TUCKER CARLSON ON OPIOIDS, COVID AND ANTIDEPRESSANTS
TUCKER CARLSON TONIGHT | JULY 25, 2022
Tucker Carlson reveals the shocking side effects of antidepressants and calls out Democrats for not holding Big Pharma accountable. His full opinion piece can be read here: https://www.foxnews.com/opinion/tucker-carlson-drugs-not-answer-every-human-problem
Jacinda’s duplicity as pupils are told to mask up again or be punished
By Guy Hatchard | TCW Defending Freedom | July 27, 2022
LAST week the New Zealand government called for mask wearing to be enforced in schools – and many schools have apparently decided to punish students who do not comply.
Asked whether she was happy with that situation, Prime Minister Jacinda Ardern ducked the question, denied the mandate, passed the buck, and still managed to appear happy for students to be punished.
She said: ‘We are really open-minded on this issue. We in fact went back multiple times to education and health and said, “Look, if you believe we should bring that mask mandate back we are happy to do that. Whatever you think is going to be in the best interest of our learners, our schools, and our health outcomes.”
‘They came back to us and said we should strongly encourage their use, but we should still allow schools to implement the policies themselves. That’s where we have landed. We have not said mask wearing is compulsory, but we are strongly encouraging it.’
You can watch the full interview here. There is plenty of spin, but not a lot of ambiguity. Head teachers have been given a green light to dust off the detention book.
Some schools are giving students detention either during lunchtime or after school (the modern equivalent of writing out ‘I will wear my mask’ a thousand times), which translates into loss of opportunities to participate in extracurricular activities and sports. This should be unacceptable and is certainly deleterious to a student at any age and may result in them becoming alienated or adversely affected emotionally or socially. Students go to school to learn and understand the process of verifying knowledge, to engage socially, and to develop skills in communication; whereby they may debate and agree or disagree with one another, without the fear of being punished or discriminated against.
There is a considerable body of scientific evidence pointing to the ineffectiveness of masks to stop transmission. Long-term mask use also poses health risks and causes significant learning deficits.
Some parents, and hence their children, will be well aware of this. A policy of punishment for non-mask wearers is the antithesis of a constructive learning environment and teaches: ‘Comply without question or face a penalty.’
School attendance in New Zealand is already at an all-time low. As a result of this move, it is going to fall further. The opportunities for constructive debate are fast disappearing in education, and we can understand why many parents are turning their thoughts to home-schooling.
The problem here is that the public is being deliberately kept in the dark about the ineffectiveness of masks and the dangers of prolonged mask-wearing. Most are following government advice, thinking that they are protecting themselves and others from Covid. They are ending the day with a headache and a sore face, but sure that they have thereby saved the world.
So far, the NZ government has kept a tight hold on the Covid narrative by warning people that alternative news sources and social media conversations are full of misinformation, whilst government announcements are closely following ‘the science’. They also give cash grants to the mainstream media and advertise to the point of saturation.
That is all set to ramp up from today. The government has concluded a formal binding agreement with Meta (Facebook and Instagram), TikTok, Google (Gmail and YouTube), Amazon (Spark) and Twitter to limit the availability of harmful content including ‘misinformation and disinformation’ in New Zealand.
In a world first, the code is described as ‘voluntary’, but it includes a ‘commitment’ to being held ‘accountable’ which allows its provisions to be ‘enforced’. How is that for doublespeak? And who is deciding what is harmful?
The mask mandate rules and the information censorship have something in common. The government is asking others to do its dirty work, then asking us to believe it has nothing to do with those others. We are not naive: we already know how this works.
The agreement cleverly conflates things that we all feel should be controlled, such as child sexual exploitation and incitement to violence, with rational discussions about drug safety and effectiveness.
YouTube has previously withdrawn Covid content from view at the private request of the Ministry of Health. Apparently this can happen if any content causes the NZ government embarrassment.
I don’t suppose it has escaped your notice that internet censorship is a tool of oppressive governments. The dangers are becoming all too obvious here, where the majority of the public, subjected to blanket government advertising, still believe that regular mRNA boosters and flu shots offer protection for life that is stronger than natural immunity.
This is all taking on a macabre aspect, because official Covid data here and in the EU is showing that boosted individuals are increasingly more likely to die with Covid than are the unvaccinated. The apparent reluctance on the part of the government to engage with the implications of this official Covid data is seriously worrying. Governments traditionally have a general duty of care when it comes to policing public health measures.
This year has been one of the wettest on record in NZ. As a result, ants are coming into homes in record numbers and you may have been struck with how expendable ant populations are.
Ant colonies appear to have a centralised administrative policy whereby any number of workers can be put at risk in the search for homes and food for queens. This is a sort of groupthink which starkly contrasts with human ethics, wherein the individual is highly valued.
Here in New Zealand, we are 90 per cent mRNA vaccinated and we currently have the highest rate of all-cause mortality in the world. Even the Ministry of Health has admitted this is not because of Covid. Yet if you follow the government advertising and press statements, you will probably be unaware of this and happily sure that ‘the science’ is being followed.
I don’t need to draw conclusions for you here. If you are following the current Covid science journal publishing, you will be well aware of mathematical arguments entirely based on collected data which are taking place within a rational framework. Ignoring or hiding these is dangerous.
The author is in New Zealand
This blog is co-authored with Narayani Hatchard.
