“We call upon the Charity Commission to conduct an independent and urgent investigation into these very serious allegations relating to the British Heart Foundation.”
Joint Open Letter from Doctors for Patients UK, HART and the UK Medical Freedom Alliance to Helen Stephenson, CEO, Charity Commission
Cc: Dr Charmaine Griffiths, CEO, British Heart Foundation (BHF)
Prof Charalambos Antoniades, BHF Chair of Cardiovascular Medicine
Rt Hon Rishi Sunak, Prime Minister
Rt Hon Steve Barclay, Secretary of State for Health and Social Care
Mr Andrew Bridgen, MP
Re: Allegations that the British Heart Foundation (BHF) is involved in concealing and withholding important information relating to harms to cardiac function caused by the novel mRNA vaccines
31 January 2023
Dear Ms Stephenson
We wish to express our deep concern, regarding allegations that the British Heart Foundation (BHF) is involved in concealing and withholding important information relating to the potential of the novel mRNA vaccines to damage cardiac tissue and function.
It was alleged in the House of Commons that staff working in a cardiology research department at Oxford University withheld information, for fear of losing funding from the pharmaceutical industry, and were therefore prioritising funding over patient safety.
Mr Andrew Bridgen MP stated in Parliament on 13 December 2022:
“It has also been brought to my attention by a whistleblower from a very reliable source that one of these institutions is covering up clear data that reveals that the mRNA vaccine increases inflammation of the heart arteries. It is covering this up for fear that it may lose funding from the pharmaceutical industry. The lead of that cardiology research department has a prominent leadership role with the British Heart Foundation, and I am disappointed to say that he has sent out non-disclosure agreements to his research team to ensure that this important data never sees the light of day. That is an absolute disgrace.”
It was subsequently asserted on GB News that the research department mentioned above was headed by Professor Charalambos Antoniades whose position is funded by the BHF. Despite GB News approaching Professor Antoniades for comment, he has made no public denial that Non-Disclosure Agreements (NDAs) were entered into by members of his department.
Doctors and the public rely on reputable and well-established charities such as the BHF to provide accurate and up-to-date information, as well as to highlight and investigate potential, novel causes of heart damage and heart disease. Concerns should be raised immediately, whenever there are doubts relating to the safety of any pharmaceutical product, so that administration of the product can be halted, protecting the public from unnecessary harm, while an investigation is carried out.
The BHF rapidly dismissed the allegations made by Mr Bridgen and called for those making the allegation to provide specific and credible information in support of it.
Due to the seriousness of the allegations, and given the absence of any public denial or clarification from Professor Antoniades, we are calling for a full and independent investigation into any suppression of data by the British Heart Foundation itself or by senior BHF grant holders.
There are a significant number of signals that COVID-19 vaccines have led to cardiac pathology, which warrants an urgent review of their safety:
The Pfizer trial saw four cardiac arrests in the vaccination group but only one in the placebo group after 6 months (although the numbers are too small to be statistically significant, this was a signal that should have been followed up).
The evidence for vaccine-induced myocarditis is well established and in older patients this may be misdiagnosed as any of the more common forms of heart disease. The rate of myocardial infarction was disproportionately high in the first three days after vaccination.
Studies in Thailand and Switzerland have shown rises in troponin levels consistent with damaged heart muscle in 3% of those vaccinated. Heart cells cannot be replaced and the resulting scarring can lead to electrical conduction issues and sudden death. 30% of the children in the Thailand study had cardiac signs or symptoms.
Vaccine-derived spike protein was detected in the heart biopsies of 9 out of 15 patients with post-vaccination myocarditis.
Vaccinated people had a rise in cardiovascular risk factors that would predict a significantly increased risk of heart disease (from 11% to 25% risk of a heart attack in 5 years). This study has been criticised for not having a control group but is the equivalent of an early phase clinical trial in demonstrating a safety concern.
An Israeli study showed a 25% increase in acute coronary syndrome and cardiac arrest calls in 16-39 year olds associated with the first and second doses of vaccine but not with COVID-19 infection.
There were 14,000 more cardiac arrest calls to ambulances in England in 2021 than 2020.
There has been a rise in cardiac excess deaths and excess deaths have been disproportionately seen in more highly vaccinated groups e.g. less deprived cohorts and people of white ethnicity.
In a report of 35 autopsies in Germany, there were 5 deaths confirmed as caused by a COVID-19 vaccine and a further 20 deaths where a contribution from the vaccination could not be excluded.
Post mortem studies have shown inflammation of the coronary arteries after vaccination, causing death four months later.
A separate post mortem report showed vaccine-derived spike protein in heart muscle, in the absence of COVID-19 infection, in a subject who had myocarditis before he died.
Australian hospitals have experienced intense service pressure since Summer 2021, despite no significant COVID-19 infection rates or reduction in healthcare capacity at that time.
Australians have seen a similarly timed rise in excess non-Covid deaths, with ischaemic heart disease being the biggest contributor. This was despite no significant volume of COVID-19 cases or reduction in healthcare before Omicron as was seen in the UK.
Systematic exploratory analysis of the possible causes in the rise in excess deaths by comparing countries, suggests a link to healthcare quality cannot be excluded but there is no link to COVID-19 or Long Covid. There is a weak link to lockdown severity but a strong correlation with vaccination.
Crucially, data has not been shared to counter the hypothesis that the mRNA vaccinations are linked to recent excess deaths caused primarily by cardiac pathology. The ONS were regularly publishing deaths by vaccination status. The last data was released for May 2022 and showed a higher mortality rate for that month in the vaccinated. No data has been shared since.
As medical professionals, and in the interest of patient safety, we demand that the British Heart Foundation immediately release the following information, in the public interest and in accordance with the requirements of the Freedom of Information Act 2000 (FOIA):
Any and all information and emails regarding potential and actual harms caused by the COVID-19 mRNA vaccines.
A copy of any Non-Disclosure Agreements that have been sent to people working at, or associated with, the British Heart Foundation and Oxford University, relating to COVID-19 vaccine safety and data.
A full list of conflicts of interests that the BHF and Oxford University have relating to the COVID-19 vaccines.
We further call upon the Charity Commission to conduct an independent and urgent investigation into these very serious allegations relating to the British Heart Foundation. Suppression of research findings, conflicts of interest and acting in the interests of commercial entities are in direct conflict with the requirements inherent in holding charitable status.
Thank you for your attention. We look forward to receiving a prompt response.
Professor Richard Ennos, MA, PhD. Honorary Professorial Fellow, University of Edinburgh
Professor John A Fairclough, BM BS, BMed Sci, FRCS, FFSEM(UK), Professor Emeritus, Honorary
Consultant Orthopaedic Surgeon
Professor Dennis McGonagle,PhD, FRCPI, Consultant Rheumatologist, University of Leeds
Professor Anthony Fryer, PhD, FRCPath, Professor of Clinical Biochemistry, Keele University
Professor Karol Sikora, MA, MBBChir, PhD, FRCR, FRCP, FFPM, Honorary Professor of Professional Practice, Buckingham University
Professor Angus Dalgleish, MD, FRCP, FRACP, FRCPath, FMedSci, Professor of Oncology, University of London; Principal, Institute for Cancer Vaccines & Immunotherapy
Professor Roger Watson, FRCP Edin, FRCN, FAAN, Professor of Nursing
Lord Moonie, MBChB, MRCPsych, MFCM, MSc, retired member of House of Lords, former Parliamentary Under-Secretary of State 2001-2003, former Consultant in Public Health Medicine
Dr Najmiah K Ahmad, BM, MRCA, FCARCSI, Consultant Anaesthetist
Dr Ali Ajaz, Consultant Psychiatrist
Dr Shiraz Akram, BDS, Dental Surgeon
Dr Sonia Allam, MBChB, FRCA, Consultant Anaesthetist
Dr Victoria Anderson, MBChB, MRCGP, MRCPCH, DRCOG, General Practitioner
Julie Annakin, RN, Immunisation Specialist Nurse
Wendy Armstrong, RN, BSc, DipHE, Practice Nurse
Dr Abby Astle, MBBChir, BA(Cantab), DCH, DGM, MRCGP, GP Principal, GP Trainer, GP Examiner
Dr Jonathan Eastwood, BSc, MBChB, MRCGP, General Practitioner
Dr Jonathan Engler, MBChB, LlB(Hons), DipPharmMed
Dr Elizabeth Evans, MA(Cantab), MBBS, DRCOG, retired Doctor, Director UKMFA
Dr Chris Exley, PhD, FRSB, retired Professor in Bioinorganic Chemistry
Dr John Flack, BPharm, PhD, retired Director of Safety Evaluation at Beecham Pharmaceuticals 1980-1989 and Senior Vice-president for Drug Discovery 1990-92 SmithKline Beecham
Dr Simon Fox, BSc, BMBCh, FRCP, Consultant in Infectious Diseases and Internal Medicine
Gayle Gerry, BSc(Hons), Registered Nurse
Sophie Gidet, RM, Midwife
Dr Cathy Greig, MBBCh(Hons), General Practitioner
Dr Ali Haggett, Mental Health Community Work, 3rd sector, former Lecturer in the History of Medicine
Mr Anthony Hinton, MBChB, FRCS, Consultant ENT Surgeon, London
Ian Humphreys, UKMFA Programme Director
Dr Keith Johnson, BA, DPhil(Oxon), IP Consultant for Diagnostic Testing
Dr C Geoffrey Maidment, MD, FRCP, retired Consultant Physician
Mr Ahmad K Malik, FRCS(Tr & Orth), Dip Med Sport, Consultant Trauma & Orthopaedic Surgeon
Dr Ayiesha Malik, MBChB, General Practitioner
Dr Imran Malik, MBBS, MRCP, MRCGP, General Practitioner
Dr Kulvinder S Manik. MBChB, MRCGP(2010), MA(Cantab), LlM(Gray’s Inn)
Dr Fiona Martindale, MBChB, MRCGP, General Practitioner
Dr Sam McBride, BSc(Hons) Medical Microbiology & Immunobiology, MBBCh, BAO, MSc in Clinical Gerontology, MRCP(UK), FRCEM, FRCP(Edinburgh), NHS Emergency Medicine & Geriatrics
Kaira McCallum, BSc, retired Pharmacist, Director of Strategy UKMFA
Mr Ian McDermott, MBBS, MS, FRCS(Tr&Orth), FFSEM(UK), Consultant Orthopaedic Surgeon
Dr Scott Mitchell, MBChB, MRCS, Emergency Medicine Physician
Dr Alistair Montgomery, MBChB, MRCGP, DRCOG, retired General Practitioner
Dr Alan Mordue, MBChB, FFPH, retired Consultant in Public Health Medicine & Epidemiology
Dr David Morris, MBChB, MRCP(UK), General Practitioner
Margaret Moss, MA(Cantab), CBiol, MRSB, Director, The Nutrition and Allergy Clinic, Cheshire
Theresa Ann Mounsey, BSc Hons in Midwifery studies.
