US still operating biolabs in Ukraine – Russian envoy
RT | March 25, 2024
The US continues to operate 30 biolabs on the territory of Ukraine as part of an illegal military-biological program, Russia’s envoy to the Netherlands has claimed.
The number of American laboratories on Ukrainian territory has been “well-known for a long time,” Vladimir Tarabrin, who is also Russia’s Permanent Representative to the Organization for the Prohibition of Chemical Weapons (OPCW), said in an interview with the Izvestia newspaper on Sunday.
The diplomat recalled that the head of Russia’s Nuclear, Chemical and Biological Protection Forces, Lieutenant General Igor Kirillov, had claimed in March 2022 that 30 such biolabs existed.
“Our armed forces discovered documents confirming the extensive military biological program deployed by the US and NATO countries on the territory of Ukraine and other former Soviet republics,” he said.
The Kiev government allegedly began destroying dangerous pathogens in the laboratories and suspending research on February 24, 2022, the day Russia launched its military operation against Ukraine, but “in 2023 the implementation of those programs resumed, only their name was changed,” Tarabrin claimed.
Asked if the number of the US biolabs in Ukraine still stands at 30, the ambassador said: “According to our data, yes.”
“It’s not surprising, therefore, that over the past 20 years, Washington has been blocking all Russian initiatives aimed at strengthening the Biological Weapons Convention (BWC) regime and creating an effective mechanism for verifying compliance with its provisions by all participating countries,” Tarabrin said.
Over the past two years Moscow has repeatedly raised concerns over an alleged network of secretive US-funded laboratories in Ukraine, publishing troves of documents captured from Kiev authorities, which it claims are linked to the operations of those facilities.
Last April, Kirillov said Russia had “no doubt that the US, under the guise of ensuring global biosecurity, conducted dual-use research, including the creation of biological weapons components, in close proximity to Russian borders.”
The US government has confirmed the existence of the biolabs in Ukraine, but insisted that they are entirely legal and not intended for military purposes, despite mostly being funded via the Pentagon. Washington has denied Moscow’s claims of the labs being used to work on bio-weapons as a “Russian disinformation campaign.”
Kirillov also said a year ago that the US biolab program in Ukraine, which was previously known as ‘Joint biological research’, was rebranded as ‘Biological control research’ so that it could continue its operations.
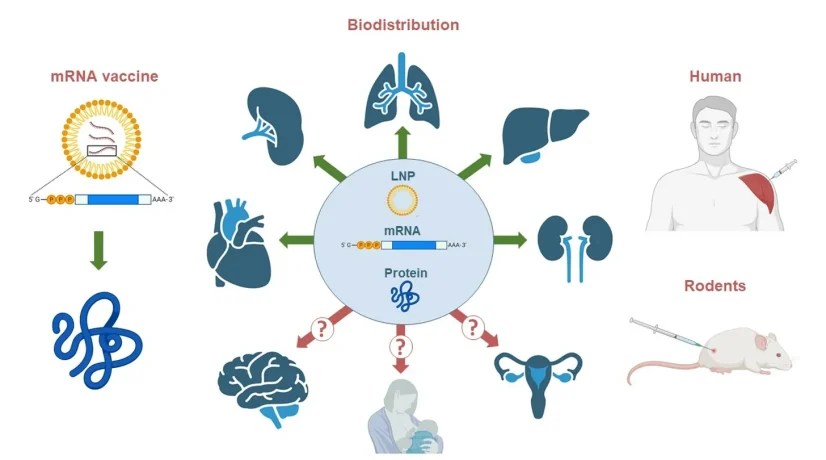
Little Known about mRNA and Spike Protein Biodistribution Three Years into Mass Vaccination Campaign
Alarming Conclusions from Russian Analysis of Studies
By Peter A. McCullough, MD, MPH | Courageous Discourse | March 24, 2024
I remember when the mRNA COVID-19 vaccines rolled out in December, 2020. I asked some of the doctors a few questions about the novel products. Where do they go in the body? How long do they last? No one knew the answers yet throngs came forward and took the jab.
Now a Russian analysis of the biodistribution data on lipid nanoparticles laced with mRNA has been published by Pateev et al. The conclusions are shocking especially considering we are three years into a global mass vaccination campaign with shots every six months.

Pateev, I.; Seregina, K.; Ivanov, R.; Reshetnikov, V. Biodistribution of RNA Vaccines and of Their Products: Evidence from Human and Animal Studies. Biomedicines 2024, 12, 59. https://doi.org/10.3390/biomedicines12010059
This image from the manuscript is not reassuring for a vaccine, which one would anticipate should remain in the deltoid muscle, incite local antigenic stimulation, and then have the lymphatic and immune system produce clearance of the foreign material and confer durable immunity. As you can see, mRNA vaccines do nothing of the sort. The widespread distribution, long duration of action, and dangerous unending production of the damaging and potentially lethal Spike protein continue to cause great alarm among doctors, scientists, and the public who are asking questions regarding the biological fate of these new products.
Pateev, I.; Seregina, K.; Ivanov, R.; Reshetnikov, V. Biodistribution of RNA Vaccines and of Their Products: Evidence from Human and Animal Studies. Biomedicines 2024, 12, 59. https://doi.org/10.3390/biomedicines12010059
The Ridiculous Psychology of Conspiracy Theory
BY IAIN DAVIS | UK Column | MARCH 21, 2024
If you watched the BBC’s REEL segment, The Psychology Behind Conspiracy Theories, it probably became clear to you that the BBC was not dealing with science but had instead wandered off into the realm of fantasy. Unfortunately, experimental psychology investigating alleged “conspiracy theory” has been disconnected from objectivity for many years.
While psychology itself has a solid empirical foundation, experimental psychology often falls short of basic scientific standards. In 2015, the Open Science Foundation found that, of 100 published experimental psychology papers, results could only be replicated in 39, and just 36 produced findings from which any meaning could be drawn.
Such a high degree of subjectivity frequently leads to woolly conclusions, promoted as scientific fact in the BBC’s REEL segment. Shortly after the introduction, we are given the expert psychologist opinion that so-called “conspiracy theorists” are likely both to be extreme narcissists and to hold “beliefs” driven by a sense of powerlessness.
Narcissists can be broadly characterised as people with a perceived, and potentially misplaced, sense of higher social status. They often have expectations that they should be treated more favourably as a result.
While narcissists possess delicate egos, they certainly don’t suffer from a sense of powerlessness. Quite the opposite: narcissists frequently have a grandiose sense of self-importance, and the expectations to go with it.
This prima facie mutual exclusion in the double definition of “conspiracy theorists” near the beginning of the BBC’s short report on the psychology of those it chose to call conspiracy theorists gave us an early clue as to the epistemological failure at the heart of nearly all academic research on the subject. In point of fact, when we look more closely at the research claiming to reveal the “psychological traits” of the alleged conspiracy theorists, we frequently encounter the worst kind of pseudo-scientific drivel.
A Loaded Question
The BBC began its “investigation” by asking:
Are some people more vulnerable to conspiracy theories, or are we all at risk?
We were immediately told that “conspiracy theories” present some sort of psychological threat to our mental health. Apparently, they harm or damage us in some way, hence the BBC’s declaration that we might be “vulnerable” to their discourse.
Which prompts the question: what is it about supposed conspiratorial thinking that causes us harm?
The BBC didn’t say, but it did air the views of a number of experts who claimed to know.
Jonas Kaplan is the assistant research professor of psychology at, and co-director of, the University of Southern California’s Dornsife Neuroimaging Center. He studies the link between neurological activity and thoughts and emotion.
As an example of his work, in 2016 he co-authored a paper which monitored neural activity in a region of the brain called the default mode network (DMN). He and his fellow researchers presented a cohort of forty people, each of whom had expressed strongly “liberal” political opinions, with so-called “counter-evidence” that was intended to contradict their beliefs.
The team monitored the effect of this supposed cognitive challenge upon the subjects’ neural response. Specific neural activity was observed, indicating that the DMN region of the brain—associated with identity—was stimulated when personal beliefs were allegedly challenged. This was interesting but, from this point forward, the research started to go wildly astray.
From their observations, Kaplan and his colleagues concluded that resistance to changing beliefs, in the face of this suggested “contradictory evidence”, was stronger for political beliefs than it was for non-political convictions. They consequently inferred that political opinions were more strongly associated with our sense of self than other kinds of beliefs we hold.
Unfortunately, the researchers ignored the gaping hole in their own methodology. They mentioned it, but didn’t seem to fully grasp the full implications of what they had done.
Rather than actually “challenge” their subjects’ beliefs with genuine contradictory evidence, they decided to make most of it up. They said:
In order to be as compelling as possible, the challenges often contained exaggerations or distortions of the truth.
For example, they told the subjects that Russia had a larger nuclear arsenal than the US. This wasn’t a “distortion” of the truth; it was a false statement.
More importantly, the neuroscientists failed to ascertain whether the subjects knew it was a lie. In the case that the subject knew the information was false—and we don’t know how many did—their views had not actually been “challenged.” This massive oversight utterly undermined the paper’s primary conclusions.
The researchers stated:
Our political participants may have been more likely to identify these distortions for the political issues, especially if they were more familiar with these issues. [. . . ] We did find that participants who rated the challenges as more credible were more likely to change their minds, and it is well known that source credibility influences persuasion.
Following their extensive experimental research, Kaplan et al. “discovered” that people were more likely to believe information if it was credible. Conversely, they were less likely to believe information if it was evidently wrong—because the researchers had made it up.
Beyond stating the obvious, Kaplan et al. then delivered subjective conclusions that were not substantiated by their own experimental data:
Our data [. . .] support the role of emotion in belief persistence. [. . .] The brain’s systems for emotion, which are purposed toward maintaining homeostatic integrity of the organism, appear also to be engaged when protecting the aspects of our mental lives with which we strongly identify, including our closely held beliefs.
The problem is that the researchers didn’t know what those emotions were. People might simply have been angry because they were lied to.
Kaplan and his colleagues did not establish that the perceived resistance to changing a belief was the result of any defensive psychological mechanism, as claimed. There was nothing in their research that distinguished between that possibility and the equally plausible explanation that the subjects rejected the “challenging information” because they knew it was wrong.
The researchers’ ostensible finding—that the subjects’ resistance to change in the face of counter-evidence was linked to identity, and therefore demonstrated an emotional attachment that could potentially overcome rational thought—was an assumption unsupported by their own experimental data. Kaplan et al. noted where neurological activity occurred, but they did not demonstrate what the associated cognitive processes were.
