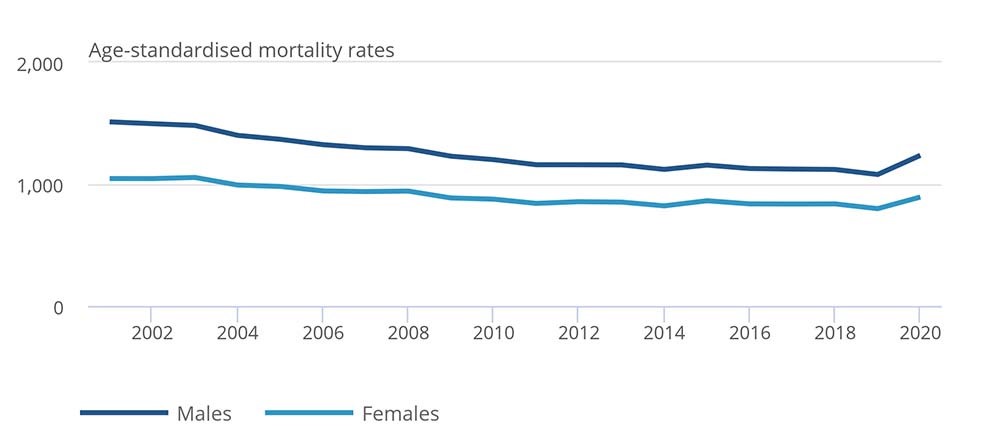

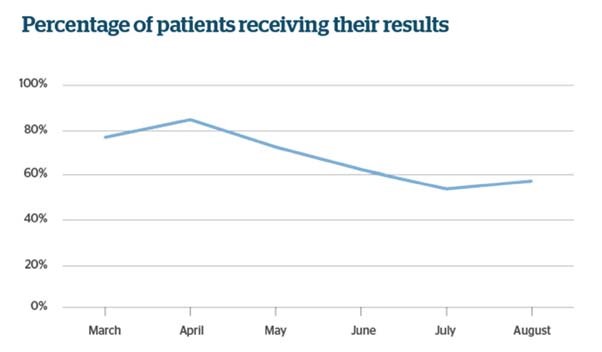
 Aletho News
Aletho News