Dr Alice Murkies, MBBS, MD, FRACGP, General Practitioner and Medical Researcher
Dr Greta Mushet, MBChB, MRCPsych, retired Consultant Psychiatrist in Psychotherapy
Dr Angela Musso, MD, MRCGP, DRCOG, FRACGP, MFPC, General Practitioner
Dr Sarah Myhill, MBBS, Dip NM, Retired GP, Independent Naturopathic Physician
Dr Christopher Newton, PhD, Biochemist, CIMMBER
Dr Rachel Nicoll, PhD, Medical researcher
Tim Nike, BSc(Hons), MCSP, HCPC, Senior Neurological Physiotherapist
Dr Richard O’Shea, MBBCH, BA(Hons) MRCGP, General Practitioner
More good news on vaccine, folks. First, you may be required to take only one Covid-19 shot per year, and if all goes well you will not even have to do that. You will be able to drink or even inhale your vaccine. No more painful injections, just a quick slurp or a snort and the job’s a good ’un. That’s you safe from the deadly virus for another year.
We could even make it fun. Why not hold Covid-19 vaccine parties? A selection of flavours in shot glasses (they don’t call them shot glasses for no reason) or add your vaccine to a vape and puff away until your immune system is primed.
I glean all this garbage from Global Health Now, the daily newsletter from the Johns Hopkins Bloomberg School of Public Health. The first story concerns how the Food and Drug Administration (FDA) in the United States is considering ‘simplifying the Covid vaccination schedule, allowing most people to get the currently available booster, regardless of how many doses they had received before that’. This means that if you are boosted up to the eyeballs or have never had one before and suddenly made the incomprehensible decision to start now, then Bob’s your uncle; roll up your sleeves.
Please note that nothing has changed; there is no new vaccine and no new threat. The FDA is just making an arbitrary decision to change the schedule. Clearly the aim is to get more people to accept the vaccination. But it is also clear that they are making this stuff up as they go along. They have no further evidence that the vaccines will work any better this way.
The information that is available to them is the abundant and accumulating evidence of vaccine harms which, incredibly, the Medicines and Healthcare products Regulatory Agency (MRHA) in the United Kingdom admits can be serious while insisting that the vaccines are safe. If truth is the first casualty of war – it certainly died early in the Covid-19 madness – logic is not far behind it. The MRHA is willing to trade off serious vaccine side effects against minimal protection from a virus which is virtually harmless to the vast majority of people. Perhaps the FDA is trying to reduce the number of boosters it says people will need in the hope that vaccine injuries will go away. Alternatively, it may be keen to accelerate the rollout before the general population wakes up to the fact that they are being conned, if they are lucky, and killed if they are not.
The potential for a drinkable/snortable/inhalable vaccine comes courtesy of US Speciality Formulations, a company which has produced the QYNDR vaccine. If QYNDR is a bit of a consonant-rich mouthful, then be informed that the official pronunciation if ‘KINDER’. And the advent of QYNDR is closer than you think. Phase 1 trials have already been completed in New Zealand (where else?) and all that is required is more funding to proceed with further trials. Apparently, it is very difficult to formulate a vaccine that survives the vicissitudes of the digestive tract.
And why do we need these vaccines? Well, according to US Speciality Formulations: ‘Covid-19 is still here and deadly.’ Also, I imagine that the inventors and investors envisage that this will make them shedloads of money. It clearly pays to perpetuate the Covid-19 narrative and to pepper it with as much panic as possible.
At some point in the panic-demic, the vaccine rollout became a juggernaut. Large and hard to stop. With the widespread and obvious extent to which people are gullible, government and drug manufacturers are willing to lie, health professionals are willing to stay silent and there are bucks to be made, it is unlikely that the juggernaut will be halted any time soon.
Who knows what’s next? Perhaps they will develop a vaccine that one can stick up one’s bottom. Whether or not they do, I strongly advise them that is what they can do with the present products.
We genuinely urge doctors involved with medical regulation not to go down with the sinking ship of authoritarian censorship and suppression of intellectual freedom. Not only is this behaviour historically illiterate and intellectually feeble, it is putting the safety of patients at risk, causing hazards to public health, runs counter to our community standards of a liberal democracy, and sits in conflict with the societal benefits of intellectual freedom that have recently been stated by the High Court of Australia.
When has there been a society that prospers because people are cancelled, removed, or ‘disappeared’ from their vital work because they dared to disagree with the ‘regime’s unquestionable truth?’ Do our modern medical authoritarians want to be looked back on with the same pathetic disdain with which we judge similar historical despots?
In this article we present two rays of hope in the context that the tide is changing. Firstly, for those doctors who genuinely want to have an open expression of ideas, there is a High Court precedent about the benefits to society of intellectual freedom where professional views asserted in the context of intellectual freedom can be expressed forcefully even if they cause offence, embarrassment, or lack of trust.
Secondly, for those doctors who continue to persecute other doctors for participating in the act of intellectual freedom, accumulated medical, ethical and legal information – we believe this warrants consideration that those doctors involved with AHPRA and the Medical Board of Australia themselves have their licenses suspended as they potentially pose a danger to the public’s health, in our opinion.
Go forth and be confident in the concept of intellectual freedom
Recent controversy has surrounded the sanctioning, by regulatory authorities, of doctors for publicly expressing views on elements of the Covid pandemic. Doctors have been punished because they sought to bring critical (if not ideologically uncomfortable) medical information to the public’s awareness.
This controversy is fundamentally about the limits of intellectual freedom doctors have within the constraints of general, and often highly subjective, Codes of Conduct that doctors must adhere to. In this context, a recent unanimous High Court of Australia judgment gives an important window into how the Court considers what the boundaries of intellectual freedom are and how the Court considers attempts by authorities to curtail such freedom under the guise of ‘conduct.’ (Find the example in detail at the end of the article.)
Although the case of Ridd v James Cook University (JCU) involved specific clauses within an Enterprise Bargaining Agreement, the High Court included valuable commentary on the societal importance of intellectual freedom from an instrumental, ethical, and historical perspective. This provides a useful context for academic freedom in general. Inherent in the developed concept of intellectual freedom is the ability to dissent against the establishment narrative. It is one of the modern marvels of living in a liberal democracy and brings tremendous benefit to society, as affirmed by the High Court:
‘Once developed, justification for intellectual freedom is instrumental. The instrumental justification is the search for truth in the contested marketplace of ideas, the social importance of which Frankfurter J spoke powerfully about.’
The Court further affirmed that:
‘Another justification is ethical rather than instrumental. Intellectual freedom plays “an important ethical role, not just in the lives of the few people it protects, but in the life of the community more generally” to ensure the primacy of individual conviction: “not to profess what one believes to be false” and “a duty to speak out for what one believes to be true.”’
Although doctors do not have a specific clause guaranteeing them the right to intellectual freedom, the High Court’s discussion of the societal benefits makes it difficult to argue that doctors should be punished for participation in the act of intellectual freedom.
There have been suggestions that the sanctioning of doctors has not necessarily been for the content of their views but how they have expressed them; invoking concepts such as incivility, rudeness, bullying, and harassment.