Building Narratives Based Upon Flawed Assumptions
The press release that accompanied publication of the Kaplan et al. paper made no such clarification. It claimed, without cause, that Kaplan’s research had effectively proven an alleged sociological and psychological truth:
A USC-led study confirms what seems increasingly true in American politics: People are hardheaded about their political beliefs, even when provided with contradictory evidence. [. . .] The findings from the functional MRI study seem especially relevant to how people responded to political news stories, fake or credible.
The above statement represented a huge leap of logic that the paper itself didn’t justify. There was little evidence that the study subjects had been “provided with contradictory evidence” (emphasis added).
Rather, they were given so-called “distortions” and highly questionable opinions. Their reasons for rejecting these had not even been ascertained.
In the same press release, Kaplan declared:
Political beliefs are like religious beliefs in the respect that both are part of who you are and important for the social circle to which you belong. [. . .] To consider an alternative view, you would have to consider an alternative version of yourself.
This is similar to the statement he later made in the BBC REEL piece on the psychology of conspiracy theory:
One of the things we see with conspiracy theories is that they are very difficult to challenge. [. . .] One of the advantages of having a belief system that’s resistant to evidence is that the belief system is going to be very stable across time. If you have to constantly update your beliefs with new evidence, there’s a lot of uncertainty. [. . .] Conspiracy theories are a way of making sense of an uncertain world.
Where did Kaplan get his opinion from? It wasn’t evident from his work. Nor did it bring us any closer to understanding the allegedly harmful nature of the suggested conspiratorial thinking.
What Is Conspiratorial Thinking?
While a definition of “conspiracy theory” isn’t mentioned directly in the BBC REEL segment, we do at least obtain a cited reference to one in the paper of another contributor, Anni Sternisko. Sternisko is a PhD candidate at New York University who researches conspiracy groups. In her co-authored paper, she cites Understanding Conspiracy Theories (Douglas et al., 2019), which does offer some definitions:
Conspiracy theories are attempts to explain the ultimate causes of significant social and political events and circumstances with claims of secret plots by two or more powerful actors.
This ludicrous premise supposedly informs the universally-accepted working definition of “conspiracy theory”. It pervades nearly all academic research on the subject, including the alleged psychological studies of those labelled as “conspiracy theorists”; and, as we are seeing with the BBC, it is being accepted unquestioningly in the mainstream media, too.
Back in the real world, no-one tries to explain “significant social and political events” with “claims of secret plots”. It is, on its face, a ridiculous notion. It might happen with regularity in BBC sitcoms, but does it happen in your social circle?
How can anyone, other than the conspirators themselves, know what a “secret plot” entails? The clue is in the wording; it’s a secret.
Generally, the people who are labelled “conspiracy theorists” by academics, politicians, the mainstream media and other interested parties are eager to highlight the evidence that exposes real plots that actually happened or are currently underway. Examples which made it to full-scale parliamentary inquiries in various Western countries include Operation Gladio, Watergate, the Iran Contra affair and so on. These aren’t “secrets”. If they were, no-one would know about them.
The so-called conspiracy theorists of the real world also point to evidence which appears to expose real plots that are yet to be officially acknowledged. For example, the study by the Department of Civil Engineering and the University of Alaska Fairbanks seems to show that the official account of 9/11 cannot possibly be true.
Taking this example, the only way to determine whether the stories we have been told about 9/11 are true or not is to examine the evidence. Again, this evidence is not and indeed cannot be a “secret”. It can be obfuscated, hidden or denied—but it cannot be known of at all if it remains ”secret”.
There are many reasons why we might hypothesise that 9/11 was, in fact, some form of false-flag attack. None of the evidence suggesting this possibility is “secret”, either. It is all in the public domain.
The logical exploration of evidence is the best way yet devised to find the truth, and has been acknowledged as such since at least Socrates’ day. Inductive, deductive and abductive reasoning all rely upon this basic approach. The key factor here is the evidence, without which the facts cannot be known.
While we can, and should, question all theories, the only way to discover the truth is first to identify and then rigorously to examine the evidence, ideally ascertaining some facts along the way.
We are at liberty to argue incessantly about various explanations of events, but there is one absolute certainty: we will never know what the truth is if we don’t explore the evidence, that very activity which is now being presented to us as suspect.
Descent Into Bathos
The Douglas et al. paper continues:
Conspiracies such as the Watergate scandal do happen, but because of the difficulties inherent in executing plans and keeping people quiet, they tend to fail. [. . .] When conspiracies fail—or are otherwise exposed—the appropriate experts deem them as having actually occurred.
As incredible as this may be, as far as these academics and researchers are concerned, unless the conspiracy is officially acknowledged by the “appropriate experts”, it remains a “secret” and therefore cannot be known. We are being sold the line that conspiracies only come into existence once they have been officially admitted.
This is, then, the completely illogical basis for academia’s alleged research of conspiracy theory. Conspiracies are only identifiable when they fail or are otherwise “officially” exposed. For these various “experts”, the consideration—by their own acknowledgement—that conspiracies are often real, and not “secrets”, renders their offered definition of “conspiracy theory” self-contradictory rubbish.
If you come to the matter with the worldview that “conspiracy theorising” is an attempt to explain events in terms of “secret plots”, then it is reasonable to deduce that said “conspiracy theory” is rather silly. If, however, you concede that these allegedly “secret plots” are not secrets at all and can be discovered by examining the evidence that exposes them, then your original premise, upon which your definition of “conspiracy theory” is based, is complete junk.
It is difficult to express the monumental scale of the idiocy entailed in the experimental psychologists’ definition of “conspiracy theory.” It is exactly the same as asserting that any evidence offered to indicate that a crime has been committed is completely irrelevant unless the police have already caught the perpetrators and their guilt proven in court.
Sure, your front door has been kicked in, your property ransacked and your possessions stolen, but—according to the psychologists of conspiracy theory—this is not evidence of a crime. The facts have yet to be established by the “appropriate experts”, and consequently the alleged crime remains a “secret” and is unknowable.
This absurd contention, based upon the logical fallacy of appeal to authority (argumentum ad verecundiam), is the foundation for all of the pseudo-scientific gibberish about conspiracy theory and theorists that follows. Douglas et al. also reveal some of the other terms often used in this so-called psychological research.
“Conspiracy belief”, “conspiracy thinking”, “conspiracy mindset”, “conspiracy predispositions”, “conspiracist ideation”, “conspiracy ideology”, “conspiracy mentality” and “conspiracy worldview”—most of these apparently serving no distinct purpose other than an attempt at elegant variation—are all terms based upon the psychologists’ own delusional beliefs. For some reason, all those researching the psychology of those they have labelled conspiracy theorist imagine, without reason, that the so-named “conspiracists” don’t have any evidence to back up their arguments.
In a moment of self-conscious admission, the Douglas et al. paper adds:
It is important for scholars to define what they mean by “conspiracy theorist” and “conspiracy theory” because—by signalling irrationality—these terms can neutralize valid concerns and delegitimize people. These terms can thus be weaponized. [. . .] Politicians sometimes use these terms to deflect criticism because it turns the conversation back onto the accuser rather than the accused.
As noted above, the scholars’ definition of “conspiracy theory” is etymologically redundant. The associated—and empty—pejorative of “conspiracy theorist” has consequently seeped into the lexicon, and it is based upon nothing but assumption and imagination.
The term “conspiracy theorist” has indeed been weaponised. It was designed to ensure that people don’t look at the evidence, wherever it is applied.
Politicians, the mainstream media, the scientific and medical authorities, and many other representatives of the establishment, right down to neighbourhood level, frequently use it to “deflect criticism” (in Douglas’ apt phrase) and to level unwarranted accusations at their critics. As outlined in Document 1035 – 960, this is precisely how the CIA envisaged that the “conspiracy theorist” label would function.
Regrettably, for most people, it is enough for someone just to be called a “conspiracy theorist” for anything subsequently proceeding from their mouth to be ignored. It doesn’t matter how much evidence they provide to support their views. The labelling system has done its job.
We might expect scientists, academics and psychologists to maintain higher standards. Unfortunately, BBC REEL’s The Psychology Behind Conspiracy Theories demonstrates that this is often not the case.
Who Is It That Is “At Risk” From Conspiracy Theories?
This reliance upon an illogical presupposition leads to profound confusion. During The Psychology Behind Conspiracy Theories, Anni Sternisko commented:
Conspiracy theories are not necessarily irrational or wrong. And I think what we are talking about in society at the moment—what is frightening us—are better explained, or better labelled, as conspiracy narratives; that is, ideas that are irrational to believe, or at least unlikely to be true—that are not necessarily theories, such that they are not falsifiable.
Sternisko appears to have been talking to her BBC interviewer about two completely different things: evidence-based arguments on one hand and irrational beliefs on the other.
Sternisko’s problem is that both the rational and the irrational are indiscriminately referred to as “conspiracy theories” in today’s academe and media. Thus, in searching for a unifying psychology to account for two diametrically opposed thought processes, the doctoral researcher cannot avail herself of suitable terminology that has gained acceptance in her professional environment and is forced by her own intellectual honesty to start coining spontaneous distinctions between alleged conspiracy “theories” and “narratives”.
This may be welcome insight, but it has become necessary only because the psychologists in her field are floundering around with a working definition of “conspiracy theory” that is ridiculous. Again, we can look to the paper by Douglas et al. to appreciate just how incoherent it is:
While a conspiracy refers to a true causal chain of events, a conspiracy theory refers to an allegation of conspiracy that may or may not be true. [. . .] To measure belief in conspiracy theories, scholars and polling houses often ask respondents—through surveys—if they believe in particular conspiracy theories such as 9/11, the assassination of JFK, or the death of Princess Diana.
This reconfirms that the only benchmark that the academics concerned have for “measuring” what they call “conspiracy theory” is the extent to which the subject agrees or disagrees with the official account of any given event. As long as their subjects unquestionably accept the official “narrative”, they aren’t considered to be “conspiracy theorists.” If they do question it, they are.
Consequently, all of the related experimental psychology is completely meaningless, because the researchers never investigate whether what they call conspiracy theory “may or may not be true”. There is no basis for their claim that “conspiracist ideation” is irrational, or even that it exists.
Without establishing the credibility of the propounded theory, the psychologists, sociologists and other researchers and scientists involved have based their entire field of research upon their own opinions. This cannot be considered science.
In this light, Anni Sternisko’s statement at last reveals something about what the BBC called the “risk” of conspiracy theory. It seems that these alternative explanations of events are not dangerous to the conspiracy theorists themselves, but rather to people like Sternisko, who find them “frightening”.