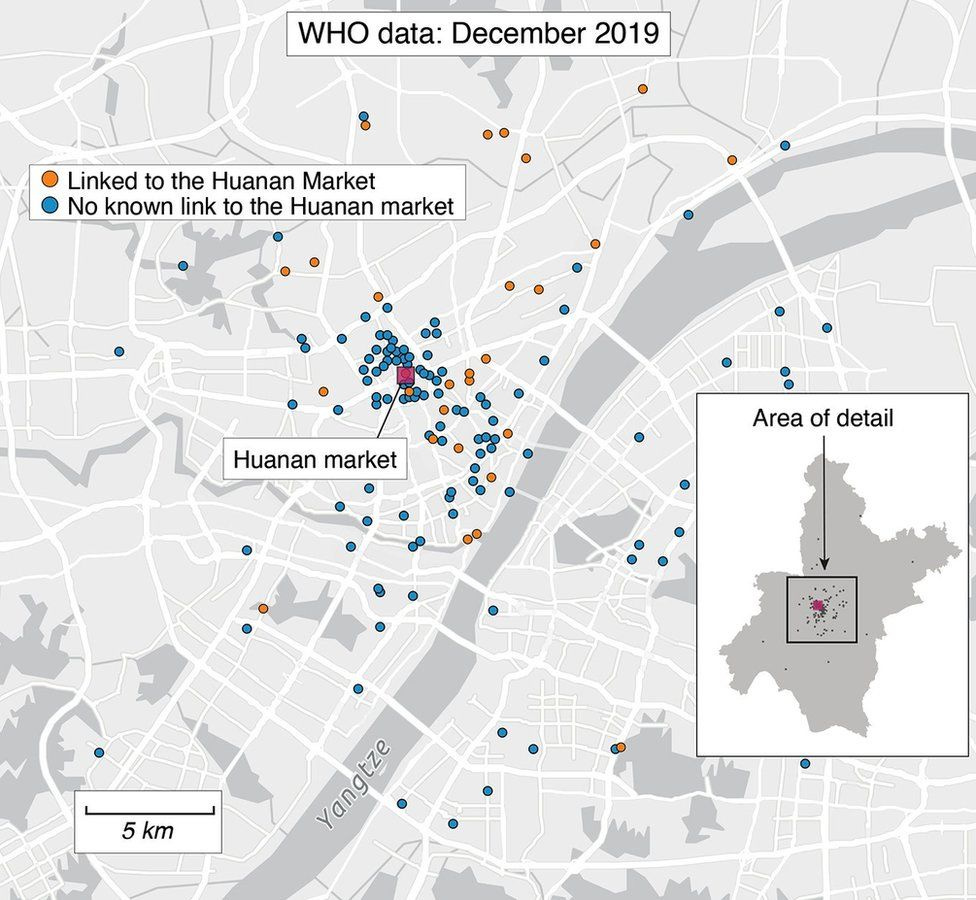
Lie Exposed: BBC Says Covid-19 Came from Wuhan Market
BBC forgot to add Wuhan Institute of Virology to the map
By Igor Chudov | July 26, 2022
BBC has a new article out, about the “origins of Covid-19”:

Great, right? If BBC says that Covid origin studies point to the Wuhan seafood market as the source of Sars-Cov-2, then it must be so, right? After all, we trust the BBC and we especially trust science and scientific studies.
BBC’s map of early cases clustering around the market, offers the only real evidence that the BBC article provides, and looks extremely convincing:
I was almost convinced myself. I was just about ready to delete all my Covid origin articles, but at the very last moment, I decided to check with Google maps on the location of the Wuhan Institute of Virology and Infectious Diseases (archive link). I placed both on the same picture as above, so you can see where they are in relation to the early outbreak cases:
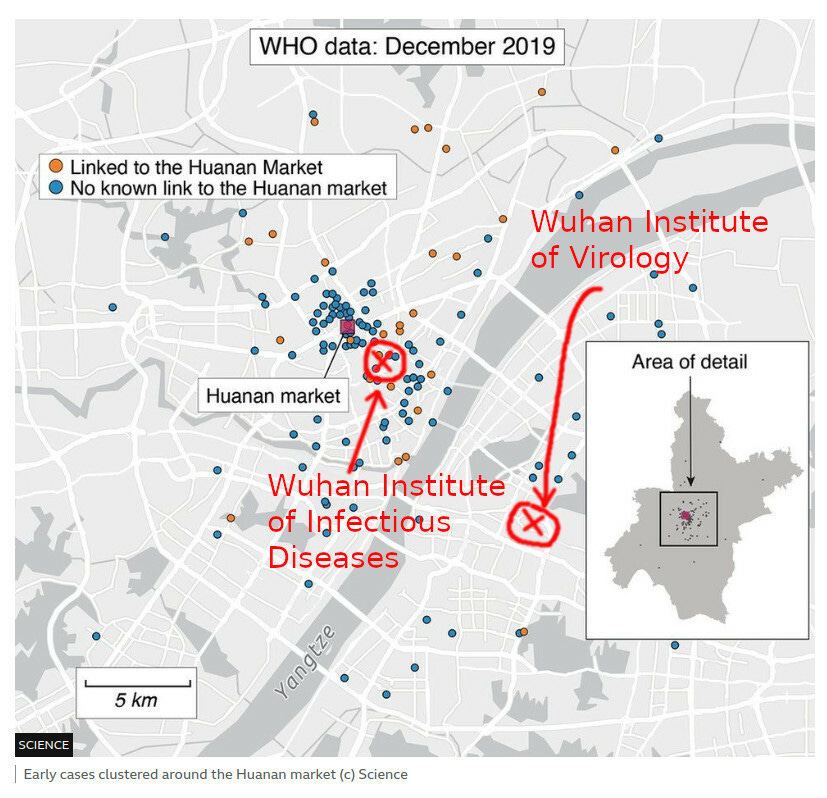
Again, the dots represent the first recorded cases of Covid-19. The circled “X”’s are WIV and WIID. Please tell me, after seeing the second picture, are you still sure about the Wuhan’s market being the source? If you are capable of elementary thinking, which all of my subscribers certainly are, you would think that the BBC article is total bunk. And of course, you would be right!
So:
- Why did BBC’s map exclude locations of WIV and WIID, which are obviously known to anyone in the news business who is writing about Covid, and are critically important to the story if they wanted to tell it truthfully?
- Because if the article included these locations, it would be obvious to any reader that the article is total nonsense and is a completely laughable attempt at misdirection.
- Therefore, BBC wanted to lie to us and mislead us by omission.
Okay, then, why did BBC decide to lie to us?
It lied because if BBC showed locations of WIV and WIID on the map, the story of Covid would sound something like this:
Dear Citizens! By pure accident, a Chinese virological laboratory released an experimental deadly virus, whose creation was funded by the NIH. But do not worry: purely by coincidence, NIH scientists also worked on a vaccine against such viruses. We are very fortunate that Moderna, with NIH help, in just TWO DAYS, was able to design a perfect vaccine against Sars-Cov-2. Never mind that previous vaccines took decades to develop. Science works faster now!
Dear Readers: you must take this vaccine. We are certain that it works and if you get vaccinated, you will not get the virus. The virus stops with every vaccinated person. If you do not take our vaccine, you will be fired from your job, will be excluded from society, and will starve for disrespecting science and authorities. This vaccine is safe for pregnancy because there is no proof that it is unsafe for pregnancy (we made sure of that).
The crazy right-wing conspiracists, rogue scientists, and discredited doctors warning that the vaccine is not safe, have been fired from their jobs, lost medical licenses, and were removed from social networks and Google. Therefore, we now have total scientific and medical consensus about the vaccine. Please believe us, because all NIH-funded scientists and still-licensed doctors agree with us. If you do not believe this, you are an ignorant, anti-science fool and a “winter of death” awaits you.