The Court explicitly addressed this issue in Ridd v JCU and was forthright in the view that intellectual freedom is not always pretty and wrapped in civility; curtailment on these grounds necessarily involves an assault on the fundamental phenomenon of intellectual freedom itself:
‘The instrumental and ethical foundations for the developed concept of intellectual freedom are powerful reasons why it has rarely been restricted by any asserted “right” of others to respect or courtesy … however desirable courtesy and respect might be, the purpose of intellectual freedom must permit of expression that departs from those civil norms.’
Furthermore, the Court reinforced the concept that there is no right against embarrassment or against lack of trust resulting from someone else’s assertions made in the course of intellectual freedom.
The Court quotes Dworkin:
‘The idea that people have that right [to protection from speech that might reasonably be thought to embarrass or lower others’ esteem for them or their own self-respect] is absurd. Of course, it would be good if everyone liked and respected everyone else who merited that response. But we cannot recognise a right to respect, or a right to be free from the effects of speech that makes respect less likely, without wholly subverting the central ideals of the culture of independence and denying the ethical individualism that culture protects.’
For the public’s safety it’s time to cancel the cancellers
It is absolutely frightening that major medico-legal organisations have issued advice to doctors to be wary about participating in intellectual freedom and that even reporting on evidence-based scientific data might put them in peril of being professionally ‘disappeared’ if that data doesn’t conform with the government’s ‘messaging.’ Is that what the community at large expects?
Sure, the regime may allow some new information if it is from a regime-approved source and disseminated in a way that the regime approves. But that defeats the whole purpose of intellectual freedom and merely perpetuates the formation of insular establishment echo chambers. A previous article showed the mass lethality of that group-think and establishment thinking during the first world war until dissident thinkers like General Sir John Monash came along.
But what about supposedly ‘bad ideas?’
Firstly, if those ideas are plausible, then as the High Court says, the truth is found in the ‘contested marketplace of ideas.’ If they are really bad ideas, then the sunlight of rigorous intellectual critique is the best disinfectant. Does driving a bad idea underground really make people think, ‘Oh well, the government told me it’s wrong, so it must be?’
Dr Li Wenliang was credited as one of the first doctors in Wuhan to sound the alarm about Covid on social media.
‘In early January (2020), he was called in by both medical officials and the police, and forced to sign a statement denouncing his warning as an unfounded and illegal rumor.’ [New York Times] Sound familiar?
And it is accepted that chilling the expression of ideas (by making people scared to speak out) is just as detrimental as the specific banning of ideas.
Scholars of history, the Australian public at large, Dr Li and the High Court of Australia, understand the importance of the developed concept of intellectual freedom.
In this context, intellectual freedom is so important to knowledge advancement through, as the High Court ruled regarding ‘the contested marketplace of ideas,’ that banning intellectual freedom (unilaterally removing that contested marketplace) poses a serious risk to public health. Therefore, should doctors associated with AHPRA or the Medical Board of Australia who have participated at all in the dangerous repression of intellectual freedom have their licences to practice medicine immediately suspended while a thorough investigation is undertaken into their fitness to practice?
What builds trust in an institution? Intellectual freedom through open scientific discourse or enforced adherence to the regime’s singular ‘truth’ under the threat of professional excommunication?
Public health is still dependent on individuals receiving informed consent about treatments, consent being specific to the individual patient.
This introduces the last issue where transparency should be favoured over repression. If any information comes to light that would materially alter someone’s decision to give/not give consent (and that information was suppressed as a result of the chilling effect on intellectual freedom by AHPRA/Medical Board’s censorship), then AHPRA and the Medical Board should be open to both civil and criminal liability for any harm caused due to the silence they fashioned.
Statements by the High Court of Australia in Ridd v James Cook University
One developed justification for intellectual freedom is instrumental. The instrumental justification is the search for truth in the contested marketplace of ideas, the social importance of which Justice Felix Frankfurter spoke powerfully about in Sweezy v New Hampshire. Another justification is ethical rather than instrumental. Intellectual freedom plays ‘an important ethical role not just in the lives of the few people it protects, but in the life of the community more generally’ to ensure the primacy of individual conviction: ‘Not to profess what one believes to be false’ and ‘a duty to speak out for what one believes to be true.’
Whilst different views might reasonably be taken about some additional restrictions upon intellectual freedom, the instrumental and ethical foundations for the developed concept of intellectual freedom are powerful reasons why it has rarely been restricted by any asserted ‘right’ of others to respect or courtesy. It is not necessary to go as far as Said’s assertion that ‘the whole point [of an intellectual] is to be embarrassing, contrary, even unpleasant’ to conclude that, however desirable courtesy and respect might be, the purpose of intellectual freedom must permit of expression that departs from those civil norms.
JCU’s submission depends upon drawing a distinction between what is said and how it is said. But such a distinction may not exist. The content of what is said often depends upon how it is said. This is particularly so when impugned speech concerns the expression of an opinion. The content of speech that expresses an opinion will often be inseparable from the strength of conviction with which the opinion is held, which is tied to the manner of expression. The message conveyed by a statement, expressed tentatively ‘It may be that it was an error for Professor Jones to claim that the earth is flat’ expresses a proposition only of possibility. It cannot be divorced from the tentative manner in which it was expressed. By contrast, ‘no reasonable person could ever claim that the earth is flat’ expresses a proposition of certainty, all the more so if it is expressed in an emphatic manner.
That interpretation aligns with the long-standing core meaning of intellectual freedom. Whilst a prohibition upon disrespectful and discourteous conduct in intellectual expression might be a ‘convenient plan for having peace in the intellectual world,’ the ‘price paid for this sort of intellectual pacification, is the sacrifice of the entire moral courage of the human mind.’ The 2016 Censure given to Dr Ridd was, therefore, not justified.
Michael Keane is adjunct associate professor, Swinburne University, Adjunct senior lecturer, Monash University and a specialist anaesthetist.
Top Cardiologist and The HighWire Contributor, Dr. Peter McCullough, was sued by health giant Baylor Scott & White, over an alleged violation of his separation agreement. On January 23rd, a Dallas County District Court dismissed the case with prejudice. Del announces the development, and offers his thoughts as well as congratulations to Dr. McCullough over the ‘win for freedom.’
The Covid emergency is over in America… in three more months says the White House. Why now? Is politics at the heart of this decision? And what does it mean for the EUA vaccines and therapies? The HighWire gets to the facts behind the headlines.
Merck’s oral antiviral pill for COVID-19, molnupiravir — marketed under the name Lagevrio — may be fueling the development of new and potentially deadly variants of COVID-19, according to the authors of a new preprint study.
The study, released Jan. 27 by a team of U.S. and U.K researchers, found, “It is possible that some patients treated with molnupiravir might not fully clear SARS-CoV-2 infections, with the potential for onward transmission of molnupiravir-mutated viruses.”
The study, which is pending peer review, followed the discovery by a middle school science and math teacher in Indiana who found numerous variants of COVID-19 emerged after molnupiravir began to be widely distributed.
“It’s not a surprise that molnupiravir could cause [the] escape of mutant virus strains or substrains into the population,” said Dr. Harvey Risch. “Its main function is to get the virus to mutate faster.”
Risch, professor emeritus and senior research scientist in epidemiology (chronic diseases) at the Yale School of Public Health, told The Defender:
“The idea is that it will mutate itself to death. But some live mutants could get out, and this paper gives evidence that they have.”
Brian Hooker, Ph.D., P.E., chief scientific officer for Children’s Health Defense, said the study’s authors scanned global SARS-CoV-2 sequence databases looking for mutations characteristic of those by molnupiravir (G-to-A and C-to-U) and found an uptick of those mutants starting in 2022 — after molnupiravir was put on the market and specifically in countries where molnupiravir was distributed.
“Although this isn’t ‘direct proof’ that the mutations came directly from molnupiravir use,” Hooker told The Defender, “the evidence is very compelling, confirming the fears of many who warned of this prior to FDA [U.S. Food and Drug Administration] approval of the drug in late 2021.”
The FDA granted molnupiravir Emergency Use Authorization (EUA) on Dec. 23, 2021, for use in mild-to-moderate COVID-19 infections in patients 18 and over.
The EUA came just one day after the FDA authorized Pfizer’s COVID-19 antiviral treatment Paxlovid.
Merck this week announced massive revenues from sales of molnupiravir in 2022, but projected a significant decrease in those sales in 2023.
The FDA on Wednesday removed the requirement that a person has to test positive for COVID-19 in order to get a prescription for molnupiravir or Paxlovid.
‘I think we are courting disaster’
Molnupiravir “works by creating mutations in the COVID-19 genome that prevent the virus from replicating in the body, reducing the chances it will cause severe illness,” according to Bloomberg.
However, according to Science, the findings of the preprint study suggest “some people treated with the drug generate novel viruses that not only remain viable, but spread.”
This finding “underscores the risk of trying to intentionally alter the pathogen’s genetic code,” leading some researchers to “worry the drug may create more contagious or health-threatening variations of COVID,” Bloomberg reported.
“It’s very clear that viable mutant viruses can survive [molnupiravir treatment] and compete [with existing variants],” Haseltine told Science. “I think we are courting disaster.”
According to the Gateway Pundit, “When one studies how Lagevrio works, this should not come as a shock. The pill attacks the COVID virus by trying to alter its genetic code.”