Questioning power is a fundamental democratic ideal, yet this PhD candidate would appear to be one of millions in Western societies who have come to feel that doing so is scary. Fear, and the resultant stress and anxiety it produces, can be very damaging to our mental health. So the BBC is right, in a sense, to highlight potential risks in this domain.
It is just that the BBC, and the groundless psychological theories it promotes, are wrong about who is at risk. It isn’t the purported “conspiracy theorists”, but rather the people who unquestioningly accept official accounts who are “vulnerable”.
What the BBC presented with its REEL segment was not an exploration of the psychology behind conspiracy theory. It was instead an exposé of the deep-rooted terror of those who apparently dare not look at the evidence cited by the people they label “conspiracy theorists”.
If their government is lying to them, then, for some reason, it seems they do not want to know. The mere thought of it petrifies them.
The researchers—who insist that it is the “conspiracy theorists” who are deluded—have constructed a mythology masquerading as scientific knowledge. Their resultant research, founded upon this myth, isn’t remotely scientific. Inevitably, the psychologists who expounded upon their own apparent delusions for the BBC soon descended into farce.
It’s Science, Don’t Laugh
Professor Sarah Gorman authoritatively informed the BBC audience that “conspiracy theorists” are so irrational they can believe two contradictory statements at the same time. We have already discussed why so much of this psychological research is flawed, but Gorman was most likely referring to a paper that isn’t just based upon assumptions; it is appallingly bad science for numerous other reasons besides.
Gorman told the BBC audience:
People are very often able to hold in their heads two conspiracy theories that are directly in conflict. So, for example, people will simultaneously believe that Princess Diana’s death was staged, and that she’s still alive and also that she was murdered. And, on the face of it this doesn’t make much sense, but the underlying principle here is that they believe that something is just not right about the official story, and it almost doesn’t matter exactly what the alternative is; just that there has to be an alternative that’s being suppressed.
Professor Gorman was almost certainly referring here to one of the formative papers in the field of experimental conspiracy theory research, Dead and Alive: Beliefs in Contradictory Conspiracy Theories (Wood, Douglas & Sutton, 2012).
Presumably, she has read it, so why she would make this statement is difficult to say. The paper is a joke.
Wood et al. conducted experiments in an effort to identify what they had already judged to be the psychological weakness of “conspiracy theorists”. They set the subjects a series of questions and rated their responses using a Likert-type scale (1 – strongly disagree, 4 – neutral response, 7 – strongly agree).
The psychologists conducting this research presented deliberately contradictory statements. For example, one arm of the study asked the subjects to indicate their level of agreement with the idea that Princess Diana was murdered and also with the suggestion that she faked her own death. Similarly, another arm asked the subjects the extent of their agreement with the notion that Osama bin Laden was killed by US Navy SEALs but also that he was still alive in captivity.
They collected the responses, analysed the results and, from this, deduced:
While it has been known for some time that belief in one conspiracy theory appears to be associated with belief in others, only now do we know that this can even apply to conspiracy theories that are mutually contradictory. This finding supports our contention that the monological nature of conspiracism is driven not by conspiracy theories directly supporting one another but by the coherence of each theory with higher-order beliefs that support the idea of conspiracy in general.
It seems that Professor Gorman, at least, is convinced by this pabulum and was willing to present it to the BBC as scientific fact. Alas—rather as with Kaplan’s paper—these scientists’ conclusions, seemingly referenced by Gorman, were not supported by their own experimental results.
Had the participants been asked to consider exclusivity, and subsequently indicated that they agreed with two or more contradictory theories, then the Wood et al. conclusion would have been substantiated. But they weren’t, so it wasn’t.
All that the participants were asked to do was to indicate their relative level of agreement. This Hobson’s choice of a study design means it is entirely possible, and logical, for a research participant of sound mind to agree strongly with one statement while agreeing somewhat with another, even if the two are “mutually contradictory”.
To illustrate this: the official account of Osama bin Laden’s death claims that he was assassinated by the US military. There is no video, forensic or photographic evidence, no witness testimony—all the members of the SEAL Team Six deployed to Pakistan for that operation have since managed to die—nor indeed anything, beyond the proclamation of politicians, to lend this tale any credibility at all. There isn’t even any evidence of a body, as bin Laden was allegedly buried at sea.

This is what happened… honest!
Consequently, if you doubt the official account (and what sane person wouldn’t), a whole range of possibilities exists. It all depends upon your evaluation of the available evidence—which by definition cannot come from the academically-vaunted official sources, because they haven’t presented any.
In such circumstances, it is perfectly legitimate to agree strongly that bin Laden died in 2011 and simultaneously to agree somewhat with the proposition that he was extraordinarily renditioned to a black-ops site somewhere. Nothing can be ruled out. There is insufficient evidence to draw any firm conclusion.
Wood et al. did not ask the study participants to exclude contradictory accounts; only to rate such accounts on a scale of plausibility. The paper’s conclusion, that the results of their experimental psychology proved “the monological nature of conspiracism” was driven by some assumed “higher-order” belief system, was pseudo-scientific claptrap.
The BBC duly conveyed Professor Gorman’s “expert” opinion that all of this somehow made sense. This is standard fare at White City. Anyone who questions the state or its narratives is a “conspiracy theorist”, as far as the BBC is concerned.
So, before we suffer any more of this nonsense, let’s politely ask these experimental psychologists to examine the evidence behind so-called conspiracy theories before they rush into making assumptions about the supposed psychology behind them. Hopefully, they won’t find the experience too frightening.
FSB reports 11 suspects detained over terrorist attack

RT | March 23, 2024
Eleven people have been detained over the terrorist attack on the Crocus Crocus City Hall concert venue outside Moscow, Russia’s Federal Security Service (FSB) has said in a statement.
The arrested suspects include “four terrorists who were directly involved in the terrorist attack on Crocus,” the statement read. Investigative work to track down other accomplices are ongoing, it added.
After carrying out the attack on Friday night, “the perpetrators tried to escape by car, fleeing towards the Russian-Ukrainian border,” the FSB said on Saturday. “The criminals intended to cross the Russia-Ukraine border and had relevant contacts on the Ukrainian side,” it added.
According to the agency, “all four terrorists” were arrested in Russia’s Bryansk Region within several hours as a result of well-coordinated actions by the security services and the police. The detainees are now being transferred to Moscow, it added.
The attack on Crocus Crocus City Hall was “carefully planned,” with the perpetrators using weapons that had been placed in a stash in advance, the FSB said.
Russia’s Investigative Committee also confirmed that four suspects, who “committed the terrorist attack” on Crocus City Hall, were detained in Bryansk Region, “not far from the border with Ukraine.”
Crocus City Hall, in the town of Krasnogorsk in Moscow’s western outskirts, was attacked by gunmen on Friday night. It happened before a concert by Russian rock band Picnic, when the venue, which has an estimated capacity of 7,500, was nearly at capacity.
The attackers shot at the crowd indiscriminately then set the building on fire. They managed to flee the scene in what was said to be a white Renault Symbol/Clio car, prompting a large-scale manhunt.
According to Russia’s Investigative Committee, the death toll in the attack has reached at least 115. The Moscow Region Health Ministry said that at least 121 people were also wounded, with 107 requiring hospitalization.
Russia explains stance on US-proposed Palestine “cease fire” resolution
Explanation of vote by Permanent Representative Vassily Nebenzia at the UNSC vote on US-proposed draft resolution on the situation in the Middle East, including the Palestinian question
Permanent Mission of the Russian Federation to the United Nations | March 22, 2024
Before the vote:
Mr. President,
For six months now, the UN Security Council has been unable to adopt a resolution demanding a ceasefire in Gaza. Time and again, the United States thwarted any attempt to do so by using a veto in cold blood as many as four times.
During that time, we have heard many different excuses from our American colleagues. For example, that it is premature to seek a ceasefire because it is necessary to give space “for Israel’s counter-terrorism efforts”; that the Council should not interfere with Washington’s “effective diplomacy on the ground”; that we should wait until Ramadan, when, they say, an agreement on a cessation of violence will definitely be made.
Now, six months later, when Gaza has been practically leveled with the ground, the US representative says without batting an eye that Washington finally starts to realize the need for a ceasefire.
This leisurely thinking process by Washington has cost the lives of 32,000 Palestinian civilians, two-thirds of them women and children.
And even now we see a typical hypocritical show, when in the wrapper of a “ceasefire” the United States is trying to sell to the members of the Security Council and the entire international community something else – a vague phrase about “defining the imperative of a ceasefire”. Such philosophy about moral imperatives looks naturally in the works of Immanuel Kant. But it is not enough to save the lives of Palestinian people. And that is not at all what the mandate of the UN Security Council suggests, which has a unique toolkit to demand a ceasefire and, if necessary, enforce it.
In an official interview to Al Hadath in Jeddah on 20 March, Secretary of State Blinken said, “Well, in fact, we actually have a resolution that we put forward right now that’s before the UNSC that does call for an immediate ceasefire tied to the release of hostages and we hope very much that countries will support that”. However, the US-proposed draft resolution does not make such call. It appears that either the US Permanent Representative to the United Nations or the US Secretary of State deliberately mislead the international community.
Colleagues,
From the very beginning, it was obvious that the “negotiations” on the draft resolution held by our American colleagues were only meant to delay time. All our comments and “red lines” were ignored, as well as the proposals of a number of other delegations. This was not a normal work on a document. It felt more like speaking into the void.
The US draft is a thoroughly politicized document, which only aims at pulling on voters’ heartstrings before the US elections by throwing them a “bone” in the form of at least some mention of a “ceasefire” in Gaza. The draft also seeks to consolidate US policy in the region through “terrorist labels” and to ensure impunity for Israel, whose criminal actions the draft gives no assessment to.
Let me also stress that the American draft contains a de facto green light for Israel to conduct a military operation in Rafah. At least, the sponsors have tried to make sure that nothing in their draft would prevent West Jerusalem from completing the deadly cleanup of southern Gaza.
That is actually what Washington wants. We already said that we will no longer pass meaningless resolutions that do not demand a ceasefire and lead us nowhere.
This draft must not pass with the majority of UNSC votes in order to send a message that Washington’s not even palliative but devious concepts are unacceptable. It will be extremely strange if those members of the Council (and they are the majority), who realize this and have been saying to us that the US draft is a flawed one, will now raise their hand in favor. If you do so, you will smear yourselves in disgrace.
Think what this will make you look in the eyes of the people of the Middle East and your own countries, if you support this hypocritical endeavor designed to disorient the international community and, in fact, undermine the authority of the Council by rendering it unable to influence the situation on the ground and making it “stay out of White House’s way”. Are you ready to play a part in this shameful show?
