Varicella-Zoster Reactivation after COVID-19 Illness versus SARS-CoV-2 Vaccination
Larger Ongoing Threat is COVID-19 Vaccination
By Peter A. McCullough, MD, MPH | Courageous Discourse | February 6, 2023
Many papers in the medical literature seem to pit a consequence such as myocarditis or stroke as either occurring as a consequence of COVID-19 illness compared with COVID-19 vaccination. Because the denominator is so large for acutely ill hospitalized patients with COVID-19 especially during the first two years of the pandemic allowing ICD code capture of comorbidities, authors erroneously conclude the illness is “more dangerous” or a “bigger risk factor.” These arguments are daft in my opinion since COVID-19 respiratory illness is treatable and a recent paper from Klaassen et al has estimated 94% are already recovered from COVID-19—so it is water under the bridge. Not true for COVID-19 vaccines which are still mandated by some ill-advised schools, employers, and agencies. One way of looking for what is a more pressing and continued problem is to survey the medical literature.
Martinez-Reviejo et al completed a literature review of varicella-zoster reactivation (shingles) and compared cases arising after vaccination and those with the respiratory infection. There were more manuscripts and cases after vaccination. However, the manifestations of varicella-zoster were more severe in those with acute COVID-19 illness which was also high in disease severity.

Martinez-Reviejo R, Tejada S, Adebanjo GAR, Chello C, Machado MC, Parisella FR, Campins M, Tammaro A, Rello J. Varicella-Zoster virus reactivation following severe acute respiratory syndrome coronavirus 2 vaccination or infection: New insights. Eur J Intern Med. 2022 Oct;104:73-79. doi: 10.1016/j.ejim.2022.07.022. Epub 2022 Aug 1. PMID: 35931613; PMCID: PMC9340059.
I found it curious the authors did not disclose the shingles vaccine status in the tables. The bottom line is that shingles can occur with severe COVID-19 and it is treatable. Acute COVID-19, however is amenable to early therapeutics so severe cases can be avoided and most of us have recovered SARS-CoV-2 infection. COVID-19 vaccination continues to be an ongoing threat for varicella-zoster reactivation syndromes, some of which are very serious including ocular damage and long-lasting painful cutaneous syndromes.
The UN calls for a “code of conduct” on social media
By Didi Rankovic | Reclaim The Net | February 7, 2023
The United Nations is becoming heavily involved in several initiatives to regulate the digital space and online speech, and judging by the priorities the organization has for 2023, outlined on Monday in New York City, this trend is only picking up steam.
UN Secretary-General Antonio Guterres spoke about those priorities and suppressing the spread of online “hate” speech via what he called misinformation and disinformation made it to the list, among issues like rights-based approach, renewable energy, and a dire warning about the world being closer than ever to total catastrophe – all mentioned in his speech.
Guterres spoke about the subject of “mis- and disinformation” on the internet as a call for action to deal with these threats.
And Guterres had “everyone with influence” in mind – governments, regulators, policymakers, technology companies, the media, civil society. It’s notable that he “squeezed in” this warning about the need to “stop the hate” on the internet in the same paragraph he spoke about UN outreach programs that concern the Holocaust and the Rwanda genocide.
He then moved on to the UN Strategy and Plan of Action on Hate Speech, which included the “call for action.”
“Stop the hate. Set up strong guardrails. Be accountable for language that causes harm,” the UN secretary-general said and explaining the plan on how to do that: by creating a code of conduct for information integrity on digital platforms.
This, Guterres noted, is part of his 2021 report titled, “Our Common Agenda.” In May 2022, a meeting was held at the UN by delegates who gathered to discuss what was dramatically dubbed as “the epidemic of misinformation and disinformation.”
The UN Department of Global Communications was tasked with drafting a code of conduct “to promote integrity in public information.”
In his speech on Monday, Guterres also accused social media platforms of using algorithms to “amplify toxic ideas and funnel extremist views into the mainstream,” and asserted that some platforms tolerate hate speech, which, according to him, is “the first step towards hate crime.”
And as stakeholders, those identified by Guterres, get together to produce the code of conduct for information integrity on digital platforms, “we will also further strengthen how focus on our mis- and disinformation are impacting progress on global issues, including the climate crisis,” he promised.
Critics wonder if this doubling-down on “the war on misinformation” by the UN will serve as an excuse for even more online censorship and if it might clash with members’ own speech protection laws.