The Gateway Pundit reported:
“Once inside a human cell, a virus can make 10,000 copies of its genetic code in a few hours. Each copy made increases the risk the virus makes a rare mistake and creates an inexact replica.
“This is how mutations happen as we have seen with COVID. A drug that deliberately alters a virus’s genetic code would greatly increase the mutation risk.”
Dr. Jonathan Li, a virologist and the director of Li Laboratory, associated with Harvard Medical School and Brigham and Women’s Hospital, told Bloomberg :
“There’s always been this underlying concern that it could contribute to a problem generating new variants. This has largely been hypothetical, but this preprint validates a lot of those concerns.”
According to Science, Haseltine and other scientists have long worried that molnupiravir would create COVID-19 mutations that “would survive and propagate — and perhaps turn out to be more transmissible or virulent than before.”
A Merck spokesperson described that theory as “an interesting hypothetical concern,” prior to the drug receiving EUA.
The same scientists also worried that aside from the virus, the DNA of those receiving the drug might also mutate, Science reported.
These concerns led “researchers and citizen scientists” to examine COVID-19 genome sequences cataloged in the international GISAID (Global Initiative on Sharing Avian Influenza Data) database, seeking to identify mutations likely to be caused by molnupiravir.
‘Clearly something is happening here’
Searching for these mutations was based on the premise that, “Rather than inducing random changes in the virus’ RNA genome, [molnupiravir] is more likely to cause specific nucleic acid substitutions, with guanine switching to adenine and cytosine to uracil,” added Science.
Through this process, Ryan Hisner, a middle school science and math teacher from Monroe, Indiana — described by Science as a “virus hunter” — ultimately “identified dozens of sequences that showed clusters of those hallmark substitutions.”
Hisner took to Twitter with his concerns, where he came into contact with Thomas Peacock, Ph.D., a virologist at the Imperial College London. They and other U.K. and U.S. researchers “systematically reviewed more than 13 million SARS-CoV-2 sequences in GISAID and analyzed those with clusters of more than 20 mutations,” according to Science.
The team found “a large subset showed the hallmark substitutions; all dated from 2022, after molnupiravir began to be widely used,” Science reported.
According to the preprint study, Molnupiravir, “acts by inducing mutations in the virus genome during replication. Most random mutations are likely to be deleterious to the virus, and many will be lethal.”
However, the researchers wrote:
“It is possible that some patients treated with molnupiravir might not fully clear SARS-CoV-2 infections, with the potential for onward transmission of molnupiravir-mutated viruses.
“We set out to systematically investigate global sequencing databases for a signature of molnupiravir mutagenesis. We find that a specific class of long phylogenetic branches appear almost exclusively in sequences from 2022, after the introduction of molnupiravir treatment, and in countries and age groups with widespread usage of the drug.
“Our data suggest a signature of molnupiravir mutagenesis can be seen in global sequencing databases, in some cases with onwards transmission.”
Peacock told Science these “signature clusters” were up to 100 times more likely to be identified in countries where molnupiravir was widely used, including the U.S., U.K. and Australia, as compared to countries such as Canada and France, where it was not in widespread use.
“Clearly something is happening here,” said Peacock.
Merck: ‘no evidence’ any antiviral agent has contributed to the emergence of circulating variants’
Theo Sanderson, Ph.D., a geneticist at the Francis Crick Institute and co-author of the preprint, told Science “We are not coming to a conclusion about risk” just yet, with regard to whether or not these mutations may lead to more severe COVID-19 variants.
Indeed, according to the preprint study, the variants identified by the researchers have not been shown to be more lethal or more evasive to immunity than other existing strains of COVID-19.
However, Haseltine illustrated the potential risk via the analogy of owning a pet lion: “Just because it didn’t bite you yesterday doesn’t mean it won’t bite you today.”
According to the Gateway Pundit :
“Merck was warned by multiple scientists their drug might create problematic mutations which would render the virus more dangerous and difficult to treat. The company decided to blow off any concerns and put Lagevrio [molnupiravir] on the market anyway.”
In 2021, Hildreth told an FDA advisory panel, “Even if the probability is very low, one in 10,000 or 100,000, that this drug would induce an escape mutant from which the vaccines we have do not cover, that could be catastrophic for the whole world actually.”
Also in 2021, Haseltine told Science :
“You are putting a drug into circulation that is a potent mutagen at a time when we are deeply concerned about new variants. I can’t imagine doing anything more dangerous.
“If I were trying to create a new and more dangerous virus in humans, I would feed a subclinical dose [of molnupiravir] to people infected.”
Two other recent studies also called out molnupiravir, questioning its effectiveness and raising concerns the drug may help lead to the development of new COVID-19 variants.
A December 2022 preprint by a team of Australian researchers, found “this commonly used antiviral can ‘supercharge’ viral evolution in immunocompromised patients, potentially generating new variants and prolonging the pandemic.”
And a study published Jan. 28 in The Lancetfound, “Molnupiravir did not reduce the frequency of COVID-19-associated hospitalisations or death among high-risk vaccinated adults in the community.”
University of Cambridge clinical microbiologist Ravindra Gupta, Ph.D., told Science that while it’s unclear whether molnupiravir will cause deadlier COVID-19 variants, the overall results of these recent studies “call into question whether molnupiravir should be used.”
Merck spokesperson Robert Josephson defended the product, telling Bloomberg, “There is no evidence that any antiviral agent has contributed to the emergence of circulating variants.”
Molnupiravir ‘different’ than Paxlovid — and ‘riskier’
Although molnupiravir is similar to Paxlovid in that both are oral antiviral treatments for COVID-19, Hooker told The Defender there are significant differences in how the two drugs work:
“Molnupiravir acts on the SARS-CoV-2 virus by directly inducing mutations in the RNA genome. This is a completely different mode of action compared to Pfizer’s product, Paxlovid, and in my estimation is quite dangerous.
“Merck claimed the mutation rate induced by molnupiravir would kill the virus and that mutants wouldn’t escape, but that has been shown to be false in studies of immunocompromised patients.”
Hooker said Paxlovid — and the COVID-19 vaccines — can potentially lead to the development of mutations as well.
But in his view, the “mechanism of action” used by molnupiravir is different — and far riskier — than Paxlovid and COVID-19 vaccines, which merely increase the virus’ lifetime in the human body, giving the virus a greater opportunity to naturally mutate.
Hooker said:
“In contrast, molnupiravir directly induces mutations and thereby vastly increases the mutation rate of the virus in the human host.
“In my estimation, this is a very dangerous way to treat such an infection, given the implications of creating random mutants.”
Merck made billions from molnupiravir — thanks to taxpayers
An analysis by Melissa Barber of the Harvard T.H. Chan School of Public Health and Dzintars Gotham of King’s College Hospital in London found the cost of production of molnupiravir was approximately $1.74 per unit — or $17.74 for a five-day regimen.
In March 2022, during his State of the Union address, President Biden announced the “Test to Treat” initiative, which allowed those who tested positive for COVID-19 at a pharmacy to obtain free antiviral pills — including molnupiravir — on the spot.
According to Reuters, sales of molnupiravir are expected to fall to about $1 billion this year, contributing to an expected decline in sales for Merck from $59.3 billion in 2022 to $57.2-$58.7 billion this year.
Merck’s stock price dropped by about 2% with Thursday’s announcement.
Despite these large earnings, overall sales of molnupiravir lagged significantly behind Paxlovid in 2022. Sales of Paxlovid reached $18.9 billion last year.
Michael Nevradakis, Ph.D., based in Athens, Greece, is a senior reporter for The Defender and part of the rotation of hosts for CHD.TV’s “Good Morning CHD.”
The Maine Board of Licensure in Medicine on Tuesday held its third hearing on the suspension of Dr. Meryl Nass related to her treatment recommendations for patients with COVID-19.
As it did on day two of the hearings, held on Oct. 27, 2022, the board focused on Nass’ alleged “sloppy” record-keeping for three patients she treated and on her prescribing of ivermectin and hydroxychloroquine for those patients.
The board initially accused Nass of “unprofessional” and “disruptive” behavior, spreading “misinformation” and prescribing hydroxychloroquine and a “deworming medication” (ivermectin) to patients.
The board’s case now rests on Nass’ alleged non-adherence to the medical “standard of care” as it pertained to ivermectin and hydroxychloroquine for treating COVID-19 and on the alleged “record-keeping” issues.
Two witnesses hired by the board — Dr. Thomas Courtney of the Maine Medical Center and Dr. Jeremy Samuel Faust, an emergency physician at Brigham and Women’s Hospital in Massachusetts and instructor at Harvard Medical School — testified during Tuesday’s proceedings, and Nass’ attorney, Gene Libby, cross-examined Courtney.
Cross-examination pokes holes in ‘expert witness’ testimony
Throughout his testimony, Courtney repeated his assertion that Nass did not follow an adequate standard of care in prescribing ivermectin and hydroxychloroquine to three patients, alleged improprieties in her communication and remote (telemedicine) consultations with the patients, and claimed Nass’ record-keeping was lacking.
But Courtney was obliged to walk back significant portions of his earlier testimony under his cross-examination by Libby.