Russia will not do this. As a permanent member of the Security Council and one of the founders of the United Nations, we recognize the global historical responsibility for the maintenance of international peace and security and cannot allow the Council to become a tool of Washington’s destructive policy in the Middle East. If this resolution were adopted, it would definitively close the debate on the need for a ceasefire in Gaza, give Israel a free hand and condemn Gaza and its entire population to extermination or expulsion.
In our work, we are not guided by what pleases Washington or its satellites who are ready to cast a vote at the US behest, but by what is necessary for the Palestinians and what promotes peace.
We urge the members of the UN Security Council to prevent this and vote against the American draft resolution.
Mr. President,
In order for the UN Security Council to still be able to implement its mandate to maintain international peace and security, a number of non-permanent UNSC members have prepared an alternative draft resolution that spells out in black and white the requirements for both a ceasefire and the unconditional release of hostages. It is a balanced and depoliticized document.
We see no reason why members of the Security Council could refuse to support it, unless a ceasefire and the release of hostages are not part of their plans. This is an attempt to allow the Council to carry out the noble functions entrusted to it. We urge to not miss it.
Thank you.
After the vote:
Mr. President,
We have now listened to the hypocritical speeches of some Council members shedding crocodile tears over the Russian and Chinese vetoes. We have explained the reasons why we did not pass this resolution. It was not because it was put forward by the United States delegation, as the American Permanent Representative tried to assure us today. I told you – those of you who voted here today – that you would cover yourselves in disgrace by voting in favor of an American text that was unacceptable to you (including those of you who are now praising it).
Do you want me to say what really happened? Not hard to guess, the scenario is not complicated at all. Your American masters, in addition to “twisting the arms” of your leaders in the capitals, said, “Don’t you worry, Russia will veto anyways, so you won’t have to go against the American draft.” That’s it, that’s the whole scenario. So stop this hypocrisy about how upset you are that Russia and China vetoed the resolution. Once again, you have covered yourselves in disgrace today by voting in favor of a draft resolution that you did not and do not really support.
Thank you.
CIA Further Discredits ‘Uyghur Genocide’ by Admitting Covert Influence Campaign
By Patrick Macfarlane | The Libertarian Institute | March 21, 2024
On March 14, Reuters released a bombshell report: in 2019 the Donald Trump White House began a clandestine CIA influence campaign to smear China’s international reputation.
According to three former U.S. officials with direct knowledge, “the CIA created a small team of operatives who used bogus internet identities to spread negative narratives about Xi Jinping’s government while leaking disparaging intelligence to overseas news outlets.” The information releases “targeted public opinion” both internationally and in China itself. Along with influencing public opinion, the campaign sought to “foment paranoia among top leaders [in China]” as they tried to trace the leaked information.
The report specifically stated that CIA operatives “promoted [corruption] allegations” against Chinese government officials and “slammed as corrupt and wasteful China’s Belt and Road Initiative.” Although these specific efforts were identified, the former U.S. officials declined to name additional narratives that were advanced.
Reuters did not confirm that the campaign has continued into the Joe Biden presidency however two “unnamed intelligence historians” told Reuters that such “presidential findings” often remain in place across administrations.
The existence of this CIA influence campaign is probable given the broader historical context.
The Trump Administration marked the extreme acceleration of the United States’ new cold war against China. This began when the Pentagon issued its 2018 National Defense Strategy, which declared a refocus from Middle East “counter-terrorism” to “Great Power Competition” with Russia and China.
Subsequently, 2019 was a banner year for Western escalation against Beijing. In October 2019, the Department of Defense created a new office focused solely on confronting China, called the “deputy assistant secretary of defense for China.” In December 2019, NATO named China as an emerging “challenge.” In 2019 and 2020, the Trump administration doubled U.S. naval transits of the Taiwan Strait over previous years and conducted approximately 1,000 reconnaissance flights over the South China Sea. Of course, when the COVID-19 pandemic arrived in 2020, it was immediately blamed on China.
The above efforts notwithstanding, the main thrust of America’s new cold war against China was informational. America sought to isolate China on the world stage by shredding its international reputation, justifying sanctions, and inhibiting trade. This was clear even before the CIA’s new revelation.
Aside from blaming that nation for COVID-19, the “Uyghur Genocide” narrative was the most prominant vehicle for achieving that goal. But just what focus, if any, does the CIA’s revelation provide to the facts of that narrative as we already know them?
Well, the CIA was there every step of the way.
2019 is the same year that an NGO called the “China Tribunal” began petitioning the UN Human Rights Council, accusing the Chinese Communist Party of conducting an industrial organ harvesting operation that preyed upon Chinese dissidents and Uyghur muslims.
In January 2021, the Trump administration weaponized this claim when Secretary of State Mike Pompeo, fresh off his post as CIA director, formally accused China of committing genocide against Uyghur muslims in its Westernmost provice, Xinjiang. To back this claim, Pompeo referred to the findings of a 2020 report written by a German sociologist named Adrian Zenz. The report was titled “Setilizations, IUDs, and Mandatory Birth Control: The CCP’s Campaign to Suppress Uyghur Birthrates in Xinjiang.” In March 2021, Zenz published an additional report, “The Uyghur Genocide: An Examination of China’s Breaches of the 1948 Convention.”
News outlets the world over declared that these reports were being made by “independent third parties.” Nothing could have been further from the truth.
The China Tribunal has direct connections to the fringe religious group Falun Gong, a Chinese spiritualist cult that runs The Epoch Times and New Tang Dynasty. Furthermore, Zenz’s reports were published by neoconservative think tanks, including the Jamestown Foundation, the Newlines Institute, and the Wallenberg Centre for Human Rights. The Jamestown Foundation itself was founded by the late CIA Director William Casey. The Newlines Institute is led, inter alia, by former employees of the “shadow CIA” private spying firm Stratfor.
Myself and others, including Max Blumenthal, Gareth Porter, and Ajit Singh have demonstrated significant statistical errors, credibility issues, mistranslations of source material, and propagandistic misrepresentations present in each report. These analyses are available elsewhere.
Each of Zenz’s reports rely in part on “leaked PRC government document[s]” to support its findings. These documents are cited by Zenz as the “Karakax List,” the “Aksu List,” and the “China Cables.”
The Karakax lists allegedly shows the reasons why 311 Uyghur individuals were interned in “reeducation camps” in Xinjiang.
The China Cables purportedly consist of “an operations manual for running mass detention camps,” four “secret intelligence briefings” from a mass Chinese Uyghur data collection system, and a regional court sentencing document where a Uyghur man was ordered 10 years’ imprisonment for telling coworkers to practice “Halal.”
According to Zenz, the Karakax List was leaked by the same source that leaked the China Cables. The International Consortium of Investigative Journalists, the organization that published the China Cables, says it received the leaks “via a chain of exiled Uyghurs,” but confirmed the document’s authenticity with several leading experts, including James Mulvenon, vice-president of Defense Group Inc, Zenz, and several intelligence sources who cannot be identified.
In 2019, the leaker identified herself as Ms. Asiye Abdulaheb, an exiled Uyghur living in the Netherlands. Ms. Abdulaheb told Dutch newspapers that she moved from China in 2009, though the documents she leaked were dated from 2017. She did not reveal how she obtained the documents.
As for the Aksu List, Human Rights watch admits it was leaked to them by Radio Free Asia, a Cold War era CIA cutout created to disseminate American propaganda across the continent.
In July 2022, Zenz jointly published a leak with the Victims of Communism Memorial Foundation, an anti-communist cold war project co-founded by President Jimmy Carter’s National Security Advisor Zbiegniew Brzezinski. Zenz gave it the ominous title “the Xinjiang Police Files.”
Zenz claims the documents are “unprecedented evidence” that “proves [the] prison-like nature of re-education camps [and] shows top Chinese leaders’ direct involvement in the mass internment campaign.” The release consists of what is claimed to be “2,800+ Images of Detainees, 300,000+ Personal records, 23,000+ Detainee Records, and 10+ Camp Police Instructions.” According to Zenz, the documents were obtained through hacking by “a third party” who broke into the computer systems of local Chinese government officials.
When the documents were made available for public scrutiny, some anomalies were detected.
For instance, some of the documents’ metadata indicated they had been edited by Zenz and a national security contractor named Ilshat Kokbore. As it turns out, Kokbore was also the president of the American Uyghur Association and was the Director for China Affairs for the World Uyghur Congress—an NGO based in Washington that receives funding from the National Endowment for Democracy. The NED was referred to as the “second CIA” by one of its founders, Allen Weinstein, because it openly performs the work that the CIA used to do covertly.
Others questioned visual anomalies in the detainee images, which suggested they may have been computer generated.
Together, Zenz used the leaks as the centerpiece of his reports accusing China on the international stage. They were cited by every major news outlet, the U.S. State department, and even by the UN High Commissioner for Human Rights.
Zenz’s reports were sold internationally as being “unbiased” and “independent,” but the Reuters revelations place CIA operatives in China “leaking intelligence” for the admitted purpose of destroying China’s international reputation. This operation ran during the primary years of the Uyghur Genocide allegations.
The full weight of this revelation cannot be overstated.
I was banned from Elon’s ‘free speech’ X app for offending power
BY KIT KLARENBERG · THE GRAYZONE · MARCH 19, 2024
Following years of pressure from Israel lobbyists and British spooks, I was finally banned by Twitter/X. What does my removal say about Elon Musk, who flaunts his opposition to censorship, while promising to build an “everything app” where you could lose access to banking and messaging for violating dubious speech codes?
On February 17, I was suspended from Twitter/X without warning. The cause was mass-reporting by Zionist activists I’d offended. My removal was justified on the basis that I violated X’s “rules against violent speech.” Having endlessly condemned violence on the platform – in particular, the Gaza genocide – I’m flummoxed. Not least because a post from one of my Zionist detractors, which openly calls for me to be “battered on a weekly basis” over my political views, remains extant today.

Despite repeated requests for clarity from X, I have no idea whether I will ever be reinstated. In February, I received from “support” stating the suspension will only be reversed after three months. But just a few sentences later, the email contradicted itself, stating in closing that the ban would last just a month. Meanwhile, whenever I log into X, my profile appears to have zero followers or follows, I cannot view or search anyone’s tweets (including my own), and my DMs are inaccessible. Have they been erased? A landing page message reads:
“Your account is permanently in read-only mode, which means you can’t post, repost, or like content. You won’t be able to create new accounts.”