Cochrane’s early and deliberate interference in the publication of efficacy of masking review results
Yet again, The Science follows politics.

There is zero evidence that this does anything
eugyppius: a plague chronicle | February 6, 2023
The Cochrane mask review I wrote about last week has hit Team Mask very hard, in fact much harder than I thought it would. They’ve been frantically coping for days now – combing through the fine print, seizing upon every moment of expressed uncertainty or caution in the paper to claim that population-wide masking might still be justified, somehow, because reasons.
The dim and eternally concerned Twitter epidemiologist Jennifer Nuzzo (who would be a disgrace to her field, if the field of public health weren’t already a disgrace) posted a hilarious nineteen-tweet thread that gathers all the typical excuses and cries to the heavens for more studies, because the “absence of evidence is not evidence of absence.” Intriguingly, as others have noted, Nuzzo used to think totally differently about the utility of masking. In 2006, our epidemiological luminary co-authored a paper on Disease Mitigation Measures in the Control of Pandemic Influenza, which flatly admits that “the ordinary surgical mask does little to prevent inhalation of small droplets” and that no data support using N95 or FFP2 respirators outside of healthcare settings. Like all pandemic authorities, Nuzzo had sensible ideas right up until the moment her ideas became important.
Tom Jefferson, the lead author of the Cochrane review, has added to the pain and embarrassment of Team Mask by granting this interview to Maryanne Demasi, in which he reiterates bluntly that “there’s no evidence that masks are effective during a pandemic,” no evidence that respirators do anything even in healthcare settings, blames misguided mask mandates on bad governmental advisers, and criticises the masking “craziness” that took root in 2020, in which “strident campaigners” – “activists, not scientists” – like “academics and politicians started jumping up and down about masks.” He also makes an observation that is often aired at the plague chronicle, namely that the failure of masks to do very much indicates that virus transmission itself is poorly understood, and far more complicated than we tend to assume. You should read the whole thing for yourself.
Here, I want to highlight one crucial point. Jefferson explains that he and his co-authors were ready to publish a review on the evidence for masking and other physical interventions in April 2020, but that Cochrane held up its appearance by “inexplicably” demanding a further peer reviewer. This effectively delayed publication by months, in precisely the period that novel mask mandates were emerging all across the world. When the review was finally cleared for publication in November – long after its chance to influence mask policies had passed – the authors were directed to insert all manner of language softening their conclusions, and Cochrane included an accompanying editorial on why “Policy makers must act on incomplete evidence in responding to COVID-19.”
Plainly, the conviction that mask mandates were necessary came first; The Science followed. All the while, though, the evidence didn’t go away. It was just suspended slightly out of view, diluted with weak excuses and deprived of influence over policy, until the ideological fervour dissipated and the plain truth could be spoken again. The lesson is that regime authorities, particularly when they enjoy the collaboration of the press and academia, can tell almost any lie, but suppressing the truth requires active effort, and sooner or later their myths come crashing down. The mask mythology was among the first to take shape, and it has been the first to fall.
In the coming months other pandemic fantasies will also begin unravel.
UPDATE: See also this interview with Tom Jefferson published today in the Daily Sceptic
A worldwide call for data transparency: Show us the data!
By Steve Kirsch | February 3, 2023
We could end the debate on COVID vaccine safety instantly. All we need is the death-vax record data. But today, that data is being concealed by the health authorities in every jurisdiction. Here’s why.
A simple database of death-vax records should be made publicly available by the CDC and other health authorities worldwide.
The death-vax records can be analyzed in seconds using a variety of totally objective methods to show whether the COVID vaccines have increased or decreased all-cause mortality in each age range.
No medical records, cause of death, etc. are required or needed. Just the age, date of death, and dates of vaccination are all that is required for each death since the start of the COVID vaccination program.
The death-vax data has been collected, but it has never been made publicly available anywhere in the world. There is no PII or HIPAA violation by disclosing the records.
There is absolutely no excuse for this data not to be made PUBLICLY available now.
Because kids are most at risk, universities in particular should be demanding data transparency of the death-vax records.
It is immoral and unethical for universities to mandate COVID vaccines if the health authorities refuse to show us the death-vax database records that would justify their use.
The death-vax data consists of one record for each death since Dec 14, 2020 to the present with these columns:
- Age
- Date of death
- Date of each COVID vaccine administered (blank if unvaccinated)
That’s it.
Does that sound like too much to ask for?