For instance, Courtney claimed Nass did not adhere to an appropriate standard of care because she failed to advise two of her patients who didn’t recover as expected to seek care at an emergency room.
But under cross-examination, he acknowledged Nass had, in fact, advised the patients to go to the ER.
Courtney also criticized Nass for not prescribing monoclonal antibodies to her patients, one of whom was pregnant.
However, when cross-examined, Courtney admitted that, unlike hydroxychloroquine, monoclonal antibodies were not recommended for pregnant women and most monoclonal antibodies available at the time Nass was advising her patients were known to be ineffective against the Omicron variant of COVID-19, the dominant strain of the virus at that time.
Libby pointed out that the pregnant patient fully recovered eight days after the onset of her illness and had a normal birth, during which she was administered hydroxychloroquine and monoclonal antibodies.
Because evidence shows monoclonal antibodies are ineffective for pregnant women, the patient’s full recovery was credited to hydroxychloroquine.
Courtney also criticized Nass for making decisions about a patient’s care, including which medications to prescribe, on the basis of incomplete medical records.
He later walked back those claims after Libby demonstrated that Nass had received extensive documentation about the condition of one of the patients from his spouse, who provided Nass with vital signs, including the patient’s blood oxygen level.
Libby noted the three patients had specifically requested not to be treated with remdesivir, had asked to be prescribed ivermectin and hydroxychloroquine — and were fully within their rights as patients to request such treatment. Courtney was obliged to concur.
Libby also pointed out that off-label prescriptions of medications such as ivermectin and hydroxychloroquine, even for uses other than their primary purpose, are well within the generally accepted standard of care for physicians, and that federal agencies such as the U.S. Food and Drug Administration (FDA) and the National Institutes of Health do not issue binding requirements in this regard.
Courtney confirmed these statements.
In another characteristic exchange, Courtney, who had previously been critical of alleged gaps in Nass’s record keeping, was forced to concede that he did not “personally have a strong opinion on it.”
Referring to Courtney’s testimony, Nass wrote on her blog that despite his “opining that I lacked the fitness to practice medicine, he was unable to identify a single thing I had done wrong in my records.”
“I sent 2 patients to the ER when they did not recover as expected, although one of the board’s initial charges against me was that I failed to do so,” Nass wrote.
She likened the board’s accusations against her to “simply throwing lots of spaghetti on the wall to try and overwhelm me with charges so I would wilt and surrender my license.”
Referring to the medical claims Courtney made, Nass wrote:
“Courtney did not know the difference between an EUA [Emergency Use Authorization] product and a licensed drug. He incorrectly repeated a false claim made only once by FDA that the EUA for HCQ [hydroxychloroquine] was withdrawn because you would need to administer a toxic dose to get benefit. He had clearly failed to give that assertion any thought. Nor had he evaluated the U.S. government literature showing it to be false.
“He thought I should have treated 2 outpatients with monoclonal antibodies, but eventually agreed that cases in December 2021 were a mix of Omicron and Delta when the patients were ill, that none of their variants had been sequenced so we did not know which variant they had, and the monoclonals would not have worked against Omicron variants, which were likely to have been present then.”
“Doctor Courtney doesn’t read journal articles,” Nass wrote. “He sticks by the recommendations of government agencies and his specialty organization, the Infectious Diseases Society of America (IDSA).”
Nass noted that the IDSA was sued by the State of Connecticut “for denying the existence of chronic Lyme disease.”
In the brief time that was available for Faust to begin his testimony, he focused on attacking the credibility of Dr. Harvey Risch, an epidemiologist at the Yale University School of Public Health, for a journal article he wrote finding that treatments such as hydroxychloroquine were effective against COVID-19.
Nass had relied in part on Risch’s findings in dispensing hydroxychloroquine to her patients. During his testimony, Faust claimed, “There’s no disagreement here among the most prestigious experts in this area” with regard to the purported lack of effectiveness of hydroxychloroquine in treating COVID-19 patients.
Nass wrote:
“Faust was the Board’s epidemiology expert. He got some of the epidemiology right and he got a lot wrong. His arrogance when he was not sure of the answer was off-putting. He insulted Yale epidemiology professor Harvey Risch. He insulted my ability to read a journal article and he had a novel theory that this was sufficient disqualification to justify revoking my license.
“No one mentioned that Dr. Courtney could not cite journal articles used for forming his opinions on COVID treatment, having solely relied on pronouncements from government agencies.
“Should his license be revoked for that? Of course not.”
Nass also wrote that Faust “publicly melted down when the mask mandate on planes was lifted,” accusing the Centers for Disease Control and Prevention of “killing babies.”
Next hearing set for March 2
The Maine board has scheduled two more hearings, the next one for March 2.
However, according to Nass, “The questioning of Dr. Faust is likely to take half a day more. Then I have 8 witnesses to go, including 3 patients who are at issue.”
About 140,000 people tuned in to Tuesday’s live broadcast of the proceedings, according to Nass.
Children’s Health Defense is providing support for Nass’ legal team.
Michael Nevradakis, Ph.D., based in Athens, Greece, is a senior reporter for The Defender and part of the rotation of hosts for CHD.TV’s “Good Morning CHD.”
It is easy to get bogged down in the technical detail of the climate debate. But science can distract us from the fact that before climate change, environmentalists made exactly the same kind of predictions that now drive arguments for draconian climate policies. The gloomy predictions of civilisation’s imminent collapse made by environmentalists in the 1970s came to nothing – the world population grew larger, wealthier, healthier and safer. This should alert us to the fact that, whether or not ‘climate change is real’, environmentalism is a radical political ideology, bent on reorganising the world, whatever the facts are. It is not merely a response to scientific discovery about our relationship with the natural world.
We should not forget this historical context of the climate debate and motivation for the climate policy agenda, because ideology is insidious, and far more powerful than scientific rationalism. Today’s radical greens, from world leaders to street-blocking narcissists, have learned not to make the mistake of their predecessors. Rather than making predictions that fail to materialise, their new trick is to claim that the ‘climate crisis’ is ‘happening now’: people are starving, diseases are rampant, storms, floods, wildfires and heatwaves kill thousands by the day, forcing millions from their homes and into poverty, all underpinned by dramatic images on TV news stories to cement the narrative without any journalistic incredulity towards official stories.
But the ‘climate crisis’ simply isn’t happening at all. Just as the world defied green predictions half a century ago, all metrics of human welfare make the opposite case: humanity is thriving like never before. And just as in the 1970s, it is ideology, not fact, which drives the green narrative. In our new film, we at Climate Debate UK attempt to show how this regressive ideology has been transmitted, using the idea of a ‘climate crisis’, from the top strata of global society, through governments and the media, to very young children, where it poisons their view of the world and their futures.
It is ideology, not mere scientific error, that has blinded people to the fact that abundant, affordable and reliable energy has made the world a much better place. Worse, it is ideology that has clouded the moral judgement of people who have wilfully turned extremely young children into instruments of the political agenda, to prevent them driving this development onward. ‘Science’ is just a fig leaf.
We all know, I hope, about the significant and sustained number of excess deaths since May 2022. Most recently, you probably saw Esther McVey MP asking if the Department of Health would commit to an urgent and thorough investigation.
Maria Caulfield MP, one of the health ministers, replied saying that it’s also happening elsewhere and there is a range of factors. Implicitly, she was refusing to investigate. Outrageous.
However, it actually reminded me that way back in February 2021, MHRA promised to do a whole range of routine population-level data analysis “to quickly detect a potential safety signal” for the Covid vaccines. It announced it here under the section “Rapid Cycle Analysis and Ecological Analysis“. It explains what it involves as follows:
[A]s COVID-19 vaccination records (i.e., those given outside of GP surgeries) begin to get updated within GP systems, the MHRA will implement a form of active surveillance known as ‘Rapid Cycle Analysis’. This method involves proactive, weekly analysis of a range of pre-defined events (theoretical side effects) to quickly identify safety signals – it again involves ‘observed vs expected’ analyses (i.e. comparing rates after vaccination to rates in unvaccinated comparator groups) but doesn’t rely on people directly reporting any concerns through the Yellow Card scheme. It is also a more robust way to quickly determine if rates are likely to be consistent with a coincidental association. It also uses the MaxSPRT approach with adjustments made for the expected delays in the recording of events presenting to and diagnosed in secondary care settings. The list of pre-defined events of special interest is not fixed and can be expanded at any time.The MHRA will also use the CPRD data to conduct ‘ecological analyses’. This involves monitoring trends in the rates of pre-defined events within given population cohorts, based on prioritisation groups for vaccine roll out, to see if they are occurring to a greater extent amongst those targeted for vaccination after it is deployed compared to historical rates from the pre-deployment period. Comparisons can also be made to trends seen in groups not targeted for vaccination at the same time. This approach is most useful when we see high vaccine uptake and is another way to quickly detect a potential safety signal.
So I had a poke around MHRA’s website to see how it is getting on with this. Not very well, it turns out.
One of MHRA’s five divisions is called Clinical Practice and Research Datalink (CPRD) and it maintains a bibliography of peer-reviewed research and reports which have used data provided by MHRA from NHS datasets for things like ICU, A&E, inpatients, outpatients, cancer registration and pregnancy. When I looked, the bibliography had been updated as recently as January 9th 2023. So well and truly up-to-date. So far, so good.