Get vaccinated! Get vaccinated! Get vaccinated! Get vaccinated!
That would be a strange and somewhat less believable story, right? It would be much easier to deal with the general public if the public believed that the virus came from Wuhan’s “wet market”. That’s why BBC is publishing such obviously dishonest articles.


A Pandemic of the Triple Vaccinated
By Ramesh Thakur | Brownstone Institute | July 26, 2022
Deborah Birx was the White House Covid-19 response coordinator under President Donald Trump. Jeffrey Tucker recently wrote a brutal takedown of her deliberate misrepresentations of science and data in order to manipulate Trump into going along with her preferred but misguided policy interventions to deal with the Covid outbreak.
In an ABC podcast on December 15, 2020, she said: “I understand the safety of the vaccine … I understand the depth of the efficacy of this vaccine. This is one of the most highly-effective vaccines we have in our infectious disease arsenal.”
Appearing on Fox News on July 22, however, she claimed: “I knew these vaccines were not going to protect against infection. And I think we overplayed the vaccines. And it made people then worry that it’s not going to protect against severe disease and hospitalization.”
This might help to explain why there has been such a concerning collapse of public confidence in leading health institutions and “authorities.”
Biden’s claim of a pandemic of the unvaccinated
During a CNN Town Hall event on July 21, 2021, President Joe Biden said: “If you’re vaccinated, you’re not going to be hospitalized, you’re not going to be in an ICU unit, and you are not going to die.”
On May 16, 2021, Dr. Anthony Fauci claimed that vaccination did not just protect the individual, but also the community, because “by preventing the spread of the virus … you become a dead end to the virus. And when there are a lot of dead ends around, the virus is not going to go anywhere.”
Relying in the judgment of his chief medical adviser, Biden took to talking about the pandemic of the unvaccinated in a two-track effort both to encourage vaccine takeup and to vilify, demonize and shame those who remained uncertain enough of the balance of benefits and short and long-term risks of the rushed Covid-19 vaccines to avoid succumbing to the multiple pressures to go along with the zeitgeist in order to get along with everyone.
We have now had both Dr. Fauci, the public face of the US management of the pandemic, revered in some quarters and reviled in others, and President Biden himself get infected with Covid, despite both being double-vaccinated and double-boosted.
Inevitably, to try and stop the official narrative on the benefits of the vaccine from unraveling completely and in order to encourage continuing vaccine and boosters takeup, they insist that their updated vaccination status helped to limit the severity of their infection. This is based on a cult-like faith, akin to self-validating and self-canceling explanations put forth by astrologers for predictions that come true and don’t, as the case may be.
Although on July 20, Fauci admitted that the data do make it clear that “vaccines – because of the high degree of transmissibility of this virus – don’t protect overly well, as it were, against infection.” Robert F. Kennedy Jr. asked why the media was not holding Fauci “accountable for the costly national policies and the lockdowns that were utterly built upon his initial assertion that the vaccines would prevent transmission and end the pandemic.”
Equally, of course, one must ask again: if vaccines don’t stop transmission, how does the government justify vaccination mandates for travel to the US?
In a matching vein, the New South Wales (NSW) Health report for the week ending 16 July claims that: “The minority of the overall population who have not been vaccinated are significantly overrepresented among patients in hospitals and ICUs with Covid-19.”
The following challenges that claim using their own data.
By drawing on the distinction between the efficacy and effectiveness of vaccines, it’s possible to argue that in NSW, rather than a pandemic of the unvaccinated, what we have witnessed is a pandemic of the triple-vaccinated.
NSW health facts
In September 2021, NSW had 844 staffed ICU beds, of which 173 (20.5 percent) were occupied by Covid-19 patients. (Australia-wide, the number of ICU beds is 2,183.) By January 2022, the number had increased to around 1,000. If necessary, this can be bumped up further by utilizing the limited number of ICU beds in private hospitals.
There are 9,500 general ward beds in public and another 3,000 beds in private hospitals in NSW. In mid-July 2022, there were 2,058 people in hospital with Covid-19 in NSW, or 21.7 percent of the public system’s capacity and 16.5 percent of the state’s total hospital beds capacity. An additional 6,500 people were in hospital for non-Covid reasons.
During the week of July 10–16, a total of 806 people were admitted to hospital with Covid-19, another 77 into ICU, and 142 people died with Covid-19 illness (though not necessarily as the primary cause of death). Moreover, of the 142 deaths, only four were aged below 60, so that people aged 60 and above accounted for 97.2 percent of all Covid-related deaths in the state.
Additionally, of the 142 dead, the vaccination status of 2 was not known. One hundred and eighteen of the remaining 140 – 84.3 percent – were at least double-vaccinated and 69 had received three doses of the vaccine: by far the biggest single cohort and almost equal to all the others combined. Hence the thought that perhaps what we are experiencing is a pandemic of the triple-vaccinated.
Efficacy vs. effectiveness
The Cambridge Dictionary defines efficacy as “how well a particular treatment or drug works under carefully controlled scientific testing conditions.” By contrast, effectiveness is defined as “how well a particular treatment or drug works when people are using it, as opposed to how well it works under carefully controlled scientific testing conditions.”
Thus doubts about the effectiveness of a new product in treating any disease can only be resolved once the vaccine is widely available and administered in the target population. GAVI (the Global Alliance for Vaccines and Immunization), now called Gavi, the Vaccine Alliance, is a partnership between the World Health Organization, Unicef, the World Bank and the Bill & Melinda Gates Foundation.
Writing for GAVI, Priya Joi offers similar definitions, describing “efficacy” as the measure of how much a vaccine prevents infection (and possibly also transmission) under ideal, controlled conditions where a vaccinated group is compared with a placebo group. She adds: “Vaccines do not always need to have an exceptionally high effectiveness to be useful, for example the influenza vaccine is 40-60% effective yet saves thousands of lives every year.”
Examining the percentage of the thrice-jabbed in hospital admissions, ICU beds, and dead against the baseline of their share in the overall population, preferably age-adjusted, is critical to calculating vaccine efficacy. I’m not sure how helpful that is to assessing the effectiveness of vaccines in keeping the absolute numbers down below the state’s or country’s capacity thresholds of hospital and ICU beds.
If the primary public health justification for universal vaccination is to reduce the burden on the health infrastructure and prevent hospitals and ICU capacity from being overwhelmed – which was indeed the main justification in the language of two-three weeks to flatten the curve – then the key question becomes: How effective are the vaccines in preventing hospital admissions and ICU occupancy? Their role in preventing infection by itself is less important than their effectiveness in controlling the severity of the disease.