In January 2024, X purged a number of prominent, predominantly left-wing users without warning or explanation. Their suspensions were lifted only after a deluge of complaints poured in to the personal account of Elon Musk, the libertarian tech maven and self-proclaimed free speech warrior who purchased Twitter with his personal fortune.
I am grateful that scores of X users have done the same following my own suspension. However, Musk has kept mum about my case. While I may not have as many followers as those abruptly defenestrated in January, my work has been widely shared on X, with some posts gaining millions of impressions. Most-viewed was my December 2023 revelation that an unadvertised and unnoticed Russian government plane was parked in Washington DC’s Dulles airport, a visit which likely represented the beginning of the Ukraine proxy war’s end.
This [number of impressions] is quite a remarkable turnaround, given the concerted effort to suppress my Twitter output for as long as I have used the platform. One of the most illuminating disclosures in the Twitter Files exposed how the hyper-censorious regime that controlled the social media platform before Musk’s takeover required explicit authorization from managers to throttle accounts with more than 100,000 followers. Until then, engineers had free rein to covertly censor, suppress and shadowban anyone they wished, however they wished, without any oversight whatsoever.
This secret protocol offered a compelling explanation for curious developments regarding my own Twitter account in Summer 2022. For 18 months following my 2021 registration for Twitter, my follower count remained stubbornly low. This was until The Grayzone unmasked celebrity “journalist” Paul Mason as a British intelligence asset who directly coordinated attacks on anti-war figures and movements with a “friend” in the Foreign Office. I was the lead investigator on this series of reports.
The exposés generated significant attention the world over. My followers duly began multiplying by hundreds daily. Curiously, however, whenever I was a few dozen shy of 10,000, the total would crash back down. Evidently, Twitter staffers – and powerful forces breathing down their necks – were absolutely determined no one saw what I had to say.
Besides the exposes of Mason I worked on, there was my October 2019 report revealing Gordon Macmillan, a senior Twitter executive, as a member of 77th Brigade, the British Army’s shadowy psychological warfare unit which specializes in the weaponization of social media.
Had Macmillan and his fellow national security cadres exacted revenge on me when I was finally banned from Twitter/X? And what does my permanent removal say about X’s new boss, Elon, who advertises X as a platform that “champions free speech,” while promising to build an “everything app” where you could presumably lose access to your bank and messaging history for violating dubious speech codes?
Frozen out of ‘everything’ by Elon
Gordon MacMillan was one of many high-ranking staffers rightly sacked from the company upon Musk’s acquisition. From my perspective, while the owner’s politics couldn’t be further removed from my own, I have largely defended and embraced the changes he has implemented.
During an October 26, 2023 all-hands meeting at Twitter/X headquarters, Musk opened his remarks by announcing that he was “transforming the company from what it was, Twitter 1.0, to the everything app.”
He vowed to establish “a single application that encompasses everything. You can do payments, messages, video, calling, whatever you’d like, from one single, convenient place.”
“We just don’t have that,” Musk lamented. “It doesn’t exist outside of China.”
I might not have been using X for “everything”, but it was an extremely useful tool in my personal and professional life. My banning offered me a stark illustration of the dangers of relying so heavily on a privately-owned social media app, especially one that provides features that are almost essential in a digital world.
Many are anxious about the rise of digital payments and currencies, for this would inevitably grant financial institutions, and governments, monopoly power over how citizens can spend their cash, and even more gravely, whether they can. Fall foul of such powerful forces, even accidentally, and you might find yourself frozen out of your life savings, perhaps forever. If X is to truly become an “everything” app, the implications of a ban will be greatly multiplied, with suspensions effectively locking a user out of every sphere of their public and private life.
We haven’t reached that point yet. But the consequences of X’s arbitrary suspension process are very real. There are now scores of people — comrades, collaborators, critics, and journalistic sources — from whom I’m now cut off, perhaps forever. Meanwhile, the contents of our conversations seem to have been rendered permanently inaccessible – except, perhaps, by Musk himself.
The vaguely-explained, arbitrary suspension means I’m not only being deprived the ability to express my opinions in a public forum, hold the powerful to account, expose hypocrisy, criminality and even genocide, and directly engage with my supporters and detractors. It also means I’ve lost a platform through which to conduct sensitive conversations with sources across the globe.
The start of something worse?
In a June 2019 op-ed, United Nations special rapporteur on torture Nils Melzer wrote that once WikiLeaks founder Julian Assange had been “dehumanized through isolation, ridicule and shame, just like the witches we used to burn at the stake, it was easy to deprive him of his most fundamental rights without provoking public outrage worldwide.” A key component of the WikiLeaks founder’s “isolation” was the Ecuadorian Embassy cutting off his internet access in March 2018.
As I previously revealed, that act was just one aspect of a wide-ranging black propaganda campaign executed by a British intelligence cutout called the Integrity Initiative. By falsely framing Assange as a Russian agent, London successfully pressured Quito into banning his personal visits as well as any and all communication with the outside world. Immediately thereafter, British police launched ‘Operation Pelican,’ a scheme designed to extract Assange from the embassy and ultimately transfer him into US custody.
Operation Pelican succeeded one year later, and Assange has festered in Belmarsh Prison, Britain’s Gitmo, ever since. As he awaits extradition to Washington, where he could face 175 years in a supermax prison, Assange has been blocked from communicating with the outside world. Press photographers were even prohibited from capturing his wedding day inside the jail on the grounds of national security. Is my Twitter/X suspension part of a similar effort to isolate me, so when the British state deprives me of my most fundamental rights, it won’t provoke public outrage?
Alternatively, recall the role Twitter/X played in the case of independent journalist Steve Sweeney, who was arbitrarily detained in Mexico while on his way to cover Nicaragua’s November 2021 election, which the US State Department had condemned. Sweeney might have languished in prison for an interminable period had word not immediately spread across Twitter, resulting in his release after three nightmarish days in custody without food or clean water. Activists in Mexico were at the forefront of the push to free Sweeney.
Since May 2023, when British counter-terror officials detained, interrogated, and digitally strip searched me for six hours without granting my right to silence or privacy, I have found travel unnerving — particularly the act of arriving at, walking through, and exiting airports.
I don’t know what information global databases display about me, which claims regarding my character have been shared with foreign governments, or whether I’ve been erroneously flagged as an international security threat.
Influential security state-tied figures like Paul Mason have openly clamored for me to be jailed as punishment for my journalistic activities. Heidi Bachram, the British pro-Israel activist who led the campaign to mass-report me on X over my solidarity with Palestine, has expressed hope that I “will never again be allowed to visit” my homeland. Her supporters have echoed the sentiment.

There are clear indications that a number of shadowy, intelligence-linked elements are monitoring my activity online. In November 2023, an Irish defense consultant who claims to have “advised government, military and civil society actors in Ukraine and other European countries regarding defence policy,” bizarrely alleged: “Klarenberg… showed his FSB signature training as [sic] early 2014.”
I have no idea what they were alluding to, and certainly have never received any training by Russian intelligence. But it’s not unreasonable to think I’d be in the military alliance’s crosshairs. That same month, the NATO Stratcom Center of Excellence described me as one of the “agents and sympathizers” of a “hostile regime” in a report which effusively advocated for the cyberbullying, harassment, stalking, and doxxing of anti-imperialists.
British censorship org targets The Grayzone?
Apparently not content with simply targeting me personally, these same forces have relentlessly attacked The Grayzone as well. In August 2022, longtime British intelligence operative Ross Burley publicly smeared The Grayzone as a “Russian propaganda outfit” and asserted it was “incredibly irresponsible for YouTube and other social media companies” to platform our journalists. The cause of his ire may have been our 2021 report on leaked files that exposed details of Britain’s wide-ranging, clandestine intelligence operations targeting Russia.
In response, Twitter took the unprecedented step of applying a “warning” label to each and every tweet linked to this report, cautioning users it contained “materials obtained through hacking.” The policy backfired, however, after countless users mocked the label and turned it into a meme. Others, meanwhile, suggested Twitter’s label simply amounted to a seal of authenticity that confirmed the leaked material’s veracity. As to the question of why the social network chose to slap this label on The Grayzone exclusively, and overlook Western-funded “OSINT” collectives such as Bellingcat which routinely publish stolen material, recent developments may provide some clue.
In February, Politico revealed that Britain’s Defence and Security Media Advisory (DSMA) Committee had been unsuccessfully attempting to woo major social media platforms to join its board. The Committee is a Ministry of Defence-run censorship mechanism tasked with dictating which security-related stories mainstream media is authorized to report. When the Committee asks British journalists and editors to withhold information from the public, they almost always comply.
Politico quoted Geoffrey Dodds, a DSMA secretary and former military official, as saying Google and Meta were among the social media giants on the Committee’s wishlist. He proposed that tech firms monitor their platforms for content relating to Britain’s “national security,” then seek the Committee’s advice on whether to censor. Yet his effort has so far been unsuccessful, as the companies reportedly “felt that they couldn’t sit on [the board] because it was too linked to government.”
Still, Dodds remained optimistic that the British government would “come up with a grand bargain with the tech giants… then hopefully, we’ll be able to get the tech giants back on board.” Politico said the Committee was “steadfast” in its determination to get social media firms aboard. Dodds remarked that moving forward, “there’s probably going to be less print, just as much broadcasting, and a continued increase in social media and online [news]… So we need to get into this game.”
Publicly-available minutes of the DSMA Committee’s June 2023 meeting show that the body’s Deputy Secretary, retired Navy Captain Jon Perkins, disclosed that between October 2022 and April 2023, material of “extreme sensitivity (in national security terms)” had been “protected from inadvertent disclosure” thanks to the Committee’s interventions with journalists. This material was “of the most sensitive nature he had seen” since joining.
While the “nature” of that “material” was unstated, Perkins may well have been referring to a series of investigations The Grayzone published throughout that precise period detailing London’s secret and pivotal role in escalating the Ukraine proxy war. Given this outlet’s reputation as a leading source of insight on the cloak-and-dagger machinations of the US and British-led Western national security state, the DSMA Committee would welcome its suppression on Twitter/X and other platforms at least as much as it did my indefinite suspension.
After years of pressure from Western security state operatives, I was finally banished from Twitter/X under the watch of the billionaire owner who has flaunted his ideological opposition to censorship. On his coming “everything app,” it seems that everything you say can and will be used against you.
Israel deploys army of bots to spread anti-UNRWA propaganda: Report
The Cradle | March 19, 2024
Israel is executing an online influence campaign using hundreds of fake social media accounts to advance “Israeli interests” among progressive western audiences, including US lawmakers, Haaretz reported on 19 March, citing an investigation by Israeli media watchdog group Fake Reporter.