Imagine my surprise when I could only find two population-level studies relating to the Covid vaccines, both relating to thrombocytopenia (low blood platelet count), one from February 2022 and one from October. So just one type of adverse event has been put through MHRA’s promised ecological analysis in the last two years. It doesn’t say much for MHRA’s commitment to use population-level data “to quickly detect a potential safety signal”.
Imagine my further surprise that none of the datasets which MHRA’s CPRD Division provides for research contains data after June 2021.
So in conclusion, all about as useless as the other strand of Covid vaccine surveillance it promised, Targeted Active Monitoring, which I noted in a recent article it quietly dropped 15 months ago.
For me, there are only two possible conclusions: either the MHRA is not doing the Covid vaccine surveillance it promised, or it is doing it and not making the results publicly available. Either way, it’s high time that MPs, the Covid Inquiry and the media started asking MHRA some searching questions.
Until Nick retired a few years ago, he was a Senior Civil Servant in a Government Department.
From: XXXXXX Sent: 30 January 2023 12:33 To: Norman Fenton Subject: Hart Group
Dear Professor Fenton,
Apologies for any intrusion, but I’m contacting you directly since the Hart Group (which I understand you to be a member of), have not replied to my earlier emails – all very busy people, I do understand.
As a small group of individuals who between us have some journalistic and medical-science history, we are working on a presentation (with a further view to establishing a website), which aims to offer a wider range of information concerning Covid policies and treatment than, it appears, is usually available through current mainstream and social media.
Given that our aim is a balanced juxtaposition and presentation of arguments, hopefully allowing better-informed opinions to be arrived at, we do have a range of “issues” we’d love to understand better in order to present them fairly.
You are (I imagine) well-placed to comment on one specific matter, and I would be enormously grateful if you would spare a minute to advise, assuming this enquiry doesn’t create any conflict of interest or other problems for you:
The Times and other media recently reported on a QMUL study* which indicates that unvaccinated individuals with certain medical conditions are more likely to suffer “serious outcomes” than vaccinated individuals. I believe presenting this this demands careful attention to context and contrasting with other possible perspectives.
Dr Aseem Malhotra in a Twitter-hosted video makes reference to de-bunking claims about how this story has been reported, but makes no reference I can find to where such a de-bunking can be found; and sadly, he too seems unavailable to comment!
Probably, Dr Malhotra’s position is not an issue you are required in any way to comment on. However, in general, I do think that those who would like to see “better”, more balanced reporting on Covid should find time to speak to others, like us, who are trying to support exactly that cause – presumably it’s in everyone’s interest. But that’s just a peripheral observation on my part!
It would be truly helpful if you can find a moment to provide some pointers to help us present a balanced picture of the study referred to above.
I should make it clear that, although I just briefly discussed this with one or two members of HART, my response below should certainty not be construed as ‘the HART response’.
The most important point to note about the QMUL study is that it certainly does not claim anything like what either you or The Times seem to think it claims, i.e it certainly does not show that “unvaccinated individuals with certain medical conditions are more likely to suffer serious outcomes than vaccinated individuals.” In fact, no comparison with a vaccinated cohort was undertaken.
All the study actually did was look at the outcomes for covid patients with pre-existing conditions like myocarditis. This is something very different to the later studies (such as those Aseem Malhotra referred to) which compared incidence of myocarditis occurring post-vaccination with the base rates for unvaccinated. So, all the study actually shows is that “that individuals with certain pre-existing medical conditions who get covid are more likely to suffer serious outcomes than those without such medical conditions who get covid.” That is hardly novel, since this has been widely known since March 2020.
In fact, the authors of the study are demonstrating a very clear bias by referring to the people in the study as ‘unvaccinated’. Of course, they were unvaccinated – it was a meta-analysis of 110 published studies between 1st Dec 2019 and 16th July 2020. There was, of course, no vaccinations anywhere during that period so referring to these people as ‘unvaccinated’ must have been done to fit a particular mischievous agenda. I am actually pleased you brought this study to my attention since it needs to be exposed for leading people like the Times and yourself to believe it was showing something that it wasn’t.
One major conclusion in the paper seems sensible – that having diabetes or hypertension or ischaemic heart disease predicts for poorer outcomes (although the same could be said for many other conditions so there is hardly anything novel in this). But the first part of the conclusion seems entirely wrong. Just because you see covid hospitalising a lot of people who had pre-existing cardiac comorbidity certainly does not mean that covid caused their comorbidity. It seems that this part of the conclusion may have been influenced by possible conflicts of interests (see below).
There are a number of other specific concerns about the study:
They included studies published from 1st Dec 2019 – but that was before covid was formally accepted to exist, so how could any study published in Dec2019/Jan2020 have patients with suspected covid? Any study published pre-mid Jan 2020 should be excluded by default, since even the flawed confirmatory PCR test was not available until then. There would be no way of knowing if ‘is covid’ results was a mix of ‘not covid’, ‘possibly covid’ and ‘probably covid’.
How is ‘suspected’ the same as ‘confirmed’? When the symptoms used for Covid marry to any number of other conditions that are common (and even endemic) then how can you say that suspected covid is even ‘a thing’?
Someone hospitalised with exacerbation of an existing condition is NOT the same thing as someone who gets a new diagnosis OF that condition after vaccination.
Including so many Chinese studies clearly biases the work – and using China and USA to predict for LMIC (in the Introduction) is strange to say the least.
A colleague also noted the link between Prof Gupta (the senior author) and the Bill and Melinda Gates Foundation and other potential conflicts of interest:
In this report Gupta is acknowledged as having provided the statistical support for a report that seeks to help the Bill and Melinda Gates Foundation and the Clinton Foundation find new ways to support medical/health research in the UK. There are also a number of links between Gupta before he came to QMUL and functions (like some project called D3140 for the Rotary Club funded by BMGF in Mumbai, and research out of Imperial College) supported by the Gates Foundation. He is also heavily involved in Wellcome Trust AND the WHO – and is listed on the minutes of meetings between the two.
Gupta and the lead author (Sher May Ng) are both on this study that was in part funded by the NIH (Grumbach acknowledges an NIH grant while at the UCal Nursing School. My colleague managed to find that she also has an NIH.GOV email address).
Co-Author Kenneth Rice has worked on studies like this with staff from BMGF.
Kenneth Rice and Gupta are two of the over 200 doctors who are part of a research collaborative called TOPMed – funded by the NIH with a combination of US Gov and BMGF money.
I hope this helps you.
Yours
Norman Fenton
For clarification of the potential conflict of interest with BMGF, Scott McLachlan has provided the following information:
Bill Gates is the world’s largest single shareholder of Covid-19 vaccine manufacturer stocks and therefore every time Pfizer, Moderna, Lilly (Eli), GSK, CureVac or even AstraZeneca (he had something like 8% in AstraZeneca shares at one point) sell a vaccine, that’s money back in his pocket. (see here)
And while fact checkers claimed Gates would not profit from Gilead (Remdesivir), he actually purchased a significant chunk of Gileadand 27,000 shares in Merck in 2018 in preparation. (Merck are one of the manufacturers who licensed to manufacture Remdesivir in their plants)
The thing that journalists get confused on is the idea that he, through his foundations, made ‘grants’ to Moderna et al. These were not ‘grants’ in the way we get grants from EPSRC or UKRI – they are grant investments. Various companies in control of the BMGF are shareholders in Pfizer and Moderna. In return for sinking $50mil+ into Moderna, Gates’s foundation took a large slice of Moderna’s shares.
Further, Gates sells access to “investment opportunities” through GAVI COVAX and AMC. The ‘investor’ (usually a rich western govt or pharma/healthcare company) gives money to GAVI in their rich country where they make profits and need a tax write-off… then, they get included in the contract with some LMIC govt to sell them vaccines. The whole model works by shifting where the pharma/healthcare company make their profits. Pharma companies ‘invest’ by subsidising vax initially and then, over time the contract shifts to the country’s govt paying extortionate rates for future vax.
As one of the links above says – as the world keeps getting sicker Gates keeps getting richer. He invested $555mil into COVID vax companies during 2019/20 and has made an estimated $4bil return. Nice work if you can get it.
Much of the analysis around Covid 19 vaccine harms revolves around counts of deaths, and excess mortality. This is perfectly understandable since “excess deaths” is a “hard” measure in that most countries are able to count the number of their citizens who have died quite accurately so this does allow for some reasonably informative inferences and international comparisons.
The same is of course not the case for “covid deaths” which even the strongest proponents of the establishment covid narrative have had to admit are affected by differences between countries in classification, testing rates, and policies.
However, as well as many countries experiencing excess deaths, there is currently a second huge problem: marked increases in the numbers registering as long-term disabled.
Because registering as disabled is usually done for the purposes of receiving financial assistance or other support from the state, there is a built-in gatekeeping function which limits spurious claims, so we can be reasonably confident that any significant increases represent genuine medical issues.