For example, a report from the Dutch health ministry found that the effectiveness of two doses of vaccines after one year had fallen overall to 0 percent against hospitalizations and minus 20 percent against ICU admission. Perhaps more pertinently in relation to NSW, Dr. Eyal Shahar notes signs in Israel of a short-term fatality rate of a third dose.
Efficacy is more helpful to an individual in assessing the relative risk of infection if vaccinated or not. Because Covid vaccines were granted emergency-use authorization and long-term efficacy and safety profiles were simply not available, doubts have persisted about the integrity, credibility and long-term reliability of data and results from the trials conducted by the vaccine manufacturers.
Moreover, as we’ve been made aware with respect to the UK, different branches of the government like the Health Security Agency and the Office of National Statistics use different and hotly contested methodologies for calculating the numbers and proportions of the population infected by Covid, which in turn determines the estimated infection fatality rate (IFR).
In any case, even if we agree that the IFR and case fatality rate (CFR) of flu and Covid are broadly comparable by now, the scale and magnitude of Covid means that similar IFR and CFR still produce vastly different orders of challenges for public health policy.
By contrast the effectiveness of the vaccines for controlling hospital admissions, ICU bed occupancy and mortality is measured by solid and reliable information that is both accurate and comprehensive in Western countries. This makes vaccine effectiveness a better policy tool for deciding on population-wide mandates while efficacy might be the more relevant for informed individual decisions.
Covid in NSW

In the period for the weeks ending May 28 to July 16, 2022 in NSW, of those whose vaccination status was known, only eight unvaccinated people were among the 3,509 who required hospital admission (Figure 1). The numbers in ICU were 5 unvaccinated and 316 with 2-4 doses (Figure 2); the number of Covid dead were 110 unvaccinated and 662 with 2–4 doses (Figure 3).
With 83 percent of people at least double-vaccinated, they accounted for 99.4, 96.3, and 85.4 percent, respectively, of NSW Covid hospital admission, ICU and deaths in these seven weeks.
In the final week of this seven-week period, of those whose vaccination status was known, there were exactly zero – zilch, nada – unvaccinated people among the 624 hospital and 59 ICU Covid-19 admissions, compared to 615 with two, three and four vaccine doses in hospital and 58 in ICU beds. Just the triple-vaccinated, who account for 68 percent of the population of NSW, made up 57.5 percent in hospital, 53.7 percent in ICU and 53.5 percent of the Covid dead.

The claim that the unvaccinated are “significantly overrepresented” in Covid-19 hospital admissions and ICU occupancy is not just misleading, it’s downright false. Seriously, do they look at the data in their own reports before drawing policy conclusions?

As knowledge about the rapidly fading efficacy of the vaccines, and in particular of each successor booster dose, has firmed, and also as the vaccine escape properties of the newer variants of Covid-19 have become better known, the equivalent question now is: are we into the era of the pandemic of the triple -vaccinated? The biggest strain on NSW hospitals and ICU beds is coming from their numbers.
Public health officials can talk and dissemble all they want about the baselines for comparisons and pretend to possess great sophistication in their understanding of the current state of the disease. They still cannot spin their way out of the hard data.
Instead they are exhibiting a severe case of cognitive dissonance in encouraging the double-vaccinated to get boosted and double-boosted. The ineffectiveness of vaccines in reducing hospital admissions and ICU demand is in itself sufficient to torpedo vaccine mandates. Doubts on their efficacy and concerns about their adverse effects and long-term safety further strengthens the case against mandates.
Ramesh Thakur, a former United Nations Assistant Secretary-General, is emeritus professor in the Crawford School of Public Policy, The Australian National University.
CHD Demands D.C. Schools Rescind COVID Vaccine Mandate, Says It Violates Federal Law
By Megan Redshaw | The Defender | July 25, 2022
Schools in Washington, D.C., will require all students ages 12 and older to get the COVID-19 vaccine before they can attend school in the fall, despite warnings from legal experts who say the mandate violates federal law.
The Office of the State Superintendent of Education announced on July 19 that student immunization requirements for the upcoming 2022-2023 school year will include the COVID-19 vaccine for all students who are of an age for which there is a vaccine fully approved by the U.S. Food and Drug Administration (FDA).
“On July 8, 2022, the FDA fully approved the COVID-19 vaccine commonly known as the Pfizer-BioNTech COVID-19 Vaccine for individuals 12 to 15 years old,” said State Superintendent of Education Christina Grant in a press release.
“The approval of the Pfizer-BioNTech COVID-19 vaccine for individuals 12 to 15 means that, unless exempted, any student age 12-15 at the start of the 2022-23 school year must have received the primary COVID-19 vaccine series or have started receiving the shot by Sept. 16, 2022,” she said.
“We want to make sure that all of our students have everything they need for a healthy start to the school year,” Grant added. “This means making sure children see their primary medical provider for a well-child visit and receive all needed immunizations.”
D.C. law requires students in all area schools, including private, parochial and independent schools, to be fully compliant with mandated vaccinations, unless they have an approved exemption. The law also requires schools to verify immunization certification for all students.
The requirement was detailed in a law the D.C. Council approved last year and is the first legislation of its kind in the region.
CHD demands D.C. Schools rescind mandate
In a letter sent today to Grant, Robert F. Kennedy, Jr., chairman and chief legal counsel for Children’s Health Defense (CHD), asked Grant to rescind the program or CHD would sue to overturn the mandate.
Kennedy said Grant’s press release was incorrect because the Pfizer-BioNTech COVID-19 vaccine was never fully approved and still remains under Emergency Use Authorization (EUA).
The FDA earlier this month granted full approval to Pfizer’s Comirnaty COVID-19 vaccine for adolescents 12 through 15 years old, without convening its vaccine advisory panel.
In August 2021, the agency granted full licensing of the Comirnaty vaccine for ages 16 and older.
However, there are no Comirnaty-labeled vaccines available in the U.S., for any age group.
Although courts have upheld many childhood vaccination requirements for licensed and approved vaccines, no court has ever upheld a mandate for schoolchildren for an EUA vaccine, according to Kennedy.
Kennedy wrote:
“In fact, a District of Columbia United States District Court held that EUA vaccines cannot be mandated to soldiers in the U.S. military, who enjoy far fewer rights than civilians. Doe #1 v. Rumsfeld, 297 F.Supp.2d 119 (2003). That court held: ‘… the United States cannot demand that members of the armed forces also serve as guinea pigs for experimental drugs.’ Id. at 135.