Optional:
- Manufacturer of each dose (blank if unvaccinated)
- State (e.g., California)
In the US, the death data is already collected by the CDC for the entire country. The immunization data is available from each state.
The CDC could quickly collect this information, do the database join, remove the PII fields, and make this database publicly available.
This would reveal to the entire world whether the vaccines are safe or not. Instantly. No more debates.
No medical records are required. No judgment is required. The analysis is all based on mathematics and the law of large numbers. If the vaccines are saving lives, we’ll know it. If the vaccines are killing people, we’ll know it.
EVERYONE should be demanding to see the death-vax record-level data. It can be easily compiled. It is dispositive. We’d know instantly whether the vaccines are safe or not. No more arguments. No more debates. No more censorship. One and done.
Yet, nobody in the mainstream infectious disease or epidemiology community seems to care about seeing this data. Nobody is calling for it. Why is that? Are they afraid of being proven they are wrong?
If the vaccine is so safe, they should be shouting for the release of this data from the rooftops because nearly 80% of the public is no longer drinking the Kool-Aid:
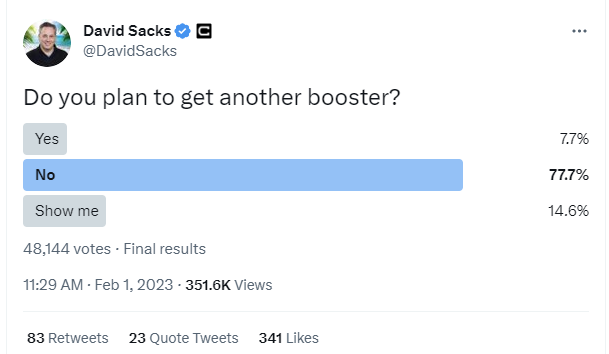
But the authorities are remaining silent and keeping the data under wraps. That can only mean one thing: the data is horrible and they know it. That’s why they are hiding it from public view.
That’s not just a hunch. I did my own data collection and analysis. Even after adjusting for the bias of the reporters (by restricting the analysis to just parents and grandparents of the reporter), the signal of harm was huge.
Science used to be about data and what the data shows. Sadly, today, science is about what the CDC says, even if there is no data in support of the recommendation whatsoever.
The most stunning example of this is the “six foot rule.” Did you know that it was entirely fabricated out of thin air? From Presidential Takedown page 49:
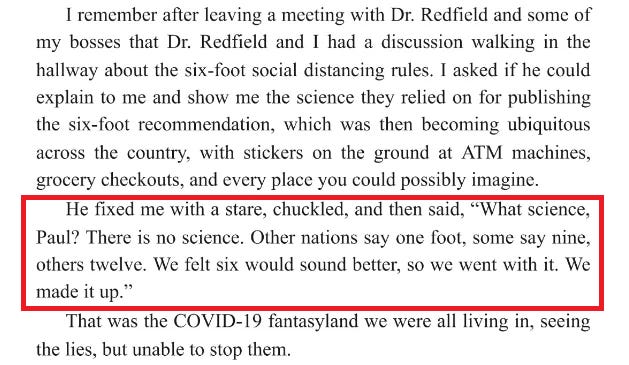
What is even more stunning is that the CDC has never admitted this publicly. This is evidence that they are a corrupt organization and the corruption goes to the very top of the organization.
We now have over two years worth of death and vaccination data for people who died after getting a COVID shot, yet nobody wants to see the record level data tied to the vaccination dates?!?!
Let me be perfectly clear:
This is an abject failure of the entire medical community for not demanding to see this data.
In the US, hundreds of millions of people participated in a massive clinical trial and have data to share with people. At least 500,000 of the participants paid the ultimate price: they sacrificed their lives to send a message to America about the vaccines. It is extremely disrespectful to these people to ignore their death data and not share it with the public. Why are we not allowing these people to share their data?
Do you think if we could ask those people right before they died, “Do you want to let others know what killed you?” Do you think they would all say, “No! Don’t let anyone know. Please keep it a secret!”?
John Beaudoin and I have been calling for the death data to be set free and made public. We have been ignored.
Why aren’t any of these organizations calling for data transparency here so we can learn the truth?
- The mainstream medical community
- Heads of state throughout the world
- The CDC
- The FDA
- The White House
- Congress
- The mainstream media
- Public health authorities
- Any doctor or nurse who recommends the jab to patients
- Universities who mandate the vaccines for students, staff, or faculty
- Any organization that supports COVID vaccines for their members, employees, or visitors
The data exists in VSD as well. But the CDC won’t allow anyone to see it.