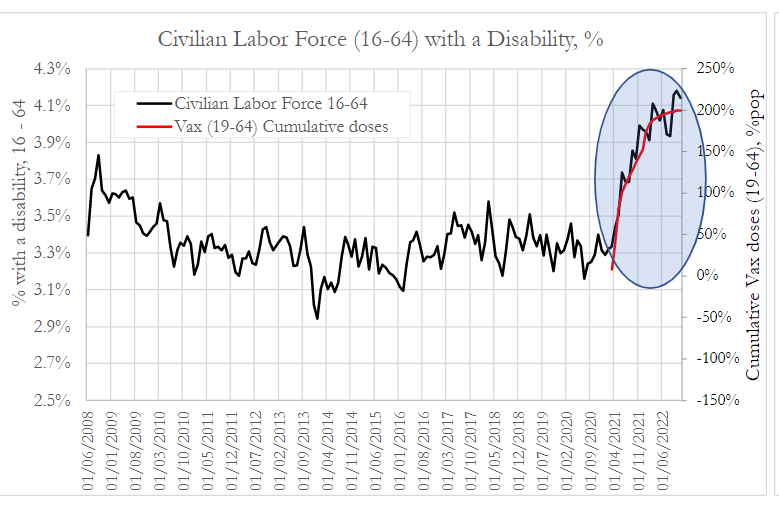
Looking at the USA first, a group called Phinance recently published an analysis of the proportion of the US civilian labor force who are registered as disabled.
This graph shows the % of workers aged 16 to 64 with a disability against the total number of Covid vaccinations administered in the same age group.
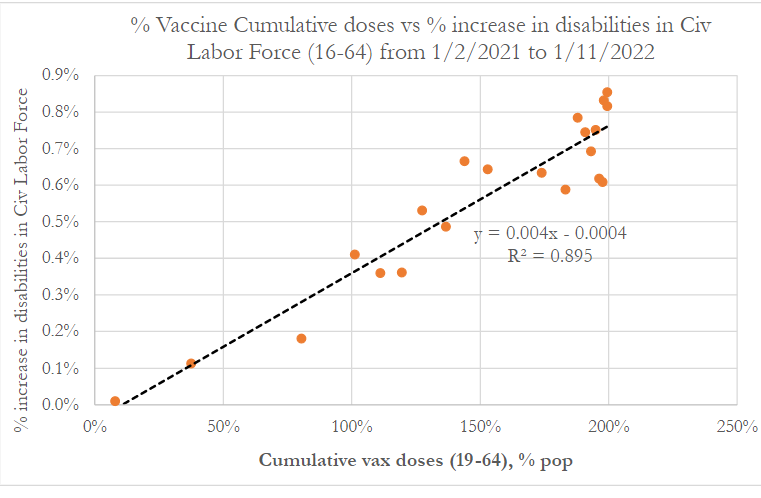
Phinance also published this graph which is a regression analysis showing a very strong correlation between the increase in the number disabled and the total number of doses given – something which actually is rather obvious from the above.
It is fair to point out that such a regression analysis should not in general be performed on cumulative series of data (ie total doses administered), but rather on discrete data (which in this case would be daily or weekly doses). If the measurements can only increase and not fall (as with cumulative data), this limits the significance of any correlation observed, as by default they will rise together.
This is less of a problem here in that only one of the 2 data points (vaccines) is cumulative (for the other axis they have used the increase in the number disabled). However, we wrote to the authors to ask why they didn’t use daily or weekly doses administered.
They responded with the not unreasonable point that because the adverse effects occur over a wide and variable period after dosing, a cumulative series is probably more informative. We agree. Just because fewer doses were given one week does not mean there were fewer people at risk of developing a post vaccination disability in that week.
The extremely experienced medical statistician who blogs as “John Dee” has performed further analysis on the US data above. The article is rather technical but in essence by applying a number of sophisticated statistical tools he concludes that using cumulative data may exaggerate but has not invalidated the findings, which should therefore be regarded as highly suggestive (though not in themselves proof of) a causal relationship.
However, the criticism of the statistical methodology was never really “on point” anyway. Science advances through testing hypotheses by questioning the available data.
The point of the analysis of the disability data was not to conclusively “prove” that the vaccines cause harm, but rather to answer the question: Is there a signal of potential concern which warrants further study? The answer to this appears to be “yes” and anyone finding excuses to not even look further should be regarded as willfully blind.
Of course, the link to vaccination could quite easily be further tested by ascertainment of the vaccination status of a representative sample of the disabled, with comparisons to disability rates in the unvaccinated. That this is not even being discussed must surely be regarded as a red flag.
When a potential signal of concern is replicated internationally, it increases the likelihood that we are dealing with a causal relationship. Not much quality data on disability rates is available from other countries, but one country which does publish some comparable data is the UK.
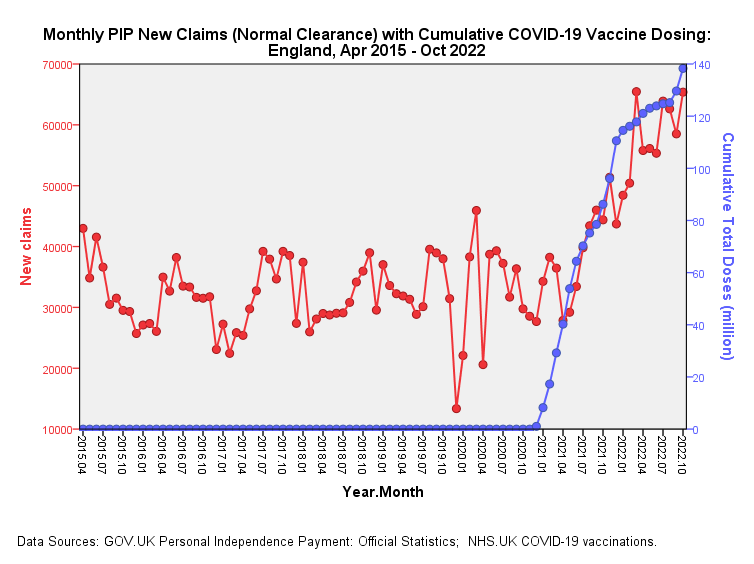
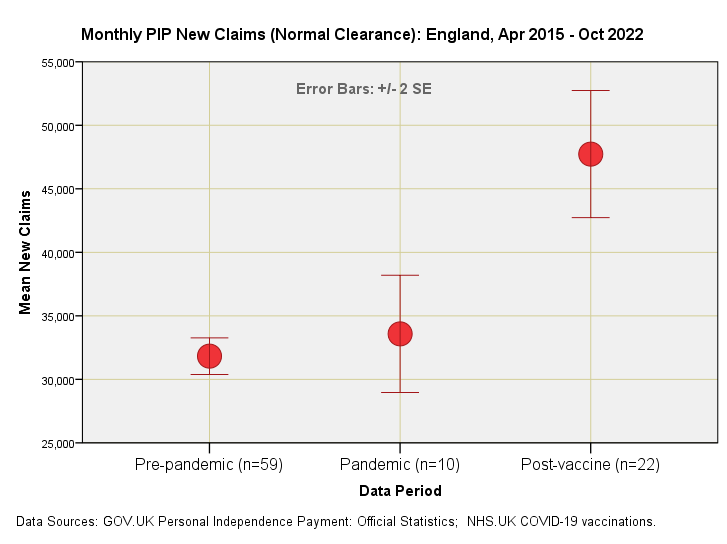
In the UK, if disabled, a state payment called a personal independence payment (PIP) can be claimed. An official UK government report states that there have been “unprecedented levels of new claims in recent quarters” (in England and Wales).
This has been reported by various news websites, including Yahoo’s article titled “The ‘astonishing’ rise in people claiming one key benefit”.
PIP data is actually downloadable from an official UK government website, and “John Dee” has performed some analysis on it which can be read here and here.
The new claims data plotted against cumulative doses administered looks like this (with thanks to John Dee for the graphs):
Clearly, this bears an uncanny resemblance to the US data above.
As he did with the US data, John has drilled deeper into the data, showing, for example that whilst claim rates in the pandemic period were similar to those in the pre-pandemic period, there is a huge uptick in the post-vaccine period, with the error bars (and statistical tests of significance) indicating that this is not just random variation.
Moreover, he has used a technique called “cross-correlation” which strongly suggests that “the increase in the month-on-month changes in total administered doses is followed three months later by a rise in month-on-month changes in new cleared claims.”
This would appear to add plausibility to the causation argument, in that three months is the period required by the government as a minimum qualifying period before an application for PIP can be filed.
Overall, these datasets surely raise huge concerns, which could be assuaged by further more detailed examination of the data, especially including vaccination status. We urge governments to carry out such an analysis, which need only be performed on a representative sample in order to generate reliable conclusions.
They’re starting to come now – the ‘debunkings’ of the Pfizer undercover video sting, in which executive Jordon Trishton Walker, “Director of Research and Development – Strategic Operations and mRNA Scientific Planning”, tells his ‘date’ that Pfizer is looking to mutate the virus “so we could create preemptively developed new vaccines, right”.
Pfizer released a statement on Friday, which notably did not deny that Dr. Walker works for the company (a fact which has anyway been confirmed via internet searches). Now the latest ‘debunking’ effort comes from Medpage Today.