“Federal law 21 U.S.C. § 360bbb-3(e)(1)(A)(ii)(III) requires that the person to whom an EUA vaccine is administered be advised, ‘of the option to accept or refuse administration of the product, of the consequences, if any, of refusing administration of the product, and of the alternatives to the product that are available and of their benefits and risks.’
“The reason for the right of refusal stems from the fact that EUA products are by definition experimental.
“Under the Nuremberg Code, a universal legal norm, no one may be coerced to participate in a medical experiment. Consent of the individual is ‘absolutely essential.’ The liability for forced participation in a medical experiment, not to mention liability for injury from such coerced medical intervention, may be incalculable.”
Commenting on the D.C. mandate, CHD President Mary Holland said, “It violates fundamental human rights and international law to force people, and especially children, to take experimental medical products.”
“We sincerely hope the District will reconsider its misguided policy for schoolchildren,” Holland added.
Another organization — Liberty Counsel — said it may also challenge the District of Columbia’s vaccine mandate.
“There is no FDA-approved COVID shot available and therefore, individuals have a right under the emergency use authorization to refuse these shots,” Matthew Staver, founder and chairman of Liberty Counsel, told The Epoch Times.
Under the Federal Food, Drug, and Cosmetic Act, people receiving an EUA product must be advised that some benefits and risks “are unknown” and given the “option to accept or refuse administration of the product.”
“It is your choice to receive or not receive [the vaccine],” Staver said. “Should you decide not to receive it, it will not change your standard medical care,” according to FDA fact sheets on EUA COVID-19 vaccines.
Several other school systems have attempted, so far unsuccessfully, to implement a COVID-19 vaccine mandate:
• Louisiana: The Louisiana Department of Health in May said it would no longer seek to make COVID-19 vaccines mandatory for the upcoming school year because the shot had not received full FDA approval for people under the age of 16.
The decision came after CHD and thousands of concerned parents on March 16 filed an amicus brief in a lawsuit seeking to stop the Louisana Department of Health from adding COVID-19 vaccines to the state’s school immunization schedule.
The joint lawsuit was filed in December 2021, by Louisiana Attorney General Jeff Landry and state Rep. Raymond Crews against Gov. John Bel Edwards after he announced COVID-19 vaccines would be mandatory for all children age 5 and over at public or private schools.
• Los Angeles: Los Angeles Unified School District (LAUSD) Superintendent Alberto Carvalho on April 28 recommended the district postpone its COVID-19 student vaccination mandate until at least July 2023 because the FDA had not fully approved the COVID-19 vaccine for all ages covering grades 7 through 12.
LAUSD officials announced last fall students 12 and older would be required to be vaccinated by the start of the 2022-2023 school year but delayed the mandate because tens of thousands of students still had not complied with the requirement.
• Washington: The Washington State Board of Health in April voted unanimously against adding COVID-19 vaccines to the requirements for students to attend K-12 schools this fall after its advisory group recommended against the requirement. The board said more data was needed about vaccines for ages 5 to 11 and raised concerns that the Pfizer-BioNTech vaccine has yet to be fully approved for ages 5 to 15.
Megan Redshaw is a staff attorney for Children’s Health Defense and a reporter for The Defender.
© 2022 Children’s Health Defense, Inc. This work is reproduced and distributed with the permission of Children’s Health Defense, Inc. Want to learn more from Children’s Health Defense? Sign up for free news and updates from Robert F. Kennedy, Jr. and the Children’s Health Defense. Your donation will help to support us in our efforts.
Ugly Covid Lies

By Ron Paul | July 25, 2022
After two years of unprecedented government tyranny in the name of fighting a virus, the prime instigators of this infamy are walking free, writing books, and openly pretending they never said the things they clearly said over and over.
Take Trump’s White House Covid response coordinator Deborah Birx, for example. She was, as the Brownstone Institute’s Jeffrey Tucker points out in a recent article, the principal architect of the disastrous “lockdown” policy that destroyed more lives than Covid itself. Birx knew that locking a country down in response to a virus was a radical move that would never be endorsed. So, as she admits in her new book, she lied about it.
She sold the White House on the out-of-thin-air “fifteen days to slow the spread” all the while knowing there was no evidence it would do any such thing. As she wrote in her new book, Silent Invasion, “I didn’t have the numbers in front of me yet to make the case for extending it longer, but I had two weeks to get them.”
She was playing for time with no evidence. As it turns out, she was also destroying the lives of millions of Americans. The hysteria she created led to countless businesses destroyed, countless suicides, major depressions, drug and alcohol addictions. It led to countless deaths due to delays in treatment for other diseases. It may turn out to be the most deadly mistake [?] in medical history.
As she revealed in her book, she actually wanted to isolate every single person in the United States! Writing about how many people would be allowed to gather, she said: “If I pushed for zero (which was actually what I wanted and what was required), this would have been interpreted as a ‘lockdown’—the perception we were all working so hard to avoid.”
She wanted to prevent even two people from meeting. How is it possible that someone like this came to gain so much power over our lives? One virus and we suddenly become Communist China?
Last week in a Fox News interview she again revealed the extent of her treachery. After months of relentlessly demanding that all Americans get the Covid shots, she revealed that the “vaccines” were not vaccines at all!
“I knew these vaccines were not going to protect against infection,” she told Fox. “And I think we overplayed the vaccines. And it made people then worry that it’s not going to protect against severe disease and hospitalization.”
So when did she know this? Did she know it when she told ABC in late 2020 that “this is one of the most highly-effective vaccines we have in our infectious disease arsenal. And so that’s why I’m very enthusiastic about the vaccine”?
If she knew all along that the “vaccines” were not vaccines, why didn’t she tell us? Because, as she admits in her book, she believes it’s just fine to lie to people in order to get them to do what she wants.
She admits that she employed “subterfuge” against her boss – President Donald Trump – to implement Covid policies he opposed. So it should be no surprise that she lied to the American people about the efficacy of the Covid shots.
The big question now, after what appears to be a tsunami of vaccine-related injuries, will anyone be forced to pay for the lies and subterfuge? Will anyone be held to account for the lives lost for the arrogance of the Birxes and Faucis of the world?
Copyright © 2022 by RonPaul Institute.
Children Don’t Need COVID Vaccines, Canadian and Australian Groups Tell Public Health Officials
By Julie Comber, Ph.D. | The Defender | July 25, 2022
Groups in Canada and Australia are urging public health officials to reconsider rolling out COVID-19 vaccines for young children, following the authorization earlier this month in both countries of Moderna’s COVID-19 vaccine for children ages 6 months to 5 years.