The data exists in every state health department. But you can’t FOIA it because it requires a join to avoid PII problems and FOIA requests are not allowed if they generate effort like that. So FOIA requests won’t work.
It’s time for everyone to demand that our health authorities “Show us the data!”
We should all refuse to comply until they produce it.
Who could ever forget the classic “Show me the money!” scene from the movie Jerry Maguire?
In the same way Tom Cruise said passionately “Show me the money,” everyone all over the world should be equally passionate with their doctors and healthcare authorities and demand: “Show me the DATA” before we agree to comply with their requests/demands regarding vaccination.
Check out this video from True North entitled “Show us the data and evidence” that described the civil disobedience in Canada:
Business owners and local politicians are pushing back against the government’s lockdown measures. Their ask of the government is simple – if you’re going to shut us down, show us the data and evidence.
The data that we have shows that the biggest harm is being done to kids.
Therefore, the biggest urgency is to put pressure on any school or university that recommends or requires the COVID vaccines to drop it immediately
Please ask the university president or head of school at any school your child attends to contact the CDC and let them know that if the CDC doesn’t make the death-vax record level data publicly available with the next 30 days, that the school will suspend their COVID vaccination policies until such time as this data is produced and scientists can analyze it. That is the only ethical thing to do.
You can refer to my article in your email.
The public health authorities have been voluntarily keeping the data secret for two years now. That data would end the debate. We should not let them continue to get away with it.
Is the FDA “doubling down” on a failed strategy?
By Maryanne Demasi, PhD | January 30, 2023
Last Thursday, the FDA convened its Vaccines and Related Biological Products Advisory Committee (VRBPAC) to discuss the future of covid vaccines.
The panel voted 21 to 0 in favour of moving towards a more simplified vaccine schedule – an annual shot which would be updated as new variants emerge – much like the annual flu shot.
Despite the unanimous vote, VRBPAC members did raise concerns about knowledge gaps and questioned the need to boost everyone, as well as the futility of chasing rapidly mutating viruses.
But it all fizzled out quickly, and the FDA promised to reconvene in May or June to discuss the data further.
That said, I had some interesting observations of my own.
We are three years into the pandemic, and the FDA has still not established a “correlate of protection” for the vaccines.
Eight covid-19 vaccine emergency use authorisations (EUAs)* have been granted, based on their ability to induce “neutralising antibodies,” a surrogate marker of protection.
The idea is, the more antibodies you produce, the better you are protected.
Except, neutralising antibodies do not predict the degree to which someone is protected from infection… and the FDA knows it.
Ofer Levy, VRBPAC member and Professor of Paediatrics at Boston Children’s Hospital first voiced his concern at the April 6, 2022 meeting.
“We’re at risk of doubling down on a failed strategy,” said Levy as the committee discussed a framework for offering annual covid shots for Americans.
“Where is the federal effort to coordinate all of that to develop a public repository around the correlate of protection, and to make sure we have the best available data for the immunogenicity when we make those decisions?”
The FDA’s top vaccine official, Peter Marks, agreed with Levy.
“There is not a clear, perfect, immune correlate of protection” admitted Marks, “We’re using poor man’s immune correlates of protection here — or poor person’s immune correlates of protection with antibody levels.”
In Dec 2022, Peter Marks reiterated these concerns in an article published in JAMA. He and his co-authors wrote:
“Therefore, unless correlates of protection that are strongly associated with duration of protection against COVID-19 can be identified, it is likely that rather than relying on immunobridging to infer vaccine effectiveness, large randomized clinical trials similar to the initial trials of the currently authorized or licensed vaccines for COVID-19 will be required to ascertain the effectiveness of these new vaccines.”
But fast forward to this latest meeting, and it becomes clear that we’re all still in the dark.
We have no correlate of protection, the FDA is relying heavily on real world studies (confounded data) and the agency still has not demanded any randomised controlled trials to show the bivalent booster can reduce severe disease or hospitalisations.
It’s no wonder doctors are coming out in droves, refusing to have any more covid shots until the FDA demands better studies.
“I don’t think we can say with credibility what the objective benefits are for someone like me to take an additional dose, nor what the rate of any rare but important side effects would be,” tweeted Todd Lee, a physician certified in Infectious Diseases and General Internal Medicine in Quebec, Canada.