The campaign is focused specifically on amplifying reports claiming the involvement of UNRWA workers in the 7 October attack on Israel. As The Cradle has reported previously, Israel provided no evidence for its claims, which were part of a campaign to compel western nations to cut funding to the agency. UNRWA plays a crucial role in delivering aid to Palestinians amid Israel’s campaign to impose famine in Gaza.
Researchers at Fake Reporter pinpointed three fake ‘news sites’ specifically created for the operation. The sites amplified reports copied from other real news outlets, such as CNN, The Wall Street Journal, The Guardian, The Jerusalem Post, and The Times of Israel, which promoted Israel’s narrative about the war.
Hundreds of fake social media accounts then intensively promoted the “reports” from the specially-created websites and other news outlets.
The three websites at the center of the campaign were established before the war in Gaza but became active only after it began.
The fake social media accounts seemed to be ‘cyborgs,’ meaning they operate using a combination of artificial intelligence and real people with fake online personalities. The avatars claimed to portray average US citizens, including white, Jewish, and African–American ones.
The avatars were all created on the same date, used the same profile photos and naming conventions, and shared other characteristics that indicate they are all part of the same network, Fake Reporter found.
Over 500 fake accounts were opened for the campaign on Facebook, Instagram, and X.
Their avatars began to post messages about a wide array of topics, including the alleged lack of safety for Jewish Americans on college campuses, discrimination against Jewish students, and false allegations Hamas committed mass rape on 7 October.
At the end of January, after acquiring tens of thousands of followers, the fake accounts pivoted toward spreading Israel’s false allegations about UNRWA employees participating in the 7 October attack.
The avatars worked to inorganically amplify the ‘shocking’ and ‘disturbing’ allegations about UNRWA.
They responded to social media posts by US lawmakers, influencers, and prominent news outlets.
The campaign’s avatars targeted posts by African–American Democratic lawmakers, including Ritchie Torres, Cori Bush, and Jamal Bowman, who received the most such comments.
Haaretz noted that targeting Democratic African–American lawmakers seemed to be an attempt to counter the wave of support they have given to Palestinians amid Israel’s ongoing campaign of Genocide in Gaza.
How the Democrats Plan to Steal the Election
By Llewellyn H. Rockwell, Jr. | March 18, 2024
Biden and Trump have clinched the nominations of their parties for President. Everybody is gearing up for a battle between them for the election in November. It’s obvious that Biden is “cognitively impaired.” In blunter language, “brain-dead”. Partisans of Trump are gearing up for a decisive victory. But what if this battle is a sham? What if Biden’s elite gang of neo-con controllers won’t let Biden lose?
How can they stop him from losing? Simple. If it looks like he’s losing, the elite forces will create enough fake ballots to ensure victory. Our corrupt courts won’t stop them. They have done this before, and they will do it again, if they have to.
I said the Democrats have done this before. The great Dr. Ron Paul explains one way they did this in 2020. The elite covered up a scandal that could have wrecked Biden’s chances:
“Move over Watergate. On or around Oct. 17, 2020, then-senior Biden campaign official Antony Blinken called up former acting CIA director Mike Morell to ask a favor: he needed high-ranking former US intelligence community officials to lie to the American people to save Biden’s lagging campaign from a massive brewing scandal.
The problem was that Joe Biden’s son, Hunter, had abandoned his laptop at a repair shop and the explosive contents of the computer were leaking out. The details of the Biden family’s apparent corruption and the debauchery of the former vice-president’s son were being reported by the New York Post, and with the election less than a month away, the Biden campaign needed to kill the story.
So, according to newly-released transcripts of Morell’s testimony before the House judiciary Committee, Blinken “triggered” Morell to put together a letter for some 50 senior intelligence officials to sign – using their high-level government titles – to claim that the laptop story “had all the hallmarks of a Russian disinformation campaign.”
In short, at the Biden campaign’s direction Morell launched a covert operation against the American people to undermine the integrity of the 2020 election. A letter signed by dozens of the highest-ranking former CIA, DIA, and NSA officials would surely carry enough weight to bury the Biden laptop story. It worked. Social media outlets prevented any reporting on the laptop from being posted and the mainstream media could easily ignore the story as it was merely “Russian propaganda.”
Asked recently by Judiciary Committee Chairman Jim Jordan (R-OH) why he agreed to draft the false sign-on letter, Morell testified that he wanted to “help Vice President Biden … because I wanted him to win the election.” Morell also likely expected to be named by President Biden to head up the CIA when it came time to call in favors.
The Democrats and the mainstream media have relentlessly pushed the lie that the ruckus inside the US Capitol on Jan. 6th 2021 was a move by President Trump to overthrow the election results. Hundreds of “trespassers” were arrested and held in solitary confinement without trial to bolster the false narrative that a conspiracy to steal the election was taking place.
It turns out that there really was a conspiracy to steal the election, but it was opposite of what was reported. Just as the Steele Dossier was a Democratic Party covert action to plant the lie that the Russians were pulling strings for Trump, the “Russian disinformation campaign” letter was a lie to deflect scrutiny of the Biden family’s possible corruption in the final days of the campaign.
Did the Biden campaign’s disinformation campaign help rig the election in his favor? Polls suggest that Biden would not have been elected had the American electorate been informed about what was on Hunter Biden’s laptop. So yes, they cheated in the election.
The Democrats and the mainstream media are still at it, however. Now they are trying to kill the story of how they killed the story of the Biden laptop. This is a scandal that would once upon a time have ended in resignation, impeachment, and/or plenty of jail time. If they successfully bury this story, I hate to say it but there is no more rule of law in what has become the American banana republic.” See here.
But the main way the election can be rigged is by fraudulent “voting.” It’s much easier to do this with digital scanning of votes than with old-fashioned ballot boxes.
Dr. Naomi Wolf explains how electronic voting machines make it easier to steal elections:
“People could steal elections in this ‘analog’ technology of paper and locked ballot boxes, of course, by destroying or hiding votes, or by bribing voters, a la Tammany Hall, or by other forms of wrongdoing, so security and chain of custody, as well as anti-corruption scrutiny, were always needed in guaranteeing accurate election counts. But there was no reason, with analog physical processing of votes, to query the tradition of the secret ballot.
Before the digital scanning of votes, you could not hack a wooden ballot box; and you could not set an algorithm to misread a pile of paper ballots. So, at the end of the day, one way or another, you were counting physical documents.
Those days are gone, obviously, and in many districts there are digital systems reading ballots.” See here.
This isn’t the first time the Left has stolen an election. It happened in the 2020 presidential election too. Ron Unz offers his usual cogent analysis:
“There does seem to be considerable circumstantial evidence of widespread ballot fraud by Democratic Party forces, hardly surprising given the apocalyptic manner in which so many of their leaders had characterized the threat of a Trump reelection. After all, if they sincerely believed that a Trump victory would be catastrophic for America why would they not use every possible means, fair and foul alike, to save our country from that dire fate?
In particular, several of the major swing-states contain large cities—Detroit, Milwaukee, Philadelphia, and Atlanta—that are both totally controlled by the Democratic Party and also notoriously corrupt, and various eye-witnesses have suggested that the huge anti-Trump margins they provided may have been heavily ‘padded’ to ensure the candidate’s defeat.” See here.
In a program aired right after Biden’s pitiful State of the Union speech, the great Tucker Carlson pointed out that Biden’s “Justice” Department has already confessed that it plans to rig the election. It will do this by banning voter ID laws as “racist.” This permits an unlimited number of fake votes:
“If Joe Biden is so good at politics, why is he losing to Donald Trump, who the rest of us were assured was a retarded racist who no normal person would vote for? But now Joe Biden is getting stomped by Donald Trump, but he’s also at the same time good at politics? Right.
Again, they can’t win, but they’re not giving up. So what does that tell you? Well, they’re going to steal the election. We know they’re going to steal the election because they’re now saying so out loud. Here is the Attorney General of the United States, the chief law enforcement officer of this country in Selma, Alabama, just the other day.
[Now Carlson quotes the Attorney General, Merrick Garland:]
“The right to vote is still under attack, and that is why the Justice Department is fighting back. That is why one of the first things I did when I came into office was to double the size of the voting section of the Civil Rights Division. That is why we are challenging efforts by states and jurisdictions to implement discriminatory, burdensome, and unnecessary restrictions on access to the ballot, including those related to mail-in voting, the use of drop boxes and voter ID requirements. That is why we are working to block the adoption of discriminatory redistricting plans that dilute the vote of Black voters and other voters of color.
[Carlson then comments on Garland:]
“Did you catch that? Of course, you’re a racist. That’s always the takeaway. But consider the details of what the Attorney General of the United States just said. Mail-in balloting, drop boxes, voter ID requirements. The chief law enforcement officer of the United States Government is telling you that it’s immoral, in fact racist, in fact illegal to ask people for their IDs when they vote to verify they are who they say they are. What is that? Well, no one ever talks about this, but the justification for it is that somehow people of color, Black people, don’t have state-issued IDs. Somehow they’re living in a country where you can do virtually nothing without proving your identity with a government-issued ID without government-issued IDs. They can’t fly on planes, they can’t have checking accounts, they can’t have any interaction with the government, state, local, or federal. They can’t stay in hotels. They can’t have credit cards. Because someone without a state-issued ID can’t do any of those things.
But what’s so interesting is these same people, very much including the Attorney General and the administration he serves, is working to eliminate cash, to make this a cashless society. Have you been to a stadium event recently? No cash accepted. You have to have a credit card. In order to get a credit card you need a state-issued ID, and somehow that’s not racist. But it is racist to ask people to prove their identity when they choose the next President of the United States. That doesn’t make any sense at all. That’s a lie. It’s an easily provable lie, and anyone telling that lie is advocating for mass voter fraud, which the Attorney General is. There’s no other way to read it. So you should know that. You live in a country where the Attorney General is abetting, in fact calling for voter fraud, and that’s the only chance they have to get their guy re-elected.” See here.
Because of absentee ballots, the voting can be spread out over a long period of time. This makes voting fraud much easier. Mollie Hemingway has done a lot of research on this topic:
“In the 2020 presidential election, for the first time ever, partisan groups were allowed—on a widespread basis—to cross the bright red line separating government officials who administer elections from political operatives who work to win them. It is important to understand how this happened in order to prevent it in the future.