The Australian Vaccine-risks Network (AVN) on July 19 sent an open letter to Dr. Brendan Murphy, secretary of Australia’s Department of Health and Aged Care, voting members of the Australian Technical Advisory Group on Immunisation and members of parliament threatening to “move forward with preparations for seeking the intervention of the Federal Court of Australia” if officials don’t respond.
The Canadian COVID Care Alliance (CCCA) on July 14 published an open letter to Canadian health officials stating their members would “be happy to meet you to discuss findings documented in this letter in greater detail.”
Both letters emphasized three arguments against authorizing the mRNA shots in young children and babies:
- Children don’t need COVID-19 vaccination because they are at extremely low risk of COVID-19.
- In any case, the mRNA shots don’t work well.
- The potential harm from the mRNA shots outweighs the benefits for young children.
Both letters also referenced the June 30 open letter to U.K. health officials from more than 70 physicians and scientists warning against vaccinating younger children against COVID-19.
The U.K. letter, written in response to the U.S. Food and Drug Administration’s (FDA) Emergency Use Authorization (EUA) in mid-June of the Moderna and the Pfizer-BioNTech COVID-19 shots for children as young as 6 months, urged U.K. health officials to not “make the same mistake” the FDA made.
All three letters referenced Søren Brostrøm, director of the Danish Health and Medicines Authority, who in June said, “We did not get much out of having children vaccinated against coronavirus last year.”
Australia’s Therapeutic Goods Administration on July 18 provisionally approved a pediatric dose of Moderna’s Spikevax COVID-19 shot for children ages 6 months to 5 years old. Rollout of the vaccines is contingent on input from the Australian Technical Advisory Group on Immunisation.
A few days earlier, on July 14, Health Canada authorized the use of Spikevax for children 6 months to 5 years of age. According to the statement, “As a result of this authorization, approximately 1.7 million children are now eligible for vaccination against COVID-19.”
Risks ‘far outweigh’ benefits for children
The 11-page CCCA letter contains 117 references and six pages of figures and graphs to support the group’s argument that “the data shows that, in the Omicron era, when population-based immunity is widespread, the risks associated with COVID-19 mRNA vaccines far outweigh the benefits in children.”
The authors of the CCCA letter criticized the FDA, stating, “no gold standard, placebo-controlled disease endpoint trials, large enough [with at least 800,000 participants] to categorically establish the clinical safety and long-term efficacy of the Pfizer COVID-19 mRNA vaccinations in children 12- to 15-years-old, 5- to 11-years-old, 2- to 4-years-old, and 6-months-old to 23-months-old have been undertaken.”
Instead, the EUA for Pfizer was “based on the preliminary results of four very small immuno-bridging trials, enrolling fewer than 3,000 participants each.”
The CCCA letter presented data from the Canadian province of Ontario, which “reported a negative dose-response effect for the COVID-19 vaccinations [original emphasis].”
The letter continued:
“In other words, the proportion of cases of COVID-19 were highest among those who had been ‘boosted,’ lower among the ‘fully inoculated’ and least among the ‘not fully inoculated’ (which includes the ‘uninoculated’).”
The authors presented graphs from the Public Health Ontario website, noting a similar pattern was observed in the 12- to 17-year-olds and the 5- to 11-year-old age groups.
“Additionally, a greater proportion of ‘boosted’ Ontarians have died, revealing that the vaccinations may be associated with serious secondary effects.”
The CCCA letter concludes:
“We trust that our research has provided you with evidence needed to adjust Canadian health policy to protect our children from undue harm. We would be happy to meet you to discuss findings documented in this letter in greater detail.”
‘Huge gap’ in Pfizer’s vaccine trial documentation
According to the authors of the AVN letter, the Pfizer documentation presented to the FDA had huge gaps in the evidence provided.
For example, the letter stated:
“The protocol was changed mid-trial. The original two-dose schedule exhibited poor immunogenicity with efficacy far below the required standard. A third dose was added by which time many of the original placebo recipients had been vaccinated.”
The AVN letter argued the Moderna shot for young children fails to meet Australia’s regulatory requirements to be granted “provisional determination” (similar to EUA in the U.S.) under regulation 10L(1)(a) of the Therapeutic Goods Regulations.
To receive provisional determination, there must be “an indication of the medicine is the treatment, prevention or diagnosis of a life-threatening or seriously debilitating condition,” the letter stated.
The authors said Australia’s health department and TGA did not “show any data or science to support a conclusion that COVID-19, and particularly the Omicron variant now widespread across Australia, is ‘life-threatening’ to infants aged 6 months up through 4 years, nor indeed that infants 6 months up through 4 years suffer ‘seriously debilitating’ symptoms when infected with COVID-19.”
The authors also addressed the issue of manipulative strategies used to promote COVID-19 vaccination of children, and said pushing unnecessary and novel mRNA-based vaccines onto young children risks undermining parental confidence in routine immunization programs.
Julie Comber is a freelance science reporter for The Defender.
© 2022 Children’s Health Defense, Inc. This work is reproduced and distributed with the permission of Children’s Health Defense, Inc. Want to learn more from Children’s Health Defense? Sign up for free news and updates from Robert F. Kennedy, Jr. and the Children’s Health Defense. Your donation will help to support us in our efforts.
Wrong, Legacy Media, Climate Change Is Not Causing Summer Heatwaves in the U.S. and Europe

By Anthony Watts | ClimateRealism | July 22, 2022
This past week, both the U.S. and Europe have had significant localized heatwaves. The one in Europe is particularly bothersome for the media, since the area is not prepared for temperatures that exceed 100°F like areas in the in the United States in places like California, Texas, and Oklahoma, where air conditioners are the norm, regularly experience. The mainstream media has uniformly blamed the heatwaves on human caused climate change. This attribution is wrong.
The headlines have been truly apoplectic, and absolutely wrong. For example:
With Record-Breaking Heat, Europe Glimpses Its Climate Future [Scientific American]
Climate change is killing people’: Europe’s extreme heatwave continues [EuroNews]
‘Climate change affects everyone’: Europe battles wildfires in intense heat [Reuters]
And in the United States, the media hype is just as wild and just as false:
Record-breaking heat waves in US and Europe prove climate change is already here, experts say [Yahoo News]
The climate crisis is driving heat waves and wildfires. Here’s how [CNN]
How the heat dome in Texas is related to climate change [Yahoo News]
Every summer in the Northern Hemisphere, it gets hot; that’s what summers do. Also, every year, a localized heatwave occurs somewhere in the world.