Similarly, Vinay Prasad, haematologist-oncologist at the University of California San Francisco vowed not to take any more shots until there were data from randomised controlled trials.
“I took at least 1 dose against my will. It was unethical and scientifically bankrupt. I am not done with that error. No more,” he tweeted.
As part of its post-marketing requirements, Pfizer is legally obligated to conduct a study involving people aged 16 to 30 to look at rates of subclinical myocarditis (i.e. underlying damage to the heart muscle without causing symptoms).
The final report was due 31 Dec 2022, but that deadline lapsed, and the FDA said nothing. There was no mention of the study, neither in the briefing notes ahead of the VRBPAC meeting, or during the meeting.
I asked the FDA directly for access to Pfizer’s study, but the agency said in an email, “You may submit a FOIA request for this information, or if you would like it more quickly, you can reach out to the manufacturer directly.”
Pfizer did not respond to my request, and the FDA refused to confirm whether it had even received Pfizer’s study, before abruptly ending our communication.
Jessica Adams, an expert in drug regulatory affairs pointed out on twitter that the FDA had quietly changed the due date for the study from 31 Dec 2022 to 30 June 2023.

So, now as it stands, millions of young people will receive boosters, mandated or not, without knowing if the vaccine is causing subclinical myocarditis.
FDA still working from home
Finally, the meeting was again held online because the majority of FDA employees are still working from home.
Since all federal employees have been mandated to take the covid-19 vaccine to “protect themselves and those around them,” why aren’t they conducting face-to-face meetings?
“FDA leaders are in a bubble. How much longer will the FDA (18,000-employees) continue to work remotely? It’s mid-day on a weekday and the parking lot is essentially empty” tweeted Marty Makary, surgeon and public policy researcher at Johns Hopkins University.
“The FDA was telling the rest of America to get vaccinated, mask up and go back to work, but the FDA mysteriously did not follow its own advice,” said David Gortler, drug safety expert and former senior advisor to the FDA commissioner.
Well, it’s as though the FDA heard the cries.
Today, the FDA announced that “staff will be transitioning to a hybrid workplace.” This transition will enable face-to-face formal meetings between FDA and industry to resume within weeks.
*FDA issued eight EUAs based on neutralising antibodies (immunobridging studies) – an unproven correlate of protection.
- Pfizer EUA – 6 months to 4 year olds
- Pfizer EUA – 5 to 11 year olds
- Pfizer EUA – 12 to 15 year olds
- Pfizer EUA booster #1
- Pfizer EUA booster #2
- Moderna EUA – 6 months to 17 year olds
- Moderna EUA – booster #1
- Moderna EUA – booster #2
Vitamin D Cuts COVID-19 Risk of Death in Half, New Study Finds. So Why Isn’t it Recommended?

BY WILL JONES | THE DAILY SCEPTIC | FEBRUARY 3, 2023
Vitamin D cuts the risk of death from COVID-19 by 51% and the risk of ICU admission by 72%, a meta-analysis of randomised controlled trials has found. The new study, published in Pharmaceuticals, is titled “Protective Effect of Vitamin D Supplementation on COVID-19-Related Intensive Care Hospitalisation and Mortality: Definitive Evidence from Meta-Analysis and Trial Sequential Analysis”. Here’s the abstract, summarising the study’s method and results.
Background: The COVID-19 pandemic represents one of the world’s most important challenges for global public healthcare. Various studies have found an association between severe vitamin D deficiency and COVID-19-related outcomes. Vitamin D plays a crucial role in immune function and inflammation. Recent data have suggested a protective role of vitamin D in COVID-19-related health outcomes. The purpose of this meta-analysis and trial sequential analysis (TSA) was to better explain the strength of the association between the protective role of vitamin D supplementation and the risk of mortality and admission to intensive care units (ICUs) in patients with COVID-19.
Methods: We searched four databases on September 20th 2022. Two reviewers screened the randomised clinical trials (RCTs) and assessed the risk of bias, independently and in duplicate. The pre-specified outcomes of interest were mortality and ICU admission.
Results: We identified 78 bibliographic citations. After the reviewers’ screening, only five RCTs were found to be suitable for our analysis. We performed meta-analyses and then TSAs. Vitamin D administration results in a decreased risk of death and ICU admission (standardised mean difference (95% CI): 0.49 (0.34–0.72) and 0.28 (0.20–0.39), respectively). The TSA of the protective role of vitamin D and ICU admission showed that, since the pooling of the studies reached a definite sample size, the positive association is conclusive. The TSA of the protective role of vitamin D in mortality risk showed that the z-curve was inside the alpha boundaries, indicating that the positive results need further studies.