Months after the election, Time magazine published a triumphant story of how the election was won by “a well-funded cabal of powerful people, ranging across industries and ideologies, working together behind the scenes to influence perceptions, change rules and laws, steer media coverage and control the flow of information.” Written by Molly Ball, a journalist with close ties to Democratic leaders, it told a cheerful story of a “conspiracy unfolding behind the scenes,” the “result of an informal alliance between left-wing activists and business titans.”
A major part of this “conspiracy” to “save the 2020 election” was to use COVID as a pretext to maximize absentee and early voting. This effort was enormously successful. Nearly half of voters ended up voting by mail, and another quarter voted early. It was, Ball wrote, “practically a revolution in how people vote.” Another major part was to raise an army of progressive activists to administer the election at the ground level. Here, one billionaire in particular took a leading role: Facebook founder Mark Zuckerberg.
Zuckerberg’s help to Democrats is well known when it comes to censoring their political opponents in the name of preventing “misinformation.” Less well known is the fact that he directly funded liberal groups running partisan get-out-the-vote operations. In fact, he helped those groups infiltrate election offices in key swing states by doling out large grants to crucial districts.
The Chan Zuckerberg Initiative, an organization led by Zuckerberg’s wife Priscilla, gave more than $400 million to nonprofit groups involved in “securing” the 2020 election. Most of those funds—colloquially called “Zuckerbucks”—were funneled through the Center for Tech and Civic Life (CTCL), a voter outreach organization founded by Tiana Epps-Johnson, Whitney May, and Donny Bridges. All three had previously worked on activism relating to election rules for the New Organizing Institute, once described by The Washington Post as “the Democratic Party’s Hogwarts for digital wizardry.”
Flush with $350 million in Zuckerbucks, the CTCL proceeded to disburse large grants to election officials and local governments across the country. These disbursements were billed publicly as “COVID-19 response grants,” ostensibly to help municipalities acquire protective gear for poll workers or otherwise help protect election officials and volunteers against the virus. In practice, relatively little money was spent for this. Here, as in other cases, COVID simply provided cover.
According to the Foundation for Government Accountability (FGA), Georgia received more than $31 million in Zuckerbucks, one of the highest amounts in the country. The three Georgia counties that received the most money spent only 1.3 percent of it on personal protective equipment. The rest was spent on salaries, laptops, vehicle rentals, attorney fees for public records requests, mail-in balloting, and other measures that allowed elections offices to hire activists to work the election. Not all Georgia counties received CTCL funding. And of those that did, Trump-voting counties received an average of $1.91 per registered voter, compared to $7.13 per registered voter in Biden-voting counties.
The FGA looked at this funding another way, too. Trump won Georgia by more than five points in 2016. He lost it by three-tenths of a point in 2020. On average, as a share of the two-party vote, most counties moved Democratic by less than one percentage point in that time. Counties that didn’t receive Zuckerbucks showed hardly any movement, but counties that did moved an average of 2.3 percentage points Democratic. In counties that did not receive Zuckerbucks, “roughly half saw an increase in Democrat votes that offset the increase in Republican votes, while roughly half saw the opposite trend.” In counties that did receive Zuckerbucks, by contrast, three quarters “saw a significant uptick in Democrat votes that offset any upward change in Republican votes,” including highly populated Fulton, Gwinnett, Cobb, and DeKalb counties.
Of all the 2020 battleground states, it is probably in Wisconsin where the most has been brought to light about how Zuckerbucks worked.
CTCL distributed $6.3 million to the Wisconsin cities of Racine, Green Bay, Madison, Milwaukee, and Kenosha—purportedly to ensure that voting could take place “in accordance with prevailing [anti-COVID] public health requirements.”
Wisconsin law says voting is a right, but that “voting by absentee ballot must be carefully regulated to prevent the potential for fraud or abuse; to prevent overzealous solicitation of absent electors who may prefer not to participate in an election.” Wisconsin law also says that elections are to be run by clerks or other government officials. But the five cities that received Zuckerbucks outsourced much of their election operation to private liberal groups, in one case so extensively that a sidelined government official quit in frustration.
This was by design. Cities that received grants were not allowed to use the money to fund outside help unless CTCL specifically approved their plans in writing. CTCL kept tight control of how money was spent, and it had an abundance of “partners” to help with anything the cities needed.
Some government officials were willing to do whatever CTCL recommended. “As far as I’m concerned I am taking all of my cues from CTCL and work with those you recommend,” Celestine Jeffreys, the chief of staff to Democratic Green Bay Mayor Eric Genrich, wrote in an email. CTCL not only had plenty of recommendations, but made available a “network of current and former election administrators and election experts” to scale up “your vote by mail processes” and “ensure forms, envelopes, and other materials are understood and completed correctly by voters.”
Power the Polls, a liberal group recruiting poll workers, promised to help with ballot curing. The liberal Mikva Challenge worked to recruit high school-age poll workers. And the left-wing Brennan Center offered help with “election integrity,” including “post-election audits” and “cybersecurity.”
The Center for Civic Design, an election administration policy organization that frequently partners with groups such as liberal billionaire Pierre Omidyar’s Democracy Fund, designed absentee ballots and voting instructions, often working directly with an election commission to design envelopes and create advertising and targeting campaigns. The Elections Group, also linked to the Democracy Fund, provided technical assistance in handling drop boxes and conducted voter outreach. The communications director for the Center for Secure and Modern Elections, an organization that advocates sweeping changes to the elections process, ran a conference call to help Green Bay develop Spanish-language radio ads and geofencing to target voters in a predefined area.
Digital Response, a nonprofit launched in 2020, offered to “bring voters an updated elections website,” “run a website health check,” “set up communications channels,” “bring poll worker application and management online,” “track and respond to polling location wait times,” “set up voter support and email response tools,” “bring vote-by-mail applications online,” “process incoming [vote-by-mail] applications,” and help with “ballot curing process tooling and voter notification.”
The National Vote at Home Institute was presented as a “technical assistance partner” that could “support outreach around absentee voting,” provide and oversee voting machines, consult on methods to cure absentee ballots, and even assume the duty of curing ballots.
A few weeks after the five Wisconsin cities received their grants, CTCL emailed Claire Woodall-Vogg, the executive director of the Milwaukee Election Commission, to offer “an experienced elections staffer that could potentially embed with your staff in Milwaukee in a matter of days.” The staffer leading Wisconsin’s portion of the National Vote at Home Institute was an out-of-state Democratic activist named Michael Spitzer-Rubenstein. As soon as he met with Woodall-Vogg, he asked for contacts in other cities and at the Wisconsin Elections Commission.
Spitzer-Rubenstein would eventually take over much of Green Bay’s election planning from the official charged with running the election, Green Bay Clerk Kris Teske. This made Teske so unhappy that she took Family and Medical Leave prior to the election and quit shortly thereafter.
Emails from Spitzer-Rubenstein show the extent to which he was managing the election process. To one government official he wrote, “By Monday, I’ll have our edits on the absentee voting instructions. We’re pushing Quickbase to get their system up and running and I’ll keep you updated. I’ll revise the planning tool to accurately reflect the process. I’ll create a flowchart for the vote-by-mail processing that we will be able to share with both inspectors and also observers.”
Once early voting started, Woodall-Vogg would provide Spitzer-Rubenstein with daily updates on the numbers of absentee ballots returned and still outstanding in each ward—prized information for a political operative.
Amazingly, Spitzer-Rubenstein even asked for direct access to the Milwaukee Election Commission’s voter database: “Would you or someone else on your team be able to do a screen-share so we can see the process for an export?” he wrote. “Do you know if WisVote has an [application programming interface] or anything similar so that it can connect with other software apps? That would be the holy grail.” Even for Woodall-Vogg, that was too much. “While I completely understand and appreciate the assistance that is trying to be provided,” she replied, “I am definitely not comfortable having a non-staff member involved in the function of our voter database, much less recording it.”
When these emails were released in 2021, they stunned Wisconsin observers. “What exactly was the National Vote at Home Institute doing with its daily reports? Was it making sure that people were actually voting from home by going door-to-door to collect ballots from voters who had not yet turned theirs in? Was this data sharing a condition of the CTCL grant? And who was really running Milwaukee’s election?” asked Dan O’Donnell, whose election analysis appeared at Wisconsin’s conservative MacIver Institute.
Kris Teske, the sidelined Green Bay city clerk—in whose office Wisconsin law actually places the responsibility to conduct elections—had of course seen what was happening early on. “I just don’t know where the Clerk’s Office fits in anymore,” she wrote in early July. By August, she was worried about legal exposure: “I don’t understand how people who don’t have the knowledge of the process can tell us how to manage the election,” she wrote on August 28.
Green Bay Mayor Eric Genrich simply handed over Teske’s authority to agents from outside groups and gave them leadership roles in collecting absentee ballots, fixing ballots that would otherwise be voided for failure to follow the law, and even supervising the counting of ballots. “The grant mentors would like to meet with you to discuss, further, the ballot curing process. Please let them know when you’re available,” Genrich’s chief of staff told Teske.
Spitzer-Rubenstein explained that the National Vote at Home Institute had done the same for other cities in Wisconsin. “We have a process map that we’ve worked out with Milwaukee for their process. We can also adapt the letter we’re sending out with rejected absentee ballots along with a call script alerting voters. (We can also get people to make the calls, too, so you don’t need to worry about it.)”
Other emails show that Spitzer-Rubenstein had keys to the central counting facility and access to all the machines before election night. His name was on contracts with the hotel hosting the ballot counting.
Sandy Juno, who was clerk of Brown County, where Green Bay is located, later testified about the problems in a legislative hearing. “He was advising them on things. He was touching the ballots. He had access to see how the votes were counted,” Juno said of Spitzer-Rubenstein. Others testified that he was giving orders to poll workers and seemed to be the person running the election night count operation.
“I would really like to think that when we talk about security of elections, we’re talking about more than just the security of the internet,” Juno said. “You know, it has to be security of the physical location, where you’re not giving a third party keys to where you have your election equipment.”
Juno noted that there were irregularities in the counting, too, with no consistency between the various tables. Some had absentee ballots face-up, so anyone could see how they were marked. Poll workers were seen reviewing ballots not just to see that they’d been appropriately checked by the clerk, but “reviewing how they were marked.” And poll workers fixing ballots used the same color pens as the ones ballots had been filled out in, contrary to established procedures designed to make sure observers could differentiate between voters’ marks and poll workers’ marks.
The plan by Democratic strategists to bring activist groups into election offices worked in part because no legislature had ever imagined that a nonprofit could take over so many election offices so easily. “If it can happen to Green Bay, Wisconsin, sweet little old Green Bay, Wisconsin, these people can coordinate any place,” said Janel Brandtjen, a state representative in Wisconsin.