The error that is common to all of these news articles is the fact that weather is not climate.
Weather is an event that might last for minutes to a few days. A heatwave is a weather event that is typically linked to large scale weather patterns, such as a high-pressure cell which can create heat-domes in the summer. Climate is an average of weather over a thirty-year period as defined by the World Meteorological Organization. Note my highlights:
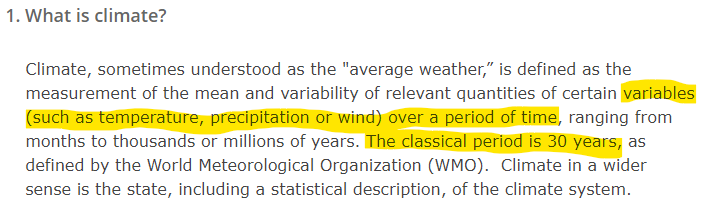
Each of these stories trying to link climate change to the heat wave does so without any proof whatsoever. They are nothing more than speculative fearmongering.
And, it isn’t limited to print and Internet media, the TV stations are overhyping it as well to make it seem like a crisis with the use of color. Figure 1 is a comparison of TV graphics on the British Broadcasting Corporation (BBC) in Summer 2012, versus Summer 2022.
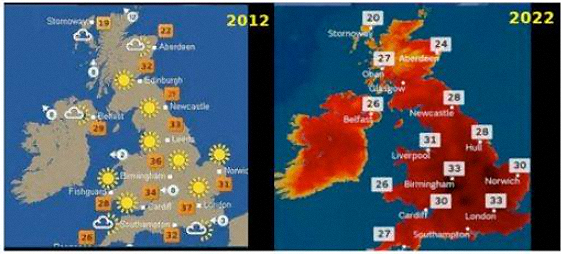
Figure 1: Comparison of TV weather Maps from the BBC in summer 2012, left, and summer 2022 right. Source: BBC
Note that in 2012, some of the temperatures were actually higher, and they didn’t need to fill in areas with red to make it look worse than it actually is.
Another thing that you won’t find reported in the BBC on in the newspapers/Internet media is the fact that while record heat was going on in Western Europe, Eastern Europe was experiencing well below average temperatures. Figure 2 below shows the juxtaposition of heat in the UK and Europe compared to the below normal temperatures in Eastern Europe, which the press has ignored.
Figure 2: Surface Temperature map for UK and Europe on July 19, 2022. Image from ECMWF output via WeatherBell Inc.
That dramatic regional temperature difference seen in Figure 2 is a sure sign of this being a weather pattern, and not global scale climate change aka global warming as the media would have you believe. The same applies to the heat wave in the U.S. as seen in Figure 3. It is regional in its scope, not global.
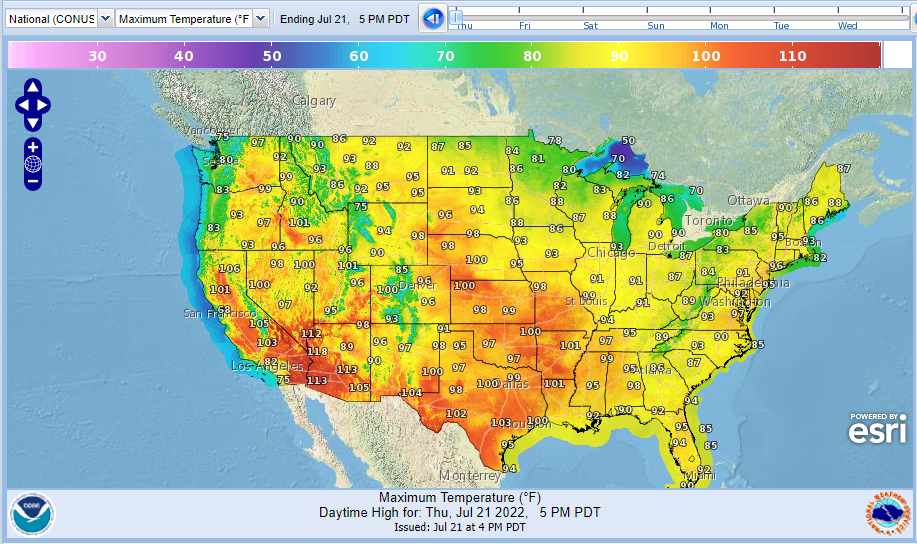
Figure 3: Maximum Temperature for the Contiguous United States July 21, 2022. Source NOAA
As reported in Climate at a Glance: U.S. Heatwaves,
… in recent decades in the United States, heat waves have been far less frequent and severe than they were in the 1930s.
The all-time high temperature records set in most states occurred in the first half of the twentieth century.
The heat wave of 1936 was far deadlier. To their credit, The Washington Post got it right in this report:
The killer U.S. heat wave of 1936 spread as far north as Canada, led to the heat-related deaths of an estimated 5,000 people, sent thermometers to a record 121 degrees Fahrenheit in Steele, N.D., and made that July the warmest month ever recorded in the United States.
But the real issue is that extended high temperatures like the U.S. and Europe have experienced this month have happened before climate change became the universal go-to for blame. It only takes a small amount of research to discover these facts.
A search of the term heatwaves, on Wikipedia, for instance, finds that a heatwave and drought in 1540 in Europe lasted for 11 months, and that a heatwave in 1757 was the hottest in the past 500 years until 2003. Also, Netweather Community TV, called the 1906 heatwave in the U.K during August and September, “one of the most exceptional heatwaves to ever occurred in the UK.” A 1911 heatwave in France contributed to more than 41,000 premature deaths. More recently, in Europe, there was a massive months-long heat wave in 1976. This came at a time when the Earth was experiencing a 30 year cooling trend, that led many scientists to warn the next ice age was looming. Wikipedia’s entry on the 1976 event reports:
The summer of 1976 was considered to be the hottest summer in Europe, and especially the United Kingdom, during the 20th century. A large high-pressure area dominated most of Europe for all of the summer months. The pressure system moved into place in late May 1976 and remained until the first traces of rain were recorded on 27 August.
. . .
For the entire period much of Europe was bathed in continual sunshine with the United Kingdom seeing an average of more than 14 hours of sunshine per day. 1976 was dubbed “the year of the ladybird” in that country due to the rise in the mass numbers of the insect brought on by the long hot period. In the United Kingdom, the summer coincided with a 16-week dry spell, the longest recorded over England and Wales since 1727.