Discussion: The results of the meta-analyses and respective TSAs suggest a definitive association between the protective role of vitamin D and ICU hospitalisation.
Despite these highly positive results, the latest official guidelines from NICE still state that vitamin D is not recommended for the prevention of COVID-19. (NICE also doesn’t recommend the use of ivermectin or budesonide.) Yet remdesivir is recommended despite the WHO finding little or no effect. Will NICE now update its guidelines? I wouldn’t count on it.
Dr. John Campbell discusses the new study in a recent video, arguing the evidence on vitamin D is now conclusive and wondering why adequate vitamin D supplementation is not being officially promoted in the U.K. The fact that the MHRA is 86% industry-funded may have something to do with it, he suggests.
Featured Video

Larry Johnson: U.S. Desperation Grows as Iran Is Winning
or go to
Aletho News Archives – Video-Images
From the Archives
A low-fat, high-carb diet has been the largest public health experiment in history. It’s past time for a rethink.
By Malcolm Kendrick | RT | November 25, 2020
New research suggests that four billion people globally will be overweight in 2050. This trend can be traced back to the ‘low-fat, high-carb’ guidelines first issued in the 70s, and should prompt a major U-turn on dietary advice.
A recent report from the Potsdam Institute predicts that by 2050 there will be four billion overweight people in the world, with one-and-a-half billion of them obese. This is not entirely surprising. The world has been getting fatter for years, and things do not seem to be slowing down.
Why is this happening? … continue
Blog Roll
 Aletho News
Aletho News- Pirates of Mediterranean: Israel does as it pleases in the Sea of Three Continents
- Minab children massacre not ‘unfortunate situation’ but ‘heinous war crime’: Tehran
- OPCW Forced To Pay Damages To Whistleblower Who Found Evidence Of False Flag In Syria
- Iran can thrive under blockade, the US and its allies cannot
- Iran slams US leadership, debunking fabrications, false war costs
- Here’s why Iran is sovereign and Germany is not
- Israel pours $730m into global propaganda machine as reputation collapses
- Leaked audios reveal pro-Israel groups ‘paid’ for US pardon of convicted drug trafficker Juan Orlando Hernandez
- Congress Extends Section 702 Spy Program 45 Days
- Zionists Are Gunning for Your Freedom of Speech
- If Americans Knew
- Israel to pour $730m into propaganda arm amid reputational crisis
- Real Cost of Iran War Likely Double the $25 Billion Figure the Pentagon Gave to Congress
- Israel conducts farthest-ever strike in long history of attacks on Gaza humanitarian aid flotillas
- In Gaza, Israel commits 10+ ceasefire violations a day – Daily Update
- US ships 6,500 tons of munitions, equipment to Israel in 24 hours
- A New Library in Gaza Rises From the Ashes of Destruction
- Israel’s top Jewish religious body ‘refuses to condemn’ smashing of Jesus statue
- Nun assaulted in Jerusalem amid ‘pattern’ of anti-Christian attacks by Israelis
- Former Tik Tok official describes massive pressure from Israel lobby
- Amid ceasefire violations and genocide, Israel commits piracy – Daily Update
- No Tricks Zone
- Oversupply Of Volatile Solar Energy Leads To Record NEGATIVE Prices!
- New Study: Extreme Heat Records, Heatwaves, Extreme Cold Records Declining Across US Since 1899
- It’s The Cold, Stupid! Cold 20 Times More Lethal Than Heat, Multiple Studies Show
- European Institute For Climate And Energy: “Climate Debate is Seldom About Science”
- New Study: The Climate May Be 5 Times More Sensitive To Solar Forcing Than Commonly Assumed
- EV Industry Reached $70 Billion In Losses In 2024 Due To Delusional Green Ideologies
- Reality Check: Maldives Have Actually Grown In Size Or Remained Stable Over Recent Decades
- Abrupt Climate Change Also Occurred NATURALLY In The Past …25 Times During Last Ice Age
- Cave Discovery Reveals Today’s Desert Climates Were Recently Far Warmer, Wetter, Teeming With Life
- German Expert: Heat Dome Led To Record Temps In Western USA…Warmer In 1934, 1936