She was right. What happened in Green Bay happened in Democrat-run cities and counties across the country. Four hundred million Zuckerbucks were distributed with strings attached. Officials were required to work with “partner organizations” to massively expand mail-in voting and staff their election operations with partisan activists. The plan was genius. And because no one ever imagined that the election system could be privatized in this way, there were no laws to prevent it.
Such laws should now be a priority.” See here.
Let’s do everything we can to publicize the steal. That way, we have a chance to prevent it.
NATO troops active in Ukraine – El Pais
RT | March 19, 2024
Active and former military personnel from NATO states have long been operating in Ukraine, overseeing Kiev’s use of Western-supplied weapons, El Pais reported on Monday.
The US-led military bloc has been involved “in virtually every possible aspect” of the hostilities aside from active combat operations, the Spanish newspaper claimed. That includes supplying weapons, providing targeting information, and training Ukrainian soldiers inside the country, El Pais reported, citing interviews conducted throughout the conflict.
Retired foreign military service members who have joined the Ukrainian armed forces as “volunteers” are also serving as de facto agents for their home nations, El Pais said. They provide “knowledge about the situation on the front, to identify the effectiveness of the weapons supplied and possible problems in their use, as well as to detect possible cases of corruption concerning the aid provided,” the outlet claimed.
The presence of current and former NATO troops has been tacitly admitted by officials, the Spanish newspaper reported. It described recent suggestions by French President Emmanuel Macron that Western nations could send soldiers to Ukraine as “taboo-breaking,” in the sense of proposing active combat roles for Western military personnel.
While a handful of Western leaders have backed Macron’s position that deployments to aid Kiev in the conflict with Russia cannot be ruled out, numerous officials – including NATO Secretary General Jens Stoltenberg – have dismissed the idea.
Moscow perceives the Ukraine conflict as a US-led proxy war against Russia, in which Ukrainians serve as ‘cannon fodder’ for Western interests. It considers foreigners fighting for Kiev as “mercenaries” who are doing the bidding of Western governments.
“We hear both French and English speech there [in the Ukraine conflict]. There is nothing good in this, first of all for them, because they die there and in large numbers,” President Vladimir Putin said last week, commenting on Macron’s remarks on potential Western troop deployments.
Senior Russian officials have suggested that more complex weapon systems provided to Kiev are highly likely operated by NATO staff, as there was not sufficient time to train Ukrainians on how to handle them.
Last month, German Chancellor Olaf Scholz revealed the involvement of British and French forces in preparing Ukrainian missile launches, as he explained why Berlin would not supply similar weapons to Kiev.
The more thoroughly exposed the CIA’s true face, the better
Mother of all disorder Illustration: Liu Rui/GT
Global Times | March 15, 2024
Reuters exclusively reported on Thursday that, according to a former US official with direct knowledge of highly confidential operations, then-US president Donald Trump authorized the Central Intelligence Agency (CIA) to launch secret operations on Chinese social media aimed at “turning public opinion in China against its government.” Many people don’t find this information surprising or even consider it “news.” The US is a habitual offender, using various covert means to foment “peaceful evolution” and “color revolutions” in other countries, with the CIA being the main force employed to this end. For other countries, the US’ pervasive influence is everywhere, visible and tangible, so there is no need for exposés.
We are still unclear what the specific purpose of the “former US official” was in leaking the information to Reuters. A CIA spokesperson declined to comment on the existence of the program, its goals or impact. A spokesperson for the Biden administration’s National Security Council also declined to comment, which means it was neither confirmed nor denied. The US intelligence community often uses a mixture of false and true information to create confusion, a tactic that was used on Edward Snowden. The Reuters report is valuable, but needs to be further processed to filter out the true and useful parts.
Firstly, this report carries a strong defense of US penetration into China. It portrays the proactive offensive of the US’ cognitive warfare against China as a passive counterattack against “cyber attacks” on the US from China and Russia. In reality, portraying themselves as the weak or victimized party and labeling their hegemonic actions as “justice” is a part of the US’ cognitive warfare against foreign countries.
One US official interviewed by Reuters even said it felt like China was attacking the US with “steel baseball bats,” while the US could only fight back with “wooden ones,” showing his exaggerated and clumsy acting skills. The US has never used a “wooden stick.” Over the past few decades, the CIA has overthrown or attempted to overthrow at least 50 legitimate international governments. There are also statistics showing that from 1946 to 2000, the US attempted to influence elections in 45 countries 81 times to achieve regime change. As a habitual offender of manipulating public opinions, the US has long established a series of tactics in its targeted propaganda, information dissemination, event creation, rumor fabrication, incitement of public opinion, and media manipulation. It constantly creates new tactics and uses new technologies according to changing circumstances. This is an open secret. The US dressing itself up as a “little lamb” only has a comedic effect, not a propaganda effect.
Next, as the US’ intervention and infiltration in other countries are covert operations, this disclosure provides an opportunity for the outside world to glimpse into the specific methods used by the US. For example, the whistleblower admitted that the CIA had formed a small team of operatives, using bogus online identities to spread damaging stories about the Chinese government while simultaneously disseminating defamatory content to overseas news agencies. This corroborates with previous statements by CIA Director William Burns, indicating increased resources being allocated for intelligence activities against China, once again confirming the existence of the US “1450” (internet water army) team targeting China.
The whistleblower admitted that the CIA has targeted public opinion in Southeast Asia, Africa, and the South Pacific region, spreading negative narratives about the Belt and Road Initiative. This indicates that in the US-instigated propaganda war against China, the global public opinion arena, especially in “Global South” countries, is their main strategic target. Various “China threat” theories circulating in third-party countries, as consistently pointed out by China, are all being operated by the US intelligence agencies behind the scenes.
The US has never concealed its hegemonic aims, nor does it regard encroachment on other countries’ sovereignty as something to be ashamed of, which is even more infuriating than the hegemonic behavior itself. American economist Jeffrey Sachs criticized the CIA’s blatant violation of international law in his commentary last month, stating that it is “devastating to global stability and the US rule of law,” leading to “an escalating regional war, hundreds of thousands of deaths, and millions of displaced people.” He also criticized the mainstream American media for failing to question or investigate the CIA. In fact, far from acting as watchdogs, mainstream American media has served as an accomplice. How many rumors manufactured by the CIA have been spread through the mouths of mainstream American media? When did they reflect and correct themselves?
We also see that the intentions of the US intelligence agencies are even more sinister. As admitted in the revelations, they aim to force China to spend valuable resources in defending against “cognitive warfare,” keeping us busy with “chasing ghosts,” and disrupting our development pace. First of all, we appreciate their reminder. At the same time, we will not allow external factors to interfere with our strategic determination to manage our own affairs well. For China and the world, the more fully, clearly, and thoroughly the CIA exposes itself, the deeper people will understand its true nature, and the stronger their ability to discern the truth will become. Keeping the CIA busy to no end or failing in their attempts is the best preventive effect.
Featured Video

Israeli Military Medics Are Training On Dead Americans
or go to
Aletho News Archives – Video-Images
From the Archives
On ‘conflict’, ‘peace’ and ‘genocide’: Time for new language on Palestine

By Ramzy Baroud | MEMO | June 12, 2021
On 25 May, famous US actor Mark Ruffalo tweeted an apology for suggesting that Israel is committing “genocide” in Gaza.
“I have reflected and wanted to apologise for posts during the recent Israel/Hamas fighting that suggested Israel is committing ‘genocide’,” Ruffalo wrote, adding: “It’s not accurate, it’s inflammatory, disrespectful and is being used to justify anti-Semitism, here and abroad. Now is the time to avoid hyperbole.”
But were Ruffalo’s earlier assessments, indeed, “not accurate, inflammatory and disrespectful”? And does equating Israel’s war on besieged, impoverished Gaza with genocide fit into the classification of “hyperbole”? … continue
Blog Roll
 Aletho News
Aletho News- Intelligence Agency Investigating CIA Whistleblower Allegations, Official Confirms
- AIPAC Favorite Ed Gallrein Wants to Bring Back the Draft
- A decade of lies: The US-funded biolab denial saga
- Mainstream US media complicit in selling Gaza genocide, sweeping new analysis finds
- US Overseas Biolabs Probe Aims to Rein in ‘Deep State’ Bureaucracy
- ‘Death to Arabs’: Settler mobs storm Jerusalem’s Muslim, Christian quarters for ‘Flag March’
- China’s position on Iran, Hormuz remains unchanged
- Israeli Military Medics Are Training On Dead Americans
- SCOTT RITTER: Russia Retaliation on Europe No Longer In Doubt
- Guatemala Admits U.S. Pressure Over Cuban Doctors
- If Americans Knew
- We Can’t Curb Nuclear Proliferation If We Don’t Acknowledge Israel’s Nukes
- 43,000 people in Gaza suffered life-changing injuries since October 2023: WHO
- Israel’s 7 October narrative under fresh scrutiny after army accused of deleting footage
- Ex-CENTCOM chief headlines lavish Israeli-American Council gala
- Israel’s 7 October rape hoax gets a 300-page reboot
- Chants of ‘death to Arabs,’ calls for destruction of Al-Aqsa Mosque in racist Jerusalem Day march
- What Fuels My Revolutionary Optimism This Nakba Day
- Gaza elders who survived the Nakba reflect on being displaced by Israel again, 78 years later
- Israel (with US assistance) perpetuates the Nakba; Palestinians remain resilient – Daily Update
- Microsoft fires head of Israeli subsidiary and other managers over surveillance of Palestinians
- No Tricks Zone
- German Expert: “No Climate Crisis” …”Warming Generally Better For Humanity”
- New Paleo Research: Modern ‘Climate Change’ Has Had No Apparent Impact On Precipitation Patterns
- 90% Subsidized… Bielefeld Germany’s €7 Million Hydrogen Garbage Truck Fleet Sits Idle
- New Study: Declining Trends In 1980-2023 Tropical Cyclone Frequency, Accumulated Energy
- 46 IPCC Scientists Break Rank, Publicly Challenge Long-Standing Dogmatic Climate Claims
- Another Study Links Warming To Cloud Forcing, Shortwave Radiation, Natural Atmospheric Circulation
- Wind Energy Is Toxic, Hazardous To Human Health, Scientific Review Shows
- Oversupply Of Volatile Solar Energy Leads To Record NEGATIVE Prices!
- New Study: Extreme Heat Records, Heatwaves, Extreme Cold Records Declining Across US Since 1899
- It’s The Cold, Stupid! Cold 20 Times More Lethal Than Heat, Multiple Studies Show