That high pressure pattern is almost identical to what has been seen in UK and Europe today. The difference is that the media today immediately goes to blame climate change rather than weather patterns, and in the case of this article in The New York Times, they even try to convince you that comparisons between the hot summers of 1976 and 2022 are somehow “misleading.”
“Yet the comparison to 1976 is misleading. The highest recorded temperature then was 35.9 degrees Celsius, whereas on Tuesday it surpassed 40 degrees.”
The BBC reported:
“Thermometers hit 40.3C at Coningsby in Lincolnshire, while 33 other locations went past the UK’s previous highest temperature of 38.7C, set in 2019.”
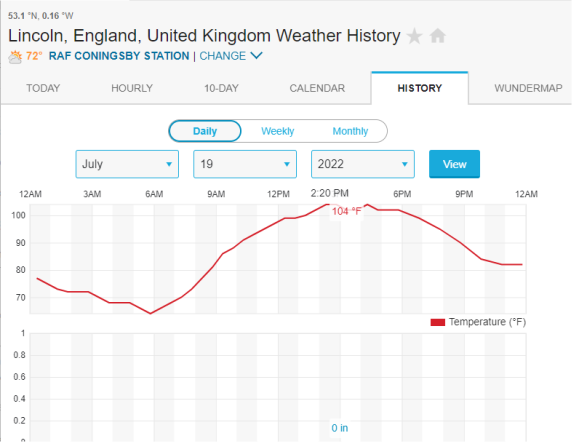
Figure 4. Graph of Temperature at RAF Base Coningsby for July 19th, 2022 showing a max temp of 104°F, Source: WeatherUndergroud.com
What the BBC and the NYT don’t tell you is that the 40 degree Celsius (104 Fahrenheit) was set at a Royal Air Force (RAF) base next to the heat absorbing sea of runway asphalt and tarmac. Figure 4 shows the temperature hour-by-hour that day and where it was recorded.
By contrast, the BBC reports “… the [previous] highest temperature ever recorded in the United Kingdom was 101.7 degrees, observed in Cambridge [at Cambridge University Botanic Garden] in July 2019.“
A botanical garden is an entirely different environment than an RAF air base. The latter would be expected to be much warmer due to the lack of shade, the heat absorbing materials present, and the hot air expelled from jet engines. So, the “misleading” claim of the NYT is really about the lack of solid journalism in reporting the environment under which these temperatures were recorded.
It is well-known that the Urban Heat Island (UHI) effect can contribute to warmer high temperatures, and given the UK went from 56 million people in 1976 to 67 million in 2020, it isn’t the least bit surprising that the UHI increased as infrastructure to support that 11 million extra people was added to that island nation.
The final word comes from meteorologist Cliff Mass, PhD, who did a thorough analysis of the short-lived heatwave event and writes (emphasis his):
The truth and overwhelming scientific evidence provide a different story: the recent European heatwave is mainly the result of natural processes but was enhanced modestly by human-caused global warming.
The situation is very much like the [Pacific] Northwest heatwave of last summer; with many of the same elements.
…
The bottom line is that the recent European heat wave was caused by an amplification of the northern hemisphere wave pattern, with global warming contributing perhaps 5-10% of the warmth. Natural variability of the atmosphere was the proximate cause of the warmth and does not represent an existential threat to the population of Europe.
Clearly, there’s no cause for alarm, no matter what the media says. But the media won’t tell you any of that, because it ruins their narrative of being able to blame the heatwave on climate change, while hoping you don’t notice their distortion of the truth about ordinary weather events we see every summer.
Featured Video

US Middle East Policy: The Growing Propensity for Genocide
or go to
Aletho News Archives – Video-Images
From the Archives
The New Baghdad Pact
By Dr Bouthaina Shaaban | February 23, 2017
A recently declassified CIA document prepared in 1983, and released on 20 January 2017, shows that the United States had at the time encouraged Saddam Hussein to attack Syria, which would have led to a vicious conflict between the two countries, thus draining their resources.
The report, which was then prepared by CIA officer Graham Fuller, indicates that the US tried adamantly to convince Saddam to attack Syria under any pretense available, in order to get the two most powerful countries in the Arab East to destroy each other, turning their attention away from the Arab-Israeli conflict. … continue
Blog Roll
 Aletho News
Aletho News- The Gratitude of the Captured
- Hezbollah denies involvement in deadly attack on UNIFIL in south Lebanon
- The prospect of an expanded and far more violent war
- Canada’s Carney Revives Online Censorship Bill
- Israeli soldiers kill UNICEF truck drivers delivering water to Gaza families
- Iran defends limits on Strait of Hormuz passage
- ‘We warned you’: Hormuz Strait back to pervious state amid US blockade
- Iran rejects uranium transfer, warns of response to naval blockade
- US Middle East Policy: The Growing Propensity for Genocide
- Daniel Davis: Iran Reopens the Strait of Hormuz
- If Americans Knew
- Israel relegates another population to life in tents – Daily Update
- Senate again fails to block weapons to Israel
- Think the Iran war is a disaster? Blame these DC think tanks first.
- Number of Palestinian Prisoners Rises By 83% Since October 2023
- With multiple “ceasefires” in place, Israel keeps on killing in Gaza and Lebanon – Daily Update
- Mearsheimer: Israel Owns Trump
- Mark Levin and Jonathan Pollard Push for Nuking Iran
- TCN: America Enables Israel’s Crimes
- Israel’s Next Leader Will Be Just Like Bibi – but Without the Corruption
- Born into war, raised across borders: The story of Gaza’s premature babies separated from their parents amid Israel’s genocide
- No Tricks Zone
- Reality Check: Maldives Have Actually Grown In Size Or Remained Stable Over Recent Decades
- Abrupt Climate Change Also Occurred NATURALLY In The Past …25 Times During Last Ice Age
- Cave Discovery Reveals Today’s Desert Climates Were Recently Far Warmer, Wetter, Teeming With Life
- German Expert: Heat Dome Led To Record Temps In Western USA…Warmer In 1934, 1936
- New Study: No Linear Warming Or Glacier Retreat Along Northern Antarctic Peninsula Since 1980s
- An Inconvenient Tree: Uncovered In Alps… Europe Much Warmer Than Today 6000 Years Ago
- New Study Reports A 60% Slowdown In Greenland’s Ice Loss Rate In The Last Decade
- Low Intensity Tornado Wrecks Major Solar Farm, Creating A Potential Toxic Dump
- New Study Finds Warming Saves Lives…Cold Temperatures 12 Times More Deadly Than Excess Heat
- German Science Blog Accuses PIK Climate Institute Of Hallucinating Climate Tipping Points