After making the odd claim that “it is currently unclear if the man in the video is actually an employee of Pfizer, and if that is his real name” (journalism isn’t what it used to be), writer Michael DePeau-Wilson notes that Pfizer’s statement “summarily debunk[ed] the claims made in the video”, as the company stated that it “has not conducted gain of function or directed evolution research” related to its “ongoing development of the Pfizer-BioNTech COVID-19 vaccine”.
While it is true that the statement does say this, it also says that “we have conducted research where the original SARS-CoV-2 virus has been used to express the spike protein from new variants of concern”. Furthermore, it admits that:
When a full virus does not contain any known gain of function mutations, such virus may be engineered to enable the assessment of antiviral activity in cells. In addition, in vitro resistance selection experiments are undertaken in cells incubated with SARS-CoV-2 and nirmatrelvir in our secure Biosafety level 3 (BSL3) laboratory to assess whether the main protease can mutate to yield resistant strains of the virus.
Despite the initial denial, then, what is being described here plainly is gain-of-function research – after all, the company is engineering the original virus to express the spike protein from new variants of concern, variants which are ‘of concern’ precisely because their spike protein has immune-evasive properties.
In case there is any doubt about this, FDA vaccine adviser Dr. Paul Offit inadvertently confirms it in the Medpage piece.
“Usually, when people talk about gaining function, they’re talking about making it so that the virus is either more deadly or more easily transmitted or that it now can jump species,” Dr. Offit says.
“[T]rying to make the virus more immune-evasive or more contagious… would be considered gain-of-function research,” he adds.
Right, so exactly what Pfizer has said it is doing – engineering “the original SARS-CoV-2 virus… to express the spike protein from new variants of concern”.
Offit tries to obfuscate, stressing that “Pfizer has been working with an mRNA platform that is coded for coronavirus spike proteins, not a whole virus”.
Yes, the vaccine does not use whole virus. But no one said it does. The matter at hand is what Pfizer is doing to the virus as part of its vaccine development research. And Pfizer is clear that it is engineering “the original SARS-CoV-2 virus… to express the spike protein from new variants of concern”. The whole virus, note.
Offit then implies that it isn’t gain-of-function research because the variant has already been created by “mother nature” and Pfizer is just reproducing what nature has already done.
If there was some evil hand back there that was trying to make the virus more immune-evasive or more contagious, that would be considered gain-of-function research, but it’s not happening. The evil hand is mother nature.
But even if the variant already exists in nature, that doesn’t mean it’s not gain-of-function research to engineer a virus to gain the immune-evasive mutation in the lab. Besides, how can you be sure you’re producing the exact same variant and not some subtly (or not-so-subtly) new and more immune-evasive variant?
Offit then appears to betray an ignorance of the process of making the vaccine, as he says the “remarkably effective” development involved sequencing SARS-CoV-2 in “a matter of months”. In fact, the virus was sequenced several times even in the last week of December 2019, and took a couple of days each time, not months.
Perhaps needing to restore his reputation with the politico-medical establishment after his criticism of the boosters last month (is this why he was given the job of defending Pfizer?), he is now effusive with praise for the mRNA vaccines. “This is the best medical achievement in my lifetime,” he says. “And my lifetime includes the development of the polio vaccine.”
Thus, despite the denials that what Pfizer is doing is gain-of-function research – denials which presumably take advantage of the fact that ‘gain-of-function’ is not rigorously defined – it’s clear that what Pfizer admits to doing falls squarely within the definition cited by Dr. Offit, namely the commonly accepted one, which includes making the virus more “immune-evasive”.
And they appear to tacitly acknowledge that, which is why they make their excuses. In Pfizer’s case, that it is “required by U.S. and global regulators for all antiviral products” and “carried out by many companies and academic institutions in the U.S. and around the world”. In Offit’s case that Pfizer was just copying “mother nature”.
In fact, though, as Dr. Robert Malone has pointed out, Pfizer has previously been upfront that it is doing this research, including in an August 2021 article in STAT News, and almost nothing in the undercover video is new. Why such a fuss was made about scrubbing it from the internet is therefore an interesting question – though this may be more linked to the sensation around it than the facts, which Pfizer’s response anyway did not deny. How could it, when those facts were already on public record?
Perhaps the main lesson, then, is that we all need to be paying more attention.
We also need to think hard about what kind of research should be allowed and what should be banned. The reaction to the Project Veritas video suggests a strong feeling that this kind of work should not be done – including when it is (supposedly) imitating what nature has already created. The fear in the public is real and justified, and relates to the folly of engineering viruses to make them worse. Can this ever be a good idea? My feeling is there’s no need to go beyond the viruses and variants nature already provides us with, and to stick to using real specimens, not engineered ones. But the current regulatory regime and scientific establishment clearly disagrees.
Whatever the right answer, we need to be able to talk about this properly. Not be subject to global, military grade censorship when someone tries to raise the topic as a matter of public concern, albeit in a sensational (and entertaining) way.
Newsweek just published an editorial by Kevin Bass, a medical school student in Texas, about how the official scientific establishment in the United States got it wrong about COVID-19. At the risk of sounding immodest, all of the realizations that he catalogues in his essay were apparent to me by May of 2020, almost three years go.
People often ask me why I perceived at the beginning of this mess that our public health officials were lying to us. The answer is simple: I am a longstanding student of history (including medical history) and of human nature. It is precisely a lack of education in history that made so many people susceptible to being manipulated and defrauded by the Bio-Pharmaceutical Complex.
Students of political history have often marveled that the Anglo-Irish statesman, Edmund Burke, made all of his accurate predictions about the French Revolution in 1790. Burke foresaw that the Jacobins would grossly mismanage everything and then resort to terror when none of their harebrained schemes worked. He predicted the bloody fiasco would end with the accession to power of a military commander.
Three years after Burke’s Reflections on the Revolution in France was published, the Reign of Terror began. Nine years later, Napoleon Bonaparte came to power through a combination of subterfuge and soldiers with fixed bayonets.
How did Burke make these predictions? He knew history and he understood human nature. He therefore saw that the Jacobins had no idea what they were doing. None of their abstract schemes acknowledged the complex reality of human affairs. Their entire conception of reality was ideological, not practical, and they insisted on imposing it with fanatical zeal.
Precisely the same is true of the Vaccine Syndicate that ran the official Pandemic Response. Its leaders are votaries of the COVID-19 Vaccine Cult, and all of their policies were in the service of getting a needle in every arm. Their monolithic policy totally ignored the complex reality of the problem.
Those familiar with history (and medical history) could see by April of 2020 that “The Science” constantly invoked by our government health agencies was an ideological construct—an Orthodoxy—and not true science. True scientific inquiry was conducted by doctors in the field who had the courage to treat the illness instead of waiting for the heralded “vaccine.”
Kevin Bass’s Newsweek is a good start. May the rest of the Official “Follow the Science” Establishment get out their forks and knives and start eating crow.
This site is provided as a research and reference tool. Although we make every reasonable effort to ensure that the information and data provided at this site are useful, accurate, and current, we cannot guarantee that the information and data provided here will be error-free. By using this site, you assume all responsibility for and risk arising from your use of and reliance upon the contents of this site.
This site and the information available through it do not, and are not intended to constitute legal advice. Should you require legal advice, you should consult your own attorney.
Nothing within this site or linked to by this site constitutes investment advice or medical advice.
Materials accessible from or added to this site by third parties, such as comments posted, are strictly the responsibility of the third party who added such materials or made them accessible and we neither endorse nor undertake to control, monitor, edit or assume responsibility for any such third-party material.
The posting of stories, commentaries, reports, documents and links (embedded or otherwise) on this site does not in any way, shape or form, implied or otherwise, necessarily express or suggest endorsement or support of any of such posted material or parts therein.
The word “alleged” is deemed to occur before the word “fraud.” Since the rule of law still applies. To peasants, at least.
Fair Use
This site contains copyrighted material the use of which has not always been specifically authorized by the copyright owner. We are making such material available in our efforts to advance understanding of environmental, political, human rights, economic, democracy, scientific, and social justice issues, etc. We believe this constitutes a ‘fair use’ of any such copyrighted material as provided for in section 107 of the US Copyright Law. In accordance with Title 17 U.S.C. Section 107, the material on this site is distributed without profit to those who have expressed a prior interest in receiving the included information for research and educational purposes. For more info go to: http://www.law.cornell.edu/uscode/17/107.shtml. If you wish to use copyrighted material from this site for purposes of your own that go beyond ‘fair use’, you must obtain permission from the copyright owner.
DMCA Contact
This is information for anyone that wishes to challenge our “fair use” of copyrighted material.
If you are a legal copyright holder or a designated agent for such and you believe that content residing on or accessible through our website infringes a copyright and falls outside the boundaries of “Fair Use”, please send a notice of infringement by contacting atheonews@gmail.com.
We will respond and take necessary action immediately.
If notice is given of an alleged copyright violation we will act expeditiously to remove or disable access to the material(s) in question.
All 3rd party material posted on this website is copyright the respective owners / authors. Aletho News makes no claim of copyright on such material.